
The Botswana ExperienceDTG
Ava Avalos, MDTechnical Advisor, Botswana Ministry of Health & Wellness
Research Associate Botswana Harvard PartnershipDirector, Careena Centre for Health

Disclosures
Expert and Advisory Committees:Abbvie, Mylan, Hetero, GSK, ViiV Healthcare
Research Support from:Mylan & ViiV Healthcare

Presentation
• Background on Botswana & its on-going ART treatment optimization
• Review preliminary findings on DTG from the Botswana Epidemiological ART Treatment Cohort Study
• Review future plans to transition patients off older and more toxic regimens to DTG

Botswana has made remarkable progress in HIV treatment and care since 2002 and is close to achieving the UNAIDS 90-90-90 targets:
§ National HIV prevalence: 18.5% (BAIS IV, 2014)
§ National incidence : 0.81% (Revised Spectrum 2018)
§ 0.9% (BCPP Standard of Care)
§ Total HIV Population: 380,000 (31/12/17)
§ ART Coverage: 86.0% (31/12/17)
§ MTCT Rate: 0.4% (2018)
§ AIDS deaths have declined by 67% between 2002-2016§ Cumulative First Line Failure Rate: 13.5% (2002-2017) § Re-treatment patients 8% initiated on DTG (2018)
Botswana’s Achievements Against HIV

Botswana ART Regimens since 20012019 TAF-ED2020 Dual Tx??

BackgroundThe decision to also introduce DTG for women of child-bearing potential included:
1) Appreciating that the Botswana-Harvard Partnership had a strong birth outcome study in place since 2014.
2) Positive outcomes in pregnancy with Raltegravir use since 2010.
3) Previous experience as the first country to use EFV for all women.
4) FDA categorized DTG as B, while still listing EFV as D

Preliminary DTG Outcomes Botswana National ART Program
§ Genotypic resistance testing (GRT) is available for all patients with virologic treatment failure on DTG.
§ With more than 82,200 patients have been initiated on DTG containing regimens (as of 30/6/18). Not one treatment naïve patient has been identified with INSTI mutations.
§ <2% Adverse Side Effects requiring treatment switches
§ Good tolerability with anti-tuberculosis medications regimens at double dosing

The Botswana Epidemiological ART Treatment Cohort Study (The BEAT)
• Botswana is now focused on swiftly addressing programmatic and logistical challenges to ensure ‘Treat All’ implementation success.
• Developing models to reliably verify the initial cost estimates and projected clinical outcomes of the 2016 Investment Case is also a priority.
• Fundamental to these efforts is developing the capacity to closely monitor and analyze clinical data, programmatic costs and epidemiological trends of Treat All and use of Dolutegravir(DTG)

The BEAT Cohort StudyCollaborators:
The Ministry of Health and Wellness (MoHW)Botswana Harvard AIDS Institute Partnership (BHP)
The University of Botswana (UB)Careena Centre for Health (CCH)
Stanford UniversityKRISP – University of KZN
Baylor Pediatric Centre for Excellence (Baylor)UNAIDS
ViiV Healthcare
Sponsor & Coordinating Centre:Botswana Harvard AIDS Institute Partnership

The BEAT Cohort Study
An observational cohort study monitoring the impact of ‘Treat All’ implementation and DTG’s efficacy and clinical outcomes over three years.
1) Treatment Naïve Patients (n=4,700)
2) Switch Patients (n=1000)
3) Highly Treatment Experienced Patients (n=300)

Study Sites4 Districts & 21 Facilities
Gaborone-‐ PMH-‐IDCC -‐ Bontleng Clinic -‐ Phase II Clinic -‐ Tlokweng Clinic-‐ Nkoyaphiri Clinic-‐ Botswana-‐Baylor Children’s Clinical
Centre of Excellence
Molepolole- Moleps IDCC- Phuthadikobo Clinic - Bokaa Clinic - Borakalalo Clinic- MCC Clinic
Mahalaype-‐ Mahalapye Clinic-‐ Airstrip Clinic-‐ Shoshong Clinic-‐ Xhosa Clinic-‐ Kalamare Clinic
Francistown-‐ Nyangabwe IDCC-‐ Area W Clinic-‐ Botswelelo Clinic-‐ Jubilee Clinic-‐ Gerald Estate Clinic

