Postural exercises&
Upper and Lower Cross Syndromes and exercises to help
by Janda
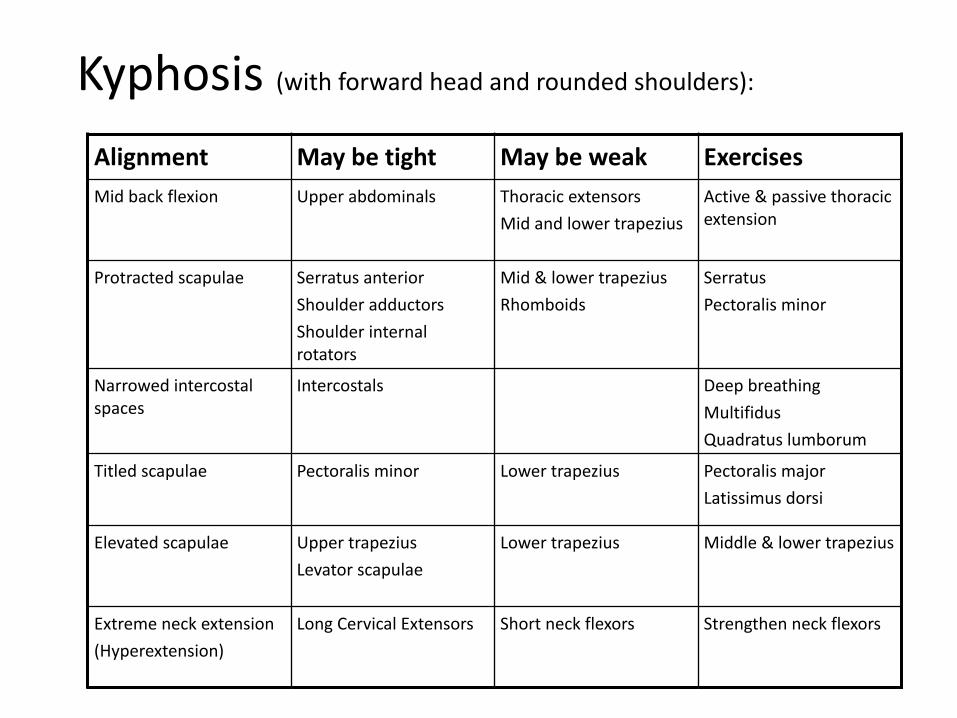
Kyphosis (with forward head and rounded shoulders):Alignment May be tight May be weak ExercisesMid back flexion Upper abdominals Thoracic extensors
Mid and lower trapeziusActive & passive thoracic extension
Protracted scapulae Serratus anterior Shoulder adductors Shoulder internal rotators
Mid & lower trapezius Rhomboids
Serratus Pectoralis minor
Narrowed intercostal spaces
Intercostals Deep breathing Multifidus Quadratus lumborum
Titled scapulae Pectoralis minor Lower trapezius Pectoralis major Latissimus dorsi
Elevated scapulae Upper trapezius Levator scapulae
Lower trapezius Middle & lower trapezius
Extreme neck extension (Hyperextension)
Long Cervical Extensors Short neck flexors Strengthen neck flexors

Lordosis:Alignment May be tight May be weak Exercises
Anterior tilt Hip flexors Abdominals Stretch hip flexors Strengthen obliques for stabilization Avoid full sit ups
Hip flexion Hip extensors Strengthen gluteals
Extreme L extension
Low back extensors
Stretch low back extensors

Flat Back:
Alignment May be tight
May be weak
Exercises
Posterior Pelvic tilt
Hamstrings Stretch hamstrings
Low back flexion Back extensors Stretch back extensors
Hip extension Hip flexors Strengthen hip flexors
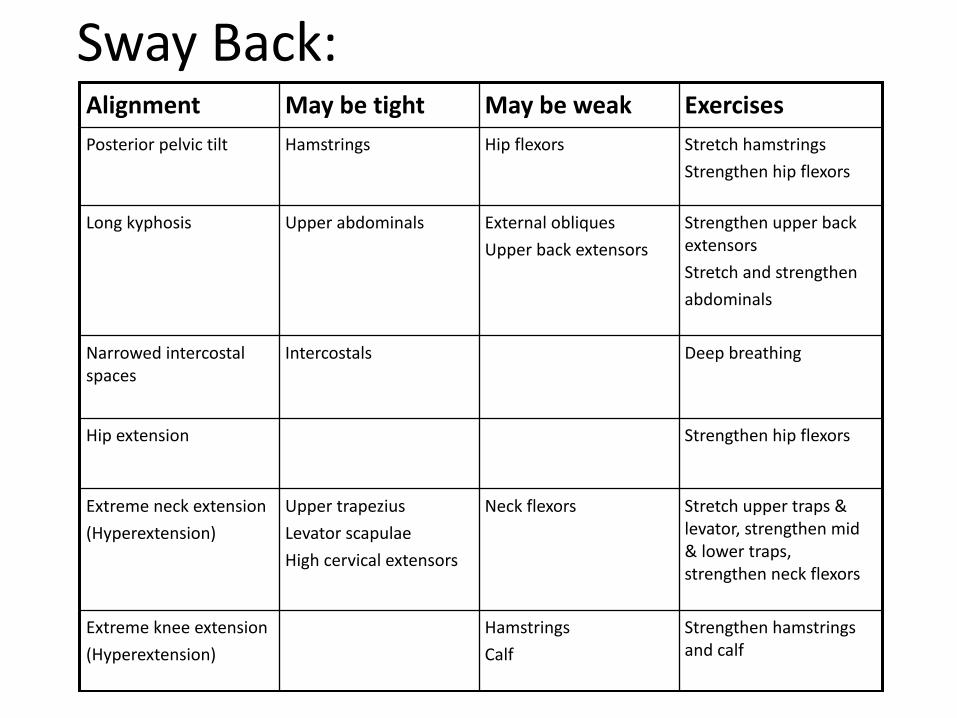
