
ASIAN DEVELOPMENT BANK
ASIAN DEVELOPMENT BANK6 ADB Avenue, Mandaluyong City1550 Metro Manila, Philippineswww.adb.org
Regional Malaria and Other Communicable Disease Threats Trust FundFinal Report
This report details the key achievements of the Regional Malaria and Other Communicable Disease Threats Trust Fund from its creation in 2013 to the first half of 2018. It provides detailed analysis of the results by outcome, profiles specific projects that serve as exemplars of the fund’s impact, and offers insights into how similar trust funds can be managed for success in future.
About the Asian Development Bank
ADB is committed to achieving a prosperous, inclusive, resilient, and sustainable Asia and the Pacific, while sustaining its efforts to eradicate extreme poverty. Established in 1966, it is owned by 67 members—48 from the region. Its main instruments for helping its developing member countries are policy dialogue, loans, equity investments, guarantees, grants, and technical assistance.
REGIONAL MALARIA AND OTHER COMMUNICABLE DISEASE THREATS TRUST FUNDFINAL REPORT
NOVEMBER 2018

ASIAN DEVELOPMENT BANK
REGIONAL MALARIA AND OTHER COMMUNICABLE DISEASE THREATS TRUST FUNDFINAL REPORT
NOVEMBER 2018

REGIONAL MALARIA AND OTHER COMMUNICABLE DISEASE THREATS TRUST FUND
Migrant and mobile populations (MMPs)reached
through community outreach events in Lao PDR and Myanmar trained
Malaria workers, health workers,
and peer educators
in Cambodia, Lao PDR,Myanmar, and Viet Nam
malaria microscopy
IEC materials developed and distributed
Mosquito protection commodities (including LLINs) distributed
Proportion of reached MMPs aware of malaria transmission
Malaria incidence significantly declined in high burdened project sites P. falciparum incidence per 1000
Cambodia Lao PDR
in Asia and the Pacific commit to the malaria elimination road map
Leaders
First ADB health bond launched
developed with Curtin University-WHO Collaborating Center on HIAHealth Impact Assessment (HIA) curriculum
targeting 262 future practitioners
Universitiesin the GMS
government and
HIAtrainingin ADB
• Included in the standard poverty and social analysis training• Integrated into the Air Quality training
HIAdemonstration
in the GMS
Transport
Energy
Urban development
Water supplyand sanitation
special economic
zones
Malaria risk maps developed and used in Cambodia, Lao PDR and Myanmar
Capacity building on Health Information System geo-enabling
Public health facility readiness to provide malaria services mapped in Viet Nam
Unique patient ID assessment tool developed and applied in the GMS
Capacity building for HL7 FHIR in Viet Nam for information systems interoperability
GMS=Greater Mekong Subregion; HIA=health impact assessment; IEC=Information, education and communication; Lao PDR=Lao People's Democratic Republic; LLIN=long-lasting insecticidal nets; MMPs=migrant and mobile populations; NRAs=National regulatory agencies; SF=substandard and falsified.
KEY ACHIEVEMENTS
Malaria elimination dashboard developed
to track progress toward the commitments
Investment cases and tool kitsfinancing malaria elimination
for
• National and regional investment cases • Business cases for private sector
engagement• Malaria elimination transmission a
nd costing model •
analysis toolmalaria elimination and addressing communicable disease threats
ADB-Global Fund memorandum of understanding for blended financing
National Regulatory Agencies (NRAs) operational capacities strengethened in the GMS
New financing mechanisms for
Country and regional NRA capacity development
road maps created
Pharmacovigilance Medical device regulation
Chemistry, manufacturing
and controls
Bioequivalence Standardized approach to
medicine reviews
countries trained on SF incidents and WHO reporting tool
6 portable devices assessed
detect malaria SF medicines
Electronic drug registration information system
established in Myanmar
Landscape analysis of health management information systems in the GMS
Malaria data analytics based on mobile phone call
records in Thailand
Cross-border information
exchangeNumber of monthly disease information
exchanged within cluster provinces in
Cambodia, Lao PDR, and Viet Nam
in 2017
$100 million
Transformational digital interventions
Viet Nam

Creative Commons Attribution 3.0 IGO license (CC BY 3.0 IGO)
© 2018 Asian Development Bank6 ADB Avenue, Mandaluyong City, 1550 Metro Manila, PhilippinesTel +63 2 632 4444; Fax +63 2 636 2444www.adb.org
Some rights reserved. Published in 2018.
ISBN 978-92-9261-364-8 (print), 978-92-9261-365-5 (electronic)Publication Stock No. TCS189605-2DOI: http://dx.doi.org/10.22617/TCS189605-2
The views expressed in this publication are those of the authors and do not necessarily reflect the views and policies of the Asian Development Bank (ADB) or its Board of Governors or the governments they represent.
ADB does not guarantee the accuracy of the data included in this publication and accepts no responsibility for any consequence of their use. The mention of specific companies or products of manufacturers does not imply that they are endorsed or recommended by ADB in preference to others of a similar nature that are not mentioned.
By making any designation of or reference to a particular territory or geographic area, or by using the term “country” in this document, ADB does not intend to make any judgments as to the legal or other status of any territory or area.
This work is available under the Creative Commons Attribution 3.0 IGO license (CC BY 3.0 IGO) https://creativecommons.org/licenses/by/3.0/igo/. By using the content of this publication, you agree to be bound by the terms of this license. For attribution, translations, adaptations, and permissions, please read the provisions and terms of use at https://www.adb.org/terms-use#openaccess
This CC license does not apply to non-ADB copyright materials in this publication. If the material is attributed to another source, please contact the copyright owner or publisher of that source for permission to reproduce it. ADB cannot be held liable for any claims that arise as a result of your use of the material.
Please contact [email protected] if you have questions or comments with respect to content, or if you wish to obtain copyright permission for your intended use that does not fall within these terms, or for permission to use the ADB logo.
Notes: In this publication, “$” refers to United States dollars. ADB recognizes “China” as the People’s Republic of China and “Hanoi” as Ha Noi. Corrigenda to ADB publications may be found at http://www.adb.org/publications/corrigenda
Printed on recycled paper
CONTENTS
Tables and Figures vii
Acknowledgments viii
Abbreviations ix
Executive Summary xi
1. Introduction 1From Control to Elimination 1Asian Development Bank and Malaria Elimination 3Leadership, Collaboration, Innovation 3The Structure of the Regional Malaria and Other Communicable Disease Threats Trust Fund 4
2. Fund Utilization and Management 6
3. Results by Outcome 8Outcome 1: Leadership 9
Rationale 10Asia Pacific Leaders Malaria Alliance Support 11Investment Cases 11Enabling Factors 12Next Steps and Sustainability Pathway 12
Outcome 2: Financing 13Rationale 14Mobilizing Financing 14Landmark Collaboration 14Enabling Factors 15Next Steps and Sustainability Pathway 15
Outcome 3: Medicines 16Rationale 17Regulatory Systems Strengthening 17Medicines Safety 18Malaria Medicines Field Testing 18Myanmar Regulatory Reform 19Enabling Factors 19Next Steps and Sustainability Pathway 19

Contentsvi
Outcome 4: Information Systems 21Rationale 22Landscape Analysis 23Malaria Surveillance 23Geospatial Technology 23Policy and Strategy 24Investment Guidance 24Viet Nam 25Enabling Factors 25Next Steps and Sustainability Pathway 26
Outcome 5: Laboratory Diagnostics and Surveillance 27Rationale 28Communicable Disease Control 2 - Additional Financing 31Laboratory Quality Assurance and Malaria Surveillance in Myanmar 31Migrant and Mobile Populations 31Enabling Factors 32Next Steps and Sustainability Pathway 32
Outcome 6: Promotion and Prevention 34Rationale 35Malaria Prevention in Infrastructure Development 35Case Study in Urban Development Project 35Case Studies in Special Economic Zones and Border Development 35Curriculum Development and Training 37Regulations and Guidelines 37Enabling Factors 38Next Steps and Sustainability Pathway 38
4. Knowledge Products and Publications 39
5. Gender Dimensions 41
6. Annex 42Annex A. RMTF Results-Based Framework 42Annex B. Glossary of Results-Based Framework Terms 75Annex C. Gender Dimensions 76Annex D: Finance 82Annex E. RMTF Recommendations for Management of Future Trust Funds 83

TABLES AND FIGURES
TABLES
1 Results of Outcome 1.1 102 Results of Outcome 1.2 113 Results of Outcome 2 144 Results of Outcome 3.1 175 Results of Outcome 3.2 186 Results of Outcome 4 227 Results of Outcome 5.1 288 Results of Outcome 5.2 289 Results of Outcome 5.3 2910 Results of Outcome 5.4 3011 Results of Outcome 6.1 3612 Results of Outcome 6.2 37
FIGURES
1 The RMTF Ecosystem 22 Cambodia - Malaria Incidence per 1,000 population 23 Lao PDR - Malaria Incidence per 1,000 population 34 Viet Nam - Malaria Incidence per 1,000 population 35 Projects of the Regional Malaria and Other Communicable Disease Threats Trust Fund 5

ACkNOwLEDGMENTS
Report preparation led by Susann Roth and Jane Parry, supported by Rosebelle May Azcuna, Liza Tabora, Randolph Dacanay, and Editha Santos. Graphic design and layout led by keisuke Taketani.
Financing partners: The Government of Australia (Department of Foreign Affairs and Trade); the Government of Canada (Department of Foreign Affairs, Trade and Development); and the Government of the United kingdom (Department for International Development).

ABBREVIATIONS
ADB Asian Development BankADF Asian Development FundAeHIN Asia eHealth Information NetworkAPLMA Asia Pacific Leaders Malaria AllianceAOP annual operational plan APMEN Asia Pacific Malaria Elimination NetworkCDC communicable disease controlCoRE Centre of Regulatory ExcellenceCSO civil society organizationDFAT Department of Foreign Affairs and Trade, AustraliaDFID Department for International DevelopmentDFTAD The Department of Foreign Affairs, Trade and Development DMC developing member countryDMS Data management systemeCDS electronic communicable disease surveillance eHealth ICT in the health sector, also called “digital health”FDA Department of Food and Drug Administration GAP gender action planGIS geographic information systemGlobal Fund/GFATM The Global Fund to Fight AIDS, Tuberculosis and MalariaGMS Greater Mekong SubregionHIA health impact assessmentHIE health information exchangeHIGAF health ICT governance architecture framework HINARI HINARI Access to Research in Health Programme HIS health information systemHISP Health Information Systems ProgrammeHL7-FHIR HL7 Fast Healthcare Interoperability Resources ICT information and communication technologyIEC information, education and communicationIOM International Organization for MigrationIRIMS integrated regulatory information management systemLLIN long lasting insecticidal netsLOMwRU Lao-Oxford-Mahosot Hospital wellcome Trust Research UnitM&E monitoring and evaluationmDMS Mobile data management systemMETCAP Malaria Elimination Transmission and Costing in the Asia PacificMMP mobile and migrant populationsMOH Ministry of HealthMOHS Ministry of Health and Sports

Regional Malaria and Other Communicable Disease Threats Trust Fundx
MORU Mahidol Oxford Research UnitMOU memorandum of understandingMPEAT Malaria Program Efficiency Analysis Tool NMCP National Malaria Control ProgrammeNGO nongovernment organizationNHL National Health Laboratory NRA National Regulatory AgencyOCO Office of Cofinancing OperationsLao PDR Lao People’s Democratic RepublicPHMP Public Health Management Plan PMU project management unitPNG Papua New GuineaPPMU provincial project management unitPRC People’s Republic of ChinaRBF results-based frameworkR-CDTA regional capacity development technical assistanceRECAP Results for Malaria Elimination and Control of Communicable Disease Threats in
Asia and the PacificRMTF Regional Malaria and Other Communicable Disease Threats Trust FundRRP Asia Pacific Regional Regulatory Partnership for Malaria Elimination RRT Rapid response teamSDG Sustainable Development GoalSEARO Regional Office for South-East Asia SERD Southeast Asia DepartmentSEZ Special Economic Zone SF substandard and falsifiedSOP standard operating procedure TA technical assistanceTGA Therapeutic Goods Administration, AustraliaUCSF/MEI University of California, San Francisco Malaria Elimination InitiativeUHC universal health coverageURC University Research Co.US United StatesVMG volunteer malaria groupwHO world Health OrganizationwPRO Regional Office for the western Pacific

ExECUTIVE SUMMARY
The Regional Malaria and Other Communicable Disease Threats Trust Fund (RMTF) was set up in December 2013. Its remit was to support multicountry, cross-border and multisector responses to urgent malaria and other communicable disease issues, with a focus on the countries of the Greater Mekong Subregion (GMS).
In 2015 the fund moved from supporting the control of malaria to eliminating the disease as a public health threat. This shift was in response to growing resistance to artemisinin-based combination therapy, which was emerging in four GMS countries: Cambodia, Myanmar, Thailand and Viet Nam. The rationale was that achieving elimination in Asia and the Pacific would prevent resistance reaching the African continent.
Over the next 5 years, the project funded projects under six broad domains: leadership, financing, medicines, information systems, laboratory diagnostics and surveillance, and promotion and prevention.
Key achievements
• Galvanized malaria elimination leadership at the highest level and provided decision support for accountability;
• Introduced innovative mechanisms for malaria elimination financing and donor collaboration;• Supported regulatory and disease control bodies to work more effectively, strengthen post-market
surveillance of anti-malarials, and to collaborate with regional counterparts;• Convened partners within countries and across borders to work toward the common goal of eliminating
malaria;• Stimulated the appetite for transformational digital interventions and improved capacity, resulting in
increased surveillance and automated reporting of malaria and communicable diseases;• Strengthened the role of health impact assessment for malaria prevention in infrastructure projects and
special economic zones in border areas.
The Department of Foreign Affairs and Trade (Australia) and Department for International Development (United kingdom) contributions came to a close in June 2018, but in each of the six domains, a sustainability pathway was left in place to ensure that the results continue to resonate, that the governments of each country involved at different levels, together with donor agencies, nongovernment organizations and the private sector, can continue to build on what has been achieved.

HFPF Steering Committee Chair WooChong Um,
Director General, Sustainable Development and Climate Change Department (SDCC)
HFPF Steering Committee MembersMichael Barrow
Director General, Private Sector Operations Department
Hun KimDirector General, South Asia Department
Amy LeungDirector General, East Asia Department
Ramesh SubramaniamDirector General, Southeast Asia Department (SERD)
Werner E. LiepachDirector General, Central and West Asia Department
Ma. Carmela D. LocsinDirector General, Pacific Department
Ayako InagakiHealth Committee Chair, Director, Human and Social Development Division, SERD
Facility ManagerN.J. Ahmad
Deputy Director General, SDCC, concurrently Chief Compliance Officer
Robert GuildChief Sector Officer
Sustainable Development and Climate Change Department (SDCC)
Health Sector SecretariatPatrick Osewe, Chief of Health Sector, Health Sector Group, Sector Advisory Service Cluster (SDSC-HEA)
Eduardo Banzon, Principal Health Specialist, SDSC-HEASusann Roth, Senior Social Development Specialist, SDSC-HEA
Sonalini Khetrapal, Health Specialist, SDSC-HEAKirthi Ramesh, Social Development Specialist, SDSC-HEA
Pura Angela Wee-Co, Associate Health Officer, SDSC-HEAHoney May Manzano-Guerzon, Operations Analyst, SDSC-HEA
Wendy Nazal Montealto, Senior Operations Assistant, SDSC-HEA
Office of Cofinancing Operations (OCO)Kai Preugschat, Head, OCO
Ilaria Caetani, Principal Financing Partnerships Specialist, OCOGuenther Mate, Principal Financing Partnership Specialist, OCO
Marites Torres, Senior Financing Partnerships Officer, OCOKatherine Barrameda, Financing Partnerships Officer, OCO
Trina Mari M. Raymundo-Samia, Financing Partnerships Analyst, OCO
GOvERNANCE STRUCTURE Regional Malaria and Other Communicable Disease Threats Trust Fund
under the Health Financing Partnership Facility (HFPF)

1. INTRODUCTION
From Control to Elimination
when the Regional Malaria and Other Communicable Disease Threats Trust Fund (RMTF) was set up in December 2013, its remit was to support, for a five-year period, the Asian Development Bank’s (ADB) developing member countries (DMCs) to develop multicountry, cross-border, and multisector responses to urgent malaria and other communicable disease issues. In 2015 the fund moved from supporting the control of malaria to eliminating the disease through a process of strengthening health systems that would also have an impact on other communicable disease threats.
Two factors led to this decision: first, growing resistance to artemisinin-based combination therapy—the last line of simple-to-use and effective malaria drugs—had been detected in four countries of the Greater Mekong Subregion (GMS): Cambodia, Myanmar, Thailand, and Viet Nam.
Second, it became clear that with the right health systems’ building blocks in place, eliminating malaria was technically feasible in Asia and the Pacific. Elimination, as defined by the world Health Organization (wHO), is “the interruption of local transmission (i.e., reduction to zero incidence of indigenous cases) of a specified malaria parasite species in a defined geographical area.” Achieving this in Asia and the Pacific could prevent resistance reaching the African continent, where it would have devastating consequences and potentially reverse the gains in global malaria control made over the previous decade.
This shift in focus is aligned with the wHO Framework for Malaria Elimination, which calls on countries to put in place the tools and systems needed to reduce the disease burden of malaria and progress toward elimination as soon as possible.1 These interventions include enhancing and optimizing vector control and case management; increasing the sensitivity and specificity of surveillance; accelerating transmission reduction, and investigating and clearing individual cases. All of these were addressed under the RMTF.
In turn, the fund’s activities tied in with the health-related Sustainable Development Goals (SDGs) and targets, in particular SDG Target 3.3: “by 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases,” and SDG target 3.8: “achieving UHC, including access to quality essential health-care services and safe, effective, quality and affordable essential medicines.”2
The GMS countries overall have made great progress in controlling malaria. Data from the ministries of health in the recent years show that the Lao People’s Democratic Republic (Lao PDR) had an 85% decline in its malaria incidence from 7.2 in 2014 to 1.2 cases per 1,000 population in 2017. The malaria incidence in Viet Nam in 2014 was already low at 0.1 cases per 1,000 population but was further reduced by 40% in 2017. Cambodia had 3.1 malaria cases per 1,000 population in 2014 and was significantly reduced to 1.6 cases per 1,000 in 2016. The country however experienced a surge in the number of malaria cases in 2017, which raised the incidence level back to 3.0 cases per 1,000.
1 wHO. 2017. A framework for malaria elimination. Geneva: wHO.2 Sustainable Development Goal 3. https://sustainabledevelopment.un.org/sdg3
http://www.who.int/malaria/publications/atoz/9789241511988/en/

2 Regional Malaria and Other Communicable Disease Threats Trust Fund
Malaria transmission in the GMS is mostly concentrated in hilly, forested areas, in border areas, and where forest goers and temporary migrants and seasonal workers reside. Such areas were targeted in the RMTF through the CDC2-AF. In the project sites of Cambodia, the malaria incidence of 31.3 cases per 1,000 in 2014, more than halved to 13.1 per 1,000 in 2017. In the Lao PDR project sites, malaria incidence was reduced by 86%, from 31.1 in 2014 to 4.2 cases per 1,000 in 2017. The malaria incidence in the Viet Nam project sites was already low at 1.4 in 2015 but was further reduced to 1.0 cases per 1,000 in 2017.
Source: Ministy of Health, Cambodia, provided August 2018.
Outcome 1
Outcome 6
LOMWRU
Government/
Head of state
UN Agencies
Ministry of Foreign
A�airs Ministryof Health
GMS Health Security Loan
ADF Health Security
ADB Health Bond
Medicine outlet
AeHIN
HIS convergence, unique health ID,
standards and interoperability
Convergence of regulatory practices in ASEANfield malaria medicine
quality testing tools
CAN DFAT
DfID
AUS DFAT
UNICEF WHO
Laboratory quality
assurance and networksImproved service delivery
ADB RMTF
$28.7 millio
n
AeHIN Asia eHealth Information NetworkADB Asian Development BankADF Asian Development Fund APLMA Asia Pacific Leaders Malaria Alliance ASEAN Association of Southeast Asian NationsCD communicable diseases CoRE-NUS Center of Regulatory Excellence, Duke-National University of Singapore Graduate Medical SchoolDFAT Department of Foreign A�airs and TradeDfID Department of International DevelopmentDMC developing member countryFDA food and drug administrationGIS geographic information system
RRP Regional Regulatory PartnershipRMTF Regional Malaria and Other Communicable Disease Threats Trust FundSEZs Special Economic ZonesSSFFCs substandard, spurious, falsely labeled, falsified, and counterfeit commoditiesUCSF University of California, San FranciscoUN United NationsUNICEF United Nations Children’s FundUoO University of OsloUSP United States PharmacopeiaWHO World Health Organization
GIT Georgia Institute of TechnologyGMS Greater Mekong SubregionHIA health impact assessmentHIS health information systemsIOM International Organization for MigrationIRIMIS integrated regulatory information systemLOMWRU Lao-Oxford-Mahosot Hospital-Wellcome Trust Research Unit MMPs migrant and mobile populationsMORU Mahidol Oxford Tropical Medicine Research UnitMSU Mahasarakham UniversityNRA National Regulatory AgencyPRCF fund People’s Republic of China (PRC) Regional Cooperation and Poverty Reduction Fund
IOM
Malaria
elimination
dashboard
APLMA
MMPs
Risk mapping, core registries,
and HIS geo-enabling
WHO
GIT
Mobile
phone
provider
Health
GeoLab
Collaborative
CoRE-NUS
$124 million
$52.5 millionreceived
$100 million
Curtin
Univ.
HIA Network
Asia Pacific
Clinics
Laboratory
RMTF Regional Malaria and Other Communicable Disease Threats Trust Fund
Outcome 3Outcome 4
Outcome 2
Outcome 5HIA in SEZs, energy, water,
urban development, tr
ansport
Reaching
MMPs
mHealth for
surveillance
Co-financing
MoU signed with the
Global Fund
Digital health
Centers of ExcellenceFDA Cambodia, Lao PDR,
and Viet Nam
LEADERSHIP
FINANCING
INFORMATION SYSTEMS
LABORATORY DIAGNOSTICS AND SURVEILLANCE
PREVENTION
Commitment for
domestic finance
for malaria and CDInvestment cases and
toolkits for financing
malaria elimination
Regionalcooperation
Infrastructure
CLINICCLINIC
USP Reporting of substandard
and falsified medicinesTesting portable
devices
for quality of
Malaria medicines
RRP
NRA capacity
assessment and
strengthening
work plans
Increased investment in Malaria and CD FDAMyanmar
Policies, IRIMIS, NRA
FDAPhilippines
Reliance policy
SIL-Asia
UCSF
PRCF funding
UoO
Digital Health
Investment Framework:
guidance and user manual
Private
Sector
ADB safeguard,
guidelines, policy,
capacity development,
demonstration projects
MEDICINES
MORU
Improved
malaria
diagnostic
capacity
Quality
assurance
Regional coordination unit
Malaria and CD data exchange,
joint outbreak investigations
AIH
Figure 1: The RMTF Ecosystem
Figure 2: Cambodia - Malaria Incidence per 1,000 population
3.1 1.8 2.4
31.3
17.3
24.9
3.5 2.1 1.7
22.2
12.2 11.5
1.6 0.9 0.8
7.33.0 4.83.0 1.8 1.4
13.1
4.4
8.9
05
101520253035
All malariacases
P.falciparum
cases
P. vivaxcases
All malariacases
P.falciparum
cases
P. vivaxcases
National
2014 2015 2016 2017
Mal
aria
cas
es p
er 1,
000
Project site
RMTF = Regional Malaria and Other Communicable Disease Threats Trust Fund.Source: Authors.

Introduction 3
Lao PDR = Lao People’s Democratic RepublicSource: Ministry of Health, Lao People’s Democratic Republic, provided August 2018.
Source: Ministry of Health, Viet Nam, provided August 2018.
Asian Development Bank and Malaria Elimination
Health is an integral part of ADB’s work, and under Strategy 2030, the bank’s new strategy agenda, it is recognized as a key building block to achieve a prosperous, inclusive, resilient, and sustainable Asia and the Pacific, while sustaining its efforts to eradicate extreme poverty.3 with its background in supporting regional health security, coupled with its commitment to investing in health, ADB is in a good position to
3 ADB. 2018. Strategy 2030: Achieving a Prosperous, Inclusive, Resilient, and Sustainable Asia and the Pacific. Manila. https://www.adb.org/documents/strategy-2030-prosperous-inclusive-resilient-sustainable-asia-pacific
support malaria elimination by strengthening health systems in the region. ADB’s established reputation and relationships with DMC governments, as well as its partnerships with other development agencies, the private sector, and civil society organizations (CSOs) have amplified the fund’s impact.
Through engagement with ADB, DMCs gain access to ADB’s technical assistance (TA) and grant funding, as well as to loans and innovative ways for countries to finance health systems strengthening. The RMTF was useful in catalyzing impact for malaria, but entrusting funds to ADB for malaria elimination also led to a return on investment beyond this goal. Many governments and donors are looking at integrative health programs, and are reaching for ways to strengthen health systems, both nationally and regionally. ADB had identified an emerging trend in government demand for health financing, to leverage past successes in vertical disease programs and begin to focus on integrated health sector and systems development.
In response to increasing demand for new types of financing to support integrated health goals, including malaria elimination, ADB engaged with the Global Fund to Fight AIDS, Tuberculosis and Malaria and other development partners. Through this consultative process with partners, donors, and governments, it became clear that funding for programs like malaria elimination required a new approach. This new approach built upon the successes of the RMTF to target blended financing for health. Partners such as the Global Fund recognize their investments are much more impactful over the long term when paired with ADB financing. This type of financing will also sustain results, such as strong health systems that prevent the reemergence of malaria.
Leadership, Collaboration, Innovation
The RMTF promoted political leadership on malaria elimination and related investments in health systems, including a higher level of sustainable domestic financing. It also mobilized more funds to tackle malaria and other communicable disease
Figure 3: Lao PDR - Malaria Incidence per 1,000 population
Figure 4: Viet Nam - Malaria Incidence per 1,000 population
05
101520253035
National Project sites
2014 2015 2016 2017
7.23.8 3.6
31.1
15.9 16.3
5.2 2.2 3.1
22.9
9.414.0
2.0 0.8 1.3
8.3
3.0 5.41.2 0.6 0.6
4.21.6 2.7
All malariacases
P.falciparum
cases
P. vivaxcases
All malariacases
P.falciparum
cases
P. vivaxcases
Mal
aria
cas
es p
er 1,
000
National Project sites
2015 2016 2017
Mal
aria
cas
es p
er 1,
000
0.1 0.1 0.1
1.4
0.8 0.7
0.1 0.0 0.0
0.9
0.6
0.3
0.1 0.0 0.0
1.0
0.7
0.3
0.00.20.40.60.81.01.21.41.6
All malariacases
P.falciparum
cases
P. vivaxcases
All malariacases
P.falciparum
cases
P. vivaxcases

4 Regional Malaria and Other Communicable Disease Threats Trust Fund
threats. Its projects contributed to the process of fostering more reliable supplies of quality medicines, improved data for evidence-based decision-making, and strengthened national malaria and other communicable disease threats programs.
Through its projects, RMTF advocated for a collaborative approach to malaria elimination that goes beyond the health sector and national governments to draw in the private sector, nongovernment agencies, and the donor community across multiple domains, with a focus on health systems strengthening, rather than on a single disease.
The fund’s activities tackled malaria at multiple levels, from regional to national and subnational. For example, the fund boosted regional leadership on malaria elimination through its collaboration of the Asia Pacific Leaders Malaria Alliance (APLMA). RMTF projects also built regional learning networks for health impact assessment (HIA) of infrastructure projects, and in medicines regulation created a regional road map for regulatory systems strengthening. This in turn informed the work of a newly created Asia Pacific Regional Regulatory Partnership for Malaria Elimination (RRP). By providing additional financing to ADB’s already well-established regional communicable disease control project, the fund was able to build on preexisting successes, especially related to financing activities and building capacity at the subnational level rather than starting from scratch to develop a regional health project.
At the national level, projects under the RMTF entailed widespread engagement with government ministries for policy dialog, advocacy, and planning, strengthening both capacity building and evidence-informed decision-making. while national level action is key, many malaria elimination initiatives are most effective at the subnational level. The fund’s projects include subnational level malaria and communicable disease reporting, laboratory systems strengthening, access to innovative information and communication tools, post-market medicines surveillance, outreach to underserved and marginalized populations, and local-level training. The fund also supported malaria-specific operational research.
The Structure of the Regional Malaria and Other Communicable Disease Threats Trust Fund
The RMTF funded a range of projects under six distinct outcomes: leadership, financing, medicines, information technology, laboratory diagnostics and surveillance, and promotion and prevention. It took as its starting point the theory of change structure of the Department for International Development (DFID) of the United kingdom, which sought to address gaps in regional cooperation, sustainable financing for regional public goods in health, adequate incentives and institutions for the medicines supply chain, timely and reliable data, and effective program management.
Projects were then developed under each of the outcomes, deliberately tailored to the prevailing malaria and other communicable disease, and health system landscape in each country. This bespoke approach enabled the fund to best meet the needs of each country, rather than using an overly simplistic, one-size-fits-all approach. while development banks and donor agencies bring their own unique expertise to every project they fund, engaging implementing partners and coordinating within a crowded development partner landscape is crucial to the success of a project. ADB took a pragmatic approach to this, partnering with whatever agencies could best support each project, be they international nongovernment organizations (NGOs), CSOs, academic institutions, government agencies, or individual expert consultants. Taken together, these six pillars of the RMTF coalesced to form a health system strengthening approach, and the fund supported countries to reach for attainment of universal health coverage (UHC).
The RMTF financed regional capacity development technical assistance (R-CDTA), standalone projects, and grant components of investment to improve health outcomes and increase health security by reducing the risk of malaria and other communicable disease threats in Asia and the Pacific.

Introduction 5
The RMTF’s financing partners were the Government of Australia (Department of Foreign Affairs and Trade, $15.8 million), the Government of Canada (Department of Foreign Affairs, Trade and Development, $0.5 million), and the Government of the United kingdom (DFID $12.4m).
In total, the RMTF management has approved a total of $18.075 million for five technical assistance projects, and $9.5 million in additional financing for ADB’s Second GMS Regional Communicable Diseases Project (CDC2) (Figure 5).
Figure 5: Projects of the Regional Malaria and Other Communicable Disease Threats Trust Fund
Source: Authors.

2. FUND UTILIZATION AND MANAGEMENT
The donors’ total investment of $28.70 million and interest income of $316,764 were used to mobilize consultants, procure equipment, provide malaria-specific health services, conduct workshops and training, and cover costs directly related to trust fund administration and management. Total support by the RMTF to specific activities of five technical assistance and three grant projects in the GMS countries amounted to $28.33 million (Annex D). The bulk of the unspent balance of the RMTF, $685,703, were savings from the planned activities of CDC2-Additional Financing which were not pursued based on the advice of the governments of Cambodia, the Lao PDR, and Viet Nam. It was agreed with The Department of Foreign Affairs, Trade and Development (DFATD) Canada that its contribution, amounting to $531,916, can remain in the fund beyond 2018
and does not need to be returned. This leaves less than $150,000 from the income earned from investments from the RMTF under the Department for International Development (DFID) of the United kingdom and Department of Foreign Affairs and Trade, Australia (DFAT) contributions.
The ADB has reported quarterly to the donors on the status of RMTF utilization using a financial reporting system that is different from that used by the donors. Because the donors found ADB’s reporting system complicated, a financial dashboard was designed for donors’ easy understanding. The RMTF financial dashboard is an RMTF financial management tool that visually summarizes the quarterly comparative trends of RMTF disbursements from 2014 to 2018, and the results of Outcome 1 to Outcome 6 in the GMS countries.

Fund Utilization and Management 7
TRUS T FUND OUTCOME S
1 S treng thened leaders hip
2 Increas ed financing
3 Quality medicines
4 Improved informations ys tems
5S treng thened laboratorydiag nos tics ands urveillance
6Prevention ofcommunicable dis eas ethreats in infras tructureprojects
TRUS T FUND AMOUNT
Over-all in million US dollars
0 1 0 20 30
Total RMTF
DFAT
DFID
DFATD
Inves tment Income
1 5.76
29.02
1 2.41
0.53
0.32
Allocation per Outcome in million US dollars
0 1 0 20 30
Outcome 1
Outcome 2
Outcome 3
Outcome 4
Outcome 5
Outcome 6
Others / Inves tmentIncome
1 4.37
3.88
3.49
3.39
0.99
2.53
0.37
FINANCIAL S TATUS
Over-all Status as of Aug 201 8
91 %
9%
RMTF
S tatus per Outcome as of Aug 201 8
92%
24%
76%
8%
21
1 00%1 9%
81 %
43
1 00%
93%
7%
5 6
% disbursed from allocated amount
% undisbursed from allocated amount
ACCOUNTING FOR RESULTS The Regional Malaria and Other Communicable Disease Threats Trust Fund

3. RESULTS BY OUTCOME
The following section presents the results and achievements for each of the RMTF six outcomes. These are presented through a financial dashboard, results-based framework indicator table, list of TA projects contributing to the outcome, and
description of key achievements. Details of each RMTF output and activity are elaborated in the results-based framework (RBF) (Annex A) and project work plans.

Results by Outcome 9
1L E A D E R S H I P
1
Strengthened leadership, decis ion-making and accountabi l i ty for malar ia e l iminat ion and address ing communicable d isease threats .
RCDTA 8485: Strengthening Regional
Response to Malaria and Other Communicable
Diseases in Asia and the Pacific
R-CDTA 8763: Results for Malaria
Elimination and Control of Communicable
Diseases Threats in Asia and the Pacific (RECAP)
– Output 1
R-CDTA 8681 :Awareness Raising to
Adopt Action forMalaria Elimination in
Asia Pacific
OUTCOME 1 : S trengthened leadership, decision-making and accountability for malaria elimination and addressing communicable disease threats
KE Y OUTCOME S
Increased commitment and collaboration for malariaelimination and addressing communicable diseasethreats
Improved use of information for decision-making andaccountability to progress toward malaria eliminationand addressing communicable disease threats
OUTCOME RE S ULTS
Countries that have endorsed the malaria elimination roadmap(As of Aug 201 8)
Timor -Leste
Pakis tan
Nepal
Bhutan Bang lades h Afg hanis tan
Viet NamVanuatuUS
ThailandS olomonIs landsS ing apore
Rus s iaPNGPhilippines
New ZealandMyanmar
Malays iaLao PDRJ apanIndones ia
IndiaCambodia
Aus tralia
Countries Malaria-endemic country Donor country
E ndors ement s tatus E ndorsed Has not endorsed
Note: List of countries provided by Asia Pacific Leaders MalariaAlliance secretariat
Other key achievements
• Malaria E limination Dashboard• Investment cases for financing malaria elimination program and the Malaria Program E fficiency Analysis Tool developed
TRUS T FUND ALLOCATION
Totalallocationin million US $
2.53 S hare in RMTF 9%
DIS BURS E ME NT HIS TORY and PROJE CTION
Q2201 4
Q3201 4
Q4201 4
Q1201 5
Q2201 5
Q3201 5
Q4201 5
Q1201 6
Q2201 6
Q3201 6
Q4201 6
Q1201 7
Q2201 7
Q3201 7
Q4201 7
Q1201 8
81 ,021
279,1 73
59,51 4
41 5,1 81
66,998
226,499
59,828
27,991
323,606
253,541
1 58,875
1 31 ,023
30,224
1 1 5,465
93,523
22,641
2,345,1 03
Quarterly disbursements
Cumulative disbursement
Note: Moved UCS F financial data from Outcome 2 to Outcome 1 .UCS F outputs contribute better under Outcome 1 toward improveduse of information for decision-making and accountability.
Brunei Darussalam
People’s Republicof China
Democratic People’s Republic
of Korea
Republic ofKorea

10 Regional Malaria and Other Communicable Disease Threats Trust Fund
Rationale
Globally, malaria infected 216 million people in 91 countries in 2016, leading to 445,000 deaths.4 Progress toward malaria elimination has stalled in many countries, and the world is failing to keep pace with wHO’s 2020 milestones that can bring about a 40% reduction in incidence and death rates by 2030. More than 2.1 billion people in Asia and
4 wHO. 2018. World Malaria Day 2018: Ready to beat malaria. Geneva: wHO. http://www.who.int/malaria/media/world-malaria-day-2018/en/
the Pacific are at risk of malaria, including 152.3 million in the GMS, making the disease a major regional public health concern. According to wHO estimates for Asia and the Pacific, there were 16.2 million malaria cases in 2016, and 30,300 deaths. with such a large-scale threat, eliminating malaria demands political and financial commitment at the highest level, for both national responses, and for regional partnerships and coordination of efforts.
Table 1: Results of Outcome 1.1Outcome 1.1 Increased commitment and collaboration for malaria elimination and addressing communicable disease threats
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 2017 2016 20171. Number of malaria-
endemic countries that endorsed the malaria elimination road map
0 13 14* 21** 1. Malaria elimination road map developed
No Yes Yes Yes
2. Number of donor countries that endorsed the malaria elimination road map
0 7 7*** 7
Progress: Achieved or on track* Cambodia, India, Indonesia, Lao People’s Democratic Republic Malaysia, Myanmar, Papua New Guinea, People’s Republic of China, Philippines, Republic of korea, Solomon Islands, Thailand, Vanuatu, Viet Nam** APLMA’s 2020 target** Australia, Brunei Darussalam, Japan, New Zealand, Russian Federation, Singapore, United StatesSource: Authors.
Asia Pacific Leaders Malaria Alliance Support
Under the leadership component of the RMTF, APLMA—an affiliation of Asian and Pacific heads of government, housed within ADB from its establishment 2014 to 2016—was supported with technical input. APLMA is now a full fledged independent entity that works to accelerate progress against malaria and to eliminate it in the region by 2030. APLMA has also been financed directly by DFAT and the Bill & Melinda Gates Foundation in addition to the collaboration and specific technical support under the RMTF.
with support under the RMTF, APLMA has introduced the Leaders’ Dashboard, a decision and accountability tool that provides visibility to national and regional progress toward malaria elimination
targets, as well as fulfillment of priority actions and identification of areas requiring attention. Support was also provided to strengthen the investment case of malaria elimination.
Investment Cases
The RMTF competitively recruited the University of California San Francisco Malaria Elimination Initiative (UCSF/MEI) to develop a series of investment cases and a toolkit for financing malaria elimination programs. The investment cases aim to generate evidence around optimal ways to increase and expand the amount of sustainable financing in support of malaria elimination. National and regional policymakers can use this evidence to inform malaria program budgeting, strategic planning, and advocacy for domestic resource

Results by Outcome 11
Table 2: Results of Outcome 1.2Outcome 1.2 Improved use of information for decision-making and accountability for malaria elimination and addressing communicable disease threats
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 2017 2016 20171. Malaria Elimination
Dashboard used to inform high-level regional policy dialog on malaria elimination
No No Yes Yes 1. Malaria Elimination Dashboard prototype
No Yes Yes Yes
2. Number of countries with data compiled from the world Health Organization (wHO) for the technical annex of the Malaria Elimination Dashboard
0 22 22 22
3. Number of countries with data compiled for Malaria Elimination Dashboard indicators
0 4 22 22
4. Malaria Elimination Dashboard finalized
No No No Yes
2. Investment cases and toolkit results used to inform high-level regional policy dialog on malaria financing
No No Yes Yes 1. Costing framework and tools developed*
No Yes Yes Yes
2. Number of countries/subregion with costing for malaria elimination* (BAN, IND, PNG, GMS)
0 2 2 4
3. Number of country/subregional investment cases developed* (BAN, IND, PNG, GMS)
0 0 4 4
4. Number of business cases for private sector investment in malaria control and elimination* (BAN/IND/PNG and GMS)
0 0 2 2
5. Malaria program efficiency analysis tool (MPEAT)*
0 0 1 1
6. Recommendations developed on financing options for the Asia and Pacific Region*
No No Yes Yes
Progress: Achieved at least 95% of targetBAN = Bangladesh, GMS = Greater Mekong Subregion, IND = India.* Upon review of the logical flow of outputs and outcomes, these outputs that were previously tracked under Outcome 2 (Financing) are moved here as these better contribute toward improved use of information for decision-making and accountability for malaria elimination and addressing communicable diseaseSource: Authors.

12 Regional Malaria and Other Communicable Disease Threats Trust Fund
mobilization. The investment cases have since been used by both APLMA and ADB in policy dialog with countries and have also informed other parts of the RMTF’s work, including the financing component, to help malaria program managers collect, organize, and track data points related to the technical efficiency of a malaria program.
National investment cases were commissioned for Bangladesh, Indonesia, and Papua New Guinea (PNG); two regional investment cases, one for the Asia and Pacific region and another specifically for the GMS, with estimates on the cost and economic and financial returns of malaria elimination through 2030; and business cases for private sector engagement in malaria elimination and communicable disease control in Bangladesh, Indonesia, PNG, and the GMS.
The RMTF also supported the development of the Malaria Program Efficiency Analysis Tool (MPEAT), to help malaria program managers collect, organize, and track data points related to the technical efficiency of a malaria program. The MPEAT has been used in Bangladesh, Indonesia, and PNG. In Bangladesh and Indonesia MPEAT was used to identify areas that need strengthening, to maximize value, reduce waste, and ultimately save resources. In the Philippines, the costing tool was used to help navigate the country’s transition from Global Fund grant support to domestic financing for malaria elimination.
The tool is designed to be used in conjunction with the Malaria Elimination Transmission and Costing in the Asia Pacific (METCAP), a transmission
model that measures allocative efficiency, created by Mahidol Oxford Tropical Medicine Research Unit (MORU), in collaboration with the USCF and the University of Cape Town. The outputs of the METCAP have been transformed into an online interactive mobile application that generates reader-friendly graphs and charts showing changes in malaria morbidity and mortality and associated program costs under different intervention scenarios.
Enabling Factors
The Leaders’ Dashboard was an effective accountability tool, and the investment cases gave much-needed tangible evidence of the potential beneficial impact of malaria elimination ADB’s involvement brought each country’s ministry of finance to the table, which gave APLMA a level of reach that it could not have otherwise attained.
Next Steps and Sustainability Pathway
APLMA is now accepted as a legitimate policy platform, and DFAT also continues to support it. The Malaria Elimination Dashboard will hold leaders accountable, as well as supporting advocacy and communication to keep the malaria agenda active.
The partnership with APLMA under the RMTF also supported the collaboration with the Global Fund, which led to the signing of a memorandum of understanding (MOU), between ADB and the Global Fund to Fight AIDS, Tuberculosis and Malaria for a proposed regional financing facility (see p. 14).

Results by Outcome 13
2 F I N A N C I N GIncreased f inancing for malar ia e l iminat ion
and address ing communicable d isease threats
2
R-CDTA 8763: Results for Malaria
Elimination and Control of Communicable Diseases Threats in Asia and the
Pacific (RECAP) – Output 2
OUTCOME 2: Increased funds for malaria elimination and addressing communicable disease threats
KE Y OUTCOME S
Increased investments for malaria elimination andaddressing communicable disease threats
Increased domestic funds for malaria elimination
OUTCOME RE S ULTS
Amount of ADB g rants madeavailable for malaria eliminationand addres s ing communicable
dis eas e threats
Amount of country loans formalaria elimination and
addres s ing communicabledis eas e threats
201 4Baseline
May 201 7S tatus
201 7 Target 201 4Baseline
May 201 7S tatus
201 7 Target
22m$
83m$ 80m$
1 44m$
1 20m$
27m$
Other key achievements
• New innovative mechanisms that mobilized financing such as ADB's first Health Bond of $1 00M and ADB-Global Fund MOU
TRUS T FUND ALLOCATION
Totalallocationin million US $
0.37 S hare in RMTF 1 %
DIS BURS E ME NT HIS TORY and PROJE CTION
Q2 201 5 Q4 201 5 Q4 201 6 Q1 201 7 Q2 201 7 Q3 201 7 Q4 201 7 Q1 201 8 Q2 201 8
25,044
1 6,71 71 4,828
1 1 6,699
1 7,841
26,326
43,838
51 9
1 5,321
277,1 33
Quarterly disbursements
Cumulative disbursements
Note: Moved UCS F financial data from Outcome 2 to Outcome 1 .UCS F outputs contribute better under Outcome 1 toward improveduse of information for decision-making and accountability.

