Testing Asbru Guidelines and Protocols
for Neonatal Intensive Care
Christian Fuchsberger,
Jim Hunter and Paul McCue

Acknowledgements
• Clinical collaborators: Christian Popow, Neil McIntosh and Yvonne Freer
• Silvia Miksch
• UK Research Councils – ESRC and EPSRC
• Austrian Research Council

Intensive Care
• Intensive!– Patients with multiple problems– High rate of intervention– Increasing sophistication of available treatments– Increased levels of monitoring
• Errors do happen– Majority are unimportant– Some are significant
• Missed symptoms and signs• Attentional overload

Intensive Care is Expensive
In 2002 • expenditure on health care as % of GDP:
– from: 10.7% (Germany) to 6.7% (Ireland) – say 8% overall
• expenditure on intensive care as % of health care costs:– from 2.6% (Netherlands) to 1% in UK – say 1.5% overall
• European GDP ~ €10,000,000 M• so ~ €12,000 M spent on intensive care• every 1% saved ~ €120 M

Solutions?
• Display the data:
• Not demonstrated to help junior nurses and doctors.
• Decision support …

Clinical Guidelines and Protocols
• Clear statements of the optimal management for a specific group of patients which, when properly applied, will improve the quality of the care they receive.
• Guideline:– often formulated nationally or internationally– often evidence-based– widely disseminated
• Protocol:– more detailed– local (one clinician or group of clinicians)– often mandatory
Computerised Guidelines
• Formal representation of a guideline
• Languages: – Guide, Prodigy, GLIF, SAGE, EON, ProForma, Asbru
• Automatic application to electronic data (EPR)
• Often envisaged as operation in ‘encounters’ with patient– 10’s or 100’s of data items– daily or weekly– possibility of clinician data input

