
Patient Safety
A review for the Clinical Excellence Commission The Centre for Clinical Governance Research in Health undertakes strategic research, evaluations and research-based projects of national and international standing with a core interest to investigate health sector issues of policy, culture, systems, governance and leadership.
CENTRE FOR CLINICAL GOVERNANCE RESEARCH
A comparative analysis of eight Inquiries in six countries

First published in 2006 by the Centre for Clinical Governance Research, Faculty of Medicine, University of NSW, Sydney, NSW 2052. Printed and bound by University of NSW.
© Don Hindle, Jeffrey Braithwaite, Jo Travaglia and Rick Iedema 2006
This book is copyright. Apart from any fair dealing for the purposes of private study, research, criticism or review as permitted under the Copyright Act, no part may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without prior written permission. Enquiries may be made to the University of New South Wales.
National Library of Australia Cataloguing-in-Publication data:
Hindle, Don
Patient Safety: a comparative analysis of eight Inquiries in six countries.
ISBN: 0 7334 2411 2.I. Braithwaite, Jeffrey. II. Travaglia, Joanne. III. Iedema, Rick. IV. University of New South Wales. Centre for Clinical Governance Research in Health. V. Patient Safety: a comparative analysis of eight Inquiries in six countries.
DESIGN LAyOUT AND PRINTING By UNSW PUBLISHING AND PRINTING SERVICES 36850

�
Contents1 Summary 5
1.1 AspectsofmostoralltheInquiries 5
1.2 Differences 7
1.3 …andtheansweris… 8
2 BristolRoyalInfirmary,UnitedKingdom 9
2.1 Context 9
2.2 TheInquiries 11
2.2.� Inquiry by the General Medical Council (�998) ��
2.2.2 Inquiry by the Department of Health (200�) ��
2.3 ConclusionsoftheInquiry 13
2.4 RecommendationsoftheInquiry 18
2.5 Discussion 23
2.6 Footnotes 25
2.6.� Dr Steven Bolsin’s perspective on Bristol 25
2.6.2 Thefinalwordsofsomeoftheothermainplayers 29
2.7 Referencesandselectedbibliography 29
3 CampbelltownandCamden,Australia 31
3.1 Context 31
3.2 TheInquiry 35
3.2.� The First Interim Report of the Special Commission of Inquiry 35
3.2.2 The Second Interim Report 42
3.2.3 The Final Report 42
3.3 ConclusionsoftheInquiry 52
3.4 RecommendationsoftheInquiry 53
3.5 Discussion 53
3.6 Referencesandselectedbibliography 54
4 CeljeHospital,Slovenia 55
4.1 Context 55
4.2 TheInquiry 60
4.3 ConclusionsoftheInquiry 61
4.4 RecommendationsoftheInquiry 64
4.5 Discussion 65
4.6 Referencesandselectedbibliography 65
2 Patient Safety: a comparative analysis of eight Inquiries in six countries
5 Glasgow’sVictoriaInfirmary,Scotland 66
5.1 Context 66
5.2 TheInquiry 66
5.3 ConclusionsoftheInquiry 66
5.4 RecommendationsoftheInquiry 67
5.5 Discussion 72
5.6 Footnotes 73
5.6.� The Report from the Ministerial Convention 73
5.6.2 The NHS Scotland Action Plan 78
5.7 Referencesandselectedbibliography 79
6 KingEdwardMemorialHospital,Australia 79
6.1 Context 80
6.2 TheInquiries 81
6.2.1 TheChildandGloverReview(2000) 8�
6.2.2 The Douglas Inquiry (200�) 8�
6.3 ConclusionsoftheInquiry 82
6.4 RecommendationsoftheInquiry 96
6.5 Discussion 97
6.6 Footnote 98
6.7 Referencesandselectedbibliography 99
7 RoyalMelbourneHospital,Australia 100
7.1 Context 100
7.2 TheInquiry 100
7.3 ConclusionsoftheInquiry 101
7.4 RecommendationsoftheInquiry 107
7.5 Discussion 109
7.6 Footnote 110
7.6.� The outcome of the legal investigation ��0
7.7 Referencesandselectedbibliography 110
8 SouthlandDHBMentalHealthServices,NewZealand 110
8.1 Context 110
8.2 TheInquiries 111
8.2.� Dr Taumoepeau’s clinical audit ���
8.2.2 Terms of Reference of the Commissioner’s Inquiry ��2
8.2.3 The process of investigation ��2

3
8.3 ConclusionsoftheInquiry 113
8.4 RecommendationsoftheInquiry 122
8.4.� General recommendations of Dr Taumoepeau’s clinical audit �23
8.5 Discussion 124
8.6 Footnote 124
8.6.1 TheReviewPanel’sreport 124
8.7 Referencesandselectedbibliography 126
9 WinnipegHealthSciencesCentre,Canada 126
9.1 Context 127
9.2 TheInquiry 128
9.2.� The Inquest (�995-�998) �28
9.2.2 Conclusions of the Inquiry �28
9.3 RecommendationsoftheInquiry 137
9.4 Discussion 138
9.5 Afootnote:implementationofrecommendations 140
9.6 Referencesandselectedbibliography 140
10 Additionalbibliography 141
11 Appendix1:Summaryofinquiries 142
11.1 BristolRoyalInfirmary,UnitedKingdom 142
11.2 CampbelltownandCamdenHospitals,Australia 146
11.3 CeljeHospital,Slovenia 147
11.4 Glasgow’s,VictoriaInfirmary,Scotland 149
11.5 KingEdwardMemorialHospital,Perth,Australia 151
11.6 RoyalMelbourneHospital,Australia 153
11.7 SouthlandDHBMentalHealthService,Southland,NewZealand 154
11.8 WinnipegHealthServicesCentre,Canada 156

4 Patient Safety: a comparative analysis of eight Inquiries in six countries

5
� Summary
This is a report of eight Inquiries into alleged poor health care. Three are from Australia: from Perth (King EdwardMemorialHospital),Melbourne(RoyalMelbourneHospital)andSydney(Campbelltown-Camden).TheremainderarefromScotland(Glasgow’sVictoriaInfirmary),England(BristolRoyalInfirmary),Slovenia(CeljeHospital),NewZealand(SouthlandDHB)andCanada(WinnipegHealthSciencesCentre).
Alltheinquiriesconcernedallegationsofpoorclinicalpractice.TheKingEdwardInquiryconcernedthetreatment of obstetrics and gynaecology cases over several years at a major tertiary referral and teaching hospital.RoyalMelbourneinvolvedinappropriatetreatmentofpatients,unprofessionalbehaviourandmedicationerrors.TheCampbelltown-CamdenInquiryrelatedtoawidevarietyofelementsofcare,predominantlyforindividualpatients.Glasgowconcernedoutbreaksofhealthcareassociatedinfectionsthatseemedtohavebeenpoorlymanaged,andBristollargelyrelatedtopooroutcomesafterpaediatricheart surgery. Celje involved alleged inadequate reporting of pathology results mainly relating to suspected malignancies.Southlandcentredonthecareofpatientswithmentalillness.Winnipegalsoconcernedpaediatricheartsurgery.Asummaryofthekeyrecommendationsandfindingsofthereviewsispresentedin Appendix �.
1.1 AspectsofmostoralltheInquiries
Thisstudydrawsonasmallandpurposivesample.ThepredominanceofEnglish-speakingcountriespartlyreflectsthedifficultiesinaccessingandtheninterpretingreportsinotherlanguages.Sloveniaappearsbyaccident:oneoftheauthorshasbeenworkinginSlovenia.
Theextenttowhichthefindingsaregeneralisableisthereforelefttothereader’sjudgment.However,itisrelevanttonotethecommonfeaturesofthesample,asfollowsinTable1.
Table1:Commonfeaturesofinquiries
n Theinquiryteamswerelargelyimpartialandobjective
n Somehealthcarewasfarbelowstandard
n Qualitymonitoringprocessesweredeficient
n Individual care providers and patients raised the concerns
n Criticswereoftenignoredorabused
n Teamworkwasdeficient
n Patientsandfamilieswerenotinformedmembersoftheteam
Theinquiryteamswerelargelyimpartialandobjective
Alltheinquirieswereconductedinanimpartialwaybydedicatedinvestigatorswhocannotbequestionedintermsoftheirmotives,energyandattentiontodetail.Itishighlyunlikelythattheirconclusionsareerroneous.Atleast,itisdoubtfultherewilleverbeanyalternativesourcesthatpresent a better picture.
Theteamshadslightdifferencesofemphasisthatprobablyreflectedthepersonalviewsoftheirleaderstosomeextent,butmostlyreflecteddifferencesintheirtermsofreference.Forexample,mostwereconductedunderaspecificlegislativeinstrumentthatconstrainedthecourseoftheinvestigation.

6 Patient Safety: a comparative analysis of eight Inquiries in six countries
Themostobviousdifferenceconcernedthebalancetobestruckbetweenfindingindividualswhowereculpable,andlearninglessonsofrelevancetothehealthcaresystem.Thissaid,alltheinquiryteamshaddifficultyinavoidingconsiderationofbothaspects.Thereweregreaterdifferencesinthetermsofreferencethaninthecontentofthefinalreports.
Somehealthcarewasfarbelowstandard
Ineverycase,theinvestigatorsconcludedthatsomeofthecarewasbelowreasonablestandards.Inafewcases,thecarewasjudgedtobefarbelowwhatthepatientshadtherighttoexpect.
Qualitymonitoringprocessesweredeficient
The agencies that had been established to monitor quality of care and therefore to protect patients fromharmwerealmostuniformlyineffective.Insomecases,thoseagencieswereasignificantconstrainttothediscoveryandrectificationoferrors.
Theroleplayedbythemedicalprofessionalassociationswasthemostcommontargetofcriticism.Whiletheytendedtoarguethatprofessionsshouldbegiventhefreedomtomanagethemselves,theyfailedonfrequentoccasionstoindicatethattheyknewwhatprofessionalresponsibilityreallymeant.
Individualhealthcareprofessionalsandpatientsraisedtheconcerns
Noneoftheincidentsofpoorcarewouldhavecometothepublic’sattentionwhentheydid,ifithad not been for a combination of dedicated health professionals and concerned patients (and theirfamilies).Onecommonthreadisthatpatientsortheirfamilieswerepersistentinthefaceofreluctanceonthepartofhealthcareorganisations‘todotherightthing’.Inmostcases,thepatientandfamiliespersistedwiththeircomplaintslargelybecausenoonewaswillingformallytoadmittoerrors and apologise.
Healthcareorganisationswhosupportedinvestigationmostlydidsoininformalways.Inseveralcases,thisobviouslyincludedgivinginformalencouragementtopatientsandfamiliestopursuetheircomplaints.
Criticswereoftenignoredorabused
Whereindividualhealthprofessionalschosetospeakout,theywerealmostuniformlyignoredatbest.Theyweretreatedwithcontemptandabuseatworst.
Teamworkwasdeficient
Manyindividualswhowerelargelycompetentanddedicatedhadineffectiveworkingrelationships.Alltheinquiryreportsdescribedthevariousmanifestationsofpoorteamwork.Forexample,allofthemmentionlowlevelsofsharingofclinicaldocumentation,andinadequateunderstandingofandrespect for the contributions of other clinical professions.
Patientsandfamilieswerenotinformedmembersoftheteam
Eachinquirymakesmentionofpoorcommunicationbetweenhealthcareorganisationsandpatients and their families or other carers. The main features are more or less constant: patients werenotadequatelyinvolvedincareplanning(anddidnotalwayshaveanadequatebasisforinformedconsent);theywereunsureoftheirrights(andfrequentlyafraidofexercisingthem);weresometimestreatedininconsiderateways(mainlybydoctors);andseldomreceivedsympatheticandhelpfulsupportwhentheymadecomplaints.

7
1.2 Differences
Fiveoftheinquirieshavehardlyanydifferencesofsubstance:Bristol,Winnipeg,KingEdward,Southland,andCelje.TheinquiriesfromGlasgowandCampbelltown-Camdenareoutliersinafewrespects,asisclearfromthefollowingcomments.Table2summarisesthemaindifferencesbetweentheinquiries.
Table2:Differencesbetweeninquiries
n The distribution of case types
n Thebalancebetweenindividualandcollectiveresponsibility
n Legal aspects of care
n The severity of problems
Thedistributionofcasetypes
TheinquiriesatBristol,KingEdward,Southland,Celje,andWinnipegfocusedonanarrowrangeofcasetypesandcareprocesses(paediatriccardiacsurgeryatBristolandWinnipeg,oncologicalpathologyatCelje,mentalillnessatSouthland,andobstetricsandgynaecologyatKingEdward).ThiswastruetoalesserextentatGlasgow,withitsemphasisonhospitalacquiredinfection.TheCampbelltown-Camdenreportisanoutlierhere,sinceitwasdirectedata set of incidents crossing several clinical specialties.
However,thedifferencemaybeonlyminorinsomerespects.ThemixofcasetypesatCampbelltown-Camdenwasatleastpartlyaconsequenceofthewaythattheconcernsemerged:thenurseswhomadetheformalcomplaintshappenedtohaveavarietyofplacesofwork.Moreover,thereissomekindoffocusonemergencycare.Ifthecomplaintshadariseninadifferentway,theremightconceivablyhavebeenmoresimilarpatterns.TheCampbelltown-Camdenteamthatundertookthefinalinvestigationschosetorestrictthemselvestoallegationsregardingindividualpatients–andindeedweredirectedtodoso.Theymighthaveproduceddifferentfindingsif(say)theyhadbeenaskedtoinvestigateemergencyservicesorpalliativecare.
Thebalancebetweenindividualandcollectiveresponsibility
TheinquiryreportsfromBristol,KingEdward,Celje,andWinnipegplacegreatemphasisoncollectiveresponsibility.ThereisrecognitionofproblemsofteamworkinGlasgow,butittendstobe less explicit for the most part.
ThesamemaybetrueofSouthland:muchofthereportfocusesonwhatindividualhealthcareprofessionalsdid.However,inbothcases(andespeciallyinthecaseofSouthland)thenatureofthelegislationunderwhichtheinquirieswereconductedrequiredtheretobesuchafocus.
TheCampbelltown-Camdenreportisagainanoutlier.Theauthorsplacemuchmoreemphasisonindividualresponsibility,andmakeparticularmentionoftheneedtoensurethathealthprofessionalswhoperformpoorlyarecensured.Indeed,theCampbelltown-CamdenInquirywasrelativelycriticalofthosewhoseemedtowanttoemphasisesystemsproblems,suchastheHealthCareComplaintsCommission.Thisseemedtoreflecttheinitialconfusionoftheinquiryteamoverthemeaningofsystemsproblems,thesystemsapproach,anda‘noblame’culture.TheWinnipegInquiryand(perhapstoalesserextent)theremaindermayhavebeenlessconfused.

8 Patient Safety: a comparative analysis of eight Inquiries in six countries
Legalaspectsofcare
Again,thenotableoutlierisCampbelltown-Camden.Legalaspectsdominateditsreport,andmuchtimewasgiventoexplainingthewaysinwhichanearlierinquirybytheHealthCareComplaintsCommissionhadfailedtoapplytherelevantlaws.
Specificmentionwasmadeofthelocalpeculiarities:“Therelevantstandardsandsystems,bothforthedeliveryofhealthservicesandfordealingwithcomplaintsaboutthem,arecreaturesofNewSouthWaleslawandgovernment.ThereisnoavoidingthespecifictextsofNewSouthWaleslegislation governing the matters examined by this Inquiry.”
Again,however,thedominantfactormighthavebeenthedifferencesintermsofreference.TheinquiryteamofCampbelltown-Camdenhadacleardirectionthatemphasisedindividualaccountabilitiesunderthelaw.Moreover,theinquiryteamitselfseemedtobemorefamiliarwith(and consequently more interested in) the legislative rather than the health care systems aspects of poor care.
Theseverityoftheproblems
Glasgowisaclearoutlierinrespectofseverity.Unliketheothers,theinquiryteamonlymademildcriticisms,anditsmainconclusionwasthattherewasnoevidencethatthedeathsatGlasgow’sVictoriaInfirmarycouldhavebeenavoided.However,theymadealargenumberofrecommendationsforchange,andsomewouldatleastimplytherehadbeenweaknessesintheprovisionofcare.Speakersataconferencecalledtodiscussthefindingsweremorecriticalonthewhole.Termsrelatedtoculturalchange,improvedcommunication,bettercoordination,andimprovedteamworkwerefrequentlyused.
1.3 …andtheansweris…
Readerswillformtheirownviewsaboutthetotalityofthediagnosesandrecommendedtreatments.However,itseemstousthatmostofthemessagesareclearandtheyarerelevanttomosthealthsystemsaroundtheworld.
Theyaresuchcompelling,universalnarrativesintheirownrightthatwehavemostlyusedtheirownwordstotellthestory,ratherthanours.Indeed,oneofushasrecentlybeenreviewingproblemsintwoquitedifferentcountries–JapanandMongolia–andanotherofushasdoneworkinSingapore,EastTimorandPapuaNewGuinea–anditishardtospotthedifferencesrelativetotheeightstoriesrecountedhere.Thissuggeststhataspectsofthewaysofthinkingandbehavingare common to health care (and to medical and nursing in particular) and they tend to be more significantthandifferencesinsocialoreconomiccircumstancesfromcountrytocountry.
OneofthemessagesworthrepeatinghasbeenwellsummarisedbySiddins(2000)andwewillthereforeusehiswords.“TheDouglasInquiryhasclearlyillustratedsystematicdeficienciesinthedelivery and regulation of obstetric and gynaecological services. Such problems are not unique totheKingEdward.Irrespectiveofthespecialty,sevenmilliondollarsofcarefulanalysisatanyAustraliantertiaryhospitalwouldhaveyieldedthesameconclusions.Whatliesatthecoreoftheproblemaregrosslydeficientindustrystandardsforquality,safetyandefficiency.”Thathisviewsare so similar to many of those expressed about the other inquiries suggests he may have captured something essential.
Twofinalpointsareworthmakingattheriskoflabouringtheseissues.Thefirstthatthereisastrongargumentforinquiries,andthehealthsystemgenerally,totakeasystemsasopposedtoprosecutorialviewofthesecases.Hardlyanyoneinthesecasesknowinglyordeliberatelytriedtoharmanyone.TheactorsinthecaseswerenotlikeDrShipman,theBritishgeneralpractitioner

9
whosystematicallykilledatleast250patientsinacoldblooded,calculatingmanner(Smith2005).Aprosecutorialapproach,ifoverusedoremployedbluntly,willlikelyhaveundesirableconsequences:clinicians,especiallydoctors,willbelesslikelytoparticipateinchangeinitiatives(Braithwaite2005a).
Thesecondpointisthatculturechangeinmedicalandhealthsettingsisneeded.Bythiswedonotmeanstructuralchange(Braithwaiteetal2005)assooftenhappensinhealthcare,butchangetothefundamentalwaysstakeholdersworktogetherandrelatetoeachotherandtheirpatientsovertime.Thisislikelytorequireconcertedeffortoverthemediumorlongterminordertoachievesustainableresults.Thereislittlesubstituteforlongitudinaleffort.Shorttermfixeshavebeentriedmanytimesinmanysettings,andthesehavenotmadetheprogressneeded.
2 BristolRoyalInfirmary,UnitedKingdom
Ofthevariousinquiriesinrecentyears,Bristolisprobablythemostwidelyknown.Ithasbeenthesubjectofwidediscussioninthemassmediaaswellasinthetechnicalliterature.
Therearevariousreasonswhyithasattractedsomuchinterest.Oneisthedegreeofdemonstrableharm:thevictimswerechildren,andmanyofthemdiedorwerepermanentlydisabled.Anotheristhethoroughnessoftheinquiryprocess:relativelydetailedandobjectiveinquirieswereundertakenbothbytheGeneralMedicalCouncil(GMC)andtheDepartmentofHealth,andtheirreportsweremadepubliclyavailableattheearliestpossibleopportunity.Perhapsthemainreasonforinterest,however,isthattheweaknessesweresoobviousandyetnothinghappenedforsolong.Inshort,itisastorythatishardtoaccept.
Webeginbydescribingtheeventsthatledtotheinquiries.BriefmentionisthenmadeoftheinquiryconductedbytheGMC,butwefocusonthelargerinquirysubsequentlyconductedbytheDepartmentofHealth.
2.1 Context
TheBristolRoyalInfirmary(BRI)andtheBristolRoyalHospitalforSickChildren(Children’sHospital)areteachinghospitalsassociatedwithBristolUniversity’sMedicalSchool.Together,theyformedtheUnitedBristolHospitalTrust–oneofthepartlycorporatisedcomponentsoftheNationalHealthService(NHS)thatemergedfromThatcher’sinternalmarketreformsofthelate1980s.WewillrefertotheBRIandtheChildren’sHospitaltocoverthetwohospitalsitesatwhichcareoccurredthatwasthesubjectoftheInquiry.Wherebothareinvolved,wewillrefertothem simply as Bristol.
Animportantareaofspecialisationisheartdiseaseinadults,childrenandinfants.Thecasesreviewedinthisreportconcernedcongenitalheartdisease–babiesbornwithheartproblems,and their subsequent treatment predominantly through open-heart surgery.
Open-heartsurgeryonbabiesisariskyenterprise.Bristolundertookpioneeringworkinthisclinicalareaduringthe1980s,inordertoprovideservicesforitscatchmentarea–muchofsouthwestEnglandandsouthWales,whichhadhistoricallybeenneglectedintermsofitsshareoftheresourcesoftheNHS.Thisneglectwasreflectedintheresourcesavailableforcardiacsurgicalcare.Therewerenationalshortagesinpaediatriccardiologistsandpaediatricnurses,buttheywereparticularlyevidentinBristol’scatchmentarea.Shortagesofresourceswerenot

�0 Patient Safety: a comparative analysis of eight Inquiries in six countries
onlyreflectedintherevenueavailabletoemployedstaff,butalsointhecapitalavailableforbuildings and equipment.
Intheearly1980s,thethenDepartmentofHealthandSocialSecurity(DHSS)establishedaprocesswherebycertainveryspecialisedservicesshouldbefundedcentrally.Theaimwastoconcentrateresourcesandexpertise.Theprocess,establishingwhatwerecalledSupra-regionalServices(SRS),wasintendedtocontroltheproliferationofunits.
Inturn,thiswouldavoidtheriskoftoomanyunitsexpendinglargeamountsofresourcesdoingonlyafewprocedures.Itwouldalsomeanthatthecliniciansinvolvedwouldencounterasufficientnumberofwhatwererarecasestoacquirethenecessaryexperienceandexpertise.
PaediatriccardiacsurgerywasoneoftheservicesdeemedsuitableforcategorisationasanSRS.Theservicewaslimitedtopaediatriccardiacsurgeryonnewbornandinfantchildrenuptooneyearofage.Bristolwasmadeoneoftheninedesignatedcentresin1984.Atthesametime,Bristolalsocontinued to carry out heart surgery on children over one year of age.
In1984,atthestartoftheperiodthatwassubjectedtoreview,therewasadesignatedserviceforbabiesunderoneyearold,whichinvolvedopen-heartsurgeryattheBRIandclosed-heartsurgeryattheChildren’sHospital.Therewasalsoaservicefundedfromlocalsourcesforchildrenoveroneyearofage,similarlydividedbetweenthetwohospitals.However,thecombinedvolumesofopen-heart operations never reached the numbers deemed appropriate to ensure economies of scale and appropriate quality.
AdversecommentsaboutaspectsofBristol’sperformancesurfacedfromtimetotime.However,theinterpretationofgoodperformancewasunderstoodindifferentways.TheeconomicrationalismoftheThatchergovernmentencouragedtheviewthatperformancewasbestequatedwiththroughput.Thiswasrelevantbothbecauseoftheassumptionofarelationshipbetweenthevolumeofcasestreatedandthedevelopmentofprofessionals’skills,andalsobecausefundingwasbasedontreating a targeted number of cases. Performance could also refer to the quality of care and patient outcomes,buttherewaslessinterestandmoreconfusionaboutsuchdefinitions.
ItwasrecognisedinBristolandintheDepartmentofHealththatthecircumstancesunderwhichpaediatriccardiacsurgerywascarriedoutinBristolwerecapableofimprovement.Fromtheearly1980s,proposalsweredevelopedtoconsolidatetheserviceononesiteinthewhollypaediatric-orientedenvironmentattheChildren’sHospital.Thiswouldavoidtheneedtocarryouttheopen-heartsurgeryattheBRIinacontextinwhichchildrenweretreatedandcaredforalongside(andtoadegreeincompetitionwith)adults.Itwasalsoplannedtoappointapaediatriccardiacsurgeon–onewhowouldoperateonlyonchildrenandnot,aswasthecasewiththecardiacsurgeonsinBristol,alsocarryoutoperationsonadultswithacquiredheartdiseases.Theseplansdidnotcometo fruition until �995.
Fromthelate1980s,doubtsandconcernsaboutaspectsoftheperformanceoftheBristol’sPaediatricCardiacSurgeryUnit(PCS)wereincreasinglyexpressedinavarietyofcontexts.SomeoftheseconcernswereexpressedbyhealthcareprofessionalsworkinginthePCS.OtherswereexpressedbyindividualsinavarietyofcontextsoutsidetheUnit.Concernsalsocirculatedintheform of rumour and some appeared in the form of unattributed reports in the media. An operation performedonJoshuaLovedayon12January1995provedtobethecatalystforaction.Joshuadiedontheoperatingtable.Anoutsidereviewwasinstituted.Paediatriccardiacsurgerywasallbuthalteduntilanewsurgeonwasappointed(Joffe1995).

��
2.2 TheInquiries
2.2.1 InquirybytheGeneralMedicalCouncil(1998)
ComplaintsweresubsequentlymadetotheGeneralMedicalCouncil(GMC)concerningtheconductoftwocardiacsurgeons(DrWisheartandDrDhasmana),andoftheChiefExecutiveoftheTrust(DrRoylance).ThecomplaintswereinstigatedbyananaesthetistwhohadbeenworkingatBRI,DrStevenBolsin.
TheGMC’sInquirywaslimitedinscope.Itonlyconsideredtherolesofthethreedoctorsagainstwhomthecomplaintshadbeenmade.Italsoonlyconsideredthecasesof53childrenofwhom29haddied,andfocusedparticularlyononetypeofsurgicalprocedure(theSwitchoperation).
Thethreedoctorswerefoundguiltyofseriousprofessionalmisconduct.DrRoylanceandDrWisheartwereremovedfromtheMedicalRegister.DrDhasmana’sregistrationwascontinued,subject to a three year restriction that he did not operate on children.
2.2.2 InquirybytheDepartmentofHealth(2001)
AgroupofparentsofchildrenwhohadundergonecardiacsurgeryattheBRIorganisedthemselvestoprovidemutualsupport.InJune1996thegroupfirstcalledforapublicinquiryintothe paediatric cardiac surgery services at the BRI. They fought against strong opposition and finallysucceededinachievingtheirgoalinJune1998,whentheSecretaryofStateforHealthannounced to Parliament the establishment of the Inquiry that is the main source of information forthispaper.TheInquiry’sreportwasreleasedin2001.
Theindicationsofpoorcare
ConcernsaboutthepaediatriccardiacsurgeryserviceinBristolwerefirstraisedasearlyas1986inavarietyoflargelyinformalways.From1988,concernsbegantoberaisedinsidetheBRI.TheleadwastakenbythejunioranaesthetistDrStevenBolsin,whowroteformallytotheChief Executive (Dr Roylance) in �990 expressing his concerns about practices in the operating room.
Hesubsequentlycollecteddataandtookthemtoanincreasingnumberofcolleagues.Accordingtotheinquiryteam,hewastypically“…advisedtotakecaretoverifyhisinformationanddiscussitwithcolleagues,includingthosewhoseworkgaverisetohisconcern.”DrBolsin’sownaccount,aspresentedbelow,issomewhatdifferentinemphasis.Inparticular,heclaimsthathisconcernswerelargelyignoredbyhismedicalcolleagues.
AmemberandanofficialoftheDepartmentofHealth’sSupra-regionalServicesAdvisoryGroup(SRSAG)hadevidenceby1992thatBristolwasperformingpoorlyintermsofmortality,yetdidnotsharethisinformationwiththeSRSAGasawhole.
ThecliniciansinBristolatleastby1990haddataontheirownpoorperformancerelativetothatofothercentresintheUK,whichcouldhavecausedthematleasttopauseandreflect.Instead,inkeepingwiththemindsetofthetime,theypressedon,drawingfalsecomfortfromtheirfiguresfor1990(whichprovedtobeanexception),andonlybelatedlyceasingtocarryoutcertainoperations on children under one year of age.

�2 Patient Safety: a comparative analysis of eight Inquiries in six countries
AnopportunitywasnottakeninJuly1994byanofficialoftheDepartmentofHealth(DOH)toinvestigate more closely the outcomes of paediatric cardiac surgery in children under one year old. Itwasonlyin1995thatpaediatriccardiacsurgerywasformallystopped(althoughsomeoperationswerestillcarriedoutafterthen).
From the start of the �990s a national database existed at the Department of Health (the Hospital EpisodeStatisticsdatabase)thatheldinformationaboutdeathsinhospitals.However,itwasnotgenerally recognised as a valuable tool for analysing the performance of hospitals.
TheanalyticalworkundertakenbyDrBolsinandotherswassubsequentlyreviewedandextendedby experts appointed by the Inquiry. The experts concluded that the data available at the time showedBristolhadasignificantlyhighermortalityrateforopen-heartsurgeryonchildrenunderonethanthatofothercentresinEngland.Between1988and1994themortalityrateatBristolwasroughlydoublethatelsewhereinfiveoutofsevenyears.Thismortalityratefailedtofollowtheoveralldownwardtrendovertimethatcanbeseeninothercentres.
Itwasfurtherconcludedthatasubstantialandstatisticallysignificantnumberofexcessdeaths,between30and35,occurredinchildrenunderoneyearofageundergoingcardiacsurgeryinBristolbetween1991and1995.‘Excessdeaths’isastatisticalmeasureofthenumberofdeathsobservedoverwhatwouldbeexpectedifthePCShadbeentypicalofotherpaediatriccardiacsurgery units in England.
Themortalityrateovertheperiodfrom1991to1995wasprobablydoubletherateinEnglandatthetimeforchildrenunderone,andevenhigherforchildrenunder30days.ThishighermortalityrateinBristolwasnotrestrictedtotheneonatalswitchandatrio-ventricularseptaldefectoperations.Evenwithouttakingthesetwohigherriskgroupsintoaccount,therewasconsiderableevidenceofdivergentperformanceinBristol.Further,differencesinmortalityratesinBristolcouldnotbeexplainedbydifferencesincasemix(anexplanationwhichsomecliniciansboththenandevennowhave adopted).
Theinquiryprocess
TheTermsofReferenceoftheDepartment’sinquirywere“…toinquireintothemanagementofthecareofchildrenreceivingcomplexcardiacsurgicalservicesattheBristolRoyalInfirmarybetween1984and1995andrelevantrelatedissues;tomakefindingsastotheadequacyoftheservicesprovided;toestablishwhatactionwastakenbothwithinandoutsidethehospitaltodealwithconcernsraisedaboutthesurgeryandtoidentifyanyfailuretotakeappropriateactionpromptly;toreachconclusionsfromtheseeventsandtomakerecommendationswhichcouldhelptosecurehigh-quality care across the NHS.”
Theinquiryteamsaysitadopted“…a‘systems’approachtoanalysis,bywhichpoorperformanceanderrorsareseenastheproductofsystemswhicharenotworkingwell,asmuchastheresultofany particular individual’s conduct.”
ThepublicinquirywasconductedbetweenOctober1998andJuly2001intwophases.Inphaseone,thefocuswasoneventsinBristol.Evidencefrom577witnesses,including238parents,wasreceivedinwriting.TheInquiryalsoreceived900,000pagesofdocuments,includingthemedicalrecordsofover1,800children.Oralevidenceofselectedwitnesseswastakenover96days.Thefocusofphasetwowasthefuture.Some180papersweresubmittedtosevenseminarsinwhich150participantsfromtheNHS,andthepublicandprivatehealthcaresectors,tookpart.

�3
Theinquiryteamconcludedtherewereindividualswhocouldandshouldonoccasionshavebehaveddifferently.InthefinalstagesoftheInquiry,eachindividualwasadvisedthattheInquirywasmindedtocommentadverselyonsomeparticularaspectofhisorherconductorbehaviour,whetheraparticularincidentorapatternofbehaviour,andwastoldoftheevidenceonwhichtheInquiryrelied.Eachhadanopportunitytomakerepresentations.ThoserepresentationsweretakenaccountofbytheInquiryinreachingitsconclusions.
2.3 ConclusionsoftheInquiry
TheDOHinquiryteamwrotethatthestoryofthepaediatriccardiacsurgicalserviceinBristolwasnotaboutbadpeople.“Norwasitanaccountofpeoplewhodidnotcare,norofpeoplewhowilfullyharmedpatients.Itisanaccountofpeoplewhocaredgreatlyabouthumansuffering,andwerededicatedandwellmotivated.Theyalmostwhollyhadgoodintentionsandworkedlonghourswithgreatdedication.”
However,theywerepartofasystemthatdelivereddemonstrablypoorcare.Themainreasons,asjudgedbytheinquiryteam,aresummarisedbelow,andforthemostpartweresystemic.Theinquiryteamsimplysaysthat“…thehealthcareprofessionalsatBristolwhoseworkwasfoundtohaveharmedpatientswere,forthemostpart,productsofasystemthathadfundamentalweaknesses.”
Underfundingwasnotthecauseofpoorcare
ThroughouttheInquiry,therewereregularreferencestounderfundinginBristol.Thosewhoraisedthemattermostlyimpliedtherewasagapbetweenthelevelofresourcesneededproperly to meet the stated goals of the paediatric cardiac surgery unit and the level actually available.
Insomesense,theseclaimswerejustified.Theinquiryteamnotedtherewereconstantshortagesinthesupplyoftrainednursingstaff,bothfortheoperatingtheatreandtheIntensiveCareUnit(ICU).Thecomplementofcardiologistsandsurgeonswasalwaysbelowtheleveldeemedappropriatebytherelevantprofessionalbodies.Theconsultantcardiologistslackedjunior support.
TheywereexpectedtocareforchildrenintheChildren’sHospital,andintheBRIoperatingtheatreandICUseveralhundredyardsawaydownasteephill,andtoholdoutreachclinicsalloverthesouthwestandsouthWales.Thecareofchildrenundergoingpaediatriccardiacsurgerywassplitbetweentwoseparatesites.Facilitiesforparents,andnecessarymedicalequipmentforchildren,hadtobefundedthroughacharitableagency,TheHeartCircle.
However,theinquiryteamacceptedtheclaimsonlytoalimiteddegree.First,itnotedthattheinadequacyinresourcesforpaediatriccardiacsurgeryatBristolwastypicaloftheNHSasawhole,andyetothersimilarhealthcareorganisationswerenotmakingthesamenumberofcatastrophicerrors.Theinquiryteamthereforeconcludedthat“…whateverwentwrongatBristolwasnotcaused bylackofresources.Othercentresexperiencedthesameorsimilardifficulties.Forexample,theshortageinqualifiednursesandincardiologistswasanationalphenomenon,affectingallcentres.Wethereforeemphasisethepointagainthat,whileunder-fundingblightedtheNHSasawhole,itdoesnotaloneprovidetheexplanationforwhatwentwronginBristol.”

�4 Patient Safety: a comparative analysis of eight Inquiries in six countries
Wenoteinpassingthat,in2000,theUKgovernmentannouncedamajorincreaseinfundingfortheNHSasawhole.ItcommitteditselftomatchingtheaveragelevelofhealthspendingfortheEuropeanUnion.However,wealsoobservethathardlyanyoftheincreasedspending(whichamountedtoanincreasefromabout7%to9%ofGDPinthreeyears)wasreflectedinincreasedservicevolumes.Mostseemstohavedisappearedintosalaryandwageincreases,andcatchingupon the decades of underspending on capital-related assets.
However,themainpointmadebytheinquiryteamissurelycorrect.Ifresourceswereinsufficienttomeetthedemand,itwouldhavemadesensetoreducethedemand,tolookforefficiencysavings,totransferthechildrentoothercentrestogaineconomiesofscaleandqualityimprovements,andso on.
TheNHSmadeerrorsinapprovingtheservice
The inquiry team expressed serious doubts about the appropriateness of establishing the Supra- regionalServicesatBristol.Theteamsaidthat“…designationhasallthequalitiesofaGreektragedy:weknowtheoutcomeandyetareunable,fromourpointintime,topreventitunfolding.”
ItwasunwiselyassumedatBristolthat,iftherewereweaknesses,theywouldbeovercomeintime.Thepoliticsofregionalequity,professionalassociationsupport,andsoonweregivenexcessiveweightandthiscloudedobjectivity.Infact,theservicefailedtoimproveinthemannerthatmanypeoplehadhoped.Bristol’shighaspirations,includingattemptstobecomeacentreforhearttransplantation,werenotmatchedbyitscapabilities.ThecircumstancesthatcausedBristoltobeaninappropriatecandidateinthefirstplacewerenotchangedbytheactofdesignation.Rather,thesenseofself-importanceandcompetencewasreinforced.Subsequently,itwasthesetofexistingconditionsthatwerethebarrierstofurtherimprovement.Theinquiryteamsaidthat“…exhaustionandlowmoraleledtostagnationandaninabilitytomoveforwardinresponsetonewdevelopments,despitethestimulusprovidedbyanewgenerationofconsultants.”
TheserviceattheBRIwaspoorlyorganised
Poororganisationoftheservicewasreflectedinseveralways.Forexample,theserviceofferingpaediatricopen-heartsurgerywassplitbetweentwosites.Ithadnodedicatedpaediatricintensivecarebeds,nofulltimepaediatriccardiacsurgeon,andtoofewnursestrainedinpaediatrics.
Aparticularconcernwasthatthecardiologistswerebasedinonehospitalandsurgeonsinanother.Thecardiologists,whowerewellregardedthroughoutthesouthwest,wereunderstaffed.Therewasa national shortage of specialists in paediatric cardiology. This meant that the cardiologists at Bristol couldnoteffectivelyparticipateinsurgeryorintensivecare.Inaddition,theprevailingnationalshortageinnursestrainedinpaediatriccarewasreflectedinBristol.Thesurgeonsoperatedonadultsaswellaschildren,andthechildrenwerenursedalongsideadultsinamixedICU.Whiletherewasaneffectivechild-centredapproachtocareattheChildren’sHospital,thiswasnotsointheBRIwhereopen-heartsurgerywascarriedoutandwherethemanagementofcareintheICUwasdescribedas‘highlydisorganisedwithconflictingdecisions’.Itwasneverreallyclearwhowasin charge.
Thesplitsiteandconsequentsplitserviceweremajorfactorsaffectingtheadequacyofcare.Unifyingthesitedidnotattractsufficientpriorityinthebargainingforresources:theclaimsforthepaediatriccardiacsurgeryservicemadebysomeoftheclinicianswerenotseenasimportantenough.However,thisdidnotcausetheclinicianstoceasetooffertheservice.Thereseemstohavebeenanoverridingsenseofpressingonandhopingthatonedaytheservicewouldbemoved

�5
ontoonesite,thatthenewhospitalforchildrenwouldbebuilt,thatthenewsurgeonwouldarrive,andthatallwouldthenbewell.
Inequitabletreatmentofthevariousclinicalprofessions
Seniordoctors(consultants)enjoyed(andstillenjoy)whatisvirtuallyajobforlife.Theirrelationshipwiththehealthcareorganisationthatemploysthemmakesitdifficulttobringabout change. Far less attractive employment conditions arrangements applied for most other categories of staff.
The inquiry team argued that all employees should be treated in a broadly similar manner. Doctors,nursesandnoncliniciansmustworktogetherashealthcareprofessionals,withcomparabletermsofemploymentandclearlinesofaccountability,iftheyaretoprovidethebestpossible care for patients.
Forthisandotherreasons,doctorshadexcessivepowerandtoolittleaccountability.Intotal,theinquiryteamconcludedthattherewas“…animbalanceofpower,withtoomuchcontrolinthehandsofafewindividuals.”Manygroups,butparticularlytheseniordoctors,hadestablisheda’clubculture’wherebytheirviewscouldbereinforcedandimposedonothers(Dyer2001).
Theabsenceofdefinedstandardsofcare
TherewerenoagreedstandardsofcareforpaediatriccardiacsurgeryorforanyotherspecialtyatBristol,butpatientswerenotawareofthis.TheinquiryteamarguedthatparentstakingtheirchildrentobetreatedinBristolassumedthatthelevelofcareprovidedwouldbegood,giventhatthecarewouldbeprovidedbyasupra-regionalcentreselectedbytheDepartmentofHealth.Theytrustedthesystemwithoutgoodreason.
Failuretoshareinformation
Theinquiryteamsaidthat“…Bristolwasawashwithdata.”Therewasenoughinformationfromthelate1980sonwardstocausequestionsaboutmortalityratestoberaisedbothinBristolandelsewherehadthemindsettodosoexisted.
However,littleifanyofthisinformationwasavailabletotheparentsortothepublic.Suchinformationaswasgiventoparentswasoftenpartial,confusingandunclear.Thereshouldhavebeenmoreopenness about clinical performance. Patients should have been able to gain access to information abouttherelativeperformanceofahospital,oraparticularserviceorconsultantunit.
Nostructuredmonitoringofquality
The clinicians in Bristol had no one to satisfy but themselves that the service that they provided wasofappropriatequality.Therewasnosystematicmechanismformonitoringtheclinicalperformance of health care professionals or of hospitals.
Theabsenceofadequatemanagementwassimplynotrecognisedbymoststaff.Theinquiryteamsaidthat“…itwouldhavetakenadifferentmindsetfromtheonethatprevailedonthepartofthecliniciansatthecentreoftheservice,andseniormanagement,tocometothisview.Itwouldhaverequiredabandoningtheprincipleswhichthenprevailed:ofoptimism,oflearningcurves,andofgradualimprovementsovertime.Itwouldhaverequiredthemtoadoptamorecautious approach rather than muddling through.”

�6 Patient Safety: a comparative analysis of eight Inquiries in six countries
Atalocallevel,therewassomerelevantactivity.Thecliniciansinvolvedinprovidingthepaediatriccardiacsurgeryservicecollectedanalyseddataonproceduresanddeaths,establishedandmaintainedcomputerisedinformationsystems,producedandcirculatedstatisticsandanalyticalreports,madeannualreturnstothenationalUKCardiacSurgicalRegisterandreceivedbackaggregated data about national performance. They also held regular meetings to discuss the results ofaudits,andreviewedindividualandseriesofcases.However,theseprocessesweremadelargelyineffectivebecauseoftheculture.Statisticswerecollectedthatrepresentedendsinthemselves,viewsaboutqualitywerealreadyestablishedandwerelargelynotinfluencedbyevidence,andanyonequestioningperformancewasconsideredtobeinexperiencedormischievous.
Atanationallevel,therewasconfusionastowhowasresponsibleformonitoringqualityofcare.The SRSAG thought that the health authorities or the Royal College of Surgeons had the matter undercontrol,theRoyalCollegeofSurgeonsthoughttheSRSAGortheTrustweresupervisingtheactivities,andsoon.Theinquiryteamsaidthattherealitywas“…no-onewasdoingit.Wecannotsaythattheexternalsystemforassuringandmonitoringthequalityofcarewasinadequate.Therewas,intruth,nosuchsystem.”
Poorteamwork
Theinquiryteamsaiditwasabletoreachoneconclusion“…thatowesnothingtohindsight.”Therewaspoorteamworkandthishadimplicationsforperformanceandoutcome.Thecrucialimportanceofeffectiveteamworkinsuchacomplicatedsurgicalareawasverywidelyrecognised,butBristolwasunabletoputthisinplace.Everyonejustacceptedthatteamworkwaspoor,andassumedthatnothing could be done to improve it.
Therewerelogisticalreasonsforthis:forexample,thecardiologistsoftencouldnotbewheretheywereneededbecauseofthesplitsite.However,themainreasonswerecultural.Theinquiryteamsaidthat“…relationsbetweenthevariousprofessionalgroupswereonoccasionspoor.Alltheprofessionalsinvolvedinthepaediatriccardiacsurgeryservicewereresponsibleforthisshortcoming.”However,itwasconcludedthatthepoorteamworkwasprimarilyaconsequenceof“…aclearlackofeffectiveclinicalleadership.Thoseinpositionsofclinicalleadershipmustbearthe responsibility for this failure and the undoubtedly adverse effect it had on the adequacy of the paediatric cardiac surgery service.”
Inappropriatemanagementculture
LikemosthealthcareorganisationsintheUK,Bristolwasmanagingthetransitionfromtheknown(theoldNHS)totheunknown(Truststatus)duringmostoftheperiodunderreview.However,unlikemostotherhealthcareorganisations,thestyleofmanagementwassuchastomakeanykindofreformdifficultandrisky.Theinquiryteamsaysthat“…thesystemsandcultureinplaceweresuchastomakeopendiscussionandreviewmoredifficult.Staffwerenotencouragedtosharetheirproblemsortospeakopenly.Thosewhotriedtoraiseconcernsfoundithardtohavetheirvoiceheard.”
TheChiefExecutivewasjudgedtobethoughtfulandprincipledinhisdevelopmentofamoreappropriatemanagementsystem,andhesucceededinmeetingtheprincipalobligationofbalancingthebooks.However,hecreatedfragmentationandignoredwaysofalleviatingtheconsequentproblems.Heestablishedasystemofseparateandvirtuallyindependentclinicaldirectorates,andgaveaclearmessagethatproblemswerenottobebroughttohimfordiscussionandresolution.Theinquiryteamsays“…therewaspowerbutnoleadership.Theenvironmentwasoneinwhichproblemswereneitheradequatelyidentifiednoraddressed.”

�7
InappropriateinvolvementoftheBoardofManagement
ThestyleofdownwardmanagementwasreflectedinthewaytheChiefExecutivehandledtheBoard.TheChairmanandtheTrustBoardwereeitherpartofthe‘club’ortreatedasoutsiders.
Referringtoinformationabouttheoutcomeofcare,MrMcKinlay,theChairmanoftheUnitedBristolHospitalTrust(UBHT)from1994onwards,toldtheinquiryteamthat:”…therewasnotraditionorcultureinUBHTthattheBoardorthecommitteesoftheBoardshouldbeinvolved.Ithoughtthatwassomethingthatwaswrong.IthoughttheBoardshouldhavesomeknowledgeofstatisticaloutcome,buttherewasatightropetobetrodtofindawayofeasingitintoplace.”
InappropriateNHSmanagement
TheproblemsshouldhavebeenidentifiedthroughexternalmonitoringatsomelevelintheNHS.However,whatwashappeningatBRIwascertainlynotadequatelyindicatedfromroutinereporting systems (or more precisely from the continual interpretation of those systems).
Thiswaspartlyaconsequenceoftheprevailingdogma.Theinternalmarkethadbeenpushedontoanunsuspecting(andlargelyconfusedoruninterested)healthcaresystem,andtheprescribedgoalswerebusinessplans,competition,andmarketforces.Theinquiryteamsays“…thiswasafeatureoftheNHSreformsin1989-1991:seniormanagerswereinvitedtotakecontrol,butlittleornosystemexistedtomonitorwhattheydidintheexerciseofthatcontrol.”
Thisisnotsurprisinginviewofthemanymantrasthatpromotedtheviewofbusinessindependence,suchas‘localautonomy’,‘freedomtoinnovate’,and‘marketcompetition’.Thesekindsofideasmighthavemadesenseinsomesectors,wherepatientshavetheknowledgeandpowertodemandbetterquality,buttheydidnotmakemuchsenseinthehealthsector.
Poorwaysofdealingwithpatients
Someparentswerehighlysatisfiedwiththecaretheyreceivedfromdoctors,nursesandothersandotherparentswerehighlydissatisfied.Themaincomplaintsweredirectedatthedoctors,andparticularlythesurgeons,whowereclaimedsometimestobeuncaringandtohavegivenmisleading information.
Intotal,whiletheevidenceispolarised,thereisastrongsensethatonmanyoccasionscommunicationbetweenparentsandsomestaffwaspoor.Theredoesnotappeartohavebeenanydeepthinkingabouthowtocommunicateinformationtoparentsinadvanceofsurgery,noranysystematisedapproachtodoingso.Someparentsfeltthattheyhadbeensignificantlyhelpedtounderstandwhatthesurgeryandsubsequentintensivecareinvolved,buttherewerealsoreportsfromparentsofdoctorsandnursesdrawingdiagramsonscrapsofpaper,orevenapapertowel.Theprocessofinformingparentswasapparentlyseentobeachorebythesurgeons.
Particularcriticismwasdirectedatthematterofinformedconsent,particularlytothesurgicalprocedure.Thecriticismtookaccountofthehighneedsofparentsforadequateinformationatanextremelystressfultime.Theinquiryteamsaidthatparentswerefacedwithdecisionsaboutamajoroperationwithanuncertainoutcomeandyettheywereoftentreatedperemptorilyorwithnothingclosetorespectandunderstanding.