14 Regional Malaria and Other Communicable Disease Threats Trust Fund
Rationale
Malaria elimination costs money, but the human and financial cost of underfunding is far higher. Securing funding entails both innovative approaches to sustainable health-care financing and ensuring that existing investments work smarter and are sustainable to achieve the most impact.
Mobilizing Financing
In 2015 the fund allocated $9.5 million to an existing project in Cambodia, the Lao PDR, and Viet Nam. However, it was the use of RMTF funding as a catalyst that enabled the fund to both focus on malaria, and to greatly amplify its impact, by raising additional ADB resources through the development of new financing mechanisms to support efforts for malaria elimination and addressing communicable disease threats.
A total of $52.5 million in grants was mobilized for health security measures from the Asian Development Fund (ADF), as well as an additional $125 million worth of loans and grants for health security in GMS countries and, most notably, the issuance of ADB’s first health bond. The private placement of $100 million issued in March 2017 was purchased by the Dai-ichi Life Insurance Company, Limited, making it the world’s first institutional investor to buy a bond that supports ADB’s health
program. The bond will support lending to countries on targeted health financing, including malaria and communicable disease programs, and ADB will continue to support the bond pipeline process for potential subsequent issues.
Landmark Collaboration
In late 2017, against a backdrop of Asia and the Pacific countries previously eligible for Global Fund grants transitioning to domestic responsibility for malaria and other communicable disease investments, the Global Fund and ADB signed a landmark MOU to find common ground and align malaria and other communicable disease funding opportunities. The MOU, signed in November 2017, was the first of its kind between the Global Fund and a development bank. The Global Fund/ADB MOU promotes ongoing coordination and future cofinancing between the two institutions, directly through projects and also through a new regional fund. There is already a project pipeline targeting health systems development and strengthening. Cofinancing opportunities for Bhutan, PNG, and Sri Lanka, as well as the GMS countries have already been mapped as a result of the MOU. The model is also proof of concept for ADB to collaborate with other donors on other health projects in future, beyond malaria, based on country needs and donor priorities.
Table 3: Results of Outcome 2Outcome Indicator 2014
BaselineStatus in Target Progress Output Indicator 2014
BaselineStatus in Target Progress2016 Q2 2018 2016 Q2 2018
1. Amount of ADB grants made available for malaria elimination and addressing communicable disease threats
$22.0m $82.5m* $82.5m* $80.0m 1. ADF health security grants for group A and B countries mobilized ($52.5m)
No Yes Yes Yes
2. Amount of country loans for malaria elimination and addressing communicable disease threats
$27.0m $144.0m* $144.0m* $120.0m 2. GMS health security funds approved ($117m as loan and $8m as grant)
No Yes Yes Yes
3. ADB Health Bond launched ($100m OCR)
No No Yes Yes
Progress: Achieved at least 95% of target * Cumulative amountADB = Asian Development Bank, ADF = Asian Development Fund, GMS = Greater Mekong Subregion, m = million, OCR = ordinary capital resources.Source: Authors.

Results by Outcome 15
Enabling Factors
Having a clear understanding of national government priorities and constraints, and establishing how public–private partnerships could appeal to both private and public sectors, paid off in terms of obtaining buy-in from both within ADB and with external partners. The success of the financing component is also a testament to the way in which the six outcomes worked together: the strong backdrop of projects that the RMTF had already developed, including the work done on what investments are needed to eliminate malaria, and the pipeline of upcoming projects gave much-needed traction to leverage the broader health sector.
Next Steps and Sustainability Pathway
A legal agreement between ADB and the Global Fund has been drafted for the design of the new Regional Health Fund. This fund will potentially finance priority strategic regional activities, provide support to countries in the region with
the highest malaria burden and least capacity to secure domestic funding, and scale up investments in national programs. It will meet demand for structured blended finance, allowing for integrated health sector development through concessional loans and innovative finance structures, including results-based grants, risk transfer mechanisms, and loan buy-downs. The vision is to provide a one-stop blended finance shop for governments to access finance that targets whole-system health programs. As a result, specific regional goals such as malaria elimination will also be expedited—with sustainable and long-term results—and health systems strengthened.
In addition, the health bond process was set up in a way that can be replicated, either for other health issuances or for related themes.
ADB has committed to health sector investment by increasing the health pipeline, providing substantial technical assistance, and integrating health in ADB country partnership strategies. The ADB Strategy 2030 also provides ample opportunity to leverage ADB’s strong infrastructure footprint for the health sector.
16 Regional Malaria and Other Communicable Disease Threats Trust Fund
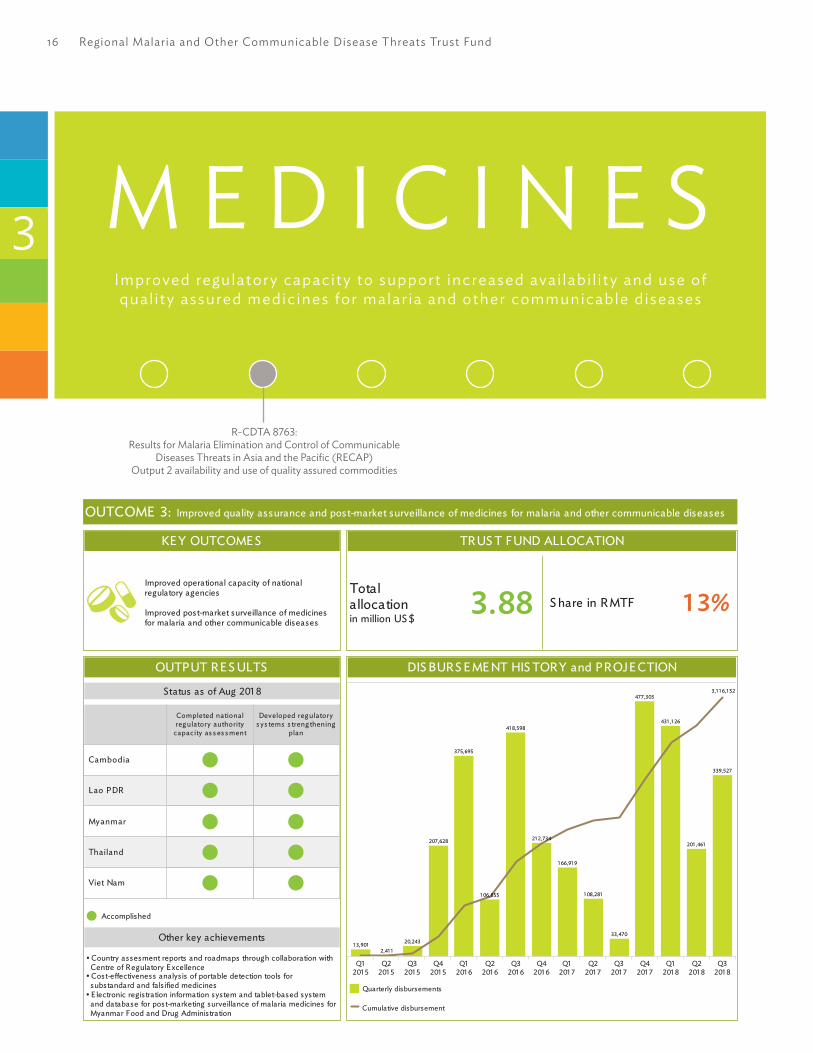
M E D I C I N E SImproved regulatory capacity to support increased avai labi l i ty and use of qual i ty assured medic ines for malar ia and other communicable d iseases
R-CDTA 8763: Results for Malaria Elimination and Control of Communicable
Diseases Threats in Asia and the Pacific (RECAP) Output 2 availability and use of quality assured commodities
3
OUTCOME 3: Improved quality assurance and post-market surveillance of medicines for malaria and other communicable diseases
KE Y OUTCOME S
Improved operational capacity of nationalregulatory agencies
Improved post-market surveillance of medicinesfor malaria and other communicable diseases
OUTPUT RE S ULTS
Status as of Aug 201 8
Completed nationalreg ulatory authority
capacity as s es s ment
Developed reg ulatorys ys tems s treng thening
plan
Cambodia
Lao PDR
Myanmar
Thailand
Viet Nam
Accomplished
Other key achievements
• Country assesment reports and roadmaps through collaboration with Centre of Regulatory E xcellence• Cost-effectiveness analysis of portable detection tools for substandard and falsified medicines• E lectronic registration information system and tablet-based system and database for post-marketing surveillance of malaria medicines for Myanmar Food and Drug Administration
TRUS T FUND ALLOCATION
Totalallocationin million US $
3.88 S hare in RMTF 1 3%
DIS BURS E ME NT HIS TORY and PROJE CTION
Q1201 5
Q2201 5
Q3201 5
Q4201 5
Q1201 6
Q2201 6
Q3201 6
Q4201 6
Q1201 7
Q2201 7
Q3201 7
Q4201 7
Q1201 8
Q2201 8
Q3201 8
339,527
201 ,461
431 ,1 26
477,303
33,470
1 08,281
1 66,91 9
21 2,734
41 8,598
1 06,855
375,695
207,628
20,243
2,41 11 3,901
3,1 1 6,1 52
Quarterly disbursements
Cumulative disbursement

Results by Outcome 17
Rationale
Eliminating malaria requires reliable supplies of safe and efficacious treatments delivered to where they are needed, but the market is plagued by substandard and falsified (SF) medicines. This undermines the work of the Global Fund to Fight AIDS, Tuberculosis and Malaria, and other development agencies bringing malaria medicines to where they are needed. Better regulation and post-marketing surveillance of malaria medicines is key to addressing this issue. This in turn requires strong national regulatory agencies (NRAs) with effective tools for testing and post-market surveillance of malaria medicines, as well as collaboration with the global community of practice tackling the international trade in SF medical products.
Regulatory Systems Strengthening
Many NRAs in Asia and the Pacific struggle to cope with marketing approvals of new health products, inspections of manufacturing and distribution facilities, and ensuring the continued quality of medicines and medical devices throughout the supply chain.5 The RMTF supported regulatory systems strengthening through collaboration with the Centre of Regulatory Excellence (CoRE), a regional capacity-building center and partner-coordinating platform for regulatory systems strengthening and convergence for Southeast Asian DMCs.
CoRE developed individual country assessment reports and road maps, which were further analyzed to develop a regional capacity development road
5 ADB. 2014. Better Regulation of Medicines Means Stronger Regional Health Security. ADB Briefs No. 54. April. Manila.
Table 4: Results of Outcome 3.1Outcome 3.1 Improved operational capacity of national regulatory agencies (NRAs)
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 Q2 2018 2016 Q2 20181. Number of countries
with improved operational regulatory capacity
0 0 3* 3 1. Number of countries with NRA capacity profiles (CAM, LAO, MYA, THA, VIE)
0 3 5 5
2. Number of countries with NRA capacity strengthening road maps (CAM, LAO, MYA, THA, VIE)
0 0 5 5
3. Training modules developed
No No Yes Yes
4. Number of countries with NRA staff trained on priority regulatory issues and gaps
0 0 5 5
Progress: Achieved at least 95% of targetCAM = Cambodia, LAO = Lao People’s Democratic Republic, MYA = Myanmar, THA = Thailand, VIE = Viet Nam.* Cambodia, the Lao PDR, and Myanmar built capacity based on the Centre of Regulatory Excellence (CoRE) needs assessment, which helped identify areas of focus and improve partner coordination. The trainings conducted for country representatives and the road map developed all encapsulate capacity building. Additionally, the targeted technical support and work in Myanmar had a direct impact on the operational capacity of its Food and Drug Administration and ad-ditional activities addressing targeted monitoring of the quality of medicines on the market, linking the quality control laboratory into the electronic information system and developing the basis of a national drug safety strategy and pharmacovigilance system.Source: Authors.

18 Regional Malaria and Other Communicable Disease Threats Trust Fund
Table 5: Results of Outcome 3.2Outcome 3.2 Improved post-market surveillance of medicines for malaria and other communicable diseases
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 Q2 2018 2016 Q2 20181. Number of countries
piloting new field detection tools
0 0 1 1 SF field detection tools
1. Formal relationships with global and local research institutions established
No Yes Yes Yes
2. Library of active ingredients and finished product profiles developed
No No Yes Yes
3. Report on results of testing and cost-effectiveness evaluation of field detection tools
No No Yes Yes
4. Recommendations on cost-effective post-market surveillance field tools for detecting SF developed
No No Yes Yes
2. Number of wPRO and SEARO countries started to report to the global substandard and falsified (SF) medical products reporting mechanism*
0 6 10 5 SF reporting
1. Number of countries with staff trained on the wHO global SF reporting mechanism
0 22 22 22
Progress: Achieved at least 95% of target SEARO = Regional Office for South-East Asia, wPRO = Regional Office for the western Pacific, wHO = world Health Organization.* wHO does not divulge information on reporting by individual countries due to confidentiality rules. Source: Authors.
map, focusing on needs that are common among the five GMS countries. Further improvements in the operational capacity of NRAs in the GMS, while meeting their diverse needs, will require a coordinated effort by development partners, and with this in mind, the regional road map was shared with the RRP and the information was subsequently incorporated into the RRP workplan.
Medicines Safety
By sensitizing NRAs to the ways in which SF medical products contribute to artemisinin resistance and the danger this poses to malaria elimination efforts, the RMTF medicines component has supported countries to participate in the wHO monitoring mechanism for SF products. The training provided jointly with wHO led to improved reporting of SF
products into the wHO Global SF medical product reporting mechanism. In addition, six countries in the wHO western Pacific Region and South-East Region have since started to report SF products for the first time.
Malaria Medicines Field Testing
The RMTF also funded the Lao-Oxford-Mahosot Hospital-wellcome Trust Research Unit (LOMwRU) to test portable devices for detecting anti-malaria medicine quality in both controlled and field conditions. This research led to advice and strategic recommendations both for DMCs looking to invest in such devices, and to device developers to make them more fit for purpose. The devices were piloted with the Lao PDR NRA, which provided invaluable insight into their usability in the

Results by Outcome 19
field by resource-constrained NRA when testing antimalarial medications.
Myanmar Regulatory Reform
Myanmar’s regulatory agency, Food and Drug Administration (FDA), Myanmar, relied on a paper-based medicines registration, and the agency’s systems did not enable it to conduct effective post-marketing surveillance of malaria medicines, or efficiently bring new medicines to market. In late 2017, ADB worked with the regulatory agency, FDA, Myanmar, to move its paper-based registration system online to an integrated regulatory information management system (IRIMS), a digital platform that processes, stores, retrieves and shares information on regulatory activities. This is vital to ensuring the country can improve its supplies of safe, reliable, high-quality antimalarial medicines, a key facet of malaria elimination efforts.
By mid-2018, an online-only product registration application process was in place, including training of the private sector applicants, manufacturers, and agents. As part of establishing an IRIMS, the FDAs’ online databases were linked to those for the management of facility inspections and of quality control (QC) laboratories.
National QC lab and inspectors can now use a tablet-based system to connect to the central registration database to know which products are registered, and to directly upload images and videos of the facility they inspect, along with the inspection report and follow-up action. The FDA also reviewed its existing list of approved products, to compare them with those used by reference authorities. After this review, the online medicines registration system was set up to automatically trigger an alert on any products submitted for registration that contain banned or obsolete active ingredients. Product information documents, which describe a medicine’s indications, contraindications, dosages, and warnings, will also rely on reference texts obtained from the Therapeutic Goods Administration, Australia (TGA).
Enabling Factors
Recognizing NRAs as partners and key stakeholders in public health, and working with them together with technical agencies, especially wHO, was key to the success of this component. Coordinating efforts with other development partners ensured messaging to NRAs and training were aligned. CoRE was well placed to gain the trust and attention of NRAs, and to ensure that this newly established entity’s work was aligned with the needs of NRAs. Similarly, LOMwRU has key expert researchers in the field and is based in one of the GMS countries with close links to the regulatory agency there, which was helpful.
In Myanmar, one of the key enablers was the fact that there was little in place already, making it relatively easy to introduce a new system. There was also an alignment of interests in the new online product registration system, as registrants also find the online system and standardized terminology it easier and cheaper to use. Inspectors in the field are now able to check which antimalarial are registered, and what the packaging should look like, which makes it easier for them to identify SF products.
Next Steps and Sustainability Pathway
Implementation of recommendations for using portable testing devices still requires GMS countries to develop better policies on post-market surveillance and build the capacity of field inspectors who can act when suspected falsified and substandard medicines are identified. More understanding of the root causes of substandard medicines is needed to ascertain whether it is due to, for example, low-quality medicines entering the market, or subsequent incorrect storage along the supply chain.
while the portable devices that were assessed showed high sensitivity to falsified medicines, these devices were not optimal for detecting substandard medicines, yet in the Lao PDR, substandard malaria drugs are more prevalent than falsified ones in

20 Regional Malaria and Other Communicable Disease Threats Trust Fund
registered drug outlets. Currently, there are no agreements on who will be responsible for building a reference library, and whether it is possible to have one at regional level.
Although there are regional bodies for capacity development, and plans are ongoing for development partner alignment and harmonization, more support is required for the Association of Southeast Asian Nations pharmaceutical working group and for building subregional (GMS) consensus on reliance policy and sharing of information on SF medicines.
In SF reporting, each country now has a designated, trained contact person on reporting SF medical products. Reporting from the region to wHO has increased as a direct result, and is expected to continue. Myanmar has had additional training of inspectors and developed a national task force and
action plan for addressing SF antimalarial medicines and other medical products. Also in Myanmar, DFAT is planning to continue funding the IRIMS work.
The capacity development plans that were developed for each NRA have been incorporated into the work of the RRP, which is helping to coordinate the actions of funding agencies and technical partners working to strengthen regulatory systems. At the national level, seven countries now have specific malaria elimination plans in place. wHO and TGA, the regulatory body for therapeutic goods in Australia, continue to be involved in supporting these efforts, and $20 million has been secured from DFAT to continue this work. The NRAs themselves have also taken up the task of regulatory system strengthening, and some have their own funding to commit to this task.

Results by Outcome 21
INFORMATION SYSTEMSIncreased use of qual i ty data , informat ion tools and technologies
to improve malar ia and other communicable d isease information systems
R-CDTA 8763: Results for Malaria Elimination and Control of Communicable Diseases
Threats in Asia and the Pacific (RECAP) Output 3
4
R-CDTA 8656: Malaria and Dengue Risk Mapping and
Response Planning in GMS in Cambodia, Myanmar and Thailand
OUTCOME 4: Increased use of quality data, information tools and technologies
KE Y OUTCOME S
Increased use of quality data, information toolsand technologies to improve malaria and othercommunicable disease information systems
eHE ALTH S OLUTIONS TE S TE D INGMS COUNTRIE S
Cambodia Myanmar Viet Nam
Unique Health IDs
GIS platform
Commong eo-reg is try
Dis eas es urveillances ys tem (eCDS v2)
HL7 and Fas tHealthcareInteroperabilityRes ources (FHIR)
TRUS T FUND ALLOCATION
Totalallocationin million US $
3.49** Increased from 2.93
S hare in RMTF 1 2%
DIS BURS E ME NT HIS TORY and PROJE CTION
Q2201 4
Q3201 4
Q4201 4
Q2201 5
Q3201 5
Q4201 5
Q1201 6
Q2201 6
Q3201 6
Q4201 6
Q1201 7
Q2201 7
Q3201 7
Q4201 7
Q1201 8
Q2201 8
Q3201 8
701 ,225
408,959
296,793
592,272
98,1 43
422,649
21 3,381
272,033
35,27755,931
93,004
1 49,854
85,738
32,7464,307
24,909835
3,488,056
Quarterly disbursements
Cumulative disbursement

22 Regional Malaria and Other Communicable Disease Threats Trust Fund
Rationale
A strong information and communication technology (ICT) backbone is crucial for countries to transition from malaria control surveillance to elimination. Strengthening health information systems through better use of ICT can help countries to unlock the data they already collect, and use it more effectively for eliminating malaria and controlling communicable diseases. In countries with numerous
disparate disease and patient-level systems and a complex ecosystem, tackling health information exchange, interoperability, and standardization directly improves the access to communicable disease data, both at the aggregate and patient levels. Interoperability efforts aimed at reducing the burden of health workers and providing seamless integration and transparency of information are needed to ensure use of the system.
Table 6: Results of Outcome 4Outcome Indicator 2014
BaselineStatus in Target Progress Output Indicator 2014
BaselineStatus in Target Progress2016 Q1 2018 2016 Q1 2018
1. Number of ICT solutions in use in malaria and other communicable disease information systems to improve and harmonize information management in GMS countries
0 0 3** 2 1. Surveillance mechanisms for malaria and communicable diseases mapped for GMS countries
No Yes Yes Yes
2. Recommendations on two ICT solutions to be used in the region
No Yes Yes Yes
3. Number of ICT solutions tested in GMS countries
0 0 5* 2
2. Number of countries utilizing harmonized geo-enabled malaria and dengue information systems
0 0 3 3 1. Number of countries with prevalence and incidence data for malaria and dengue analyzed
0 1 3 3
2. Number of countries with developed capacity of government public health experts for application of GIS-based visualization
0 1 3 3
3. Number of countries with GIS-based visualization system of malaria and dengue incidence and risk established and methodology evaluated
0 0 3 3
4. Number of countries with policy recommendations for targeting mobile populations in malaria and dengue surveillance and control programs communicated to Ministries of Health***
0 0 0 3
Progress: Achieved at least 95% of target Continued until Q4 2018 through additional funding for the workGMS = Greater Mekong Subregion, GIS = geographic information system, ICT = information and communication technology.* Unique Health ID in Cambodia; GIS platform in Cambodia, Myanmar, and Viet Nam; common geo-registry in Cambodia and Myanmar; Disease surveillance system (eCDS v2) in Viet Nam; HL7 and Fast Healthcare Interoperability Resources (FHIR) in Viet Nam.**GIS platform, common geo-registry and eCDS v2.***Policy recommendations are being developed currently and will be finalized as population movement results are shared and discussed with ministry of health (MOH) staff. Additional funding support has been secured by MORU to complete this work.Source: Authors.
Results by Outcome 23
6 Digital Health Infrastructure: The Backbone of Surveillance for Malaria Elimination - https://www.adb.org/sites/default/files/publication/210856/digital.
7 Funded under Outcome 5.8 ADB. 2016. The Geography of Universal Health Coverage. ADB Briefs No. 55. April. Manila.
Landscape Analysis
An RMTF-funded analysis of the landscape of health management information systems and malaria information systems in GMS countries found that most tools are used to manage malaria programs separately, without a common backbone or standards. A key finding was that support was needed so that a standards-based information system to benefit malaria and other communicable disease information system management could be built. To eliminate malaria, foundational components of surveillance are unique patient identification, the ability to track cases over the treatment course, and access to continuous timely surveillance data for both subnational and national stakeholders.
The analysis recommended several interventions, which informed subsequent projects under this outcome: implementation of good data management practices and digital health governance structure, agreement on digital health information standards and technical interoperability solutions, geo-enabling of the health information system, and implementation of unique health identifiers to link vertical disease information systems.6 The analysis showed that the gaps were not only technological, but also include the governance and enterprise architecture needed for the tools of ICT to be useful. Human resources for health information systems (HIS) were another key area for development under the project.
Malaria Surveillance
A low-cost software solution for hospital-based reporting of dengue cases in Myanmar was developed by MORU for piloting by the Myanmar Ministry of Health and Sports. MORU also trained local healthcare workers in high malaria risk areas in Cambodia and northeast Thailand to collect GPS data for village-level malaria risk mapping, a key step to local targeting of elimination activities. This uses a low-cost, high precision method developed by
MORU and the Asia eHealth Information Network (AeHIN) geographic information systems (GIS) Lab/Health GeoLab Collaborative with support from ADB. MORU mapped malaria and dengue surveillance data in Cambodia, Myanmar, and Thailand.
The project used data analytics based on call records, climate data, and travel surveys, to better understand the patterns of malaria infection and other communicable diseases (such as dengue) with regard to internal and cross-border migration. A consortium of research groups together with MORU analyzed mobile phone call records in Thailand to model the impact of population movement patterns on malaria and dengue distribution, and also analyzed travel survey data from patients with malaria in Cambodia, the Lao PDR, Myanmar, Thailand, and Viet Nam.
In Myanmar, data management systems for malaria surveillance were strengthened, including the use of mobile data management system (mDMS) for case reporting, and analytical tools for decision-making (see Outcome 5, pp.27).7 The project worked with grassroots volunteer malaria workers to improve routine, real-time case reporting through a mobile data management system piloted in the three townships. The mDMS, a smartphone-based app, was developed by Save the Children with the National Malaria Control Programme (NMCP), but RMTF funding enabled widespread piloting of the app for volunteer malaria workers and the initial results helped improve the app to make it more efficient and more user-friendly.
Geospatial Technology
The geographic dimension of malaria is key to enhancing disease surveillance and elimination through improved situational intelligence.8 In turn, ICT is key to geo-enabling a country HIS through geospatial technologies including GIS and the availability of a common registry of the geographic

24 Regional Malaria and Other Communicable Disease Threats Trust Fund
objects core to public health (e.g., health facilities, administrative and reporting divisions, villages). RMTF funding supplied computer hardware and GIS software to Cambodia, Myanmar, Thailand, and Viet Nam, and also ran spatial data management and GIS training for national disease control program staff from the same countries, with the addition of Bangladesh and the Lao PDR.9 This initiative has now grown into the Health GeoLab Collaborative to bring more partners into the effort to geo-enable health systems in Asia and the Pacific and develop common geo-registries. RMTF funding also supported Cambodia, Myanmar, and Thailand to map and analyze national surveillance data for malaria and dengue.10
In Viet Nam, geospatial technology was applied to map the availability of malaria services in public health facilities and the readiness of these facilities to provide these services. This was done in nine districts with high malaria transmission rates. Results highlighted resource gaps in facilities to provide preventive, diagnostics, and treatment services. The same technology and assessment methodology have also been further applied by the malaria program.
Policy and Strategy
As governance was identified as a key gap in the malaria information systems landscape analysis, ADB developed a health ICT governance architecture framework (HIGAF), required for successful implementation and sustainability of digital health solutions. After consultation and close collaboration with health sector ICT experts in the region, the framework was further refined, leading to the creation of HIGAF 2.0, designed specifically to meet the evolving needs of DMCs in the region.11
key to continuity of care is the ability to track malaria-infected subjects wherever they connect with service delivery through a unique health identifier, and the RMTF supported the development of a tool for unique patient ID assessment, which was then applied in Cambodia, the Lao PDR, Myanmar, and Viet Nam.12 At the same time, policy recommendations from a brief on unique patient health IDs informed Cambodia’s strategy on national patient ID management, and the respective implementation plan. Mapping the country’s existing setup brought together different stakeholders at country level to decide on the country’s digital health vision and mission and develop potential next steps.
Investment Guidance
A working paper, Guidance for Investing in Digital Health, was published in May 2018, together with an accompanying website.13,14 The outcome of this work will inform decisions on developing digital health investments. This includes the strengthening of health systems as a whole, as well as the solutions required to address specific health challenges, such as malaria. The guidance demonstrates that investing simply in digitalizing the malaria surveillance and care system is not a value-for-money investment, and that there must first be a digital health foundation in place. Moreover, only a phased and well-planned investment in digital health can add significant value to malaria surveillance and at the same time remain sustainable. This is especially important to consider for development partners who tend to support the digitalization of vertical disease programs. The practicalities of delivering these outcomes while providing socioeconomic benefits have been addressed by developing an accompanying Digital
9 ADB. 2018. Building Capacity for Geo-Enabling Health Information Systems: Supporting Equitable Health Services and well-Being for All. ADB Briefs No. 88. February. Manila.
10 https://healthgeolab.net/.11 Transforming Health Systems Through Good Digital Health Governance. https://www.adb.org/sites/default/files/publication/401976/sdwp-
051-transforming-health-systems.pdf.12 ADB. 2018. Unique Health Identifier Assessment Tool Kit. Manila.13 ADB. 2018. Guidance for Investing in Digital Health. Manila. https://www.adb.org/sites/default/files/publication/424311/sdwp-052-guidance-
investing-digital-health.pdf.14 Digital Health: Strategy and investment. https://sites.google.com/view/digitalhealthasia/home.

Results by Outcome 25
Health Impact Framework (DHIF).15 The DHIF helps DMCs to understand how to invest in digital health for vertical disease programs while taking a health sector enterprise approach. Developed from over 60 digital health case studies from many countries, the framework helps decision makers make better informed decisions about planned socioeconomic and financial impacts. It can be applied to several projects simultaneously so decision makers can find an optimal fit of projects.
Viet Nam
Viet Nam was a focus country under the RMTF information systems component, and the projects there illustrate the importance of digital health improvements to support malaria elimination and communicable disease control. There were a number of interrelated RMTF-funded initiatives in digital health to improve the country’s generation and use of health data for malaria elimination. These initiatives helped the government establish a health ICT policy and develop an action plan to standardize national systems. The RMTF was also used to fund engagement for buy-in and training of health workers in the new policy and enhanced disease surveillance systems that are cased-based and include malaria and other communicable diseases.
with support under the RMTF, Viet Nam has adopted a digital health governance framework and decided to use the health-care standard HL7 FHIR as a practical solution to health data exchange and information systems interoperability. HL7 FHIR is a draft standard describing data formats and elements and an application programming interface for exchanging electronic health records especially in complex information systems so that patient data can be shared at all levels. Such data sharing is essential for countries to test, track, and treat and all malaria cases.
Before the involvement of the RMTF, in 2014 Viet Nam’s Ministry of Health (MOH), the US Center for Disease Control and Prevention, and
private sector international partners had already begun collaborating to build a data warehouse using the electronic health disease surveillance system (eCDS). The government recognized that an enhanced eCDS system could reduce the time needed to generate disease surveillance reports, improve access to data on vaccine coverage rates, enhance early outbreak detection on a case-level basis, and allow for real-time malaria surveillance.
One important goal was to implement digital health solutions to ensure timely reporting for all notifiable diseases, including malaria, as mandated by Viet Nam’s health policy. To bring all this work together, in February 2017, the MOH and the ADB met to identify a strategy and develop a workplan of activities and action for collaboration between the country’s health agencies. Further strengthening of disease surveillance at local health facility levels, including for malaria, was identified as a priority with system interoperability and provincial training as a next step.
Enabling Factors
For most of the ICT projects under the RMTF, once local champions were identified, either within government or in partner organizations with a strong local presence, projects gained traction. Countries also benefited from guidance in establishing or enhancing their vision for digital health in disease surveillance, and policy design, rather than implementation of small-scale technical pilots, which can lead to even more fragmentation, as seen in malaria programs. Making the most of ADB’s convening power, the RMTF projects brought together partners in ways they had not collaborated before, including separate ministries and departments within the same country, as well as uniting development partners to work more collaboratively toward a common goal. Another key enabler was deployment of both short-term international consultant experts and day-to-day engagement with local consultants.
15 Standards and Interoperability Lab for Asia. http://www.sil-asia.org/lab-assets/

26 Regional Malaria and Other Communicable Disease Threats Trust Fund
The Viet Nam project succeeded because ADB brought key government decision makers together to get the foundations in place—standards, governance, and enterprise architecture—before launching in with new information systems. ADB was able to rally stakeholders and capitalize on the country leadership’s commitment to malaria and communicable disease surveillance as a health priority. The introduction of geo-enabling tools for surveillance, health information standardization, interoperability for vertical disease programs, community level information systems such as the Digital Health Frame were wholeheartedly embraced by the MOH. The decision to work with countries on their health-related ICT needs for malaria elimination existed at the start of the RMTF, but the project took off in Viet Nam in the latter part due to its right timing and commitment by all key stakeholders.
Next Steps and Sustainability Pathway
ADB helped establish both the Health GeoLab Collaborative, a collective of both institutions and individuals involved in geospatial technologies for health. Funding from the Bill & Melinda Gates Foundation is supporting continued geo-enabling work in Viet Nam, MORU’s risk mapping work in five GMS countries, and digital solutions to develop tools to support malaria elimination in Cambodia, the Lao PDR, and Viet Nam. Analysis of call data records to determine the impact of human mobility on malaria and dengue is ongoing.
ADB loans are in the pipeline for Viet Nam with an ICT component funded with an ADF grant to support the rollout of electronic health records with automated reporting of communicable diseases and malaria cases into vertical disease reporting systems. The Clinton Health Access Initiative and the National Institute of Malariology, Parasitology and Entomology, and Viettel Telecom and the Health Information Systems Programme Viet Nam continue to collaborate on developing the country’s malaria management system aligned to new standard operating procedures and reporting forms for malaria case and foci reporting and investigation. Viet Nam is making its own investments in patient portals and cloud-based health information systems to support national information systems.
To further ensure the timely subnational patient-level disease information, ADB supported the local health report automation by providing technical resources specific to District Health Information System (DHIS 2) that provides standardized health reporting from the 12,000 local health communes. This countrywide grassroots system will be connected with the district hospitals and national data center and is crucial in the timely access to patient-level communicable disease reporting and generation of the national health statistics. To help ensure standardization and disease reporting interoperability, ADB supported provincial-level MOH training of trainers and the drafting of standard operating procedures for reporting, which will also contribute to the sustainability of this project’s achievements.

Results by Outcome 27
LABORATORY DIAGNOSTICS AND
SURVEILLANCEImproved capacity of laboratory d iagnost ics and survei l lance systems
for malar ia and other communicable d iseases , inc luding cross-border coordinat ion5
G0448/G0449/G0450: CAM/LAO/VIE: Additional
financing for Second Greater Mekong Subregion
Communicable Diseases Control Project (CDC2)
RCDTA 8959: Malaria and
Communicable Diseases Control in the
GMS
OUTCOME 5: Improved capacity of laboratory diagnostics and surveillance system for malaria, including cross border coordination
KE Y OUTCOME S
Improved diagnostic and surveillance capacity formalaria
Improved cross-border coordination for malaria
S UPPORT TO COUNTRIE S
Cambodia Lao PDR Myanmar Viet Nam
S treng theningprovincialmalariadiag nos tic ands urveillancecapacity
S treng theningcros s -bordercoordinationfor malaria
Addres s ingmalaria amongmobile andmig rantpopulations
TRUS T FUND ALLOCATION
Totalallocationin million US $
1 4.37 S hare in RMTF 50%
DIS BURS E ME NT HIS TORY and PROJE CTION
Q4 201 5 Q1 201 6 Q2 201 6 Q3 201 6 Q4 201 6 Q1 201 7 Q2 201 7 Q3 201 7 Q4 201 7 Q1 201 8 Q2 201 8 Q3 201 8
1 8,759
1 ,600,1 39
287,81 4
1 ,423,535
805,089
1 ,368,347
2,855,652
1 76,22921 8,44075,698
4,560,429
25,81 9
1 3,41 5,950
Quarterly disbursements
Cumulative disbursement

28 Regional Malaria and Other Communicable Disease Threats Trust Fund
Rationale
Track, test, and treat is the mantra of malaria elimination, but this chain of events breaks down unless laboratory diagnostics and surveillance
systems are strong and well-functioning. The RMTF aimed to leverage ADB’s existing projects in communicable disease control that improved diagnostics and surveillance in the GMS, including to remote places and hard-to-reach populations, and strengthened cross-border cooperation.
Table 7: Results of Outcome 5.1Outcome 5.1 Increased diagnostic testing for malaria in project areas of Cambodia, Lao PDR, and Viet Nam
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 2017 2016 20171. Annual blood
examination per 100 pop at risk for malaria in the project areas*
Diagnostic capacity for malaria
1. Proportion of health facilities in project areas equipped with malaria diagnostic equipment
CAM 0 0 83 80
LAO 0 100 100 70CambodiaPreah Vihear Province
11.2 6.7 8.4 10.0 VIE** 78 78 100 1002. Proportion of laboratory
staff in target provinces trained in malaria diagnosis
CAM 0 0 100 100
LAO 0 0 96 70
VIE 0 100 100 100Lao PDR Champassack Province
12.7 7.9 9.2 10.0
Attapeu Province 25.5 13.4 18.5 10.0
Saravane Province 14.2 8.3 8.4 10.0
Sekong Province 17.4 12.1 14.6 10.0
Viet Nam Binh Phuoc Province
12.5 15.6 10.5 10.0
Dak Nong Province 12.8 10.4 13.3 10.0
Progress: Achieved at least 95% of target Substantial progress achievedCAM = Cambodia, LAO = Lao People’s Democratic Republic, VIE = Viet Nam.* Data from the Ministry of Health** Of the 182 commune health stations in the project areas, only 40 required new microscopes for malaria testingSource: Authors.
Table 8: Results of Outcome 5.2Outcome 5.2 Improved surveillance and response for malaria and other communicable diseases in project areas of
Cambodia, Lao PDR, and Viet Nam including in cross-border areas
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 2017 2016 20171. Proportion of disease
outbreaks (including malaria) in project areas reported within 24 hours
Surveillance capacity for malaria
1. Proportion of health facilities and laboratories in project areas equipped with electronic reporting instruments for malaria surveillance
CAM 0 0 100 100
LAO 0 0 100 50CambodiaPreah Vihear
100 100 100 80 VIE** 100 100 100 100
2. Proportion of health facilities in target provinces with staff trained in malaria surveillance with electronic reporting instrument
CAM 0 0 100 100
LAO 0 32 77 20
VIE 0 50 50* 80
continued on next page

Results by Outcome 29
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 2017 2016 2017Lao PDR Champassack
100 100 100 80 Cross-border coordination and response for malaria
Attapeu 50 100 100 80 3. Number of coordinated cross-border action plans developed based on GMS malaria elimination strategy in targeted border provinces
CAM 0 0 1 1
Saravane 100 80 100 80 LAO 0 2 2 2
Sekong 100 60 83 80 VIE*** 0 - - 3
Viet Nam Binh Phuoc
100 100 100* 80 4. Number of village health workers at border provinces trained in malaria control and treatment
CAM 0 0 331 332
Dak Nong 100 100 100* 80 LAO 0 0 322 60
2. Proportion of border disease outbreaks (including malaria) in project areas reported across borders within 24 hours
VIE 0 236 236* 40
Cambodia Preah Vihear
NA NA NA 50
Lao PDR Champassack
100 100 100 50
Attapeu 50 100 100 50
Saravane 100 80 100 50
Sekong 100 60 83 50
Viet Nam Binh Phuoc
100 100 100* 50
Dak Nong 100 100 100* 50
Progress: Achieved at least 95% of target Substantial progress achievedCAM = Cambodia, LAO = Lao People’s Democratic Republic, NA – no outbreaks of regional or international relevance, VIE = Viet Nam.* As of Q1 2017** Facilities already have the needed equipment*** No specific cross-border action plans were developed by provinces but six cross-border activities were incorporated into the provincial annual operational plans that were all implementedSource: Authors.
Table 8: continued
Table 9: Results of Outcome 5.3Outcome 5.3 Increased diagnostic testing for malaria in project areas of Myanmara,b,c
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 Q2 2018 2016 Q2 20181. National malaria
diagnostic quality assurance guidelines endorsed by the National Malaria Control Program
Diagnostic capacity for malaria
1. Proportion of health facilities in project areas equipped with malaria diagnostic equipment**
44 0 100 100
Mon State No No Yes Yes 2. Proportion of laboratory staff in target provinces trained in malaria diagnosis***
24 0 96 100
Sagaing Region No No Yes Yes 3. National malaria diagnostic quality assurance guidelines developed
No No Yes Yes
continued on next page
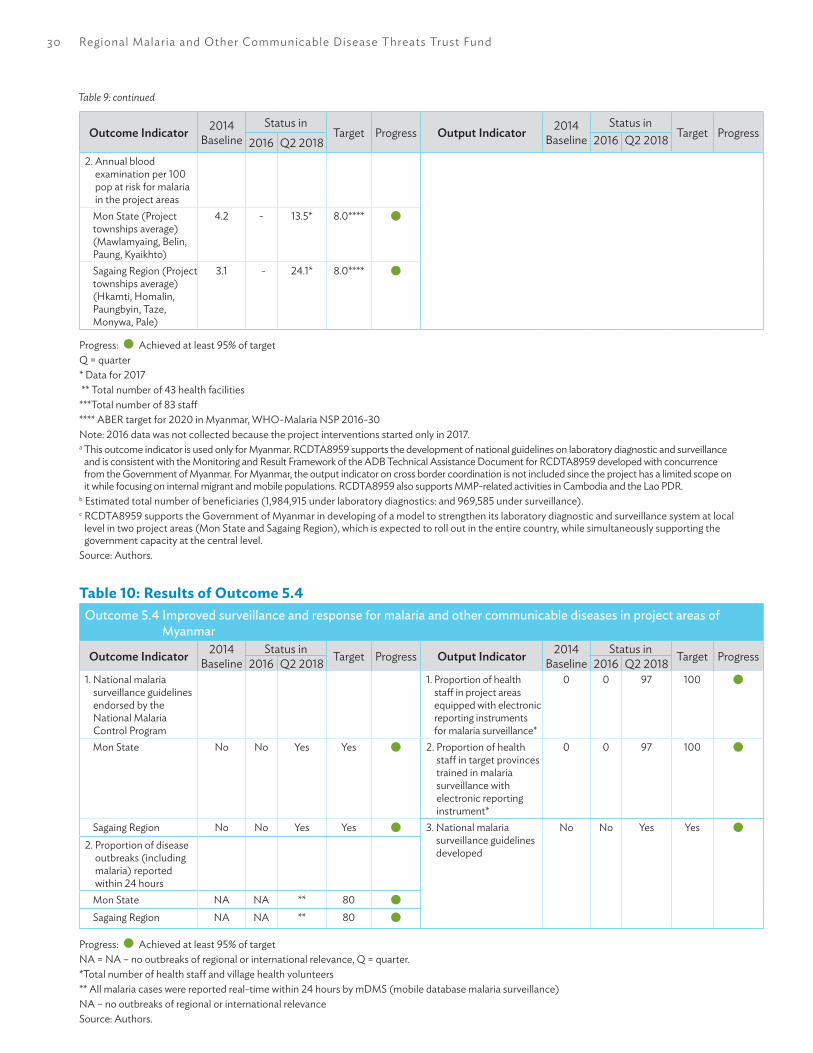
30 Regional Malaria and Other Communicable Disease Threats Trust Fund
Table 9: continued
Outcome Indicator 2014Baseline
Status inTarget Progress Output Indicator 2014
BaselineStatus in
Target Progress2016 Q2 2018 2016 Q2 2018
2. Annual blood examination per 100 pop at risk for malaria in the project areas
Mon State (Project townships average)(Mawlamyaing, Belin, Paung, kyaikhto)
4.2 - 13.5* 8.0****
Sagaing Region (Project townships average)(Hkamti, Homalin, Paungbyin, Taze, Monywa, Pale)
3.1 - 24.1* 8.0****
Progress: Achieved at least 95% of targetQ = quarter* Data for 2017 ** Total number of 43 health facilities***Total number of 83 staff**** ABER target for 2020 in Myanmar, wHO-Malaria NSP 2016-30Note: 2016 data was not collected because the project interventions started only in 2017.a This outcome indicator is used only for Myanmar. RCDTA8959 supports the development of national guidelines on laboratory diagnostic and surveillance
and is consistent with the Monitoring and Result Framework of the ADB Technical Assistance Document for RCDTA8959 developed with concurrence from the Government of Myanmar. For Myanmar, the output indicator on cross border coordination is not included since the project has a limited scope on it while focusing on internal migrant and mobile populations. RCDTA8959 also supports MMP-related activities in Cambodia and the Lao PDR.
b Estimated total number of beneficiaries (1,984,915 under laboratory diagnostics: and 969,585 under surveillance).c RCDTA8959 supports the Government of Myanmar in developing of a model to strengthen its laboratory diagnostic and surveillance system at local
level in two project areas (Mon State and Sagaing Region), which is expected to roll out in the entire country, while simultaneously supporting the government capacity at the central level.
Source: Authors.
Table 10: Results of Outcome 5.4Outcome 5.4 Improved surveillance and response for malaria and other communicable diseases in project areas of
Myanmar
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 Q2 2018 2016 Q2 20181. National malaria
surveillance guidelines endorsed by the National Malaria Control Program
1. Proportion of health staff in project areas equipped with electronic reporting instruments for malaria surveillance*
0 0 97 100
Mon State No No Yes Yes 2. Proportion of health staff in target provinces trained in malaria surveillance with electronic reporting instrument*
0 0 97 100
Sagaing Region No No Yes Yes 3. National malaria surveillance guidelines developed
No No Yes Yes2. Proportion of disease
outbreaks (including malaria) reported within 24 hours
Mon State NA NA ** 80Sagaing Region NA NA ** 80
Progress: Achieved at least 95% of target NA = NA – no outbreaks of regional or international relevance, Q = quarter.*Total number of health staff and village health volunteers** All malaria cases were reported real-time within 24 hours by mDMS (mobile database malaria surveillance)NA – no outbreaks of regional or international relevanceSource: Authors.