• Data volume– continuous physiological data (heart rate, oxygen, carbon dioxide,
blood pressures) as often as every second – 100,000’s of data items
– sporadic data – lab results, blood gases, …– ‘paperless’ ICU – data input from nurses and doctors
• Complex abstractions– bridge the gap between raw data and guideline– some data not available electronically (sight, touch, …)
• Automatic application– medical staff have no time to answer questions
• Continuous advice provision– system often has access to actions taken by staff
Computerised Guidelinesin Intensive Care
What do we need for development?
• Formal language: Asbru (Shahar, Miksch and Johnson,1998)
• Guideline (protocol)• Translation of guideline• Visualisation of guideline• Data Abstraction• Execution Engine: AsbruRTM• Test Data• Infrastructure• Evaluation
NB: All testing is off-ward
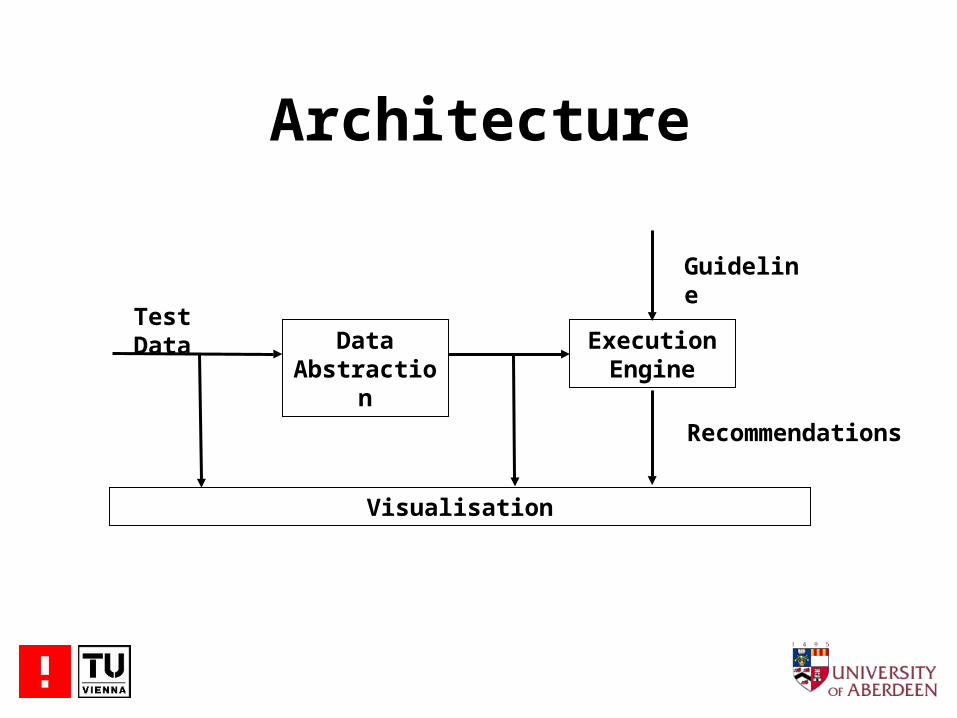
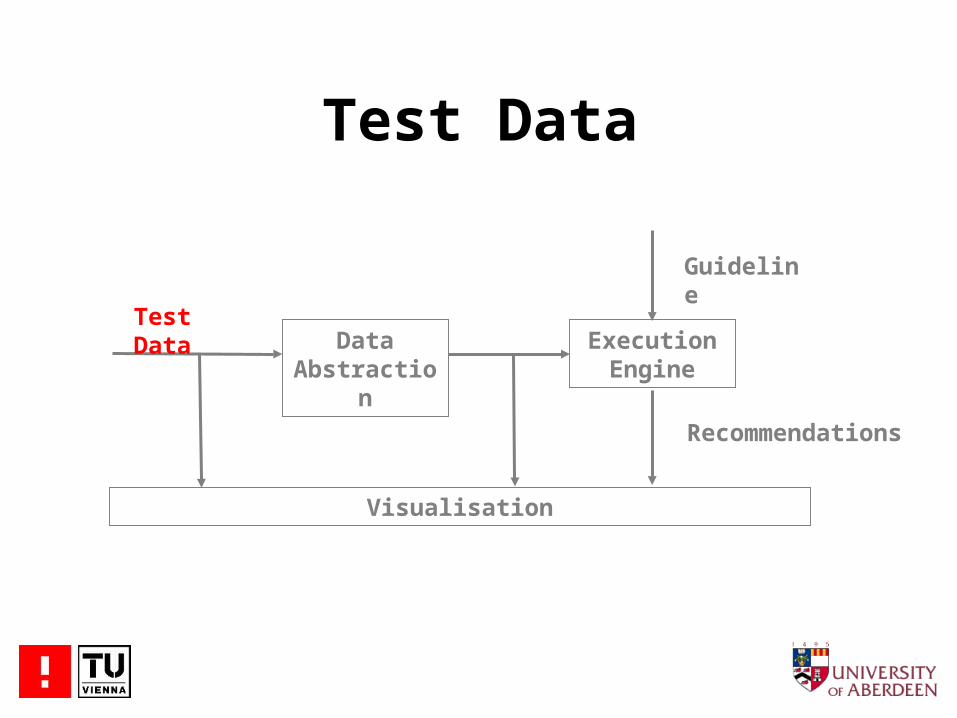
Architecture
Data Abstraction
Execution Engine
Test Data
Visualisation
Guideline
Recommendations

Guideline
Data Abstraction
Execution Engine
Test Data
Visualisation
Guideline
Recommendations

Guideline
• Maintain suitable oxygen (O2) level in the blood (as measured) …
• … by adjusting the fraction of inspired oxygen (FiO2) on the ventilator
IF O2 > O2-High THEN
Rec_FiO2 = FiO2 - 5
IF O2-High> O2 > O2-Low THEN
Rec_FiO2 = FiO2
IF O2-Low > O2 THEN
Rec_FiO2 = FiO2 + 10
O2-High
O2-Low
O2
FiO2 -
FiO2 +
8 kPa
6 kPa

