
PREGNANCY OUTCOME FOLLOWING FIRST TRIMESTER MATERNAL EXPOSURE TO THE NEWER
SELECTIVE SEROTONIN REUPTAKE INHIBITORS
Nathalie A. Kulin
A thesis submitted in conformitv with the requirements
for the degree of Master of Science
Graduate Department of Pharmacology
University of Toronto
O Copyright by Nathalie A. Kulin 1997

National Library Bibliothèque nationale du Canada
Acquisitions and Acquisitions et Bibliographie Services services bibliographiques
395 Wellington Street 395, nie Wellington Ottawa ON K1A O N 4 Ottawa ON K1A ON4 Canada Canada
The author has granted a non- L'auteur a accordé une licence non exclusive licence allowing the exclusive permettant à la National Library of Canada to Bibliothèque nationale du Canada de reproduce, loan, distribute or seiI reproduire, prêter, disîribuer ou copies of this thesis in microform, vendre des copies de cette thèse sous paper or electronic formats. la forme de microfiche/film, de
reproduction sur papier ou sur format électronique.
The author retains ownership of the L'auteur conserve la propriété du copyright in this thesis. Neither the droit d'auteur qui protège cette thèse. thesis nor substantial extracts fkom it Ni la thèse ni des extraits substantiels may be printed or otherwise de celle-ci ne doivent être imprimés reproduced without the author's ou autrement reproduits sans son permission. autorisation.

PREGNANCY OUTCOME FOLLOWING FIRST TRIMESTER MATERNAL EXPOSURE TO THE NEWER SELECTIVE SEROTONIN REUPTAKE INHIBITORS
Master of Science, 2997
Nathalie A. Kulin Department of Pharmacology, University of Toronto
The main objective of this study was to determine if first trimester use of the newer
selective serotonin reuptake inhibitors (SSRIs), fluvoxamine, paroxetine and/or
sertraline increases the baseline risk of having a child with a major malformation.
The secondary outcornes of interest were pregnancy outcome, gestational age a n d
birth weight.
Women who called a participating teratogen information service regarding tirst
trimester use of one of the above SSRIs were contacted at a later date to ascertain
pregnancy outcome. These women were compared to a control group consisting of
women not exposed to anv known human teratogen in their pregnancy.
X total of 267 exposed women were followed up: 26 women used fluvoxamine, 97
women used paroxetine, and 147 women used sertraline (1 woman used both
flwoxamine and sertraline, and 2 women used both paroxetine and sertralinei.
There rïere 9 liwborn infants with major malformations in the exposed group and
9 in the control group (p = 0.91). The number of live births in the esposed group
were 227 versus 235 in the control group (p = 0.14). There was no difference in
either birth weights (3439 g in the exposed group, 3145 g in the control group, p =
0.91) or gestational age (39.4 weeks in the exposed group, 39.4 weeks in the control
group, p = 0.71). These results do not suggest an associated increase in risk of major
malformations. Although reassuring, a larger study is required to definitively label
these drugs as safe for use in pregnancy.

I am grateful for the support and guidance of my supervisor, Gidi.
Dr. Ingeborg Radde was an inspiration to me. Her experience was invaluable to the
development of this thesis.
Anne Pastuszak graciously donated much time and effort to aiding me with the
studv design and cvriting of this thesis.
Thank-you to my fellow grad students: Myla, Paul, Cindy, and the honourary grad
student, Gilda. And thanks to my best pal and fellow grad student, Kristen tor
enduring al1 the "Big Adventures" and numerous trips to the Second Cup.
This thesis is dedicated to my parents.

1 . Introduction ...................................................... .. ........................................ 1
1.1. Historv of Modem Teratology ................................................................. 1
1 . 2. Pus t-Marketing Surveillance Methodology ......................................... 4
1.2.1. Case Reports and Case Series ................... .... ..................... 4
1.2.2. Case-Control Studies ................................................................... 6 - 1.2.3. Cohort Studies .............................................................................. 1
1.2.4. Randomized Clinical Trials ...................................................... 7
1.3. Background Information ......................................................................... '1
... 1.3.1. Baseline Risk for Anomalies in the General Population 9
1.3.2. Definition of Malformation ................................................ 11 q q 1 . J J . Prepanc): Outcornes ................................................................. 11
1.3.4. Definition of Teratogen ........................................................... 12
1.3.5. Teratogen Information Services ............................................ 13
1 .4 . Depression .................... .. ......................................................................... 15
1 . 1. 1 . Historv of ht idepressant Medica tions ............................. 15
1.5. Selective Serotonin Reup ta ke Inhib itors ......................................... 17 -
1 .> .I. Mechanism of Action .......................................................... 27 1.5.2. Advantages and Disnd~rantages ........................................... 17 - 1 .J. 3. Pharmacology ............................................................................. 19 -
............................................................................. 1.3.4. Teratogenicity 20
1.6. Hvpothesis ................................................................................................. 2-4
1.7. Objectives ................................................................................................... 24 3- 2 . blethods ..................................................................................................................... 3
- 2.1. Study Design .............................................................................................. 2s
2.2. Pa tient Selection ....................................................................................... 26
7.1.1. Sample Size Calculation .......................................................... 26
2.3. Data Collection .......................................................................................... 28
2.4. Da ta Analysis ............................................................................................. 29
3 . Results ....................................................................................................................... 51
3.1. Data CoIiection .......................................................................................... 31
3.2. Cornbined SSRIs .................................................................................... 35

3 . d.1. Materna1 Demographics ........................................................... 33
3.7.1. Major Structural Malformations ..................... .... .......... 37
3.2.3. Pregnancv Outcome .................................................................. 40
3.2.4. Other Findings ........................................................................... 41
3.3. Fluvoxamine ............................................................................................. 43 7 1 . .............................*............-.....***........ J.J . 1 Ma temal Demographics 43
3.3.2. Major Structural Malformations ........................................ 4-4 3 3 1 J.J.J. Pregnancy Outcome .................................................................. 45
2.4. Paroxetine .................................................................................................. 46
.?.A. 1 . Materna! Demographics ........................................................... 4h
3 - 4 2 Major Structurai Malformations .......................................... 4S
3.4.3. Pregnancv Outcome .................................................................. 49 - .................................................................................................... 3.5. Sertraline 30 . .
............................... ......................... 3.3.1. Materna1 Demographics ... >O m ........................................... 3.3.2. Major Structural Malformations 32
-7 3.5.3 . Pregnancy Outcome ................................................................. 33
........................ Esposed From First Trimester to Third Trimester ... 54
............................... 3.6.1. Ma terna 1 Demographics ......................... ... 34
........................................... 3.6.7. Major Structural Malformations 56 -
3.3.3. Pregnancy Outcome ................................................................ 56
on ................................................................................................................. 58
................. Research Implications - Nul1 Hypothesis Not Rejected 5S ........................................... 4.1.1. Major Structural Malformations 5S
Limitations of the Study ........................................................................ 63
4.2.1. Recall Bias ................................................................................... 63
4.2.2. Loss ot Follow-up ...................................................................... 6-4
4.2.3. Demographic Differences Between Exposed and Control
Croups .................................................................................................... 64
4.2.4. Initial Stuclv .............................................................................. 65
Recommenda tions for F L ~ ture Research ........................................... 66
Recommenda tions for Counselling a t Motherisk ........................... 67
4.4.1. Women Planning Pregnancy and Pregnant Women
Planning t« Use a Newer SSRI ................................................... h7

4.4.2. Women Who Are Currently P r e p a n t and Using a Newer
SSRI ........................................................................................................ h i
Appendix 1 - Figures ................................................................................................. hS
Appendix II - Known Human Teratogens ............................................................ S3
References .................................................................................................................... S-l

LIST OF TABLES
Table 1 - Summarv of Epidemiological Study Types Used for Reproductive Outcome
Studies
Table 1 - Safety and Tolerability of TCAs vs SSRIs
Table 3 - Pharmacokinetics of the Four SSNs
Table 4 - Sample Size Calculations
Table 5 - Matemal Demographics - Motherisk Cases Included vs Lost
Tabk 6 - Cases Contributed bv Centre
Table 7 - Materna1 Demographics - Motherisk vs Other OTIS Centres
Table S - Breakdown by Exposure and Trimester of Exposure
Table 9 - Maternal Demographics: SSRI-Exposed vs BPG
Table 10 - Major Structural Malformations
Table I l - Major Structural Evlalformations - All SSRIs
Table 12 - Major Structural Malformations - All SSRis
Table 13 - Preg-tancy Outcome - Al1 ÇSMs
Table 14 - Birth Weiglit and Gestational Age for Live-Born Children - Al1 SSRIs
Table 15 - Other Findings
Table 16 - Maternal Demographics: Fluvoxamine-Exposed ï s BPG
v i i
Table 17 - Major Structural Malformations - Fluvoxamine
Table 18 - Pregnancv Outcorne - Fluvoxamine
Table 19 - Birth Weight and Gestational Age for Live-Born Children -Fl~i~.oxamine
Table 20 - Rilaterna1 Demographics: Paroxeti~e-Exposed vs BPG
Table 21 - Major Structural Malformations - Paroxetine
Table 22 - Pregnancv Outcome - Paroxetine
Table 23 - Birth GVeight and Gestational Age for Liw-Born Children - Paroxetine
Table 24 - Ma ternal Demographics: Sertraline-Exposed vs BPG
Table 23 - Major Structural Malformations -Sertr a 1' ine
Table 26 - Major Structural bhlformations -Sertr a 1' me
Table 27 - Pregnancy Outcome - Çertraline
Table 2S - Birth Weight and Gestational Age for Live-Born Children - Sertraline
Table 39 - Materna1 Demographics: SSRI-Exposed irom First Trimester to Tliird
Trimester i rs BPG
Tablé 30 - Major Structural Malformations - Exposed from First Trimester to Third
Trimester
Table 31 - Birth Weight and Gestational Age - Exposed from First Trimester to Third
Trimes ter

Table 32 - Birth Weight of SSRI-Exposed Non-Smokers 1-s BPG

Figure 1 - Motherisk Intake Form
Figure 2 - Motherisk Clinic Form
Figure 3 - Chernical Structures of the Selective Serotonin Reuptake Inhibitors
Figure 4 - Motherisk Follow-Up Form
Figure 5 - Motherisk Follorv-Up Letter to Offspring's Health Care Provider

BPG - baseline population group
CYP - cvtochrome P450
LMP - last menstrual period
MAO-I -monoamine oxidase inhibitor
SSRI - selective serotonin reuptake inhibitor
TC A - tricyclic antidepressant
TIS - teratogen information service

1.1. HISTORY OF MODERN TERATOLOGY
Throughout history, there have been many theories as to the causes of birth defects.
These theories ranged from maternai dreams to messages from the gods. Howewr,
it was not until the realization that certain environmental factors such as rnatern~l
rubella infection' could result in birth defects that the science of modern human
teratology emerged. The term teratogen is used tn describe a substance that could
have an adverse effect on the fetus. A more thorough definition is oifered in
section 1.3.4.
In 1958 a German pharrnaceutical Company marketed a d r u g labelled as a safe
sedatitee that kvas found to be an effective anti-emetic in earlv pregnancv. Soon after
thalidomide's introduction, reports of an outbreak of a series of Lincornmon
s tr~ictural malformations in newborns began to appear-r3. Phocornelia (limh
reduction) spontaneouslv occurs at a rate of about 0.14 per 1000 births, but betrveen
September 1960 and August 1961 that rate increased to 1 in 1000 births in Cermanv4.
The mothers of the children born cvith this structural defect took thalidomide
between the 20th to 35th slay post-conception, a time when the limbs are h rming in
the tetus. Thalidomide embryopathy is also associated with defects of interna1
organs, such as the heart, and the eves and earsï.
Until this time the placenta was thought to protect the developing fetus from the
effects of materna1 medication. After the thalidomide tragedy, however, heaith care
professionals and the public began to question the role of drugs in human
malformation and scientists strived to identify teratogens via animal s t~idies and
other experimental models. [n 1962 the United States Food and Drug
Administration introduced the first requirements for preclinical tosicologv testing,
inciuding reproductive studies, for new drug applications.

Today, during preclinical testing, the drug must be tested for teratogenic potential
and other reproductive endpoints such as fertility and matemal function in at least
two animal speciesb. During animal testing confounding variables can be
controlled. A confounder is a variable independently associated with a disease and
exposure which may affect the outcome. Despite the advantages of animal testing,
the extrapolation of i r i i1iil0 animal data to human pregnancy has been questioned
for several reasons. While animal studies have identified almost al1 teratogens
since thalidomide, thev have a high rate of false positives. tn a sample of 350 agents
tested in animais Shepard; found that 55"L of them were positive for being
teratogenic. This would mean that of the 1600 agents tested in animals 880 are
terntogens, yet in humans onlv about 30 agents have been found to be teratogenic.
There are several reasons for the high rate of teratogrnicitv reported in mimai
studies. The dosages tl-iat are given are not comparable to human doses, different
dosing methods such as intraperitoneal injection are often used, and animals have
different embrvonic development, pharmacokinetics, target organ sensitivi ty and
metabolic pathwayss. Thus far, there are no predictive i r i oitro tests availnble for
testing the human teratogeiiicity of drugs since our knowledge of o r s a n
dev elopment is still limited.
There are three phases of premarketing clinical testing. During phase 1, the clrug is
tested in sel.eral healthv volunteers to determine the safe human dosage, Iniman
pharmacokinetics and pharmacodynarnics. I t is onlv in phase II that the medication
is given to a small cohort of patients with the target disease to determine i f there are
anv differences from the phase I findings. Finallv, phase [ I I is an extension o t phase
11, but consists of larger numbers of patients, usually between 500-3001) people. In
this phase, randomized clinical trials are performed to test efficacy, yet rare aclverse
drug reactions mav easilv be missed.
During phase IV the manufacturer is required to monitor for adverse d r u g events
after the drug has been approved. Such events include rare side effects, chronic
toxicity and drug interactions. O f en such events are spontaneously reported to the
drug Company and Health Protection Branch by health care professionals. These
reports may include pregnant women who inadvertently took the medication.

Pregnant women are excluded from the premarketing clinical trials as it is medically
unethical to test drugs in human pregnancy. This results in a lack of d r ~ i g satetv
information tor a large segment of the population - narnelv women of child-benring
age. it is currentiy estimated that over half of al1 pregnancies are unplannedu.
Given that many women will not realize that they are pregnant until about five to
six rveeks after their last menstrual period (LMP), many of them inadvertantlv use
medications during this time whose fetal safety has not yet been determined. Often
the mother is unable to stop the medication because there is no alternative
treatment. For example, seizure disorders must continue to be treated with
medications throughout pregnancy in spite of the risk to the fetus. The mean age o f
Lvomen having children has also increased and this increase in age is paralleleci by
an increase in medical problems and medication uselu.
The raritv of human teratology studies, the increase in medication Lise and the
number of new medications available makes post-marketing surveillance a n
important requirement for determining the safetv of drugs in human pregnnncv.