Sway Back:Alignment May be tight May be weak ExercisesPosterior pelvic tilt Hamstrings Hip flexors Stretch hamstrings
Strengthen hip flexors
Long kyphosis Upper abdominals External obliques Upper back extensors
Strengthen upper back extensors Stretch and strengthen abdominals
Narrowed intercostal spaces
Intercostals Deep breathing
Hip extension Strengthen hip flexors
Extreme neck extension (Hyperextension)
Upper trapezius Levator scapulae High cervical extensors
Neck flexors Stretch upper traps & levator, strengthen mid & lower traps, strengthen neck flexors
Extreme knee extension (Hyperextension)
Hamstrings Calf
Strengthen hamstrings and calf
“when muscle imbalances occur some muscles become inhibited and weak, while others become tight. Such imbalances lead to tissue changes that may result in inappropriate patterns of movement”
Vladimir Janda, MD, DSc
Janda’s syndromes are based on:
Different types of muscles responding to faulty loading in different ways.
Different types of muscles have predominance of slow and fast twitch fibres.
Slow twitch -‐ postural -‐ tend to lengthen and weaken under faulty loading
Fast twitch -‐ tend to shorten and tighten under faulty loading.
Sub-‐types of muscles fibres are still being discovered.
Faulty loading -‐ can be through activity which predominantly targets certain muscle groups or through deconditioning
A good reference for an overview of postural analysis is Chaitow and Delaney. “Clinical Application of Neuromuscular Techniques (Churchill Livinsgstone) 2000”