Results by Outcome 31
Communicable Disease Control 2– Additional Financing
The additional financing for malaria-related activities directed efforts toward controlling and eliminating malaria elimination through regional and country structures and processes already established under the ADB Communicable Disease Project 2 (CDC2). By allocating investments to the continuation of an existing ADB project, the RMTF was able to take previous gains, elevate them, and include malaria-specific interventions. Malaria activities funded under the RMTF complemented and augmented the national malaria programs in Cambodia, the Lao PDR, and Viet Nam and were synchronized with donor partners’ ongoing involvements in malaria and in addressing the spread of artemisinin resistance in the region.
In all three countries, the project’s activities strengthened and sustained vector control, promoted behavioral change, and strengthened malaria diagnosis, treatment, and surveillance capabilities. Through this project the RMTF was able to work at the grassroots level in cross-border areas, an otherwise extremely challenging environment in which to make an impact. The project brought about cooperation between the national malaria program and the communicable disease control (CDC) program at the central, provincial, and district levels. The two programs selected intervention sites together and jointly defined their priorities and resources needs for those sites.
In the areas identified for coverage by the RMTF project, support included provision of computer hardware, microscopes and other lab equipment; diagnostic supplies; and updating of lab standard operating procedures (SOPs) and quality assurance manuals and guidelines. The national malaria programs noted improvement in the quality of clinical diagnostic and case management through training conducted on malaria case management and treatment, surveillance for provincial and district health staff, and village health workers. Cross-border activities included disease information exchange, which included malaria and joint outbreak response simulation exercises.
Laboratory Quality Assurance and Malaria Surveillance in Myanmar
The RMTF-funded TA8959 project developed manuals, SOPs, and algorithms for malaria laboratory quality assurance for Myanmar. By bringing together the National Health Laboratory (NHL) and the NMCP, the project changed the way the two agencies worked together, which in turn also helped the NHL work with other disease agencies.
Data management systems for malaria surveillance in the project areas was strengthened, including the use of mobile data management system (mDMS) for case reporting, and analytical tools for decision-making. It worked with grassroots volunteer malaria workers to improve routine, and real-time case reporting through a mobile data management system piloted in the three townships. The mDMS, a smartphone-based app, was developed by Save the Children with the NMCP, but RMTF funding enabled widespread piloting of the app for volunteer malaria workers and the initial results helped improve the app to make it more efficient and more user-friendly. The NMCP and other development partners are reviewing the mDMS together with another mobile app developed by wHO for facility-based health workers.
Migrant and Mobile Populations
In Cambodia, the Lao PDR, and Myanmar, the RMTF extended the reach of the health system by training and equipping village health volunteers and migrant workers for malaria diagnosis and treatment, and mobile traders as volunteer peer educators to conduct health education and prevention. These volunteers formed the first line of defense against communicable diseases. The International Organization for Migration (IOM) worked with the national malaria programs in the three countries to develop innovative approaches to address malaria needs of migrant and mobile populations in work settings such as gold and jade mines, rubber plantations, and dam construction sites.
32 Regional Malaria and Other Communicable Disease Threats Trust Fund
One of the key successes of the project is the engagement of the private sector by tapping and mobilizing camp site and construction managers as malaria volunteers. The managers were granted permission by the corporation heads to implement malaria control and prevention programs in their respective worksites. A final review mission in March 2018 found that mobile traders from the Lao PDR and Viet Nam, who ply around the district and who were trained as malaria peer educators, were found to effectively reach mobile and migrant populations (MMPs) with systematic malaria monitoring and have good coordination with the village volunteers.
Enabling Factors
Overall, building on existing project management units and the regional cooperation mechanisms established under the CDC2 project in Cambodia, the Lao PDR, and Viet Nam accelerated the achievements of the CDC2 AF in the provinces and districts and institutionalized malaria-specific SOPs.
In Myanmar, bringing together two different actors—the national health laboratories and the national malaria control program—under a common framework was transformational. with common SOPs and manuals on laboratory quality assurance, they were able for the first time to synchronize their reporting. Recruiting the right partners was also key: University Research Co. LLC (URC), and the IOM were chosen for their existing strong and deep presence in Myanmar and the Lao PDR. They brought with them an understanding of the local landscape, and existing relationships that could not be quickly achieved by a new player, smoothing the way for a good consultation process with country counterparts.
Next Steps and Sustainability Pathway
Case Detection and Laboratory TestingIn the Lao PDR, the reduction in malaria incidence can also be attributed to government efforts,
including discouraging illegal logging and people going into forests, and increased army patrols. Malaria cases may start to rise if these efforts are not sustained, through cooperation with the private sector and the military.
There is need to sustain and expand ICT infrastructure for better case reporting, as well as staff competencies on facility management, infection control, disease management through more health-care worker training. There is also a need to strengthen subnational financial management, so that funds reach the districts where they are required, to properly implement the 1–3–7 malaria elimination strategy.16
In Cambodia, as for the other GMS countries, mechanisms for microscopy skills retention and laboratory quality assurance should be in place, as fewer malaria cases will be seen during the elimination phase. while laboratory staff in Cambodia, for example, have stated a preference to use rapid diagnostic tests rather than microscopy, since this is easier, health-care workers should actually perform microscopy for malaria diagnosis. This is in line with the country’s malaria elimination strategy, which states that each case must be confirmed by microscopy before treatment can be provided, as recommended by wHO. The technical support under CDC2-AF was able to provide microscopes, training on microscopy, and updated guidelines. The microscopes provided can digitally capture and share digital image of the blood smears. This cuts down diagnosis time and should facilitate timely treatment.
The country’s medicine stocking and redistribution policy and processes should be adjusted. Cambodia experienced stockouts of malaria testing kits and medicines in 2018. The malaria program claims that this was due to the unexpected increase in the malaria cases, and there were difficulties restocking. Extra supplies from other provinces could not be directly channeled to the facilities where they were needed, as these commodities had to be first be channeled back to the central level.
16 The 1–3–7 malaria elimination strategy entails reporting of malaria cases within 1 day, confirmation and investigation within 3 days, and response to prevent further transmission within 7 days.
Results by Outcome 33
Malaria P. vivax cases are increasing and this requires glucose-6-phosphate dehydrogenase (G6PD) testing and close supervision during treatment, patient counseling and access to blood transfusion services for G6PD-deficient individuals. This will require health facilities and service providers in malaria endemic areas to have the right laboratory equipment and commodities, training, and mechanisms for medical supervision of G6PD-deficient cases.
Cross-Border Information ExchangeCambodia, the Lao PDR, and Viet Nam have started to exchange data on an agreed list of communicable diseases of public health significance. However, the frequency and timeliness of information exchange can still be improved, and data standards, such as for case definition, need to be aligned.
Migrant and Mobile PopulationsIn discussions with the members of the Cambodia malaria program, it is clear that MMPs are still one of the main sources of malaria transmission and drug resistance. It also appears that the government does not have the capacity to address MMP issues, which include a general lack of access to health services, especially for foreign MMPs and undocumented workers. Some tend to self-medicate and travel to home countries to access health services. The issue of malaria elimination among MMPs must be integrated into the national health strategy, and addressing the issue of how to reach MMPs will also require stronger collaboration with the private sector.
Another challenge is sustaining the motivation, skills, and work of malaria health volunteers and peer educators as malaria incidence goes down and when Global Fund grant support for GMS countries ends and financing switches to their governments instead. In Cambodia, the government cannot pay for activities that are conducted beyond 20 kilometers from the health facilities, and most MMPs are forest goers. The government therefore relies on NGOs, which also have flexible systems that allow them to pay for volunteer health workers people outside the public health system. Treatment compliance among MMPs is also challenging. The first dose of malaria treatment is usually administered at the health facility, but problems remain with ensuring completion of treatment doses.
In Myanmar, the project with URC started under the RMTF will continue through Defeat Malaria Activity funded by the United States Agency for International Development. The Global Fund is working on funding support for IOM–Myanmar to continue its work on malaria and migrant and mobile population in the RMTF project sites. Central and provincial health offices in Cambodia and the Lao PDR have committed to sustain mobilization of village volunteers, particularly training of mobile traders as outreach and peer educators. This model was piloted under CDC2-AF has been expanded to the other provinces using Global Fund grants.

34 Regional Malaria and Other Communicable Disease Threats Trust Fund
P R O M OT I O N A N D P R E V E N T I O N
Increased capacity to apply heath impact assessment to consider determinants of health and communicable d iseases in infrastructure projects
6R-CDTA 8763:
Results for Malaria Elimination and Control of Communicable Diseases Threats in Asia and the Pacific (RECAP)
Output 6 communicable diseases addressed in infrastructure projects
OUTCOME 6: Increased capacity to address communicable diseases in infrastructure projects
KE Y OUTCOME S
Increased capacity to address communicablediseases in infrastructure projects
HE ALTH IMPACT AS S E S S ME NTDE MONS TRATION PROJE CT
Cambodia Lao PDR Myanmar Thailand Viet Nam
E nerg y
Trans port
Urbandevelopment
Water s upply
Water ands anitation
S pecialeconomiczones
TRUS T FUND ALLOCATION
Totalallocationin million US $
3.39** Increased from 2.96
S hare in RMTF 1 2%
DIS BURS E ME NT HIS TORY and PROJE CTION
Q3201 5
Q4201 5
Q1201 6
Q2201 6
Q3201 6
Q4201 6
Q1201 7
Q2201 7
Q3201 7
Q4201 7
Q1201 8
Q2201 8
Q3201 8
307,61 0303,01 4
584,1 21
830,849
1 52,594
1 98,1 33
268,81 0241 ,670
68,740
1 93,328
1 20,1 5891 ,836
26,741
3,387,604
Quarterly disbursements
Cumulative disbursement

Results by Outcome 35
Rationale
Infrastructure projects have a health dimension that can be assessed, the impact ameliorated, and the benefits magnified to prevent malaria and other communicable diseases, and promote healthy development. The current public health challenges that stem from the interface of development and environmental and social change include the impacts of developing economic corridors and special economic zones (SEZs), issues of air quality, water and food security, and growing mobility. Antimicrobial resistance and poor coverage of informal often mobile and migrant population groups working in infrastructure development projects also justify the need for HIA.
Malaria Prevention in Infrastructure Development
The promotion and prevention component of the RMTF promoted HIA as a means to mitigate vector-borne diseases risks in large-scale infrastructure projects and improve community health outcomes. Large infrastructure projects attract mobile and migrant populations—those most at risk of malaria. The RMTF created an opportunity to advance HIA, particularly in the GMS, as a good practice to ensure project designs can safeguard and promote human health. The promotion of HIA was timely given the current public health challenges that stem from the interface of development and environmental and social change.
In the GMS countries, HIA policies and practice and efforts to include HIA as a formal part of infrastructure development planning and investment practice have been at different stages of development. Under the RMTF, HIA was promoted as an intersectoral approach to protecting and promoting community health and safety. Capacity for HIA practice expanded in the GMS in the past 2 years with RMTF support. The project became a catalyst for renewed interest for HIA as a development planning tool drawing attention to health risks and health co-benefits and facilitating healthy design and management of infrastructure projects.
An interrelated package of support was provided, to GMS countries and at regional level, for capacity development. To demonstrate HIA good practice, case studies were conducted in various sectors, i.e., energy, SEZs and border development, transport, urban development, and water and sanitation. These case studies, considering both community and occupational health and safety, offered recommendations to manage risks and benefits as part of the project planning, design and implementation.
Case Study in Urban Development Project
An HIA was developed for Mandalay Urban Services Improvement Project 1, which included a Public Health Management Plan (PHMP) with health indicators for monitoring of community health impacts. Stakeholder consultations promoted collaboration between project stakeholders and public health authorities for the implementation of the PHMP and discussion of institutional arrangements for the monitoring and management of vector-related diseases such as malaria and their environmental determinants. The meetings also enabled discussions on strengthening the capacity of local public health and environmental conservation teams to support public awareness and education campaigns. Project stakeholders, including government local health and environment staff, were trained on HIA.
Case Studies in Special Economic Zones and Border Development
HIAs were initiated in three SEZs—Savannakhet (Savan-SENO), the Lao PDR; Mukdahan, Thailand; Thilawa, Myanmar and in a border economic zone—Yunnan Lincang Border Economic Cooperation Zone Development, People’s Republic of China (PRC). In the PRC, HIA involved rapid scoping and an analysis of health risks such as vector-borne diseases and impacts and recommendations for mitigation. The recommendations, developed in partnership with local health officials, were required to protect both workers and community members, include malaria services and supplemental to the

36 Regional Malaria and Other Communicable Disease Threats Trust Fund
Table 11: Results of Outcome 6.1Outcome 6.1 Increased capacity to apply health impact assessment (HIA) in infrastructure projects at country level
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 Q2 2018 2016 Q2 20181. Number of countries
that started to apply HIA in infrastructure projects (LAO, THA)
0 0 2 2 Situational analysis and needs assessment
1. Number of HIA country profiles (CAM, LAO, MYA, THA, VIE)
0 0 5 5
2 Number of infrastructure projects that applied HIA (Savannakhet, Mukdahan, Hongsa)
0 0 3 3 Country HIA guidelines
2. Number of countries with country HIA guidelines developed
0 0 3 3
3. Regional HIA framework for special economic zones developed
0 0 1 1
Capacity development
4. HIA training modules developed
No No Yes Yes
5. Number of countries with staff trained in HIA
0 0 4 4
6. HIA curriculum developed for graduate public health and environmental programs
No No Yes Yes
7. Number of countries that integrated HIA curriculum into graduate public health and environmental programs
0 0 4 4
8. Number of countries that started to offer HIA in graduate public health and environmental programs
0 0 4 4
9. Regional network of HIA experts and universities established
0 0 1 1
Policy and governance
10. Number of countries with costed HIA proposal
0 0 5 5
11. Number of countries with HIA policies in place or developed
0 0 3 3
12. Number of countries with intersectoral coordination on HIA
0 0 3 3
13. Number of HIA policy briefs developed
0 0 2 2
Progress: Achieved at least 95% of target CAM = Cambodia, HIA = health impact assessment, Lao PDR = Lao People’s Democratic Republic, MYA = Myanmar, THA = Thailand, VIE = Viet Nam.Source: Authors.

Results by Outcome 37
existing environment impact assessment and management plan.
HIA in the three SEZs enabled the development of an HIA framework for SEZs in the GMS, which can serve as a management tool for the continued development of healthy economic zones in the subregion.17 Country-specific guidelines were also produced for the Lao PDR, Myanmar, and Thailand reflecting their local context and specific requirements. Cross-border cooperation has also been promoted, with the Lao PDR and Thailand bilateral cooperation agreement for joint health surveillance and reporting, particularly in the affected border areas between Savannakhet and Mukdahan SEZs.
Curriculum Development and Training
To increase HIA capacity in the region key government agencies and universities should cooperate to improve the skills and knowledge of those currently involved in HIA, and build a new generation of HIA experts. In partnership with the wHO Collaborating Center for Impact Assessment at Curtin University (wHO CC-Curtin University) three curricula were developed—a standalone HIA course; HIA in environmental impact assessment;
and HIA in planning, environment, or health courses. Using adapted curricula, certificate courses were subsequently offered by six GMS universities and parallel training workshops were led by health ministries. Over 600 HIA practitioners from key government agencies and staff from the private sector have been trained on basic principles and practice of HIA, application of tools, exploring decision-making criteria and options for institutional arrangements between the health and environment sectors to support a coordinated approach to HIA. within ADB, ADB staff have been trained on HIA as part of staff development training program, using the bank’s own funding.
Regulation and Guidelines
To ensure infrastructure projects do not inadvertently increase the risk of malaria and undermine efforts to eliminate the disease, national legislation for HIA implementation is essential. In the GMS, both the Lao PDR and Thailand have an HIA policy as part of their healthy public policy since 2006 and 2000, respectively. Technical assistance through RMTF made possible a review of HIA policy and implementation and the development of sector-specific guidelines for these countries. In Cambodia, Myanmar, and
17 ADB. 2018. A Health Impact Assessment Framework for Special Economic Zones in the Greater Mekong Subregion. Manila.
Table 12: Results of Outcome 6.2Outcome 6.2 Increased capacity to apply HIA at ADB
Outcome Indicator 2014Baseline
Status in Target Progress Output Indicator 2014Baseline
Status in Target Progress2016 Q2 2018 2016 Q2 20181. Number of
ADB-supported infrastructure projects in malaria-endemic areas that applied HIA* (CAM, MYA, VIE)
0 0 4 4 1. ADB HIA tools developed (sourcebook and checklists)
No Yes Yes Yes
2. ADB HIA training modules developed
No Yes Yes Yes
3. Number of ADB staff trained in HIA
0 30 30 30
4. ADB HIA tools integrated into ADB processes
No No Yes Yes
Progress: Achieved at least 95% of target *Desktop review ADB = Asian Development Bank, CAM = Cambodia, HIA = health impact assessment, MYA = Myanmar, VIE = Viet Nam.Source: Authors.

38 Regional Malaria and Other Communicable Disease Threats Trust Fund
Viet Nam, the RMTF has enabled discussion between ministries of health and ministries of environment on the integration of health into the well-functioning environment impact assessment processes. Moreover, HIA guidelines have been prepared for these countries for further intergovernmental review led by each country’s ministry of health. Country and sector-specific guidelines allow for more explicit community health and workers’ health and safety components in infrastructure development, which can be used as part of the malaria elimination effort in these countries.
within ADB, an HIA sourcebook has been developed, providing clear procedures to ensure commitment for community and occupational health and safety are met in the development and implementation of projects. Following this new guideline, advocacy for HIA in large projects continues, including consultation with safeguards staff on stronger monitoring of health impacts from projects to mitigate risks of malaria. Further, an addendum on health has been proposed for inclusion in the ADB Handbook on Poverty and Social Analysis. This could support the assessment of community health attributes of a project.
Enabling Factors
At the country level, the key to success of every project was the presence of a local champion within the country counterpart agencies, and also engagement of local consultants who could carry the work of the international consultants forward in the local language. keeping HIA highly visible within ADB over a protracted period of time paid off, both in terms of creating demand for HIA training, and for advocacy for resources to continue the work started under the RMTF. The project came at a time when a tipping point could be reached within ADB, and the bank has become the only multilateral financing institutions with so much experience in
HIA to share with development partners. Engaging with the wHO CC-Curtin University on HIA to develop curricula and then disseminating them through local universities was a very successful strategy to mainstream HIA and make local training in it sustainable.
Next Steps and Sustainability Pathway
Countries still have unexploited opportunities to formally adopt national HIA guidelines and other HIA tools, particularly in the provinces. within the health sector, institutional arrangements must govern HIA with clear and functional links to other MOH departments and health programs. There is a need to further strengthen intersectoral cooperation to apply HIAs and implement PHMP to mitigate risks of malaria and other communicable disease threats as it relates to development projects. This requires clear institutional arrangements between public health, environment, and planning authorities, including at provincial level.
Governments still need to agree on the nature of HIA, not only in terms of health risk assessment with a view to mitigation, but also in identification of health opportunities to promote health co-benefits from development projects., such as through provision of health services to MMPs who often work in large development projects, integrated border development projects or SEZs. To encourage and sustain improvements in the practice of HIA, a network was established jointly with the wHO CC-Curtin University. It is envisaged that the HIA Network Asia Pacific will facilitate collaboration between countries and HIA practitioners, including research and sharing of good practices.18 The GMS Health Cooperation Strategy and Action Plan for 2018–2022 will guide forward programming and mobilizing resources for health cooperation, and includes HIA as one of the strategic and operational priorities. This provides additional opportunities to expand HIA work in the GMS.
18 About the HIA Network Asia Pacific. http://www.hianetworkasiapac.com/about/

4. kNOwLEDGE PRODUCTS AND PUBLICATIONS
Regional Malaria and Other Communicable Disease Threats Trust FundADB. 2015. Malaria Elimination: An entry point for strengthening heath systems and regional security, and a public health best buy. Manila. https://www.adb.org/sites/default/files/publication/178203/malaria-elimination.pdf
LeadershipM. Counahan et al. 2018. Investing in Regional Health Security for Sustainable Development in Asia and the Pacific. ADB Sustainable Development Working Paper Series No. 56. Manila: Asian Development Bank. https://www.adb.org/publications/regional-health-security-asia-pacific
MedicinesS. Roth et al. 2018. Strong Regulation of Medical Products: Cornerstone of Public Health and Regional Health Security. ADB Briefs. No. 99. Manila: Asian Development Bank. https://www.adb.org/sites/default/files/publication/456866/adb-brief-099-strong-regulation-medical-products.pdf
S. Roth et al. 2018. Portable Screening Devices for Medicines Quality: Putting Power into the Hands of Regulators in Low-Resource Settings. ADB Briefs. NO.101. Manila: Asian Development Bank. https://www.adb.org/sites/default/files/publication/461051/adb-brief-101-screening-devices-medicine-quality.pdf
S. Roth et al. 2016. Strong Supply Chains Transform Public Health. ADB Briefs. No. 72. Manila: Asian Development Bank. https://www.adb.org/sites/default/files/publication/214036/strong-supply-chains.pdf
S. Roth et al. 2016. Better Regulation of Medicines Means Stronger Regional Health Security. ADB Briefs. No. 54. ADB Briefs No. 54, Manila: Asian Development Bank. https://www.adb.org/sites/default/files/publication/184392/better-regulation-medicine.pdf
Information TechnologyADB. Forthcoming. Digital Health Convergence Meeting Toolkit.
P. Drurry et al. 2018. Guidance for Investing in Digital Health. ADB Sustainable Development Working Paper Series. No.52. Manila: Asian Development Bank. https://www.adb.org/sites/default/files/publication/424311/sdwp-052-guidance-investing-digital-health.pdf
ADB. 2018. Unique Health Identifier Assessment Tool Kit. Manila https://www.adb.org/documents/unique-health-identifier-assessment-toolkit
A. Marclo et al. 2018. Transforming Health Systems Through Good Digital Health Governance. ADB Sustainable Development Working Paper Series. No.

40 Regional Malaria and Other Communicable Disease Threats Trust Fund
51. Manila: Asian Development Bank. https://www.adb.org/publications/transforming-health-systems-good-digital-health-governance.
S. Ebener et al. 2018. Building Capacity for Geo-Enabling Health Information Systems: Supporting Equitable Health Services and well-Being for All. ADB Briefs. No. 88. Manila: Asian Development Bank. https://www.adb.org/publications/building-capacity-geo-enabling-health-information-systems.
S. Mellor et al. 2016. Digital Health Infrastructure: The Backbone of Surveillance for Malaria Elimination. ADB Briefs. No. 69. Manila: Asian Development Bank. https://www.adb.org/sites/default/files/publication/210856/digital-health-infrastructure.pdf.
M. Stahl et al. 2018. On the Road to Universal Health Coverage Every Person Matters. ADB Briefs. No. 56. Manila: Asian Development Bank. https://www.adb.org/sites/default/files/publication/183512/uhc-every-person-matters.pdf
S. Roth et al. 2016. The Geography of Universal Health Coverage. ADB Briefs. No. 55. Manila: Asian Development Bank. https://www.adb.org/sites/default/files/publication/183422/geography-uhc.pdf
S. Roth et al. 2015. Universal Health Coverage By Design. ADB Briefs. No. 36. Manila: Asian Development Bank. https://www.adb.org/sites/default/files/publication/160117/universal-health-coverage-design-ict.pdf
Promotion and PreventionADB. 2018. A Health Impact Assessment Framework for Special Economic Zones in the Greater Mekong Subregion. Manila. https://www.adb.org/publications/health-impact-assessment-framework-economic-zones-gms.
ADB. 2016. Greater Mekong Subregion Health Impact Assessment Project: Project Brief. Manila. https://www.adb.org/publications/gms-health-impact-assessment-project-brief.
OthersADB and world Health Organization. 2016. Monitoring Universal Health Coverage in the Western Pacific. Framework, indicators and dashboard. Manila. https://www.adb.org/sites/default/files/publication/203926/uhc-western-pacific.pdf.

5. GENDER DIMENSIONS
ADB’s Strategy 2020 identifies gender equity as one of the five drivers of change that are emphasized in all of its operations. ADB’s commitment to gender equality is integral to the management of the RMTF. ADB loans and grants meeting specific requirements include a gender action plan (GAP), with a clear monitoring and evaluation framework.
There are several specific gender issues related to malaria and other communicable diseases, which are considered under the RMTF implementation. Men are more at risk to contract malaria through occupational exposure during night time in rubber plantations, forests and mines, for example. On the other hand, women shoulder the main burden of taking care of sick family members, and pregnant women are more vulnerable to develop severe malaria. However, typically there is a lack of sex-disaggregated data in national malaria information systems. In terms of malaria project staffing, although there are more female than male village-level malaria workers, at the management level in national malaria programs, there are more men than women. In some settings, such as plantations deep in forested areas where it was difficult or dangerous for women to work, it was more appropriate to work with male volunteers rather than females.
Gender activities were integrated into the implementation of the main activities of the project, notably the additional financing to Second GMS Regional Communicable Diseases Control Project,
which specifically included gender action plans for each country to address some of the issues raised above.
Some key achievements for Cambodia, the Lao PDR, and Viet Nam are detailed in the following tables, according to three dimensions: (i) enhancement of opportunities for female staff in Center for Disease Control systems and improved gender analysis in regional CDC systems; (ii) improved responsiveness of CDC to gender/ethnic issues in targeted districts and/or province and increased participation and awareness of women in CDC prevention in project location; and (iii) enhanced gender-awareness and responsiveness of CDC project management.
Highlights include the fact that 100% of surveillance and response data in the Lao PDR is sex-disaggregated. In Viet Nam, data collected since 2016 is disaggregated and in Cambodia, malaria and other key communicable disease data has been sex-disaggregated. This data is widely used in project plans across the three countries. All three have also shown marked increased in hiring of new female staff, increasing the overall proportion of female staff from 44% in 2012 to 54% in 2016 Cambodia, and from 45% in 2014 to 61.7% in 2016 in the Lao PDR. women are equally represented in the ranks of volunteer health workers (VHw) in the Lao PDR, account for 44% of VHws trained since 2012 in Cambodia, and accounted for the majority trained in Viet Nam.

6. A
NN
Ex
Ann
ex A
: RM
TF R
esul
ts-B
ased
Fra
mew
ork
IMPA
CTRe
duce
d ris
k to
the
Asia
and
the
Paci
fic re
gion
and
glo
bally
from
drug
-res
istan
t mal
aria
and
oth
er c
omm
unic
able
dise
ase
thre
ats
REG
ION
AL
AN
D N
ATIO
NA
L O
UTC
OM
EIn
crea
sed
natio
nal a
nd re
gion
al c
apac
ity to
impl
emen
t stra
tegi
es a
nd e
nsur
e re
spon
se
KEY
OU
TCO
MES
TH
AT A
DB
STRA
TEG
ICA
LLY
CON
TRIB
UTE
S TO
:
OU
TCO
ME
1LE
AD
ERSH
IPSt
reng
then
ed le
ader
ship
, de
cisio
n-m
akin
g and
acc
ount
-ab
ility f
or m
alar
ia e
limin
atio
n an
d ad
dres
sing c
omm
unic
able
di
seas
e th
reat
s
OU
TCO
ME
2FI
NA
NCI
NG
Incr
ease
d fin
anci
ng fo
r mal
aria
el
imin
atio
n an
d ad
dres
sing
com
mun
icab
le d
iseas
e th
reat
s
OU
TCO
ME
3M
EDIC
INES
Impr
oved
regu
lato
ry c
apac
ity
to su
ppor
t inc
reas
ed av
aila
bil-
ity a
nd u
se o
f qua
lity-
assu
red
heal
th p
rodu
cts f
or m
alar
ia
and
othe
r com
mun
icab
le d
is-ea
ses
OU
TCO
ME
4IN
FORM
ATIO
N
SYST
EMS
Incr
ease
d us
e of
qua
lity d
ata,
in
form
atio
n to
ols a
nd te
chno
l-og
ies t
o im
prov
e m
alar
ia a
nd
othe
r com
mun
icab
le d
iseas
e in
form
atio
n sy
stem
s
OU
TCO
ME
5LA
BORA
TORY
D
IAG
NO
STIC
S A
ND
SU
RVEI
LLA
NCE
Impr
oved
cap
acity
of l
abor
a-to
ry d
iagn
ostic
s and
surv
eil-
lanc
e sy
stem
for m
alar
ia a
nd
othe
r com
mun
icab
le d
iseas
es,
incl
udin
g cro
ss-b
orde
r coo
r-di
natio
n
OU
TCO
ME
6PR
OM
OTI
ON
AN
D
PREV
ENTI
ON
nc
reas
ed c
apac
ity to
app
ly
heal
th im
pact
ass
essm
ent
to c
onsid
er d
eter
min
ants
of
heal
th a
nd c
omm
unic
able
di
seas
es in
infra
stru
ctur
e pr
ojec
ts
Regi
onal
Cap
acity
Dev
elop
-m
ent T
echn
ical
Ass
istan
ce
(RCD
TA) 8
485
RCD
TA 8
681
RCD
TA 8
763
RCD
TA 8
763
RCD
TA 8
763
RCD
TA 8
763
RCD
TA 8
656
RCD
TA 8
959
& C
DC
II-A
FG
448
CAM
G44
9 LA
OG
450
VIE
RCD
TA 8
763

Annex 43
FOCU
SIN
G O
N R
ESU
LTS
PRO
GRE
SS T
OW
ARD
KEY
OU
TCO
MES
AN
D O
UTP
UTS
OU
TCO
ME
1: LE
AD
ERSH
IPSt
reng
then
ed le
ader
ship
, dec
ision
-mak
ing,
and
acco
unta
bilit
y for
elim
inat
ing m
alar
ia a
nd a
ddre
ssin
g com
mun
icab
le d
iseas
e th
reat
s O
utco
me
1.1 In
crea
sed
com
mitm
ent a
nd c
olla
bora
tion
for m
alar
ia e
limin
atio
n an
d ad
dres
sing
com
mun
icab
le d
iseas
e th
reat
s
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
1620
1720
1620
171.
Num
ber o
f mal
aria
-end
emic
cou
ntrie
s th
at e
ndor
sed
the
mal
aria
elim
inat
ion
road
map
013
14*
21**
1. M
alar
ia e
limin
atio
n ro
ad m
ap
deve
lope
dN
oYe
sYe
sYe
s
2. N
umbe
r of d
onor
cou
ntrie
s tha
t en
dors
ed th
e m
alar
ia e
limin
atio
n ro
ad
map
07
7***
7
Prog
ress
: A
chie
ved
or o
n tra
ck* C
ambo
dia,
Indi
a, In
done
sia, L
ao P
eopl
e’s D
emoc
ratic
Rep
ublic
Mal
aysia
, Mya
nmar
, Pap
ua N
ew G
uine
a, P
eopl
e’s R
epub
lic o
f Chi
na, P
hilip
pine
s, Re
publ
ic o
f kor
ea, S
olom
on Is
land
s, Th
aila
nd, V
a-nu
atu,
Vie
t Nam
** A
PLM
A’s 2
020
targ
et**
Aus
tralia
, Bru
nei D
arus
sala
m, J
apan
, New
Zea
land
, Rus
sian
Fede
ratio
n, S
inga
pore
, Uni
ted
Stat
es
Stor
y be
hind
the
num
bers
•Th
e A
sia P
acifi
c Lea
ders
Mal
aria
Allia
nce
(APL
MA)
wor
ks to
advo
cate
for e
limin
atin
g mal
aria
and
addr
essin
g thr
eats
from
com
mun
icab
le d
iseas
es. I
t pro
mot
es re
gion
al co
ordi
natio
n at
the
high
est
leve
l. APL
MA
has
succ
essf
ully
bro
kere
d le
ader
-leve
l Eas
t Asia
Sum
mit
Stat
emen
ts o
n m
alar
ia e
limin
atio
n sin
ce 20
14. I
n ea
rly 20
17, f
ourte
en h
eads
of g
over
nmen
t rea
ffirm
ed th
eir c
omm
itmen
t and
w
elco
med
pro
gres
s in
the
impl
emen
tatio
n of
the
prop
osed
act
ions
in th
e en
dors
ed A
sia P
acifi
c Le
ader
s’ M
alar
ia E
limin
atio
n Ro
ad M
ap.

44 Annex
Out
com
e 1.2
Impr
oved
use
of i
nfor
mat
ion
for d
ecisi
on-m
akin
g an
d ac
coun
tabi
lity f
or m
alar
ia e
limin
atio
n an
d ad
dres
sing
com
mun
icab
le d
iseas
e th
reat
s
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
1620
1720
1620
171.
Mal
aria
Elim
inat
ion
Das
hboa
rd u
sed
to
info
rm h
igh-
leve
l reg
iona
l pol
icy d
ialo
g on
mal
aria
elim
inat
ion
No
No
Yes
Yes
1. M
alar
ia E
limin
atio
n D
ashb
oard
pr
otot
ype
No
Yes
Yes
Yes
2. N
umbe
r of c
ount
ries w
ith d
ata
com
pile
d fro
m th
e w
orld
Hea
lth
Org
aniza
tion
(wH
O) f
or th
e te
chni
cal
anne
x of t
he M
alar
ia E
limin
atio
n D
ashb
oard
022
2222
3. N
umbe
r of c
ount
ries w
ith d
ata
com
pile
d fo
r Mal
aria
Elim
inat
ion
Das
hboa
rd in
dica
tors
04
2222
4. M
alar
ia E
limin
atio
n D
ashb
oard
fin
alize
dN
oN
oN
oYe
s
2. In
vest
men
t cas
es a
nd to
olki
t res
ults
us
ed to
info
rm h
igh-
leve
l reg
iona
l po
licy d
ialo
g on
mal
aria
fina
ncin
g
No
No
Yes
Yes
1. Co
stin
g fra
mew
ork a
nd to
ols
deve
lope
d*N
oYe
sYe
sYe
s
2. N
umbe
r of c
ount
ries/
subr
egio
n w
ith
cost
ing f
or m
alar
ia e
limin
atio
n*
(BA
N, I
ND
, PN
G, G
MS)
02
24
3. N
umbe
r of c
ount
ry/s
ubre
gion
al
inve
stm
ent c
ases
dev
elop
ed*
(BA
N, I
ND
, PN
G, G
MS)
00
44
4. N
umbe
r of b
usin
ess c
ases
for p
rivat
e se
ctor
inve
stm
ent i
n m
alar
ia c
ontro
l an
d el
imin
atio
n*
(BA
N/IN
D/P
NG
and
GM
S)
00
22
5. M
alar
ia p
rogr
am e
ffici
ency
ana
lysis
tool
(MPE
AT)*
00
11
6. R
ecom
men
datio
ns d
evel
oped
on
finan
cing
opt
ions
for t
he A
sia a
nd
Paci
fic R
egio
n*
No
No
Yes
Yes
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
BAN
= B
angl
ades
h, IN
D =
Indi
a, G
MS
= G
reat
er M
ekon
g Sub
regi
on.
* Upo
n re
view
of t
he lo
gica
l flow
of o
utpu
ts a
nd o
utco
mes
, the
se o
utpu
ts th
at w
ere
prev
ious
ly tr
acke
d un
der O
utco
me
2 (F
inan
cing
) are
mov
ed h
ere
as th
ese
bette
r con
tribu
te to
war
d im
prov
ed u
se o
f in
form
atio
n fo
r dec
ision
-mak
ing a
nd a
ccou
ntab
ility f
or m
alar
ia e
limin
atio
n an
d ad
dres
sing c
omm
unic
able
dise
ase
Stor
y be
hind
the
num
bers
Mal
aria
elim
inat
ion
dash
boar
d
•Th
e A
PLM
A M
alar
ia E
limin
atio
n D
ashb
oard
is a
dec
ision
and
acc
ount
abilit
y too
l tha
t pro
vide
s visi
bilit
y to
natio
nal a
nd re
gion
al p
rogr
ess t
owar
d m
alar
ia e
limin
atio
n ta
rget
s, as
wel
l as f
ulfil
lmen
t of
prio
rity a
ctio
ns a
nd id
entifi
catio
n of
are
as re
quiri
ng a
ttent
ion.
Tw
enty
mal
aria
-end
emic
cou
ntrie
s hav
e ag
reed
to u
se th
e da
shbo
ard
and
its a
ssoc
iate
d te
chni
cal a
nnex
to in
form
hig
h-le
vel r
egio
nal
polic
y dia
log o
n m
alar
ia e
limin
atio
n. T
he d
ashb
oard
dat
a was
gath
ered
from
the
APL
MA
coun
tries
usin
g a q
uest
ionn
aire
, and
the
tech
nica
l ann
ex u
ses t
he la
test
dat
a fro
m th
e w
orld
Mal
aria
Rep
ort
2017
pub
lishe
d in
Nov
embe
r 201
7. Th
e A
PLM
A M
alar
ia E
limin
atio
n D
ashb
oard
was
pre
sent
ed a
nd d
iscus
sed
as a
tool
to in
form
hig
h-le
vel r
egio
nal p
olic
y di
alog
on
mal
aria
elim
inat
ion
durin
g th
e A
PLM
A S
enio
r Offi
cial
’s M
eetin
g in
Dec
embe
r 201
7 an
d pu
blic
atio
n vi
a th
e A
PLM
A w
ebsit
e is
due
by th
e en
d of
201
8.
cont
inue
d on
nex
t pag
e