�8 Patient Safety: a comparative analysis of eight Inquiries in six countries
Therewasnoobviousprocess:nocarefullywrittenmaterials;noscheduledtimeforparentstoreflectontheinformationandthenaskformore;andnoformalattempttoinvitequestionsandanswerthem.TheinquiryteamnotedthattherewereseriouslyinadequatepracticesatBristolbuthowthedoctorsbehavedwouldnothavebeenregardedaspoorpracticeelsewhereatthattime.
Someparentssaidtheyweregivensupportandcounselling,andcommentedfavourablyonit.However,otherparentssaidthattheyreceivednocounsellingatall.Manyparentswerecriticalaboutthewayinwhichtheywereinformedoftheirchild’sdeath.Again,thecriticismsweremostlydirectedatdoctors:parentsweregenerallyfavourablyimpressedbythesensitivityandsupportshownbythenursingstaff.TheUBHTconcededinitsevidencethattheserviceitprovidedwasinsufficienttomeettheneedsofsomeparents.
Thecentralproblem:destructiveorganisationalcultures
Itisclearfromtheconclusionssummarisedabovethatthemainproblemswereculturalratherthanconsequencesof(say)logisticalproblems,resourcelimitations,oralackofknowledge.Indeed,the inquiry team made repeated reference to the organisational and professional cultures – the establishedwaysofthinkingandactingthatwereacceptedwithoutquestionbymostpeopleinvolved.Some(butnotall)ofthosepatternswerejudgedtohavecontributedtocarethatwasdemonstrably poor in both objective and subjective terms.
Theinquiryteamsaid,inconclusion,thatsomeofthoseinvolved“…lackedinsightandtheirbehaviourwasflawed.Manyfailedtocommunicatewitheachother,andtoworktogethereffectivelyfortheinterestsoftheirpatients.Therewasalackofleadership,andofteamwork.”
Attributionofprimaryresponsibility
Forthemostpart,theinquiryteamchosetoemphasisethateveryonewastoblameandyeteveryonewasaprisoner.However,itmadespecificmentionofafewindividualswho“…displayedflawsintheirapproachtomanagement…showedalackofleadershipandinsight…or…failedtotreatparentswithappropriaterespectandcandour.”InadditiontothethreedoctorscensuredbytheGMC,theinquiryteamcriticisedtheClinicalDirectorofChildren’sServicesandtheDirectorofOperations(andNurseAdviser)attheUBHT.
TheinquiryteamalsonamedpeopleathigherlevelsintheNHS,mainlyfortheirfailuretotakeactionwithrespecttostrongevidenceofinadequatecareatBristol.TheyweretheMedicalSecretaryoftheSRSAG,aSeniorMedicalOfficerintheDepartmentofHealth,andthePresidentoftheRoyalCollegeofSurgeons(whowasalsoamemberoftheSRSAG).
2.4 RecommendationsoftheInquiry
TheinquiryteamstressedtheimportanceoflearninglessonsfromBristol.Initsview,itwasnotpossibletosaythat“…eventssimilartothosewhichhappenedinBristolcouldnothappenagainintheUK,orindeedthattheyarenothappeningatthismoment.”
Itsmainrecommendationsareoutlinedbelow.Inmakingthem,theinquiryteamstressedsomeguidingprinciplesincludingthefollowing:
n The complexity of the NHS must be recognised. There are no easy solutions
n PatientsmustbeatthecentreoftheNHS,andthusthepatient’sperspectivemustbeincludedinthepolicies,planninganddeliveryofservicesateverylevel
n Systemsofcare,andfacilities,aswellasindividuals,affectthequalityofhealthcare.Qualitymust include all aspects of care: clinical and non clinical. Patients’ safety must be the foundation of quality

�9
n Learningfromerror,ratherthanseekingsomeonetoblame,mustbethepriorityinordertoimprove safety and quality. Openness and transparency are as crucial to the development oftrustbetweenhealthcareprofessionalsandpatients,astheyaretothetrustbetweentheNHS and the public.
Thecareofchildren
Severalrecommendationsweremadeinthisregard,andtheyneedonlybesummarisedbrieflyhere.First,theremustbemorecoordination,andgreaterintegrationshouldbeaconsequenceof design rather than the actions of a subset of dedicated individuals.
Second,theidealarrangementforchildren’sacutehospitalservicesisachildren’shospital,close to an acute general hospital. Specialist care must be concentrated in a limited number of centreswherethestaffhavethenecessaryskillsandexperience.
Third,theremustbestandardsforthecareofchildren,someofwhichmustbemandatory.There must be incentives to improve children’s care. There must be plans for the publication of information about the quality and performance of children’s health care services.
Fourth,allhealthcarestaffwhotreatchildrenmusthavetrainingincaringforchildren.Theyshouldalsobetrainedincommunicatingwithyoungpeopleandparents.
Respect,honesty,andgoodcommunicationbetweenpatientsandclinicians
Thequalityofhealthcarewouldbeenhancedbyagreaterdegreeofrespectandhonestyintherelationshipbetweenhealthcareprofessionalsandpatients.Futuredoctors,nursesandotherhealthcareprofessionalsmustbeadequatelytrainedincommunicationskillsduringtheirinitialeducation.
Theinquiryteamarguedthatgoodcommunicationisessential.However,itwasinformedbytheRoyalCollegeofSurgeonsofEnglandthat“…itistheareaofgreatestcompromiseinthepractices of most surgeons in the NHS and the source of most complaints”.
Thebasicdrivingforceshouldbeasenseofpartnershipbetweenthepatientandhealthcareprofessionals. Partnership depends critically on the free and honest exchange of information. Thisisparticularlyimportantwhenthingsgowrong.Notonlydoesthisshowrespecttopatients.Anerror,onceacknowledged,alsoallowslessonstobelearned.
The inquiry team argued there are four fundamental principles in this regard: trust can only besustainedbyopenness;opennessmeansthatinformationbegivenfreely,honestlyandregularly;itisoffundamentalimportancetobehonestaboutthetwinconcernsofriskanduncertainty; and the informing of patients must be regarded as a process and not a one off event.
Hospitalsmusthaveanintegratedsystemofsupportandcounsellingforpatientsandcarers,staffedbywelltrainedprofessionalswithlinkstosystemsoutside.Suchasystemiscentraltocare,notanafterthought.Thereshouldbeaclearsystemintheformofa‘onestopshop’inevery Trust for addressing the concerns of patients about the care provided or the conduct of a health care professional.
Finally,itshouldnotbeaquestionofthehealthcareprofessionaljudgingwhattheparentneedstoknow:itistheparentwhoshouldmakethatdecision.Theoldwayofthinkingmustbeabandoned – that patients should be protected from too much information.

20 Patient Safety: a comparative analysis of eight Inquiries in six countries
Leadershipandmanagement
The inquiry team argued that the highest priority needs to be given to improving the leadership and managementoftheNHSateverylevel.First,thereareimplicationsforthegovernmentwithrespectto the health sector: it must manage the NHS; and it must establish effective systems to regulate the quality of health care that are appropriately competent and independent. The inquiry team did notdefineindependence.Fromwhatisstatedelsewhereinitsreport,wemustassumethemainrequirementwasindependencefromthoseagenciesorindividualsdeliveringcare.Perhapstheinquiry team meant independence from government.
Second,chiefexecutivesofhealthcareorganisations(Trustsinthiscase)mustbesupportedandenabledtocarryouttheirtaskofmonitoringandimprovingthequalityofhealthcare.Thisisparticularlythecase,giventhattheyhavebecomelegallyresponsibleforthistask.Inter alia,thisrequiresthechiefexecutivestoensurethatallemployees,includingconsultants,haveasimilaremploymentrelationshipwiththeTrust.
Third,themanagementboardsofhealthcareorganisationsmustbeabletoleadhealthcareatthelocal level. Executive directors should be selected on agreed criteria and appropriately trained. Non executives should play an active role in the affairs of the organisation.
Finally,thequalityofhealthcareshouldberegulatedthroughbodiessuchastheNationalInstitutefor Clinical Excellence and the Commission for Health Improvement. These bodies should be independentofgovernment.Thereshouldbeanindependentoverarchingbody,theCouncilfortheQualityofHealthcare,tocoordinateandintegratetheactivitiesofthesebodies.ThisCouncilshouldreport both to the Department of Health and to Parliament.
Competenthealthcareprofessionals
Healthcareprofessionalsmusthaverelevantanduptodateskillsandexpertise,andeducationalsystems are fundamentally important in this respect. They must be educated in communication skillsaswellastheprinciplesandorganisationoftheNHS,thedevelopmentofteamwork,sharedlearningacrossprofessionalboundaries,clinicalaudit,andleadership.
Medicalschools,schoolsofnursingandmanagementschoolsshouldbeencouragedtodevelopjointcourses.Futurehealthcareprofessionalsmustworkinmultidisciplinaryteams;sharedlearningshouldthereforebeginassoonaspossible.Acommoncurriculumforthefirstyearofundergraduateeducation of all health care professionals should be developed.
A system of regulation should be in place to ensure that health care professionals acquire and maintainprofessionalcompetence.Regulationincludeseducation,registration,training,continuingprofessionaldevelopment,revalidationanddiscipline.
Medical schools must ensure that the criteria for selecting future doctors include the potential to be versatile,flexibleandsensitive.Theymustalsoensurethathealthcareprofessionalsarenotdrawnfromtoonarrowanacademicandsocioeconomicbase.
ContinuingProfessionalDevelopment(CPD),periodicappraisalandrevalidationmustbecompulsory for all health care professionals. There should be an overarching mechanism to coordinate and align the activities of the various bodies (such as the General Medical Council and theNursingandMidwiferyCouncil)toensurethattheyservepatients’interests.
ThismechanismshouldbeanewindependentCouncilfortheRegulationofHealthcareProfessionals. This Council too should report to the Department of Health and to Parliament. Senior managersintheNHSshouldbesubjecttoCPD,periodicappraisalandrevalidation.

2�
Thereshouldbepositiveincentivestoencourageseniorclinicianstotakeonseniormanagerialroles,includingspecialcategoriesofregistrationwithprofessionalbodiesandtheabilitytomoveoutofandbackintoclinicalpracticeaftersuitableretraining.Thereshouldbeappropriatetrainingforseniorcliniciansbeforetakingontheseroles.
Wheresurgeonsorothercliniciansundertakeaninvasiveclinicalprocedureforthefirsttime,theyshouldbeproperlytrainedanddirectlysupervised,iftheprocedureisalreadyestablished.Inthecaseofanew,untriedinvasiveclinicalproceduretheymustseekpermissionfromthelocalresearchethicscommittee.Patientsareentitledtoknowabouttheexperienceofsurgeonsor other clinicians before giving consent.
Finally,theemployermustcarrytheprimaryresponsibilityfordealingwithpoorperformanceandmisconduct. Professional codes of conduct should be incorporated into health care professionals’ contracts.Itisfortherelevantprofessionalregulatorybodytodecidewhetherthehealthcareprofessional’s registration should be affected.
Thesafetyofcare
The inquiry team noted that about 5% of the 8.5 million patients admitted each year to hospitals inEnglandandWalesexperienceanadverseeventthatmaybepreventablewiththeexerciseofordinarystandardsofcare.Howmanyoftheseeventsleadtodeathisnotknownbutitmaybeashighas25,000peopleayear.
The components of safe care are much more than the actions or competence of health care professionals:theyincludethephysicalenvironment,equipment,workingarrangements,teamworkandgoodcommunication.
TheNHSisstillfailingtolearnfromthethingsthatgowrongandhasnosystemtoputthisright.Thereforeacultureofsafetyinwhichsafetyiseveryone’sconcernmustbecreated.Safetyrequiresconstantvigilance.Giventhaterrorshappen,theymustbeanalysedwithaviewtoanticipateandavoidthem.Acultureofsafetycruciallyrequiresthecreationofanopen,free,nonpunitiveenvironmentinwhichhealthcareprofessionalscanfeelsafetoreportadverseeventsand near misses (sentinel events). The Government’s proposed National Patient Safety Agency shouldbeanindependentagencytowhichcertainsentineleventsarereportedforanalysiswithaviewtodisseminatinglessonsthroughouttheNHS.
The culture of blame is a major barrier to the openness required if sentinel events are to be reported,lessonslearnedandsafetyimproved.Thesystemofclinicalnegligenceispartofthiscultureofblame.Itshouldbeabolishedandreplacedbyeffectivesystemsforidentifying,analysing,learningfromandpreventingerrorsandothersentinelevents.Anexpertgroupshouldconsideralternativestoclinicalnegligence,includinganalternativeadministrativesystemofcompensatingthosewhosufferharmarisingfrommedicalcare.
Incentivesforreportingsentineleventsshouldbeintroduced,wherebyhealthcareprofessionals’contractswouldprovidethattheywouldbeimmunefromdisciplinaryactionfromtheiremployerorprofessionalregulatorybodyiftheyweretoreportasentineleventwithin48hours.Confidentialreporting should be ensured and failure to report should attract possible disciplinary action.
An approach to safety based on designing safer systems and equipment should be encouraged. The NationalPatientSafetyAgencyshouldbringtogetherinterestedpartiestotacklesomeofthemorepersistentcausesofunsafepractices.Finally,anexecutivedirectorontheBoardofManagementshould be responsible for putting into operation the organisation’s strategy and policy on safety and a non executive director should provide leadership to promote a culture of safety.

22 Patient Safety: a comparative analysis of eight Inquiries in six countries
Careofanappropriatestandard
Patients are entitled to care and treatment of an appropriate standard informed by current knowledge.However,untilwellintothe1990s,thenotiondidnotexistthatthereshouldbeexplicitstandardsofcarethatallhealthcareprofessionalsshouldseektomeetandwhichwouldapplytopatientsacrosstheNHS.Itisnowwidelyacceptedthatthisstateofaffairshastochange.Patientsareentitledtoexpectthattheircarewillbeofsuchqualityasisconsonantwithgoodpractice,based on sound evidence. Recent developments give cause for optimism. These include statutory responsibilityofTrustsforthequalityofhealthcare,thedevelopmentofclinicalguidelinesthroughtheNationalInstituteforClinicalExcellence,andthemonitoringofperformancethroughtheCommission for Health Improvement.
Thereremainsinsufficientcoordinationinsettingstandards.Guidelinesappearfromavarietyofbodiesgivingrisetoconfusionanduncertainty.Moreover,thereareweaknessesinmonitoringperformanceinrelationtothesestandards,whetherattheleveloftheTrustornationally.Inparticular there is no mechanism for surveillance to ensure that patterns of poor performance are recognised and addressed.
Forthefuture,standardsforclinicalcaremustbesetbytheNationalInstituteforClinicalExcellence.Indoingso,itmustdrawontheexpertiseparticularlyoftheRoyalColleges.Standardsmustbepatientcentred.Theymustnotbetheproductofindividualprofessionalgroupstalkingtothemselves.Theymustincorporatetheconceptofteamworkandtherespectiveresponsibilitiesofmembersoftheteam.Somestandardsshouldbeobligatory,whereasothersshouldbeachievedover time.
ParentstakingtheirchildrentobetreatedinBristolassumedthatthelevelofcareprovidedwouldbegood,giventhatthecarewouldbeprovidedbyasupra-regionalcentreselectedbytheDepartmentofHealth.Theytrustedthesystem.Fewhadanyideathattherewerenoagreedstandards of care for paediatric cardiac surgery or for any other specialty.
Insummary,theremustbetwodevelopments.First,theremustbeagreedandpublishedstandardsofclinicalcareforhealthcareprofessionalstofollow,sothatpatientsandthepublicknowwhattoexpect.Second,theremustbestandardsforhospitalsasawhole.HospitalsthatdonotmeetthesestandardsshouldnotbeabletoofferserviceswithintheNHS.
Genericstandardsforhealthcareorganisations(licensingandaccreditation)
Theinquiryteamrecommendedwhatittermedgenericstandards.BytheseitmeantstandardsthatdefinetheminimumcapabilitiesbelowwhichorganisationsshouldnotbepermittedtoprovideNHSservices.Thestandardsrelatetosuchmattersasthestateofthebuildingsandofequipment,thequality of leadership and the health care organisation’s policies and procedures for ensuring that care is safe and of good quality.
Healthcareorganisationsmustperiodicallyundergoaprocessofrevalidation.Revalidationwouldmean that the organisation could continue to offer health care services. The Commission for Health Improvementwouldberesponsiblefortheprocessofvalidation.Intimetheprocessofvalidationshouldbeextendedtodiscrete,identifiableserviceswithinahealthcareorganisation.
Monitoringofperformancedependsonaccesstorelevantinformation,butinthepasttherehavebeengreatdifficultiesincollectingit.Therehasalsobeenaseparationbetweenadministrativeandclinicalsystemsthattheinquiryteam’sexpertsdescribedas‘wastefulandanachronistic’.

23
Infuture,themultiplemethodsandsystemsforcollectingdatamustbereduced.Datamustbecollectedasthebyproductofclinicalcare.Atanationallevel,themonitoringofclinicalperformanceshouldbebroughttogetherandcoordinatedbyonebody,anindependentOfficeforMonitoringHealthcarePerformancethatwouldbepartoftheCommissionforHealthImprovement. It could also carry out a surveillance role.
Publicinvolvementthroughempowerment
Thepublicareentitledtoexpectthatmeansexistforthemtobecomeinvolvedintheplanning,organisation and delivery of health care. A patient centred service is one that is designed to address the needs of the particular sectors of the public it exists to serve. Strategic planning at nationallevel,anddecisionsatlocallevelmustinvolvethepublic.
The principles that should inform future policy about involving the public and patients in the NHS includethefollowing:
n Patientsandthepublicareentitledtobeinvolvedwhereverdecisionsaretakenaboutcareinthe NHS
n The involvement of patients and the public must be embedded in the structures of the NHS and permeate all aspects of health care
n The public and patients should have access to relevant information
n Health care professionals must be partners in the process of involving the public
n Theremustbehonestyaboutthescopeofthepublic’sinvolvement,sincesomedecisionscannot be made by the public
n There must be transparency and openness in the procedures for involving the public and patients
n The mechanisms for involvement should be evaluated for their effectiveness
n Thepublicandpatientsshouldhaveaccesstotrainingandfundingtoallowthemfullytoparticipate
n Thepublicshouldberepresentedbyawiderangeofindividualsandgroupsandnotbyparticular patient groups.
TheNHSmusttakeaccountofandrespondtotheinterestsandneedsofthepubliconadailybasis. Patients must be involved in those processes designed to secure the competence of healthcareprofessionals,andparticularlyinthosebodieschargedwithsettingstandardsforeducation,trainingandContinuingProfessionalDevelopment.
The priority for involving the public should be that their interests are embedded into all organisationsandinstitutionsconcernedwithqualityofperformanceintheNHS:inotherwords,thepublicshouldbe‘ontheinside’,ratherthanrepresentedbysomeorganisation‘ontheoutside’.
2.5 Discussion
TherearetwoindisputableaspectsoftheBristolcase.First,thecareprovidedwaspoor.Second,manypeople,bothpowerfulandpowerless,knewthistobethecasebutdidlittleornothingtoresolve the problems.

24 Patient Safety: a comparative analysis of eight Inquiries in six countries
Aswenotedatthestart,itisastorythatishardtobelieve.Thisisnotbecausetheunderlyingproblemswerefoundtobeunique.Indeed,weseemtobeabletofindthemwheneverwewanttodo so. As Siddins (2003) puts it in the context of the similar inquiry of obstetric and gynaecological servicesataPerthhospital,“…suchproblemsarenotuniqueto(thathospital).Irrespectiveofthespecialty,sevenmilliondollarsofcarefulanalysisatanyAustraliantertiaryhospitalwouldhaveyieldedthesameconclusions.”Thisviewhasbeenexpressedabouthospitalsinothercountries.Forexample,Maisonneuve,Matillon,MillatandMarescaux(2004)madeasimilarclaimaboutthesituation in France.
ThemainreasonforincredulityabouttheBristolstorymaybetheevidenceofthedegreetowhichtheproblemsweredemonstrablywidespread.TheDepartmentofHealth’sInquiryproducedalonglistofsenior,powerful,andknowledgeablehealthprofessionalswhowouldhavedonesomethinginaworldfullofobjectiveandvaluefreescientists.Therewasatleastgoodreasontoaskiftheremightbeaproblemworthyofinvestigation.Formanyofthehealthprofessionals,theevidenceshouldhavebeenseentobeoverwhelming.Itisnotthatwedoubtweareallprisonersofcircumstancestosomedegree,butthatwefindithardtohavetoacceptthatthisistrue.
The main conclusions of the Department of Health’s Inquiry are hardly disputable. The problems weredeeprootedandlargelyconcernedorganisationalcultures,andclinicalprofessionalculturesinparticular.Manyauthorshavesubscribedtothisview.Forexample,VanDerWeyden(1998)arguedthatitwaslessamatterofhumanimperfectionthanofsystemicfailure.
Hindle(1998)arguedthat“…evaluationbasedonevidencemustplayapart,butitisinsufficientbyitself.DrBolsinwasinvolvedinthedevelopmentoftoolsforthemeasurementofriskadjustedoutcomesincardiacsurgery,andtheyservedtoconfirmhisconcernsaboutclinicalpracticeatBristol.However,hisscientificanalysesfailedtopersuadeseniormanagerstotakeaction.”
The large quantity of literature describing lessons to be learned from Bristol might lead one to believetheproblemswillberapidlysolved.However,itcouldbearguedthatthe‘clubs’arealreadyrebuildingtheirfirewalls.Treasure(1998),writingintheBritishMedicalJournal,notedthattheRoyalCollege of Surgeons of England and the Society of Cardiothoracic Surgeons established a ’rapid response group’ so that a member of the council of the college and a senior cardiac surgeon can be onsitewithin48 hours,tolistenandadviseonaction.“Thisisanattemptbythe profession to protect patients from continuing poor performance and also to safeguard surgeons from inappropriate fault finding(since cardiacsurgeonsnowfeelverymuchunderscrutinyandvulnerable in a climate of criticismandblame).”Theemphasismightbeonthelatterpurpose.Hesaidthat,“…ifwedonotmonitor ourselves effectivelythereislittledoubtthatitwillbeimposedupon us.” He expressed the hopethiswouldbesufficientto“…allayanxietiesabouttheprofessionsupposedlymonitoring itself.”
He noted that cardiac surgeons established bases for performance assessment long before most otherspecialties.However,whentheprocesseswereestablished,therewas“…atacitassumptionthat the patients and surgeons in the dataset wereanonymousandwouldremainso.”Theuseofthedatabase“…toassessone’sownpracticewasamatterofhonour andpersonalreflection.”However,changesweretakingplacewherebycodingwouldallowunsatisfactoryresultstobetracedto the surgeon and poor performance investigated. Theanonymityofferedbycodingisnotional“…and may be the last vestige ofabeliefinconfidentialityforsurgicalresultsthatforyears washeldtobe sacrosanct.”

25
There is also a sense of pessimism in the anonymous article published in the British Medical Journal(Anon �998) shortly after the results of the GMC became public. The author reported witnessingsimilarlydisturbingpatternsofpoorcare,anddescribedtheirfrustrationandregretatnot feeling able to intervene.
Twodistinguishedclinicianswereinvitedtocommentontheanonymousauthor’squestionastowhatshouldhavebeendone.Oneofthemsaidtheappropriateactionwasclear:thejuniordoctor should use an existing mechanism described in Department of Health guidelines as predisciplinaryprocedures.However,thiscommentatoradmittedthatthejuniordoctor,likemanydoctors,maynothaveknownabouttheexistence ofthismechanism.Strangely,thisfirstcommentator focused on clinical incompetence arising from impairment due to age or illness.
The second commentator clearly accepted that poor clinical practice is not restricted to those whowillsoondieorbesenttopension.Henotedthatafocusontheindividualisillogicalanyway,since“…mostavoidableerrorsinhealthcarearenotdueto the incompetence of individuals.”
Itwasalsopointlesstoasserttheauthor’sdutytoprotectpatientsbecausethiswouldrequireanunusualdegreeofheroism.“Weshouldapplaudheroes,andhopethat theyareamongus,but to base our hope of remedy in ordinary systems on the existence of extraordinary courage is insufficient.”
Rather,thefirstessentialsteptoimprovedpatientsafetyisdisclosureofrisk.Hepresentedtheanalogyoftheairlineindustry,inwhichtheprevailingcultureisthatjuniorpilotsaretrainedtospeakup.Hissuperiorswouldhavebothpraisedhimfordoing soandtakenhisinformationintoa sophisticated and respectful system of investigation and remedy.
TheBristolinquiriesstressedonepointanditcannotbeignored.Thereweresystemsproblems,and systems problems require systems solutions. This surely discounts any act that applies toselectedindividuals(suchascompulsoryretirement).Lessobvious,butsurelyequallyvalid,itdiscountsanypossibilitythatclinicians,howeverwellrepresentedtheymightbebytheirprofessionalsocieties,arecapableofcuringthemselves.
2.6 Footnotes
2.6.1 DrStevenBolsin’sperspectiveonBristol
Asnotedearlier,ananaesthetistwhohadbeenworkingatBRI,DrStevenBolsin,formallycomplainedtotheGMCconcerningtheconductoftwocardiacsurgeons(DrWisheartandDrDhasmana),andoftheChiefExecutiveoftheTrust(DrRoylance).HiscomplaintswereonefactorthatledtotheGMC’sInquiryin1998.However,hisinvolvementwentbackmuchearlier,as he has explained in several published papers.
One of the more interesting and accessible is that published by the Medical Journal of Australia (Bolsin1998).DrBolsindescribedhow,asearlyas1987,therewastalkbehindcloseddoorsintheUKDepartmentofHealthaboutworryingresultsofpaediatriccardiacsurgeryattheBRI.
In1988,DrBolsinbeganworkthere.Hehadnotheardthewhispers,butsoonbecameconcernedandbegantocompiledata.DrBolsinnotedthelongsurgerytimesoverall,andthelongdurationoftheperiodduringwhichtheheartwasoffline(andhencedeprivedofoxygen).Hesuspectedthiscouldbeassociatedwithhigherdeathratesandinjuries(likebraindamage).
26 Patient Safety: a comparative analysis of eight Inquiries in six countries
In1990,hebeganaskingquestionsatinternalclinicalteammeetings,butwastoldthathisexpressionsofconcern“…wereneitherhelpfulorconstructive”.HethereforewrotetoseniormanagementattheBRI,statinghisviewthatsomethingwaswrong.
EventsduringthisperiodareconfirmedinthereportoftheDepartmentofHealth’sinquiryteam.Theyreportedthat,inmid1990,DrBolsin“…spokeofhisconcernstoDrBrianWilliams,ChairoftheDivisionofAnaesthesiaattheBRI.DrWilliamsstatedthatDrBolsinhadnodataatthetime.InAugust1990,DrBolsinwrotetoDrRoylanceaboutwhatheconsideredtobeamisleadingstatementintheappendixtotheapplicationforTruststatussubmittedbytheUBHT.Inhisletter,healsoreferredtomortalityforopen-heartsurgeryforunder-onesas“…oneofthehighestinthecountry,andtheproblemshouldbeaddressed”.Hesubsequentlytoldtheinquiryteamthatheexpected this letter to be treated as raising a concern and that he expected a response.
Theinquiryteamreportedthatseveralotherpeoplewereawareofthecontentsoftheletter.OnewasDrTrevorThomas,ChairoftheMedicalAuditCommitteeatUBHT,whohadadvisedDrBolsinon the drafting of this letter. Inter alia,hesuggestedthatDrBolsinshouldsendacopyofthelettertoMrGeoffreyMortimer,thenChairoftheHealthAuthority.AcopywasalsosenttoMrChristopherDean Hart as Chair of the Hospital Medical Committee at the BRI. Mr Hart later told the inquiry team thathesawtheletterasconcernedwiththeapplicationforTruststatusratherthanacomplaintabout poor clinical practice. Dr Roylance also told the inquiry team much the same story: that he sawtheletterasbeingaboutTruststatus,andthathetelephonedDrBolsintorespondonthatissue. Dr Roylance said that he did not see the letter as requiring an investigation of open-heart paediatric cardiac surgery.
Manyotherseniordoctorsbecameawareoftheclaimsataboutthistime.Forexample,inmid1991therewasameetingbetweenthecardiacanaesthetistsatUBHT,theClinicalDirectoroftheDirectorateofAnaesthesia,andthePresidentoftheAssociationofAnaesthetistsofGreatBritainandIreland(DrPeterBaskett)atwhichDrBolsin’sconcernswerediscussed.Atthismeeting,DrBaskettsaidthatDrBolsinshouldnotbethevehicleforcriticismofthePCSservice,andshould‘keephisheaddown’.
On28July1991anauditmeetingwasheldjointlybetweenthecardiologists,cardiacsurgeonsandanaesthetists.DrBolsindraftedminutes,referringtoaproblemwithmortalitywhichheexpressedashavingbeen“…thoughttobereachingcrisisproportions”,basedonthedifferencesbetweenthefiguresintheAnnualReportsandthenationalfigures.DrBolsinthoughthewasreflectingwhattheAuditGrouptoldhim,buthewassubsequentlytoldafterproducingtheminutesthattheywerenotrepresentativeandhewasnottoproducethemeveragain.DrBolsinwastoldbyDrWisheartthat“…theseminuteswillnotbecirculated,thisisnothowwedothings.Idonotwantyoukeepingminutes again.”
ThusaccordingtoDrBolsin’saccount(whichwasconfirmedbytheInquiry),nothinghappenedeventhoughhisclaimswouldsurelyhavebeenofconcerntomostlaypeopleandhadbeenseenbyseveralseniorofficialswithclearresponsibilitiesforpatientcare.Thesurgerythereforecontinuedasbefore.
Indeed,therewasgrowingconcernaboutthesituationatDrBristolinthecommunityatlarge.Forexample,in1992thesatiricalmagazine‘Private Eye’ publishedsixarticles(14February,27March,8May,3July,9Octoberand20November)criticisingthePCSservicesattheBRI.Thearticlesin
‘Private Eye’ wereraisedinformallyatameetingoftheTrustBoardofManagementbuttreatedasnomorethanmaliciousgossip.Norecordofthediscussionwasmadeintheminutes.Incidentally,theauthorofthearticleswassubsequentlyfoundtobeageneralpractitioner.Amongotherswith

27
whomDrBolsindiscussedhisdataatthattimewereseniordoctorsintheUniversityofBristol(includingtheDeanoftheFacultyofMedicine),atvariousothertertiaryhospitalsandmedicalfaculties,andattheDepartmentofHealth.
DrBolsintriedtoreducehisinvolvementinpaediatriccardiacsurgery.However,hecontinuedtocollectdata,andpresentedadetailedanalysistotheBristolRoyalInfirmary’sseniormanagementin1993.Hisdatasuggestedchildrenwerethreetimesmorelikelytodiethanthenationalaverage,andonesurgeonhad20timeshighermortalityratesforsomeprocedures.
ThisperiodintheBristolstorywasalsoreportedbytheDepartmentofHealth’sinquiryteam.They noted that Dr Bolsin began to gather data about the PCS service in �989. In �99� he showedthemtoProfessorPrys-Roberts,ProfessorofAnaesthesiaattheBristolUniversityMedical School (and later President of the Royal College of Anaesthetists �994-�997). Professor Prys-Robertsadvisedhimtocollectmoredatabeforereachinganyview.Inthesummerof1991DrBolsincirculatedminutesofameetingbetweentheanaesthetists,thesurgeonsandthecardiologists,whichincludedreferencetoanauditoftheoutcomesinchildrenundergoingPCS.
Laterthatsameyear,DrBolsinwashelpedbyaseniorlecturer(DrBlack)inanaesthesiafromtheUniversityofBristolandtheybegantocompileandcollatedatainamorerigorousway.Inearly1992,DrBolsinagainsawProfessorPrys-Robertswithhandwrittendata.Hewasadvisedtogetfurtherdatathatcouldthenbesharedwithothers.DrBolsinthenworkedwithDrBlacktoproducedatawhichwereshowntocolleaguesintheDepartmentofAnaesthesiainthespringof�993 in the form of a report titled ‘Analysis of Paediatric Cardiac Mortality Data from UBHT 1990–92’. DrBolsinsubsequentlyshowedhisdatatoaneverwideninggroup,butnottothesurgeonswhosepracticewasmostinquestion–DrWisheartandDrDhasmana.
Stillnothingwasdone,andthereforeDrBolsinapproachedtheDepartmentofHealth.ThisledtoaninformalagreementinDecember1994thatsomeoftheriskyprocedureswouldnotbeperformedpendingfurtherinvestigations.However,DrBolsindiscoveredthatoneoftheseprocedureshadbeenscheduledanyway,onan18montholdchildcalledJoshuaLoveday.Heurgentlybegantotalkwithanyonewhowouldlistenabouthavingitmovedtoanotherhospital.TheDepartmentofHealthtoldtheHospital’sChiefExecutivetodojustthis,butherefused.Onthenightprecedingtheoperation,therewasameetingofanaesthetistsandsurgeonsatwhichDrBolsinarguedtheoperationshouldnotproceed.Hewasinaminorityofone,andthefollowingdaythechilddiedontheoperatingroomtable.
DrBolsinandhiswifewereveryupset.Theyhadthoughtofgoingtotalkwiththechild’sparentsabouttherisks(eventhoughthismightrepresentprofessionalmisconduct),buthadnotdoneso,andfeltguilty.Inshort,hehadfounditdifficulttobreakthelongstandingtraditionthatoneconsultant does not interfere in the clinical judgement of another.
ThiseventwasrecountedbytheDepartmentofHealth’sinquiryteam.TheysaidthataclinicalmeetingwasheldshortlybeforethescheduledoperationonJoshuaatwhichallseniormedicalstaffwerepresent.Thepurposeofthemeetingwastodiscusswhethertoproceedwiththeoperation,anditwasdecidedatthestartthatonlyclinicalfactorsshouldbeconsidered.Allthosepresentagreedthattherewerenoclinicalreasonsfornotproceedingwiththeoperation.Whilenotobjectingonclinicalgrounds,DrBolsindissentedonthebasisofwhatDrWisheartrememberedas‘institutionalreasons’with‘politicalconsequences’.DrWisheartwasawarethatDrRoylancewasconsideringtheinstitutionofanindependentreviewofpaediatriccardiacsurgery–butDrWisheartdidnotrevealthistoothers.Thustherewasnosenseofopennessinpursuit of the truth. One of the cardiac surgeons at the BRI explained the style of this meeting:

28 Patient Safety: a comparative analysis of eight Inquiries in six countries
therewasaculture“…ofexplainingorjustifying...mediocreorpoorresultsonthebasisofcaseseverityratherthandirectingattentiontoproducingbetterresults”.Ifproblemswereadmittedatall,thenitwasinaccordancewiththeargumentthat“…actuallytheresultsarenotverygoodbutitisbecausetheyarebadpatients...andwearedoingourbest”.
Inearly1995theDepartmentofHealthfinallydidwhatitshouldhavedoneatleasteightyearspreviously:requestedaninquirybyexternalexperts.Theappointedexperts,DrStuartHunterandProfessorMarcdeLeval,submittedareportthatwashighlycriticalindraft,buttheywerepressuredbytheBristolRoyalInfirmaryChiefExecutivetoeliminatethemorenegativecommentsbeforeitwasformallypresentedtoUBHT.However,itwasstillsignificantlycritical.TheDepartmentofHealth’sinquiryteamsubsequentlyrevieweditcarefully,andquotedtheauthorsassayingthat“…itisnotpossibletodeterminethecauseofthesepoorresults(oftheneonatalArterialSwitchoperation).Toblamesurgicalskillasthesolereasonwouldbeshortsighted.Itismostlikelyamultifactorialandmultidisciplinaryproblem.”Ifnothingelse,itwasamajorstimulustoaction,becausesomeofitsconclusionsfoundtheirwayintothemassmedia,andthestoryfinallybrokeonthe front page of the Daily Telegraph in April �995.
DrBolsinreceivedfewkindwordsasaresult.Hehad‘letthesidedown’and‘broughtmedicineintodisrepute’.BRImanagersthreatenedhimwithdismissalandchangedhisdutiestohisdisadvantage.ThiscontributedtohisdecisiontomovetoTheGeelongHospitalinVictoriainFebruary1996.Shortlyafterwards,hewrotetotheGMC,askingthataninquirybeconducted.Thismightseemasensibleandobviousactiontotake,giventhattheGMCisdefinedbylegislationtohaveprimaryresponsibilityformaintainingprofessionalstandards.However,therealitybearslittlerelationtologic.DrBolsinnotedhisbeliefthatheistheonlydoctorevertohavetakensuchaction–tohavebeenadoctorwhomadeaformalcomplaintaboutanotherdoctor.Asnotedabove,theGMCInquirycompleteditsinvestigationinJune1998,findingthreepaediatriccardiacsurgeonsguiltyofseriousprofessional misconduct.
Incidentally,Klein(1998)arguedthattheGMC’sactionswerewelcome.“Iftherewereany doubts abouttheGMC’scommitmenttoitscontractwiththepublic, about its determination to demonstrate the profession’s collective acceptanceofresponsibilityformaintainingcompetenceinpractice, they havebeendispelled.Andthatshouldsendapowerfulmessage both to the profession itself and to thepublic.”ThisseemstoundervaluethesignificanceofDrBolsin’sclaimthathewasthefirstevertoseekitssupport.
DrBolsinarguedthathedidhisbest“…tostandupforthebestinterestsofthepatientandforthatIsufferedatthehandsofaprofessionthatlocallywasnotpreparedtostopchildrenfromdyingunnecessarilyinthepracticeofpowerfulmen”.TheDepartmentofHealth’sinquiryteamexpressedasimilarview:thathedidwhatwasgenerallytherightthingtodo,althoughwithhindsighthemighthavebeenmoreeffectiveinafewcircumstances.Thatsaidtheinquiryteamacceptedhehadbeenbraveandethicalinanincrediblydifficultsituation.“ThedifficultiesheencounteredrevealboththeterritorialloyaltiesandboundarieswithinthecultureofmedicineandoftheNHS,andalsotherealitiesofpowerandinfluence.”
29
2.6.2 Thefinalwordsofsomeoftheothermainplayers
Theinquiryteaminitsreport,gaveselectedquotesfromthetestimoniesofsomeofthemainplayers.Thefollowingseemtobeofparticularrelevance.
Present Chief Executive of the United Bristol Health care Trust.
“OnbehalfoftheTrust,Ishouldliketosaysorrytothechildrenandfamiliesofthosewhoused the paediatric cardiac services in Bristol in the past. It is clear to me that a substantial numberofparentsandchildrendidnotreceivethestandardofcaretheywereentitledtoexpect.Ihaveseenatfirsthandhowpainfulanddistressingithasbeenformanyparentstorememberandreflectagainontheeventsofthepast.Iwouldliketopaytributetotheirbravery and composure under the most extreme circumstances.”
Counsel for the Department of Health.
“TheDepartmentofHealthacceptsthatitisresponsibleandisaccountableforanyfailingsofthesystemsthatwereinplaceduringtheperiodcoveredbytheInquiry.UltimateresponsibilityrestswiththeDepartmentofHealthandtheSecretaryofState.
ItnowseemsclearthattherewasconfusionandthereforesystemicfailingswithregardtothewayinwhichtheSRSAGdealtwiththespecialtyofneonatalinfantcardiacsurgery.Thediligenceoftheinquiryteamhasuncoveredthisconfusionandthesystemicfailingthatwaspreviouslynotknowntothedepartment.Alltheseareacceptedandareacauseofgreatregret.”
One of the censured consultant cardiac surgeons.
“Allthesethingshaveruinedmeprofessionally,financially,myfamilylifehasgoneandIhavelostconfidenceinmyself.ThisisthefirsttimeinthelasttwoyearsthatIhavebeenabletospeaktoanyaudienceforthreedays.
AllthiscouragehasreallycomefromsupportthatIhadfrommycloserelatives,andtherearestillpatientsandparentswhohavecontinuedtosupportme,makingmefeelthatIamstilltrustedinsomecorners.Again,Iemphasise,whateversufferingIhavegonethrough,andIamgoingthrough,isnomatchtothesufferingthatyouhadwiththelossofyourchild,andIwishIcouldturntheclockback.Icannotsayanymore.”
Another of the censured consultant cardiac surgeons.
“Iwishthiseveningtorepeatandtoofferagainmydeepestregretandsympathytoallparentswhosechildrendiedatthetimeoforaftertheiroperation.Insayingthis,mysympathy and regret go to parents and families on all sides of this particular debate. The lowestpointofasurgeon’slifeiswhenachilddiesunderhisorhercare.”
2.7 Referencesandselectedbibliography
Alaszewski,A.(2002).TheImpactoftheBristolRoyalInfirmaryDisasterandInquiryonPublicServicesintheUK.Journal of Interprofessional Care,16(4):371-8.
Anon (�998). Five Times: Coincidence or Sometimes More Serious. British Medical Journal,6(3�6): 7�46.
Bolsin,S.(1998).ProfessionalMisconduct:theBristolCase.Medical Journal of Australia,�69(7): 369–72.

30 Patient Safety: a comparative analysis of eight Inquiries in six countries
Bolsin,S.(2002).MortalityandVolumeofCasesinPaediatricCardiacSurgery:PaperConfirmsPoor Quality of Paediatric Heart Surgery at Bristol during �99�-5. British Medical Journal,324(7345): �095-6.
Casey,A.(1999).WideningRipplesfromBristol.Paediatric Nursing,11(8):3.
Department of Health (�998). A First Class Service: Quality in the New NHS. London: Department of Health.
Department of Health (200�). The Report of the Public Inquiry into Children’s Heart Surgery at the Bristol Royal Infirmary 1984-1995: Learning from Bristol.London:TheStationaryOffice.
Dickson,N.(2001).LongHaulbeforeNHSisShipshapeafterBristol.Nursing Times,97(30):22.
Dyer,C.(2001).BristolInquiryCondemnsHospital’s’ClubCulture’.British Medical Journal,323(7306): �8�.
Faunce,T.A.andBolsin,S.N.(2004).ThreeAustralianWhistleblowingSagas:LessonsforInternaland External Regulation. Medical Journal of Australia, �8�(�): 44-7.
Hindle,D.(1998).TrustingtheSurgeon:ATornadofromBristol.Australian Health Review,21(4):4-7.
Joffe,H.S.(1995).HospitalBannedfromDoingNeonatalHeartOperations.British Medical Journal,3�0(6988): ��95.
Klein,R.(1998). Competence,ProfessionalSelf-Regulation,andthePublicInterest.British Medical Journal,316(6June):1740-42.
Leatherman,S.(2003).The Quest for Quality in the NHS. London:NuffieldTrust.
Maisonneuve,H.,Matillon,Y.,Millat,B.andMarescaux,J.(2004).LessonsLearnedfromBristol.Annales de Chirurgie, �29(2): ��4-8.
Mayor,S.(2001).MortalityforPaediatricCardiacSurgeryatBristolwasTwicethatatOtherCentres.British Medical Journal,323(7305):125.
Ramsay,S.(1999).UK“Bristolcase”InquiryFormallyOpened.Lancet,353(9157):987.
Savulescu,J.(2002).BeyondBristol:TakingResponsibility.Journal of Medical Ethics, 28(5): 28�-2.
Siddins,M.(2003).CommentaryontheKingEdwardInquiry:LessonsweFailtoLearn.Australian Health Review, 26(�): 28–9.
Swan,N.(1997).MedicalScandalatOneoftheMostRespectedUKHospitals.The Health Report,RadioNationalTranscript,May12:1–11.Availableat:http://www.abc.net.au/rn/talks/8.30/helthrpt/stories/s10683.htmAccessedon3March,2006.
Swan,N.(1997).ASevereCaseofSurgicalMisconduct.The Health Report. Radio National Transcript,May12:1–11.Availableat:http://www.abc.net.au/rn/talks/8.30/helthrpt/hstories/hr120597.htmAccessedon3March,2006.
Tingle,J.(2002).GovernmentResponsetoBristolInquiry:IsittooAmbitious?British Journal of Nursing,11(3):150.
Treasure,T.(1998).LessonsfromtheBristolCase.Moreopenness-onRisksandonIndividualSurgeons’ Performance. British Medical Journal,316(7146):1685-6.
Treasure,T.(2000).ImprovingSurgicalCare:LookingBeyondIndividualCompetence.Quality in Health Care,9(1):2-3.

3�
UKDepartmentofHealth(2002).LearningfromBristol:TheDHResponsetotheReportofthePublicInquiryintoChildren’sHeartSurgeryattheBristolRoyalInfirmary1984-1995.DepartmentofHealth:Crown.
VanDerWeyden,M.(1998).TheBristolCase,theMedicalProfessionandTrust.Medical Journal of Australia,169(7):352–3.
3 CampbelltownandCamden,Australia
Theprocessofthisinvestigationwasprolonged,mainlybecauseoftheallegedslowandtechnicallyflawedfirstattemptoftheexternalinvestigationmadebytheHealthCareComplaintsCommission(HCCC)thatbeganinNovember2002andwasreplacedbyaSpecialCommissionofInquiryinDecember2003.TheCommissionreleasedaninterimreportinMarch2004toredresssomeofthewidespreadpublicconcern.Itcorrectedmostoftheflawsbutcontainedincompletefindings.ThefinalreportwasreleasedinJuly2004,butmostoftheallegationsagainstindividualclinicianswerereferredforinvestigationbyotherbodies,suchastheNSWMedicalCouncil.
3.1 Context
TheCampbelltownandCamdenHospitalsarethemainhealthcareorganisationsintheMacarthur Health Service. This in turn is part of the organisation constituted by (the then) South WesternSydneyAreaHealthService,oneoftheseventeenauthoritiestowhichsignificantresourceallocationandcareprovisionresponsibilitieswerethendelegatedbytheNSWDepartment of Health.
RumoursofsignificantdiscontentregardingthequalityofcareatCampbelltownandCamdenbegantocirculatewithintheNSWhealthsectorasearlyas1998,andwererampantby2001.However,itwasnotuntillate2002thattherumourswereofficiallyrecognisedandbecamefrontpagenews.Atthattime,agroupofnursesformallypresenteditsconcernstotheDepartmentandthefirstoftwomajorandhighprofileinquirieswasinitiated.
Theallegationsresultedinwidespreadconcerninthecommunityatlarge,andinNewSouthWalesinparticular.Thisisreflectedinthecommentsexpressedincallstoradiotalkshows,letterstotheeditorinnewspapers,andcontributionstovariousinternetchatsitesthathavecontinuedfor18months.ThefollowingareexamplestakenfromtheSydneyMorningHerald’sinternetfeedbacksiteshortlyafterthecontentsofthefirstformalInquirywerereleased.
Nurses are at fault
“Nursesarenotprofessionalsbutmereworkers.Theirattitudetowardsdoctorsisappallingwithaconstantpowerstruggleabouttaskstobedonewhenallthedoctorwantsisforthepatienttogetbetter.Nursesrarelyworkovertimewhereasdoctorscanwork36-hourshifts.”
Bureaucrats are at fault
“Thesystemisrotten.Thosewhoworkatthecoalfaceknowit.Thebureaucratswholookonfromthecomfortoftheirair-conditionedofficeswillneveracknowledgeit.”
“Theadministratorswhoknownothingabout“health”or“medicine”causetheproblems.More beds and more quality nursing staff are needed.”

32 Patient Safety: a comparative analysis of eight Inquiries in six countries
Lawyers are at fault
“Thelawyershavebeenmakinganabsolutepacketwiththeirlegalactionsagainstdoctorswhoworkunbelievablylonghourstosavepeople’slives.”
Doctors are at fault
“Ihaveexperiencedthemostdisgustingtreatmentandwitnessedthemostappallingbehaviourby clinicians in recent years.”
“Whywasitthatonlynurseshadthestrengthandresolvetoblowthewhistle?Wherewerethedoctors?Theyhavefailedtheirdutyofcarebynotreportingsystemfailures.”
Politicians are at fault
“Weshouldn’tblamethedoctorsandnurses.They’redoingtheirbesttoworkwithverylimitedresourceswhileworkingverylonghours.Theblameshouldbeaimedtowardthepoliticians.”
“Themainproblemisnotthefederalgovernmentbutthestategovernment.Whyhavetwogovernmentlevelsinvolved,thusgivingthemtheopportunitytoblameeachother?”
“Itisnotsurprisingthegovernmentdidn’tknowwhatwashappeninginSaddam’sIraq,giventheyknownothingaboutwhatishappeninginourhospitals”
“Mostpatientswhowaitinemergencyforhoursbeforetreatmentoradmissiontoahospitalbedthinktheircaseistheexception.Thereisnoaccountabilityforpatientcarebyhospitalboardsandgovernmentswhotrytofoolthepublicintothinkingthatproblemsareduetotheaccuseddoctors.”
Nurses are the heroes
“Whywerethenurseswhobecamewhistleblowerscrucifiedbythehealthcaresector?Whydidn’tthehospitalactuallysupportthesepluckyindividuals?Iftheyhadobeyedinstructions,wewouldnothavehadaninquiryintothelevelofcareinourhospitals.”
“Congratulationsforallwhobroughtthislatestscandaltothepublic’sattention.Youdeservetobe nominated for Australians of the year!”
Thesedonotrepresentarepresentativesample,ofcourse.Noristhereanyguaranteethatthecommentsarewellinformedorimpartial.Theyarepresentedheremerelytoindicatethedegreeofconcerninthecommunityatlarge,andtheextenttowhichviewshavebeenpolarised.
Theeventsweresubjecttoextensivepublicexposureintheprofessionalmedia.Forexample,itwasclaimedbyoneofthenurseswhobroughttheformalcomplaintsthattheprocessofinvestigationadoptedbytheHealthCareComplaintsCommission(seebelow)waspoorlyplanned,andfailedtoaddressmanyoftheallegations.ShearguedthattheCommission“…seemedreluctanttoinvestigateanythingthatmanagementweredirectlyresponsiblefor”(Stateline,ABCTelevision,14November 2003).
Onthesametelevisionprogram,aDemocrats’memberofparliamentarguedthat,regardlessoftheveracityoftheincidentsunderinvestigation,thereweredeeprootedproblemsofqualityofcare.“Idon’tthinkthere’severbeenareallygoodqualitycontrolprogramthroughoutthehealthsystem.Asresourcesgettight(andobviouslyinhospitalsthatarehardertostaff)theproblemsareworse.”Healsocriticisedthe’adversarial’medicalindemnitysystemthatcreatesincentivestohidemistakes.

