
SM2015 - BELIZE
SM2015 Initiative
Innovative Approaches
May 2012

Content
—Health profile—Health System
SM2015
—Objective—Components—Methodology

Demographic transition
— A reduction in the fertility rate (3.3 to 2.7) and increase in life expectancy (73 years) have resulted in population aging
— More than half of the population is below 25 years – 55.6%

Epidemiological transition
— Double burden – increasing non-communicable and degenerative diseases related to lifestyle, behaviors and a longer life-span, combined with the continued occurrence of communicable diseases related to poverty, sanitation, environmental conditions, malnutrition and sexual risk behaviors
— NCD’s are among the main causes of morbidity and mortality

— Maternal and infant mortality are low compared to other countries of the region and appear to be declining
147
101
161
113
82
139
100
134
42
82
58
111
40
64
134
42
85
43
53.9 53.7
0
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
Maternal Mortality Ratio 1991-2011
04-05 Surveillance system
05 Protocols Training
09 Quality improvement MNC
10 Protocols Training
Source: MOH, Health Statistical abstracts
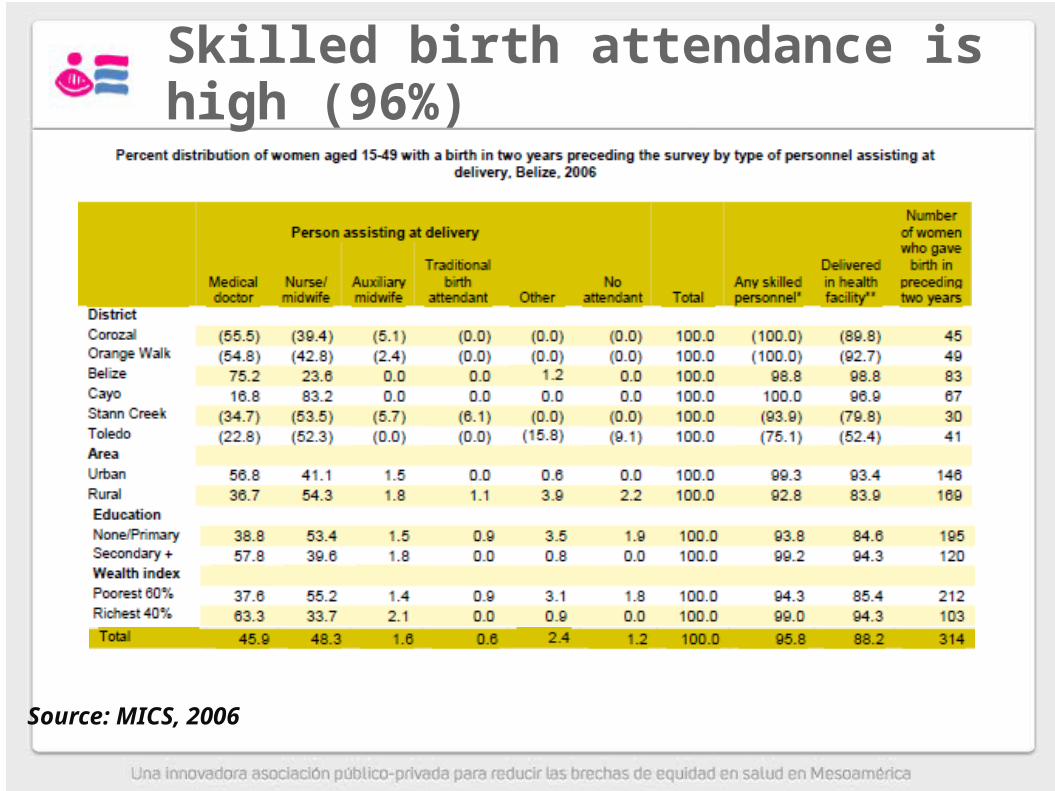
Skilled birth attendance is high (96%)
Source: MICS, 2006

Process—Planning and resource mobilization—Standards and indicators—Training —Policy—Framework—Monitoring tools
Demonstration phase in 2 hospitals—70% reduction in neonatal death—65% reduction in birth asphyxia
Spread to rest of hospitals in 2011
Adapted from University Research Company LLC., maternal and neonatal care package [Nicaragua Office]
Quality improvement of maternal and neonatal care since 2009
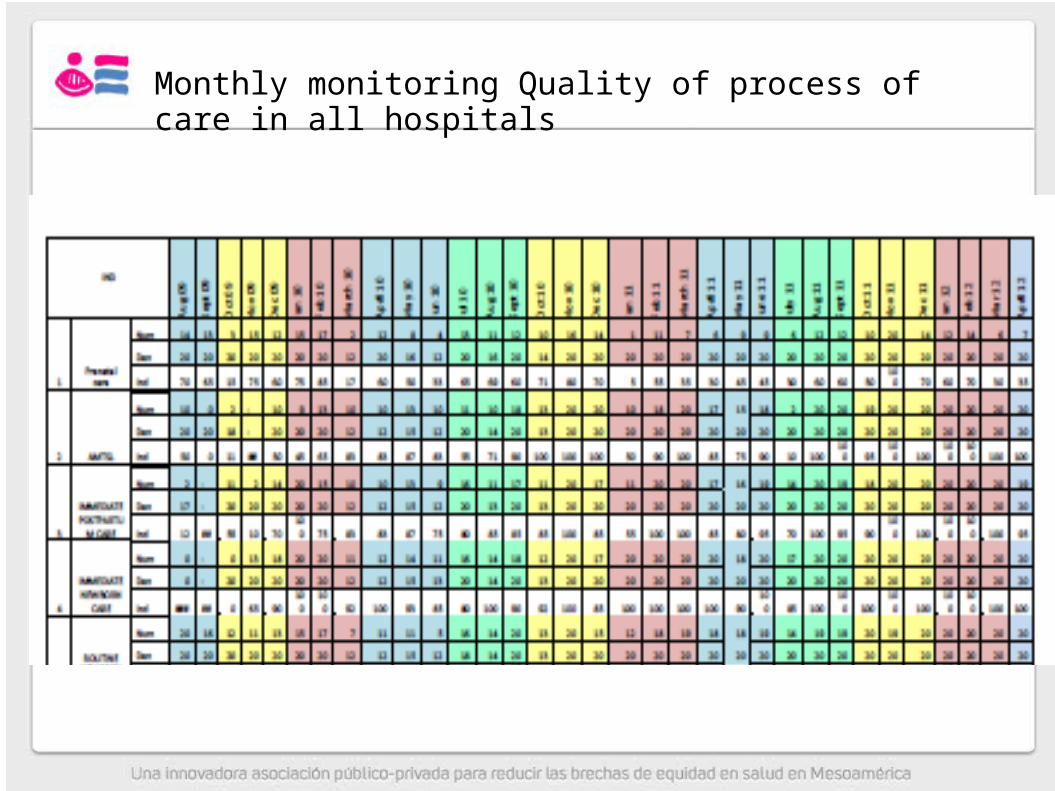
Monthly monitoring Quality of process of care in all hospitals
Strategy sample: random selection and convenience,
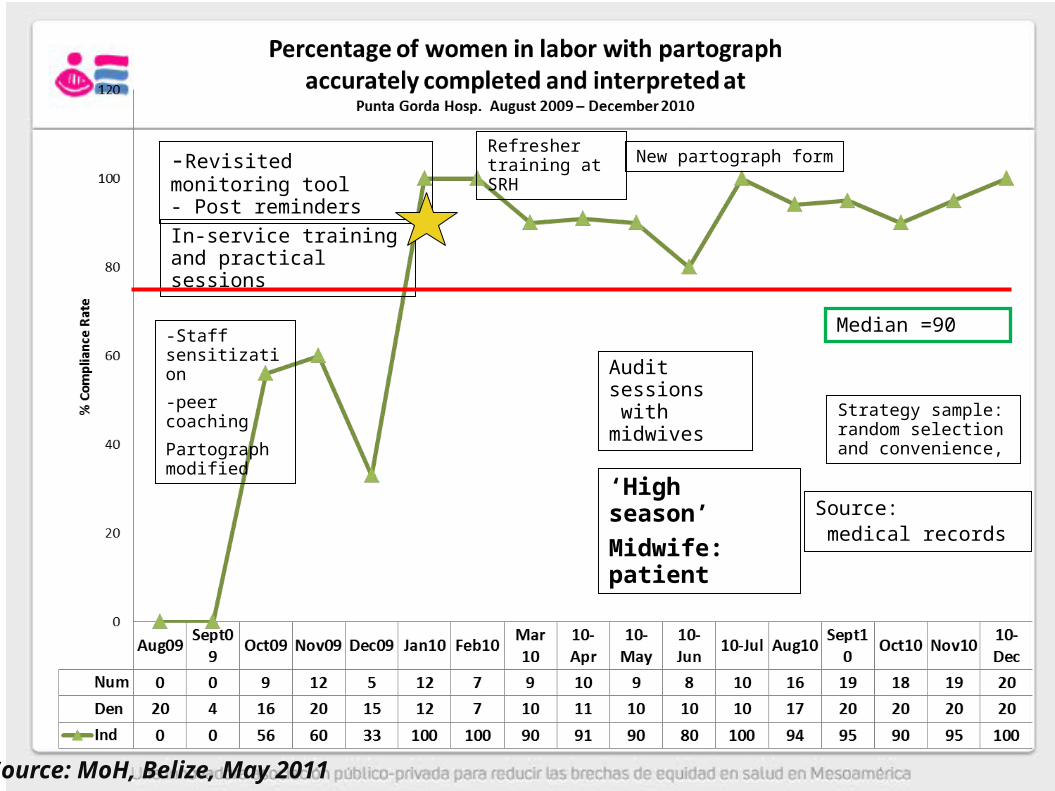
-Staff sensitization
-peer coaching
Partograph modified
-Revisited monitoring tool- Post reminders
In-service training and practical sessions
‘High season’
Midwife: patientSource: medical records
Refresher training at SRH
Audit sessions with midwives
New partograph form
Median =90
Source: MoH, Belize, May 2011
