
APPROVED:
Darrell Hull, Major Professor Mariam Boesch, Committee Member Becky Glover, Committee Member Mai Chang, Committee Member Abbas Tashakkori, Chair of the Department of
Educational Psychology Jerry R. Thomas, Dean of the College of
Education Mark Wardell, Dean of the Toulouse Graduate
School
SPATIAL ABILITY IN REGISTERED NURSES
Janet E. Gardner, RN, MPH
UNIVERSITY OF NORTH TEXAS
May 2014
Dissertation Prepared for the Degree of
DOCTOR OF PHILOSOPHY

Gardner, Janet E. Spatial ability in registered nurses. Doctor of Philosophy (Educational
Research-Research, Measurement and Statistics), May 2014, 152 pp., 4 tables, 2 figures,
references, 139 titles.
Spatial ability is the skill associated with mental relations among objects, the process of
maintaining the physical aspects of an object after mentally rotating it in space. Many studies
report a strong association of spatial ability with success in various areas of health care,
especially surgery, radiology and dentistry. To date, similar investigations in professional
nursing could not be located.
Registered nurses, employed in an acute care multi-hospital setting, were surveyed using
the Shipley-2Block Pattern Test, the Group Embedded Figures Test, and a newly created test of
general nursing knowledge. The sample size of 123 nurses was composed of 31 male nurses and
92 female nurses. Data was collected between May and August of 2013 and analyzed using R,
version 2.15.2.
The present study did not demonstrate a statistically significant effect for gender
differences on two measures of spatial ability. However, Cohen’s d effect sizes for mean gender
differences in the present study are consistent with prior studies. This may suggest the nursing
profession is comparable with other professions where males perform higher than females on
spatial ability. The present study should be considered an initial step toward evaluating the
relevance of spatial ability in the performance of nursing care.

Copyright 2014
by
Janet E. Gardner
ii

iii
ACKNOWLEDGEMENTS
Thank you to my dissertation committee (Dr. Darrell Hull, Dr. Mariam Boesch, Dr.
Becky Glover, and Dr. Mai Chang). Your guidance, encouragement, and expertise were
wonderful. I respect you and truly appreciate all of you.
To my family – there are not enough words to describe my love and appreciation. To
Mom and Dad (Dr. Fred and Margaret Gardner) – you were always inspiring and supportive –
through the entire process. You believed in me and allowed me to believe in myself. Growing
up a “Gardner” has provided so many blessings – determinism, strength, faith, and above all,
unconditional love. I was raised with love, support, faith, and an overwhelming amount of
stubbornness. I am the person today because of you. Thank you. As I’ve said before – I am
proud to be a Gardner. Mom – I miss you. However, I knew you were winking at me
throughout this journey. I feel your strength.
To my siblings (Kristen, Nancy, David, Paul, and Mark) – what a journey! It has been
long and challenging – fun most of the time – I cannot imagine sharing the experience with
anyone else. Thanks for hanging in there with me.
To my children: Benjamin and Matthew. You are a constant source of strength and
inspiration. I love you so much. May this journey be the beginning of many more in our family.

iv
TABLE OF CONTENTS
Page
ACKNOWLEDGEMENTS ........................................................................................................... iii LIST OF TABLES ......................................................................................................................... vi LIST OF FIGURES ...................................................................................................................... vii SPATIAL ABILITY IN REGISTERED NURSES ........................................................................ 1
Abstract ............................................................................................................................... 1
Aim ......................................................................................................................... 1
Background ............................................................................................................. 1
Design ..................................................................................................................... 1
Methods................................................................................................................... 1
Findings................................................................................................................... 2
Conclusion .............................................................................................................. 2
Summary Statement ................................................................................................ 2
Introduction ......................................................................................................................... 3
Changes in Nursing ................................................................................................. 5
Spatial Ability ....................................................................................................... 10
The Study .......................................................................................................................... 13
Aim ....................................................................................................................... 13
Design ................................................................................................................... 13
Sample/Participants............................................................................................... 13
Data Collection ..................................................................................................... 14
Data Analysis ........................................................................................................ 18
Reliability .............................................................................................................. 19
Results ............................................................................................................................... 19
Discussion ......................................................................................................................... 23
Gender Differences in Spatial Ability................................................................... 24
Years of Nursing and Spatial Ability .................................................................... 24
Professional Nursing Certifications Predict General Nursing Knowledge ........... 25
Significance........................................................................................................... 26
Limitations ............................................................................................................ 26

v
Conclusions ....................................................................................................................... 27
References ......................................................................................................................... 27 ADVANCED EDUCATION AND CERTIFICATIONS FOR NURSING – DO THEY MAKE A DIFFERENCE?............................................................................................................................. 36
Introduction ....................................................................................................................... 36
Professional Nursing ............................................................................................. 36
Magnet Recognition Program ............................................................................... 38
Nursing Education ................................................................................................ 40
Certifications ......................................................................................................... 42
Challenges for Nursing ......................................................................................... 43
Spatial Ability ....................................................................................................... 50
The Study .......................................................................................................................... 56
Aim ....................................................................................................................... 56
Design ................................................................................................................... 57
Participants ............................................................................................................ 57
Data Collection ..................................................................................................... 58
Data Analysis ........................................................................................................ 63
Reliability .............................................................................................................. 63
Results ............................................................................................................................... 64
Discussion ......................................................................................................................... 66
Predictors of General Nursing Knowledge ........................................................... 66
Significance........................................................................................................... 67
Limitations ............................................................................................................ 68
Conclusions ....................................................................................................................... 68
References ......................................................................................................................... 68 APPENDIX A. NURSING KNOWLEDGE ASSESSMENT ...................................................... 78 APPENDIX B. DEMOGRAPHIC AND WORK HISTORY QUESTIONNAIRE ..................... 88 APPENDIX C. COMPLETE UNABRIDGED RESULTS .......................................................... 92 APPENDIX D. EXTENDED LITERATURE REVIEW ........................................................... 126
COMPREHENSIVE REFERENCES ......................................................................................... 142

vi
LIST OF TABLES
Page
Table 1 Descriptive Statistics...................................................................................................... 20
Table 2 Summary of Regression Models with Effects Predicting Shipley 2 Block Pattern Test and Group Embedded Figures Test (N = 122) ............................................................................. 22
Table 3 Summary of Regression Models with Effects Predicting General Nursing Knowledge (N = 117) ........................................................................................................................................... 23
Table 4 Descriptive Statistics...................................................................................................... 64
Table 5 Summary of Regression Model with Effects Predicting Professional Certification (N = 116) ............................................................................................................................................... 65
Table 6 Summary of Regression Model with Effects Predicting Education (N = 116) .............. 65

vii
LIST OF FIGURES
Page
Figure 1. Schematic representation and comparisons of Carroll's three-stratum, Cattell–Horn's extended Gf–Gc, and the integrated Cattell–Horn–Carroll models of human cognitive abilities. (McGrew, 2009). ........................................................................................................................... 11
Figure 2. Schematic representation and comparisons of Carroll's three-stratum, Cattell–Horn's extended Gf–Gc, and the integrated Cattell–Horn–Carroll models of human cognitive abilities. (McGrew, 2009). ........................................................................................................................... 53

1
SPATIAL ABILITY IN REGISTERED NURSES
Abstract
Aim
To examine individual differences in spatial ability among professional registered nurses.
Background
Spatial ability is the skill associated with mental relations among objects, the process of
maintaining the physical aspects of an object after mentally rotating it in space. Many studies
report a strong association of spatial ability with success in various areas of health care,
especially surgery, radiology and dentistry. To date, similar investigations in professional
nursing could not be located.
Design
Cross-sectional.
Methods
Registered nurses, employed in an acute care multi-hospital setting, were surveyed using
the Shipley-2Block Pattern Test, the Group Embedded Figures Test, and a newly created test of
general nursing knowledge. The sample size of 123 nurses was composed of 31 male nurses and
92 female nurses. Data was collected between May and August of 2013 and analyzed using R,
version 2.15.2.

2
Findings
The present study did not demonstrate a statistically significant effect for gender
differences on two measures of spatial ability. However, Cohen’s d effect sizes for mean gender
differences in the present study are consistent with prior studies. This may suggest the nursing
profession is comparable with other professions where males perform higher than females on
spatial ability.
Conclusion
The present study should be considered an initial step toward evaluating the relevance of
spatial ability in the performance of nursing care.
Summary Statement
Why is this research needed?
With continual changes in health care, evaluating nurses for general knowledge, skills,
and traits may enhance our understanding of the nursing profession and the skills or abilities
possessed by successful nursing practitioners.
What are the key findings?
• Sex is a predictor of spatial ability, in favor of males.
• Professional specialty certification is a predictor for general nursing knowledge.
How should the findings be used to influence policy/practice/research/education?
• Additional research will be needed to evaluate the importance of spatial ability within

3
nursing, specifically the possibility of spatial ability assessments as a screening tool for
enrollment to nursing school.
• The present study provides an adapted general nursing knowledge assessment that is
both brief and exhibits good reliability.
Keywords: nursing, spatial ability, individual differences, nurse knowledge, nursing
students, gender, education
Introduction
Medicine, healthcare and nursing are rooted in scientific findings and practices. Barrett
(2002) defines nursing as a basic science and describes the practice of nursing as the scientific art
of applying knowledge of humans in combination with their environment for their well-being.
Nursing informatics, a nursing specialty approved in 1992 by the American Nurses Association,
is using information and technology to advance the field of nursing, bridging the gap from the art
of nursing to the science of nursing (Bond, 2009; Saba, 2001).
For more than 50 years, a link between those successful in science and spatial ability has
been consistently demonstrated (Wai, Lubinski & Benbow, 2009). Spatial ability is described by
Voyer, Voyer, and Bryden (1995) as a collection of different skills or abilities instead of a
unitary construct. The construct of spatial ability is often divided into sub-factors depending on
the emphasis given to a specific aspect of mental process on visualizing images (Maedo & Yoon,
2013; Pittalis & Christou, 2010). Researchers often differ on the number of dimensions for
spatial ability but most agree with the inclusion of spatial visualization (Maedo & Yoon, 2013).
Spatial visualization, often referred to as visual spatial processing, involves the spatial
transformation of objects, the ability to mentally rotate a two-dimensional or three-dimensional

4
object rapidly and accurately, while maintaining the characteristics of the object (Maeda &
Yoon, 2013). Mental rotation testing, commonly used as an assessment tool for spatial ability, is
known to be highly sensitive for gender differences in favor of males (Debelak, Gittler, &
Arendasy, 2014; Nazareth, Herrara, & Pruden, 2013; Voyer, Voyer, & Bryden, 1995).
Spatial ability, specifically mental rotation, is associated with success in the learning of
anatomy and physiology, as well as basic courses in medical training (Hegarty, Keehner,
Khooshabeh, & Montello, 2009; Hoyek et al., 2009; Langlois et al., 2009; Stransky, Wilcox, &
Dubrowski, 2010; Stull, Hegarty, & Mayer, 2009). For complex surgeries, visual spatial ability
has been related to competency and quality of results (Wanzel, Hamstra, Anastakis, Matsumoto,
& Cusimano, 2002). The ability to mentally rotate an object in 3 dimensions, visualizing
structures from several viewpoints with three dimensional images, carries significant importance
in surgeons learning spatially complex surgical technical skills, echoing other studies where
surgical skills are strongly dependent on spatial skills (Brandt & Davies, 2006; Stransky et al.,
2010). Health care studies for spatial ability have been published on surgeons, radiologists, and
dentists; however, nurses are lacking in published studies (Hegarty et al., 2009).
Although most nurses are not familiar with the term spatial ability, activities associated
with spatial ability are part of everyday activities as a registered nurse. When auscultating heart
sounds a nurse mentally visualizes the anatomy of the heart to evaluate adverse sounds. Nurses
mentally visualize the features of the trachea, larynx and esophagus while inserting a nasogastric
tube for successful placement as it is a blind insertion. PICC (peripherally inserted central
catheter) lines and peripheral intravenous lines are activities that also require mental
visualization for placement as they are essentially blind insertions. These are but a few examples
of spatial ability in nursing. Making use of simulated mental imagery to solve problems is the

5
basis of visual processing, Gv (McGrew, 2013). As spatial visualization is a common construct
for spatial ability, the present study focuses on visual processing for assessing registered nurses
for spatial ability.
Changes in Nursing
Role Changes
Over the past 50 years, changes in nursing such as job demands, technology, work
environments, patient acuity, litigation, salaries, education, and uniforms have dramatically
impacted the role of the professional nurse (Blanche, 2010). Nurses monitor complex
physiological data, operate lifesaving equipment, administer high cost health care programs and
coordinate the delivery of multiple patient services (Weld & Bibb, 2009).
Changes in Job Skills
Nurses must use critical thinking skills with assessment, interpretation, and decision
making to provide patient care, ensuring patient safety at all times. Clinical knowledge is
estimated to double every 18 months (van Terheyden, 2007). Medical practices,
pharmaceuticals, regulations and standards of care require constant assimilation of new
information. As health care technology advances and patients require higher levels of care,
nurses must incorporate new practices and workflows to meet the changes (Kalisch & Begeny,
2010). Integrating technology to improve clinical nursing practice enhances patient care quality;
therefore, today’s nurse must utilize technology to support their workflow as well as support
their patient’s use of increased technology (Bond, 2009; Saba, 2001). Creation of EHRs
(electronic health record) using CPOE (computerized physician order entry) and interfacing of

6
various electronic applications has created a complex and dynamic work environment for nurses
(Institute of Medicine [IOM], 2010). Expansion of biometric devices such as automated insulin
pumps and implantable cardiac defibrillators require nurses to continually expand the use of
technology in patient care.
The practice of nursing care is discipline specific, but also requires multidisciplinary
knowledge in such areas as respiratory therapy, pharmacy, rehabilitation, and surgery (Giuliano,
Tyer-Viola, & Lopez, 2005). Nurses must be proactive problem solvers and collaborative
interdisciplinary team members (Hodges, 2011). Foundational science and math knowledge in
areas such as anatomy and physiology, pharmacology and human behavior are necessary for
nurses in today’s workplace. The nurse is the last safety check in the chain of events from
prescription to medication administration, before reaching the patient (Leufer & Cleary-
Holdforth, 2013). Nurses must use basic math functions and algebraic equations to calculate
doses of medications (Maag, 2004). Research has shown spatial visualization abilities to be
positively related with performance on math tasks, as well as tasks in science, technology, and
engineering (Hinze et al., 2013).
Advances in Medical Care
Many advances in medical care have resulted in greater numbers of hospitalized patients,
more critically ill patients upon admission to hospitals, and aging patients as well as improved
survival from critical events (Kuehn, 2007; Lynn & Redman, 2005). Increased patient acuity
levels with shortened lengths of hospital stays create intensive and accelerated health care
processes (Hirschkorn, West, Hill, Cleary, & Hewlett, 2010). Nurses complete an average of
100 tasks per shift, with an interruption every 3 minutes, often resulting in cognitive overload

7
(Hendren, 2011). All of these improvements and changes rely on tremendous knowledge and a
skill set that allows the nursing professional to deliver optimal care demanded in such situations.
Gender Participation in Nursing
The current nursing workforce contains a disproportionate number of females. While
most disciplines within the health professional workforce have become more gender balanced,
the same has not been true for nursing. The number of men who become nurses has grown in the
last two decades however men account for only 7% of the current RN workforce (US
Department of Health and Human Services, 2010). Stereotypes, role support, and academic
acceptance are some challenges men encounter when entering the nursing profession (IOM,
2011). Moreover, there is little recognition of unique skills or abilities of males as nurses, and
the turnover rate for male nurses is twice that of females (Hsu, Chen, Yu, & Lou, 2010). While
more men are being drawn to nursing, especially as a second career, the field of nursing must
continue to recruit men as their unique perspectives and skills are important to the profession and
will help contribute additional diversity to the workforce (IOM, 2011). Given the disparity
between the number of males and females employed as professional nurses, gender differences in
ability are important to determining skill acquisition/possession across the entire field of nursing.
Licensing and Certification
RN licensure indicates entry-level competence to the nursing field where certification
verifies specialty knowledge, skills, experience and clinical judgment (American Association of
Critical-Care Nurses, 2013; American Board of Nursing Specialties, 2005). Certification reflects
self-mastery with an emphasis on self-evaluation (Crist, Russell, & Farber, 2012). Specialty

8
certifications include, at a minimum, a practice component with required knowledge testing
(Briggs, Brown, Kesten, & Heath, 2006; Grief, 2013).
Professional Certification and Patient Outcomes
The connection between certified nurses and quality patient care is well established (Crist
et al., 2012). Specialty nurse certification is increasing in value as more evidence suggests that
certification is a factor in improving patient outcomes (Fleischman, Meyer, & Watson, 2011,
2011; Timmerman, 2008). RNs with a BSN degree and a specialty certification are associated
with improved patient outcomes, decreased mortality, and decreased failure to rescue in general
surgical patients (Kendall-Gallagher, Aiken, Sloane, & Cimiotti, 2011).
Competency or Proficiency
There has been little progress in the nursing profession towards the development of a
general tool to evaluate overall nursing knowledge and skills outside of nursing schools (IOM,
2011; Long, Mitchell, Young, & Rickard, 2013). The National Council of State Boards of
Nursing (NCSBN) requires all nurse licensing candidates to pass an examination that measures
the competencies required to perform safe and effective patient care as a newly licensed entry-
level nurse, namely the NCLEX-RN (National Council Licensure Examination for Registered
Nurses), and graduate from an accredited school of nursing (National Council of State Boards of
Nursing, 2013). Upon graduation from an accredited school of nursing and passing the NCLEX-
RN, the student applies for a nursing license allowing the individual to practice nursing within
the state where the requirements were met (Simon, McGinniss, & Krauss, 2013). The HESI
(Health Education Systems, Inc.) Exit Exam, an external independent assessment of a student’s

9
competency at a higher cognition level of application, analysis, and synthesis, is often
administered to senior level nursing students to determine a student’s readiness to take the
NCLEX-RN (Schooley & Kuhn, 2013).
Currently, in most states a nurse is considered proficient or competent upon initial
licensing, with assumed proficiency or competency going forward unless otherwise discovered
(Tilley, 2008). Tilley (2008) describes the confusion associated with competency and
proficiency as related to two different uses of the terms: initial licensure and ongoing
maintenance.
Nursing Shortage
The nursing profession is experiencing a national workforce shortage of critical
proportion (Juraschek, Zhang, Ranganathan & Lin, 2012). This shortage is predicted to worsen,
with an expected national shortage of 300,000 to 1 million RNs in 2020, and continued shortages
throughout the country through 2030 (Juraschek et al.). A report from the U.S. Department of
Health and Human Services (2010) predicted a nursing shortage equating to a 36% shortage.
The aging RN workforce strongly impacts the projected nursing shortage (Juraschek et
al., 2012). Nurses that were 50 years of age or older comprised 25% of the nursing workforce in
1980, 33% of the nursing workforce in 2000, and 45% of the nursing workforce in 2008
(Juraschek et al.; US Department of Health and Human Services, 2010). It is estimated that 55%
of currently employed nurses plan to retire before 2020 (Hirschkorn et al., 2010). Social support
from supervisors and coworkers, job demands, and self-efficacy were reported to be significantly
related to job dissatisfaction, while demands and support from coworkers were related to
intention to leave the profession (Peterson, Hall, O’Brien-Pallas, & Cockerill, 2011). Job

10
dissatisfaction was a strong determinant of turnover among new nursing graduates, with
interpersonal relationships having the strongest impact (Cho, Lee, Mark, & Yun, 2012). The
shortage of nursing educators also has impacted the nursing shortage (Rich & Nugent, 2010). In
2012, U.S. nursing schools declined almost 80,000 qualified applicants for baccalaureate and
graduate nursing programs due to a lack of faculty, clinical sites, clinical preceptors and budget
constraints (AACN, 2014). Higher financial compensation in clinical settings is enticing current
and potential nursing faculty away from the academic setting (AACN).
Spatial Ability
General Cognitive Ability - g
Charles Spearman introduced the first theory of intelligence in 1904, identifying general
mental ability as a trait based on his findings that all mental test scores were positively correlated
(Floyd, McGrew, Barry, Rafael, & Rogers, 2009; Jensen, 1987). General cognitive ability has
been identified as the primary predictor for occupational success in the United States (Kane &
Brand, 2003).
Raymond Cattell suggested human intelligence is comprised of two complementary
intelligence factors--crystallized and fluid intelligence (Horn & Cattell, 1966). John Horn
furthered Cattell’s research in 1965 by adding six broad factors, resulting in the Cattell-Horn Gf-
Gc theory (Kane & Brand, 2003; McGrew, 2009).
Carroll’s research proposed a hierarchical model of intelligence, describing cognitive
abilities in terms of a three-stratum model (Carroll, 1997; Kane & Brand, 2003). Stratum 1 is
composed of a large number of narrow abilities, such as language development, reading, and
spelling. Stratum II consists of 10 broad abilities, such as fluid intelligence, crystallized

11
intelligence, general memory and processing speed (Kane & Brand, 2003). The highest stratum,
Stratum III, consists of only one single factor, g, generalized intelligence (Carroll, 1997).
Cattell-Horn-Carroll Theory
The Cattell Horn Carroll (CHC) theory of intelligence was developed by merging the
Cattell-Horn Gf-Gc model with Carroll’s three-tiered stratum model to form a broader
hierarchical model of g (Floyd, Evans, & McGrew, 2003; McGrew, 2009). General cognitive
ability, g, is the highest level of the hierarchy at Stratum III (Bickley, Keith, & Wolfe, 1995;
Parkin & Beaujean, 2012). Figure 1 provides a visual illustration, comparing Carroll's three-
stratum, Cattell–Horn's extended Gf–Gc, and the integrated Cattell–Horn–Carroll models of
human cognitive abilities (McGrew, 2009).
Figure 1. Schematic representation and comparisons of Carroll's three-stratum, Cattell–Horn's extended Gf–Gc, and the integrated Cattell–Horn–Carroll models of human cognitive abilities. (McGrew, 2009).

12
The present study focuses on the Stratum II broad ability of visual processing, Gv.
Higher Gv ability allows an individual to see more than the object by imagining the object from a
different view after mental rotation, mentally taking a complex item apart and reassembling the
item (Schneider & McGrew, 2013). Lower Gv levels decrease an individual’s ability to perform
mental rotations causing the person to wait until an object is physically rotated to see the change
(Schneider & McGrew, 2013).
Gender Differences in Spatial Ability
Findings supporting gender differences in spatial ability are abundant; and, mental
rotation testing is consistently more sensitive to gender differences than other spatial ability tasks
(Brownlow, McPheron, & Acks, 2003; Ceci & Williams, 2010; Geary, Gilger, & Elliott-Miller,
1990; Geiser, Lehmann, & Eid, 2008; Jansen & Heil, 2010; Terlecki, Newcombe, & Little, 2008;
Voyer et al., 1995; Voyer & Doyle, 2010). With the imbalance among the number of male and
female nurses and the commonly accepted finding of males performing higher than females on
mental rotation tests for spatial ability, looking at spatial ability in nurses could provide
additional information to address gender differences and nursing shortages within the profession.
Several explanations for gender differences in spatial ability have been provided, such as
socioeconomic status (SES), environmental, or biological factors (Levine, Vasilyeva, Lourenco,
Newcombe, & Huttenlocher, 2005). Brain maturation, hormonal changes, personal beliefs and
motivation have also been reported as possible explanations for gender differences in spatial
abilities (Moe & Pazzaglia, 2006; Kozaki & Yasukouchi, 2009; Yilmaz, 2009).

13
The Study
Aim
The aim of the present study is to assess registered nurses for spatial ability, and
determine if individual differences exist as a function of gender, years of work experience,
working environment, and number of professional certifications. The research questions guiding
the investigation are as follows:
Research Question 1: Are individual differences in spatial ability related to gender in RNs?
Research Question 2: Is spatial ability of RNs, as defined by either the Shipley-2 Block or Group Embedded Figures Test, related to years of experience, gender, and work environment (critical or non-critical care)?
Research Question 3: Is spatial ability, work environment, years of nursing experience, number of certifications possessed, and gender predictive of a measure of nursing content knowledge (a proxy for nurse competency)?
Design
The present study utilized a cross-sectional research design. Cross-sectional studies
involve data collection at a defined time. This type of study collects data to make inferences
about a population of interest at one point in time; often described as snapshots of a population
(Carlson & Morrison, 2009).
Sample/Participants
Sixteen acute care hospitals within a multi-hospital setting were used to establish a
population of registered nurses for the present study. Contact was made with supervisors of
selected nursing groups with a request that they provide information about the study to the RNs
within their group and the need for research participants. Respondents were screened for

14
eligibility and provided with study information and informed consent forms. The sample
consisted of 123 registered nurses (Mage = 44.47 years, SD = 9.98) employed with an acute care
multi-hospital setting. Male nurses accounted for 31 of the total participants (Mage = 42.87 years,
SD = 8.94), with a range of professional certifications from 0 to 4 (Mcert = 1.32, SD = 0.94), and a
range of nursing experience years from 1 to 38 (Myrs = 14.71, SD = 8.98). Female nurses
accounted for 92 of the total participants (Mage = 45.01 years, SD = 10.29), with a range of
professional certifications from 0 to 6 (Mcert = 1.42, SD = 1.21), and a range of nursing
experience years from 3 to 46 (Myrs = 19.05, SD = 10.69).
Eligibility for inclusion required participants to be currently employed as a registered
nurse at one of the 16 acute care hospitals. Speaking and understanding English did not exclude
any participant from the present study, as English language competency is a requirement for
employment.
Data Collection
Sampling Procedures
After obtaining Institutional Review Board approval recruitment of RN nurse participants
began with an attempt to obtain equal participation of females and males. Because of the small
sampling frame for males, emphasis was placed on identification and securing male participants.
After exhausting all available nurse supervisors, a total of 31 males who agreed to participate in
the study were identified. Consequently, to maintain adequate statistical power, additional female
participants were recruited (n = 92) resulting in a total sample of 123 (25% male).

15
Research Methods
Each participant was scheduled for an individual research appointment, in which the
nurse was individually administered a battery of assessments, using the same protocol for
administration for all participants. The protocol order was as follows: a brief demographic and
work history survey, the Shipley-2 Block Pattern Test, the Group Embedded Figures Test, and a
test of general nursing knowledge. Each of these measures is described below.
Instrumentation
Demographic and Work History
The demographic and work history survey included each participant’s name, date of
birth, gender, highest level of completed education, years worked as RN, current work place
environment, and identification of the titles of the professional certifications currently held. The
American Nurses Credentialing Center (ANCC) lists 25 professional specialty certifications for
RNs (American Nurses Credentialing Center, 2013). The present study included additional
certifications such as Advanced Critical Life Support (ACLS) and Sexual Assault Nurse
Examiner (SANE).
Shipley-2 Block Pattern Test
The Shipley-2 Block Pattern Test is a nonverbal assessment of fluid cognitive ability in
the spatial (Gv) domain (Western Psychological Services, 2012). The revision and
restandardization of the original 1940 Shipley Institute of Living Scale, along with the adaptation
of Kohs Block Design Test resulted in the current version of the Shipley-2 Block Pattern Test
(Beaujean et al., 2011). Administering a non-verbal block patterns test provides a method of

16
measuring abstract thinking ability in an easily understandable way (DARA Thailand, Drug and
Alcohol Rehab Asia, 2008). The Shipley-2 Block Pattern Test is a 2-page paper-and-pencil
assessment, composed of 26 multiple choice-matching items in which participants view a
stimulus mosaic block diagram that has an essential piece(s) missing, and determine from a
variety of provided graphics, which piece(s) is needed to complete the stimulus graphic (Shipley,
Gruber, Martin, & Klein, 2009). The participant has 10 minutes to complete the tasks. The
Block Pattern test has a mean internal consistency of 0.92 for adults. This instrument can be
administered individually or in a group setting, is a quick measure of intellectual functioning,
and has been standardized for use with children ages 7 to 19 years, and adults ages 17 to 89 years
(Shipley et al.).
Group Embedded Figures Test
The Group Embedded Figures Test (GEFT), developed in 1977, is an adaptation of the
original 1971 Embedded Figures Test (EFT) and can be administered in individual or group
settings to examine cognitive functioning in the spatial (Gv) domain (Witkin, Oltman, Raskin, &
Karp, 2002). The GEFT has a reported reliability of r = 0.89 for males and females (Rittschof,
2010). This measurement tool is the most widely recognized measure for cognitive styles of
field-dependence and field-independence (Beres, Magyar, & Turscanyi-Szabo, 2012; Blanton,
2004).
Finding common geometric shapes in a larger design provides information about field
dependence and field independence (Thompson & Melancon, 1987). As reported by Khatib and
Hosseinpur (2011), field-independent respondents tend to view concepts analytically, have less
difficulty with problem solving, and are intrinsically motivated. Field-dependent individuals

17
often struggle to solve problems, tend to be extrinsically motivated, and are reported to learn
better when the organization and structure is provided to them (Robinson, Kitchel, & Garton,
2009). A high GEFT score (15-18) indicates the individual can separate the simple figure from
the complex figure and has habits associated with field-independence (Blanton, 2004).
According to Blanton (2004), a low GEFT score (0-5) indicates the individual has tendencies
towards field-dependence. Individuals with mid-range GEFT scores (6-14) are associated with a
combination of field-dependence and field-independence (Blanton, 2004).
Participants are provided a booklet with simple visual figures embedded inside
progressively more complicated visual figures. The GEFT contains 18 complex figures, each
with an embedded simple figure. The participant’s task on each item is to locate a previously
seen simple figure within a larger complex figure which is organized as to obscure the simple
figure (Khatib & Hosseinpur, 2011). Participants must ignore confusing visual information to
find and outline the hidden figure (Noble, Miller, & Heckman, 2008). The test includes three
sections. The first section, with a time limit of two minutes, has seven practice examples that
demonstrate the process for each participant. The first section is not included in the total score of
the GEFT. The second and third sections each consist of 9 items, with a 5-minute time limit for
each section. Scoring is based on the number of simple forms correctly identified within the
second and third sections, ranging from 0 to 18 (Guillot, Champely, Batier, Thiriet & Collet,
2007).
General Nursing Knowledge
There has been little progress in the nursing profession towards the development of a
general tool to evaluate overall nursing knowledge and skills outside of nursing schools (Long et

18
al., 2013). Assessing general nursing knowledge and fundamental competencies identifies areas
for professional development and educational needs; as well as ensuring nurse capabilities are
matched to patient needs (O'Leary, 2012). As there are no validated tools for assessing general
nursing knowledge outside of certification/licensing exams, an assessment was created using
sample review questions for the NCLEX-RN exit exam and the HESI exit exam (Suhonen,
Schmidt, & Radwin, 2007) as a proxy for nursing competency.
The NCBSN does not provide, recommend, or endorse any specific review program for
the NCLEX-RN exam (National Council of State Boards of Nursing, 2013). Sample review
questions from free on-line NCLEX-RN and HESI Exit Exam study websites were selected to
create the knowledge assessment for the present study. From an item pool (n = 192) of NCLEX-
RN and HESI Exit Exam review questions, a random sample of items were selected from each
topical area, resulting in an assessment containing 52 items.
Ethical Considerations
Institutional Review Board approval was obtained from the multi-site hospital and the
author’s institution. All participants completed informed consent forms approved for the present
study.
Data Analysis
Statistical analysis was performed using R, version 2.15.2 (R Development Core Team,
2013). Data was screened for normality and missing data prior to analysis. Six observations
were missing from the general nursing knowledge survey. One observation was missing from
each of the survey tools (Shipley-2-Block pattern test and Group Embedded Figures Test).