33
“Thatmeansyouneverlearnfromthemandyoukeeponmakingthesamemistake.”Alsointhesameprogram,theChairofTheHealthCareQualityTaskforcearguedthattheproblemswereexacerbatedbyaspectsofmedicaleducation,whichhave“…producedaculturethatdoesnotallowforerror,thatdoctorsarenotsupposedtomakemistakes.”
Manyassociatedissueswereraisedwhilethefirstandthesecondinquirieswereunderwaythatincreased the degree of political debate and added confusion to the central issue of questionable clinicalpractice.Forexample,improprietywasclaimedwithregardtothereappointmenttoaseniorpositioninNSWHealthoftheCEOofMacarthurAreaHealthServiceaftershewasapparently pressed to resign because of the incidents that led to the Inquiry.
AlsotherewereseveralactionstakenbytheMinisterthatmighthavebeenconsideredtoprejudice the inquiry process. Inter alia,hemadewhatweretermedsweepingmanagement,supervisoryandrecruitmentchangesatMacarthurAreaHealthService.Whenquestioned,theMinistersaid“…therehadtobeachangeinthemanagementculture.Therehadtobeachangeinmanagementapproach,andtogetthat,youhavetogetachangeintheteam.”Inshort,whileattemptswerebeingmadetoconductanopenandfairconsiderationoftheallegations,manypeoplewereconfusedandothersseemedtobeprejudgingthefindings.
Thehistoryofthecomplaints
Thehistorycomprisesfourmainphasestodate,eachofwhichisdescribedinturnbelow.First,therewasaperiodofdiscontentlastingatleastfouryears,duringwhichinformalandpartlyformalcomplaintsweremade,mainlybynurses,aboutmedicalcareattheCampbelltownandCamdenHospitals.Second,therewasashortperiodinNovember2002duringwhichtheMinister for Health and the Department of Health heard formal complaints and directed the Health Care Complaints Commission (HCCC) to investigate them.
Third,therewastheperiodofinvestigationbytheHCCCthatlastedfromNovember2002toDecember2003.Severalreportswereissuedduringtheperiodthatraisedasignificantdegreeof concern about the effectiveness of this investigation.
Finally,therewastheSpecialCommissionofInquirythatwasappointedbytheNSWgovernment on 26 December 2003. The Commissioner observed during a public hearing on26March2004thattheSpecialCommissionofInquirywas“…appointedbyreasonofdissatisfactionwiththeoutcomeofcomplaintsprocessintheHealthCareComplaintsCommission.”Aninterimreportwasissuedon31March2004,andafinalreporton30July,2004,fromwhichmostofthefollowinghasbeentaken.
Thenurses’complaintsarefrustrated
Thenursesclaimedtheymadeavarietyofattemptstoencourageactionwithregardtopoorcarefor three or four years before they delivered their formal complaints to the Department of Health. Theseclaimswerecontested.However,thereisgoodreasontobelieveatleastsomeofthenurses’ claims may be substantiated.
Inshort,itwasadvancedthatmanynurses,andnotonlythosewhobroughttheformalcomplaints,madearangeofinformalandinformalcomplaintsbutnoseriouseffortsweremadetoaddressthem.Oneofthenursesadvancedsheandothernurseswerecalled‘troublemakers’bymanagers,andwereencouragedtoleave.Othernursesclaimedtheywereharassed,intimidatedandostracisedwhentheytriedtoalertauthoritiestoentrenchedproblems(Stateline,ABCTelevision,14November2003).Otherassertionsincludedthedestructionofrecords

34 Patient Safety: a comparative analysis of eight Inquiries in six countries
by hospital administrators and managers in Macarthur Health Service – both medical records in whichtherewasevidenceofpoorcareandreportsofincidentsmadebynursesandothers.Oneofthenursesclaimedthatsheandotherswhomadeadverseincidentreportsweregivenfinancialincentivestoencouragethemtoleave,afterwhichdocumentsweredestroyed.
TheMinistertakesaction
TheissuefirstcametotheformalnoticeoftheDepartmentofHealthon5November2002.Atthattime,fournursesandasolicitormetwiththethenMinisterforHealth.EachofthenurseshadbeenemployedatorwasonleavefromCampbelltownorCamdenHospitals.Theymadearangeofallegationsofmismanagement,patientneglectandafailureofmanagementtoaddresstheirconcerns.OnthatdaytheMinisteraskedtheDirector-GeneraloftheDepartmentofHealthtoinvestigatetheallegationsimmediatelyandinterviewthenursesasamatterofurgency.HeinturnaskedtheDirectorofAuditintheDepartmentofHealthtomakeaninitialinvestigation
On12November2002,theDirectorofAuditreportedtotheDirector-General.Sheprovidedasummaryoverviewofherfindings,whichhadbeenmadefollowinginterviewswithmostofthenurseswhoattendedthemeetingwiththeMinisteraswellastwoothernurses.
On18November2002,theDirector-GeneralreferredtheallegationsmadebythenursestotheHCCCforinvestigation.TheHCCCwasprovidedwithasummaryoftheinitialallegationsmadeandthepreliminaryfindingsoftheDirectorofAudit.Some18filesoffurthermaterialswereprovidedon21November2002,togetherwithastatutorydeclarationverifyingthecomplaintbytheDirector-General.
TheHealthCareComplaintsCommissioninvestigationisconducted
TheHCCCappearstohaveinterpretedthecomplainttobeagainstMacarthurHealthService,ratherthanagainstindividualhealthcareprofessionals.Thiswassubsequentlyarguedtohavebeenamistake,aswillbeseenbelow.Itproducedan‘InterimPhase1’reportattheendofJanuary2003.Thisfollowedinterviewswithsomebutnotallofthenursesandsomemanagersandotherstaffinthe Macarthur Health Service.
AcopyofitsreportwasprovidedtotheDirector-GeneraloftheDepartmentofHealth,theChiefExecutiveofSouthWesternSydneyAreaHealthServiceandtheMinisterforHealth.TheletteraccompanyingthatreporttotheDirector-Generalstated“…therehavebeennosubstantiatedallegationsofsignificantdeparturesfromStateornationalstandardsinhealthcare”.Thereportnotedthatitspurposewastoupdatethepartiestothecomplaintabouttheprogressoftheinvestigation,butitcontainedsomeconclusions.
Anotherreportwasreleased18August2003(eightmonthslater)thatwastitled“PreliminaryInvestigationReport”.ItwasprovidedonlytoSouthWesternSydneyAreaHealthServiceforthestatedpurposeofprovidingitwithanopportunitytomakesubmissions.SouthWesternSydneyAreaHealthService’sresponsewasprovidedon20October2003.
ThefinalreportwasprovidedtotheDirector-GeneraloftheDepartmentofHealthandtheActingChiefExecutiveofSouthWesternSydneyAreaHealthServiceon9December2003.Itisentitled’InvestigationReport–CampbelltownandCamdenHospitals–MacarthurHealthService’.
TheHCCCreporteditsanalysisof47specificclinicalincidentsthatoccurredbetweenJune1999andFebruary2003.Intheexecutivesummary,theHCCCstatedthattheevidenceobtainedaboutthose incidents strongly supported the allegations by the nurse informants about the standard ofcare,insomeincidentssopoorthatthepatientssufferedseveredeteriorationinhealth.The

35
InvestigationReportclaimedtohaveidentifiedpatternsofinadequatecareandtreatmentattheHospitals.TheHCCCdelivereditsReporttotheDirector-General,whopublisheditaswasunderstood to be necessary under the Health Care Complaints Act.
In December 2003 the Minister moved to dismiss the Health Care Complaints Commissioner for NSW.HealsoannouncedtheestablishmentofaSpecialCommissionofInquiryonthematter.
TheSpecialCommissionofInquiryisappointed
InDecember2003,theGovernorofNSWappointedBretWalkerSCtoleadaSpecialCommissionofInquiryintoCampbelltownandCamdenHospitals.Hisreporttitled‘InterimReportoftheSpecialCommissionofInquiryintoCampbelltownandCamdenHospitals’wasreleasedon31March2004.Forconvenience,wewillrefertotheSpecialCommissionastheinquiryteaminthefollowingdiscussion.
3.2 TheInquiry
3.2.1 TheFirstInterimReportoftheSpecialCommissionofInquiry
TheinquiryteamwasinstructedtoinquireintoandreportonallegationsofunsafeorinadequatepatientcareatCampbelltownandCamdenHospitalsandotherrelatedmattersmadeinasetofLetters Patent – formal documents resulting from formal complaints made by a group of nurses. Thescopewassubsequentlywidenedtocoverallthenurseswhohadmaderelevantallegationsaboutpatientcareatthetwohospitals.
TheInquirywasconductedundertheSpecialCommissionsofInquiryAct1983.DetailsofitsprovisionsanditsrelationshipswithotherlegislationaredescribedinsomedetailintheReportbut are not relevant to the purpose of this paper.
Theterm‘interimreport’isclearlyexplained.First,thereareotherrelevantmattersaboutwhichinvestigationsareincomplete.Second,withrespecttothosemattersdiscussedinthereport,thefindingsarefinal.Theinquiryteamsays“…itisnotaprovisionalreport:theviewsinitandtherecommendationsmadeinitarefinalwithrespecttothemattersthatareaddressedinthisinterim report.”
The inquiry team chose not to give the concerned doctors and nurses the opportunity to question itsfindings.Rather,itsimplyrecommendedthattheirconductbethesubjectofstatutoryinvestigationandconsiderationofdisciplinaryprosecution,duringwhichprocesstheywouldbeafforded ample opportunities to refute any allegations against them. The report does not name theconcerneddoctorsandnurses.ThepowertodisciplinemedicalpractitionersornursesresideswiththeMedicalTribunal,NursesTribunalandthosewhoadministerotherformsofprofessionaldiscipline.TheHCCChasthepowertoinitiateproceedingsbeforeaMedicalorNurses Tribunal.
Theinquiryteam’scommentsontheinvestigationbytheHealthCareComplaintsCommission
Asweindicatedabove,theinquiryteamwashighlycriticaloftheinvestigationundertakenbytheHCCC,andwewillonlybrieflycoverthereasonshere.Thefocuswillbeonthehealthcareaspects.

36 Patient Safety: a comparative analysis of eight Inquiries in six countries
First,theinquiryteambelievedtheHCCCwaswrongintreatingtheMacarthurHealthServicetobethesubjectofthecomplaint.Second,oncethisdecisionhadbeenmade,theHCCCshouldnothavereportedthatcomplaintsagainstspecificclinicianshadbeensubstantiated.Third,thereportshouldnot have been published before the clinicians had been through disciplinary adjudications.
Theinquiryteamrejectedtheideathatthenurseinformants’allegationswereagainstahealthorganisation (the Macarthur Health Service) rather than against clinicians. It stated that a complaint concerning the conduct of a doctor alleging that he or she has demonstrated inadequate care is“…undoubtedlyacomplaintagainstthedoctor.”TheHCCCwaswronginissuingareportthatsubstantiatesallegationsofinadequatecareonthepartofidentifiabledoctors,withoutregardingthoseallegationsasacomplaintagainstthatdoctor.“Thiswasoffensivetoasenseoffairness.Itdeniedthedoctorsanopportunitytomakesubmissionsagainsttheconclusionthattheallegationsweresubstantiated”.
Whyaninterimreport?
FailuresonthepartoftheHCCCwerethemainreasonswhytheinquiryteamchosetoreleaseaninterimreport:itwasadeviceforensuringaspromptaresumptionorcommencementofformalinvestigationofthemoreseriousallegationsaspossible.Theinquiryteamundertookaprocessofratingtheseriousnessoftheallegations,sothattheymightbeaddressedinorder.
Themostseriouscaseswerejudgedtobethosewheretheimportantfunctionofdealingwithcomplaintsagainstdoctors(ornurses)hadbeeninadequatelyhandledbytheHCCC.Atablewaspublishedbytheinquiryteamthatwassaidtoillustrate“…howbadlytheHealthCareComplaintsCommissionperformedincomplyingwiththestraightforwardrequirementsofthecomplaintssysteminforce.”Thishadnotonlyledtounfairtreatmentofthecliniciansconcerned,butalso“…deniedformorethanayeartheefficientadministrationoftheassessment,investigationanddecisionbytheHealth Care Complaints Commission of many complaints against a number of doctors and nurses.”
Inapublichearingon26March2004,shortlybeforereleaseoftheinterimreport,theSpecialCommissioneremphasisedtheimportanceofpromptaction.“ItisdifficulttooveremphasiseforacommissionofthekindIamconducting,thehighpublicimportanceofensuringthatlawswhichregulatethosewhomayadministermedicalprocedureswithalltheriskstolifeandlimb,thehighpublicimportanceofensuringthatthoselawsoperateswiftlyandafterthoroughinvestigation.”
Themethodofinquiry
InDecember2003,theinquiryteamplacedadvertisementsinnewspapersinSydney(andspecificallyintheMacarthurarea)seekinginformationandtheexpressionofviews.Theinquiryteamalsoreceived115writtenresponses,manyaboutthetreatmentreceivedbyindividualsandsome commenting on issues of reform of the health system.
ConsiderationoftheHealthCareComplaintsCommissionReport
ThefirsttermofreferencerequiredtheinquiryteamtoconsidertheHCCC’sreport.Inparticular,theinquiryteamshouldconsiderthefindingsconcerningallegationsmadeaboutthetreatmentprovidedto69patientsatCamdenandCampbelltownhospitalsbetween1999and2003.
The HCCC provided �80 folders containing information gathered during its investigation. The contentsofthosefolderswerereviewedbyinquirystaff.Thereportdidnotnamethepatientsorthepractitioners but simply allocated code numbers. In 2� of the 69 cases the HCCC had been unable to identify the patient from the information provided by the nurse informants or from other available sources,andconsequentlytheywerenotinvestigatedbytheHCCC.

37
SUBMISSIONS,INTERVIEWS,ANDREVIEWOFADDITIONALDOCUMENTS
Theinquiryteamcategorisedthe48identifiedcasesaccordingtotheseriousnessoftheconductofindividualsinvolvedinthecare.Themostseriouswerereviewedfirst.
Theinquiryteamcommunicatedwitheachpatientorfamilymemberwhosetreatmentwasthesubjectofreview.ItobtainedthemedicalrecordsforeachpatientfromMacarthurHealthServiceandanyotherhospitalwheretheyrelevantlyreceivedtreatment.Summonsesfortheproductionofdocumentswereissuedinseventeencases,mainlytoMacarthurHealthService,seekingmedicalandotherrecords.MacarthurHealthServiceassistedwiththeidentificationofthenamesandpositionsofvariousmedicalpractitionersandnurses,whichwasadifficulttaskdueto the near illegibility of some of the medical records.
TheInquiryalsoconsideredthesubmissionsmadebythenurseinformants,submissionsbythepatientorfamilyofthepatientandthefindingsofanyreviewconductedbyMacarthurHealthService into the treatment of the patient.
Sixexpertswerethenengagedbytheinquiryteaminthefieldsofemergencymedicine,psychiatry,anaesthetics,nursing,obstetricsandgynaecologyandsurgery.Theinquiryteammet each expert one or more times to discuss the treatment provided to each patient and the standardofcareprovidedbyeachrelevantmedicalpractitionerornurse.Theirassistancewasjudgedtohavebeen“…extremelyvaluableandindeedessential”.
Aftergaininganunderstandingoftheclinicalissues,theinquiryteaminterviewedeachnurseinformantinrelationtoeachcaseinwhichtheywereinvolved.Alleightnurseswereinterviewed,oneoveranumberofsessions.Theinterviewsgeneratedover500pagesoftranscript.Duringtheinterviews,mostofnurseswerelegallyrepresented.Attheinterviews,theviewsofeachnurseweresoughtontheclinicalissuesinvolvedandimportantly,whatfurtheractiontheybelievedshouldbetakeninadditionto,ordifferentfrom,thatrecommendedbytheHCCC.Interviewsalsotookplacewithotherparticipantsinthetreatmentorwithfamilymembersofpatients.
Theinitialgoaloftheinquiryteamwastoidentifythosehealthpractitionerswhoseapparentconductwarrantedinvestigationwithaviewtosomeformofactionbeingtaken.Inthisway,conclusionsweredrawnaboutthestandardofcaredeliveredin44cases.Thefinalfourweretobe resolved later.
TheinquiryteamtheninformedtheHCCCofitsopinions,thusprovidingacomplaintonwhichtheHCCCisrequiredtoact.Eachpractitionerwillthusbeaffordedtheopportunitytoknowthecomplaint against him or her and respond to it and to any action the HCCC may propose at the end of the investigation.
ConclusionsoftheSpecialCommission:conductwarrantinginvestigation
The inquiry team recommended that the HCCC investigate the conduct of �2 medical practitionersinrespectofthecareoftenpatients.Theteamreportedithadmade“…substantialprogressinidentifyingthosenurseswhoseconductwarrantsinvestigationbytheHealthCareComplaints Commission”.
TheReportdidnotnamethedoctors,butratherlabelledthemDr1throughtoDr12.Theselabelsareusedinoursummarybelow.

38 Patient Safety: a comparative analysis of eight Inquiries in six countries
MASTECTOMYOFTHEWRONGBREAST
Dr1wasavisitingmedicalofficer(surgeon).Drs2and3weresurgicalregistrars.Dr1obtainedconsentfromtherelativeofapatienttoperformamastectomyonthepatient.Theconsentformwasincompleteandreferredtothewrongsiteforthemastectomy.TheprocedurewasperformedwitheachofDrs1,2and3participating.Thewrongbreastwasremoved.Thediseasedbreastwaslaterremoved.
FAILURETORECORDPELVICFRACTURE
Dr4wasacareermedicalofficer(locum).Inrelationtoapatientwhohadfallennexttothebed,herecorded in the medical notes the results of his examination of the patient. An x-ray and examination thefollowingdaydetectedapelvicfracture.Dr4hadnotrecordedthathedetectedapelvicfracture.ItisallegedbyawitnessthatDr4didnotcarryouttheexaminationthathehadrecordedinthemedical records.
COMPLICATIONSOFALAPAROSCOPICCHOLECYSTECTOMY
Dr5wasavisitingmedicalofficer(surgeon).Dr2wasasurgicalregistrar.Dr5performedalaparoscopiccholecystectomyonapatient,withtheassistanceofDr2.Thepatientdiedfivedaysafterthesurgery,apparentlyfrompostoperativeintra-abdominalsepsis.Thiscomplicationhadnotbeen promptly diagnosed or treated.
INAPPROPRIATEDISCHARGEOFTWOPATIENTS
Dr6wasavisitingmedicalofficer(physician)whohadvisitingrightsattheCampbelltownandCamdenHospitals.Hedischargedtwopatientsfromhospital.Oneofthemdiedbeforereachinghome,andtheotherdiedwithinlessthan24hoursafterdischarge.
FAILURETODIAGNOSEISCHAEMICFOOT
Dr7wasavisitingmedicalofficer(surgeon)whohadvisitingrightsatCampbelltownandCamdenHospitals.Dr8wasacareermedicalofficer(emergency).Theyhadresponsibilityforthecareofanelderlypatientwhodevelopedanischaemicfoot.Dr8didnotdiagnosethecondition.Dr7didnotreviewthepatientwhenthediagnosiswasmadebyathirdmedicalpractitioner.
FAILURETOACTPROMPTLYREGARDINGAPOSSIBLEPERFORATEDPEPTICULCER
Dr7,avisitingmedicalofficer(surgeon)andDr8,acareermedicalofficer(emergency)treatedapatientwhopresentedwithapossibleperforatedpepticulcer.Aperiodofabout12hourselapsedbeforethepatientwastransferredfromahospitalthatdidnotperformotherthandaysurgerytoonethat did. The patient died six days after the transfer.
PRESCRIBINGOFDRUGTOWHICHPATIENTWASKNOWNTOBEALLERGIC
Dr9wasacareermedicalofficer(emergency)whoattendedapatientwhohadattemptedsuicide.Heisrecordedashavingprescribedandadministeredadrugtowhichthemedicalnotesindicatedthepatientwasallergic.
INCORRECTTREATMENTOFACUTEASTHMA
Dr10wasacareermedicalofficer(anaesthetics).Dr11wasavisitingmedicalofficer(physician).Drs10and11treatedapatientwhohadacuteasthma.Dr11isrecordedasprovidingcertainadvicetoDr10,butDr10didnotfollowit.Dr10administeredcertaindrugstothepatient,whodiedfourhours after admission to the hospital.
39
FAILURETOACTPROMPTLYTORESUSCITATE
Dr12wasacareermedicalofficer(emergency)whotreatedapatientwhoattendedacutelyunwell.Thepatient’ssystolicbloodpressurewaslowandthepatientrequiredresuscitation.Dr12didnotcontactthevisitingmedicalofficerpromptly.Hedidnotresuscitatethepatient,andthepatient died �2 hours later after being transferred to another hospital.
ConclusionsoftheSpecialCommission:conductwarrantingperformanceassessment
TheHCCCcanreferacomplaint,orpartofacomplainttoanotherpersonorbodyifitappearsto raise issues requiring investigation by the other person or body. The Medical Practice Act permits the Medical Board to assess the professional performance of a registered medical practitioner if there is reason to suspect that person’s professional performance is unsatisfactory. Professionalperformancereferstotheknowledge,skillsorattitudespossessedandappliedbythepractitionerinthepracticeofmedicine.Unsatisfactorymeansbelowthestandardreasonablyexpected of a practitioner of an equivalent level of training or experience.
The inquiry team recommended that the HCCC should consider referral to the Medical Board theconductoffivemedicalpractitionersinrelationtotheirtreatmentoffivepatients.TheinquiryteamlabelledthemDrAthroughtoDrD,andDr12(theemergencydoctorasnotedabove).
FAILURETOREQUESTSPECIALISTCONSULTATIONFORPREGNANTWOMAN
DrAwasanobstetricsandgynaecologyregistrarwhotreatedapregnantwomanwithahistoryofasthma.Thespecialistobstetricianwasnotaskedtoattendthepatientuntilaboutfourhoursafterherpresentation.Shewastransferredtoanotherhospitalwheresheandherbabysurvived.
INAPPROPRIATE DISCHARGE
DrBwasacareermedicalofficer(emergency)whotreatedapatientwhohadpresentedwithsharppain.DrBrecommendedtothevisitingmedicalofficerDr6thatthepatientbedischarged,ten hours after presenting. The patient died less than �6 hours later.
FAILURETOCOUNSELONENDOFLIFEMATTERS
DrCwasanintensivecareregistrarwhoconservativelytreatedanelderlypatient.TherewasnorecordofdiscussionsbetweenDrCandthepatientorthepatient’sfamilyconcerningendoflifematters.
FAILURETOPRESCRIBEANTIBIOTICS
DrDwasamedicalregistrarandDrCanintensivecareregistrar.Themedicalpractitionerstreatedapatientwhoattendedthehospitalatabout4.30amandultimatelydiedsomesevenhourslater.Foralengthyperiodfollowingtheadmission,themedicalpractitionersdidnotprescribe antibiotics.
Thewaytheclinicianswereidentified
Asnotedearlier,theinquiryteamheldapublichearingon26March2004.Boththeinvolveddoctorsandinvolvednurseswerelegallyrepresented.Themainpurposewastoallowtheinquiryteamtooutlineitslikelyconclusionsandrecommendations,andreceivecommentsfromlegal representatives and other interested parties.

40 Patient Safety: a comparative analysis of eight Inquiries in six countries
Itsmainconcernwaswhether,eventhoughnameswerenotdisclosedinitsReport,theremightbesufficientinformationtoallowfortheidentificationandpublicdisclosureofidentities.Atthehearing,theinquiryteamreferredto“…someofthemostseriousallegationsonecouldimagineagainstmedicalpractitioners,includingallegationsofgrosslysubstandardtechnicalskillaswellasgrosslyuncaringattitudes.”Anadditionalcauseofconcernwasthattheinquiryteam’sfindingsweremostlyrelatedtocareprovidedbytwoormorehealthprofessionals.Allegationsofsubstandardcareorofuncaringconduct“…cannotbedoneasjoblots.”Theindividualsmustbeheldresponsibleindividuallyiftheyhaveindividuallyfallenshortoftheappropriatestandard,andeachindividualmust have the proper opportunity to dispute his or her culpability.
Commentsonthequalityofmedicalrecords
Theinquiryteamtookcaretoavoidaddressingsystemicissues,forreasonsnotedbelowunderitsplannedfollowupactions.However,theCommissionerdidmakesomegeneralcommentsduringthe course of the public hearing on 26 March 2004.
TheCommissionernotedthat“…theInquiryhasbeenhamperedbydefectsinrecordswhichmayor may not be sinister.” He held the opinion at that time that the defects that most hampered the Inquirywerenotsinister–thatis,aconsequenceofadeliberateattempttoconcealinformation.Rather,hearguedtheyweremostcommonlyaconsequenceoftheinabilityorunwillingnessoftheclinicians“…tofollowthebasicinstructionthattheyshouldpreparetheirrecordslegiblyandclearly,makingsurethattheyname,sign,dateandtimeallentries.”
Henotedthatthedesignersofthemedicalrecordformswerepresumablyawareoftheimportanceofsodoing,andofthelikelihoodthattherewouldbelowcompliance.Thiswasconcludedfromthefact that most of the medical record forms examined during the Inquiry repeated the elementary messageoneverypage.TheCommissionerthoughtthatthemessagemighthave“…becomeoutwornbyrepetition.”
HethenspeculatedthathiswasprobablynotthefirstInquirytoexperiencetheproblem.Itwaspossiblethatmuchtimeandmoneyhadbeenwastedduringinquiriesintomedicalconductinthewesternworld,asaconsequenceof“…theinabilityorrefusalofpractitioners–alasmostlydoctors,notnurses–topreparerecordsinawaythatthosefollowinginthecareofthepatient,andcertainlythosefollowinginthescrutinyoftheirconduct,wouldfindstraightforwardtouse.”Hefurtherspeculatedthatitwas“…acauseforhumouronthepartofsomemedicalpractitionersthattheirhandwritingisillegible.ItshouldbeclearfromtheexperienceofwastedmoneyinthisInquirytryingtodecipherthehandwritingofdoctors,thatthereisnocauseforhumouratallinthisimpositiononthe public.”
“Thatmattermeansthattherecordsarenotalwaysstraightforwardtodecipherand,intheordinarywayofanyrecordskeptbyhumanbeings,itmeansthattheymaynotalwaysberelieduponwithconfidenceateverypoint.That,again,neednotbeasinistermatter.Itiscommonplacethatpeoplemakeerrorsanddatesandtimesandsometimesaboutmattersmoreseriousthanthat.However,therehasalreadybeenoccasionintheinterviewswithnurseinformantsforthemtodrawtomyattentionandformetoagreewiththeirobservationsthatinquiteafewreportingcasestherecordsaredeficient–thatis,thingsarenotrecordedwhich,inthenatureofthings,shouldhavebeenrecorded.”
Finally,theCommissionernotedthatsomeofthemostseriousallegationsofpoorclinicalpracticeinvolvedmattersnotappearinginmedicalrecords.Healsonotedtheobverse,wheretherewererecords that the allegation substantially demonstrated could not be true.

4�
Plannedfollowupworkbytheinquiryteam
Atthetimeofpublicationofitsinterimreport,theinquiryteamwasinvestigatingsevenothercaseswheretherewereunidentifiedallegations.Theoutcomeswouldbedescribedintheinquiryteam’sfinalreport.Investigationswouldalsocontinueregardingthepossibilityofinappropriateconduct by nurses.
InthenextphaseoftheInquiry,considerationwouldbegiventothesuggestionthatthemedicalandnursingdisciplinarysystemisexcessivelyconcernedwithblameandtherebysacrificessystemicimprovement.Theinquiryteamwouldprovideopportunitiesforthosewhotookthatviewtoexplainanddefendit.Theinquiryteamdid,however,indicateitspreliminaryopinionthattheInquiry“…discreditsthenotionthatindividualaccountabilitythroughprofessionaldisciplineisinconsistentwithsystemicimprovementofclinicalcareandinstitutionaladministration.”
The inquiry team further argued that the heath system requires individual professionals to do theirworkwell.Systemwideimprovement“…cannotpossiblyrequireremovalofthepossibilityofdisciplinarysanctionforthosewhofallbadlybelowproperstandardsofconduct.Itwillbeinterestingtodiscoverinthenextphasehowseriousthesesuggestionsare,whichhavebeenreported to the effect that the disciplinary system is an impediment to improvement of the heath system.”
ThenextphaseoftheInquirywouldalsoconsidersomeideasarisingfromthefirststageoftheInquirywhereby“…formalarrangementsaremadeforcontinuousattentiontosystemicimprovement,apartfrom,independentofbutinformedbythedisciplinarysystemadministeredby the Health Care Complaints Commission and the registration authorities.” The inquiry team sawtheseideasasbeingfoundedonsomekindof‘clinicalexcellencecommission’,andtakingaccountofrecentexperiencewithTheNSWInstituteofClinicalExcellencethathasinvolvedattemptingtoenhanceitskindofapproach.
Finally,theinquiryteamexpresseditsviewthatthebodychargedwithaddressinghealthcarecomplaintsshouldnothave,orseeitselfashaving,afrontlineroleinthemonitoring,forthepurposeofimprovement,ofclinicalcare.Rather,theintelligencewhichshouldbeusedforcontinuousimprovementwillincludebutwillnotberestrictedtotheharshlessonsofdisciplinarycomplaintsdeterminedadverselyagainstdoctors,nursesandhospitals.Theinquiryteamarguedthat“…itisinherentlyunlikelythatanapproachtocontinuousimprovementwhichrestricteditselftothelessonsthrownupbydealingwithdelinquentorincompetentpractitionerswouldbean adequate means of discharging that function.”
ChangesattheHealthCareComplaintsCommissionin2004
AnActingCommissioneroftheHCCCwasappointedinDecember2003,whoimmediatelybegantomakestructuralandadministrativechanges.Inter alia,heestablishedanewteamofinvestigatorstoaddressissuesrelatingtotheCampbelltownandCamdencomplaints.ItdidnotcontainanyoftheHCCCstaffpreviouslyinvolved,andwasheadedbycounselfromtheprivatebarandlocatedawayfromtheHCCC’soffices.
Otherchangeshaveincludedimprovedwaysofinvolvinglegalandmedicalexpertsatanearlierstageofinquiry,andthesettingofaperformancestandardthatrequires90%ofinvestigationstobecompletedwithin12monthsofcommencement.Thisisconsistentwiththeviewsoftheinquiry team. Inter alia,theteamsaidthatthedelayininvestigationsandprosecutionsovertheCampbelltownandCamdenaffairhadbeendeplorable.

42 Patient Safety: a comparative analysis of eight Inquiries in six countries
3.2.2 TheSecondInterimReport
TheinquiryteamissuedanotherreportinJune2004.ItfocusedalmostexclusivelyonthelegalprocessesoftheInquiry.Inparticular,itaddressedcriticismsoftheHCCC’sprocessesbyafacultymemberoftheNSWInstituteforClinicalExcellence,whichwerewidelydistributedthroughatechnical publication.
Thecoreofthecriticismwasthattheinquiryteamhadbeenunfairinreferringdoctorsforpossibledisciplinaryaction,withouttheirbeinggivenanopportunitytogivetheirviewsabouteventseithertothe HCCC or the Special Commission. The Commissioner strongly refuted the criticism mainly on thegroundsthattheywouldhavetheopportunityatalaterdate.Intotal,theinquiryteamdefendeditsapproachonthegroundsthatit“…wasintendedtosecuretheproperbalancemandatedbylawbetweenaccountablecomplaintsprocedure,patientconfidentialityandtheappropriateprivacyforhealthpractitionersagainstwhomcomplaintsmayhavebeenmadebutagainstwhomnoadversefindingscouldyetbemadelawfully,ifever.”
TheReportaddedlittleelse,otherthanprovidinganupdateonthestateoftheinvestigations.Itnotedthatall48incidentsidentifiedbytheHCCChadbeeninvestigated,ashad56oftheadditionalallegations from the nurse informants.
Finally,theReportincludedanAppendixlistingthedoctorsandnurseswhoshouldbeinvestigated,orhavetheirperformanceassessed.TheAppendixwassubmittedwitharecommendationthatitshould not be published.
3.2.3 TheFinalReport
ThefinalreportoftheSpecialCommissionofInquiryintoCamdenandCampbelltownhospitalswasreleasedonJuly30,2004.Muchoftheworkofmostinteresthere,however,hadbeencompletedthroughpublicationoftheinterimreports.Thusdecisionshadalreadybeentakenregardingthelargemajorityoftheallegationsofpoorcare,andviewsformedregardingthetreatmentofthosecomplaintsintheearlierinvestigationsoftheHCCC.Withregardtothesubstance,thefinalreportconsequentlyaddedverylittle.Forexample,itrepeateditsrecommendationsregardingfurtherinvestigationofsomedoctorsandnursesbutaddedasmallnumberforwhomitsinvestigationshadnotbeencompletedwhentheinterimreportshadbeenpublished.
Theinquiryteamagainstressedthatthetwopreviousreportswereinnowaysupercededbythefinalreport.Therearehardlyanyreferencestotheneedtoadjustthecontentsofthosereports,andadjustmentsarealmostwhollyamplifications.
Intotal,thefinalreportislargelyabagoflooseends–aswillbeevidentfromthefollowingdescription.ThemainpartisadetailedreviewoftheinvestigationsundertakenbytheHCCC.OtherlengthysectionsconcernchangesthathavetakenplacewithintheMacarthurHealthServiceandelsewhereinthelastfewyearswithregardtopatientsafety,anddiscussionoftechnicalissuessuchasthebalancetobestruckbetweenindividualaccountabilityandcontinuousqualityimprovement.
Itisfarfromeasytoread,mainlybecauseofthecomplexity(andquestionablelogic)ofitsstructure.Forexample,recommendationsappearintwochapters(andnotattheendofthedocumentasisclaimed in the Preface). There is no easily located summary. The section that most resembles a summary is contained in a chapter headed ‘Preface’. Discussion of the investigations conducted by theHCCCismainlycontainedinthreechapters(whereoneislargelydevotedtorecommendations)andoneAppendix,butitappearsinseveralotherchapters.

43
Thereisasectiontitled‘Introduction’thatdoeslittlemorethaninformthereaderofwhatheorshealreadyknows–thatthissectionissomewherenearthestartofthereport.Underthisheading is a variety of only loosely connected topics such as the nature of the Macarthur Health Service,anddifferencesbetweenthisInquiryandotherssuchasBristolandtheKingEdwardMemorial Hospital.
Wehavedoneourbesttopresentthereport’scontentsinaformthatismeanttobeeasiertounderstand,buthaveavoidedanymajordeparturesfromthestructureoftheoriginaldocument.Thismightmeanwehavefallenbetweentwostools.
Abalanceisneededbetweenindividualaccountabilityandsystemsimprovements
Clinicalprofessionalsmustbeaccountablefortheirerrors,butlegalprocessesshouldbethelastresort.Theycomprise“…analmostmarginal–butveryimportant–componentdesignedforrelatively rare and extreme events.”
Otherroutineprocessesforidentifyingandinvestigatingproblems,andthetakingofcorrectiveactions,arelikelytobemorebeneficialoverall.TheyshouldincludetechniqueslikerootcauseanalysisasbeingpromotedbythenewlyestablishedClinicalExcellenceCommission.
ComparisonswiththeBristolandKingEdwardInquiries
Chapter1brieflysummarisedtheBristolandKingEdwardMemorialHospitalInquiriesinitsownfinalreport.Ratherimprecisely,theReportsaid“…therehavebeentwosignificantInquiriesintothedeliveryofhealthcareatspecificinstitutionsoverthelastfiveyears,inEnglandandWesternAustralia.”Weassumetheinquiryteammeanttosaytherehavebeentwothatcaughtitsattention.
Otherwise,thesummariesarereasonablyaccurate(ifmissingsomeimportantdetails).Ofparticularrelevancehere,theinquiryteamfailedtoreporttheBristolInquiry’sstartingconclusionthatitwasnotanaccountofbadpeople.Rather,thehealthcareprofessionalsatBristol“…whoseworkwasfoundtohaveharmedpatientswere,forthemostpart,productsofasystemthathadfundamentalweaknesses.”Theinquiryteamdid,however,notethattheKingEdwardMemorialHospitalObstetricsandGynaecologicalServiceswerecharacterisedby“…acultureofblame,unsupportiveofopendisclosureoferrorsandadverseevents.”
Itisnotsurprisingthattheinquiryteamthereforeemphasisedthelocalpeculiarities.“Therelevantstandardsandsystems,bothforthedeliveryofhealthservicesandfordealingwithcomplaintsaboutthem,arecreaturesofNewSouthWaleslawandgovernment.ThereisnoavoidingthespecifictextsofNewSouthWaleslegislationgoverningthemattersexaminedbythisInquiry.”
Wewouldargue,however,thatthereweremoreimportantdifferencesintheprocessofinquirythaninthekindsofhealthcareproblemsbeinginvestigated.Theinquiryteamhadacleardirectionthatemphasisedindividualaccountabilitiesratherthansystemicproblems.Moreover,theinquiryteamitselfseemedtobemorefamiliarwith(andconsequentlymoreinterestedin)thelegislative rather than the health care systems aspects of poor care.
Assessmentofcareonthebasisofcomparativestatisticalanalysis
Chapter1includessomecommentsontheextenttowhichitwaspossibletoassesshospitalperformanceonthebasisofstatisticalanalysis.AfeatureoftheBristolandKingEdwardMemorialHospitalInquirieswasthatstatisticalcomparisonsweremadethatshowedthereweresignificantlyhigherratesofpoorpatientoutcomesthanatsimilarhospitalsforthecasetypesunder investigation.

44 Patient Safety: a comparative analysis of eight Inquiries in six countries
Incontrast,theinquiryteamwasunabletofindanycomparativestatisticsthatsuggestedsignificantlydifferentoutcomesfortheCampbelltownandCamdenHospitals.Threecommentsoftheinquiryteamonthisstateofaffairsareworthyofnote.
First,theinquiryteamconcludedthat“...unfortunatelyitisnotpossibletogaugethegenuinequalitiesofhealthcareattheCampbelltownandCamdenHospitalsbyuseofthekindoffiguresthatare available.”
Second,theinquiryteamreferredtoarticlespublishedintheMedicalJournalofAustraliainApril2004byseveraldoctorsassociatedwiththeMacarthurHealthService,inwhichtheauthorsimpliedthatthehospitalshadextremelylowratesofadverseevents(Frankumetal,2004).Theinquiryteamaskedtheprimaryauthortoexplainthebasisforhisconclusions.Theauthor“...agreedthattherewerenodata...whichenablesonetoapplyanybenchmarkorcomparisonfortheCampbelltownandCamdenHospitals.”Theinquiryteam’sreportthusimpliesthatthecontentsoftheletterwereatleastmisleading.
Third,theinquiryteamreporteddiscussionswiththeformerGeneralManagerofMacarthurHealthService,duringwhichshedescribedbenchmarkingactivitiesinwhichtheServicehadbeeninvolvedsince1996.TheactivitieswereconductedbytheHealthRoundtableLimited(inwhichmanyotherAustralian hospitals have been involved). The inquiry team concluded that the information thus generatedwaslimitedinitsutilityinmanyways,atleastforthepurposeofassessingqualityofcare.
Takentogether,thesecommentsareofsomefuturerelevance.Theysuggestthatroutinestatisticalcollectionswereinadequateintermsofthemonitoringofaspectsrelatingtopatientsafety.However,itshouldalsobenotedthatthecasescoveredbytheCampbelltownandCamdenHospitalsweredifferentfromthosecoveredatBristolandKingEdwardMemorialHospitalinthattheyinvolvedlownumbersofcasesofmanytypes.Therewasmoreinherentvariability,andthefocusoftheInquirywastowardsspecificallegationsfrommanysourcesratherthanaglobalconcernforaparticulartype of treatment.
Usingthe‘systemsapproach’
Theinquiryteamwasnotfamiliarwiththeterm‘systemsapproach’atthestartofitswork,andhadnotgraspedtheideaadequatelyattheend.Thusitmakesuseofthetermininaccurateandmisleadingways,asillustratedbythefollowingextractfromChapter1ofthefinalreport.
(The Bristol) Inquiry adopted a systems approach to its analysis. By this they mean poor performance and errors were seen as the product of systems which were not working well, as much as the result of any particular individual’s conduct.
Inthescientificcontext,systemsareobjectsandevents,andthecauseandeffectrelationshipsbetweenthem.Therelationshipscanbesimpleandunidirectionalortheymaybelinkedtogetherin long chains. Any one factor can exert a control function (causing a change in another) and a dependent function (being changed by another). The essence of the systems approach involves placingasmuchemphasisonidentifyinganddescribingtheconnectionsbetweenobjectsandevents as on identifying and describing the objects and events themselves.
Thustheinquiryteam’sdescriptionisillogical.Thesystemsapproachisexactlywhatonemightexpect:itisanapproachtoanalysisratherthanaparticularkindoffinding.Inter alia,itinvolvestakingspecialcaretoensurerelationshipsaretakenintoaccount.Giventhatrelationshipsaretypicallycomplicatedinhealthcare,itmightbeexpectedthatthesystemsapproachwouldbeparticularly useful.

45
Theapproach,whenapplied,doesnotnecessarilyleadtotheconclusionthatproblemsareaconsequence of a multiplicity of interconnected factors. It might be that the causes are located inonlyapartofthesystem.AsystemsapproachtoarecenttraincrashintheUKledtotheconclusionthatonlyonefactorwasimportant–thatofthetraindriverexperiencingseriousillhealth.
TheBristolinquiryteamdidseemtohaveadoptedasystemsapproach.Inourview,theydidlittlemorethanfollowasmanylinesofinvestigationthatthey(orothers)thoughtmightberelevant.However,itisreasonabletosaythattheyfoundsystemsproblems(orproblemsthatweresystemic).
Thiswouldhavebeenthecase,regardlessoftheinvestigativeapproachtheyhadtaken,aslongastheywerededicatedintheirtaskofunderstandingwhathadhappened.OnthisanalysisoftheWalkerinquiry,however,itisplainthatitdidnotapprehendwhatasystemsanalysisofcaremight add to understanding.
Therelevantlegislation
Thelargestpartofthefinalreportconcernslegislation.Chapter2describestheprocessofinvestigationofthecomplaintsregardingtheCampbelltownandCamdenhospitals(andtheMacarthurHealthService)bytheHCCC.Itrepeatsandamplifiestheconcernsoftheinquiryteam.
Chapter3extendsthediscussionoftheHealthCareComplaintsAct,andaddsdiscussionofrelated legislation – and the Medical Practice Act and the Nurses Act in particular. Chapter 4 then proposes legislative changes. The inquiry team’s main conclusion is that the legislation needsonlyminormodifications.
Individualaccountabilityandthenoblameculture
There are frequent references to the ideas of ‘individual accountability’ and the idea of the ‘no blame’culture.Bytheindividualaccountabilityapproach,theinquiryteamsuggestsensuringthatactionistakenagainstindividualswheretheirconductwassignificantlyinappropriate.Bythenoblameapproach,theinquiryteammeanttheincreasinglypopularideathatthefocusshouldbeonfindingandfixingproblemssotheyarelesslikelytooccurinthefuture–andthatthisrequireshealthcareorganisationstobeconfidenttheywillnotbecensured.TherelationshipsbetweenthesetwoapproacheswerediscussedinseveralpartsoftheInquiry’sreports,butthewholeofChapter5ofthefinalreportisdevotedtothem.
Forsomereason,theinquiryteamcametobelieveatanearlystagethattherewereseriousadvocatesoftheviewthattheseweremutuallyexclusive.Thisisunderstandable,becausesomepeopleinterviewedduringthecourseoftheInquirywereeitherunabletoexplaintheirideasclearly,hadnotthoughtthroughthematter,orboth.Itisevidentthatthe‘noblameculture’hasbecomeacatchphraseinhealthcare,likemanyothersbeforeit.Manypeopleuseitregularlyinordertobeseentobeuptodate,butfailtotakethetroubletounderstandwhatitmeans.
Initsfinalreport,theinquiryteamrecognisedithadbeenmisledtosomeextent.Itsaidthat“…the purported opposition of these dual approaches to investigating events or incidents in health carewasfictitious.Nooneseriouslymaintainedthatweshouldneverblame(thatis,attributefaultto)adelinquentdoctorornurse.Ifanyonehadpersistedwithsuchanextremeview,onequestionforhimorherinthisInquirywouldhavebeenwhetherthisimmunityfromindividualaccountabilitywouldextendtocriminalresponsibilityaswell.Theposingoftheseapproachesas

46 Patient Safety: a comparative analysis of eight Inquiries in six countries
rivalsormutuallyexclusivealternativeswasmererhetoric.Itwasacatchywaytoemphasisethatinsensitive or overly vindictive disciplinary action can be counterproductive in relation to the overall improvement of health care standards.”
Theinquiryteamsaiditwasobviousthat,insomecases“…thereneedstobeindividualaccountability.Inothercases,inthenatureofthingsmuchmorenumerous,seekingtoassignblameorfaultinaderogatorywayshouldbeavoided.”Severalexpertswereinvitedtomeetwiththeteam,andthediscussionsshowed“…thenoblameideatobesomewhatofastrawman.”Itwas“…hightimethatthetwocampsstrucktheirseparatetentsandtravelledtogether.Thechimeraofnofaultinhealth care should be banished. But the equal absurdity of expecting that all adverse outcomes – or evenmanyofthematall–areduetosomehaplessdoctor’sornurse’sfaultforwhichtheyshouldbe blamed or condemned should also be exploded.”
Theargumentsarenotwellpresentedbutaresurelycorrect.Toparaphrasethefindings,therearecircumstancesinwhichfearofdiscoveryandpublicblamecanindeedcauseindividualstoconcealerrors–andconsequentlydelaythetakingofcorrectiveactionstoreduceclinicalerrorsinfuture.However,therearealsocircumstancesinwhich,ifthereisnoriskofindividualblameandsanction,healthcareorganisationswillfailtotakeadequatecare.
Abalancehastobestruckthatisfarfromeasytofind.Onecomplicatingfactoristheextenttowhichtheindividualknewtheactwaserroneousatthetime.Anotheriswhetherpunishmentofamistakewillserveasaguidetootherstoavoidsimilarmistakesinfuture,orsimplyencouragethemtoconcealthemistakes.Inshort,thereisalmostalwaysacomplicatedsetofrelevantfactorsthataredifficulttoassess.
Perhapsthemostseriouserrorofallisthatofassumingtherearesimpleanswers.Inthepast,therehavebeenmanypeoplewhohavepromotedincreasedpunishmentasthesolutiontopoorclinicalpractice.Theyweremostlywrong,butthatisnoexcuseforpresentinganequallysimplisticmodelof‘noblame’.Healthcareisacomplicatedenterprise,anditisunderstandablewhymanypeoplechoosetoadoptslogans.Inthepast,itwasqualityassurance.ThiswasfollowedbyTQMandTQI,andnowwehavepatientsafetyandnoblame.
Theinquiryteamhasrightlycriticisedanoversimplifiedviewoftheworld.However,itmighthavecommittedasimilarerrorbyitsoversimplifiedviewofthecombinedapproach“…thatbodeswellformedicalandnursingprofessionsintentoncontinuousimprovementandfiercelyopposedtothebetrayal of public trust threatened by undetected and unsanctioned delinquencies.”
Weagreethatamixofapproachesisneeded,butthisleavesseveralaspectsunresolved.Ifthenurseordoctorisunsurewhattodo,andsubsequentlyconcludesamistakewasmade,heorshemustdecidewhethertoreporttheincident(andhopetobenefitfromanoblameview)ornottoreport it (for fear of being found guilty of a delinquent act). The issue not adequately addressed in theinquiryteam’sreportishowborderlinecasesshouldbehandled.Webelieveitisnecessarytoerronthesideofavoidanceofcensure,butthisviewneedstobeoperationalised.Thepresentguidelines and operating rules attempt to do this but there are surely some opportunities for improvement.Equallyrelevant,itisnecessarytoaddressnotonlythepointsoflawandregulation,but also the perceptions of clinicians. This last matter is not explicitly addressed in the inquiry team’s report.

47
Summaryofthefindings
Chapter6summarisesthecompletesetofallegationsthatwereinvestigated.Asnotedearlier,theyarealsosummarisedintabularforminanAppendix.TheprocesswaslargelydeterminedbytheallegationsthathadbeenconsideredbytheHCCC,althoughrelatedallegationswereuncoveredbytheinquiryteamthathadbeenoverlookedforavarietyofreasons.
Intotal,67allegationswereinvestigated,ofwhich11werereferredforfurtherconsiderationbyotherbodies(mainlybytheHCCC).Someweredismissedbecausetheywereinconsistentwiththeavailableevidence.Otherswerenotreferredbecausetheevidencewasinconclusive(andtherewaslittlelikelihoodofadditionalevidencebeinglocated).
Coverupallegations
InChapter7,theinquiryteamdiscussesthethreeallegationsmadebynurseinformantsto the effect that persons in authority had attempted to conceal evidence of poor care. One claimwasthatadoctorhadbeenaskedtodeletereferencetounreasonabledelayinseekingaconsultationforapatientintheEmergencyDepartment.Theinquiryteamsaiditwasnotdesirablepracticeforsucharequesttobemade,butthedoctorhadnotinfactagreedtotherequest.Thereforenofurtheractionwasrequired.
Asecondallegationwasthatmanagershadremovedordestroyedpatientrecords.Theinquiryteamdecidednottoexplorethisallegationindetail,butratherreferreditforinvestigationbytheIndependent Commission Against Corruption.
ThethirdallegationwasthatstaffoftheHCCChadrefusedtoinitiateinvestigationsontwocases as requested by a nurse informant. The inquiry team concluded that there had been nocoverup.Rather,therehadclearlybeen“…anunfortunatemisunderstandingorcrossedpurposes.”Thenurse-informant’sexperiences“…madehersensitivetoanythinginthenatureofarebufftowhatshesawasanattempttoraisemattersforofficialattention”.TheHCCCstaffmember’sreluctancetoactwasunderstandableifnotnecessarilycorrect.
Raisingconcernsaboutpatientcare
Chapter 8 discusses the issue of raising concerns about the appropriateness of clinical practice. InthecontextofthisInquiry,severalnurseshadmadeallegationsofdifficultiesencounteredwhentheyraisedconcernsaboutpatientcare.Onewasthattheformalprocessofreportingbywayofincidentreportswasflawedinseveralways.Inparticular,nursesallegedthatsomeofthereportsweremislaidordestroyed,thattherewasdiscouragementoftheprocessofreporting,thattherewaslittleornofeedbackregardingtheprocessingoftheirreports,andthatthereseemed to be no attempts to address the causes of poor care that they had reported.
LOSS OF INCIDENT REPORTS
Theinquiryteamattemptedtotracetheincidentreportssubmittedbythenurses.Itwasconcludedthatthesystemofreceipt,registration,processing,andfilingofreportswasinadequateinmanyrespects.Papercopiesseemedtohavedisappeared,andthepartialprocessofmaintenanceofcomputerrecordsalsohadelementaryweaknesses.
However,theinquiryteamcouldfindnoevidenceofdeliberatelossordestructionoftheincidentreports.Itconcludedthattherewasnoreasontobelievethat“…MacarthurHealthServiceattempted to cover up any incidences of allegedly unsafe patient care or treatment by the removal or destruction of incident reports.”

48 Patient Safety: a comparative analysis of eight Inquiries in six countries
ACTION AND FEEDBACK TO REPORTERS OF PROBLEMS
Theinquiryteamdidnotfindevidenceofdeliberateattemptstoavoidgivingfeedbacktothosewhoreportedproblems,ortotakecorrectivemeasureswherenecessary.Thesystemwassimplyinefficient,andthiswasformallyacknowledgedbyseniormanagers.Theinquiryteamconcludethiswasunfortunate.“Itisabasicprincipleofgoodcomplaintmanagementtorespondtothosewhotaketimetoregistertheirconcerns,andadvisethemoftheactionsthathavebeentakenasaresultoftheinformationtheyprovided.Anysystematicfailuretodosowillinevitablyleadtoajustifiablefrustrationbytheauthorsofconcerns,probablyresultinginadisinclinationtospeakupinthefuture.”
Theinquiryteamwasalsocriticaloftheprocessesofreviewofincidentreports.ThiswasparticularlythecasefortheCriticalCareReviewCommittee.It“…didnotoperateaswellasitshouldhave.Thetimewhichelapsedbetweenanincidentanditsconsideration…wasunacceptableinanumberof cases.”
ACULTUREOFDISCOURAGEMENTOFINCIDENTREPORTING
Nurseshadassertedthat,atallstagesofreportingandactingonincidentreports,therewasacultureofdiscouragement.Theinquiryteamconcludedthismightbethecase,butifsotherewasno evidence to suggest any particular individuals merited censure.
Itsfindingswereequivocalregardingnurses’allegationsofbullyingandharassmentofthembyseniorstaff,onthegroundsthattheywerebeingexcessivelycriticalofsafetymanagement.Theinquiryteamwasconcerned,however,aboutthewaythatcomplaintswereaddressedthatrelatedtoathirdparty–suchaswhereonenursehadcomplainedaboutcareprovidedbyanothernurseandtheresponsiblemanagerhaddeclinedtotakeactionbecausethecomplainantwasnotondutyatthetimetheincidentsoccurred.Theinquiryteamnotedthatfirsthandknowledgewaspreferable,but“…nursesshouldnotbepreventedordiscouragedfromsubmittinganincidentreportaboutmatterstheyhavenotwitnessed.”
Theinquiryteamconcludedthattherewereproblems,buttheyweremoreareflectionofpoorstaffrelationsthanofinsufficientconcernforpatientsafety.Theallegationsmostlyserved“…toillustratethenurses’frustrationswithaspectsoftheMacarthurHealthServiceandhighlightthelevelofinterpersonalconflictwhichappearstohaveexistedinsomeareaswithinthehospitals.”
Wewouldnoteherethatinterpersonalconflictscanhaveseriouseffectsonperformanceinalltypesofsystems,andtheinquiryteammighthaveexpressedagreaterdegreeofconcernoverthisaspectofoperations.Forexample,therehavebeenwelldocumentedincidentsintheairlineindustry,includingthecaseofaBritishAirwayscrashthattookplacewhenacockpitargumentwasunderway–andwherethepilotconsequentlyignoredclearwarningsofimminentdisaster.
Theinquiryteamsimplysaidthatpoorrelations“…shouldnotbelefttofesterbutshouldbedealtwithpromptlybymanagementthroughforumswhichareestablishedandknown.”Itfailedtosuggestexactlyhowsuchaprocessmightbeestablishedandmaintained.
Theinquiryteamreviewedvariousstepsthathavebeentakenrecentlywithregardtothehandlingof adverse events. These included outputs of the Australian Council for Safety and Quality in Health Care(suchastheOpenDisclosureStandard),theNSWDepartmentofHealth,andtheSouthWesternSydneyAreaHealthService.Theinquiryteamwasgenerallysatisfiedwithrecentprogress.
Particularattentionwasgiventotheprocessofrootcauseanalysis,whichwasjudgedtohavesomeutility.Thedebateaboutconfidentialitywasdescribed,includingtheargumentthatatleastsomeelements of the analysis might be concealed in order to ensure full participation of health care staff. Theinquiryteamconcludedtherewascurrentlynoevidencetosuggestthatfearsofharmthrough

49
fulldisclosurearejustified,butrecommendedthatareviewofthesemattersbeconductedafterthreeyearsofuseofrootcauseanalysisinvolvinglimitedprotectionofconfidentiality.Itsupported the statement of the Chair of the Australian Council for Safety and Quality in Health Carethat“…(rootcauseanalysis)mustbeusedassomethingtoinformthesystemandimprovement,notsomethingtohidebehindtoavoidthetruth”.
Employmentdisciplineagainstnurseinformants
Chapter9discussestheemploymentdisciplinaryactionsthatweretakenbytheMacarthurHealthServiceagainstfourofthenurseinformantswhoarguedthattheactionswereinappropriate.TwoofthenursesclaimedthatacultureexistedwherebythemanagementofMacarthurHealthServiceimplementedunfairdisciplinaryprocesses,whichinvolvedprocedurallyunfairinvestigationsandtheimpositionofsanctions,afterthenursesraisedallegationsofinadequatepatientcare.Asaconsequence,theirallegationswerediscreditedandignored.
TheinquiryteamconcludedtherewasnoevidencelinkingtheincidentreportingbythenurseinformantstothesubsequentdisciplinaryactiontakenbyMacarthurHealthService.However,theSouthWesternSydneyAreaHealthServiceacceptedthattheactionstakenagainstthetwonurseswereprocedurallyflawed,andmadeafullapologyinJanuary2004forthetreatmenttheyreceived.
AthirdnurseagainstwhomdisciplinaryactionwastakenbyMacarthurHealthServicein2002arguedthattheactionagainstherhadbeenharshandunwarranted.ShesubsequentlyreceivedanapologyfromtheNewSouthWalesDepartmentofHealth.
ThefourthnursewhowasthesubjectofdisciplinaryactionbyMacarthurHealthServicealsoarguedthatthiswasaconsequenceofhermakingcomplaintsaboutpatientcare.Again,theinquiryteamconcludedthatthedisciplinaryactionwasnotinresponsetoherraisingconcernsaboutpatientcare.Again,shereceivedanapologyfromMacarthurHealthServicewithregardtothedisciplinaryactiontakenagainstherandthedetailswereremovedfromherdisciplinaryfile.
Recordsofindividualpatients’care
InChapter10,theinquiryteamagainraiseditsconcernsaboutthequalityofroutinepatientcarerecords. It stated that its investigations had been seriously impeded by the poor quality of notes inthepatients’medicalrecords.Mostoftheproblemsrelatedtodoctors.Nursingentriesweregenerallyofasuperiorqualitywithnotonlylegiblewritingbutthenameofthenurseprintednextto his or her signature.
Itsaidthat“…withoutexception,enormousdifficultieswereexperiencedbyallconcerned.”Althoughtherewasaclearstatementatthetopofthepageofeachrecordthattheclinicianmustsignandprinthisorhersurnameanddesignation(initials)forallentries,mostoftheentriesbymedicalpractitionerswereeithertotallyorpartlyindecipherable.“Inmanycasesthenameofthedoctorwhoapparentlyhadsignedhisorhernameremainsamystery.”Theinquiryteamsaidthatthesituationwasnottothecreditofthoseresponsiblefortrainingorsupervisingthedoctors.Theinquiryteamdidnotknowwhetherdoctorswereunableorsimplyunwillingtofollowtheinstructions.
Sympathywasexpressedforthedegreeofworkpressureformostdoctors.Theinquiryteamdidnotsaywhethertheybelievedalldoctorswerealwaysundersimilarpressureofwork,orwhetheritbelievedthatnurses’higherlevelsofcompliancewereaconsequenceofbeinglessbusy.

