Download - Preformed Metal Crown 16-1
Preformed metal crowns
Fiona GilchristClinical Lecturer in Paediatric
Dentistry

Aims
• To discuss the indications and contra-indications of preformed metal crowns
• To discuss different techniques for placing preformed metal crowns
Learning objectives
• Participants should:– Understand the reasons for using preformed metal
crowns
– Have knowledge of different preparation techniques
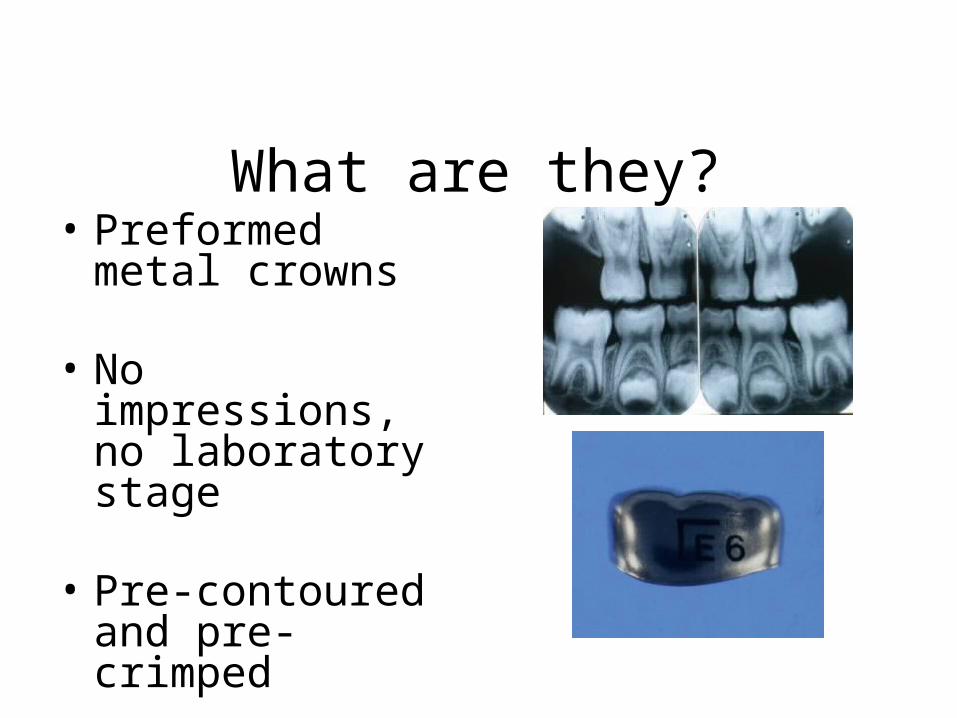
What are they?• Preformed metal
crowns
• No impressions, no laboratory stage
• Pre-contoured and pre-crimped
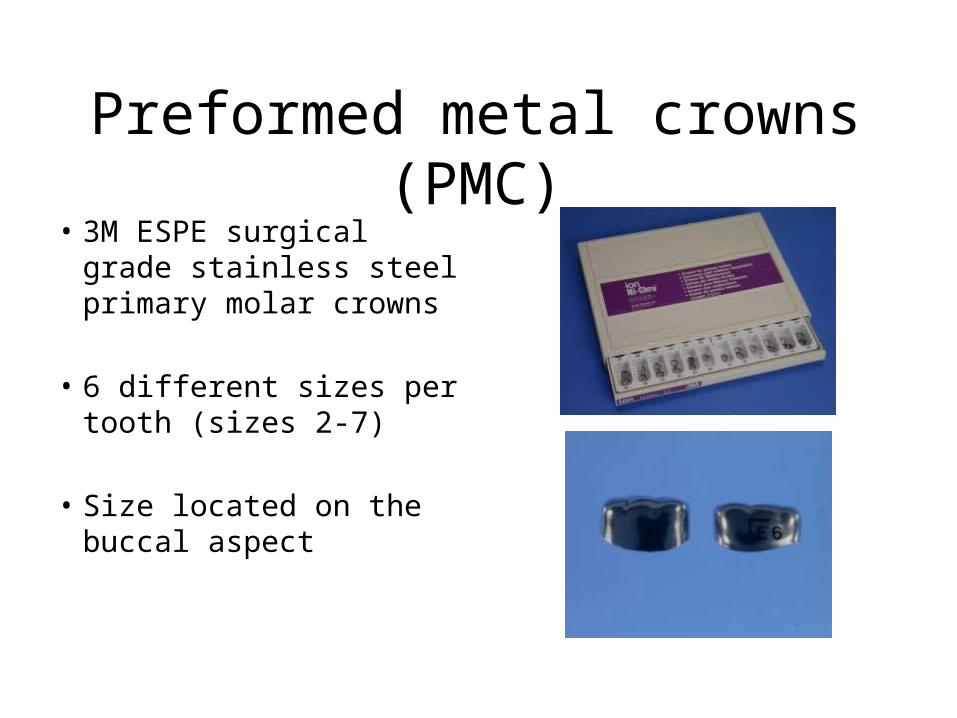
Preformed metal crowns (PMC)• 3M ESPE surgical grade
stainless steel primary molar crowns
• 6 different sizes per tooth (sizes 2-7)
• Size located on the buccal aspect
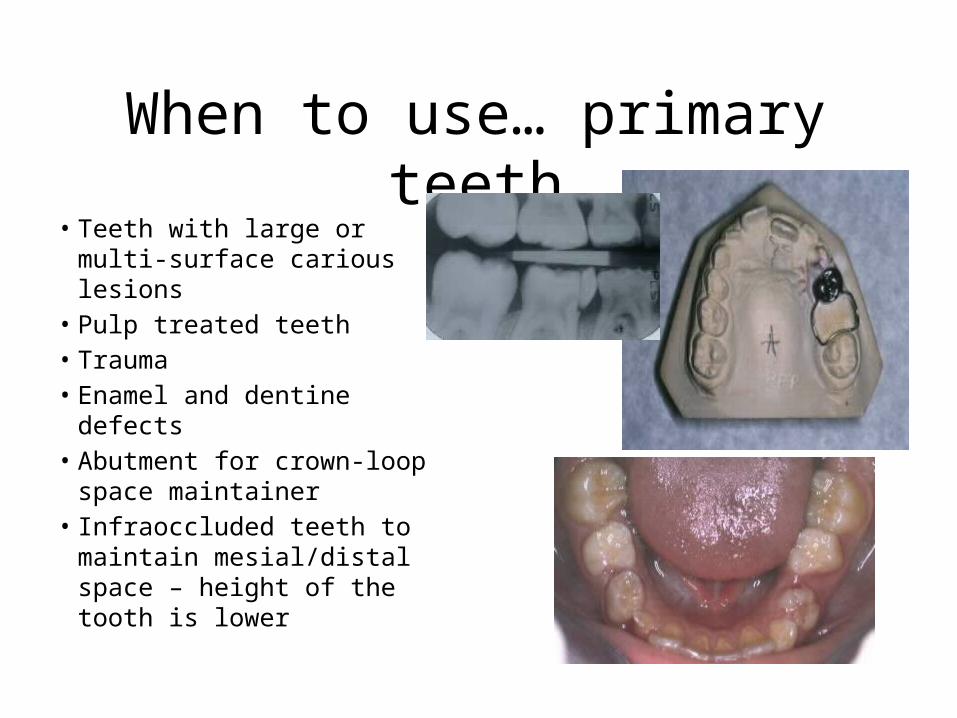
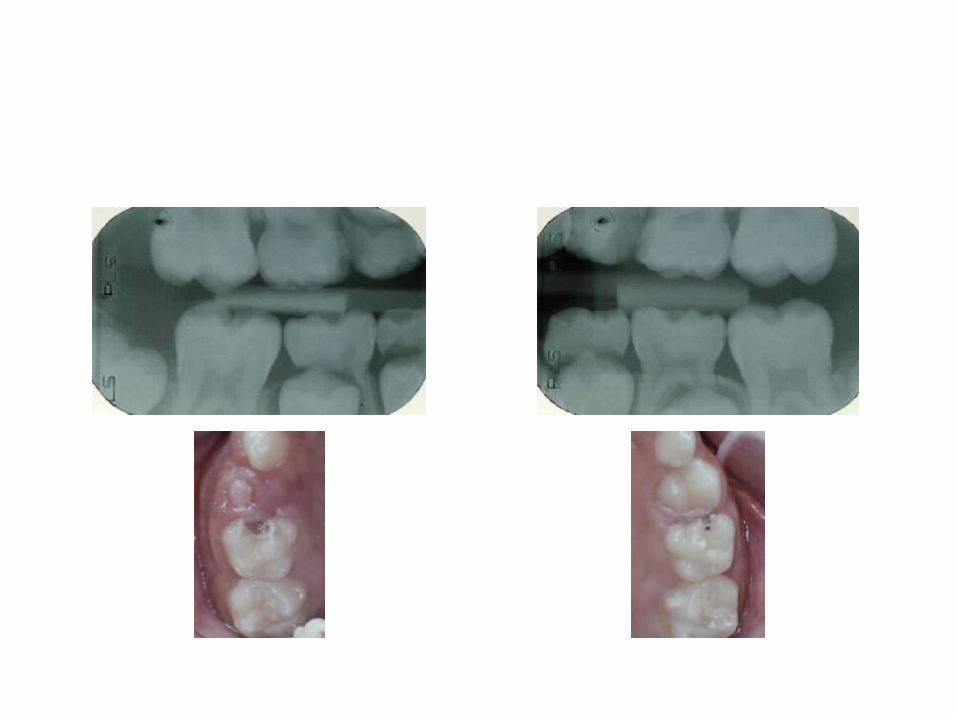
When to use… primary teeth• Teeth with large or multi-
surface carious lesions• Pulp treated teeth• Trauma• Enamel and dentine defects• Abutment for crown-loop