Guideline<!-- ################# PtcO2 too <!-- ################# PtcO2 too high--><if-then-else> <simple-condition> <comparison type="greater-than"> <left-hand-side> <parameter-ref name="PtcO2"/> </left-hand-side> <right-hand-side> <numerical-constant value="8"/> </right-hand-side> </comparison> </simple-condition> <then-branch> <variable-assignment variable="REC_SETTING:VENTILATOR:Rec_FiO2"> <operation operator="subtract"> <parameter-ref name="VENTILATOR:FiO2"/> <numerical-constant value="5"/> </operation> </variable-assignment> </then-branch></if-then-else>
Coded by hand
IF O2 > O2-High THEN Rec_FiO2 = FiO2 - 5

Guideline
• Also simple guideline to maintain suitable oxygen
(CO2) level in the blood (as measured) …
• … by adjusting respiration rate on the ventilator
Test Data
Data Abstraction
Execution Engine
Test Data
Visualisation
Guideline
Recommendations

Test Data
• Taken from the ‘Neonate’ database(Hunter, Ferguson, Freer, Ewing, Logie, McCue and McIntosh, 2003)
• Continuous monitoring of physiological variables– 1 second; heart rate, blood pressure, O2, CO2 …
• Discontinuous numerical data– Ventilator settings, blood gas, laboratory results
• Discontinuous symbolic data– Observations of physical state– Actions taken by the staff
‘Neonate’ Database
• 407 hours• 31 individual babies• Background information
– sex, gestation, weight at birth, …• Anonymised• Microsoft Access• Available

Discontinuous Data
Individual records
Actions 19,610
Observations 1,831
Settings 4,512
Laboratory results 1,343
Blood gas 2,187
Medication 148
Comments 2,443
Observer present 403
TOTAL 32,477

Subset Used
• measured O2 (OX) sampled 1/second
• measured CO2 (CO) sampled 1/second
• FiO2 setting when changed
• respiration rate when changed
• actions taken

Data Abstraction
Data Abstraction
Execution Engine
Test Data
Visualisation
Guideline
Recommendations
Data Abstraction
• Compression – median value every 60 seconds• Artefact removal (Cao et al., 1999)
– limit-based detector flags as artefact values outside extreme centiles
– deviation-based detector flags as artefact values which cause the standard deviation to exceed a limit
– correlation-based detector: uses lower standard deviation limits when a ‘correlated’ channel is flagged

Execution Engine
Data Abstraction
Execution Engine
Test Data
Visualisation
Guideline
Recommendations
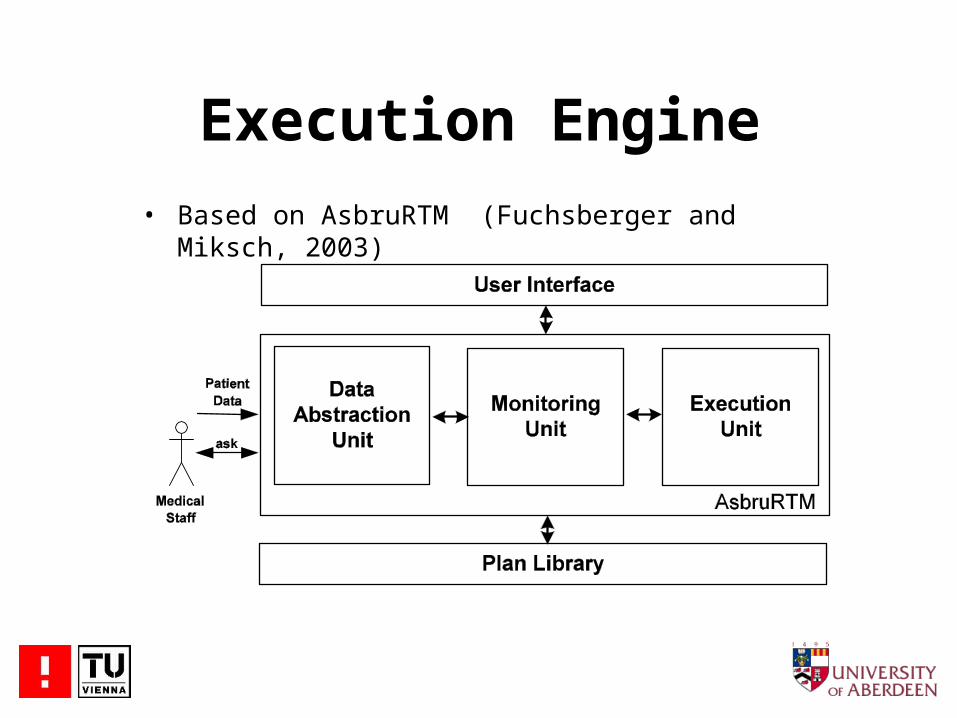
Execution Engine
• Based on AsbruRTM (Fuchsberger and Miksch, 2003)