50 Patient Safety: a comparative analysis of eight Inquiries in six countries
Theinquiryteamseemedtobelievethatthereweretechnologicalsolutions.Givenmoderntechnologies“…itisextraordinarythatnosystemhasbeenidentifiedtoovercometheobviousdifficultywithhandwrittenrecords.”Referencewasmadetoonehospital’spracticeofusingtypewrittennotesandtypewrittenrecordsofthosewhohaveenteredandareresponsibleforthenotes,andofanotherhospital’suseofpartlycomputerisednotes.ReferencewasalsomadetothesystemthatwasactivatedinMay2004(Healthelink),whichgivesgeneralpractitioners,specialists,EmergencyDepartmentcliniciansandalliedhealthworkersonlineaccesstotheirpatients’medicalhistories.Mentionwasalsomadeoftrialsunderwayofthenationalelectronichealthrecordsystem,HealthConnect.
Thereportdoesnotdrawconclusionsabouttheextenttowhichcomputerisationshouldbeused.TheteamsaiditwasbeyondthescopeofthisInquiry“…tosolvethisseeminglyendemicproblem.”However,intheabsenceofanelectronicrecord,theremustbeimprovementsinthewaythathandwrittenrecordsaremaintained.
Clinicalpracticeissues:endoflifecareandmedicalemergencies
Chapters11and12discusstwoaspectsofclinicalpracticethatwereraisedinseveralofthecaseswheretheinquiryteamfoundreasontoreferforfurtherinvestigation.Careshortlybeforedeathwasan issue in �0 of the 47 cases examined. The inquiry team noted recent changes in the guidelines providedtoclinicians.Itdecidednottogivespecificadvice.Itsimplynotedthatsuchguidelinesshouldexistandbeupdatedasnecessary.Moreover,seriouseffortsshouldbemadetoeducatestaff as to the importance of the principles and the need for documentation of any discussions.
Withrespecttomedicalemergencies,theMacarthurHealthServiceintroducedacareprocessinvolvingmedical emergency teams in �996. The main component of the process is that clinical staff can call fortheassistanceofexperiencedstaffwhentheybelieveamedicalemergencyexists.Somenurseinformantswerecriticalofthewaytheprocesswasused,andtheinquiryteamtendedtoagree.
Theinquiryteamconcludedthatoneimportantproblemwasthatthereweredifferentviewsastowhethertheprocedurewasmandatoryordiscretionary.SouthWesternSydneyAreaHealthServiceacceptedtheHCCC’sfindingsthattherehadbeenfourincidentswherenocallforassistancewasmadewhenitwasindicated.Theinquiryteamsaidthatamandatoryproceduremakesnosenseifstaffarenotadequatelyeducatedinitsuseorwheretherearenosanctionsfornoncompliance.
TherolesoftheClinicalExcellenceCommission
Chapter13ofthefinalreportdiscussedtheproposedClinicalExcellenceCommission,whichistohavefivemainactivities:apatientsafetyriskidentificationprogram;regularauditofpatientsafety systems in health care organisations; training and development programs; development and implementationofclinicalriskframeworks;andresearchintopatientsafetysystemsandqualityimprovements.
TheinquiryteamnotedtheoverlapandconsequentpotentialformisunderstandingsbetweentheClinical Excellence Commission (CEC) and the Health Care Complaints Commission (HCCC). It thereforeexpresseditsviewsontherespectiverolesofthetwoagencies,asfollows.
1. TheCECshouldberesponsibleforinvestigatingandmakingrecommendationswithrespecttosystemsissuesthathavethepotentialtohaveanareaorStatewidesignificance.
2. Complaints about patient care received in public hospitals can be made to the clinician concerned,thehospital,theAreaHealthServiceortheHCCC.IntheeventtheCECreceivesacomplaint it should be referred to one of the above.

5�
3. The HCCC has the primary responsibility for investigating serious complaints against individuals and initiating any necessary disciplinary action.
4.WhereaninvestigationbytheHCCCraisesquestionsofasystemicnature,andthoseissuesarespecifictotheindividualorganisationorpersonthesubjectoftheallegations,theHCCCshouldenterdiscussionswiththeCECastothebestforuminwhichtheyshouldbeinvestigated.
5.FollowinganydiscussionsbetweentheCECandtheHCCCwithrespecttoanyinvestigationbeingundertakenbytheHCCCwithsystemicimplications,andwhentheresultofthatdiscussionisthattheHCCCistocontinuethatinvestigation,anyrecommendationsmadebytheHCCCtogetherwithanyotherinformationrequiredbytheCECshouldbeforwardedtothe Clinical Excellence Commission.
6.WhileitisnotexpectedthatintheordinarycourseofitsworktheCECwillreceiveinformationconcerningtheconductofindividuals,shouldthatarise,theCECshouldreportanyconcernsit has to the Director-General of Health. The three levels of concerns set out in the November 2001DepartmentofHealthpublication“Modelpolicyonthemanagementofacomplaintorconcernsaboutaclinician”shouldguidetheClinicalExcellenceCommission.ItwillthenbeamatterfortheDirector-GeneraltoconsiderwhetheracomplaintshouldbemadetotheHCCC.
7. TheCECshouldhaveaccesstoallcomplaintdataheldbytheHCCC.ItwouldbeexpectedthatthatwouldamounttoasmallcomponentoftheinformationavailabletotheCECbecause,bydefinition,thatmaterialisbiasedtowardstheexceptionalortheegregious.Itwouldbeexpectedthatitsworkwouldbeinformedbyresearch,medicalliterature,itsownauditsandinformationgeneratedbytheColleges,tonameafewobvioussources.
8. The CEC should have access to all causation statements and recommendations made as a resultofarootcauseanalysisinNewSouthWales.
9.TheCECshouldnotbebound,astheHCCCis,byanyequivalentofsec91oftheHealthCare Complaints Act.
Theinquiryteamarguedthattherecouldbemanydifficultissuesinpractice.Itwouldbeextremely important to ensure there is good communication so that the HCCC involves the CEC indiscussionswhereacomplaintmaywellhaveasignificantsystemiccomponent.
Thestateofplayatmid2004
Chapter �4 contains information about the changes that had occurred since the time the incidentshadoccurredthatledtotheInquiry.TheinformationwasderivedfromseveralsourcesincludinginterviewswithseniorstaffoftheSouthWesternSydneyAreaHealthService,andvarious reports from bodies such as the Australian Council of Health Care Standards.
PerhapsthemostusefulpartofthisChapterisasummaryoftheconclusionsofareviewcommissionedbytheDepartmentofHealthandundertakenbyProfessorBarraclough,theChair of the Australian Council for Safety and Quality in Health Care. The report notes that the MacarthurHealthServicehadlowerratiosofstafftoinpatientbeddaysthansimilarhealthcareorganisations,andparticularlylowratiosofdoctors.Italsohadadisproportionatenumberofinexperienced staff.

52 Patient Safety: a comparative analysis of eight Inquiries in six countries
Weaknesseswereidentifiedincareprocessesincludingdischargeplanning,collaborationbetweenhospitalsandnonhospitals,andmultidisciplinaryteamwork.Particularmentionwasmadeoftheculturalproblems.Theyincludedalackofwillingnesstoencouragetheopendiscussionofproblemsin the interests of continuous improvement.
Mandatoryreportingofpatientsafetyproblems
InChapter15ofthefinalreport,theinquiryteamnotedthereweretwomainoptionswithregardtoreporting–voluntaryandmandatory.Voluntaryreportingmightinvolveamixofencouragement,persuasion,andassistancetoclinicians.Theinquiryteamnotedthat,atpresent,thereisavarietyofsystemsinplacethatincludecodesofconduct,contractualprovisions,andunwrittenprofessionalethical obligations.
Theinquiryteamwasunsureastotheappropriatenessofrequiringthereportingofproblems.Ifthisapproachweretaken,itwouldbenecessarytohavesanctionsfornoncompliancethatmightinvolvecriminalpunishment,removalofrightstopractise,orvariousfinancialpenalties.TheCommissionersaidthesesanctionswouldbeharsh“…andIsuspectnotfittingtothecrime.Ihavenotbeenpersuadedofthebenefitsofuniversalmandatoryreportingwithrespecttoalladverseeventsinhealth.”However,hesaidthatconsiderationshouldbegiventoincorporatingmandatoryreporting into health care organisations contracts. This seems an imprecise conclusion: mandatory reportingpresentsthesamegeneralproblemsregardingsanctions,regardlessoftheinstrumentsused to specify compulsion.
3.3 ConclusionsoftheInquiry
The conclusions may be grouped under four main headings: nurses’ allegations of poor care; the investigationsoftheHCCC;theinternalsystemsthatwereintendedtocontrolpatientsafetyinthetwohospitals;andthebalancetobestruckbetweenindividualclinicianresponsibilityandthesystemsviewoferrors.
SOMEOFTHENURSES’ALLEGATIONSOFPOORCAREMERITEDFURTHERINVESTIGATION
Manyoftheclaimsseemedtobesupportedbysufficientevidencetojustifytheirbeinginvestigatedfurther.Theinquiryteampresentedasummarytablethatshowspreciselywhichallegationsjustifiedinvestigationsbytheappropriatebody,andwhichdidnot.
Otherallegationsmadebythenurseinformantsweredismissed,mainlybecauseitwasnotpossibletofindadequateevidence.Inasmallnumberofcases,theinquiryteamconcludedtherehadbeenmisunderstandings,orthattheallegedbehaviourcouldbejudgedinappropriatebutnotdeservingofcensure.Anexamplewaswhereonedoctorwasaskedbyanotherdoctortomodifyheraccounttotheinquiryteamsothatitwaslesscriticalofthehospital’sperformance.
THEINVESTIGATIONSOFTHEHEALTHCARECOMPLAINTSCOMMISSIONWEREDEFICIENT
Thenurseinformants’dissatisfactionwiththeinvestigationsoftheHCCCwerelargelyjustified.Itsinvestigationswereinadequateinseveralrespects.Minorchangesmaybeneededinthelegislation,butthemainproblemwasthattheHCCCfailedtofollowtheexistinglegislationinthiscase.
THEHOSPITALSSHOULDHAVEHADBETTERWAYSOFHANDLINGPATIENTSAFETYPROBLEMS
ThemanagersattheCampbelltownandCamdenhospitals,andintheMacarthurHealthService,didnotactillegallyorinanunethicalway.Rather,theyfailedtoestablishadequatesystemsforpatient safety or failed to ensure compliance.

53
Manyoftheproblemsthatledtotheinquiriescouldhavebeenhandledthrough“...betterinternalhospitalprocedures,moreopendiscussionbetweenprofessionalcolleagues,andfullerdisclosurestopatientsandfamilies.”ImprovementsarealreadyunderwaywithintheMacarthurHealth Service that should address the inquiry team’s main concerns if they are appropriately implemented.
3.4 RecommendationsoftheInquiry
WenotedtheseveralrecommendationsonlegislativechangethatappearedinChapter4ofthefinalreport.ThelastChaptercontainstwootherrecommendations.
First,SouthWesternSydneyAreaHealthServiceshouldensurethatpoliciesareinplacethatareconsistentwiththeprinciplesintheseveraldocumentsnotedelsewhere.TheseincludetheOpenDisclosureStandard,BestPracticeComplaintsHandling,andtheModelforManagingConcerns about a Clinician.
Second,attentionshouldbepaidtorootcauseanalysis.Inter alia,teamsundertakingrootcauseanalysisshouldbefullyawareofthelevelsofseveritywithparticularreferencetotheguidelines regarding the conduct of an individual that should be referred to senior managers forfurtheraction.Theyshouldalsobeawareofconfidentialityguidelines–andparticularlytheneedtoprotectindividualsinaccordancewiththeHealthAdministrationActwhileensuringthere is publication of a causation statement and recommendations (and direct provision of the publication to involved patients).
Furthermore,areviewshouldbeconductedoftheeffectivenessofrootcauseanalysisaboutthreeyearsaftertherecommendedprotectionisprovided,inordertoensurethereisanappropriatebalancebetweentheusefulnessoftheinformationgeneratedandtheprotectionafforded.Finally,documentscreatedbytherootcauseanalysisprocessshouldbemadeavailabletotheHCCCwhenithasarelevantcomplaint.Thatinformationshouldnotbeadmissibleinstatutorydisciplinaryproceedingsorelsewhere.
3.5 Discussion
TheeventsatCamdenandCampbelltownhospitalssparkedaseriesofinquiriesandreviewswhichinturnresultedinsignificantchangestotheNewSouthWaleshealthsystemasawhole.TheInquiriesconductedbytheHCCCandtheSpecialCommissionwereonlythebeginning.ThesewerefollowedbyareviewbyParliamentaryCommitteesoftheHCCCanditsassociatedlegislation,aswellasaseparateParliamentaryreviewofcomplaintshandlingsystemsacrossNewSouthWales.
Ofthe47incidentswhichledtotheinquiriesatCamdenandCampbelltown,21werereferredtotheNSWCoronerbytheHCCCandtheDOH,withanadditionalfourcasesreferredbytheLeaderoftheOppositionandtheNewSouthWalesAttorneyGeneral.Afurther14caseswerereferredtotheCoronerbytheSouthWesternSydneyAreaHealthService(SWSAHS)ClinicalReferenceGroup.Anumberofthehealthprofessionalsinvolvedwerealsoreferredtovariousbodies.Intotal,15doctors,11nursesandonephysiotherapistwerereferredtotheHCCC.Ofthedoctors,fivewerealsosenttotheNewSouthWalesMedicalBoard.TheMisterforHealthatthetimeoftheeventswasreferredtotheIndependentCommissionAgainstCorruption(ICAC)overallegationsabouthisintimidationofthe’whistleblowernurses’asweretheoriginalallegations made by the nurses.

54 Patient Safety: a comparative analysis of eight Inquiries in six countries
DuringoraftertheprocessoftheinquiriestheCEOandtheentireBoardofSWSAHS,aswellastheHealthServicesCommissionerweredismissed,aswastheGeneralManageroftheMacarthurAreaHealthService(althoughshewasredeployedtoanotherAreaHealthService).TheNSWhealthsystemwasrestructured,reducingthenumberofAreaHealthServicestoeight.AsaresultoftheCommission’srecommendationstheClinicalExcellenceCommissionwasestablished,withresponsibilitiesaspreviouslydiscussed.Sotoowasastatewidesystemforassessingandreportingadverseeventswasinstigated,alongwithanobligatoryrootcauseanalysisprocess.
In2004,theNSWDeputyStateCoronerheldaninquestinto14ofthedeathsfoundthattherewasnofurthercauseforinvestigation.Anadditional20caseswerefinalisedbytheDeputyStateCoronereitherbyhisdispensingofholdingofaninquest,orbydecliningtoassumejurisdiction.ThefinalfivecaseswerestillunderinvestigationbytheNSWPoliceForceStrikeForceCossa.
ThelegislationdeterminingthepowersanddutiesoftheHCCCwasamendedandcameintoeffectin2005,givingtheHCCCthepowertorequiretheprovisionofevidence,includingalltypesofmedical,hospitalandpracticerecords.InformationcollectedbytheHCCCaspartofaninquirycannowbeusedindisciplinaryproceedings,althoughnotincivilorcriminalsuits.Whistleblowersweregiven extra protection under the act and the HCCC obliged to ensure that all relevant parties to an inquiry.
InSeptember2005ICACreleasedareportontheirinvestigationsofSWSAHS.Inthatreport(andassociateddocuments)theyexoneratedtheMinisterofchargesofintimidation,theHCCCCommissionerofchargesofcorruptionandfoundthattherewasno,orinsubstantial,evidenceofcorruptioningeneralatCamdenandCampbelltownHospitals.ICACalsofoundagainsttheallegationsthatthewhistleblowershadbeensubjecttoreprisalsandthatsomeofthenursesinvolvedhadbeenoffered’hushmoney’.Theydid,however,formallyreferallegationsofthefalsificationofpatientrecords,byadoctoratthehospitalstotheSpecialCommissionofInquiryintoCamdenandCampbelltownHospitals,whodeterminedthattheallegationoffalsifiedpatientnoteswarrantedinvestigationwithaviewtodisciplinaryproceedings,andsointurnreferredthemattertothe HCCC.
TheHCCCsentlettersto14ofthedoctors,ninenursesandthephysiotherapist,regardingtheirconductatCamdenandCampbelltown.Anotherthreedoctorsandfournursesreceivedpeercounselling.OfthedoctorssenttotheNewSouthWalesMedicalBoard,twoofthefivehavebeencleared of the complaints against them.
3.6 Referencesandselectedbibliography
FrankumB,AttreeD,GatenbyA,EagarS,AouadA,RosenfeldD,DewanPA,EllardJHT,VanDerWeydenMB.The“CamAffair”:AnIsolatedIncidentorDestinedtobeRepeated?Medical Journal of Australia, �80(7): 362-266.
Health Care Complaints Commission (2000). Investigation Report: Campbelltown and Camden Hospitals Macarthur Health Service. Sydney: Health Care Complaints Commission.
VanDerWeyden,M.B.(2004).The“CamAffair”:AnIsolatedIncidentorDestinedtobeRepeated?Medical Journal of Australia, �80(3):�00-�.
Walker,B.(2004).Interim Report of the Special Commission of Inquiry into Campbelltown and Camden Hospitals – 31 March 2004.Availableat:http://www.lawlink.nsw.gov.au/Lawlink/Corporate/ll_corporate.nsf/vwFiles/Interim_Report_31March2004.pdf/$file/Interim_Report_31March2004.pdfAccessed3March,2006.

55
Walker,B.(2004).Second Interim Report of the Special Commission of Inquiry into Campbelltown and Camden Hospitals–1June,2004.Availableat:http://www.lawlink.nsw.gov.au/special_commissionAccessedon4June,2004.
Walker,B.(2004).Final Report of the Special Commission of Inquiry into Campbelltown and Camden Hospitals – 30 July 2004.Availableat:http://www.lawlink.nsw.gov.au/special_commissionAccessedon10August,2004.
4 CeljeHospital,Slovenia
ThefollowingisasummaryoftheofficialreportonproblemsofpatientsafetyatCeljeHospitalinSloveniarelatingtopathology.Thereportitself,titledReport on the delays of the laboratory results at the Department of Morphology and Cytology at Celje Hospital, May 2003 is available in the Slovenian language onthewebsiteoftheSlovenianMinistryofHealth(SloveniaMinistryofHealth2003).Wewillrefertoitsauthorsasthereviewteambelow.
4.1 Context
AnoverviewoftheSlovenianhealthsystem
More detailed descriptions of the context are available in English in several documents available intheliterature.See,forexample,Keber(2002)andAlbreht,Cesen,Hindleetal(2002).ThisbriefsummaryistakenfromHindle(2003).
Whentheopportunityarosein1990,manyoftheconstituentpartsofYugoslaviawerereadytopresstheirlongheldaspirationsforindependence.Sloveniawasthemostfortunate:itwaswealthier,morehomogeneousinethnicandsocialrespects,andwasfirsttoestablishitself.
Itbeganitsindependencewithacomplicatedsystemofhealthinsurancethathadgrowninscopeandorganisationalcomplexityovertime.By1993,ithadenactedlegislationtocreateauniversalandcompulsoryhealthinsuranceschemeoperatedbyagovernmentagency,andcreated a small voluntary insurance sector mainly to cover copayments.
Before1990,thepatternofhealthservicesprovisionwaslargelybasedonpopulation-basednormsandwashighlyequitableforthemostpart.Serviceswerealmostexclusivelygovernmentowned,andhealthprofessionalssalariedemployees.Publichealthservicesandhospitalcarehaveremainedlargelyingovernmenthandssinceindependence.However,therehasbeenanincrease in non government participation in community based services (and especially primary medicalcare).Whethergovernmentsalariedorprivatepractitioners,GPsarepaidmainlyonacapitation basis.
Intotal,Sloveniawassensitivetoworldwidetrendsthatemergedinthemid1980s:economicrationalism; reduction of government involvement in (and hence responsibility for) health care; emphasis on organisation rather than clinical practice changes; and attempts to increase competitioninfinancing,purchasing,andcareprovision.However,itshistoryofsocialismandstrongsenseofnationalidentityweremitigatingfactors.Intheevent,thegovernmenthaschosentoretainitsdominantpositioninthehealthsector,whileencouragingahighdegreeofprivatisationelsewhere.

56 Patient Safety: a comparative analysis of eight Inquiries in six countries
ThepercapitaGDPofSlovenia(population2million)onlyfellmarginallyafter1990,andincreasedsteadilysincethentoreachUS$9800in2000.ThisplacesitbelowtheEuropeanUnionaverage,but higher than Greece and Portugal. It spends about 8% of GDP on health.
ThehealthstatusoftheSlovenianpopulationisrelativelyhighforseveralreasons,includingthesound investments that have been made in primary health care and environmental health. Slovenia hashadalonghistoryofsuccessfulpublichealthservicesandresearch,andhasalsoestablishedawelltrainedclinicalworkforce.
Thelevelofefficiencyofthehealthsectorisnotwellunderstood,butitappearstobehigherthanin all other transition economies in Central and Eastern Europe. Many efforts have been made tocontainhealthcarecosts,especiallysince1990,withmoderatesuccess.Forexample,ithasintroducedpercasepaymentofhospitalsbyDRG,andiscurrentlyredesigningmanyofitsservicestopromotecareintegrationacrosssettings.However,itsuffersfromremnantsofthesystemsandculturesestablishedinsocialistdaysthatfailedtoencourageandrewardinitiative.
QualityofcaremayapproachEuropeanUnionlevelsinsomerespects(Keber2002).However,thereisashortageofreliabledatathatispartlyaconsequenceofweaknessesinclinicalworkprocesscontrol.Amajorreformprojecthasbeenunderwaythatisdirectedatresourceallocationandcareprovisiononthebasisofclinicalpathways.
AshorthistoryoftheproblemsatCeljeHospital
TheInquiryaroseoutofsignificanterrorsmadebyCeljeHospital(theHospital)withrespecttotreatmentofpatientswhorequiredpathologytestsrelatingtoarangeofsymptomsincludingsuspected cancer. Most of the problems originated in practices of the Department of Morphology and Cytology (the Department) regarding the examination of tissue specimens and reporting of the results.
Theprocesswastypicalforhospitalsindevelopedandreasonablywellfundedhealthsystemswithwelltrainedstaff.Theattendingdoctorwouldorderatest,specimenswouldbetakenonthewardorintheoutpatientclinicanddispatchedwithatestorderformdefiningthepatient,theresponsibledoctor,andtypeofinvestigation,thespecimenwouldbetested,areportwouldbewrittenbyapathologist,andthereportdeliveredtotheorderingdoctor.Therewastheopportunitytoindicatethedegreeofurgencybutitwasrarelyrelevant.Theorderingdoctorassumedthatthepathologystaffwoulddotheirbestwiththeirlimitedresources,andanywayitwouldnotbeappropriatetointerferein their decisions.
OnefeatureisworthmentioningthatdifferentiatesthetypicalprocessinSlovenianrelativetoOECDhospitals,atleasttoasmalldegree.NursingstaffinSlovenianhospitalsaremorelikelytoactinsupportingadministrativeroles.Thisisareflectionofthepossiblygreatergapbetweendoctorsandnurses.Inshort,someadministrativetasks(inthiscase,thecompletionanddispatchoftheorderformandspecimentotheDepartment)arehandledbynursesthatwouldbemorelikelytobehandledbytheorderingdoctororajuniordoctorelsewhere.Thismaybeofrelevancehere,because it adds more people to the chain of communication.
ActivitiesintheDepartmentwerethemselvescomplicatedandpoorlycoordinated.Forexample,therewaspoormanagementofworkflows,allocationofworkloads,andmonitoringofperformance.Ofparticularrelevancehere,theassignmentofworktothetwofulltimepathologistswasmanagedinalargelyidiosyncraticway.Unprocessedtestresultswereallowedtoremaininaseriouslyunbalancedstateforseveralyears.Themainproblemwasnot,however,inappropriateallocationof

57
theworkbutratheragrossimbalanceintherateofprocessingbythetwopathologists.Themainconsequencewasanaccumulationofunreportedtestresultswithoneofthepathologists.
Delaysinthereturnofthepathologists’reportswereconsequentlycommon.Inthesecircumstances,itwasusuallytheorderingdoctorwhotookaction.Inprinciple,theorderingdoctor(oranotherclinicianattheorderingdoctor’srequest)couldtelephonetheDepartment,askaboutthecurrentstatusofthereport,andifnecessarytalkdirectlytothepersonbestabletoclarify the situation.
Inthecaseunderstudy,themostappropriatepersonwasthepathologistwhowasbuildingthebacklogofunreportedtests.However,thisrarelyresultedinanadequateresponse.Itdid,however,resultinasenseofdisturbanceofthepeace(thestateofuneasycoexistenceofthetribes)andthereforeovertimethedirectrouteoftelephonecommunicationwithpersonresponsibleforthedelaybecamearareevent.Itwasmoretroublethanitwasworth,especiallyinviewofthefactthattheprocessoftelephoneinquirywastimeconsumingandoftenunsuccessful.Asiscommoninsuchcircumstances,theweaknessesinthesystembecameacceptablebecausetherewasnosolutionapparenttothoseinvolved.Overtime,theweaknessesceasedtoberecognised.
The most common method of inquiry about delayed results came to be through a less direct channel:theresponsibledoctorwouldrequestactionbythenursingstaff;thenursingstaffwouldtelephonetheadministrativestaffintheDepartment;theadministrativestaffwouldwriteanotetothepathologist;andthepathologistwouldthenreadthenoteandpassamessagebackthroughthesamechannels.Sometimesthepathologistwouldfailtorespondatall.Inothercases,hewouldgiveexcusessuchaspressureofwork,andonoccasionshewouldplacetheparticularorderhigherinhisprioritylist.Apartofthegamewasanimplicitacceptanceoftherulethat,ifoneoffendedthepathologist,thismightmeanalossoffavourabletreatmentinfuture.Anotherrulewasthatitwaseasierinmanywaystoacceptthantochallengetheexcuses.IfthepathologistweretogivetheexcusethattheDepartmentisunderfundedandoverworked,itisplausibletomostpeopleinanorganisationwithacultureofblamingallinternalproblemsonexternalagencies–theignorantinsurers,thetraitorousMinister,orthepatientswithunreasonableexpectationsandunwillingnesstopaytoobtaincarefromtheprivatesector.
Theabilityofcleverpeopletobeabletoacceptillogicalbutmorecomfortableanswersiswellillustratedinthereviewteam’sreport.Itnotedthattheorderingdoctorswerefrequentlyirritatedbytheabsenceoftimelyresults.Thereviewteamreportedthatthisledthedoctorsfromtimetotime“…toexpressformalandinformalcriticismsofmostofthestaffintheDepartment,butnotofthepathologistwhowasresponsibleformostoftheproblems.”ItbecameclearduringthesubsequentInquirythattheorderingdoctorsweremostlywellawareoftherealcause.
Indeed,thereviewteamconcludedthatnearlyeveryoneinvolvedwasawareoftheproblems.“ThepathologistsintheDepartmentknewaboutthedelaysasdidthedoctorswhoorderedthetests,theheadsofdepartments,thehospital’sMedicalDirector,theexecutivecommitteeoftheHospital,thenurses,thelaboratorytechnicians,andotherstaff.Yet,theproblemremainedunsolved.”
Overtime,itbecameanunspokenbutalmostuniversallyacceptedruleofoperationthattests,whenordered,shouldnotbeexpectedtobereceivedontime–orindeedreceivedatall.Thismayseemsurprising.However,similarlyillogicalbehavioursarecommoninallsystems.Thepatternsofillogicalbehaviourareeasiertosee(oraremorelikelytobeunacceptable)insystemsotherthanone’sown.

58 Patient Safety: a comparative analysis of eight Inquiries in six countries
ThepatternofacceptanceextendedtoseniormanagersintheHospital.Fornearlyadecade,theHospital’s managers made no serious attempt to enquire formally into the problem. From time to time,thematterwasraisedandthenexcusesweremade:weareunderfunded;wecoulddisturbrelationswithmedicalstaffatatimewhentherearemoreurgentmatterstoattendtothatrequirethedoctors’support;wedonothavethedata;moreresearchisneeded;andsoon.
TheHospital’sBoardofManagementclaimeditdidnotknowofthesituation,exceptinoutline.SomeBoardmemberssaidduringtheInquirythattheyhadheardtherewasaproblem,butseniorexecutiveshadadvisedthemthatitwasprobablyminorortemporary.
ThereviewteamconcludedthatBoardmembersandseniorHospitalexecutivesshouldhaveknown–itwouldhavebeeneasytofindout.Atleastsomeofthemknewenoughtohavebeenconcerned,butpreferrednottotaketheleadinfindingoutforsure.Thereviewteamwrotethat“…themostdisturbing aspect is that hospital managers did nothing.”
Processesforthecontrolofclinicalwork
Thereweresevenmainsystemsinplacetocontrolclinicalwork–andhencetoavoidtheproblemsthatarose.Indeed,inSloveniathesystemsarerequiredbylaw.
Allofthemwereseriouslyinadequate.First,therewasasystemofinternalaudit,operatedbyasetofwhataretermedClinicalExpertsSupervisoryCommitteeslinkedthroughaClinicalCouncil.Eachcommitteehadcleartermsofreference,similartothoseofqualityassurancecommitteesinAustralianhospitals.ThustherewasacommitteeattheHospitalthatwasspecificallyrequiredtomonitorthequalityofpathologyservices.Itsmembershipincludedseniorstaffwithclearresponsibilities to the Board of Management for supervision of quality. It also included clinicians directlyinvolvedintheprocessesofordering,undertaking,reporting,andanalysingresultsofpathologytestsonadailybasis.Changesweremadein1995toimprovetheprocesses,butthereviewteamobservedthattheywere“…carriedoutonthebasisofgutfeeling”.
Second,therewastheSlovenianMedicalAssociation,whichisrequiredbylawtotakeresponsibilityfor the establishment and monitoring of professional matters. Processes in place included the right toundertakeinquiries,toencourageandthenreviewcomplaintsfromhealthprofessionalsandpatients,periodicreviewoftheperformanceofteamsandindividualclinicians,provisionofadviceasrequired,andthereportingofconcernstotheMinistryofHealthwhereperformanceplacedpatientsafetyatrisk.
Third,thereweretheindividualspecialtyassociations.Inthiscase,thesocietiesofpathologyandoncologywereclearlyexpectedtoexertsomedegreeofcontrol.However,ashascommonlybeennotedelsewhere,theassociationsactedtocontroltherisksofadversepublicity(andtoprotecttheirmembers’ livelihood) rather than to protect patients.
Fourth,thereisroutineadministrativesupervisioncarriedoutbytheMinistryofHealth.ThistakesmanyformsandincludestheappointmentofaseniorMinistryofHealthofficialtothemanagementboards of care provider agencies.
Fifth,therearevariouscontrolmethodsappliedbytheHealthInsuranceInstituteofSlovenia.Thisis a semi-independent agency that acts as the primary purchaser of services from health care organisationsthatarecoveredbythenationalcompulsoryhealthinsurancescheme.Itspowersaresignificantinprinciple:itisempoweredtoauditcareanddenypaymentsifitisjudgedtobeinappropriate. It can (and does) negotiate the inclusion of particular standards of care into the annualpurchaser-providercontracts.Ithasalargeteamofauditors(predominantlydoctors)whohavethepowertorequirethesubmissionofclinicaldocumentationforreviewandtomakesite

59
visits for inspection purposes. Health care organisations regularly complain about the excessive poweroftheauditorsandthedegreetowhichtheyexaminethedetailsofindividualpatientcareepisodesbeforeapprovingpayment.However,ithasbeenobservedthattheinspectionmethodshavesystematicweaknessesincludingadominantinterestincontrollingcostsratherthancontributingtoimprovedqualityofcare.Ithasalsobeenclaimedthatthereisalackofevidenceagainstwhichtheappropriatenessofcareisjudged–muchoftheauditingdependsontheapplicationoftheauditors’personaljudgementstotheretrospectivereviewofindividualcases.TheproblemsattheHospitalseemtosupporttheclaimofineffectiveness,atleastintermsofidentifying problems of patient safety.
Sixth,thereareperiodicexternalauditsinwhichparticipationisvoluntaryforthemostpart.Forexample,theHospitalunderwenttwomajorreviewsduringtheperiodthatdemonstrablypoorcarewasbeingprovidedbytheDepartmentundertheauspicesoftheEuropeanFoundationforQualityManagementpilotstudyforanExcellenceAward.ThereviewersnevercameacrossanyproblemsintheDepartment.Asitwasaselfassessmentexercise,noneoftheproblemsofdelayedlaboratoryresultswerereported;theevaluatorsdidnotfindoutaboutthepoorqualityofcare or severe problems.
Finally,therearesystemsintheDepartmentitselfthatwereintendedtoimprovecontrolofwork.Theyincludedrelativelysophisticatedequipmentwiththeabilitytocompilecomputerrecordsandhenceprovidemanagementinformation.However,duringtheperiodunderstudy,theDepartmenthadhardlyanyauditableperformancestandards,noshort-orlongtermplans,andkeptnoformalrecordsofmeetings.
Towardspublicdisclosure
Itisnotentirelytruethat“…hospitalmanagersdidnothing”formorethanadecade.Rather,theydidaslittleaswasjudgednecessarytokeeptheproblemundercontrol(ratherthanasmuch as possible to solve it).
Thefirstsignsofconcernamongpatientsappearedin1994.Therecordsarepoorregardingthedetails.However,itiscertainthatthenumberofcomplaintsincreasedafterthat,probablybecauseconcernsspreadbywordofmouthamongpatientsandtheirfamilies.Confidentialcommentsbysomenursesarelikelytohavestimulatedthepatientsandfamiliestoact.Asiscommoninmosthealthcaresystems,nursesaremoreeasilyapproachableandmorelikelytospeakthetruth–atleastwithregardtodoctors’behaviour–ifthereislittleriskofbeingidentifiedasatroublemaker.
TheHospitaltookvariousstepstocontrolthepublicitythatwerelargelysuccessful.Theyincludedtheconductofaninquiry,theimprovementofinternalsupervisionprocesses(atleastinprinciple),andcounsellingpatientsandfamiliesaboutthelackofevidencethatanyofthecarewasinappropriate.Incontrast,theHospitaldidalmostnothingtodefineandresolvetheunderlyingproblems.Forexample,noattemptwasmadepreciselytomeasurethenumbersandtypesofteststhathadnotbeencompleted.Therewerenowrittenreportsonthenatureandsizeof the problem.
Theerrorscontinuedtooccurafter1994,andtherewereperiodicincreasesinrisksofpublicdisclosure.Therewasanincreaseininternalconcernsin1999,whentherewasachangeinthemanagementoftheDepartment.Thisledtodecisionstoreducethedelaysinfuture,andthesewerelargelysuccessful:theratesofdelayandnoncompletiondeclinedsharply.However,thenewmanagerstoppedshortofreviewingthepreviousproblems.Itwashopedthattheremainingbacklogwouldlargelyremainunnoticedandtheunderlyingcauseswoulddissipateinduecourse.

60 Patient Safety: a comparative analysis of eight Inquiries in six countries
Thiswasunfortunatebecausemuchwouldhavebeenlearnedaboutwaysofavoidingsimilarproblemsinfuture.Moreover,itwouldhavebeenappropriatetoconsidertheextenttowhichpreviouspracticeshadharmedpatients,particularlyinviewofthefactthatmanyrecentpatientsmightcontinuetobeexposedtorisksthroughtheabsenceoftestresults.
In2001,theMedicalDirectorreachedagreementwiththeClinicalCounciltoincreasethedegreeandrigourofperiodicinternalreviews.InJanuary2002,theMedicalDirectordeterminedthataformalinternalinquiryshouldtakeplaceregardingpathology,whichatleastacknowledged(butunderstated)theproblems.TheMedicalDirectorthentookthefirstformalactiontoinformtheoutsideworld:hewroteaconfidentiallettertotheSlovenianMedicalChamber–theofficialbodyresponsible for medical professional matters that is roughly equivalent to the Medical Council in theUK.TheletterwasdirectedtotheEthicsCommitteeoftheMedicalChamber,andsuggesteditmightwishtoconsiderwhetheractionswereneeded.
Foramixofreasons,theMedicalChambertooknoofficialactionforsixmonths.Itisunclearwhetheritwouldeverhaveacted,becauseitsdeliberationswereovertakenbyevents:thestorybrokeinthemassmediainearlyOctober2002.
Thecircumstancesarenotentirelyclear,buttheweightofevidenceisthatitfinallybecameevidentthatthemattercouldnotbecontained.OneofthecontributingfactorswasameetingbetweentheHospital’sGeneralManagerandtheBoard,atwhichhewasinformedhiscontractwouldnotberenewed.Beforeleavingthebuilding,henotedsomeproblemsthattheBoarditselfshouldhaveidentifiedandassistedwithresolution,includingtheunprocessedpathologyreports.Onestepledtoanother,andinterestedpartiesbegantobecomeextremelyactiveinanticipationofopeninvestigations.Itwasthereforeonlyamatteroftimebeforethemediabecameinvolved.
TheMinisterforHealth,adistinguishedclinician,tookimmediateaction:hehadnotpreviouslyknowntherewasanykindofproblem.HerequestedareportfromtheHospitalandimmediatelyappointedaCommitteeofInquirywithinvolvementoftheMedicalChamber.ShortlyaftertheCommitteebeganwork,thePoliceannounceditwasinitiatinginvestigationsinresponsetopubliccomplaints. The Ministry of Health and the Police held discussions and agreed a collaborative processwherebyanylegalactionswouldbedelayeduntilatechnicalinquiryhadbeenconducted.However,thePolicewouldremainfullyinformedoftheInquiry’sprogress.
4.2 TheInquiry
Thereviewteamactedwithconsiderablespeedanddiligence.Itconducteditsinitialinvestigationsoveraperiodoffourweeks,includingsitevisitsandinterviews,andprovidedaninitialreportforcommentbytheHospital.Carefulreviewsweremadeoftheclinicalrecords,questionnaireswerewidelydistributedtoHospitalstaffandtheresultsanalysed,opinionsweresoughtontheinitialfindingsfromtheAssociationofPathologistsandForensicMedicine,andmembersoftheHospitalBoardwereinvestigated.
TheMedicalChamberwasfullyinvolved,anditscommentsweretakenintoaccountatallstages.Indeed,itwasrequestedtoprovidewrittencommentsatseveralstagesinparttoensurethatthefindingsofthereviewteamwouldbeendorsedbytheMedicalChamberoncetheybecamepublic.
Thereviewteamestablishedarigorousandlogicalmethodofinvestigation.First,itexaminedperformance in terms of the processing of pathology tests. A total of 28�5 delayed or incomplete test reportswasidentifiedintheperiodbetween1985and2000.Thiswasfarmorethanwasestimatedfromallotherhospitalsoverthesameperiod,andentirelyinconsistentwithestablishedguidelinesfortheSlovenianhealthcaresystem–andindeedwiththeHospital’sownstandardsandoperatingrules.

6�
Second,allplausiblehypothesesthatmightexplainthepoorclinicalpracticeweretested.Theseincludedattemptstoassociatetheerrorswiththevolumeortypeofpathologytestingundertaken.Thiswasinherentlysensible.Itwasalsounavoidableintheevent,becauseitwasrepeatedlyclaimedbysomepartiesduringthecourseoftheInquirythattheworkloadwasexcessive,andthiscontributedtothebacklogoftesting.Theclaimwasquestionableintheextreme:iftheworkloadwereexcessive,itwouldbewithinthepoweroftheHospitaltomakeformalcomplaintstofundingagencies.Moreover,itcouldsimplyhaveturnedpatientsaway,thusgivingthepublictheopportunitytoregistertheirviewsaboutresourcing.
Nevertheless,thereviewteamcorrectlychosetotaketheclaimsseriously,andthereforemadeavarietyofanalysestotestitsveracity.Forexample,workloadswerecomparedacrosspathologistsandovertimeattheHospital,andcomparedtotheworkloadsoverthesameperiodatotherhospitals.Theinternationalliteraturewasreviewedtoassessdifferencesinworkloadsandclinicalpractice.Intheseandothercases,thehypotheseswererejected.TheHospitalhadanaveragevolumeofworkperpathologist,comparedwithotherSlovenianhospitals.ThetotalworkoftheHospitalfluctuatedovertheperiodfrom1985to2000,butthenumberoferrorswasnotassociatedinanysignificantway.Thenumberoferrorsbypathologistwasunrelatedtotheirindividualworkloads.
Inshort,manyhypothesesweretestedandsubsequentlyrejectedandtheonlyonethatwassupportedbytheevidencewasthatoneseniorpathologisthadbeeninefficientorotherwisehadfailedtoperforminaccordancewithreasonableexpectations.Itisinterestingthatthesamepathologisthadbeengivenanationalawardin2002fordistinguishedservicetothehealthofSlovenians.
Thereviewteam’sfinalreportwaspresentedtotheMinisterinMay2003,sevenmonthsafteritbeganitsinvestigations.TheMinistertookoneweektoreviewthereport,andissuedhiscommentsinwritingandthroughapressconference.Thereportwassubsequentlythesubjectofintensereviewanddiscussioninthemedia.Theheadlineinthemainnationalnewspaperonthedayafterthepressconferencesays“Ministerblamesthesystem”.
4.3 ConclusionsoftheInquiry
Therearemanyrelatedconclusionsthatreflectthelinkagesbetweentheunderlyingcauses.Wehavearrangedthemundersixheadingsbelow,buttheyarenotmutuallyexclusive.
Managementinformation
Withregardtoinformation,thereviewteamnotedtherewashardlyanythatmightfacilitatethemonitoringofperformance.Itexpressedtheviewthatinformationsystemsabletosupportbothinternalandexternalbenchmarkingneededtobeestablished.Thisshouldbepossibleby2005,bywhichtime“…thehospitalaccreditationprocesswillhavebeenestablished.”
However,thismightbemissingthemainpoint:informationindicatingthatperformancewaspoorwaseverywhere–manycliniciansknewitforsure;manypatientswereawaretherewereproblems;andthemassmediafounditimmediatelytheywereadvisedtolook.Asnotedelsewhere,hospitalswheresimilardisastershaveoccurredhavetypicallypassedsuccessfullythroughaccreditationprocessesduringtheperiodswhenpoorcarewasbeingdelivered.Theproblemishardlyeveralackofdatabutratherareluctanceorinabilitytoactonthem.

62 Patient Safety: a comparative analysis of eight Inquiries in six countries
Authority,responsibility,andaccountability
Forthemostpart,thereviewteamdidnotbelievetheproblemswerecausedbyindividuals.Inthisrespect,itsconclusionsareverysimilartothosefrominquiriesinothercountries.Forexample,theinquiryreportnotesthat,likeBristol,thiswas“…notastoryofgoodorbadpeople,orgoodorbaddoctorsandnurses.Itwasnotastoryaboutpeoplewhointentionallywantedtoharmpatients.”
Itwasnotedthatmostdoctorsappearedtotakeseriouslytheirresponsibilitiestotheirownpatients.Forthemostpart,theyappearedtoordertestsappropriately,tissuesampleswerecompetentlytaken,testingwashandledineffective(althoughnotalwaysinefficient)ways,testresultswerecompetentlyanalysed,andsensibledecisionstakenregardingsubsequentcare.Theproblemslaymostlyattheinterfaces.Forexample,iftestresultswerenotreturnedinatimelymanneritwasassumedthateitherthedelayswereunavoidableorthatsomeoneelsewouldnotetheproblemandtakeappropriateaction.Itwasrarethatcomplaintswereopenlymade(althoughmanydoctorsinformallyadmittedtheirongoingconcerns).Overtime,whatmighthaveseemedatfirsttobeintolerable performance became the accepted norm.
Thereportidentifiedtwoimportantaspectsofmedicalculturethataffectedviewsaboutresponsibility.First,theindividualdoctorsbelievedtheirworkshouldnotbesubjecttooversightbyanyoneelse:unlike(say)nurses,doctorsspokeof‘mypatient’ratherthan‘ourpatient’.Thiswasassociatedwiththebeliefthat,ifonedoctor’sworkshouldnotbethesubjectofcommentbyotherdoctors,thenthatdoctorshouldextendthesameprivilegeofautonomytoallotherdoctors.Second,therewasnoonewhobelievedheorshehadaresponsibilitytomanagetheentireexperienceofpatientsfromadmission to discharge.
Thesignificanceofmedicalculturewasstronglyemphasisedinthereviewteam’sreport.Theynoted,forexample,thatmanyoftheHospitalstaffinterviewed(fromvirtuallyeveryprofession)volunteeredtheopinionthat“…protectionofmedicalascendancywasfarmoreimportantthansolvingtheproblem.”
Theweaknesseswerenot,however,restrictedtomedicalculture.Nurses,doctors,administrators,and other groups did not have a common understanding of the distribution of responsibilities. For example,nursesdidnotbelievetheywereresponsibleforcommentingonerrorsmadebyseniordoctors.Administratorsatalllevelsdidnotbelieveitwastheirresponsibilitytocriticiseclinicalpractice.Thereviewteamsaidthatmedicalculturewasdefinedlargelybyasenseofindividualautonomy,andthat“…tribalbehaviourwasfartoodeveloped.”
Thereportsaysthat,althoughoneofthepathologistswasthemostculpable,thesystemasawholewasatfaultinthat“…itwasdesignedtopreventsuchasituation.ItispreciselybecauseofthelackofasuccessfulsupervisionandundefinedprocessesthatitwasnotpossibletofindoutwhatwasactuallyhappeningwithinDepartment.”
Arelatedconcernwasthat“…powerwasinthehandsofafewpeople”andthattherewasamismatchbetweenpowerandresponsibility.Further,responsibilitywasnotclearlyassociatedwithaccountability.Somedoctorsclaimedtheywereaccountableonlytotheirpatients.Evenwheretherewasademonstrablecommitmenttoaccountability,however,theprocesseswherebyitwasexercisedweregrosslyinadequate.
Forexample,ifadoctorwishestobefullyaccountabletohisorherpatients,theremustbeaprocesswherebyitoccursinasatisfactoryway.Forthemostpart,patientsdidnotknowtheyhadarighttoreviewtheirdoctors’actions.Wheretheywereawareoftheirrights,therewerenoadequateprocesseswherebypatientswereadvisedandsupportedinestablishingaprocesstoexercisethose

63
rights.Theywerenotinformedaboutnormalpracticesofcareprovision(whattheyhadarighttoexpect),orofwaysofinterrogatinghealthcareorganisationssotheymightdeterminewhethercareprocesseswereadequate.
Intotal,thereweremismatchesbetweenpower,responsibility,andaccountability.Thosewiththemostpowerdidnotalwaysacceptresponsibility,andtheywerehardlyeveraccountableinasatisfactoryway.Thereportsaidthat“...itwasrarelyclearwhowasresponsible,andthoseincharge largely ignored their responsibilities.”
Inadequateempowermentofpatients
Whileafewpatientstookaction,andthereforecontributedtopublicdisclosureofthesituation,mostsimplyaccepteddoctors’explanationswithoutquestion.Thereviewteamreportedthat“…mostpatientswereconvincedthatthelevelofcaretheyreceivedwasgood.Theytrustedthehospital.Nooneknewthingswerenottakencareofproperly.”
Itwasnotedthatpatientempowermentwasgenerallyunsatisfactory.Anexamplewasgivenofthesituationwhereresultsweredelayedindefinitelyandpatientsaskedwhy.Thereviewteamreportedthatitwasnotuncommonfortheresponsibledoctorsimplytosaythat“…itisnotmyfaultifthepathologyresultsarenotready”and“thatthepatientshouldtelephonetheDepartmentifheorshewantedsomethingdone.”
Onrareoccasions,patientsbecameincreasinglycomplainingofdelays.Insomeofthesecases,itbecamethepracticetoreturntheirsamplesandsuggestthepatientsshouldthemselvestakethemtoanotherlaboratoryelsewhereforexamination.
AsthetruthprogressivelybecameevidenttolargenumbersofHospitalstaff,therewastheopportunitytoacceptsomeoftheresponsibilityandatleasttoapologiseinageneralway.Thereviewteam’sreportnotes,however,thatthiswasnothappeningeveninthelastphasesoftheirwork.“No-oneapologisedtothepatients,eventothosewhohadsubsequentlybeenfoundtohave been seriously harmed.”
Discouragementofcomplaints
Therewasanorganisationalculturethatdiscouragedtheadmissionoferrors.Staffwerediscouragedfromraisingproblems,andparticularlyfromraisingproblemsthatimpliedmedicalmistakes.“Ifanyonedidcomplain,no-onetookanynoticeornoonetookthecomplaintseriously.”Therewasasensethat,ifcomplaintsweremaderepeatedly,itwasasignofincompetence or disloyalty.
Afailuretouseformalinstructions
Mostoftherulesandguidelinesregardingoperationofpathologyserviceswerenotwrittendown.Iftheyhadbeenwrittendownatsomestage,theoverwhelmingmajorityofstaffwouldnothaveknownwheretofindthem.Wherechangesinproceduresweretobemade,theadvicewasalmostalwaysprovidedorally.
This appeared largely to be a consequence of the dominance of medical culture. Senior doctors werenotexpectedtohavetomaketheefforttowriteinstructionstosubservientstaff(meaningineffectalmosteveryone).Ifsubservientstaffwishedtomakenotesbasedonoralinstructions,theymightdosooftheirowninitiative.

