So, You Think You Know
What You Are Looking For –
What is Hiding From You?
Carol Calabrese, R.N., B.S., C.I.C.
Senior Clinical Advisor – Infection Prevention
Indiana Annual Fall Conference
Conflict of Interest
I am employed by Diversey, however, the
content of this presentation was developed
solely from my experience as an Infection
Preventionist and Evidence Based literature
Goals and Objectives
Describe 2 different types of rounds
State 3 goals of conducting rounds
Identify the process(s) in which solutions to the findings are
acted upon

IC.01.03.01, EP 1:
The [organization] identifies risks for acquiring and
transmitting infections based on the following: Its
geographic location, community, and population served.
(See also NPSG.07.03.01, EP 1)

Rounding Types
Rounding to Influence
Environment of Care Rounds
Infection Prevention Rounds
Point Prevalence

Rounding to Influence
Rounding to influence:
is one element of an evidence-based bundle of
leadership methods used in highly reliable
organizations that is focused on driving the
successful execution of specific safety or
infection control practices.

EOC – Environment of Care
EC.04.01.01: The [organization] collects information to
monitor conditions in the environment
EP 1: The [organization] establishes a process(s) for
continually monitoring, internally reporting, and investigating
the following: Utility systems management problems, failures,
or use errors

Environment of Care
Frequency
Who performs
The physical building
The equipment used to support patient care or safely operate
the building or space the people – including those working in
the hospital, other patients and anyone else who enters the
EOC
The people – including those working in the hospital, other
patients and anyone else who enters the EOC

EC Toolbox
Environment of Care documentation checklist
https://www.jcrinc.com/my-account/free-resources/
Infection Prevention Rounds

ENVIRONMENTAL HYGIENE TJC/CMS ASSESSMENT TOOLHOSPITAL EXAMPLE
TAG Environmental Hygiene TJC/CMS Assessment YES NOUnable to
Observe N/A Number Follow Up Notes
2.D.1 /LLD #4
During environmental cleaning procedures, personnel wear appropirate
PPE to prevent exposure to infectious agents or chemicals (PPE can include
gown, gloves, masks, and eye protectetion
X
Use of PPE was noted when entering rooms of patients
on Precautions. However, when dispensing chemicals,
staff verbalized that PPE is not used.
2.D.2
Environmental surfaces in patient care areas are cleaned and disinfected
using an EPA - registered disinfectant on a regular basis (e.g., daily), when
spills occure and when surfaces are visibly contaminated. Note: High- touch
surevaces (e.g., bed rails, overbed table, bedside commode, lavatory
surfaces in patient bathrooms) are cleaned and disinfected more frequently
than minimal touch surfaces
x
This is not well defined. High touch surfaces, based upon
P/P are only cleaned once per day. Education regarding
increased cleaning frequency and expectations needs to
be evaluated and supported by senior leadership
2.D.3
After a patient vacates a room, all visibly and potentially contaminated
surfaces are throughly cleaned and disinfected and towels and bed linens
are replaced with clean towels and bedlinens
X *? Use of approved products
2.D.4
Cleaners and Disinfectants, including disposable wipes, are used in
accordance with manufacturer's instructions (e.g., dilution, storage, shelf -
life, contact time)
x
*Wipes used for room disinfection are not designed for
cleaning. They are like a paper towel and lack the design
to clean
2.D.5Separate clean (laundered if not disposable) cloths are used to clean each
room and corridorx x
2.D.6
Mop heads and cleaning cloths are laundered at least daily using appropiate
laundry techniques (e.g., following manufacturer instructions when
laundering microfiber items).
x A combination of string and microfiber mobs are used.
2.D.7
The hospital decontaminates spills of blood or other body fluids according
to its policies and procedures, using appropiate EPA - registered
disinfectants.
x
2.D.8
The hospital has established and follows a schedule for areas/equipmentto
be cleaned/serviced regularly (e.g., HVAC equipment, refrigerators, ice
machines, eye wash stations, scrub sinks)
x
Facilities is responsible for the cleaning of ice machines.
An ice machine was noted to have considerable build up
at the dispenser and around draingage area.
2.D.14
Reusable noncritical patient - care devices (e.g., blood pressure cuffs,
oximeter probes) are disinfected on a regular basis (e.g., after use on each
patient, once daily or once weekly) and when visable soiled.
x x
ER tech observed conducting turnover cleaning, partically
cleaned top surface of mattress, side rails were not
cleaned/disinfected. Cables and bld pressure cuff
cleaned, however, no other surfaces in the bay were
disinfected.
2.D.15
For patients on Contact Precautions, if dedicated, dsiposable devices are not
available, noncritical patient - care devices are disnfected after use on each
patient,
X
Disinfectants, both a quat/alcohol and bleach were
availble in the majority of patient rooms. Bleach should
only be available if pt with CDI, C auris, or Norovius -
some equipement have brackets to hold disinfectant
container while others don't. Did not observe equipment
being wiped between patients. One nurse stated that
they use bleach on everything.
2.D.16/TJC LLD #1/NsgTracer #2, There is clear disgnation of responsibility for disinfection of reusable
noncritical patient - care devices.x
Staff verbalized that they are unsure of whO is to clean
certain equipment or who is cleaning the invasive
procedural area of the Hybrid Cath Lab - the hybrid cath
lab can be used to perform, open heart surgery,
placement of ICD and/or pacemakers. There is not clear
distincition of a "restricted" area entering the
department. Flies found (6) dead on floor in core area of
this department.