Annex 45
Stor
y be
hind
the
num
bers
Inve
stm
ent c
ases
and
tool
kit f
or fi
nanc
ing
mal
aria
elim
inat
ion
•To
asse
ss th
e ec
onom
ic ra
tiona
le fo
r mal
aria
elim
inat
ion,
thre
e na
tiona
l leve
l inve
stm
ent c
ases
in B
angl
ades
h, In
done
sia, a
nd P
apua
New
Gui
nea (
PNG
), as
wel
l as t
wo
regi
onal
inve
stm
ents
case
s in
the
Gre
ater
Mek
ong S
ubre
gion
(GM
S), a
nd th
e w
hole
Asia
and
Pac
ific
regi
on, w
ere
com
plet
ed in
June
201
7. Ea
ch c
ase
estim
ates
the
cost
and
eco
nom
ic a
nd fi
nanc
ial r
etur
ns o
f mal
aria
elim
inat
ion
thro
ugh
2030
. Nat
iona
l and
regi
onal
pol
icym
aker
s can
use
this
evid
ence
to in
form
mal
aria
pro
gram
bud
getin
g, st
rate
gic p
lann
ing,
and
advo
cacy
for d
omes
tic re
sour
ce m
obiliz
atio
n. T
hey a
lso ai
m to
ge
nera
te e
vide
nce
arou
nd o
ptim
al w
ays t
o in
crea
se a
nd e
xpan
d th
e am
ount
of s
usta
inab
le fi
nanc
ing i
n su
ppor
t of m
alar
ia e
limin
atio
n.•
Mod
elin
g and
ingr
edie
nt a
ppro
ache
s wer
e us
ed to
cos
t mal
aria
elim
inat
ion
by 2
030.
A c
ostin
g too
l for
the
mod
elin
g app
roac
h an
d m
athe
mat
ical
tran
smiss
ion
mod
els f
or p
roje
ctin
g mal
aria
bur
den
acro
ss 2
2 co
untri
es in
Asia
and
the
Paci
fic h
ave
been
com
plet
ed. T
he c
ostin
g too
l usin
g the
ingr
edie
nt a
ppro
ach
was
impl
emen
ted
in B
angl
ades
h an
d In
done
sia.
•Th
e ec
onom
ic a
nd s
ocia
l ben
efits
of e
limin
atio
n w
ere
estim
ated
thro
ugh
the
Mal
aria
Elim
inat
ion
Tran
smiss
ion
and
Cost
ing
in th
e A
sia P
acifi
c (M
ETCA
P), a
tran
smiss
ion
mod
el c
reat
ed b
y th
e M
ahid
ol-O
xfor
d Tr
opic
al M
edic
ine
Rese
arch
Uni
t (M
ORU
), in
col
labo
ratio
n w
ith th
e M
EI a
nd th
e U
nive
rsity
of C
ape
Tow
n. It
is th
e fir
st m
ulti-
spec
ies m
odel
to b
e ex
clus
ivel
y de
velo
ped
for t
he
Asia
and
Paci
fic re
gion
. It ca
n pr
ojec
t tra
nsm
issio
n re
duct
ions
and
pred
ict e
limin
atio
n ba
sed
on a
num
ber o
f sce
nario
s. Fo
ur co
unte
rfact
ual s
cena
rios w
ere m
odel
ed, in
clud
ing o
ne b
usin
ess-
as-u
sual
sc
enar
io an
d th
ree
reve
rse
scen
ario
s tha
t sim
ulat
ed th
e po
tent
ial im
pact
of s
calin
g dow
n th
e m
alar
ia p
rogr
am. T
he si
x elim
inat
ion
scen
ario
s wer
e m
odel
ed se
quen
tially
to in
crea
se in
com
plex
ity an
d in
the
num
ber o
f int
erve
ntio
ns in
clud
ed. A
cros
s all 1
0 sc
enar
ios,
thre
e as
sum
ptio
ns ar
ound
the
likel
ihoo
d of
arte
misi
nin
resis
tanc
e w
ere
appl
ied,
the
use
of m
ass d
rug a
dmin
istra
tion
(MD
A), a
nd th
e sc
ale u
p of
LLI
Ns t
o 80
%. F
or ea
ch co
untry
, the
min
imum
scen
ario
that
wou
ld ac
hiev
e mal
aria
elim
inat
ion
was
det
erm
ined
, defi
ned
as 1 y
ear w
ith le
ss th
an o
ne re
porte
d cl
inic
al ca
se. T
hese
addi
tiona
l sc
enar
ios p
rodu
ced
a tot
al o
f 80
scen
ario
s (w
ith an
d w
ithou
t res
istan
ce; w
ith an
d w
ithou
t MD
A; a
nd w
ith an
d w
ithou
t LLI
N sc
ale
up to
80%
). In
addi
tion,
the
effec
t of i
mpr
oved
targ
etin
g of m
alar
ia
inte
rven
tions
was
sim
ulat
ed o
n co
sts b
y red
ucin
g int
erve
ntio
n co
vera
ge b
y 30%
am
ong t
he P
AR
for a
ll sce
nario
s, w
ith a
nd w
ithou
t the
resis
tanc
e an
d M
DA
ass
umpt
ions
.•
The o
utpu
ts o
f the
MET
CAP
have
bee
n tra
nsfo
rmed
into
an o
nlin
e int
erac
tive m
obile
appl
icat
ion
that
gene
rate
s gra
phs a
nd ch
arts
show
ing c
hang
es in
mal
aria
mor
bidi
ty an
d m
orta
lity a
nd as
soci
ated
pr
ogra
m c
osts
und
er th
e di
ffere
nt in
terv
entio
n sc
enar
ios.
It is
curre
ntly
in B
eta
form
, and
can
be
acce
ssed
at:
http
://w
ww.
met
capm
odel
.net
•Bu
ildin
g on
the
Sept
embe
r 201
4 fo
rum
“Opp
ortu
nitie
s for
Cor
pora
te S
ecto
r Eng
agem
ent i
n M
alar
ia C
ontro
l in
Asia
-Pac
ific”
co-
host
ed b
y A
PLM
A a
nd th
e w
HO
in th
e A
sia a
nd P
acifi
c re
gion
, th
e M
EI g
ener
ated
four
bus
ines
s cas
es o
n pr
ivat
e se
ctor
eng
agem
ent i
n m
alar
ia e
limin
atio
n on
e fo
r the
cou
ntrie
s in
the
GM
S an
d on
e fo
r Ban
glad
esh,
Indo
nesia
, and
PN
G. T
hese
bus
ines
s cas
es
asse
ss th
e m
otiv
ator
s, en
able
rs a
nd in
cent
ives
rega
rdin
g pr
ivat
e se
ctor
inve
stm
ent i
n m
alar
ia e
limin
atio
n an
d th
eir p
artic
ipat
ing
in p
ublic
-priv
ate
partn
ersh
ips.
In th
e G
MS,
pro
duct
ivity
is th
e m
ost
frequ
ently
stat
ed m
otiv
ator
for c
ompa
nies
to in
vest
in h
ealth
and
the
abse
nce
of sk
illed
wor
kers
is se
en a
s hav
ing
a m
ajor
impa
ct o
n pr
oduc
tivity
. The
mos
t com
mon
ena
bler
was
the
gove
rnm
ent
(bot
h lo
cal a
nd n
atio
nal)
prov
idin
g cl
ear i
nstru
ctio
ns o
n w
here
the
priv
ate
sect
or c
an c
ontri
bute
. In
addi
tion,
rele
vant
info
rmat
ion
on th
e ch
alle
nges
at h
and
wou
ld e
nabl
e th
e pr
ivat
e se
ctor
to
iden
tify s
olut
ions
and
reso
urce
s nee
ded.
Res
pond
ents
iden
tified
tax i
ncen
tives
and
reco
gniti
on aw
ards
as v
iabl
e in
cent
ives
to p
rom
ote
priv
ate
sect
or in
volv
emen
t in
mal
aria
elim
inat
ion.
•Th
e M
PEAT
was
dev
elop
ed b
y th
e M
EI to
hel
p m
alar
ia p
rogr
am m
anag
ers c
olle
ct, o
rgan
ize, a
nd tr
ack
data
poi
nts r
elat
ed to
the
tech
nica
l effi
cien
cy o
f a m
alar
ia p
rogr
am. M
PEAT
ena
bles
use
rs to
co
mpa
re sp
ecifi
c epi
dem
iolo
gica
l, fina
ncia
l, and
ope
ratio
nal in
dica
tors
bet
wee
n tw
o ye
ars a
nd ag
ains
t per
form
ance
targ
ets s
et b
y the
pro
gram
. The
MPE
AT h
as b
een
used
in B
angl
ades
h, In
done
sia
and
PNG
, Ban
glad
esh,
and
Indo
nesia
to id
entif
y are
as th
at n
eed
stre
ngth
enin
g, w
ith th
e ob
ject
ive
of m
axim
izing
valu
e, re
duci
ng w
aste
, and
ulti
mat
ely s
avin
g res
ourc
es.
•A
mon
g th
e effi
cien
cy a
reas
incl
uded
is p
rocu
rem
ent o
f goo
ds a
nd s
ervi
ces;
targ
etin
g of
ser
vice
s an
d in
terv
entio
ns; c
hoic
e of
bes
t val
ue/h
ighe
st im
pact
stra
tegi
es a
nd v
ertic
al v
ersu
s in
tegr
ated
pr
ogra
mm
ing;
and
colla
bora
tion
with
oth
er p
rogr
ams a
nd p
artn
ers.
•Th
e po
ssib
ility
of e
stab
lishi
ng a
regi
onal
hea
lth fu
nd fo
r add
ress
ing
the
heal
th se
curit
y th
reat
from
infe
ctio
us d
iseas
es w
as e
xplo
red.
Mal
aria
is o
ne o
f the
seve
ral i
nfec
tious
dise
ases
of c
once
rn in
th
e A
sia an
d Pa
cific
regi
on an
d po
litic
al le
ader
s and
pub
lic h
ealth
exp
erts
are
awar
e of
the
thre
at to
hea
lth se
curit
y pos
ed b
y bot
h dr
ug re
sista
nce
and
emer
ging
dise
ase
thre
ats.
The
curre
nt fi
nanc
ial
land
scap
e fo
r mal
aria
and
mal
aria
elim
inat
ion
in th
e A
sia a
nd P
acifi
c re
gion
was
exa
min
ed a
nd o
ppor
tuni
ties f
or re
sour
ce m
obiliz
atio
n, in
clud
ing a
n in
nova
tive
regi
onal
hea
lth fu
nd, w
ere
disc
usse
d.
This
fund
wou
ld p
oten
tially
fina
nce
prio
rity s
trate
gic r
egio
nal a
ctiv
ities
, pro
vide
supp
ort t
o co
untri
es in
the
regi
on w
ith th
e hi
ghes
t mal
aria
bur
den
and
leas
t cap
acity
to se
cure
dom
estic
fund
ing,
and
scal
e up
inve
stm
ents
in n
atio
nal p
rogr
ams.
A re
gion
al re
sour
ce m
obiliz
atio
n st
rate
gy w
as d
evel
oped
, whi
ch p
rovi
des a
sum
mar
y of
the
curre
nt st
ate
of re
sour
ces a
vaila
ble
for m
alar
ia e
limin
atio
n an
d re
com
men
ds ke
y opp
ortu
nitie
s to
mob
ilize
addi
tiona
l res
ourc
es fo
r nat
iona
l mal
aria
elim
inat
ion
in th
e A
sia an
d Pa
cific
regi
on. T
he re
port,
bas
ed o
n a r
egio
nal r
esou
rce
mob
ilizat
ion
fram
ewor
k, pr
ovid
es a
n ov
ervi
ew o
f dem
and
for m
alar
ia e
limin
atio
n re
sour
ces,
curre
nt su
pply
of r
esou
rces
, and
reco
mm
ends
key
opp
ortu
nitie
s to
fill t
he re
sour
ce g
ap. T
he re
sour
ce m
obiliz
atio
n fra
mew
ork
and
repo
rt in
clud
e po
litic
al c
apita
l and
the
polit
ical
env
ironm
ent f
or p
olic
y re
form
s, in
clud
ing
reco
mm
ende
d fis
cal r
efor
ms t
o in
crea
se h
ealth
fina
ncin
g. It
assu
mes
that
the
dem
and
for a
dditi
onal
re
sour
ces h
as b
een
dete
rmin
ed a
nd th
at th
e un
derly
ing
evid
ence
and
inve
stm
ent c
ase
for e
limin
atio
n ha
s bee
n de
velo
ped.
The
stra
tegy
leve
rage
s on
the
findi
ngs o
f the
inve
stm
ent c
ases
, priv
ate
sect
or b
usin
ess c
ases
, and
the
Asia
and
Pac
ific
regi
on fi
nanc
ing a
sses
smen
t, an
d ai
ms f
or a
n in
crea
se in
reso
urce
s for
elim
inat
ion
thro
ugh
to 2
030.
It o
utlin
es th
e pr
oces
ses a
nd p
riorit
y act
ions
that
ne
ed to
be
unde
rtake
n to
mob
ilize
and
sust
ain
the
nece
ssar
y res
ourc
es to
ena
ble
the
regi
on to
ach
ieve
its g
oal o
f a m
alar
ia-f
ree
Asia
and
Pac
ific
regi
on b
y 203
0.
Box c
ontin
ued
cont
inue
d on
nex
t pag
e
46 Annex
Stor
y be
hind
the
num
bers
•D
issem
inat
ion
mee
tings
on
the
inve
stm
ent c
ases
wer
e co
nduc
ted
with
mal
aria
pro
gram
s, lo
cal p
artn
ers,
and
stak
ehol
ders
in B
angl
ades
h, In
done
sia, a
nd P
NG
. The
hig
h-le
vel fi
ndin
gs o
f the
in
vest
men
t cas
es an
d re
com
men
datio
ns fr
om p
rivat
e sec
tor b
usin
ess c
ases
and
MPE
AT w
ere d
iscus
sed
at th
e Sen
ior B
udge
t Offi
cial
s mee
ting i
n To
kyo
in M
ay 20
17. P
rodu
cts f
rom
this
body
of w
ork
wer
e sha
red
with
atte
ndee
s of t
he w
HO
Stra
tegi
c Adv
isory
Gro
up in
New
Del
hi in
Nov
embe
r 201
7, an
d th
e MPE
AT w
as fe
atur
ed in
the J
oint
Sen
ior B
udge
t Offi
cial
s Net
wor
k for
Fisc
al S
usta
inab
ility
of H
ealth
Sys
tem
s for
Asia
in D
ecem
ber 2
017.
Join
t Mal
aria
wee
k fro
m D
ecem
ber 4
–8 in
Nay
Pyi
Taw
, Mya
nmar
hig
hlig
hted
this
wor
k, co
-spo
nsor
ed b
y A
PLM
A a
nd th
e A
sia a
nd P
acifi
c M
alar
ia
Elim
inat
ion
Net
wor
k (A
PMEN
). Se
vera
l ses
sions
inco
rpor
ated
the
findi
ngs,
incl
udin
g: A
PMEN
wor
ksho
p on
the
MPE
AT (4
Dec
embe
r 201
7), A
DB
Regi
onal
Mal
aria
Tru
st F
und
(5 D
ecem
ber 2
017)
, A
PLM
A S
enio
r Offi
cial
s Mee
ting
(6 D
ecem
ber 2
017)
, RA
I DG
’s m
eetin
g (7
Dec
embe
r 201
7), a
nd th
e M
inist
eria
l Mee
ting
on M
alar
ia E
limin
atio
n–G
MS
and
Chin
a (8
Dec
embe
r 201
7). T
he th
ree
natio
nal in
vest
men
t cas
es an
d tw
o re
gion
al in
vest
men
t cas
es, t
he M
ETCA
P, p
rivat
e se
ctor
bus
ines
s cas
es, a
nd th
e M
PEAT
are
all a
vaila
ble
onlin
e at
ww
w.sh
rinki
ngth
emal
aria
map
.org
and
are
bein
g sh
ared
with
key
par
tner
s. A
Q&
A w
ith B
en R
olfe
(chi
ef e
xecu
tive
office
r, A
PLM
A), S
usan
n Ro
th (
seni
or d
evel
opm
ent s
peci
alist
, AD
B), a
nd R
ima
Shre
tta (
asso
ciat
e di
rect
or o
f eco
nom
ics
and
finan
cing
, UCS
F M
EI) w
as p
rodu
ced.
Thi
s wor
k has
also
bee
n fe
atur
ed in
the
New
Yor
k Tim
es a
nd N
atur
e.
Box c
ontin
ued

Annex 47
OU
TCO
ME
2: F
INA
NCI
NG
Incr
ease
d fin
anci
ng fo
r mal
aria
elim
inat
ion
and
addr
essin
g com
mun
icab
le d
iseas
e th
reat
s
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
16Q
2 20
1820
16Q
2 20
181.
Am
ount
of A
DB
gran
ts m
ade
avai
labl
e fo
r mal
aria
elim
inat
ion
and
addr
essin
g co
mm
unic
able
dise
ase
thre
ats
$22.
0m$8
2.5m
*$8
2.5m
*$8
0.0m
1. A
DF
heal
th se
curit
y gra
nts f
or gr
oup
A
and
B co
untri
es m
obiliz
ed ($
52.5
m)
No
Yes
Yes
Yes
2. A
mou
nt o
f cou
ntry
loan
s for
m
alar
ia e
limin
atio
n an
d ad
dres
sing
com
mun
icab
le
dise
ase
thre
ats
$27.0
m$1
44.0
m*
$144
.0m
*$1
20.0
m2.
GM
S he
alth
secu
rity f
unds
ap
prov
ed (
$117
m a
s loa
n an
d $8
m
as gr
ant)
No
Yes
Yes
Yes
3. A
DB
Hea
lth B
ond
laun
ched
($
100m
OCR
)N
oN
oYe
sYe
s
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
* Cu
mul
ativ
e am
ount
AD
B =
Asia
n D
evel
opm
ent B
ank,
AD
F =
Asia
n D
evel
opm
ent F
und,
GM
S =
Gre
ater
Mek
ong S
ubre
gion
, m =
milli
on, O
CR =
ord
inar
y cap
ital r
esou
rces
.
Stor
y be
hind
the
num
bers
•Be
fore
the
deve
lopm
ent o
f the
RM
TF, A
DB
had
inve
sted
$49
milli
on in
com
mun
icab
le d
iseas
e co
ntro
l ($2
2 m
illion
as g
rant
for C
ambo
dia
and
the
Lao
PDR,
and
$27
milli
on lo
an fo
r Vie
t Nam
). U
sing
the
RMTF
fund
s, an
add
ition
al gr
ant o
f $9.
5 milli
on w
as re
leas
ed in
201
5 for
Cam
bodi
a, th
e La
o PD
R, a
nd V
iet N
am.
•Th
e RM
TF w
as c
atal
ytic
in ra
ising
add
ition
al A
DB
fund
s to
sup
port
effor
ts fo
r mal
aria
elim
inat
ion
and
addr
essin
g co
mm
unic
able
dise
ase
thre
ats.
A to
tal o
f $52
.5 m
illion
has
bee
n m
obiliz
ed fo
r hea
lth
secu
rity
mea
sure
s for
all
coun
tries
elig
ible
for t
he A
sian
Dev
elop
men
t Fun
d (A
DF)
as p
er A
DB’
s con
cess
iona
l ass
istan
ce p
olic
y. A
n ad
ditio
nal $
125
milli
on w
orth
of l
oans
and
gra
nts f
or h
ealth
secu
rity
in
GM
S co
untri
es w
as a
lso a
ppro
ved
in N
ovem
ber o
f 201
6.•
whi
le th
e ta
rget
has
bee
n m
et fo
r inc
reas
ed fi
nanc
ing,
AD
B co
ntin
ues t
o su
ppor
t fina
ncin
g m
echa
nism
s for
hea
lth, m
ost n
otab
ly th
roug
h th
e iss
uanc
e of
AD
B’s fi
rst h
ealth
bon
d. T
he b
ond
was
a p
rivat
e pl
acem
ent o
f $10
0 m
illion
issu
ed in
Mar
ch 20
17 a
nd w
ill su
ppor
t len
ding
to co
untri
es o
n ta
rget
ed h
ealth
fina
ncin
g, in
clud
ing m
alar
ia a
nd co
mm
unic
able
dise
ase
prog
ram
s. A
DB
will
cont
inue
to su
ppor
t the
bo
nd p
ipel
ine
proc
ess f
or p
oten
tial s
ubse
quen
t iss
ues.
The
AD
B he
alth
bon
d pr
ivat
e pl
acem
ent i
s a fi
rst o
f its
kind
, bot
h re
gion
ally
and
glob
ally.
AD
B is
asse
ssin
g the
pot
entia
l for
a fu
rther
AD
B he
alth
bon
d iss
uanc
e in
201
8, p
endi
ng a
suita
ble
heal
th p
roje
ct p
ipel
ine.
•A
DB
also
dev
elop
ed a
publ
ic–p
rivat
e pa
rtner
ship
s (PP
Ps) i
nves
tmen
t brie
f for
the
heal
th se
ctor
to p
rom
ote
incr
ease
d su
ppor
t for
hea
lth P
PPs i
nclu
ding
thos
e se
rvic
es th
at co
uld
bene
fit m
alar
ia e
limin
atio
n an
d co
mm
unic
able
dise
ases
. The
hea
lth P
PP b
rief i
nclu
ded
a de
taile
d re
view
of t
he b
road
er h
ealth
sys
tem
s st
reng
then
ing
ecos
yste
m re
quire
d to
sup
port
succ
essf
ul P
PPs,
incl
udin
g le
sson
s fro
m o
ther
se
ctor
s and
pro
gram
s on
build
ing s
ucce
ssfu
l PPP
pro
gram
s.•
In D
ecem
ber 2
017,
AD
B sig
ned
a m
emor
andu
m o
f und
erst
andi
ng (M
OU
) with
the
Glo
bal F
und
(GF)
, the
firs
t of i
ts k
ind
betw
een
the
GF
and
a de
velo
pmen
t ban
k. Th
e M
OU
is d
esig
ned
to (i
) pro
mot
e in
stitu
tiona
l coo
rdin
atio
n, (i
i) de
velo
p a
proj
ect p
ipel
ine
targ
etin
g hea
lth sy
stem
s dev
elop
men
t and
stre
ngth
enin
g for
mal
aria
, TB
and
HIV
and
AID
S el
imin
atio
n an
d co
ntro
l, and
(iii)
supp
ort g
over
nmen
ts’
trans
ition
al fi
nanc
e. T
he M
OU
was
dev
elop
ed in
coor
dina
tion
with
AD
B’s O
ffice
of C
ofina
ncin
g Ope
ratio
ns (O
CO),
the
Hea
lth S
ecto
r Gro
up, r
egio
nal d
epar
tmen
ts, a
nd th
e G
F re
gion
al te
ams.
The
MO
U
proc
ess a
llow
ed A
DB
and
the
GF
to d
iscus
s det
aile
d fin
anci
ng a
nd co
llabo
ratio
n m
odal
ities
, incl
udin
g res
ults
and
inpu
ts-b
ased
gran
t fina
ncin
g, an
d bl
ende
d fin
anci
ng m
odal
ities
bas
ed o
n pa
ralle
l and
join
t co
finan
cing
. Sin
ce th
e M
OU
sign
ing,
the
focu
s has
bee
n on
iden
tifyi
ng a
nd a
sses
sing
cofin
anci
ng o
ppor
tuni
ties.
The
inno
vativ
e fin
ance
con
sulta
nt h
as b
een
wor
king
with
AD
B re
gion
al d
epar
tmen
ts a
nd
the
GF
to fa
cilit
ate
proj
ect m
appi
ng a
nd c
ofina
ncin
g—a
proj
ect t
hat e
ncom
pass
es m
alar
ia a
nd o
ther
com
mun
icab
le d
iseas
es fo
r Bhu
tan,
PN
G, a
nd S
ri La
nka,
as w
ell a
s the
GM
S co
untri
es. P
relim
inar
y di
scus
sions
wer
e al
so h
eld
to su
ppor
t the
GF
and
Paci
fic Is
land
nat
ions
disc
uss a
pro
cure
men
t sys
tem
to su
ppor
t nat
iona
l pur
chas
ing a
nd p
rice
effec
tiven
ess.
cont
inue
d on
nex
t pag
e

48 Annex
Stor
y be
hind
the
num
bers
•Fr
om Ja
nuar
y 20
18 to
June
201
8 ke
y pa
rtner
wor
ksho
p an
d co
llabo
ratio
n m
eetin
gs (n
ot fi
nanc
ed u
nder
the
RMTF
) wer
e he
ld in
Gen
eva
(OCO
, GF
Mar
ch 2
018)
, Sin
gapo
re (A
DB
SDCC
, OCO
, reg
iona
l de
partm
ents
, and
GF
coun
terp
arts
and
APL
MA
dur
ing A
pril 2
018)
, and
Mel
bour
ne (w
orld
Mal
aria
Con
gres
s, Ju
ly 2
018)
. Dur
ing t
hese
mee
tings
the
follo
win
g wer
e ac
hiev
ed:
»D
evel
opm
ent o
f a d
etai
led
conc
ept n
ote
high
light
ing c
olla
bora
tion
fram
ewor
ks, o
utlin
es o
f inn
ovat
ive
finan
cing
pilo
ts fo
r five
coun
tries
bet
wee
n G
F an
d A
DB,
dra
ft fra
mew
ork a
gree
men
ts, t
he “R
egio
nal
Fina
ncin
g Fa
cilit
y” p
relim
inar
y de
sign
pitc
h bo
ok, a
dra
ft m
onito
ring
and
eval
uatio
n (M
&E)
fram
ewor
k, an
d de
taile
d m
eetin
g, w
orks
hop
and
pane
l pre
sent
atio
ns a
nd m
ater
ials
to s
uppo
rt pa
rtner
di
scus
sions
;»
Go-
ahea
d by
par
tner
s (A
PLM
A, G
F to
dat
e, p
endi
ng c
onfir
mat
ion
of in
volv
emen
t bet
wee
n th
ree
mor
e pa
rtner
s) to
faci
litat
e de
taile
d fu
nd d
esig
n in
clud
ing a
con
cret
e pr
ojec
t pip
elin
e of
col
labo
ratio
n/co
finan
cing
that
supp
orts
hea
lth se
ctor
dev
elop
men
t inc
ludi
ng m
alar
ia a
nd o
ther
com
mun
icab
le d
iseas
es;
»So
cial
izatio
n of
the
prop
osed
regi
onal
fina
ncin
g fac
ility t
o br
oade
r sta
keho
lder
s inc
ludi
ng w
orld
Ban
k, w
HO
, aca
dem
ia, a
nd b
ilate
ral;
»Fo
rmal
izing
a kn
owle
dge
shar
ing n
etw
ork b
etw
een
AD
B O
CO, S
DCC
, APL
MA
and
the
Inte
r-A
mer
ican
Dev
elop
men
t Ban
k on
expe
rienc
es w
ith m
ultid
onor
faci
litie
s to
supp
ort m
alar
ia an
d ot
her h
ealth
in
nova
tive
finan
cing
mec
hani
sms;
and
»Fa
cilit
atin
g di
scus
sions
bet
wee
n G
F an
d pa
rtner
s, an
d A
DB
regi
onal
dep
artm
ent s
taff
to d
iscus
s in
tegr
atio
n of
cofi
nanc
ing
or p
aral
lel fi
nanc
ing
on p
roje
cts
in B
angl
ades
h, B
huta
n, S
ri La
nka,
PN
G,
Solo
mon
Isla
nds a
nd th
e La
o PD
R.
Box c
ontin
ued

Annex 49
OU
TCO
ME
3: M
EDIC
INES
Impr
oved
regu
lato
ry c
apac
ity to
supp
ort i
ncre
ased
avai
labi
lity a
nd u
se o
f qua
lity-
assu
red
heal
th p
rodu
cts f
or m
alar
ia a
nd o
ther
com
mun
icab
le d
iseas
es
Out
com
e 3.
1 Im
prov
ed o
pera
tiona
l cap
acity
of n
atio
nal r
egul
ator
y age
ncie
s (N
RAs)
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
16Q
2 20
1820
16Q
2 20
18
1. N
umbe
r of c
ount
ries w
ith im
prov
ed
oper
atio
nal r
egul
ator
y cap
acity
00
3*3
1. N
umbe
r of c
ount
ries w
ith N
RA
capa
city
pro
files
(CA
M, L
AO, M
YA,
THA
, VIE
)
03
55
2. N
umbe
r of c
ount
ries w
ith N
RA
capa
city
stre
ngth
enin
g roa
d m
aps
(CA
M, L
AO, M
YA, T
HA
, VIE
)
00
55
3. T
rain
ing m
odul
es d
evel
oped
No
No
Yes
Yes
4. N
umbe
r of c
ount
ries w
ith N
RA st
aff
train
ed o
n pr
iorit
y reg
ulat
ory i
ssue
s an
d ga
ps
00
55
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
CAM
= C
ambo
dia,
LAO
= L
ao P
eopl
e’s D
emoc
ratic
Rep
ublic
, MYA
= M
yanm
ar, T
HA
= T
haila
nd, V
IE =
Vie
t Nam
.* C
ambo
dia,
the
Lao
PDR,
and
Mya
nmar
bui
lt ca
paci
ty b
ased
on
the
Cent
re o
f Reg
ulat
ory E
xcel
lenc
e (C
oRE)
nee
ds a
sses
smen
t, w
hich
hel
ped
iden
tify a
reas
of f
ocus
and
impr
ove
partn
er c
oord
inat
ion.
The
tra
inin
gs c
ondu
cted
for c
ount
ry re
pres
enta
tives
and
the
road
map
dev
elop
ed a
ll enc
apsu
late
cap
acity
bui
ldin
g. A
dditi
onal
ly, th
e ta
rget
ed te
chni
cal s
uppo
rt an
d w
ork i
n M
yanm
ar h
ad a
dire
ct im
pact
on
the
oper
atio
nal c
apac
ity o
f its
Foo
d an
d D
rug A
dmin
istra
tion
and
addi
tiona
l act
iviti
es a
ddre
ssin
g tar
gete
d m
onito
r-in
g of t
he q
ualit
y of m
edic
ines
on
the
mar
ket,
linki
ng th
e qu
ality
con
trol la
bora
tory
into
the
elec
troni
c in
form
atio
n sy
stem
and
dev
elop
ing t
he b
asis
of a
nat
iona
l dru
g saf
ety s
trate
gy a
nd p
harm
acov
igila
nce
syst
em.
Stor
y be
hind
the
num
bers
•w
ith A
DB
supp
ort,
the
CoRE
, a re
gion
al c
apac
ity b
uild
ing
cent
er a
nd p
artn
er-c
oord
inat
ing
plat
form
for r
egul
ator
y sy
stem
s st
reng
then
ing
and
conv
erge
nce
for S
outh
east
Asia
n de
velo
ping
mem
ber
coun
tries
, was
est
ablis
hed
in c
olla
bora
tion
with
the
Gov
ernm
ent o
f Sin
gapo
re (w
hich
pro
vide
d $1
0 m
illion
in c
ofina
ncin
g), D
uke-
NU
S, w
HO
, Uni
ted
Stat
es P
harm
acop
eia
(USP
) and
oth
er p
artn
ers.
•Bu
ildin
g on
the
wH
O p
rofil
ing t
ool, a
mor
e pr
actic
al re
gula
tory
syst
em p
rofil
ing i
nstru
men
t (RS
PI) t
o as
sess
NRA
capa
bilit
y, es
peci
ally
rela
ted
to re
gula
ting a
nti-m
alar
ias a
nd o
ther
com
mun
icab
le d
iseas
es
med
icin
e, h
as b
een
deve
lope
d an
d ca
paci
ty ga
p an
alys
is ha
s bee
n co
nduc
ted
by C
oRE
for t
he N
RAs i
n Ca
mbo
dia,
the
Lao
PDR,
Mya
nmar
, Tha
iland
, and
Vie
t Nam
.•
Base
d on
the
capa
city
pro
files
, prio
rity t
rain
ing n
eeds
wer
e id
entifi
ed in
the
area
s of f
ound
atio
ns a
nd p
roce
sses
of r
egul
ator
y pra
ctic
e, p
ost-
mar
ket s
urve
illanc
e an
d m
edic
al d
evic
e re
gula
tion.
•Co
urse
curri
cula
and
train
ing m
ater
ials
wer
e dev
elop
ed fo
r pha
rmac
ovig
ilanc
e, m
edic
al d
evic
e reg
ulat
ion,
and
good
regu
lato
ry p
ract
ice.
Tra
inin
gs in
the L
ao P
DR
and
Cam
bodi
a on
phar
mac
ovig
ilanc
e wer
e co
nduc
ted
in A
ugus
t 201
7 an
d tra
inin
g on
med
ical
dev
ices
was
con
duct
ed in
Cam
bodi
a in
Nov
embe
r 201
7.•
Coun
try c
apac
ity b
uild
ing
road
map
s wer
e de
velo
ped,
disc
usse
d w
ith th
e N
RAs a
nd fi
naliz
ed. I
n ad
ditio
n, a
regi
onal
dev
elop
men
t roa
d m
ap, w
hich
info
rms t
he A
ssoc
iatio
n of
Sou
thea
st A
sian
Nat
ions
(A
SEA
N) p
roce
ss o
f con
verg
ing r
egul
ator
y pra
ctic
es, w
as p
repa
red.
•Co
RE h
as b
een
parti
cipa
ting
in th
e Re
gion
al R
egul
ator
y Pa
rtner
ship
(w
hich
focu
ses
on re
gula
tion
of a
ntim
alar
ials)
, whi
ch h
as s
een
its c
apac
ity g
ap a
nalys
es in
tegr
ated
into
the
natio
nal w
ork
plan
s de
velo
ped
by th
e pa
rtner
ship
.•
CoRE
has
con
duct
ed a
dditi
onal
trai
ning
ses
sions
in S
inga
pore
on
regu
lato
ry p
ract
ices
as
part
of it
s re
gula
r act
iviti
es. R
egul
ator
s fro
m V
iet N
am a
nd T
haila
nd h
ave
atte
nded
som
e of
thes
e se
ssio
ns to
ad
dres
s ide
ntifi
ed c
apac
ity is
sues
usin
g the
ir ow
n fu
ndin
g.•
The
key a
chie
vem
ent h
as b
een
the
deve
lopm
ent o
f cap
acity
dev
elop
men
t pla
ns th
at w
ill su
ppor
t the
har
mon
izatio
n of
regu
lato
ry st
reng
then
ing e
fforts
by p
artn
ers a
nd a
coh
eren
t app
roac
h fa
cilit
ated
by
CoRE
.
cont
inue
d on
nex
t pag
e

50 Annex
Stor
y be
hind
the
num
bers
•Th
e su
cces
s for
impl
emen
ting p
lans
for r
egul
ator
y cap
acity
bui
ldin
g lar
gely
dep
ends
on
the
conv
ictio
n of
the
NRA
on
the
need
for s
yste
ms s
treng
then
ing,
coup
led
with
a cl
arity
on
how
this
prog
ress
can
be
achi
eved
. The
RSP
I was
dev
elop
ed to
iden
tify g
aps i
n th
e reg
ulat
ory s
yste
ms,
so th
at w
ith th
e res
olut
ion
of th
ese g
aps,
the r
egul
ator
y cap
acity
of t
he N
RA ca
n be
bro
ught
to th
e nex
t lev
el to
mee
t the
nee
ds
of th
e he
alth
care
syst
em. T
he fi
ndin
gs fr
om R
SPI a
re in
corp
orat
ed w
ith in
puts
from
ext
erna
l reg
ulat
ory s
take
hold
ers e
.g., in
dust
ry a
ssoc
iatio
n, p
harm
acy a
ssoc
iatio
ns, t
o ac
hiev
e a
degr
ee o
f val
idat
ion
and
trian
gula
tion,
and
cove
rs fr
om o
rgan
izatio
nal s
truct
ure,
gove
rnan
ce, a
nd h
uman
reso
urce
s to
the
key r
egul
ator
y fun
ctio
ns. T
he N
RAs w
ere
prov
ided
with
thei
r ind
ivid
ual c
ount
ry as
sess
men
t rep
orts
on
the
gaps
in th
eir r
egul
ator
y sys
tem
s, as
wel
l as a
road
map
on
the
reco
mm
ende
d ac
tions
to h
elp
stre
ngth
en th
eir s
yste
ms.
Thes
e do
cum
ents
pro
vide
the
nece
ssar
y inf
orm
atio
n an
d pr
actic
al re
com
men
datio
ns
to h
elp
the N
RAs p
riorit
ize th
eir s
teps
in b
uild
ing r
egul
ator
y cap
acity
and
faci
litat
e tim
ely a
cces
s to
qual
ity h
ealth
pro
duct
s. Re
gula
tory
grow
th an
d pr
ogre
ss, a
s of a
ny ch
ange
s in
a lar
ge an
d co
mpl
ex sy
stem
, is
chal
leng
ing t
o m
easu
re. A
long
itudi
nal s
tudy
is re
quire
d ov
er a
few
year
s to
capt
ure
the
impa
ct o
f int
erve
ntio
ns fo
r reg
ulat
ory s
yste
ms s
treng
then
ing.
It sh
ould
also
be
note
d th
at su
ch gr
owth
dep
ends
on
the
polit
ical
, soc
ial, a
nd c
ultu
ral in
fluen
ces,
and
ther
efor
e a
mul
tipro
nged
app
roac
h w
ould
be
requ
ired.
Effo
rts to
pur
sue
such
an
appr
oach
wou
ld re
quire
subs
tant
ial in
vest
men
t and
com
mitm
ent.
•In
vie
w o
f the
mul
tiple
org
aniza
tions
that
are
cur
rent
ly a
ssist
ing
the
NRA
s in
regu
lato
ry c
apac
ity b
uild
ing,
ther
e is
a ne
ed to
coo
rdin
ate
thes
e tra
inin
g ac
tiviti
es w
ith th
e pr
imar
y go
al to
incr
ease
the
effici
ent a
nd e
ffect
ive
use
of re
sour
ces.
Aga
in, s
uch
coor
dina
tion
wou
ld re
quire
cla
rity
on th
e ne
eds o
f the
var
ious
NRA
s. Th
e as
sess
men
t rep
orts
from
the
AD
B-Co
RE p
roje
ct w
ere
shar
ed (u
nder
term
s of
confi
dent
ialit
y with
the
resp
ectiv
e N
RAs)
with
vario
us p
artn
ers a
t the
regi
onal
pla
tform
, incl
udin
g wH
O, A
PLM
A, a
nd T
hera
peut
ic G
oods
Adm
inist
ratio
n. In
addi
tion,
the
info
rmat
ion
from
the
coun
try
road
map
s fo
r reg
ulat
ory
syst
ems
stre
ngth
enin
g of
the
NRA
s in
the
GM
S w
ere
utiliz
ed a
nd c
ontri
bute
d to
the
deve
lopm
ent o
f a re
gion
al w
ork
plan
for r
egul
ator
y sy
stem
s st
reng
then
ing.
Thro
ugh
this
wor
k pl
an, t
echn
ical
par
tner
s can
indi
cate
the
area
s of c
omm
itmen
t in
regu
lato
ry tr
aini
ng, w
hich
has
to m
ove
way
from
a si
lo-e
d, d
iseas
e-sp
ecifi
c ap
proa
ch. T
his i
nitia
tive
forti
fies t
he e
ffort
for p
artn
er
enga
gem
ent a
nd su
ppor
ts m
easu
res f
or su
stai
nabi
lity o
f effo
rts in
the
GM
S.
Box c
ontin
ued

Annex 51
Out
com
e 3.
2 Im
prov
ed p
ost-
mar
ket s
urve
illan
ce o
f med
icin
es fo
r mal
aria
and
oth
er c
omm
unic
able
dise
ases
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
16Q
2 20
1820
16Q
2 20
181.
Num
ber o
f cou
ntrie
s pilo
ting n
ew fi
eld
dete
ctio
n to
ols
00
11
SF fi
eld
dete
ctio
n to
ols
1. Fo
rmal
rela
tions
hips
with
glob
al a
nd
loca
l res
earc
h in
stitu
tions
est
ablis
hed
No
Yes
Yes
Yes
2. L
ibra
ry o
f act
ive
ingr
edie
nts a
nd
finish
ed p
rodu
ct p
rofil
es d
evel
oped
N
oN
oYe
sYe
s
3. R
epor
t on
resu
lts o
f tes
ting a
nd
cost
-effe
ctiv
enes
s eva
luat
ion
of fi
eld
dete
ctio
n to
ols
No
No
Yes
Yes
4. R
ecom
men
datio
ns o
n co
st-e
ffect
ive
post
-mar
ket s
urve
illanc
e fie
ld to
ols f
or
dete
ctin
g SF
deve
lope
d
No
No
Yes
Yes
2. N
umbe
r of w
PRO
and
SEA
RO
coun
tries
star
ted
to re
port
to th
e gl
obal
su
bsta
ndar
d an
d fa
lsifie
d (S
F) m
edic
al
prod
ucts
repo
rting
mec
hani
sm*
06
105
SF re
porti
ng
1. N
umbe
r of c
ount
ries w
ith st
aff tr
aine
d on
the
wH
O gl
obal
SF
repo
rting
m
echa
nism
022
2222
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
* wH
O d
oes n
ot d
ivul
ge in
form
atio
n on
repo
rting
by i
ndiv
idua
l cou
ntrie
s due
to c
onfid
entia
lity r
ules
.
Stor
y be
hind
the
num
bers
•A
DB
esta
blish
ed fo
rmal
rela
tions
hips
with
glob
al an
d lo
cal r
esea
rch
inst
itutio
ns w
ith e
xper
tise
in m
alar
ia re
sista
nce
and
qual
ity m
edic
ines
for i
mpr
ovin
g evi
denc
e on
use
of p
ost-
mar
ket s
urve
illanc
e to
ols f
or q
ualit
y te
stin
g of
ant
i-mal
aria
ls. A
lite
ratu
re su
rvey
of c
urre
nt te
chno
logi
es w
as c
ompl
eted
and
11 m
edic
ine-
qual
ity fi
eld
dete
ctio
n de
vice
s wer
e id
entifi
ed fo
r ass
essm
ent.
Thei
r lib
rarie
s w
ere
deve
lope
d w
here
nec
essa
ry a
nd p
aram
eter
s ass
esse
d in
pre
para
tion
for t
he fi
eld
eval
uatio
n in
a m
ock p
harm
acy.
•Th
e m
ock p
harm
acy h
as b
een
esta
blish
ed an
d th
e de
vice
s shi
pped
to th
e La
o PD
R fo
r fiel
d te
stin
g. Th
e La
o PD
R N
RA in
spec
tors
wer
e tra
ined
on
the
oper
atio
n of
the
devi
ces,
and
field
test
ing w
ith
the
Lao
NRA
was
com
plet
ed b
y the
end
of D
ecem
ber 2
017.
An
asse
ssm
ent o
f the
cost
-effe
ctiv
enes
s of t
he d
evic
es an
d an
anal
ysis
of th
eir p
erfo
rman
ce h
as b
een
com
plet
ed an
d a m
ultis
take
hold
er
mee
ting,
incl
udin
g re
gula
tors
and
insp
ecto
rs fr
om G
MS
NRA
s, to
disc
uss t
he re
sults
and
the
impl
icat
ions
for t
he u
se o
f sel
ecte
d de
vice
s in
prac
tice,
was
hel
d in
Apr
il 20
18. T
he v
iew
s fro
m th
e w
orks
hop
wer
e in
corp
orat
ed in
to th
e fin
al re
port.
•Tr
aini
ng o
n SF
med
icin
es re
porti
ng in
to th
e wH
O gl
obal
surv
eilla
nce m
echa
nism
was
cond
ucte
d jo
intly
by w
HO
and
USP
with
AD
B su
ppor
t. SF
repo
rting
is la
ggin
g in
the A
sia an
d Pa
cific
coun
tries
. Th
eref
ore,
all w
HO
/Reg
iona
l Offi
ce fo
r the
wes
tern
Pac
ific
(wPR
O) a
nd w
HO
/Sou
thea
st A
sia D
epar
tmen
t (SE
ARO
) cou
ntrie
s wer
e ta
rget
ed b
eyon
d th
ose
in th
e G
MS.
•To
supp
ort G
MS
coun
tries
dire
ctly
and
fost
er cr
oss-
bord
er co
llabo
ratio
n, a
high
-leve
l mee
ting w
ith h
eads
of N
RAs f
ollo
wed
by a
han
ds-o
n tra
inin
g wor
ksho
p w
as ar
rang
ed in
conj
unct
ion
with
wH
O
(Apr
il 201
7). A
nat
iona
l wor
ksho
p on
Stra
tegi
es to
Com
bat S
ubst
anda
rd an
d Fa
lsifie
d M
edic
al P
rodu
cts w
as th
en h
eld
in M
yanm
ar (N
ovem
ber 2
017)
in w
hich
a na
tiona
l coo
rdin
atio
n m
echa
nism
to
com
bat S
F m
edic
al p
rodu
cts w
as d
iscus
sed
and
adop
ted.
Thi
s was
follo
wed
by a
nat
iona
l tra
inin
g wor
ksho
p fo
r Mya
nmar
Food
and
Dru
g Adm
inist
ratio
n (F
DA)
insp
ecto
rs o
n ho
w to
pre
vent
, det
ect
and
resp
ond
to S
F m
edic
al p
rodu
cts.
wH
O w
ill pr
ovid
e fu
rther
follo
w-u
p in
201
8 as
wel
l as l
ook t
o fu
rther
nat
iona
l wor
ksho
ps.
•A
cons
ulta
nt w
as e
ngag
ed to
assis
t the
Mya
nmar
FD
A d
evel
op an
SF
actio
n pl
an (a
nd im
plem
ent a
nti-m
alar
ial s
peci
fic re
com
men
datio
ns) a
nd im
plem
enta
tion
of ca
paci
ty-s
treng
then
ing a
ctiv
ities
. ke
y in
form
atio
n re
sour
ces w
ere
prov
ided
to th
e FD
A, a
com
pute
rized
inte
grat
ed re
gist
ratio
n an
d in
form
atio
n sy
stem
wer
e im
plem
ente
d w
hich
, fol
low
ing
train
ing
of re
gula
tors
and
app
lican
ts in
N
ovem
ber 2
017,
was
fully
ope
ratio
nal b
y Fe
brua
ry 2
018.
Tec
hnic
al su
ppor
t was
also
pro
vide
d to
the
Mya
nmar
FD
A in
dev
elop
ing
a dr
aft m
echa
nism
for r
espo
ndin
g to
SF
med
ical
pro
duct
s and
or
gani
zing a
nat
iona
l wor
ksho
p to
disc
uss t
his,
follo
wed
by a
trai
ning
wor
ksho
p fo
r NRA
insp
ecto
rs o
n SF
med
ical
pro
duct
s with
inpu
t fro
m w
HO
and
USP
(Nov
201
7).
cont
inue
d on
nex
t pag
e

52 Annex
Stor
y be
hind
the
num
bers
•A
dditi
onal
ly, th
e qu
ality
con
trol l
abor
ator
y w
as li
nked
into
the
elec
troni
c in
form
atio
n sy
stem
and
a m
odul
e fo
r com
pany
regi
stra
tions
to b
e m
anag
ed th
roug
h th
e el
ectro
nic
info
rmat
ion
syst
em
deve
lope
d. P
rovi
ncia
l ins
pect
ors w
ere
prov
ided
with
tabl
ets b
y w
hich
they
cou
ld a
cces
s the
cen
tral d
atab
ase
in re
al-t
ime
to c
heck
regi
stra
tion
stat
us a
nd p
rodu
ct c
hara
cter
istic
s as w
ell a
s sub
mit
thei
r rep
orts
. Cur
rent
ly re
gist
ered
med
icin
es w
ere
asse
ssed
for p
atie
nt sa
fety
risk
s and
a n
atio
nal d
rug s
afet
y stra
tegy
and
pha
rmac
ovig
ilanc
e sy
stem
pro
pose
d fo
r im
plem
enta
tion.
•Th
e M
yanm
ar F
DA
has
bee
n su
ppor
ted
in m
oves
that
pro
mot
e gr
eate
r reg
ulat
ory
harm
oniza
tion
and
conv
erge
nce
havi
ng jo
ined
the
wH
O C
olla
bora
tive
Regi
stra
tion
Sche
me,
par
ticip
ated
in th
e A
SEA
N Jo
int A
sses
smen
t Pro
cedu
re fo
r reg
istra
tion
of m
edic
al p
rodu
cts a
nd jo
ined
the
Upp
sala
Mon
itorin
g Ce
ntre
(a w
HO
col
labo
ratin
g ce
nter
on
phar
mac
ovig
ilanc
e) a
s an
asso
ciat
e m
embe
r. Th
e M
yanm
ar F
DA
has
also
par
ticip
ated
in th
e A
sia–P
acifi
c Re
gion
al R
egul
ator
y Par
tner
ship
.
Box c
ontin
ued

Annex 53
OU
TCO
ME
4: IN
FORM
ATIO
N S
YSTE
MS
Incr
ease
d us
e of
qua
lity d
ata,
info
rmat
ion
tool
s, an
d te
chno
logi
es to
impr
ove
mal
aria
and
oth
er c
omm
unic
able
dise
ase
in
form
atio
n sy
stem
s
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
16Q
1 201
820
16Q
1 201
81.
Num
ber o
f ICT
solu
tions
in u
se in
m
alar
ia a
nd o
ther
com
mun
icab
le
dise
ase
info
rmat
ion
syst
ems t
o im
prov
e an
d ha
rmon
ize in
form
atio
n m
anag
emen
t in
GM
S co
untri
es
00
3**
21.
Surv
eilla
nce
mec
hani
sms f
or m
alar
ia
and
com
mun
icab
le d
iseas
es m
appe
d fo
r G
MS
coun
tries
No
Yes
Yes
Yes
2. R
ecom
men
datio
ns o
n tw
o IC
T so
lutio
ns to
be
used
in th
e re
gion
No
Yes
Yes
Yes
3. N
umbe
r of I
CT so
lutio
ns te
sted
in G
MS
coun
tries
0
05*
2
2. N
umbe
r of c
ount
ries u
tilizi
ng
harm
onize
d ge
o-en
able
d m
alar
ia a
nd
deng
ue in
form
atio
n sy
stem
s
00
33
1. N
umbe
r of c
ount
ries w
ith p
reva
lenc
e an
d in
cide
nce
data
for m
alar
ia a
nd
deng
ue a
naly
zed
01
33
2. N
umbe
r of c
ount
ries w
ith d
evel
oped
ca
paci
ty o
f gov
ernm
ent p
ublic
hea
lth
expe
rts fo
r app
licat
ion
of G
IS-b
ased
vi
sual
izatio
n
01
33
3. N
umbe
r of c
ount
ries w
ith G
IS-b
ased
vi
sual
izatio
n sy
stem
of m
alar
ia a
nd
deng
ue in
cide
nce
and
risk e
stab
lishe
d an
d m
etho
dolo
gy e
valu
ated
00
33
4. N
umbe
r of c
ount
ries w
ith p
olic
y re
com
men
datio
ns fo
r tar
getin
g mob
ile
popu
latio
ns in
mal
aria
and
den
gue
surv
eilla
nce
and
cont
rol p
rogr
ams
com
mun
icat
ed to
Min
istrie
s of
Hea
lth**
*
00
03
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
C
ontin
ued
until
Q4
2018
thro
ugh
addi
tiona
l fun
ding
for t
he w
ork
GM
S =
Gre
ater
Mek
ong S
ubre
gion
, GIS
= ge
ogra
phic
info
rmat
ion
syst
em, I
CT =
info
rmat
ion
and
com
mun
icat
ion
tech
nolo
gy.
* Uni
que
Hea
lth ID
in C
ambo
dia;
GIS
pla
tform
in C
ambo
dia,
Mya
nmar
, and
Vie
t Nam
; com
mon
geo-
regi
stry
in C
ambo
dia
and
Mya
nmar
; Dise
ase
surv
eilla
nce
syst
em (e
CDS
v2) i
n Vi
et N
am; H
L7 a
nd
Fast
Hea
lthca
re In
tero
pera
bilit
y Res
ourc
es (F
HIR
) in
Viet
Nam
.**
GIS
pla
tform
, com
mon
geo-
regi
stry
and
eCD
S v2
.**
*Pol
icy r
ecom
men
datio
ns a
re b
eing
dev
elop
ed c
urre
ntly
and
will
be fi
naliz
ed a
s pop
ulat
ion
mov
emen
t res
ults
are
shar
ed a
nd d
iscus
sed
with
min
istry
of h
ealth
(MO
H) s
taff.
Add
ition
al fu
ndin
g sup
-po
rt ha
s bee
n se
cure
d by
MO
RU to
com
plet
e th
is w
ork.