64 Patient Safety: a comparative analysis of eight Inquiries in six countries
Adifferentviewofmanagement
Therewasanalmostcompleteabsenceofrecognitionthatclinicalworkneededtobecollectivelymanaged,atleastinpart.Oneofthepathologistsnotresponsiblefortheerrorsbecameincreasinglyconcerned – not only about the incomplete tests but also of other aspects of pathology services. In1996(andagainin1997)heraisedhisconcernswithseniorhospitalmanagersandproposedthathisownworkloadbereducedsohemightdevote30%ofhistimetoclinicalmanagement.Hisproposalswererejectedonthegroundsthattherewereseriousbudgetaryproblems.TheHospitalwasinfactexperiencingdeficits,butshouldhavebeenabletomanageaseffectivelyasotherhospitals given the essentially equitable methods of resource allocation.
A more appropriate response from Hospital managers might have been increased effort to control thewaste.However,thepathologistwasgiventhemessagethathisadviceonbudgetplanningwasnotappreciated.Theinseparablelinksbetweenfinancialandclinicalmanagementwereignoredoratleastundervalued.Thereportsayssimplythat“…systems,processesandavailableresourcesinfluencethequalityofworkwithintheinstitutionaswellascareitself.”
4.4 RecommendationsoftheInquiry
Therecommendationsofthereviewteammaybeeasilydeducedfromitsconclusions.Thecentralrecommendationwasthattheremustbeimprovementsinclinicalteamwork.Thisdependsonincreasedunderstandingandrespectofdifferencesbetweenclinicalprofessions,establishingforumsinwhichmultidisciplinaryteamscanopenlydiscussmultidisciplinaryproblems,therefocusingofattentiononthepatientandawayfromprofessionandenterprise,establishingaviewthatadmissionoferrorsisasignofstrengthratherthanofweakness,andsoon.Thepatient“…mustbeplacedatthecentreofthecareprocess.”Mistakesareinevitable,andwhentheyoccurweshouldlearnfromthem.Wemust“…avoidplacingtheblameonindividuals,andinsteadinterpretthemassystemproblemsforwhichweareallresponsible.”
Thereviewteamreferredseveraltimestotheneedtoacceptthatchangesinclinicalculturewilltakesometimeandeffort.However,itenvisagedthepotentialforearlyimprovementsmainlybymakinggreateruseofclinicalpracticeguidelinesandclinicalpathwaysaspracticalmanifestationsofanewformofclinicalculture.Theseinstruments“…arenotmagicians’wands,buttheycouldhavesolvedmanyofthecomplexitiesthatledtobadcareattheHospital.Atpresenttherearenobetterwaysanywhereintheworldtomoveforwardinprovidingthekindofcarethatallcitizenshavearighttoexpect.”
Littlewassaidaboutthecontextwithinwhichchangesinclinicalpracticeshouldbemade.However,thereviewteamsaidthat“…itisimportanttodefinethemissionoftheHospitalandshareitwithallstaff.”Thereshouldbemoretrustandmorecommunication.Forexample,itwouldhelpif“…awardsforeffectivework…aresharedamongallstaff,ratherthanonlytotheBoardofManagement”andthatthepracticeofpassingtheblamedownwardsweretocease.TherewasalsoanacceptanceofthecontributionofotherelementsofthesystemtowhathadhappenedatCeljeHospital.“Changesneedtotakeplaceatalllevelsfromthegovernmenttocareprovideragencies.”Moreover,patientsneedtobekeyplayersintheprocessofreform.Itwasnotonlynecessarytoprovidecarewithrespectandhonesty,butalsotoincorporatepatientsineveryprocessfromplanningtoevaluation.

65
4.5 Discussion
Oneofus(ProfessorHindle)wasworkinginSloveniain2002,whenrumoursaboutthepossibilityofareviewwerebeginningtocirculate.Hewasinvitedatthattimetomakeapresentation at a conference of hospital directors in Ljubljana and he chose to describe the case ofpaediatricsurgeryattheBristolRoyalInfirmaryandaskwhetheritwasrelevanttoSlovenia.OnehospitalGeneralDirectorsaid“…youhavepretendedtotalkaboutBristolbutyouareactuallyholdingupamirrorinwhichwemightseeourselves.”HehappenedtobetheGeneralDirectorofoneofthebesthospitalsProfessorHindlehasseenanywhereintheworld.
Thisseemsrelevantintwoways.First,theCeljeHospitalstorysayslittleabouttheSlovenianhealthcaresystemandmuchaboutproblemsofhealthcareanywhereintheworld.Second,therearewaystomakeradicalimprovements;eveniftheworldisunkindasmallgroupofhospital staff can start a revolution if they have the understanding and the commitment to do so.
Shortlyaftertheofficialreportwasreleased,theMinistryofHealthintroducedarequirementinthehospitals’annualagreementswherebytheywouldeachperformaselfassessmentoftheappropriatenessofadmissionsmakinguseofanadaptationoftheAppropriatenessEvaluationProtocol(Ceglar,Hindle,andMarusic2003).Mosthospitalsreportedlowlevelsofinappropriateadmission,buttherewasanoutlier:whathadappearedtoProfessorHindletobethe best hospital had the highest rates of error. The Ministry of Health subsequently introduced anadditionalbudgetelementfromwhichfundswereallocatedindirectproportiontothesizeofthereportederrors.Therearetwowaysofinterpretingthis:thatthehospitalswiththeworstperformancewerebeingquiteinappropriatelyrewarded;orthattheMinistrywasmakingasmallcontributiontochangingtheculturewherebyadmissionoferrorshasinthepastledtopenalties.Thelatteristhecorrectinterpretation,andthissuggeststhatSloveniaisontherighttrack.
4.6 Referencesandselectedbibliography
Albreht,T.,Cesen,M.,Hindle,D.,Jakubowski,E.,Kramberger,B.,Petric,V.K.,Premik,M.andToth,M.(2002).Health Care Systems in Transition: Slovenia. Copenhagen: European ObservatoryonHealthCareSystems,WHORegionalOfficeforEurope.
Ceglar,J.,Hindle,D.andMarusic,D.et al (2003). Controlling Admissions to Hospital: A Trial of a Modified Utilisation Review Protocol in Slovenia. �9thPatientClassificationSystemsEuropeConference,WashingtonDC,08.-11.October2003.
Hindle,D.(2003).AComparisonofHealthInsuranceinSloveniaandCroatia.Australian Health Review, 26(�):�06-�5.
Keber,D.(2002).HealthCareinSlovenia.Australian Health Review,25(3):1-5.
Slovenia Ministry of Health (2003). Report on the Delays of the Laboratory Results at the Department of Pathology-Morphology and Cytology at Celje Hospital, May 2003. Available at: www2.gov.si/mz/Accessedon10December,2004.

66 Patient Safety: a comparative analysis of eight Inquiries in six countries
5 Glasgow’sVictoriaInfirmary,Scotland
5.1 Context
Severalinquiries,bothformalandinformal,tookplaceinScotlandin2002and2003withregardtooutbreaksofhealthcareassociatedinfection(HAI)thatoccurredoverseveralyears.Actionsweredeemednecessarymainlybecauseofwidespreadpublicconcern(andmassmediainterest)thatarosefromtheoutbreaksofsalmonellainfectionattheVictoriaInfirmary,Glasgow,inDecember2001andJanuary2002(Meikle2002).Threepeoplediedandalargenumberwereinjuredorplacedatrisk.
5.2 TheInquiry
Themaininstrumentofinquirywasagroup(hereaftercalledtheinquirygroup)thatwasestablishedbyNHSScotlandunderthechairmanshipofDrBrianWatt(2002).Asaconsequenceofpublicationofitsreport,theMinisterforHealthandCommunityCarecalledaConventionofexpertsandinterestedpeoplefromacrossScotlandinJune2002,towhichseveraloverseasexpertswerealsoinvited(NHSScotland2002).InthefollowingsectionwesummarisetheWattReport.Insection5.6,footnotes,weoutlinethemainconclusionsfromtheConvention,andpresentthecontentsoftheNHSScotlandActionPlan(TheScottishExecutive2002)whichwasshaped,inpart,bytheoutcomes of the inquiries.
Theinquirygroupworkedasateam,interviewingindividualsfromrelevantorganisationsasawholewherepossible.Theinquirygroupdrewontheseinterviews,andinterviewsconductedwithstafffromtheScottishExecutive,professionalopinionandrelevantguidelines,inordertomaketheirfindings.
5.3 ConclusionsoftheInquiry
Themainconclusionwasthattheoutbreakofsalmonellainfectionwasunfortunate,buttherewas“…noevidencethatthedeathsatGlasgow’sVictoriaInfirmarycouldhavebeenavoided.”Theinquirygrouparguedthatitwaspossibletoreducethechancesofhospitalacquiredinfection,buttheycannot be eliminated entirely.
Criticsofthefindingshavemainlyconcentratedonwhattheyseeasalogicalflaw.Ifthedeathswerenotpreventable,whydidtheinquirygroupmakesomanyrecommendationsforchange?Muchdependsonhowthemainconclusionisinterpreted.Forexample,itmightmeanthatthedeathswerenotpreventablegiventheresourcesandprocessesinplaceatthetime.Ontheotherhand,itmightbeinterpretedtomeanthattheresourcesandprocesseswereadequategiventheknowledgeandwillingnesstopaythatappliedatthetime,butthecommunity’sexpectationswerechangedbythe public debate about the deaths.
The only reasonable basis for judgement is an analysis of the recommendations that are summarisedbelow.Thereadermustaskwhetheranyoftherecommendedactionscouldandshouldhavetakenplacebeforetheoutbreaksandconsequentpublicity.Itisourviewthatatleastsomeoftherecommendedactionsshouldhavebeeninplace–theywouldhavecostlittleornothing,anddidnotpresentanysignificantlogisticalortechnicalproblems.

67
DrWattarguedthattheriskisalwayspresent,nomatterwhatisdone.“Youcannotbringitdowntoanabsolutezero.Itislikethebrakesinyourcarfailing.Youcanminimisetheriskbyhavingthecarservicedbutthebrakescanstillfail.Ourmeasuresagainsthospitalacquiredinfectionareratherlikeadamagainstwater.Wehaveidentified47holesinthedam.Ifwecanplugthe47holesthatwillobviouslyhelp.”
5.4 RecommendationsoftheInquiry
ThefollowingsummarywascompiledfromtheReport of the review of the circumstances surrounding the onset of the outbreak of salmonella infection at the Victoria Infirmary, Glasgow, in December 2001 and January 2002.
Initspreamble,theReportnotesthesignificanceofhospitalacquiredinfection(HAI).Itnotonlyaffectsindividualsbutfrequentlytransmittootherswhorightlyhaveanexpectationthattheywillbe protected from cross infection. There is a distinct and immediate public health implication andthepublichasanexpectationthatcoherentadvicetothemwillbeforthcoming.Evenquitesmalloutbreaksofcross-infectionwillhaveanimpactonhealthserviceprovision,becausemoreresourceswillberequiredandalso(andoffurtherconcerntothepublic)thereislikelytobetemporaryclosureofservicessuchaswardsorwholehospitals.
Theinquirygroupmade47majorrecommendations.Thereisnoeasilyunderstoodstructure,andwehavecreatedastructurebelowtofacilitateunderstanding.Eachoftheheadingsis,however,derivedfromtermsusedintheinquirygroup’sreport.
Compliancewithexistingrulesandguidelines
Theinquirygroupoftenimplied(andoccasionallymadespecificreferenceto)theappropriatenessofmanyoftheexistingoperatingprocedures.However,itnotedtherewasseldomfullcomplianceandreferredtotheneedforauthoritiestoaddressthis.Forexample,itstatedthat“…theScottishExecutiveHealthDepartmentshouldreinforcethegoodpracticecontainedwithintheScottishHealthFacilitiesNote30(InfectionControlinthebuiltenvironment:design and planning).”
Auditing
Theinquirygrouplinkedpoorcompliancetoinadequateauditingprocessesthatwereobservedatmostlevelsinthesystem.Inhealthcareorganisations,itwasnecessaryformanagersto“…putinplacestructuredauditsofhandwashingforallgroupsofstaff,includingmedical,bank,agencyandnightstaff.”Thereshouldberegularauditingofcompliancewithfoodhandlingrules,and“…appliancesusedforstoringorpreparingfood(whetherinthewardorelsewhere)shouldbe subject to appropriate inspection and the results recorded.”
Externalagencieswerealsoadvisedtobemorevigilant.Forexample,theClinicalStandardsBoardforScotlandwasurgedtomakesuretherearereliablemechanismsinplacetomonitorcompliancewithitscleaningservicesstandards.Healthcareorganisationswereadvisedtopaymoreattentiontoexternalauditreports.Forexample,managersofTrustsshouldpaymoreattentiontoreportsfromAuditScotland,andthentakeappropriateactiontorespondtothem.

68 Patient Safety: a comparative analysis of eight Inquiries in six countries
Refinementofoperatingprocedures
Manyoftherecommendationsconcerntheneedtomakeminorchangesintheoperatingrulesthemselves.Forexample,clinicalstaffshouldbemorecloselyinvolvedinthereviewofcleaningmethods.Theinquirygroupsaidthat“…thecleaningspecificationinwardsanddepartmentsshouldbesetbytheseniornurseresponsibleforthearea,andeachwardordepartmentalmanager,incollaborationwiththerelevantInfectionControlTeam(ICT)andDomesticServicesManager.Cleaningagainstthisspecificationshouldbesubjecttorigorousmonitoringandactiontocorrectdeficiencies.Failuretomeetthespecificationshouldbesubjecttoformalauditandreviewwithineach hospital and be subject to public disclosure.”
Further,thereshouldbemorespecificitywithregardtodealingwithgrosscontaminationfrombodyfluids(blood,urine,faecesandsoon).Detailedguidelinesshouldbeavailableineveryhospitalforthedecontaminationofstaff,togetherwithappropriatefacilities(washing,showering,cleaninguniforms). All health care organisations should have a staff uniform policy that ensures all staff uniformsarelaunderedbyaserviceaccreditedbytheNHS,thewidespreadpracticeofstafftravellingtoandfromworkin(potentiallycontaminated)uniformsceases,andthatadequatestaffchanging and decontamination facilities are provided. There should be improvements in guidelines forthehandlingofpatientswithloosestoolsordiarrhoea.
Severalrecommendationsweremadewithregardtopatientmovements.Forexample,thereshouldbenationalconsiderationofoptionstoreducethemovementofpatientsbetweenwardsinhospitals“…sothatthelikelihoodofoutbreaksoccurringisminimisedandwhentheydooccurtheyarecontainedwithinasdefinedalocationaspossible.”Further,controlofanoutbreakmustincluderestrictionofstaffmovementbetweenwardsanddepartments.Whenpatientsrequireinfectioncontrolprecautionstobeimplemented,thenursesprovidingthecareshouldwherepossiblebethe‘named nurse’. This should minimise the number of contacts of both the patient and the nurse.
Otherimprovementstooperatingproceduresconcernstandardsrelatingtonewbuildingsandrefurbishmentprojects,moreprecisionwithregardtoadvicefortemporarystaffincludingthosefromnursingagenciesandbanks,andrulesforstaffscreeninginoutbreaksofinfection.
Accountability
One of the most important sections of the inquiry group’s report concerns accountability: too many staffwereawareofpotentialproblemsbutdidnotbelieveitwastheirresponsibilitytoact.Theinquirygrouprecommendedthatwardordepartmentalmanagers“…shouldhaveunambiguousresponsibility and be held accountable for all aspects of hygiene in their area. They must have commensurateauthority,skillsandresources(timeandmoney)todischargethisresponsibility.”
Trust managers needed to ensure there are policies that clearly identify the accountabilities of nursinganddomesticstaffinthecleaningofwardfurnitureandapparatusincludingbaths,foodtrolleysandclinicalequipment.Thepoliciesmustpreciselyidentifywhohasoverallresponsibility.
Itwasimportanttoensuretherewerestaffspecificallyresponsibleforinfectioncontrol.Eachhealthcareorganisationshouldhaveadesignatedandtrainedinfectioncontroldoctor“…whowillnormallyleadtheInfectionControlTeam.”Thisshouldnormallybeaconsultantmicrobiologistwhowillhavedesignatedsessionsandaclearlydefinedjobdescription.Inthecaseofahealthcareorganisationwithoutlaboratoryfacilities(suchasaPrimaryCareTrust)itshouldformalisearrangementswithasuitablytrainedandappropriatelyresourcedindividual.

69
Clearaccountabilityshouldexistwithregardtomanagementofincidents.Theinquirygrouprecommendedthereshouldbean‘issuemanager’assoonasaseriousoutbreakoccursandirrespectiveoftheroutethroughwhichnotificationhascome.Thereshouldalsobeclearaccountabilityforinformationmanagementincludingbriefingsforstaffandthepublicassociatedwithanoutbreak.
Severaladditional(anddiverse)commentsweremadeaboutaccountability.Forexample,there should be a lead Infection Control Nurse (ICN) in each Trust. There should be ‘infection controlchampions’atwardlevelthatcancomplement,butnotreplace,therolesoftheICT.TheyshouldnotbeusedassubstitutesforICNs.Rather,theyshouldassistinthedeliveryofa comprehensive infection control service and be integral members of an enlarged ICT. They shouldhaveclearlydefinedroles,alloweddedicatedtimeforinfectioncontroldutiesandbeappropriately trained and supervised.
Reportingsystems
Severalrecommendationsaremaderegardingroutinedocumentationprocesses.Forexample,exposure of staff to faeces should be documented through the Incident Reporting Procedure asthoroughlyasexposuretoanyotherbiological(body)fluids.Nursingnotesandcareplansshouldclearlyreflecttheneedforentericprecautionsinindividualssufferingfromloosestoolsordiarrhoea.Ingeneral,nursingdocumentationshouldbeimprovedsothatkeyinformationandadvice relating to infection control measures can be communicated to all relevant staff.
Contactswith,andadvicegivenby,anymemberoftheICTshouldbedocumentedbyboththeindividualsprovidingandreceivingtheadvice.Thiswouldbeinadditiontoinfectioncontrolcareplans.Nursingdocumentationshouldbeimprovedsothatkeyinstructionsrelatingtoinfectioncontrol measures can be communicated to all relevant staff.
Whenproblemsarise,thereshouldbespecificdocumentationprocesses.Forexample,allincidentreportsshouldprovidesufficientdetailsofkeyfactorsinthespreadofinfectiontoallowproper audit. The recommendations of an earlier report (Pennington �997) should be extended tocoveralloutbreaks.Inparticular,oncompletionofinvestigations,aminimumdatasetshouldbeprovidedtorelevantauthoritiesinastandardisedway.Forlarge(orotherwisesignificant)outbreaksafullwrittenreportshouldbecompletedandconsiderationgiventoitspublication.
Appropriate documentation should be made of screening of relevant staff in the case of an outbreak.Healthcareorganisationsshouldtakemeasurestoimprovethequalityofclinicalinformation on laboratory request forms for investigation purposes.
Aclassificationsystemforinfectionoutbreaksshouldbedevelopedandimplemented.Theinquirygroupprovidedanexampleofaclassificationandreportingsysteminitsreport.Theclassificationandcountingrulesshouldapplyinallcircumstances.ThustheNHSshouldmakeuseof“…aconsistentsetofcriteriathatislinkedtoariskmanagementclassificationdescribinginfectionoutbreaks.”Thelevelofoutbreak(intermsofriskcategory)mustdeterminethelevelofaction required and the level of communication.
Finally,thereshouldbemoreandbetterinformationaboutcosts.Theinquirygrouprecommended that NHS Scotland should adopt a program budgeting approach to infection control and that each Trust and each Board be required to provide details of the resources devoted to infection control. The details should be supplied as part of the documentation provided to the Clinical Standards Board for Scotland at the time of individual health care

70 Patient Safety: a comparative analysis of eight Inquiries in six countries
organisationreviews.TheNHSScotlandshouldconveneaworkinggrouptodevelopmethodsoftrackingandcalculatingthecostsofinfectionsandtheircontrol.
Communicationprocesses
Theinquirygroupwasparticularlyconcernedaboutthewaynewsoftheoutbreakswascommunicated. Much of the concern related to mass media reports. Thus the inquiry group recommendedthat“…TrustsandBoardsensurethattherearesufficientresourcestoappointadequatelevelsofcommunicationprofessionals.”However,theydidnotwanttoleaveeverythinginthehandsofsuchpeople.Theyarguedthat’PressOfficetoPressOffice’communicationshouldbeadditionalto,ratherthanasubstitutefor,professionalcommunication.
Communicationbetweenofficialsneededtobeimproved.Forexample,ifanyoutbreakswereconsideredatanystagetobefood-borne,boththeNHSScotlandandtheFoodStandardsAgencyshould be promptly informed.
Educationandtraining
Almosteverypartofthehealthcaresystemwasconsideredbytheenquiygrouptorequiremoretraining.Thusascientificmeetingshouldbeorganisedatwhichexperienceandideasrelatingtothespecificinfectioncontrolchallengesofoldbuildingsbeshared,andthefindingsshouldbewidelydistributedtothosewithresponsibilityfortheupgradingandmaintenanceofbuildings.
All health care organisation should regularly assess the competencies of nursing staff in infection control,andensurethatstructuredtrainingprogramswereestablished.NHSScotlandshouldworkwithnursingagencyproprietorstoestablishwaysofmanagingcompetenciesininfectioncontrol.Similar assessment and training programs should be put in place for medical and allied health professionals.Allstaffatwardordepartmentlevelthathandlefoodshouldreceivetraininginfoodhygienecommensuratewiththeirdutiesandincompliancewithfoodsafetyregulations.
The managers of safety in health care organisations (and especially the responsible clinicians whoshouldincludeconsultantsinPublicHealthMedicine)shouldbetrainedinthemanagementofHAIandplayamoreprominentroleinsurveillanceandhospitaloutbreakmanagement.Theyshouldnormallyleadallinfectionoutbreakswithintheirorganisation.EachHealthBoardshouldholdregularsimulatedoutbreakexercises(possiblyeverytwoyears),withadequatedebriefingafterwards.ThedocumentationofsuchexercisesistobeprovidedtotheClinicalStandardsBoardat the time of their inspections.
Moreresources
Ofthe47majorrecommendations,onlytworeferdirectlytoresourceshortfalls.First,themanagersofeachhealthcareorganisationmustensurethatlevelsofbasicwardequipment(suchashoistslingsandcommodes)aresufficienttoreducethecommunaluseofsuchequipmentandreducetheriskofcross-infectionduetoinadequatedecontamination.
Second,managersmustensurethatresourcesareinplacetoensuretherearesufficientnumbersofinfectioncontrolstaff.Thestaffshouldbesufficienttohavedailycontactwithwardsorotherhealthcarepremises,visiteachfacilityatleastweekly,provideadvicetowardanddepartmentalnursingstaffonthenursingcareofpatientswhoareatriskoforwhohaveinfection,beresponsibleforasystematiccompetencyprogramininfectioncontrolforallhealthcareworkersattheirplaceofwork(includingmedical,agencyandbankstaff),undertakesystematichandwashingaudits

7�
includingthoseinvolvingnightandweekendhealthcareworkers,andprovideanoncallserviceto advise on infection control matters on a 24 hour basis.
Theinquirygroupdidnotmakeanyestimatesofthecostimplications.However,duringtheInquiryitwasarguedthatthecostofadequateresourcestoreduceinfectionstoanacceptablelevelwasprobablynomore(andpossiblyless)thanhavinginadequateresourcesthatresultedinmajoroutbreaksofthekindsthathadrecentlybeenexperienced.
Teamworkandleadership
Theinquirygroup’sreportplacesmuchemphasisontheneedforbetterteamwork.Nogreateffortwasmadetodefinewhatthismightmean,butmaybededucedfromageneralthemethatpervadesthereport:toomanypeopleinallpartsofthesystemwereworkingonthebasisthatsomeoneelsewasincharge,buttherewasnocommonunderstandingastowhomthatmightbe.
Theinquirygrouprecommendedthattheteamestablishedtomanageoutbreaks(theOutbreakControlTeamorOCT)shouldalwaysbechairedbysomeonewithcompetenceandauthorityinhealth care associated infection. The local Consultant in Public Health Medicine (CPHM) should chairOCTsformajoroutbreaks.Inthisway,therewillbeaclearindicationthattheTeamisledbyanindividualexternaltothehealthcareorganisationwhohascloselinkswiththelocalNHSBoardandwithcommunitysurveillance.InthecaseofotherhospitaloutbreakstheCPHMshould be consulted regarding chairmanship of the team.
ThereshouldbeclearroledefinitionsforthemembersoftheOCT,andtheirresponsibilitiesshouldbedocumented.TheteamshoulddevelopandpublishanOutbreakControlPlan.
Senior managers of each health care organisation (at the level of Executive Director and above) shouldbefullyengagedfromanearlystageinmanagingoutbreakseitherasfullandactivemembers of the OCT or as a separate support team to the OCT. Senior management support shouldincludeaseniorcommunicationmanagerwhocanensurethatstaff,relativesandthepublicarepromptlyinformedoftheoutbreakandaregivenappropriatepublichealthmessages.
TheChiefExecutiveofahealthcareorganisationorHealthBoard(dependingonwhethertheoutbreakisprimarilyinthehospitalorcommunityrespectively)shouldassumetheunambiguousresponsibilityforensuringeffectiveinternalandexternalcommunicationincludingthemedia,and appropriate government departments and agencies.
EachHealthBoardshouldhaveanappropriatelyconstitutedICTwhichtakestheleadinstrategicaspectsofinfectioncontrolintheirarea,formulatesandagreesinfectioncontrolpolicies,coordinatesthemanagementofalloutbreakswheretheMajorOutbreakPlanisinvoked,hasadesignatedleader,linkseffectivelywithriskmanagementcommitteesandclinicalgovernancecommittees,andprovidesassistanceandadvicetoTrustICTswhenrequestedandwhenappropriate.
LargeTrustsshouldhaveanappropriatelyconstitutedICTwhichpreventsandmanageshealthcareassociatedinfectionwithintheirTrust,implementsagreedBoardandTrustpoliciesininfectioncontrol,hasadesignatedleader,linkseffectivelywithriskmanagementcommitteesandclinicalgovernancecommittees,andliaisescloselyandcooperateswith,andprovidesmembership for the Health Board ICT.

72 Patient Safety: a comparative analysis of eight Inquiries in six countries
Thecultureofopenness
Thereissurprisinglylittledirectmentionoftheneedformoreeffectivecommunicationwithinhealthcareorganisations.However,adegreeofconcerncanbededucedfromthegeneraldiagnosisofcausesoffailurestoactwithinthoseagenciestoreducerisksandtakepromptactiontocontroloutbreaks.Theinquirygroupfocusedonrecommendingchangesthatwouldimproveopennessbutavoideddirectlylinkingitsmeasurestoprevailingclinicalcultures.
Itwas,however,lessreticenttocriticiseotherpartsofthehealthcaresystem.Forexample,itarguedthatinternalcommunicationwithinandbetweentheScottishExecutiveandNHSorganisationsmustbe“…improvedandclarifiedsoastoreflecttheopennesscultureandthisisemulatedincommunicationwithrelevantagencies(suchastheFoodStandardsAgency,ScottishWater,andtheScottishEnvironmentalProtectionAgency).
Italsorecommendedchangesindealingwiththemassmedia(andhencethepublicatlarge).Itrecommendedthat,atbothlocalandScottishExecutivelevels,morestrenuouseffortsshouldbemade“…totapthepotentialofthemediatoimprovethepublicunderstandingofinfectioncontrolissues.ThiswillrequireamoreopenrelationshiptobedevelopedbetweentheNHSandthemediabased on mutual trust. There should be presumption of early disclosure to the public and the media ofoutbreaksofinfection.”
5.5 Discussion
TheobjectivesoftheWattInquiryweretoa)reviewthecircumstancessurroundingtheoutbreakofsalmonellainfections,b)assessthemanagementoftheoutbreakandreductionoffurtherexposures,c)assesshowtheNHSTrustmanagedtheoverallsituationincludingcommunicationwiththepublicandotherorganisations,andd)drawconclusionsandmakerecommendationstohelpreducerisksoffutureoutbreaks.DespitethemajorfindingoftheInquirythatlittlecouldhavebeendonetoavoidthedeathsattheGlasgowInfirmary,theInquiryproduced47recommendationsfor various levels of the health care system in Scotland ranging from the Scottish Executive and theNHS,throughtohospitalsandtheirBoards,toindividualclinicians.Themainfindingsandrecommendationsoftheinquirygroupinrelationtotheseobjectiveswereacceptedbymostknowledgeablepeople,althoughasmallminoritywascritical–mainlyonthegroundsthatsomeoftheinvestigatorsweretoocloselyassociatedwiththesponsoringagency.
TheInquiryhadtwomajorflowoneffects.Asaresultofrecommendation13“thatascientificmeetingbeorganisedatwhichexperienceandideasrelatingtoinfectioncontrolchallenges…beshared…“aMinisterialConvention(discussedin5.6.1below)wasconvened,bringingtogetherexperts and practitioners in an innovative approach to understanding and preventing HAI. The secondwastheembeddingofanumberoftheInquiry’srecommendationsintheNHSScotlandActionPlan(discussedinsection5.6.2).ThePlanreflectedmanyofthemajorconcernsoftheInquiryreport,includingtheneedforanincreaseinresourcesforhealthservices,andafocusonimprovingtheteamworkofstaff.

73
5.6 Footnotes
5.6.1 TheReportfromtheMinisterialConvention
TheConventiontookplaceon28June2002atGlasgowCaledonianUniversity.Therewerethreemainaims:todiscussthecurrentHAIagendawithaviewtostrengtheningconsensusamongkeyplayers;todevelopaplanfortakingforwardactiontoreducetheriskofHAIinScotland;andtoraisetheprofileofstepsbeingtakentotackleHAIinScotland.
Itdrewtogetherseniorpeoplefromarangeofbackgrounds.TheyincludedpublichealthspecialistsandpathologistsfromaroundScotlandandfromoverseas.TheMinisterattended,togetherwithward-basedprofessionalsandsupportstaff.
TheConventionhadtwocomponents.Thefirstwasaseriesofpresentationsonpolicyandpractice as they relate to HAI and infection control. These provided context for more focused discussions.
ThesecondwascomposedofeightparallelworkshopsonHAI-relatedtopics.Theintentionoftheworkshopswastodrawtogetherconclusionsonwhatwashappening,thestrengthsandweaknesses,andwhatactionsmightbeneededinthefuture.TheworkshopthemesweredevelopedafterareviewoffeedbackfromhealthcareservicesaboutHAI.Theywereledbyindividualswithrecognisedexpertiseandexperienceinthetopicsunderdiscussion.
TheChairsoftheworkshopssubmittedasummaryofthekeypointsarisinginthemattheendoftheday.Thekeyissuesraisedanddiscussedandtheconclusionsreachedinthepresentationsandworkshopsarepresentedinthenextsectionofthisreport.
Part1:presentedpapers
Thefollowingaresummariesofthemostrelevantaspectsofthepresentations.Noattempthasbeen made to report all contents of the papers.
Consultant Microbiologist, Clinical Standards Board for Scotland
“TherecentincreaseinHAIpartlyreflectsmoreefficientreportingofcases.Howevertherearefactorsthatincreasethelikelihoodofinfectionincludingchangesinthepatientmix,morecomplicatedtreatments,andinappropriateuseofantibiotics.Healthcaremethodsandfundinglevelshavenotalwayskeptpacewithincreasedexpectationsofpatients.
Actionsarebeingtakentoincreasepatientsafety.Theyincludebetterplansthatincorporateauditabletargets,improvedinformationsystems,andincreasedtraining.Theremust be a cultural change and additional resources.”
CEO of Highland Acute NHS trust
“Implementationofbettermethodsofcarerequireseffectiveleadership,clearaccountability,the“right”values,andincreasedresources.Leadershipisimportantatalllevels.BoardsandCEOshaveanessentialparttoplay.Equallyimportant,seniorcliniciansfromalldisciplines should recognise the priority of the issue. Getting these different parties to feel ownershipofinfectioncontrolisthemainchallenge.
Therightvaluesincludeanoblameculture,openness,partnershipwithpatientsandongoing learning and development. Additional resources are needed but they are not sufficient.Thereisalwaysscopeforinnovationintheapplicationofexistingresources.”

74 Patient Safety: a comparative analysis of eight Inquiries in six countries
Consultant Microbiologist, Tayside Acute NHS Trust
“EffectiveactiontocontrolHAIrequireschangesinsystems,cultureandmanagementandthereisnoquickoreasysolution.Systemsincludestructuresandprocesses,policiesandprocedures,educationandtraining,auditandsurveillance.Cultureincludespublicperceptionswhichmayunderestimatetherisks,givingHAIlowpriorityrelativetootherhealthissues,whilepublic demands may exacerbate the problem.
ManagementoffacilitiesisessentialtoHAIcontrol:spaceandconfigurationofpatientareas;bedoccupancyandpatientmovementmaybecriticalfactors.Delayeddischarges,excessiveworkloadandshortcutsofconveniencecanaddtotheproblem,whileadequateinformationtechnology structures and resources can form part of the solution.
Leadership is essential: strategic leadership in Boards and Trusts; clinical leadership by medical and nursing directors; professional leadership by infection control nurses and microbiologists;andgeneralleadershipatalllevelsofthehealthservicetoinfluenceandpersuade colleagues that infection control has high priority and practices must change. ExperiencesuggeststhatamajorproblemintacklingHAIisalackofaccountabilityandunclearlinesofresponsibility,probablyreflectingthelowpriorityaffordedtoinfectioncontrolintherecentpast.Thismustchangewithchiefexecutivesputtingmeasuresinplacetoensuregoodinfectioncontrolwithintheirorganisations,withresponsibilitiesclearlysetdownatalllevels and clear lines of accountability.
RiskassessmentinthecontextofHAIentailsidentifying,evaluating,rankingandtreatingrisks,withongoingmonitoringandreview.Fullcommunicationandconsultationisessential.Valuesshouldincludeopenness,partnership,learninganddevelopment,withinano-blameculture.”
Infection Control Nurse, Ayrshire and Arran Acute Hospital NHS Trust
“EffectiveactiontocontrolHAInecessitatesareturntobasics.Weneedtofocusouractiononhandhygiene,environmentalcleanliness,decontamination,personalprotectiveequipment,safedisposalpractices,andisolationofpatientswherenecessary.
Allstaffneedtoknowtheirroleintheseareas.CombatingHAIisthereforeakeyclinicalgovernanceissue.Trustneedanappropriateframeworktoimprovepracticewhichinvolveseducationandtraining,riskmanagement,researchanddevelopment,andclinicalaudit,withinfection control at the core.”
Consultant Microbiologist, Danish Ministry of Health
“HAIisnotaproblempeculiartotheUK.AstudyoftheprevalenceofnosocomialinfectioninuniversityhospitalsandtertiarycarecentresinvariousEuropeancountriesbetween1984and1996foundprevalenceratesrangingfrom4.4%to14.8%;theUKfigurewas11.2%in1993.Denmarkhasapopulation(5.3million)similartothatofScotland.TheprevalenceofHAIinDenmarkfellfrom12.1%in1979to8.0%in1999,duetoaseriesofmeasuresespeciallyimprovementsincatheterisation.LearningfromwhathasprovedeffectiveinDenmark,cantherefore usefully guide efforts in Scotland.
Since1977theNationalCentreforHospitalHygienehasprovidedguidelines,surveillance,adviceandresearch.Ineachcounty,oneclinicalmicrobiologylaboratory,situatedattheuniversityhospitalorthemajorregionalhospital,haslocalinfectioncontrolresponsibility.

75
Infection control doctors are clinical microbiologists and regular courses are run to give nursesspecificinfectioncontroltraining.
DenmarkhasnoregulationstargetedatpreventingHAIinhospitals,althoughtherehasbeensomepoliticaldebateaboutthis.Nationalstandardshavebeenelaboratedbetween1998and2002.Thereisagrowingfocusonqualityassuranceinhospitalsbutsofaronlyonehospitalisfullyaccredited.Thenumberofofficialcomplaintsabouttreatmentinhospitals is increasing.
DanishexperienceisthattheprevalenceofHAIisinverselytonursepatientratios.AUSstudyoftherelationbetweenadverseoutcomesamongmedicalpatientsandtheproportionof registered nurse hours to medical patients found that urinary tract infections and hospital acquiredpneumoniashadstrongstatisticallysignificantassociationswithlowratios.
Thereisaneedforsimplesurveillancesystemsthatprovideeffectivefeedback.Theremustbeimprovedcommunicationbetweenclinicalmicrobiologistsandcliniciansatlocallevel,and education of infection control nurses.
A �990 study compared antibiotic policy in intensive care units in a number of countries. InDenmark32%ofunitshadwrittenguidelinesandarestrictedantibioticlist,21%hadinformedmutualconsentandarestrictedantibioticlist,and47%hadneither.InScotlandthecorrespondingfigureswere13%,16%and71%.”
Part2:parallelworkshops
EQUIPMENT,ENVIRONMENTANDPATIENTMANAGEMENT
Effective action to reduce HAI by improving the clinical environment and equipment depends on riskmanagementandprioritisation.Resourcesarelimitedandthosemanaginghospitalsandotherclinicalservicesneedtosecureagreementontargetingactiononrisk-basedpriorities.Theroleoftheinfectioncontroldoctorispivotal,andtheymusthavegoodcommunicationwiththemanagers of facilities including building design and cleaning.
THEPROMOTIONOFGOODPRACTICEINHYGIENEANDINFECTIONCONTROL
Education is vital but it must involve all staff: support services; nursing; and junior and senior medicalstaff.Astandardisedtrainingpackageonhygieneshouldbedeveloped.
However,educationandtrainingcanonlygosofar.Thepromotionofgoodstandardsofhygienebehaviourisacorporateresponsibility,butthebehaviourofapoorlycompliantmemberofstaffcan compromise the integrity of the entire system. Lines of responsibility must be clearer and theroleofanyinfectioncontrolchampioninrelationtothismustbeclarified.Acceptabilityoftheconcept of cleanliness champions has still to be established.
Clinicalgovernancesystemsshouldauditcompliancewithhygiene-relatedstandardsinclinicalcare.Amultidisciplinaryapproachisnecessarywithasmuchemphasisonprimarycareasonsecondary care.
ANTIMICROBIAL RESISTANCE AND PRESCRIBING
Nationalmonitoringofantibioticprescribingisvoluntaryandthereforeincomplete.Ingeneral,informationaboutantibioticresistanceinScotlandisscarce,butwemaybeapproachingacrisis.

76 Patient Safety: a comparative analysis of eight Inquiries in six countries
Clearguidelinesonantibioticprescribingarelacking.Guidelinesaremorelikelytobeeffectiveifresourcesarededicatedtotheirimplementationandtomonitoring.Juniormedicalstaffshouldhaveclearguidelinesonidentificationofsepsis,recognitionoftheseverityofillness,andtheuseofantibioticsintreatingit.Communicationroutesbetweenservicesmustbeimprovedtoensureallrelevant health care professionals are fully informed of a patient’s medical history and thus minimise the chance of further infection.
Information systems should be developed to monitor and audit the prescribing of antibiotics. Multidisciplinary antibiotic prescribing teams should be formed to promote prudent prescribing throughout health care systems. The involvement of pharmacists in frontline education about antibiotics and monitoring antibiotic prescribing should be secured.
PUBLICCOMMUNICATIONANDPATIENTINVOLVEMENT
TheperceptionsofHAIheldbypatientsandthepublicareimportant.Patientsneedtoknowaboutthattherearerisksassociatedwithhealthcare.Themethodsusedtoinformthemaboutthisshouldseektoallayunnecessaryanxiety.
The media constitute the principal source of public information. Media reporting on HAI can be unhelpfulbutitcanhaveavaluableroleinraisingpublicawareness.Reportingofthecurrent8-9%prevalenceofHAIinhospitalinpatients,coupledwithhighprofilereportingofoutbreaksofHAIandassociateddeaths,isacauseofunderstandablepublicconcern.ItisimportantthattheNHSencourages balanced and informed reporting.
Healthcareorganisationsshouldacknowledgethatpatientsareentitledtoappropriateinformationbeforehospitaladmission.Thereshouldbepublicinvolvementinplanningandauditinglocalriskmanagement programs. There should be central guidance to health care organisations regarding disclosureofinformationinrelationtoHAI,inparticularinthecaseofoutbreaks.
ROLES,RESPONSIBILITIESANDORGANISATIONALDEVELOPMENT
Ifinfectioncontrolistobemanagedeffectively,itmustbecomeintegraltothejobsofeveryoneinvolvedinprovidingpatientcare,includingnonclinicalsupportservices.Itisnotsufficientforspecialistservicesdevotedtoinfectioncontroltoworkinisolation,howeverwellresourcedtheymight be.
Managerial responsibility must be driven from the top of the organisation through the managerial line.Theremustbeaculturewherethisisintrinsic,andwhichisreinforcedbyappropriateeducationand training.
Theroleoftheinfectioncontroldoctorisacknowledgedtobeofprimaryimportance,butcurrentlevelsofsupportrarelyreflectthis.Infectioncontroldoctorsmusthaveallocatedsessionaltimetobeeffective,andshouldbearesourceavailabletobothacuteandprimaryhealthcareorganisations.Surveillanceisanimportantpartofinfectionandcommunicablediseasecontrol,withappropriateallocation of responsibility.
THERISKMANAGEMENTOFHAIBYHEALTHCAREORGANISATIONS
ThepolicyofNHSScotlandinvolvesmanagingHAIthrougharisk-basedapproach.Riskmanagementcomprisesaculture,processesandstructuresthataredirectedtowardstheeffective management of potential opportunities and adverse effects. The approach is intended to satisfyethicalrequirements,toprotecthealth,tocomplywithlegalobligations,toensurepoliticalaccountability,toreducefinancialliabilitiesandtomaintainreputation.

77
NHScareprovidersdonothavesufficientresourceorexpertisetoassessandmanagetheriskofHAIadequately.Thechallengeistodisseminatemodelsofexcellence,toensurecompliance,andtointegrateinfectioncontrolintotheriskmanagementprocesssothatitbecomesacorepart of routine practice.
Allstaffshouldbeawareoftheessentialcontributionofinfectioncontroltopatientsafety.Theymustbecontinuallyeducated,frominductiononwards,toreinforcegoodpractice.Theneedforcommitmenttoreducingriskstopatientsmustbeembeddedfromthefirstdayoftrainingand reinforced continuously. Particular emphasis should be paid to members of the medical professionwhoareoftenseenastheworstoffenderswithregardtohandhygiene.
Riskmanagersensureongoingcommunicationaboutpatientsafetyissuesthroughouttheorganisation. There should be less focus on structure and process and more on cultural issues and sustained commitment to change.
Emphasisshouldbeplacedonassessingtheriskofinfectionresultingfromthepatient’sjourneythroughcare,integratingwhereappropriateacuteandprimarycarethroughoutahealthepisode.Riskmanagementshouldentailapragmatic,integrated,wholesystemapproach.
Thereshouldbeimprovedleadershipandincreasedempowerment.Aculturalchangetowardsteamworkandmutualrespectwouldmotivateindividuals,encouragingprideinthejobandinpatient care. There should be less regulation and more facilitation.
SURVEILLANCEANDRESEARCH
ThedevelopmentofanationalHAIdatabaseisasignificantstep.Buttheprogramhaslimitations: data are collected in relation to a small number of procedures; they only covers bacteraemias;andincidenceisnotrelatedtoriskfactorssuchastheuseofintravenousdevices.
Priority should be given to methods for surveillance of infection presenting after discharge from hospital.ItisalsoimportanttodevelopearlywarningsystemsforpossibleHAIoutbreaks.
HAI-RELATED STANDARDS
Draftstandardsforinfectioncontrol,decontaminationofreusablemedicaldevicesandcleaningserviceswereissuedin2001.Allbutoneofthe15standardsreflectstructuresandprocessessupportinginfectioncontrolandaffectingclinicaloutcomes.Theremainingstandard,forhandhygiene,ismostdirectlyrelatedtoclinicalpracticeanditsinclusionreflectstheimportanceofthe topic and the strength of the supporting evidence base.
ByJanuary2002,mosthealthcareorganisationshadreportedselfassessmentsagainstthestandards. An interim report revealed several shortcomings. Most health care organisations did nothaveplanstoaddressthefullimplicationsofHAI,andinfectioncontroloftendependedonlimitedresourceswithsmallnumbersofstaffexpectedtocoverlargesites.Itwasconcludedthatinfectioncontrolisdifficulttomanagebecauseofthediversityofindividualsandgroupswithrelatedinterestsandresponsibilities.Itwasapparentthatmoreefficientorganisationalandmanagement processes could improve quality and reduce costs.
The organisational culture may encourage different staff members to have different perceptions ofrisk.Allstaffmustsharethesameobjectivesandtoacceptthatallhavearesponsibilityforhighstandardsofinfectioncontrol.Theremustbeemphasisonqualitycontrolswithopencommunicationsystemstofacilitatelearningfromanymistakesmade.Operationaldifficultiesinimplementingstandardsincludestaffingshortages,timeconstraintsandcontractingout,diminishingtheopportunitiesforateamwork,partnershipapproach.Excessivemovementof

78 Patient Safety: a comparative analysis of eight Inquiries in six countries
patients,shortageofbedsandrapidpatientthroughputcanallmakeinfectioncontrolmoredifficult.Contracting out of domestic services can hinder maintaining infection control procedures and standards.
Infectioncontrolmustbeintegratedintothemainstreamriskmanagementsystemoftheorganisation.Policies,proceduresandguidelinesmustbeuptodateandaccessible;theremaybevalueinacentralnationalresourceofpolicies,proceduresandguidelines.Allstaffshouldreceiveinstructiononinfectioncontrolatinductionwithongoingeducationtomaintaincurrentknowledge.Awarenessofcoreinfectioncontroltopicsshouldbecompulsoryforallstaff,likeotherhealthandsafetyissuessuchasfiresafety.
Thebasicissueofhandhygieneishowtochangeculture.Thisaffectsalllevelsofstaffbuttheremaybeparticulardifficultyinconvincingclinicians,includingseniordoctors,oftheimportanceofinfectioncontrolingeneralandhandhygieneinparticular.Effectiveactionmustbetakenonnonperformingstaffwithinacultureofsupportratherthanblame.
Compliancewithstandardscanbemonitoredthroughpeerreview,patientinspection,healthcareaccreditation,formalprofessionalreview,NHSinspection,externalformalaudit,statutoryinspectionorinvestigation.Peerreviewiscurrentlythemaininstrumentbutistimeconsuming.
5.6.2 TheNHSScotlandActionPlan
ThisPlanwasreleasedaftertheoutbreaksandtakesaccountofsomeofthefindingsoftheWattReport.Itstressesfourmainprinciples,asfollows:
n unifiedmechanismsforreportingandanalysiswhenthingsgowrong
n amoreopencultureinwhicherrorsorservicefailurescanbereportedanddiscussed
n systemsforensuringthat,wherelessonsareidentified,thenecessarychangesareputintopractice
n amuchwiderappreciationofthevalueofthe‘systems’approachinpreventing,analysingandlearning from errors.
Additional measures are proposed under three headings: promoting good infection control and hygienepracticeinwards,otherclinicalsettingsandsupportservices;ensuringthatgoodhygieneandinfectioncontrolpracticeisinplaceandworkingthroughouthealthcareorganisations;andensuringthattheperformanceofhealthcareorganisationsinScotlandisofsufficientqualityandeffectiveness to reduce the incidence of HAI.
Considerableemphasisisgiventomediacoverage.Theforewordstatesthat“…recenteventshaveshownthatthereisdangerofpublicconfidenceintheNHS’sabilitytodelivergoodqualityeffectivecare to the population being eroded by ongoing coverage of infections in health care settings. The negative impact of scare stories on other sectors of society such as food production and retail is wellrecognised.”Thisseemssomewhatmisguided,giventhatthemassmediahaveoftenbeenthe most effective channels for informing the public of problems that the professional bodies have attempted to conceal.
ThePlan’sauthorsclaimthatmajorimprovementshaveoccurredoverthelasttwoyearsbymostoftheNHSinScotlandtoimproveinfectioncontrolservices.However,moreeffortisneededincludingtheinvestmentofadequateresourcestobeusedinthemostcosteffectivemannerpossible,nationalcoordination,andflexibleandinnovativelocalimplementationoftheActionPlan.Actionsarespecifiedwithaviewtomorepreciseestimationofthecostimplicationsofimplementingtheproposedmeasures,andofthesystemcostsofinfections.

79
ParticularemphasisshouldbegiventocompliancewithanNHSScotlandCodeofPracticeforthelocalmanagementofhygieneinwardsandotherclinicalunits,mandatoryhygieneandinfectioncontrolinductiontrainingprogramsandotherHAI-relatededucationalinitiatives,andthedefinitionoftechnicalrequirementsforcleaningprocesses.Finally,itisessentialtoincreasethecommitmentofallstafftoimproveinfectioncontrol,andthisimpliestheempowermentofstaff.Makingthishappenpartlyrequiresmoreresources.Equallyimportantareattitudesandculture,increasedacceptanceofresponsibilitybylocalmanagers,andsharingandlearningfromgoodandpoorexperiences.NHSandprofessionalandstafforganisationshaveakeyroleinpromoting good hygiene and infection control.
5.7 Referencesandselectedbibliography
Meikle,J.(2002).HospitalInquiryintoSalmonellaDeaths:ChecksSuggestBugthatKilledThree Brought in by Patient. The Guardian,18January.
NHS Scotland (2002). NHS Scotland Action Plan. Available at: http://www.scotland.gov.uk/library3/health/onh-00.aspAccessed3March,2006.
Pennington Group (�997). Report on the Circumstances Leading to the 1996 Outbreak of Infection with E.coli O157 in Central Scotland, the Implications for Food Safety and the Lessons to be Learned.Edinburgh:TheScottishOffice.
The Scottish Executive (2002) Preventing Infections Acquired while Receiving Health Care: The Scottish Executive’s Action Plan to Reduce the Risk to Patients, Staff and Visitors 2002 - 2005. Available at: http://www.scotland.gov.uk/library5/health/preventinfect.pdfAccessed19May,2006.
Watt,B.(2002).Report of the Review of the Circumstances Surrounding the Onset of the Outbreak of Salmonella Infection at the Victoria Infirmary, Glasgow, in December 2001 and January 2002. Scotland: NHS Scotland.
6 KingEdwardMemorialHospital,Australia
ConcernsaboutobstetricandgynaecologyservicesattheKingEdwardMemorialHospitalinPerth,atertiaryreferralhospitalincreasedprogressivelyduringthe1990s,notonlyamongstaffbutalsoamongpatients.Aseriesofinformalandformalreviewstookplace,buttheyfailedtoresolvetheproblemsorreduce public concern.
In1999,anewChiefExecutivewasappointed.Heimmediatelytookaction,andthisledtothecommissioning of a major external Inquiry by the Minister for Health in 200�.
TheInquiryreportedthattherewas“…evidenceofexemplaryclinicalandnon-clinicalcare.”However,italsofoundthatmostoftheconcernsaboutpoorcarewerejustified.ThereweremanyseriousproblemswiththeHospital’sclinicalandadministrativepractices.Inadequateprocessesofcareandofresponsestoproblems“…resultedinseriousadverseeventsandpoorclinicaloutcomesforwomenandtheirfamilies.”
Manychangesneededtobemadeiftheproblemsweretobeovercome.Theyincludedchangesinorganisationalculturethatincludedacceptanceofopendisclosureofproblems,improvedmethodsofexternalmonitoring,andbetterprocessesforrecordingandrespondingtoincidentsandadverseevents.