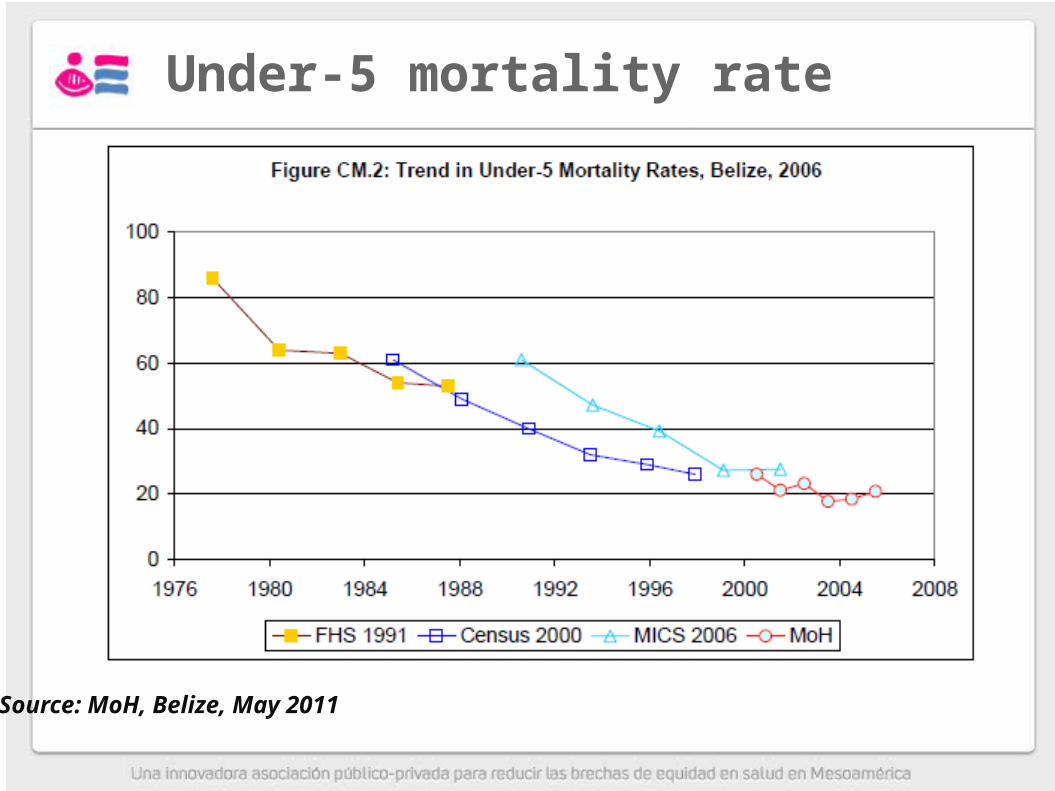
Under-5 mortality rate
Source: MoH, Belize, May 2011

Analysis of protected cohorts against Measles/Rubella by year of birth and Vaccination
Strategies 1962-2010
0
10
20
30
40
50
60
70
80
90
100
Y ear of Birth
% V
ac
cin
ate
d
0
10
20
30
40
50
60
70
80
90
100
% V
ac
cin
ate
d
Routine MMR1 coverage MMR2 coverage 2nd dose MMR 2000 (1-4yrs)95% Measles vaccine 1986 (9mths-3yrs) 91%Measles F/U 1995 (1-4yrs) 85%
Rubella Mass
campaign
(females)
(1998)
MMR vaccine
5-35 yrs
Rubella Mass
Campaign (males)
(2004)
MMR vaccine
5-35 yrs
Coverage 97%
Measles "Big
Bang" (1991)
MMR vaccine
9mths-14 yrs
Coverage 82%
Source: MOH reports to EPI-CAREC

Under nutrition (low height for age) is persistent among certain populations – MICS2006
Poorest/richest– three foldIndigenous / Maya12-23 months of age
Stunting in < 5 year old LSMS 2001 – 17.9MICS 2006 – 17.6
Stunting Standard I Class1996 – 13.72009 - 12.2

Unmet need for reproductive health services, and teenage pregnancy is a priority concern
Adolescent birth rate / 1,000 females 15-19