There are several tvpes of epidemiologic studies that can be used to assess the
relationship between materna1 drug exposure and fetal outcome. Çummarized
below are the different study types aimed to determine the safetv of drugs in
pregnancy in increasing order of validity, validity being the degree to which a
measurement reflects the "true" value of what is being measured. The advantages
and disadvantages of each tvpe of study are summarized in Table 1.
1.2.1. CASE REPORTS AND CASE SERIES
A case report describes a patient with an exposure and a subsequent outcome.
Seïeral such patients mav constitute a case series. A case report studv is simple and
quick to perform since it is often retrospective. As there are no controls in a case
report studv, i t is purelv descriptive and statistical cornparison cannot be performed.
Xnother issue is that often only patients with ~inusual outcornes are noted a n d case
reports d o not include the frequency for the rate of exposure in the general
population. Crise reports or case series, however, are useful for generating
hypotheses for turther evaluation by a study which aims to test the hvpothesis (1.r-,
analvtic s tudy). Most case report findings are not supported by further
epidemiologic studies and are due to chance occurence. In the case of a rare or new
exposure, thouph. it mav be the only study design initially available.
Des pi te tl-ieir limitations, case reports and case series c m be helpful in tera tology.
Thalidomide is the best known esample of a teratogen suspected bv a case series'.
Though not generaliznble to all patients, case reports are an important tool in
assessing the risks of new drugs or drugs to cvhich pregnant women are rnrely
exposed. For esample, if the medication is infrequently iised in women of
childbearing age and causes a rare malformation, a small number of cases can
eçtablish the association. Conversely, if the medication is commonlv used by
pregnant rvomen. a few cases may onlv reflect the b a d i n e risk of malformation (see
Section 1.3.1.) unless a specific pattern of malformation is noted.


Spontaneous reporting to the drug company during phase IV regarding pregnancv
exposures essentially is a case series. There are many limitations to these
spontaneous reporting systems. For example, the cases are a mixture of prospective
and retrospecive reports and the amount of information is often limited and not
well documented regarding the exposure and timing of exposure11. There is a large
potential for bias in retrospective cases, as women having a child with a
malformation are more likelv to be reported to the drug company by their health
care providers than a mother who has a normal outcome. Several driig
manufacturers, however, are now creating prospective registries for women esposed
to their product during pregnancy.
In a case-control studv, the patient's disease status is determined first and for each
case there is at least one control patient without the disease selected for comparis«n.
The investigator then retrospectively determines the patient's e spos~i res bv
interviewing the patient and /or checking the patient's medical records. Case- control studies are inexpensive and quick to perform. Recall bias is the differing
abilities of cases and controls to rernember past events and is a major flaw in this
study type since it is retrospective. Another tlaw is that confounders arc not
controlled. To minimize contounders in this type of studv, two approaches mav bc
taken. If one c m predict the confounders, the controls may be matched bv the
confounder. I f a confounder is suspected after the studv is cornplete, one mav
stratifv the confounders during analvsis. This study torm is ideal for a rare outcorne.
In human reproductive outcome studies, the mother of a child with the suspected
anomaly is interviewed about previous exposures. The controls a r e usually
children with a clifferent tvpe of malformation since mothers of malformed infants
may have better recall of events occurring in their pregnancy than mothers of
normal childrenl2. An example of a confounder associated with pregnancy
outcome studies is materna1 cigarette smoking, rvhich results in an increased rate of
spontaneous abortion and lower birth weight for live-born childrenl? This type ot
study c m be performed to test findings found in case reports or cohort studies (see
below).

Essentiallv in a cohort s tudv information about the risk factor (exposure) is
determined and the patient is followed over time to see whether o r not disease
occurs. It is contrasted to a case-control study in that selection is based upon the
presence or absence of a predefined exposure rather than a disease. Cohort studies
provide information on the incidence of the outcome after exposure. This tvpe ot
study c m be retrospective, but more often is prospective. Recall bias is less likelv in
a prospective cohort when compared to a case-control studv since the exposure of
interest is recorded at the time of initial interview.
In human reproductive outcome studies, exposure is first determined m c l the
woman is then hllowed ~ i p after her expecteci date ot delivery. The baseline risk in
the general population for major birth defects is low (see section 1.3.1) and specific
defects have even lower rates. Neural tube defects such as spina bifida and
anencephaly, for example, occur at a rate of 1.3 per 1000 births. When a drug causes
a defect, it causes a specific type of defect or series of defects. The rarer an outcome,
the larger the sample size required
groups. Statistical power, the ability
two g r o ~ p s , is infl~iencecl bv sample
specific birth defect the sample size
risk is large and often inhibitory from
in order to detect a difference between the
of a studv to detect a true difference between
size. In the case of a rare outcome suc11 as a
required to rule out definitivelv an increased
a time or cost perspective when cornpared to a
case-control studv. This tvpe of study is useful for hypothesis generation for fut~ire
case-control studies and ruling out a large increase in the baseline risk.
The epidemiologic studies mentioned abo1.e have a11 been obsernt ional ( i . r* . the
investigator hes not intervened in patient treatment). A randomized clinical trial is
interventional and is the "gold standard" of epidemiological studies since unknown
or unmeasurable confounders are controlled for as the patients are randomlv
allocated to one of at least two treatment arms in the study. This type of st~ici\? is
often very expensive to perform and time-consuming when compared to the above-
mentioned studv tvpes. As described earlier, medical ethics prevents the testing in

human pregnancv of drugs for the purposes of determining whether or not a rirug is
terri togenic.

The following sections deal with background information needed to pertorm ri
human reproductive outcome epiderniologic study. In the first section various
studies addressing the baseline risk of major malformation are discussed. The
second section defines major structural malformation. The third section
summarizes diffcrent endpoints of pregnancy outcomes. The fourth section details
further the definition ot a teratogen. In the final section a description of a teratogen
information service is given.
1.3.1. BASELINE RISK FOR ANO~IALIES IN THE GENERAL POPULATION
Every pregnant woman has a certain chance of giving birth to a child with a major
structural malformation. This risk is independent of exposure to medications,
radiation and infectious diseases, as well as materna1 age or disease s t a t u during
pregnancy. This risk is termed the baseline rate of major malformation.
There have been several studies examining the rate of malformation in the general
pop~ilation. The results differ for each studv due to dissimilar definitions o t
malformation, methods of ascertaining presence o t malformations and pop~ilations
being studied. These issues will be explored in this section.
Marcien ct.d.l-' performed gross rnorphologic examinations on 1412 Caiicasian
births (including stillbirths) within 4s hours of birth. The infants had tu be n t Ieast
20 iveeks gestational age (from the first day of materna1 LMP) to be included in the
study. Marden s t . d detined a major malformation as one that has adverse effect on
either the function or social acceptability of the individual, and 90 chilclren (7.O1'L)
were diagnosed with a major malformation. Tl-iey defined a minor maliurmatic~n
as one having neither medical nor cosmetic consequences ta the patient. There
were 609 children ( 3 . S ) diagnosed with having one or more minor
malformations without anv major malformation.
A studv with similar design to that of Marden et ni. was published in ls>S71-?
Caucasian live-born singleton infants were randomly selected and had surface

examinations within four davs of birth. Excluded were infants of diabetic mothers
or mothers who used phenytoin in pregnancy. The definitions of major and minor
malformations were the same as those used in the studv - by - Marden rt 111. Unlike
Marden et al., however, malformations found bv additional diagnostic tests ordered
bv the infant's pedia trician were also included for analvsis. OnIv mal formations
diagnosed by 5 davs of age were included. Of the 4305 infants esamined, 162 had
major malformations (3.Sc)L) and 1652 had minor malformations (3S.-L":t).
Due to the dispara te methodologies in the above studies, many potentially
classifiable malformations were missed. A malformation such as an ectopic kidnev
would be missed by a surface examination and also is not likely to be diagnoseci
tvithin two davs ot birth.
The iirst large scale studv included 5330 live-born children and was published in
19541h. The measured outcorne \vas anv type ot anomaly, including mental
deticiencv. The children were followed ~ i p t» one vear of age rvhere possible. Stxen
percent of the children (n = 336) were diagnosed with an anomaly.
Tittelve urban medical centres in the United States participâted in a studv that
included 53,357 children born between 1959 - 1966 making this the largest s t~ idv to
date';. .ksessed were al1 singleton births including lSSl fetal and neonatal deaths.
.A congenital anomal!. was defined as a g r o s physical or anatomic developmental
m o m a l v that WCIS present at birth or detected ciuring the tirst vear of Me.
Malformations that rvere no longer detectable at one year of age rvere not c~tcgorized
ùs a malformation. Assignment as major or minor malformation was arbitrarv and
based on experience and expert advice. Thirteen percent of the births (n = 69 11) ivere
diagnosed with only minor malformations: 6911 (13.0'10) and 4422 tvere diaanosrd
with a major malformation (8.3'%,).
Heinonenlhssessed singleton births, including stillborns at 14 ~iniversitv-affiliated
hospitals in the United States. Children were follorved up for varying lengths of
time ,ind 91% of l i w borns were examined at the one vear mark. Of thc JO,ZS2
singleton births, 1393 (2.8'!:1) were determined to have a major malformation. The

malformations were each assigned as major or minor, although the criteria for this
categoriza tion were not explained.
In summary, the baseline rate of major malformation in the general population
ranges from 7'1;) to 8.30% depending on the definition of malformation and the
methods emploved in the study.
A mistake commonly encountered is the assurnption that "defect", "anomalv", and
"mal formation" are equivalen t terms, which is no t so. Anomalv encomp'isses al1
structural aberrations of the normal and defect is also a broad term tliat n-iav involve
morphologic, enzymatic. genetic, and/or chromosoma1 anornalieslu. The definition
of a malformation is quite precise. it is a change in form rather than f ~ ~ n c t i o n ~ ~ .
Spranger et ( 1 1 . 3 ) define a malformation as a rnorphologic defect of a n organ, part oi
an organ, or larger region of the body resulting from an intrinsically ( i .c . , inherited)
abnormal deïeloprnental process. I f an anomaly is due to an extrinsic interference
ivith an otherwise normal process, it is ri d i s r ~ p t i o n ~ ~ . It is o f e n impossible t o
determine in the postnatal period if a n anomaly is due to an intrinsic or cstrinsic
factor (or some combina tion o t the tivo) during pregnancv?
One other tvpe of structural anomaly exists. A deformation is an abnormnl form,
shape, or position of a part of the bodv caused by intrinsic or extrinsic meclinnical
to rces?
Pregnancv outcome can be categorized into two main groups: live birth, and ietal
death. Fetal death inclride abortions and stillbirths. Abortions can occur
spontaneouslv (ix., "miscarriage") or by medical intervention. An abortion hv medical intervention is called a therapeutic abortion and can be performed for a
variety of reasons. In the case of an ectopic pregnancy, a therapeutic abortion must
be performed to save the motherfs life. In most western countries a therapeutic

abortion will be performed upon the request of the mother. This ma- be due to
social reasons, materna1 medical conditions or detects detected in the fetus bv one ot
the prenatal tests commoniv administered to preçnant women.
A fetal death can occur an! time in the pregnancv and the terminology used to
describe the death varies with the gestational age when the death occurs. Currently,
the World Health Organization considers a death before 34 weeks ps t -LMP of
pregnancy a spontaneous abortion and one after that time a stillbirth? Prior to thùt
definition, the World Heaith Organization delineated the point between
spontaneous abortion and stillbirth as 30 weeks", a definition still accepted os valid
by many. Warburton r t nl. further divide spontaneous abortions into earlv and
late? An "earlv spontaneous abortion" occurs before 14 weeks post-LMP and a "la te
spontaneous abortion" occurs between 14 and 30 weeks post-LMP. The reason h r
this division is that the majority of spontaneous abortions before the week have
gross chromosoma1 abnormalities. The fetal death rate before 20 weeks wns 15.3'0
'inci c7t 20 cveeks or more was 2.1°0 in a 1971 striciv? There are severai rne~lications
and environmental exposures, such as cigarette smoking", that increase the fetal
death rate.
The term tera togen is clerived from the Gree k words k i n t o s (monster) and , p p i l
(producing). A teratogen is clefined as an environmental influence that has an effect
o n the embrvo o r tetus after fertilization, but beiorc birth and primarilv C~ILISCS
morphologie mnlformations and disruptions? Altliough teratogens c m act at any
time in pregnancy, they act essentially during the first S weeks of embryogenesis.
Schardein'" offers a broader definition of teratogen. I t is an agent that induces
structural mal formation, metabolic or physiological dysfunction, or psychological or
behavioural alterations or deficits in the offspring, detected either at birth or in a
defined postnatal period.
Shepard has m a d e a list of criteria which can be used as a guideline in the
determination of teratogenicity. The fi rst three criteria are considered essential. The
criteria are as follows:
Proven maternal exposure to agent a t critical tirnets) (i .r. , when the structure is
forrning) in prenatal development
Consistent findings by two or more epidemiologic studies of high quality.
a. Control of confounding factors
b. Sufficient numbers
c. Exclusion of positive and negative bias factors
d. Prospective studies if possible
e. Relative risk of six or more (?)
Careful delineation of the clinical cases. A specific defect or svndrome i f present
is very help hil.
Rare enl-ironmental exposure associated with rare defect. Probablv three o r
more cases.
Teratogenicity in animals important but not essential.
The association should make biologic sense.
Proof in esperirnental animals that the agent acts in an unaltered state.
Terntogen information sen-ices (TISs) plav an important role in the postrnarketing
suri-eillance of medication use during pregnancy. These programs ofter risk
âssessment counselling for pregnant women exposed to medications and also a n
opportunity tor prospective collection of d rug exposures in pregnancy.
Collaboration among TIS centres allows for larger sample sizes to be compiled and 7 - 7 y 79 several such studies have successfully been completed-i .-. I- . There are c~irrentlv 50
members of the Organization of Teratogen Information Services in North America,
including the Motherisk Program.
The Motherisk Program in Toronto, Ontario was established in 1985 to provide risk
assessments regarding maternal medication in pregnancy and lactation and the
possible effects on the fetus or baby. Motherisk is a telephone counselling service for

both the public and health care professionals. Currently 750 calls are answered by the Motherisk team in a n average week. Information is documented for each cal1
and callers are required to provide a demographic, medical, and pregnancy history
(Figure 1, ail figures can be found in Appendix 1). Patients concerned about a
knocvn teratogenic exposure or an exposure for which there is not enough evidence
to definitivelv label as non-teratogenic (cg. new medications) are referred to a clinic
for face-to-face counselling with one of the tearn's phvsicians. In the c h i c the
phvsician records a more thorough medical and demographic history (Fig~ire 3.
Subsequent to the clinic visit, a summary letter is sent to the patient's health care
provider regarding the information relayed during session.
Betrveen 5 and 10% of the queries regard medications used to treat depression.