19
These observations were deleted prior to analysis. Descriptive statistics were performed to
evaluate the data. Multivariate analyses of variance, followed by t-tests and multiple regression,
were conducted. The internal consistency reliability of each continuously scored measure was
computed using Cronbach’s alpha.
Reliability
Internal consistency reliability was examined using Cronbach’s alpha, a commonly used
index of test reliability (Tavakol & Dennick, 2011). Alpha values ≥ 0.90 are considered
excellent, and scores ≤ 0.90 and ≥ 0.70 are considered good (Adamson et al., 2011). Both the
Shipley-2 Block (26 items, α = 0.81) and the GEFT (18 items, α = 0.89) were determined to have
good reliability in this sample. The test of general nursing knowledge (52 items, α =.74) also
possesses acceptable reliability in this sample. As the test of general nursing knowledge is a
newly created/adapted measure in addition to the fact that the test is rather brief for addressing a
very wide range of content, and since a Cronbach’s alpha of 0.70 or greater is often considered
acceptable for research purposes (Bland & Altman, 1997), the assessment performs adequately
for the present study.
Results
Study participants (n = 123) were registered nurses working within an acute care multi-
hospital setting. Descriptive statistics are provided in Table 1.
The t-test on the two measures of spatial ability, Shipley-2 Block, and GEFT, revealed no
statistically significant mean differences for sex, Shipley-2 Block, t(121) = 1.70, p = 0.092, and
GEFT, t(121) = 1.07, p = .285. However, Cohen’s d effect sizes for mean sex differences in the

20
present study are consistent with prior studies (Voyer et al., 1995) for Shipley-2Block (d = 0.35
[95% CI = -0.06:0.76]) and GEFT (d = 0.22 [95% CI = -0.19:0.63]).
Table 1 Descriptive Statistics
Variable N Minimum Maximum Mean SD
Age 25 66 44.47 9.98 Years as RN 1 46 17.96 10.43 Proficiency Certifications 0 6 1.40 1.14 GEFT 0 18 10.07 4.98 Shipley 5 25 16.04 4.28
Gender
Male (Mage = 42.87 years) 31 Female (Mage = 45.01 years) 92
Ethnicity Asian Pacific 7 Black 9 Hispanic 5 White 101 Other 1
Education Assoc/Diploma 20 Bachelor Degree - Nursing 59 Bachelor Degree - Other 2 Master Degree - Nursing 37 Master Degree - Other 5
Critical Care Work Environmnet (N=56) Surgery/PACU 11 ICU 28 NICU 12 Emergency Dept 5
Non-Critical Care Work Environment (N=67) Ambulatory 1 Medical/Surgical 47 OB/Women 19

21
GEFT scores were reviewed for field-dependence and field-independence. Nurses with
GEFT scores of 15-18, (n = 30) were considered field-independent (Mmale = 16.82, SD = 1.25;
Mfemale = 16.32, SD = 1.16) and comprised 24.6% of all participants. The majority of
participants, (n = 68) had GEFT scores of 6-14 (Mmale = 9.75, SD = 2.26; Mfemale = 9.63, SD =
2.45). Nurses with GEFT scores of 0-5 (n = 23) are considered field-dependent, (Mmale = 3.0, SD
= 1.63; Mfemale = 2.63, SD = 1.78).
MANOVA was conducted to determine if the independent variables of sex, age, years
working as RN, the number of professional certifications, working in a critical care work
environment or a measure of general nursing knowledge impacted scores on the Shipley-2 Block
or GEFT. A one-way MANOVA revealed a significant multivariate main effect for GEFT
(F(1,114) = 6.66, p<.011) and Shipley-2 Block (F(1,114) = 12.5, p<.0006). The number of
years working as an RN was the only variable that was statistically significant for GEFT
(F(1,114) = 8.81, p = .004) and Shipley-2 Block (F(1,114) = 11.77, p = .0008).
Table 2 provides results that include years of nursing experience, sex, and work
environment regressed onto Shipley-2 Block scores for the first model tested, the same predictor
variables regressed onto GEFT scores for the second model tested. Both models are statistically
significant, where “Years of Experience as an RN” is predictive of spatial ability. The models
indicate that nurses with greater years of nursing experience have lower levels of spatial ability.

22
Table 2 Summary of Regression Models with Effects Predicting Shipley 2 Block Pattern Test and Group Embedded Figures Test (N = 122)
The final model, Table 3, examined spatial ability, sex, chosen work environment
(critical or non-critical), years working as an RN, and the number of professional certifications
regressed onto the measure of general nursing knowledge. This model was not significant, and
no interaction effects were present on sex or work environment. Moreover, spatial ability as
measured by the Shipley-2 Block or GEFT did not predict general nursing knowledge. However,
the number of professional certifications possessed by nurses did correlate with general nursing
knowledge, as would be expected.

23
Table 3 Summary of Regression Models with Effects Predicting General Nursing Knowledge (N = 117)
Discussion
Unlike previous studies of spatial ability in health care, the present study examined
registered nurses exclusively. The present study contains similar but slightly different measures
of spatial ability that permit replication analyses. Additionally, the study contains a newly
developed brief measure of general nursing knowledge constructed from existing items that was
shown to possess adequate reliability and convergent validity with professional certifications
held by RNs. This brief measure may be of value for future studies and should be subjected to
further psychometric investigation to determine, among other features, the internal factorial
structure and whether key areas of nursing are not addressed.

24
Gender Differences in Spatial Ability
The majority of studies in spatial ability have reported a significant sex difference in
favor of males. The present study did not demonstrate a statistically significant effect for sex
differences on two measures of spatial ability, Shipley-2 Block or GEFT. However, Cohen’s d
effect sizes for mean sex differences on both assessments are consistent with prior studies, where
meta-analytic mean sex differences across 286 studies were estimated to be ESweighted = 0.37
(Voyer et al., 2009). This outcome from the present study may suggest the nursing profession is
comparable with other professions where males perform higher than females on spatial ability. In
that male nurses from the present study outperform female nurses on measures of spatial ability
the findings from the present study may support screening to increase enrollment in nursing
schools for those possessing the trait.
Years of Nursing and Spatial Ability
An increase in the number of years of experience held by nurses appears to be negatively
related to greater spatial ability, regardless of sex, consequently nurses with fewer years of
experience possess greater spatial ability. Perhaps, the increased requirements and
competitiveness for admission to nursing school in recent years has changed the composition of
nurses currently entering the profession. Nursing programs now require students to possess
strong science and math skills for success, skills that have been consistently correlated with
spatial ability. It seems plausible that continued insistence on science and math would increase
the presence of spatial ability in the profession, and conversely, the screening of those without
such abilities may result in the selection of more males to the nursing workforce if the effect size

25
differences presented represent significant differences in male/female participants in the
profession.
Inpatient work environments, categorized as critical or non-critical in the present study,
did not explain individual differences in spatial ability. Historically, individuals with higher
levels of spatial ability have been correlated with more complex work environments. Critical
care nursing areas typically encompass advanced technology and require nurses to critically
think under pressure. The present findings may suggest that spatial abilities are fundamental to
many areas of nursing and not specific to any given working environment. Perhaps the various
nursing work environments, critical and non-critical, include elements of complexity specific to
the department.
Professional Nursing Certifications Predict General Nursing Knowledge
While more work needs to be done to improve the newly developed measure of general
nursing knowledge, the final model(s) indicated that general nursing knowledge was only
indicated by the number of professional certifications obtained by the nurse. While professional
certifications are role-specific, recognizing individuals with increased expertise in specialty areas
of nursing (American Nurses Credentialing Center, 2013), RNs must complete eligibility
requirements prior to applying for certification examinations such as a minimum degree
(Bachelor of Science in Nursing), a minimum number of continuing education hours in the area
of specialty, and a minimum number of hours/experience/practice in the area of specialty.
It seems logical nurses with professional certifications would score well on a measure of
nursing knowledge given that professional certification indicates superior knowledge, skills and
patient care in an area of specialty, exceeding basic nursing information (Bell-Kotwall, Frierson,

26
& Kuiper, 2012). Nurses with a professional specialty certification would be expected to have
mastery far above foundational nursing information measured by a general nursing knowledge
tool.
Years of nursing work history did not predict general nursing knowledge. While this low
correlation is likely influenced by the fact that this measure represents current nursing
knowledge and practice representative of nursing school curriculum, it appears as though nurses
do not appear to be acquiring such skills as a result of time on the job. More interesting for the
present study is that years of experience were significantly correlated with spatial ability. These
alternative findings suggest that the general nursing knowledge assessment possesses
discriminant validity for varying outcomes (spatial ability and years of work).
Significance
The present study contributes to the literature on spatial abilities in a previously
unstudied population of workers. Given demand for qualified nurses, shifting skill requirements,
and gender imbalance in the nursing workforce, the present study provides information that
might be useful with nursing student recruitment or screening for nursing schools.
Limitations
A limitation with the present study is the sample participants are all employed in one of
sixteen acute care multi-centered hospital locations. The omission of RNs working outside of
acute care (e.g., ambulatory settings, school settings, academia, or private practice) poses a
limitation to the generalization of the present study. The sample of nurses may not be
representative of nurses in general.

27
Additionally, restricting participation to only registered nurses somewhat limits the
findings. Considering the various roles in nursing (Licensed Vocational Nurse, Nurse Aide,
Nurse Assistant, Nurse Technician) the findings may not be appropriate for these roles.
Conclusions
Activities and skills using spatial ability are omnipresent in many areas of professional
nursing every day. Auscultating breath sounds for proper placement of an endotracheal tube
requires a nurse to mentally visualize the pulmonary system. Listening for the presence or
absence of abnormal breath sounds in patients with shortness of breath requires mental imagery
of the lungs to determine a plan of action. Nurses mentally visualize the features of the trachea,
larynx and esophagus while inserting a feeding tube for successful placement as it is a blind
insertion. Insertions of ewald tubes and foley catheters are activities that also require mental
visualization for proper placement. These are but a few examples of spatial ability in nursing.
Assuming the sample for the present study is representative of RNs in general, nurses
with more experience, ones that are likely to be leaving the profession soon, do not possess
spatial abilities to the extent as those with fewer years of experience. It is important that the field
is adapting or reflecting abilities related to the needs of a complex work environment, and it
appears as though this is occurring throughout the entire profession, not just the more complex
areas. More attention to the shifting nature of the nursing work environment is warranted to
assure that the field continues to progress and adapt to present needs.
References
Adamson, K.A., Parsons, M., Hawkins, K., Manz, J.A., Todd, M., & Hercinger, M. (2011) Reliability and internal consistency findings from the C-SEI. Journal of Nursing Education, 50(10), 583-586. doi:10.3928/01484834-20110715-02

28
American Association of Colleges of Nursing - AACN. (2014). Fact sheet: Nursing faculty shortage. Retrieved February 7, 2014 from https://www.aacn.nche.edu/media-relations/fact-sheets/nursing-faculty-shortage
American Association of Critical-Care Nurses. (2013). Nurse certification benefits patients, employers and nurses position statement. Retrieved November 9, 2013 from www.aacn.org/wd/certifications/content/benefitstoptempnrs.pcms?menu=certification
American Board of Nursing Specialties. (2005, March 5). A position statement on the value of nursing specialty certification. Retrieved November 9, 2013 from http://www.nursingcertification.org/
American Nurses Credentialing Center (2013). ANCC Certification Center, 2009. Retrieved from http://www.nursecredentialing.org/Certification
Barrett, E. A. (2002). What is nursing science? Nursing Science Quarterly, 15(1), 51-60.
Beaujean, A. A., Firmin, M. W., Attai, S., Johnson, C. B., Firmin, R. L., & Mena, K. E. (2011). Using personality and cognitive ability to predict academic achievement in a young adult sample. Personality and Individual Differences, 51, 709-714. doi:10.1016/j.paid.2011.06.023
Bell-Kotwall, L., Frierson, D., & Kuiper, R. (2012). Are certified nurses better professionals? Nursing Management, 43(6), 30-35, doi:10.1097/01.NUMA.0000413641.52774.2c.
Beres, I., Magyar, T., & Turcsanyi-Szabo, M. (2012). Towards a personalized, learning style based on collaborative blended learning model with individual assessment. Informatics in Education, 11(1), 1-28.
Bickley, P. G., Keith, T. Z., & Wolfle, L. M. (1995). The three-stratum theory of cognitive abilities: Test of the structure of intelligence across the life span. Intelligence, 20, 309-328. doi:10.1016/0160-2896(95)90013-6
Blanche, J. (2010). Nursing 50 years back and today: How the nursing field has changed over the last 50 years. Retrieved from http://www.healthecareers.com/article/nursing-50-years-back-and-today-how-the-nursing-field-has-changed-over-the-last-50-years/158432
Bland, J.M., & Altman, D. G., (1997). Statistics notes. Cronbach’s alpha. British Medical Journal (Clinical research ed.), 314, 572.
Blanton, E. L. (2004). The influence of students’ cognitive style on a standardized reading test administered in three different formats. (Doctoral dissertation). University of Central Florida, Orlando, FL
Bond, C. S. (2009). Nurses, computers and pre-registration education. Nurse Education Today, 29(7), 731-734. doi:10.1016/j.nedt.2009.02.014

29
Brandt, M. G., & Davies, E. T. (2006). Visual-spatial ability, learning modality and surgical knot tying. Canadian Journal of Surgery, 49(6), 412-416.
Briggs, L. A., Brown, H., Kesten, K, & Heath, J. (2006). Certification. A benchmark for critical care nursing excellence. Critical Care Nurse, 26(6), 47-53.
Brownlow, S., McPheron, T. K., & Acks, C. N. (2003). Science background and spatial abilities in men and women. Journal of Science Education and Technology, 12(4), 371-380. doi:10.1023/B:JOST.0000006297.90536.7c
Carlson, M. D. A., & Morrison, R. S. (2009) Student design, precision, and validity in observational studies. Journal of Palliative Medicine 12(1), 77-82. doi:10.1089/jpm.2008.9690
Carroll, J. B. (1997). Psychometrics, intelligence, and public perception. Intelligence, 24(1), 25-52.
Ceci, S. J., & Williams, W. M. (2010). Sex differences in math-intensive fields. Current Directions in Psychological Science, 19(5), 275-279. doi: 10.1177/0963721410383241
Cho, S-H., Lee, J. Y., Mark, B. A., & Yun, S-C. (2012). Turnover of new graduate nurses in their first job using survival analysis. Journal of Nursing Scholarship, 44(1), 63-70. doi:10.1111/j.1547-5069.2011.01428.x
Crist, K. S., Russell, B. S., & Farber, M. R. (2012). The value of certification and the CIC credential. American Journal of Infection Control, 40(4), 294-295
DARA Thailand, Drug and Alcohol Rehab Asia. (2008). Retrieved July 30, 2012, from DARA, Drug and Alcohol Rehab Asia: http://alcoholrehab.com/alcohol-rehab
Debelak, R., Gittler, G., & Arendasy, M. (2014). On gender differences in mental rotation processing speed. Learning and Individual Differences 29, 8-17. doi:10.1016/j.lindif.2013.10.003
Fairchild, R. M. (2010). Practical ethical theory for nurses responding to complexity in care. Nursing Ethics,17(3), 353–362. doi: 10.1177/0969733010361442
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175-191.
Fleischman, R. K., Meyer, L, & Watson, C. (2011). Best practices in creating a culture of certification. AACN Advanced Critical Care 22(1), 33-49. doi: 10.1097/NCI.0b013e3182062c4e
Floyd, R. G., Evans, J. J., & McGrew, K. S. (2003). Relations between measures of Cattell-Horn-Carroll (CHC) cognitive abilities and mathematics achievement across the school-age years. Psychology in the Schools, 40(20), 155-171. doi: 10.1002/pits.10083

30
Floyd, R. G., McGrew, K. S., Barry, A., Rafael, F., & Rogers, J. (2009). General and specific effects on Cattell-Horn-Carroll broad ability composites: Analysis of the Woodcock-Johnson III normative update Cattell-Horn-Carroll factor clusters across development. School Psychology Review, 38(2), 249-264.
Geary, D. C., Gilger, J. W., & Elliott-Miller, B. (1990). Gender differences in three-dimensional mental rotation: A replication. Journal of Genetic Psychology, 153, 115-117.
Geiser, C., Lehmann, W., & Eid, M. (2008). A note on sex differences in mental rotation in different age groups. Intelligence, 36, 556-563. doi: 10.1016/j.intell.2007.12.003
Giuliano, K. K., Tyer-Viola, L., & Lopez, R. P. (2005). Unity of knowledge in the advancement of nursing knowledge. Nursing Science Quarterly, 18(3), 243-248. doi: 10.1177/0894318405277527
Gottfredson, L. S. (2002). Where and why g matters: Not a mystery. Human Performance, 15(1/2), 25-46. doi:10.1207/S15327043HUP1501&02_03
Grief, C. L., (2013). Advocating for registered nurse specialty certification, Journal of Emergency Nursing, 39(3), 248-249. doi: 10.1016/j.jen.2013.02.006
Guillot, A., Champely, S., Batier, C., Thiriet, P, & Collet, C. (2007). Relationship between spatial abilities, mental rotation and functional anatomy learning. Advances in Health Sciences Education, 12, 491-507. doi: 10.1007/s10459-006-9021-7
Hegarty, M., Keehner, M., Khooshabeh, P., & Montello, D. R. (2009). How spatial abilities enhance, and are enhanced by, dental education. Learning and Individual Differences 19(1), 61-70. doi: 10.1016/j.lindif.2008.04.006
Hendren, R. (2011, April 19). Nurse executives focus on complexity of care delivery. Retrieved April 20, 2011, from HealthLeadersMedia.com: http://www.healthleadersmedia.com/content/NRS-265126/Nurse-Executives-Focus-on-Complexity-of-Care-Delivery
Hinze, S. R., Williamson, V. M., Shultz, M. J., Williamson, K. C., Deslongchamps, G., & Rapp, D. N. (2013). When do spatial abilities support student comprehension of STEM visualizations? Cognitive Processing, 14(2), 129-142. doi:10.1007/s10339-013-0539-3
Hirschkorn, C. A., West, T. B., Hill, K. S., Cleary, B. L., & Hewlett, P. O. (2010). Experienced nurse retention strategies: What can be learned from top-performing organizations. Journal of Nursing Administration, 40(11), 463-467. doi:10.1097/NNA.0b013e3181f88fd3
Hodges, H. F. (2011). Preparing new nurses with complexity science and problem-based learning. Journal of Nursing Education 50(1), 7-13, doi:10.3928/01484834-20101029-01

31
Horn, J. L. & Cattell, R. B. (1966). Refinement and test of the theory of fluid and crystallized general intelligences. Journal of Educational Psychology 57(5), 253-270. doi:10.1037/h0023816
Hoyek, N., Collet, C., Rastello, O., Fargier, P., Thiriet, P., & Guillot, A. (2009). Enhancement of mental rotation abilities and its effect on anatomy learning. Teaching and Learning in Medicine, 21(3), 201-206. doi: 10.1080/10401330903014178
Hsu, H.-Y., Chen, S.-H., Yu, H.-Y., & Lou, J.-H. (2010). Job stress, achievement motivation and occupational burnout among male nurses. Journal of Advanced Nursing 66(7), 1592-1601. doi: 10.1111/j.1365-2648.2010.05323.x
Institute of Medicine. (2010). The future of nursing: Focus on education. Retrieved from http://www.iom.edu/Reports/2010/The-Future-of-Nursing-Leading-Change-Advancing-Health/Report-Brief-Education.aspx
Institute of Medicine. (2011). The future of nursing: Leading change, advancing health. Retrieved from http://www.nap.edu/catalog/12956.html
Jansen, P., & Heil, M. (2010). Gender differences in mental rotation across adulthood. Experimental Aging Research, 36, 99-104. doi: 10.1080/03610730903422762
Jensen, A. R. (1987). Individual differences in mental ability. In J. A. Glover & R. R. Ronning (Eds.)., Historical foundations of educational psychology (pp. 61-88). New York: Plenum Press.
Juraschek, S. P., Zhang, X., Ranganathan, V. K., & Lin, V.W W. (2012). Unites States registered nurse workforce report card and shortage forecast. American Journal of Medical Quality 27(3), 241-249. doi:10.1177/1062860611416634
Kalisch, B. J. & Begeny, S., (2010). Preparation of nursing students for change and innovation. Western Journal of Nursing Research 32(2), 157-167. doi:10.1177/0193945909335052
Kane, H., & Brand, C. (2003). The importance of spearman's g as a psychometrical, social, and educational construct. The Occidental Quarterly, 3(1), 7-30.
Kendall-Gallagher, D., Aiken, L. H., Sloane, D. M., & Cimiotti, J. P. (2011). Nurse specialty certification, inpatient mortality, and failure to rescue. Journal of Nursing Scholarship, 43(2), 188-194. doi: 10.1111/j.1547-5069.2011.01391.x
Khatib, M., & Hosseinpur, R. M. (2011). On the validity of the group embedded figure test (GEFT). Journal of Language Teaching and Research, 2(3), 640-648.
Kozaki, T., & Yasukouchi, A. (2009). Sex differences on components of mental rotation at different menstrual phases. International Journal of Neuroscience, 119, 59-67. doi:10.1080/00207450802480101

32
Kuehn, B. M. (2007). No end in sight to nursing shortage: Bottleneck at nursing schools a key factor. Journal of the American Medical Association, 298(14), 1623-1625. doi:10.1001/jama.298.14.1623
Langlois, J., Wells, G. A., Lecourtois, M., Bergeron, G., Yetisir, E., & Martin, M. (2009). Spatial abilities in an elective course of applied anatomy after a problem-based learning curriculum. Anatomical Sciences Education, 2, 107-112. doi:10.1002/ase.84.
Lawrence, L. A. (2011). Work engagement, moral distress, education level, and critical reflective practice in intensive care nurses. Nursing Forum 46(4), 256-268. doi: 10.1111/j.1744-6198.2011.00237.x
Leufer, T., & Cleary-Holdforth, J. (2013). Let’s do no harm: Medication errors in nursing: Part 1. Nurse Education in Practice 13(3), 213-6. doi: 10.1016/j.nepr.2013.01.013
Levine, S. C., Vasilyeva, M., Lourenco, S. F., Newcombe, N. S., & Huttenlocher, J. (2005). Socioeconomic status modifies the sex differences in spatial skill. Psychological Science, 16(11), 841-845. doi:10.1111/j.1467-9280.2005.01623.x
Long, D. A., Mitchell, M. L., Young, J., & Rickard, C. M. (2013). Assessing core outcomes in graduates: Psychometric evaluation of the Paediatric Intensive Care Unit-Knowledge and Skills Test. Journal of Advanced Nursing, 00(0). 1-11. doi:10.1111/jan.12241
Lubinski, D. (2000). Scientific and social significance of assessing individual differences: "Sinking shafts at a few critical points". Annual Review of Psychology, 51, 405-444. doi:10.1146/annurev.psych.51.1.405
Lynn, M. R., & Redman, R. W. (2005). Faces of the nursing shortage: Influences on staff nurses' intentions to leave their positions or nursing. Journal of Nursing Administration, 35(5), 264-270.
Maag, M. (2004). The Effectiveness of an interactive multimedia learning tool on nursing students' math knowledge and self-efficacy. Computers, Informatics, Nursing, 22(1), 26-33.
Maeda, Y., & Yoon, S. Y. (2013). A meta-analysis on gender differences in mental rotation ability measured by the Purdue Spatial Visualization Tests: Visualization of Rotations (PSVT:R). Educational Psychology Review, 25, 69-94. doi: 10.1007/s10648-012-9215-x
McGrew, K. S. (2009). CHC theory and the human cognitive abilities project: Standing on the shoulders of the giants of psychometric intelligence research. Intelligence, 37, 1-10. doi:10.1016/j.intell.2008.08.004
McGrew, K. (2013, October 14). CHC Theory: Visual-spatial processing (Gv) definition. Retrieved from http://www.iqscorner.com/2013/01/chc-theory-visual-spatial-processing-gv.html

33
Miner, D. C. (2012). Transforming the nursing workforce in New York: The value of baccalaureate preparation in nursing. Journal of the New York State Nurses Association 43(2), 17-36.
Moe, A., & Pazzaglia, F. (2006). Following the instructions! Effects of gender beliefs in mental rotation. Learning and Individual Differences, 16, 369-377. doi:10.1016/j.lindif.2007.01.002
National Council of State Boards of Nursing. (2005). Business Book: NCSBN 2005 Annual meeting. Mission Possible: Building a Safer Nursing Workforce through Regulatory Excellence. Chicago, IL: Author.
National Council of State Boards of Nursing. (2013). NCLEX-RN examination. Detailed test plan for the national council licensure examination for registered nurses, item writer/item reviewer/nurse educator version. Retrieved from https://www.ncsbn.org/index.htm
Nazareth, A., Herrara, A., & Pruden, S. M. (2013). Explaining sex differences in mental rotation: Role of spatial ability experience. Cognitive Processing 14(2), 201-204. doi:10.1007/s10339-013-0542-8
Noble, K. A., Miller, S. M., & Heckman, J. (2008). The cognitive style of nursing students: Educational implications for teaching and learning. Journal of Nursing Education, 47(6), 245-253.
O’Leary, J. (2012). Comparison of self-assessed competence and experience among critical care nurses. Journal of Nursing Management, 20(5), 607-604. doi:10.1111/j.1365-2834.2012.01394.x
Parkin, J. R., & Beaujean, A. A. (2012). The effects of Wechsler Intelligence Scale for Children – Fourth Edition cognitive abilities on math achievement. Journal of School Psychology, 50(1), 113-128. doi:10.1016/j.jsp.2011.08.003
Peterson, J., Hall, L. M., O’Brien-Pallas, L., & Cockerill, R. (2011). Job satisfaction and intentions to leave of new nurses. Journal of Research in Nursing 16(6), 536-548. doi:10.1177/1744987111422423
Pittalis, M., & Christou, C., (2010). Types of reasoning in 3D geometry thinking and their relation with spatial ability. Educational Studies in Mathematics, 75(2), 191-212. doi:10.1007/1s0 649-01 0-9251 -8
R Core Development Team (2013). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/.
Rich, K. L., & Nugent, K. E. (2010). A United States perspective on the challenges in nursing education. Nursing Education Today 30(3), 228-232. doi:10.1016/j.nedt.2009.10.015

34
Rittschof, K. A. (2010). Field dependence-independence as visuospatial and executive functioning in working memory: Implications for instructional systems design and research. Educational Technology Research and Development 58(1), 99-114. doi:10.1007/s11423-008-9093-6
Robinson, J. S., Kitchel, T., & Garton, B. L. (2009). using agricultural education graduates’ GEFT scores to assess their level of job satisfaction. Journal of Southern Agricultural Education Research, 59, 28-43.
Saba, V. K. (2001). Nursing informatics: Yesterday, today and tomorrow. International Nursing Review 48(3), 177-187. doi:10.1046/j.1466-7657.2001.00064.x
Schneider, W. J., & McGrew, K. (2013). Individual differences in the ability to process information. In, B. J. Irby, G. Brown, R. Lara-Alecio, & S. Jackson (Eds.), The Handbook of Educational Theories. (p. 767-782). Information Age Publishing, Inc. Retrieved from http://www.iapsych.com/articles/schneider2013.pdf
Schooley, A., & Kuhn, J. R. (2013). Early indicators of NCLEX-RN performance. Journal of Nursing Education, 52(9), 539-542, doi:10.3928/01484834-20130819-08
Shipley, W. C., Gruber, C. P., Martin, T. A., & Klein, A. M. (2009). Shipley-2 Manual. Los Angeles: Western Psychological Services.
Simon, E. B., McGinnis, S. P., & Krauss, B. J. (2013). Predictor variables for NCLEX-RN readiness exam performance. Nursing Education Perspectives, 34(1), 18-24. doi:10.5480/1536-5026-34.1.18
Stransky, D., Wilcox, L. M., & Dubrowski, A. (2010). Mental rotation: Cross-task training and generalization. Journal of Experimental Psychology: Applied, 16(4), 349-360. doi:10.1037/a0021702
Stull, A. T., Hegarty, M., & Mayer, R. E. (2009). Getting a handle on learning anatomy with interactive three-dimensional graphics. Journal of Educational Psychology, 101(4), 801-816. doi:10.1037/a0016849
Suhonen, R., Schmidt, L. A., & Radwin, L. (2007). Measuring individualized nursing care: assessment of reliability and validity on three scales. Journal of Advanced Nursing, 59(2), 77-85. doi:10.1111/j.1365-2648.2007.04282.x
Tavakol, M., & Dennick, R. (2011). Making sense of Cronbach’s alph. International Journal of Medical Education, (2), 53-55. doi:10.5116/ijme.4dfb.8dfd
Terlecki, M. S., Newcombe, N. S., & Little, M. (2008). Durable and generalized effects of spatial experience on mental rotation: Gender differences in growth patterns. Applied Cognitive Psychology, 22, 996-1013. doi:10.1002/acp.1420

35
Thompson, B., & Melancon, J. G. (1987). Measurement characteristics of the group embedded figures test. Educational and Psychological Measurement, 47, 765-772. doi:10.1177/0013164490502011
Tilley, D. D. S. (2008). Competency in nursing: A concept analysis. The Journal of Continuing Education in Nursing 39(2), 58-64.
Timmerman, D. (2008). 015 – Promoting clinical excellence by supporting nurses through certification. Journal of Pediatric Nursing 23(2), pp e13 – e14. doi: 10.1016/j.pedn.2008.01.046
U.S. Department of Health and Human Services, Health Resources and Services Administration, Health Professionals, Workforce Analysis. (2010). The registered nurse population: Findings from the 2008 national sample survey of registered nurses (2010). Retrieved from http://bhpr.hrsa.gov/healthworkforce/rnsurveys/rnsurveyfinal.pdf
Van Terheyden, N. (2007, Nov 26). Clinical knowledge doubles every 18 months. Message posted to http://speechrecognition.wordpress.com/tag/clinical-knowledge/
Voyer, D., & Doyle, R. A. (2010). Item type and gender differences on the mental rotations test. Learning and Individual Differences, 20, 469-472. doi:10.1016/j.lindif.2010.04.010
Voyer, D., Voyer, S., & Bryden, M. P. (1995). Magnitude of sex differences in spatial abilities: A meta-analysis and consideration of critical variables. Psychological Bulletin, 117(2), 250-270. doi:10.1037/0033-2909.117.2.250
Wai, J., Lubinski, D., & Benbow, C. P. (2009). Spatial ability for STEM domains: Aligning over 50 years of cumulative psychological knowledge solidifies its importance. Journal of Educational Psychology 101(4), 817-835. doi:10.1037/a0016127
Wanzel, K. R., Hamstra, S. J., Anastakis, D. J., Matsumoto, E. D., & Cusimano, M. D. (2002). Effect of visual-spatial ability on learning of spatially-complex surgical skills. The Lancet, 359, 230-231. doi:10.1016/S0140-6736(02)07441-X
Weld, K. K., & Bibb, S. C. G. (2009). Concept Analysis: Malpractice and modern-day nursing practice. Nursing Forum 44(1), 2-10. doi:10.1111/j.1744-6198.2009.00121.x
Western Psychological Services. (2012, May). Test with confidence. Retrieved May 2012, from http://portal.wpspublish.com/portal/page?_pageid=53,248007&_dad=portal&_schema=PORTAL
Witkin, H. A., Oltman, P. K., Raskin, E., & Karp, S. A. (2002). Group embedded figures test sampler set, manual and sample figures and scoring. Available at mindgarden.com
Yilmaz, H. B. (2009). On the development and measurement of spatial ability. Retrieved January 15, 2011, from International Electronic Journal of Elementary Education: http://www.iejee.com/1_2_2009/yilmaz.pdf