1995 - 992010 - 73
Contraceptive use prevalence rate MICS2006:
1999 – 56%2006 – 34%

Adolescent Health
• There were 1,356 live births to mothers in the 15-19 year age group, which represents 18.1% of the total live births.
• There was an average of 24 live births to mothers under 15 years.
• From 2001-2005, there were 145 (41 males and 104 females) new HIV Infections in adolescents 10-19 years
• 6.9% of total new HIV Infections (16 ) occurred in the 10-14 age-group;
• Early initiation of sexual activity and the prevalence of STIs are public health concerns in this age group.
• Fourteen suicides and self-inflicted injuries were reported in the 10-19 age group during 2001-2005.
Belize Health Agenda, 2007-2011
Objective
The SM2015 Operation in Belize seeks to:
Increase the coverage of quality reproductive, maternal, neonatal and child health care in the poorest geographic areas and increase the use of information in decision making to reduce neonatal death and increase the use of family planning among adolescents
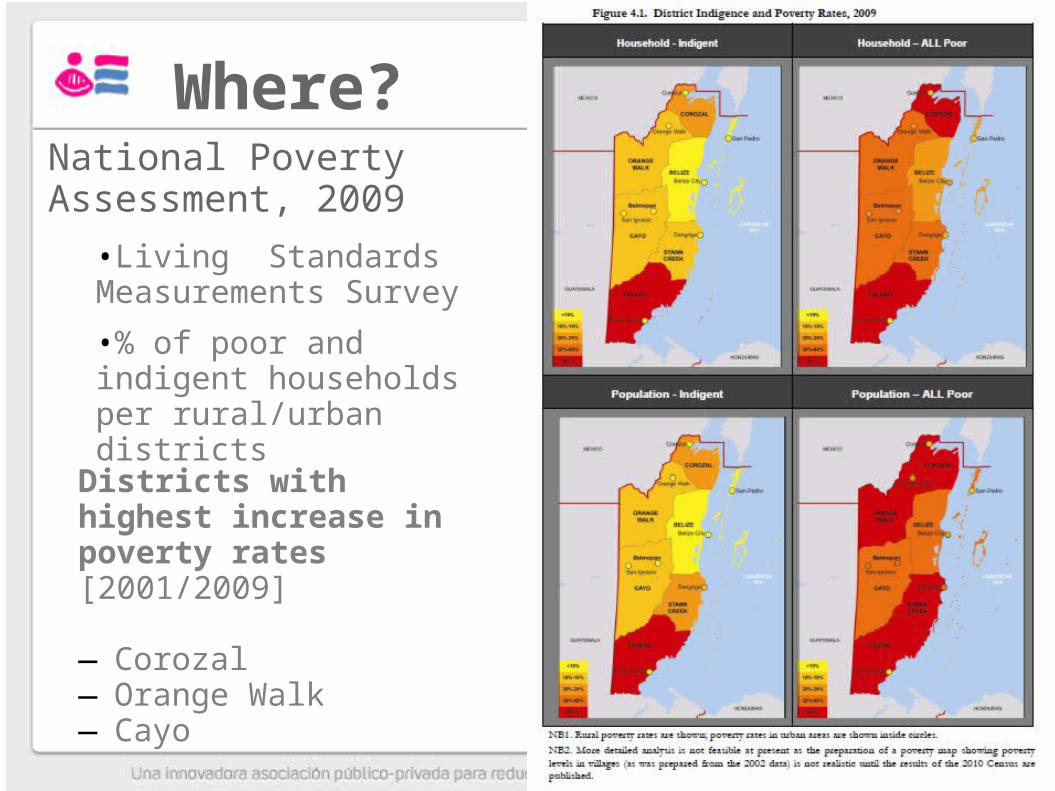
Where?