MONTHLY INFECTION CONTROL ROUNDS
DATE RECORDER
Completed by:DQM/Infection Control Practioner, or designee
Specific Directions: Indicators with an * require sampling of 10 observations or interactions. Record as number met, i.e., 8/10
INDICATOR MET NOT MET N/A ACTION TAKEN IMMEDIATELY FOLLOW-UP NEEDED
HALLS & COMMON AREAS
Floors are clean, free of trash and boxes on floors
Lights are free of dust/bugs
*
Furniture is clean & in good repair (nurse station & visitor areas)
Bottom storage shelves have 6" clearance for cleaning
Linen carts are covered
Linen carts are in good repair
Nothing stored on top of linen carts

PERSONNEL STANDARDS Compliant: YES Compliant: NO DESCRIPTION/COMMENTS
Attire:
Properly tied surgical masks
Surgical caps/hood covering all hair
Dress code followed:
Jewelry
Fanny packs
Long sleeves
Turtlenecks
Shirts tucked
Only those in appropriate attire enter the OR
Surgical Hand Scrub
Product used Name product:
Correct procedure for product
Nail cleaner used for first case
No artificial nails, natural nails correct length
Sterile Field:
Sterile items left open no > than 30 minutes prior to patient entering room
Scrubbed persons maintain sterility of sterile gown, gloves, supplies
Hands remain above waist
Sterile field constantly monitored
Items introduced into sterile field opened, dispensed, transferred by methods to maintain sterility/integrity
Items/devices dropped below level of the OR table are considered contaminated
All personnel moving in/around sterile field do so in manner to maintain sterility
Adjacent sterile fields not at disparate heights
Separation of sterile team from non-sterile team maintained
Staff do not turn back to sterile field
Traffic in and out of room kept to minimum
ADDITIONAL STANDARDS Compliant: YES Compliant: NO DESCRIPTION/COMMENTS
Anesthesiology:
Drainage bags kept off the floor
Aseptic practice used for IV tubing, fluids, medications
Aseptic practice used for all invasive procedures: (epidurals, blocks, IV insertion)
Anesthesia cart appears clean
Cleans shared equipment (e.g, stethoscope) between cases
OSHA/Bloodborne Pathogens
Appropriate eye protection used
Sharps containers not overfull
Shoe covers/boots if indicated
Surgeons/first assistants double gloved (recommended)
Circulators wear latex/nitrile gloves for handling contaminated items. Performs hand hygiene after glove removal
Sharps are passed in a basin or by using neutral zone rather than by hand
Sharps safety devices Devices used:
General Infection Control:
Patients with communicable disease handled appropriately
Sterile team removes gloves and washes hands at end of case
Policies regarding flash sterilization are followed
Personnel appear free from communicable disease (no open skin lesions on hands/face)
Observers comply with “Observers Protocol” for Surgical Services
Clean, sterile, and soiled items are kept separate
Patient transported via clean corridor
OR OBSERVATION CHECKLIST
Date of observation: ______ Time: from ________ to ________ OR# ________ Observers:
____________________________________
Procedure(s): _______________________ Service: _____ Attending: _____________ Anesthesia
Attending: ____________ # Persons in OR: ____
Specify parts of procedure observed:
___________________________________________________________________________________