80 Patient Safety: a comparative analysis of eight Inquiries in six countries
6.1 Context
KindEdwardMemorialHospital(theHospital)providesinpatientandoutpatientservices,neonatalintensive care and specialist emergency services. At the time of the Inquiry it had 250 inpatient beds and60neonatalcots.Itisthestate’sonlymajorteachinghospitalinobstetricsandgynaecology,andisacentreformidwiferytrainingandpostgraduatemedicaltraininginobstetricsandgynaecology.
AsWesternAustralia’sonlytertiaryreferralserviceforobstetricsandgynaecology,itthereforereceivesandtreatsthemostdifficultandcomplexcases.About5000gynaecologicaloperationsareperformedeachyear,thereareabout5000births,andalmost10000femalespresentattheEmergency Centre for gynaecological or obstetric treatment.
Thesocioeconomicmixofpatientswaschangingintheperiodduringwhichpoorcarewassubsequentlythesubjectofinvestigation.Inparticular,therewasadeclineinthenumberofprivatelyinsuredlowriskwomen.Thiswascounterbalancedbyanincreaseintheproportionofhighriskpatients.Theyincludedpatientsfrompoorersocioeconomicbackgrounds,whowereunbookedandpresentedlateinpregnancy,someofwhomhadmorbidobesityorsubstanceabuseproblems,andwhoweresubjecttodomesticviolenceandotherseveresocietalproblems.
Further,theHospital(likemanyothers)wasexperiencingsignificantorganisationalandmanagerialchanges.TheyincludedthemergerwithPrincessMargaretHospitalforChildrenin1993,twochangesofchiefexecutives,theestablishmentofadevolvedmanagementstructurein1996,andreplacementofitsownBoardofManagementwiththeMetropolitanHealthServiceBoardin1997(whichcoveredallgovernmenthospitalsinthemetropolitanarea).ThesubsequentInquiryconcludedthatthechangeswerenotaprimarycauseofpoorclinicalpractices,buttheycontributedto their severity.
Unresolvedproblems(1990to2000)
In1990,theHealthDepartmentofWesternAustraliacommissionedtheProfessorofObstetricsandGynaecologyattheUniversityofWesternAustraliatoreportonthestate’sfutureobstetric,gynaecological and neonatal service requirements. The report recommended changes at King EdwardMemorialHospital,includingrevisionofobstetricstaffinglevels.
However,therecommendationswerenotimplementedbytheHospital.ThiswasdespitetheHospital’sclinicalstaffrepeatedlyraisingtheirconcernsaboutstaffinglevelswithHospitalmanagementthroughoutthe1990s.NorwasthereanyevidencethattheHospitalmanagementconveyedthisinformationtotheHealthDepartmentofWesternAustralia.
ThenewChiefExecutivetakesaction(1999)
ThenewChiefExecutiveonappointmentwasimmediatelyconcernedaboutseveralaspectsofprocessandperformance.HewrotetotheChiefExecutiveOfficeroftheMetropolitanHealthService Board explaining his concerns. They included the absence of an overall clinical quality managementsystem,problemsinidentifyingandrectifyingclinicalissuesbyseniormanagement,inadequatesystemstomonitorandreportadverseclinicalincidents,theabsenceofaproperandtransparentsystemtodealwithpatientcomplaintsandclaims,ashortageofqualifiedclinicalspecialists(particularlyafterhours),inadequatesupervisionofjuniormedicalstaff,andthepossibility of substandard patient care.

8�
The Chief Executive also outlined changes he had established to address these issues and recommendedadditionalchanges.AfterconsultationwiththeHealthDepartment’sChiefMedicalOfficer,theChiefExecutiveprovidedevidenceofpoorpracticeattheHospital.
The Chief Executive’s concerns led the Metropolitan Health Service Board to commission a reviewbyanindependentseniorclinician.ThisreviewsupportedtheChiefExecutive’sview,raisedadditionalconcerns,andrecommendedamoredetailedinvestigationintotheHospital’sobstetric and gynaecological services.
6.2 TheInquiries
6.2.1 TheChildandGloverReview(2000)
InconsultationwiththeCommissionerofHealthandtheMinister,theChiefMedicalOfficerandtheMetropolitanHealthServiceBoardcommissionedtheChildandGloverReviewin2000(ChildandGlover2000).Thistwoweekreviewidentifiedsignificantprocessandperformanceissues.
TheReview’sfindingsledtoincreasedpublicconcern,andavigorouspublicdebatetookplacethroughthemassmedia.ThedebatewasheightenedbyahighdegreeofoppositiontothefindingsfromindividualdoctorsandfromtheWesternAustralianbranchoftheAustralianMedicalAssociation.ItwassubsequentlyshownthattheviewsofChildandGloverwerefullyjustified.
6.2.2 TheDouglasInquiry(2001)
Aftersomedeliberationin2001,theMinisterforHealth,inconsultationwiththePremier,agreedto establish the Douglas Inquiry under the Hospitals Act and the Public Sector Management Act. TheInquirywasledbyNeilDouglas,alawyer,andwerefertohisinquiryteambelow.
TheInquiry’stermsofreference
TheInquiry’sbriefwas“toinquireintotheprovisionofobstetricandgynaecologicalservicesatKingEdwardMemorialHospital”overtheperiod1990to2000.TheInquiryfocusedonsystemicandorganisationaldeficienciesandconsideredmanagementandclinicalpractices,policiesandprocesses.TheInquirywastorecommendchangestoaddressthesedeficiencies.
Method
Over18monthstheInquiryaccessedinformationfrommorethan1,600patientclinicalfilesfromtheHospital.Italsoanalysed605patientclinicalfilesand293writtensubmissions.Itinterviewed70formerHospitalpatients,reviewedvariousconsultants’reports,comparedtheHospital’sclinicalperformancedatawithdatafromsimilarAustralianservices,read106transcriptsfromcurrentandformerHospitalstaff,andreviewedotherdocumentsfromtheHospitalandelsewhere.Casereviewfocusedonthemanagementofselectedhighriskobstetricandgynaecologicalcasesrequiringcomplexcare,asthesewerethecasestheHospitalwasexpectedtomanagewell.

82 Patient Safety: a comparative analysis of eight Inquiries in six countries
LimitationsoftheInquiry
TheInquiry’sbriefwastoexaminemanagementandclinicalpracticesandrecommendchangestoimprovethesafetyandqualityofthecareprovided.ItwasbeyondtheInquiry’sbrieftodeterminetheoverallincidenceofgoodorpooroutcomesforthereviewperiod.
TheInquirycommissionedacomparativeanalysisofperinatal,obstetricandgynaecologicalclinicalindicatorresultsbetweentheHospitaland13otherAustralianhospitals.Thereliabilityoftheseinterhospitaldatacomparisonswaslimitedbydemographicdifferences,relianceonroutinelycollecteddataanddifficultiesadjustingforvariability.However,whiletheauthorsadvisedreaderstoconsidertheresultsinlightoftheselimitations,theybelievedtheirfindingsweresufficientlyvalidtoidentifymajordifferencesbetweenthehospitalsandtorecommendfurtherinvestigationintoseveralresults.
Withtheexceptionoftheclinicalindicatorcomparison,theInquiryfocusedononehospital’sperformance.InallotheraspectsoftheInquiry’swork,itavoidedmakinganassessmentoftheHospital’sstrengthsandweaknessesrelativetootherhospitals.ThereisconsequentlynowayofknowingfromtheinquiryreportalonehowtheHospital’sperformancecompareswithotherAustralianhospitals.However,therearesomeobviousopportunitiesforgeneralisationofboththeproblems and the required solutions.
6.3 ConclusionsoftheInquiry
TheconclusionsoftheDouglasInquirywerearrangedundereightmainheadings:clinicalpractice;clinical policies and guidelines; incident reporting and management; reporting deaths to the Coroner; staffandstaffingmatters;patientinvolvement;qualityimprovement;andotherleadershipandmanagementissues.Wehaveretainedtheheadingsbelow,althoughthereissignificantoverlapacross issues.
Clinicalpracticeandperformance
Theinquiryteamreportedmanyinstancesofexcellentclinicalpractice,andofseriouseffortstoimprove.However,itwascommonthatissuesraisedbystaffwithclinicaldirectorsandnonclinicaladministratorswerelargelyignored.Othertacticswereregularlyemployed,includingreferralofproblems to largely ineffective committees.
Themainproblemsthatremainedunaddressedwerenonexistentorsubstandardcareplanningandcoordination,poormanagementofhighriskcasesandmedicalemergencies,lackofsupervisionofjuniormedicalstaff,inadequatestaffskillsprofileintheAdultSpecialCareUnit,substandarddocumentationadverselyaffectingcarecontinuity,andpoormethodsofidentifying,reviewingandresponding to adverse events.
CARE PLANNING AND COORDINATION
Detailedcareplansweregenerallynonexistent.Poorcareplanningwasparticularlyaproblemincasesofpre-termlabourorpre-termruptureofthemembranes.Insomecases,consultantsmademajorchangestocareplanswithoutprovidinganywrittenrationale.Casereviewsandstaffinterviewshighlightedarepeatedlackofcarecoordinationandasensethatnoonewasreallyincharge.Sometimessomanyclinicianswereinvolvedinacasethatpatients,familiesandstaffreceivedconflictingadviceandfragmentedcare.

83
MANAGEMENT OF HIGH RISK CASES AND COMPLEx CARE
Juniordoctorsdeliveredmostofthecareatthemostcrucialtimesfor70%ofthe372highriskobstetriccasesreviewed.Thiscareincludedclinicalassessment,clinicalmanagementdecisionmakingandintervention.Consultantswereinvolvedatthemostcrucialtimesin21%ofhighriskcasesandseniorregistrarswereinvolvedatthemostcrucialtimesin9%ofthese.Hospitalmanagement and staff frequently raised the inadequacy of the supervision of junior doctors. ParticularproblemswereevidentintheDeliverySuite,theAdultSpecialCareUnitandtheEmergencyCentre,wherejuniordoctorsgaveunsupervisedcaretohighriskpatientsrequiringcomplexcare.Thereweremanyoccasionswhenregistrars(oftenjuniorsthemselves)werebusysomewhereelseandunabletorespondtourgentrequests.Juniordoctorswereoftenlefttomanagedifficultcaseswithouthelpandwithoutthenecessaryskillstodothejobsafely.
Asanexample,juniordoctorswereoftenresponsibleforwomenwhopresentedtotheEmergencyCentrewithpotentialectopicpregnancies.Sometimestheyfailedtodiscussacaseortohavethecasereviewedbyaregistrarorsomeonemoresenior.TheHospitallackedapolicy to support the management of ectopic pregnancy.
Anotherlongtermandwidespreadproblemwasjuniordoctors’inabilitytointerpretaccuratelyandrespondtoabnormalfoetalhearttraces(cardiotocographyorCTGs),ataskassignedtothemforwhichtheylackedtrainingandsupervision.
MEDICAL AND OBSTETRIC EMERGENCIES
Thereweremanyseriousproblemsfoundwiththemanagementofpatientswithpostoperativeshockandhaemorrhage.Fluidandelectrolytebalancewaspoorlymanaged,andcasereviewsrevealedinadequatemanagementofantepartumhaemorrhage,ruptureduterusinlabour,majorpost-partumhaemorrhage,hypertensivecrisisandnewbornresuscitation.TheHospitallackedclearandcurrentpoliciesforsuchcasesandlackedsuitablestafftrainingprogramsthataddressed these situations.
ADULTSPECIALCAREUNIT
WomenneedingfullintensivecarewereputatriskbybeingadmittedtotheAdultSpecialCareUnitbecausecarewaslefttounsupervisedjuniordoctors.TheUnithadnospecialist’intensivists’onitsteamandonlyonenurseontheUnithadintensivecaretraining.
TheUnithadahistoryofpoorcarecoordinationandinadequatesupervisionofjuniordoctors.Juniordoctorslackedadesignatedsupervisorandthey,andnonspecialistnurses,wereoftenlefttodealwithhighlycomplex,sometimeslifethreateningsituations.Clinicalaccountabilitywaslacking,withnoonedoctordesignatedas‘incharge’ofacase.OfthewomenwhodiedintheUnitbutwereexpectedtolive,ahighproportionhadradicalgynaecologicalandbowelsurgery.Thesewererecognisedhighriskcasesrequiringintensive care in the immediate post-operative period.
DOCUMENTATION
Documentationwasoftenincomplete,lackingimportantclinicalinformationneededtosupportcontinuityofcare.Ofallcasesreviewed,thecareplanwasinadequateornonexistentin20%ofcasesandimportantdocumentationwasinadequatein35%ofcasesandmissing in �5% of cases.

84 Patient Safety: a comparative analysis of eight Inquiries in six countries
The quality and completeness of documentation varied across the Hospital. Outcomes of discussionswithseniorstaffwererarelynoted.Inmostcasesitwasimpossibletodeterminetheextent of a consultant’s involvement in decisions about care. Senior medical staff provided some of theworstexamplesofpoorrecordkeepinganditwasrareforaconsultanttodocumentaplanorrecord care.
Mostentrieswereillegibleandmostsignatureswereindecipherable.Filenotesweredisjointed,incompleteanddisorganised.Pre-operativeassessmentwasusuallyabsentandmanynotesweresketchyanddifficulttounderstand.Privatephysiciansgenerallyfailedtorecordantenatalcareasareference for the Hospital clinicians.
CLINICAL ERRORS
Thecasesreviewedincludedcomplexcasesknowntobeatincreasedriskofclinicalerrors.Ofthe372highriskobstetriccasesreviewed,errorswerecommon.Themostfrequentwere’failuretorecognise a serious and unstable condition’ and ’inappropriate omissions’.
Ofthecasesreviewed,oneormoreclinicalerrorsoccurredin47%ofcasesand50%wereveryserious.Juniorresidentsmadeerrorsin76%ofhighriskcases,juniorregistrarsin65%ofhighriskcases,midwivesin60%ofhighriskcases,levels5and6registrarsmadeerrorsin34%ofhighriskcases,andconsultantsmadeerrorsin28%ofhighriskcases.
Ahighproportionoferrorswasratedasveryserious.Forallobstetricandgynaecologycasesreviewed,moreobstetricscaseerrorsoccurredoutsidebusinesshourswhentherewerefewerstaffandlesssupervisionforjuniordoctors,andthesewereoftenratedasveryserious.Theerrorsweremorecommonduringlabouranddelivery.Gynaecologicalcaseerrorsweremorecommonpost-operatively.Contributingfactorswerepoorcarecoordination,delayedcareandunsupervisedjuniorstaff.Nonexistentorinadequatepolicywasamoreprominentcontributingfactoringynaecologycases.
COMPARING PERFORMANCE
TheInquiryestablishedaConsortiumtocomparetheHospital’sobstetric,neonatalandgynaecologicalpracticesandperformancewiththoseof13tertiaryreferralhospitalsinNewSouthWales,QueenslandandSouthAustraliausingroutinelycollectedperinatal,hospitalmorbidityandneonataldata.TheConsortiumsupplieddetailedspecificationsoftheitemsrequired,notedthepreferredsourcedatabases,collectedandexamined37clinicalinformationitems,andattemptedtoidentifystatisticallysignificantdifferences.
Therewereanalyticalweaknesses,buttheConsortiumidentifiedsomeproblemareas.Theyincludedhighratesofstillbirths,obstetricinterventions,hysterectomiesfollowingpost-partumhaemorrhage,maternaldeaths,deathsfollowinggynaecologicalprocedures,andtransfersoffemalestotheAdultSpecialCareUnitduringadmissionsforlaparoscopicproceduresandhysterectomies. The Consortium recommended that the Hospital improved the quality and completeness of its monitoring information.
Clinicalpoliciesandguidelines
Policyandguidelinedevelopment,deployment,compliancemonitoringandreviewwerenotedasdeficitsduringthereviewperiod.Someindividualsmadeaconcertedefforttoimprove,buttheHospitallackedaneffectiveorganisationwideapproachtotheseactivities.

85
Overmanyyears,theHospitalfailedtoaddressseveralrelatedweaknesses.Theyincludedad hoc,untimelyandinfrequentdevelopmentandreviewprocesses,absenceofclearresponsibilityformanagingtheprocesses,delayedornonexistentapprovalofrevisedornewpoliciesandguidelines,lackofcommitmenttoamultidisciplinaryinvolvement,retentionofobsoletepoliciescontrarytobestavailableevidence,inadequateinvolvementofpatientsandfamiliesinpolicyandguidelinedevelopment,inadequateconsultationwithstaffaboutpolicyandguidelinechanges,inadequatedistributionanddeploymentofpoliciesandguidelines,anuncleardistinctionbetweenmandatoryanddiscretionarypoliciesandguidelines,inconsistentterminology,unclearlinesofauthorityforpolicyandprocedurereviewordeviation,andlackofastrategytomonitorandensurecompliance(althoughcompliancewaslow,particularlyamongsessional consultants).
Seniordoctorsweresometimesreluctanttoinvolvethemselvesinpolicymattersduetothetimerequiredtodothiswork.Juniordoctorsormidwivesandnursestendedtoworkonthesematters.Achievingaconsensusoftenappearedtotakepriorityoverthebestavailableevidence.Howeverconsensuswasseldomreached,soindecisionremained,resultinginoutdatedpoliciesand practices.
Theinquiryteamgaveseveralspecificexamplesofproblemswithpoliciesandguidelines.OnewasthatittooktheHospitalfouryearstoamendtheVitaminKAdministrationProtocolafteranincidentwithVitaminKadministrationinOctober1997.AbabyreceivedtwoVitaminKdosesin the birthing area. Several email exchanges about the incident failed to result in action to addresstheproblem.InApril1999,moreemailexchangesfocusedonareputableinterstatepositionstatementonVitaminKadvisingagainstitsadministrationinabirthingarea.Againtheemaildiscussionsfailedtoresultinaction.MoreemaildiscussionsfollowedandanewVitaminKprotocolwaseventuallyfinalisedinMay2001.
Anotherexamplewasthepoormanagementofpatientswithectopicpregnancies,whichwasidentifiedinJanuary1998.TheHospitalremainedwithoutapolicyattheendof2000.In1998,apatient’sectopicpregnancywasmissedindiagnosis.ThecurrentevidencesuggestedthatthepreferredmethodofmanagingectopicpregnancieswasbylaparoscopicprocedurebuttheHospital continued to perform laparotomies rather than laparoscopy for ectopic pregnancy. The incidentandtheevidencegeneratedmuchdiscussion,butthediscussionfailedtoeffectchange.Theissuewasconsideredbysometobetoocomplextoovercome.
Thebladdercarepolicytook24monthstoformulate.Thefinaldocumentprovidednoevidenceofliteraturerevieworclinicaltrialsasthebasisforitsdevelopment.Mostofthedevelopmenttimewasspenttryingtoachieveconsensus.
TherewereproblemswiththecordbloodRhtestingprocedurefromSeptember1997toJuly1999.Itwasintroducedasanewroutinetest,butdoctorsoftendidnotsigntheform.TheHospital’s Pathology Service estimated the Obstetrics Service missed approximately 20% of Rh-negativewomen.Auditresultsindicatedthatatleast63Rh-negativewomenweremissedin18months.Eventuallymidwivesweregivenauthoritytosigntheform.
Hospitalpolicystatedthataseniordoctormustsigntheconsentformsformajorsurgery,howeverjuniordoctorsweresigningconsentformsforcaesareansections.Evidencesuggestedthatforatleasttwoyears,residentshadlittleoptionbuttosignconsentformsformajorsurgery.

86 Patient Safety: a comparative analysis of eight Inquiries in six countries
TheInquirycommissionedfourexpertconsultantstoreviewseveralHospitalpoliciesandguidelines.TheyincludedtheClinicalGuidelines(1998),JuniorMedicalStaffManual(1998),GuidelinesforMidwiferyPracticeObstetricWards(1999),EmergencyCentreManual(1998),ProtocolforFoetalHeartMonitoring(1996),andProtocolforPerinealSuturing(dateomitted).
Theexpertconsultantsidentifiedmanydeficiencies.Themostcommonwerenoreferencetobestavailableevidenceandinsufficientreferencing,brevityandincompletecoverageofthetopic,nodevelopmentorreviewdateandnoauthor(s)listed,insufficientguidanceonwhentoreferacasetoamoreseniorclinician,inadequatedelineationanddescriptionoftheresponsibilitiesofclinicalstaff,nominimumskilllevelspecified,inconsistenciesbetweenthemanuals,invitationstostafftomodifytheguidelines,andirregularandinfrequentdocumentupdating.
Incidentreportingandmanagement
Thereweresignificantproblemswithincidentandadverseeventreportingandfollowupfrom1990to2000.Managementofcomplaintsandpotentialmedicalnegligencecaseswasalsopoorduringthistime.Overmanyyears,persistentproblemsincludedthelackofaclearandcurrentpolicyonreportingandrespondingtoincidentsandadverseevents,lackofasystemtoreport,reviewandrespondtoincidentsandadverseevents,lackofreportsforseriousincidentsandadverseevents,lackofaccountabilityonthepartofseniorcliniciansforidentifying,reportingandrespondingtoadverseevents,lackofinformationandsupportforpatientsandfamiliesexperiencingadverseevents,substandardmanagementofcomplaintsandpoortreatmentofcomplainantsandtheirfamilies,andmedicalmismanagementofcasesresultinginseriousadverseeventsanddeath.
HOSPITALPOLICY,STAFFATTITUDESANDOPINIONS
TheHospitaldefinedanincidentas“anyeventorcircumstancewhichcouldhavecaused,ordidcause,harm,sufferingorlosstoapatientorvisitor”.Twotospitaldocumentsreferredtotherequirementsforincidentreporting—apolicyonaccidentandincidentreportingandanaccident/incidentformwereinplacethroughoutmuchofthereviewperiod.Thesedocumentsappliedtoallincidentsincluding’nearmisses’andrequiredstafftoreportallincidentsimmediately,followedbyawrittenreporttothedivisionaldirectorwithin24hoursoftheincidentoccurring.
Manyincidentswerereportedorallyandneverdocumented.Itwasdifficulttodeterminewhoreportedanincident,howitwasreported,towhomitwasreported,andifanyactionwastakenfollowingtheincident.
The reporting process changed little over the �� years and a ’culture of blame’ prevailed during thistime.Staffgenerallyagreedthataccident/incidentformswereforreportingincidentsaboutintravenousdruguseandpatientfallsratherthanadversepatientoutcomesornearmisses,incidentreportingwasvoluntary,adverseeventswerereported“onlyifthestaffmemberfeelsstronglyenoughaboutit”andtheincidentreportingprocessappliedexclusivelytomidwivesandnurses.
Whenaskedaboutreportingincidentsandadverseevents,seniordoctorsraisedmanyconcerns.Theyincludedthetimeandpaperworkinvolved,fearofblameandlitigation,theirdiscomfortwithreportingseriousincidentsandbeingaccountableforactionsanddecisions,suspicionsthatmidwivesreportedincidentstocausediscomfortfordoctors,andthepotentiallyadverseeffectaformalincidentreportingsystemwouldhaveoncommunicationandteamwork.

87
UNDERREPORTINGOFINCIDENTSANDADVERSEEVENTS
Intheabsenceofafunctioninghospitalsystem,midwivesestablishedtheirownprocedurestoreportadverseeventsintheformofapaper-basedregister.Theregisterwasanunofficialandincompleterecordidentifying47incidentsfortheperiodJuly1998toJune2000.Ofthese,theInquiryreviewed30indetail,and19involvedmoderatelyunsafeorveryunsafepractices.
Ofthe605clinicalfilesreviewed,71caseswithmoderatelyunsafeorveryunsafepracticesoccurredintheObstetricsClinicalCareUnitfromJuly1998toJune2000.Ofthese,only19wererecordedin the Register. Staff frequently used email to report obstetric incidents. Staff in the Gynaecology ClinicalCareUnitreliedonwordofmouthratherthanemailtoreportincidents.TheUnithadnoregisterofincidentsandlessdocumentaryevidenceofincidentreporting.Whenaskedabouttherateofincidentreporting,seniorclinicianswereconfidentthatallincidentswerereported.
In1999,problemswithincidentreportingwerefrequentlydiscussed.Staffwereconfusedaboutwhowasclinicallyaccountableforreportingandrespondingtoincidentsandadverseevents.This confusion resulted in the Director of Medical Services often not receiving incident reports or onlyreceivingthemiftheywereassociatedwithpotentiallitigation.
TheHospitalCounselbecameawareofunderreportingofseriousincidentsin1999.Hesubsequently reported his concerns to the recently appointed Chief Executive about the lackofincidentreportingpolicy,thenumberofreportedincidentsandadverseevents,poorunderstandingoftherequirementsforincidentreportingamongstaff,andtheabsenceofaproper register of reported incidents.
POTENTIAL MEDICAL NEGLIGENCE CLAIMS
In1999,evidencepointedtoclinicalmismanagementofatleastfivecases,withthreeresultinginbabiesdyingandtwobeingbraindamaged,andpotentiallymultimilliondollarclaimsagainsttheHospital.Stafffailedtoreportmanyseriousincidents,includingincidentsresultinginmedicalnegligenceclaimsagainsttheHospital.Onsomeoccasions,thefirstnoticeofanadverseeventwasalawyer’sletterorothercorrespondencefromoutsidetheHospital.
TheChiefExecutiverespondedbydirectingthatallincidentsbereportedtohim,directingthattheHospital’slegalcasesbehandledbytheHospitalCounsel,commissioninganindependentauditbyErnstandYoung,anauditcompany,oftheHospital’sincidentreportingprocesses,andreportingthesituationtotheMetropolitanHealthServiceBoard.TheErnstandYoungReportfoundtherewasnodefinitionofwhatconstitutesaclinicalincident,nocurrentprocedurerequiringthereportingofclinicalincidents,andnopracticalmethodofidentifyingclinicalincidentshiddeninthecasefiles.
PROBLEMSWITHTHEQUALITYIMPROVEMENTACT
TheWesternAustralianHealthServices(QualityImprovement)Act1994providesfortheprotection of a quality improvement committee from disclosing its proceedings if the committee is registered under the Act and if it consistently and continuously meets the requirements of the Act.
Bytheendof2000,theHospitalhadnotregisteredanyofitscommitteesundertheAct.Seniordoctors said they failed to document incidents and adverse events because they believed the requirementsoftheActwereimpractical.TheywereconcernedthattheActrestrictedthedistributionofminutesofaregisteredcommitteetoothercommittees,andthatmemberswererestrictedfromdiscussingthecontentofameetinginothervenues.Thisbeingthecase,anincidentmightberaisedinanyofseveralcommittees,requiringtheHospitaltoregisteralargenumberofcommitteestoprotectsuchdiscussionfromdisclosure.Thiswasconsideredunworkable.

88 Patient Safety: a comparative analysis of eight Inquiries in six countries
TheInquiryconcludedthattheclaimedproblemswiththeActwereoverstated.Forexample,theprohibitionsondisclosuredidnotapplytoreportstoarelevantgoverningbody.Moreover,theHospitalhadtheoptionofreducingthenumberofcommitteesreviewingincidents,therebylimitingthe number requiring registration under the Act.
MANAGEMENT OF MEDICAL NEGLIGENCE CASES
Therewasevidenceofsignificantdelaysfromthetimeanincidentoccurredtolodgingareport.Thesedelaysraiseddoubtsaboutthetimelinessofpreparingthereportaftertheincident,andthereportcontentandaccuracy.Inthisregard,theHospitalfailedtomeetpublicexpectationsaboutinvestigatingseriouscomplaints,andhadlittlecapacitytolearnfromfailures.
ExamplesaregivenintheinquiryreportofpotentialmedicalnegligencecasesthatwereexaminedbytheHospitalCounselin2000,andfoundtohavebeenmishandled.Oneconcernedawomanwhosearterywasperforatedduringsurgery,thusrequiringcorrectivesurgery.Theinvolvedstafffailedtoreporttheincident.Fourmonthslater,theHospitalCounselreceivedaFreedomofInformationapplicationfromthepatient’slawyers.Untilthattime,theCounselwasunawaretheincidenthadoccurred.Cliniciansinvolvedintheincidentfailedtocompletewitnessstatementsatthetimeoftheincidentorsoonafter,andhospitalmanagersfailedtoinvestigatetheincidentandnotify the medical litigation insurer.
Anotherexampleconcernedawomanwhowasadmittedinlabour.Shehadahistoryofpermanentbackinjuryfromaseriouscaraccidentandattendedananaestheticpainclinictwicepriortodeliveryto ensure adequate and appropriate pain relief in labour. Staff delayed inserting the epidural and onceinserted,itfailedtoprovideadequatepainrelief.Herbabywasdeliveredbyvacuumextraction,followedbymanualremovalofretainedplacenta.Thewomanexperiencedamassivepost-partumhaemorrhage,sheandherbabywereinshockandrequiredresuscitation.ThewomanwasadmittedtointensivecareandthebabywasadmittedtotheSpecialCareNursery.
Thewomanwasdischargedagainstherwishesandreadmittedtwodayslaterwithendometritisand‘retainedproducts’.SheremainedintheHospitalforfivedaysonintravenousantibioticsandsufferedongoingpelvicpain,dyspareuniaandpelvicinfectionfollowingthebirth.
Onemonthafterthebirth,thewomanformallycomplainedtotheHospitalabouthertreatment.Atthetimeofthecomplaint,nursescompletedwitnessstatementsandforwardedthemtotheNursingDirector.Twomonthslaterthewomanmetwiththreestaffmemberstodiscussherissues.Amonthlater,shewrotetotheChiefExecutivestatingthathercomplaintremainedunresolved,andshehadyettoreceivecopiesofthewitnessstatementsaspromisedatthemeeting.
Fivemonthslater,theHospitalreceivednoticeofanimpendingclaimagainsttheHospitalfromthewoman’ssolicitors.Twomonthsafterreceiptofthenotice(andtenmonthssincetheincident)thedoctorsinvolvedinthecaseforwardedtheirwitnessstatementstotheirDirector.
MEETINGSTOREVIEWANDRESPONDTOINCIDENTSANDADVERSEEVENTS
Meetingswereheldfromtimetotimetoconsiderincidentsandadverseevents.Howeverreportableincidents,definitionsandproceduresforincidentreportingandlinesofresponsibilityforincidentreportingremainedunclear.Themeetingsalsofailedtoaddressthestrongcultureofblame,unclearaccountabilityforreportingandrespondingtoincidentsandadverseevents,unacceptabledelaysinresponseorlackofresponsetoincidentsandadverseevents,doctors’resistancetotheinvolvementofnursesandmidwivesinincidentreview,andineffectiveorabsentmeasurestoensurechangesoccurredandwerecommunicatedtoclinicians.

89
Thesituationimprovedin2000,afterthenewlyappointedChiefExecutivedirectedthatchangesbemadeinincidentreportingandrelatedmatters.However,theinquiryteamconcludedthatconsiderablymoreworkwasrequiredtoaddressthelongstandingproblems.
ReportingdeathstotheCoroner
The Inquiry found that the Hospital failed to report several reportable deaths to the Coroner duringthereviewperiod.Reportabledeathsincludethosethatappearedtohavebeenunexpected,unnaturalorviolent,orthoseoccurringduringananaesthetic.Ofthe605casesreviewed,eightreportabledeathswerefoundandsentbytheinquiryteamtotheCoroner.Ofthese,thecareofwomenandbabieswasrated‘veryunsafe’insixcasesand‘moderatelyunsafe’ in one case. The Coroner advised that none of these deaths had been reported previously.
ACTIVITIESOFTHEMATERNALANDTHEPERINATALANDINFANTMORTALITYCOMMITTEES
TheWesternAustralianGovernmentestablishedtheMaternalMortalityCommitteeandthePerinatal and Infant Mortality Committee under the Health Act �9�� to examine maternal and perinatal deaths. Both committees functioned ineffectively over the �� years covered by the Inquiry.
Thereappearedtobesignificantflawsinthelegislation.VariousprovisionsoftheHealthActgovernreportingofperinatalandinfantdeaths.Manyoftheseareinconsistent,andimposemultiplereportingrequirementsonhospitals.Forexample,asinglestillbirthmayrequiresixreportsregulatedbyfiveseparatestatutoryprovisions.
Compliancewithreportingandinvestigatingmaternal,perinatalandinfantdeathswasinadequate. The inquiry team concluded that many aspects of the legislation governing the reportingandinvestigationofmaternal,perinatalandinfantdeathsappeartohavebeenignoredoroverlookedbytheCommitteesinthestudyperiod,includingprovisionswithsubstantialpenaltiesfornoncompliance.SignificantdefinitionaldifferencesexistedbetweentheCommitteesandtheAct,furthercompoundingtheproblemsassociatedwithreportingthesedeaths.
TheExecutiveDirectorforPublicHealthfailedtocomplywithstatutoryobligationsforissuinganinvestigatoradirectiontocompleteaninvestigationwithinaspecifiedtimeframe.Theresultwasdelaysofuptofiveyearsforinvestigationsofdeaths.
WhileinvestigatingtheHospital’smaternaldeaths,theMaternalMortalityCommitteedelayedinvestigationsforapproximatelyfiveyearsforthreeofthefouridentifieddeaths.Thefourthinvestigationwasdelayedovertwoyears.TheCommitteeproducedonetwopagereportfortheyears �989 to �99�.
Ofthe2,476identifiedperinatalandinfantdeathsinWesternAustraliafrom1990–1999,only150wereinvestigatedandreviewedbythePerinatalandInfantMortalityCommittee.TheCommitteerarelymet,andtherewasevidencethatitactedbeyonditspowersbyexcludingcategoriesofdeathsfrominvestigationandreview.TheCommitteealsofailedtorevealthe‘de-identified’substanceofcommentstoanyonebeyondthepeopledirectlyinvolvedinmanagingparticularcases.Before1991,theCommitteeproduced10reportsandpublished17educationalpapers.Afterthatdate,itfailedtoproduceanyreportsorpapers.

90 Patient Safety: a comparative analysis of eight Inquiries in six countries
Staffandstaffingmatters
TheHospitalhadsignificantlongtermproblemswithconsultantcover,accountabilityforclinicalcare,supervisionandtrainingofjuniordoctors,credentialling,andprovisionofadmittingprivileges.Therewasevidenceofseriousproblemswithperformancemanagementandwiththeconsultantappointmentandreappointmentprocesses.Overmanyyears,persistentproblemsincludeddeficienciesinconsultantcoverandchronicunderstaffing,lackofsuccessionplanning,poorlydefinedclinicalresponsibilityandaccountability,inadequatesupervisionofjuniordoctors,particularlywhenmanagingcomplexcases,inadequateorientationandtrainingprogramsforjuniordoctors,lackofanyformalandeffectivecredentiallingprogramfordoctors,inadequatearrangementsforapprovingadmittingrightsforvisitingdoctors,inadequaterecruitmentandappointmentproceduresforseniordoctors,andlackofaneffectiveperformancemanagementprogram.
CONSULTANTCOVER
Therewasevidenceofmanydiscussionsovermanyyearsabouttheproblemswithconsultantcover,particularlyforhighriskcases.Factorscompoundingtheproblemincludedsmallconsultantnumbersandinadequateconsultantuse,budgetconstraintsandrecruitmentdifficulties,themixoffulltimeandsessionalconsultants,andthedecreasingprofileoftheUniversityDepartment.
However,littlewasdonetochangethesituationuntilthearrivalofthenewChiefExecutivein1999andeventhenthereweredelays.Clinicalleadersfailedtoprovideaclearquantitativeevaluationofpresentandfutureconsultantcoverneedsfortheirareaofresponsibility,despiterepeatedrequestsfromtheChiefExecutive.JointinputfromtheHospitalExecutiveandtheDirectoratestodeterminerequiredcoverwasadifficultanddrawnoutprocess.TheChiefExecutivefinallyreceivedalistofoneunit’smedicalstaffingrequirementsaftereightmonthsandrepeatedrequests.TherewasalsoasignificantdelayinsecuringsufficientcoverfortheDeliverySuite,andtheroleofDeliverySuiteConsultant lapsed for approximately three years from mid �996.
CLINICALACCOUNTABILITY
Therewereseriousandongoingproblemswithclinicalaccountabilityoverthe11years.Staffspentmuchtimediscussingtheissue,tothepointthatitwasdescribedasa‘runningsore’.Consultantsidentifiedasresponsibleforclinicalcarewerenomorethannominallyresponsible.Therewerenumerousdiscussionsaboutwhichdoctor’snameshouldappearonapatient’sbedcard,buttheissuewasneversatisfactorilyresolved.
Duringallthis,juniordoctorsfacedwithdifficultclinicalcaseshesitatedandoftendidnotcallaconsultant for advice for fear of being labelled as unable to cope. Despite hospital policy requiring juniordoctorstoseekseniorclinicianadvicewhennecessary,theculturewasunsupportiveofthisapproach,resultingindelayedordeficientcare.
TherewererepeatedproblemsconcerningconsultantlinesofresponsibilityintheLabourWard.Theproblemsappearedtobeduetocliniciansrepeatedlyfailingtocomplywithpolicy,andclinicalmanagersfailingtoenforcecompliance.Theproblemwasdebatedformorethantwoyears,anddespitesolutionsbeingoffered,remainedunresolved.
JUNIORDOCTORS’SUPERVISION
SeniorHospitalstaffhadbeenawareofproblemswiththesupervisionofjuniordoctorssincetheearly1990s,buttheytooklimitedactionuntil2000.Oneproblemwasthatahighproportionofemergencyadmissionsoccurredafterbusinesshourswhen(withafewexceptions)onlyjunior

9�
doctorswereonduty.Casecomplexityafterbusinesshourswassimilartothatduringbusinesshours.However,juniordoctorsreceivedlittleornosupervisionfromtheconsultants,whowereconsideredthe‘lastlinkinthechainofcommand’andwereonlyrosteredondutyinbusinesshours.Hospitalpolicywastohaveaseniordoctoroncallratherthanonsiteafterhours.
Juniordoctorswereexpectedtodecideforthemselveswhentheyneededassistance,ratherthanseniordoctorsdeterminingwhenajuniorwassufficientlycompetenttoprovideunsupervisedcare.Whenaskedhowjuniordoctors’performancewasassessed,aseniordoctorexplainedtotheinquiryteamthat“…wejusthaveafeelforthesepeople”.
Juniordoctorswerereluctanttocallseniordoctorsandtherewasevidencethatseniordoctorssometimesfailedtorespondtojuniordoctors’callsforassistance.Midwives(andotherseniornurses)thereforeplayedanunofficialbutimportantroleintrainingandadvisingjuniordoctors.However,asinmanyhospitals,therewasnoformalrecognitionofthischannelofcommunication,andthereforeitwaslargelyunmanaged–andconsequentlynotsubjecttoformalreviewintheinterestsofimprovement.
Improvementstojuniordoctors’supervisionweremadein1999.However,theinquiryteamconcludedthatfurtherchangeswereneededtomaintainsafelevelsofsupervision.
CREDENTIALLING
TheHospitaldefinedcredentiallingastheprocessbywhichmanagement“…determinedtheclinicalprivilegesthat…allowamedicalpractitionertopractiseintheHospital”.Credentiallingprocesseswerelongconsideredinneedofimprovement.
Theywereraisedasaseriousissuein1991andagainin1994duringtheaccreditationprocessundertakenbytheAustralianCouncilonHealthCareStandards.Inter alia,theHospitalwasadvisedtoreviewitscredentiallingprocessassoonaspossible.However,hardlyanychangesweremade,andtheHospitallackedanadequateformalcredentiallingprocessuntilJune2000.
In1995,partlyinresponsetotheintroductionofnewtechnologies(includingendoscopicprocedures),theDirectoroftheGynaecologyClinicalCareUnitadvisedUnitstaffthatacredentiallingstatuslistwouldbedeveloped.However,thelistwasnotpublisheduntil1997,anditwasnotregularlyupdatedorwidelycirculated.
Therewasnoevidenceofacredentiallingcommitteemeetingfrom1997to1999.In1999,gynaecologyandoperatingsuitestaffwerestillrelyingontheoriginalcredentiallinglistthatwasdevelopedin1995.ThecredentiallingcommitteewasfinallyestablishedinFebruary2000,butthecredentiallingprocessitselfwasyettobeestablished.Thereweremanyexamplesofadirectorverballygrantingcredentiallingstatusovermanyyearswithlittlebasis.Operatingsuiteandbookingstaffoftenreceivednonotificationofthesearrangements.ThecontinuinginadequacieswerenotedintheChildandGloverReportin2000.
TheTermsofReferenceofthecredentiallingcommitteewerefinallyendorsedinJune2000.However,theymadenomentionofthecredentiallingofregistrarsorjuniormedicalstaff,andconsultantscontinuedtotheircompetencywithoutanyclearlydefinedcriteria.TheCommitteemet again in August 2000. It adopted a formal credentialling policy and a credentialling applicationformwasacceptedatitsSeptembermeeting.TheCommitteedidnotmeetagainuntil March 200�.

92 Patient Safety: a comparative analysis of eight Inquiries in six countries
ADMITTINGPRIVILEGES
Therewasasimilardegreeofimprecisionandconfusionregardingadmittingprivilegesforassociateconsultantsoverthe11yearsthatwerereviewed.Thepolicywasadjustedin1994,andremainedunchangeduntilJune2000.Thepolicyrequiredasmallcommitteetoreviewassociateconsultantadmittingprivilegesonanannualbasis.However,therewasnoevidenceofreviewsoranyaccreditation of general practitioner obstetricians.
ORIENTATION AND TRAINING PROGRAMS
TheHospitallackedaneeds-basedorientationprogramforjuniordoctors.Theprogrammainlyaddressedadministrativeaspectsofwork,anddidlittletohelpdoctorstounderstandclinicalprocessesanddeveloptheirownclinicalskills.Nordidtheprogramprovideanysupportforajuniordoctormovingfromaclinicalareatoanother.TheHospitalalsolackedanorientationprogramforregistrars.
Theneedsofjuniordoctorsfromoverseaswereoverlookeddespitetherebeingevidencethattakingtheirknowledgeforgrantedledtomishaps.Staffraisedmanysuggestionsregardingimprovementsintheorientationprogram,butitremainedunchangedoverthe11years.Theinquiryreportgaveseveralexamplesofdeficientornonexistenttrainingprograms,andsomearesummarisedbelow.
POSTGRADUATEMEDICALPROGRAM
Thisprogramwasdescribedas“…ahaphazardcollectionoftutorialsandclinicalmeetings”thathadneverbeenformallyplannedandhadnolearningframework.Itfailedtoidentifyoraddresspostgraduatelearningneedsinanyorganisedwayandtooknoaccountoftheresidents’andregistrars’rosters.Oneconsequencewasthatitwaspoorlyattendedbecauseresidentsandregistrarswerenotgiventimeofffromtheirclinicalresponsibilities.However,manyseniorcliniciansattributedpoorattendancetolackofcommitmentonthepartofthejuniordoctors.
TheHospitalwasanaccreditedRoyalAustralianandNewZealandCollegeofObstetriciansandGynaecologists(RANZCOG)traininghospital,andwasrequiredtomeetRANZCOGstandards.The1991RANZCOGaccreditationreportidentifiedsignificantdeficienciesincludinginadequatesupervisionofjuniordoctorsbyconsultantsoutsidebusinesshours,aninadequateongoingtutorialprogram,andpoorprogramscheduling.TheReportoftheRANZCOGreviewvisitin1993statedthatthedeficiencieshadbeenremedied.However,theInquiryfoundthatthiswasnotthecase.RANZCOGdidnotassesstheHospitalagainduringthereviewperiod.
GYNAECOLOGICALSURGICALTRAINING
Doctorsexperiencedtoofewgynaecologicalsurgicaltrainingopportunities.Thiswasmainlybecauseofshortageofavailablegynaecologicalsurgery,cancellationofelectivesurgeryduetobudgetcuts,andmorepatientsusingotherhospitalsforgynaecologicalcare.
Only consultants (and not registrars) received supervision and training in laparoscopic surgery from1995to1999.InOctober2000,theHospitalintroducedacompulsorytrainingprograminendoscopicsurgerybutfailedtoestablishaframeworkwherebytrainingwouldbeformalandongoing.
CARDIOTOCOGRAPHY(CTG)INTERPRETATION
Senior doctors at the Hospital recognised the importance of training clinicians in CTG as early as 1989.In1990,theHospital’s1990FoetalMonitoringServiceManualdirectedthatallnewstaffmustbecompetentinCTG,trainingcoursesmustbeconductedeverythreetofourmonths,andcompetencymustbeverifiedbywrittenexaminations.

93
However,practicewasinconsistentwithwrittenpolicy,andconcernswereexpressedregardingtheskillsofresidentsandregistrarsininterpretingCTGsovermanyyears.RecommendationsregardingcompulsoryCTGtrainingcoursesforregistrarsandresidentswerenotimplemented.TheHospitallackedasystemtoensurethatregistrarsandresidentsattendedformaltraining,weretrainedbeforeworkingintheLabourWard,andhadtheircompetencycheckedbeforetheyassessed and managed a patient using CTG.
TherewereinconsistentapproachestotrainingmidwivesanddoctorsinCTGinterpretation.Juniordoctors’trainingwasirregularandinfrequent,andthismeantthattheresponsibilityforinterpretationwasoftendevolvedtomidwivesintheLabourWard.Themidwives,ratherthantheregistrars,wereoftentheteachersofresidentsregardingtheinterpretationofCTGtracesintheLabourWard.NoonehadsoleresponsibilityforcoordinatingCTGtrainingforjuniordoctors.MidwiveshadawellorganisedandregularCTGtrainingprogram.Theinquiryreportnotedthattraining inconsistencies in CTG interpretation remained at the end of 2000.
PERINEALSUTURING
Similarproblemsexistedwithjuniordoctors’lackofskillsinperinealsuturing.TheHospitalfailedtoimplementasuitableeducationprogram,noonehadsoleresponsibilityforensuringdoctorsweretrainedintheprocedure,andtheHospitallackedaprocesstoensuredoctorswerecompetent to perform the procedure.
Bothmidwivesanddoctorsdidperinealrepairs,andmidwiveshadawelldevelopedtrainingprogram including a system for supervision and competency assessment. Doctors had no formaltrainingprogramandthetrainingtheyreceivedwasad hocandinformalwithnoskillsassessment.
Juniordoctorswereexpectedtocallforsupervisioniftheyfelttheyneededit,buttherewereexamples of incompetent practice by residents and registrars. The Hospital held perineal-suturingworkshopsfordoctorsin1997and2001.Amidwifeconductedtheworkshopsandattendancewasvoluntary.
EMPLOYMENTISSUES
Thereweresignificantdeficienciesinprocessesofrecruitment.Thedevolvedmanagementstructuremeantthatreliancewasplacedontheclinicaldirectors’abilityandwillingnesstomanage,andtheirpositiondescriptionsreflectedthis.However,therealitywasthatatleastsomemedicaldirectorsdidnotaddresstheirmanagementresponsibilitieswithdiligencewithregard to staff appointments.
Manyexampleswerepresentedintheinquiryreport,althoughitsinvestigationswereconstrained because the Hospital had destroyed a large proportion of the documentation regarding appointments. One involved the appointment in �996 of the Medical Director of the ObstetricsClinicalCareUnit,wherenoconsiderationwasgiventothemanagementskillsoftheapplicants.
Anotherexampleconcernedtherecruitmentofasessionalconsultantanaesthetist.Hewasappointedwithoutsubmittingaformalapplication,withoutbeinginterviewed,andwithoutaresponsefromeitherofthetworeferees.Fivemonthsafterrecruitment,theanaesthetist’sclinicaljudgementandskillswerequestionedonseveraloccasionsregardingadversepatientoutcomes.Theanaesthetist’sappointmentwasterminatedamonthlater.