36
ADVANCED EDUCATION AND CERTIFICATIONS FOR NURSING – DO THEY MAKE A
DIFFERENCE?
Introduction
Professional Nursing
Over the past 50 years, changes in nursing, such as job demands, work environments,
litigation, salaries, education, uniforms, and technology, have dramatically impacted the role of
the professional nurse (Blanche, 2010). In today’s health care environment, nurses monitor
complex physiological data, operate lifesaving equipment, administer high cost health care
programs and coordinate the delivery of multiple patient services (Weld & Bibb, 2009). The
states of New York and New Jersey have proposed all nurses, by 2020, have a minimum of a
bachelor of science degree in nursing to enter the profession (Maneval & Teeter, 2010). During
the 1980s, a master’s degree became the minimum requirement for an advanced nurse
practitioner and a Doctor of Nurse Practice (DNP) will be required by 2015 (McBride, 1999).
Medicine, healthcare and nursing are rooted in scientific findings and practices. Barrett
(2002) defines nursing as a basic science and describes the practice of nursing as the scientific art
of applying knowledge of humans in combination with their environment for their well-being.
Both understanding scientific problem solving and having a strong knowledge base in science
are critically important in training nursing students for clinical practice (Johnston & McAllister,
2008). A recent study with over four thousand nursing students, compared admission criteria for
nursing programs with a standardized RN fundamentals assessment (Wolkowitz & Kelley,
2010). Wolkowitz and Kelley (2010) reported science coursework as a statistically significant
predictor and the strongest predictor for nursing program success. Scores for biology and

37
chemistry coursework were significant predictors for success with readiness practice exams for
RN licensing (Simon, McGinniss & Krauss, 2013).
The nursing profession requires expertise in both science and math (Maag, 2004).
Prerequisite requirements for entrance into the Bachelor of Science in Nursing (BSN) program in
Texas include courses in biology, microbiology, chemistry, pharmacology, anatomy and
physiology. The nursing profession requires nurses to develop areas of specialized knowledge
within a broad knowledge base, extensive skill sets, and work in a high stress environment
assuming great responsibilities (Brodie, Andrews, Thomas, Wong & Rixon, 2004).
Skill sets required for professional nursing are complex and extensive. The practice of
nursing care is discipline specific, but also requires multidisciplinary knowledge, in such areas as
respiratory therapy, pharmacy, rehabilitation and surgery (Giuliano, Tyer-Viola, & Lopez, 2005).
Foundational science and math knowledge is required in areas such as anatomy and physiology,
pharmacology and human behavior. Registered nurses working today utilize skills in
assessment, critical thinking, and communication extensively – and must be able to act quickly
and decisively. Giuliano, Tyler-Viola, & Lopez (2005) reported that nursing knowledge must be
grounded in assessment, interpreting and describing events, predicting outcomes and selecting
appropriate nursing care.
Weakness in these required skills can have disastrous consequences. The nurse is the last
person in the chain of events from prescription to medication administration, before reaching the
patient (Leufer & Cleary-Holdforth, 2013). In the United States alone, over eight million
families had at least one family member affected by a medication or medical error (Maag, 2004).
Nurses must use basic math functions and algebraic equations to calculate doses of medications
and determine intravenous (IV) drip rates (Maag, 2004). In addition to the math computations

38
necessary to deliver medication safely, nurses must utilize critical thinking and nursing judgment
to review the accuracy and appropriateness of a physician’s order, and know the pharmacological
implications of all medications they administer to the patients.
Nurses are an essential member of every hospital quality team, as nursing is associated
with quality performance metrics (Kohlbrenner, Whitelaw, & Cannaday, 2011). Nursing
performance is more important today than ever before as individuals and communities have
access to hospital performance and outcome measures by accessing Hospital Consumer
Assessment of Healthcare Providers and Systems (HCAHPS) scores (Leibert, 2011). The Joint
Commission Leadership Standards identified RNs as the most important contributor of patient
safety and quality (Kohlbrenner et al., 2011).
Magnet Recognition Program
Hospitals strive to obtain Magnet recognition, a credentialing indicating quality patient
care, innovations in professional nursing practice, and nursing excellence (American Nurses
Credentialing Center, 2013). Recognition as a Magnet Hospital by the American Nurses
Credentialing Center (ANCC) is the gold standard for excellence in nursing practice (Parsons, &
Cornett, 2011). The Magnet recognition program began in 1983 when the American Academy
of Nursing (AAN) Task Force on Nursing Practice in Hospitals conducted a study to identify
work environments that attract and retain well-qualified nurses who promote quality patient,
resident and client care. There are currently 393 hospitals with Magnet recognition,
approximately 6.9% of all registered hospitals in the United States, with 31 in the state of Texas
(ANCC, 2013).

39
A Magnet hospital is a workplace where nursing staff turnover is low, nurses have high
job satisfaction, patients have exemplary outcomes, and nurses have a voice in patient care and
are involved with data collection (“Credentialing requirements,” 2013). Consumers, as well as
many regulatory agencies, trust a Magnet designation as the ultimate credential for superior
quality nursing (ANCC, 2013).
The ANCC is acclaimed for the credentialing programs to certify and recognize nurses in
areas of specialty, recognize healthcare systems for promoting safe work environments, and
accredit continuing nursing education organizations (ANCC, 2013). Magnet credentialing is
governed by the ANCC as the focus is on nursing processes and nurses (“Credentialing
requirements,” 2013). A Magnet culture encompasses empowerment, shared decision making,
and accountability for nurses (Frellick, 2013; Long, McGee, Kinstler & Huth, 2011). Frellick
(2013) describes the 14 Forces of Magnetism, included visionary nursing leadership, creating a
workplace that encourages publication, having strong nursing representation at the top levels of
management, and empowering nurses in patient care. To provide clarity and direction, the
ANCC reconfigured the 14 Forces of Magnetism into 5 Model Components (ANCC, 2013). The
updated model represents a greater focus on outcome measurement while retaining the 14 Forces
of Magnetism as the foundation (ANCC, 2013). The five components of the updated model are
(a) transformational leadership, (b) structural empowerment, (c) exemplary professional practice,
(d) new knowledge, innovation and improvements, and (e) empirical quality results (ANCC,
2013). Global issues in nursing and health care, while not a component, includes various issues
and challenges facing health care and nursing today (ANCC, 2013). Global issues envelope all
of the five model components (ANCC, 2013).

40
Nursing education is an important segment of the Magnet recognition program. Minimal
educational requirements for different nursing roles are included, and the requirements have
increased over the years (ANCC, 2013). ANCC (2013) requires the Chief Nursing Officer
(CNO) to hold a master’s degree in nursing. Per the ANCC (2013), 75% of all nurse managers
within an organization must hold a minimum of a bachelor’s of science in nursing (BSN).
Effective January 1, 2013, the education requirement for nurse managers was expanded; 100% of
nurse managers must have a BSN or graduate degree in nursing (Hawkins & Shell, 2012). The
ANCC (2013) has strongly encouraged Magnet organizations to increase their number of BSN
prepared nurses without specifically stating a minimum number. Hawkins and Shell (2012)
report a typical Magnet facility has 48.4% of direct care BSN prepared nurses currently. All
organizations applying for magnet status after June 1, 2013, must provide an action plan that
includes a goal for 80% of registered nurses attaining a degree in nursing (BSN or graduate
degree) by 2020 (ANCC, 2013).
Nursing Education
Three common avenues to obtain an RN license are a 2-year associate degree program
(ADN), a 3-year diploma program, and a 4-year BSN (Lawrence, 2011). According to Lawrence
(2011), nursing care provided by four year and higher-degree educationally prepared nurses is
potentially related to lower patient mortality. Miner (2012) challenges the nursing profession to
abandon the multiple pathways in nursing education and join in adopting the BSN as the entry
level education required for nursing practice. The states of New York and New Jersey have
proposed all nurses, by 2020, have a minimum of a Bachelor of Science degree in nursing to
enter the profession (Maneval & Teeter, 2010). During the 1980’s, a Master’s degree was

41
established as the minimum requirement for an advanced nurse practitioner. A Doctorate of
Nurse Practice (DNP) will be the minimally accepted requirement by 2015 (McBride, 1999).
A BSN education, although not the cure for all that is expected of nurses in the future,
does introduce nursing students to a wider range of competencies in areas such as quality
improvement, leadership, public health, and health care policy (Institute of Medicine [IOM],
2010). An increase in the number of nurses with a BSN would establish a workforce positioned
to achieve education at the master’s and doctoral levels (IOM, 2010). According to the Institute
of Medicine (IOM), there is a great demand across the nursing profession for master and doctoral
prepared nurses to serve as nurse researchers, primary care providers, and nursing instructors
(IOM, 2011).
The IOM (2010) recommends new approaches and educational models for nursing.
Basic concepts that apply across many situations should be taught instead of requiring rote
memorization (IOM, 2010). The IOM (2010) requests nursing competencies move from task-
based proficiencies to higher-level competencies which would provide a foundation for care
management and decision-making skills in multiple settings. New competencies in decision
making, quality improvement, and team leadership should be incorporated in all parts of nursing
education (IOM, 2011).
Nursing education should serve as a platform for lifelong learning, including
opportunities for transition to higher degree programs (IOM, 2011). According to the IOM
(2010), nurses with an initial ADN degree are just as likely as BSN prepared nurses to seek a
higher degree. Approximately two-thirds of nurses today receive an ADN as their initial degree
and approximately 80% of these nurses fail to move beyond a BSN degree (IOM, 2011). As
advanced nursing degrees are required for nursing faculty, the high numbers of nurses starting
42
with ADN pose a challenge to have sufficient nursing faculty available to instruct nursing
students (IOM, 2011). Currently, 13% of nurses have a graduate degree in nursing; however, less
than 1% of nurses have doctoral degrees (IOM, 21012). As doctoral prepared nurses are needed
as faculty members to teach future nurses the IOM (2012) recommends doubling the number of
doctoral trained nurses by 2020.
Certifications
Licensing and Certification
RN licensure indicates entry-level competence to the nursing field where certification
verifies specialty knowledge, skills, experience and clinical judgment (American Association of
Critical-Care Nurses, 2013; American Board of Nursing Specialties, 2005). Certification reflects
self-mastery with an emphasis on self-evaluation (Crist, Russell, & Farber, 2012). According to
Wynd (2003), nursing professionalism is significantly related to years of nursing experience,
higher educational degrees in nursing, professional organizational memberships and specialty
certification. Nurses with specialty certification have expressed feelings of personal
accomplishment, personal and professional satisfaction (Knudson, 2013).
Specialty certifications, respected by nursing staff, employers, and patients, include, at a
minimum, a practice component with required knowledge testing (Briggs, Brown, Kesten, &
Heath, 2006; Grief, 2013). Nursing specialty certifications provide benefits to the certified
nurse, the nursing profession, and the community, including improved patient safety and a
commitment to lifelong learning (Williams & Counts, 2013). The American Nurses
Credentialing Center (ANCC) is the nationally recognized agency to provide professional

43
nursing credentialing programs to certify and recognize nurses in areas of specialty (ANCC,
2013).
The majority of hospitals in the United States seek accreditation from the Joint
Commission (Williams & Counts, 2013). Many hospitals apply for the Malcolm Baldrige
National Quality Award, the American Association of Critical-Care Nurses Beacon Award for
Excellence, and for Magnet recognition (Williams & Counts, 2013). All of these programs,
whether accrediting, recognizing or awarding, include nursing certifications as an integral factor
in demonstrating nursing excellence (Fleischman, Meyer, & Watson, 2011; Williams & Counts,
2013).
Professional Certification and Patient Outcomes
The connection between certified nurses and quality patient care is well established (Crist
et al., 2012). Specialty nurse certification is increasing in value as more evidence suggests that
certification is a factor in improving patient outcomes (Fleischman et al., 2011; Timmerman,
2008). Studies indicating a correlation between CIC (Certification in Infection Prevention and
Control) and reduced infection rates and improved outcomes are starting to be reported (Crist et
al., 2012). RNs with a BSN degree and a specialty certification are associated with improved
patient outcomes, decreased mortality, and decreased failure to rescue in general surgical patients
(Kendall-Gallagher, Aiken, Sloane, & Cimiotti, 2011).
Challenges for Nursing
Role Changes
Over the past 50 years, changes in nursing such as those related to job demands,

44
technology, work environments, patient acuity, litigation, salaries, education, and uniforms have
dramatically impacted the role of the professional nurse (Blanche, 2010). In today’s health care
environment, nurses monitor complex physiological data, operate lifesaving equipment,
administer high cost health care programs and coordinate the delivery of multiple patient
services (Weld & Bibb, 2009). The high demands of academic knowledge and clinical expertise
are often unexpected to individuals new to the profession (Brodie et al, 2004; Andrews, Thomas,
Wong, & Rixon, 2004). Nursing informatics, a nursing specialty approved in 1992 by the
American Nurses Association, is using information and technology to advance the field of
nursing, bridging the gap from the art of nursing to the science of nursing (Bond, 2009; Saba,
2001).
Changes in Job Skills
Nurses must use critical thinking skills with assessment, interpretation, and decision
making to provide patient care, ensuring patient safety at all times. Clinical knowledge is
estimated to double every 18 months (van Terheyden, 2007). Medical practices,
pharmaceuticals, regulations and standards of care require constant assimilation of new
information. Health care professionals must stay in a continual mode of learning as the field of
health care is constantly changing (Hodges, 2011). Providing continual education and training to
nurses and health care providers is challenging as individuals often have different learning styles
(Fleming, Mckee, Huntley-Moore, 2011; Lockie, van Lanen, & McGannon, 2013).
As health care technology advances and patients require higher levels of care, nurses
must incorporate new practices and workflows to meet the changes (Kalisch & Begeny, 2010).
Using integrating technology to improve clinical nursing practice enhances the quality of patient

45
care (Saba, 2001). Today’s nurse must use technology to support workflow as well as support
the patient’s use of increased technology (Bond, 2009). The technology required by nurses may
vary; however, the core skills of basic computer proficiency, information technology, and
information systems for health care practice that comprise the foundations of nursing informatics
are essential for all nurses (Bond, 2009).
The American Recovery and Reinvestment Act (ARRA) of 2009 included incentives for
use of health information technology (HIT) for meaningful use (IOM, 2011). Creation of EHRs
(electronic health record) using CPOE (computerized physician order entry) and interfacing of
various electronic applications has created a complex and dynamic work environment for nurses
(IOM, 2011). Expansion of biometric devices such as automated insulin pumps and implantable
cardiac defibrillators require nurses to continually expand the use of technology in patient care.
Skill sets required for professional nursing are complex and extensive. The practice of
nursing care is discipline specific, but also requires multidisciplinary knowledge in such areas as
respiratory therapy, pharmacy, rehabilitation, and surgery (Giuliano et al., 2005). Nurses must
be proactive problem solvers and collaborative interdisciplinary team members (Hodges, 2011).
Foundational science and math knowledge are required for nurses in areas such as anatomy and
physiology, pharmacology and human behavior. Registered nurses working today extensively
utilize skills in assessment, critical thinking, and communication and must be able to act quickly
and decisively. Giuliano, Tyler-Viola, & Lopez (2005) reported that nursing knowledge must be
grounded in assessment, interpreting and describing events, predicting outcomes and selecting
appropriate nursing care
The nurse is the last safety check in the chain of events from prescription to medication
administration, before reaching the patient (Leufer & Cleary-Holdforth, 2013). In the United

46
States alone, over 8 million families had at least one family member affected by a medication or
medical error (Maag, 2004). Nurses must use basic math functions and algebraic equations to
calculate doses of medications and determine intravenous (IV) drip rates (Maag, 2004).
Research has shown spatial visualization abilities to be positively related with performance on
math tasks, as well as tasks in science, technology, and engineering (Hinze et al., 2013). In
addition to the math computations necessary to deliver medication safely, nurses must also
utilize critical thinking and nursing judgment to review the accuracy and appropriateness of a
physician’s order and know the pharmacological implications of all medications they administer
to their patients.
Nurses are associated with quality performance metrics and are therefore essential
members of every hospital quality team (Kohlbrenner et al., 2011). Nursing performance is
more important today than ever before as communities can access hospital performance and
outcome measures by accessing Hospital Consumer Assessment of Healthcare Providers and
Systems (HCAHPS) scores (Leibert, 2011). The Joint Commission Leadership Standards
identified RNs as the most important contributor of patient safety and quality (Kohlbrenner et al.,
2011)
Advances in Medical Care
Many advances in medical care have resulted in greater numbers of hospitalized patients,
more critically ill patients upon admission to hospitals, and aging patients as well as improved
survival from critical events (Kuehn, 2007; Lynn & Redman, 2005). Increased patient acuity
levels with shortened lengths of hospital stays create intensive and accelerated health care
processes (Hirschkorn, West, Hill, Cleary, & Hewlett, 2010). The practice of a clinical nurse can

47
be challenging and chaotic, often impacted by personnel shortages, decreasing resources, and
seemingly unending documentation (Kramer et al., 2013). Nurses complete an average of 100
tasks per shift, with an interruption every 3 minutes, often resulting in cognitive overload
(Hendren, 2011). All of these improvements and changes rely on tremendous knowledge and a
skill set that allows the nursing professional to deliver optimal care demanded in such situations.
Nursing Shortage
Predictions
The nursing profession is experiencing a national workforce shortage of critical
proportion (Juraschek, Zhang, Ranganathan & Lin, 2012). The current shortage of Registered
Nurses (RNs) in the Unites States is unlike any previous nursing shortage to date (Goodin,
2003). Beginning in 1998, the United States has experienced an increasing RN deficit, primarily
due to the growing elderly population and aging nurses (Juraschek et al., 2012). This shortage is
predicted to worsen, with an expected national shortage of 300,000 to 1 million RNs in 2020,
and continued shortages throughout the country through 2030 (Juraschek et al., 2013). The
shortage in the number of working RNs is projected to begin around 2015 and will continue to
increase threefold, more than any nursing deficit previously experienced in the US over the past
50 years (Buerhaus, 2008). A report from the U.S. Department of Health and Human Services
(2010) predicted a nursing shortage equating to a 36% shortage.
Aging Workforce
The aging RN workforce strongly impacts the projected nursing shortage (Juraschek et
al., 2012). Nurses that were 50 years of age or older comprised 25% of the nursing workforce in

48
1980, 33% of the nursing workforce in 2000, and were accountable for 45% of the nursing
workforce in 2008 (Juraschek et al.; US Department of Health and Human Services, 2010). A
survey conducted in 2013 reported that 55% of the current RN workforces is age 50 or older
(Budden, Zhong, Moulton, & Cimiotti, 2013). It is estimated that 55% of currently employed
nurses plan to retire before 2020 (Hirschkorn et al., 2010).
Job Dissatisfaction
Social support from supervisors and coworkers, job demands, and self-efficacy were
reported to be significantly related to job dissatisfaction, while demands and support from
coworkers were related to intention to leave the profession (Peterson, Hall, O’Brien-Pallas, &
Cockerill, 2011). Job dissatisfaction was a strong determinant of turnover among new nursing
graduates, with interpersonal relationships having the strongest impact (Cho, Lee, Mark, & Yun,
2012). Cho, Lee, Mark & Yun (2012) reported nurse’s dissatisfaction with work content to be
impacting nursing turnover (Cho et al., 2012). Nurses new to the profession are often
disillusioned when what they learned nursing should be is different from the reality of nursing
practice in their work place (Cho et al., 2012).
Nursing Faculty Shortage
There are many factors for the nursing shortage with a shortage of nursing educators
being one of the factors (Rich & Nugent, 2010). The American Association of Colleges of
Nurses (AACN) reported shortages of nursing school faculty across the country are limiting
nursing student enrollment capacity (AACN, 2014). In 2012, U.S. nursing schools declined
almost 80,000 qualified applicants for baccalaureate and graduate nursing programs due to a lack

49
of faculty, clinical sites, clinical preceptors and budget constraints (AACN, 2014). Higher
financial compensation in clinical settings is enticing current and potential nursing faculty away
from the academic setting (AACN, 2014).
Addressing the Nursing Shortage
In addressing the nursing shortage created by increasing demand for nursing services,
caused partially from an aging population and increased rates of insurance coverage, the nursing
workforce must expand by encouraging younger individuals to join the profession (IOM, 2011).
Identifying reasons why nurses are leaving the profession is another important step in addressing
the impending nursing shortage. Nurse leaders and managers play critical roles in supporting
new graduates with developing interpersonal relationships among nursing staff and other
personnel (Cho et al., 2012). Addressing the new nurse’s dissatisfaction with their work content
poses many challenges. Ensuring nursing students have realistic nursing experiences during
school may address this issue (Cho et al., 2012). Clear job descriptions and clear expectations
provided to potential nursing students may assist with providing students a realistic picture of the
nursing profession.
Another process to address the predicted nursing shortage would be to ensure those
entering the profession possess essential aptitudes for a career in nursing. In this manner, the
profession of nursing might benefit from alignment with current strategies of early identification
of individuals with potential for success, as is being done in science, technology, engineering,
and math (STEM) fields.
Students often enter the field of nursing with common misconceptions, such as nursing is
a subordinate occupation, requiring only common sense and little intellectual capacity (Brodie et

50
al., 2004). Students are surprised, even overwhelmed, by the required high academic standards
in nursing. The unexpected demands of academic knowledge and clinical expertise have been
identified as a source of nursing student attrition (Brodie et al., 2004) Acquiring the required
knowledge and skills often overwhelms students preparing for a nursing career. Through their
nursing education, students learn to accept and value the tremendous knowledge, skill set and
responsibilities of nurses (Brodie et al., 2004). Harvey and McMurray (1997) reported that 81%
of students dropping from a pre-nursing course cited a perceived discrepancy between the
content of their course and their preconceived ideas of the nursing profession. Failure to
recognize that nursing is based on science and requires a complex and specialized skill set with
the ability to think critically and act decisively underlies much of that perceived discrepancy
(Harvey & McMurray, 1997).
Spatial Ability
General Cognitive Ability - g
Charles Spearman introduced the first theory of intelligence in 1904, identifying general
mental ability as a trait based on his findings that all mental test scores were positively correlated
(Floyd, McGrew, Barry, Rafael, & Rogers, 2009; Jensen, 1987). Spearman proposed general
intelligence, g, as the identified factor that accounted for correlations among cognitive ability
tests (Carroll, 1997). Researchers generally agree that intelligence is not the amount of
information people have but their ability to recognize, acquire, organize, update, select and apply
information (Gottfredson, 1997).
General cognitive ability (g) is the capacity to work with cognitive complexity, more
specifically, complex informational processing (Gottfredson, 1997; 2002). An application

51
definition of general cognitive ability (g) is the aptitude to learn moderately complex material
quickly and efficiently and the ability to prevent cognitive errors (Gottfredson, 2002). The g
factor is the main underlying construct for most ability tests, accounting for the majority of these
tests’ predictive ability, and is the most important predictor of job performance (Gottfredson,
2002). Gottfredson (2002) reports the more a test is g-loaded, the greater the test predicts
performance in school, employment, and income. General cognitive ability has been identified
as the primary predictor for occupational success in the United States (Kane & Brand, 2003).
Raymond Cattell suggested human intelligence is comprised of two complementary
intelligence factors--crystallized and fluid intelligence (Horn & Cattell, 1966). Crystallized
intelligence, gc, represents specific knowledge that one obtains from learning, education and
experience, such as general information, vocabulary, and math. In contrast, fluid intelligence, gf,
represents the capacity to solve problems, think logically, and reason independent of acquired
knowledge (Jensen, 1987). John Horn furthered Cattell’s research in 1965, confirming the gf/gc
relationship as well as identifying new broad factors of visual processing, auditory processing,
long term storage and retrieval, cognitive processing speed, and short term memory (Kane &
Brand, 2003). These findings resulted in an expanded theory of intelligence, the Cattell-Horn
Gf-Gc theory (McGrew, 2009).
Carroll (1997) reported general cognitive ability (g) is more likely an indicator of how
fast an individual can learn rather than an indicator of an individual’s capability of learning.
Carroll’s research proposed a hierarchical model of intelligence, describing cognitive abilities in
terms of a three-stratum model (Carroll, 1997; Kane & Brand, 2003). Stratum 1 is composed of
a large number of narrow abilities, such as language development, reading, and spelling.
Stratum II consists of 10 broad abilities, such as fluid intelligence, crystallized intelligence,

52
general memory and processing speed (Kane & Brand, 2003). The highest stratum, Stratum III,
consists of only one single factor, g, generalized intelligence (Carroll, 1997). Halpern (1998)
reports critical thinking skills are often associated with higher order cognitive skills, in
comparison to simpler or lower order thinking skills.
Cattell-Horn-Carroll Theory
The Cattell Horn Carroll (CHC) theory of intelligence was developed by merging the
Cattell-Horn Gf-Gc model with Carroll’s three-tiered stratum model to form a broader
hierarchical model of g (Floyd, Evans, & McGrew, 2003; McGrew, 2009). CHC theory allows
researchers to assess the relationships between cognitive abilities and academic achievements, an
important element of learning and education (McGrew & Wendling, 2010). Keith and Reynolds
(2010) report the CHC theory provides the best description of human intelligence functions as
both a working theory for describing and understanding cognitive abilities and a guide for
development of new assessment tools.
General cognitive ability, g, is the highest level of the hierarchy at Stratum III (Bickley,
Keith, & Wolfe, 1995; Parkin & Beaujean, 2012). Stratum II contains 10 broad CHC abilities
with visual processing, Gv, being one of the ten (Rozencwajg, Schaffer, & Lefebvre, 2010).
Making use of simulated mental imagery to solve problems is the basis of visual processing
(McGrew, 2013). Visual-spatial ability includes many specific perceptual abilities, being
cognizant of complex visual patterns, being aware of where items are located in space, in
addition to visualizing objects as they would appear from a different angle (Schneider &
McGrew, 2012; 2013). According to McGrew (2009), Gv abilities are often measured by tasks
that require retaining the spatial orientation of an object after the object has been moved or

53
changed. Figure 2 provides a visual illustration, comparing Carroll's Three-Stratum, Cattell–
Horn's Extended Gf–Gc, and the integrated Cattell–Horn–Carroll models of human cognitive
abilities (McGrew, 2009).
Figure 2. Schematic representation and comparisons of Carroll's three-stratum, Cattell–Horn's extended Gf–Gc, and the integrated Cattell–Horn–Carroll models of human cognitive abilities. (McGrew, 2009).
General cognitive ability, g, is the highest level of the hierarchy at Stratum III (Bickley et
al., 1995; Parkin & Beaujean, 2012). Stratum II contains 10 broad CHC abilities: (a) fluid
intelligence, (b) quantitative knowledge, (c) crystalized intelligence, (d) reading and writing
ability, (e) short-term memory, (f) visual processing, (g) auditory processing, (h) long-term
retrieval, (i) processing speed, and (j) decision/reaction time/speed (Rozencwajg et al., 2010).
Over 100 narrow abilities are included in Stratum I and are subsumed under the broader abilities
in Stratum II (Parkin & Beaujean, 2010)

54
The current study focused on the broad ability of visual processing, Gv. Visual-spatial
ability, using simulated mental imagery to solve problems, includes many specific perceptual
abilities, being cognizant of complex visual patterns, being aware of the location of items in
space, in addition to visualizing objects as they would appear from a different angle (McGrew,
2013; Schneider & McGrew, 2012; 2013). According to McGrew (2009), Gv abilities are often
measured by tasks that require retaining the spatial orientation of an object after the object has
been moved or changed. Higher Gv ability allows an individual to see more than the object by
imagining the object from a different view after mental rotation, mentally taking a complex item
apart and reassembling the item (Schneider & McGrew, 2013). Lower Gv levels decrease an
individual’s ability to perform mental rotations causing the person to wait until an object is
physically rotated to see the change (Schneider & McGrew, 2013). McGrew (2013) explains
that after the eyes have transmitted visual information, the visual system of the brain performs a
number of basic computations, such as edge detection, light/dark perception, color-
differentiation, and motion-detection. These activities are used by more high level processors to
create more complex aspects of the image, such as spatial configuration (McGrew, 2013).
Spatial Ability and Job Performance
General cognitive ability, g, is a significant component of individual differences in job
performance associated with informational processing skills (Lubinski, 2000). Greater levels of
g are associated with higher levels of performance in all jobs and within all dimensions of
performance (Gottfredson, 2002). Health care organizations are frequently described within the
context of complexity, situations involving people working independently and collectively to
manage an unpredictable work environment over time (Fairchild, 2010). Individuals with high

55
general cognitive ability are needed in the nursing profession. As nursing requires strong
information processing activities for successful patient care assessing individuals considering
entering the nursing profession for general cognitive ability, specifically spatial visualization,
might be beneficial.
Spatial Ability in Health Care
Over 50 years of research exists on the importance of using spatial ability, specifically in
the realm of science, technology, engineering, and math (STEM), for selection and instruction in
education (Wai, Lubinski, & Benbow, 2009). Spatial ability, often neglected in complex work
environments, is a powerful systematic source of individual differences (Lubinski, 2010). Snow
(1999) expressed concern about the absence of spatial ability in applied educational settings:
There is good evidence that [spatial ability] relates to specialized achievements in fields such as architecture, dentistry, engineering, and medicine…Given this plus the longstanding anecdotal evidence on the role of visualization in scientific discovery... it is incredible that there has been so little programmatic research on admissions testing in this domain. (p. 136) A recent study with over 4000 nursing students, compared admission criteria for nursing
programs with a standardized RN (Registered Nurse) Fundamentals assessment (Wolkowitz &
Kelley, 2010). Wolkowitz and Kelley (2010) reported science coursework as a statistically
significant predictor and the strongest predictor for nursing program success. Scores for biology
and chemistry coursework were significant predictors for success with readiness practice exams
for RN licensing (Simon et al., 2013). As science is fundamental for nursing education and
higher spatial ability levels are associated with success in math, nursing should consider joining
efforts with educational departments in evaluating spatial ability in efforts to identify potential
candidates to enter professional nursing.
56
Health care professions must use critical thinking skills with assessment, interpretation,
and decision making to provide patient care, ensuring patient safety at all times. The field of
medicine is constantly changing, requiring health care professions to stay in a continual mode of
learning (Hodges, 2011). Clinical knowledge is estimated to double every 18 months (van
Terheyden, 2007). Medical practices, pharmaceuticals, regulations and standards of care require
constant assimilation of new information. Providing continual education and training to health
care providers is challenging as individuals often have different learning styles (Fleming et al.,
2011; Lockie et al., 2013).
Spatial ability, specifically mental rotation, is associated with success in the learning of
anatomy and physiology, basic courses in medical training (Hegarty, Keehner, Khooshabeh, &
Montello, 2009, Hoyek et al., 2009; Langlois et al., 2009; Stransky, Wilcox & Dubrowski, 2010;
Stull, Hegarty & Mayer, 2009). For complex surgeries, visual spatial ability has been related to
competency and quality of results (Wanzel, Hamstra, Anastakis, Matsumoto & Cusimano, 2002).
The ability to mentally rotate an object in 3 dimensions, visualizing structures from several
viewpoints with three dimensional images, carried significant importance in learning spatially
complex surgical technical skills, echoing other studies that found surgical skills to be strongly
dependent on spatial skills (Brandt & Davies, 2006; Stransky et al., 2010).
The Study
Aim
The aim of the present study was to survey registered nurses for education history, years
of nursing experience, and specialty certifications to determine if there are individual differences
in education and specialty certifications. The research questions were:

57
Research Question 1: Does the education of an RN, general nursing knowledge or years worked as an RN have an impact on the number of professional certifications obtained? Research Question 2: Does the number of certifications a nurse has obtained, general nursing knowledge, or years worked as an RN predict a nurse’s education?
Design
The present study utilized a cross-sectional research design. Cross-sectional studies
involve data collection at a defined time. This type of study collects data to make inferences
about a population of interest at one point in time; often described as snapshots of a population
(Carlson & Morrison, 2009).
Participants
Sixteen acute care hospitals within a multi-hospital setting were used to establish a
population of registered nurses for the present study. Contact was made with supervisors of
selected nursing groups with a request that they provide information about the study to the RNs
within their group and the need for research participants. Respondents were screened for
eligibility and provided with study information and informed consent forms. The sample
consisted of 123 registered nurses (Mage = 44.47 years, SD = 9.98) employed with an acute care
multi-hospital setting. Male nurses accounted for 31 of the total participants (Mage = 42.87 years,
SD = 8.94), with a range of professional certifications from 0 to 4 (Mcert = 1.32, SD = 0.94), and a
range of nursing experience years from 1 to 38 (Myrs = 14.71, SD = 8.98). Female nurses
accounted for 92 of the total participants (Mage = 45.01 years, SD = 10.29), with a range of
professional certifications from 0 to 6 (Mcert = 1.42, SD = 1.21), and a range of nursing
experience years from 3 to 46 (Myrs = 19.05, SD = 10.69).

