
Reducing Mortality in AKI/ SEPSIS Patients
Aintree University Hospital
DEBBIE COWELL/SUE GALLAGHER 2015

Reduction Of Mortality Rates Within Aintree
There are two national measures of mortality which help us to compare how we are performing compared to other organisations:
– Hospital Standardised Mortality Ratio (HSMR)– Standardised Hospital Mortality Index (SHMI)
Aintree, along with other hospitals, previously focused on HSMR. This was a key focus of our Quality Strategy, and we consistently had a better than average rating. However, when SHMI was introduced, a different picture emerged. Under SHMI, we had a very high ratio, one of the highest in the country. Professor Sir Bruce Keogh, the NHS Medical Director, has stressed that mortality indicators are not absolute indicators of quality of care but should be seen as ‘smoke signals’ to ensure focus on improvement.
DEBBIE COWELL/SUE GALLAGHER 2015
The Avoidable Mortality Reduction Group Aintree’s response to this challenge is the creation of the Avoidable Mortality Reduction Group.The group consists of multi-disciplinary clinicians who are leading work to reduce avoidable mortality at Aintree. The Outreach support project is one such group that has been introduced to ensure the early recognition and management of patients at risk of AKI/SEPSIS/Pneumonia through a system of coordinated alerts, the purpose being early identification of those patients at risk and prompt implementation of appropriate care bundles known to reduce patient overall mortality.
DEBBIE COWELL/SUE GALLAGHER 2015
TEAM MEMEBERSShirley Brady Clinical Manager Critical Care /Project Lead
Outreach Support Team Ext 2371
Sue Gallagher Specialist Nurse Critical Care Outreach/Met/AKI/Sepsis OSN Lead bleep 5540
Debbie Cowell Specialist Nurse Critical Care Outreach/Met/AKI/Sepsis OSN Lead bleep 5540
DR Thangavelu Chandrasekar
Consultant Nephrologist AKI Lead
DR Nihat Bhuiyan Consultant Critical Care Sepsis Lead
DR Neil Mercer Consultant Anaesthetist AVMRG Lead DEBBIE COWELL/SUE GALLAGHER
2015

Aim of project• Reduce mortality rates within the trust in this cohort of
patients• Deliver High Quality Safe Patient Care of patients with AKI/
SEPSIS• Raise awareness of AKI/ SEPSIS throughout the Trust• Ensure standardised care of AKI and Sepsis throughout the
trust through the introduction of care bundles, • Reduction in 30 day mortality in patients presenting with
sepsis within 12-18 months( initial overall mortality stood at 28% at start of project)
• Reduction within the trust in AKI level 1-3 Patients Initial aim was to reduce by 30%.
DEBBIE COWELL/SUE GALLAGHER 2015

Aim Primary Drivers
AimReduce
mortality rates in patients who
have AKI / Sepsis
Identification of AKI stages 1-3 Identification of Sepsis, severe sepsis, septic shock
Effective intervention and monitoring
Robust IT systems
Medical and nursing engagement
Secondary Drivers
1.Effectively identify patients at risk of AKI/Sepsis2.Development of patient criteria i.e. WBC >20000 for Sepsis3.AKI Bundle ( creatinine rise as per guidelines) 4.Increase staff understanding of AKI/Sepsis through education and training i.e. HDU ,ALERT,RN induction, F1 induction5. Urgent communication of appropriate patients to own team and Critical Care
Implementation of AKI and Sepsis six care bundles throughout the trust.
Development of patient documentation and patient information leaflet
Development of IT data base to feed appropriate patient information and blood results to outreach support team
via SIGMA 3 times a day
Funding ….the project to maintain sustainabilityTeam expansion to incorporate increased work load of
outreach team
Audit .Work with business intelligence collating and analysing the
patient data and provide monthly reports on trust mortality
Approval from trust board clinical effectiveness board
DRIVER DIAGRAM
DEBBIE COWELL/SUE GALLAGHER 2015