94 Patient Safety: a comparative analysis of eight Inquiries in six countries
Deficiencieswereidentifiedinnineothercasesofseniormedicalappointmentsthatwereabletobeinvestigated.Theyincludedincompletedocumentation,failuretocontactreferees,failuretouseaconsistentselectionprocess,andlackofinputfromamedicaladministratororahumanresources specialist.
Therewerealsoproblemswithconsultantreappointment.Underthe1987Award,sessionalconsultantsshouldhavebeenappointedforfiveyears,andthereforetheyshouldhavebeenconsideredforreappointmentin1992.However,thefirstrecordedreappointmentofconsultantsoccurredinMarch1997.ThereappointmentprocesswassuperficialandtheSelectionCommittee’sperformancewassubstandard.TheCommitteeregardeditselfashavingresponsibilityforthefinalstepinappointingandreappointingconsultants,buttheChiefExecutiveshouldhavebeenresponsibleaccordingtotheAward.ThelonghistoryofCommitteeappointmentrecommendationsbeingacceptedwithoutquestionceasedwhenthenewChiefExecutivewasappointedin1999.
PERFORMANCE MANAGEMENT
Therewaslittleevidenceofmanagersorseniordoctorsparticipatinginperformancemanagement,andtheHospitalhadnoformalperformancemanagementprogramuntil1997.Theprogramwasjudgedunsuitableformidwives,andthereforetheyestablishedtheirowninformalperformancemanagement process.
Consultantperformanceappraisalswererarelydone,althoughhospitalpolicyrequiredthemtooccureverythreeyearsthroughacommitteeprocess.Registrars’performanceappraisalswereconductedbytheHospitaluntil1996,andthenbytheRoyalAustralianandNewZealandCollegeofGynaecology(whichfailedtogivetheHospitalaccesstothereviews).Residents’performanceappraisalswereconductedregularlyfrom1990to2000.However,someappraisalformswerecompletedafteraresidentleftanarea,andtheregistrarsassessingtheresidentsmayhavehadinsufficientexperiencetoappraiseperformance.
Patientinvolvement
TheInquiryinvestigatedtheperceptionsofwomenandtheirfamiliesregardingtheirinvolvementintreatmentandtheirinteractionswithstaff.Methodsincludedsecondaryanalysisof605clinicalfilereviewsand68interviewsofwomenwhoattendedtheHospital.Thefilereviewsrelatedtohighriskobstetricandgynaecologicalcases,andtheinterviewswerewithformerpatientswhoforwardedsubmissionsinresponsetotheInquiry’snewspaperadvertisements.
Theperceptionsofmanywomenandtheirfamilieswerethattheyreceivedlittleornoinformationabouttheirtreatmentoptions,risksorerrorsofcare.Duringthereviewperiod,womenandtheirfamilies reported inadequate information about their treatment and little or no involvement in decisionsaboutcare,inadequateinformationaboutincidentsandtheirfollowup,poortreatmentanddisrespectwhenmakingacomplaint,lackofsupportwhentheyexperiencedpooroutcomesoradverseevents,andpoorcommunicationwithHospitalstaffduringpotentialmedicalnegligencecasereviews.TheReportgaveseveralexamplesoftheperceptionsofwomenandtheirfamiliesaboutpoortreatmentandpoorcommunicationbystaff,asfollows:
n Failuretoprovideanadequateexplanationofpooroutcome.Awomanbelievedshereceivedincompleteandinaccurateinformationaboutthereasonswhyherbabydiedandfeltthatshewasbeingblamedforthecomplicationsthatoccurred.Inanothercase,parentsstatedthatstafffailedtocommunicatewiththemforsomehoursaftertheirbabybecameunexpectedlyill
n Failuretoincludeawomanandherpartnerindecisions.Aprivatepatientwantedtobetreatedasapublicpatient,butwassubsequentlygivenprivatestatus,whichresultedinexpensesshecouldnot afford to pay

95
n Lackofsensitivity,respect,dignityandsupport.Awomandescribedthedifficultysheexperiencedwithherunsettledbabyandwithpost-nataldepression,andsaidshefeltmisunderstoodandunsupported.Inanothercase,grievingparentsstatedtheywereputinanoldwardaloneandnoonecametoinformorsupportthemforseveralhours.Anotherexampleconcernedawomanwhoallegedthatadoctorrefusedtoperformacaesareansectionwhenshefeltherlifewasindanger.Thecaesareanwaseventuallydonebutthewomanhadtobemanagedinintensivecare.
CUSTOMERCOMPLAINTSPOLICY
Theinquiryteamconcludedthiswasoneofthefewexamplesofhospitalpolicythatdealtcomprehensivelyandclearlywiththesubject.However,therewereproblemsinpractice.Theyincludednoclearadviceforpatientsandfamiliesregardingthecomplaintsprocess,lackofrespectamonghospitalstaffforcomplainants,poorcoordinationofresponsetocomplaints,insufficientinformationtopatientsandfamiliesaboutwhatwentwrongandwhatwasbeingdonetorectifythesituation,nosinglefilingorcoordinationsystem,complainantsreceivingseverallettersratherthanone,andcomplaintsgenerallynotconsideredimprovementopportunities.
Qualityimprovement
Therewasnoevidenceofaneffectivehospitalwideprogramtomonitorandimprovethesafetyandqualityofcareduringthereviewperiod.Overmanyyears,theHospital’sprocedureswereinadequatewithregardtomonitoringkeyaspectsofcareandrespondingtopoorperformance,responsestorecommendationsarisingfromaccreditationprocesses,evaluationoftheeffectivenessofdepartmentlevelqualityimprovementactivities,andmanagementsupportforongoing improvements in the safety and quality of care.
TheHospitalwasaccreditedatonestagebytheAustralianCouncilonHealthcareStandards.However,thefocuswasonhospitalstructuresandprocessesratherthanthequalityofcare.AssessmentofqualityofcarewasgenerallylefttoHospitalstaffthroughinternalqualityimprovement programs. The inquiry team concluded that the accreditation process of that time wereinsufficienttoprovideassuranceofqualityattheHospital.
Therewaslittleevidenceofqualityassuranceactivityfrom1990to1993.Somedepartmentsconductedactivities,buttheextentandeffectivenessoftheseactivitieswasunclear.Inlate1993,staffdevelopednewdocumentationonthenatureofandplansforhospitalwidequalityimprovement.However,activitiesonthegroundremainedsubstantiallythesame.
Theresponsibilityforidentifyingandaddressingproblemsinpatientcareandsafetywasdevolvedtothedepartments.Therewasnoevidencethatthedirectoratesestablishedeffectivequalitymonitoringandimprovementsystems,andtheExecutiveandBoardofManagementplayednopartinthisprocess.Thequalityimprovementcommitteestructurewasestablished,butqualityactivitiesandoutcomeswereseldomreportedbeyonddepartmentlevel.TheInquiryfoundnoevidenceofclinicalquality activities being considered and coordinated by the Executive or the Board and no evidence of leadership to ensure safe and appropriate patient care.
TheChiefExecutivereportedseveraldeficienciestotheMetropolitanHealthServiceBoardin2000.They included failure to implement processes and systems to identify problems in patient care and safetyortomeasurethestandardofpatientcare,failuretocoordinateandoverseethemanagementoftheclinicalqualityprogram,failuretoconductclinicalauditsofpatientcareandsafety,nocontinuous or ongoing quality improvement (but rather ad hocqualityactivities),failuretofocusontheoutcomesofqualityactivitiesortofollowupandimplementtheresultsofthoseoutcomes,lackof

96 Patient Safety: a comparative analysis of eight Inquiries in six countries
coordinationbeyonddepartmentleveloftheclinicalqualityprogram,andvaryinglevelsofsupportfromstaff for quality improvement (and particularly little support from the medical staff).
Otherleadershipandmanagementissues
TheHospitalfailedtoaddressproblemsassociatedwiththedevolvedmanagementstructure,andfailed to resolve long standing clinical and management problems affecting the safety and quality of care. The �995 Business Plan to change to the devolved management structure involved establishing’ClinicalDirectoratesProductLineManagement’.Theprimarygoalwastodevolveresponsibility and authority to clinical staff to support better patient care. This structural change failedtoresolveandinsomecases,exacerbatedunclearaccountabilityandresponsibilityforthequalityandmanagementofclinicalcare,unclearlinesofauthorityandresponsibilityforcompliancewithHospitalpolicy,ill-definedorabsentsystemsforcarecoordination,safetyandquality,andlackofdecisionmakingonimportantandlongstandingpatientandstaffwelfareissues.
Themanagementstructurewasmeanttodevolveresponsibilityandauthoritytoclinicalstafftosupport clinical decisions and improve communication for more integrated quality patient care. But the structure had no senior management involvement to strengthen and support the devolution and clinicalservicedecisions,andnoonemadedecisionsorchangestoaddressproblems.Decisionswereputinthe‘toohard’basket.Problemswereignoredordenied,orthepeopleraisinganissuewerecriticised.Longstandingmatterswerereferredtooneormorecommittees,generatingmuchcorrespondencewithlittleornosubsequentactionorproblemresolution.
Insomecases,thereasongivenforfailingtochangeoutdatedpoliciesortocompareperformancewithsimilarservices,wasthattheHospitalwas“aunique,world-classservice”anditwasassumedthatclinicalservicecomparedfavourablywithotherorganisations,althoughthiswasnevertested.TherewasalsolittleeffortontheHospital’sparttoimproveitsrelationshipwiththeUniversity.Astrong,effectiverelationshiphadthepotentialtoimprovetheHospital’sevidencebaseforobstetricand gynaecological practice.
A’sinkorswim’mentalityprevailedduringthereviewperiodandjuniordoctorswereexpectedtomanagecomplexcaseswithoutsupervision,andwereexpectedtoknowwhentheyneededsupervision.Therewasnorigorousprocesstodeterminewhenjuniordoctorswerecompetenttoprovidecare,juniordoctorswerereluctanttoseekhelpfromseniordoctorsandseniordoctorswereunresponsivewhenaskedtohelp.
6.4 RecommendationsoftheInquiry
Theinquiryteammade159recommendations,andthislastsectionprovidessomeexamplesofchangesandimprovementswhichhavebeguntobemadesincetheInquiry.Theprocessofimprovementhasbeenmonitoredinseveralways,includingamonthlyreviewbyacommitteechairedbytheDeputyDirector-GeneraloftheHealthDepartmentofWesternAustralia.TheMinisterhasreportedquarterlytoParliamentontheimplementationprocess.Followingaresomeexamplesof improvements:
SUPERVISIONOFJUNIORDOCTORS
Inearly2000,managementimprovedsupervisionofjuniordoctors,withleveloneregistrarsbeingsupervisedbyaseniorregistrarwhenajuniorisrosteredtoworkafterbusinesshours.RevisedHospitalpolicyalsorequiresaleveloneregistrarworkingintheLabourWardtobesupervisedbyasenior registrar onsite at all times.

97
AFTERHOURSCONSULTANTCOVER
InSeptember2000,managementapprovedthe’OncallAgreement’,requiringtheoncallconsultanttodothreeclinicalroundsduringtheweekdaysandalatenightroundonweekendsintheDeliverySuiteandAdultSpecialCareUnit.In2000,therewasstillnorequirementfor24hour onsite senior medical staff presence.
INCIDENT REPORTING
The Hospital established an incident reporting committee in �999. A single incident reporting systemisinplace,andmoreincidentshavebeenreportedsincethen.TheInquiryconsideredthesetoberudimentarychanges,withmoreworkneededtocreateapositiveworkenvironmentwhereerrorsaretransparent,andpeoplefeelcomfortabletodiscussincidentsasimprovementopportunities.
Several other changes and improvements have been initiated or are planned. They include revisingandupdatingclinicalguidelinesfordoctorsintheclinicalhandbook,updatingandreferencingthemidwiferypolicyandproceduremanuals,developingalistofsentineleventsandindicatorstoidentifyhighriskcases,reviewingandrevisingthedoctors’orientationprogram,reviewingalldoctors’positiondescriptions,reviewingthetermsofreferenceofkeyexecutivecommittees,receivingapprovalfromtheHealthDepartmentofWesternAustraliatopurchasenewcentralisedfoetalmonitoringequipment,makingprogresswithmedicalandnursingperformanceappraisals,establishingqualityplans,rejoiningtheAustralianCouncilonHealthcareStandardsandundergoingafullsurveyinMarch2002,establishingtheCredentiallingCommitteeanddefinedcredentiallingcriteria,andappointingfoursenioracademic obstetrics and gynaecology doctors.
6.5 Discussion
AreportontheKingEdwardMemorialHospitalInquirywasissuedbytheAustralianCouncilforSafety and Quality in Health Care in 2002. One of its sections provides a comparison of the King EdwardandBristolcases,andwesummariseandcommentbrieflyonitasawayofdrawingouttheissuesidentifiedintheKEMHreport.
The Australian Council for Safety and Quality in Health Care (the Council) describes the general contextoftheBristolcase,drawingmainlyfromfoursources(Swan1997a;Swan1997b;UKDepartment of Health 2002). It then notes several similarities.
First,bothcases“…arosefromwhistleblowersreportingseriousproblemsratherthantheproblemsbeingidentifiedandaddressedorpreventedthroughrigorousandroutinesafetyandqualitymonitoringsystems.”ItisfurtherstatedthatthewhistlebloweratBristolwasananaesthetist(DrBolsin)andatKingEdwarditwastherecentlyappointedChiefExecutive.
Thisseemsareasonablestatementtous,althoughanoversimplificationintheBristolcase.Aswehavenotedelsewhere,DrBolsinwasaprimaryactorbutmanymoreotherpeoplewereinvolvedinvariousroles–andnotonlyaswhistleblowers.
Thereportsfromtheinquiriesbothrecommendedwidespreadchangesatgovernment,boardandmanagementlevel.Thecoreoftherecommendationswastheestablishmentof“…acultureofInquiryandopendisclosure”andtheintroductionof“…systemstomonitorandimprovethesafety and quality of health care.”

98 Patient Safety: a comparative analysis of eight Inquiries in six countries
Inbothcases,eitherdirectlyorindirectly,therespectiveDepartmentofHealthreceivedinformationabout management and clinical performance problems that had not been addressed over a significantperiodoftime.Hereagain,theremaybeanoversimplification.TheUKDepartmentofHealthwassurelymoreculpableinthatithadbeeninformedofproblemsoveraperiodofeightyearsbeforeittookaction.
WeagreewiththelistofproblemsprovidedbytheCouncil.ItsreportnotesthatboththeBristolandtheKingEdwardInquiriesfoundevidenceof
n a closed culture and environment unsupportive of openly disclosing errors and adverse events
n failure of management to respond effectively to clinical problems raised by staff
n nonexistentorineffectivequalitysystemstomonitor,reportandrespondtoperformanceproblems
n nonexistentorineffectivesystemstoidentify,reportandrespondtoerrorsandadverseevents
n poorcommunicationwithpatientsandfamilies,particularlywhenthingswentwrong
n poor management of complaints and potential medical negligence cases
n inadequatetrainingandcredentiallingtoensurecliniciansweresufficientlyskilled
n inadequatestate-levelmorbidityandmortalitymonitoringandreviewsystems
n poor clinical and emotional outcomes for patients and families.
Thereweredifferencesofemphasis,however.Forexample,inthecaseofBristoltherewassomerelatively good comparative information on performance (including the statistics compiled by Dr Bolsin under a national research grant).
TheCouncilthennotedsomedifferences.Inparticular,itarguesthat“…BristolwelcomedanInquiryandactivelysupportedtheprocess.Incontrast,KingEdwardtoleratedtheprocessandtheWesternAustralian branch of the Australian Medical Association actively and publicly fought it (Media search:KingEdwardInquiry).Mediareviews(Mediasearch:BristolInquiry)suggestBristolactivelyengagedpublicinterestandparticipationintheprocess.Awebsitewasestablishedtoinformthepublic on the Inquiry’s proceedings and progress.” (Australian Council for Safety and Quality in Health Care 2002:27).
Wedonotagreeentirelywiththisview.ItistruethatBristolestablishedprocessestoinformandinvolvethepublicatlarge,butthislargelyoccurredonlyaftertheinquiryprocesswasunderway.Aswestateelsewhereinthismonograph,seniorstaffofthehospitalfoughtfiercelytoavoidpublicdisclosureoveraperiodofseveralyears.NorcanweseeanyreasontobelievethatthemedicalprofessionalassociationsintheUKwerelessinsularthantheAustralianMedicalAssociation.
6.6 Footnote
ThereportissuedbytheAustralianCouncilforSafetyandQualityinHealthCare(2002),alsoincludescommentsontheprocessoftheInquiryitself.Thecommentsareworthyofattentionhere.
First,theCouncilarguedthattherewerecontradictionsbetweentheTermsofReferenceoftheInquiryandthefinalcontentoftheReport.Inparticular,theinquiryteamhadbeendirectedtofocusonsystemsissuesratherthantheperformanceofindividuals.However,throughouttheReport,individualswerenamedandindividualbehaviourandactionswererecordedindetail.

99
TheCouncilarguedthatthevalueoftheinformationaboutindividualswasquestionable,particularlytothecommunityatlarge.Moreover,itprobablymadelittlecontributiontounderstanding and learning from systemic problems.
Second,itwasnotedthattheInquiryexperiencedstatutoryauthorityrestrictionsthathinderedtheefficiencyandeffectivenessofitswork.Witnessesandcounselhadinsufficientstatutoryprotection from personal liability under the Hospitals and Health Services Act and the Public SectorManagementAct,andtheInquiryhadinsufficientpowertoreferseriousmatterstotherelevantstateorCommonwealthauthority.
TheInquiryalsolackedassurancethatinformationandevidencegiventoorobtainedbytheInquirywouldbeprotectedfrompublicationaftertheInquirywascomplete.TheCouncilarguedthat,whenaninquiryisnecessary,itmaybemoreappropriateandusefultothehealthcaresystem,togivetheinquiryteamthepowerandprotectionavailableundertheRoyalCommissionAct.
Finally,theCouncilwasconcernedaboutthetimeandresourcesconsumedbytheInquiry,inrelation to its overall impact on the safety and quality of the health care system. The Inquiry occurredover18monthsandcost$7million,primarilytoidentifymanagementandclinicalproblems at one hospital. The Council argued that the resources might have been better applied totheestablishmentof“…effective,routinesafetyandqualitymonitoringstructuresandprocesses across the health care system that support and enable the improvement of safety and quality of health care.”
Asafootnote,webelievethesecriticismsmaybeunjustified.Weareparticularlydoubtfulofthelogicofthelast.Siddins(2003)notedthattheCommonwealth-StatesMedicareAgreementof1995allocated$658milliontofiveyearsofqualityimprovement.“Thisexpendituremayhavesilencedacommunitydemand.Regrettably,ithascontributedlittletowardsmeetinganurgentcommunityneed.In2003,nofundamentalreformhasbeenachievedwhereitismostneeded–atthecoalfaceofdailyclinicalpractice.”GiventhatasignificantproportionofthefundingwastosupporttheworkoftheAustralianCouncilforSafetyandQualityinHealthCare,wethinkitisalittleunfortunatethattheCouncilshouldimplythat$7millionspentontheDouglasInquirywasof questionable value.
6.7 Referencesandselectedbibliography
Australian Council for Safety and Quality in Health Care (2002). Lessons from the Inquiry into Obstetrics and Gynaecological Services at King Edward Memorial Hospital 1990-2000. Available at: http://www.health.wa.gov.au/kemhinquiry/index.htmlaccessedon3March,2006.
Child,A.andGlover,P.(2000).Report on the Obstetrics and Gynaecological Services at King Edward Memorial Hospital.ReporttotheMetropolitanHealthServiceBoard,WesternAustralia.Perth: Metropolitan Health Service Board.
Cowan,S.(2000).Yes,Minister,it’saWhitewash.The West Australian,25October:16.
Douglas,N.,Robinson,J.andFahy,K.(2001).InquiryintoObstetricsandGynaecologicalServicesatKingEdwardMemorialHospital.Perth:GovernmentofWesternAustralia.
Egan,C.(2000).MoodyRejectsGagContract.The Weekend Australian,28October:9.
Egan,C.(2000).Record-KeepingunderScrutiny.The Australian,25October:6.
Hickman,B.andEgan,C.(2000).Doctorsno-StateofHealth.The Weekend Australian,23October.

�00 Patient Safety: a comparative analysis of eight Inquiries in six countries
Hills,J.(2000).WhyDidsomanyBabiesDie?Sydney Morning Herald,8October:10.
Siddins,M.(2003).CommentaryontheKingEdwardInquiry:LessonsweFailtoLearn.Australian Health Review, 26(�): 28–9.
Weber,M.(2004).KingEdwardHospitalBabyDeathstobeInvestigated.PM,RadioNationalTranscript,12February.Availableat:http://www.abc.net.au/pm/content/2004/s1043963.htm Accessedon3March,2006.
7 RoyalMelbourneHospital,Australia
7.1 Context
InMarch2002,seriousallegationsweremadepublicconcerningtheconductofnursingstaffattheRoyalMelbourneHospital(RMH),whichispartofthelargercaredeliveryagencycalledMelbourneHealth.TheallegationsbecamethesubjectofinvestigationbytheCoronerandVictorianPolice.TheNursesBoardofVictoriasuspendedtheregistrationoftwonursesbutpostponeditsinvestigationsuntil the Coroner’s investigation had been completed. The Executive and Board of Melbourne Healtheachconductedseparateinvestigationsintoissuesassociatedwiththeallegations.Theoutcomeoflegalproceedingsispresentedinthefinalsectionofthispaper.
7.2 TheInquiry
Inviewofthehighlevelofpublicconcern,theMinisterforHealthimmediatelyrequestedtheHealthServicesCommissioner(HSC)toconductanindependentinquiry.Itwastoaddressgeneralissues,ratherthantheparticularcomplaintsthatwerethesubjectoflegalproceedings.MostofthefollowinghasbeentakenfromtheHSCreport(HealthServicesCommission2002).
TheTermsofReferenceindicatedsomebroadtopicsonwhichtheHSCwastoreport.TheyreflectedmattersthatwereunderinvestigationbytheCoronerandthePolice:medicationsmanagement; incident reporting systems; standards of documentation related to patient care; nursingmanagementandoverseeingofclinicalpracticeatwardlevel;andsystemsforstaffsupport.Theunderlyingagendawasthatofreassuringthepublicatlargethatstepswouldbetakentoprotecttheirsafety.ThustheHSCwasspecificallyrequestedtoadviseonanyaspectsofcarethatmightbeimprovedintheVictorianhospitalsectorasawhole.
TheHSCreceivedcooperationfromtheRMHandtheDepartmentofHumanServices,anditwasthereforenotnecessarytoinvokeformalpowers.Fortheseandotherreasons,theInquiryreportedhererepresentsastudyofpotentialriskstopatientsafetyratherthananinvestigationofparticularfailings.
MethodofconductoftheInquiry
TheHSCwasexpectedtoreportwithinthreemonths.Theshorttimeframewasunderstandable,giventhegovernment’sconcernforreassuringthepublicasrapidlyaspossible.Itsignificantlyconstrained the investigation team. It had to rely heavily on the assembly of opinions through interviewswithindividualsandgroups,theexaminationofasmallsampleofmedicalrecords,onsiteobservations,andconsultationwithexperts.

�0�
SuchanapproachwasinevitablyopentobiasonthepartofinvestigatorstoagreaterdegreethanmightbeexpectedfromotherinquiriessuchasBristolandCampbelltown-Camden.OtherlimitationsadmittedbytheHSCteamincludedalackofcomparativedata,aninabilitytointerviewstaffwhowouldhavebeenimportantinformantsbuttheynolongerworkedatRMH,theinfeasibilityofconductinginterviewsofpatientsandtheirfamiliesorcarers,andinsufficienttimefortheretobeacomprehensivecallforwrittensubmissions.
7.3 ConclusionsoftheInquiry
The conclusions are arranged under �2 main headings in the summary of the inquiry team’s report,andaslightlydifferentstructureisusedinthemainbodyofitsreport.Wehaveretainedthegeneralstructureofthesummarysection,butmodifiedsomeoftheheadingsandsplittwoofthesectionstomake15headingsinall.
SectorwideorganisationalchangesthataffectedRMH
HospitalsinVictoria(andparticularlythelargemetropolitanpublichospitalslikeRMH)hadbeensubjectedtomanychangessince1995.Onemajorchangewastheformationofhospitalnetworks,whereby35previouslyseparatefacilitieshadbeenaggregatedtoformsevenhospitalgroups(HealthCareNetworks)onapredominantlygeographicalbasis.In2000,changesweremadewiththeintentionofreducingthedegreeofaggregation,andthesevenhospitalgroupsbecame12.Anotherstatedgoalofthereviewwastocounteract“…anundueemphasisoncommercial viability at the expense of considerations such as the quality of patient care.”
Theinquiryteamconcludedthatthepredominantlystructuralchangesthatoccurredbetween1995and2000hadhadanadverseimpactonstaffmoraleandstandards.Theycoincidedwithcomplexitiesexperiencedbyallmetropolitanhospitalsincludingthefinancialimplicationsofscientificandtechnologicalchanges,increasedpublicscrutiny,increasingdemandsforservices,longwaitinglists,higherpatientacuityandshorterlengthofstay,widespreadnursingshortagesand increasing use of casual staff.
Effectsoffrequentchangesinseniormanagement
From1995until2000RMHexperiencedconsiderableleadershipinstability,whichwasthesource of much critical comment by staff. The inquiry team noted that staff considered there had beenalackofaccountability,afailuretoincludestaffindecisionmaking,alackofvisionandtoomuchfocusonfiscalmatters.Thisresultedinmistrustofmanagement,poorstaffmoraleandadrop in standards of care for patients.
Staffexpressedmoreconfidenceincurrentleadership.However,theyarguedthattherewerestillfewtangibleresultsatthelevelofservicedelivery.
Nursingleadership
TherehadbeenfiveDirectorsofNursingbetween1995and2000.Theirworkloadswereheavy,in part because of the organisational changes and the increased emphasis on productivity.
Theirdifficultieswereincreasedasaconsequenceofalargereductioninmiddlemanagementpositionsinnursing.Theinquiryteamconcludedthatnursingmanagerswere“…unabletomakethenecessarystructuraladjustmentstoprovideadequatesupportandmentoringtothelargenursingworkforce.”

�02 Patient Safety: a comparative analysis of eight Inquiries in six countries
Thesituationappearedtohaveimprovedafter2000.Theinquiryteamconcludedthatthenewnursingmanagershaveastrongcommitmentto“…re-establishstructurestoensurestaffarewellsupported to provide good patient care.”
Thecorporatevision
Theinquiryteamconcludedtherehadbeenalackoforganisationalcohesioninthepast.Itwasreportedthat‘somesenioradministrators’believe“…acultureofelitismexistswhichhasbeenconducivetoanattitudeofcomplacencyandlackofaccountability.Althoughthereisindividualandteam-basedcommitmenttoexcellencein-patientcareatRMH,organisationalgoals,valuesandmissionhavenotbeenwellarticulated.”
However,improvementswerebeingmade.Theyincluded“…thedevelopmentofafullyintegratedandsystematicapproachtopatientcareincludingtheimplementationofaconsultativeframeworktoachievechangesinstaffdevelopment,researchandeducationprograms,promotionofethicalbehaviour,andpatient-focusedcareandteamwork.”Astrategicplanhadbeencompletedandapproved by the Board.
Organisationalstructures
Weaknessesoffragmentation,andofconfusionoverresponsibilitiesandaccountabilities,hadcharacterisedtheRMHinthepast.However,managementteamshadbeenestablishedtoproviderelevantleadershipatthedivisionallevel.Suchteamswerecommittedtobeingfullyinformedaboutlocalandcorporateissuesinordertobecompetent,tofeedinformationupanddowntheorganisationalstructureandinfluencepolicy.Divisionsnowhaveacomprehensiveinfrastructurethatincludedfinancialandhumanresourcemanagementexpertise.
Theinquiryteamnotedthattheneworganisationstructuresappeartobewidelysupportedbymanagers.“ConsensusofopinionamongseniormanagersisthatthenewstructureisthebesttheyhaveexperiencedwithinRMH.Theyconsideritwellplannedandresourced,providinggoodaccesstotheCEOandlinemanagement.However,itwasalsonotedthatsomenursesarecriticalofthefailureofRMHmanagementtoincludethemindecisionmaking.Theyconsidermanagementtobeoverlymedicallyoriented,andthatnursingexpertiseisneithersoughtnorvalued”(page22).
Methodsofmanagementofclinicalwork
Operatingrulesandguidelineswereinadequateinthepast,andwereassociatedwithlowlevelsofcomplianceinsomerespects.Improvementshadbeenmadeoflate.However,theyappearedtobepoorlyunderstoodbelowmanagementlevel.RMHstilldidnothaveadocumentednursingphilosophy or nursing objectives.
Theinquiryteamarguedthatclinicalgovernancewasstillnotwidelyunderstoodandthenecessarystructuresandprocesseswerestillevolving.Beforeaneworganisationalstructurewasimplementedin2002,clinicaldivisionswereunderresourcedintermsofadministrativeandsupervisory capacity.
RMHhadarangeofqualityassuranceandimprovementprograms,buttheywerenoteffectivelyintegrated.Staffsaidduringinterviewsthattherehadbeenafailuretoinvestininfrastructure,including capital equipment and administrative support. The various clinical groups therefore had to relyontheirownresources,andthisledtoinconsistenciesincludingindatacollectionandstoragemethods.

�03
Thereweredifferencesinorganisationalstructures.Forexample,medicalstaffhadadivisionalreportingsystemforqualityactivitieswhereasnursingassignedqualitymanagementtotheNurseUnitManagerandclinicalnurses.OneconsequencewasthatmuchdependedontheknowledgeandinterestofeachNurseUnitManager.Someclinicalunitshadmovedtowardsamultidisciplinaryapproach,anditwasclaimedthatthisoftenmeantthenurseshadtocarrytheburdenduetoalackofinterestamongotherprofessions.
Theinquiryteamsuggestedthereshouldbe“…aformalsystemofrecognitionandrewardforindividualsandgroupswhoachievesignificantqualityimprovements.”Thiswouldprovidepositivestaffreinforcement,andavehicleforpublicisingqualityimprovementactivities.
Relationshipsbetweenprofessions
TheinquiryteamconcludedthatrelationshipsbetweenmedicalandnursingstaffatRMHweregenerallysatisfactory.However,somerespondentssuggestedtherewerecircumstancesinwhichrelationshipshaddeterioratedovertheyears,tothedetrimentofpatientcare.Forexample,theinquiryteamwasadvisedthatnursingstaffinsomewardsandunitswerereluctanttoaccompanydoctorsonwardandunitrounds–andtheinformantssuggestedthisrequiredimmediate attention. The reasons for reluctance are not given in the inquiry report.
Somerespondentswereconcernedabout“…whattheyperceivedasadividebetweenmedicalandnursingstaffandwantedtoimprovethesituation.”However,theywerenotabletomakeanyspecificsuggestionsaboutappropriatecorrectiveaction.TheinquiryteamconcludedthatfurtherinvestigationandevaluationbyRMHmanagerswasrequired.
Theinquiryteamrecognisedthattherewereproblemsofcommunicationofvariousotherkinds.Indeed,themajorityofrespondentsmentionedpoorcommunication“…asamajorsourceofpatient and staff dissatisfaction.”
Oneofthecorrectivemeasuresalreadytakeninvolveddefininglinesofcommunicationandprovidinginformationsessionsatwhichtheycouldbeclarified.Thechannelshavebeenlinkedto position descriptions.
However,theremaybealongwaytogo.Theinquiryteamnotedtherewerelargedifferencesofopinionabouttheadequacyofcorporatecommunicationatseniormanagement,middlemanagementandoperationalorclinicallevels.Nurseclinicianssaidtheyfeltpowerlessandfrustratedbyafailureonthepartofmanagementtolistentotheirconcerns,ideasandopinions.Onecommentmadeinaninterviewisquotedintheinquiryteam’sreport.
“Oneofthegreatdifficultiesiscommunication,particularlyforapersononnightduty–thingshardly ever reach you. There is a huge neglect in that respect. The current leaders do listen. Beforethat–no,absolutelynot.Nursingstaffdonotreceivefeedbackonissuestheyraisewithadministration.”However,somenursesacknowledgedthatstaffdonotalwaystakeadvantageofopportunitiesmadeavailabletothembymanagementandfailtoaccepttheirownresponsibilities for informing themselves of organisational issues.
Managementofmedications
The inquiry team noted that most adverse events relating to medication error do not occur as aresultofasinglemistakebyaparticularindividual,butbecauseofafaultinthehealthcaresystemthatdoesnotallowtheerrortoberecognised.Theerrorratesarehigherwherewardstocksupplysystemsareused.

�04 Patient Safety: a comparative analysis of eight Inquiries in six countries
Theteamfurthernotedthaterrorratescanbereducedbyguidelinesandprotocols,druginformationandadvisoryservices,computeriseddecisionsupportsystems,androutineevaluation.Specialmeasures are required for dangerous drugs.
TheInquirywasadvisedthattherehadbeenadeclineintherigourofmedicationcontrolatRMHinrecentyears.However,stepswerebeingtakentoimprovethesituation.Forexample,nursingpoliciesandproceduresrelatingtodrugadministrationandcontrolatRMHhadbeenunderreviewsince2001.Specificproblemswerenotedbytheinquiryteamtohavenowbeenaddressed:drugsawaitingreturntopharmacyweresometimesnotstoredinlockedfacilitiesbutleftinopenwardareas;keystothedangerousdrugcupboardandthedrugcupboardwerekepttogetherandwerenotalwaysappropriatelylocated;thecheckingfordrugsofaddictiondidnotalwaysoccurinaccordancewithstandards;andtherewereinadequatecontrolsoverdrugsloanedbetweenwards.
However,someproblemsremainedtobeadequatelyresolved.Staffinterviewedbytheinquiryteamarguedthatthereplacementofimprestdrugsbytechnicianshadreducedefficiency,specialistareassuchastheIntensiveCareUnitandEmergencyDepartmentthatrequirespeedyaccesstolifesavingdrugsstoredtheminunlockedfacilities,andsomenurseswereadministeringdrugsthatwereoutsidetheirscopeofpractice.Theinquiryteamarguedthatcontrolofsometypesofdangerous(Schedule4)drugscouldbeimproved.Auditingproceduresshouldbestrengthened,andthereshouldbeanexplicit‘zerotolerance’policytowardsthetheftormisuseofdrugs.
Staffwereworkingwithadualsystemofoldandnewpolicies,andthiswascausingconfusionandneededtobeaddressed.Beforetheallegationsofmisconduct,therehadbeennohospitalwidemonitoringofcompliancewithmedicationpoliciesandprocedures,includingcompliancewithlegislativerequirements.TheinquiryteamsuggestedthattheresponsibilityforimprovingthesituationwouldbemostappropriatelyassignedtotheDirectorofPharmacy.
Managementofincidents
RMHhadaClinicalRiskManagementCommittee,butitwasdeficientinmanyrespects–includingthe absence of nurse clinicians. RMH had not established systems for collecting data on sentinel eventsandforundertakinglimitedadverseoccurrencescreening,althoughtheDepartmentofHuman Services requires public hospitals to do so.
AnewprocessforthemanagementofadverseeventswasintroducedinMarch2002.However,staffsuggestedmanyweaknessesduringinterviews.Forexample,theyresentedthewordingonthereportingformthatimpliedthecausewasafailuretoprovideadequatenursingcare,whereastheincident may have been stimulated by other processes.
Theyalsotoldtheinquiryteamthatmanyincidents,includingseriousones,werenotbeingreported.TherewasalackofconsistencythroughoutRMHwithregardtodeterminingtherangeofincidentstobereported.Staffcomplainedthattheyreceivedlittleornofeedbackaboutincidentreports,andthishashadadetrimentaleffectonstaffrelationshipsandmorale.Finally,somestaffconsideredthat,inthepast,theRMHhadacultureofblamethatdiscouragedreporting.Itwasuncleartotheinquiryteamwhetherthishadbeenovercome.
Managementofcomplaintsfromstaffandpatients
Intherecentpast,manystaffhadtakentheviewthattherewaslittlepointinmakingcomplaints.Theircomplaintswereseldomappreciated,andtheyrarelyresultedinactionbytheHospitalmanagement.

�05
Patientcomplaintswerehandledmoreeffectively.TheRMHhadafulltimecomplaintsliaisonofficer,whoprovidedstafftraininginadditiontodirectsupportforpatients,theirfamiliesandcarers.Theinquiryteamargued,however,thatthecomplaintsliaisonofficerdidnothaveadequate administrative support.
Nursingstaffing
Likeotherhospitals,theRMHhadbeenadverselyaffectedbythewidespreadshortageofnursesandhadbeenobligedtoemployahighnumberofcasualstaff.However,fundinghadbeen improved of late to increase the number of permanent nursing staff and this had begun to have a positive impact.
The inquiry team noted that the number of nurse educators had been reduced dramatically between1995and2000.Overatwoyearperiodthesituationhadimprovedasaconsequenceof increasing the number of nurse educators from three to 20. Priority had been given to supportingnewlygraduatednurses,andtheprofessionalneedsofothernursingstaffwerenotyet being met. Nursing staff indicated that RMH did not have formal mechanisms for nurses to raiseethicalissues,receivefeedback,orgainimmediateadviceandsupportwhendealingwithethicalproblemsencounteredintheirwork.
Supportsystemsfornursingstaff
The inquiry team argued that resource constraints during the late �990s had had a serious adverse impact on nursing support services at the RMH. A combination of factors including highworkloads,exposuretostressfulsituations,poorrosterandshiftworkarrangements,andareductioninstaffsupportpositionsresultedinlowstaffmoraleandadropinstandardsofcare.Morerecently,budgetshadbeenimprovedtoredresstheseproblemsbutfullrecoverywouldtaketime.
Theinquiryteamnotedthatnurseswereassusceptibleasanyotherprofessionalgrouptoemotionalandphysicalhazardsintheworkplace.Nurseswithimpairments(forsuchreasonsasthroughillnessorsubstanceabuse)requiredassistance,butthishadnotbeenforthcominguntilveryrecentlyatRMH.ItwassuggestedthatahealthprogramfornursesshouldbeestablishedthatcouldbemodelledonthatforVictoriandoctors.
TheRMHhadrecognisedtheneedtodevelopprocessesthatvalue,supportanddeveloptheskillsofnurses.Theinquiryteamarguedthattherewasaneedtomanagecomplicatedinteractionsbetweendiverseprofessionalgroups,andbetweenthemandhighlyvulnerable,oftentraumatised,patientsandfamilies.“Situationsofconflictcanoccur”and“…itistheresponsibilityoftheorganisationtohaveprocessesinplacetoreducetheserisksandtoresolveconflictasquicklyaspossible.RMHhadanaggressionmanagementcommitteebutthishasnotbeen operational for some time. Clear and consistent policies need to be developed to ensure aggression,whateveritssource,isreducedandaddressed.”
Theorientationofnewstaff
RMHhadageneralorientationprogramthatwasintendedtoserveallkindsofnewstaff,andtheprogramwasperiodicallyreviewedbytheHumanResourcesUnit.ThegeneralprogramwasaugmentedbyprogramsthatwererelevantonlytospecificprofessionsorunitswithintheHospital.Thesemorespecificprogramsweredesignedandmanagedbytheprofessionsorunitsconcerned.Theinquiryteamconcludedthattheydifferineffectiveness.Thisistobeexpected,giventhatsomewereformalandothersinformal,andsomewereevaluatedwhileothersarenot.

�06 Patient Safety: a comparative analysis of eight Inquiries in six countries
Clinicaldepartmentsallocatedtimetoallowforstafforientation.Mostofthemhadamentorshipschemethatwasinitiatedduringorshortlyaftertheorientationperiod.Themostsignificantcomponentsoforientation(thoserelatingtopatientcare)werethereforelesssubjecttoevaluationand continuous improvement. The same may be said of mentoring.
Theinquiryteamnotedtherewasnoorientationprogramthatwasspecifictotheneedsofnurseunitmanagers.Thiswasconsideredtobeamissedopportunitybecause“…awell-designedandeffectively implemented formal orientation program for nurse unit managers that incorporates managementexpectationsofclinicalgovernance,communicationandstaffsupport,wouldprovideopportunities for enhanced leadership and be a catalyst for cultural change.” The inquiry team made nomentionoftheriskthat,iforientationandmentoringwerelargelyspecifictoparticularfunctionsorprofessions,thismightservetoreinforceprofessionalsubcultures.
Standardsofclinicaldocumentation
Thestandardshaddeclinedinsomerespectsinrecentyears,andRMHhadrecentlygiventhismatterincreasedattention.However,theinquiryteamconcludedthatmuchremainedtobedone.Forexample,anewproceduremanualwasproducedin2001thatmainlyaddresseddocumentationinmedicalrecords.However,therewerenostandardsregardingmanyaspectsofmedicalrecordsmanagement.
AtthetimeoftheInquiry,theHealthInformationManagerreportedhewasunawareofanyrecentcontentauditsofmedicalrecords,butexpressedacommitmenttoconductingsuchauditsinthefuture. The inquiry team therefore conducted a limited medical record audit that revealed poor standardsofdocumentation,andrecommendedtheproblemsbeaddressedwithsomeurgency.
Theauditinvolvedasampleof60medicalrecordsofpatientsdischargedoveratwoweekperiodinFebruary2002.Thefocuswasthequalityofnursingdocumentation,whichwasevaluatedagainststandardsinthemedicalrecordsproceduremanualnotedabove.Itwasnoted,however,thatmanyaspectsofdocumentationwerenotcoveredbythemanualintermsofprescribedstandards.
Therewaslittleuniformityofcontent,andadditionalconfusionhadbeencausedbythepartialuseofclinicalpathways.Thepathwayformswereintendedtodocumenttheentireepisodeofcare,butthiswasnotthecaseinpractice.Rather,therewasamixofpathwayandnonpathwaydocumentation.
Thereweremanyspecificproblems.Forexample,thewardsinwhichpatientswerelocatedwerenotidentifiedintheprogressnotes,signatureswereoftenillegible,alertswerenotappropriatelydocumentedforthreepatientswhohadareportedallergytoamedication,irrelevantandredundantinformationwasfrequentlyincluded,therewasahighlevelofduplicationofinformation,andsomeoftheentrieswerenotdated.
RMHnursemanagerswerealmostuniversallycriticalofthequalityofdocumentationofpatientcare,whilenurseclinicianswerelessinclinedtocomment.Nursemanagerswereconsciousoftheformallackofmonitoringandevaluationofdocumentationstandards.Severalinterestingcommentsweremadeduringinterviews.Forexample,itwassaidthatpaperworkvariesfromwardtoward.Ifyouarepartofthenursingstaffbankandfloatingasanagencynurse,thiswasverydifficult.Staffwerenotfamiliarwiththepatients.Documentationwasdoneeverytimepeopleseeapatient,whetherornotwetheygivethemawashortheyhaveafullbedchange.
Finally,manyoftheauditedrecordsdemonstratedapoorunderstandingoftheneedtodocumenttheimplementationandevaluationofcare.Forexample,therewasalackofdocumentationoftheoutcomesofcare.Inalmostalloftheauditedrecords,therewasafailuretoindicatefollowup assessment. Serious omissions included failure to document the outcomes of medications

�07
administered for pain. One medical record documented �� doses of a narcotic administered forpainwithoutwrittenevaluationofeffect.Amongtherecordswheretherewasfollowupdocumentation,itwasoftensubstandardintermsofitsspecificity.
Careplanningandevaluation
Manyweaknesseswerereportedbytheinquiryteam.First,therewasnohospitalwidestandardfornursingassessment.Thedocumentationauditshowedthatassessmentwasfrequentlyinadequate,andoftenrelatedonlytopresentingsymptoms.
Assessmentprocesseswerebetterinspecialistareas.Forexample,documentedassessmentofelectivesurgicalpatientswasofahigherstandardbecausetheyundergopreadmissionscreeningthatprovidesdatafromwhichcareisplanned.Dischargeplanningwasevidentonmostrecords,andtheDischargeRiskAssessmentformwasusuallycompleted.Medicalassessmentwasusuallyclearandcomprehensive,althoughnotalwaysdated.
Second,avarietyofmethodsandtoolswereusedtoplananddocumentpatientcare.Clinicalpathwayswereinuse,buttherewerenotableweaknesses.Theinquiryteamnotedtherewaslittleconsistencyofdesignandnoapparentorganisationwiderules,manypathwayswerenotmultidisciplinary,poorformdesignmeantmanyweretimeconsumingtouse,andtherewaslittleevidence of structured approaches to the recording and analysis of variances.
7.4 RecommendationsoftheInquiry
Theinquiryteammade73recommendations,mostofwhichcanbededucedfromthediagnosticinformationprovidedabove.Wewillgroupthembelowandgiveemphasistothoserecommendationsthatseemmostimportantinthecontextofourreviewofinquiries.
PARTICIPATION AND OPENNESS
RMH should continue to cultivate trust in management by maintaining consistent and transparentmanagementpractices,communicatingtheRMHvision,andencouragingparticipationfromallstaffindecisionmaking.Leadershipdecisionsshouldbedocumented,communicated and evaluated.
RESPECTANDINVOLVEMENTOFNURSES
RMHshoulddemonstratethatitvaluestheknowledgeandexpertiseofnursecliniciansbyinvolvingrepresentativeclinicalnursesonRMHcommittees,includingstrategicplanningandpolicymakingcommittees.ThisshouldincludeinvolvementofclinicalnurserepresentativesontheClinicalRiskManagementCommittee.
Nursing leaders should engage all nurses in the development of a nursing philosophy that incorporatestheartandscienceofnursingaspractisedatRMH,andcommunicateittoexistingandnewnursingstaff.Formalmechanismsshouldbeestablishedwherebynursesmayraiseethicalissues,receivefeedback,andgainimmediateadviceandsupportwhendealingwithethicalproblemsencounteredduringthecourseoftheirwork.
COMPLIANCEWITHRULESANDGUIDELINES
RMHshouldensurethatallstandards,policiesandproceduresaredevelopedaccordingtobestpracticeapproaches.Theyshouldbeeasilyaccessibleforconsultationbystaff,trainingshouldbeprovidedtoensurestaffunderstandthem,andcomplianceshouldbemonitored.

�08 Patient Safety: a comparative analysis of eight Inquiries in six countries
CONTINUOUSQUALITYIMPROVEMENT
RMHshouldfinaliseaqualitymanagementplanthatintegrateswithMelbourneHealth’sstrategicdirections and meets the quality requirements of external accrediting bodies and the Department of HumanServices.TheplanshouldincludeaclinicalgovernancepolicyandaframeworkforreportingthatsupportstheBoardandseniormanagementinfulfillingtheirresponsibilitiestomonitorandaddress issues relating to safety and quality of care.
An individual should be assigned to coordinate all aspects of quality and accreditation. Resources shouldbeallocatedtoeducateandsupportstafftofulfiltheirresponsibilitytomonitor,evaluateandcontinually improve the services they provide.
COMMUNICATIONACROSSANDWITHINPROFESSIONS
RMHshouldfurtherinvestigaterelationshipsbetweenmedicalandnursingstaffandimplementstrategies to improve their communication and interaction related to patient care. Managers should continuetomonitornursingrelationshipstoensurenurses,andparticularlyjuniornurses,feelconfidentoftherespectoftheirpeers.
Sharedaccountabilitiesshouldbedefinedforcommunicationandaprocessestablishedforeducating staff and monitoring the effectiveness of communication across the organisation. The Hospitalshoulddevelopstrategiesforlisteningactivelytostaffissues,andshouldprovideimprovedopportunitiesforstafffeedback.Thereshouldbeareviewoforganisationalcultureandsatisfactionlevelsofnonmanagementstaff,andstrategiesdevelopedtoaddressadverseculturalandmoraleissues.
IMPROVEDMANAGEMENTOFMEDICATIONS
RMHshouldreviewthedesignofitsindividualpatientmedicationstoragesystemtoensurethatrisksofmedicationerrorsareminimisedandaccesstoindividualpatientmedicationstoragecontainersisappropriatelyrestricted,documentedandaudited.
RMHshouldreviewproceduresgoverning‘loaning’ofdrugsbetweenwardsandobtainingnonimprestitemsafterhours,medicationstoragefacilitieswithintheIntensiveCareUnitandtheEmergencyDepartment,ensuringmedicationsarestoredappropriatelyandsecurelytopreventunauthorisedaccess,auditingofdrugstockstoensurecompliancewithdrugstorage.TheDirectorofPharmacyshouldbegiventheresponsibilityformonitoringandaddressingcompliancewithlegislation.
TheRMHMedicationRiskCommitteeshoulddevelopcomprehensivefeedbackmechanismstoenablestafftolearnfromerrors,andshouldimplementproactivepreventativestrategiesthatlinktoquality programs. The potential should be explored for the introduction of a standardised medication chartforallVictorianhospitalstodecreasetheincidenceofmedicationerrors.
RISKMANAGEMENTANDPATIENTSAFETY
TheRMHshoulddevelopahospitalwideprogramformeetingDepartmentofHumanServicesrequirements for reporting sentinel events and limited adverse occurrence screening. The Hospital’s policyandreportingmethodsshouldberevisedtoensurereportinglinesareunambiguous,timelinesforalllevelsofactionareclearlystated,thereareclearandeffectivefeedbackloops,keyperformanceindicatorsarepracticalandrelevant,andpolicychangesrelatedtoadverseeventsarecaptured appropriately and implemented through the quality improvement program.

�09
TheRMHshouldensurethereareappropriateeducationalprogramsonclinicalriskmanagementforallstaff.Educationonclinicalriskmanagementshouldbeincludedinorientationprogramsforallnewstaff.
COMPLAINTS PROCESSES
Thereshouldbeimprovedmethodsofmanagementofstaffcomplaintsandstafffeedback,toensureallcomplaintsareregisteredandactioned,andfeedbackisprovided.Themethodsshouldincludeprovisionforfurtherreviewofseriouscomplaintswherethestaffmemberisdissatisfiedwiththeoutcomeoftheinitialmanagementofthecomplaint.TheHospitalshouldmakesureallstaffarefamiliarwiththeprovisionsoftheWhistleblower Protection Act 2001(Vic)and processes are in place for its implementation.
CLINICALDOCUMENTATION
The RMH should produce improved standards for the handling of medical records. Nursing leaders should contribute standards for nursing documentation and provide relevant education to all clinical staff. There should be improved standards for documentation of care planning and outcome evaluation.
7.5 Discussion
TheMelbourneHospitalInquirywasnotableforthesupportitreceivedfromkeystakeholders,including the management and staff of the hospital involved (Health Services Commissioner: 2004).AfollowupanalysisoftheInquiryproducedbytheCommissioner’sofficein2004gavesomeinterestinginsightsastowhythismightbeso.
InOctoberof2004,theHealthServicesCommissioner’sOfficepublishedananalysisintotheRoyalMelbourneHospitalInquiry.Theanalysisdocumented“…thebackgroundandmanagementofasuccessful,speedyandcostefficientinvestigationandprovidesa“roadmap”whichmaybeusefulinassistinganyrelevantfutureinquiriesintohospital-basedincidents”(HealthServicesCommissioner,2004:3).
Thereportidentifiedtheneedforcleartermsofreferenceforinquiries,drawnupinconsultationbetweenCommissioner’sandMinister’sofficessoastoavoid(asintheCamdenandCampbelltownHCCCInquiry)confusionoverthefocusofinquiries.Inquiryteamsaretobeselectedcarefully,inordertoensureacombinationofappropriateskills,strongcommitmenttotheinquiryprocess,aclearunderstandingoftheexpectationsandworkloadofaninquiry,andinordertopromoteopenandhonestcommunicationbetweenteammembers.
Communicationissuesmadeupthebulkofthesuggestionsforaneffectiveinquiryprocess.Informationtostakeholdersshouldtobehandledinatimelymannersoastoreduceanxietyandtoensurethatinformationisreceivedbystakeholdersbeforeitisreleasedtothemedia.Inthesamevein,hospitalstaffaretobeinformedofthespecificpurpose,inquiryandreportingmethodsofaninquiry,includingtheprinciplethatqualityimprovement,andnotblame,istheobjective of most inquiries. Team members are to be made freely available to staff. Dialogue betweeninquiriesandotherparallelinvestigations,suchasthoseheldbyCoroners,MedicalCouncils and Registration Boards amongst others are considered highly important.
Theformofevidencetobeincluded(suchaswrittensubmissions)ininquiriesistobedetermined and publicised before the commencement of the inquiry process. At the end of the process,copiesofthedraftoftheinquiryreportsaretobesuppliedtoanyonesubjecttoadverse

��0 Patient Safety: a comparative analysis of eight Inquiries in six countries
comments,priortotheirrelease.Finally,interestedparitiesattheperipheryoftheInquiryaretobeencouragedtobeinvolvedininquiries,onthebasisthattheymightprovideuseful,butunexpectedinformation(HealthServicesCommissioner,2004).
7.6 Footnote
7.6.1 Theoutcomeofthelegalinvestigation
TheCoronerinvestigated80deathsfromtheNeurologyWardattheRMH,mainlyasaconsequenceoftheclaimbyacolleagueofthetwoaccusednursesthattheyhadplannedtokillonepatientusinginsulinandhadactuallyacceleratedthedeathofanotherpatient.ThedeathswerethesubjectofaninitialInquirybyhospitalauthoritieswhentheclaimsweremadeintwoanonymousnotessenttomanagement in October 200� (Butcher 2003).
ThePoliceandtheCoronerwerenotifiedinMarch2002,afteraprivateinvestigatorfortheHospitalsubmitted reports on the death of one patient and on allegations of misconduct and unprofessional behaviour.Duringtheirinvestigationsintothosetwodeaths,Policewereinformedthatathirdpatienthad died in suspicious circumstances involving the administration of morphine. These three deaths werethefocusoftheinquest.
The investigations had been rendered more complicated because one of the accused nurses had admittedshewasinvolvedinthedeathofoneofthepatients.Shehadbeensufferingatthetimefroma“…drug-abuseproblemcombinedwithadegreeofmentalinstability”.
TheCoroner,inhisinquestonthethreedeaths,concludedthateachappearedtobefromnaturalcauses.However,heinclinedtoaccepttheevidenceuncoveredduringthePoliceinvestigationthatindicatedtherewereseriousdeficienciesintherecordingnurseactivity,lackofsupervisionandleadership,andlittleornoaccountabilityofprescriptiondrugsontheward.
7.7 Referencesandselectedbibliography
Butcher,S.(2003).TwoNursesClearedoverDeaths.Melbourne Age,31May.
Health Services Commissioner (2002). Royal Melbourne Hospital Inquiry Report. Report by the Health Services Commissioner to the Minister for Health, the Hon. John Thwaites MP under Section 9(1)(m) of the Health Services (Conciliation and Review) Act 1987. Available at: http://www.health.vic.gov.au/hsc/rmh_report0802.pdfAccessedon3March,2006.
Health Services Commissioner (2004). Analysis of the Inquiry Held by the Health Services Commissioner 2002, into an Incident at the Royal Melbourne Hospital, Victoria. Available at: http://www.health.vic.gov.au/hsc/analysisrmh.pdfAccessedon3March,2006.
8 SouthlandDHBMentalHealthServices,NewZealand
8.1 Context
MrMarkBurtonbecameaclientoftheMentalHealthServiceofSouthlandDistrictHealthBoard(SouthlandDHB)inJuly1998.TheMentalHealthServiceoperatedatseveralsitesandincludedcommunity-andhospital-basedfacilities.MrBurtonreceivedcarefromtheQueenstownCommunity
���
MentalHealthTeamandhadtwicebeenhospitalisedasavoluntarypatientinWard12ofSouthlandHospital,Invercargill.
Thesecondinpatientepisodelastedfor50days.HewasdischargedfromWard12on30March2001.Onedaylater,hekilledhismother.
Inresponsetopubliclyexpressedconcerns,aclinicalauditwasinitiatedbySouthlandDHB.TheauditwasconductedbyapsychiatristwithnoconnectionstoSouthland–DrBridgetTaumoepeaufromWellington.Herreport,releasedinSeptember2001,expressedmanyconcerns about the quality of care that had been provided. The Southland DHB’s Director of MentalHealththencommentedpubliclythatthereporthighlightedproblemswithSouthlandDHB’s Mental Health Services that needed to be addressed.
InOctober2001,theHealthandDisabilityCommissioner(theCommissioner)initiatedanindependentinquirythatreporteditsfindingsinOctober2002.IttookaccountoftheCoroner’s inquest into Mrs Burton’s death that reported in December 200�. The report by the Commissioner (Health and Disability Commissioner 2002) is the main source of the summary providedbelow.
The Commissioner examined clinical practices in great detail as they related to the care of MrBurton,andconcludedtherehadbeenmanydeficiencies.Althougheachdeficitsingularlymaynothavebeenresponsiblefortheoutcome,intotaltheyresultedinpoorcare.Therewereinadequatemonitoringandcontrolmechanismstoensurethatstaffpractisedsafely,thatincidentandriskmanagementstrategieswereinplace,andthatpoliciesandprocedureswerefollowed.CommunicationwithMrBurton’sfamilywereinadequate,dischargeplanningwasineffective,andtherewasanotablelackofcoordinationbetweentheinpatientandthecommunitycareteams.The“…overallpictureisoneofsloppycarethatwaslaxandlaissez-faire.”
Inter alia,theCommissionerrecommendedthatthereshouldbecompetencereviewsofmanyclinicians,internalauditingandstafftrainingprocessesshouldbeenhanced,carepathwaysimproved,effortsmadetodevelopacultureofcriticalappraisal,aqualityimprovementstrategydevelopedandmonitored,andimprovementsmadetocommunicationprocessesandsystems.HereferredhisfindingstotheDirectorofProceedingsforthepurposeofdecidingwhetherfurtheractionshouldbetaken.
8.2 TheInquiries
8.2.1 DrTaumoepeau’sclinicalaudit
Dr Taumoepeau’s report outlined the context and summarised the care that Mr Burton had received.Shedrewconclusionsonitsappropriateness.
VirtuallyallofherfindingswereconfirmedduringthemoredetailedinvestigationconductedbytheHealthandDisabilityCommissioner,andthereisconsequentlynoneedtodescribethemhere.However,shehadfewerconstraintsonthescopeofherinvestigationthantheCommissioner.Shethereforechosetoaddressthegeneralmethodsofworkofthementalhealth services team rather than merely those aspects of Mr Burton’s care. This led her to presenting recommendations about improvement of those processes in future. They differ onlyinminorwaystotherecommendationsoftheCommissioner,buttheyareworthnoting.Wewillsummarisetheminalatersectionofthepaper.However,wewillfirstsummarisetheCommissioner’sreportbecauseitpresentsthebackgroundnecessarytointerpretationofherconclusions.