54 Annex
Stor
y be
hind
the
num
bers
•A
nalys
is of
exis
ting s
urve
illanc
e sy
stem
s in
Cam
bodi
a, th
e La
o PD
R, M
yanm
ar, a
nd V
iet N
am h
ighl
ight
ed th
e ne
ed to
mai
nstre
am a
nd h
arm
onize
exis
ting m
alar
ia a
nd o
ther
com
mun
icab
le d
iseas
e in
form
atio
n sy
stem
into
the
rout
ine
heal
th m
anag
emen
t inf
orm
atio
n sy
stem
(HM
IS) t
o ov
erco
me
fragm
enta
tion
of su
rvei
llanc
e sy
stem
s and
to a
llow
surv
eilla
nce
for m
alar
ia e
limin
atio
n (is
sue
brie
f pub
lishe
d). T
he an
alys
is re
com
men
ds th
e us
e of
uni
que
patie
nt h
ealth
iden
tifier
s to
help
conn
ect t
he va
rious
verti
cal d
iseas
e m
anag
emen
t pro
gram
s, su
ch as
mal
aria
, to
enab
le b
ette
r del
iver
y of
car
e an
d en
sure
trea
tmen
t cou
rses
for m
alar
ia a
re b
eing
com
plet
ed. A
tool
for u
niqu
e pa
tient
ID a
sses
smen
t was
dev
elop
ed a
nd a
pplie
d in
Cam
bodi
a, th
e La
o PD
R, M
yanm
ar, a
nd V
iet N
am.
Polic
y re
com
men
datio
ns fr
om a
brie
f on
uniq
ue p
atie
nt h
ealth
IDs i
nfor
med
Cam
bodi
a’s n
atio
nal p
atie
nt id
entifi
catio
n (I
D) m
anag
emen
t stra
tegy
and
the
resp
ectiv
e im
plem
enta
tion
plan
. The
se
polic
y re
com
men
datio
ns a
re a
lso d
issem
inat
ed th
roug
h th
e A
sia e
Hea
lth In
form
atio
n N
etw
ork,
a pe
er-t
o-pe
er le
arni
ng p
latfo
rm fo
r gov
ernm
ent e
xper
ts. A
s som
e co
untri
es m
ove
to e
lect
roni
c he
alth
reco
rds (
EHR)
, and
aut
omat
ed re
porti
ng in
to v
ertic
al d
iseas
es in
form
atio
n sy
stem
s thr
ough
EH
Rs, g
over
nmen
t-m
anda
ted
natio
nal I
Ds w
ill be
util
ized
with
linka
ges t
o ot
her s
yste
ms (
such
as
soci
al se
curit
y). F
or V
iet N
am, a
sing
le E
HR
syst
em is
cur
rent
ly b
eing
dev
elop
ed a
nd w
ill be
pilo
ted
in 2
019.
The
find
ings
from
Vie
t Nam
’s ID
and
man
agem
ent i
nfor
mat
ion
syst
ems s
tock
-tak
ing
wer
e di
ssem
inat
ed d
urin
g an
EHR
wor
ksho
p in
Feb
ruar
y 201
8. P
oten
tial u
sage
of a
uni
que
heal
th ID
was
inco
rpor
ated
into
the
exec
utiv
e su
mm
ary f
or M
OH
. The
Vie
t Nam
gove
rnm
ent d
ecid
ed to
us
e its
Soc
ial S
ecur
ity (V
SS) n
umbe
r as t
he u
niqu
e nu
mbe
r for
linki
ng va
rious
pat
ient
regi
stra
tion
syst
ems.
Pote
ntia
l nex
t ste
ps o
n ho
w to
use
the
VSS
num
ber a
s an
enab
ler f
or in
tero
pera
bilit
y wer
e in
trodu
ced
in a
n el
ectro
nic
med
ical
reco
rds w
orks
hop
and
in te
chni
cal m
eetin
gs w
ith M
OH
. In
June
201
8, a
wor
ksho
p w
as h
eld
for M
OH
EH
A a
nd p
rivat
e se
ctor
hea
lth in
form
atio
n sy
stem
s (H
IS)
solu
tion
prov
ider
s on
best
pra
ctic
e in
iden
tity m
anag
emen
t and
mas
ter p
atie
nt in
dex.
•A
s co
untri
es b
ecom
e m
ore
awar
e of
the
impo
rtanc
e of
link
ing
thei
r exis
ting
data
silo
s w
ithin
the
heal
th s
ecto
r, an
d as
they
hav
e to
rely
on
rout
ine
info
rmat
ion
syst
ems
whe
n m
alar
ia c
ases
are
de
crea
sing,
the
deve
lopm
ent o
f stra
tegi
c mas
ter p
lans
on
HIS
is an
impo
rtant
step
to gu
ide
coun
tries
in th
e rig
ht d
irect
ion.
Cam
bodi
a alre
ady fi
naliz
ed it
s dra
ft H
MIS
mas
ter p
lan,
with
AD
B su
ppor
t. M
yanm
ar re
leas
ed it
s st
rate
gic
actio
n pl
an fo
r stre
ngth
enin
g he
alth
info
rmat
ion
2017
–202
1.Vie
t Nam
’s In
form
atio
n Te
chno
logy
(IT)
Dev
elop
men
t Pla
n 20
16–2
020
was
use
d to
est
ablis
h se
vera
l ne
w in
tero
pera
bilit
y po
licie
s with
the
MO
H in
201
8. A
dditi
onal
ly, A
DB
supp
orte
d th
e re
view
of t
he d
raft
vers
ion
1 of t
he E
nter
prise
Arc
hite
ctur
e w
ith fo
cus o
n th
e es
tabl
ishm
ent o
f a st
rate
gy fo
r in
tegr
atio
n an
d in
tero
pera
bilit
y of
exis
ting
info
rmat
ion
syst
ems a
cros
s the
dire
ctor
ates
(pre
vent
ive
and
cura
tive)
that
incl
udes
a st
anda
rds-
base
d ap
proa
ch a
nd a
mor
e co
mpr
ehen
sive
vers
ion
2 ar
chite
ctur
e. G
iven
the
MO
H p
lans
for a
nat
iona
l dat
a ce
nter
, AD
B pr
ovid
ed te
chni
cal e
xper
t res
ourc
e fo
r gui
danc
e in
bes
t pra
ctic
es in
nat
iona
l dat
a ce
nter
s.•
In m
any
GM
S co
untri
es, t
he w
ork
on in
tero
pera
bilit
y of
clie
nt a
nd fa
cilit
y re
gist
ries i
s ong
oing
, as i
s con
verg
ence
of c
omm
unic
able
dise
ases
info
rmat
ion
syst
ems a
nd h
ealth
IT g
over
nanc
e. It
is
beco
min
g in
crea
singl
y cl
ear t
hat s
igni
fican
t inv
estm
ents
in b
ackb
one
info
rmat
ion
and
com
mun
icat
ion
tech
nolo
gy (
ICT)
infra
stru
ctur
e, p
roce
ss im
prov
emen
ts, a
nd c
apac
ity d
evel
opm
ent a
re
requ
ired
and
that
thos
e ca
n al
so b
e le
vera
ged
by u
sers
out
side
the
heal
th se
ctor
. AD
B w
orke
d w
ith V
iet N
am e
stab
lish
a Hea
lth IC
T ac
tion
plan
. As o
ne o
f the
com
pone
nts a
nd to
faci
litat
e on
goin
g in
tero
pera
bilit
y tes
ting a
nd kn
owle
dge
base
d on
exis
ting n
atio
nal p
olic
ies,
the
Stan
dard
s and
Inte
rope
rabi
lity L
ab fo
r Asia
is a
ssist
ing V
iet N
am e
stab
lish
its in
tero
pera
bilit
y lab
at t
he M
OH
EH
A.
•To
achi
eve i
nter
oper
abilit
y, ca
paci
ty b
uild
ing a
nd go
vern
ance
in h
ealth
care
, sta
ndar
ds b
ased
on
natio
nal p
olic
ies i
s crit
ical
. In V
iet N
am, A
DB
faci
litat
ed a
natio
nal in
tero
pera
bilit
y wor
ksho
p in
Mar
ch
2018
and
hel
d fo
llow
-up
mee
tings
with
pub
lic a
nd p
rivat
e so
lutio
n pr
ovid
ers t
o ad
vanc
e kn
owle
dge
and
use
of H
ealth
Lev
el S
even
(HL7
) FH
IR fo
r int
erop
erab
ility i
n di
seas
e su
rvei
llanc
e an
d EH
R.
AD
B m
ade r
ecom
men
datio
ns re
gard
ing i
nter
oper
abilit
y for
the l
ocal
hea
lth co
mm
une l
evel
info
rmat
ion
syst
ems (
12,0
00 st
atio
ns) a
nd as
siste
d th
e MO
H to
esta
blish
a Vi
et N
am In
tero
pera
bilit
y lab
.•
Trai
ning
hea
lth w
orke
rs in
new
ly e
nhan
ced
dise
ase
surv
eilla
nce
syst
ems i
s key
to e
nsur
ing
use,
impr
ovin
g da
ta q
ualit
y an
d pr
omot
ing
com
preh
ensiv
e re
porti
ng o
f com
mun
icab
le d
iseas
es. I
n Vi
et
Nam
, AD
B su
ppor
ted
eigh
t lar
ge p
rovi
ncia
l lev
el e
lect
roni
c co
mm
unic
able
dise
ase
surv
eilla
nce
(eCD
S) tr
aini
ngs,
and
supp
orte
d tra
inin
g in
clin
ical
term
inol
ogy
(cod
ing)
for t
he M
OH
Vie
t Nam
A
dmin
istra
tion
of M
edic
al S
ervi
ces.
AD
B al
so e
valu
ated
dig
ital h
ealth
trai
ning
pro
gram
s and
cou
rses
and
form
ulat
ed a
set o
f rec
omm
enda
tions
on
how
to im
prov
e an
d su
stai
n eH
ealth
cap
acity
at
univ
ersit
ies.
•w
orki
ng c
lose
ly w
ith V
iet N
am’s
Gen
eral
Dep
artm
ent o
f Pre
vent
ive
Med
icin
e, A
DB
impl
emen
ted
the
initi
al s
yste
ms
deve
lopm
ent o
f the
Dig
ital H
ealth
Fra
me
aim
ed a
t diss
emin
atin
g ou
tbre
ak
info
rmat
ion
to c
omm
unity
leve
l. In
supp
ort o
f thi
s new
syst
em, s
erve
r equ
ipm
ent w
as p
rocu
red.
•N
umer
ous c
ount
ries c
ontin
ue to
inve
st in
DH
IS2 i
mpl
emen
tatio
n as
an in
form
atio
n sy
stem
to ai
d na
tiona
l hea
lth st
atist
ics r
epor
ting.
In la
te 20
17, V
iet N
am in
stitu
ted
polic
y to
utiliz
e D
HIS
2 at g
rass
ro
ots l
evel
to a
id in
the
annu
al h
ealth
stat
istic
s rep
ortin
g, w
hich
is n
ow a
mul
tiyea
r man
ual c
ompi
latio
n pr
oces
s. A
DB
is su
ppor
ting
the
repo
rt au
tom
atio
n by
pro
vidi
ng te
chni
cal r
esou
rces
(HIS
P Vi
et N
am).
Supp
orte
d ac
tiviti
es in
clud
e M
OH
trai
ning
of t
he tr
aine
rs an
d dr
aftin
g of s
tand
ard
oper
atin
g pro
cedu
res (
SOPs
) for
nat
iona
l sca
le. w
ith V
iet N
am’s
plan
to im
plem
ent a
rem
odel
ed lo
cal
heal
th c
omm
une
stru
ctur
e na
tionw
ide,
AD
B w
orke
d w
ith th
e M
OH
EH
A a
nd th
e D
epar
tmen
t of P
lann
ing
and
Fina
nce
deve
lop
term
s of r
efer
ence
for l
ocal
to n
atio
nal l
evel
info
rmat
ion
flow
and
in
tero
pera
bilit
y. Th
e sy
stem
will
utiliz
e D
HIS
2 for
hea
lth st
atist
ics r
epor
ting,
esta
blish
the
EHR
and
enab
le H
IS in
tero
pera
bilit
y. Th
e lo
cal h
ealth
com
mun
e w
ill en
com
pass
pre
vent
ativ
e an
d cu
rativ
e se
ctor
s, in
clus
ive
of d
iseas
e su
rvei
llanc
e.•
In V
iet N
am, A
DB
team
ed u
p w
ith th
e Cl
into
n H
ealth
Acc
ess
Initi
ativ
e an
d th
e N
atio
nal I
nstit
ute
of M
alar
iolo
gy, P
aras
itolo
gy a
nd E
ntom
olog
y (N
IMPE
) to
eva
luat
e th
e co
untry
’s eC
DS
and
deve
lope
d a s
et o
f rec
omm
enda
tions
for d
evel
opin
g the
mal
aria
man
agem
ent s
yste
m. T
he G
ener
al D
epar
tmen
t of P
reve
ntiv
e Med
icin
e and
NIM
PE ar
e to
esta
blish
step
s for
an in
tegr
ated
not
ifiab
le
dise
ase
surv
eilla
nce
syst
em (u
sing e
CDS)
and
mal
aria
man
agem
ent s
yste
ms.
AD
B al
so su
ppor
ted
the
cond
uct o
f fac
ility a
sses
smen
t to
info
rm o
n m
alar
ia se
rvic
e re
adin
ess a
nd av
aila
bilit
y in
publ
ic
heal
th fa
cilit
ies i
n ni
ne d
istric
ts o
f Vie
t Nam
with
hig
h m
alar
ia tr
ansm
issio
n ra
tes.
A c
ostin
g to
ol b
ased
on
the
resu
lts o
f the
faci
lity
asse
ssm
ent w
as d
evel
oped
to p
rovi
de e
stim
ates
of t
he c
ost o
f ad
dres
sing c
urre
nt a
nd e
mer
ging
reso
urce
gaps
ove
r five
-yea
r tim
e sc
ale.
Res
ults
wer
e di
scus
sed
in a
foru
m th
at b
roug
ht to
geth
er N
IMPE
offi
cial
s and
mal
aria
staff
at p
rovi
ncia
l and
dist
rict l
evel
.•
To in
stitu
tiona
lize
mal
aria
elim
inat
ion
surv
eilla
nce,
a s
tand
ards
-bas
ed, g
eo-e
nabl
ed in
form
atio
n sy
stem
has
to b
e in
pla
ce w
ith ro
utin
e pr
oces
ses
linke
d to
an
inte
rope
rabl
e he
alth
info
rmat
ion
exch
ange
. The
pro
ject
sign
ifica
ntly
adv
ance
d th
e po
licy
dial
og o
n an
ent
erpr
ise a
rchi
tect
ure
appr
oach
to H
IS a
s cou
ntrie
s go
thro
ugh
thei
r dig
ital t
rans
form
atio
n. T
his w
ill en
sure
that
futu
re IC
T he
alth
inve
stm
ents
are
sust
aina
ble,
effi
cien
t, eff
ectiv
e an
d di
rect
ly c
ontri
butin
g to
cou
ntry
’s da
ta a
nd in
form
atio
n ne
eds.
The
scop
e of
the
activ
ities
also
incl
uded
wor
k on
a h
ealth
IT g
over
nanc
e fra
mew
ork,
whi
ch w
ill he
lp to
addr
ess d
ata s
harin
g, pr
ivac
y and
secu
rity i
ssue
s. U
ntil t
hose
are
addr
esse
d, d
ata s
harin
g am
ong a
genc
ies a
nd co
untri
es w
ill no
t be
poss
ible
. Mor
eove
r, the
pro
ject
bui
lt th
e cap
acity
of M
OH
s to
man
age h
ealth
ICT
proj
ects
and
ensu
re th
at d
evel
opm
ent p
artn
ers s
uppo
rt eH
ealth
solu
tions
for c
omm
unic
able
dise
ase a
nd m
alar
ia p
rogr
ams a
re sc
alab
le an
d su
stai
nabl
e.
cont
inue
d on
nex
t pag
e
Annex 55
Stor
y be
hind
the
num
bers
•Th
e ge
ogra
phic
dim
ensio
n of
mal
aria
and
deng
ue is
key t
o en
hanc
ing d
iseas
e su
rvei
llanc
e an
d m
alar
ia e
limin
atio
n th
roug
h im
prov
ed si
tuat
iona
l inte
lligen
ce. I
t also
pro
vide
s a u
niqu
e co
ntex
t to
link
verti
cal d
iseas
e pro
gram
s tog
ethe
r thr
ough
the g
eo-e
nabl
emen
t of t
he H
IS. A
mon
g the
nin
e ele
men
ts d
efini
ng th
e HIS
geo-
enab
ling f
ram
ewor
k, tw
o ar
e dire
ctly
rela
ted
to IC
T so
lutio
ns: (
i) Th
e use
of
geo
spat
ial t
echn
olog
ies i
nclu
ding
GIS
; (ii)
the
avai
labi
lity o
f a c
omm
on g
eo-r
egist
ry to
ena
ble
the
para
llel h
ostin
g, m
aint
aini
ng a
nd u
pdat
ing
of th
e m
aste
r list
s for
the
geog
raph
ic o
bjec
ts c
ore
to
publ
ic h
ealth
(hea
lth fa
cilit
ies,
adm
inist
rativ
e an
d re
porti
ng d
ivisi
ons,
villa
ges.
•M
ORU
and
the
Hea
lth G
eoLa
b Co
llabo
rativ
e (H
GLC
, for
mer
ly A
eHIN
GIS
lab)
wor
ked
toge
ther
to st
reng
then
the
tech
nica
l cap
acity
of t
he N
atio
nal M
alar
ia C
ontro
l Pro
gram
s (N
MCP
s) a
s wel
l as
oth
er ke
y MO
H e
ntiti
es in
Ban
glad
esh,
Cam
bodi
a, M
yanm
ar, T
haila
nd, a
nd V
iet N
am th
roug
h: (i
) The
dev
elop
men
t of r
efer
ence
mat
eria
l to
ensu
re th
e us
e te
chno
logy
to b
e em
bedd
ed in
good
ge
ospa
tial d
ata m
anag
emen
t pra
ctic
es (d
ocum
enta
tion
and
prom
otio
n of
the
conc
ept o
f com
mon
geo-
regi
stry
for e
xam
ple)
; (ii)
The
pro
visio
n of
appr
opria
te e
quip
men
t (ha
rdw
are
and
softw
are)
; (ii
i) Th
e co
nduc
t of N
atio
nal a
nd R
egio
nal t
rain
ings
(also
atte
nded
by
the
Lao
PDR)
; (iv
) Ons
ite a
nd re
mot
e te
chni
cal s
uppo
rt in
map
ping
and
ana
lysis
of su
rvei
llanc
e da
ta fo
r the
who
le c
ount
ry
for m
alar
ia a
nd d
engu
e; (v
) The
col
lect
ion
of g
eogr
aphi
c co
ordi
nate
s in
the
field
to im
prov
e so
me
of th
e ke
y la
yers
of i
nfor
mat
ion
need
ed fo
r mal
aria
elim
inat
ion;
(vi)
The
anal
ysis,
map
ping
, and
pr
esen
tatio
n in
diff
eren
t for
ums o
f cou
ntry
wid
e m
alar
ia a
nd d
engu
e su
rvei
llanc
e da
ta (C
ambo
dia,
Mya
nmar
, and
Tha
iland
).•
In ad
ditio
n to
the
abov
e, in
itial
wor
k on
asse
ssin
g the
rela
tions
hip
betw
een
clim
ate,
fore
st, a
nd m
alar
ia u
sing w
eath
er st
atio
n an
d re
mot
e se
nsin
g sat
ellit
e da
ta h
as b
een
com
plet
ed w
ith fu
rther
wor
k on
goin
g. A
nalys
is of
cal
l det
ail r
ecor
ds in
Tha
iland
has
bee
n co
mpl
eted
to m
odel
the
impa
ct o
f pop
ulat
ion
mov
emen
t pat
tern
s on
mal
aria
and
den
gue
dist
ribut
ion.
Fin
al a
ppro
val f
or th
is is
pend
ing
from
the
natio
nal r
egul
ator
in M
yanm
ar. T
rave
l sur
vey d
ata
from
pat
ient
s with
mal
aria
in C
ambo
dia,
the
Lao
PDR,
Mya
nmar
, Tha
iland
, and
Vie
t Nam
has
bee
n an
alyz
ed a
nd sh
ared
.•
The
AeH
IN G
IS L
ab h
as c
onve
rted
into
the
HG
LC in
Dec
embe
r 201
7 to
brin
g m
ore
partn
ers,
and
ther
efor
e re
sour
ces,
to c
ount
ries i
n A
sia a
nd th
e Pa
cific
to c
ontin
ue th
e w
ork
star
ted
unde
r the
um
brel
la o
f the
RM
TF. A
t the
tim
e of
clo
sing t
he R
ECA
P te
chni
cal a
ssist
ance
(TA)
, the
HG
LC co
unts
16-m
embe
r ins
titut
ions
incl
udin
g the
MO
H e
ntiti
es in
volv
ed in
the
HIS
geo-
enab
ling p
roce
ss
and
his p
rovi
ding
reso
urce
s acc
essib
le p
rinci
pally
to th
e 30
low
and
mid
dle-
inco
me
coun
tries
in A
sia a
nd th
e Pa
cific
.•
Polic
y re
com
men
datio
ns fo
r ta
rget
ing
mob
ile p
opul
atio
ns in
mal
aria
and
den
gue
surv
eilla
nce
and
cont
rol p
rogr
ams
have
bee
n de
velo
ped
for
Cam
bodi
a, M
yanm
ar, a
nd T
haila
nd. T
he fi
nal
reco
mm
enda
tions
will
be p
rovi
ded
once
the
resu
lts o
f the
pop
ulat
ion
mov
emen
t ana
lysis
usin
g ca
ll da
ta re
cord
s hav
e be
en sh
ared
and
disc
usse
d w
ith M
OH
staff
. Add
ition
al fu
ndin
g su
ppor
t has
be
en se
cure
d by
MO
RU to
com
plet
e th
is w
ork.
•In
crea
sed
inve
stm
ent i
n di
gita
l hea
lth c
an s
uppo
rt im
prov
ed m
alar
ia s
urve
illanc
e an
d re
spon
se. P
art o
f AD
B’s
digi
tal h
ealth
stra
tegy
gui
danc
e an
d di
gita
l hea
lth im
pact
fram
ewor
k in
clud
es a
n ex
ampl
e of
an
inve
stm
ent c
ase
stra
tegy
for m
alar
ia se
rvic
es a
nd a
n im
plem
enta
tion
guid
e. It
was
diss
emin
ated
to G
MS
coun
tries
in a
regi
onal
wor
ksho
p du
ring
the
2018
Prin
ce M
ahid
ol A
war
ds
Conf
eren
ce.
Box c
ontin
ued

56 Annex
OU
TCO
ME
5: L
ABO
RATO
RY D
IAG
NO
STIC
S A
ND
SU
RVEI
LLA
NCE
Impr
oved
cap
acity
of l
abor
ator
y dia
gnos
tics a
nd su
rvei
llanc
e sy
stem
for m
alar
ia a
nd o
ther
com
mun
icab
le d
iseas
es, in
clud
ing c
ross
-bor
der c
oord
inat
ion
Out
com
e 5.
1 Inc
reas
ed d
iagn
ostic
test
ing
for m
alar
ia in
pro
ject
are
as o
f Cam
bodi
a, L
ao P
DR,
and
Vie
t Nam
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
1620
1720
1620
171.
Ann
ual b
lood
exa
min
atio
n pe
r 100
pop
at
risk
for m
alar
ia in
the
proj
ect a
reas
*D
iagn
ostic
cap
acity
for m
alar
ia
1. Pr
opor
tion
of h
ealth
fa
cilit
ies i
n pr
ojec
t are
as
equi
pped
with
mal
aria
di
agno
stic
equ
ipm
ent
CAM
0 0
83
80
LAO
010
010
0 7
0Ca
mbo
dia
Prea
h Vi
hear
Pro
vinc
e11
.2 6
.7 8
.410
.0VI
E**
7878
100
100
2. Pr
opor
tion
of la
bora
tory
st
aff in
targ
et p
rovi
nces
tra
ined
in m
alar
ia
diag
nosis
CAM
0 0
100
100
LAO
0 0
96
70
VIE
010
010
010
0La
o PD
R Ch
ampa
ssac
k Pr
ovin
ce12
.7 7
.9 9
.210
.0
Atta
peu
Prov
ince
25.5
13.4
18.5
10.0
Sara
vane
Pro
vinc
e14
.2 8
.3 8
.410
.0
Seko
ng P
rovi
nce
17.4
12.1
14.6
10.0
Viet
Nam
Bi
nh P
huoc
Pro
vinc
e12
.515
.610
.510
.0
Dak
Non
g Pro
vinc
e12
.810
.413
.310
.0
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
S
ubst
antia
l pro
gres
s ach
ieve
dCA
M =
Cam
bodi
a, L
AO =
Lao
Peo
ple’s
Dem
ocra
tic R
epub
lic, V
IE =
Vie
t Nam
.* D
ata
from
the
Min
istry
of H
ealth
** O
f the
182
com
mun
e he
alth
stat
ions
in th
e pr
ojec
t are
as, o
nly 4
0 re
quire
d ne
w m
icro
scop
es fo
r mal
aria
test
ing

Annex 57
Out
com
e 5.
2 Im
prov
ed su
rvei
llanc
e an
d re
spon
se fo
r mal
aria
and
oth
er c
omm
unic
able
dise
ases
in p
roje
ct a
reas
of
Cam
bodi
a, L
ao P
DR,
and
Vie
t Nam
incl
udin
g in
cro
ss-b
orde
r are
as
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
1620
1720
1620
171.
Prop
ortio
n of
dise
ase
outb
reak
s (in
clud
ing m
alar
ia) i
n pr
ojec
t are
as
repo
rted
with
in 2
4 ho
urs
Surv
eilla
nce
capa
city
for m
alar
ia
1. Pr
opor
tion
of h
ealth
faci
litie
s and
la
bora
torie
s in
proj
ect a
reas
equ
ippe
d w
ith e
lect
roni
c re
porti
ng in
stru
men
ts fo
r m
alar
ia su
rvei
llanc
e
CAM
00
100
100
LAO
00
100
50Ca
mbo
dia
Prea
h Vi
hear
100
100
100
80VI
E**
100
100
100
100
2. P
ropo
rtion
of h
ealth
faci
litie
s in
targ
et
prov
ince
s with
staff
trai
ned
in m
alar
ia
surv
eilla
nce
with
ele
ctro
nic
repo
rting
in
stru
men
t
CAM
00
100
100
LAO
032
7720
VIE
050
50*
80La
o PD
R Ch
ampa
ssac
k 10
010
010
080
Cros
s-bo
rder
coo
rdin
atio
n an
d re
spon
se fo
r mal
aria
Atta
peu
50
100
100
803.
Num
ber o
f coo
rdin
ated
cro
ss-
bord
er a
ctio
n pl
ans d
evel
oped
ba
sed
on G
MS
mal
aria
elim
inat
ion
stra
tegy
in ta
rget
ed b
orde
r pr
ovin
ces
CAM
00
11
Sara
vane
100
80
100
80LA
O
02
22
Seko
ng10
0 6
0 8
380
VIE*
**0
--
3
Viet
Nam
Bi
nh P
huoc
100
100
100*
804.
Num
ber o
f villa
ge h
ealth
wor
kers
at
bord
er p
rovi
nces
trai
ned
in m
alar
ia
cont
rol a
nd tr
eatm
ent
CAM
00
331
332
Dak
Non
g10
010
010
0*80
LAO
0
032
260
2. P
ropo
rtion
of b
orde
r dise
ase
outb
reak
s (in
clud
ing m
alar
ia) i
n pr
ojec
t are
as
repo
rted
acro
ss b
orde
rs w
ithin
24
hour
s
VIE
023
623
6*40
Cam
bodi
a Pr
eah
Vihe
arN
AN
AN
A50
Lao
PDR
Cham
pass
ack
100
100
100
50
Atta
peu
50
100
100
50
Sara
vane
100
80
100
50
Seko
ng10
0 6
0 8
350
Viet
Nam
Bi
nh P
huoc
100
100
100*
50
Dak
Non
g10
010
010
0*50
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
S
ubst
antia
l pro
gres
s ach
ieve
dCA
M =
Cam
bodi
a, L
AO =
Lao
Peo
ple’s
Dem
ocra
tic R
epub
lic, N
A –
no
outb
reak
s of r
egio
nal o
r int
erna
tiona
l rel
evan
ce, V
IE =
Vie
t Nam
.* A
s of Q
1 201
7**
Faci
litie
s alre
ady h
ave
the
need
ed e
quip
men
t**
* No
spec
ific
cros
s-bo
rder
act
ion
plan
s wer
e de
velo
ped
by p
rovi
nces
but
six c
ross
-bor
der a
ctiv
ities
wer
e in
corp
orat
ed in
to th
e pr
ovin
cial
ann
ual o
pera
tiona
l pla
ns th
at w
ere
all im
plem
ente
d

58 Annex
Stor
y be
hind
the
num
bers
•Th
e ad
ditio
nal fi
nanc
ing
for m
alar
ia-r
elat
ed a
ctiv
ities
aim
ed to
dire
ct e
fforts
tow
ard
mal
aria
con
trol a
nd e
limin
atio
n th
roug
h re
gion
al a
nd c
ount
ry s
truct
ures
and
pro
cess
es a
lread
y es
tabl
ished
und
er th
e A
DB
Com
mun
icab
le D
iseas
e Pro
ject
2 (C
DC2
). M
alar
ia ac
tiviti
es fu
nded
und
er th
e RM
TF co
mpl
emen
ted
and
augm
ente
d th
e nat
iona
l mal
aria
pro
gram
s in
Cam
bodi
a, th
e Lao
PD
R, an
d Vi
et N
am an
d w
ere s
ynch
roni
zed
with
don
or p
artn
ers’
ongo
ing i
nvol
vem
ents
in m
alar
ia a
nd in
add
ress
ing t
he sp
read
of a
rtem
isini
n re
sista
nce
in th
e re
gion
.•
The
RMTF
con
tribu
ted
to th
e sig
nific
ant d
ecre
ase
in th
e in
cide
nce
of P
. fal
cipar
um m
alar
ia in
the
proj
ect s
ites (
from
17.3
case
s per
1000
pop
ulat
ion
in 2
014
to 1.
8 in
201
7 in
the
proj
ect s
ites o
f Cam
bodi
a, a
nd fr
om
15.9
in 2
014
to 1.
6 in
201
7 in
the
proj
ect s
ites o
f the
Lao
PD
R).
Lao
PDR
•Th
e st
rate
gies
and
activ
ities
fund
ed u
nder
the
RMTF
in th
e La
o PD
R w
ere
iden
tified
in co
nsul
tatio
n w
ith d
evel
opm
ent p
artn
ers a
nd st
akeh
olde
rs w
orki
ng in
mal
aria
to e
nsur
e th
at th
e RM
TF in
vest
men
ts w
ould
lead
to
valu
e fo
r mon
ey a
nd re
ap m
axim
um re
sults
with
out d
uplic
atin
g effo
rts.
•In
the
proj
ect s
ites,
vect
or su
rvei
llanc
e an
d co
ntro
l gui
delin
es a
nd tr
aini
ng m
anua
ls w
ere
upda
ted,
vect
or c
ontro
l equ
ipm
ent w
ere
prov
ided
, and
staff
and
villa
ge h
ealth
wor
kers
wer
e tra
ined
.•
Beha
vior
al c
hang
e co
mm
unic
atio
n/IE
C m
ater
ials
wer
e de
velo
ped
targ
etin
g spe
cific
aud
ienc
es vi
a TV
and
radi
o ca
mpa
igns
. Reg
ular
mob
ile h
ealth
edu
catio
n se
ssio
ns w
ere
cond
ucte
d in
scho
ols a
nd vi
llage
s in
high
pr
eval
ence
are
as.
•Pr
ovin
cial
and
dist
rict h
ealth
staff
wer
e tra
ined
on
mal
aria
cas
e m
anag
emen
t and
trea
tmen
t whi
le vi
llage
hea
lth w
orke
rs w
ere
also
trai
ned
on m
alar
ia c
ontro
l and
surv
eilla
nce.
•SO
Ps a
nd g
uide
lines
wer
e up
date
d an
d tra
inin
gs c
ondu
cted
on
mal
aria
dia
gnos
is an
d m
icro
scop
y an
d la
bora
tory
qua
lity
assu
ranc
e. A
ll di
stric
t-le
vel f
acilit
ies
in th
e pr
ojec
t site
s w
ere
alre
ady
equi
pped
with
m
icro
scop
es. H
emog
lobi
nom
eter
s w
ere
requ
este
d in
stea
d to
add
ress
the
high
inci
denc
e of
P. v
ivax
case
s in
the
Lao
PDR.
Rel
evan
t sta
ff w
ere
train
ed o
n th
e us
e of
the
mac
hine
and
on
the
adm
inist
ratio
n of
pr
imaq
uine
for P
. viva
x tre
atm
ent.
•Th
e pr
ojec
t sup
porte
d m
alar
ia c
ase
surv
eilla
nce
and
repo
rting
at c
entra
l, pr
ovin
cial
and
dist
rict l
evel
s, in
clud
ing
pass
ive
and
activ
e ca
se d
etec
tion
and
dire
ctly
obs
erve
d tre
atm
ent.
Staff
from
cen
tral,
prov
inci
al
dist
rict a
nd c
heck
poin
ts w
ere
prov
ided
with
tele
phon
e ca
rds f
or d
iseas
e su
rvei
llanc
e an
d re
porti
ng. T
hey w
ere
also
trai
ned
on th
e D
HIS
2 re
porti
ng sy
stem
for m
alar
ia.
•Cr
oss-
bord
er d
iseas
e in
form
atio
n ex
chan
ge in
clud
ed m
alar
ia. A
ll pro
vinc
ial a
nnua
l ope
ratio
ns p
lan
incl
uded
mal
aria
targ
ets a
nd a
ctiv
ities
.
Cam
bodi
a•
The
RMTF
supp
ort i
n th
e pr
ojec
t site
in C
ambo
dia
(Pre
ah V
ihea
r) w
as to
pilo
t P. fa
lcipa
rum
elim
inat
ion
stra
tegi
es a
nd in
terv
entio
ns.
•Th
roug
h th
e RM
TF, t
he q
ualit
y of
pro
vinc
ial l
abor
ator
y se
rvic
es w
as im
prov
ed th
roug
h tra
inin
g an
d su
ppor
tive
supe
rvisi
on o
f lab
orat
ory
staff
, pur
chas
e of
labo
rato
ry e
quip
men
t (Lo
op-m
edia
ted
isoth
erm
al
ampl
ifica
tion
[LA
MP]
, mic
rosc
opes
), m
ater
ials,
reag
ents
, and
oth
er la
bora
tory
con
sum
able
s. LA
MP
devi
ces w
ere
prov
ided
for t
he d
etec
tion
of m
alar
ia c
ases
with
low
par
asite
den
sity.
The
mic
rosc
opes
pro
vide
d ha
d m
ount
ed c
amer
as to
cap
ture
and
shar
e di
gita
l im
ages
of t
he b
lood
smea
rs, s
horte
ning
dia
gnos
is tim
e an
d su
bseq
uent
ly re
sulti
ng to
tim
ely
treat
men
t. Th
e pr
ovisi
on o
f suc
h m
icro
scop
es c
ompl
emen
ted
the
inno
vativ
e m
icro
scop
y qua
lity a
ssur
ance
and
con
trol p
roce
dure
s tha
t wer
e im
plem
ente
d in
the
targ
et h
ealth
faci
litie
s.•
The
qual
ity o
f clin
ical
dia
gnos
tic a
nd c
ase
man
agem
ent w
as im
prov
ed th
roug
h th
e tra
inin
g of
hea
lth st
aff o
n m
alar
ia c
linic
al m
anag
emen
t, m
anag
emen
t of s
tock
s and
supp
lies,
and
the
re-e
stab
lishm
ent o
f the
fu
nctio
ns o
f villa
ge m
alar
ia w
orke
rs a
nd tr
aini
ng th
em to
impr
ove
thei
r ski
lls o
n cl
inic
al d
iagn
osis
and
case
man
agem
ent.
•Th
e su
rvei
llanc
e an
d re
spon
se sy
stem
was
exp
ande
d to
incl
ude
the
prov
ision
of t
rain
ing
to h
ealth
staff
and
villa
ge m
alar
ia w
orke
rs o
n pr
oper
dat
a m
anag
emen
t and
repo
rting
, rea
l-tim
e ca
se n
otifi
catio
n, v
illage
st
ratifi
catio
n an
d in
dex
case
inve
stig
atio
n. S
hifti
ng fr
om a
pre
viou
sly p
assiv
e ca
se d
etec
tion
syst
em a
t pub
lic h
ealth
faci
litie
s to
a ne
w m
odel
that
com
bine
s exis
ting
pass
ive
syst
em a
nd a
ctiv
e sy
stem
of s
cree
ning
m
alar
ia c
ases
at c
omm
uniti
es a
nd h
ouse
hold
s res
ulte
d in
Incr
ease
d ca
se d
etec
tion
rate
in th
e pr
ojec
t site
s. Fo
ci in
vest
igat
ions
wer
e al
so c
ondu
cted
alo
ng w
ith a
ctiv
e ca
se d
etec
tion
and
inve
stig
atio
n.•
A d
igita
l dat
a de
vice
(DD
D) w
as in
trodu
ced
and
used
by
heal
th c
ente
r sta
ff an
d vi
llage
mal
aria
wor
kers
for r
eal-t
ime
mal
aria
pos
itive
cas
es re
porti
ng a
nd n
otifi
catio
n us
ing
a st
anda
rdize
d te
mpl
ate
with
com
plet
e se
t of i
nfor
mat
ion
for c
ase
inve
stig
atio
n. M
OH
repo
rted
that
the
use
of th
e D
DD
has
impr
oved
mal
aria
surv
eilla
nce
and
resp
onse
.•
The
proj
ect a
lso e
ngag
ed re
gist
ered
priv
ate
prov
ider
s in
case
det
ectio
n, q
ualit
y tre
atm
ent,
follo
w-u
p, d
ata
man
agem
ent,
and
case
repo
rting
. wor
ksho
ps o
n ph
arm
acov
igila
nce
(mal
aria
dru
g us
e) w
ere
prov
ided
to
heal
th p
rofe
ssio
nal in
bot
h pu
blic
and
priv
ate
sect
ors.
Ratio
nal u
se o
f ant
i-mal
aria
l dru
gs w
as e
ncou
rage
d w
ith su
ppor
tive
supe
rvisi
on, a
nd p
artn
ersh
ip w
ith p
rivat
e pr
ovid
ers w
as e
stab
lishe
d.•
The
proj
ect s
uppo
rted
the
form
atio
n of
mal
aria
elim
inat
ion
task
forc
e co
mpr
ised
of p
rovi
ncia
l hea
lth o
ffice
s, lo
cal a
utho
ritie
s, no
n-he
alth
age
ncie
s, an
d de
velo
pmen
t par
tner
s ope
ratin
g in
the
proj
ect s
ites.
•IE
C m
ater
ials
wer
e de
velo
ped
and
diss
emin
ated
thou
gh m
ulti-
med
ia c
hann
els,
incl
udin
g billb
oard
s tar
getin
g mig
rant
and
mob
ile p
opul
atio
ns (M
MPs
) on
mal
aria
pre
vent
ion.
•D
iseas
e in
form
atio
n ex
chan
ge a
mon
g bor
der p
rovi
nces
incl
uded
mal
aria
. All p
rovi
ncia
l ann
ual o
pera
tions
pla
n al
so in
clud
ed m
alar
ia ta
rget
s and
act
iviti
es.
•Th
e st
rate
gy a
nd in
itiat
ives
dev
elop
ed b
y RM
TF in
Pre
ah V
ihea
r for
mal
aria
elim
inat
ion
was
repo
rted
by M
OH
to h
ave
been
exp
ande
d to
oth
er a
reas
in th
e co
untry
.
cont
inue
d on
nex
t pag
e

Annex 59
Stor
y be
hind
the
num
bers
Viet
Nam
•Th
e m
alar
ia s
ituat
ion
in th
e pr
ojec
t site
s in
Vie
t Nam
rem
aine
d re
lativ
ely
stab
le s
ince
201
6 w
ith v
ecto
r con
trol c
over
age
mai
ntai
ned
as p
lann
ed, a
nd th
e di
agno
sis a
nd tr
eatm
ent o
f mal
aria
follo
wed
the
MO
H
prot
ocol
.•
Trai
ning
s on
mal
aria
surv
eilla
nce
was
pro
vide
d to
88
prov
inci
al an
d di
stric
t sta
ff, an
d 19
4 co
mm
une
staff
. Tra
inin
gs o
n la
bora
tory
tech
niqu
es an
d on
the
use
of m
icro
scop
es w
ere
prov
ided
to 30
pro
vinc
ial a
nd d
istric
t st
aff.
•Su
perv
ision
s wer
e fie
lded
to th
e pr
ovin
cial
mal
aria
cen
ters
, dist
rict h
ealth
cen
ters
, and
com
mun
e he
alth
stat
ions
.•
Four
roun
ds o
f mal
aria
surv
eilla
nce,
act
ive
case
det
ectio
n an
d tre
atm
ent w
ere
cond
ucte
d in
four
dist
ricts
of B
inh
Phuo
c.•
Four
roun
ds o
f mon
itorin
g the
pro
hibi
ted
circ
ulat
ion
and
use
of m
onot
hera
py, c
ount
erfe
it an
d po
or q
ualit
y dru
gs at
the
med
ical
stat
ions
and
phar
mac
ies w
ere
cond
ucte
d in
the
dist
ricts
and
tow
ns o
f the
two
proj
ect
prov
ince
s. N
o vi
olat
ions
to th
e re
gula
tions
wer
e de
tect
ed.
•Th
e pr
ojec
t sup
porte
d or
ient
atio
n w
orks
hops
on
mal
aria
con
trol f
or C
ambo
dia–
Lao
PDR–
Viet
Nam
bor
der p
rovi
nces
(Oct
ober
–Dec
embe
r 201
6 an
d Fe
brua
ry–M
arch
201
7).
•M
onth
ly in
form
atio
n sh
arin
g inc
ludi
ng m
alar
ia w
as c
ondu
cted
in 13
of 1
4 bo
rder
pro
vinc
es in
Vie
t Nam
. All p
rovi
ncia
l ann
ual o
pera
tions
pla
n al
so in
clud
ed m
alar
ia ta
rget
s and
act
iviti
es.
Box c
ontin
ued

60 Annex
Out
com
e 5.
3 In
crea
sed
diag
nost
ic te
stin
g fo
r mal
aria
in p
roje
ct a
reas
of M
yanm
ara,
b,c
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
16Q
2 20
1820
16Q
2 20
181.
Nat
iona
l mal
aria
dia
gnos
tic q
ualit
y as
sura
nce
guid
elin
es e
ndor
sed
by th
e N
atio
nal M
alar
ia C
ontro
l Pro
gram
Dia
gnos
tic c
apac
ity fo
r mal
aria
1. Pr
opor
tion
of h
ealth
faci
litie
s in
proj
ect
area
s equ
ippe
d w
ith m
alar
ia d
iagn
ostic
eq
uipm
ent*
*
440
100
100
Mon
Sta
te
No
No
Yes
Yes
2. P
ropo
rtion
of l
abor
ator
y sta
ff in
targ
et
prov
ince
s tra
ined
in m
alar
ia d
iagn
osis*
**24
096
100
Saga
ing R
egio
nN
oN
oYe
sYe
s3.
Nat
iona
l mal
aria
dia
gnos
tic q
ualit
y as
sura
nce
guid
elin
es d
evel
oped
No
No
Yes
Yes
2. A
nnua
l blo
od e
xam
inat
ion
per 1
00 p
op
at ri
sk fo
r mal
aria
in th
e pr
ojec
t are
asM
on S
tate
(Pro
ject
tow
nshi
ps av
erag
e)(M
awla
mya
ing,
Belin
, Pau
ng, k
yaik
hto)
4.2
-13
.5*
8.0*
***
Saga
ing R
egio
n (P
roje
ct to
wns
hips
av
erag
e)(H
kam
ti, H
omal
in, P
aung
byin
, Taz
e,
Mon
ywa,
Pal
e)
3.1
-24
.1*8.
0***
*
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
Q =
qua
rter
* Dat
a fo
r 201
7 **
Tot
al n
umbe
r of 4
3 he
alth
faci
litie
s**
*Tot
al n
umbe
r of 8
3 st
aff**
** A
BER
targ
et fo
r 202
0 in
Mya
nmar
, wH
O-M
alar
ia N
SP 2
016-
30N
ote:
201
6 da
ta w
as n
ot c
olle
cted
bec
ause
the
proj
ect i
nter
vent
ions
star
ted
only
in 2
017.
a Thi
s out
com
e ind
icato
r is u
sed
only
for M
yanm
ar. R
CDTA
8959
supp
orts
the d
evel
opm
ent o
f nat
iona
l gui
delin
es o
n lab
orat
ory d
iagno
stic
and
surv
eilla
nce a
nd is
cons
isten
t with
the M
onito
ring a
nd R
esul
t Fra
mew
ork
of th
e AD
B Te
chni
cal A
ssist
ance
Doc
umen
t for
RCD
TA89
59 d
evel
oped
with
conc
urre
nce f
rom
the G
over
nmen
t of M
yanm
ar. F
or M
yanm
ar, t
he o
utpu
t ind
icato
r on
cros
s bor
der c
oord
inat
ion
is no
t inc
lude
d sin
ce th
e pr
ojec
t has
a lim
ited
scop
e on
it wh
ile fo
cusin
g on
inte
rnal
migr
ant a
nd m
obile
pop
ulat
ions
. RCD
TA89
59 al
so su
ppor
ts M
MP-
relat
ed ac
tiviti
es in
Cam
bodi
a and
the L
ao P
DR.
b E
stim
ated
tota
l num
ber o
f ben
efici
arie
s (1,9
84,9
15 u
nder
labo
rato
ry d
iagn
ostic
s: an
d 96
9,58
5 un
der s
urve
illanc
e).
c RCD
TA89
59 su
ppor
ts th
e G
over
nmen
t of M
yanm
ar in
dev
elop
ing o
f a m
odel
to st
reng
then
its l
abor
ator
y dia
gnos
tic a
nd su
rvei
llanc
e sy
stem
at l
ocal
leve
l in tw
o pr
ojec
t are
as (M
on S
tate
and
Sag
aing
Re-
gion
), w
hich
is e
xpec
ted
to ro
ll out
in th
e en
tire
coun
try, w
hile
sim
ulta
neou
sly su
ppor
ting t
he go
vern
men
t cap
acity
at t
he c
entra
l leve
l.