1.4. DEPRESSION
Depression is among the most common disorders in the ivorld today. The
.American Psvchiatric Association's fourth edition ot' the Diagnostic and Statistiçal
Manual of Mental Disorders (DSM-IV)30 defines a major depressive episode as a
period of at least two weeks during which there is either depressed mood o r the loss
of interest o r pleasure in neariy al1 activities. Two terms commonlv used to
quantifv the rate of depression in the population are the one-year prevalence rate
and the lifetime prevalence rate. The first term refers to the
population who suffered t'rom depression in the year prior to
second term reiers to the percentage of people who have
depression in their lifetime.
The one-vear prevalence rate for major depressive disorder by
ttstimated to be 7°0 among rvomen of child-bearing age (1s
percentage of the
interview and the
DSM-III criteria is
to 44 ~ - e a r s ) - ' ~ . A
pop~ilation of Canadian h7omen aged 18 to 64 in Edmonton, Alberta had a lifetime
prer-alence rate O C major depression of 12.3"O". In an Ontario sample of rural and
urban populations, of the people who were diagnosed with depression 63.8":) in the
urban sample and 73.0"0 in the rural sample were womenx. The prei-alence rate ot
depression in Canadian women aged 1s to 71 vears was 1U.S1!L and for women aged
25 to 44 this rate was 8.6'!iJ3-1. A 1995 ltalian d rug prescription monitoring studv
randomly selected Y743 subjects of which 5.4% received a prescription for an
antidepressant within n 30 month period? The ratio of female to male was tnw to
one. In summarv, women of childbearing age have a high rate »f depression and
this is reflected in prescrihing patterns.
The first medication closs found to be effective in treating depression was the
monoamine oxidase inhibitors (MAO-Is), drugs that were initially produced in an
attemp t to find effective anti-tuberculosis treatrnent? They mediate their et'kct bv inhibiting monoamine osidase, an enzyme which destrovs excess amine
neurotransmitters in the presynaptic receptors. This increases the amount of
neurotransmitter available to act upon the postsynaptic receptors and ultimatelv

downregulates these receptors. The MAO-Is, however, are associated with
numerous adverse effects as well as food and drug interactions leading to poor
patient cornpliance and toxicitv. As a result the MAO-1s are not comrnonlv
prescribed today. Since they are not widelv used, information regarding satetv ot
MAO-1s in pregnancy is sparse.
The development of the tricyclic antidepressants (TCAs) was the result of an '~tternpt to improve the antipsvchotic effectiveness of the phenothiazines-;:. Thev inhibit the
reuptake of serotonin and norepinephrine at the presynaptic receptors. By
preventing reuptake, the drugs keep the neurotransmitter in contact with the
postsynaptic receptors and therebv cause postsynaptic receptor downregulation. The
TCXs have not been associated with an increased risk of maior structural
mal formation in p r e g n a n ~ y ~ ~ .
A recent addition to the drug therapies available for the treatment of depression are the selectiïe serotonin reuptake inhibitors (SSRIs). In Januarv 1988 fluoretine
(ProzacG) was marketed in the United States. Since this time several newer SSRIs
have been introduced, namely sertraline (Zoloft'"), fluvoxarnine (Luvox~ '~) , and
paroxetine (Paxil"'). The term "newer SSRI" herein reters to fluvosamine, a me. paroxetine and/or sertr 1'
Dcspite their use bv women of child-bearing age, little is known about the eifects of
the newer SSRls f luvoxamine, paroxetine, and sertraline on human pregnancv
outcome. This stridv dealt cvith the risk of the use of these medications in
pregnancv in regards to major structural malformations and p repancy outcome.

1.5. SELECTIVE SEROTONTN REUPTAKE INHIBITORS
The SSRIs block the serotonin reuptake carrier. Since serotonin reuptake is the
major mechanism of serotonin inactivation after its release into the synaptic cleft
there is an increase in concentrations of serotonin in the synapse available to act
upon the presynaptic autoreceptors and postsynaptic receptors. The constant
stimulation of the autoreceptors eventually results in their desensitization. This
desensitization causes a greater amount of serotonin (Le., enhances serotonergic
neurotransmission) to be released into the synaptic clett per impulse. Initiallv the
rate of firing decreases, but after approximately 14 days the rate has recowred to
baseline. The net result is an increase in the amount of serotonin in the synaptic
cleft. I t has been hypothesized that the time delay of 14 days correlates with the
onset of antidepressant activity.
1.5.2. ADVANTAGES AND DISADVANTAGES
While the SSRIs sl-rare some similarities with the TCAS, therc are also sewra l
clifferences that have made them popular with but11 patients and phvsicians. Prior
to the introduction of the SSRIs, the TCAs were the most commonly prescribed
antidepressants so thev will be used as a comparison drug ciass in the followinp,
sections.
A. Safetv and Tolerability
While the SSRls affect only the serotonin reuptake carrier, the TCAs are relativelv
nonspecific and act upon ri wide range of neuroreceptor systems inclading the
ùcet~lcholine, histamine, u-adrenergic, norepinephrine and serotonin receptorç, of
which only the norepinephrine and serotonin receptors mediate the desired eifect.
Furthermore, the TCAs also directlv stabilize membranes. Due to these additional
effects the sidr effect and toxicitv profiles of the TCAs are quite different irom those
of the SSRls (Table 2).

From Preçkom. l996jS.
Table 2 - Safety and Tolerability of TCAs vs SSRIS
The TCAS are iverv cardio-toxic in an overdose situation due to inhibition ot tlie tast
sodium channels in the heart. It is possible for as little as five times the therapeutic
dose of a TC;\ to be lethal? Given that patients who suffer from depression art.
between 13 t» 30 times more likely to at tempt suicide than the normal
popuIationJ*P41, the combination of the narrow therâpeutic window of the TCAs and depression is very dangerous. Since the SSMs do not affect the fast sodium
channels they are not cardio-toxic and are relatively safe in an overdose.
SSRIs
1 O ttr
low
low
1 O
low
high
Consideration
Safe ty
overdose lethalitv risk
alcoliol potentiation
Toterability
anticholinergic adverse eïents
antihistarnine adverse events anti-ul adrenergic adverse events
serotonin adverse events
Drug interactions are a n important factor to consider when prescribing ai-itidepressants since &en they are used on a long-term basis. The TCAS Iiaw a
great potential for pharrnacodynamic drug interactions. Anxietv is otten ,issociated
with depression and patients may be prescribed a sedative to counter the symptoms.
This can be problematic with concomitant TCA use, because TCAs potentiatt.
ethanol and sedatives due to their antihistaminergic effects. Another example of a
pharmacodvnamic drug interaction is with p-blockers and other antihvpertensive
medications. The TCAs block a-adrenergic receptors thus lowering peripherd
resistance which can have an additive effect with p-blockers. Inhibition of the tast
sodium channels also po ten tia tes P-blockers.
TCAs
high
high
higl-i
high
high
locv
Common side effects associa ted with TC .As include dizziness, tremors, swea ting,
constipation, drowsiness and dry mouth. Side effects commonly encountered with

the SSRis are sweating, nausea, nervousness and drowsiness. The side effects of the
SSRIs are more tolerable to the patient than those of the TCAs resulting in increased
patient c ~ m p l i a n c e ~ ~ .
B. Efficacv A meta-analvsis of the literature found that there was no significant difference in
effectiveness between the TCAs and the SSRIsq?
C . Sim~licity
Due to the side effects and narrow therapeutic index of TCAs, they are often started
at a sub-therapeutic dosage to allow the patient ta adapt to the side etfects and for the
phvsician to titrate the dose upward to avoid toxicity. Conversely, patients can be
started on a therapeutic dose oi their SSRI immediately thus obtaining a therapeutic
effect more quickly.
The chernical structures of the four SSRIs differ (Figure 3). The pharmacokinetics
between the cirugs also Vary (Table 3) . For example, fluoxetine has a l-idf-lifc of S4
hours and the half-life of it's active metabolite, norfluoxetine, is 146 hours. The
tl-iree newer SSRIs have half-lives of 24 hours, though the half-life of sertraline's
active metabolite, desmethylsertraline, is 66 hours. Desmethylsertraline is a much
less potent inhibitor of serotonin reuptake than the parent compound, so its
contribution to the clinical efficacy of the drug is minimal.

Table 3 - Pharrnacokinetics of the Four SSRIs
parameter FLLJO FLUV PAR0 SERT
extent of absorption (%) 80 94 64 >44
time to ~ e a k concentration (h) 4-8 2-8 2-8 6-10
volume of distribution (L) 25 20 17 N A
pro tein binding ("4)) 95 77 95 97
elimination half Me (h) parent compound 84 -- 7 ? 24 26
active metabolite 146 n o n e none 66
FLUO = ftuoxetine; FLUV = fluvosamine; NA = not available; PARO = paro~etinc;
SERT = sertraline. From Finley, 199-L4-'.
Each of the SSRIs is metabolized bv different enzymes'" Cytochrome P450 (CYP)
ID6 is partiallv responsible for the metabolism of' fluoxetine, thouoh the rernainder
has not been established. Paroxetine is metabolized by CYP I D 6 a t lou
concentrations and at higher concentrations is metabolized by a n unidentifieci low-
affinity enzyme. The enzyme responsible for the metabolism of fluvoxamine is
unknown, but is thought to be CYP 1A2. Sertraline is demethylated by CYP 3A3/4.
A, Fluoxetine
In pregnant rots treated with ~ i p to 7.4 mg/kg fluoxetine prior to and throughout
gestation no effects were noted in either fetal morphology or pregnancy outcorne.".
In pregnant rats and rabbits given oral fluoxetine during organogenesis at doses up to 40 mg/kg/day and 15 mg/kg/day respectively, there were no changes in eitl-ier
pregnancv outcorne or rate of major malformations in the p u p d h .
The company that produces fluoxetine, Eli Lilly, has prospectively followed up 544
fluoxetine-exposed pregnancies-'? Of these pregnancies 91 were terminated, 7 2
resulted in spontaneous abortion and two were stillbirths. The remainder were l i w
births with thirteen major malformations reported in this group. Additiondly
there were 2s major malformations reported to the company retrospectively. There

was no pattern to the malformations in either the prospective or the retrospective
group.
In 1993 Pastuszak c t al? published the results of a prospective multi-centre cohort
on pregnancv outcome of 128 women exposed to fluoxetine in their first trimester
compared to two age-matched control groups. The first control group consisted of
women who had taken a tricyclic antidepressant in their first trimester (74 women)
and the second group of women who had not been exposed to a human teratogen
(12s women). No statistical difference was found between the three groups in either
the rate of major malformations or pregnancy outcome.
Another s t u d v ~ ~ r o s p e c t i v e l y followed 228 p r e p a n t women who used fluoxetine
at some time in their pregnancy. Of the 173 pregnancies that ended in a live-birth,
162 women wed fluoxetine in the first trimester. There was no signif iant
ciifference in the rate of major structural malformations and deformations between
164 liïeborn children (this includos two twin pregnancies) exposed to fluoxetine in
the first trimester and 226 livebom children in the control group.
Finâilv, a recent meta-analvsis summarized al1 the available prospective st~idies
regarding iirst trimester exposure to fluoxetine? Of the 367 pregnancies, there [vas
no associated increased risk in the rate of major structural malformations.
B. Fluvoxamine
In pregnant rats and rabbits given fluvoxamine during organogenesis in doses of up
to SO mg/kg/dav and 40 mg/kg/day respectively, neither pregnancy outcome nor
fetal morphology were affected-?O.
Prescription-event monitoring in Britain revealed 31 cases of women exposed in
pregnancy to the SSRI fluvoxamine? The outcornes for 21 of these pregnancies are
known. One of these women was exposed in the second/third trimester and
subsequently had a non-malformed child. Three women had unknown exposure
times in their pregnancy. One of these women had a non-malformed child, one
terminated the pregnancy and the third had a spontaneous abortion. The
remainder of the women were exposed to fluvoxamine in the first trimester. Of

these there were five spontaneous abortions, one ectopic pregnancy and tour
terminations. One of the terminations was due to detection of a chromosomal
abnormality (matemal age = 40). There were eight live births including a set of
twins. No malformations were recorded in this group. There is one case report in
the literature of a mother who took the dmg throughout her pregnancy who had a
non-rnalforrned child52.
C . Paroxetine
Pregnant rats and rabbitç dosed with up to 5.1 mg/kg/day and 43 mg/kg/day of
paroxetine during organogenenesis did not differ from their controls in either
pregnancy outcome or fetal morphology-;j. The dose given was SU times the
recommended human dose. Another s tudv performed on rats and rabbits
administered up to 8.3 (rat) and 1.7 (rabbit) times the maximum recommended
human dose vielded similar re~ul ts - '~ .
The British prescription-event monitoring system recorded 71 paroxetine esposed pregnancies and their outcornes'? Of these, 63 women were exposed in the first
trimester. Exposure times for the remaining 8 pregnancies were unknown. For the
62 known pregnancy outcomes, there were 12 elective abortions, 9 spontaneous
abortions and 43 live births. There were three sets of twins among the live births
and one twin rvas stillborn (cause unknown). There were no malformations
reported for anv of the live births.
Spontaneous reports to the company have not shown any pattern of malformations
due to paroxetine use in pregnancy5".
D. SertraIine
Teratology studies performed in pregnant rats and rabbits at up to 80 mg/kg/dav did
not show sertraline to affect fetal morphology" (Zoloft product monograph, 1994).
The therapeutic human concentration is about 3 mg/ kg/day.
The company that produces sertraline, Pfizer, has nine reports of patients who
received the medication while pregnant. There were 5 non-malformed children
born, one elective termination and 3 spontaneous abortionsYs.

In summarv, none of the SSRIs have been shown to be teratogenic in mimals .
With the exception of fluoxetine, there are no controlled epidemiologic studies
regarding the teratogenic potential of the SSRIs in human pregnancy. Since each of
the SSRIs has a similar mechanism of action, it is possible for them to be studied
together in regards to teratogenic potential.

Matemal exposure to the newer SSRIs fluvoxamine, paroxetine, and/or sertraline
in the first trimester rvill not increase the baseline rate of major structural
malformations.
Primarv Obiective: To record and compare the rates of major structural malformations between the
esposed studv group and a control group rcpresenting the baseline population of
pregnnnt women.
Secondarv Obiectives:
To record and compare the distribution ot pregnancy outcome, gestational nge
and weight of livebom infants at delivery, hetween the exposed and the baseline
population control groups.

This was a prospective cohort design with one control group consisting of ivomen
who were not exposed to anv known teratogen at any time in their pregnancy and
who represented the baseline population group (BPG) of pregnant women. Botl i the
exposed and the control groups were ivomen who voluntarily contacted a teratogen
in torma tion service.