space maintainer• Infraoccluded teeth to
maintain mesial/distal space – height of the tooth is lower
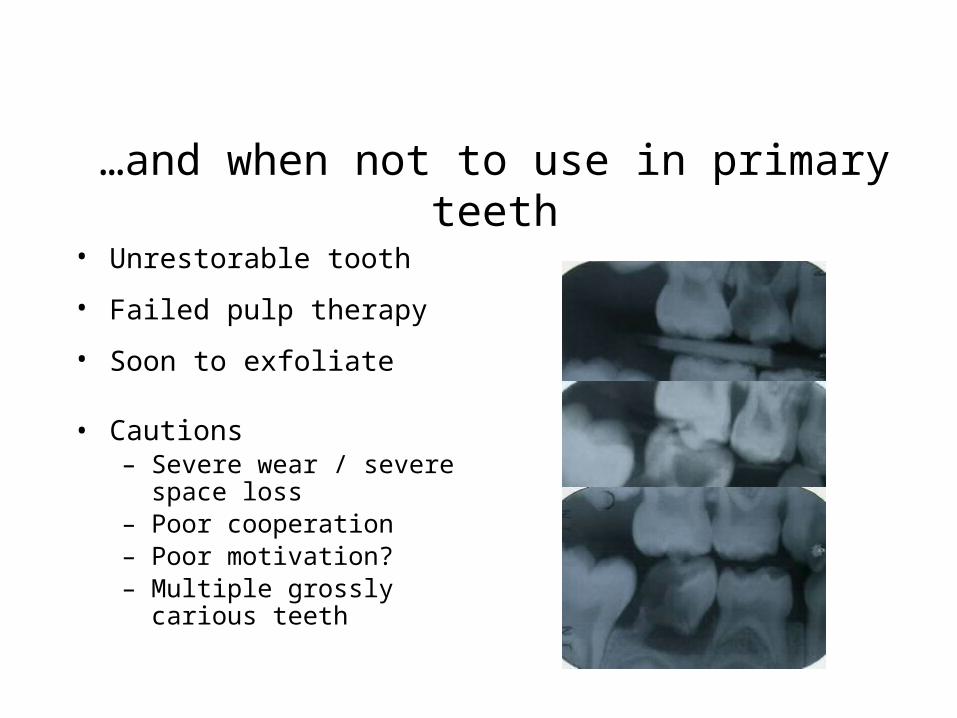
…and when not to use in primary teeth• Unrestorable tooth
• Failed pulp therapy
• Soon to exfoliate
• Cautions– Severe wear / severe space loss– Poor cooperation– Poor motivation?– Multiple grossly carious teeth
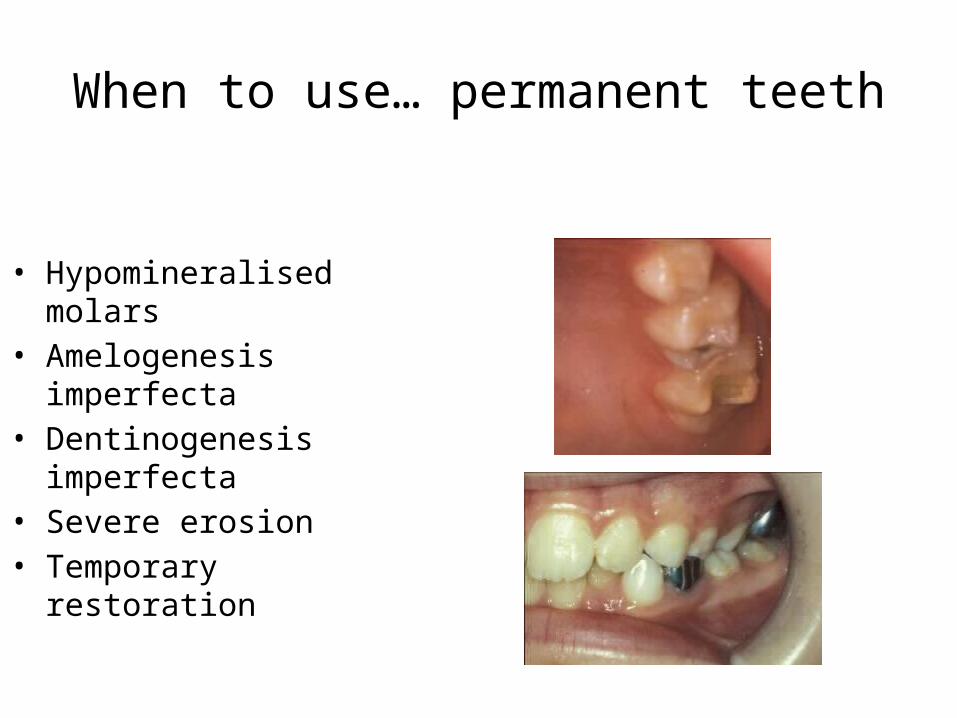
When to use… permanent teeth
• Hypomineralised molars• Amelogenesis imperfecta• Dentinogenesis imperfecta• Severe erosion• Temporary restoration
Advantages of PMCs
• Straightforward technique• Quick and cheap• Evidence of excellent longevity, low failure
rates, compare well with other materials• Failure, if occurs, is easily corrected
Disadvantages
• Poor aesthetics• May impede eruption of adjacent teeth if too
big• May cause gingival inflammation if cement not
removed completely• Theorectical nickel allergy risk
Evidence
• Randall, Vrijhoef and Wilson (2000)
• Systematic review