58
Eligibility for inclusion required participants to be currently employed as a registered
nurse at one of the 16 acute care hospitals. Speaking and understanding English did not exclude
any participant from the study as English language competency is a requirement for employment.
Data Collection
Sampling Procedures
Using G*Power3.1 (Faul, Erdfelder, Lang, & Buchner, 2007), an a priori estimate of
sufficient sample size required to achieve power (1 - β) = .80 was conducted. Targeting a
medium effect size (Cohen’s d = 0.5) with α = 0.05, the initial sample estimate was N = 102,
assuming the sample allocation ratio was 1:1 for females and males. After obtaining Institutional
Review Board approval recruitment of RN nurse participants began with an attempt to obtain 51
females and 51 males. Because of the small sampling frame for males, emphasis was placed on
identification and securing male participants. After exhausting all available nurse supervisors, a
total of 31 males who agreed to participate in the study were identified. Consequently, to
maintain adequate statistical power, additional female participants were recruited (N = 92)
resulting in a total sample of 123 (25% male).
Research Methods
Each participant was scheduled for an individual research appointment, in which they
were individually administered a battery of assessments using the same protocol for
administration for all participants. The protocol order was as follows: a brief demographic and
work history survey, the Shipley-2 Block Pattern Test, the Group Embedded Figures Test, and a
test of general nursing knowledge. Each of these measures is described.

59
Each participant was scheduled for an individual research appointment, in which the nurse was
individually administered a battery of assessments, using the same protocol for administration
for all participants. The protocol order was as follows: a brief demographic and work history
survey, the Shipley-2 Block Pattern Test, the Group Embedded Figures Test, and a test of
general nursing knowledge. Each of these measures is described below.
Instrumentation
Demographic and Work History
The demographic and work history survey included each participant’s name, date of
birth, gender, highest level of completed education, years worked as RN, current work place
environment, and identification of the titles of the professional certifications currently held. The
American Nurses Credentialing Center (ANCC) lists 25 professional specialty certifications for
RNs (American Nurses Credentialing Center, 2013). The current study included additional
certifications such as Advanced Critical Life Support (ACLS) and Sexual Assault Nurse
Examiner (SANE).
Shipley-2 Block Pattern Test
The Shipley-2 Block Pattern Test is a nonverbal assessment of fluid cognitive ability in
the spatial (Gv) domain (Western Psychological Services, 2012). The revision and
restandardization of the original 1940 Shipley Institute of Living Scale, along with the adaptation
of Kohs Block Design Test resulted in the current version of the Shipley-2 Block Pattern Test
(Beaujean et al., 2011). Administering a non-verbal block patterns test provides a method of
measuring abstract thinking ability in an easily understandable way (DARA, Drug and Alcohol

60
Rehab Asia, 2008). The Shipley-2 Block Pattern Test is a 2-page paper-and-pencil assessment,
composed of 26 multiple choice-matching items in which participants view a stimulus mosaic
block diagram that has an essential piece(s) missing, and determine from a variety of provided
graphics, which piece(s) is needed to complete the stimulus graphic (Shipley, Gruber, Martin, &
Klein, 2009). The participant has 10 minutes to complete the tasks. Per the Shipley 2 Manual
the Block Pattern test has a mean internal consistency of 0.92 for adults. This instrument can be
administered individually or in a group setting, is a quick measure of intellectual functioning,
and has been standardized for use with children ages 7 to 19 years, and adults ages 17 to 89 years
(Shipley et al., 2009).
Group Embedded Figures Test
The Group Embedded Figures Test (GEFT), developed in 1977, is an adaptation of the
original 1971 Embedded Figures Test (EFT) and can be administered in individual or group
settings to examine cognitive functioning in the spatial (Gv) domain (Witkin, Oltman, Raskin, &
Karp, 2002). The GEFT has a reported reliability of r = 0.89 for males and females (Rittschof,
2010). This measurement tool is the most widely recognized measure for cognitive styles of
field-dependence and field-independence, measuring a style of cognitive perceptual ability
(Beres, Magyar, & Turscanyi-Szabo, 2012; Blanton, 2004).
Finding common geometric shapes in a larger design provides information about field
dependence and field independence (Thompson & Melancon, 1987). Field-independent
respondents are often more autonomous in the development of restructuring skills, required
during technical tasks with which the individual is not necessarily familiar (Khatib &
Hosseinpur, 2011). As reported by Khatib and Hosseinpur (2011), field-independent
61
respondents tend to view concepts analytically, have less difficulty with problem solving, and are
intrinsically motivated. On the other end of the spectrum, field-dependent individuals often
struggle to solve problems, tend to be extrinsically motivated, and are reported to learn better
when the organization and structure is provided to them (Robinson, Kitchel, & Garton, 2009). A
high GEFT score (15-18) indicates the individual can separate the simple figure from the
complex figure and has habits associated with field-independence (Blanton, 2004). According to
Blanton (2004), a low GEFT score (0-5) indicates the individual has tendencies towards field-
dependence. Individuals with mid-range GEFT scores (6-14) are associated with a combination
of field-dependence and field-independence (Blanton, 2004).
Participants are provided a booklet with simple visual figures embedded inside
progressively more complicated visual figures. The GEFT contains 18 complex figures, each
with an embedded simple figure. The participant’s task on each item is to locate a previously
seen simple figure within a larger complex figure which is organized as to obscure the simple
figure (Khatib & Hosseinpur, 2011). Participants must ignore confusing visual information to
find and outline the hidden figure (Noble, Miller, & Heckman, 2008). The test includes three
sections. The first section, with a time limit of two minutes, has seven practice examples that
demonstrate the process for each participant. The first section is not included in the total score of
the GEFT. The second and third sections each consist of 9 items, with a 5-minute time limit for
each section. Scoring is based on the number of simple forms correctly identified within the
second and third sections, ranging from 0 to 18 (Guillot, Champely, Batier, Thiriet & Collet,
2007).

62
General Nursing Knowledge
There has been little progress in the nursing profession towards the development of a
general tool to evaluate overall nursing knowledge and skills outside of nursing schools (Long,
Mitchell, Young, & Rickard, 2013). Assessing general nursing knowledge and fundamental
competencies identifies areas for professional development and educational needs; as well as
ensuring nurse capabilities are matched to patient needs (O'Leary, 2012). As there are no
validated tools for assessing general nursing knowledge outside of certification/licensing exams,
an assessment was created using sample review questions for the NCLEX-RN exit exam and the
HESI exit exam (Suhonen, Schmidt, & Radwin, 2007) as a proxy for nursing competency.
The NCBSN does not provide, recommend, or endorse any specific review program for
the NCLEX-RN exam (National Council of State Boards of Nursing, 2013). Sample review
questions from free on-line NCLEX-RN and HESI Exit Exam study websites were selected to
create the knowledge assessment for the present study. Content for the NCLEX-RN and HESI
Exit exams, based on client needs, is grouped into four categories, with subcategories for two of
the four groups (National Council of State Boards of Nursing, 2013).
• Safe Effective Care Environment
o Management of Care
o Safety and Infection Control
• Health Promotion and Maintenance
• Psychosocial Integrity
• Physiological Integrity
o Basic Care and Comfort
o Pharmacological and Parenteral Therapies

63
o Reduction of Risk Potential
o Physiological Adaptation
From an item pool (n = 192) of NCLEX-RN and HESI Exit Exam review questions, a random
sample of items were selected from each topical area, resulting in an assessment containing 52
items.
Ethical Considerations
Institutional Review Board approval was obtained from the multi-site hospital and the
author’s institution. All participants completed informed consent forms approved for the present
study.
Data Analysis
Statistical analysis was performed using R, version 2.15.2 (R Development Core Team,
2013). Data was screened for normality and missing data prior to analysis. Six observations
were missing from the nurse proficiency survey. Six observations were missing from general
nursing knowledge survey. These observations were deleted prior to analysis. Descriptive
statistics were performed to evaluate the data. The internal consistency reliability of each
continuously scored measure was computed using Cronbach’s alpha.
Reliability
Internal consistency reliability was examined using Cronbach’s alpha, a commonly used
index of test reliability (Tavakol & Dennick, 2011). Alpha values ≥ 0.90 are considered excellent
and scores ≤ 0.90 and ≥ 0.70 are considered good (Adamson et al., 2011). The test of general

64
nursing knowledge (54 items, α =.74) also possesses acceptable reliability in this sample. As the
test of general nursing knowledge is a newly created measure, a Cronbach’s alpha of 0.70 or
greater is considered acceptable (Bland and Altman, 1997).
Results
Study participants (n = 123) were registered nurses working within an acute care multi-
hospital setting. Descriptive statistics are provided in Table 4.
Table 4 Descriptive Statistics
Variable N Minimum Maximum Mean SD
Age 25 66 44.47 9.98Years as RN 1 46 17.96 10.43Proficiency Certifications 0 6 1.40 1.14GEFT 0 18 10.07 4.98Shipley 5 25 16.04 4.28
GenderMale (M age = 42.87 years) 31Female (M age = 45.01 years) 92
EthnicityAsian Pacific 7Black 9Hispanic 5White 101Other 1
EducationAssoc/Diploma 20Bachelor Degree - Nursing 59Bachelor Degree - Other 2Master Degree - Nursing 37Master Degree - Other 5
Critical Care Work Environmnet (N =56)Surgery/PACU 11ICU 28NICU 12Emergency Dept 5
Non-Critical Care Work Environment (N =67)Ambulatory 1Medical/Surgical 47OB/Women 19
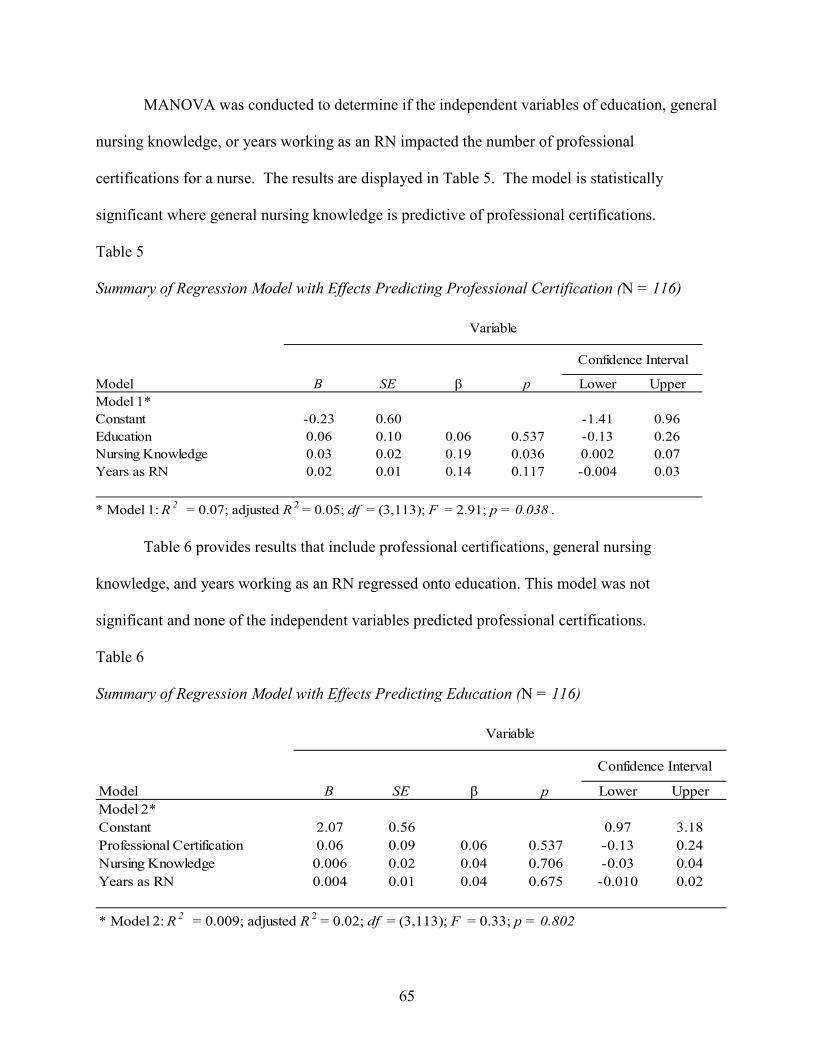
65
MANOVA was conducted to determine if the independent variables of education, general
nursing knowledge, or years working as an RN impacted the number of professional
certifications for a nurse. The results are displayed in Table 5. The model is statistically
significant where general nursing knowledge is predictive of professional certifications.
Table 5 Summary of Regression Model with Effects Predicting Professional Certification (N = 116)
Model B SE β p Lower UpperModel 1*Constant -0.23 0.60 -1.41 0.96Education 0.06 0.10 0.06 0.537 -0.13 0.26Nursing Knowledge 0.03 0.02 0.19 0.036 0.002 0.07Years as RN 0.02 0.01 0.14 0.117 -0.004 0.03
* Model 1: R 2 = 0.07; adjusted R 2 = 0.05; df = (3,113); F = 2.91; p = 0.038 .
Variable
Confidence Interval
Table 6 provides results that include professional certifications, general nursing
knowledge, and years working as an RN regressed onto education. This model was not
significant and none of the independent variables predicted professional certifications.
Table 6 Summary of Regression Model with Effects Predicting Education (N = 116)
Model B SE β p Lower UpperModel 2*Constant 2.07 0.56 0.97 3.18Professional Certification 0.06 0.09 0.06 0.537 -0.13 0.24Nursing Knowledge 0.006 0.02 0.04 0.706 -0.03 0.04Years as RN 0.004 0.01 0.04 0.675 -0.010 0.02
* Model 2: R 2 = 0.009; adjusted R 2 = 0.02; df = (3,113); F = 0.33; p = 0.802
Variable
Confidence Interval

66
Discussion
Unlike previous studies of professional nursing certification, the present study examined
registered nurses across various work environments. Additionally, the present study examined
registered nurses exclusively for spatial ability. The study contains similar but slightly different
measures of spatial ability that permit replication analyses. The study contains a newly
developed brief measure of general nursing knowledge constructed from existing items that was
shown to possess adequate reliability and convergent validity with professional certifications
held by RNs. This brief measure may be of value for future studies, and should be subjected to
further psychometric investigation to determine, among other features, the internal factorial
structure and whether key areas of nursing are not addressed.
Predictors of General Nursing Knowledge
While more work needs to be done to improve the newly developed measure of general
nursing knowledge, it seems apparent from the first model that professional certifications are
impacted by general nursing knowledge. In other words, nurses with a mastery of general
nursing knowledge are more apt to obtain professional nursing certifications.
Professional certifications are role-specific, recognizing individuals with increased
expertise in specialty areas of nursing (American Nurses Credentialing Center, 2013). RN’s
must complete eligibility requirements prior to applying for certification examinations. There
are various required criteria, dependent on the certification; however most specialty certifications
require a minimum degree (Bachelor of Science in Nursing), a minimum number of continuing
education hours in the area of specialty, and a minimum number of hours/experience/practice in
the area of specialty.

67
One can understand that nurses with a mastery of general nursing knowledge would also
be likely to obtain professional certifications, given that professional certification indicates
superior knowledge, skills and patient care in an area of specialty, exceeding basic nursing
information (Bell-Kotwall, Frierson, & Kuiper, 2012). Nurses with a professional specialty
certification would be expected to have mastery far above foundational nursing information
measured by a general nursing knowledge tool. A possible explanation why years of nursing
experience did not predict nursing knowledge or professional certifications may be based on the
concept that length of time working in nursing doesn’t necessarily imply increased knowledge.
Nurses who work in single field of practice for many years might not achieve specialty skills or
advanced knowledge. Another explanation is that the current nursing profession is diverse,
providing many options of work specialties. A nurse may move frequently between different
work areas. In this situation, the nurse would not be able to obtain the required work history in
any given area of specialty to allow the nurse to apply for certification.
Significance
The present study adds to the overall knowledge base on professional nursing
certifications and general nursing knowledge. The present study contributes to the vast literature
on spatial abilities in a previously unstudied population of workers. Given the present demand
for qualified nurses, the shifting skill requirements, and gender imbalance in the nursing
workforce, the present study provides information that might be useful with nursing student
recruitment. The fact that gender differences have been reported with spatial ability in
professions outside of nursing and the history of nursing as a predominantly female career, the

68
present study enhances the current literature on spatial ability and gender differences,
specifically in health care.
Limitations
A limitation with the present study is the sample participants are all employed in one of
sixteen acute care multi-centered hospital locations. The omission of RNs working outside of
acute care (ambulatory setting, school setting, academia, or private practice) poses a limitation to
the generalization of the present study. The present study sample of nurses may not be
representative of nurses in general.
Additionally, restricting participation to only registered nurses added restrictions to the
findings. Considering the various roles in nursing (Licensed Vocational Nurse, Nurse Aide,
Nurse Assistant, Nurse Technician) the present study may have limited findings.
Conclusions
In the continually changing field of professional nursing, ensuring nurses have a mastery
of general nursing knowledge is vital to all patients. Additionally, as health care is assessed and
reported on patient outcomes and as hospitals are competing for national recognition, it is
important to increase the number of nurses with professional certifications. The next step will be
to establish ways to encourage more nurses to obtain professional certifications and advanced
nursing degrees.
References
Adamson, K.A., Parsons, M., Hawkins, K., Manz, J.A., Todd, M., & Hercinger, M. (2011) Reliability and internal consistency findings from the C-SEI. Journal of Nursing

69
Education, 50(10), 583-586. doi:10.3928/01484834-20110715-02
American Association of Colleges of Nursing - AACN. (2014). Fact sheet: Nursing faculty shortage. Retrieved February 7, 2014 from https://www.aacn.nche.edu/media-relations/fact-sheets/nursing-faculty-shortage
American Association of Critical-Care Nurses. (2013). Nurse certification benefits patients, employers and nurses position statement. Retrieved November 9, 2013 from www.aacn.org/wd/certifications/content/benefitstoptempnrs.pcms?menu=certification
American Board of Nursing Specialties. (2005, March 5). A position statement on the value of nursing specialty certification. Retrieved November 9, 2013 from http://www.nursingcertification.org/
American Nurses Credentialing Center (2013). ANCC Certification Center, 2009. Retrieved from http://www.nursecredentialing.org/Certification
Barrett, E. A. (2002). What is nursing science? Nursing Science Quarterly, 15(1), 51-60.
Beaujean, A. A., Firmin, M. W., Attai, S., Johnson, C. B., Firmin, R. L., & Mena, K. E. (2011). Using personality and cognitive ability to predict academic achievement in a young adult sample. Personality and Individual Differences, 51, 709-714. doi:10.1016/j.paid.2011.06.023
Bell-Kotwall, L., Frierson, D., & Kuiper, R. (2012). Are certified nurses better professionals? Nursing Management, 43(6), 30-35, doi:10.1097/01.NUMA.0000413641.52774.2c.
Beres, I., Magyar, T., & Turcsanyi-Szabo, M. (2012). Towards a personalized, learning style based on collaborative blended learning model with individual assessment. Informatics in Education, 11(1), 1-28.
Bickley, P. G., Keith, T. Z., & Wolfle, L. M. (1995). The three-stratum theory of cognitive abilities: Test of the structure of intelligence across the life span. Intelligence, 20, 309-328. doi:10.1016/0160-2896(95)90013-6
Blanche, J. (2010). Nursing 50 years back and today: How the nursing field has changed over the last 50 years. Retrieved from http://www.healthecareers.com/article/nursing-50-years-back-and-today-how-the-nursing-field-has-changed-over-the-last-50-years/158432
Bland, J.M., & Altman, D. G., (1997). Statistics notes. Cronbach’s alpha. British Medical Journal (Clinical research ed.), 314, 572.
Blanton, E. L. (2004). The influence of students’ cognitive style on a standardized reading test administered in three different formats. (Doctoral dissertation). Department of Graduate Studies and Research, University of Central Florida, Orlando, FL
Bond, C. S. (2009). Nurses, computers and pre-registration education. Nurse Education Today, 29(7), 731-734. doi:10.1016/j.nedt.2009.02.014

70
Brandt, M. G., & Davies, E. T. (2006). Visual-spatial ability, learning modality and surgical knot tying. Canadian Journal of Surgery, 49(6), 412-416.
Briggs, L. A., Brown, H., Kesten, K., & Health, J. (2006). Certification: A benchmark for critical care nursing excellence. Critical Care Nurse, 26(2), 47-53.
Brodie, D. A., Andrews, G. J., Andrews, J. P., Thomas, G. B., Wong, J., & Rixon, L. (2004). Perceptions of nursing: Confirmation, change and the student experience. International Journal of Nursing Studies, 41, 721–733.
Budden, J. S., Zhong, El. H., Mouton, P., & Cimiotti, J. P. (2013). Supplement: The National Council of State Boards of Nursing and the State Nursing Workforce Centers 2013 National workforce survey of registered nurses. Journal of Nursing Regulation, 4(2). S1-S72.
Buerhaus, P. I. (2008). Current and future state of the US nursing workforce. Journal of the American Medical Association, 300(20), 2422-2424. doi:10.1001/jama.2008.729.
Carlson, M. D. A., & Morrison, R. S. (2009) Student design, precision, and validity in observational studies. Journal of Palliative Medicine 12(1), 77-82. doi:10.1089/jpm.2008.9690
Carroll, J. B. (1997). Psychometrics, intelligence, and public perception. Intelligence, 24(1), 25-52.
Cho, S-H., Lee, J. Y., Mark, B. A., & Yun, S-C. (2012). Turnover of new graduate nurses in their first job using survival analysis. Journal of Nursing Scholarship, 44(1), 63-70. doi:10.1111/j.1547-5069.2011.01428.x
Credentialing requirements for magnet status hospitals. (2013). Retrieved November 18, 2013, from http://educationcareerarticles.com/education-articles/higher-education-articles/credentialing-requirements-for-magnet-status-hospitals/
Crist, K. S., Russell, B. S., & Farber, M. R. (2012). The value of certification and the CIC credential. American Journal of Infection Control 40(4), 294-295
DARA Thailand, Drug and Alcohol Rehab Asia. (2008). Retrieved July 30, 2012, from DARA, Drug and Alcohol Rehab Asia: http://alcoholrehab.com/alcohol-rehab
Fairchild, R. M. (2010). Practical ethical theory for nurses responding to complexity in care. Nursing Ethics,17(3), 353–362. doi: 10.1177/0969733010361442
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175-191.

71
Fleischman, R. K., Meyer, L, & Watson, C. (2011). Best practices in creating a culture of certification. AACN Advanced Critical Care 22(1), 33-49. doi: 10.1097/NCI.0b013e3182062c4e
Fleming, S., Mckee, G, & Huntley-Moore, S. (2011). Undergraduate nursing students’ learning styles: A longitudinal study. Nurse Education Today 31(5), 444-449, doi:10.1016/j.nedt.2010.08.005
Floyd, R. G., Evans, J. J., & McGrew, K. S. (2003). Relations between measures of Cattell-Horn-Carroll (CHC) cognitive abilities and mathematics achievement across the school-age years. Psychology in the Schools, 40(20), 155-171. doi: 10.1002/pits.10083
Floyd, R. G., McGrew, K. S., Barry, A., Rafael, F., & Rogers, J. (2009). General and specific effects on Cattell-Horn-Carroll broad ability composites: Analysis of the Woodcock-Johnson III normative update Cattell-Horn-Carroll factor clusters across development. School Psychology Review, 38(2), 249-264.
Frellick, M. (2013, April). A path to nursing excellence. Hospitals and Health Networks. Retrieved November 18, 2013, from http://www.hhnmag.com/hhnmag/jsp/articledisplay.jsp?dcrpath=HHNMAG/Article/data/04APR2011/0411HHN_FEA_workforce&domain=HHNMAG
Giuliano, K. K., Tyer-Viola, L., & Lopez, R. P. (2005). Unity of knowledge in the advancement of nursing knowledge. Nursing Science Quarterly, 18(3), 243-248. doi: 10.1177/0894318405277527
Gottfredson, L. S. (1997). Why g matters: The complexity of everday life. Intelligence, 24 (1), 79-132. doi: 10.1016/S0160-2896(97)90014-3
Gottfredson, L. S. (2002). Where and why g matters: Not a mystery. Human Performance, 15(1/2), 25-46. doi:10.1207/S15327043HUP1501&02_03
Goodin, H. J. (2003). Integrative literature reviews and meta-analysis: The nursing shortage in the Unites States of America: an integrative review of the literature. Journal of Advancing Nursing, 43(4), 335-350. doi: 10.1046/j.1365-2648.2003.02722_1.x
Grief, C. L., (2013). Advocating for registered nurse specialty certification, Journal of Emergency Nursing, 39(3), 248-249. doi: 10.1016/j.jen.2013.02.006
Guillot, A., Champely, S., Batier, C., Thiriet, P, & Collet, C. (2007). Relationship between spatial abilities, mental rotation and functional anatomy learning. Advances in Health Sciences Education, 12, 491-507. doi: 10.1007/s10459-006-9021-7
Halpern, D. F. (1998). Teaching critical thinking for transfer across domains. American Psychologist, 53(4), 449-455.
Harvey, V. C., & McMurray, N. E. (1997). Students’ perceptions of nursing: Their relationship to attrition. Journal of Nursing Education, 36(8), 383-389.

72
Hawkins, J. E., & Shell, A. (2012). Magnet hospitals are attracted to the BSN but what’s in it for nurses? Nursing 2013, 42(3), 50-52.
Hegarty, M., Keehner, M., Khooshabeh, P., & Montello, D. R. (2009). How spatial abilities enhance, and are enhanced by, dental education. Learning and Individual Differences, 19, 61-70. doi: 10.1016/j.lindif.2008.04.006
Hendren, R. (2011, April 19). Nurse executives focus on complexity of care delivery. Retrieved April 20, 2011, from HealthLeadersMedia.com: http://www.healthleadersmedia.com/content/NRS-265126/Nurse-Executives-Focus-on-Complexity-of-Care-Delivery
Hinze, S. R., Williamson, V. M., Shultz, M. J., Williamson, K. C., Deslongchamps, G., & Rapp, D. N. (2013). When do spatial abilities support student comprehension of STEM visualizations? Cognitive Processing, 14(2), 129-142. doi:10.1007/s10339-013-0539-3
Hirschkorn, C. A., West, T. B., Hill, K. S., Cleary, B. L., & Hewlett, P. O. (2010). Experienced nurse retention strategies: What can be learned from top-performing organizations. Journal of Nursing Administration, 40(11), 463-467. doi:10.1097/NNA.0b013e3181f88fd3
Hodges, H. F. (2011). Preparing new nurses with complexity science and problem-based learning. Journal of Nursing Education 50(1), 7-13, doi:10.3928/01484834-20101029-01
Horn, J. L. & Cattell, R. B. (1966). Refinement and test of the theory of fluid and crystallized general intelligences. Journal of Educational Psychology 57(5), 253-270. doi:10.1037/h0023816
Hoyek, N., Collet, C., Rastello, O., Fargier, P., Thiriet, P., & Guillot, A. (2009). Enhancement of mental rotation abilities and its effect on anatomy learning. Teaching and Learning in Medicine, 21(3), 201-206. doi: 10.1080/10401330903014178
Institute of Medicine. (2010). The future of nursing: Focus on education. Retrieved from http://www.iom.edu/Reports/2010/The-Future-of-Nursing-Leading-Change-Advancing-Health/Report-Brief-Education.aspx
Institute of Medicine. (2011). The future of nursing: Leading change, advancing health. Retrieved from http://www.nap.edu/catalog/12956.html
Jensen, A. R. (1987). Individual differences in mental ability. In J. A. Glover & R. R. Ronning (Eds.)., Historical foundations of educational psychology (pp. 61-88). New York: Plenum Press.
Johnston, A. N., & McAllister, M. (2008). Back to the future with hands-on science: Students' perceptions of learning anatomy and physiology. Research Briefs, 47(9), 417-421.