The sample consisted of women who contacted either Motherisk or another of the
teratogen information services (TE) participating in this studv. Al1 women wh»
met the inclusion criteria were included in the s t~ idv . The control group miisistd
of women randomly selected from pregnancies tollowed u p bv the Motherisk
Program. One control rvoman was selected for each SSRI-exposed woman.
Inclusion Criteria - Exposed Grouv
pregnant women who voluntarily contacted one of nine TISs for counstilling
about exposure to either to Ruvoxamine, paroxetine, and/or sertraline in rveeks
two to thirteen post-LMP
Inclusion Criteria - Baseline Population Control Grouv
pregnant rvomen not exposed io any knorvn human teratogen (see Appendis I I )
Exclusion Criteria
exposure to a known human teratogen anvtime during pregnancv (both groups)
esposure to any of the drugs of interest in secondhhird trimester onlv (exposed
groupl
Table -L outlines the nurnber of live births in each group required to cietect an
increase of a specific magnitude in the observed proportion of major structural
malformations. The svmbol Pi represents the baseline risk of major structural
malformations in the control group ( i . ~ . , BPG) and for this study is considered to be
5% in liïeborn children (sec section 1.3.1.). The svrnbol Pl represents the observeci
proportion oi major structural malformations in the esposecl group detectable in the
studv sample size. Relative risk (RR) is the ratio of the incidence of major structural
malformations in exposed women to the incidence of major structural
malformations in the BPG. The final colun-in in Table 4 indicates the nurnber ot
liveborn children in each group that is needed to rule out this speciiied relative risk.

Based on these values a total of 227 liveborn infants exposed t» a newer S R I in the
first trimester of pregnancy would allow a relative risk of 2.3 to be rulecl out i f LI
difference does exist.
Table 4 - Sample Size Calculations'
pl RR n
Each of the newer SSRIs were separatelv compared to the control group, ancl post-
hoc analvsis was performed to determine the relative risk that was detectable by their respective sample sizes with SOCXI power and an alpha of 0.05. Additionally,
pregnancies o t rvomen who used a newer SSRI through three trimesters iïere
separately analvzed in the same way.

2.3. DATA COLLECTION
Women or their health care providers who contacted the Motherisk program for
counselling about fluvoxamine, paroxetine, and/or sertraline between February -1st' 1992 and Xpril ~ 1 s t ' 1995 were followed-up. I f the caller to Motherisk was a
health care provider, he/she was asked to obtain permission for Motherisk to contact the mother regarding pregnancy outcome. These women were interviewed
by phone using the standard Motherisk follow-up form (Figure 4). The
q~~est ionnaire covered a variety of topics regarding pregnancy and pregnancy
outcome. These included obstetrical history, maternal disease, drug and
environmental exposures during pregnancy, delivery information, and neonatal
health. A11 mothers of live-born children were also asked permission to contact thc
child's doctor so as to corroborate the medical details of the follow-up. Letters were
sent to the child's doctor requesting maternal obstrical records and medicai details about the child's health (Figure 5). 1f a response was not received within two
months, the letter was fased, and if a response was still not receiveci, the doctor was
telep honed.
Other TISs were contacted and asked to send follow-up information about women
who Iiad ïoluntarilv contacted their centre for counselling about fluwsarnine,
paroxetine, and /or sertraline use in pregnancï.

2.4. DATA ANALYSIS
Analysis was performed primarily using the Statview Program? Fisher's exact
tests, relative risks and confidence intervals were generated by the Epi Info
Programho.
Continuous variables (materna1 age at conception, gestational age a t live birth, birth
rveight), expressed herein as mean 2 standard cieviation, were analvzed using an
unpaireci Çt~icient's t-test for parametric data and Wilcoxon rank-sum test for non-
parametric data. Nominal data variables (gravidity, parity, previous spontaneous
abortion/stilIt?irth, previous therapeutic abortion/ectopic pregnancy, alcohol
exposure, tobacco exposure, pregnancv outcorne, major structural mnlfornintions)
were analyzed using a ~2 test. I f there was a small espected frequency in the
nominal data, a Fisher's exact test was performed. X small espected frequency was
defined as one that \vas Iess than five. The reiative risk and 95% confidence
inter1.d~ were calculated for major struct~iral malformations.
Several TISs in the United States and Canada collaberated on this study. Since each
centre serves a different patient population it is possible that the demographics of
patients differed. To discern if this was the case, demographic characteristics
(gravidity, paritv, previous spontaneous abortion/stillbirth, previo~is therapeutic
abortion/ectopic pregnancy, alcohol exposure, tobacco exposure, materna1 age at
conception) were statistically compared between Motherisk and a cohort CI' al1 the
other centres.
Firs tlv, all the exposed pregnancies were analyzed together. Secondly, first trimester
exposures to each of the newer SSRIs, namely fluvoxamine, paroxetine and
sertraline, were nnalyzed separatelv as were women exposed to any of the newer
SSRIs through three trimesters O t pregnancy.
The primarv outcome of interest in this work was the rate of major structural
malformations. It is thus important that "malformation" and what was considered
"major" in this work be defined.

In the posrnatal period it is often impossible to determine if an anomalv is due to an
intrinsic or extrinsic factor iri rltrro (or some combination of the two)'u, therefore
this work did not make anv attempt to differentiate between the two in statistical
analvsis and simplv referred to both as a "structural malformation". An exception
#as made in cases where i t was clearly a chromosomal anomalv trisomv 3).
These cases were excluded from the analysis of major structural maltormntions.
De formations were reported as "other findingsrr but were not statisticallv annlvzed.
The definitions of H e i n o n e d b e r e used to differentiate major from minor
malformations, because this reference offers the most thorough List of
malformations ilassified as major o r minor. Al1 case information and
malformation classification were reviewed bv a geneticist a t the Hospital tor Sick
Children.
The secondnry outcomes of interest were the pregnancy outcome and the gestational
age and weight of liwborn infants at delivery. Pregnancy outcome was categorized
as: live birth, stillbirth (fetal death 230 weeks post-LMP), therapeutic abortion.
ectopic pregnancv, earlv spontaneous abortion (fetal death 51-1 weeks post-LM'), and
late spontaneous abortion (fetal death >14 weeks, but c30 weeks post-LMP).
Gestational age was recorded a s number ot iveeks post-LMP, and birth weii$~t ivas
recordeci in grams.

3.1. DATA COLLECTION
X total of 207 women or their health care providers contacted Motherisk between
February P t , 1992 and ApriI ~ l s t , 1995 regarding exposure to either Au~msnrnine,
paroxetine, and/or sertraline. Of these, 150 were followed up and the remaining 57 women were lost to follow-up. Of the 150 women interviewed, only 93 rvere
included in the study. The other 5s women were excluded for a varietv of reasons.
Twentv-five of the wornen contacted Motherisk when they were planning a
pregnancy and had not become pregnant by the time follow-up was attempteci, 16 of
the women did not use the medication at al1 in pregnancy, 6 women or their l-iealth
care professionals refused to participate, 6 women were esposed to a known human
teratogen during their pregnancies, 3 women used the medication after the first
trimester, one patient could not speak English, and one womnn hnd committcd
suicicie.
X cornparison ot demographic variables between the Motherisk cases included (n =
92) in the study and those lost to follow-up (n = 57) did not show any significant ciifferences between the groups for any of the variables except for alcol-iol
consumption (Table 5). Women who rvere included in the study reported more
alcohol intake than the women who rvere lost to follow-up.

Table 5 - Matemal Demographics - Mothensk Cases Included vs Lost
variable included lost p-value
-- - -
previous spontaneous abortion (SA) SA = O
SA = l+
previous therapeutic abortion (TA)
TA=O
TA = 1+
tobacco consumption
Y- no
alcohol consumption
Yes no
age (yrs)
'Sornt. ot' the lcist c'ascs were ivomen plmning pregnancv at the timc ot initial inter\'ieiv i~~l-io
Iiad never been prt.gncmt.

In total, 267 ivomen who met the study inclusion criteria were tollowed up by
Motherisk and other OTIS centres (Table 6 ) . The demographics of women collectecl
by Motherisk (n = 92) were not statistically different when compared to those
collected from al1 the other centres combined (n = 175) (Table 7).
Table 6 - Cases Contributed by Centre
centre n %
Toronto O N 92 34.5
Tampa FL
Farmington, CT 32 12.0
Salt Lake Citv, UT 11 4.1
London O N 6 -. 3 - 7

Table 7 - Matemal Demographics - Motherisk vs Other OTIS Centres
variable Motherisk O ther* p-value
gravidity (g) g = l 23 34 t i . 3
g = 2+ 69 130
parity (p) p = O 36 59 0.9s
p = l + 36 96
previous spontaneous abortion (ÇA)
SA = O 68 S2 0.30
SA = l+ 24 19
previous therapeutic abortion (TA) TA = O 76 78
TA = l+ 16 23
tobacco consump tion
Yes no
alcohol consumption
Y- no
materna1 age at conception
' Sts.crnl centres ticici missins information ior various parameters.

-411 the women used a newer SSRI in the first trimester, but most stopped use in the
first trimester (Table 8). Some women, however, used the medication beyond the
first trimester and into the second or third trimester. There were 49 wcnmen who
used a newer SSRI through three trimesters ot pregnancy.
Table 8 - Breakdown by Exposure and Trimester of Exposure trimes ter total ('/O) fluvoxamine paroxetine sertraline
Sc\.cral ccntre-; had cases ot tiVorncn tvlio iaLlcd after :ising CI nc\\.t.r SSRI in the first
trinw,ter, but ivcrc ~mable to pro\.idc accuratc information regarding stop dates u t rncciicationc;.
Clne t\.ornnn iiscd paroxetine in the first trimester .and sertraline in the third trimester. Slic
ic; tiieretore classified under first trimester paroxetine use.
$ Four Lvornen used more than one of the newer SSRIs, therefore the totals for tlic indi \ . id~i~i l
SSNs d u not add rip to 267.
Four of the women used two different SSRIs in their pregnancy. One ot these
wnmen usecl sertraline through three trimesters and f luwwmine for one week in
the first trimester. Two women used paroxetine in the first trimester and switched
to sertraline at 10 weeks post-LiMP. Both of these women used sertraline t» term.
Finallv, one cvoman used paroxetine in the first trimester and sertraline in he r third . .
trimes ter.
Tl-iere were signif ican t differences between the SSRI-exposed group
several variables (Table 9). Women in the SSRI-exposed group l-iad
and the BPG for
higher graviditv

and higher numbers ot prelrious therapeuetic abortion, and thev reported a higher
rate of smoking.
Table 9 - Matemal Dernographics: SSRI-Exposed vs BPG
variable* SSRI- BPG p-value exposed
gravidity (g) g = 1 er = 2+
previous spontaneous abortion (SA) SA=O 157 205 0.91
SA = 1+ 49 61
previous therapeutic abortion (TA) TA = O 166
TA = 1+ 40 -
tobacco consumption
Yes no
- -
alcohol consumption
Yes no
matemal age at conception
* Sarrral centres had missing iniormation for various parameters.

The cases of children born tvith structurai malformations are described in Table IO
on the following page. For the SSRI-exposed women, the medication, dose and
time-frame of use are also outlined.

3 -fi r; u w
A CI
3 > . C.
Y
c; - 3
5 J 1 - -n f i J
C L
.n y: 0 /
Cc,
u
CZ
13 TL, -4
-5
-5 - -4
l- II
u . . . - - 2 C t: f - a r c L

Ln summarv, there were 7 confirrned cases o i major structural malformations in the
children of women exposed to a newer SSM in the first trimester. Adclitionallv,
there were trvo children with unconfirmed diagnosis. Due to these, statistical
analvsis was performed twice, once excluding (Table 11) and once including (Table
12) these two cases as major structural malformations. In the control group, 9 of the
children were born with a major structural malformation. Note that major
structural malformations were only assessed for live-bom children, so that the totâls
reflect the number of live births and not the total cohort. The number ot [ive-Lwrn
children in the SÇRI-expose group was 222, and the number in the BPG [vas 233.
Table Il - Major Structural Malformations - Al1 SSRls
major structural SSRI-exposed BPG p-value
malformation
ves 7 9 0.S9
-- - - . - . -- . -. -. .
relative risk (95% confidence interval) = 0.82 (0.31-2-17)
Table 12 - Major Structural Malformations - All SSRIs
major structural SSRI-exposed BPG p-value
malformation
total 333 335
relative risk (95% confidence intervail = 1.06 (0.43-2.62)

When pregnancy outcome was compared, there were no significant differences
betiveen the groups (Table 13). Trvo neonrital deaths occurred in the BPG. Both
children died shortly al'ter delivery. No defects were observecl in the tirst cliild, but
the second child had a venticular-septal defect. In the SSRI-exposed & - qroup, «ne
child died at three weeks of age after an operation to repair an unspecitieci heart
defect.
Table 13 - Pregnancy Outcome - Al1 SSRIs
pregnancy outcome SSRI-exposed BPG p-value
live birth --- 377 -33 O. 24 31-
- -
early spontaneous abortion 24 16 0.25
6 -
late spontaneous abortion 3 1 .O
therapeutic abortion 15 9 t1.30
ectopic pregnancy 0 O
s tillbirth O 7 O .50
X cornparison cif hirth weight and gestational age for live-born children between the
two jiroups did not reveal nnv statisticallv significant difterences (Table 14). Eight O t
the live-born children in the SSRI-exposed group were of low birth weight (i-s.. less
thnn 2500 g), and 15 of the live-born children in the BPG were of Iow birth weight.
Sixteen children in the SSRI-exposeci group were premature (i.tV., born at less than 37
weeks post-LMP), and 13 children in the BPG were premat~ire.
Table 14 - Birth Weight and Gestational Age for Live-Born Children
- AI1 SSRIs
variable SSRI-exposed fn) BPG (n) p-value
birth weight (g) 3439 + 505 (218) 3445 I 610 (235) 0.92
gestational age 39.4 + 1.7 (204) 39.4 11: 1.9 (235) 0.72
(wks)