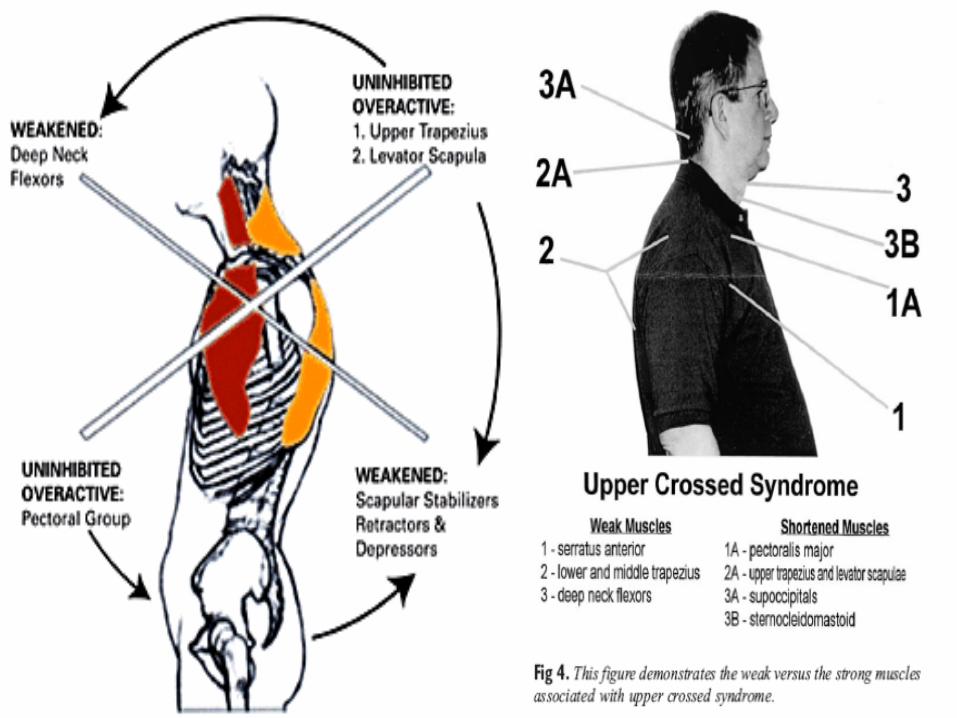
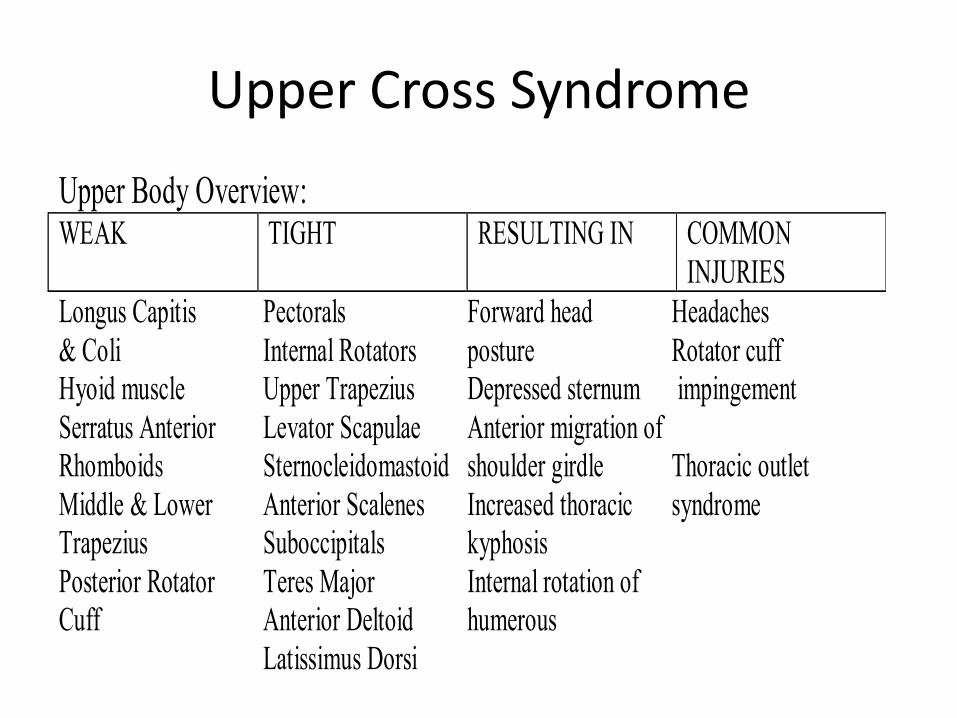
Upper Cross Syndrome
Upper Body Overview: WEAK
TIGHT RESULTING IN COMMON INJURIES
Longus Capitis Pectorals Forward head Headaches & Coli Internal Rotators posture Rotator cuff Hyoid muscle Upper Trapezius Depressed sternum impingement Serratus Anterior Levator Scapulae Anterior migration of Rhomboids Sternocleidomastoid shoulder girdle Thoracic outlet Middle & Lower Anterior Scalenes Increased thoracic syndrome Trapezius Suboccipitals kyphosis Posterior Rotator Teres Major Internal rotation of Cuff Anterior Deltoid humerous Latissimus Dorsi
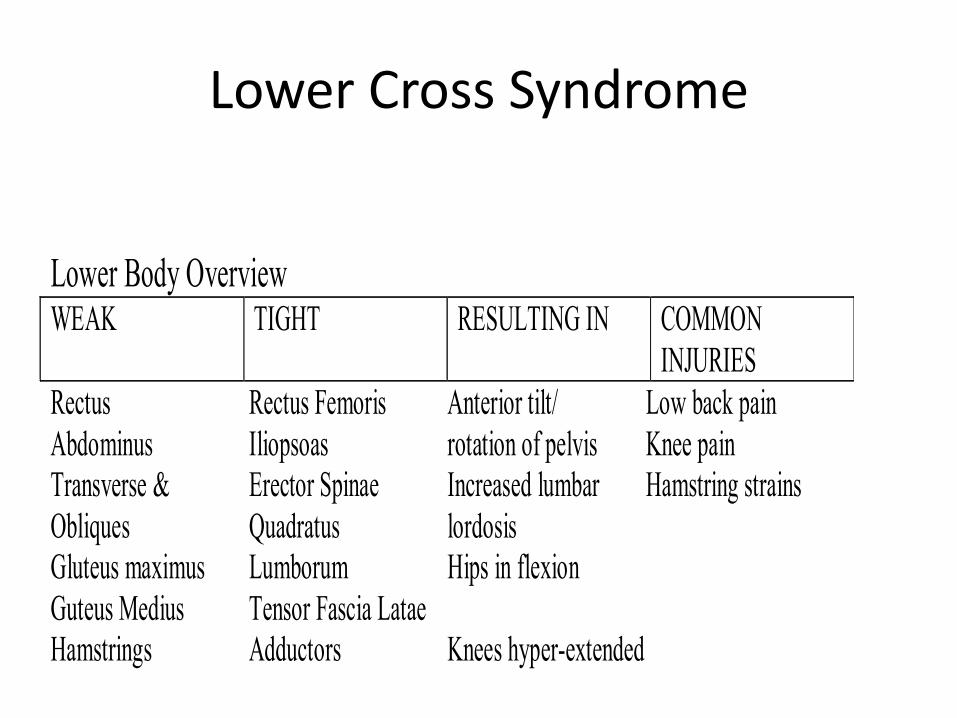
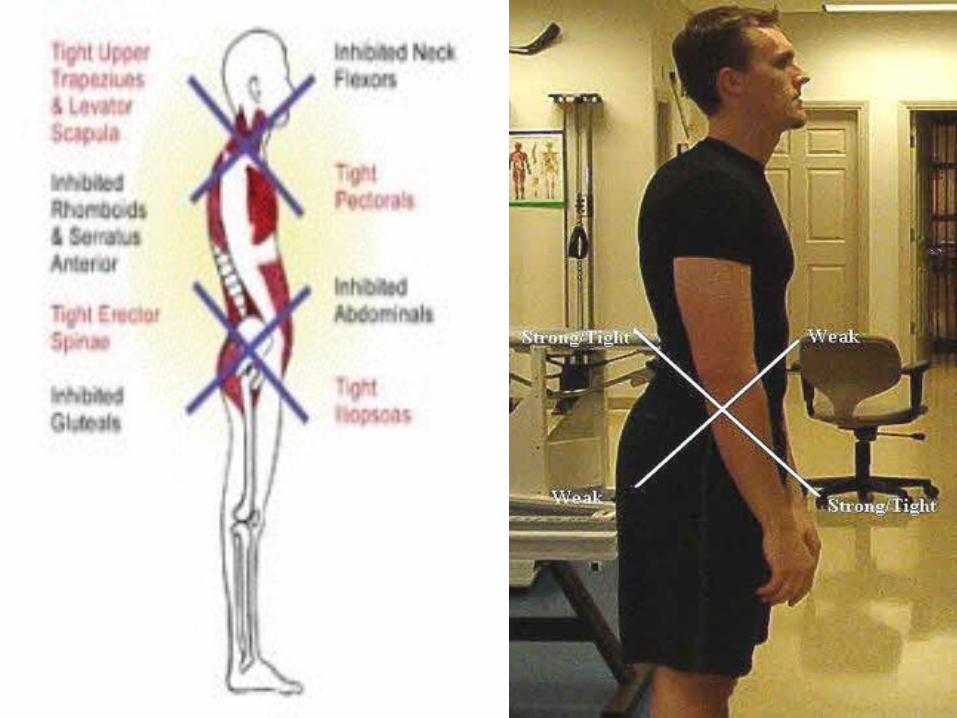
Lower Cross Syndrome
Lower Body Overview WEAK TIGHT RESULTING IN COMMON
INJURIES Rectus Rectus Femoris Anterior tilt/ Low back pain Abdominus Iliopsoas rotation of pelvis Knee pain Transverse & Erector Spinae Increased lumbar Hamstring strains Obliques Quadratus lordosis Gluteus maximus Lumborum Hips in flexion Guteus Medius Tensor Fascia Latae Hamstrings Adductors Knees hyper-extended
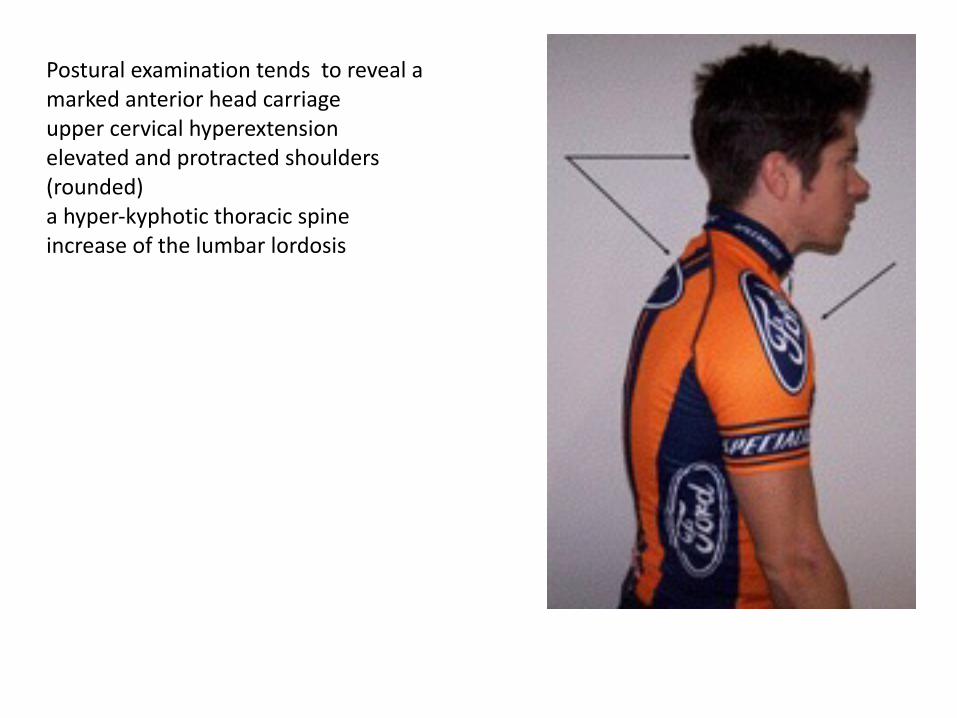
Postural examination tends to reveal a marked anterior head carriage upper cervical hyperextension elevated and protracted shoulders (rounded) a hyper-‐kyphotic thoracic spine increase of the lumbar lordosis

Symptoms