73
Juraschek, S. P., Zhang, X, Ranganathan, V. K., & Lin, V.W W. (2012). Unites States registered nurse workforce report card and shortage forecast. American Journal of Medical Quality 27(3), 241-249. doi:10.1177/1062860611416634
Kalisch, B. J. & Begeny, S., (2010). Preparation of nursing students for change and innovation. Western Journal of Nursing Research 32(2), 157-167. doi:10.1177/0193945909335052
Kane, H., & Brand, C. (2003). The importance of spearman's g as a psychometrical, social, and educational construct. The Occidental Quarterly, 3(1), 7-30.
Keith, T. Z., & Reynolds, M. R. (2010). Cattell-Horn-Carroll abilities and cognitive tests: What we've learned from 20 years of research. Psychology in the Schools, 47(7), 635-650. doi:10.1002/pits.20496
Kendall-Gallagher, D., Aiken, L. H., Sloane, D. M., & Cimiotti, J.P. (2011). Nurse specialty certification, inpatient mortality, and failure to rescue. Journal of Nursing Scholarship, 43(2), 188-194. doi:10.1111/j.1547-5069.2011.01391.x
Khatib, M., & Hosseinpur, R. M. (2011). On the validity of the group embedded figure test (GEFT). Journal of Language Teaching and Research, 2(3), 640-648.
Kohlbrenner, J., Whitelaw, G., & Cannaday, D. (2011). Nurses critical to quality, safety, and now financial performance. The Journal of Nursing Administration, 41(3), 122-128. doi:10.1097/NNA.0b013e31820c71f9
Kramer, M., Maguire, P., Schmalenberg, C., Halfer, D., Budin, W. C., Hall, D. S., Goodloe, L., Klaristenfeld, J., Teasley, S. Forsey, L., & Lemke, J. (2013). Components and strategies of nurse residency programs effective in new graduate socialization. Western Journal of Nursing Research 35(5), 566-589. doi:10.1177/0193945912459809
Kuehn, B. M. (2007). No end in sight to nursing shortage: Bottleneck at nursing schools a key factor. Journal of the American Medical Association, 298(14), 1623-1625. doi:10.1001/jama.298.14.1623
Kundson, L. (2013). Nursing certification provides recognition for nurses, employers. AORN Connections 97(3), pp. c9 -c11. doi: 10.1016/S0001-2092(13)00130-0
Langlois, J., Wells, G. A., Lecourtois, M., Bergeron, G., Yetisir, E., & Martin, M. (2009). Spatial abilities in an elective course of applied anatomy after a problem-based learning curriculum. Anatomical Sciences Education, 2, 107-112. doi:10.1002/ase.84.
Lawrence, L. A. (2011). Work engagement, moral distress, education level, and critical reflective practice in intensive care nurses. Nursing Forum 46(4), 256-268. doi: 10.1111/j.1744-6198.2011.00237.x
Leibert, M. (2011). Performance of integrated delivery systems: Quality, service and cost implications. Leadership in Health Services 24(3), 196-206, doi:10.1108/17511871111151108

74
Leufer, T., & Cleary-Holdforth, J. (2013). Let’s do no harm: Medication errors in nursing: Part 1. Nurse Education in Practice 13(3), 213-6. doi: 10.1016/j.nepr.2013.01.013
Lockie, N. M., Van Lanan, R. J., McGannon, T. (2013). Educational implications of nursing students' learning styles, success in chemistry, and supplemental instruction participation on national council licensure examination-registered nurses performance. Journal of Professional Nursing 29(1), 49-58. doi: 10.1016/j.profnurs.2012.04.003
Long, D. A., Mitchell, M. L., Young, J., & Rickard, C. M. (2013). Assessing core outcomes in graduates: Psychometric evaluation of the Paediatric Intensive Care Unit-Knowledge and Skills Test. Journal of Advanced Nursing, 00(0). 1-11. doi:10.1111/jan.12241
Long, L. E., McGee, S., Kinstler, A., & Huth, M. M. (2011). Aligning the forces of magnetism to achieve exemplary professional practice. Journal of Pediatric Nursing 26(2), 108-113. doi: 10.1016/j.pedn.2010.12.004
Lubinski, D. (2000). Scientific and social significance of assessing individual differences: "Sinking shafts at a few critical points". Annual Review of Psychology, 51, 405-444. doi:10.1146/annurev.psych.51.1.405
Lynn, M. R., & Redman, R. W. (2005). Faces of the nursing shortage: Influences on staff nurses' intentions to leave their positions or nursing. Journal of Nursing Administration, 35(5), 264-270.
Maag, M. (2004). The Effectiveness of an interactive multimedia learning tool on nursing students' math knowledge and self-efficacy. Computers, Informatics, Nursing, 22(1), 26-33.
McBride, A. B. (1999). Breakthroughs in nursing education: Looking back, looking forward. Nursing Outlook 47(3), 114-119. doi:10.1016/S0029-6554(99)90005-2
McGrew, K. S. (2009). CHC theory and the human cognitive abilities project: Standing on the shoulders of the giants of psychometric intelligence research. Intelligence, 37, 1-10. doi:10.1016/j.intell.2008.08.004
McGrew, K. (2013, October 14). CHC Theory: Visual-spatial processing (Gv) definition. Retrieved from http://www.iqscorner.com/2013/01/chc-theory-visual-spatial-processing-gv.html
McGrew, K. S., & Wendling, B. J. (2010). Cattell-Horn-Carroll cognitive-achievement relations: What we have learned from the past 20 years of research. Psychology in the Schools, 47(7), 651-674.
Miner, D. C. (2012). Transforming the nursing workforce in New York: The value of baccalaureate preparation in nursing. Journal of the New York State Nurses Association 43(2), 17-36.

75
National Council of State Boards of Nursing. (2013). NCLEX-RN examination. Detailed test plan for the national council licensure examination for registered nurses, item writer/item reviewer/nurse educator version. Retrieved from https://www.ncsbn.org/index.htm
Noble, K. A., Miller, S. M., & Heckman, J. (2008). The cognitive style of nursing students: Educational implications for teaching and learning. Journal of Nursing Education, 47(6), 245-253.
O’Leary, J. (2012). Comparison of self-assessed competence and experience among critical care nurses. Journal of Nursing Management, 20(5), 607-604. doi:10.1111/j.1365-2834.2012.01394.x
Parkin, J. R., & Beaujean, A. A., (2012). The effects of Wechsler Intelligence Scale for Children – Fourth Edition cognitive abilities on math achievement. Journal of School Psychology, 50(1), 113-128. doi:10.1016/j.jsp.2011.08.003
Parsons, M. L., & Cornett, P. A. (2011). Sustaining the pivotal organization outcome: Magnet recognition. Journal of Nursing Management 19(2), 277-286. doi: 10.1111/j.1365-2834.2011.01224.x
Peterson, J., Hall, L. M., O’Brien-Pallas, L., & Cockerill, R. (2011). Job satisfaction and intentions to leave of new nurses. Journal of Research in Nursing 16(6), 536-548. doi:10.1177/1744987111422423
R Core Team (2013). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/.
Rich, K. L., & Nugent, K. E. (2010). A United States perspective on the challenges in nursing education. Nursing Education Today 30(3), 228-232. doi:10.1016/j.nedt.2009.10.015
Rittschof, K. A. (2010). Field dependence-independence as visuospatial and executive functioning in working memory: Implications for instructional systems design and research. Educational Technology Research and Development 58(1), 99-114. doi:10.1007/s11423-008-9093-6
Robinson, J. S., Kitchel, T., & Garton, B. L. (2009). using agricultural education graduates’ GEFT scores to assess their level of job satisfaction. Journal of Southern Agricultural Education Research, 59, 28-43.
Rozencwajg, P., Schaeffer, O., & Lefebvre, V. (2010). Arithmetic and aging: Impact of quantitative knowledge and processing speed. Learning and Individual Differences 20(5), 452-452. doi:10.1016/j.lindif.2010.04.009
Saba, V. K. (2001). Nursing informatics: Yesterday, today and tomorrow. International Nursing Review 48(3), 177-187. doi:10.1046/j.1466-7657.2001.00064.x

76
Schneider, W. J., & McGrew, K. (2012). The Cattell-Horn-Carroll model of intelligence. In, D. Flanagan & P. Harrison (Eds.), Contemporary Intellectual Assessment: Theories, Tests, and Issues (3rd ed.) (p. 99-144). New York: Guilford. Retrieved from http://www.iapsych.com/articles/schneider2012.pdf
Schneider, W. J., & McGrew, K. (2013). Individual differences in the ability to process information. In, B. J. Irby, G. Brown, R. Lara-Alecio, & S. Jackson (Eds.), The Handbook of Educational Theories. (p. 767-782). Information Age Publishing, Inc. Retrieved from http://www.iapsych.com/articles/schneider2013.pdf
Shipley, W. C., Gruber, C. P., Martin, T. A., & Klein, A. M. (2009). Shipley-2 Manual. Los Angeles: Western Psychological Services.
Simon, E. B., McGinnis, S. P., & Krauss, B. J. (2013). Predictor variables for NCLEX-RN readiness exam performance. Nursing Education Perspectives, 34(1), 18-24. doi:10.5480/1536-5026-34.1.18
Snow, R. E. (1999). Commentary: Expanding the breadth and depth of admissions testing. In S. Messick (Ed.) Assessment in higher education (pp. 133-140), Hilldale, NJ: Erlbaum
Stransky, D., Wilcox, L. M., & Dubrowski, A. (2010). Mental rotation: Cross-task training and generalization. Journal of Experimental Psychology: Applied, 16(4), 349-360. doi:10.1037/a0021702
Stull, A. T., Hegarty, M., & Mayer, R. E. (2009). Getting a handle on learning anatomy with interactive three-dimensional graphics. Journal of Educational Psychology, 101(4), 801-816. doi:10.1037/a0016849
Suhonen, R., Schmidt, L. A., & Radwin, L. (2007). Measuring individualized nursing care: assessment of reliability and validity on three scales. Journal of Advanced Nursing, 59(2), 77-85. doi:10.1111/j.1365-2648.2007.04282.x
Tavakol, M. & Dennick, R. (2011). Making sense of Cronbach’s alph. International Journal of Medical Education, (2), 53-55. doi:10.5116/ijme.4dfb.8dfd
Thompson, B., & Melancon, J. G. (1987). Measurement characteristics of the group embedded figures test. Educational and Psychological Measurement, 47, 765-772. doi:10.1177/0013164490502011
Timmerman, D. (2008). 015 – Promoting clinical excellence by supporting nurses through certification. Journal of Pediatric Nursing 23(2), pp e13 – e14. doi: 10.1016/j.pedn.2008.01.046
U.S. Department of Health and Human Services, Health Resources and Services Administration, Health Professionals, Workforce Analysis. (2010). The registered nurse population: Findings from the 2008 national sample survey of registered nurses (2010). Retrieved from http://bhpr.hrsa.gov/healthworkforce/rnsurveys/rnsurveyfinal.pdf

77
Van Terheyden, N. (2007, Nov 26). Clinical knowledge doubles every 18 months. Message posted to http://speechrecognition.wordpress.com/tag/clinical-knowledge/
Wai, J., Lubinski, D., & Benbow, C. P. (2009). Spatial ability for STEM domains: Aligning over 50 years of cumulative psychological knowledge solidifies its importance. Journal of Educational Psychology 101(4), 817-835. doi:10.1037/a0016127
Wanzel, K. R., Hamstra, S. J., Anastakis, D. J., Matsumoto, E. D., & Cusimano, M. D. (2002). Effect of visual-spatial ability on learning of spatially-complex surgical skills. The Lancet, 359, 230-231. doi:10.1016/S0140-6736(02)07441-X
Weld, K. K., & Bibb, S. C. G. (2009). Concept Analysis: Malpractice and modern-day nursing practice. Nursing Forum 44(1), 2-10. doi:10.1111/j.1744-6198.2009.00121.x
Western Psychological Services. (2012, May). Test with confidence. Retrieved May 2012, from http://portal.wpspublish.com/portal/page?_pageid=53,248007&_dad=portal&_schema=PORTAL
Williams, H. F., & Counts, C. S. (2013). Certification 101: The pathway to excellence. Nephrology Nursing Journal 40(3), 197-209.
Witkin, H. A., Oltman, P. K., Raskin, E., & Karp, S. A. (2002). Group embedded figures test sampler set, manual and sample figures and scoring. Available at mindgarden.com
Wolkowitz, A. A., & Kelley, J. A. (2010). Academic predictors of success in a nursing program. Journal of Nursing Education, 49(9), 498-503. doi:10.3928/01484834-20100524-09
Wynd, C. A. (2003). Current factors contributing to professionalism in nursing. Journal of Professional Nursing 19(5), 251-261, doi:10.1016/S8755-7223(03)00104-2

78
APPENDIX A
NURSING KNOWLEDGE ASSESSMENT

79
Name:
Date:
Sample Questions from NCLEX (National Council Licensure Examination)
1. What is the first intervention for a patient experiencing chest pain and an Sp02 of 89%? a. Administer morphine b. Administer oxygen c. Administer sublingual nitroglycerin d. Obtain an electrocardiogram (ECC)
2. Which of the following signs and symptoms usually signifies rapid expansion and impending
rupture of an abdominal aortic aneurysm? a. Abdominal pain b. Absent pedal pulses c. Chest pain d. Lower back pain
3. In which of the following types of cardiomyopathy does cardiac output remain normal?
a. Dilated b. Hypertrophic c. Obliterative d. Restrictive
4. Which of the following interventions should be your first priority when treating a patient
experiencing chest pain while walking? a. Have the patient sit down b. Get the patient back to bed c. Obtain an ECG d. Administer sublingual nitroglycerin.
5. Which of the following positions would best aid breathing for a patient with acute pulmonary
edema? a. Lying flat in bed b. Left side-lying position c. High Fowler’s position d. Semi-Fowler’s position
6. A pregnant woman arrives at the emergency department (ED) with abruptio placentae at 34
weeks’ gestation. She’s at risk for which of the following blood dyscrasias? a. Thrombocytopenia b. Idiopathic thrombocytopenic purpura (ITP). c. Disseminated intravascular coagulation (DIC) d. Heparin-associated thrombosis and thrombocytopenia (HATT).

80
7. A 16-year-old patient involved in a motor vehicle accident arrives in the ED unconscious and severely hypotensive. He’s suspected to have several fractures of his pelvis and legs. Which of the following parenteral fluids is the best choice for his current condition? a. Fresh Frozen Plasma (FFP) b. 0.9% sodium chloride solution c. Lactated Ringer’s solution d. Packed red blood cells
8. Corticosteroids are potent suppressors of the body’s inflammatory response. Which of the
following conditions or actions do they suppress? a. Cushing syndrome b. Pain receptors c. Immune response d. Neural transmission
9. A patient infected with human immunodeficiency virus (HIV) begins zidovudine therapy
(AZT). Which of the following statements best describes this drug’s action? a. It destroys the outer wall of the virus and kills it b. It interferes with viral replication c. It stimulates the immune system d. It promotes excretion of viral antibodies
10. A 20-year-old patient is being treated for pneumonia. He has a persistent cough and
complains of severe pain on coughing. What could you tell him to help him reduce his discomfort? a. “Hold your cough as much as possible” b. "Place the head of your bed flat to help with coughing." c. "Restrict fluids to help decrease the amount of sputum." d. "Splint your chest wall with a pillow for comfort."
11. A 19-year-old patient comes to the ED with acute asthma. His respiratory rate is 44 respirations per minute, and he appears to be in acute respiratory distress. Which of the following actions should you take first? a. Take a full medical history b. Give a bronchodilator by nebulizer c. Apply a cardiac monitor to the patient d. Provide emotional support for the patient.
12. A firefighter who was involved in extinguishing a house fire is being treated for smoke inhalation. He develops severe hypoxia 48 hours after the incident, requiring intubation and mechanical ventilation. Which of the following conditions has he most likely developed? a. Acute respiratory distress syndrome (ARDS) b. Atelectasis c. Bronchitis d. Pneumonia.

81
13. Which of the following measures best determines that a patient who had a pneumothorax no longer needs a chest tube? a. You see a lot of drainage from the chest tube b. Arterial blood gas (ABG) levels are normal c. The chest X-ray continues to show the lung is 35% deflated d. The water-seal chamber doesn’t fluctuate when no suction is applied
14. Which of the following nursing interventions should you use to prevent footdrop and
contractures in a patient recovering from a subdural hematoma? a. High-top sneakers b. Low-dose heparin therapy c. Physical therapy consultation d. Sequential compressive device.
15. Which of the following signs of increased intracranial pressure (ICP) would appear first after head trauma? a. Bradycardia b. Large amounts of very dilute urine c. Restlessness and confusion d. Widened pulse pressure.
16. When giving intravenous (I.V.) phenytoin, which of the following methods should you use?
a. Use an in-line filter b. Withhold other anticonvulsants c. Mix the drug with saline solution only d. Flush the I.V. catheter with dextrose solution.
17. After surgical repair of a hip, which of the following positions is best for the patient’s legs
and hips? a. Abduction b. Adduction c. Prone d. Subluxated
18. Which of the following factors should be the primary focus of nursing management in a patient with acute pancreatitis? a. Nutritional management b. Fluid and electrolyte balance c. Management of hypoglycemia d. Pain control
19. After a liver biopsy, place the patient in which of the following positions?
a. Left side-lying, with the bed flat b. Right side-lying, with the bed flat c. Left side-lying, with the bed in semi-Fowler’s position d. Right side-lying, with the bed in semi-Fowler’s position
82
20. Which of the following potentially serious complications could occur with therapy for hypothyroidism? a. Acute hemolytic reaction b. Angina or cardiac arrhythmia c. Retinopathy d. Thrombocytopenia
21. Adequate fluid replacement and vasopressin replacement are objectives of therapy for which
of the following disease processes? a. Diabetes mellitus b. Diabetes insipidus c. Diabetic ketoacidosis d. Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
22. Patients with Type 1 diabetes mellitus may require which of the following changes to their daily routine during periods of infection? a. No changes b. Less insulin c. More insulin d. Oral diabetic agents
23. On a follow-up visit after having a vaginal hysterectomy, a 32-year-old patient has a
decreased hematocrit level. Which of the following complications does this suggest? a. Hematoma b. Hypovolemia c. Infection d. Pulmonary embolus (PE)
24. A patient has partial-thickness burns to both legs and portions of his trunk. Which of the
following I.V. fluids is given first? a. Albumin b. D5W c. Lactated Ringer’s solution d. 0.9% sodium chloride solution with 2 mEq of potassium per 100 ml
25. Which of the following techniques is correct for obtaining a wound culture specimen from a
surgical site? a. Thoroughly irrigate the wound before collecting the specimen b. Use a sterile swab and wipe the crusty area around the outside of the wound c. Gently roll a sterile swab from the center of the wound outward to collect drainage d. Use a sterile swab to collect drainage from the dressing
26. A patient tells you that her urine is starting to look discolored. If you believe this change is
due to medication, which of the following patient's medication does not cause urine discoloration?
83
a. Sulfasalazine b. Levodopa c. Phenolphthalein d. Aspirin
27. You are responsible for reviewing the nursing unit's refrigerator. If you found the following drug in the refrigerator it should be removed from the refrigerator's contents? a. Corgard b. Humulin (injection) c. Urokinase d. Epogen (injection)
28. A second year nursing student has just suffered a needlestick while working with a patient
that is positive for AIDS. Which of the following is the most important action that nursing student should take? a. Immediately see a social worker b. Start prophylactic AZT treatment c. Start prophylactic Pentamide treatment d. Seek counseling
29. A thirty five year old male has been an insulin-dependent diabetic for five years and now is unable to urinate. Which of the following would you most likely suspect? a. Atherosclerosis b. Diabetic nephropathy c. Autonomic neuropathy d. Somatic neuropathy
30. You are taking the history of a 14 year old girl who has a (BMI) of 18. The girl reports inability to eat, has induced vomiting and severe constipation. Which of the following would you most likely suspect? a. Multiple sclerosis b. Anorexia nervosa c. Bulimia d. Systemic sclerosis
31. A 24 year old female is admitted to the ER for confusion. This patient has a history of a
myeloma diagnosis, constipation, intense abdominal pain, and polyuria. Which of the following would you most likely suspect? a. Diverticulosis b. Hypercalcemia c. Hypocalcaemia d. Irritable bowel syndrome
32. Rhogam is most often used to treat____ mothers that have an ____ infant.
a. RH positive, RH positive b. RH positive, RH negative

84
c. RH negative, RH positive d. RH negative, RH negative
33. A new mother has some questions about (PKU). Which of the following statements made by
a nurse is not correct regarding PKU? a. A Guthrie test can check the necessary lab values b. The urine has a high concentration of phenylpyruvic acid c. Mental deficits are often present with PKU d. The effects of PKU are reversible
34. A patient has taken an overdose of aspirin. Which of the following should a nurse most
closely monitor for during acute management of this patient? a. Onset of pulmonary edema b. Metabolic alkalosis c. Respiratory alkalosis d. Parkinson's disease type symptoms
35. A fifty-year-old blind and deaf patient has been admitted to your floor. As the charge nurse
your primary responsibility for this patient is? a. Let others know about the patient's deficits b. Communicate with your supervisor your concerns about the patient's deficits c. Continuously update the patient on the social environment d. Provide a secure environment for the patient
36. A nurse is caring for an infant that has recently been diagnosed with a congenital heart defect. Which of the following clinical signs would most likely be present? a. Slow pulse rate b. Weight gain c. Decreased systolic pressure d. Irregular WBC lab values
37. A mother has recently been informed that her child has Down's syndrome. You will be
assigned to care for the child at shift change. Which of the following characteristics is not associated with Down's syndrome? a. Simian crease b. Brachycephaly c. Oily skin d. Hypotonicity
38. A patient has recently experienced a myocardial infarction (MI) within the last 4 hours.
Which of the following medications would most likely be administered? a. Streptokinase b. Atropine c. Acetaminophen d. Coumadin

85
39. A nurse is putting together a presentation on meningitis. Which of the following microorganisms has not been linked to meningitis in humans? a. S. pneumonia b. H. influenza c. N. meningitis d. Cl. difficile
40. A nurse is administering blood to a patient who has a low hemoglobin count. The patient
asks how long do RBC's last in my body? The correct response is a. The life span of RBC is 45 days b. The life span of RBC is 60 days c. The life span of RBC is 90 days d. The life span of RBC is 120 days
41. A 65 year old man has been admitted to the hospital for spinal stenosis surgery. When does
the discharge training and planning begin for this patient? a. Following surgery b. Upon admit c. Within 48 hours of discharge d. Preoperative discussion
42. A nurse is making rounds taking vital signs. Which of the following vital signs are abnormal?
a. 11 year old male – 90 pulse, 22 resp/min., 100/70 mm Hg b. 13 year old female – 105 pulse, 22 resp/min., 105/60 mm Hg c. 5 year old male- 102 pulse, 24 resp/min., 90/65 mm Hg d. 6 year old female- 100 pulse, 26 resp/min., 90/70mm Hg
43. When you are taking a patient's history, she tells you she has been depressed and is dealing
with an anxiety disorder. Which of the following medications would the patient most likely be taking? a. Elavil b. Calcitonin c. Pergolide d. Verapamil e.
Sample Questions from HESI Exit Exam (Health Information Systems, Inc.) 44. A client’s caregiver is learning how to care for a client’s wound and drains. Which technique
of cleansing, if taught to the caregiver, would decrease the chance of the client developing an infection? a. Cleansing from the area of most drainage to the least drainage b. Cleansing from the area of most inflammation to the least inflammation c. Cleansing from the drain site outward away from the drain site d. Cleansing from a few inches away from the drain and moving to the inner portion of the
drain

86
45. The healthcare provider performs peritoneal dialysis on a client, after which 2 liters of fluid are drained. What action should the nurse complete first? a. Assess for signs and symptoms of infection b. Palpate for a thrill c. Auscultate for a bruit d. Assess vital signs
46. A client is prescribed to receive one-quarter strength tube feeding at 40 ml per hour. If the
nurse has 80 ml of full strength tube feeding solution, how many hours of feeding is available? __________ (numeric value only)
47. Following a stressful life event, a client comes into the Emergency Department for evaluation. Which manifestation demonstrates severe anxiety or panic? a. Dilated pupils b. Blurred vision c. Diminished hearing d. Faster respirations
48. A nurse is assigned to four patients. Which patient is the highest priority for this nurse to assess? a. A patient who is 72 hours post-op from a hernia repair with abdominal distention and
fever b. A patient who is 36 hours post right lower lobe lobectomy c. A patient in overhead traction for a knee injury d. A patient with diabetes and a blood glucose of 100 mg/dL
49. A patient is experiencing pulseless ventricular tachycardia (VT). What action should the nurse preform first? a. Administer epinephrine intravenously b. Prepare the patient for synchronized cardioversion c. Administer procainamide intravenously d. Prepare the patient for defibrillation
50. The nurse is instructing a client newly diagnosed with diabetes – on the signs and symptoms
of hypoglycemia. Which of the following should the nurse include in the instructions? Select all that apply a. Tremors b. Irritability c. Bradycardia d. Nausea e. Hypertension
51. The nurse in the emergency department is using the simple triage and rapid transport (START) system to assess victims of a hurricane. Which statement correctly describes a yellow disaster tag? a. A yellow disaster tag means critical injuries and requires immediate intervention

87
b. A yellow disaster tag means no critical injuries and can ambulate c. A yellow disaster tag means injuries need attention, but are not life-threatening d. A yellow disaster tag means deceased or likely to die
52. A patient is demonstrating atrial fibrillation with a heart rate of 54 beats per/minute. Which
of the following should the nurse do regarding the prescribed digoxin (Lanoxin) to the patient? a. Administer the scheduled dose of digoxin while maintaining cardiac telemetry
monitoring b. Administer the scheduled dose of digoxin and continue to monitor the patient’s heart rate c. Administer the scheduled dose of digoxin and notify the patient’s healthcare provider d. Hold the scheduled dose of digoxin and inform the patient’s healthcare provider

88
APPENDIX B
DEMOGRAPHIC AND WORK HISTORY QUESTIONNAIRE

89
Name
Date of Birth
Gender
Female
Male
Ethnicity
White
Hispanic or Latino
Black or African American
Native American or American Indian
Asian / Pacific Islander
Other
What is the highest degree or level of school you have completed?
If currently enrolled, highest degree received. Some college credit, no degree Associate degree Yes / No Bachelor’s degree Yes / No
Specific Degree Major Area of Focus
Master’s degree Yes / No Specific Degree Major Area of Focus
Professional degree Yes / No Specific Degree Major Area of Focus
Doctorate degree Yes / No

90
Specific Degree Major Area of Focus
How long have you worked as a Registered Nurse? How many years have you (did you) worked in Patient-Care as a Registered Nurse? If not currently in patient care - how many years since you preformed bed-side patient care?
Do you own any professional certifications? No Yes – for Registered Nurses
CMSRN: Certified Medical-Surgical Registered Nurse ACLS: Advanced Cardiac Life Support (ACLS) Adult Nurse Practitioner-Board Certified (ANP-BC) Advanced Oncology Certified Nurse (AOCN) Advanced Practice Nurse (APN) Advanced Practice Certified Bariatric Nurse (CBN) Certified Case Manager (CCM) Certified Clinical Nurse Specialist (CCNS) Certified Critical Care Nurse (CCRN) Certified Dialysis Nurse (CDN) Certified Emergency Nurse (CEN) Certified Hospice and Palliative Care Nurse (CHPN) Certified Hyperbaric Registered Nurse (CHRN) Certified in Infection Control/Prevention (CIC) Certified Nurse Educator (CNE) Certified Nurse Leader (CNL) Certified Ostomy Care Nurse (COCN) Certified Pediatric Emergency Nurse (CPEN) Certified Registered Nurse Anesthetists (CRNA) Certified Wound, Ostomy, Continence Nurse (CWOCN) Certified Wound Specialist (CWS) Oncology Certified Nurse (OCN) Registered Nurse Clinical Specialist (RNCS) Registered Nurse Certified Specialist (RNCS) Sexual Assault Nurse Examiner (SANE) Other Other
What most-closely describes your work environment?
Surgery/PACU Medical/Surgical Department Intensive Care Unit (Cardiac ICU)

91
NICU Ambulatory Setting Emergency Department Non-Patient Care Other

92
APPENDIX C
COMPLETE UNABRIDGED RESULTS

93
Low GEFT Medium GEFT High GEFT
23 total 68 total 30 total
Mean 2.74 Mean 9.65 Mean 16.5
SD 1.71 SD 2.40 SD 1.20
Males (n=7) Males (n=12) Males (n=11)
Mean 3 Mean 9.75 Mean 16.8
SD 1.63 SD 2.61 SD 1.25
Females (n=16) Females (n=56) Females (n=19)
Mean 2.63 Mean 9.62 Mean 16.32
SD 1.78 SD 2.45 SD 1.16

94
Low GEFT Scores
Males & Females
Gender GEFT2 0 Column12 51 5 Mean 2.739130432 2 Standard Error 0.356849361 5 Median 32 4 Mode 52 5 Standard Deviation 1.711389422 1 Sample Variance 2.928853752 3 Kurtosis -1.36591951 1 Skewness -0.03142961 4 Range 52 3 Minimum 02 4 Maximum 52 5 Sum 632 1 Count 231 21 22 31 22 02 12 42 1
23 122 18.9%
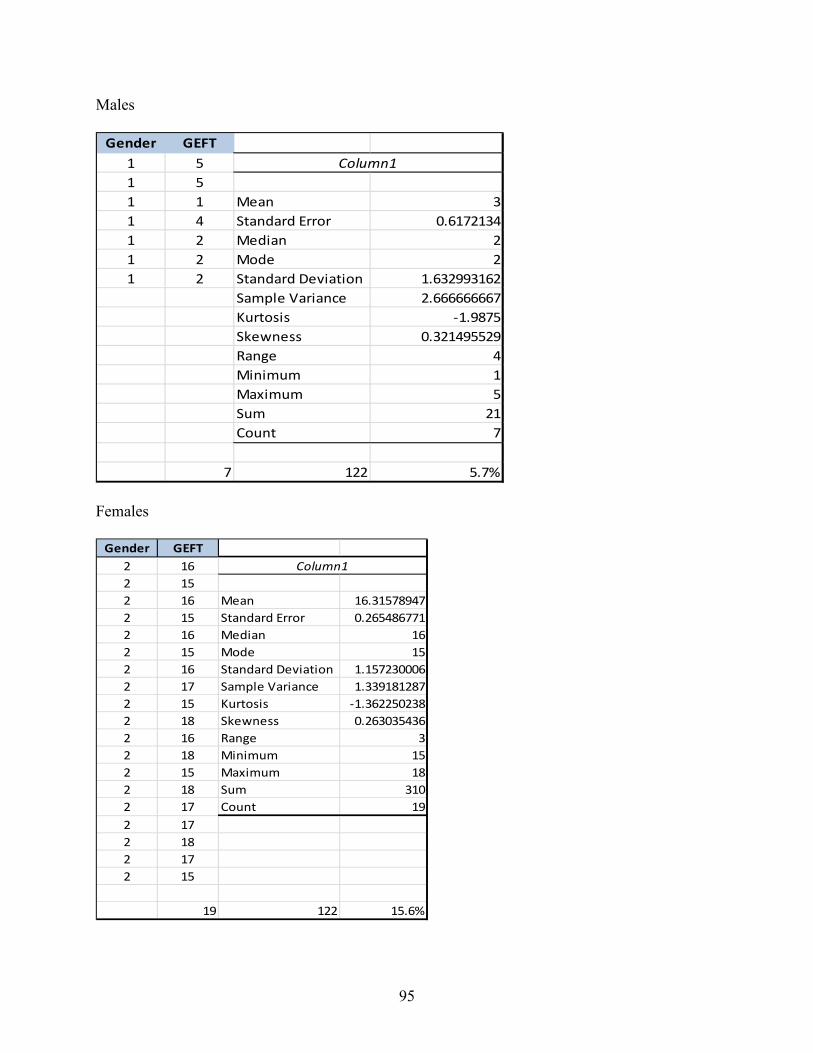
95
Males
Gender GEFT1 5 Column11 51 1 Mean 31 4 Standard Error 0.61721341 2 Median 21 2 Mode 21 2 Standard Deviation 1.632993162
Sample Variance 2.666666667Kurtosis -1.9875Skewness 0.321495529Range 4Minimum 1Maximum 5Sum 21Count 7
7 122 5.7%
Females
Gender GEFT2 16 Column12 152 16 Mean 16.315789472 15 Standard Error 0.2654867712 16 Median 162 15 Mode 152 16 Standard Deviation 1.1572300062 17 Sample Variance 1.3391812872 15 Kurtosis -1.3622502382 18 Skewness 0.2630354362 16 Range 32 18 Minimum 152 15 Maximum 182 18 Sum 3102 17 Count 192 172 182 172 15
19 122 15.6%