SURGERY INFECTION PREVENTION & CONTROL CHECKLISTScore: 0=non-compliant or 1 = compliant for each measure assessed. Mark N/A if not assessed.Compliance rate: _____/______ measures met OVERALL________%
CATEGORY SCORE COMPONENTS
PREOPERATIVE AREA
HAND HYGIENE
Hand hygiene performed:performed before & after patient contactafter removing glovesbefore performing invasive proceduresafter contact with blood, body fluids, or contaminated surfaces
Alcohol based hand rubs available
Standard Precautions used for all patients
HAIR REMOVAL
Clippers used for needed hair removal
OPERATIVE AREA
PPE
Personal protective equipment, including mask with face shield or mask with goggles, donned when splashing is likely
Appropriate PPE available & used
ATTIRE
Rings, watches, bracelets must be removed before beginning surgical hand scrub
All jewelry is confined within scrub attire or removed when personnel enter the semirestricted or restriced zones of the surgical suite
A fluid-resistant mask is worn in the restricted zones of the operating suite.
Hair covering: covers & contains all hair
Artificial fingernails or extenders are restricted. Natural nails are kept < 1/4 inch long.
New mask per case, not hanging around neck
Shoe covers removed when soiled, torn & when leaving the surgical area
Hoods cover facial hair.
SHARPS
Sharps disposal in rigid containers enforced.
Sharps containers replaced when 3/4 full.
EQUIPMENT
Mattresses & vinyl coverings intact on all positioning equipment (OR beds, arm boards, roller, etc)
Stored equipment has dust covers
ENVIRONMENT
OR lighting intact
Operating rooms are terminally cleaned daily
Floors & horizonatal surfaces cleaned on a daily basis
Department maintained in a clean & orderly manner
Traffic is restricted to authorized appropriately attired personelL
Required use of disinfectants & germicides in accordance with manufacturers' instructions.
Appropriate use of facility & medical equipment, including air filtration equipment, UV lights, etc.
Fluid warmers <104 degrees F
Blanket warmers <130 degrees F
Emergency carts: code carts, malignant hyperthermia cart checked for expired supplies & medications.
Linen and waste bags remain in the OR room until the patient has been transferred out of the room
Red bag waste handled appropriately
OSHA compliant eyewash/shower equipment available in decontamination & clean processing areas; tested weekly
INTRAOPERATIVE
ASEPSIS SURGICAL ENVIRONMENT
Sterile technique used for all sterile procedures.
Scrubbed persons wear sterile gowns & gloves
Sterile drapes used to establish a sterile field
Items used within sterile field are sterile
sterile field is monitored and maintained.
All items introduced onto a sterile field are opened, dispensed, & transferred by methods that maintain sterility & integrity.
All personnel moving within or around a sterile field maintain integrity of sterile field.
Policies & procedures for basic aseptic technique are written, reviewed annually, & readily available within the practice setting.
Surgical counts completed appropriately: sponge count per package
Surgical instruments counted by type or grouping
VIALS/MEDICATIONS
Single dose (single-use) vials used for only one patient.
Measures specific to safe practices for injecting medications & saline or other infusates.
Multi-dose injectable medications used for only one patient
No multiple-use fluids (e.g., alcohol, betadine, lubricant)
Medications locations secured. (e.g., satellite pharmacy, anesthesia carts)
OTHER
DISINFECTION
Blood glucose meters disinfected between patients
OneSource: Employees knowledgeable of reference used for access to manuracturer recommendations.
Disinfection of medical equipment is done according to manufacturer recommendations.
STORAGE & TRANSPORT
Items are stored in a manner that will not compromise sterility
No expired supplies
Sterile supplies stored in closed cabinets or open shelves with solid bottoms, or bottom shelves with liners.
Linen stored & covered.
Supplies are removed from their outside (shipping/transport) containers before entering the operating room.
Items transported are covered or contained during transport.
Soiled items are covered in containers or case carts during transport from the individual operating room through the semirestricted zone to a decontamination area for temporary storage until reprocessing.
All soiled items are contained & stored separately from clean or sterile items.
Transport carts have solid bottom shelf
Carts, covers, and containment devices are disinfected between uses.
REFERENCEs:
1. Allen George, Frye Cathy. Infection Control A practical guide for health care facilities. Operating Room, Chapter 6.2. APIC text of infection control & epidemiology. Available from: http://text.apic.org/item-49/chapter-45-surgical-services. Retrieved May 22, 2014.