Measures and data
Outreach Support Team Outcomes - Narrative (10/09/2015)
Numbers of Patients Reviewed
Month Patients reviewed
% of Trust Inpatients
% of AKI/Sepsis/Pneumonia
Inpatients
Approximately 80% of patients reviewed are clinically assessed; 20% are telephone triaged/advice.
DEBBIE COWELL/SUE GALLAGHER 2015
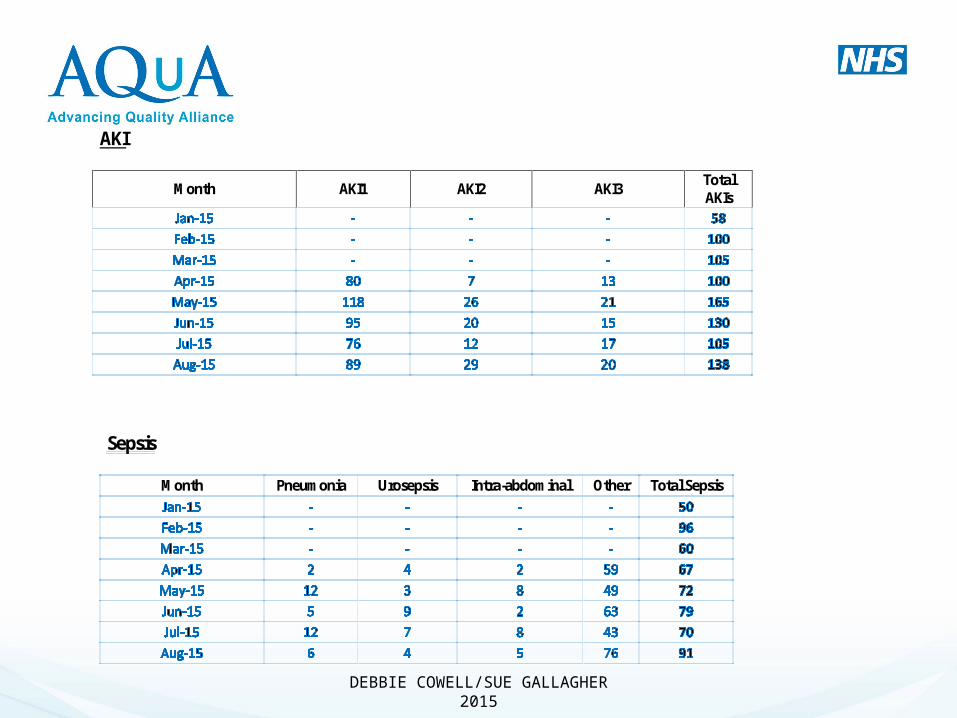
AKI
Month AKI1 AKI2 AKI3 Total AKIs
Sepsis
Month Pneumonia Urosepsis Intra-abdominal Other Total Sepsis
DEBBIE COWELL/SUE GALLAGHER
2015
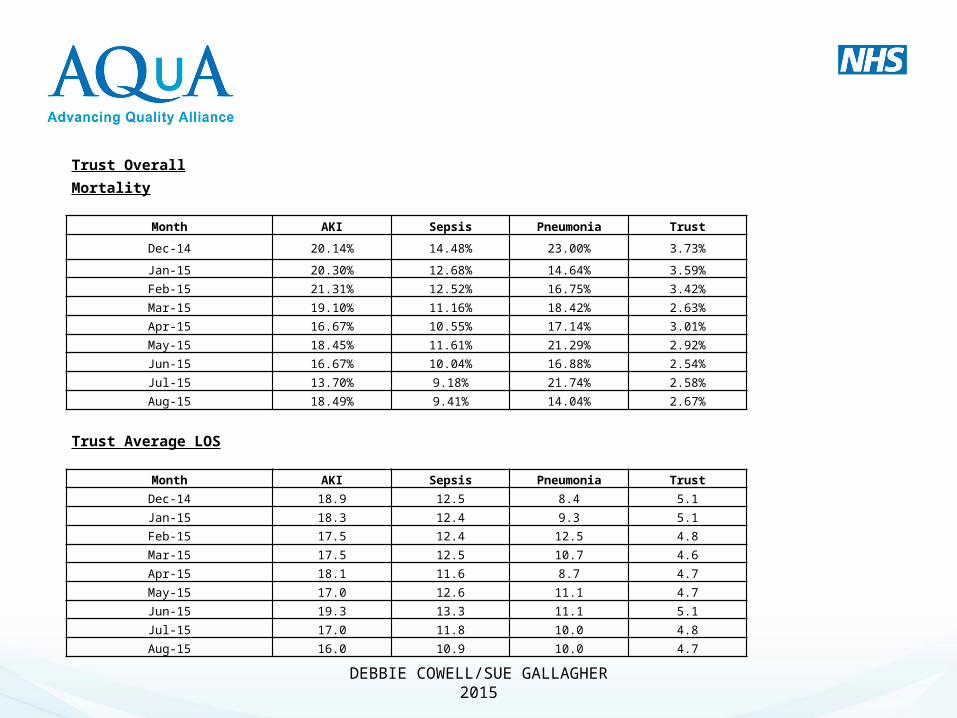
Trust Overall Mortality
Month AKI Sepsis Pneumonia Trust
Dec-14 20.14% 14.48% 23.00% 3.73%
Jan-15 20.30% 12.68% 14.64% 3.59%
Feb-15 21.31% 12.52% 16.75% 3.42%
Mar-15 19.10% 11.16% 18.42% 2.63%
Apr-15 16.67% 10.55% 17.14% 3.01%
May-15 18.45% 11.61% 21.29% 2.92%
Jun-15 16.67% 10.04% 16.88% 2.54%
Jul-15 13.70% 9.18% 21.74% 2.58%
Aug-15 18.49% 9.41% 14.04% 2.67%
Trust Average LOS
Month AKI Sepsis Pneumonia Trust
Dec-14 18.9 12.5 8.4 5.1
Jan-15 18.3 12.4 9.3 5.1
Feb-15 17.5 12.4 12.5 4.8
Mar-15 17.5 12.5 10.7 4.6
Apr-15 18.1 11.6 8.7 4.7
May-15 17.0 12.6 11.1 4.7
Jun-15 19.3 13.3 11.1 5.1