Districts with highest increase in poverty rates [2001/2009]
—Corozal—Orange Walk—Cayo
National Poverty Assessment, 2009
•Living Standards Measurements Survey
•% of poor and indigent households per rural/urban districts

Component 1: Strengthening use of data to improve MCH service quality
• Expansion of the Collaborative Improvement Model to reduce maternal and child mortality
• Expansion and Utilization of the Belize Health Information System in decision making at the local level
• System of facility based-incentives at the MoH Clinics in the Northern and Western Regions for expanding coverage and quality
• Cross-country exchange and training to improve quality of care
Component 2: Improving Community Based Care
• Monitoring and Evaluation of Community Health Workers (CHW)• Currently rolling out community based nutrition initiatives
that include breast-feeding promotion, growth-monitoring, and waiting for results to decide about rolling out sprinkles
• Incentives for Community Health Workers who reach targets• Currently receive $50 US, exploring incentives that would
improve working conditions such as Basic supplies and equipment for CHW and developing a recognition system
• Improved coordination and training of CHW (recognition of high-risk cases)

Component 3: Increasing the Coverage of Reproductive Health Services
• Increased access to 5 modern family planning methods
• Capacity-building in counseling for Patient/Users
• Differentiated services designed and used by adolescents
Making pregnancy safer : Prenatal, postnatal care, skilled birth attendance, managing complicated pregnancy, childbirth and patients in postnatal period, managing complications
Immediate and routine newborn care, Managing Complicated neonates
Multiple micronutrient supplementation: females 15-49, children
Fortified food: pregnant women and children
Growth promotion and development: community, facilities
5/7 hospitals certified as baby Friendly
Contraceptive methods: public sector and NGO
Supplies procured thru UN Agencies [UNFPA, UNICEF] and IDA Foundation.
Prevention mother to child transmission: HIV & syphilis…….
Interventions

Technical assistance in Maternal and child health including reproductive
health services
Quality improvement of services utilizing collaborative model
—Updating of protocols, standards and indicators, framework and tools for the monitoring of process of care in all areas under the project
Integrated RH services for adolescents
Management of RH supplies
Data management [Belize Health Information System]
Community based care
Health System Structure
Ministry of Health
• Operates in six districts: Belize, Corozal, Orange Walk , Cayo Stann Creek and Toledo
• Employs Service Level Agreements with District Level
• Limited planning function, financing of health supply
• Interest in introducing incentives
National Health Insurance • Started in 2001 and operates in
three areas: Toledo, Stann Creek and South Side Belize
• Utilizes P4P through contracts with PCP in private and public health centers
• Provides free services to all eligible (poorest) populations
• Focuses on pre-natal and postnatal care and deliveries, and primary care for chronic illnesses such as diabetes, hypertension, and asthma.

Health System Network
1 National Referral Hospital
3 Regional Hospitals
Stann Creek, Beloman,
Orange Walk
3 Community Hospitals
Toledo, Corazol, y San Ignacio
Poly-Clinic 2
Health Posts-no
permanent staff
Mobile Units Community
Health Workers
Poly-Clinic 1 (primary care)
NHI Details (1)
• The NHI pays the clinics a monthly member capitation payment• Clinics have an incentive to register as many people as they can
• Each month, the NHI pays clinics 70 percent of the member capitation payment upfront.