• Ten studies, 1975 -1997, duration 1.6 - 10 yrs
• Failure rate 1.9 – 30.3% for SSCs vs. 11.6 – 88.7% for amalgam
• SSCs had greater longevity, reduced retreatment need
• All studies favoured treatment with SSCs
Selling them
• Parents often don’t like the look of them
• Children love them!– Princess/Barbie teeth– Tooth jewellery– Pirate tooth– Bling!
Things to tell the patient/parent
• They stay on until the tooth falls out• They need to be brushed just like normal
teeth• The glue tastes a bit like lemons/salt and
vinegar crisps• They feel a bit funny to bite on to start with
Patient/parent experiences
Special toothMy tooth feels betterMakes me feel like a
princess
I say I’m from Mars
I don’t really like the look of the
silver crowns but if they are helping my
son’s teeth then that’s all that
matters
Call it a pirate tooth
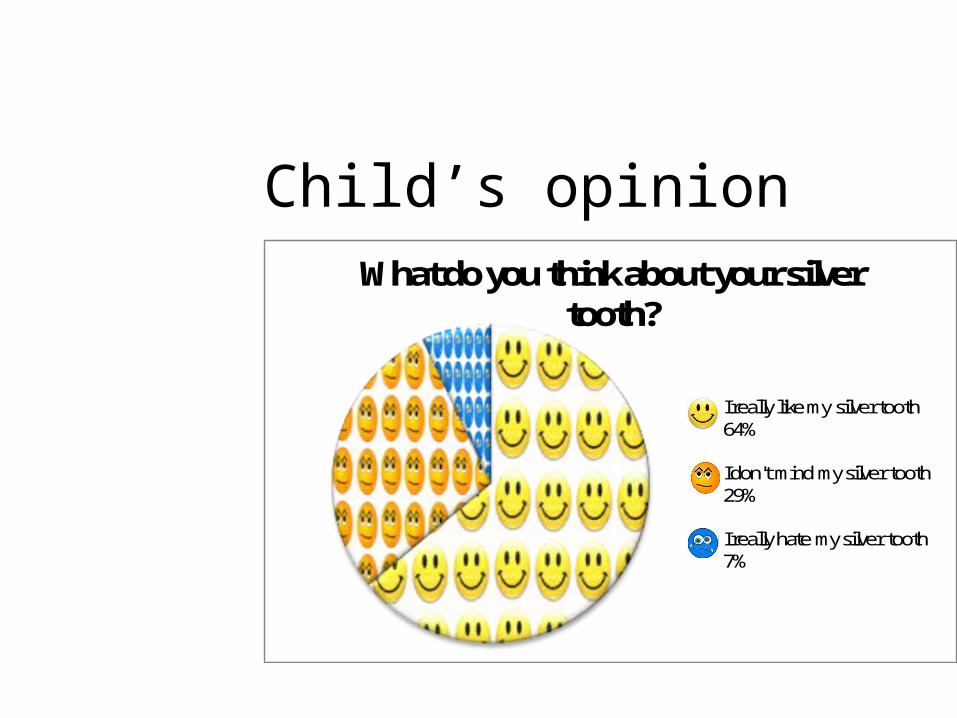
Child’s opinionWhat do you think about your silver
tooth?
I really like my silver tooth 64%
I don't mind my silver tooth 29%
I really hate my silver tooth 7%