96
Mid-Range GEFT Scores
Males & Females
Column1
Mean 9.647058824Standard Error 0.29164899Median 10Mode 6Standard Deviation 2.404999183Sample Variance 5.784021071Kurtosis -1.05784774Skewness -0.04055415Range 8Minimum 6Maximum 14Sum 656Count 68
68 122 55.7%
Males
Gender GEFT1 10 Column11 91 6 Mean 9.751 12 Standard Error 0.652791211 12 Median 10.51 6 Mode 121 7 Standard Deviation 2.2613350841 12 Sample Variance 5.1136363641 11 Kurtosis -0.7959545681 11 Skewness -0.8172163481 11 Range 61 10 Minimum 6
Maximum 12Sum 117Count 12
12 122 9.8%

97
Females
Column1
Mean 9.625Standard Error 0.327884304Median 10Mode 6Standard Deviation 2.453661457Sample Variance 6.020454545Kurtosis -1.064920831Skewness 0.06952405Range 8Minimum 6Maximum 14Sum 539Count 56
56 122 45.9%

98
High GEFT Scores
Males & Females
Gender GEFT2 16 Column12 152 16 Mean 16.52 15 Standard Error 0.2184059282 16 Median 162 15 Mode 181 16 Standard Deviation 1.1962585352 16 Sample Variance 1.4310344831 18 Kurtosis -1.537777041 18 Skewness 0.064745761 16 Range 31 18 Minimum 152 17 Maximum 181 15 Sum 4952 15 Count 302 181 18 30 122 24.6%1 152 162 182 151 161 182 182 171 172 172 182 172 15

99
Males
Gender GEFT1 16 Column11 181 18 Mean 16.818181821 16 Standard Error 0.3770262061 18 Median 171 15 Mode 181 18 Standard Deviation 1.2504544631 15 Sample Variance 1.5636363641 16 Kurtosis -1.6955110871 18 Skewness -0.337861661 17 Range 3
Minimum 15Maximum 18Sum 185Count 11
11 122 9.0%
Females
Gender GEFT2 16 Column12 152 16 Mean 16.315789472 15 Standard Error 0.2654867712 16 Median 162 15 Mode 152 16 Standard Deviation 1.1572300062 17 Sample Variance 1.3391812872 15 Kurtosis -1.3622502382 18 Skewness 0.2630354362 16 Range 32 18 Minimum 152 15 Maximum 182 18 Sum 3102 17 Count 192 172 182 172 15
19 122 15.6%

100
describe(TotalData) var n mean sd median trimmed mad min max range skew kurtosis se Gender 1 123 1.75 0.44 2 1.81 0.00 1 2 1 -1.13 -0.73 0.04 Age 2 123 44.47 9.98 44 44.51 13.34 25 66 41 0.00 -1.05 0.90 Ethnicitgy 3 123 1.36 0.87 1 1.11 0.00 1 5 4 2.44 4.91 0.08 YrsRN 4 123 17.96 10.43 16 17.29 10.38 1 46 45 0.57 -0.52 0.94 ProfCert 5 123 1.40 1.14 1 1.25 0.00 0 6 6 1.50 2.84 0.10 CritCare 6 123 0.46 0.50 0 0.44 0.00 0 1 1 0.18 -1.98 0.05 GEFT 7 122 10.07 4.98 10 10.20 5.93 0 18 18 -0.14 -0.95 0.45 Ship 8 122 16.04 4.28 16 16.01 4.45 5 25 20 -0.06 -0.33 0.39 NsProf 9 117 33.63 6.18 34 34.23 4.45 13 47 34 -0.93 1.05 0.57
model1 = lm(GEFT ~ Gender, data = TotalData) > summary(model1) Call: lm(formula = GEFT ~ Gender, data = TotalData) Residuals: Min 1Q Median 3Q Max -9.9032 -3.7912 0.2088 4.1808 8.2088 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 12.015 1.864 6.446 2.51e-09 *** Gender -1.112 1.036 -1.073 0.285 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 4.981 on 120 degrees of freedom (1 observation deleted due to missingness) Multiple R-squared: 0.009511, Adjusted R-squared: 0.001257 F-statistic: 1.152 on 1 and 120 DF, p-value: 0.2852 model2 = lm(Ship ~ Gender, data = TotalData) > summary(model2) Call: lm(formula = Ship ~ Gender, data = TotalData) Residuals: Min 1Q Median 3Q Max -10.6593 -3.0358 0.3407 2.8387 9.3407

101
Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 18.6632 1.5885 11.749 <2e-16 *** Gender -1.5019 0.8828 -1.701 0.0915 . --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 4.245 on 120 degrees of freedom (1 observation deleted due to missingness) Multiple R-squared: 0.02355, Adjusted R-squared: 0.01541 F-statistic: 2.894 on 1 and 120 DF, p-value: 0.09148
Cohen’s D GEFT – 0.22 CI 95% -0.19, 0.63 Ship – 0.35 CI 95% -0.06, 0.76
describe(TotalData) var n mean sd median trimmed mad min max range skew kurtosis se Gender 1 123 1.75 0.44 2 1.81 0.00 1 2 1 -1.13 -0.73 0.04 Age 2 123 44.47 9.98 44 44.51 13.34 25 66 41 0.00 -1.05 0.90 Ethnicitgy 3 123 1.36 0.87 1 1.11 0.00 1 5 4 2.44 4.91 0.08 YrsRN 4 123 17.96 10.43 16 17.29 10.38 1 46 45 0.57 -0.52 0.94 ProfCert 5 123 1.40 1.14 1 1.25 0.00 0 6 6 1.50 2.84 0.10 CritCare 6 123 0.46 0.50 0 0.44 0.00 0 1 1 0.18 -1.98 0.05

102
GEFT 7 122 10.07 4.98 10 10.20 5.93 0 18 18 -0.14 -0.95 0.45 Ship 8 122 16.04 4.28 16 16.01 4.45 5 25 20 -0.06 -0.33 0.39 NsProf 9 117 33.63 6.18 34 34.23 4.45 13 47 34 -0.93 1.05 0.57
model2 = lm(NsProf ~ Gender + YrsRN + CritCare + Ship + GEFT + ProfCert, data = TotalData) > summary(model2) Call: lm(formula = NsProf ~ Gender + YrsRN + CritCare + Ship + GEFT + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max -22.1379 -2.2533 0.4572 4.1180 14.2843 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 30.69585 3.96380 7.744 5.54e-12 *** Gender -1.05033 1.42881 -0.735 0.4639 YrsRN 0.08664 0.05821 1.488 0.1395 CritCare 0.49184 1.22044 0.403 0.6877 Ship -0.07582 0.16266 -0.466 0.6421 GEFT 0.25543 0.14047 1.818 0.0718 . ProfCert 1.21518 0.55285 2.198 0.0301 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.075 on 108 degrees of freedom (8 observations deleted due to missingness) Multiple R-squared: 0.0989, Adjusted R-squared: 0.04884 F-statistic: 1.976 on 6 and 108 DF, p-value: 0.07537
confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) 22.83890356 38.5527959 Gender -3.88247574 1.7818076 YrsRN -0.02874094 0.2020290 CritCare -1.92728481 2.9109738 Ship -0.39823848 0.2466047

103
GEFT -0.02299918 0.5338622 ProfCert 0.11934469 2.3110143 lm.beta(model2) Gender YrsRN CritCare Ship GEFT ProfCert -0.07354619 0.14937463 0.03963988 -0.05188952 0.19748704 0.20788059
Ns Knowledge - Ship
model2 = lm(NsProf ~ Gender + YrsRN + CritCare + Ship + ProfCert, data = TotalData) > > summary(model2) Call: lm(formula = NsProf ~ Gender + YrsRN + CritCare + Ship + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max -22.7190 -2.4493 0.5181 4.3084 14.8793 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 31.10673 3.98762 7.801 3.8e-12 *** Gender -0.97839 1.43945 -0.680 0.4981 YrsRN 0.07567 0.05793 1.306 0.1942 CritCare 0.52446 1.22328 0.429 0.6690 Ship 0.07143 0.14346 0.498 0.6195 ProfCert 1.05517 0.52707 2.002 0.0478 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.123 on 110 degrees of freedom (7 observations deleted due to missingness) Multiple R-squared: 0.06757, Adjusted R-squared: 0.02519 F-statistic: 1.594 on 5 and 110 DF, p-value: 0.1676 > confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) 23.20421058 39.0092448 Gender -3.83103763 1.8742485 YrsRN -0.03913260 0.1904771 CritCare -1.89978828 2.9487004 Ship -0.21287995 0.3557409 ProfCert 0.01064035 2.0997091

104
> lm.beta(model2) Gender YrsRN CritCare Ship ProfCert -0.06860544 0.13046020 0.04243895 0.04888565 0.18958015
Ns Knowledge – GEFT
model3 = lm(NsProf ~ Gender + YrsRN + CritCare + GEFT + ProfCert, data = TotalData) > > summary(model3) Call: lm(formula = NsProf ~ Gender + YrsRN + CritCare + GEFT + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max -22.3615 -2.2209 0.5429 4.1619 14.6736 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 29.86885 3.19356 9.353 1.19e-15 *** Gender -0.96315 1.41329 -0.681 0.4970 YrsRN 0.08840 0.05644 1.566 0.1202 CritCare 0.41159 1.20904 0.340 0.7342 GEFT 0.20577 0.11976 1.718 0.0886 . ProfCert 1.20742 0.54202 2.228 0.0279 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.04 on 110 degrees of freedom (7 observations deleted due to missingness) Multiple R-squared: 0.09392, Adjusted R-squared: 0.05274 F-statistic: 2.281 on 5 and 110 DF, p-value: 0.05147 > lm.beta(model3) Gender YrsRN CritCare GEFT ProfCert -0.06749675 0.15232735 0.03328598 0.16194206 0.20677670 > confint(model3, level = 0.95) 2.5 % 97.5 % (Intercept) 23.53996784 36.197739 Gender -3.76395679 1.837648 YrsRN -0.02344788 0.200243 CritCare -1.98445256 2.807630

105
GEFT -0.03155930 0.443096 ProfCert 0.13325819 2.281590
Nurse Knowledge
model4 = lm(NsProf ~ YrsRN + CritCare + GEFT + ProfCert, data = TotalData) > > summary(model4) Call: lm(formula = NsProf ~ YrsRN + CritCare + GEFT + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max -22.7051 -2.4607 0.5967 4.2388 14.2100 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 28.15238 1.95870 14.373 <2e-16 *** YrsRN 0.08205 0.05553 1.478 0.1423 CritCare 0.70953 1.12451 0.631 0.5294 GEFT 0.20770 0.11943 1.739 0.0848 . ProfCert 1.19471 0.54040 2.211 0.0291 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.025 on 111 degrees of freedom (7 observations deleted due to missingness) Multiple R-squared: 0.0901, Adjusted R-squared: 0.05731 F-statistic: 2.748 on 4 and 111 DF, p-value: 0.0318 > confint(model4, level = 0.95) 2.5 % 97.5 % (Intercept) 24.27108366 32.0336722 YrsRN -0.02798200 0.1920910 CritCare -1.51875856 2.9378241 GEFT -0.02896921 0.4443602 ProfCert 0.12387992 2.2655385 > lm.beta(model4) YrsRN CritCare GEFT ProfCert 0.1413970 0.0573813 0.1634587 0.2045992

106
Nurse Knowledge
model5 = lm(NsProf ~ YrsRN + CritCare + Ship + ProfCert, data = TotalData) > > summary(model5) Call: lm(formula = NsProf ~ YrsRN + CritCare + Ship + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max -23.0748 -2.6421 0.5852 4.2991 14.4666 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 29.22248 2.85943 10.220 <2e-16 *** YrsRN 0.07022 0.05723 1.227 0.2225 CritCare 0.82338 1.13872 0.723 0.4712 Ship 0.08083 0.14245 0.567 0.5716 ProfCert 1.03672 0.52510 1.974 0.0508 . --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.109 on 111 degrees of freedom (7 observations deleted due to missingness) Multiple R-squared: 0.06366, Adjusted R-squared: 0.02991 F-statistic: 1.887 on 4 and 111 DF, p-value: 0.1178 > lm.beta(model5) YrsRN CritCare Ship ProfCert 0.12105193 0.06662802 0.05531544 0.18626508 > confint(model5, level = 0.95) 2.5 % 97.5 % (Intercept) 23.556321222 34.8886434 YrsRN -0.043194614 0.1836248 CritCare -1.433057871 3.0798220 Ship -0.201447312 0.3630983 ProfCert -0.003789251 2.0772363
GEFT and Gender
Females
describe(FeGEFT) var n mean sd median trimmed mad min max range skew kurtosis se

107
Gender 1 92 2.00 0.00 2 2.0 0.00 2 2 0 NaN NaN 0.0 GEFT 2 91 9.79 4.76 10 9.9 5.93 0 18 18 -0.13 -0.81 0.5 Males
> describe(MaleGEFT) var n mean sd median trimmed mad min max range skew kurtosis se Gender 1 31 1.0 0.00 1 1.00 0.00 1 1 0 NaN NaN 0.00 GEFT 2 31 10.9 5.61 11 11.16 7.41 1 18 17 -0.28 -1.32 1.01
summary(MaleGEFT) Gender GEFT Min. :1 Min. : 1.0 1st Qu.:1 1st Qu.: 6.0 Median :1 Median :11.0 Mean :1 Mean :10.9 3rd Qu.:1 3rd Qu.:16.0 Max. :1 Max. :18.0 > summary(FeGEFT) Gender GEFT Min. :2 Min. : 0.000 1st Qu.:2 1st Qu.: 6.000 Median :2 Median :10.000 Mean :2 Mean : 9.791 3rd Qu.:2 3rd Qu.:13.000 Max. :2 Max. :18.000 NA's :1
model2 = lm(NsProf ~ Gender + YrsRN + CritCare + Ship + GEFT + ProfCert, data = TotalData) > summary(model2) Call: lm(formula = NsProf ~ Gender + YrsRN + CritCare + Ship + GEFT + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max -22.1379 -2.2533 0.4572 4.1180 14.2843

108
Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 30.69585 3.96380 7.744 5.54e-12 *** Gender -1.05033 1.42881 -0.735 0.4639 YrsRN 0.08664 0.05821 1.488 0.1395 CritCare 0.49184 1.22044 0.403 0.6877 Ship -0.07582 0.16266 -0.466 0.6421 GEFT 0.25543 0.14047 1.818 0.0718 . ProfCert 1.21518 0.55285 2.198 0.0301 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.075 on 108 degrees of freedom (8 observations deleted due to missingness) Multiple R-squared: 0.0989, Adjusted R-squared: 0.04884 F-statistic: 1.976 on 6 and 108 DF, p-value: 0.07537
confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) 22.83890356 38.5527959 Gender -3.88247574 1.7818076 YrsRN -0.02874094 0.2020290 CritCare -1.92728481 2.9109738 Ship -0.39823848 0.2466047 GEFT -0.02299918 0.5338622 ProfCert 0.11934469 2.3110143 lm.beta(model2) Gender YrsRN CritCare Ship GEFT ProfCert -0.07354619 0.14937463 0.03963988 -0.05188952 0.19748704 0.20788059
model2 = lm(NsProf ~ Gender + YrsRN + CritCare + Ship + ProfCert, data = TotalData) > > summary(model2) Call: lm(formula = NsProf ~ Gender + YrsRN + CritCare + Ship + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max

109
-22.7190 -2.4493 0.5181 4.3084 14.8793 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 31.10673 3.98762 7.801 3.8e-12 *** Gender -0.97839 1.43945 -0.680 0.4981 YrsRN 0.07567 0.05793 1.306 0.1942 CritCare 0.52446 1.22328 0.429 0.6690 Ship 0.07143 0.14346 0.498 0.6195 ProfCert 1.05517 0.52707 2.002 0.0478 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.123 on 110 degrees of freedom (7 observations deleted due to missingness) Multiple R-squared: 0.06757, Adjusted R-squared: 0.02519 F-statistic: 1.594 on 5 and 110 DF, p-value: 0.1676 > confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) 23.20421058 39.0092448 Gender -3.83103763 1.8742485 YrsRN -0.03913260 0.1904771 CritCare -1.89978828 2.9487004 Ship -0.21287995 0.3557409 ProfCert 0.01064035 2.0997091 > lm.beta(model2) Gender YrsRN CritCare Ship ProfCert -0.06860544 0.13046020 0.04243895 0.04888565 0.18958015
model3 = lm(NsProf ~ Gender + YrsRN + CritCare + GEFT + ProfCert, data = TotalData) > > summary(model3) Call: lm(formula = NsProf ~ Gender + YrsRN + CritCare + GEFT + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max -22.3615 -2.2209 0.5429 4.1619 14.6736 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 29.86885 3.19356 9.353 1.19e-15 ***

110
Gender -0.96315 1.41329 -0.681 0.4970 YrsRN 0.08840 0.05644 1.566 0.1202 CritCare 0.41159 1.20904 0.340 0.7342 GEFT 0.20577 0.11976 1.718 0.0886 . ProfCert 1.20742 0.54202 2.228 0.0279 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.04 on 110 degrees of freedom (7 observations deleted due to missingness) Multiple R-squared: 0.09392, Adjusted R-squared: 0.05274 F-statistic: 2.281 on 5 and 110 DF, p-value: 0.05147 > lm.beta(model3) Gender YrsRN CritCare GEFT ProfCert -0.06749675 0.15232735 0.03328598 0.16194206 0.20677670 > confint(model3, level = 0.95) 2.5 % 97.5 % (Intercept) 23.53996784 36.197739 Gender -3.76395679 1.837648 YrsRN -0.02344788 0.200243 CritCare -1.98445256 2.807630 GEFT -0.03155930 0.443096 ProfCert 0.13325819 2.281590
Nurse Knowledge
model4 = lm(NsProf ~ YrsRN + CritCare + GEFT + ProfCert, data = TotalData) > > summary(model4) Call: lm(formula = NsProf ~ YrsRN + CritCare + GEFT + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max -22.7051 -2.4607 0.5967 4.2388 14.2100 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 28.15238 1.95870 14.373 <2e-16 *** YrsRN 0.08205 0.05553 1.478 0.1423 CritCare 0.70953 1.12451 0.631 0.5294

111
GEFT 0.20770 0.11943 1.739 0.0848 . ProfCert 1.19471 0.54040 2.211 0.0291 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.025 on 111 degrees of freedom (7 observations deleted due to missingness) Multiple R-squared: 0.0901, Adjusted R-squared: 0.05731 F-statistic: 2.748 on 4 and 111 DF, p-value: 0.0318 > confint(model4, level = 0.95) 2.5 % 97.5 % (Intercept) 24.27108366 32.0336722 YrsRN -0.02798200 0.1920910 CritCare -1.51875856 2.9378241 GEFT -0.02896921 0.4443602 ProfCert 0.12387992 2.2655385 > lm.beta(model4) YrsRN CritCare GEFT ProfCert 0.1413970 0.0573813 0.1634587 0.2045992
model5 = lm(NsProf ~ YrsRN + CritCare + Ship + ProfCert, data = TotalData) > > summary(model5) Call: lm(formula = NsProf ~ YrsRN + CritCare + Ship + ProfCert, data = TotalData) Residuals: Min 1Q Median 3Q Max -23.0748 -2.6421 0.5852 4.2991 14.4666 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 29.22248 2.85943 10.220 <2e-16 *** YrsRN 0.07022 0.05723 1.227 0.2225 CritCare 0.82338 1.13872 0.723 0.4712 Ship 0.08083 0.14245 0.567 0.5716 ProfCert 1.03672 0.52510 1.974 0.0508 . --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 6.109 on 111 degrees of freedom

112
(7 observations deleted due to missingness) Multiple R-squared: 0.06366, Adjusted R-squared: 0.02991 F-statistic: 1.887 on 4 and 111 DF, p-value: 0.1178 > lm.beta(model5) YrsRN CritCare Ship ProfCert 0.12105193 0.06662802 0.05531544 0.18626508 > confint(model5, level = 0.95) 2.5 % 97.5 % (Intercept) 23.556321222 34.8886434 YrsRN -0.043194614 0.1836248 CritCare -1.433057871 3.0798220 Ship -0.201447312 0.3630983 ProfCert -0.003789251 2.0772363
describe(FeGEFT) var n mean sd median trimmed mad min max range skew kurtosis se Gender 1 92 2.00 0.00 2 2.0 0.00 2 2 0 NaN NaN 0.0 GEFT 2 91 9.79 4.76 10 9.9 5.93 0 18 18 -0.13 -0.81 0.5 Males
> describe(MaleGEFT) var n mean sd median trimmed mad min max range skew kurtosis se Gender 1 31 1.0 0.00 1 1.00 0.00 1 1 0 NaN NaN 0.00 GEFT 2 31 10.9 5.61 11 11.16 7.41 1 18 17 -0.28 -1.32 1.01
summary(MaleGEFT) Gender GEFT Min. :1 Min. : 1.0 1st Qu.:1 1st Qu.: 6.0 Median :1 Median :11.0 Mean :1 Mean :10.9 3rd Qu.:1 3rd Qu.:16.0 Max. :1 Max. :18.0 > summary(FeGEFT) Gender GEFT

113
Min. :2 Min. : 0.000 1st Qu.:2 1st Qu.: 6.000 Median :2 Median :10.000 Mean :2 Mean : 9.791 3rd Qu.:2 3rd Qu.:13.000 Max. :2 Max. :18.000 NA's :1 model1 = lm(ProfCert ~ Gender + Age + YrsRN + CritCare + NsProf, data = TotalData) > summary(model1) Call: lm(formula = ProfCert ~ Gender + Age + YrsRN + CritCare + NsProf, data = TotalData) Residuals: Min 1Q Median 3Q Max -1.6855 -0.6731 -0.2352 0.4012 4.4062 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) -1.57331 0.99094 -1.588 0.1152 Gender 0.20355 0.25477 0.799 0.4260 Age 0.03438 0.01932 1.780 0.0779 . YrsRN -0.01384 0.01863 -0.743 0.4591 CritCare 0.14856 0.21465 0.692 0.4903 NsProf 0.03654 0.01644 2.223 0.0283 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.078 on 111 degrees of freedom (6 observations deleted due to missingness) Multiple R-squared: 0.09855, Adjusted R-squared: 0.05794 F-statistic: 2.427 on 5 and 111 DF, p-value: 0.0396 lm.beta(model1) Gender Age YrsRN CritCare NsProf 0.07944383 0.31186643 -0.13264569 0.06708066 0.20324641 > confint(model1, level = 0.95) 2.5 % 97.5 % (Intercept) -3.536919623 0.39029637 Gender -0.301284531 0.70839200 Age -0.003898324 0.07265873 YrsRN -0.050757323 0.02307591 CritCare -0.276785062 0.57390217

114
NsProf 0.003962146 0.06912764
model2 = lm(ProfCert ~ Age + NsProf, data = TotalData) > summary(model2) Call: lm(formula = ProfCert ~ Age + NsProf, data = TotalData) Residuals: Min 1Q Median 3Q Max -1.5572 -0.6006 -0.2527 0.4078 4.5680 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) -0.832147 0.672730 -1.237 0.2186 Age 0.022658 0.009905 2.288 0.0240 * NsProf 0.035328 0.016155 2.187 0.0308 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.07 on 114 degrees of freedom (6 observations deleted due to missingness) Multiple R-squared: 0.08891, Adjusted R-squared: 0.07292 F-statistic: 5.562 on 2 and 114 DF, p-value: 0.004956 > lm.beta(model2) Age NsProf 0.2055346 0.1964812 > confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) -2.164819390 0.50052600 Age 0.003037082 0.04227926 NsProf 0.003325738 0.06733121 lm.beta(model2)
confint(model2, level = 0.95)
model4 = lm(ProfCert ~ YrsRN + Gender + Age + CritCare + NsProf + Ship + GEFT, data = TotalData) > summary(model4)

115
Call: lm(formula = ProfCert ~ YrsRN + Gender + Age + CritCare + NsProf + Ship + GEFT, data = TotalData) Residuals: Min 1Q Median 3Q Max -1.8969 -0.5858 -0.1822 0.4099 4.4051 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) -2.009226 1.090808 -1.842 0.0683 . YrsRN -0.002661 0.018377 -0.145 0.8851 Gender 0.202942 0.245521 0.827 0.4103 Age 0.025485 0.019155 1.331 0.1862 CritCare 0.197693 0.206441 0.958 0.3404 NsProf 0.035979 0.015984 2.251 0.0264 * Ship 0.048909 0.027526 1.777 0.0784 . GEFT -0.019960 0.024155 -0.826 0.4104 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.031 on 107 degrees of freedom (8 observations deleted due to missingness) Multiple R-squared: 0.1217, Adjusted R-squared: 0.0642 F-statistic: 2.117 on 7 and 107 DF, p-value: 0.04776 > lm.beta(model4) YrsRN Gender Age CritCare NsProf Ship GEFT -0.02681870 0.08306735 0.24148272 0.09313683 0.21031920 0.19567378 -0.09021042 > confint(model4, level = 0.95) 2.5 % 97.5 % (Intercept) -4.171624838 0.15317354 YrsRN -0.039090750 0.03376841 Gender -0.283774500 0.68965777 Age -0.012486292 0.06345688 CritCare -0.211553002 0.60693823 NsProf 0.004292693 0.06766586 Ship -0.005658458 0.10347728 GEFT -0.067844033 0.02792352
model4 = lm(ProfCert ~ YrsRN + Gender + Age + CritCare + NsProf , data = TotalData) > summary(model4)

116
Call: lm(formula = ProfCert ~ YrsRN + Gender + Age + CritCare + NsProf, data = TotalData) Residuals: Min 1Q Median 3Q Max -1.6855 -0.6731 -0.2352 0.4012 4.4062 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) -1.57331 0.99094 -1.588 0.1152 YrsRN -0.01384 0.01863 -0.743 0.4591 Gender 0.20355 0.25477 0.799 0.4260 Age 0.03438 0.01932 1.780 0.0779 . CritCare 0.14856 0.21465 0.692 0.4903 NsProf 0.03654 0.01644 2.223 0.0283 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.078 on 111 degrees of freedom (6 observations deleted due to missingness) Multiple R-squared: 0.09855, Adjusted R-squared: 0.05794 F-statistic: 2.427 on 5 and 111 DF, p-value: 0.0396 > lm.beta(model4) YrsRN Gender Age CritCare NsProf -0.13264569 0.07944383 0.31186643 0.06708066 0.20324641 > confint(model4, level = 0.95) 2.5 % 97.5 % (Intercept) -3.536919623 0.39029637 YrsRN -0.050757323 0.02307591 Gender -0.301284531 0.70839200 Age -0.003898324 0.07265873 CritCare -0.276785062 0.57390217 NsProf 0.003962146 0.06912764 >
model4 = lm(ProcCert ~ YrsRN + Educ + Gender + Age + CritCare + NsProf + Ship + GEFT, data = NewStudyData) > summary(model4)

117
Call: lm(formula = ProcCert ~ YrsRN + Educ + Gender + Age + CritCare + NsProf + Ship + GEFT, data = NewStudyData) Residuals: Min 1Q Median 3Q Max -1.9317 -0.5655 -0.1989 0.4084 4.2033 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 0.11067 1.03005 0.107 0.9147 YrsRN 0.01269 0.01064 1.192 0.2365 Educ -0.01521 0.08602 -0.177 0.8601 Gender -0.16483 0.25045 -0.658 0.5122 Age -0.01462 0.01055 -1.385 0.1695 CritCare -0.05261 0.21889 -0.240 0.8106 NsProf 0.03829 0.01784 2.147 0.0346 * Ship 0.06350 0.03062 2.074 0.0411 * GEFT -0.03275 0.02780 -1.178 0.2421 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.02 on 86 degrees of freedom (28 observations deleted due to missingness) Multiple R-squared: 0.1238, Adjusted R-squared: 0.04233 F-statistic: 1.519 on 8 and 86 DF, p-value: 0.1624 > lm.beta(model4) YrsRN Educ Gender Age CritCare NsProf Ship GEFT 0.12894753 -0.01814479 -0.06907019 -0.14125591 -0.02529827 0.22729902 0.26357211 -0.15220040 > confint(model4, level = 0.95) 2.5 % 97.5 % (Intercept) -1.937007032 2.158346020 YrsRN -0.008468674 0.033844463 Educ -0.186204806 0.155791324 Gender -0.662712892 0.333056714 Age -0.035592551 0.006358147 CritCare -0.487738994 0.382522263 NsProf 0.002834153 0.073748748 Ship 0.002630272 0.124367029 GEFT -0.088010509 0.022519135

118
model4 = lm(ProcCert ~ YrsRN + Educ + Gender + Age + NsProf + Ship + GEFT, data = NewStudyData) > summary(model4) Call: lm(formula = ProcCert ~ YrsRN + Educ + Gender + Age + NsProf + Ship + GEFT, data = NewStudyData) Residuals: Min 1Q Median 3Q Max -1.9140 -0.5980 -0.1903 0.3847 4.2331 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 0.06472 1.00666 0.064 0.9489 YrsRN 0.01246 0.01054 1.182 0.2404 Educ -0.01500 0.08555 -0.175 0.8612 Gender -0.15061 0.24205 -0.622 0.5354 Age -0.01478 0.01047 -1.412 0.1615 NsProf 0.03860 0.01769 2.182 0.0318 * Ship 0.06384 0.03042 2.099 0.0387 * GEFT -0.03358 0.02743 -1.224 0.2243 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.015 on 87 degrees of freedom (28 observations deleted due to missingness) Multiple R-squared: 0.1232, Adjusted R-squared: 0.0527 F-statistic: 1.747 on 7 and 87 DF, p-value: 0.1086 > lm.beta(model4) YrsRN Educ Gender Age NsProf Ship GEFT 0.12666555 -0.01790063 -0.06311281 -0.14287028 0.22913526 0.26500406 -0.15606063 > confint(model4, level = 0.95) 2.5 % 97.5 % (Intercept) -1.936124683 2.065565878 YrsRN -0.008493669 0.033420384 Educ -0.185035475 0.155031234 Gender -0.631705658 0.330482694 Age -0.035596987 0.006028473 NsProf 0.003433716 0.073767859 Ship 0.003382228 0.124305034 GEFT -0.088105747 0.020953327 >