Gaborone - Treatment Naïve Preliminary Results (n=743)
Demographics
Gender: Female (58%)Age – Median [Q1, Q3]
Combined: 35 yrs [18, 71]
Male: 36 yrs [19, 64]
Female: 33 yrs [19,63]
Median Time on DGT: 12 months [2, 19]

The BEAT Gaborone DistrictPreliminary Results
• Chart reviews completed on 1,327 patients on DTG containing regimens:
743 Treatment Naïve (Cohort 1)489 Switches to DTG (Cohort 2)95 Highly Treatment Experienced (Cohort 3)
1,098 (83%) with electronic VL results at 12 months95.9% achieved viral load <400 copies/mL
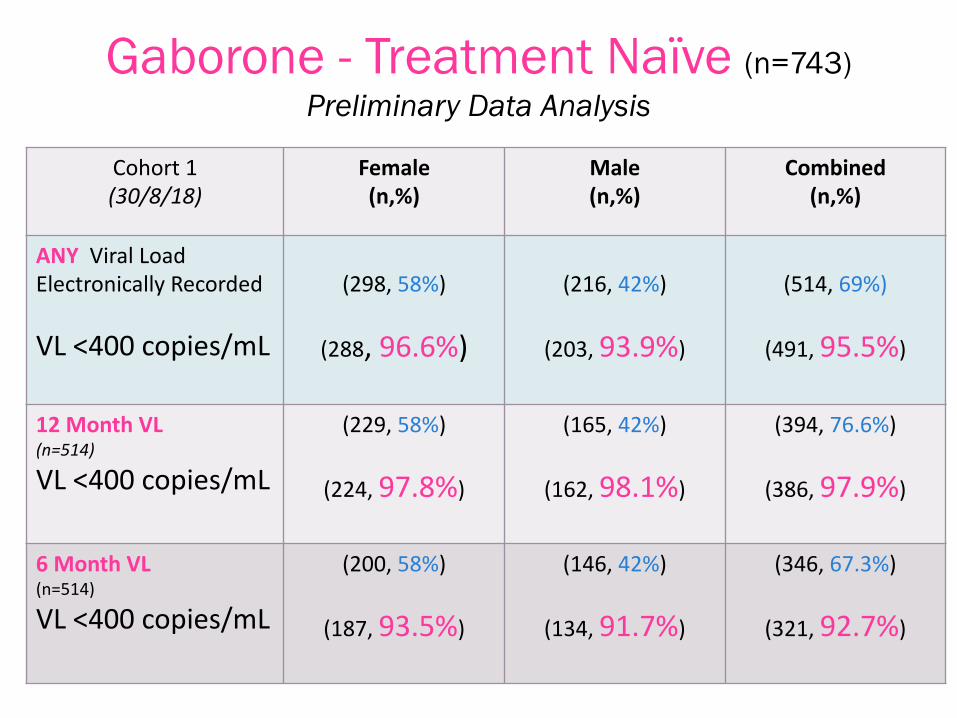
Gaborone - Treatment Naïve (n=743)Preliminary Data Analysis
Cohort 1(30/8/18)
Female(n,%)
Male(n,%)
Combined(n,%)
ANY Viral Load Electronically Recorded
VL <400 copies/mL
(298, 58%)
(288, 96.6%)
(216, 42%)
(203, 93.9%)
(514, 69%)
(491, 95.5%)
12 Month VL(n=514)
VL <400 copies/mL
(229, 58%)
(224, 97.8%)
(165, 42%)
(162, 98.1%)
(394, 76.6%)
(386, 97.9%)
6 Month VL(n=514)
VL <400 copies/mL
(200, 58%)
(187, 93.5%)
(146, 42%)
(134, 91.7%)
(346, 67.3%)
(321, 92.7%)