• The remaining 30 percent of the payment depends on how the clinic performs on groups of indicators that lead to scores for efficiency• 70 percent of the withheld amount
• quality (20 percent of the withheld amount)
• and administrative processes (10 percent of the withheld amount)
• If an indicator is not fully achieved, then the proportional weight is deducted from the clinic’s total potential payment for that month
Source: Michelle Vanzie, Natasha Hsi, Alix Beith, and Rena Eichler (2010): Using Supply-side Pay for Performance to Strengthen Health Prevention Activities and Improve Efficiency: The Case of Belize. USAID Health Systems 2020, P$P Case Studies.
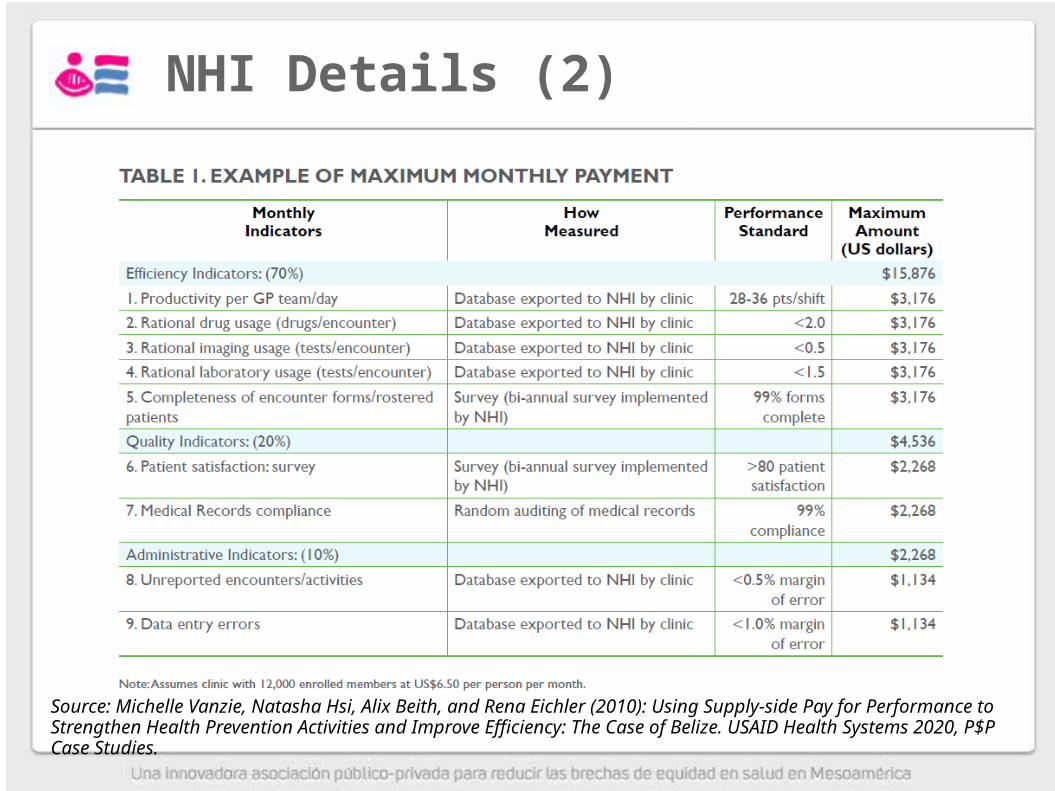
NHI Details (2)
Source: Michelle Vanzie, Natasha Hsi, Alix Beith, and Rena Eichler (2010): Using Supply-side Pay for Performance to Strengthen Health Prevention Activities and Improve Efficiency: The Case of Belize. USAID Health Systems 2020, P$P Case Studies.