Parent’s opinion
57%29%
7%
0% 7%
I have no concerns about how the silver crown looks
Strongly agee
Agree
No opinion
disagree
strongly disagree

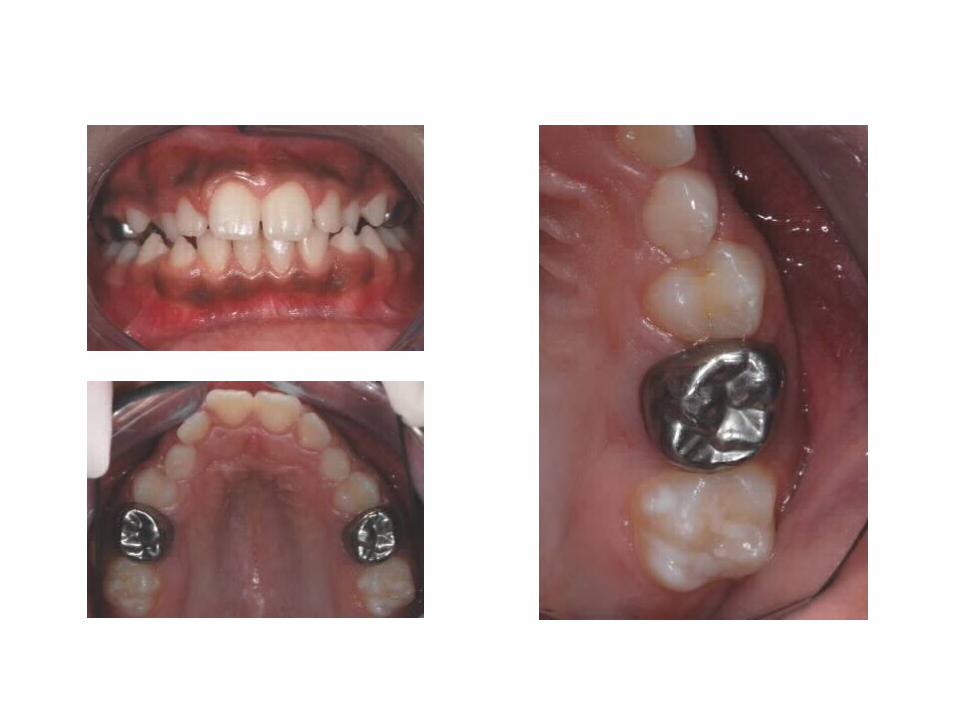
Chris, age 5

Age 7, at follow-up, 2 years after completion of treatment


Conventional technique
You will need …
• Essential materials– Whole box of crowns – Topical/LA – Diamond burs – Adams pliers– Cement– Dental tape - knotted

You will need …
• Optional materials– Rubber dam– Crown scissors – Crimping pliers– Orthodontic band seater
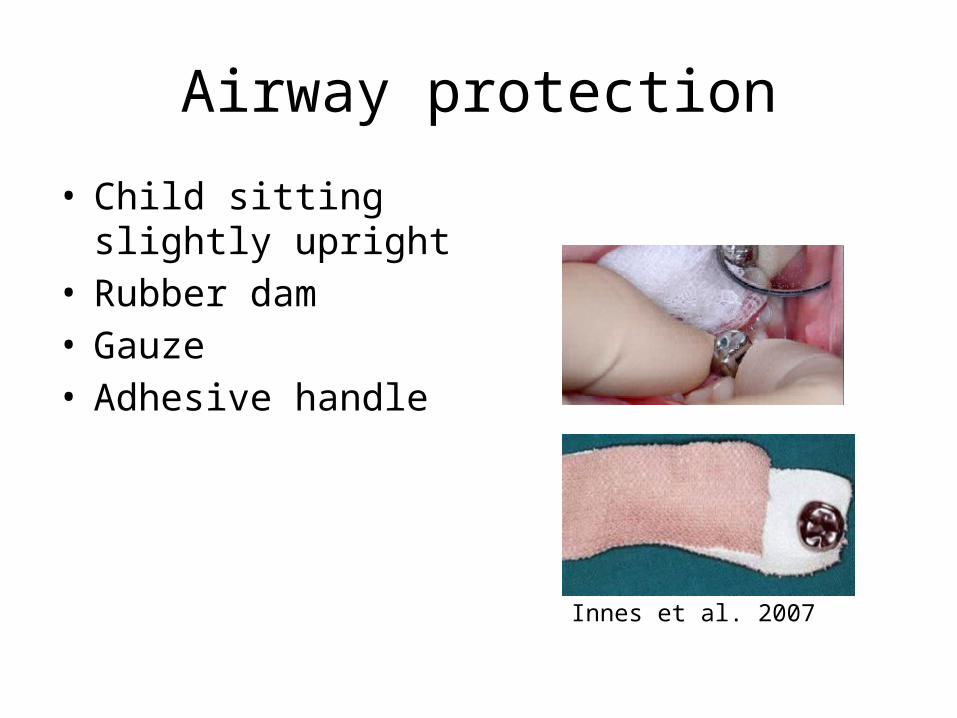
Airway protection
• Child sitting slightly upright
• Rubber dam• Gauze• Adhesive handle
Innes et al. 2007