Molepolole District Preliminary Data
• 709 Chart reviews completed 78.9% (560) with viral load results at 12 months – All Cohorts:
4 (<1%) VL >400 copies/mL6 (1%) LTFU3 (<1%) Deaths (2 TB related, I unknown)
2 (<1%) Toxicity Grade 3
97.6% (548/560)Viral Load <400 copies/mL at 12 months

Adverse Side Effects to DTG
• No pattern has emerged from any recorded side effects requiring treatment switch (Grade 3)– Symptoms have included: rash, GI irritation,
myositis, Itching,
• No deaths related to DTG initiations• Most patients reporting ASE have had
complicated treatment histories • TB related deaths linked to physician error

Switches to DTG Outcomes(Preliminary Data -‐ April 2018)
Reason for Switch #
% VL <400DTG for 6 months
%VL 400DTG for 12 months
GuidelinesSimplification
33 10/11 (90.9%) 20/22 (90.9%)
Toxicities 173 85/87 (97.7%) 85/86 (98.8%)
Tx Failure 135 27/37 (72.9%) 94/98 (95.9%)
Totals 341 122/135(90.3%)
199/206(96.6%)

Toxicities: Reasons for Switches to DTG(Preliminary Data – April)
Main Toxicities Number Percentage
Lipodystrophy(NRTI)
78 45.0%
Diarrhea (LPV/r) 22 12.7%
CNS (EFV) 11 6.35%
Other 62 35.8%
<5% Others include: Gynecomastia (EFV), Skin Discolorations (AZT), Renal Insufficiency (TRU), Liver, neuropathies, GI
TOTAL 173

Highly Treatment Experienced
From the 93 HTE placed on DTG containing regimens:
• 79.5 % (74/93) achieved VL <400 copies/ml.
• 21.5% (20/93) had VL >400 copies/ml
• Only 4 patients were found to have developed INSTI mutations.
• Three of these patients were failing Raltegravir containing regimens at the time of DTG switch.

Patient/Gender
Year starting ART
#ART Regimens
Months on DTG ContainingRegimens
RT Mutations
PRMutations
INSTIMutations
VL as of30/8/18
1/F 2004 5 21 K101E,G190S, M184V
None Q148R <400
2/M 2004 4 32 K103N,V106M
None G118R,E138K
<400
3/M 2002 10 29 K65R, D67N, K70R, M184V,Y181C,K219N
V32I, I47V,I54L, I84V, V32I
T97A, E138K, G140A, S147G, Q148R
4,524
4/M 2004 8 27 A62V,K65R, M98G, M184V
I50V, I54V, A71V, V82M, L90M
A128T, E138K, G140A, Q148K
543

HTE Patients Causes of Treatment Failure/SwitchDocumented Cause of Tx Failure/Switch
# of Patients % of HTE Cohort
Poor Adherence (missed/late doses)
84 88.4%
Resistance (mutations) 53 55.8%
Toxicities/Side Effects
46 48.4%
Defaulting Rx 40 42.1%Other 31 32.6%Major Toxicities/Side Effects: Lipodystrophy, Neuropathy, and GI Effects;; Other: Mental Health, OIs (TB, Cryptococcal Meningitis)Preliminary Data: April 2018

48.4% (46/95) HTE Patients had a documented hx of defaulting.o Average times defaulted: 2.4 times
Documented Defaulting DataHighly Treatment Experienced

The Tsepamo StudyRevisited

• Tsepamo 2-‐year analysis: EFV/TDF/FTC, the first-‐line WHO recommended regimen, is safer than older ART regimens in pregnancy
1. Zash et al. CROI 2017Prior Findings in Tsepamo
10% 12% 18% 21% 20% 23%
29%
36%42%
47% 48%45%
HIV-‐uninfected(N=34,616)
EFV/TDF/FTC (N=2,503)
NVP/TDF/FTC(N=775)
NVP/ZDV/3TC(1,403)
LPV-‐r /TDF/FTC (N=237)
LPV-‐r/ZDV/3TC(N=169)
Zash et al. CROI 2017
Any adversebirth outcome
Severe adverse birth outcome