Annex 61
Out
com
e 5.
4 Im
prov
ed su
rvei
llanc
e an
d re
spon
se fo
r mal
aria
and
oth
er c
omm
unic
able
dise
ases
in p
roje
ct a
reas
of M
yanm
ar
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
16Q
2 20
1820
16Q
2 20
181.
Nat
iona
l mal
aria
surv
eilla
nce
guid
elin
es
endo
rsed
by t
he N
atio
nal M
alar
ia
Cont
rol P
rogr
am
1. Pr
opor
tion
of h
ealth
staff
in p
roje
ct
area
s equ
ippe
d w
ith e
lect
roni
c re
porti
ng
inst
rum
ents
for m
alar
ia su
rvei
llanc
e*
00
9710
0
Mon
Sta
te
No
No
Yes
Yes
2. P
ropo
rtion
of h
ealth
staff
in ta
rget
pr
ovin
ces t
rain
ed in
mal
aria
surv
eilla
nce
with
ele
ctro
nic
repo
rting
inst
rum
ent*
00
9710
0
Saga
ing R
egio
nN
oN
oYe
sYe
s3.
Nat
iona
l mal
aria
surv
eilla
nce
guid
elin
es
deve
lope
dN
oN
oYe
sYe
s
2. P
ropo
rtion
of d
iseas
e ou
tbre
aks
(incl
udin
g mal
aria
) rep
orte
d w
ithin
24
hour
sM
on S
tate
N
AN
A**
80
Saga
ing R
egio
nN
AN
A**
80
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
N
A =
NA
– n
o ou
tbre
aks o
f reg
iona
l or i
nter
natio
nal r
elev
ance
, Q =
qua
rter.
*Tot
al n
umbe
r of h
ealth
staff
and
villa
ge h
ealth
volu
ntee
rs**
All m
alar
ia c
ases
wer
e re
porte
d re
al-t
ime
with
in 2
4 ho
urs b
y mD
MS
(mob
ile d
atab
ase
mal
aria
surv
eilla
nce)
NA
– n
o ou
tbre
aks o
f reg
iona
l or i
nter
natio
nal r
elev
ance
Stor
y be
hind
the
num
bers
•Th
e RM
TF T
A in
Mya
nmar
was
des
igne
d to
dev
elop
(i) a
mod
el to
stre
ngth
en c
apac
ities
for l
abor
ator
y dia
gnos
tics a
nd su
rvei
llanc
e fo
r mal
aria
and
com
mun
icab
le d
iseas
e at
loca
l and
nat
iona
l leve
ls, a
nd
(ii) a
mod
el to
stre
ngth
en h
ealth
serv
ice
deliv
ery s
yste
m fo
r MM
P, fo
cusin
g on
inte
rnal
MM
P w
ith in
volv
emen
t of t
he p
rivat
e se
ctor
.
On
mal
aria
labo
rato
ry q
ualit
y as
sura
nce
and
mal
aria
surv
eilla
nce
in M
yanm
ar•
The T
A fo
cuse
d on
stre
ngth
enin
g dat
a man
agem
ent s
yste
ms f
or m
alar
ia su
rvei
llanc
e inc
ludi
ng th
e upg
radi
ng o
f ana
lytic
al to
ols f
or d
ecisi
on-m
akin
g, sc
ale u
p an
d m
aint
enan
ce o
f dat
a man
agem
ent s
yste
ms,
coop
erat
ion
with
vol
unte
er m
alar
ia w
orke
rs (
VMw
) on
rout
ine
repo
rting
, and
real
-tim
e re
porti
ng. T
he a
ssist
ance
also
focu
sed
on u
pgra
ding
labo
rato
ry d
iagn
ostic
qua
lity
assu
ranc
e by
impl
emen
ting
a pr
ofici
ency
test
ing a
nd c
ross
chec
king
syst
em in
pro
ject
tow
nshi
ps b
ased
on
the
revi
sed
mal
aria
qua
lity a
ssur
ance
(QA)
man
uals
and
SOPs
and
thro
ugh
train
ing o
n ex
pand
ed m
alar
ia m
icro
scop
y.
•Th
e N
MCP
with
supp
ort f
rom
par
tner
s dev
elop
ed a
mob
ile D
ata
Man
agem
ent S
yste
m (m
DM
S) p
ilote
d in
the
Maw
lam
yine
, Bel
in a
nd H
kam
ti to
wns
hips
to st
reng
then
the
qual
ity o
f mon
thly
mal
aria
dat
a re
porti
ng an
d to
est
ablis
h re
al-t
ime
notifi
catio
n of
mal
aria
pos
itive
case
s fro
m V
Mw
s, ba
sic h
ealth
staff
(BH
S), h
ospi
tals
and
the
priv
ate
sect
or. T
he n
otifi
catio
n is
done
via S
MS/
Vibe
r or m
obile
appl
icat
ion
to th
e St
ate/
Regi
on a
nd T
owns
hip
Vect
or-B
orne
Dise
ase
Cont
rol o
ffice
s (VB
DC
) dat
a fo
cal p
erso
n. C
ase
inve
stig
atio
n is
expe
cted
to b
e co
nduc
ted
by B
HS
with
in 72
hou
rs a
nd p
ublic
hea
lth re
spon
se b
y th
e To
wns
hip
VBD
C w
ithin
7 d
ays.
Surv
eilla
nce
equi
pmen
t for
the
mD
MS
wer
e pr
ocur
ed a
nd d
istrib
uted
to vi
llage
volu
ntee
rs. T
rain
ings
on
mD
MS
wer
e pr
ovid
ed to
BH
S an
d vo
lunt
eers
at t
owns
hip
leve
l.
•Co
mm
oditi
es fo
r sur
veilla
nce
wer
e pr
ocur
ed an
d di
strib
uted
to th
e ce
ntra
l hea
lth o
ffice
s, re
gion
al an
d st
ate
and
tow
nshi
p m
edic
al o
ffice
s: ce
ntra
l ser
ver a
t NM
CP, 3
1 lap
tops
, 200
mob
ile p
hone
s for
villa
ge
heal
th w
orke
rs, 2
1 ext
erna
l har
d di
sk d
rives
, 11 p
rinte
rs a
nd 4
4 ca
rtrid
ges,
8 pr
ojec
tors
and
scre
ens,
and
12 S
IM c
ard
rout
ers.
Labo
rato
ry e
quip
men
t wer
e al
so p
rocu
red
and
dist
ribut
ed: 3
1 mic
rosc
opes
with
4
for t
he N
atio
nal H
ealth
Lab
orat
ory (
NH
L), 1
0 fo
r Sag
aing
and
17 fo
r Mon
, mic
rosc
ope
with
dig
ital c
amer
a fo
r NH
L, 5-
head
ed m
ultiv
iew
ing
teac
hing
mic
rosc
ope
for N
HL,
lab
equi
pmen
t and
reag
ent f
or
mal
aria
mic
rosc
opy,
cabi
nets
and
ben
ches
for t
he la
bs, 1
3 des
ktop
com
pute
rs a
nd fo
ur p
rinte
rs, a
nd 10
gene
rato
rs fo
r Sag
aing
regi
on.
•D
iffer
ent t
rain
ings
wer
e co
nduc
ted
afte
r the
dist
ribut
ion
of la
b eq
uipm
ent,
nam
ely:
on la
b Q
A an
d m
icro
scop
y for
lab
tech
nici
ans,
on la
b qu
ality
cont
rol c
ross
chec
king
by N
MCP
, pan
el te
stin
g by N
HL,
and
on-t
he-jo
b/re
fresh
er c
ours
es.
cont
inue
d on
nex
t pag
e

62 Annex
Stor
y be
hind
the
num
bers
•A
join
t mon
itorin
g an
d qu
ality
ass
uran
ce s
yste
m w
as e
stab
lishe
d, a
nd m
onito
ring
and
supe
rvisi
on w
ere
cond
ucte
d in
col
labo
ratio
n w
ith N
MCP
and
NH
L. T
he S
OPs
and
man
ual o
n M
icro
scop
y an
d La
bora
tory
QA
wer
e ap
prov
ed b
y th
e U
nion
Min
ister
of t
he m
inist
ries o
f hea
lth (M
OH
s) in
Apr
il 20
17, a
nd th
e m
anua
l was
app
rove
d by
the
MO
HS-
NM
CP in
Sep
tem
ber 2
017
for n
atio
nwid
e us
e. T
hese
m
ater
ials
have
bee
n di
strib
uted
nat
ionw
ide
and
used
for t
rain
ing M
OH
staff
in th
e pr
ojec
t are
as. L
ikew
ise, a
mal
aria
mic
rosc
opy a
lgor
ithm
and
mal
aria
refe
renc
e sli
de p
oste
rs w
ere
deve
lope
d fo
r use
by l
ab
tech
nici
ans n
atio
nwid
e.
•La
b an
d su
rvei
llanc
e ini
tiativ
es u
nder
the p
roje
ct w
ill be
repl
icat
ed b
y NM
CP in
oth
er p
arts
of t
he co
untry
supp
orte
d by
the D
EFEA
T M
alar
ia p
roje
ct o
f Uni
ted
Stat
es A
genc
y for
Inte
rnat
iona
l Dev
elop
men
t.
On
reac
hing
mob
ile a
nd m
igra
nt p
opul
atio
ns in
Cam
bodi
a, th
e La
o PD
R an
d M
yanm
ar•
A m
alar
ia vu
lner
abilit
y and
risk
asse
ssm
ent t
ool (
heal
th fa
cilit
y and
mal
aria
serv
ices
map
ping
, mig
ratio
n an
d m
obilit
y pro
file a
nd m
ovem
ent,
beha
vior
and
awar
enes
s ass
essm
ent)
was
dev
elop
ed an
d us
ed in
pr
ojec
t site
s in
Cam
bodi
a, th
e La
o PD
R, a
nd M
yanm
ar. R
esul
ts w
ere
shar
ed d
urin
g the
Glo
bal M
alar
ia w
eek i
n N
ay P
yi T
aw in
Dec
embe
r 201
7. In
the
Lao
PDR,
trac
king
of M
MP
mov
emen
t was
cond
ucte
d in
targ
et vi
llage
s to
mon
itor t
he tr
end
in m
ovem
ent o
f MM
Ps in
clud
ing f
ores
t and
hos
t com
mun
ities
, and
to id
entif
y the
loca
tions
in w
hich
they
stay
.
•Tr
aini
ng o
n ba
selin
e as
sess
men
t res
earc
h an
d da
ta co
llect
ion
tech
niqu
es w
as co
nduc
ted
in C
ambo
dia,
the
Lao
PDR,
and
Mya
nmar
. Villa
ge h
ealth
volu
ntee
r and
pee
r edu
cato
r tra
inin
g was
also
cond
ucte
d in
the
proj
ect s
ites i
n th
e La
o PD
R an
d M
yanm
ar w
ith 11
0 vo
lunt
eers
par
ticip
atin
g.
•M
obiliz
atio
n of
mig
rant
wor
kers
and
/or t
heir
fam
ily m
embe
rs tr
aine
d as
mal
aria
vol
unte
ers
as a
com
mon
app
roac
h w
as a
dopt
ed a
s ag
reed
with
the
MO
H o
f Cam
bodi
a, th
e La
o PD
R an
d M
yanm
ar.
Volu
ntee
r tra
inin
g and
out
reac
h ac
tiviti
es fo
r MM
Ps h
ave
been
con
duct
ed. T
he tr
aini
ng in
form
ed o
n m
alar
ia ve
ctor
s, sy
mpt
oms,
diag
nosis
, tre
atm
ent,
and
prev
entio
n.
•Th
ere w
ere 1
,956
out
reac
h pa
rtici
pant
s in
the L
ao P
DR
(1,0
82 in
kho
ng d
istric
t and
874
in P
houv
ong d
istric
t) w
hile
in M
yanm
ar th
ere w
ere 1
3,760
par
ticip
ants
in th
e thr
ee p
roje
ct to
wns
hips
. Vol
unte
ers h
ave
carri
ed o
ut IE
C se
ssio
ns in
wor
ksite
s as w
ell a
s pro
ject
site
s in
proj
ect a
reas
. Mal
aria
eve
nts,
cam
paig
ns, a
nd w
orld
Mal
aria
Day
cele
brat
ions
wer
e he
ld to
attra
ct p
ublic
’s at
tent
ion
on th
e w
ork o
f vol
unte
ers
and
avai
labi
lity o
f rap
id d
iagn
ostic
test
serv
ices
and
trea
tmen
t.
•To
pro
mot
e su
stai
nabi
lity a
nd h
arm
oniza
tion
with
nat
iona
l sys
tem
s, sp
ecifi
c effo
rts h
ave
been
mad
e to
ens
ure
that
activ
ities
and
case
dat
a wer
e in
corp
orat
ed in
to th
e re
porti
ng sy
stem
s of N
atio
nal M
alar
ia
Cent
ers.
The v
olun
teer
s pro
vide
d te
stin
g and
trea
tmen
t ons
ite ac
cord
ing t
o na
tiona
l gui
delin
es, w
ith al
l cas
e dat
a for
pat
ient
s tes
ted
and
outc
omes
reco
rded
and
com
mun
icat
ed fo
r inc
lusio
n in
the n
atio
nal
syst
ems f
ollo
win
g exis
ting m
alar
ia p
atie
nt re
gist
er fo
rmat
s and
guid
elin
es fo
r eas
e of i
nteg
ratio
n in
to n
atio
nal r
epor
ting.
Mal
aria
volu
ntee
rs fi
ll in
mon
thly
repo
rt fo
rms a
nd su
bmit
to to
wns
hip
and/
or d
istric
t le
vel h
ealth
team
s, w
ho su
bseq
uent
ly su
bmit
mon
thly
dat
a to
pro
vinc
ial, s
tate
and
subs
eque
ntly
cen
tral le
vel.
•Th
e wor
ksite
pro
ject
in M
yanm
ar d
istrib
uted
long
-last
ing i
nsec
ticid
al n
ets p
rovi
ded
by th
e Nat
iona
l Mal
aria
Con
trol P
rogr
am. T
he p
roje
ct in
the L
ao P
DR
on th
e oth
er h
and,
guid
ed b
y the
reco
mm
enda
tions
of
the
situa
tiona
l ass
essm
ent,
dist
ribut
ed h
amm
ock n
ets,
mos
quito
coi
ls, sp
rays
, and
pat
ches
targ
etin
g for
est-
goer
s and
MM
Ps.
•Te
chni
cal i
nput
to C
ambo
dia’s
MO
H O
pera
tiona
l Gui
delin
es fo
r Mob
ile, M
igra
nt a
nd o
ther
Und
erse
rved
Pop
ulat
ions
in th
e Co
ntex
t of M
alar
ia E
limin
atio
n w
as p
rovi
ded
thro
ugh
the
proj
ect.
Agr
eem
ent
was
also
reac
hed
by th
e M
OH
of t
he th
ree
coun
tries
on
the
defin
ition
of M
MPs
.
•Th
e La
o PD
R’s c
entra
l and
pro
vinc
ial h
ealth
offi
ces c
omm
itted
to su
stai
n (i)
the
train
ing
and
mob
ilizat
ion
of m
obile
trad
ers f
rom
the
Lao
PDR
and
Viet
Nam
who
ply
aro
und
the
dist
rict,
as m
alar
ia p
eer
educ
ator
s and
can
effe
ctiv
ely
reac
h M
MPs
; (ii)
the
iden
tifica
tion
and
train
ing
of th
e ca
m o
r wor
ksite
man
ager
s and
/or d
irect
ors a
s vol
unte
ers,
effec
tive
appr
oach
to e
ngag
e th
e pr
ivat
e se
ctor
in m
alar
ia
prev
entio
n an
d tre
atm
ent;
(iii)
deve
lopm
ent o
f inn
ovat
ive
info
rmat
ion
and
educ
atio
n/be
havi
oral
cha
nge
com
mun
icat
ion
mat
eria
ls fo
r spe
cific
MM
P ta
rget
s, (iv
) sys
tem
atic
iden
tifica
tion
and
mon
itorin
g of
MM
Ps th
roug
h ou
treac
h ac
tiviti
es o
f the
trai
ned
volu
ntee
r hea
lth w
orke
rs; a
nd (v
) dev
elop
men
t and
use
of r
epor
ting f
orm
s for
MM
Ps th
at ca
n in
form
the
natio
nal m
alar
ia re
porti
ng sy
stem
. In
Mya
nmar
, sim
ilar a
ppro
ache
s wer
e co
nduc
ted
whe
re 55
wor
ksite
man
ager
s wer
e en
gage
d as
volu
ntee
rs a
nd vi
llage
hea
lth vo
lunt
eers
in p
lant
atio
ns, g
old
and
jade
min
es tr
aine
d an
d m
obiliz
ed.
•In
Mya
nmar
, the
pro
ject
inte
rven
tion
for M
MPs
in th
e pr
ojec
t site
s will
be su
stai
ned
by th
e G
F.
Box c
ontin
ued

Annex 63
OU
TCO
ME
6: P
ROM
OTI
ON
AN
D P
REVE
NTI
ON
Incr
ease
d ca
paci
ty to
app
ly h
eath
impa
ct a
sses
smen
t to
cons
ider
det
erm
inan
ts o
f hea
lth a
nd c
omm
unic
able
dise
ases
in in
frast
ruct
ure
proj
ects
Out
com
e 6.
1 Inc
reas
ed c
apac
ity to
app
ly h
ealth
impa
ct a
sses
smen
t (H
IA) i
n in
frast
ruct
ure
proj
ects
at c
ount
ry le
vel
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
16Q
2 20
1820
16Q
2 20
181.
Num
ber o
f cou
ntrie
s tha
t sta
rted
to
appl
y HIA
in in
frast
ruct
ure
proj
ects
(L
AO, T
HA)
00
22
Situ
atio
nal a
nalys
is an
d ne
eds a
sses
smen
t
1. N
umbe
r of H
IA c
ount
ry p
rofil
es (C
AM
, LA
O, M
YA, T
HA
, VIE
)0
05
5
2 N
umbe
r of i
nfra
stru
ctur
e pr
ojec
ts th
at
appl
ied
HIA
(Sav
anna
khet
, Muk
daha
n,
Hon
gsa)
00
33
Coun
try H
IA gu
idel
ines
2. N
umbe
r of c
ount
ries w
ith c
ount
ry H
IA
guid
elin
es d
evel
oped
00
33
3. R
egio
nal H
IA fr
amew
ork f
or sp
ecia
l ec
onom
ic zo
nes d
evel
oped
00
11
Capa
city
dev
elop
men
t
4. H
IA tr
aini
ng m
odul
es d
evel
oped
N
oN
oYe
sYe
s
5. N
umbe
r of c
ount
ries w
ith st
aff tr
aine
d in
HIA
00
44
6. H
IA c
urric
ulum
dev
elop
ed fo
r gra
duat
e pu
blic
hea
lth a
nd e
nviro
nmen
tal
prog
ram
s
No
No
Yes
Yes
7. N
umbe
r of c
ount
ries t
hat i
nteg
rate
d H
IA c
urric
ulum
into
grad
uate
pub
lic
heal
th a
nd e
nviro
nmen
tal p
rogr
ams
00
44
8. N
umbe
r of c
ount
ries t
hat s
tarte
d to
off
er H
IA in
grad
uate
pub
lic h
ealth
and
en
viro
nmen
tal p
rogr
ams
00
44
9. R
egio
nal n
etw
ork o
f HIA
exp
erts
and
un
iver
sitie
s est
ablis
hed
00
11
Polic
y and
gove
rnan
ce
10. N
umbe
r of c
ount
ries w
ith c
oste
d H
IA
prop
osal
0
05
5
11. N
umbe
r of c
ount
ries w
ith H
IA p
olic
ies
in p
lace
or d
evel
oped
00
33
12. N
umbe
r of c
ount
ries w
ith in
ters
ecto
ral
coor
dina
tion
on H
IA
00
33
13. N
umbe
r of H
IA p
olic
y brie
fs d
evel
oped
00
22
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
CA
M =
Cam
bodi
a, H
IA =
hea
lth im
pact
ass
essm
ent,
Lao
PDR
= La
o Pe
ople
’s D
emoc
ratic
Rep
ublic
, MYA
= M
yanm
ar, T
HA
= T
haila
nd, V
IE =
Vie
t Nam
.

64 Annex
Stor
y be
hind
the
num
bers
•A
DB
wor
ked
at th
ree
leve
ls (c
ount
ry, r
egio
nal,
with
in A
DB)
to im
prov
e H
IA in
the
regi
on. T
he a
im w
as th
at im
prov
ed H
IA w
ill co
ntrib
ute
to b
ette
r com
mun
ity h
ealth
out
com
es a
s wel
l as h
elp
miti
gate
ve
ctor
-bor
ne d
iseas
es ri
sks i
n la
rge-
scal
e in
frast
ruct
ure
proj
ects
sinc
e m
any m
obile
and
mig
rant
peo
ple
are
invo
lved
in co
nstru
ctio
n sit
es. C
ount
ry-le
vel a
ctiv
ities
conc
entra
ted
in th
e fiv
e G
MS
coun
tries
i.e.
Cam
bodi
a, th
e La
o PD
R, M
yanm
ar, T
haila
nd, a
nd V
iet N
am.
•Si
tuat
iona
l ana
lysis
and
need
s ass
essm
ent o
n H
IA w
ere
cond
ucte
d in
the
five
GM
S co
untri
es. T
hese
coun
tries
are
at va
rious
stag
es o
f HIA
dev
elop
men
t and
pra
ctic
e. A
ll five
coun
tries
hav
e th
e po
tent
ial t
o ha
rnes
s HIA
as p
art o
f the
ir m
alar
ia p
reve
ntio
n an
d co
ntro
l mea
sure
s and
AD
B bu
ilt o
n th
is op
portu
nity
to a
ccel
erat
e H
IA in
the
GM
S.•
Coun
try p
ropo
sals
with
wor
k pl
ans a
nd b
udge
t est
imat
es h
ad b
een
prep
ared
in N
ovem
ber 2
016,
whi
ch d
efine
d ke
y ac
tiviti
es to
ach
ieve
stro
nger
nat
iona
l HIA
pra
ctic
e. B
ased
on
thes
e co
untry
pro
posa
ls,
natio
nal H
IA c
oord
inat
ors,
who
had
wor
ked
clos
ely w
ith c
ount
ry c
ount
erpa
rts, w
ere
recr
uite
d to
ens
ure
timel
y im
plem
enta
tion
of a
ctiv
ities
and
to h
ave
inst
itutio
nal a
rrang
emen
ts in
pla
ce.
•D
evel
opm
ent o
f HIA
cap
acity
at t
he c
ount
ry le
vel r
equi
red
inte
rsec
tora
l coo
rdin
atio
n an
d co
llabo
ratio
n be
twee
n th
e M
OH
, the
Min
istry
of E
nviro
nmen
t (M
oE)
and
othe
r rel
ated
gov
ernm
ent o
ffice
s. A
lthou
gh th
ere w
ere n
o fo
rmal
inst
itutio
nal a
rrang
emen
ts b
etw
een
thes
e con
cern
ed m
inist
ries A
DB
was
able
to fa
cilit
ate c
olla
bora
tion
betw
een
them
. Thi
s ena
bled
bet
ter u
nder
stan
ding
amon
g gov
ernm
ent
stak
ehol
ders
on
the
need
to e
xplic
itly i
nteg
rate
hea
lth in
to e
xistin
g im
pact
ass
essm
ents
(i.e
., env
ironm
ent a
nd so
cial
) and
con
sequ
ently
dro
ve th
e m
omen
tum
for H
IA.
•D
evel
opm
ent o
f HIA
capa
city
also
requ
ired
build
ing t
he sk
ills o
f exis
ting s
taff
both
from
the
publ
ic a
nd p
rivat
e se
ctor
s to
have
HIA
pra
ctiti
oner
s tha
t can
mee
t the
nee
ds fo
r effe
ctiv
e H
IA in
the
long
-ter
m.
Trai
ning
in H
IA fo
cuse
d on
aw
aren
ess c
reat
ion,
know
ledg
e ex
pans
ion
and
skills
dev
elop
men
t with
the
basic
prin
cipl
es a
nd p
ract
ice
of H
IA, t
he a
pplic
atio
n of
tool
s in
a re
alist
ic m
anne
r, ex
plor
ing
deci
sion-
mak
ing
crite
ria a
nd o
ptio
ns fo
r ins
titut
iona
l arra
ngem
ents
bet
wee
n th
e he
alth
and
env
ironm
ent s
ecto
rs in
supp
ort o
f coo
rdin
ated
app
roac
h to
HIA
. Tra
inin
g in
HIA
targ
eted
gov
ernm
ent s
taff
from
MO
H
and
MoE
.•
To g
ener
ate
exam
ples
of g
ood
prac
tices
, cas
e st
udie
s to
dem
onst
rate
HIA
wer
e un
derta
ken
in n
omin
ated
pro
ject
s of v
ario
us se
ctor
s (i.e
., ene
rgy,
road
dev
elop
men
t, sp
ecia
l eco
nom
ic zo
nes [
SEZs
], w
ater
an
d sa
nita
tion,
and
urb
an d
evel
opm
ent)
. HIA
dem
onst
ratio
n id
entifi
ed th
e ne
ed fo
r stro
nger
com
pone
nts o
n co
mm
unity
hea
lth a
nd sa
fety
and
yie
lded
reco
mm
enda
tions
for P
ublic
Hea
lth M
anag
emen
t Pl
an th
at in
clud
e cl
ear s
peci
fic in
dica
tors
to e
nabl
e m
onito
ring a
nd re
porti
ng o
n he
alth
out
com
es a
nd p
ossib
le ri
sks t
o co
mm
unity
hea
lth.
•So
und
polic
y an
d re
gula
tory
fram
ewor
ks w
ere
impo
rtant
con
sider
atio
ns in
stre
ngth
enin
g H
IA p
ract
ice
in th
e G
MS.
Sup
port
was
pro
vide
d fo
r the
dev
elop
men
t of n
atio
nal H
IA g
uide
lines
. Gov
ernm
ent
coun
terp
arts
from
Cam
bodi
a, M
yanm
ar, a
nd V
iet N
am h
ave
com
plet
ed th
eir r
espe
ctiv
e dr
aft H
IA g
uide
lines
, inc
ludi
ng th
e in
tegr
atio
n of
hea
lth in
to th
e en
viro
nmen
t im
pact
ass
essm
ent.
The
Lao
PDR
revi
ewed
10 ye
ars o
f HIA
exp
erie
nce
and
disc
usse
d th
e up
datin
g of e
xistin
g nat
iona
l HIA
guid
elin
e as
wel
l as t
he d
evel
opm
ent o
f sec
tora
l gui
delin
es. T
he L
ao P
DR
com
plet
ed a
dra
ft H
IA gu
idel
ine
spec
ific
for e
nerg
y sec
tor,
spec
ifica
lly fo
r the
rmal
pow
er p
lant
s.•
A G
MS
HIA
fram
ewor
k for
SEZ
s was
pro
duce
d pr
ovid
ing e
nhan
ced
guid
ance
for i
dent
ifyin
g, m
itiga
ting,
and
man
agin
g hea
lth ri
sks a
nd im
pact
s rel
ated
to th
e inc
reas
ed in
dust
rial a
nd ec
onom
ic d
evel
opm
ent
in S
EZs a
nd e
cono
mic
cor
ridor
s. Th
e fra
mew
ork
prom
otes
in-c
ount
ry H
IA p
roce
sses
and
resp
onse
to re
late
d tra
nsbo
unda
ry is
sues
incl
udin
g th
ose
asso
ciat
ed w
ith m
obile
and
mig
rant
wor
ker p
opul
atio
ns
in S
EZs a
nd e
cono
mic
cor
ridor
s. Th
e H
IA fr
amew
ork
posit
ione
d pe
ople
dire
ctly
affe
cted
by
SEZ
deve
lopm
ent a
t the
cen
ter a
s the
y di
rect
ly in
terfa
ce w
ith th
e SE
Z an
d its
ass
ocia
ted
activ
ities
. The
HIA
Fr
amew
ork f
or S
EZs f
or th
e G
MS
can
be a
cces
sed
at h
ttps
://w
ww.
adb.
org/
publ
icat
ions
/hea
lth-i
mpa
ct-a
sses
smen
t-fra
mew
ork-
econ
omic
-zon
es-g
ms
•Co
untry
-spe
cific
HIA
guid
elin
es fo
r SEZ
s for
the L
ao P
DR
and
Thai
land
hav
e bee
n de
velo
ped
base
d on
coun
try re
ques
ts. H
IA fo
cal f
rom
MO
H o
f the
se co
untri
es ar
e now
elev
atin
g the
se gu
idel
ines
at p
olic
y le
vel. M
yanm
ar g
over
nmen
t also
reac
hed
out f
or T
A o
n th
e de
velo
pmen
t of m
anag
emen
t pla
ns fo
r Thi
law
a SE
Z, sp
ecifi
cally
on
the
man
agem
ent o
f haz
ardo
us m
ater
ials,
was
te, v
ecto
r-bo
rne
dise
ases
and
em
erge
ncy p
repa
redn
ess a
nd re
spon
se. T
oget
her w
ith th
e Th
ilaw
a SEZ
Man
agem
ent C
omm
ittee
and
repr
esen
tativ
es fr
om b
usin
ess s
ecto
r, the
man
agem
ent p
lans
wer
e re
view
ed an
d in
the
proc
ess o
f bei
ng
put i
nto
effec
t in
Thila
wa S
EZ. T
he fr
amew
ork w
as al
so ap
plie
d in
an in
tegr
ated
bor
der d
evel
opm
ent p
roje
ct at
one
of t
he b
orde
rs b
etw
een
Mya
nmar
and
the P
eopl
e’s R
epub
lic o
f Chi
na (P
RC),
at th
e Lin
cang
bo
rder
are
a. In
crea
sed
risks
form
impo
rted
mal
aria
from
Mya
nmar
and
the
need
to p
rovi
de h
ealth
serv
ices
to m
igra
nt a
nd m
obile
pop
ulat
ion
grou
ps h
ave
been
iden
tified
.•
Bila
tera
l coo
pera
tion
betw
een
the
Lao
PDR
and
Thai
land
on
trans
boun
dary
hea
lth is
sues
was
ano
ther
impo
rtant
initi
ativ
e. M
OH
and
MoE
from
bot
h co
untri
es in
clud
ing
at p
rovi
ncia
l and
dist
rict l
evel
s ag
reed
to a
join
t hea
lth su
rvei
llanc
e in
rela
tion
to p
roje
cts i
n en
ergy
sect
or i.e
., Hon
gsa
ther
mal
pow
er p
lant
loca
ted
at x
ayab
oury
, Lao
-Nan
, Tha
i bor
der;
and
in S
EZs i
.e. t
he L
ao P
DR
Sava
n-SE
NO
SEZ
and
Th
aila
nd M
ukda
han
SEZ
both
loca
ted
in th
e bo
rder
of t
hese
two
coun
tries
.•
Colla
bora
tion
with
aca
dem
ic in
stitu
tions
has
bee
n in
itiat
ed to
hel
p su
stai
n H
IA c
apac
ity d
evel
opm
ent i
nclu
ding
in e
xpan
ding
HIA
teac
hing
and
rese
arch
in th
e re
gion
. HIA
cur
ricul
a (s
tand
alon
e H
IA, H
IA
in e
nviro
nmen
t im
pact
ass
essm
ent,
HIA
shor
t cou
rse
for h
ealth
, pla
nnin
g or
env
ironm
ent)
wer
e de
velo
ped
with
Cur
tin U
nive
rsity
-wH
O C
olla
bora
ting
Cent
er in
HIA
, whi
ch w
as u
sed
for H
IA c
ertifi
cate
co
urse
offe
ring
in fi
ve G
MS
univ
ersit
ies (
i.e., U
nive
rsity
of H
ealth
Sci
ence
s, U
nive
rsity
of P
ublic
Hea
lth Y
ango
n, M
ahid
ol U
nive
rsity
, Han
oi M
edic
al U
nive
rsity
, Ho
Chi M
inh
City
Uni
vers
ity o
f Med
icin
e an
d Ph
arm
acy)
. The
sam
e ha
s bee
n ad
opte
d to
upd
ate
curre
nt c
urric
ulum
of p
ublic
hea
lth a
nd e
nviro
nmen
t fac
ultie
s of fi
ve G
MS
univ
ersit
ies.
•In
col
labo
ratio
n w
ith C
urtin
Uni
vers
ity-w
HO
Col
labo
ratin
g Ce
nter
in H
IA, a
n H
IA n
etw
ork
was
est
ablis
hed
as a
key
reso
urce
to c
ount
ries o
n gu
idel
ines
and
tool
s, re
sear
ch a
nd p
olic
y de
velo
pmen
t. Th
e ne
twor
k al
so se
rves
as c
olla
bora
tion
and
know
ledg
e sh
arin
g pl
atfo
rm fo
r HIA
pra
ctiti
oner
s. M
ore
info
rmat
ion
abou
t the
HIA
Net
wor
k A
sia P
acifi
c ca
n be
acc
esse
d at
htt
p://w
ww.
hian
etw
orka
siapa
c.co
m/
abou
t/

Annex 65
Out
com
e 6.
2 In
crea
sed
capa
city
to a
pply
HIA
at A
DB
Out
com
e In
dica
tor
2014
Base
line
Stat
us in
Targ
et
Prog
ress
O
utpu
t Ind
icat
or20
14Ba
selin
eSt
atus
inTa
rget
Pr
ogre
ss20
16Q
2 20
1820
16Q
2 20
181.
Num
ber o
f AD
B-su
ppor
ted
infra
stru
ctur
e pr
ojec
ts in
mal
aria
-en
dem
ic a
reas
that
app
lied
HIA
* (C
AM
, MYA
, VIE
)
00
44
1. A
DB
HIA
tool
s dev
elop
ed (
sour
cebo
ok
and
chec
klist
s)N
oYe
sYe
sYe
s
2. A
DB
HIA
trai
ning
mod
ules
dev
elop
edN
oYe
sYe
sYe
s
3. N
umbe
r of A
DB
staff
trai
ned
in H
IA0
3030
30
4. A
DB
HIA
tool
s int
egra
ted
into
AD
B pr
oces
ses
No
No
Yes
Yes
Prog
ress
: A
chie
ved
at le
ast 9
5% o
f tar
get
*Des
ktop
revi
ew
AD
B =
Asia
n D
evel
opm
ent B
ank,
CAM
= C
ambo
dia,
HIA
= h
ealth
impa
ct a
sses
smen
t, M
YA =
Mya
nmar
, VIE
= V
iet N
am.
Stor
y be
hind
the
num
bers
•D
emon
stra
tion
of H
IA w
as o
rigin
ally
con
duct
ed in
four
AD
B-fin
ance
d pr
ojec
ts, n
amel
y Ca
mbo
dia
Rura
l wat
er S
uppl
y an
d Sa
nita
tion
Sect
or, M
anda
lay
Urb
an S
ervi
ces
Impr
ovem
ent P
roje
ct 1,
Ein
du-
kaw
kare
ik R
oad
Impr
ovem
ent,
and
Ho
Chi M
inh
City
was
tew
ater
and
Dra
inag
e Sys
tem
Impr
ovem
ent.
Thes
e pro
ject
s ser
ved
as H
IA ca
se st
udie
s und
erta
ken
in co
ordi
natio
n w
ith go
vern
men
t cou
nter
parts
an
d pr
ojec
t tea
ms.
The
HIA
incl
uded
a s
trong
focu
s on
mal
aria
and
oth
er c
omm
unic
able
dise
ases
. Sco
ping
and
val
idat
ion
of fi
ndin
gs th
roug
h de
sk re
view
(i.e
., lit
erat
ure
and
seco
ndar
y da
ta)
and
site
insp
ectio
ns a
nd in
terv
iew
s, an
d re
port
writ
ing
has b
een
com
plet
ed. T
here
has
incr
ease
d de
man
d am
ong
AD
B pr
ojec
t offi
cers
to c
ondu
ct H
IA fo
r new
pro
ject
s, an
d in
itial
HIA
scop
ing
was
con
duct
ed fo
r Yu
nnan
-Lin
cang
Bor
der E
cono
mic
Coo
pera
tion
Zone
Dev
elop
men
t Pro
ject
, and
Vie
t Nam
Hea
lth H
uman
Res
ourc
e D
evel
opm
ent P
roje
ct 2
. Clo
se c
olla
bora
tion
with
pro
ject
team
s enc
oura
ged
bette
r un
ders
tand
ing a
nd p
ract
ice
of H
IA.
•A
n H
IA s
ourc
eboo
k w
as d
evel
oped
to p
rovi
de te
chni
cal g
uida
nce
and
good
pra
ctic
e ex
ampl
es to
AD
B st
aff o
n ho
w to
opt
imize
com
mun
ity h
ealth
and
saf
ety
in A
DB
proj
ects
. Exp
erie
nces
from
the
dem
onst
ratio
n pr
ojec
ts p
rovi
ded
valu
able
inpu
ts to
the
sour
cebo
ok. T
he so
urce
book
was
pre
sent
ed a
t the
201
8 sp
ring
mee
ting
of th
e M
ultil
ater
al F
inan
cial
Inst
itutio
ns w
orki
ng G
roup
on
Envi
ronm
enta
l So
cial
Sta
ndar
ds. I
t inc
lude
s rec
omm
enda
tions
to in
clud
e m
alar
ia a
nd o
ther
vect
or-b
orne
dise
ase
spec
ific
ques
tions
in ra
pid
envi
ronm
enta
l ass
essm
ent t
ools.
•Fi
nanc
ed fr
om o
ther
sour
ces,
seve
ral H
IA in
trodu
ctor
y cou
rses
wer
e or
gani
zed
for A
DB
staff
and
facu
lty st
aff fr
om C
urtin
Uni
vers
ity an
d ot
her H
IA e
xper
ts se
rved
as re
sour
ce p
erso
ns. L
esso
ns fr
om R
MTF
re
late
d H
IA a
ctiv
ities
wer
e sh
ared
. with
AD
B bu
dget
, an
inte
nsiv
e H
IA c
ours
e Sa
fegu
ards
Dee
p D
ive, L
abor
Stan
dard
s and
Hea
lth Im
pact
Ass
essm
ent h
as b
een
deve
lope
d.

