Download - Prone Position

PRONE POSITIONRESCUE THEAPY FOR SEVERE ARDS
PRONE POSITION
Acute Respiratory Distress Syndrome (ARDS) is defined as a:
“syndrome of acute and persistent lung inflammation with increased vascular permeability” (Hansen-Fletcher et al)
PRONE POSITION
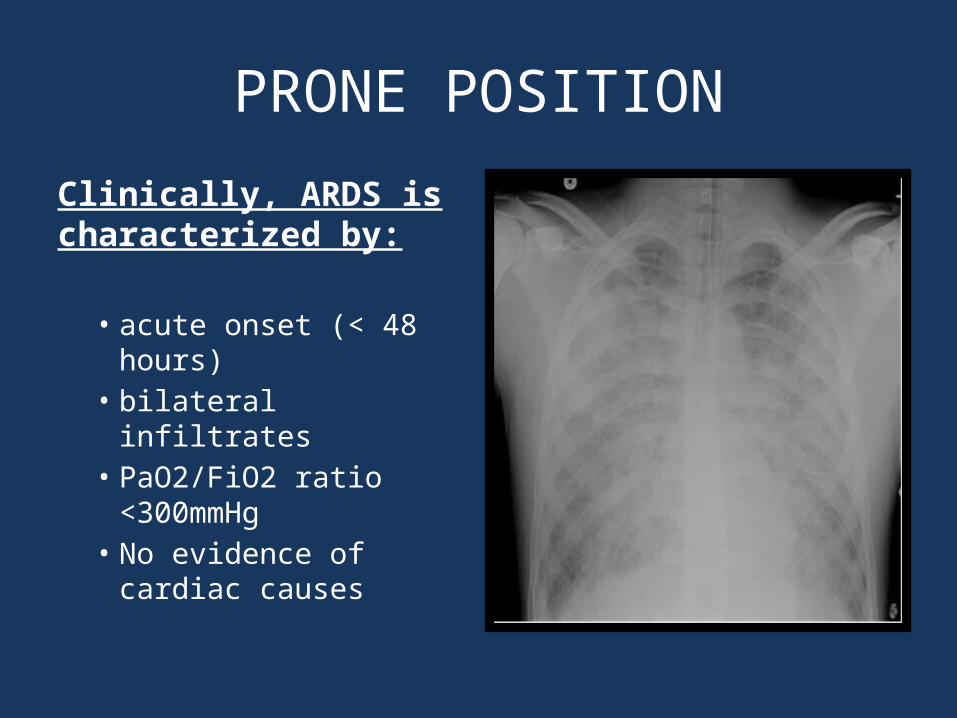
Clinically, ARDS is characterized by:
• acute onset (< 48 hours)
• bilateral infiltrates• PaO2/FiO2 ratio
<300mmHg• No evidence of
cardiac causes
PRONE POSITION• ARDS is classified by its cause:
– Direct lung injury: pneumonia, aspiration, inhalation injuries, ect..
– Indirect lung injury: sepsis, OD, massive blood transfusions, ect..
• Its severity (PaO2/Fio2 ratio):
– mild (200-300 mmHg)
– moderate (100-200 mmHg)
– severe (<100mmHg)

PRONE POSITION
Recovery Stage
• Slow restoration of lung function
Proliferative Stage
• 7—21 days• Alteration of lung tissue• Poor Compliance• Decreased Edema
Exudative Stage
• 0-7 days• Edema (peaks 048hrs)• Inflammation
Typically, lung dysfunction is the worst during the first 0-48hours and may last for up to a week.

PRONE POSITIONTreatment of ARDS:
• Treat underlying cause (i.e. sepsis)• Lung protective ventilation (low Vt +
adequate PEEP)• Avoid a positive fluid balance
However, in severe cases of ARDS (low pH, O2 and high CO2 and airway pressure) standard therapy main fail.
Rescue therapy may be needed: prone position
Prone Position
ECMO

PRONE POSITION
Indications for the prone position:
Capital Health Prone Criteria:
• ARDS
• < 48 hours
• Pa02/FiO2 <200mmHg

PRONE POSITIONRelative contraindications for the prone position:
• Elevated ICP• Intestinal ischemia• Obesity• Recent Abdominal Surgery
Absolute contraindications for the prone position:
• spinal cord instability,• unstable facial fractures• anterior burns, open abdomen• increased abdominal pressures• unstable pelvic fractures.
PRONE POSITIONThe Prone Position:
• Improves perfusion to the lungs → Better V:Q matching
• The diaphragm drops and the heart shift forward → Improved compliance
• Improved lung recruitment
• Lung Protective
• Indicated:• Moderate to Severe ARDS• Early (<48hours)• Duration: 12 – 16 hours

PRONE POSITION
• In healthy lungs the distribution of perfusion is effected by gravity.
• The apex and the middle of the gets more ventilation (V) than perfusion(Q). V>Q
• At the base, the lungs get more perfusion (Q) than ventilation (V). V<Q
• Atelectasis and inflammation of the lungs leads to worsening V:Q matching

PRONE POSITION
Perfusion (Q) of the anterior and base of the lungs improves in the prone position.
• The improved V:Q matching may improve oxygenation.

PRONE POSITION
The diaphragm drops and the heart shift forward → Improved compliance
May lower airway pressure
May improve VT and MV (↓CO2)
May reduce lung protective (↓ atelectotrauma, barotrauma & volutrauma)

PRONE POSITIONNURSING CARE:• Ensure adequate sedation and analgesia (meet goal
RASS)• Ensure adequate paralysis (meet TOF goal)• ABG PRN to assess oxygenation (PaO2) &
ventilation (PaCo2)• Reposition arms Q2H (see prone policy)• Check Q2H for pressure areas• Family education
PRONE POSITION
IN CONCLUSION:• Current research (PROSEVA) demonstrates
that the prone position is may be beneficial in severe ARDS (<48 hours).
• Duration 16-24 hours• Inexpensive compared and easy to perform• May be lung protective (improve compliance) • May improve oxygen and ventilation (better
V:Q matching)

PRONE POSITION
THANK YOU!