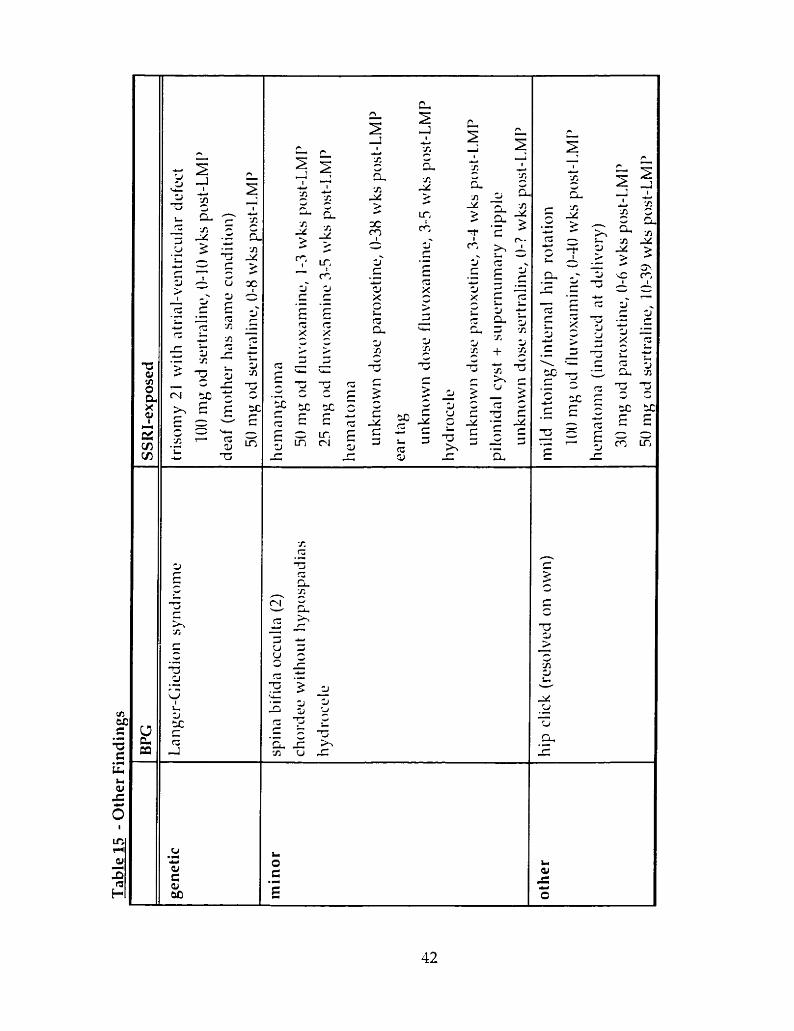
Table 15 on the following page lists the other findings, including minor
maiformations, genetic svndromes and deformations.
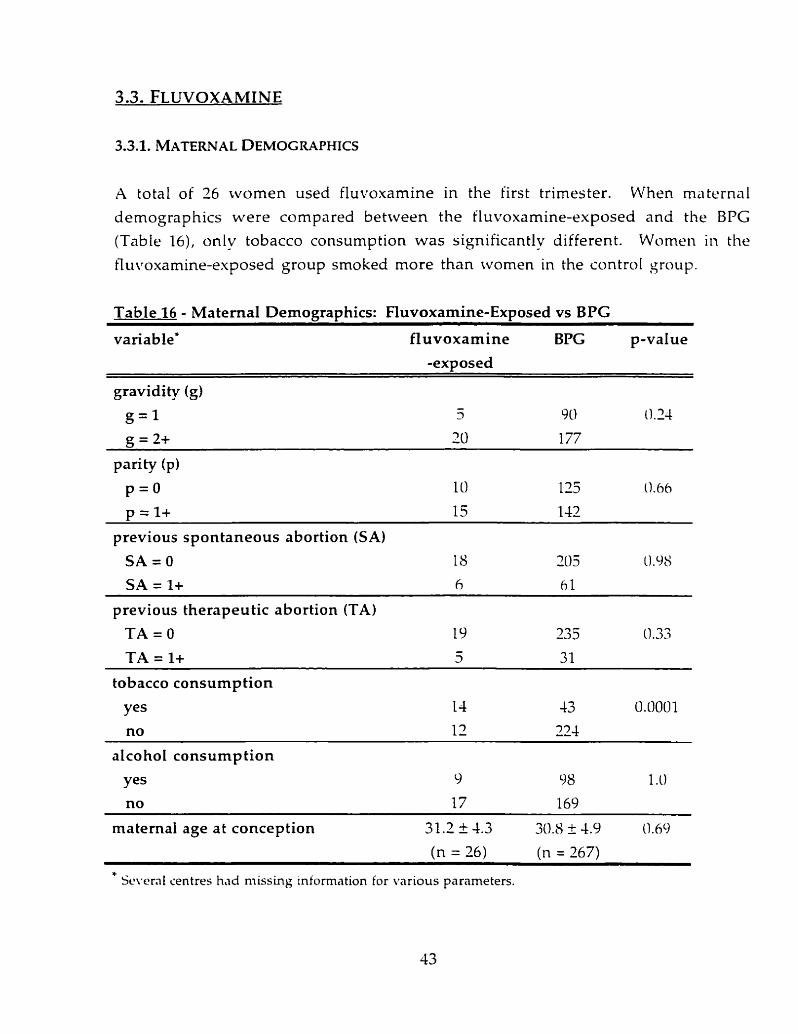
A total of 26 tvomen used fluvoxamine in the iirst trimester. When materna1
demographics were compared between the Cluvoxamine-exposed and the BPG (Table 16), onlv tobacco consumption was significantlv different. Women in the
iluvoxamine-exposed group smoked more than ivomen in the control group.
Table 16 - Materna1 Demographics: Fluvoxamine-Exposed vs BPG
variable* fluvoxamine BPG p-value
gravidity (g)
g = 1
g = 2+
previous spontaneous abortion (SA)
SA = O
SA = 1+
previous therapeutic abortion (TA)
TA=O TA = 1+
tobacco consumption
Yes no
alcohol consump tion
Yes no
materna1 age at conception
---- - - -
* Se\.craI centres h.id missing information for various parameters.

Most of the fluvoxamine-exposed women were using the drug at the time tiiet-
conceived (n=17, data available for 24 women). The mode for dailv dose was 50 mg
(n=ii , data available for 23 women). The highest reported daily dose was 200 mg.
There were no major structural malformations in the liveborn children of wornen
who used fluvoxamine in the first trimester (Table 17). This tvas nat ~tatistica11v
different from the control group.
Table 17 - Major Stmctural Malformations - Fluvoxamine
major structural fluvoxamine- BPG malformation exposed
p-value
ves 0 9 1 .O
total O- 37 235
relative risk (95% confidence interval) = 1.00 (0.83-1.21)
There was a ratio of 10.7:l for non-exposed women to fluvoxamine-exposed wornen
whose pregnancies ended in a live birth. The relative risk detectable by the wmple
size, using the same parameters as the sample size calculâtion in Table 4 h.., CL =
0.05, a = 0.80, and a baseline risk of 0.05 in the general population for major
structural malformation), was 5.6. This altows a 38% risk of major structural
malformation due to flwoxamine use in the first trirnester of pregnancy to he ruled
c'iut.

Tables 18 and 19 outline the pregnancy o~itcomes of the fluvoxamine-esposed
women and the BPG. There was no signifiant differences between the trvo groups
in anv of the outcornes. There were no differences in either the birth tveight or the
gestational age of Iive-barn children. One child was premature and was oi loti- birth
weight in the fluvoxamine-exposed group.
Table 18 - Pregnancy Outcome - Fluvoxamine
pregnancy outcome fluvoxamine- BPG p-value exvosed
live birth - 77 235 0.54 -
earlv spontaneous abortion - 7 16 0.67 -
O -
late spontaneous abortion 3 1 .O
theraveutic abortion - 3 9 0.25
ectopic pregnancy O O
stillbirth O - 7 1 .O
Table 19 - Birth Weight and Gestational Age for Live-Born Children
- Fluvoxamine
variable - -
fluvoxamine- BPG (n)
exposed (n) p-value
- - - - - -
birth weight (g ) 3434 + 529 (22) 3445 I 6 10 (235) 0.93
gestational age 39.3 F 1.8 (21) 39.4 -t 1.9 (235) 0.77

A total of 97 women were exposed to paroxetine in the first trimester. When
demographics of these women were compared to those of the BPG (Table
paroxetine-exposed women were found to smoke more than their controls but were
similar in al1 other variables measured.
Of the cases cvith information on the medication start date (n=72), most of the
women started paroxetine before thev were pregnant (n = 63). The dailv close rangeci
t'rom 10 to 61) mg (information amilable for 69 rvomen) and the mode t ïas dosage
kvas 30 mg od (n=39).

Table 20 - Materna1 Demographics: Paroxetine-Exposed vs BPG
variable paroxe tine- BPG p-value
exposed* . - - -. . - - - -
gravidity (g) g = 1 24 90 O. IS
g = 2+ 70 177
parity (p) p = O 38 125 0.51
p = l+ 53 142
previous spontaneous abortion (SA) SA=O
SA = l+ - - - - - - - - - - - -
previous therapeutic abortion (TA) TA = O 54 235 0.23
TA = 1+ 12 31 - -
tobacco consumption
Yes no
- -
alcohol consumption
Yes no
materna1 age at conception
* Seirerd centres h.id missing intorrnation ior i-arious parameters.

Five of the offspring born to ivomen exposed to paroxetine had a major structural
malformation (reier to Table 10). When statisticallv compared, the rates between the
two groups were not significantly different (Table I l ) .
Table 21 - Major Structural Malformations - Paroxetine
maj or structural paroxetine- BPG p-value
malformation exposed -
Yes 3 9 0.34
total 76 235
relative risk (95% confidence intemal) = 0.57 (0.20-1.68)
The ratio of non-exposed women in the BPG to parosetine-exposed women u-ho
had live-born children tvas 3.1:l. This allows a relative risk of 3.1 (17%) to be ruled
out for an increased risk of major structural maiformation due to paroxetine.

Tables 22 and 23 outline the pregnancy outcomes of the paroxetine-exposeci women
and the BPG. When the rate of live birth was compared to al1 other outcomes
between the two groups, women in the paroxetine-exposed group had a significantly
lower rate. Neither birth weight nor gestational age were statisticallv difterent
between the two groups. Eight children born to mothers who used parosetine in
pregnancy were premature and five were of low birth rveight.
Table 22 - Pregnancy Outcorne - Paroxetine
pregnancy outcome paroxe tine- BPG p-value
exposed
Iive birth 76 235 0.03
early spontaneous abortion 12 16 0.07
Iate spontaneous abortion 3 5 0.44
therapeutic abortion 6 9 0.24
ectopic pregnancy O O - s tillbirth O 3 1.0
o n e child in thc BPG m d onc child in the paroretinr-exposed group clicri in the nronotal
periocl
Table 23 - Birth Weight and Gestational Age for Live-Born Children - Paroxe tine
variable paroxe tine- BPG (n) p-value
exposed (n)
birth weight (g) 3424 _+ 600 (74) 3443 k 610 (235) 0.79
gestational age 39.2 i 1.9 (66) 39.4 k 1.9 (235) 0.29

A total of 147 women used sertraline in the first trimester. The maternai
demographics for these women and their controls are described in Table 24. The
women in the control group had a lower gravidity then the sertraline-eposeci
women. CVomen in the sertraline-exposed group smoked more than the women in
the BPG.
The majoritv of the sertraline-exposed women were using the drug at the time of
conception (n= 102, information available for 115 women). Dosage da ta were
available for 93 women. The dailv dosage mode was 50 mg ( n = 3 ) , and the daiiy
close ranged from 23 mg to 150 mg.

Table 24 - Matemal Demographics: Sertraline-Exposed vs BPG
variable* sertraline- BPG p-value
gravidity (g)
g = 1
-- - - - - -
previous spontaneous abortion (SA)
SA = O
SA = 1+ - - -
previous therapeutic abortion (TA) TA = O
TA = 1+
tobacco consumption
yes
no
alcohol consumption
Yes no
materna1 age at conception
* Sc\.crûl ccntrcs Iiad missing intorrnation for various parameters.

There were two children with confirmed major structural malformations in the
offspring of women who used sertraline in the first trimester ( T d d e 10).
Additionallv, there rvere two other anomalies reported without enough
information to label ciefinitively as major structural malformations. Due t» these
two cases, cornparison of major structural malformations between the two groups
was performed excluding these cases (Table 25) and including them (Table 26). The
two groups did not differ in either analysis.
Table 25 - Major Structural Malformations - sertraline
major structural sertraline- BPG p-value
malformation exposed
ves 7 - 9 O. 34
relative risk (95% confidence interval) = 0.51 (0.14-1.80)
Table 26 - Major Structural Malformations - Sertraiine
major structural sertraline- BPG p-value
malformation exposed
total 127 235
relative risk (9SoA confidence interval) = 0.82 (0.26-2.62)
There was a ratio of 1.9:l of women in the BPG to sertraline-exposed women whose
pregnancies resulted in a live birth. Post-hoc analysis reveals that the relative risk
of major structural malformation d u e to sertraline that may be ruled out h y this
shidv was 2.9, or 14.5'%.

The pregnancv outcornes of the women who used sertraline in the Cirst trimester
and their controls are summarized in Tables 27 and 28. There ivere no significrint
differences between the two groups for any of the variables measured. Tivo oi the
children in the sertraline-exposed group had low birth weight and 7 r w r e
prematurely born.
Table 27 - Pregnancy Outcome - Sertraline
pregnancy outcome sertraline- BPG p-value exposed
Iive birth 127 235 0.75
early spontaneous abortion 10 16 0. 9 1
3 - late spontaneous abortion 3 1 .O
therapeutic abortion 7 9 0.66
ectopic pregnancy O 0 - s tillbirth O - 7 0.54
one child in the BPG died in the neonatal prriod
Table 28 - Birth Weight and Gestational Age for Live-Born Children - Sertraline
variable sertraline- exposed (n)
BPG (n) p-value
- - - - -
birth weight (g) 3440 f 339 (125) 3445 I 610 (235) 0.93
gestational age 39.5 + 1.6 (120) 39.4 k 1.9 (235) 0.86
iwks)

3.6. EXPOSED FROM FIRST TRIMESTER TO THIRD TRIMESTER
A total of 49 women used one or more of the newer SSRIs through three trimesters
o t pregnancv. Al1 of these pregnancies resulted in a live birth. There were no
statistical differences betrveen the exposed and control groups for anv of the
Jemographic variables, except for increased use of tobacco in the esposecl g o u p (Table 29).

Table 29 - Materna1 Demographics: SSRI-Exposed from First Trimester to
Third Trimester vs BPG
variable' SSRI- BPG p-value exposed
gravidity (g) g = 1
previous spontaneous abortion (SA)
SA=O
SA = 1+
previous therapeutic abortion (TA) TA=O TA = 1+
tobacco consumption
alcohol consump tion
Yes no
materna1 age at conception
* Several ccntres h.id rnissing inionnation for various p.iranietcrs.

In the group of women exposed to a newer SSRI from the first trimester into the
third trimester of pregnancv, there were three major structural malformations (cases
#18S, #205 and #170). This did not statisticallv differ from the proportion of major
structural malformations in the control group (Table 30).
Table 30 - Major Structural Malformations - SSRI-Exposed From First Trimester
to Third Trimester
major structural SSRI-exposed BPG malformation
p-value
ves 9 0.44
- . -
total 49 235
relative risk (95% confidence interval) = 1.60 (0.45-5.69)
There was a ratio of -1.8 control pregnancies to each pregnancv exposed to a newer
SSRI through three trimesters of pregnancy. This ratio and the sample size oi 49
pregnancies nllows a relative risk of 4 to be ruled out.
The birth weights and the gestational ages oi the children were not different
between the tivo groups (Table 31). Since the women who were exposed to a newer
SSRI ~int i l the third trimester al1 had live born children, nominal pregnrincv
outcornes were not compared to the BPG. Three of the 49 cl-iildren born in the
SSRI-exposed group had low birth weight and 4 were premature.