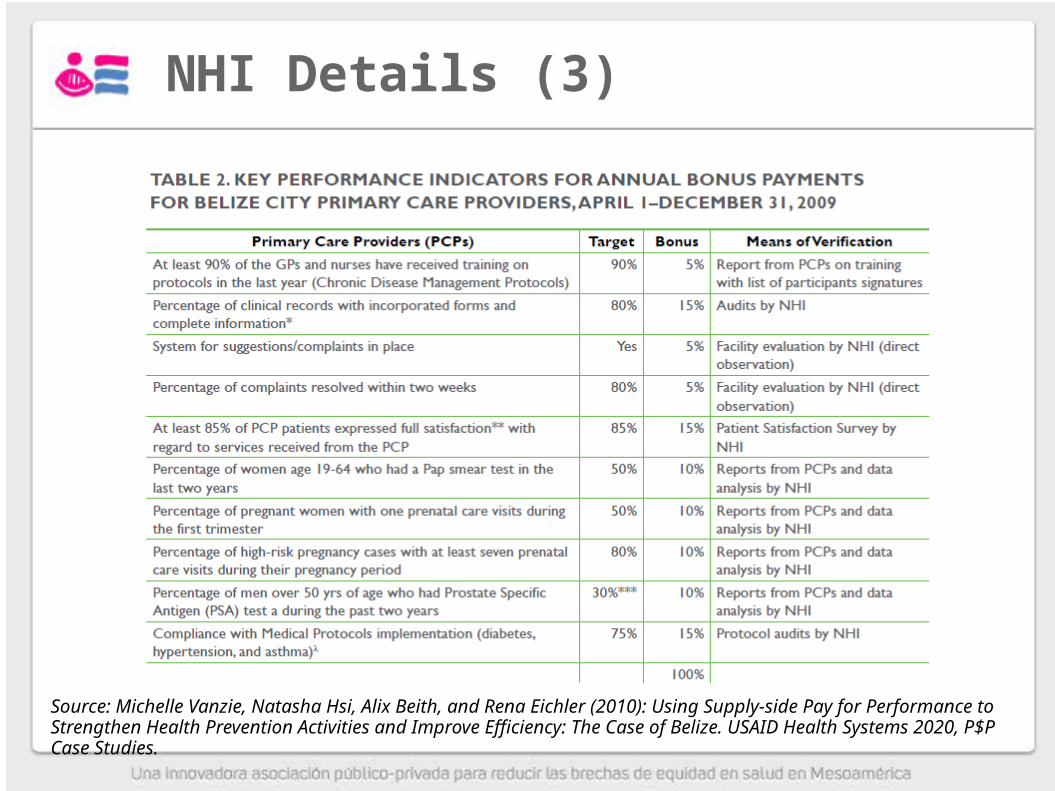
NHI Details (3)
Source: Michelle Vanzie, Natasha Hsi, Alix Beith, and Rena Eichler (2010): Using Supply-side Pay for Performance to Strengthen Health Prevention Activities and Improve Efficiency: The Case of Belize. USAID Health Systems 2020, P$P Case Studies.

Goals 18 monthsIndicador Target Source of verification
Health facilities that have the necessary inputs for providing emergency obstetric and neonatal care according to the norms
75% Health Facility Survey
Health facilities that have the necessary inputs for providing pre- and post natal care according to the norms
85% Health Facility Survey
Health facilities that have submitted a Quality Improvement Fund (QIF) proposal to the national quality audit team
75% Health Facility Survey
Health facilities that have the necessary inputs to provide child health care according to the norms
85% Health Facility Survey
Health facilities that have implemented Quality of Care job aid tools for reproductive health
85% Health Facility Survey
Health facilities that can submit and receive data from the Belize Health Information System (BHIS)
85% Health Facility Survey
Health facilities that have permanent availability of all 5 types of modern family planning methods (injectable, barrier, oral, IUD, permanent) according to the norms
85% Health Facility Survey
Health facilities that have sexual and reproductive health (SRH) educational materials specifically targeted at adolescents
85% Health Facility Survey
Norms for improving the quality of reproductive and child health and nutrition services and for the establishment of a community platform of services adopted
Yes Norm Approved
Community health workers (CHW) trained in the community platform85% Health Facility Survey
District HECOPAB Officers that are currently monitoring the CHWs 85% Health Facility Survey
Health facilities with a mechanism in place for carrying out patient satisfaction surveys85% Health Facility Survey
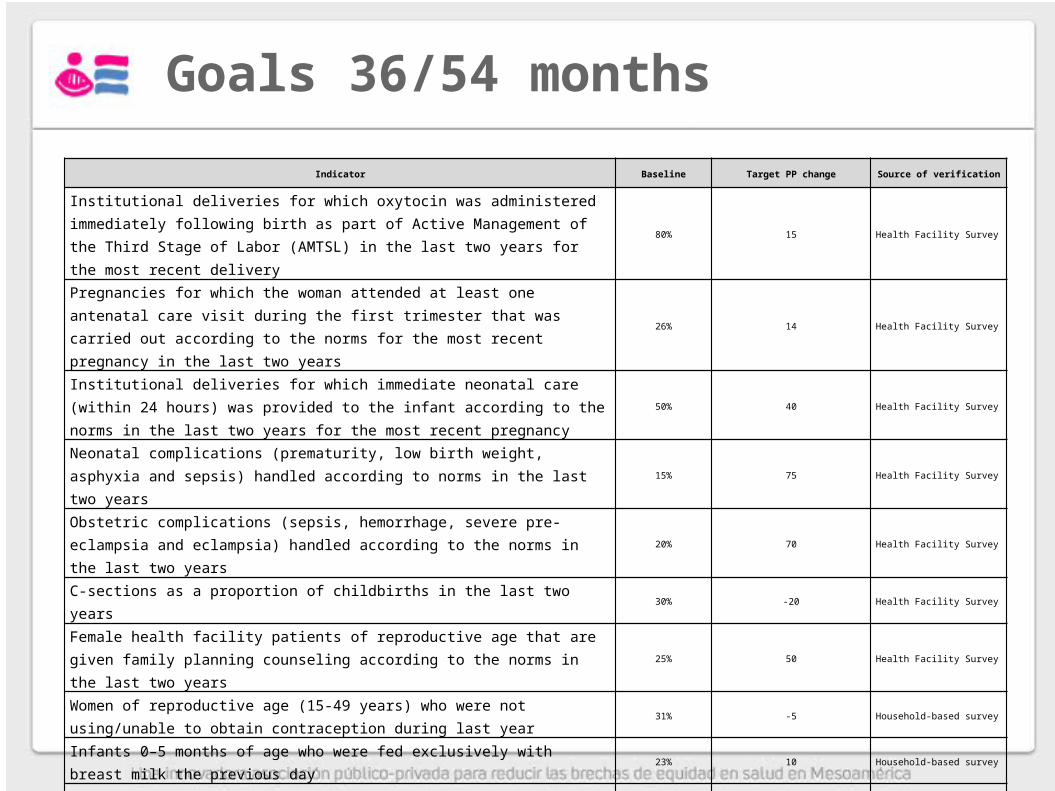