119
model2 = lm(ProfCert ~ NsProf + Educ + YrsRN, data = AllData) > summary(model2) Call: lm(formula = ProfCert ~ NsProf + Educ + YrsRN, data = AllData) Residuals: Min 1Q Median 3Q Max -1.5597 -0.6128 -0.2424 0.3300 4.5383 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) -0.225492 0.599112 -0.376 0.7073 NsProf 0.034963 0.016466 2.123 0.0359 * Educ 0.058848 0.095107 0.619 0.5373 YrsRN 0.015109 0.009556 1.581 0.1166 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.085 on 113 degrees of freedom (6 observations deleted due to missingness) Multiple R-squared: 0.07161, Adjusted R-squared: 0.04696 F-statistic: 2.905 on 3 and 113 DF, p-value: 0.03786 > lm.beta(model2) NsProf Educ YrsRN 0.19444816 0.05623644 0.14480382 > confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) -1.412440079 0.96145679 NsProf 0.002341278 0.06758456 Educ -0.129575208 0.24727111 YrsRN -0.003822160 0.03404081
model2 = lm(Educ ~ ProfCert + NsProf + YrsRN + GEFT + Ship, data = AllDataEduc) > summary(model2) Call: lm(formula = Educ ~ ProfCert + NsProf + YrsRN + GEFT + Ship, data = AllDataEduc) Residuals:

120
Min 1Q Median 3Q Max -1.29682 -0.32760 -0.03629 0.67472 1.13892 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 2.4998021 0.4430133 5.643 1.34e-07 *** ProfCert 0.0434170 0.0628704 0.691 0.4913 NsProf 0.0020605 0.0107025 0.193 0.8477 YrsRN 0.0003972 0.0064917 0.061 0.9513 GEFT 0.0214634 0.0159041 1.350 0.1800 Ship -0.0428175 0.0180777 -2.369 0.0196 * --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 0.6789 on 109 degrees of freedom (8 observations deleted due to missingness) Multiple R-squared: 0.05524, Adjusted R-squared: 0.01191 F-statistic: 1.275 on 5 and 109 DF, p-value: 0.28 > lm.beta(model2) ProfCert NsProf YrsRN GEFT Ship 0.067735375 0.018791049 0.006244613 0.151336821 -0.267249361 > confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) 1.62176423 3.377839976 ProfCert -0.08119005 0.168024140 NsProf -0.01915155 0.023272521 YrsRN -0.01246922 0.013263580 GEFT -0.01005799 0.052984808 Ship -0.07864686 -0.006988115 model2 = lm(ProfCert ~ Educ + NsProf + YrsRN + GEFT + Ship, data = AllData) > summary(model2) Call: lm(formula = ProfCert ~ Educ + NsProf + YrsRN + GEFT + Ship, data = AllData) Residuals: Min 1Q Median 3Q Max -1.8143 -0.5921 -0.1408 0.3589 4.5827 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) -1.021736 0.719901 -1.419 0.1587 Educ 0.100837 0.093269 1.081 0.2820 NsProf 0.035002 0.015871 2.205 0.0295 *

121
YrsRN 0.018641 0.009674 1.927 0.0566 . GEFT -0.022070 0.024205 -0.912 0.3639 Ship 0.050308 0.027702 1.816 0.0721 . --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.029 on 109 degrees of freedom (8 observations deleted due to missingness) Multiple R-squared: 0.1086, Adjusted R-squared: 0.06774 F-statistic: 2.657 on 5 and 109 DF, p-value: 0.02631 > lm.beta(model2) Educ NsProf YrsRN GEFT Ship 0.10032061 0.20460880 0.18786239 -0.09974584 0.20127049 > confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) -2.448556732 0.40508544 Educ -0.084019513 0.28569302 NsProf 0.003547526 0.06645727 YrsRN -0.000532802 0.03781531 GEFT -0.070043429 0.02590324 Ship -0.004596184 0.10521284
summary(AllData) Age Gender Educ YrsRN ProfCert CritCare GEFT Ship NsProf Min. :25.00 Min. :1.000 Min. :1.000 Min. : 1.00 Min. :0.000 Min. :0.0000 Min. : 0.00 Min. : 5.00 Min. :13.00 1st Qu.:36.00 1st Qu.:1.500 1st Qu.:2.000 1st Qu.:10.00 1st Qu.:1.000 1st Qu.:0.0000 1st Qu.: 6.00 1st Qu.:13.25 1st Qu.:31.00 Median :44.00 Median :2.000 Median :2.000 Median :16.00 Median :1.000 Median :0.0000 Median :10.00 Median :16.00 Median :34.00 Mean :44.47 Mean :1.748 Mean :2.447 Mean :17.96 Mean :1.398 Mean :0.4553 Mean :10.07 Mean :16.04 Mean :33.63 3rd Qu.:53.00 3rd Qu.:2.000 3rd Qu.:4.000 3rd Qu.:25.00 3rd Qu.:2.000 3rd Qu.:1.0000 3rd Qu.:14.75 3rd Qu.:19.00 3rd Qu.:37.00 Max. :66.00 Max. :2.000 Max. :4.000 Max. :46.00 Max. :6.000 Max. :1.0000 Max. :18.00 Max. :25.00 Max. :47.00 NA's :1 NA's :1 NA's :6 > describe(AllData) var n mean sd median trimmed mad min max range skew kurtosis se

122
Age 1 123 44.47 9.98 44 44.51 13.34 25 66 41 0.00 -1.05 0.90 Gender 2 123 1.75 0.44 2 1.81 0.00 1 2 1 -1.13 -0.73 0.04 Educ 3 123 2.45 1.08 2 2.43 1.48 1 4 3 0.41 -1.22 0.10 YrsRN 4 123 17.96 10.43 16 17.29 10.38 1 46 45 0.57 -0.52 0.94 ProfCert 5 123 1.40 1.14 1 1.25 0.00 0 6 6 1.50 2.84 0.10 CritCare 6 123 0.46 0.50 0 0.44 0.00 0 1 1 0.18 -1.98 0.05 GEFT 7 122 10.07 4.98 10 10.20 5.93 0 18 18 -0.14 -0.95 0.45 Ship 8 122 16.04 4.28 16 16.01 4.45 5 25 20 -0.06 -0.33 0.39 NsProf 9 117 33.63 6.18 34 34.23 4.45 13 47 34 -0.93 1.05 0.57
model2 = lm(ProfCert ~ Educ + NsProf + YrsRN , data = AllData) > summary(model2) Call: lm(formula = ProfCert ~ Educ + NsProf + YrsRN, data = AllData) Residuals: Min 1Q Median 3Q Max -1.5597 -0.6128 -0.2424 0.3300 4.5383 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) -0.225492 0.599112 -0.376 0.7073 Educ 0.058848 0.095107 0.619 0.5373 NsProf 0.034963 0.016466 2.123 0.0359 * YrsRN 0.015109 0.009556 1.581 0.1166 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.085 on 113 degrees of freedom (6 observations deleted due to missingness) Multiple R-squared: 0.07161, Adjusted R-squared: 0.04696 F-statistic: 2.905 on 3 and 113 DF, p-value: 0.03786 > lm.beta(model2) Educ NsProf YrsRN 0.05623644 0.19444816 0.14480382 > confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) -1.412440079 0.96145679 Educ -0.129575208 0.24727111 NsProf 0.002341278 0.06758456

123
YrsRN -0.003822160 0.03404081
model2 = lm(Educ ~ ProfCert + NsProf + YrsRN , data = AllData) > summary(model2) Call: lm(formula = Educ ~ ProfCert + NsProf + YrsRN, data = AllData) Residuals: Min 1Q Median 3Q Max -1.6375 -0.5442 -0.3873 1.4403 1.7442 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 2.074273 0.558879 3.711 0.000321 *** ProfCert 0.057380 0.092735 0.619 0.537321 NsProf 0.006257 0.016570 0.378 0.706418 YrsRN 0.004013 0.009532 0.421 0.674573 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.071 on 113 degrees of freedom (6 observations deleted due to missingness) Multiple R-squared: 0.008735, Adjusted R-squared: -0.01758 F-statistic: 0.3319 on 3 and 113 DF, p-value: 0.8023
model2 = lm(ProfCert ~ Educ + YrsRN , data = AllData) > summary(model2) Call: lm(formula = ProfCert ~ Educ + YrsRN, data = AllData) Residuals: Min 1Q Median 3Q Max -1.6838 -0.5160 -0.2772 0.4798 4.7619 Coefficients: Estimate Std. Error t value Pr(>|t|)

124
(Intercept) 1.014680 0.303132 3.347 0.00109 ** Educ 0.040281 0.095667 0.421 0.67447 YrsRN 0.015876 0.009913 1.602 0.11189 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.139 on 120 degrees of freedom Multiple R-squared: 0.02309, Adjusted R-squared: 0.006811 F-statistic: 1.418 on 2 and 120 DF, p-value: 0.2461
model2 = lm(ProfCert ~ Educ + NsProf + YrsRN, data = AllData) > summary(model2) Call: lm(formula = ProfCert ~ Educ + NsProf + YrsRN, data = AllData) Residuals: Min 1Q Median 3Q Max -1.5597 -0.6128 -0.2424 0.3300 4.5383 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) -0.225492 0.599112 -0.376 0.7073 Educ 0.058848 0.095107 0.619 0.5373 NsProf 0.034963 0.016466 2.123 0.0359 * YrsRN 0.015109 0.009556 1.581 0.1166 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.085 on 113 degrees of freedom (6 observations deleted due to missingness) Multiple R-squared: 0.07161, Adjusted R-squared: 0.04696 F-statistic: 2.905 on 3 and 113 DF, p-value: 0.03786 > lm.beta(model2) Educ NsProf YrsRN 0.05623644 0.19444816 0.14480382 > confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) -1.412440079 0.96145679 Educ -0.129575208 0.24727111 NsProf 0.002341278 0.06758456 YrsRN -0.003822160 0.03404081

125
model2 = lm(Educ ~ ProfCert + NsProf + YrsRN, data = AllData) > summary(model2) Call: lm(formula = Educ ~ ProfCert + NsProf + YrsRN, data = AllData) Residuals: Min 1Q Median 3Q Max -1.6375 -0.5442 -0.3873 1.4403 1.7442 Coefficients: Estimate Std. Error t value Pr(>|t|) (Intercept) 2.074273 0.558879 3.711 0.000321 *** ProfCert 0.057380 0.092735 0.619 0.537321 NsProf 0.006257 0.016570 0.378 0.706418 YrsRN 0.004013 0.009532 0.421 0.674573 --- Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 Residual standard error: 1.071 on 113 degrees of freedom (6 observations deleted due to missingness) Multiple R-squared: 0.008735, Adjusted R-squared: -0.01758 F-statistic: 0.3319 on 3 and 113 DF, p-value: 0.8023 > lm.beta(model2) ProfCert NsProf YrsRN 0.06004501 0.03641581 0.04024327 > confint(model2, level = 0.95) 2.5 % 97.5 % (Intercept) 0.96703226 3.18151404 ProfCert -0.12634381 0.24110456 NsProf -0.02657075 0.03908515 YrsRN -0.01487203 0.02289758

126
APPENDIX D
EXTENDED LITERATURE REVIEW

127
Nursing Education
Three common avenues to obtain an RN license are a 2-year associate degree program
(ADN), a 3-year diploma program, and a 4-year BSN (Lawrence, 2011). Miner (2012)
challenges the nursing profession to abandon the multiple pathways in nursing education and
join in adopting the BSN as the entry level education required for nursing practice. The states of
New York and New Jersey have proposed all nurses, by 2020, have a minimum of a Bachelor of
Science degree in nursing to enter the profession (Maneval & Teeter, 2010).
A BSN education, although not the cure for all that is expected of nurses in the future,
does introduce nursing students to a wider range of competencies in areas such as quality
improvement, leadership, public health, and health care policy (Institute of Medicine [IOM],
2010). An increase in the number of nurses with a BSN would establish a workforce positioned
to achieve education at the master’s and doctoral levels (IOM, 2010). The number of doctoral
trained nurses must be doubled by 2020 to meet the needs for nurse researchers, primary care
providers, and nursing instructors (IOM, 2011, 2012). Currently, 13% of nurses have a graduate
degree in nursing; however, less than 1% of nurses have doctoral degrees (IOM, 21012).
Changes in Nursing
Role Changes
Over the past 50 years, changes in nursing such as those related to job demands,
technology, work environments, patient acuity, litigation, salaries, education, and uniforms have
dramatically impacted the role of the professional nurse (Blanche, 2010). In today’s health care
environment, nurses monitor complex physiological data, operate lifesaving equipment,
administer high cost health care programs and coordinate the delivery of multiple patient

128
services (Weld & Bibb, 2009). The high demands of academic knowledge and clinical expertise
are often unexpected to individuals new to the profession (Brodie et al., 2004).
Changes in Job Skills
Nurses must use critical thinking skills with assessment, interpretation, and decision
making to provide patient care, ensuring patient safety at all times. Clinical knowledge is
estimated to double every 18 months (van Terheyden, 2007). Medical practices,
pharmaceuticals, regulations and standards of care require constant assimilation of new
information. Health care professionals must stay in a continual mode of learning as the field of
health care is constantly changing (Hodges, 2011).
As health care technology advances and patients require higher levels of care, nurses
must incorporate new practices and workflows to meet the changes (Kalisch & Begeny, 2010).
Using integrating technology to improve clinical nursing practice enhances the quality of patient
care (Saba, 2001). Today’s nurse must use technology to support workflow as well as support
the patient’s use of increased technology (Bond, 2009). The technology required by nurses may
vary; however, the core skills of basic computer proficiency, information technology, and
information systems for health care practice that comprise the foundations of nursing informatics
are essential for all nurses (Bond, 2009).
Creation of EHRs (electronic health record) using CPOE (computerized physician order
entry) and interfacing of various electronic applications has created a complex and dynamic
work environment for nurses (IOM, 2011). Expansion of biometric devices such as automated
insulin pumps and implantable cardiac defibrillators require nurses to continually expand the use
of technology in patient care.

129
Skills required for professional nursing is complex and extensive. The practice of
nursing care is discipline specific, but also requires multidisciplinary knowledge in such areas as
respiratory therapy, pharmacy, rehabilitation, and surgery (Giuliano, Tyer-Viola, & Lopez,
2005). Nurses must be proactive problem solvers and collaborative interdisciplinary team
members (Hodges, 2011). Foundational science and math knowledge are required for nurses in
areas such as anatomy and physiology, pharmacology and human behavior. Registered nurses
working today extensively utilize skills in assessment, critical thinking, and communication and
must be able to act quickly and decisively.
The nurse is the last safety check in the chain of events from prescription to medication
administration, before reaching the patient (Leufer & Cleary-Holdforth, 2013). Nurses must use
basic math functions and algebraic equations to calculate doses of medications and determine
intravenous (IV) drip rates (Maag, 2004). Research has shown spatial visualization abilities to
be positively related with performance on math tasks, as well as tasks in science, technology, and
engineering (Hinze et al., 2013).
Nurses are associated with quality performance metrics and are therefore essential
members of every hospital quality team (Kohlbrenner, Whitelaw, & Cannaday, 2011). Nursing
performance is more important today than ever before as communities can access hospital
performance and outcome measures by accessing Hospital Consumer Assessment of Healthcare
Providers and Systems (HCAHPS) scores (Leibert, 2011). The Joint Commission Leadership
Standards identified RNs as the most important contributor of patient safety and quality
(Kohlbrenner et al., 2011)

130
Advances in Medical Care
Many advances in medical care have resulted in greater numbers of hospitalized patients,
more critically ill patients upon admission to hospitals, and aging patients as well as improved
survival from critical events (Kuehn, 2007; Lynn & Redman, 2005). Increased patient acuity
levels with shortened lengths of hospital stays create intensive and accelerated health care
processes (Hirschkorn, West, Hill, Cleary, & Hewlett, 2010). Nurses complete an average of
100 tasks per shift, with an interruption every 3 minutes, often resulting in cognitive overload
(Hendren, 2011). All of these improvements and changes rely on tremendous knowledge and a
skill set that allows the nursing professional to deliver optimal care demanded in such situations.
Gender Participation in Nursing
The current nursing workforce contains a disproportionate number of females. While
most disciplines within the health professional workforce have become more gender balanced,
the same has not been true for nursing. The number of men who become nurses has grown in the
last two decades however men account for only 7% of the current RN workforce (US
Department of Health and Human Services, 2010). Stereotypes, role support, and academic
acceptance are some challenges men encounter when entering the nursing profession (IOM,
2011). Moreover, there is little recognition of unique skills or abilities of males as nurses, and
the turnover rate for male nurses is twice that of females (Hsu, Chen, Yu, & Lou, 2010). While
more men are being drawn to nursing, especially as a second career, the field of nursing must
continue to recruit men as their unique perspectives and skills are important to the profession and
will help contribute additional diversity to the workforce (IOM, 2011). Given the disparity

131
between the number of males and females employed as professional nurses, gender differences in
ability are important to determining skill acquisition/possession across the entire field of nursing.
Certifications
Licensing and Certification
RN licensure indicates entry-level competence to the nursing field where certification
verifies specialty knowledge, skills, experience and clinical judgment (American Association of
Critical-Care Nurses, 2013; American Board of Nursing Specialties, 2005). Certification reflects
self-mastery with an emphasis on self-evaluation (Crist, Russell, & Farber, 2012). According to
Wynd (2003), nursing professionalism is significantly related to years of nursing experience,
higher educational degrees in nursing, professional organizational memberships and specialty
certification.
Specialty certifications include, at a minimum, a practice component with required
knowledge testing (Briggs, Brown, Kesten, & Heath, 2006; Grief, 2013). The American Nurses
Credentialing Center (ANCC) is the nationally recognized agency to provide professional
nursing credentialing programs to certify and recognize nurses in areas of specialty (ANCC,
2013). The majority of hospitals in the United States seek accreditation from the Joint
Commission (Williams & Counts, 2013). Many hospitals apply for the Malcolm Baldrige
National Quality Award, the American Association of Critical-Care Nurses Beacon Award for
Excellence, and for Magnet recognition (Williams & Counts, 2013). All of these programs,
whether accrediting, recognizing or awarding, include nursing certifications as an integral factor
in demonstrating nursing excellence (Fleischman, Meyer, & Watson, 2011; Williams & Counts,
2013).

132
Professional Certification and Patient Outcomes
The connection between certified nurses and quality patient care is well established (Crist
et al., 2012). Specialty nurse certification is increasing in value as more evidence suggests that
certification is a factor in improving patient outcomes (Fleischman et al., 2011; Timmerman,
2008). RNs with a BSN degree and a specialty certification are associated with improved patient
outcomes, decreased mortality, and decreased failure to rescue in general surgical patients
(Kendall-Gallagher, Aiken, Sloane, & Cimiotti, 2011).
Competency or Proficiency
The National Council of State Boards of Nursing (NCSBN) requires all nurse licensing
candidates to pass an examination that measures the competencies required to perform safe and
effective patient care as a newly licensed entry-level nurse, namely the NCLEX-RN (National
Council Licensure Examination for Registered Nurses), and graduate from an accredited school
of nursing (National Council of State Boards of Nursing, 2013). Upon graduation from an
accredited school of nursing and passing the NCLEX-RN, the student applies for a nursing
license allowing the individual to practice nursing within the state where the requirements were
met (Simon, McGinniss, & Krauss, 2013). The HESI (Health Education Systems, Inc.) Exit
Exam, an external independent assessment of a student’s competency at a higher cognition level
of application, analysis, and synthesis, is often administered to senior level nursing students to
determine a student’s readiness to take the NCLEX-RN (Schooley & Kuhn, 2013).
Currently, in most states a nurse is considered proficient or competent upon initial
licensing, with assumed proficiency or competency going forward unless otherwise discovered
(Tilley, 2008). Tilley (2008) describes the confusion associated with competency and

133
proficiency as related to two different uses of the terms initial licensure and ongoing
maintenance.
There has been little progress in the nursing profession towards the development of a
general tool to evaluate overall nursing knowledge and skills outside of nursing schools (IOM,
2011; Long, Mitchell, Young, & Rickard, 2013). Definitions of nursing proficiency or
competency are difficult to find as there is little consensus about a definition or the concept of a
competency measurement (Tilley, 2008). Tilley (2008) outlined the defining attributes of
competency as (a) application of skills in all domains for the practice role, (b) instruction that
focuses on specific outcomes or competencies, (c) allowance for increasing levels of
competency, (d) accountability of the learner, (e) practice-based learning, (f) self-assessment,
and (g) individualized learning experiences. The NCSBN (2005) defines competency as “the
application of knowledge and the interpersonal, decision-making, and psychomotor skills
expected for the practice role, within the context of public health” (p. 81). Competency
assessments should evaluate thinking in action, confidence in decision making, and information
retrieval for the inclusion of best practices (Allen et al., 2008).
Nursing Shortage
Predictions
The nursing profession is experiencing a national workforce shortage of critical
proportion (Juraschek, Zhang, Ranganathan & Lin, 2012). This shortage is predicted to worsen,
with an expected national shortage of 300,000 to 1 million RNs in 2020, and continued shortages
throughout the country through 2030 (Juraschek et al.). A report from the U.S. Department of
Health and Human Services (2010) predicted a nursing shortage equating to a 36% shortage.

134
Aging Workforce
The aging RN workforce strongly impacts the projected nursing shortage (Juraschek et
al., 2012). Nurses that were 50 years of age or older comprised 25% of the nursing workforce in
1980, 33% of the nursing workforce in 2000, and were accountable for 45% of the nursing
workforce in 2008 (Juraschek et al.; US Department of Health and Human Services, 2010). A
survey conducted in 2013 reported that 55% of the current RN workforces is age 50 or older
(Budden, Zhong, Moulton, & Cimiotti, 2013). It is estimated that 55% of currently employed
nurses plan to retire before 2020 (Hirschkorn et al., 2010).
Job Dissatisfaction
Social support from supervisors and coworkers, job demands, and self-efficacy were
reported to be significantly related to job dissatisfaction, while demands and support from
coworkers were related to intention to leave the profession (Peterson, Hall, O’Brien-Pallas, &
Cockerill, 2011). Job dissatisfaction was a strong determinant of turnover among new nursing
graduates, with interpersonal relationships having the strongest impact (Cho, Lee, Mark, & Yun,
2012). Nurses new to the profession are often disillusioned when what they learned nursing
should be is different from the reality of nursing practice in their work place (Cho et al., 2012).
Nursing Faculty Shortage
There are many factors for the nursing shortage with a shortage of nursing educators
being one of the factors (Rich & Nugent, 2010). In 2012, U.S. nursing schools declined almost
80,000 qualified applicants for baccalaureate and graduate nursing programs due to a lack of
faculty, clinical sites, clinical preceptors and budget constraints (AACN, 2014). Higher

135
financial compensation in clinical settings is enticing current and potential nursing faculty away
from the academic setting (AACN).
Addressing the Nursing Shortage
One step in addressing the predicted nursing shortage would be to ensure those entering
the profession possess essential aptitudes for a career in nursing. In this manner, the profession
of nursing might benefit from alignment with current strategies of early identification of
individuals with potential for success, as is being done in science, technology, engineering, and
math (STEM) fields.
Students often enter the field of nursing with common misconceptions, such as nursing is
a subordinate occupation, requiring only common sense and little intellectual capacity (Brodie et
al., 2004). Students are surprised, even overwhelmed, by the required high academic standards
in nursing. The unexpected demands of academic knowledge and clinical expertise have been
identified as a source of nursing student attrition (Brodie et al., 2004) Acquiring the required
knowledge and skills often overwhelms students preparing for a nursing career. Harvey and
McMurray (1997) reported that 81% of students dropping from a pre-nursing course cited a
perceived discrepancy between the content of their course and their preconceived ideas of the
nursing profession. Failure to recognize that nursing is based on science and requires a complex
and specialized skill set with the ability to think critically and act decisively underlies much of
that perceived discrepancy (Harvey & McMurray, 1997).

136
Spatial Ability
General Cognitive Ability - g
Charles Spearman introduced the first theory of intelligence in 1904, identifying general
mental ability as a trait based on his findings that all mental test scores were positively correlated
(Floyd, McGrew, Barry, Rafael, & Rogers, 2009; Jensen, 1987). Spearman proposed general
intelligence, g, as the identified factor that accounted for correlations among cognitive ability
tests (Carroll, 1997). General cognitive ability (g) is the capacity to work with cognitive
complexity, more specifically, complex informational processing (Gottfredson, 1997; 2002). An
application definition of general cognitive ability (g) is the aptitude to learn moderately complex
material quickly and efficiently and the ability to prevent cognitive errors (Gottfredson, 2002).
General cognitive ability has been identified as the primary predictor for occupational success in
the United States (Kane & Brand, 2003).
Raymond Cattell suggested human intelligence is comprised of two complementary
intelligence factors--crystallized and fluid intelligence (Horn & Cattell, 1966). Crystallized
intelligence, gc, represents specific knowledge that one obtains from learning, education and
experience; fluid intelligence, gf, represents the capacity to solve problems, think logically, and
reason independent of acquired knowledge (Jensen, 1987). John Horn furthered Cattell’s
research in 1965 by adding six broad factors, resulting in the Cattell-Horn Gf-Gc theory (Kane &
Brand, 2003; McGrew, 2009).
Carroll’s research proposed a hierarchical model of intelligence, describing cognitive
abilities in terms of a three-stratum model (Carroll, 1997; Kane & Brand, 2003). Stratum 1 is
composed of a large number of narrow abilities, such as language development, reading, and
spelling. Stratum II consists of 10 broad abilities, such as fluid intelligence, crystallized

137
intelligence, general memory and processing speed (Kane & Brand, 2003). The highest stratum,
Stratum III, consists of only one single factor, g, generalized intelligence (Carroll, 1997).
Cattell-Horn-Carroll Theory
The Cattell Horn Carroll (CHC) theory of intelligence was developed by merging the
Cattell-Horn Gf-Gc model with Carroll’s three-tiered stratum model to form a broader
hierarchical model of g (Floyd, Evans, & McGrew, 2003; McGrew, 2009). General cognitive
ability, g, is the highest level of the hierarchy at Stratum III (Bickley, Keith, & Wolfe, 1995;
Parkin & Beaujean, 2012). Stratum II contains 10 broad CHC abilities with visual processing,
Gv, being one of the ten (Rozencwajg, Schaffer, & Lefebvre, 2010). Making use of simulated
mental imagery to solve problems is the basis of visual processing (McGrew, 2013). Visual-
spatial ability includes many specific perceptual abilities, being cognizant of complex visual
patterns, being aware of where items are located in space, in addition to visualizing objects as
they would appear from a different angle (Schneider & McGrew, 2012; 2013). According to
McGrew (2009), Gv abilities are often measured by tasks that require retaining the spatial
orientation of an object after the object has been moved or changed. Figure D.1 provides a
visual illustration, comparing Carroll's three-stratum, Cattell–Horn's extended Gf–Gc, and the
integrated Cattell–Horn–Carroll models of human cognitive abilities (McGrew, 2009).

138
Figure D.1. Schematic representation and comparisons of Carroll's three-stratum, Cattell–Horn's extended Gf–Gc, and the integrated Cattell–Horn–Carroll models of human cognitive abilities (McGrew, 2009).
Stratum II contains 10 broad CHC abilities: (a) fluid intelligence, (b) quantitative
knowledge, (c) crystalized intelligence, (d) reading and writing ability, (e) short-term memory,
(f) visual processing, (g) auditory processing, (h) long-term retrieval, (i) processing speed, and
(j) decision/reaction time/speed (Rozencwajg, et al., 2010). Over 100 narrow abilities are
included in Stratum I and are subsumed under the broader abilities in Stratum II (Parkin &
Beaujean, 2010)
The current study focused on the broad ability of visual processing, Gv. Higher Gv
ability allows an individual to see more than the object by imagining the object from a different
view after mental rotation, mentally taking a complex item apart and reassembling the item
(Schneider & McGrew, 2013). Lower Gv levels decrease an individual’s ability to perform
mental rotations causing the person to wait until an object is physically rotated to see the change

139
(Schneider & McGrew, 2013). McGrew (2013) explains that after the eyes have transmitted
visual information, the visual system of the brain performs a number of basic computations, such
as edge detection, light/dark perception, color-differentiation, and motion-detection. These
activities are used by more high level processors to create more complex aspects of the image,
such as spatial configuration (McGrew, 2013).
Spatial Ability in STEM – to Include Nursing
Over 50 years of research exists on the importance of using spatial ability, specifically in
the realm of science, technology, engineering, and math (STEM), for selection and instruction in
education (Wai, Lubinski, & Benbow, 2009). Spatial ability, often neglected in complex work
environments, is a powerful systematic source of individual differences (Lubinski, 2010). Snow
(1999) expressed concern about the absence of spatial ability in applied educational settings:
There is good evidence that [spatial ability] relates to specialized achievements in fields such as architecture, dentistry, engineering, and medicine…Given this plus the longstanding anecdotal evidence on the role of visualization in scientific discovery... it is incredible that there has been so little programmatic research on admissions testing in this domain. (p. 136) A recent study with over 4000 nursing students, compared admission criteria for nursing
programs with a standardized RN Fundamentals assessment (Wolkowitz & Kelley, 2010).
Wolkowitz and Kelley (2010) reported science coursework as a statistically significant predictor
and the strongest predictor for nursing program success. Scores for biology and chemistry
coursework were significant predictors for success with readiness practice exams for RN
licensing (Simon, McGinniss & Krauss, 2013). As science is fundamental for nursing education
and higher spatial ability levels are associated with success in math, nursing should consider

140
joining efforts with educational departments in evaluating spatial ability in efforts to identify
potential candidates to enter professional nursing.
Gender Differences in Spatial Ability
Findings supporting gender differences in spatial ability are abundant; and, mental
rotation testing is consistently more sensitive to gender differences than other spatial ability tasks
(Brownlow, McPheron, & Acks, 2003; Ceci & Williams, 2010; Geary, Gilger, & Elliott-Miller,
1990; Geiser, Lehmann, & Eid, 2008; Jansen & Heil, 2010; Terlecki, Newcombe, & Little, 2008;
Voyer et al., 1995; Voyer & Doyle, 2010). With the imbalance among the number of male and
female nurses and the commonly accepted finding of males performing higher than females on
mental rotation tests for spatial ability, looking at spatial ability in nurses could provide
additional information to address gender differences and nursing shortages within the profession.
Several explanations for gender differences in spatial ability have been provided, such as
socioeconomic status (SES), environmental, or biological factors (Levine, Vasilyeva, Lourenco,
Newcombe, & Huttenlocher, 2005). Brain maturation, hormonal changes, personal beliefs and
motivation have also been reported as possible explanations for gender differences in spatial
abilities (Moe & Pazzaglia, 2006; Kozaki & Yasukouchi, 2009; Yilmaz, 2009).
Sex roles in play activities, parental expectations, and educational experiences all
influence the development of a child (Yilmaz, 2009). Boys are more likely than girls to
participate in spatial activities, such as building blocks, models, athletic sports, and video games
in childhood (Baenninger & Newcombe, 1995; Cherney, 2008). Practice effects from
participation in these spatial activities likely contribute to correlation with higher spatial ability
test scores in males (Baenninger & Newcombe, 1995).