Point Prevalence
PPE for
Isolation
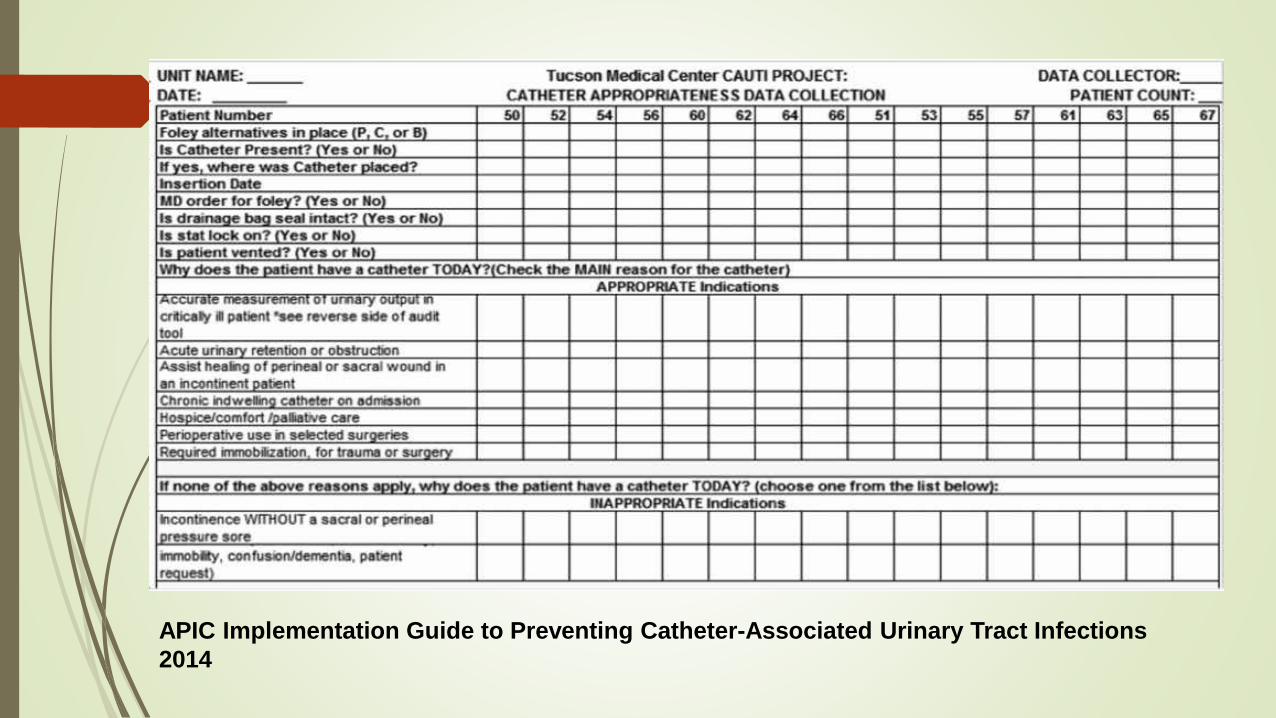
APIC Implementation Guide to Preventing Catheter-Associated Urinary Tract Infections
2014
Rounding Goals
Identify Compliance
Build relationships
Discuss concerns
Identify what is going well

In The News
Clinical Leadership & Infection Control
Bone, blood, bugs found on instruments at Denver hospital after surgical
breach, report says
Written by Alyssa Rege | June 14, 2018

Clinical Leadership & Infection Control
Infection Prevention Rounds: 15 Items to Address
March 21, 2011
https://www.beckersasc.com/asc-quality-infection-control/infection-
prevention-rounds-15-items-to-address.html
ww.apic.org/ambulatorynewsletter.