66 Annex
KEY
ACT
IVIT
IES
AN
D M
ILES
TON
ESPR
OG
RESS
ING
TO
WA
RD R
ESU
LTS
OU
TCO
ME
1: LE
AD
ERSH
IPSt
reng
then
ed le
ader
ship
, dec
ision
-mak
ing,
and
acco
unta
bilit
y for
elim
inat
ing m
alar
ia a
nd a
ddre
ssin
g com
mun
icab
le d
iseas
e th
reat
s
2015
2016
2017
Out
com
e 1.1
Incr
ease
d co
mm
itmen
t and
co
llabo
ratio
n fo
r m
alar
ia e
limin
atio
n an
d ad
dres
sing
com
mun
icab
le d
iseas
e th
reat
s
Dev
elop
men
t of m
alar
ia e
limin
atio
n ro
ad m
apPr
esen
tatio
n of
the
mal
aria
elim
inat
ion
road
map
in th
e A
PLM
A S
enio
r O
ffici
als M
eetin
gsM
ilest
one:
Mal
aria
elim
inat
ion
road
map
end
orse
d by
19 h
eads
of
gove
rnm
ent
Mile
ston
e: O
ne a
dditi
onal
mal
aria
elim
inat
ion
road
m
ap e
ndor
sed
by h
ead
of go
vern
men
tA
PLM
A b
ecom
es in
depe
nden
t
Out
com
e 1.2
Impr
oved
us
e of
info
rmat
ion
for d
ecisi
on-m
akin
g an
d ac
coun
tabi
lity f
or
mal
aria
elim
inat
ion
and
addr
essin
g co
mm
unic
able
dise
ase
thre
ats
Dev
elop
men
t of c
once
pt n
ote
and
desig
n of
the
Mal
aria
Elim
inat
ion
Das
hboa
rdM
ilest
one:
Das
hboa
rd c
once
pt
pres
ente
d at
regi
onal
wor
ld H
ealth
O
rgan
izatio
n (w
HO
) mee
tings
Dat
a co
mpi
latio
n fo
r the
Mal
aria
Elim
inat
ion
Das
hboa
rd te
chni
cal a
nnex
Dat
a co
mpi
latio
n fo
r the
Mal
aria
Elim
inat
ion
Das
hboa
rd in
dica
tors
Mile
ston
e: P
artia
l dat
abas
e fo
r the
Mal
aria
El
imin
atio
n D
ashb
oard
dev
elop
edM
ilest
one:
Lea
ders
das
hboa
rd p
roto
type
app
rove
d by
Asia
Pac
ific
Lead
ers M
alar
ia A
llianc
e (A
PLM
A)
Seni
or O
ffici
als M
eetin
g
Cont
inue
dat
a co
mpi
latio
n fo
r the
Mal
aria
Elim
inat
ion
Das
hboa
rd
indi
cato
rsFi
naliz
atio
n of
the
Mal
aria
Elim
inat
ion
Das
hboa
rdPr
esen
tatio
n of
the
Mal
aria
Elim
inat
ion
Das
hboa
rd in
the
2017
APL
MA
Se
nior
Offi
cial
s Mee
ting
Mile
ston
e: A
rrang
emen
ts fo
r das
hboa
rd p
ublic
atio
n m
ade
Revi
ew o
f reg
iona
l fun
ding
mod
els
Dev
elop
men
t of m
alar
ia e
limin
atio
n fra
mew
ork a
nd
cost
ing t
ools
Colle
ctio
n of
dat
a in
cou
ntrie
sM
ilest
one:
Dra
ft fra
mew
ork c
ostin
g too
ls fo
r m
alar
ia e
limin
atio
n de
velo
ped
Cont
inue
col
lect
ion
of d
ata
in c
ount
ries
Dev
elop
men
t of c
ount
ry a
nd su
breg
iona
l inve
stm
ent c
ases
Mile
ston
e: C
ount
ry a
nd su
breg
iona
l inve
stm
ent c
ases
at fi
nal s
tage
s of
deve
lopm
ent p
rodu
ced
Dev
elop
men
t of f
ram
ewor
k, to
ols a
nd c
olle
ctio
n of
dat
a fo
r priv
ate
sect
or b
usin
ess c
ase
stud
ies
Mile
ston
e: D
raft
busin
ess c
ases
for t
he p
rivat
e se
ctor
dev
elop
edD
evel
opm
ent a
nd a
pplic
atio
n of
tool
kit f
or a
sses
sing e
ffici
ency
gain
sM
ilest
one:
Too
lkit
appl
ied
in a
t lea
st o
ne c
ount
ryD
evel
opm
ent o
f fra
mew
ork a
nd c
olle
ctio
n of
dat
a fo
r dev
elop
men
t of
reco
mm
enda
tions
for fi
nanc
ing o
ptio
nsM
ilest
one:
Dra
ft re
port
on re
com
men
datio
ns fo
r fina
ncin
g opt
ions
av
aila
ble
Pres
enta
tion
of in
vest
men
t cas
es, t
oolk
it fo
r ass
essin
g effi
cien
cy ga
ins,
and
reco
mm
enda
tions
for fi
nanc
ing o
ptio
ns in
the
APL
MA
Sen
ior
Offi
cial
s Mee
ting
Mile
ston
e: P
rese
ntat
ion
of th
e fin
anci
ng to
ols a
gree
d w
ith A
PLM
A in
th
e ne
xt A
PLM
A S
enio
r Offi
cial
s Mee
ting
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d

Annex 67
OU
TCO
ME
2: F
INA
NCI
NG
Incr
ease
d fin
anci
ng fo
r mal
aria
elim
inat
ion
and
addr
essin
g com
mun
icab
le d
iseas
e th
reat
s
2015
and
201
620
17Q
1 and
Q2
2018
Out
com
e 2.
1 In
crea
sed
finan
cing
fo
r mal
aria
elim
inat
ion
and
addr
essin
g co
mm
unic
able
dise
ase
thre
ats
Cond
uct o
f con
sulta
tions
on
finan
cing
mal
aria
el
imin
atio
nM
ilest
one:
New
fina
ncin
g mec
hani
sms f
or m
alar
ia
elim
inat
ion
iden
tified
Revi
ew o
f inn
ovat
ive
finan
ce, p
ublic
-priv
ate
partn
ersh
ip m
odel
s, an
d fin
anci
al m
arke
ts p
rodu
cts t
o id
entif
y pot
entia
l mod
els
Dev
elop
men
t of c
once
pt p
aper
for A
DF
regi
onal
he
alth
secu
rity
Mile
ston
e: C
once
pt a
nd e
ligib
ility c
riter
ia fo
r AD
F gr
ant o
n re
gion
al h
ealth
secu
rity s
et a
side
appr
oved
; A
DF
gran
t pro
posa
ls ap
prov
edD
evel
opm
ent o
f pro
ject
for G
MS
heal
th se
curit
y loa
nM
ilest
one:
GM
S he
alth
secu
rity l
oan
appr
oved
Dev
elop
men
t of c
once
pt p
aper
for A
DB
heal
th b
ond
Mile
ston
e: D
raft
conc
ept p
aper
for A
DB
heal
th b
ond
prod
uced
Cont
inue
d di
alog
s on
inno
vativ
e fin
anci
ng fo
r mal
aria
el
imin
atio
n an
d re
spon
se to
com
mun
icab
le d
iseas
e th
reat
sM
ilest
one:
AD
B he
alth
bon
d la
unch
ed
wor
k with
AD
B re
gion
al d
epar
tmen
ts, id
entif
y and
m
ap c
ofina
ncin
g opp
ortu
nitie
s with
GFA
TM a
nd/o
r ot
her d
onor
sO
rgan
ize th
e fir
st c
olla
bora
tion
mee
ting b
etw
een
partn
ers t
o su
ppor
t the
AD
B-G
FATM
mem
oran
dum
of
und
erst
andi
ng, in
clud
ing d
iscus
sion
on c
ofina
ncin
g op
portu
nitie
s, an
d a
deta
iled
desig
n of
ble
nded
fin
anci
ng m
odal
ities
(loa
n bu
ydow
ns, g
rant
s, ris
k tra
nsfe
rs, g
uara
ntee
s)M
ilest
one:
Cofi
nanc
ing o
ppor
tuni
ties a
re id
entifi
ed
and
furth
er d
evel
oped
into
“pro
ject
map
ping
” for
di
scus
sion
with
GFA
TM-A
DB
Mile
ston
e: A
DB-
GFA
TM m
eetin
gs h
eld
with
con
cret
e co
llabo
ratio
n an
d in
vest
men
t prio
ritie
s agr
eed
upon
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d
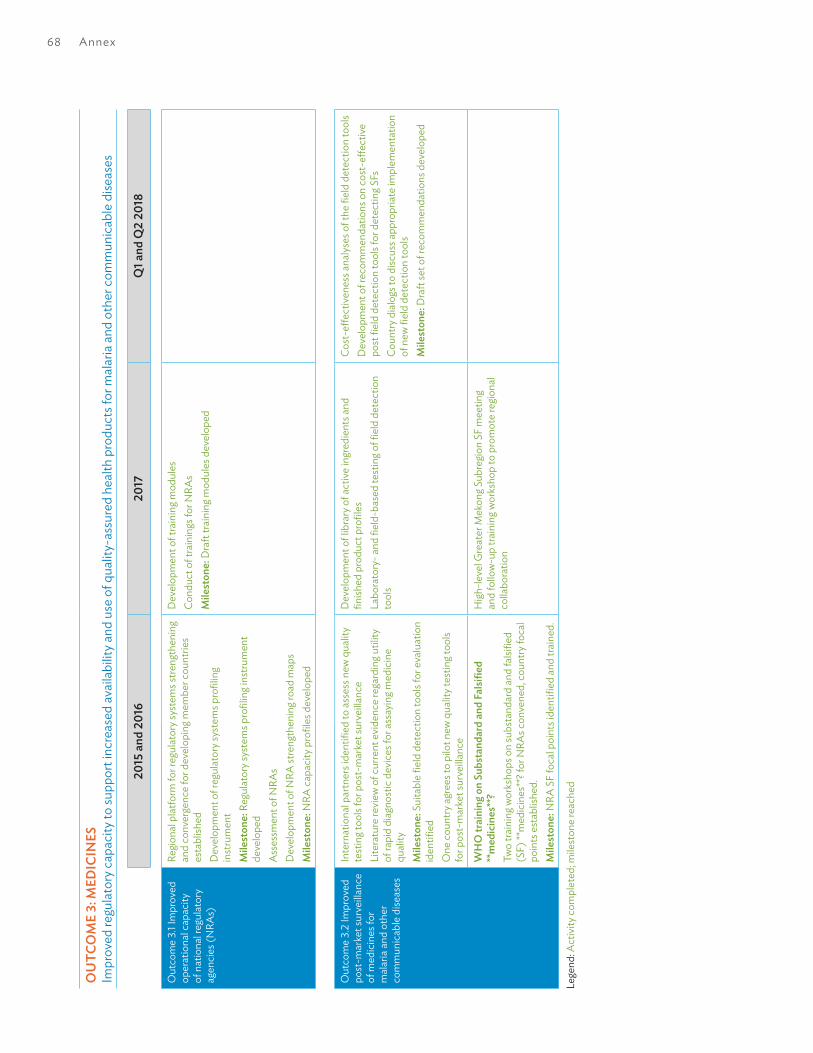
68 Annex
OU
TCO
ME
3: M
EDIC
INES
Impr
oved
regu
lato
ry c
apac
ity to
supp
ort i
ncre
ased
avai
labi
lity a
nd u
se o
f qua
lity-
assu
red
heal
th p
rodu
cts f
or m
alar
ia a
nd o
ther
com
mun
icab
le d
iseas
es
2015
and
201
620
17Q
1 and
Q2
2018
Out
com
e 3.
1 Im
prov
ed
oper
atio
nal c
apac
ity
of n
atio
nal r
egul
ator
y ag
enci
es (N
RAs)
Regi
onal
pla
tform
for r
egul
ator
y sys
tem
s stre
ngth
enin
g an
d co
nver
genc
e fo
r dev
elop
ing m
embe
r cou
ntrie
s es
tabl
ished
Dev
elop
men
t of r
egul
ator
y sys
tem
s pro
filin
g in
stru
men
tM
ilest
one:
Reg
ulat
ory s
yste
ms p
rofil
ing i
nstru
men
t de
velo
ped
Ass
essm
ent o
f NRA
sD
evel
opm
ent o
f NRA
stre
ngth
enin
g roa
d m
aps
Mile
ston
e: N
RA c
apac
ity p
rofil
es d
evel
oped
Dev
elop
men
t of t
rain
ing m
odul
esCo
nduc
t of t
rain
ings
for N
RAs
Mile
ston
e: D
raft
train
ing m
odul
es d
evel
oped
Out
com
e 3.
2 Im
prov
ed
post
-mar
ket s
urve
illanc
e of
med
icin
es fo
r m
alar
ia a
nd o
ther
co
mm
unic
able
dise
ases
Inte
rnat
iona
l par
tner
s ide
ntifi
ed to
ass
ess n
ew q
ualit
y te
stin
g too
ls fo
r pos
t-m
arke
t sur
veilla
nce
Lite
ratu
re re
view
of c
urre
nt e
vide
nce
rega
rdin
g util
ity
of ra
pid
diag
nost
ic d
evic
es fo
r ass
ayin
g med
icin
e qu
ality
Mile
ston
e: S
uita
ble
field
det
ectio
n to
ols f
or e
valu
atio
n id
entifi
edO
ne c
ount
ry a
gree
s to
pilo
t new
qua
lity t
estin
g too
ls fo
r pos
t-m
arke
t sur
veilla
nce
Dev
elop
men
t of l
ibra
ry o
f act
ive
ingr
edie
nts a
nd
finish
ed p
rodu
ct p
rofil
esLa
bora
tory
- and
fiel
d-ba
sed
test
ing o
f fiel
d de
tect
ion
tool
s
Cost
-effe
ctiv
enes
s ana
lyses
of t
he fi
eld
dete
ctio
n to
ols
Dev
elop
men
t of r
ecom
men
datio
ns o
n co
st-e
ffect
ive
post
fiel
d de
tect
ion
tool
s for
det
ectin
g SFs
Coun
try d
ialo
gs to
disc
uss a
ppro
pria
te im
plem
enta
tion
of n
ew fi
eld
dete
ctio
n to
ols
Mile
ston
e: D
raft
set o
f rec
omm
enda
tions
dev
elop
ed
WH
O tr
aini
ng o
n Su
bsta
ndar
d an
d Fa
lsifie
d **
med
icin
es**
?Tw
o tra
inin
g wor
ksho
ps o
n su
bsta
ndar
d an
d fa
lsifie
d (S
F) **
med
icin
es**
? for
NRA
s con
vene
d, c
ount
ry fo
cal
poin
ts e
stab
lishe
d.M
ilest
one:
NRA
SF
foca
l poi
nts i
dent
ified
and
trai
ned.
Hig
h-le
vel G
reat
er M
ekon
g Sub
regi
on S
F m
eetin
g an
d fo
llow
-up
train
ing w
orks
hop
to p
rom
ote
regi
onal
co
llabo
ratio
n
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d

Annex 69
2015
and
201
620
17Q
1 and
Q2
2018
Out
com
e 3.
2 Im
prov
ed
post
-mar
ket s
urve
illanc
e of
med
icin
es fo
r m
alar
ia a
nd o
ther
co
mm
unic
able
dise
ases
Mya
nmar
NRA
stre
ngth
enin
gCo
ordi
natio
n m
eetin
gs h
eld
with
Mya
nmar
NRA
Mile
ston
e: D
raft
5-ye
ar d
evel
opm
ent p
lan
for
phar
mac
eutic
als-
rela
ted
com
pone
nts o
f NRA
agr
eed
Com
pute
rized
med
icin
es re
gist
ratio
n an
d in
form
atio
n sy
stem
inst
alle
d an
d tra
inin
g con
duct
edM
ilest
one:
Tra
inin
g mod
ules
dev
elop
ed a
nd sc
hedu
les
agre
ed w
ith N
RAM
ilest
one:
Reg
istra
tion
and
info
rmat
ion
softw
are
used
in
one
uni
t in
the
NRA
Cond
ucte
d re
view
of p
atie
nt sa
fety
of r
egist
ered
m
edic
ines
, dev
elop
ed im
plem
enta
tion
plan
for
phar
mac
ovig
ilanc
e ce
nter
. Mya
nmar
NRA
join
s wH
O
Colla
bora
tive
Regi
stra
tion
Sche
me,
par
ticip
ates
in
ASE
AN
Join
t Ass
essm
ent P
rogr
amm
e an
d jo
ins w
HO
ph
arm
covi
gila
nce
netw
ork.
Agr
eem
ent w
ith A
ustra
lian
NRA
to u
se p
atie
nt in
form
atio
n le
aflet
s.M
ilest
ones
: (i)
Oth
er A
SEA
N N
RA a
gree
to a
form
al
exch
ange
of i
nfor
mat
ion;
(ii)
Mya
nmar
NRA
join
s the
w
HO
HIN
ARI
syst
em; (
iii) N
ew w
ritte
n SO
Ps a
nd
deci
sion
trees
impl
emen
ted;
(iv)
Sta
ndar
d pa
tient
in
form
atio
n le
aflet
s ado
pted
Mya
nmar
nat
iona
l wor
ksho
p on
SF
med
ical
pro
duct
s he
ld, n
atio
nal S
F co
ordi
natio
n m
echa
nism
ado
pted
an
d M
yanm
ar N
RA in
spec
tors
trai
ned
on S
F re
spon
se.
Mile
ston
e: N
atio
nal c
oord
inat
ion
mec
hani
sm to
co
mba
t SF
med
icin
es a
dopt
ed
Com
pute
rized
info
rmat
ion
syst
em e
xten
ded
and
linke
d to
qua
lity c
ontro
l labo
rato
ry a
nd p
ost-
mar
ketin
g in
spec
tion
mod
ule
NRA
insp
ecto
rs e
quip
ped
and
train
ed to
hav
e el
ectro
nic
acce
ss a
nd re
porti
ng w
ith c
entra
l re
gist
ratio
n da
taba
se.
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d

70 Annex
OU
TCO
ME
4: IN
FORM
ATIO
N S
YSTE
MS
Incr
ease
d us
e of
qua
lity d
ata,
info
rmat
ion
tool
s and
tech
nolo
gies
to im
prov
e m
alar
ia a
nd o
ther
com
mun
icab
le d
iseas
e in
form
atio
n sy
stem
s
2015
and
201
620
17Q
1 and
Q2
2018
Incr
ease
d us
e of
qua
lity
data
, info
rmat
ion
tool
s an
d te
chno
logi
es to
im
prov
e m
alar
ia a
nd
othe
r com
mun
icab
le
dise
ase
info
rmat
ion
syst
ems
Inve
ntor
y of s
urve
illanc
e m
echa
nism
s for
mal
aria
and
co
mm
unic
able
dise
ases
in G
MS
coun
tries
Stak
ehol
der a
nd ID
syst
em m
appi
ng in
MYA
, CA
M,
and
LAO
Set u
p in
tero
pera
bilit
y lab
orat
ory i
n Ca
mbo
dia
Mile
ston
e: R
epor
t on
avai
labl
e ID
s
Stak
ehol
der a
nd ID
syst
em in
vent
ory i
n Vi
et N
amID
tool
kit d
evel
opm
ent
Dev
elop
bus
ines
s cas
e fo
r uni
que
heat
h ID
Mile
ston
e: D
raft
ID to
olki
t ava
ilabl
eM
ilest
one:
Rec
ruitm
ent o
f loc
al a
nd in
tern
atio
nal
cons
ulta
nts t
o su
ppor
t VIE
Dev
elop
guid
elin
es fo
r set
up
of c
ore
heal
th
info
rmat
ion
exch
ange
(HIE
) ele
men
tsPr
ovid
e te
chni
cal r
esou
rces
for t
estin
g exis
ting s
yste
ms
for s
tand
ards
-bas
ed in
tero
pera
bilit
yPr
ovid
e tra
inin
g at p
rovi
ncia
l leve
l for
not
ifiab
le d
iseas
e su
rvei
llanc
e sy
stem
Prov
ide
Ente
rpris
e A
rchi
tect
ure
revi
ew a
nd te
chni
cal
assis
tanc
e in
dat
a st
anda
rds i
nclu
ding
term
inol
ogy
serv
ices
Supp
ort V
IE se
t up
func
tioni
ng h
ealth
stee
ring
com
mitt
eeSu
ppor
t VIE
dev
elop
dat
a sh
arin
g and
secu
rity r
elat
ed
polic
ies
Supp
ort V
IE in
test
ing e
xistin
g sys
tem
s for
in
tero
pera
bilit
y via
HL7
FH
IR C
onne
ctat
hon
Supp
ort V
IE in
iden
tifyi
ng a
nd d
evel
opin
g loc
al/g
rass
ro
ot le
vel I
CT so
lutio
ns vi
a Ep
iHac
k eve
ntSu
ppor
t VIE
in b
uild
ing c
apac
ity in
HL7
stan
dard
s in
clud
ing F
HIR
. Con
duct
a C
onne
ctat
hon
with
na
tiona
l dise
ase
repo
rting
syst
ems t
o es
tabl
ish
prog
ram
min
g int
erfa
ces f
or d
ata
exch
ange
.Su
ppor
t VIE
con
duct
ass
essm
ent o
f fac
ility s
ervi
ce
read
ines
s for
mal
aria
Mile
ston
e: D
raft
data
col
lect
ion
tool
dev
elop
edSu
ppor
t des
ign
of th
e VI
E M
alar
ia M
anag
emen
t Sy
stem
Supp
ort V
IE te
st n
ew m
alar
ia re
porti
ng/in
vest
igat
ion
form
thro
ugh
usin
g a m
obile
app
licat
ion
Mile
ston
e: D
esig
n of
mob
ile a
pp d
evel
oped
Dev
elop
dig
ital h
ealth
stra
tegy
guid
ance
and
dig
ital
heal
th im
pact
fram
ewor
kM
ilest
one:
Dra
ft di
gita
l hea
lth st
rate
gy gu
idan
ce a
nd
digi
tal h
ealth
impa
ct fr
amew
ork i
nclu
des a
n ex
ampl
e of
an
inve
stm
ent c
ase
stra
tegy
for m
alar
ia se
rvic
es a
nd
an im
plem
enta
tion
guid
e.
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d; C
ance
lled
due
to c
hang
e in
par
tner
s’ pr
ojec
t tim
elin
e m
akin
g the
act
ivity
/mile
ston
e un
feas
ible

Annex 71
2015
and
201
620
17Q
1 and
Q2
2018
Incr
ease
d us
e of
qua
lity
data
, info
rmat
ion
tool
s an
d te
chno
logi
es to
im
prov
e m
alar
ia a
nd
othe
r com
mun
icab
le
dise
ase
info
rmat
ion
syst
ems
Brai
nsto
rmin
g mee
ting w
ith E
sri in
Red
land
s, Ca
lifor
nia
Rele
ase
of th
e jo
int w
HO
-AD
B po
licy b
rief o
n th
e ge
ogra
phy o
f Uni
vers
al H
ealth
Cov
erag
e (U
HC
)O
ffici
al L
aunc
h of
the
AeH
IN G
IS L
ab a
nd fi
rst
miss
ion
to M
yanm
arRe
leas
e of
the
high
ly d
iscou
nted
Esr
i GIS
softw
are
bund
les
Rele
ase
of th
e H
IS ge
o-en
ablin
g fra
mew
ork
Firs
t miss
ion
to C
ambo
dia
Firs
t miss
ion
to V
iet N
amFi
naliz
atio
n of
the
HIS
geo-
enab
ling p
ilot p
roje
ct in
M
yanm
arIn
clus
ion
of H
IS ge
o-en
ablin
g int
o th
e H
MIS
m
aste
r pla
n (C
ambo
dia)
and
stra
tegi
c ac
tion
plan
fo
r stre
ngth
enin
g hea
lth in
form
atio
n 20
17–2
021
(Mya
nmar
)Co
mm
on ge
o-re
gist
ry w
orks
hop
in P
hnom
Pen
hM
eetin
g with
Esr
i to
ensu
re th
e su
stai
nabi
lity o
f the
so
ftwar
e bu
ndle
s for
Min
istrie
s of H
ealth
in c
ount
ries
and
rele
ase
of A
cces
sMod
5.0
Rele
ase
of th
e co
mm
on ge
-reg
istry
guid
ance
Conv
ersio
n of
the
AeH
IN G
IS L
ab in
to th
e H
GLC
Fina
lizat
ion
of th
e pi
lot p
roje
ct in
Cam
bodi
aFi
naliz
atio
n of
the
inst
itutio
naliz
atio
n pr
oces
s in
Mya
nmar
Laun
ch o
f the
HG
LC k
now
ledg
e Re
posit
ory
Subn
atio
nal le
vel t
rain
ing o
n ge
ospa
tial d
ata
and
tech
nolo
gies
in C
ambo
dia
and
Mya
nmar
Fina
lizat
ion
of th
e pi
lot p
roje
ct in
Vie
t Nam
Proo
f of c
once
pt d
emon
stra
ting t
hat t
he H
MIS
/HCP
pl
atfo
rm in
Cam
bodi
a ca
n se
rve
as c
omm
on ge
o-re
gist
ryRe
leas
e of
the
new
gene
ratio
n of
Esr
i sof
twar
e bu
ndle
sD
HIS
2 a
s com
mon
geo-
regi
stry
wor
ksho
p co
-or
gani
zed
with
the
Uni
vers
ity o
f Oslo
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d
2015
and
201
620
17Q
1 201
8
Incr
ease
d us
e of
qua
lity
data
, info
rmat
ion
tool
s an
d te
chno
logi
es to
im
prov
e m
alar
ia a
nd
othe
r com
mun
icab
le
dise
ase
info
rmat
ion
syst
ems
Com
pila
tion
and
anal
ysis
of p
reva
lenc
e an
d in
cide
nce
data
for m
alar
ia a
nd d
engu
e an
alyz
edM
ilest
one:
At l
east
one
cou
ntry
with
pre
vale
nce
and
inci
denc
e da
ta fo
r mal
aria
and
den
gue
anal
yzed
Cond
uct o
f tra
inin
gs o
f app
licat
ion
of G
IS-b
ased
vi
sual
izatio
nM
ilest
one:
At l
east
one
cou
ntry
trai
ned
on a
pplic
atio
n of
GIS
-bas
ed vi
sual
izatio
n
Cond
uct o
f tra
inin
gs o
f app
licat
ion
of G
IS-b
ased
vi
sual
izatio
nM
ilest
one:
Six
coun
tries
trai
ned
on a
pplic
atio
n of
GIS
-ba
sed
visu
aliza
tion
Mile
ston
e: A
nalys
is an
d m
appi
ng o
f mal
aria
inci
denc
e da
ta c
ompl
eted
for t
hree
cou
ntrie
s and
den
gue
inci
denc
e da
ta fo
r tw
o co
untri
esD
evel
opm
ent o
f GIS
-bas
ed vi
sual
izatio
n sy
stem
. Sy
stem
has
bee
n de
liver
ed to
nat
iona
l pro
gram
s in
Cam
bodi
a an
d M
yanm
ar w
ith fu
rther
dev
elop
men
t an
d tra
inin
g ong
oing
. Tha
iland
alre
ady h
ave
thei
r ow
n sy
stem
and
disc
ussio
ns a
re o
ngoi
ng a
bout
how
this
can
best
be
com
plem
ente
d w
ith su
ppor
t fro
m A
DB.
Mile
ston
e: A
t lea
st o
ne c
ount
ry w
ith d
raft
plan
for
GIS
-bas
ed vi
sual
izatio
n sy
stem
Dev
elop
men
t of p
olic
y rec
omm
enda
tions
for n
atio
nal
prog
ram
s on
targ
etin
g mal
aria
and
den
gue
surv
eilla
nce
and
cont
rol*
Mile
ston
e: P
olic
y rec
omm
enda
tions
for n
atio
nal
prog
ram
s on
targ
etin
g mal
aria
and
den
gue
surv
eilla
nce
and
cont
rol a
re d
rafte
d*
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d
*Pol
icy r
ecom
men
datio
ns a
re b
eing
dev
elop
ed c
urre
ntly
and
will
be fi
naliz
ed a
s pop
ulat
ion
mov
emen
t res
ults
are
shar
ed a
nd d
iscus
sed
with
MO
H st
aff. A
dditi
onal
fund
ing s
uppo
rt ha
s bee
n se
cure
d by
M
ORU
to c
ompl
ete
this
wor
k.
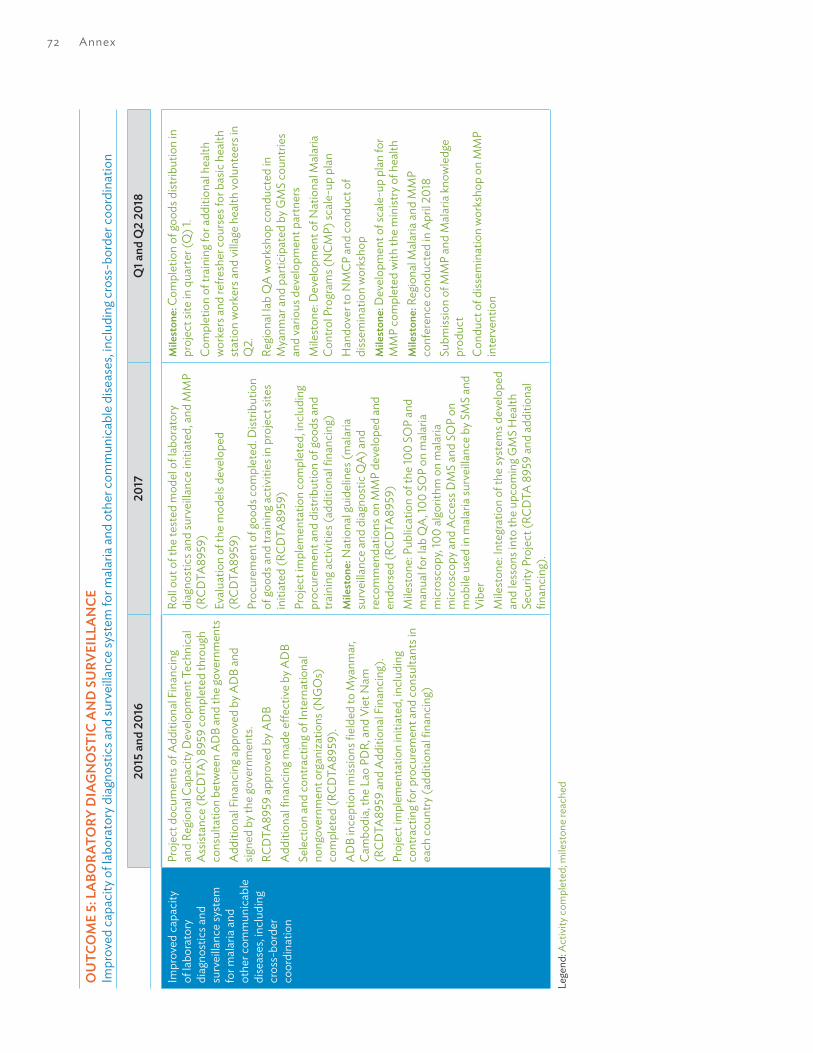
72 Annex
OU
TCO
ME
5: L
ABO
RATO
RY D
IAG
NO
STIC
AN
D S
URV
EILL
AN
CEIm
prov
ed c
apac
ity o
f lab
orat
ory d
iagn
ostic
s and
surv
eilla
nce
syst
em fo
r mal
aria
and
oth
er c
omm
unic
able
dise
ases
, incl
udin
g cro
ss-b
orde
r coo
rdin
atio
n
2015
and
201
620
17Q
1 and
Q2
2018
Impr
oved
cap
acity
of
labo
rato
ry
diag
nost
ics a
nd
surv
eilla
nce
syst
em
for m
alar
ia a
nd
othe
r com
mun
icab
le
dise
ases
, incl
udin
g cr
oss-
bord
er
coor
dina
tion
Proj
ect d
ocum
ents
of A
dditi
onal
Fin
anci
ng
and
Regi
onal
Cap
acity
Dev
elop
men
t Tec
hnic
al
Ass
istan
ce (R
CDTA
) 895
9 co
mpl
eted
thro
ugh
cons
ulta
tion
betw
een
AD
B an
d th
e go
vern
men
tsA
dditi
onal
Fin
anci
ng a
ppro
ved
by A
DB
and
signe
d by
the
gove
rnm
ents
.RC
DTA
8959
app
rove
d by
AD
BA
dditi
onal
fina
ncin
g mad
e eff
ectiv
e by
AD
BSe
lect
ion
and
cont
ract
ing o
f Int
erna
tiona
l no
ngov
ernm
ent o
rgan
izatio
ns (N
GO
s)
com
plet
ed (R
CDTA
8959
).A
DB
ince
ptio
n m
issio
ns fi
elde
d to
Mya
nmar
, Ca
mbo
dia,
the
Lao
PDR,
and
Vie
t Nam
(R
CDTA
8959
and
Add
ition
al F
inan
cing
).Pr
ojec
t im
plem
enta
tion
initi
ated
, incl
udin
g co
ntra
ctin
g for
pro
cure
men
t and
con
sulta
nts i
n ea
ch c
ount
ry (a
dditi
onal
fina
ncin
g)
Roll o
ut o
f the
test
ed m
odel
of l
abor
ator
y di
agno
stic
s and
surv
eilla
nce
initi
ated
, and
MM
P (R
CDTA
8959
)Ev
alua
tion
of th
e m
odel
s dev
elop
ed
(RCD
TA89
59)
Proc
urem
ent o
f goo
ds c
ompl
eted
. Dist
ribut
ion
of go
ods a
nd tr
aini
ng a
ctiv
ities
in p
roje
ct si
tes
initi
ated
(RCD
TA89
59)
Proj
ect i
mpl
emen
tatio
n co
mpl
eted
, incl
udin
g pr
ocur
emen
t and
dist
ribut
ion
of go
ods a
nd
train
ing a
ctiv
ities
(add
ition
al fi
nanc
ing)
Mile
ston
e: N
atio
nal g
uide
lines
(mal
aria
su
rvei
llanc
e an
d di
agno
stic
QA)
and
re
com
men
datio
ns o
n M
MP
deve
lope
d an
d en
dors
ed (R
CDTA
8959
)M
ilest
one:
Pub
licat
ion
of th
e 10
0 SO
P an
d m
anua
l for
lab
QA
, 100
SO
P on
mal
aria
m
icro
scop
y, 10
0 al
gorit
hm o
n m
alar
ia
mic
rosc
opy a
nd A
cces
s DM
S an
d SO
P on
m
obile
use
d in
mal
aria
surv
eilla
nce
by S
MS
and
Vibe
rM
ilest
one:
Inte
grat
ion
of th
e sy
stem
s dev
elop
ed
and
less
ons i
nto
the
upco
min
g GM
S H
ealth
Se
curit
y Pro
ject
(RCD
TA 8
959
and
addi
tiona
l fin
anci
ng).
Mile
ston
e: C
ompl
etio
n of
good
s dist
ribut
ion
in
proj
ect s
ite in
qua
rter (
Q) 1
.Co
mpl
etio
n of
trai
ning
for a
dditi
onal
hea
lth
wor
kers
and
refre
sher
cou
rses
for b
asic
hea
lth
stat
ion
wor
kers
and
villa
ge h
ealth
volu
ntee
rs in
Q
2.Re
gion
al la
b Q
A w
orks
hop
cond
ucte
d in
M
yanm
ar a
nd p
artic
ipat
ed b
y GM
S co
untri
es
and
vario
us d
evel
opm
ent p
artn
ers
Mile
ston
e: D
evel
opm
ent o
f Nat
iona
l Mal
aria
Co
ntro
l Pro
gram
s (N
CMP)
scal
e-up
pla
nH
ando
ver t
o N
MCP
and
con
duct
of
diss
emin
atio
n w
orks
hop
Mile
ston
e: D
evel
opm
ent o
f sca
le-u
p pl
an fo
r M
MP
com
plet
ed w
ith th
e m
inist
ry o
f hea
lthM
ilest
one:
Reg
iona
l Mal
aria
and
MM
P co
nfer
ence
con
duct
ed in
Apr
il 201
8Su
bmiss
ion
of M
MP
and
Mal
aria
know
ledg
e pr
oduc
tCo
nduc
t of d
issem
inat
ion
wor
ksho
p on
MM
P in
terv
entio
n
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d
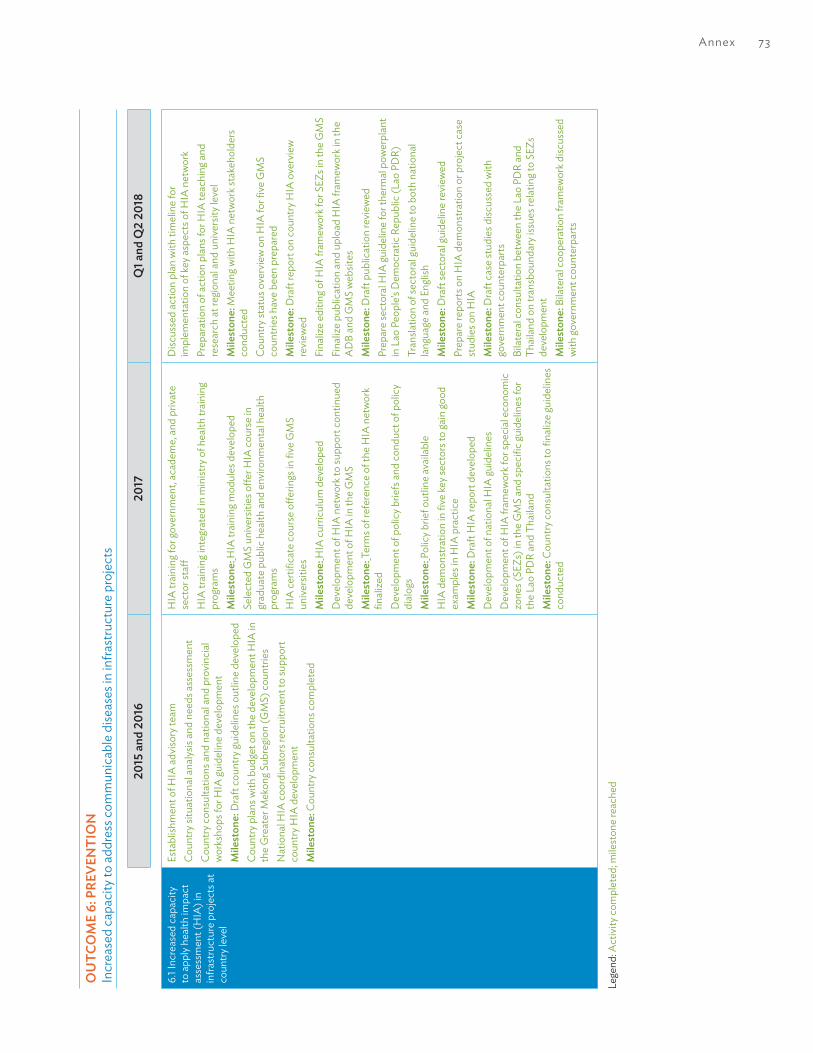
Annex 73
OU
TCO
ME
6: P
REVE
NTI
ON
Incr
ease
d ca
paci
ty to
add
ress
com
mun
icab
le d
iseas
es in
infra
stru
ctur
e pr
ojec
ts
2015
and
201
620
17Q
1 and
Q2
2018
6.1 I
ncre
ased
cap
acity
to
app
ly h
ealth
impa
ct
asse
ssm
ent (
HIA
) in
infra
stru
ctur
e pr
ojec
ts a
t co
untry
leve
l
Esta
blish
men
t of H
IA a
dviso
ry te
amCo
untry
situ
atio
nal a
nalys
is an
d ne
eds a
sses
smen
tCo
untry
con
sulta
tions
and
nat
iona
l and
pro
vinc
ial
wor
ksho
ps fo
r HIA
guid
elin
e de
velo
pmen
tM
ilest
one:
Dra
ft co
untry
guid
elin
es o
utlin
e de
velo
ped
Coun
try p
lans
with
bud
get o
n th
e de
velo
pmen
t HIA
in
the
Gre
ater
Mek
ong S
ubre
gion
(GM
S) c
ount
ries
Nat
iona
l HIA
coo
rdin
ator
s rec
ruitm
ent t
o su
ppor
t co
untry
HIA
dev
elop
men
tM
ilest
one:
Cou
ntry
con
sulta
tions
com
plet
ed
HIA
trai
ning
for g
over
nmen
t, ac
adem
e, a
nd p
rivat
e se
ctor
staff
HIA
trai
ning
inte
grat
ed in
min
istry
of h
ealth
trai
ning
pr
ogra
ms
Mile
ston
e: H
IA tr
aini
ng m
odul
es d
evel
oped
Sele
cted
GM
S un
iver
sitie
s offe
r HIA
cou
rse
in
grad
uate
pub
lic h
ealth
and
env
ironm
enta
l hea
lth
prog
ram
sH
IA c
ertifi
cate
cou
rse
offer
ings
in fi
ve G
MS
univ
ersit
ies
Mile
ston
e: H
IA c
urric
ulum
dev
elop
edD
evel
opm
ent o
f HIA
net
wor
k to
supp
ort c
ontin
ued
deve
lopm
ent o
f HIA
in th
e G
MS
Mile
ston
e: T
erm
s of r
efer
ence
of t
he H
IA n
etw
ork
final
ized
Dev
elop
men
t of p
olic
y brie
fs a
nd c
ondu
ct o
f pol
icy
dial
ogs
Mile
ston
e: P
olic
y brie
f out
line
avai
labl
eH
IA d
emon
stra
tion
in fi
ve ke
y sec
tors
to ga
in go
od
exam
ples
in H
IA p
ract
ice
Mile
ston
e: D
raft
HIA
repo
rt de
velo
ped
Dev
elop
men
t of n
atio
nal H
IA gu
idel
ines
Dev
elop
men
t of H
IA fr
amew
ork f
or sp
ecia
l eco
nom
ic
zone
s (SE
Zs) i
n th
e G
MS
and
spec
ific
guid
elin
es fo
r th
e La
o PD
R an
d Th
aila
ndM
ilest
one:
Cou
ntry
con
sulta
tions
to fi
naliz
e gu
idel
ines
co
nduc
ted
Disc
usse
d ac
tion
plan
with
tim
elin
e fo
r im
plem
enta
tion
of ke
y asp
ects
of H
IA n
etw
ork
Prep
arat
ion
of a
ctio
n pl
ans f
or H
IA te
achi
ng a
nd
rese
arch
at r
egio
nal a
nd u
nive
rsity
leve
lM
ilest
one:
Mee
ting w
ith H
IA n
etw
ork s
take
hold
ers
cond
ucte
dCo
untry
stat
us o
verv
iew
on
HIA
for fi
ve G
MS
coun
tries
hav
e be
en p
repa
red
Mile
ston
e: D
raft
repo
rt on
cou
ntry
HIA
ove
rvie
w
revi
ewed
Fina
lize
editi
ng o
f HIA
fram
ewor
k for
SEZ
s in
the
GM
SFi
naliz
e pu
blic
atio
n an
d up
load
HIA
fram
ewor
k in
the
AD
B an
d G
MS
web
sites
Mile
ston
e: D
raft
publ
icat
ion
revi
ewed
Prep
are
sect
oral
HIA
guid
elin
e fo
r the
rmal
pow
erpl
ant
in L
ao P
eopl
e’s D
emoc
ratic
Rep
ublic
(Lao
PD
R)Tr
ansla
tion
of se
ctor
al gu
idel
ine
to b
oth
natio
nal
lang
uage
and
Eng
lish
Mile
ston
e: D
raft
sect
oral
guid
elin
e re
view
edPr
epar
e re
ports
on
HIA
dem
onst
ratio
n or
pro
ject
cas
e st
udie
s on
HIA
Mile
ston
e: D
raft
case
stud
ies d
iscus
sed
with
go
vern
men
t cou
nter
parts
Bila
tera
l con
sulta
tion
betw
een
the
Lao
PDR
and
Thai
land
on
trans
boun
dary
issu
es re
latin
g to
SEZs
de
velo
pmen
tM
ilest
one:
Bila
tera
l coo
pera
tion
fram
ewor
k disc
usse
d w
ith go
vern
men
t cou
nter
parts
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d

74 Annex
2015
and
201
620
17Q
1 and
Q2
2018
6.2
Incr
ease
d ca
paci
ty to
ap
ply H
IA a
t AD
BPr
elim
inar
y disc
ussio
ns w
ith A
DB
man
agem
ent t
o ad
opt H
IA in
AD
B-su
ppor
ted
infra
stru
ctur
e pr
ojec
tsD
raft
prop
osed
cha
nges
to A
DB’
s env
ironm
enta
l and
so
cial
impa
ct a
sses
smen
t too
l to
inco
rpor
ate
mal
aria
an
d ot
her c
omm
unic
able
dise
ase
thre
ats
Mile
ston
e: In
tern
al c
onsu
ltatio
ns sc
hedu
led
Incl
usio
n of
hea
lth in
the
exist
ing r
apid
env
ironm
ent
asse
ssm
ent
Mile
ston
e: U
pdat
ed c
heck
list d
iscus
sed
with
sect
or
grou
pD
evel
opm
ent o
f HIA
trai
ning
mod
ules
for t
rain
ing o
f A
DB
staff
HIA
trai
ning
for A
DB
staff
thro
ugh
exist
ing t
rain
ing
prog
ram
s suc
h as
the
stan
dard
pov
erty
and
soci
al
anal
ysis
train
ing
Mile
ston
e: O
utlin
e of
HIA
trai
ning
mod
ules
disc
usse
d
Org
anize
HIA
dem
onst
ratio
n in
key s
ecto
rs to
pro
vide
ev
iden
ce in
HIA
pra
ctic
eD
evel
opm
ent o
f HIA
repo
rt w
ith p
ublic
hea
lth
man
agem
ent p
lan
Mile
ston
e: D
raft
HIA
repo
rt di
scus
sed
Dev
elop
men
t of H
IA so
urce
book
to se
rve
as gu
idan
ce
in H
IA p
ract
ice
for A
DB
staff
Inco
rpor
ate
to d
raft
sour
cebo
ok go
od p
ract
ice
and
othe
r exp
erie
nces
from
the
HIA
dem
onst
ratio
nM
ilest
one:
Dra
ft H
IA so
urce
book
disc
usse
dPl
an fo
r add
ition
al H
IA tr
aini
ng fo
r AD
B st
aff in
clud
ing
for r
esid
ent m
issio
n st
aff in
201
8M
ilest
one:
AD
B fu
nds f
or a
dditi
onal
HIA
trai
ning
ap
prov
ed
Fina
lize
editi
ng o
f HIA
sour
cebo
okFi
naliz
e pu
blic
atio
n an
d up
load
HIA
Sou
rceb
ook i
n th
e A
DB
and
GM
S w
ebsit
esM
ilest
one:
Dra
ft pu
blic
atio
n re
view
ed b
y AD
B m
anag
emen
tFi
naliz
e H
IA E
-lear
ning
mat
eria
ls fo
r AD
B k-
Lear
n sit
e in
clud
ing v
ideo
and
aud
io o
ptio
nsM
ilest
one:
E-le
arni
ng m
ater
ials
disc
usse
d w
ith
k-Le
arn
team
Cond
uct H
IA in
trodu
ctor
y cou
rse
for A
DB
staff
Dev
elop
HIA
trai
ning
pro
gram
for f
urth
er A
DB
staff
tra
inin
gM
ilest
one:
AD
B bu
dget
disc
usse
dPr
esen
tatio
n of
HIA
initi
ativ
es a
t the
sprin
g mee
ting o
f M
ultil
ater
al F
inan
cial
Inst
itutio
ns w
orki
ng G
roup
on
Envi
ronm
enta
l and
Soc
ial S
afeg
uard
sM
ilest
one:
AD
B sa
fegu
ards
staff
agr
ee o
n th
e pr
esen
tatio
n m
ater
ial
Lege
nd: A
ctiv
ity c
ompl
eted
; mile
ston
e re
ache
d

Annex 75
Annex B: Glossary of Results-Based Framework Terms
Impact Changes in conditionsMillennium Development Goals (MDGs), health, social, economic, cultural, civil society, environmental, political.
Positive and negative long-term effects on identifiable population groups produced by a development intervention, directly or indirectly, intended or unintended.
Outcome Changes in capacity and performance of the primary duty-bearersChanges in behaviors and attitudes, social action, viability, institutional, policy formulation, decision-making, norms, knowledge, efficiency, competencies, opinions, standards. Achieved though the combination of RMTF investments.
The changes in institutional performance or behavior among individuals or groups that occur between the completion of outputs and the achievement of goals.
Output What implementers produceGoods and services, change in skills and capabilities, systems, evaluations, new products, reports, publications produced. Outputs are linked to project outputs.
The changes in skills or abilities, or the availability of new products and services that result from the completion of activities within a development intervention.
Activities What implementers doDevelop curriculum, train, evaluate, recruit, procure, facilitate, develop action plans, work with media, etc.
Actions taken or work performed through which inputs, such as funds, technical assistance and other types of resources are mobilized to produce specific outputs.
Inputs What stakeholders invest inHuman or financial resources, personnel, equipment, technology, time.
Milestone Sets out how much of a target or what specific steps toward that target will be complete by specific dates.
References:
International Labour Office. 2011. Applying Results-Based Management in the International Labour Organization, A Guidebook, Version 2. Geneva.
United Nations Development Group. 2011. Results-based Management Handbook. New York.