Table 31 - Birth Weight and Gestational Age - SSRI-Exposed From First Trimester to Third Trimester
variable SSRI-exposed (n) BPG (n) p-value
birth weight (g) 3333 k 569 (48) 3445 k 610 (235) 0.24
gestational age 39.0 + 1.9 (48) 39.4 + 1.9 (235) 0.14

4.1. RESEARCH IMPLICATIONS - NULL HYPOTHESIS NOT RETECTED
First trimester exposure to the necver SSRIs did not increase the rate of major
structural malformations when compared to a control group of women rvho were not exposed to anv known teratogen in pregnancy. When each drug was ânalvzed
separately, results were similar.
.A structural malformation c m be associated with a d rus if exposure occurred a t the
time of structure formation. For example, thalidomide caused phocornelia onlv if
taken when the limbs were forming. Therefore, major structural malformations in
the SSRI-exposed group are individually assessed for overlap between timing of
drug exposure and organ formation in the foliowing paragraphs.
du pli catin^ renal svstems
Duplex ureters are cornmon (the approximate rate is 1/150), often inherited anomalies that rire frequentlv a s ~ m p t o m a t i c ' ~ ~ ~ C I t riras not possible to determine i f
cases #9 and #12 were inherited, so thev were classified as major structural
malformations rather than genetic anomalies in this study. This tvpe of
malformation is thought to occur when the pelvic end of the ureteric b ~ i d is expanding and dividing, approximateiy between 8 to 13 rveeks post-LMPh3. The
mather had stopped the medication before the 8 week point in both cases. therefore
neither case is likelv to be associated with the use of sertraline.
aeenesis of the corpus cailosum
Xgenesis of the corpus callosum is a complete M u r e of the allosal commissural
fibers to cross the midline and form the corpus callosum. The rate of this defect
ranges from 1 /1670 to 3 /1000f~~ , though it is likely higher since i t often goes
~indiagnosed when not associated with a syndrome"? Though the corpus callosum

forms between weeks 13-22 post-LMP, Barkovich and Norman (53) be1it.w that
agenesis of the corpus callosum is due to damage a t about 10 weeks post-LMP, before
the structure develops. Materna1 exposure to paroxetine (case #77) occurred
between 6 and 14 weeks post-LMP, so an association with the drug cannot be ruled
out.
ovarian cvsts
Neonatal ovarian cvsts are primarily of follicular origin and likelv develop et about
30 weeks post-LMP during folliculogenesis~~~. Thev mav form in response to
excessive stimulation of the fetal ovary by both placental and maternai hormones.
Neonatal cysts tend to occur more frequently in the offspring of mothers who had
diabetes, toxemia, or rhesus immunization during pregnancv. These comp l i a tions
a re hvpothesized to either increase placental secretion of human chorionic
gonadotropin or increase placental permeabilitv to human chorionic gonadotropin.
Case #170 did not suffer from anv of these complications and used parosetine
throughout her pregnancy; thus,the drug might be associated with the defect. The
ovarian cvsts were diagnosed at 7 months of pregnancy by ultrasound. Thev were
surgically removed in the neonatai period, along with an ovary and a fallopien tube.
bilateral clubfoot
Tho~igh clubfoot occurs rela tively frequentlv ( 3 . W 1000) 1" the etiology ot this defect
is ~ inknorvd~? Orthopedic surgeons hâve tounci clubfoot in products of conception
as early as 12 weeks post-LMPhY. Clubfoot can occur with varyinç degrees of severity,
and though tliere is currentlv no svstem for defining the severitv, the bilateral
clubfoot of the child in the SSRI-exposed group was corrected surgicallv so i t c m be
essumed that i t tuas CI seiverer forrn. As the mother of the child with c lubhot had
used parosetine tintil 31 weeks post-LMP, it is possible that the drug rvas associated
with the defect.
cardiac defects
The h a r t forms t'rom week 5 to week 11 post-LMP. Cardiac malformations occur in
about 5 to 8 of every 1000 live births? There were two cases of a child born with a
cardiac malformation. In one case (#197) the mother used sertraline until S weeks
post-LMP and in the other case (#222) the mother used paroxetine in the first

trimester for an unspecified arnount of time. In case #197, the drug exposure and
time of heart formation overlap. In case #222, while it is known that the mother
ujed paroxetine in the first trimester, a stop date (if any) is unknown, so rvhether
drug use and heart formation overlap is undetermined. In both cases the
underlying structural malformation was not recorded by the teratogen information
service. however case #272 needed an operation to repair the malformation at threr
weeks postnntally, thus i t can be assumed that this was a major structural
malformation. There was not an exact diagnosis for case #197, which ma)- have
been a minor cardiac malformation such as a left vena cava. Since there was no!
enough information to label definitively the anomaly as either major o r minor,
sensitivity analvsis was performed including and excluding case #197 as a major
structural malïormation. Given the Lack of information in both cases, it is difficult
to assess whether the drug could have been associated with either defect.
external auditorv cana1 stenosis
This defect is normally associated with a genetic syndrome or microtia (hypoplasia
of the auricle) and isolated external auditory canal stenosis is quite rare (2/100,000)3'.
The child of case #200 was awaiting testing to confirm diagnosis of estemal auditor!.
canal stenosis without microtia when the family moved and the teratosen
information service lost touch with the farnily. This child may have subsequently
been tested and found to have one of the several genetic syndromes associated with
this defect. but as this \vas unknown the case was included as a major structural
malformation. Since diagnosis was not cont'irmed a sensitivitv analvsis was
performed. The external car forms from 7 1 / 2 weeks to 24 weeks post-LM? As the
mother stopped using sertraline at 6 weeks post-LMP, this defect is not likely
attributable to use of sertr a 1- me.
pvloric stenosis
Pvloric stenosis is the hvpertrophv of the muscular pyloric canal, leading to a
thickening of the pvloric wall and a reduction in the size of the lumen? It is a
relativelv cornmon defect (3,4000) and usuallv arises in the late perinatal period or
early postnatal life? Rollins" performed ultrasound examination in the neonatal
period on 1400 consecutive infants which were al1 negative for pyloric stenosis, yet
nine children later developed pyloric stenosis. However, pyloric stenosis can occur

in early embryogenesis. I t can also be a familial trait or associated kvith genetic
svnctromes (70). Since the rnother ~ised paroxetine throughout her pregnancv and i t
is ~inknown if the pvloric stenosis was present at birth, the defect mav be associated
with the drug.
In summarv, of the nine major structural malformations reported in the SSRI-
exposecl group, an association between the newer SSRI and the defect mav not be
ruled out for six of them.
4.1.2. PREGNANCY OUTCOME
There were no differences between the SSRI-exposed women and the BPG in any of
the measured pregnancv outcome variables. When each SSRI was analyzed
separa tely, paroxetine-exposed rvomen had a significan tlv lower rate of li\-e birth
than the BPG. I t must be remembered that a large number of cornparisons were
performed in this study, and this finding may be due to chance (type I error). I f the
lorver lil-e birth rate in the paroxetine-exposed group was clinically significant, ive
~ v o u l d espect to see a corresponding increase in another nominal pregiiancy
uutcome variable, such as rate of early spontaneous abortion. Since this was not
seen, likelv this finding is not clinically significant, though further studies rïit1.i
larger sample sizes ma y chri- this.
Children born to mothers who smoke have been tound to have a significantl>r lower
birth weight than the offspring of non-smoking womenï3. Therefore, it is curious
that although there was a higher rate of tobacco consumption in the SSRI-esposed
group, there was no difference in the birth weight of live-born children wlien
compared to the control group. Children exposed to one of the newer SSRIs i i i
i r t~v-o may have a higher birth weight. To determine if this is so, post-hoc analysis
compared the birth weights of liveborn children born to SSRI-exposed mothers who
did not smoke to the birth weights of the liveborn chiidren in the control group
(Table 32). Nci s ta tistical difference was seen.

Table 32 - Birth Weight of SSRI-Exposed Non-Smokers vs BPG
SSRI-exposed BPG p-value
There are se~*eral possible explanations. In this study, a woman was considered a
smoker if she reported tobacco consurnption at anv time during pregnancy. If the
woman reported smoking at the time of initial interview, but quit a t 10 cveeks oi
gestation, she was still categorized as a smoker. It is known that if a woman quits
smoking earlv in pregnancy, the effect of smoking on birth weight is negated?
Additionallv, there is a dose-response seen between the amount of cigaret tes
smoked per dav and the decrease in birth weight, the higher the number of
cigarettes, the lower the birth weight? [f a woman in the SSRI-exposed group rvas
smoking one cigarette a day, the birth weight may not have changed to an\ -
significant extent. Since the amount of cigarettes smoked per day and exactlv when
in pregnancy the cvoman smoked were not recorded in this study, it is not possible
to take the above factors into account when analyzing birth weight and tobacco
consump tion.

4.2. LIMITATIONS OF THE STUDY
Recall bias is a potential in any retrospective studv. In this study mothers were
interviewed earlv in pregancv about their current esposure historv, hcnvever,
follow-up required maternai recall of events occurring in pregnancy after the initial
interview. These could not have changed, however, either the primarv outcome
measure (major structural malformations) or the primary independant variable
(esposure to a newer SSRI), however, recall bias mav have affected two ot the
secondary outcome measures of interest, namely birth weight and gestational age.
A recent studv found that there was a high correlation between maternal recall and
medical records for gestational age and birth weight7K However, there was a poor
correlation for post-deliverv complications/problems and pregnancy complications.
These results did not significantlv differ when the time between delil-erv and
maternal interview \vas taken into consideration. Additionallv, a l tho~igh
klotherisk routinelv requests the labour and delivery forms t'rom the child's
plivsician, otten the phvsician does not have these forms because either he/shc is
iiot the mother's physician or he/she simply did not receive a copv. From my
experience interviewing patients. though questions regarding pregnancy and
delivery complications are asked, the rnothers a re uncertain of the mecliccil
definitions. For cxample, when asked about k ta l distress they mav recall that "the
heart-rate went up, so yes, there was fetal distress", but wlien the deliverv report is
received, this \vas not defined as fetal distress. Therefore, this thesis did not ~7naIvze
ma ternal pregnancv complications and post-delivery complications.

A patient was considered lost in the following events:
phone nurnber not in service/wrong phone number, no new listing in phone
book/directorv assistance
no answer after contact attempted over a period of two months a i least 10
tirnes/phone number on different days, at different times
no longer at work place, no forwarding phone number
patient deceased
The concern with follow-up loss is if there is a difference in pregnancv outcome in
the women included in the study and those who were iost to follow-up. A s there is
no way to determine whether or not this is the case, baseline maternal
demographics were compared between women included in the s t ~ i d v and tl-iose who
were lost to follow-up.
When the Motherisk cases that were successfullv followed up were compared to
those that were lost to follow-up (Table 3, almost none of the variables differed
statistically between the two groups, except for ethanol consumption. The ~vornen
who were interviewed after pregnancy reported a higher rate ot ethanol
consumption. Though Motherisk records ethanol and tobacco use on intakc and
clinic forms, it is a report about the mother's current habits. During follon--up, the
motlwr is asked about exposures throughout the pregnancy. This mav account for
the difference in ethanol reporting between the two groups.
4.2-3. DEMOGRAPHIC DIFFERENCES BETWEEN EXPOSED AND CONTROL GROUPS
I f there are differences in the maternal baseline demographic variables, it may
indicate that women from two different populations are being observed. I f this is
truc, the groups mav not be comparable due to confounding variables.
Wumen in the SSRI-exposed group smoked more than those in the BPG (Table 9).
This is not surprising as it is well documented that tobacco consumption is
associated with depression;;t's? This pattern was also seen when each of the

SSRIs were analvzed separately. Women in the SSRI-exposed group had a
significantlv higher graviditv and number of previous therapeutic abortions when
compared to the control group. The higher number of previous therapeutic
abortions is likelv associated to the higher gravidity. When each drug was analvzed
separatelv, hoivever, onlv sertraline-exposed mothers had a higher rate of graviditv
compared to the control group. Post-partum depression occurs in about 1>"1, of
women after the birth of a child". Additionally, depression commonlv occurs after
a spontaneous abortion"' S. If women were treated by an antidepressant due to
post-partum depression or depression following a fetal death, this mav esplain the
finding of higher gravidity in the SSRI-exposed group.
This studv could only rule out a 2.5-fold increase in baseline risk. However, many
known teratogens cause an increase in baseline risk below this level. Valproic acid
for example, increases the risk of neural tube defects from about 0.13":, to 1-2%"'.
Though this is a 17-fold increase in the risk for neural tube defects, i t is onlv a 1.4-
M d increase in the baseline risk for major structural malformation. The sample
size of this strtdv would not have been able to detect an increase of that size. Future
studies with larger sample sizes would increase the power to detect a smaller
increase in the baseline risk of major structural malformation.

4.3. RECOMMENDATIONS FOR FUTURE RESEARCH
Although this studv has provided initial results on the safetv of the newer SSRis in prepancy, future study is required. While each of the drugs studied beiong to the
same drug class, thev are distinct in their structure, pharmacokinetics ancl
metabolism. For these reasons, each d rug should be studied indiviiluallv. Concurrently, the sample sizes couid be increased. As mentioned above, an increase
in sarnple size is necessary to rule out a smaller relative risk. Future cohort studies
are thus needed.
It is becoming evident that not only structure c m be affected by drug exposures, but
brain tunction as well. In the case of medications such as antidepressants and
antiseizure drugs with their primary site of action on the brain, this concern mav be
well-fo~~nded. For example, children exposed to pheny toin in trtrro haci lower
global intelligence quotients (IQs) thân a control g r o u p u . Rejiarding
antidepressants, ri recent study exarnined the neurodevelopment of pre-school
children whose mothers hâd used fluoxetine or tricyclic antidepressants in the first
trimester of pregancy? Of the children assessed, 55 had been exposed to fluoxetine
and ranged in age from 16 to S6 months (mean, 33 f 14). The global intelligence
quotient (LQ) of these children (117 + 17) did not differ t'rom the two control groups
consistirtg of children esposed to tricyclic antidepressants (n = 80, IQ = 11s + L7, and
children not exposed to anv known teratogen (n = 8-4, IQ = 113 k 14). A s « testecl and
not iound to differ were language and behavioural development. This stuciv was
onlv able to identify structural abnormalities, yet the full picture of fetal drug safety
includes exploration of functional abnormalities. Future studies on the cl-iildren
esposed to the newer SSRis i l i iriero followed-up by Motherisk are therefore
warranteci.