Execution Engine
CORBA
Simplified and data abstraction done externally

Detailed Architecture
Rec_Resp_Rate
MD[OX]+CMD[OX]OX
CO
Median
Median
ArtiDetector AsbruRTM
MD[CO]
Rec_FiO2
FiO2
Resp_Rate
Guideline
MD[CO]+C
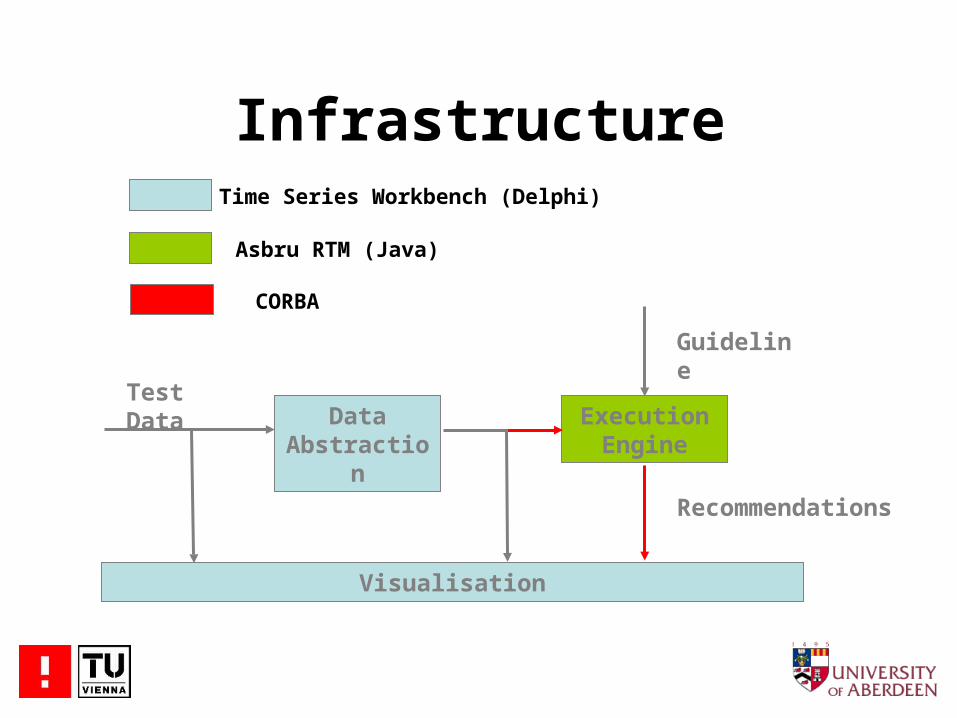
Infrastructure
Data Abstraction
Execution Engine
Test Data
Visualisation
Guideline
Recommendations
Time Series Workbench (Delphi)
Asbru RTM (Java)
CORBA

Results

Where now?
• Can we derive abstractions for more complex guidelines which may refer to data which is not available electronically?
• How do we deliver advice in a ‘continuous’ environment when the guideline can “see” what the clinical staff are doing?
• How do we integrate the work of different groups?

Distributed Infrastructure
Clients
Test Data
Filters(Data Abstraction)
Guidelines
Servers
Plots
Execution Engines
Guideline Visualisation
Data and Recommendation
VisualisationTest
Management
Internet








