
Shiva Sharma
PMHx – HTN, Cholecystectomy, hysterectomy, C-Section
PC Rash on left leg Found to be erythematous


Plan? Biopsy Showed melanoma
Now what? Surgery? Scan? Chemotherapy? Radiotherapy? Palliative measures?
CT – scan No evidence of metastatic disease
WLE of satellite lesionConsideration for
electrochemotherapy Patient not keen for this

What options are left? Patient discussed at Melanoma MDM Decided she may benefit from ILI vs ILP

160,000 new cases of melanoma diagnosed each year
More common in women and Caucasians living in sunny climates
Highest rates of incidence in Australia, New Zealand, North America, and northern Europe
48,000 melanoma related deaths world wide

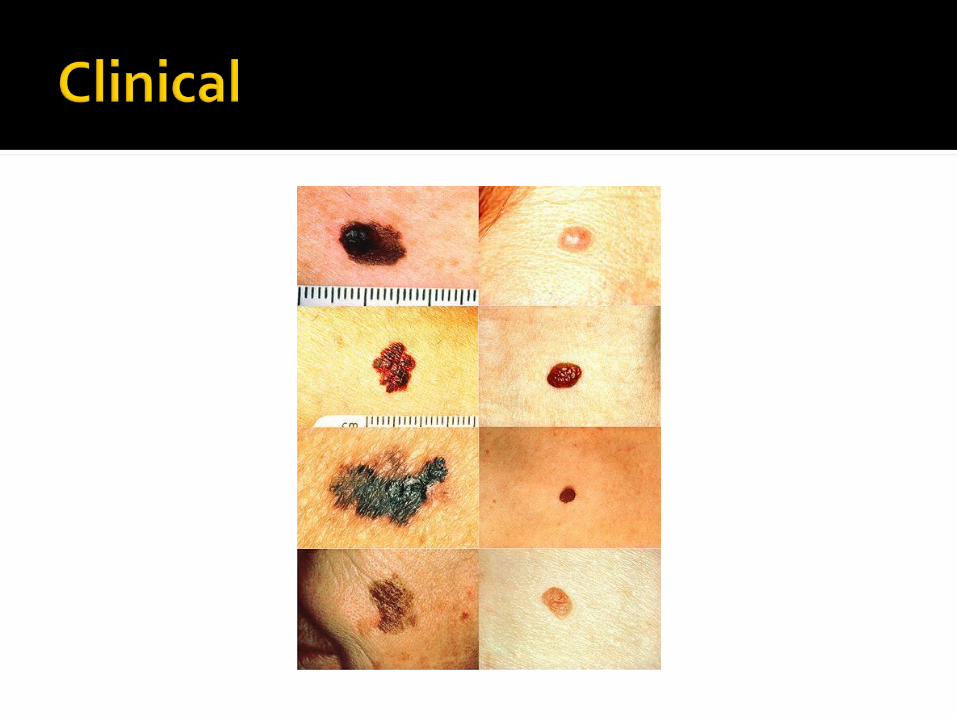
1. Superficial spreading melanoma: Most common; begins initial radial
growth phase then invasion 2. Lentigo maligna melanoma:
Long radial growth phase, Most common in elderly and in sun-
exposed areas
3. Acral lentiginous: Most common form in darkly pigmented
patients Occurs on palms and soles, mucosal
surfaces, in nail beds and mucocutaneous junctions
More aggressive 4. Nodular:
Invasive growth from onset Poor prognosis


Problem How to treat advanced and recurrent
melanoma 10% of patients will develop in-transit
metastases defined by tumour recurrence occurring
between the primary tumour and the regional lymph node.
5ysr = 12% Median survival is 19months

Options ? Surgery Radiotherapy Chemotherapy
Systemic vs Isolated chemotherapy Advantages Disadvantages
ILP First described in 1957 Requires surgical placement of catheters to
the femoral artery and vein Patient on extracorporeal bypass for
procedure High dose chemotherapeutic agent given More invasive
Longer recovery time ILI
First described by Thomson etal. 1998Alternative method to ILP