Technique
1. Topical/LA2. Remove caries3. Pulpotomy/pulpectomy if needed4. Prepare tooth5. Select crown6. Adapt crown or modify prep7. Cementation
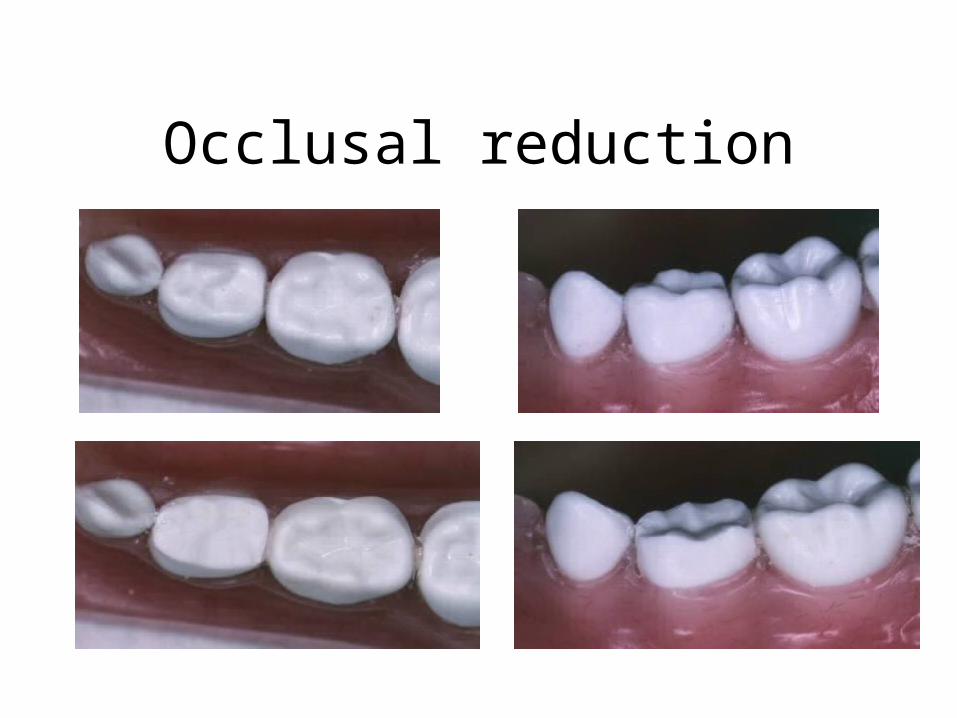
Occlusal reduction

Mesial and distal reduction

Finishing touches

Select a crown
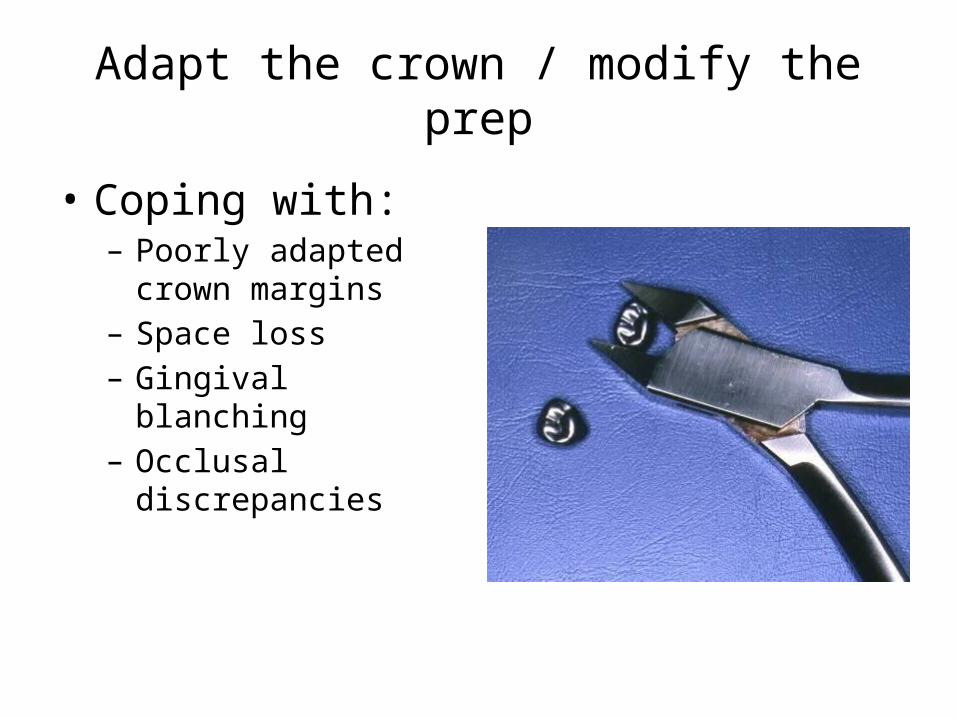
Adapt the crown / modify the prep
• Coping with: – Poorly adapted crown
margins – Space loss – Gingival blanching– Occlusal discrepancies
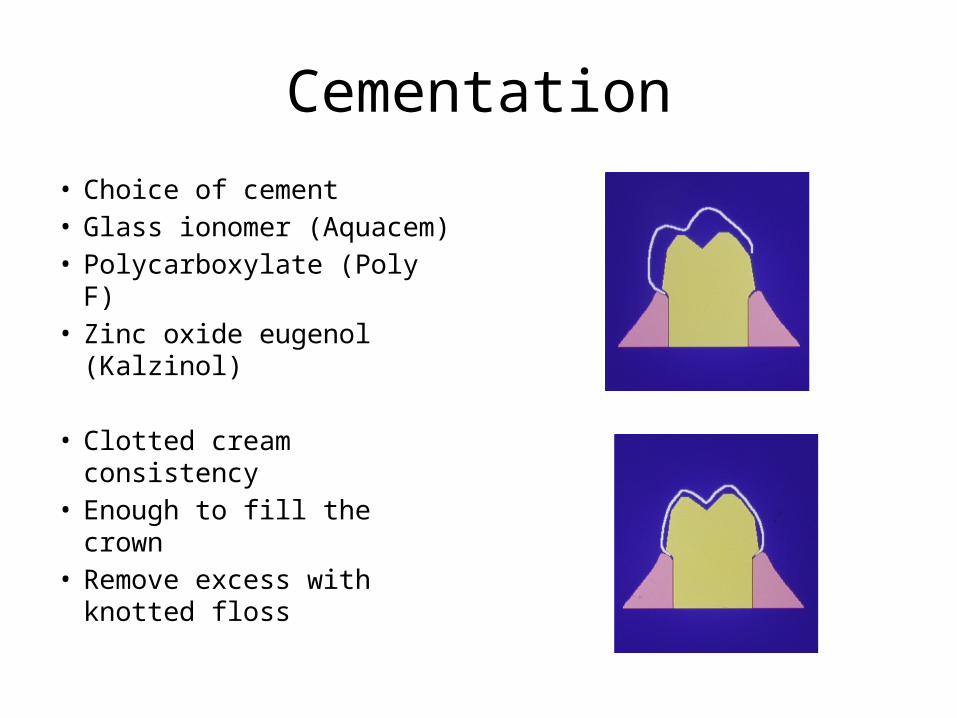
Cementation
• Choice of cement• Glass ionomer (Aquacem)• Polycarboxylate (Poly F)• Zinc oxide eugenol
(Kalzinol)
• Clotted cream consistency• Enough to fill the crown• Remove excess with
knotted floss