Goals 36/54 months
Indicator Baseline Target PP change Source of verification
Institutional deliveries for which oxytocin was administered immediately following birth as part of Active Management of the Third Stage of Labor (AMTSL) in the last two years for the most recent delivery
80% 15 Health Facility Survey
Pregnancies for which the woman attended at least one antenatal care visit during the first trimester that was carried out according to the norms for the most recent pregnancy in the last two years
26% 14 Health Facility Survey
Institutional deliveries for which immediate neonatal care (within 24 hours) was provided to the infant according to the norms in the last two years for the most recent pregnancy
50% 40 Health Facility Survey
Neonatal complications (prematurity, low birth weight, asphyxia and sepsis) handled according to norms in the last two years
15% 75 Health Facility Survey
Obstetric complications (sepsis, hemorrhage, severe pre-eclampsia and eclampsia) handled according to the norms in the last two years
20% 70 Health Facility Survey
C-sections as a proportion of childbirths in the last two years 30% -20 Health Facility Survey
Female health facility patients of reproductive age that are given family planning counseling according to the norms in the last two years
25% 50 Health Facility Survey
Women of reproductive age (15-49 years) who were not using/unable to obtain contraception during last year
31% -5 Household-based survey
Infants 0–5 months of age who were fed exclusively with breast milk the previous day 23% 10 Household-based survey
Mothers with a child 0-23 months that that can recognize 3 out of 5 signs of danger 20% 40 Household-based survey
Percentage of children aged 6-23 months that consumed 60 sachets of micronutrients in the last 6 months
0 30 Household-based survey
Mothers who gave their children (0-5 9 months) ORS and zinc supplements during the last episode of diarrhea in the two weeks
0 40 Household-based survey