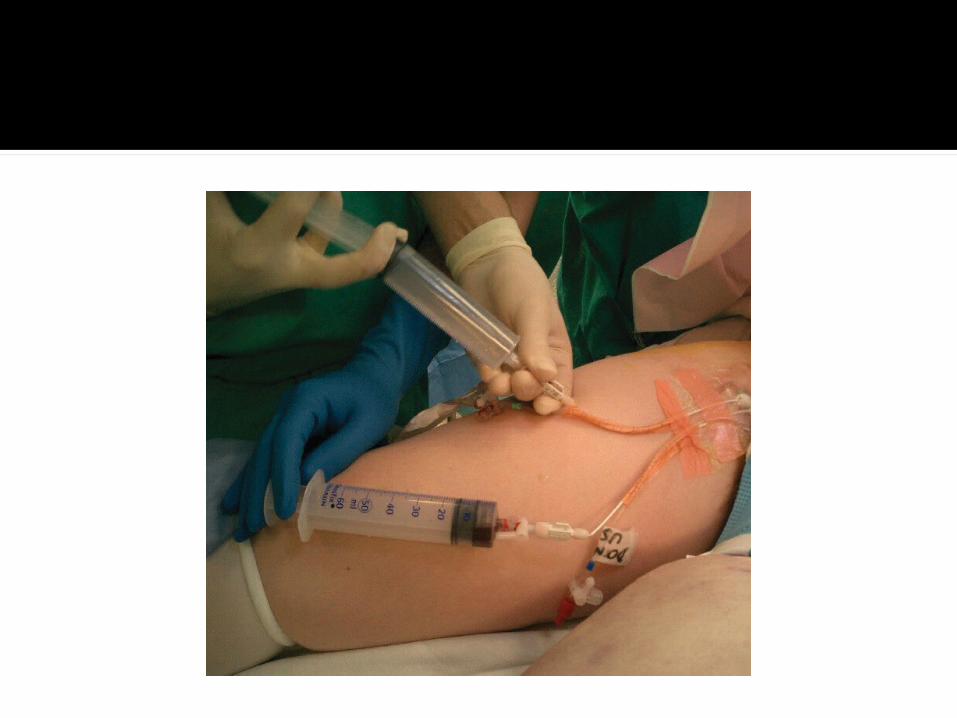
Prophylactic LMWHPre-op limb measurements done by OTUnder radiological guidance 2 catheters
placedContra-lateral groin access site to the
femoral artery and vein (8Fr and 6Fr)Leg kept warm to induce hyperthermiaTransferred to theatre


General anaesthetic30ml of PapaverineTourniquet placedMelphalan and Dactinomycin in
400ml Normal Saline infused over 25min
Circulated over 20minFlushed with 1L Hartmans’

Tourniquet removed Catheters withdrawn
Direct pressure applied for 20min Post-Op care
Leg elevated Regular peripheral pulse checks CK levels Look for signs of Compartment Syndrome Thrombosis

Grade I: no visible effect Grade II: slight erythema and/or oedema Grade III: considerable erythema and/or
oedema Grade IV: extensive epidermolysis
and/or obvious damage to deep tissues with a threatened or actual compartment syndrome
Grade V: severe tissue damage necessitating amputation



ILP and ILI overall response rates approximating 80% complete response rate 30%–50%
Systemic chemotherapy/immunotherapy overall response rates rarely >20% complete response rates rarely >1%–2%
Not a cure for disease Palliative measure to reduce morbidity and
avoid amputation

Isolated Limb Infusion: Technique Description and Clinical Application; Cronin C. etal. J Vasc Interv Radiol 2009; 20:837–841
Isolated limb infusion with cytotoxic agents: a simple alternative to isolated limb perfusion: Thompson JF, etal. Semin Surg Oncol 1998; 14:238 –247.
Isolated limb infusion for melanoma, Z. Al-Hilli etal Surgeon, 1 October 2007 310-12
Harrison’s Manual of Internal Medicine 17th Ed Pp 364-365
Mayo Clinic Internal Medicine Review 8th Ed Pp 173-174