Across the board
Items that need to be addressed across the
facility

Got Singles
Are departments using items sold as “single use” that they are “cleaning” and using again?
Salter Labs ThermiSense Sensor Cadwell Adult Kit

Transport of Instruments
TJC
AAMI
Accreditation and Certification
4-1-1 on Survey Enhancements: New scoring revisions for
IC.02.02.01 now in effect
Infection Control (IC) standard IC.02.02.01 — which requires
hospitals to reduce the risk of infections associated with
medical equipment, devices and supplies — continues to be
one of the most commonly cited standards listed as
noncompliant. In 2017, 72 percent of surveyed hospitals and
critical access hospitals were found to be noncompliant with
this standard.
After a careful evaluation of high-level disinfection (HLD) and
sterilization process steps, The Joint Commission has refined
its scoring to focus on the process steps that pose the highest
risk to patients if they fail.
Sept 5, 2018

Central Supply
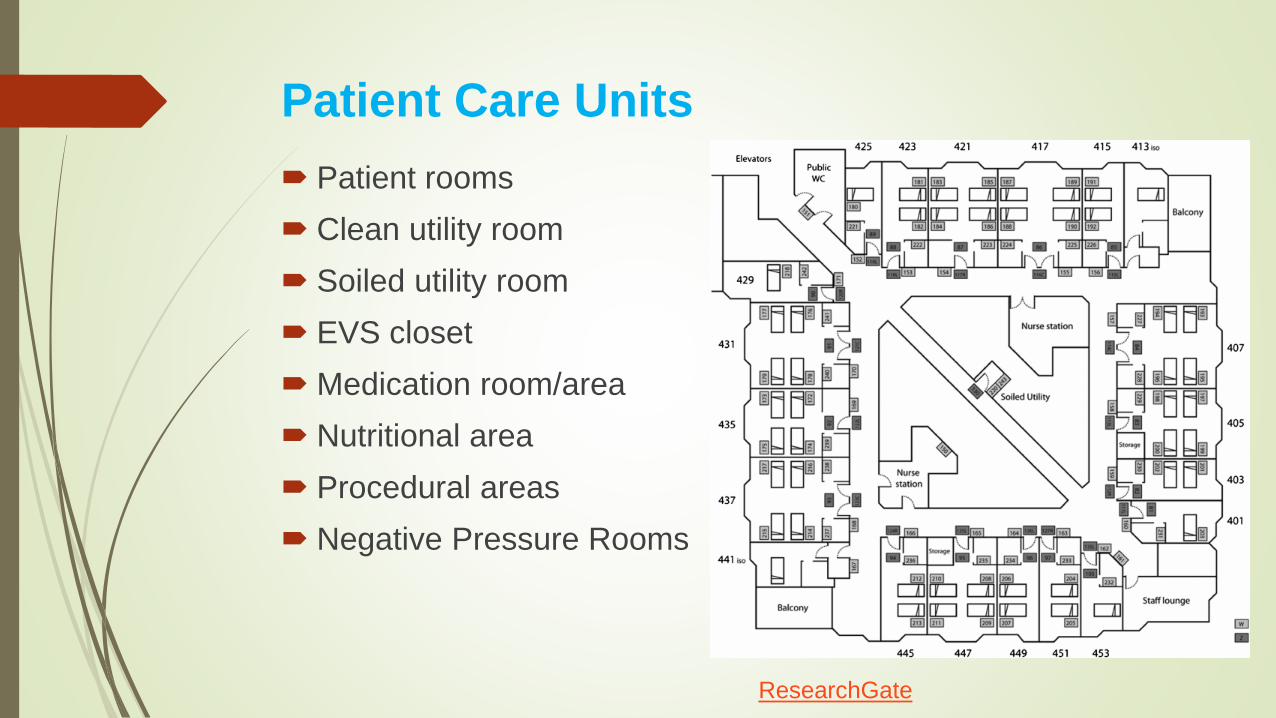
Patient Care Units
Patient rooms
Clean utility room
Soiled utility room
EVS closet
Medication room/area
Nutritional area
Procedural areas
Negative Pressure Rooms
ResearchGate

Endoscopy/Bronchoscopy
Process for transporting used
Storage
Re-processing – “Hang Time”
https://www.hmark.com/7day.php
Linen/Laundry Services
Curtain changing rotation
Tour of where laundry services are done
Transportation of clean and soiled laundry
Use the Healthcare Laundry Accreditation
Council’s standards as assess the facility