4.4. RECOMMENDATIONS FOR COUNSELLING AT MOTHERISK
4.4.1. WOMEN PLANNING PREGNANCY AND PREGNANT WOMEN PLANNING TO U S E A
NEWER SSRI
Though the results of this study are reassuring, the sample size (POWER) was too
small to draw definitive conclusions (see section 4.3.5). As there are manv other
antidepressants such as fluosetine and the TCAS" currently aïailable fur which
more data regarding pregnancy exist, counselling should direct the woman or her
health care provider towards a different antidepressant medication. Further, since
Çluoxetine and the tricvclic antidepressants have been found to be also safe in
neurodevelopmental studies", they should be the cirugs of choice. If the woman is
unable to use u different anti-depressant (Le.. when previous trials with fluoxetine
and tricvclic antidepressants have been unsuccessful), a clinic appointment with one
ut the Motherisk team phvsicians should be arranged to ensure that the intorrnation
is clearly understood by both the patient and the patient's health care provider.
4.4.2. WOMEN WHO ARE CL'RRENTLY PREGNANT AND USING A NEWER SSRI
Although the newer SSRIs did not cause a large increase in the baseline risk t'or
major structural malformations, a smaller increase cannot yet be ruied out due to
the sample size. The patient and/or health care provider, therefore, sl-iould be
counselled that a n initial study did not demonstrate an increased risk, but thùt therc
are other antidepressant medications for which there is more experience with use in
pregnancy. Separate analysis of each of the newer SSRIs did not suggest an increased
risk of major structural malformations, however, the sample size varied between
the drugs. While both sertraline and paroxetine had a relativelv large sample size (n =147 and n=97 respectively), for an initial prospective cohort studv, the sample size
available for t'lu\-oxamine kvas quite small (n=26). Based on these sample sizes,
women usin): fluvoxamine should be offered a c h i c visit to thoroughly review the
information xailable with a team physician. Women using either paroxetine or
sertraline may be counselled over the phone regarding the results of the s t~ idy , and
i f she is anxious, a clinic visit should be suggested.


Figure I - Mothensk Intake Form
~ O C I
mmpldcd O pasrd ln rJIow0 -pCPrv 0VK;OWG:
aiicofbinh h o ? YQ ~ 0 0 ~ v i s e d O lun~:
oooiplacd by: R c r d by: > Hdrh cnrd P
G P S A TA- & ï ~ i a p r * i a n ~ ? k o ~ a
Gdncy N o 0 Y u
H u n N o 0 Ya
Hypprnisioa N o 0 Ya
Diabcia N o 0 Yes
Rcspirztory N o 0 .Yu
Thymid N o 0 Y u
Fsychiairic N o 0 Ya
Epilepq N o 0 Yu
Viumin suppIerncnutian? N o 0 Ycs:
O<her
Cilnlc date: bring transhtor O
Refend ha& ta MD for suqqesfi~n of medications 5 1

Figure 2 - Motherisk Clinic Fonn
1 MOTHERISK PROGRAM ANTENATAL CLlNlC FOR DRUGICHEMICAL RlSK COUNSULING THE OlVlSlON OF CLlNlCAL PHARMACOLOGY. HOSPiTAl FOR
SlGK CHILDREN. TORONTO, ONTARIO
MOTHERISK NUMBER CONSULTATION DATE (dmily)
MATERNAL DATA
NAME: Biological fethcr's name:
Addrmss: Address: crme as mocher [ ]
Ikte of b l m (m) ~ i t e of blrlh (-1 HOm tdophoru: ( ) Homa Ukphono: rrns [ 1 [ 1
Work tikphonm: ( ) Wark toiophoru : ( )
Contraception

Last Menstrual Period (w ~ y d r -y - days r - days bleeü-ü~
Expected Dellvery Date (-1 Cunent Gestational Age - wk [ j ,-th [ 1 b v : & a a + I l u-[l
Regnancy dlagnosd at wks [ ] manths [ 1 By whkb rnthod? [ 1 bbod tasi [ 1 urina lm [ ] uttrasaund
PRlMARY E X P O S U INFORMATfON
A. Over-ihe-counter and PmscripUon Medicallons OR Radbtlon

B. Chernical Exposures
Ocaipation Tik: matemalD ~aternatu
STAR7 DATE of oxposum STOP DA= of exposrar
Siart date 1 1 1
, Additional Room on page 8
3

ADDKIONAL MATERNAL EXPOSURES & HlSTORY
Genetic Disease or Malformations ND ~a Relative of mother Condition ReMk of
biokfflcal father Condttkn

PAST MATERNAL MEDICAL HISTORY
Cancer NO YU Cardiovascular NO YU mntrai nemous systarn NO Y O Diabetes ND YU Epitepsy NR YU Hematology NU Yu Hypertension NO YU Rena t disease NU YU Thyroid disesse NU YU
BlOLOGlCAL F ATHER DATA
ORUG NAME
Indication for meâht iun kbnc &tails &bout madical wnditiùn
Tobacco NU Y a cgarsnss per day (1 wsek [ ] rvsdrend [ j manth [ ]
Cocaine NO YU duringpiqnancy p e r d a y [ ~ w e e k [ ~ ~ ~ [ l Marijuana NO Y U d n p w o p n y p c r d a ~ [ l - k [ l - - j [ l mmI1 LSD N Y a during pragnancy p e r d a ~ [ l w - k [ I ~ ~ [ l m~mil
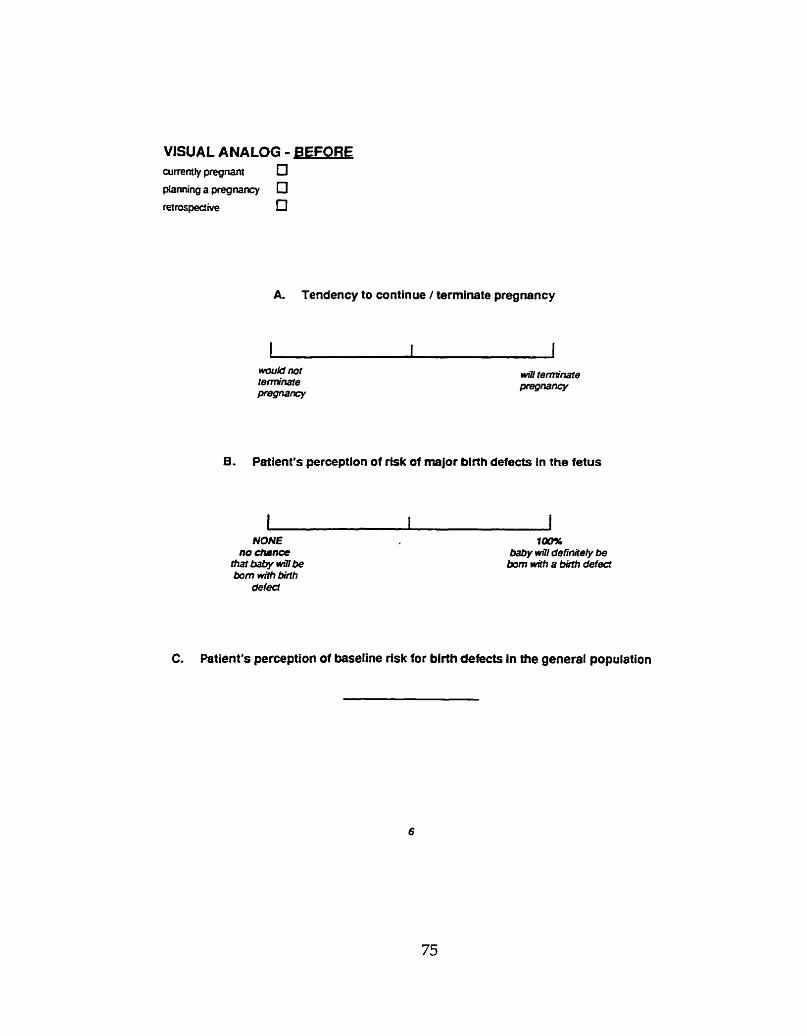
A. Tendency to continue / terminate pregnancy
B. Patient's perception of rfsk of major birth defects In the fetus
1 I I NONE f4MC
no diSnce baby w3i definite@ be ttiaibabywüfbe barn wüh a bhfh defect h m wilh brilh
defed
CI Petient's perception of basellne risk for birth defects in the general population
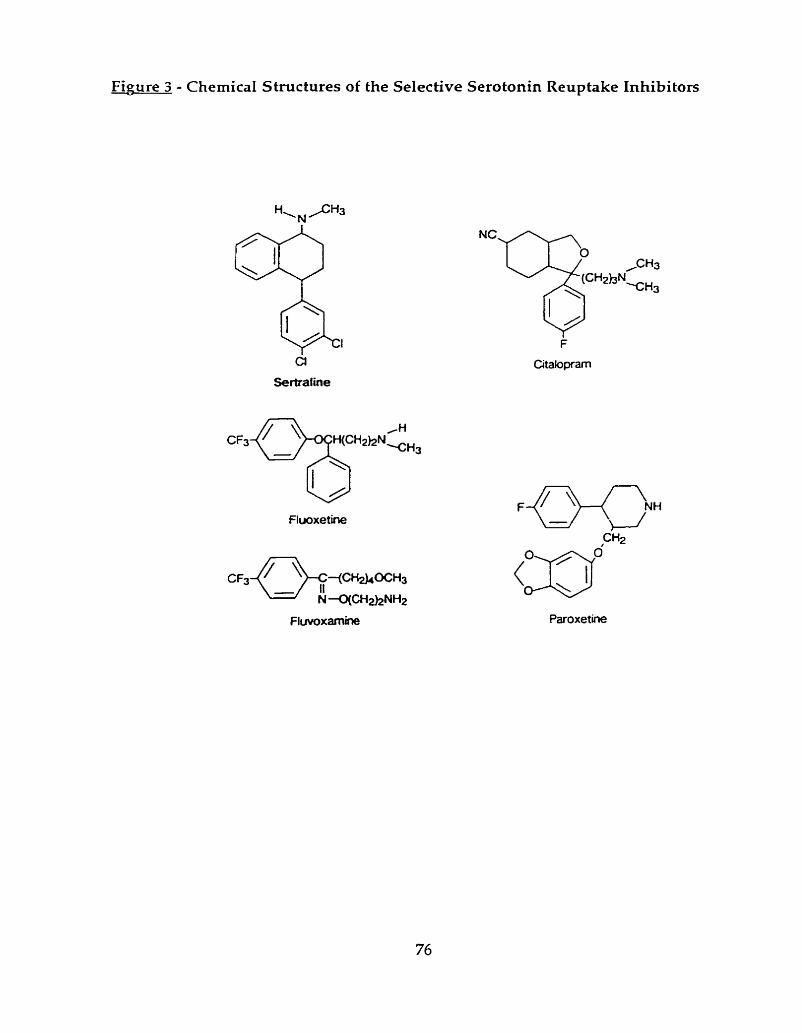
Figure 3 - Chernical Structures of the Selective Serotonin Reuptake Inhibitors

Fiaure 4 - Motherisk Follow-Up Form
Pregnancy Follow Up Form MOTHERISK PROGRAM
Clinic Number
Date of lntewiew lntem-ewer
A. GENERAL
B. PREGNANCY OUTCOME
C. OISEASES COMPUCATlNG PREGNANCY

D. MPOSURES DURING PREGNANCY
Did you u s any zhing for ilkglu, mxkty, -16, c o i r d l p d o ~ dqwudon. dlirrhu, hudich., haartburn, pal% mlght
Ouupauon during prcgnuicy *job da4iption (WWT W U SHE DO?) stanrd smppcd Rclsan
QCPOSURES? c)icmid 0"" OP: wmpuœr o n 0 O F &n O F noidvibracion ana

E. TESTS DURlNG PREGNANCY
Chononic villus nmpling Alpha-fcco prorcin üitnsound
F. DELIVERY INFORMATION
Matemal Neonatal
We*r prc-prcg-cy - Ib k g HospiuJ/City
For wr own documentation, which wll help aher women expasad 10 the same dnigs ttrat you were exposed to. wuild yw d w e wiih os wtiether ywr chi@ was bom with any birth defeds?

G, NEONATAL HEALTH
OTHER
H. MILESTONES
Darc lerta s a i t Dace lccrer rcccivcd
1. CONSENT -
Wo wlouid Iiki to wnd a kttn to your chlWa doctorto conilnn mrdW chtalh of t h im tolbwup. Mey m hnn your wibil p.nnl#lon to wnd thb?
OBTAlNEO COUSEKT 0 no O p*

Fieure 5 - Motherisk Follow-Up Letter to Offspring's Health Care Provider
5 5 5 UNIVERSITY A M N U E TOROKïO. OhTANO CWAD.4 M5C 1- THE HOSPITAL FOR SICK CHILDREN PHONE (416) 813-I5O<)
Dr.
b Dr. :
Re: D.O.B.
On I W X X G . your patient's rnother was counselled by rhc Motherisk Program at
the Hospital For Sick Children. During a telephone interview to ascertain pregnancy
outcorne. we were given verbal consent to contact you to corrobonte the medical
details of XXX's health.
If available, would you send us a copy of the hospiral's labour and delivcry f o m
and a copy of the hospital's neonatd assessrnent r o m ? In addition. would you
pl- cornplere the attached form and return it to us ar the hlotherisk Program?
Thrink you for your anticipated CO-openrion.
Yours sincerely .
NathaIie A. Kulin BSc /Or Gideon Koren. MD. ABMT. FRCP(C).
Direcior. Morherisk h o p m

Mother's Name: Chiid's Name:
Original: patient number: Return forms to: Nathalie A. Kulin
Regarding the development of this child:
A. Major anomalies [ 1 no [ ] yes Description:
B. ,Minor anomalies [ ] no [ 1 yes Descriprion:
C. This child was 1st examined on (dd.mrn.yyl. At that m i l :
wcight
height 1 lengrh
head circurnference
D, Hosprtal labour & delivery fomts are included
Hospital nconatal assessrnent forms are included
Signaturc of physician:

Alcohol
Androgens
ACE inhibitors
Carbarnazepine
Coumarin
Cvclophosp hamide
Diethylstilbestrol
Dipheny lhydantoin
Etretinate
Iso tre tinoin
Lithium
Me thvlmercury
Misoprostol
Propylthiouracil
Radiation (fetal dose of 10 radsi)
Thalidomide
Valproic Xcid

Gregg NkI. Congenitâl cataract follorving yerman measles in the rnother.
Transactions of the Op thalmological Society of Aus tralia l9-U ;X5--L6.
McBride WC. Thalidomide and congenital abnorrnalities [letter]. Lancet
l%I;2: 135s.
Lenz W. Thalidomide and congenital abnormalities [letter]. Lancet 1962; 1A3.
Lenz W. Limb defects: ovenViervs and recommendations. Progress in Clinical
and Biological Research 1985;163C:73-75.
Smithells RW. Dcfects and disabilities of thalidomide cl-iildrcn. British Medical
Journal i973;1:269-272.
International Conference on Harmonisation of Technical Requirements tor
Registrntion of PI-iarrnaceuticals Steering committee. [CH harmonised tripartite
wideline: detection of toxicitv to reproduction for rnedicinal products. lYC1?. h
Shepard TH. Catalog of teratogenic agents. 5th ed. Baltimore: Johns Hopkins
Press, 19S6.
Hm-tminki K, Vineis P. Extrapolation of the evidence o n teratogenicit~. O t
chemicals between humans and experimental animals: chemicals other than
d rugs. Tera togenesis, Carcinogenesis, and Mu tagenesis l985;5:251-3lS.
Piccinino LI. Unintended pregnancy and childbearing. In: Wilcox LS, Marks JS, eds. From data to action: CDC's public health surveillance for women, infants,
and children. Atlanta, GA: US Department of Health and Human Services,
Public Health Service, Centers for Disease Control and Prevention, lC)9,5:/3-S3.