• complained of chronic neck pain and stiffness • chronic upper thoracic pain patterns • symptoms as being constant • aggravated by reading, poor posture and by prolonged sitting
• Associated with micro-‐traumatic shoulder injuries
Examination
• Cervical ranges of motion restrictions with the report of pulling muscular pain elicited at the end ranges
• Positive cervical Kemp’s test bilaterally • Thoracic ranges of motion restrictions • Tender myofascial trigger points were detected in the suboccipital, SCM, levator scapulae, and upper trapezii muscle groups bilaterally
Workshop exercises• 1. Dysphasic recruitment -‐ Hamstring substitution – Lie prone – Someone presses flat of fingers on hamstrings and glut. max. – Perform small hip extension – Which muscle fires first – Clue: hams. are mobilisers, glut. max. is a stabiliser. Which should fire first?
– Think of clinical implications – Problems with this test? Hams are eccentric contractors that stabilise a flexed and wtb knee followed by concentric contractors for mobilisation at midrange
Workshop exercises
• 2. Muscle tension control -‐ Gluteus maximus tension test (just because it’s convenient – use another muscle if you wish!) – Stand and grab buttocks (YOUR OWN) – Clench to 25%, 50%, 75%, 100%, 75%, 50% 25% and 0% – Who felt the last 25% was actually more or less than 25% on the way down?
– What does this tell you about your ability to sense your muscle force/tension/control?

Workshop exercises
• 3. Body awareness –Multisegmental multifidus (local stabiliser) – Place fingers at about L4,5, just lateral to spinous process
– Tense muscle ??? – Now keep fingers there and raise other arm in front of you
– Now bring it down and note when it switches on and off
– Now stand in sway posture and repeat
Workshop exercises
• 5. Rigidity dysfunction -‐ ability to separate segments when required – Stand up, hands on hips – Bend knees and move knees from side to side
• Who can dissociate rotation? If not what clinical consequences might you see?
Workshop exercises
• 6. Waiter’s bow -‐ Postural awareness – Stand up and place hands on hips – Bow forward from hips and stop when you think you are flexing at your spine
– Repeat with tape on skin • Who was right? What might this mean to your patient feedback when they report symptoms/ swear they have been doing your exercises?
• 50 deg of hip flexion should occur prior to spinal flexion
Workshop exercises
• 7. Finding motion in the right place – Stand up – Someone stand behind you with their finger pointing to touch your lumbar spine
– You aim to extend your upper spine without moving away from the finger
– If you can’t, stand with feet under couch, leaning against it so you feel just balanced
– Repeat. – Observers note where change in motion occurs – Repeat away from couch…can you do it yet??