Operating Rooms
OR turnover
Monitoring of traffic flow
Decontamination room
Foley and central line insertion
Line access
Terminal Cleaning
Instruments handling
Immediate Use SterilizationGetty Images
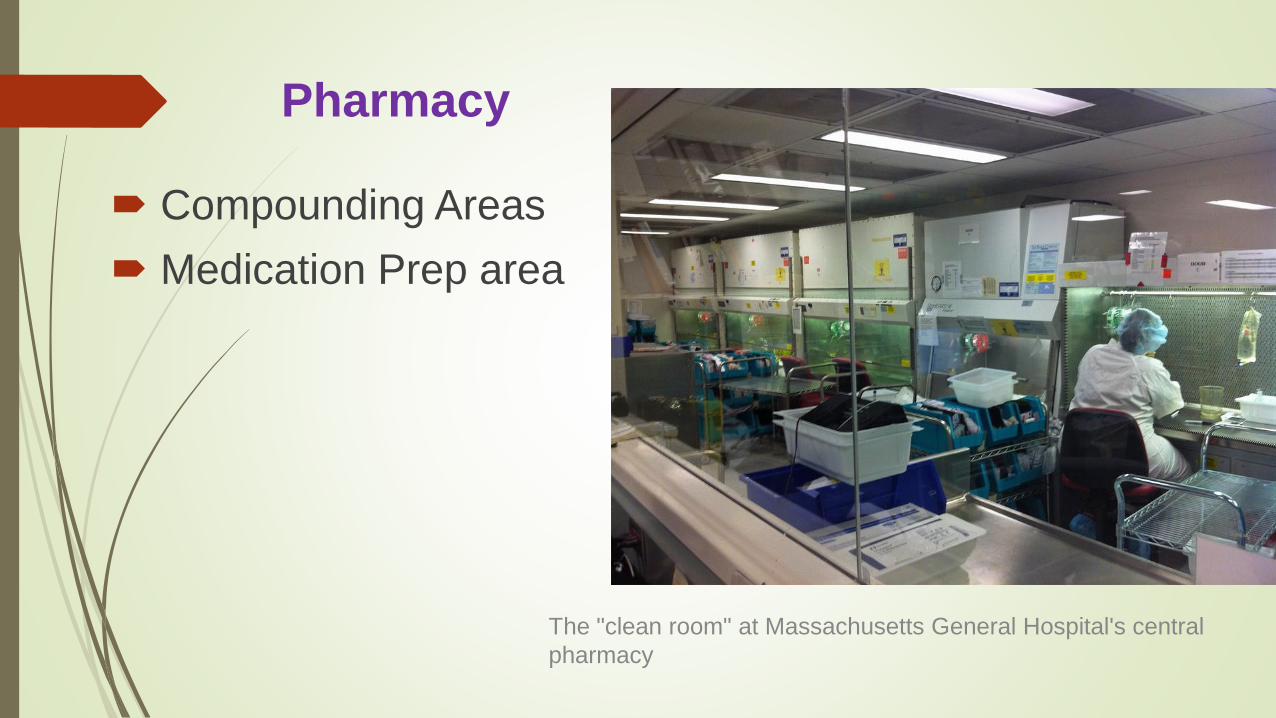
Pharmacy
Compounding Areas
Medication Prep area
The "clean room" at Massachusetts General Hospital's central
pharmacy
Radiology
Interventional Radiology – room turnover and
terminal daily cleaning, traffic flow pattern, hospital
provided scrubs
Management of injectable dyes
Cleaning of equipment and lead aprons
Foley management in MRI
Insertion of Central Line
Dyes
Multi-dose vials

Cardiac Catheterization Lab/Interventional
Radiology
Scrubs – hospital provided – attire
Room turnover/Terminal cleaning logs
Doors/traffic flow
Ventilation
Dust
Aseptic technique
Management of contaminated instruments

Respiratory Therapy
Bronchoscopy scope HLD
Humidifiers and dehumidifiers
Sleep lab – CPAP equipment, Thermistors,
monitor cables
Cleaning of ventilator equipment
? Use of multi – dose inhalers

Sterile supplies where they don’t
belong
Rooms without temp and humidity control
Rotation of stock
Checking for outdates
Dust control
Shoe Leather Rounding – Going for a
Walk!
Being visible is good
Staff invariably have questions
related to their area, or perhaps
outside of the hospital
Being approachable is good
We don’t always need to have
paper in hand, so to speak!
Shoe Leather Infection ControlMifa

What do you do with all the findings?
Reporting – to whom, what and when
Resolution of findings

The APIC /JCR
Infection Prevention and
Control Workbook Third Edition
Summary
What are possible concerns that can be observed across the organization
Infection Prevention covers the breath and depth of an organization
It is important to have a process of reporting and resolution
There are many different types of rounds to aide in identifying what may need to be addressed