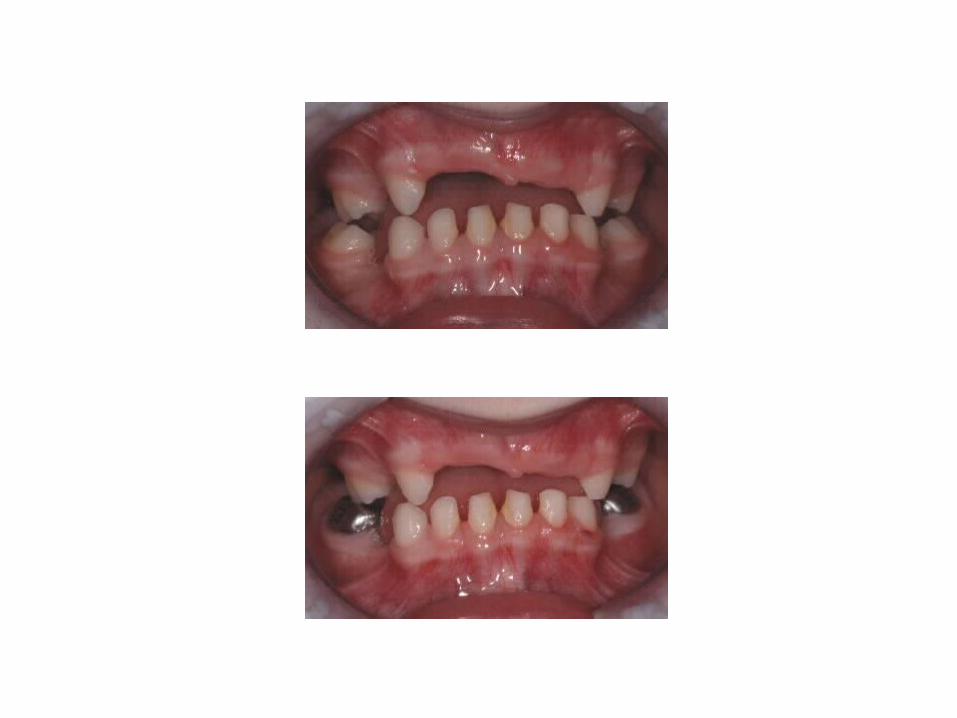
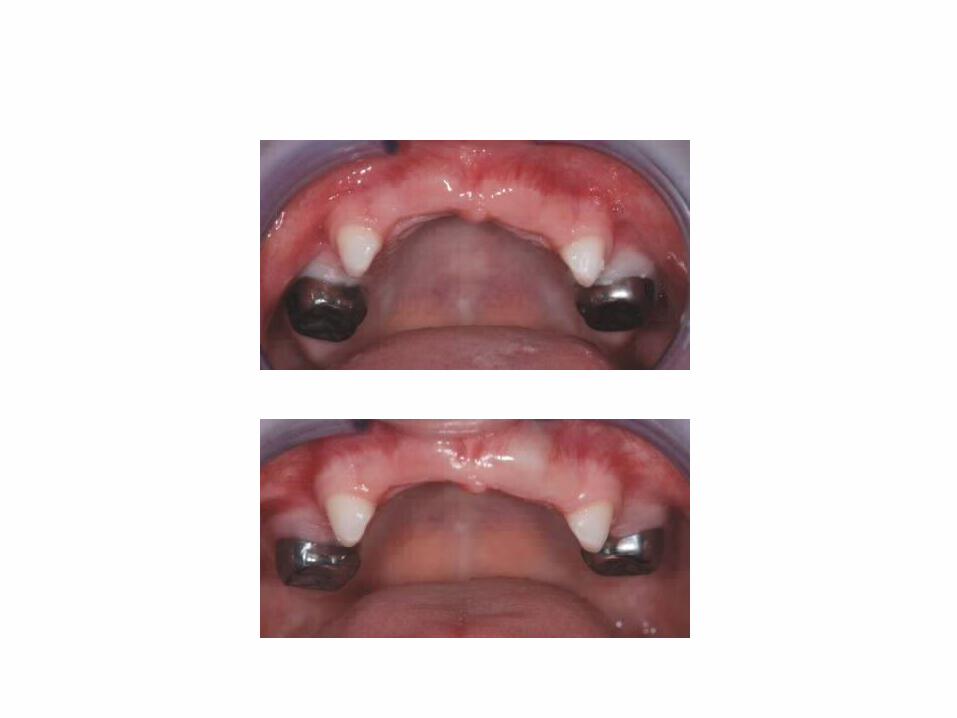
James, age 8