76 Annex
Ann
ex C
: Gen
der D
imen
sions
CAM
BOD
IA (r
eflec
ts w
ork
unde
r the
Com
mun
icab
le D
iseas
e Co
ntro
l (CD
C) 2
and
CD
C2-A
dditi
onal
Fin
anci
ng)
1. To
enh
ance
the
oppo
rtun
ities
and
cont
ribut
ion
of fe
mal
e st
aff in
CD
C sy
stem
s and
to im
prov
e ge
nder
ana
lysis
in re
gion
al C
DC
syst
ems
Prom
ote
the
incr
ease
d tra
inin
g of w
omen
in
CDC
surv
eilla
nce
and
resp
onse
Year
Tota
l num
ber o
f RRT
/CD
C st
affN
umbe
r of f
emal
e RR
T/CD
C st
affN
umbe
r of t
rain
ed
staff
Num
ber o
f tra
ined
fem
ale
staff
Perc
enta
ge o
f tr
aine
d fe
mal
e st
aff
2015
1,328
383
978
318
83
2016
1,486
423
1,242
381
90
Q3
2017
1,569
448
1,373
412
92RR
T=ra
pid
resp
onse
team
, CD
C =
com
mun
icab
le d
iseas
e co
ntro
lSo
urce
: Pro
ject
Dat
a Co
llect
ion
Form
of e
ach
proj
ect p
rovi
nce
Proa
ctiv
ely t
arge
t fem
ale
labo
rato
ry st
aff fo
r tra
inin
gA
ll (75
/75)
fem
ale
labo
rato
ry st
aff fr
om 12
pro
vinc
es in
clud
ing P
reah
Vih
ear w
ere
train
ed o
n th
e us
e of
new
equ
ipm
ent a
nd n
ew ra
pid
test
s.In
Pre
ah V
ihea
r pro
vinc
e, o
ne re
fresh
er tr
aini
ng o
n m
icro
scop
y and
clin
ical
man
agem
ent w
as p
rovi
ded
to 3
8 la
bora
tory
staff
(nin
e ar
e fe
mal
e).
Enco
urag
e an
d m
onito
r the
hiri
ng o
f new
fe
mal
e st
affTh
ere
was
an
incr
ease
in th
e pe
rcen
tage
of n
ew fe
mal
e CD
C/m
alar
ia st
aff, f
rom
44%
in 2
012
to 5
4% in
201
6.So
urce
: Pro
ject
Dat
a Co
llect
ion
Form
of e
ach
proj
ect p
rovi
nce
2011
–201
7
Colle
ct sp
ecifi
c se
x-di
sagg
rega
ted
data
in a
ll su
rvei
llanc
e fo
rms a
nd re
porti
ng d
ocum
enta
tion
Dat
a fo
r the
com
mun
icab
le d
iseas
e su
rvei
llanc
e sy
stem
, incl
udin
g for
Sev
ere
Acu
te R
espi
rato
ry In
fect
ion,
Influ
enza
-like
Illn
ess a
nd m
alar
ia, a
re a
ll se
x-di
sagg
rega
ted.
Out
brea
k dat
a, m
alar
ia su
perv
ision
che
cklis
t, tra
inin
g and
/or w
orks
hop,
hou
seho
ld su
rvey
and
villa
ge d
emog
raph
ic a
sses
smen
t re
sults
are
sex-
disa
ggre
gate
d, a
s app
ropr
iate
.
Reac
h m
ore
wom
en, in
clud
ing i
n th
e G
reat
er
Mek
ong S
ubre
gion
(GM
S) a
nnua
l join
t rev
iew
of
nat
iona
l mal
aria
pol
icie
s and
stra
tegi
es
Nat
iona
l mal
aria
stra
tegi
c pl
an h
as b
een
deve
lope
d fo
r 201
6–20
20. I
nter
vent
ions
for w
omen
and
chi
ldre
n in
the
plan
incl
udes
the
prov
ision
of b
ed
nets
to w
omen
with
chi
ldre
n un
der 5
year
s of a
ge, t
he p
rovi
sion
of a
nten
atal
mal
aria
scre
enin
g for
wom
en a
t hea
lth c
ente
r and
villa
ge le
vel, a
nd
train
ings
on
the
usag
e of
long
-last
ing i
nsec
ticid
al n
ets f
or w
omen
.
Inco
rpor
ate
gend
er-r
elat
ed c
onte
nt in
to c
ur-
ricul
um tr
aini
ng m
odul
es, h
uman
reso
urce
de
velo
pmen
t pla
ns a
nd c
ross
-bor
der a
ctiv
ities
The
Gen
der M
ains
tream
ing S
trate
gy a
nd A
ctio
n Pl
an 2
014–
2018
of M
inist
ry o
f Hea
lth (M
OH
), Ca
mbo
dia
was
dev
elop
ed fo
r stre
ngth
enin
g com
-m
unic
able
and
non
-com
mun
icab
le se
rvic
es, a
nd a
dvoc
ates
for t
he in
clus
ion
of ge
nder
dim
ensio
n in
add
ress
ing t
hese
dise
ases
.A
ll sev
en C
DC/
mal
aria
trai
ning
cur
ricul
a an
d IE
C m
ater
ials
incl
uded
gend
er c
onte
nts.
Hea
lth w
orkf
orce
Dev
elop
men
t Pla
n 20
16–2
020
endo
rsed
by M
OH
on
1 Mar
ch 2
016
incl
uded
gend
er-r
elat
ed c
onte
nt.
2. T
o im
prov
e re
spon
siven
ess o
f CD
C to
gen
der a
nd e
thni
c iss
ues i
n ta
rget
ed d
istric
ts o
r pro
vinc
es a
nd to
incr
ease
the
part
icip
atio
n an
d aw
aren
ess o
f wom
en in
CD
C pr
even
tion
in p
roje
ct
loca
tions
Colle
ct, u
se, a
nd a
naly
ze se
x-di
sagg
rega
ted
data
in
com
mun
ity-b
ased
CD
C as
sess
men
ts a
nd
plan
s
Dem
ogra
phic
ass
essm
ents
bet
wee
n 20
13 a
nd 2
014
for 1
80 m
odel
hea
lthy v
illage
s use
d an
d an
alyz
ed se
x-di
sagg
rega
ted
data
. In
2014
, the
bas
elin
e su
rvey
col
lect
ed se
x-di
sagg
rega
ted
data
.D
ata
colle
ctio
n fo
rms w
ith c
ompo
nent
s for
gend
er a
nd in
dige
nous
peo
ple
wer
e de
velo
ped
and
intro
duce
d to
all p
rovi
ncia
l impl
emen
tatio
n ag
en-
cies
for c
ompl
etio
n.In
stitu
tiona
l and
trai
ning
dat
a fro
m 2
011 t
o 20
17 a
re d
isagg
rega
ted
by se
x and
eth
nici
ty.
Proa
ctiv
ely t
rain
wom
en a
s villa
ge h
ealth
volu
n-te
ers a
nd/o
r wor
kers
A to
tal o
f 2,9
25 o
ut o
f 6,3
83 (4
6%) f
emal
e he
alth
volu
ntee
rs w
ere
train
ed si
nce
2012
.
Ensu
re th
at a
t lea
st h
alf o
f new
ly se
lect
ed vi
llage
he
alth
volu
ntee
rs a
nd/o
r wor
kers
in d
istric
ts a
re
fem
ale
Ove
r the
CD
C2 a
nd C
DC2
-Add
ition
al F
inan
cing
(AF)
pro
ject
per
iod,
11 p
roje
ct p
rovi
nces
hav
e re
crui
ted
616
(47%
) new
fem
ale
villa
ge h
ealth
wor
k-er
s out
of t
he 1,
298
new
ly re
crui
ted
villa
ge h
ealth
wor
kers
.

Annex 77
Syst
emat
ical
ly in
clud
e ge
nder
-spe
cific
issu
es
into
the
train
ing a
ctiv
ities
impl
emen
ted
by th
e pr
ojec
t
Ther
e w
ere
two
train
ings
on
gend
er in
Qua
rter (
Q) 2
201
7, on
e in
Rat
anak
iri p
rovi
nce
with
47
parti
cipa
nts (
22 fe
mal
e), a
nd o
ne in
Stu
ng T
reng
pr
ovin
ce w
ith 4
4 pa
rtici
pant
s (23
fem
ale)
.In
Q3
2017
, tw
o tra
inin
gs o
n ge
nder
and
/or i
ndig
enou
s peo
ple
and
on C
DC
wer
e co
nduc
ted,
one
in P
reah
Vih
ear p
rovi
nce
and
the
othe
r in
Mon
-du
lkiri
pro
vinc
e.
Inte
grat
e ge
nder
issu
es a
nd ta
rget
ed a
ctio
ns fo
r w
omen
in jo
int a
ctio
n pl
ans f
or m
alar
ia p
reve
n-tio
n an
d re
spon
se in
the
bord
er p
rovi
nces
Join
t act
ion
plan
was
dev
elop
ed in
Q2
2017
. Cro
ss-b
orde
r mee
ting w
ith n
eigh
borin
g cou
ntry
of P
reah
Vih
ear w
as o
rgan
ized
on 19
–20
June
201
7. G
ende
r iss
ues p
erta
inin
g to
join
t act
ion
plan
hav
e no
t bee
n id
entifi
ed.
3. T
o en
hanc
e th
e ge
nder
aw
aren
ess a
nd re
spon
siven
ess o
f CD
C pr
ojec
t man
agem
ent
Tailo
r the
gend
er a
ctio
n pl
an to
nat
iona
l and
pr
ovin
cial
con
text
sG
ende
r Act
ion
Plan
201
2–20
15 w
as d
evel
oped
and
app
rove
d by
MO
H o
n 4
Janu
ary 2
013.
Thi
s has
bee
n im
plem
ente
d at
bot
h ce
ntra
l and
pro
vin-
cial
leve
ls sin
ce 2
012,
and
in P
reah
Vih
ear P
rovi
nce
in Q
4 20
15.
Inte
grat
e ge
nder
-rel
ated
act
iviti
es a
nd b
udge
t al
loca
tion
in a
nnua
l ope
ratio
nal p
lans
In th
e 20
17 a
nnua
l ope
ratio
nal p
lan,
five
targ
eted
pro
vinc
es a
lloca
ted
budg
et fo
r gen
der a
ctiv
ities
.
App
oint
gend
er re
pres
enta
tives
in p
rogr
am
man
agem
ent u
nit o
r pro
ject
impl
emen
ting u
nit/
SC
Prov
inci
al a
nd n
atio
nal g
ende
r/ind
igen
ous p
eopl
e fo
cal p
oint
s hav
e be
en va
lidat
ed, u
pdat
ed a
nd tr
aine
d in
all 1
2 pr
ojec
t pro
vinc
es. T
here
are
cur
-re
ntly
17 ge
nder
and
indi
geno
us p
eopl
e fo
cal p
oint
s and
7 o
f the
m a
re w
omen
.
Recr
uit a
soci
al d
evel
opm
ent s
peci
alist
to c
over
ge
nder
issu
es/g
ende
r act
ion
plan
impl
emen
ta-
tion
One
soci
al d
evel
opm
ent e
xper
t and
one
nat
iona
l soc
ial d
evel
opm
ent s
peci
alist
wer
e en
gage
d in
201
7.
Cond
uct g
ende
r sen
sitiv
e an
d/or
gend
er a
ctio
n pl
an tr
aini
ng fo
r pro
ject
staff
All 1
39 (3
2 ar
e fe
mal
e) p
roje
ct st
aff w
ere
train
ed o
n ge
nder
sens
itivi
ty a
nd o
n th
e ge
nder
act
ion
plan
. Tra
inin
g-of
-tra
iner
s was
con
duct
ed in
201
3 by
the
MO
H G
ende
r Mai
nstre
amin
g Act
ion
Gro
up, a
nd c
asca
de tr
aini
ngs w
ere
cond
ucte
d by
pro
vinc
ial t
eam
for a
ll RRT
staff
and
oth
er h
ealth
st
aff w
ith a
tota
l of 6
10 (2
35 fe
mal
es) p
artic
ipan
ts b
etw
een
2013
and
201
5.
Incl
ude
gend
er is
sues
in p
roje
ct p
lann
ing a
nd
man
agem
ent w
orks
hops
A c
heck
list t
o en
sure
gend
er is
sues
are
inco
rpor
ated
in w
orks
hops
and
tech
nica
l tra
inin
gs h
as b
een
deve
lope
d an
d pr
esen
ted
in th
e pr
ogra
m m
an-
agem
ent u
nit a
nd p
roje
ct im
plem
entin
g uni
t tra
inin
g in
May
201
7.
Prom
ote
wom
en’s
parti
cipa
tion
in p
roje
ct
man
agem
ent
A to
tal o
f 32
out o
f 139
(23%
) pro
gram
man
agem
ent u
nit a
nd p
roje
ct im
plem
entin
g uni
t sta
ff w
ere
fem
ales
in th
e 11
pro
ject
pro
vinc
es.
Sour
ce o
f dat
a: L
ist o
f gov
ernm
ent c
ount
erpa
rt st
aff.

78 Annex
LAO
PEO
PLE’
S D
EMO
CRAT
IC R
EPU
BLIC
(LA
O P
DR)
(refl
ects
wor
k un
der t
he C
DC2
and
CD
C2-A
F)1:
To e
nhan
ce th
e op
port
uniti
es a
nd co
ntrib
utio
n of
fem
ale
staff
in C
DC
syst
ems a
nd to
impr
ove
gend
er a
naly
sis in
regi
onal
CD
C sy
stem
s
Prom
ote
the
incr
ease
d tra
inin
g of w
omen
in
CDC
surv
eilla
nce
and
resp
onse
110
out o
f the
134
(82%
) fem
ale
surv
eilla
nce
and
resp
onse
staff
wer
e tra
ined
. The
201
7 Co
mpe
tenc
y Rep
ort e
stim
ates
that
87%
of s
urve
illanc
e an
d re
spon
se st
aff a
re h
ighl
y com
pete
nt.
Am
ong t
he C
DC
staff
, 1,3
95 o
f the
1,74
1 (>8
0%) f
emal
es h
ave
been
trai
ned.
Sour
ce: P
rovi
ncia
l Tra
inin
g and
Gen
der S
urve
y 201
7
Proa
ctiv
ely t
arge
t fem
ale
labo
rato
ry st
aff fo
r tra
inin
g14
7 ou
t of t
he 16
2 (9
1%) f
emal
e la
bora
tory
staff
wer
e tra
ined
.So
urce
: Pro
vinc
ial T
rain
ing a
nd G
ende
r Sur
vey 2
017
Colle
ct sp
ecifi
c se
x-di
sagg
rega
ted
data
in a
ll su
rvei
llanc
e fo
rms a
nd re
porti
ng d
ocum
enta
-tio
n
100%
of s
urve
illanc
e an
d re
spon
se d
ata
are
sex-
disa
ggre
gate
d.So
urce
: Mon
thly
repo
rts o
n ou
tbre
aks a
nd n
otifi
able
dise
ase
case
s
Reac
h m
ore
wom
en, in
clud
ing i
n th
e G
MS
annu
al jo
int r
evie
w o
f nat
iona
l mal
aria
pol
icie
s an
d st
rate
gies
The
proj
ect t
arge
ted
actio
ns to
reac
h w
omen
and
is in
clud
ed in
the
GM
S an
nual
join
t rev
iew
of n
atio
nal m
alar
ia p
olic
ies a
nd st
rate
gies
. The
Na-
tiona
l Stra
tegy
for M
alar
ia C
ontro
l and
Elim
inat
ion
asse
sses
risk
and
iden
tifies
targ
ets a
nd st
rate
gies
. You
ng m
ale
fore
st w
orke
rs a
re o
verw
helm
ingl
y th
e m
ost a
t-ris
k gro
up, a
lthou
gh th
e re
port
iden
tifies
MM
Ps (i
nclu
ding
wom
en) a
nd e
thni
c gr
oups
con
duct
ing s
lash
-and
-bur
n fa
rmin
g also
to b
e po
tent
ially
at-
risk.
wom
en a
re re
cogn
ized
to b
e im
porta
nt in
fam
ily w
elfa
re a
nd fo
r ens
urin
g the
use
of l
ong-
last
ing i
nsec
ticid
al n
ets.
The
stra
tegy
is
ther
efor
e to
con
tinue
to e
mph
asize
and
mar
ket b
ed n
ets t
o ho
useh
olds
, par
ticul
arly
thro
ugh
wom
en a
nd w
ives
Inco
rpor
ate
gend
er-r
elat
ed c
onte
nt in
to c
ur-
ricul
um tr
aini
ng m
odul
es, h
uman
reso
urce
de
velo
pmen
t pla
ns a
nd c
ross
-bor
der a
ctiv
ities
Gen
der c
onte
nts a
re re
flect
ed in
CD
C tra
inin
g cur
ricul
a at
inst
itutio
n, m
odel
hea
lth vi
llage
s, an
d co
mm
unity
leve
ls.H
uman
reso
urce
dev
elop
men
t pla
ns a
re ge
nder
resp
onsiv
e. (e
.g. u
ses s
ex-d
isagg
rega
ted
data
, has
quo
ta fo
r fem
ale
staff
to p
artic
ipat
e in
trai
ning
s)So
urce
: Pro
vinc
ial r
epor
ts, w
orks
hop
repo
rts a
nd p
lans
Enco
urag
e an
d m
onito
r the
hiri
ng o
f new
fe
mal
e st
aff20
14 –
261
of t
he 5
78 (4
5%) C
DC
staff
are
fem
ale
2016
– 3
84 o
f the
622
(62%
) CD
C st
aff a
re fe
mal
e20
16-2
017
– 16
of t
he 2
3 (7
0%) n
ew p
roje
ct m
anag
emen
t uni
t sta
ff ar
e fe
mal
eSo
urce
: Pro
vinc
ial T
rain
ing a
nd G
ende
r Sur
veys
201
4 an
d 20
17
2. T
o im
prov
e re
spon
siven
ess o
f CD
C to
gen
der i
ssue
s in
targ
eted
dist
ricts
/pro
vinc
es a
nd to
incr
ease
the
part
icip
atio
n an
d aw
aren
ess o
f wom
en in
CD
C pr
even
tion
in p
roje
ct lo
catio
ns
Colle
ct, u
se, a
nd a
naly
ze se
x-di
sagg
rega
ted
data
in
com
mun
ity-b
ased
CD
C as
sess
men
ts a
nd
plan
s
All p
roje
ct p
lans
and
ass
essm
ents
use
sex-
disa
ggre
gate
d da
ta: e
.g., p
roje
ct c
ondu
cts f
ocus
grou
ps fo
r ind
igen
ous p
eopl
e re
sear
ch, h
ouse
hold
su
rvey
s, tra
inin
g rep
orts
, and
out
brea
k and
surv
eilla
nce
data
Sour
ce: T
rain
ing a
nd G
ende
r Sur
veys
, Hou
seho
ld S
urve
ys, r
egul
ar re
porti
ng o
n tra
inin
g and
wor
ksho
ps a
nd su
rvei
llanc
e
Proa
ctiv
ely t
rain
wom
en a
s villa
ge h
ealth
volu
n-te
ers a
nd w
orke
rs
2,49
3 ou
t of t
he 2
,977
(84%
) tra
ined
villa
ge h
ealth
wor
kers
wer
e fe
mal
e.So
urce
: Pro
vinc
ial T
rain
ing a
nd G
ende
r Sur
vey 2
017
Ensu
re th
at a
t lea
st h
alf o
f new
ly se
lect
ed vi
llage
he
alth
volu
ntee
rs a
nd w
orke
rs in
dist
ricts
are
fe
mal
e
453
out o
f 916
(50%
) new
villa
ge h
ealth
wor
kers
wer
e fe
mal
e (T
he p
roje
ct se
t up
crite
ria th
at e
ach
villa
ge m
ust h
ave
one
mal
e an
d on
e fe
mal
e vi
llage
hea
lth w
orke
r).
Sour
ce: C
ompe
tenc
y Sur
vey 2
017
Proa
ctiv
ely o
utre
ach
and
targ
et w
omen
in
com
mun
ity-b
ased
CD
C or
mal
aria
act
iviti
es a
nd
cam
paig
ns u
sing g
ende
r-se
nsiti
ve IE
C m
etho
ds
and
mat
eria
ls
2014
Com
mun
ity E
vent
s - 2
57 o
ut o
f the
646
(40%
) par
ticip
ants
wer
e fe
mal
e.20
14 V
illage
Man
agem
ent G
roup
Eve
nts -
157
out o
f the
342
(46%
) par
ticip
ants
wer
e fe
mal
e.20
17 C
omm
unity
Eve
nts 2
,883
out
of t
he 4
,550
(63%
) par
ticip
ants
wer
e fe
mal
e.20
17 V
MG
Eve
nts –
1,98
6 of
the
3,34
1 (59
%) p
artic
ipan
ts w
ere
fem
ale.
Sour
ce: P
rovi
ncia
l Tra
inin
g and
Gen
der S
urve
ys 2
014
and
2017
Syst
emat
ical
ly in
clud
e ge
nder
-spe
cific
issu
es
into
the
train
ing a
ctiv
ities
impl
emen
ted
by th
e pr
ojec
t
All t
rain
ing a
ctiv
ities
are
gend
er m
ains
tream
ed. T
rain
ings
and
mod
el h
ealth
villa
ge tr
aini
ng c
urric
ula
incl
ude
gend
er is
sues
.So
urce
: Rep
orts
from
trai
ning
und
erta
ken
3. T
o en
hanc
e th
e ge
nder
aw
aren
ess a
nd re
spon
siven
ess o
f CD
C pr
ojec
t man
agem
ent
Tailo
r the
Gen
der A
ctio
n Pl
an to
nat
iona
l and
pr
ovin
cial
con
text
s N
atio
nal g
ende
r act
ion
plan
is u
nder
impl
emen
tatio
n an
d w
as re
vise
d in
Apr
il 201
3.G
ende
r act
ion
plan
, and
des
ign
and
mon
itorin
g fra
mew
ork p
rogr
ess a
re u
pdat
ed q
uarte
rly.
Sour
ce: G
ende
r act
ions
and
act
iviti
es re
porte
d in
pro
vinc
ial A
OPs
, Qua
rterly
Rep
orts

Annex 79
Inte
grat
e ge
nder
-rel
ated
act
iviti
es a
nd b
udge
t al
loca
tion
in a
nnua
l ope
ratio
nal p
lans
Ann
ual o
pera
tiona
l pla
ns in
clud
e ge
nder
act
iviti
es a
nd b
udge
t allo
catio
n.G
ende
r tra
inin
gs w
ere
cond
ucte
d at
pro
vinc
ial, d
istric
t, he
alth
cen
ter,
and
mod
el h
ealth
villa
ge le
vels.
Sour
ce: A
OP
subm
itted
to th
e pr
ojec
t
App
oint
gend
er re
pres
enta
tives
in p
rogr
am
man
agem
ent u
nit a
nd p
roje
ct im
plem
entin
g uni
t or
SC
Qua
rterly
repo
rts in
clud
e ge
nder
act
ion
plan
and
Indi
geno
us P
eopl
e up
date
s. A
ll dat
a (e
.g. o
utbr
eaks
and
trai
ning
s) a
re se
x-di
sagg
rega
ted
Sour
ce: Q
uarte
rly R
epor
ts h
ave
a st
anda
rd ge
nder
and
indi
geno
us p
eopl
e se
ctio
n
Recr
uit a
soci
al d
evel
opm
ent s
peci
alist
to c
over
ge
nder
issu
es a
nd ge
nder
act
ion
plan
impl
emen
-ta
tion
Inte
rnat
iona
l gen
der s
peci
alist
was
recr
uite
d an
d m
obiliz
ed in
Janu
ary 2
012.
Loca
l spe
cial
ist re
crui
ted
and
mob
ilized
in N
ovem
ber 2
012
Sour
ce: R
esea
rch
and
field
stud
ies u
nder
take
n an
d re
ports
com
plet
ed
Gen
der s
ensit
iveo
r Gen
der A
ctio
n Pl
an tr
aini
ng
for p
roje
ct st
affSe
rvic
e tra
inin
g - 2
,451
staff
trai
ned
(59%
are
fem
ale)
Trai
ning
man
agem
ent –
701
staff
trai
ned
(41%
are
fem
ale)
Gen
der a
ctio
n pl
an tr
aini
ng –
690
staff
trai
ned
(72%
are
fem
ale)
Incl
ude
gend
er is
sues
in p
roje
ct p
lann
ing a
nd
man
agem
ent w
orks
hops
Gen
der i
s mai
nstre
amed
into
all w
orks
hops
. Gen
der i
s em
phas
ized
in p
rovi
ncia
l tra
inin
g act
iviti
es.
Sour
ce: w
orks
hop
repo
rts
Prom
ote
wom
en’s
parti
cipa
tion
in p
roje
ct m
an-
agem
ent
2014
- 51
out
of 9
8 (5
2%) p
roje
ct im
plem
entin
g uni
t sta
ff w
ere
fem
ale
2017
- 41
out
of 8
5 (4
8%) p
roje
ct im
plem
entin
g uni
t sta
ff w
ere
fem
ale
Sour
ce: P
rovi
ncia
l Tra
inin
g and
Gen
der S
urve
y 201
7

80 Annex
VIET
NA
M (r
eflec
ts w
ork
unde
r the
CD
C2 a
nd C
DC2
-AF)
1. To
enh
ance
the
oppo
rtun
ities
and
cont
ribut
ion
of fe
mal
e st
aff in
CD
C sy
stem
s and
to im
prov
e ge
nder
ana
lysis
in re
gion
al C
DC
syst
ems
Prom
ote
the
incr
ease
d tra
inin
g of w
omen
in C
DC
surv
eilla
nce
and
resp
onse
In Q
2 20
17, 9
5 ou
t of 2
21 (4
3 %
) fem
ale
staff
of p
rovi
ncia
l pro
ject
man
agem
ent u
nit (
PPM
U)s
in D
ak N
ong a
nd B
inh
Phuo
c w
ere
train
ed.
In 2
016,
186
out o
f 222
(84
%) f
emal
e st
aff o
f Dak
Non
g and
Bin
h Ph
uoc
PPM
Us w
ere
train
ed.
In 2
015,
2,2
33 o
ut o
f 4,3
32 (5
6 %
) fem
ale
staff
of 2
0 PP
MU
s wer
e tra
ined
.Tr
aini
ng to
pics
: Stre
ngth
en st
aff c
apac
ity fo
r sur
veilla
nce,
ana
lysis
and
repo
rting
of i
nfec
tious
dise
ases
(Den
gue
feve
r, H
FMD
, etc
.) at
all
leve
lsD
ata
sour
ce: P
rovi
ncia
l rep
ort
Proa
ctiv
ely t
arge
t fem
ale
labo
rato
ry st
aff fo
r tra
inin
gIn
Q2
2017
, 5 o
ut o
f 8 (6
3 %
) fem
ale
staff
of D
ak N
ong a
nd B
inh
Phuo
c PP
MU
s wer
e tra
ined
.In
201
6, 7
out
of 1
3 (5
4 %
) fem
ale
staff
of D
ak N
ong a
nd B
inh
Phuo
c PP
MU
s wer
e tra
ined
.In
201
5, 14
1 out
of 5
65 (2
5 %
) fem
ale
staff
of 2
0 PP
MU
s wer
e tra
ined
.Tr
aini
ng to
pics
: labo
rato
ry b
iosa
fety
; man
ual o
pera
tion
of la
b eq
uipm
ent;
sam
plin
g, pr
eser
vatio
n, te
stin
g, an
d sa
mpl
e tra
nspo
rting
te
chni
ques
; use
of e
nzym
e-lin
ked
imm
unos
orbe
nt a
ssay
equ
ipm
ent f
or d
engu
e te
stin
g; m
etal
test
ing t
echn
ique
s for
Ars
enic
, mer
cury
, ca
dmiu
m in
food
.D
ata
sour
ce: P
rovi
ncia
l rep
ort
Colle
ct sp
ecifi
c se
x-di
sagg
rega
ted
data
in a
ll sur
veil-
lanc
e fo
rms a
nd re
porti
ng d
ocum
enta
tion
Dat
a on
cas
es/d
eath
are
sex-
disa
ggre
gate
d ac
cord
ing t
o Ci
rcul
ar N
o. 4
8/20
10/T
T-BY
T th
at gu
ides
the
decl
arat
ion,
info
rmat
ion
and
repo
rting
of c
omm
unic
able
dise
ases
. Thi
s circ
ular
was
repl
aced
by C
ircul
ar 5
4/TT
-BYT
dat
e 28
Dec
201
5 th
at re
quire
s sex
-disa
ggre
gate
d da
ta. T
he e
CDS
(ele
ctro
nic
repo
rting
syst
em fo
r com
mun
icab
le d
iseas
es) a
lso re
quire
s sex
-disa
ggre
gate
d in
form
atio
n an
d pr
ojec
t pro
v-in
ces a
re c
ompl
ying
.D
ata
sour
ce: P
rovi
ncia
l rep
ort
Inco
rpor
ate
gend
er-r
elat
ed c
onte
nt in
to c
urric
ulum
tra
inin
g mod
ules
, hum
an re
sour
ce d
evel
opm
ent p
lans
an
d cr
oss-
bord
er a
ctiv
ities
100%
PPM
Us d
evel
oped
gend
er p
lan
and
is in
tegr
ated
in m
ajor
act
iviti
es su
ch a
s tra
inin
gs, w
orks
hops
, and
com
mun
icat
ions
.D
ata
sour
ce: P
rovi
ncia
l rep
ort
Enco
urag
e an
d m
onito
r the
hiri
ng o
f new
fem
ale
staff
In 2
015,
113
of th
e 21
6 (5
2.3%
) new
ly h
ired
staff
wer
e fe
mal
e.In
201
6, n
o ne
w st
aff w
ere
recr
uite
d fo
r Dak
Non
g and
Bin
h Ph
uoc
PPM
Us.
In Q
2, 2
017:
1 of
the
3 (3
3.3%
) new
ly h
ired
staff
was
fem
ale
for D
ak N
ong P
PMU
. No
new
staff
recr
uitm
ent f
or B
inh
Phuo
c PP
MU
.D
ata
sour
ce: P
roje
ct M
anag
emen
t Uni
t/Pro
vinc
ial R
epor
t
2. T
o im
prov
e re
spon
siven
ess o
f CD
C to
gen
der/e
thni
c iss
ues i
n ta
rget
ed d
istric
ts/p
rovi
nce
and
to in
crea
se th
e pa
rtic
ipat
ion
and
awar
enes
s of w
omen
in C
DC
prev
entio
n in
pro
ject
loca
tion
Colle
ct, u
se a
nd a
naly
ze se
x-di
sagg
rega
ted
data
in c
omm
unity
-bas
ed C
DC
asse
ssm
ents
an
d pl
ans
Som
e of
the
mai
n co
mm
unity
-bas
ed a
sses
smen
ts h
ave
used
and
ana
lyze
d se
x-di
sagg
rega
ted
data
incl
udin
g pro
ject
surv
eys o
n w
orm
s and
re-
sear
ches
on
CDC.
Dat
a so
urce
: Pro
vinc
ial r
epor
t
Proa
ctiv
ely t
rain
wom
en a
s villa
ge h
ealth
volu
n-te
ers/
wor
kers
Year
Tota
l tra
ined
VH
Ws
Num
ber o
f tra
ined
fem
ale
VHW
s %
of t
rain
ed fe
mal
e VH
Ws
Not
e
2015
4,75
92,
707
56.9
20 P
PMU
s
2016
236
191
80.9
Dak
Non
g and
PPM
U B
inh
Phuo
c PP
MU
s
Q2
2017
228
192
84.2
Dak
Non
g and
PPM
U B
inh
Phuo
c PP
MU
s
VHw
= vi
llage
hea
lth w
orke
rSo
urce
: Pro
vinc
ial r
epor
t/Res
ults
of r
esea
rche
s

Annex 81
Ensu
re th
at a
t lea
st h
alf o
f new
ly se
lect
ed vi
l-la
ge h
ealth
volu
ntee
rs/w
orke
rs in
dist
ricts
are
fe
mal
e
In 2
011,
48 o
ut o
f 86
(55.
8%) n
ew vi
llage
hea
lth w
orke
rs w
ere
fem
ale.
In 2
012,
68
out o
f 123
(55.
3%) n
ew vi
llage
hea
lth w
orke
rs w
ere
fem
ale.
In 2
013,
87
out o
f 149
(58.
4%) n
ew vi
llage
hea
lth w
orke
rs w
ere
fem
ale.
In 2
014,
89
out o
f 146
(61%
) new
villa
ge h
ealth
wor
kers
wer
e fe
mal
e.In
201
5, 6
5 ou
t of 9
5 (6
8.4%
) new
villa
ge h
ealth
wor
kers
wer
e fe
mal
e.A
ccum
ulat
ed fi
gure
= 3
57 o
ut o
f 599
(59.
6%) n
ew vi
llage
hea
lth w
ere
fem
ale.
Dat
a so
urce
: Pro
vinc
ial r
epor
t
Syst
emat
ical
ly in
clud
e ge
nder
-spe
cific
issu
es
into
the
train
ing a
ctiv
ities
impl
emen
ted
by th
e pr
ojec
t
Und
er th
e pr
ojec
t man
agem
ent u
nit’s
inst
ruct
ions
, PPM
Us i
nteg
rate
d ge
nder
issu
es in
to tr
aini
ngs a
nd w
orks
hops
.Th
e pr
ojec
t con
duct
ed ge
nder
-spe
cific
trai
ning
cou
rses
(pro
cess
and
impl
emen
tatio
n of
loca
l hum
an re
sour
ce d
evel
opm
ent p
lans
, gen
der a
war
e-ne
ss a
nd im
plem
enta
tion
of ge
nder
- in
tegr
ated
act
iviti
es.).
Gen
der i
ssue
s are
inte
grat
ed in
som
e as
pect
s of C
DC
train
ings
with
prio
rity g
iven
to w
omen
of r
epro
duct
ive
age
in th
e ta
rget
pop
ulat
ion.
For
ex-
ampl
e: va
ccin
atio
n (m
easle
s, ru
bella
, tet
anus
, etc
.), p
rom
otio
n of
pub
lic c
omm
unic
atio
n on
wor
m in
fect
ion
in th
e co
mm
unity
, per
iodi
c de
wor
min
g, et
c.D
ata
sour
ce: P
rovi
ncia
l rep
ort
3. T
o en
hanc
e th
e ge
nder
awar
enes
s and
resp
onsiv
enes
s of C
DC
proj
ect m
anag
emen
t
Tailo
r the
Gen
der A
ctio
n Pl
an to
nat
iona
l/pro
-vi
ncia
l con
text
s Ce
ntra
l Gen
der A
ctio
n Pl
an w
as d
evel
oped
, intro
duce
d an
d pa
rtly i
mpl
emen
ted
by P
PMU
s.D
ata
sour
ce: P
MU
repo
rt
All a
nnua
l ope
ratio
nal p
lans
incl
ude
gend
er-
rela
ted
activ
ities
and
bud
get a
lloca
tions
Ann
ual o
pera
tiona
l pla
ns in
clud
e ge
nder
and
eth
nic
min
ority
targ
ets f
or 2
0 PP
MU
s.D
ata
sour
ce: P
roje
ct A
OP
App
oint
gend
er re
pres
enta
tives
in p
rogr
am
man
agem
ent u
nit a
nd p
roje
ct im
plem
entin
g un
it/SC
Staff
hav
e be
en a
ssig
ned
to m
onito
r and
sum
mar
ize p
roje
ct p
rogr
ess o
f pro
ject
man
agem
ent u
nit a
nd P
PMU
.D
ata
sour
ce: P
MU
/PPM
U re
ports
Recr
uit a
soci
al d
evel
opm
ent s
peci
alist
to c
over
ge
nder
issu
es/G
ende
r Act
ion
Plan
impl
emen
-ta
tion
Two
gend
er c
onsu
ltant
s wer
e re
crui
ted
and
deve
lope
d ge
nder
and
eth
nic
min
ority
pla
n.D
ata
sour
ce: P
MU
repo
rt
Cond
uct g
ende
r sen
sitiv
e or
Gen
der A
ctio
n Pl
an tr
aini
ng fo
r pro
ject
staff
Cond
ucte
d tra
inin
g-of
-tra
iner
s on
gend
er se
nsiti
vity
and
Gen
der A
ctio
n Pl
an in
June
201
2 fo
r 16
peop
le. T
hese
trai
ners
and
a n
atio
nal s
peci
alist
th
en c
asca
ded
train
ings
to 13
0 of
320
staff
from
pro
ject
man
agem
ent u
nit,
20 P
PMU
s, 4
IHEs
, 3 IM
PEs (
Inst
itute
of M
alar
iolo
gy, P
aras
itolo
gy a
nd
Ento
mol
ogy)
.In
201
5, th
e pr
ojec
t man
agem
ent u
nit c
ondu
cted
a tr
aini
ng o
n ge
nder
, min
ority
/gen
der a
ctio
n pl
an fo
r 30
out o
f 277
pro
ject
staff
from
pro
ject
m
anag
emen
t uni
t and
20
PPM
Us (
incl
udin
g foc
al p
oint
s for
gend
er is
sues
in 2
0 PP
MU
s). T
he fo
cal p
oint
then
org
anize
d tra
inin
g ses
sions
for 2
10
staff
at t
he lo
cal le
vel.
Dat
a so
urce
: PM
U/P
PMU
repo
rts
Cond
uct g
ende
r sen
sitiv
e or
Gen
der A
ctio
n Pl
an tr
aini
ng fo
r pro
ject
staff
In 2
011–
2015
, 29
out o
f the
47
(62%
) pro
ject
man
agem
ent u
nit s
taff
wer
e fe
mal
e, a
nd 6
3 ou
t of t
he 2
66 (2
4%) P
PMU
staff
wer
e fe
mal
e.In
201
6–20
17, 1
7 ou
t of t
he 3
3 (2
6%) P
PMU
staff
of D
ak N
ong a
nd B
inh
Phuo
c w
ere
fem
ale.
Dat
a so
urce
: PM
U/P
PMU
s rep
ort
Prom
ote
wom
en’s
parti
cipa
tion
in p
roje
ct
man
agem
ent
In 2
011–
2015
, 29
out o
f the
47
(62%
) pro
ject
man
agem
ent u
nit s
taff
wer
e fe
mal
e, a
nd 6
3 ou
t of t
he 2
66 (2
4%) P
PMU
staff
wer
e fe
mal
e.In
201
6–20
17, 1
7 ou
t of t
he 3
3 (5
2%) p
roje
ct m
anag
emen
t uni
t sta
ff w
ere
fem
ale,
5 o
ut o
f the
19 (2
6%) P
PMU
staff
of D
ak N
ong a
nd B
inh
Phuo
c w
ere
fem
ale.
Dat
a so
urce
: PM
U/P
PMU
s rep
ort

82 Annex
Annex D: Finance
ASIAN DEVELOPMENT BANKADMINISTRATOR FOR
REGIONAL MALARIA AND OTHER COMMUNICABLE DISEASE THREATS TRUST FUND
STATUS OF GRANT AS OF 31 AUGUST 2018
(ExPRESSED IN US DOLLARS)
CONTRIBUTION RECEIVED:Government of Australia (DFAT) 15,756,300 Government of UkNI (DFID) 12,414,880 Government of Canada (DFATD) 531,916
NET CONTRIBUTION AVAILABLE 28,703,096 Investment Income 316,764 TOTAL AMOUNT AVAILABLE 29,019,860
AMOUNT UTILIZED FOR:Outcome 1: Leadership (2,345,103)Outcome 2: Financing (277,133)Outcome 3: Medicines (3,116,152)Outcome 4: Information Systems (3,488,056)Outcome 5: Laboratory Dianostic and Surveillance (13,415,950)Outcome 6: Promotion and Prevention (3,387,604)Direct Charges (858,464)Administrative Costs, Audit, Financial Costs (1,445,695) (28,334,157)
UNUTILIZED BALANCE 685,7031/
1/ Unutilized Balance 685,703
Less: DFATD/Canada Contribution (531,916)
DFATD/Canada Investment Income (5,870)
DFID/DFAT Unutilized Balance 147,917
Annex 83
Annex E: RMTF Recommendations for Management of Future Trust Funds
• Background research is essential to ensure efforts are aligned with government needs and that they take into account the prevailing environment in terms of private sector and other agency involvement.
• Meeting donor reporting requirements is a key part of successful fund management, and it is useful to have donor involvement at the beginning, preferably at the country fact-finding mission stage, so that data collection can be organized in a way that meets donor requirements. For the same reason, it is also important to involve an evaluation and monitoring expert from the outset.
• Delays due to constraints on counterparts should be anticipated and built into project design so that projects can evolve as circumstances change.
• Local counterpart and government champions can expedite projects and greatly increase their chance of success.
• International and locally based consultants have complementary skills and both are needed to achieve sustainable results.
• when working at the grassroots level, people and civil society organizations can be trusted to know the needs of local community, and are often the best placed to get results from interventions if they are genuinely involved from the planning stage onwards and empowered to take charge of projects.
• Innovation entails risk, and it should be expected that a proportion of projects will fail. Lessons should be shared.
• Close collaboration with development partners is important to avoid duplication, silos, and unsustainable results.
• It is common for some of the funds to be returned when a project ends, and this does not necessarily signal project failure. Sometimes activities are less expensive than anticipated.

ASIAN DEVELOPMENT BANK
ASIAN DEVELOPMENT BANK6 ADB Avenue, Mandaluyong City1550 Metro Manila, Philippineswww.adb.org
Regional Malaria and Other Communicable Disease Threats Trust FundFinal Report
This report details the key achievements of the Regional Malaria and Other Communicable Disease Threats Trust Fund from its creation in 2013 to the first half of 2018. It provides detailed analysis of the results by outcome, profiles specific projects that serve as exemplars of the fund’s impact, and offers insights into how similar trust funds can be managed for success in future.
About the Asian Development Bank
ADB is committed to achieving a prosperous, inclusive, resilient, and sustainable Asia and the Pacific, while sustaining its efforts to eradicate extreme poverty. Established in 1966, it is owned by 67 members—48 from the region. Its main instruments for helping its developing member countries are policy dialogue, loans, equity investments, guarantees, grants, and technical assistance.
REGIONAL MALARIA AND OTHER COMMUNICABLE DISEASE THREATS TRUST FUNDFINAL REPORT
NOVEMBER 2018