10 Cunningham FK, Leveno FG. Childbearing among older women - the message
is cautiouslv optimistic. New England Journal of Medicine 1995;333:1002-1004.
I l Koren G. New expectations for the role of clinical pharmacologists and industrv
in protecting unborn babies and their mothers. Canadian Journal oi Cliniial
Pharmacology 1997;4:62-63.
I I Werler MM, Pober BR, Nelson K. Holmes LB. Reporting accuracy among
mothers of malformed and nonmaiformed infants. American Journal of
Epidemiology 1989;129:415-421.
13 Schneiderman IF. Nonmedical drug and chemical use in pregnâncy In: Koren
G , editor. Maternai- fetal toxicology: a clinician's guide. 2nd rev. cd. N e w York:
Marcel Dekker, 1994:301-319.
14 Marden PM, Smith DW, McDonald MJ. Congenital anomalies in the newborn
infant, including minor variations. Journal of Pediatrics 1964; 64:357-371.
15 Leppig KA, Werler MM, Cann CI, Cook CA, Holmes LB. Predictive value of
minor anomalies: association with major malformations. Journal of Pcdiatrics
19S7;l lO:53l-337.
16 McIntosh RI blerritt KK, Richards MR, Samuels MH, Bellows MT. Incidence of
çongenital mal formations: a stud y of 5,964 pregnancies. Pedia trics l%-l; l-L:505-
421.
17 Mvrianthopoulos NC, Chung CS. Congenital malformations in singletons:
epidemiol»gical survey. Miami FL: Svmposin Specialists, 1974.
18 Heinonen OP. Birth defects and drugs in pregnancy. Littleton MA: Publishing
Sciences Group, 1977.

Shepard TH. Human teratogenicitv. In: Barness L, editor. Advances in pediatrics.
Chicago: Year Book Medical Publishers, 1986.
Spranger J, Benirschke K, Hall JG, Lenz W, Lowry RB, Opitz JM, Pinskv L, Schwarzacher HG, Smith DW. Errors of morphogenesis: concepts and terms.
Pedia trics l982;lOO: 160-165.
World Health Organiza tion. Manual of the in terna tional s ta tistical ciassifica tiim
of diseases, injuries and causes of death. Geneva: World Health Organization,
1957.
World Health Organization. Manual of the international statistical classification
of diseases, injuries and causes of death. Geneva: World Health Organization,
1979.
Warburton D, Stein 2, Kline J, Susser M. Chromosome abnormalities in
spontaneous abortion: data from the New York City studv. In: Porter IH, Hook
EB, editors. Human embrvonic and fetal death. New York: Academic Press,
198W61-2S6.
Shapiro HS, Levine HS, Abramowitz M. Factors associatrd with early and late
tetal loss. Proceedings of the Eighth Annual Meeting of the American
Association o t Planned Parenthood Phvsicians, Advances in Planned
Parenthood, Vol VI, Excerpta bledica, 1971.
Hall JG, Stevenson RE. Terminology. In: Hall JG, Stevenson RE, Goodman RM, editors. Human malformations and related anomalies volume 1. Newf York:
Oxford University Press, 199321-30.
Schnrdein JL. Chemically induced birth defects. New York: Marcel Dekker, 1985.
Pastuszak A, Schick-Boschetto B. Zuber C, Feldkamp M, Pinelli M. Silm S.
Donnenfeld A, kIcCormxk M, Leen-Mitchell M, Woodland C, Gardner A, Horn

!VI, Koren G. Pregnancv outcome following first-trimester exposure to tluoxetine
I Prozac). Journal of the American Medical Association 2993;269:2246-3348.
2s Donnenfeld AE, Pastuszak A, Salkoff-Noah J, Schick B, Rose NC, Kclren G.
Methotrexate exposure prior to and during pregnancy [letter]. Teratologv
1994;19:79-81.
29 Jacobson SJ, Jones K, Johnson K, Ceolin L, Kaur P, Sahn D, Donnenfeld AE,
Rieder M, Santelli R, Smythe J, Pastuszak, Einarson T, Koren, G. Prospective
multicentre studv of pregnancv outcome after lithium exposure during first
trimes ter. Lance t 1992;339:530-533.
30 Xmerican Psvchiatric Orgnanization. Diagnostic and sta tistical mnnual ot
mental disorders. 4th ed. Washington, DC: American Ps~ch i a tric Organization,
1994.
31 Weissman MM, Leaf PJ, Tischler CL Blazer DG, Karno Ad, Livingston-Bruce M. Florio LP. Affective disorders in five United States communities. Psvchologicai
Medicine 1988;lS:141-153.
32 Weissman MM, Bland RC, Canino GJ, Faravelli C, Greenwald S. Hwu HG, Jovce
PR, Karam EG, Lee CK, Lellouch J, Lepine JP, Newman SC, Rubio-Stipec M, Wells JE, Wickramaratne PJ, Wittchen H, Yeh EK. Cross-national epiderniology
of major depression and bipolar disorder. Journal of the American Medical
Association 1996; 276293-299.
33 Parikh SV, Wesvlenki D, Goering P. Wong J. Mood disorders: rural /~irban
differences in prei~alence, health care utilization, and disnbilitv in Ontario.
Journal of Affective Disorders 1996;38:57-65.
34 Statistics Canada. National Population Health Survev. Prevalence of depression,
by age and sel. Ottawa: Statistics Canada, 1995.

35 Arpino C, Da Cas R, Donini G, Pasquini P, Rascetti R, Traversa G. Use and
misuse of antidepressant drugs in a random sample of the population of Rome,
Italv. Acta Psychiatrica Scandinavica 1995;92:7-9.
36 Crane GE. Iproniazid (Marsilid) phosphate, a therapeutic agent for mental
disorders and debilitating disease. Psychiatry Research Reprints l957;Y: 142- 152.
37 Kuhn R. The treatment of depressive states wi th G - 2 3 4 4 (imipramine
hvdrochloride). American journal of Psvchia try . 1958; 1 15:-i59-46-L.
38 Preskorn SH. Clinical pharmacology of selective serotonin reuptake inhibitors.
Caddo OK: Professional Communications, 1996.
39 Preskorn SH, Irwin HA. Toxicity of tricyclic antidepressants - kinetics,
mechanisms, intervention: a review. Journal of Clinical Psvchiatrv. 1982;43:151-
7 56.
40 Guze SB, Robins E. Suicide among primary affective clisorders. British Journal of
Ps ychiatry 1970;117:437-438.
41 Hagnell O, Lanke J, Rorsman B. Suicide rates in the Lundbv s t~idv: mental
illness as a ris k factor for suicide. Neuropsvchobiology 1981 ;7:XS-E3.
42 Preskorn SH. Comparison of the tolerabilitv of bupropion, tluusetinc,
imipramine, nefazodone, paroxetine, sertraline and venlafaxine. Journal of
Clinical Psychiatry. 1995b;56(suppl 6 ) : l X l .
43 Janicak PG, Davis JM, Preskorn SH, Syd FJ Jr. Principles and practices of
psychopharmcotherapy. Baltimore, MD: Williams and Wilkins, 1993.
44 Finlev PR. Selective serotonin reuptake inhibitors: pharmacologic profiles and
potential therapeutic distinctions. Annals of Pharmaco therapy l994;B: 1359-1369.

Hovt J4, Bvrd RA, Brophv GT. Reproduction study ot fluoxetine livdrochloricle
administered in the diet to rats [abstract]. Tera tology 1989;39:459A.
Bvrd RA, Markham JK. Developmental toxicolooy studies of t ' l i io~etine
hvdrochloride administered orally to rats and rabbits. Fundamental and Applied
Toxicology l994;22:5ll-j 18.
Goldstein DI, Marvel DE. Psvchotropic medications during pregnancv: risk to tlie
k tus [letter]. Journal of the American Medical Association 1993;270:2177.
Chambers DC, Johnson KA, Dick LM, Felix RJ, Jones KL. Birth outcomes in
pregnant women taking fluoxetine. New England Journal of blcciicine
l996;335:1010-1015.
Xddis A, Koren G. Safetv of fluoxetine during the first trimester of pregnancy:
meta-analv tical review of epiderniological studies [abstrnct]. Tern t«I»gv
1997;55:37-35.
Product information. Luvox. Solvav Kingswood, 1991.
Edwards JG, Inman WHW, Wilton L, Pearce GL. Prescrip tion-event monitoring
of 10401 patients treated with fluvoxamine. British Journal of Psvchiatrv
2 9%;l6M87-395.
Szabadi E. Fluvoxamine withdrawal svndrome [letter]. British Journal of
Psvchia trv lC)92;l6U:X+284.
Baldwin !A, Davidson EJ, Pritchard AL. Ridings JE. Reproductiw tosicologv ot
paroxetine. Acta Psychiatrica Scandinavica 1989;350:37-39.
Product information. Paxil. Smi thKline Beecham Pharmaceri ticals, 2995.

53 Inman W, Kübota K, Pearce G, Wilton L. PEM report number 6. Paroxetine.
Pharmacoepidemiology and Dmg Safety 1993;2:393-422.
56 Personal cornmunica tion with SrnithKline Beecham Pharmaceuticals, 19%.
57 Product information. Zoloft. Pfizer Pharmaceuticals, 1994.
58 Persona1 communication tvith Pfizer Pharmaceti ticals, 1996
59 Statview SE + Graphics [computer program]. Version 1.03. U.S.A.: ;\bacus
Concepts, 1988.
60 Epi Info [computer program]. MS-DOS version. U.S.A.: Centers for Disease
Control and Prevention (CDC), 1994.
61 Atwell JD, Cook PL, Howell CJ, Hyde 1, Parker BC. Familial incidence of bitid and
double ureters. Archives of Disease in Childhood 2974;49:390-393.
62 Whitaker J, Danks DM. A studv of the inheritance of duplication of the kidnevs
and ureters. Journal of Urology 1966;95:176-178.
63 Gray SW, Skandalakis JE. Ernbrvology for surgeons: the embrvological hasis for
the treatment of congenital defects. Philadelphia: WB Saunders, 1971.
64 Hrinter AGW. Brain. In: Stevenson RE, Hall JG, Goodman RM, editors. Human
malformations and related anomalies: volume II. New York: Oxford University
Press, 2993: 1-107.
65 Barkovich AI, Norman D. Anomalies of the corpus callosum: correlation with
tur ther anomalies of the brain. American Journal of Roentgenology
1988;151:171-179.

Schmahmann S, Haller JO. Neonatal ovarian cysts: pathogenesis, diagnosis and
management. Pedia tric Radiology l997;W: lOl-lO5.
Carroll NC. Clubfoot: what have we learned in the 1,751 quarter centurv? Journal
of Pediatric Orthopedics 1997;17:1-2.
Settle GW. The Anatomv of congenital talipes equinovarus: sixteen dissected
specimens. The Journal of Bone and Joint Surgery 1963;45A:1341-1354.
Larsen WJ. Human embryology. New York: Churchill Livingstone, 1993.
Carev JC. Esternal car. In: Stevenson RE, Hall JG, Goodman RM, editors. Human
malformations and related anomalies: volume II. Nen7 York: Oxford Uniwrsitv
Press, 1993: 193-229.
Hoyme HE. The upper gastrointestinai s r s t em . In: Stevenson RE, Hall JG, Goodman RM, editors. Human malformations and related anomalies: vcilumt.
II. N e w York: Oxford Universitv Press, 2993415-443.
Rollins MD, Shields MD, Quinn RJM et al. Pvluric stenosis: congenital LN-
acquired. Archives of Disease in Childhood 1989;64:138-139.
Fox SH, Koepsell TD, Daling JR. Birth weight and smoking during pregnancl- - effect modification bv materna1 age. American Journal of Epiderniology
1994;139:1003-1015.
Ahlsten G, Cnattingi~is S, Lindmark G. Cessation of smoking during pregnancv
improves foetal growth and reduces infant morbiditv in the neonata1 perioci.
Acta Paediatrica l993;82: 177-182.
Ellard GA, Johnstone FD, Prescott RJ, Ji-Xian W. Jian-Hua M. Smoking during
pregnancy: the dose dependence of birthweight deficits. British Journal of
Obstetrics and Gvnaecology 1996;103:806-813.

76 Oison JE, Shu XO, Ross ]A, Pendergrass T, Robison LL. Medical record
validation of ma ternally reported birth characteristics and pregnancv-rela ted
events: a report from the children's cancer g r o u p Xmerican Journal of
Epidemiology 1997;145:58-67.
77 Son BK, klarkovitz JH, Winders Sr Smith D. Smoking, nicotine dependence, and
depressive svmptoms in the CARDIA study. Effects of educntional status.
Arnerican Journal of Epidemiology 1997;145:110-116.
78 Breslau N. Psychiatrie cornorbiditv of smoking and nicotine dependence.
Behaviour Gene tics 1995;25:%-lOl.
79 Tamburrino MB, Lynch DJ, Nage1 RW, Stadler N, Pauling T. Screening women
in family practice settings: association between depression and smoking
cigarettes. Familv Practice Research Journal 1994;14:323-337.
SO OrHara MW, Neunaber DJ, Zekoski EM. Prospective studv of postpartum
depression: prevalence, course, and predictive factors. Journal of Abnormal
Psvchology 1984;93: 133-1 7'1.
81 Tl-iapar Ak, Thapar .A. Psychological sequelae of miscarriage: a controlled studv
usin the general health questionnaire and the hospital anxietv and cleprssion
scn le. Bri tis11 Jorirnal of General Practice 1992;42:94-96.
X3 Neugehauer R, Kline J, O'Connor P, Shrout P, Johnson J, Skodol A, CViçks J,
Susser M. Depressive symptoms in women in the six months after miscarriage.
American Journal of Obstetrics and Gynacologv 1992;166:104-109.
Y3 Chitayat Dr Hodgkinson K. Neural tube dehcts: embryology, inheritance and
prenatal diagnosis. In: Koren G, editor. Folic acid for the prevention of neural
tube dekcts. Proceedings of the Periconcep tua1 Fola te and Prevention of Neu ral

Tube Defects: Developing a Canadian Consensus; 1993 Julv 16; Toronto (ON): ,Mo theris k, 19951-29.
Scolnik D, Nulman 1, Rovet J, Gladstone D, Czuchta D, Gardner HA, (;laclutont.
RI Ashbv P, Weksberg R, Einarson T, Koren G. Neurodevelopment of children exposed in utero to phenytoin and carbarnazepine monotherapy. Journal of the
American Medical Association I994;271:76ï-ï7O.
Nulman 1, Rovet J, Stewart DE, Wolpin J, Gardner HAI Theis JGW, Kulin NA, Koren G. Neurodevelopment of children exposed in utero to antidepressant
clrugs. New Fngland Journal of Medicine 1997;336:258-362.

lMACjt LVALUATION TEST TARGET (QA-3)
APPLIED INIAGE . lnc - = 1653 East Main Street - -. , , Rochester. NY 14609 USA -- --= Phone: 7 t 61482-0300 -- -- - - Fax: 7 1 6/288-5989
O 1993. Applled Image. lnc.. Ail Rlghis Resewed