Liam, age 6

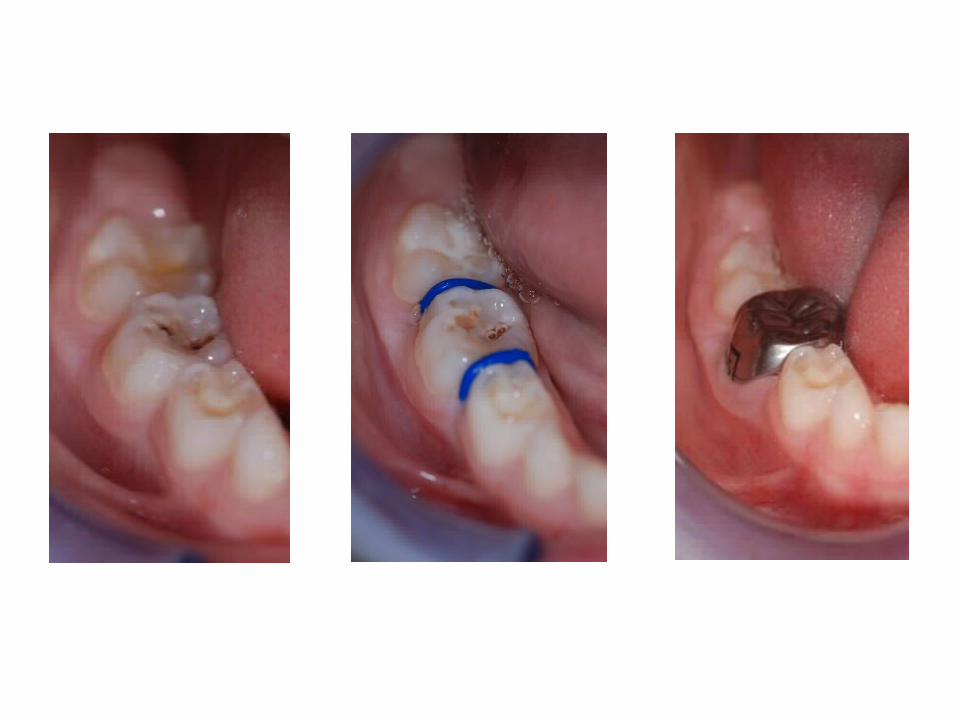
The Hall technique
The Hall Technique
• No tooth preparation• No local analgesia • No try-in• Not for extensively carious teeth• Caries not removed, but sealed into the tooth
to isolate it from the mouth
The Hall Technique
• Tooth asymptomatic• Child not at risk of endocarditis• Pre-operative radiograph• +/- separators• Airway protection• Occlusion
The Hall Technique
• Innes N, Evans DJP, Stirrups DR (2007)– Split mouth RCT– 132 children, aged 3-10– 17 GDPs in Tayside, Scotland– Clinical and radiographic follow-up