141
Gender differences in spatial ability may also result from different solution strategies.
Mental rotation strategies are often categorized in two groups--analytic strategies and holistic
strategies (Janssen & Geiser, 2010). Analytic strategies employ comparing specific details and
using reasoning strategies, unlike holistic strategies that utilize mental transformations (Janssen
& Geiser, 2010). According to Arendasy, Sommer and Gittler (2010), females are more likely to
lose their internal mental representations or lose track during the transformational process.
Holistic mental rotation strategies are reported to be more effective when compared to
perspective change strategies, and females tend to utilize less effective perspective change
strategies (Arendasy, Sommer, & Gittler, 2010). According to Janssen and Geisler (2010)
individuals can be identified as rotators or non-rotators, dependent on the strategy they use for
mental rotation testing.
Spatial Ability and Job Performance
General cognitive ability, g, is a significant component of individual differences in job
performance associated with informational processing skills (Lubinski, 2000). Greater levels of
g are associated with higher levels of performance in all jobs and within all dimensions of
performance (Gottfredson, 2002). Health care organizations are frequently described within the
context of complexity, situations involving people working independently and collectively to
manage an unpredictable work environment over time (Fairchild, 2010). Individuals with high
general cognitive ability are needed in the nursing profession. As nursing requires strong
information processing activities for successful patient care assessing individuals considering
entering the nursing profession for general cognitive ability, specifically spatial visualization,
might be beneficial.

142
COMPREHENSIVE REFERENCES
Adamson, K.A., Parsons, M., Hawkins, K., Manz, J.A., Todd, M., & Hercinger, M. (2011) Reliability and internal consistency findings from the C-SEI. Journal of Nursing Education, (50)10, 583-586. doi:10.3928/01484834-20110715-02
Allen, P., Lauchner, K., Bridges, R. A., Francis-Johnson, P., McBride, S. G., & Olivarez, A. (2008). Evaluation continuing competency: A challenge for nursing. The Journal of Continuing Education in Nursing 39(2), 81-85. doi:10.3928/00220124-20080201-02
American Association of Colleges of Nursing - AACN. (2014). Fact Sheet: Nursing Faculty Shortage. Retrieved February 7, 2014 from https://www.aacn.nche.edu/media-relations/fact-sheets/nursing-faculty-shortage
American Association of Critical-Care Nurses. (2013). Nurse certification benefits patients, employers and nurses position statement. Retrieved November 9, 2013 from www.aacn.org/wd/certifications/content/benefitstoptempnrs.pcms?menu=certification
American Board of Nursing Specialties. (2005, March 5). A position statement on the value of nursing specialty certification. Retrieved November 9, 2013 from http://www.nursingcertification.org/
American Nurses Credentialing Center (2013). ANCC - American Nurses Credentialing Center - ANCC., 2009. Retrieved from http://www.nursecredentialing.org/Certification
Arendasy, M. E., Sommer, M., & Gittler, G. (2010). Combining automatic item generation and experimental designs to investigate the contribution of cognitive components to the gender difference in mental rotation. Intelligence, 38(5), 506-512. doi:10.1016/j.intell.2010.06.006
Baenninger, M., & Newcombe, N. (1995). Environmental input to the development of sex-related differences in spatial and mathematical ability. Learning and Individual Differences, 7(4), 363-379. doi:10.1016/1041-6080(95)90007-1
Barrett, E. A. (2002). What is nursing science? Nursing Science Quarterly, 15(1), 51-60.
Beaujean, A. A., Firmin, M. W., Attai, S., Johnson, C. B., Firmin, R. L., & Mena, K. E. (2011). Using personality and cognitive ability to predict academic achievement in a young adult sample. Personality and Individual Differences, 51, 709-714. doi:10.1016/j.paid.2011.06.023
Bell-Kotwall, L., Frierson, D., & Kuiper, R. (2012). Are certified nurses better professionals? Nursing Management, 43(6), 30-35, doi:10.1097/01.NUMA.0000413641.52774.2c.
Beres, I., Magyar, T., & Turcsanyi-Szabo, M. (2012). Towards a personalized, learning style based on collaborative blended learning model with individual assessment. Informatics in Education, 11(1), 1-28.

143
Bickley, P. G., Keith, T. Z., & Wolfle, L. M. (1995). The three-stratum theory of cognitive abilities: Test of the structure of intelligence across the life span. Intelligence, 20, 309-328. doi:10.1016/0160-2896(95)90013-6
Blanche, J. (2010). Nursing 50 years back and today: How the nursing field has changed over the last 50 years. Retrieved from http://www.healthecareers.com/article/nursing-50-years-back-and-today-how-the-nursing-field-has-changed-over-the-last-50-years/158432
Bland, J.M., & Altman, D. G., (1997). Statistics notes. Cronbach’s alpha. British medical journal (Clinical research ed.), 314, 572.
Blanton, E. L. (2004). The influence of students’ cognitive style on a standardized reading test administered in three different formats. (Doctoral dissertation). University of Central Florida, Orlando, FL
Bond, C. S. (2009). Nurses, computers and pre-registration education. Nurse Education Today, 29(7), 731-734. doi:10.1016/j.nedt.2009.02.014
Brandt, M. G., & Davies, E. T. (2006). Visual-spatial ability, learning modality and surgical knot tying. Canadian Journal of Surgery, 49(6), 412-416.
Briggs, L. A., Brown, H., Kesten, K., & Health, J. (2006). Certification: A benchmark for critical care nursing excellence. Critical Care Nurse, 26(2), 47-53.
Brodie, D. A., Andrews, G. J., Andrews, J. P., Thomas, G. B., Wong, J., & Rixon, L. (2004). Perceptions of nursing: Confirmation, change and the student experience. International Journal of Nursing Studies, 41, 721–733.
Brownlow, S., McPheron, T. K., & Acks, C. N. (2003). Science background and spatial abilities in men and women. Journal of Science Education and Technology, 12(4), 371-380. doi:10.1023/B:JOST.0000006297.90536.7c
Budden, J. S., Zhong, El. H., Mouton, P., & Cimiotti, J. P. (2013). Supplement: The National Council of State Boards of Nursing and the State Nursing Workforce Centers 2013 National workforce survey of registered nurses. Journal of Nursing Regulation, 4(2). S1-S72.
Buerhaus, P. I. (2008). Current and future state of the US nursing workforce. Journal of the American Medical Association, 300(20), 2422-2424. doi:10.1001/jama.2008.729.
Carlson, M. D. A., & Morrison, R. S. (2009) Student design, precision, and validity in observational studies. Journal of Palliative Medicine 12(1), 77-82. doi:10.1089/jpm.2008.9690
Carroll, J. B. (1997). Psychometrics, intelligence, and public perception. Intelligence, 24(1), 25-52.
144
Ceci, S. J., & Williams, W. M. (2010). Sex differences in math-intensive fields. Current Directions in Psychological Science, 19(5), 275-279. doi: 10.1177/0963721410383241
Cherney, I. D. (2008). Mom, let me play more computer games: They improve my mental rotation skills. Sex Roles, 59, 776-786.
Cho, S-H., Lee, J. Y., Mark, B. A., & Yun, S-C. (2012). Turnover of new graduate nurses in their first job using survival analysis. Journal of Nursing Scholarship, 44(1), 63-70. doi:10.1111/j.1547-5069.2011.01428.x
Credentialing requirements for magnet status hospitals. (2013). Retrieved November 18, 2013, from http://educationcareerarticles.com/education-articles/higher-education-articles/credentialing-requirements-for-magnet-status-hospitals/
Crist, K. S., Russell, B. S., & Farber, M. R. (2012). The value of certification and the CIC credential. American Journal of Infection Control, 40(4), 294-295
DARA Thailand, Drug and Alcohol Rehab Asia. (2008). Retrieved July 30, 2012, from DARA, Drug and Alcohol Rehab Asia: http://alcoholrehab.com/alcohol-rehab
Debelak, R., Gittler, G., & Arendasy, M. (2014). On gender differences in mental rotation processing speed. Learning and Individual Differences 29, 8-17. doi:10.1016/j.lindif.2013.10.003
Fairchild, R. M. (2010). Practical ethical theory for nurses responding to complexity in care. Nursing Ethics, 17(3), 353–362. doi: 10.1177/0969733010361442
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175-191.
Fleischman, R. K., Meyer, L, & Watson, C. (2011). Best practices in creating a culture of certification. AACN Advanced Critical Care 22(1), 33-49. doi: 10.1097/NCI.0b013e3182062c4e
Fleming, S., Mckee, G, & Huntley-Moore, S. (2011). Undergraduate nursing students’ learning styles: A longitudinal study. Nurse Education Today 31(5), 444-449, doi:10.1016/j.nedt.2010.08.005
Floyd, R. G., Evans, J. J., & McGrew, K. S. (2003). Relations between measures of Cattell-Horn-Carroll (CHC) cognitive abilities and mathematics achievement across the school-age years. Psychology in the Schools, 40(20), 155-171. doi: 10.1002/pits.10083
Floyd, R. G., McGrew, K. S., Barry, A., Rafael, F., & Rogers, J. (2009). General and specific effects on Cattell-Horn-Carroll broad ability composites: Analysis of the Woodcock-Johnson III normative update Cattell-Horn-Carroll factor clusters across development. School Psychology Review, 38(2), 249-264.

145
Frellick, M. (2013, April). A path to nursing excellence. Hospitals and Health Networks. Retrieved November 18, 2013, from http://www.hhnmag.com/hhnmag/jsp/articledisplay.jsp?dcrpath=HHNMAG/Article/data/04APR2011/0411HHN_FEA_workforce&domain=HHNMAG
Geary, D. C., Gilger, J. W., & Elliott-Miller, B. (1990). Gender differences in three-dimensional mental rotation: A replication. The Journal of Genetic Psychology, 153, 115-117.
Geiser, C., Lehmann, W., & Eid, M. (2008). A note on sex differences in mental rotation in different age groups. Intelligence, 36, 556-563. doi: 10.1016/j.intell.2007.12.003
Giuliano, K. K., Tyer-Viola, L., & Lopez, R. P. (2005). Unity of knowledge in the advancement of nursing knowledge. Nursing Science Quarterly, 18(3), 243-248. doi: 10.1177/0894318405277527
Goodin, H. J. (2003). Integrative literature reviews and meta-analysis: The nursing shortage in the Unites States of America: an integrative review of the literature. Journal of Advancing Nursing, 43(4), 335-350. doi: 10.1046/j.1365-2648.2003.02722_1.x
Gottfredson, L. S. (1997). Why g matters: The complexity of everday life. Intelligence, 24(1), 79-132. doi: 10.1016/S0160-2896(97)90014-3
Gottfredson, L. S. (2002). Where and why g matters: Not a mystery. Human Performance, 15(1/2), 25-46. doi:10.1207/S15327043HUP1501&02_03
Grief, C. L., (2013). Advocating for registered nurse specialty certification, Journal of Emergency Nursing, 39(3), 248-249. doi: 10.1016/j.jen.2013.02.006
Guillot, A., Champely, S., Batier, C., Thiriet, P, & Collet, C. (2007). Relationship between spatial abilities, mental rotation and functional anatomy learning. Advances in Health Sciences Education, 12, 491-507. doi: 10.1007/s10459-006-9021-7
Halpern, D. F. (1998). Teaching critical thinking for transfer across domains. American Psychologist, 53(4), 449-455.
Harvey, V. C., & McMurray, N. E. (1997). Students’ perceptions of nursing: Their relationship to attrition. Journal of Nursing Education, 36(8), 383-389.
Hawkins, J. E., & Shell, A. (2012). Magnet hospitals are attracted to the BSN but what’s in it for nurses? Nursing 2013, 42(3), 50-52.
Hegarty, M., Keehner, M., Khooshabeh, P., & Montello, D. R. (2009). How spatial abilities enhance, and are enhanced by, dental education. Learning and Individual Differences, 19, 61-70. doi: 10.1016/j.lindif.2008.04.006
Hendren, R. (2011, April 19). Nurse executives focus on complexity of care delivery. Retrieved April 20, 2011, from HealthLeadersMedia.com:

146
http://www.healthleadersmedia.com/content/NRS-265126/Nurse-Executives-Focus-on-Complexity-of-Care-Delivery
Hinze, S. R., Williamson, V. M., Shultz, M. J., Williamson, K. C., Deslongchamps, G., & Rapp, D. N. (2013). When do spatial abilities support student comprehension of STEM visualizations? Cognitive Processing, 14(2), 129-142. doi:10.1007/s10339-013-0539-3
Hirschkorn, C. A., West, T. B., Hill, K. S., Cleary, B. L., & Hewlett, P. O. (2010). Experienced nurse retention strategies: What can be learned from top-performing organizations. Journal of Nursing Administration, 40(11), 463-467. doi:10.1097/NNA.0b013e3181f88fd3
Hodges, H. F. (2011). Preparing new nurses with complexity science and problem-based learning. Journal of Nursing Education 50(1), 7-13, doi:10.3928/01484834-20101029-01
Horn, J. L. & Cattell, R. B. (1966). Refinement and test of the theory of fluid and crystallized general intelligences. Journal of Educational Psychology 57(5), 253-270. doi:10.1037/h0023816
Hoyek, N., Collet, C., Rastello, O., Fargier, P., Thiriet, P., & Guillot, A. (2009). Enhancement of mental rotation abilities and its effect on anatomy learning. Teaching and Learning in Medicine, 21(3), 201-206. doi: 10.1080/10401330903014178
Hsu, H.-Y., Chen, S.-H., Yu, H.-Y., & Lou, J.-H. (2010). Job stress, achievement motivation and occupational burnout among male nurses. Journal of Advanced Nursing 66(7), 1592-1601. doi: 10.1111/j.1365-2648.2010.05323.x
Institute of Medicine. (2010). The future of nursing: Focus on education. Retrieved from http://www.iom.edu/Reports/2010/The-Future-of-Nursing-Leading-Change-Advancing-Health/Report-Brief-Education.aspx
Institute of Medicine. (2011). The future of nursing: Leading change, advancing health. Retrieved from http://www.nap.edu/catalog/12956.html
Janssen, A. B., & Geiser, C. (2010). On the relationship between solution strategies in two mental rotation tasks. Learning and Individual Differences, 20, 473-478. doi:10.1016/j.lindif.2010.03.002
Jensen, A. R. (1987). Individual differences in mental ability. In J. A. Glover & R. R. Ronning (Eds.)., Historical foundations of educational psychology (pp. 61-88). New York: Plenum Press.
Johnston, A. N., & McAllister, M. (2008). Back to the future with hands-on science: Students' perceptions of learning anatomy and physiology. Research Briefs, 47(9), 417-421.
Juraschek, S. P., Zhang, X, Ranganathan, V. K., & Lin, V.W W. (2012). Unites States registered nurse workforce report card and shortage forecast. American Journal of Medical Quality 27(3), 241-249. doi:10.1177/1062860611416634

147
Kalisch, B. J. & Begeny, S., (2010). Preparation of nursing students for change and innovation. Western Journal of Nursing Research 32(2), 157-167. doi:10.1177/0193945909335052
Kane, H., & Brand, C. (2003). The importance of spearman's g as a psychometrical, social, and educational construct. The Occidental Quarterly, 3(1), 7-30.
Keith, T. Z., & Reynolds, M. R. (2010). Cattell-Horn-Carroll abilities and cognitive tests: What we've learned from 20 years of research. Psychology in the Schools, 47(7), 635-650. doi:10.1002/pits.20496
Kendall-Gallagher, D., Aiken, L. H., Sloane, D. M., & Cimiotti, J.P. (2011). Nurse specialty certification, inpatient mortality, and failure to rescue. Journal of Nursing Scholarship, 43(2), 188-194. doi:10.1111/j.1547-5069.2011.01391.x
Khatib, M., & Hosseinpur, R. M. (2011). On the validity of the group embedded figure test (GEFT). Journal of Language Teaching and Research, 2(3), 640-648.
Kohlbrenner, J., Whitelaw, G., & Cannaday, D. (2011). Nurses critical to quality, safety, and now financial performance. The Journal of Nursing Administration, 41(3), 122-128. doi:10.1097/NNA.0b013e31820c71f9
Kozaki, T., & Yasukouchi, A. (2009). Sex differences on components of mental rotation at different menstrual phases. International Journal of Neuroscience, 119, 59-67. doi:10.1080/00207450802480101
Kramer, M., Maguire, P., Schmalenberg, C., Halfer, D., Budin, W. C., Hall, D. S., Goodloe, L., Klaristenfeld, J., Teasley, S. Forsey, L., & Lemke, J. (2013). Components and strategies of nurse residency programs effective in new graduate socialization. Western Journal of Nursing Research 35(5), 566-589. doi:10.1177/0193945912459809
Kuehn, B. M. (2007). No end in sight to nursing shortage: Bottleneck at nursing schools a key factor. Journal of the American Medical Association, 298(14), 1623-1625. doi:10.1001/jama.298.14.1623
Kundson, L. (2013). Nursing certification provides recognition for nurses, employers. AORN Connections 97(3), pp. c9 -c11. doi: 10.1016/S0001-2092(13)00130-0
Langford, R., & Young, A. (2013). Predicting NCLEX-RN success with the HESI exit exam: Eighth validity study. Journal of Professional Nursing 29(2, Suppl 1), S5-S6, doi:10.1016/j.profnurs.2012.06.007
Langlois, J., Wells, G. A., Lecourtois, M., Bergeron, G., Yetisir, E., & Martin, M. (2009). Spatial abilities in an elective course of applied anatomy after a problem-based learning curriculum. Anatomical Sciences Education, 2, 107-112. doi:10.1002/ase.84.
Lawrence, L. A. (2011). Work engagement, moral distress, education level, and critical reflective practice in intensive care nurses. Nursing Forum 46(4), 256-268. doi: 10.1111/j.1744-6198.2011.00237.x

148
Leibert, M. (2011). Performance of integrated delivery systems: Quality, service and cost implications. Leadership in Health Services 24(3), 196-206, doi:10.1108/17511871111151108
Leufer, T., & Cleary-Holdforth, J. (2013). Let’s do no harm: Medication errors in nursing: Part 1. Nurse Education in Practice 13(3), 213-6. doi: 10.1016/j.nepr.2013.01.013
Levine, S. C., Vasilyeva, M., Lourenco, S. F., Newcombe, N. S., & Huttenlocher, J. (2005). Socioeconomic status modifies the sex differences in spatial skill. Psychological Science, 16(11), 841-845. doi:10.1111/j.1467-9280.2005.01623.x
Linn, M. C., & Petersen, A. C. (1985). Emergence and characterization of sex differences in spatial ability: A meta-analysis. Child Development, 56, 1479-1498.
Lockie, N. M., Van Lanan, R. J., McGannon, T. (2013). Educational implications of nursing students' learning styles, success in chemistry, and supplemental instruction participation on national council licensure examination-registered nurses performance. Journal of Professional Nursing 29(1), 49-58. doi: 10.1016/j.profnurs.2012.04.003
Long, D. A., Mitchell, M. L., Young, J., & Rickard, C. M. (2013). Assessing core outcomes in graduates: Psychometric evaluation of the Paediatric Intensive Care Unit-Knowledge and Skills Test. Journal of Advanced Nursing, 00(0). 1-11. doi:10.1111/jan.12241
Long, L. E., McGee, S., Kinstler, A., & Huth, M. M. (2011). Aligning the forces of magnetism to achieve exemplary professional practice. Journal of Pediatric Nursing 26(2), 108-113. doi: 10.1016/j.pedn.2010.12.004
Lubinski, D. (2000). Scientific and social significance of assessing individual differences: "Sinking shafts at a few critical points". Annual Review of Psychology, 51, 405-444. doi:10.1146/annurev.psych.51.1.405
Lubinski, D. (2010). Spatial ability and STEM: A sleeping giant for talent identification and development. Personality and Individual Differences 49(4), 344-351. doi:0.1016/j.paid.2010.03.022
Lynn, M. R., & Redman, R. W. (2005). Faces of the nursing shortage: Influences on staff nurses' intentions to leave their positions or nursing. Journal of Nursing Administration, 35(5), 264-270.
Maag, M. (2004). The Effectiveness of an interactive multimedia learning tool on nursing students' math knowledge and self-efficacy. Computers, Informatics, Nursing, 22(1), 26-33.
Maeda, Y., & Yoon, S. Y. (2013). A meta-analysis on gender differences in mental rotation ability measured by the Purdue Spatial Visualization Tests: Visualization of Rotations (PSVT:R). Educational Psychology Review, 25, 69-94. doi: 10.1007/s10648-012-9215-x

149
Maneval, R. E. & Teeter, M. M. (2010). The student perspective on RN-Plus-10 legislation: A survey of associate degree and diploma nursing program students. Nursing Education Perspectives, 31(6), 358-361.
McBride, A. B. (1999). Breakthroughs in nursing education: Looking back, looking forward. Nursing Outlook, 47(3), 114-119. doi:10.1016/S0029-6554(99)90005-2
McGeown, S., Goodwin, H., Henderson, N., & Wright, P. (2012). Gender differences in reading motivation: Does sex or gender identity provide a better account? Journal of Research in Reading, 35(3), 328-336. doi:10.1111/j.1467-9817.2010.01481.x
McGrew, K. S. (2009). CHC theory and the human cognitive abilities project: Standing on the shoulders of the giants of psychometric intelligence research. Intelligence, 37, 1-10. doi:10.1016/j.intell.2008.08.004
McGrew, K. (2013, October 14). CHC Theory: Visual-spatial processing (Gv) definition. Retrieved from http://www.iqscorner.com/2013/01/chc-theory-visual-spatial-processing-gv.html
McGrew, K. S., & Wendling, B. J. (2010). Cattell-Horn-Carroll cognitive-achievement relations: What we have learned from the past 20 years of research. Psychology in the Schools, 47(7), 651-674.
Miner, D. C. (2012). Transforming the nursing workforce in New York: The value of baccalaureate preparation in nursing. Journal of the New York State Nurses Association 43(2), 17-36.
Moe, A., & Pazzaglia, F. (2006). Following the instructions! Effects of gender beliefs in mental rotation. Learning and Individual Differences, 16, 369-377. doi:10.1016/j.lindif.2007.01.002
National Council of State Boards of Nursing. (2005). Business Book: NCSBN 2005 Annual meeting. Mission Possible: Building a Safer Nursing Workforce through Regulatory Excellence. Chicago, IL: Author.
National Council of State Boards of Nursing. (2013). NCLEX-RN examination. Detailed test plan for the national council licensure examination for registered nurses, item writer/item reviewer/nurse educator version. Retrieved from https://www.ncsbn.org/index.htm
Nazareth, A., Herrara, A., & Pruden, S. M. (2013). Explaining sex differences in mental rotation: Role of spatial ability experience. Cognitive Processing 14(2), 201-204. doi:10.1007/s10339-013-0542-8
Noble, K. A., Miller, S. M., & Heckman, J. (2008). The cognitive style of nursing students: Educational implications for teaching and learning. Journal of Nursing Education, 47(6), 245-253.

150
O’Leary, J. (2012). Comparison of self-assessed competence and experience among critical care nurses. Journal of Nursing Management, 20(5), 607-604. doi:10.1111/j.1365-2834.2012.01394.x
Parkin, J. R., & Beaujean, A. A., (2012). The effects of Wechsler Intelligence Scale for Children – Fourth Edition cognitive abilities on math achievement. Journal of School Psychology, 50(1), 113-128. doi:10.1016/j.jsp.2011.08.003
Parsons, M. L., & Cornett, P. A. (2011). Sustaining the pivotal organization outcome: Magnet recognition. Journal of Nursing Management 19(2), 277-286. doi: 10.1111/j.1365-2834.2011.01224.x
Peterson, J., Hall, L. M., O’Brien-Pallas, L., & Cockerill, R. (2011). Job satisfaction and intentions to leave of new nurses. Journal of Research in Nursing 16(6), 536-548. doi:10.1177/1744987111422423
Pittalis, M., & Christou, C., (2010). Types of reasoning in 3D geometry thinking and their relation with spatial ability. Educational Studies in Mathematics, 75(2), 191-212. doi:10.1007/1s0 649-01 0-9251 -8
R Core Team (2013). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/.
Rich, K. L., & Nugent, K. E. (2010). A United States perspective on the challenges in nursing education. Nursing Education Today 30(3), 228-232. doi:10.1016/j.nedt.2009.10.015
Rittschof, K. A. (2010). Field dependence-independence as visuospatial and executive functioning in working memory: Implications for instructional systems design and research. Educational Technology Research and Development 58(1), 99-114. doi:10.1007/s11423-008-9093-6
Robinson, J. S., Kitchel, T., & Garton, B. L. (2009). using agricultural education graduates’ GEFT scores to assess their level of job satisfaction. Journal of Southern Agricultural Education Research, 59, 28-43.
Rozencwajg, P., Schaeffer, O., & Lefebvre, V. (2010). Arithmetic and aging: Impact of quantitative knowledge and processing speed. Learning and Individual Differences 20(5), 452-452. doi:10.1016/j.lindif.2010.04.009
Saba, V. K. (2001). Nursing informatics: Yesterday, today and tomorrow. International Nursing Review 48(3), 177-187. doi:10.1046/j.1466-7657.2001.00064.x
Schneider, W. J., & McGrew, K. (2012). The Cattell-Horn-Carroll model of intelligence. In, D. Flanagan & P. Harrison (Eds.), Contemporary Intellectual Assessment: Theories, Tests, and Issues (3rd ed.) (p. 99-144). New York: Guilford. Retrieved from http://www.iapsych.com/articles/schneider2012.pdf

151
Schneider, W. J., & McGrew, K. (2013). Individual differences in the ability to process information. In, B. J. Irby, G. Brown, R. Lara-Alecio, & S. Jackson (Eds.), The Handbook of Educational Theories. (p. 767-782). Information Age Publishing, Inc. Retrieved from http://www.iapsych.com/articles/schneider2013.pdf
Schooley, A., & Kuhn, J. R. (2013). Early indicators of NCLEX-RN performance. Journal of Nursing Education, 52(9), 539-542, doi:10.3928/01484834-20130819-08
Shipley, W. C., Gruber, C. P., Martin, T. A., & Klein, A. M. (2009). Shipley-2 Manual. Los Angeles: Western Psychological Services.
Simon, E. B., McGinnis, S. P., & Krauss, B. J. (2013). Predictor variables for NCLEX-RN readiness exam performance. Nursing Education Perspectives, 34(1), 18-24. doi:10.5480/1536-5026-34.1.18
Snow, R. E. (1999). Commentary: Expanding the breadth and depth of admissions testing. In S. Messick (Ed.) Assessment in higher education (pp. 133-140), Hilldale, NJ: Erlbaum
Stransky, D., Wilcox, L. M., & Dubrowski, A. (2010). Mental rotation: Cross-task training and generalization. Journal of Experimental Psychology: Applied, 16(4), 349-360. doi:10.1037/a0021702
Stull, A. T., Hegarty, M., & Mayer, R. E. (2009). Getting a handle on learning anatomy with interactive three-dimensional graphics. Journal of Educational Psychology, 101(4), 801-816. doi:10.1037/a0016849
Suhonen, R., Schmidt, L. A., & Radwin, L. (2007). Measuring individualized nursing care: assessment of reliability and validity on three scales. Journal of Advanced Nursing, 59(2), 77-85. doi:10.1111/j.1365-2648.2007.04282.x
Tavakol, M. & Dennick, R. (2011). Making sense of Cronbach’s alph. International Journal of Medical Education, 2, 53-55. doi:10.5116/ijme.4dfb.8dfd
Terlecki, M. S., Newcombe, N. S., & Little, M. (2008). Durable and generalized effects of spatial experience on mental rotation: Gender differences in growth patterns. Applied Cognitive Psychology, 22, 996-1013. doi:10.1002/acp.1420
Thompson, B., & Melancon, J. G. (1987). Measurement characteristics of the group embedded figures test. Educational and Psychological Measurement, 47, 765-772. doi:10.1177/0013164490502011
Tilley, D. D. S. (2008). Competency in nursing: A concept analysis. The Journal of Continuing Education in Nursing 39(2), 58-64.
Timmerman, D. (2008). 015 – Promoting clinical excellence by supporting nurses through certification. Journal of Pediatric Nursing 23(2), pp e13 – e14. doi: 10.1016/j.pedn.2008.01.046

152
U.S. Department of Health and Human Services, Health Resources and Services Administration, Health Professionals, Workforce Analysis. (2010). The registered nurse population: Findings from the 2008 national sample survey of registered nurses (2010). Retrieved from http://bhpr.hrsa.gov/healthworkforce/rnsurveys/rnsurveyfinal.pdf
Van Terheyden, N. (2007, Nov 26). Clinical knowledge doubles every 18 months. Message posted to http://speechrecognition.wordpress.com/tag/clinical-knowledge/
Voyer, D., & Doyle, R. A. (2010). Item type and gender differences on the mental rotations test. Learning and Individual Differences, 20, 469-472. doi:10.1016/j.lindif.2010.04.010
Voyer, D., Voyer, S., & Bryden, M. P. (1995). Magnitude of sex differences in spatial abilities: A meta-analysis and consideration of critical variables. Psychological Bulletin, 117(2), 250-270. doi:10.1037/0033-2909.117.2.250
Wai, J., Lubinski, D., & Benbow, C. P. (2009). Spatial ability for STEM domains: Aligning over 50 years of cumulative psychological knowledge solidifies its importance. Journal of Educational Psychology 101(4), 817-835. doi:10.1037/a0016127
Wanzel, K. R., Hamstra, S. J., Anastakis, D. J., Matsumoto, E. D., & Cusimano, M. D. (2002). Effect of visual-spatial ability on learning of spatially-complex surgical skills. The Lancet, 359, 230-231. doi:10.1016/S0140-6736(02)07441-X
Weld, K. K., & Bibb, S. C. G. (2009). Concept Analysis: Malpractice and modern-day nursing practice. Nursing Forum 44(1), 2-10. doi:10.1111/j.1744-6198.2009.00121.x
Western Psychological Services. (2012, May). Test with confidence. Retrieved May 2012, from http://portal.wpspublish.com/portal/page?_pageid=53,248007&_dad=portal&_schema=PORTAL
Williams, H. F., & Counts, C. S. (2013). Certification 101: The pathway to excellence. Nephrology Nursing Journal 40(3), 197-209.
Witkin, H. A., Oltman, P. K., Raskin, E., & Karp, S. A. (2002). Group embedded figures test sampler set, manual and sample figures and scoring. Available at mindgarden.com
Wolkowitz, A. A., & Kelley, J. A. (2010). Academic predictors of success in a nursing program. Journal of Nursing Education, 49(9), 498-503. doi:10.3928/01484834-20100524-09
Wynd, C. A. (2003). Current factors contributing to professionalism in nursing. Journal of Professional Nursing 19(5), 251-261, doi:10.1016/S8755-7223(03)00104-2
Yilmaz, H. B. (2009). On the development and measurement of spatial ability. Retrieved January 15, 2011, from International Electronic Journal of Elementary Education: http://www.iejee.com/1_2_2009/yilmaz.pdf