Jul-15 17.0 11.8 10.0 4.8
Aug-15 16.0 10.9 10.0 4.7
DEBBIE COWELL/SUE GALLAGHER 2015

Key achievements• Development of a bespoke web based system• Quality dashboard to demonstrate outcome measures• Implementation of Care bundles throughout the trust• AKI/Sepsis education training incorporated into:_F1 TrainingHDU Study DayAlert CourseRN InductionRole development team expansion• On going up to date training in all clinical areas• Proven reduction in mortality rates throughout the trust in patients with
AKI/Sepsis DEBBIE COWELL/SUE GALLAGHER
2015
Lessons learnt• Learning through trial and error ( paper work, data
base, consultant input, educational issues, asking for advice )
• Need for continual reassessing and need for change • Hospital politics, funding issues• Changes in team dynamics• Overcoming resistance to change• Outreach Team journey
DEBBIE COWELL/SUE GALLAGHER 2015

WHAT SHOULD AQUA DO DIFFERENTLY
DEBBIE COWELL/SUE GALLAGHER 2015
ANY QUESTIONS
DEBBIE COWELL/SUE GALLAGHER 2015




![Cowell - Tiger [1928] (Schirmer)](https://cdn.vdocuments.us/doc/165x107/577cda4d1a28ab9e78a54f96/cowell-tiger-1928-schirmer.jpg)