Main outcomes after 2 years
Innes and Evans (2007)
(n=124 conventionally treated teeth + 124 Hall teeth)
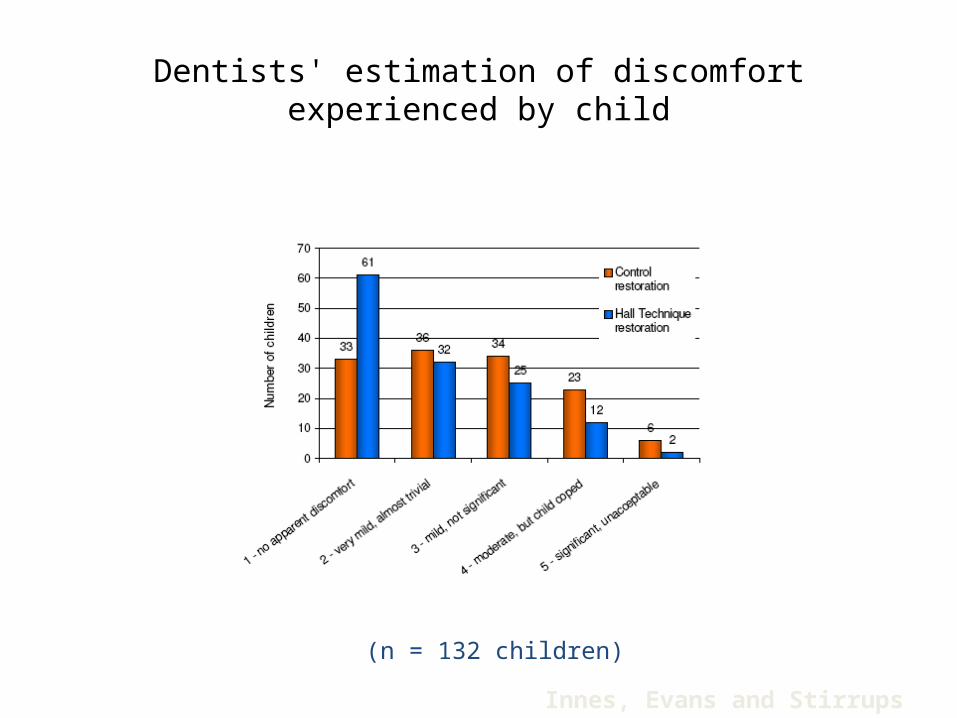
Dentists' estimation of discomfort experienced by child
(n = 132 children)
Innes, Evans and Stirrups (2007)
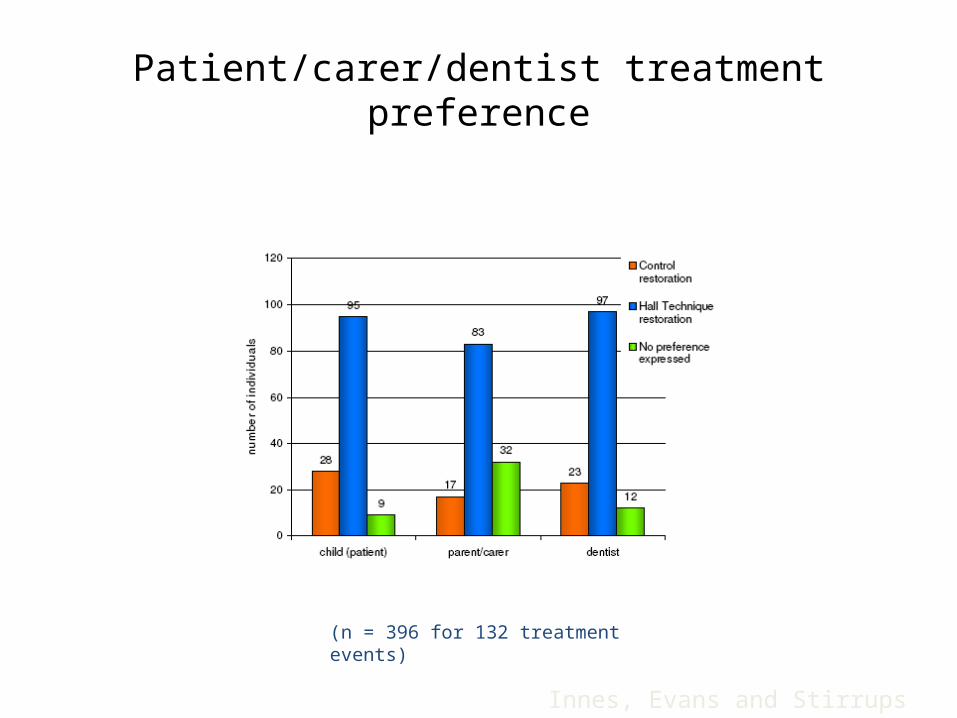
Patient/carer/dentist treatment preference
(n = 396 for 132 treatment events)
Innes, Evans and Stirrups (2007)
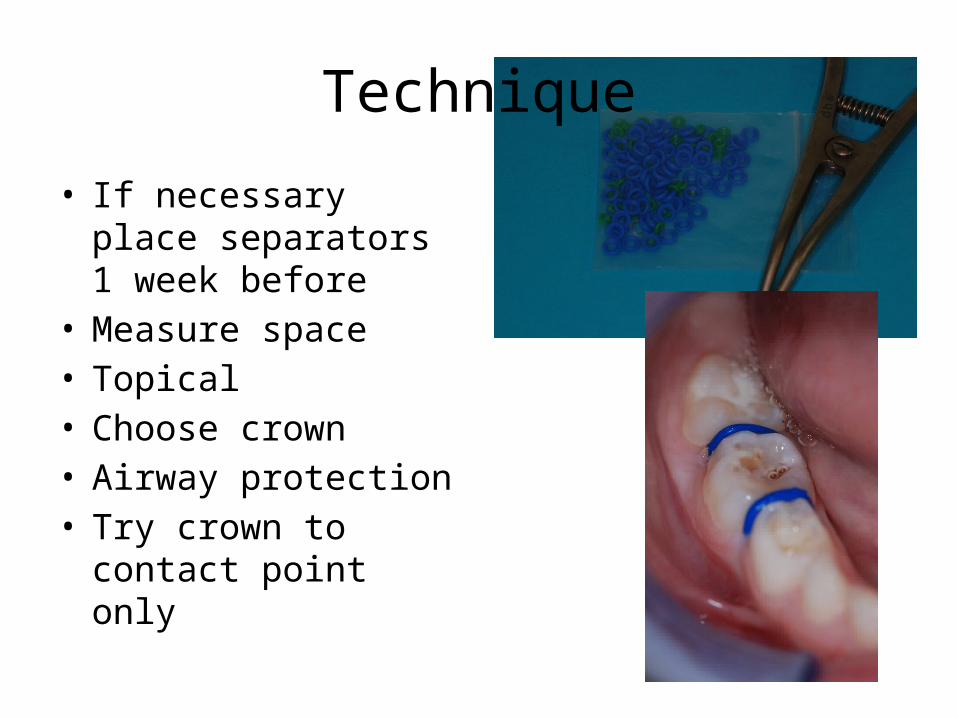
Technique
• If necessary place separators 1 week before
• Measure space • Topical• Choose crown• Airway protection• Try crown to contact
point only
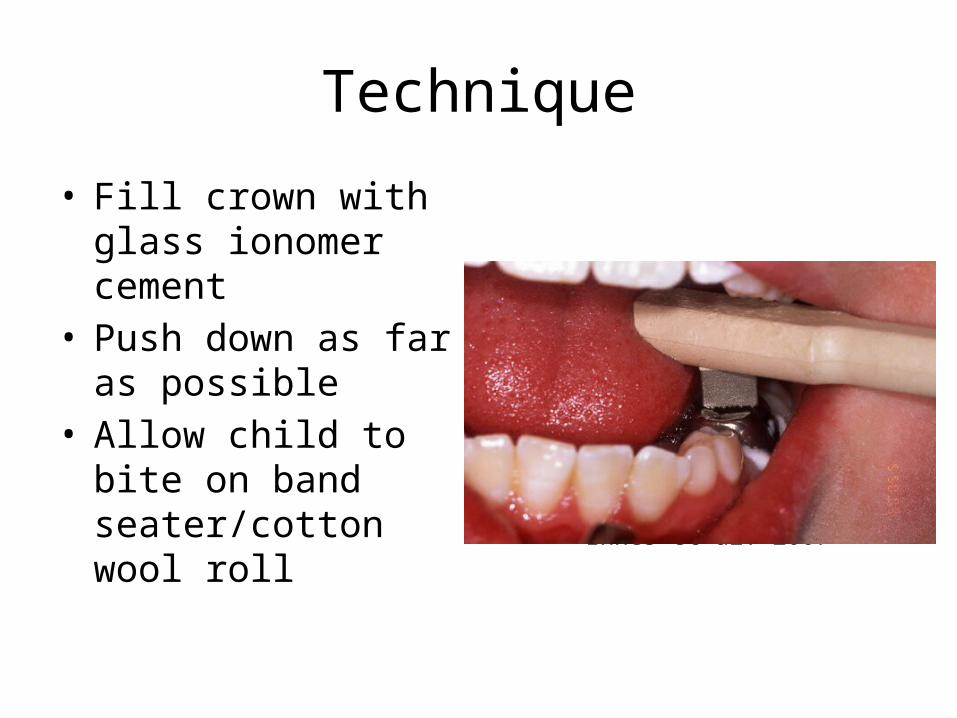
Technique
• Fill crown with glass ionomer cement
• Push down as far as possible
• Allow child to bite on band seater/cotton wool roll
Innes et al. 2007
Technique
• Remove excess cement with wet gauze
• Get child to bite together
• Remove further cement with gauze
• Knotted floss between contact points
Patient instructions
• May be a little uncomfortable afterwards
• Advice about analgesia
• Occlusion will be propped open but will settle


Further reading• Innes N, Evans D. The Hall Technique. A child centred approach to managing the
carious primary molar. A Users Manual. University of Dundee. www.scottishdental.org/?o=1404
• Welbury R R, Duggal M S, Hosey M T. Paediatric Dentistry. Oxford Medical Publications, 2005, Ch 9.
• Kindelan SA et al. Stainless steel preformed crowns for primary molars, UK National Clinical Guidelines in Paediatric Dentistry. International Journal of Paediatric Dentistry, 1999; 9:311-314. http://www.bspd.co.uk/publications.html