11% 11%
34% 35%
DTG/TDF/FTC(845)
EFV/TDF/FTC(N=4593)
Any Adverse Birth OutcomeaRR* (95% CI)
1.0 (0.9,1.1) ref
Severe Birth Outcome aRR* (95% CI) 1.0 (0.8,1.2) ref
Total and Severe Adverse Birth Outcomes
*Models adjusted for maternal age, educational attainment and gravida
Any adversebirth outcome
Severe adverse birth outcome

1,3% 1,2% 1,8% 2,2% 1.8%
4,4%
HIV-‐uninfected (N=34,616)
TDF/FTC/EFV(N=2,503)
TDF/FTC/NVP (N=775)
ZDV/3TC/NVP (1,403)
TDF/FTC/LPV-‐r (N=237)
ZDV/3TC/LPV-‐r (N=169)
Neonatal DeathaRR* (95% CI) ref 1.6 (0.8,3.1) 1.9 (1.1,3.3) 1.6 (0.6,4.7) 4.0 (1.8,9.2)
Neonatal Death (<28 days)
*Model adjusted for maternal age, educational attainment and gravida

1.3% 1.3%
DTG/TDF/FTC(845)
EFV/TDF/FTC(N=4593)
Neonatal DeathaRR* (95% CI) 1.0 (0.5,1.9) ref
Neonatal Death <28 days
*Models adjusted for maternal age, educational attainment and gravida

2,1% 2,4% 2,9%
6,1%4.2% 3,6%
HIV-‐unexposed(N=34,616)
TDF/FTC/EFV (N=2,503)
TDF/FTC/NVP (N=775)
ZDV/3TC/NVP (1,403)
TDF/FTC/LPV-‐r (N=237)
ZDV/3TC/LPV-‐r (N=169)
StillbirthaRR* (95% CI) ref 1.2 (0.7,1.9) 2.3 (1.6,3.3) 1.8 (0.9,3.5) 1.6 (0.7,3.5)
Stillbirth
*Model adjusted for maternal age, educational attainment and gravida

2.1% 2.3%
DTG/TDF/FTC(845)
EFV/TDF/FTC(N=4593)
StillbirthaRR* (95% CI) 0.9 (0.6,1.5) ref
Stillbirth
*Models adjusted for maternal age, educational attainment and gravida

Tsepamo UpdateAdditional funding from NICHD to expand sites performing examinations of all births. – On covers 72% of all births in country– Full data set expected to be finalized 3/31/2019– Date review by monitoring committee after each 200
births, will release an update only if significant safety issue
• CDC funding to expand to additional sites using same protocol with the National Programme
• Together, these efforts will cover 94% of births in Botswana.• Expect additional 900-1200 deliveries after DTG exposure
at conception and in early pregnancy

The Neural Tube Defect signal required a closer look and new
considerations……

Improving HIV + Women’s Health
• 60% of HIV positive women of child bearing age are <26 years old
• 80% of women are single at time of delivery• 50% of HIV positive women who became pregnant
did not desire pregnancy• 80-90% of women use condoms as their primary
contraceptive method.• Complications secondary to abortion are now the
number one cause of maternal mortality. in Botswana

DTG Use in WomenImproving Contraceptive Options
Screening women of child bearing potential into those desiring pregnancy and those that do not has provided an opportunity to: • Develop clear and straight forward
algorithms for contraceptives & ART use• More accurately forecast contraceptive
commodities

Improving Contraceptive Options
• Botswana will continue to allow women to decide for themselves whether to use DTG
• Transitioning all women off older and more toxic regimens will begin in January 2019
Reproductive choice and safe guarding HIV positive women pregnancy outcomes - across
all ART regimens – is the goal.

Transition Plans
Phase Phase I Phase II Phase III Phase IVTarget Initiation Date
Nov 2018 over 2 months
December 2018over 6 months
Jun 2019 over 6 months
Dec 2019 over 6 months
Transition Group
Truvada + DTG patients à TLDTAF-‐ED
NVP based regimens à TLD or DTG or TAF-‐ED
LPV/r based regimens àTAF-‐ED
EFV based regimens àTAF-‐ED
Phase I
Phase II
Phase IIIPhase IV
~New Patients on TLD
328,692 333,192347,293
361,693
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
Patients undergoing logistics "transition" of ARVs by Phase
Phase I Phase II Phase III Phase IV ~New Patients on TLD Adult Patients
376,093
• ART Supply chain plan completed• Revised guidelines for ART treatment and
corresponding contraception in process• Sensitization to facilities to begin in
December• Assistance to clinicians via WhatsApp,
SMS, call line.• Viral load reagents supply chain issues to
be improved
Status of Transition

DTG
In the history of developing ART – there has never been a drug developed that has had its patents released as quickly, been developed and distributed by generic companies as swiftly or been made available across most LMICs within such a short time.
There are likely more than 1 million people receiving DTG world-wide.
And while this very encouraging -As with ALL OTHER ART regimens –
its use comes with both challenges and opportunities
DTG

Further NTD Study Outcomes
• No further evidence of an increased risk of infant neural tube defects related to the use of dolutegravir or other integrase inhibitors in early pregnancy has emerged in safety reviews conducted over the past few months, researchers reported at the International Congress on Drug Therapy in HIV Infection (HIV Glasgow) on Monday 29/10/18

Canada• The Canadian Perinatal HIV Surveillance Program reported on
NTD in 2423 infants born to mothers receiving antiretroviral therapy between 2007 and 2017, of whom 2325 were exposed to antiretroviral drugs during the first trimester of pregnancy. A total of 170 were exposed to an integrase inhibitor (80 to dolutegravir, 76 to raltegravir and 28 to elvitegravir). Two neural tube defects were reported, neither in infants exposed to dolutegravir. However, the study did find a threefold higher rate of congenital abnormalities in infants exposed to elvitegravir during the first trimester.

Frankfurt
• The Frankfurt HIV Cohort reported on the outcomes of mothers and infants exposed to integrase inhibitors during pregnancy. Two hundred and seventy-‐eight women in the cohort became pregnant between 2008 and 2018, of whom 52 were exposed to integrase inhibitors (48 to raltegravir, 4 to dolutegravir). No neural tube defects were observed.

Central & Eastern EuropeThe Eastern and Central European Network Group conducted a survey of dolutegravir use in 20 countries in the region, of which seven centres in six countries were able to provide detailed information about dolutegravir exposure. Four hundred and fifteen women took dolutegravir, 28 during pregnancy (24 commenced before conception and 4 after conception). No neural tube defects were reported but the investigators emphasised the importance of gathering data on other risk factors that may affect birth outcomes. In the dolutegravir-‐treated women, only 22 were taking folic acid supplements, four were smoking prior to conception, three were using psychoactive substances and seven were using concomitant medication.

Countries where the use of DTG is patented:
Algeria AzerbaijanBelarus Bosnia & HerzegovinaBrazil ChinaColombia KazakhstanMacedonia MexicoRussia SerbiaTrinidad & TobagoTurkey

Final Thoughts
• Due to its proven efficacy, tolerability and cost effectiveness - even with the possibility of neural tube defects - the benefits of offering the use of DTG in women of child-bearing potential in Botswana far outweigh the risks.
• The NTD signal continues to fade – The Tsepamo Study results will be finalized by March 2019.
• In the meantime, the NTD signal gives the global HIV community a unique opportunity to highlight all cause mortality in birth outcomes, advocate for and fund better ART regimens and effective contraceptive methods and improve pharmcoviligance for ALL ART regimens.

Botswana Ministry of Health & WellnessDepartment of HIV/AIDS Prevention & Care
Botswana-Harvard AIDS InitiativePinkie Melamu
Rebecca Zash & Roger ShapiroBUMMHI
Careena Centre for HealthCDC-PEPFAR – Elliot Raizes
Dannae Brown & Vani VannappagariViiV Healthcare
Heston Phillips, UNAIDSChelsea Morronni. MD
Meghan MurphyUniversity of Botswana
USAIDITPC, Othoman Mellouk
The BEAT Cohort Study TeamAfro-Cab
Many Thanks