��2 Patient Safety: a comparative analysis of eight Inquiries in six countries
8.2.2 TermsofReferenceoftheCommissioner’sInquiry
TheTermsofReferencewereinfluencedbytwofactors:thehighdegreeofpublicconcern,andthecontentsofthelegislationunderwhichtheCommissionerwaspermittedtoact.Thefocuswasthepatients’rightsasspecifiedbythelegislation.TheCommissionerdeterminedtoinvestigatewhetherthoserightshadbeenbreachedwithregardtocommunicationwithpatientsandtheirfamilies,dischargeplanninganddischargeprocesses,andcoordinationbetweenclinicalteams.ThesewerethespecificindicationsintheActwithregardtoqualityofcare.
8.2.3 Theprocessofinvestigation
TheCommissionerwasrequiredundertheActtonotifyagenciesandindividualhealthcareprofessionalsthattheywereunderinvestigation.SelectionoftheagenciesandindividualswasinfluencedbyDrTaumoepeau’sreport,andbyaformallettertotheCommissionerfromMrBurton’sfather.Amongotherissues,MrBurton’sfathercomplainedaboutthestandardofcareprovidedtohissonbythedoctorresponsibleforhiscare,andthelackofsupervisionofthatdoctorbySouthlandDHB’sClinicalDirectorofMentalHealthServices.Intotal,thoseinvestigatedwereeitherdirectly involved in Mr Burton’s clinical care or carried management responsibility.
MrBurton’sfatheralsocomplainedofmattersthathadcausedhimandhisfamilyfurtherharm,butwhichtheCommissionerjudgedwereoutsidehisjurisdiction.TheyincludedcommentsmadebySouthlandDHBstaff(inparticular,theGeneralManagerandtheClinicalDirector)followingtherelease of Dr Taumoepeau’s report.
TheCommissionerappointedaninvestigationteamoffiveindependentadvisorsandaprojectmanager.TheybeganbyreviewingthereportbyDrTaumoepeau,evidencefromtheinquest,andadditional materials made available by Southland DHB including Mr Burton’s clinical records.
Theinvestigationteamvisitedthelocationswherecarehadbeenprovided,andinterviewedallstaffunderinvestigation.TheyalsointerviewedotherhealthcareprofessionalsandmembersofMrBurton’sfamily.Interviewswereconductedfacetofaceorbytelephone,taperecorded,transcribedandreturnedtotheintervieweesforcheckingandsigning.
TheCommissionerformedaprovisionalviewonthequalityofcareprovided.Thiswasprovidedtoallpersonswhoseperformancewasunderinvestigation.TheirresponsesweretakenintoaccountinformingthefinalopinioncontainedintheInquiry’sofficialreport.
Particularweightwasgiventotheclinicalnotesthatweremadewhilecarewasbeingprovided.TheCommissionerconsideredthiswasimportantbecause,duringthecourseoftheseveralformalandinformalinquiries“…theinpatientstaffmostdirectlyinvolvedclearlydiscussedtheperiodofMrBurton’shospitalisationand,notsurprisingly,developedacommonviewofwhathadoccurredwhileMrBurtonwasinhospital.”
The health care professionals under investigation made several allegations of unfairness over theinquiryprocess.Onewasthattheyhadbeencriticisedwithregardtothelanguagetheyhadused,andthisreflectedanundueemphasison‘politicalcorrectness’.TheCommissionernotedthat,duringthecourseofinvestigation,hisadvisorshadindeedreportedtheuseoflanguagetheyconsideredpaternalisticandstigmatising.However,hesupportedhisadvisorsinthisregard.“Thisisanaspectofpracticethatrequireslittletimetocorrect,butwhichcanhaveanimportanteffectontheattitudesandvaluesofstaff.”Everypatienthastherighttobetreatedwithrespectand“…useof appropriate language is an essential element of respect and is not merely a matter of semantics or political correctness.”

��3
AnothercriticismoftheInquirywasthatitwasaffectedby‘hindsightbias’:theinquiryteamknewthattherehadbeenanadverseoutcome(thehomicide)andwasawareofDrTaumoepeau’sreport;andthatthisaffectedtheirjudgement.TheCommissionerrecognisedtherisksbutarguedhehadtakenappropriatestepstominimisethem.Inter alia,heattemptedtoensurehisassessmentofthequalityofcarewasnotinfluencedbythedeathofMrBurton’smother.
Someintervieweesarguedthattheyfoundthequestionsaskedbytheinvestigationteamconfusing.TheCommissionerrejectedthisargument.Withoneexception,allstaffinterviewedwereaccompaniedbyalawyer(andthepersonwithoutalawyerwasaccompaniedbyasupportperson).Duringthecourseoftheinterviewsstaffwereableto,anddidinfactaskforclarificationwheretheydidnotunderstandaquestion.Theirlawyerswereavailabletoassist,object,andseekclarificationifnecessary.Therewasanopportunityduringallinterviewsforstafftospeakprivatelywiththeirlawyer.
8.3 ConclusionsoftheInquiry
TheinquiryreportcontainsadetaileddescriptionofthecareprovidedtoMrBurtonwhilehewasunderthecareofSouthlandDHB’sMentalHealthServicebetween10February2001and30March2001.Alltheavailableclinicalrecordsweresummarisedandaugmentedwithcommentsfromthehealthcarestaffconcerned,andfromotherpersonsincludingmembersofMrBurton’sfamilywhererelevant.
Onthebasisofanalysisofdocumentationandtheevidenceprovidedthroughinterviews,theCommissioner concluded that Mr Burton did not receive services of an appropriate standard. TherewereactsandomissionsbyindividualsandbySouthlandDHBthatbreachedMrBurton’srights under the legislation.
Itwasconcludedthattherewasnosingleactorsingleindividualwhomightbeheldtocarrytheprimary responsibility for the poor care. The Commissioner’s advisors made reference to the analogy by Reason (2000) that clinical disasters may be considered to be the consequence of a chance alignment of minor errors.
Thisis“…theSwisscheesemodelofsystemaccidentsinwhichsuccessiveholesinthelayersofdefences,barriersandsafeguardslineup.”Therewere“…numerousholesinthischeese,somany and some of such proportion that they lined up to create large gaps through the substance oftheservice.Althougheachdeficitsingularlymaynothavebeenresponsiblefortheoutcome,the substance or quality of the service appears in this case to have been so compromised that theriskofoccurrenceofadverseeventswasnotmanagedatalleffectively.”
Intotal,therewereinadequatemonitoringandcontrolmechanismstoensurethatstaffpractisedsafely,thatincidentandriskmanagementstrategieswereinplace,andthatpoliciesandprocedureswerefollowed.CarewaspoorwithregardtoallofthespecificTermsofReference.ContactandcoordinationwithMrBurton’sfamilywasinfrequentandlargelyad hoc.Whencontacttookplace,thesubstanceofthecommunicationwasfrequentlyinappropriateinbothstyleandcontent.TheCommissionernotedthat“…muchofthetimethefamilywasleftinthedarkaboutwhatwasgoingon.”
Dischargeplanningwascareless,imprecise,lackingdetail,andpoorlycoordinated.Theinquiryreportsaid“…itisnothardtoseewhyMrTrevorBurtonconsidersthathissonwasessentiallykickedoutintoaflattolookafterhimself”.

��4 Patient Safety: a comparative analysis of eight Inquiries in six countries
Thedischargeprocessitselfwasofdoubtfulquality.TheMentalHealthServicefailedtoformaclearpictureofthepatient’sconditionatdischarge,andtoconsiderwithcarethepossibleimplicationsforpostdischargewellbeing.TheprocesstookinadequateaccountoftheavailableinformationaboutMrBurton’sdisturbedsleeppatterns,alcoholabuse,andpsychoticbehaviours.
Finally,therewasanotablelackofcoordinationbetweentheQueenstownCommunityMentalHealthTeam(whichhadconsiderablepreviouscontactwithMrBurton)andtheInvercargillCommunityMentalHealthTeam.TheirinvolvementwasconsideredessentialtoensuringMrBurton’s successful discharge into the community.
AccordingtotheCommissioner,theweaknessesinMrBurton’scarewereaninevitableconsequenceoftheoverallstyleofworkofSouthlandDHB’sMentalHealthService.Itwascharacterised by attitudes of complacency and laissez-faire.ThecareprocessesweresuchthatthefamilyofMrBurtonhad“…everyrighttofeelthatthehealthsystemfailedthem.”TheprocessesthatweredeficientweredescribedindetailintheCommissioner’sreport.Thebehaviourofeachofthemainpartieswasdiscussedinturn,andissummarisedbelow.
Theattendingdoctor
TheattendingdoctorwasaMedicalOfficerSpecialScale(orsimplyMOhere).Thepositionwasintendedtobeoccupiedbyapsychiatrist,butthiswasnotthecaseduetoclaimedrecruitmentdifficulties.Whenrecruited,hewasgiventobelievehewouldworkundersupervisionbecauseofhislimitedknowledgeofpsychiatry,andthatarrangementswouldbemadetoensureitwasavailablewhenneeded.TheCommissionerconcludedthearrangementswereinadequate.TheMOreportedintheinterviewthathecouldobtainareasonabledegreeofaccesstotheClinicalDirector.Unfortunately,theMOdidnotconsiderthatheneededtodiscussissuesrelatingtoMrBurton’scare.The Commissioner concluded that the MO underestimated his need for supervision.
TheMOarguedthattherewastheopportunityforadequatediscussionofindividualpatientswithbothnursingstaffandconsultantpsychiatristsduringtheweeklyreviewrounds.Hearguedthatthisopportunitywasinfacttaken,andthathewasgivennoindicationthatthewayhewasmanagingMrBurton might be inappropriate.
However,theinquiryteamconcludedthattherecordsavailabledidnotsupporttheMO’sassertion,anddidnotshowthattheadviceofotherscontributedinanysignificantwaytoMrBurton’smanagement.AtoneofthefiveweeklymeetingswhileMrBurtonwasapatient,noconsultantpsychiatristwaspresent.Theinquiryteam’sadvisorsconcludedthat“…asaforumforsupervisoryinputonaregularbasisfromamoreexperiencedmemberofthemedicalstaff,themeetingswouldhave been of limited value.”
TheMO’sworkwascriticisedinalmosteveryrespect.Hedidnotrecordhisadmissionassessmentonastandardisedassessmentform,andwhatherecordedwasincomplete.Forexample,therewasnodetailaboutthenatureofthreateningbehaviourorprecipitatingfactors,themainconcernsofthefamily,orsocialcircumstances.Therewasnomedicalhistory,andnorecordofquantityorfrequencyofuseofalcoholandcannabis.Someofthedeficiencieswereresolvedlater,butmanyremainedunresolvedatthetimeMrBurtonwasdischarged.
TheMOdidnotdevelopanddocumentanadequatetreatmentplan.Forexample,hedidnotidentifytheneedfortheclinicalteamtounderstandthenatureofMrBurton’spsychoticexperiences,orensureeffectivetreatmentandmanagementoftherisksofpsychoticphenomena.Hedidnotgivesystematicandadequateattentiontomattersheidentifiedaspriorities,suchasMrBurton’sdrugandalcoholuse.Therewerenosystematicattemptstofindaresidentialfacilitythatwouldaddress

��5
substance abuse. He did not give adequate attention to Mr Burton’s mental state and did not adequatelyassesswhethertherewasanimprovementinMrBurton’spsychoticsymptoms.
HefailedtomonitorMrBurton’smedicationafterthedoseofolanzapinewasincreasedonadmission.Therewasnoevidenceofregularsystematicreviewoftheeffectivenessofthetreatmentorthepatient’stoleranceofit.Hedidnotsufficientlyspecifythecircumstancesinwhichthe‘asrequired’medication(whichheprescribedonadmission)wastobeused.
TheMOfailedtomanageclinicalrisk.Forexample,hedidnotcompletean‘Assessmentofrisk’form.HedidnotreviewMrBurton’sassessedlevelofriskfollowingincidents–suchaswhenthepatientreturnedtothewardapparentlyintoxicatedandbehavinginathreateningmanner.HedidnotmakeaformalassessmentofrisksbeforeitwasdecidedthatMrBurtonwouldhaveaweekoftrialleave,orbeforedischarge.
SimilarconcernswereexpressedbytheCommissionerwithregardtoleaveplanninganddischargeplanning.Withrespecttothelatter,theMOprescribedathreemonthsupplyofmedicationbuttherewasnorecordofhishavingdiscussedwiththepatienttheneedtoadheretotheprescribeddose,orofstrategiestomonitoradherenceortorestrictsupply.TherewasnoevidenceofacomprehensivereviewofMrBurton’smentalstateonMarch302001(whentheplantodischargewasconfirmed),amentalstateexamination,orareviewofriskfactors.NorwasthereanyrecordofdiscussionofMrBurton’ssubstantialuseofalcoholintheweekoftrialleave,ortheimplicationsforhismentalstate.
Further,theMOdischargedMrBurtonwithoutthecommunitykeyworkerattendingthedischargemeeting(aftertheMOchangedthemeetingtimewithoutadvisingher).HefailedtoensuretherewereadequatearrangementstomonitorMrBurtoninthedaysfollowinghisdischarge.
Adischargemeetingwasplannedfor11amon30MarchatwhichMrBurton,theMO,andrelevantnursingandsocialworkstaffweretobepresent.MrBurtonarrivedearlyattheinpatientunitanddidnotwanttostayuntilthearrangedtime,sotheMOagreedtobringthemeetingforwardwithoutadvisingthekeyworkerorensuringthatshecouldattend.Themeetingwasheldwithouther,andthepatientwasdischargedwithoutarrangementsinplaceforfollowupcarebythekeyworker,oranopportunityforhertoprovideinputintotheappropriatenessofdischargingMr Burton at that time.
Finally,theMOdidnotexerciseduecareintermsofhelpingtofindappropriateaccommodationafter discharge. The records did not support the MO’s claim that the issue of accommodation wasdiscussedatlengthandwithcarewithMrBurtonandhisfamily.TheCommissionerconcludedthattwoaspectswereinadequatelyhandled:thesearchforresidentialprogramsto address drug and alcohol use; and a more complete needs assessment to address those aspects of support necessary for improving Mr Burton’s ability to cope in the community. Referralwasmadeforneedsassessment,buttheMOdidnotsubsequentlychecktheoutcome–includingwhethertheinformationrequiredtoplanongoingcarehadbeenobtained.
The Commissioner concluded that consideration should have been given to compulsory confinementofMrBurton.Therewasevidenceofamentaldisorder,ahistoryofproblemswithmedicationconcordance,andreluctantengagementwithtreatmentplans.Atleast,theMOshouldhavediscussedthiswithaseniorcolleaguebuthedidnotdoso.

��6 Patient Safety: a comparative analysis of eight Inquiries in six countries
Finally,theCommissionerwascriticaloftheMO’seffortstoinvolvethepatient’sfamily,whowerelovingandinterestedinbeinginvolvedinhisassessment,careandprogressreview.Thepatient’sfather reported that he had little information about some aspects of inpatient care. He felt that hehadtoinitiatemostofthecontactwiththeclinicalteam,andeventhenlittleinformationwasprovided. The MO told the inquiry team that the Mr Burton family (other than the father) gave theimpressionthattheydidnotwanttobeinvolvedinthepatient’scareanymore.Intotal,theCommissionerconcludedthattheMOdidtoolittletoinvolvethefamily,discusstheirconcerns,outlinethelikelycourseoftreatmentandproposedplans,orensureappropriateinvolvementofthefamily in the treatment process.
TheMOalsofailedtomakeadequateclinicalrecords.Theinquiryreportsaidthathisentriesinthepatient’snoteswere‘scanty’,hefailedtodocumentatreatmentplan,anddidnotdocumentthe rationale for leave. The MO admitted to the Inquiry that his clinical records did not meet anappropriatestandard,andacknowledgedthatitwouldbe“…hardtojustifythatamountofdocumentation”.
EnrolledNurseA
Patientsatthehospitalweretypicallyassignedtwonurses–aprimarynurse(usuallyastaffnurseandanassociatenurse(usuallyanenrollednurse)).EnrolledNurseAwasMrBurton’sassociatenursefromthedayhewasadmitted.ShewasalsoMrBurton’sde facto primary nurse before Staff NurseAtookontheroleasdescribedlater.
TheCommissionerconsideredithadbeeninappropriatetoallowEnrolledNurseAtoperformthedutiesoftheprimarynurse.However,shehadprovidedappropriatecare,andcouldnotbeheldresponsibleforhavingbeengivenresponsibilitiesabovewhatwasdefinedbytheoperatingrules.
StaffNurseA
TheperformanceofStaffNurseAwasmorestronglycriticised.Inparticular,sheperformedpoorlywithregardtoplanningandevaluatingMrBurton’scare,coordinatinghiscarewhileontrialleave,dischargeplanning,directingandsupervisingEnrolledNurseA,andensuringconsistencyinqualityof care.
ShedidnotundertakeacomprehensivenursingassessmentwhenshebecameMrBurton’sprimarynurse,nordidsheupdatehisexistingcareplan.Shedidlittlewithregardtocoordinatingcarewithother members of the clinical team or involving the patient and his family. She failed to ensure there wasanadequatedischargeplan.
Whenquestionedaboutherfailuretoperformacomprehensivenursingassessment,sheclaimedthiswasbecausesheconsideredthatsuchassessmentsshouldbeinstigatedbythedoctorsratherthan nurses. She also said that she did not update Mr Burton’s nursing care plan because there had beennochangeinthelevelofriskassessedbythedoctors.
TheCommissionerrecognisedthereweresystemdeficiencies,includinglimitationsoftheprimarynursingsystem,whichplacedStaffNurseAinadifficultpositionattimes.However,heconcludedthe problems mainly originated in substandard performance of the particular nurse.
SocialWorkerA
SocialWorkerAwasjudgedtohaveprovidedcareofaninadequatestandard.Forexample,hefailedtopaysufficientattentiontoclinicalaspects(includingfailuretoreadthenotesrelatingtoMrBurton’spastcare).HedemonstratedapoorunderstandingofMrBurton’smentalillness,andthis

��7
adverselyaffectedthecareheprovided.HehadnoknowledgeorskillstoassessMrBurton’smentalstate,failedtocreateeffectivecareplans,anddidnotgiveappropriaterecommendationsto other members of the team.
SocialWorkerAarguedthathewasworkingwithina‘dysfunctionalsystem’.TheroleheshouldhaveplayedwithintheteamcaringforMrBurtonwasilldefinedandnotfullyunderstoodbyother members of that team. The managers at Southland DHB should therefore accept some responsibilityforthefactthathehadbeenplacedinapositionthathewasnotprofessionallyequippedtofill,andinateamthatcouldnot(orwouldnot)givehimappropriatecollegialsupport.
ThisviewwasacceptedinpartbytheCommissioner.Withregardtosupervisionoftheperiodoftrialleave,forexample,SocialWorkerAwasgivenataskforwhichhewaspoorlyequipped.HewasgivennoclearguidancebytheMOorStaffNurseAwithregardtowhathewasexpectedtomonitorwhileMrBurtonwasonleave,nortoldthatMrBurtonpresentedunusualrisks.However,inotherrespects,theinquiryteamconcludedthereweredeficitsinSocialWorkerA’sperformance,withinthescopeofworkforwhichheshouldhavehadsufficientexperienceandtraining.
MentalHealthNeedsAssessor
TheMentalHealthNeedsAssessorwasassignedtoundertakeanassessmentofMrBurtonwhilehewasintheinpatientmentalhealthunit,andthiswasclearlyspecifiedintheoperatingrules and guidelines to be an essential part of the patient’s discharge planning. The clinical team madeareferralforMrBurtontohaveaneedsassessmentbuthewasdischargedbeforetheassessmentwascompleted.
The Needs Assessor documented the partially completed assessment on the approved assessment form and made an effort to involve Mr Burton and his parents in the process. However,shefailedtoprovidealltherelevantinformationtotherestoftheteam,partlybecauseshewasgiventheimpressionbyothersintheclinicalteamthattheassessmentwasneitherurgentnorimportant.TheCommissionerwascriticalofherlackofassertivenessinherinteractionwiththeclinicalteamonceshehadgatheredinformationthatsheherselfconsideredimportant to the discharge plan.
AlcoholandDrugServicesCounsellor
TheAlcoholandDrugServicesCounsellorworkedatRhannaClinic,whichispartofSouthlandDHB’sMentalHealthServices.MrBurtonwasreferredtotheClinicbyWard12staffalmostamonthafterhewasadmittedtohospital.TheAlcoholandDrugServicesCounsellorwasassignedthereferralandundertookanalcoholanddrugassessment.
TheCommissionerwascriticalofonlyoneaspectofthework:theCounsellorfailedtodocumentany overall conclusions or recommendations after he completed his assessment. This surprised theInquiry’sexperts,asonepurposeofaspecialisedassessmentistoprovideamoreexpertperspectivethanisavailablefromageneralclinician.Suchanassessmentshouldbefollowedbysomeconclusioninrelationtoitsfindings.TheexpertsconcludedthattheAlcoholandDrugServices Counsellor’s failure to document conclusions or recommendations indicated he did not appreciate the important role of a specialist service in the spectrum of care.
The Counsellor noted in response to the provisional opinion that he did include in his report the client’sexpectationsandadischargeplan,andthusitshouldhavebeenapparentthatMrBurtonwasunwillingtoaddresshisalcoholanddrugproblem.Thiswasnotacceptedassufficient
��8 Patient Safety: a comparative analysis of eight Inquiries in six countries
reason: the Commissioner concluded that it represented poor practice to the extent that other membersoftheclinicalteamweredeniedtheopportunitytogainamoreindepthinsightfromthespecialised assessment.
Managementandleadership
TherewerethreepeoplewhohadtheprimarymanagementandleadershipresponsibilitiesforSouthland DHB’s Mental Health Services: the Clinical Director; the Patient Services Manager; and theTeamLeader.AccordingtotheInquiry,theyeachfailedtofulfiltheirstatutoryresponsibilities.
ClinicalDirector
TheClinicalDirectorwasSouthlandDHB’sseniorpsychiatrist,withlinemanagementresponsibilitiesforallmentalhealthservicesmedicalstaff.Heorshewasexpectedtoprovideleadership,ensureclinicalserviceswereprovidedeffectively,andfacilitatethetraininganddevelopmentofmedicalstaff as appropriate. Inter alia,theClinicalDirectorwasrequiredtoassesstheperformanceofmedicalstaff,establishandmonitorclinicalstandardsofpractice(includingpeerreview,clinicalauditandqualityassuranceactivities),andensurethatclinicalnoteswereadequatelymaintained.
The inquiry team concluded the Clinical Director failed to provide adequate clinical leadership. Hedidnotrealisethatthemonitoringandreviewingthestandardsofpracticeofmedicalstaffwererequiredbyhispositiondescription.Moreover,hefailedpreciselytodefinetherolesandresponsibilities of medical staff involved in the provision of mental health services.
HispositiondescriptionclearlyassignedtohimtheresponsibilityforreviewingtheMO’sperformanceandensuringthathemetrecognisedstandardsofclinicalpractice.However,heregardedtheMOasapsychiatristeventhoughhehadnospecialistqualificationandlimitedformaltraininginpsychiatry.Moreimportantly,hefailedtospecifythelimitsontheMO’srighttoprovideunsupervisedcare.TheClinicalDirectorsaidthathethoughtitwouldbe‘ungentlemanly’toreviewtheMO’sstandardofpracticeandthathewasnotawareofthenecessitytobe‘lookingoverhisshoulder’ortobecheckingonhiminanyway.Hisassumptionwasthataqualifiedandresponsiblephysicianwouldbringhisconcernstoacolleagueifhefelthewasnotmanaging.
InresponsetotheCommissioner’sprovisionalopinion,theClinicalDirectorarguedthattheexpertadvisorsseemedunabletodistinguishbetweensupervisionandoversightandthat“…whattheyseemtodeemappropriatewouldbemoreaccuratelydescribedassurveillance”.HestatedthatcommentsaboutthelegalrequirementsforoversightnotbeingmetwereincorrectandreferredtheCommissionertotheguidelinesforgeneraloversightpublishedbytheMedicalCouncilofNewZealand.
TheCommissionerconcludedthattherewasindeedadifferencebetweensupervisionandoversight,butneitheroversight(asrequiredbylaw)norsupervisionhadbeenundertakenbytheClinicalDirector in relation to the MO.
TheCommissionernotedthattheClinicalDirectorappearedtohavenoknowledgeofwhatwasinhispositiondescription.Indefenceofhisemployee,theChiefExecutiveOfficerofSouthlandDHBarguedthattheClinicalDirector’s“…lackofin-depthfamiliaritywithagenericjobdescriptionisbothtrivialandunderstandable”.TheCEOarguedfurtherthatitwassufficientforstafftobeawareonlyofthegeneralintentoftheirpositiondescriptions,especiallygiventhatpracticeschangeovertime.TheClinicalDirectorhadamoralobligationtoaddresstheclinicalissuesfirst,regardlessofthescope of practice envisaged by his position description.

��9
TheCommissionerdisputedthisview.HenotedthattheClinicalDirectorhadsomekeyresponsibilitiesinhispositiondescriptionofwhichheneededtohavebeenawareinordertocarryouthisresponsibilities.Inparticular,heoughttohavebeenawarethatmonitoringandreviewingthestandardsofpracticeofmedicalstaffwasacriticalduty.
TheClinicalDirectorarguedthatcomplexityandoverworkweremajorfactors.Thementalhealthserviceswereseriouslyunderresourcedandtherewasalackofexperiencedstaff.Theinquiryteamacceptedthattherewereextremepressures,butconcludedthattheClinicalDirectorfailedtotakereasonableactionstoensurethattheMOwasoperatingwithinanappropriatescopeofpractice,andthathewasadequatelysupervised.
PatientServicesManager
ThePatientServicesManagerwasamemberofSouthlandDHB’sseniormanagementteamandreporteddirectlytotheChiefExecutive.Hermaintaskswere“…todevelop,provideandmonitorthedeliveryofhighquality,patientfocused,effectiveclinicalservices;developastyleofleadership,andmanagementsystemsandprocesses,thatreflectSouthernHealth’svalues;andenablethepeoplewithinmentalhealthservicestoactivelycontributetothecontinuousimprovement of health services and their delivery.”
Herperformancewasjudgedtobesatisfactoryinmostrespects.However,sheperformedinanunsatisfactorywaywithregardtoensuringtherewereadequatestaffinglevels.Forthemostpart,understaffingwasacorporateerroronthepartofSouthlandDHB.However,thePatientServicesManagercouldhavehandledsomemattersmoreeffectively.Inparticular,sheshouldnot have given so large a role to the part time Team Leader.
Norshouldshehaveassignedasocialworkerwhohadnopriorexperienceofmentalhealth.Shewasresponsibleforhispositiondescription,andfailedinherdutybynotensuringitspecifiedknowledgeofmentalillnessasarequirement,especiallyinviewofthefactthatthepositiondescriptionrequiredhimtoworkautonomouslywithpatientswithmentalillness.Similarly,sheshouldhaveseenthattheAlcoholandDrugServicesCounsellorhadinsufficienttrainingandsupporttoprovideMrBurtonwithservicesofanappropriatestandard.
TeamLeader
The Team Leader had overall responsibility for the management and leadership of the inpatient mental health unit. This included responsibility for the budget. It also included responsibility for aspects of the team’s clinical practice.
Inparticular,shewasresponsibleforensuringthatpoliciesandprocedureswereestablishedandimplemented,includingensuringthatindividualtreatmentanddischargeplansweredevelopedinconsultationwithpatients,families,andothercaregivers.Thenursingstaff,RecreationCoordinator,SocialWorkerandOccupationalTherapistreportedtotheTeamLeader.Themedicalstaffdidnot.Inspiteofthewiderangeofresponsibilities,shewasonlyemployedfor30hoursperweek.
WenoteasanasidethattheexclusionofmedicalstafffromtherequirementtoreporttotheTeamLeadermighthavebeenproblematicintermsofensuringcohesion.Thisaspectisnot,however,raisedintheCommissioner’sreport.
TheCommissionerconcludedthat,ingeneral,theTeamLeaderranacohesiveteamwithahighdegreeofloyaltyandcommitmenttothework.Hermanagementofthewardresultedinarelativelystablenursingworkforceinthefaceofnationalmentalhealthstaffshortages.

�20 Patient Safety: a comparative analysis of eight Inquiries in six countries
However,aspectsofherworkwerecriticised.First,therewasnoevidenceofaconsistentmethodofallocationofprimarynursestopatients.Norweretherereliableandpermanentrecordsoftheassignmentsofaprimarynurse.TheTeamLeaderadmittedtherewereweaknesses,mostofwhichderivedfromexistingpracticeswhenshetookoverthejob.Inparticular,assignmentswerelargelyamatterdecidedbynegotiationamonggroupsofnurses.Inadequateruleswereinplacetocoverproblemareas,suchasnurseabsencesonleave.Stepswerebeingtakentoovercometheproblems.
Second,theinquiryteamwascriticaloftheTeamLeader’sfailuretoensureenrollednurseswerenotgiven(ortook)aninappropriatelevelofresponsibilityforplanning,implementingandcoordinatingcare.Thiswasrelatedtotheissueofallocationofprimarynurses.WhiletheCommissioneracceptedthattheinadequateprocesseswerealreadyinplacewhentheTeamLeaderwasappointed,heconsideredthereshouldhavebeentimetoaddressthembeforeMrBurton became a victim.
Third,theTeamLeaderwasresponsibleforensuringpatientshadclinicallysoundcareplansthattookaccountoftheviewsofpatientsandtheirfamilies.Thehospitalusedacomputerisedcareplanningapplication.However,itwasnotusefulforcareplanninginthementalhealthsetting,andtherewerelowlevelsofcomplianceamongthenursingstaff.TheCommissioneracceptedthattheTeamLeaderwasaddressingtheneedforimprovednursingcareplans.However,hewascriticalofthefactthatMrBurton’scareplanwasmadebyanenrollednurse,andthatitwasnevercheckedand updated or amended as necessary by a registered nurse.
Finally,theinquiryteamconcludedthattheTeamLeaderfailedtorealisethatnursingstaffshouldbeactivelyinvolvedintheprocessofriskassessment,ratherthansimplyfollowingthedoctor’slead.TheCommissionerconsidereditwasamistaketoencourageorallownursestoplayapassiverole.
Corporateresponsibility:SouthlandDHB
Theinquiryteamconcludedthatthestandardsforthementalhealthservicethatwerespecifiedinpositiondescriptions,policystatements,andproceduraldocumentationweregenerallyadequate.However,somestaffwerenotawareofthestandards.Atbest,theyhadonlyageneralideaoftheircontents.Inthisandotherways,thestandardswerenotsatisfactorilyimplemented.
Awidespreadfailuretofollowthestandardscontributedtoandfacilitatedmistakesbyindividualclinicians.Asnoted,theCommissionerconcludedthattheTeamLeaderandtheClinicalDirectordidnotexertsufficientleadershiptoensurecompliance.Moreover,thePatientServicesManagerdidnot apply adequate processes to monitor compliance and its effects on the quality of clinical practice.
The inquiry team concluded that the inadequate performance of these and other staff responsible forthecareofMrBurtonwasaconsequenceofsystemicweaknessesinthemonitoringandcontrolmechanisms in Southland DHB’s Mental Health Service. The concerned staff carried personal responsibilitiesforaspectsofpoorcare,buttheywerealsovictimsofinappropriatecultures.
Theexamplewasgivenofthemaintenanceofclinicalrecords.TheMO’sfailuretokeepadequaterecordswasnotedearlier.However,manyoftheotherstaffinvolvedinMrBurton’scaredidnotgenerate good records. The Commissioner referred to frequent use of the term ‘settled’ to describe MrBurton’smentalstate.Heconsideredthistermtohavelittlemeaning.“Itconveysasensethattherewerenobehaviouralproblemsobserved,butgivesnoideaastowhetherclinicalphenomenasuchasdelusions,hallucinations,orevennegativesymptomsofschizophrenia(suchasanergia,amotivation,withdrawal)orofmooddisorderwereevident,orsoughtafterandunabletobeassessed.Thesedetailsaretheessentialcriteriaagainstwhichclinicalprogresscanbemeasured.”

�2�
Intotal,documentationofMrBurton’ssymptomswassoinadequatethat“…anobserveruninvolvedinhiscarewouldnotbeabletodetermineaccuratelywhetherBurtonwasreallyillinanyway,orwhatprogresshehadmade.”
Patientdocumentationwasofpoorqualityinspiteofseveralattemptstoimprove.In1999,forexample,SouthlandDHBintroducedintegratedclinicalnotes.Allclinicalrecordsforapatientwererequiredtobestoredtogethertopromotecontinuityofcarethroughoutthementalhealthservice.Allmembersofthemultidisciplinaryteamwererequiredtodocumentpatientcare,variances,progressandtreatmentintheintegratednotes.
TheserequirementswerenotmetinMrBurton’sclinicalrecords.Forexample,needsassessorskepttheirrecordsseparatelyinthesocialworkdepartmentuntiltheneedsassessmentwascompleted.Copiesofincidentformswerenotkeptintheclinicalrecords.
TheMentalHealthNeedsAssessor,RecreationCoordinatorandtheAlcoholandDrugServicesCounsellorinvolvedinMrBurton’scaredidnotmakeanyentriesinMrBurton’sclinicalrecords–anddidnotrealisetheywereexpectedtodoso.
SouthlandDHBwasconsideredtoberesponsibleforseveralotherhospitalwideweaknesses.Onewasinadequatecompliancewithincidentreportingrules.WithrespecttoMrBurton’scare,theCommissionerconcludedtherewereatleasttwooccasionsonwhichanincidentformshouldhavebeencompletedbutwasnot.Whereanincidentwasinfactreported,therewasnoevidencetoshowitwasinvestigatedinaccordancewiththerules.
ParticularconcernwasexpressedbytheCommissionerregardingweeklyteamreviews,whichprovidedtheonlyopportunityforclinicalstafftoreviewthepracticeofcolleaguesandtooffersupportandguidance.ThedocumentationfromthereviewsundertakeninrelationtoMrBurtonsuggestedthatsignificantinformationwasnotdiscussed–suchashispersistingpsychoticsymptoms,variousincidentsthatoccurredduringhisinpatientcare,andthepossibleuseofcompulsory assessment and treatment.
Anotherhospitalwideweaknessconcernedtherolesandfunctionsoftheclinicaldirectors.TheCommissionerarguedthatclinicianswhoaregivenresponsibilitiessuchasthosethatappliedatSouthlandDHBmustbegiventrainingandthetimeandsupporttodeveloptheirskills.Inthecaseofmentalhealthservices,thiswasnotthecase.Forexample,therewasnoreductionintheClinicalDirector’sclinicalworkloadwhenhewasappointedasClinicalDirector.TheGeneralManagerofHospitalServicesatSouthlandDHBadmittedtherewasnoformalguidanceordirectiongiventoclinicaldirectorsabouthowtomanage,includinghowtosettheirpriorities.
Indeed,SouthlandDHBhadallowedtheviewtobeformedthatclinicalleadershipshouldtakeabackseatrelativetotheprovisionofclinicalcare.Itappearedthatnoconsiderationwasgivento the possibility that a focus on the immediate care of individual patients might mean they (and futurepatients)mightsufferfromunresolvedsystemicproblems.Atleast,managersofalltypesseem to have been reluctant to face this dilemma.
Severalreferencesaremadetofailurestocommunicateandcollaborate.Forexample,itisnotedthatthePatientServicesManagerwantedtoworkinpartnershipwiththeClinicalDirector,andinitiallysaidthatshefeltshedid.However,shesubsequentlyadmittedthattherelationshiptooneof‘cooperativeendeavour’.TheevidenceshowedthatthePatientServicesManagerandtheClinicalDirectordidnotinfactalwaysworktogethereffectively.TheCommissionernotedthat“…asuccessfulpartnershiprequiresawillingnesstobuildapartnershiponbothsidesbasedoncommongoals,andacommitmenttoclinicalandfinancialaccountabilityandtobetter

�22 Patient Safety: a comparative analysis of eight Inquiries in six countries
healthoutcomesforpatients.DevelopingapartnershipbetweenclinicalleadersandmanagementisakeyfactorinbuildingaqualityculturewithintheNewZealandhealthsystem(MalcolmandWright2002)”.
Manyotherexamplesofpoorteamworkwereprovided.ThePatientServicesManagerconsideredthattheClinicalDirectorhadanimportantroleinthemonitoringofstandardsbutthisviewwasnotsharedbytheClinicalDirector.Theyidentifieddifferenttrainingprioritiesfortheservice,andtherewasnoevidencetosuggesttheyhaddiscussedtrainingissues.Theyagreedtodisagreeonsuchmattersasinternalclinicalreviewandincidentreporting.
Intotal,theCommissionerconcludedthatSouthlandDHB’sMentalHealthServicewaspoorlymanaged.Thereweresomanyorganisationalshortcomingsthatqualityofcareformentalhealthpatientswasinevitablycompromised.Theriskofadverseeventswasnotmanagedeffectively.Southland DHB must accept corporate responsibility for this state of affairs.
8.4 RecommendationsoftheInquiry
TheCommissionergaveprecedencetoasimplecorrectivemeasure:lettersofapology,signedbytheClinicalDirector,theMO,thePatientServicesManager,theTeamLeader,StaffNurseA,theMentalHealthNeedsAssessor,SocialWorkerA,andtheAlcoholandDrugServicesCounsellorshould be dispatched to Mr Burton and to his family. Southland DHB should also offer letters of apology.
Theremainderoftherecommendationsfallundereightmainheadings.First,thetwodoctorswhoseperformancewasmostcriticised(theMOandtheClinicalDirector)shouldhavetheircompetencereviewedbytheMedicalCouncilofNewZealand.
Second,selfassessmentwascalledfor.Allthestaffwhoseperformancewasreviewedandcriticisedwereaskedtoreviewtheirownpracticesinlightofthisreport.
Third,SouthlandDHBwasadvisedtoreviewandimprovetheperformanceofthosehealthcareprofessionalswhoseperformancewasdeficient.Forexample,thetrainingandsupervisoryneedsofthe Clinical Director and the Patient Services Manager should be addressed. Performance criteria fortheTeamLeader’spracticeshouldbedefined.Thequalifications,skillsandexperienceoftheMentalHealthNeedsAssessorshouldbereviewed.ThecompetenceoftheSocialWorkerandtheAlcohol and Drug Services Counsellor should be assessed.
Fourth,SouthlandDHBwasadvisedtotakealargenumberofspecificactionstoaddresstheunderlyingcausesofpoorcare.Theycanbetakenfromtheconclusionssummarisedabove.
Ofparticularimportance,thehospitalshoulddevelopinternalauditandmonitoringprocessesdirectedatcompliancewithpoliciesandproceduredocuments.Immediateattentionshouldbegiventopatientassessment,patientrecordanddocumentation,incidentreporting,riskassessmentandmanagement,qualitycareandtreatment,discharge,supervision,andfamilyandcarerparticipation.Thisshouldincludethereviewofpolicyandprocedureimplementationmechanismstoensureadequateattentiontothesedocumentsinorientationofnewstaff.
Fifth,attentionshouldbegiventodevelopingacultureofcontinuousqualityimprovement.Thisshouldincludeestablishingacultureofcriticalappraisalandreflectionbyallinpatientstaffandbyseniormedicalstaff.Theinitialpriorityshouldbetoreviewtheimpactofchangesininpatientteamweeklyreviewprocesses(attendanceandactiveparticipationofallseniormedicalstaff,presentationofcases,documentationofoutcomes,communicationofdecisions).

�23
Sixth,effortsshouldbemadetoimprovenursingstandardsformentalhealthnursing.Thisshouldincludetheidentificationofspecificskillsthatneedtobeimproved.
Seventh,staffingstructuresandemploymentconditionsshouldbereviewed.Thisshouldincludeconsiderationoftheestablishmentofprocessestoprovideprofessionalsupportfornurses,acomprehensivementalhealthnursingclinicalcareerpathway,andanimprovedmodelofnursingassignment to patients.
Finally,stepsshouldbetakentoimprovecommunicationandcoordination.Thisshouldincludebetter integration of support services such as needs assessment and drug and alcohol services.
8.4.1 GeneralrecommendationsofDrTaumoepeau’sclinicalaudit
WenotedearlierthatDrTaumoepeau’sreportpresentedanalmostidenticalpictureofthequalityofMrBurton’scaretothatpresentedbytheCommissioner.However,shemademoregeneralrecommendationsaboutcareprocesses.Thesearesummarisedbelow.
First,theminimumrequirementisthateachpatientmusthaveafullmentalstatusexaminationrecordedatadmissionandafullreviewofthatmentalstatusexaminationclosetothetimeofdischarge. This is primarily the responsibility of the medical staff. The alcohol and drug history takenbythemedicalstaffinthementalhealthservicesshouldbedetailed,regardlessofwhetherornotthepatientwillsubsequentlybereferredtothedrugandalcoholservices.
Second,themedicalstaffmustoutlineatleastthebasictreatmentplanandensurewhichindividualswillcarryoutthatplan.Thismustoccurimmediatelyafterassessment.
Third,documentationshouldbeimproved.Documentationmustbecompletedonadmissionanddischargeandatotherkeytimes(suchaswhenthereisamarkedchangeinthepatient’ssituation or referral to a different part of the service).
Fourth,theinpatientweeklyreviewformisinadequateinthatitdoesnotassiststaffinassessingtreatmentgoalsandtaskstobeundertaken.Thereviewreportformisbetterandcouldbeadapted for both inpatient and outpatient use. It should include such issues as barriers to discharge,andindicatetaskstobeundertaken,bywhomandinwhattimeframe.Ifthepatientisbeingreviewedasaninpatientonaweeklybasistheformshouldbesentasamatterofcourseto the patient’s community team.
Fifth,itistheresponsibilityofmedicalstafftoensuretheyadequatelyreadthenoteswhentheyreviewapatient.However,thereshouldalsobeaprocesswherebystaffofotherclinicalprofessions(andespeciallynursingstaff)canhighlightpatientsofconcernwhoneedreviewbythe medical staff.
Sixth,incidentreportsshouldbefiledintheclinicalnotesinchronologicalorderalongsideprogressnotes.Staffshouldbeclearaboutthethresholdforfillinginanincidentreportandthereshouldbealistavailabletostaffastowhichincidentsrequireareporttobewritten.Anoteoftheincidentsshouldbeincludedintheweeklyreview.
Seventh,medicalofficersneedtohaveformalandregularsupervisionbyaconsultantpsychiatrist. The Terms of Reference of supervision should be recorded and should include frequency,lengthofsupervisionsessionsandcontent.Thecontentshouldincludearequirementforthemedicalofficertopresentallnewpatientstothepsychiatristandtofollowuponrecommendationsmadebythepsychiatrist.Inotherwords,themedicalofficershouldbetreatedas a registrar in terms of supervision and accountability.

�24 Patient Safety: a comparative analysis of eight Inquiries in six countries
Eighth,trainingshouldbeprovidedincertainareasincludingriskassessmentandmentalstatusexamination.Competenciesshouldbeidentifiedifthesearenotalreadyinplaceforalldisciplines.Thereshouldberegulartrainingsessionsforthemultidisciplinaryteam,andallmultidisciplinaryteam members should be encouraged to present at those sessions. Medical staff should be required toattendpeerreviewandclinicalrevieweducationalsessions.
8.5 Discussion
WhiletheSouthlandInquiryisdistinguishable,amongsttheotherinquiriesinthisreport,indealingwithasingleincident,theprocess,findingsandoutcomesofthisinquiryareremarkablysimilartothoseotherinquiries.Aswithotherinquiries,additionalinvestigationswerealsoconducted.TheCommissioner’sexpertpanelproducedaseparatereport,whichisoutlinedinsection8.6below.Acoronialinvestigationintothedeathoftheclient’smotherwasalsoheld.
TheSouthlandInquirypainstakinglysiftedthroughtheroles,responsibilitiesandfailuresofeachofthecliniciansandmanagersinvolvedinthecase.Itsultimatefindingwasthattheincidentinvolvedarosefromacombinationofindividualandbroadersystemsfactors,ratherthanasinglecause.TheCommissionerwascarefultoensurethatthisconclusiondidnotresultinadilutionofresponsibilityforwhatoccurred.IndeedhearguedthatbothindividualandcorporateresponsibilityneededtobetakenforthedeathofMrsBurton,andtheimpactontheBurtonfamilyasawhole.Tothisend,andunlikeotherinquiriesinthisinstance,theCommissionerorderedallthestaffinvolved,andtheBoard,towriteformallettersofapologytothefamily.
IntheaftermathoftheInquiry,theHealthandDisabilityCommissioner’sOfficeissueddisciplinaryproceedings against three registered health professionals involved in the case. Disciplinary charges werefiledbeforetheMedicalPractitionersDisciplinaryTribunalagainsttheMedicalOfficerandtheClinicalDirectoroftheservice.In2003theMOwasfoundguiltyof17chargesofprofessionalmisconduct.Hewasbannedfrompractisingmedicineforsixmonths,andreceivedafine.AdisciplinarychargewasalsofiledwiththeNursingCouncilagainstoneofthestaffnurses(identifiedas‘A’intheInquiry).ThecoronialinquiryfoundthatMarkBurtonshouldnothavebeenreleased.Itdidnot,however,singleoutcliniciansforcomment,referringrathertotheshortageofpsychiatristsand the need for better staff training.
8.6 Footnote
8.6.1 TheReviewPanel’sreport
TheCommissioner’sexpertgroup(thereviewpanel,RP)producedaseparatereportin2002.Thisisappendedtotheinquiryreport.Forthemostpart,itisidenticalincontenttothemainbodyoftheCommissioner’sreport.However,thereisoneelementthatisdiscussedingreaterdetailandgiven greater emphasis – the idea of quality improvement. The RP also used the terms total quality management and continuous quality improvement as if they had identical meanings.
TheRPnotedthatqualityimprovementwasthethemeofareportcommissionedin1992bytheCanterburyAreaHealthBoard(Bonneretal1992).TheRParguedthattheframeworkpresentedinthereportappliedasmuchnowasitdidthen.Theauthors’frameworkforgoodqualitycarecomprisedoptimaloutcomes,minimalriskstopatients,clientsandstaff,patientsatisfactionandtheefficientuseofresources.
�25
AccordingtotheRP,“…totalqualitymanagementseekscontinuousimprovement,involvingeveryonewithanemphasisonqualityinallprocesses.Theroleofmanagementistoprovideleadership,communicateaclearvision,andprovidethesupportandeducationtocreatetherequiredculturalchangewithintheorganisation.Teamsshouldbeempoweredtocontinuouslyimprove the process and build quality into the system.”
The Ministry of Health had incorporated these ideas into its �997 publication titled ‘National MentalHealthStandards’.Oneofthethemeswasthatmentalhealthserviceorganisationsshould“…promotecontinuousqualityimprovement”inorderto“…ensurethatservicesofferthehighestlevelofcaretothosewhousetheseservices.Theythusprovidesomeusefuldirectionforclinicalandoperationalleaderswithinanorganisation.”
SouthlandDHBhadtakensomestepstoincorporatestandardsintoitsmentalhealthservicesoperatingrulesandguidelines.TheRPconcludedthatthoserulesandguidelineshadbeenwelldesignedandsubsequentlysubjectedtoregularreviewandupdatingtotakeaccountofchangesinpracticestandardsandrecommendationsfromincidentreviews.
Themainproblem,accordingtotheRP,wasthatmanyoftherulesandguidelineshadsimplynotbeenputintopracticeindaytodaycareprovision.Thereweredeficienciesintermsofboththeestablishmentofacultureofqualityimprovement,andintheprocessesofcarethatshouldhave been the subject of continuous improvement.
Particularattentionwasgiventodeficitsinleadershipatthelevelofthehospitalandatthelevelofthementalhealthservicesteam.Thedeficitsincludedalackofmutualunderstanding,ineffectivecommunication,andfailuretoestablishforumsinwhichproblemscouldbeopenlydiscussed.
TheRPnotedseveralsymptomsoftheseproblems.Forexample,“…theClinicalDirectorreportedthathedoesnotfindaspecifiedreportingrelationshiptotheorganisation’smedicaladvisorstobeuseful,andhelargelydoesnotuseit.”TheGeneralManagersimplyacceptedstandardsofpracticeweresatisfactory“…withoutevidenceofclearsystemsforreviewofperformance for medical staff.”
Individualsraisedconcerns.Buttherewasseldomanywillingnesstohavethemdiscussedinteam meetings.
Forexample,onememberoftheteamnotedachangeinMrBurton’sbehaviourthatmighthavebeenduetoalcoholuseandwasconcernedtodocumentitbut“…thereappearstohavebeennofollowupbyotherstaff.”TheMentalHealthNeedsAssessornoticedachangeinBurton.“Shewasconcernedenoughtodiscussitwiththenursepresentatthetime,butthenursemadenorecordofthis.”SocialWorkerA,whenconductingthedrugandalcoholassessment,obtainedinformation not gathered by any member of the inpatient team. He documented this but the teamoverlookedit.Finally,anewgraduatenursewasconcernedthatMrBurtonhadcontactedhisfatherandwasexpressingparanoidideas.Shefeltthattheconcernsintheletterhadtobetakenseriously,buttheywerenot.

�26 Patient Safety: a comparative analysis of eight Inquiries in six countries
8.7 Referencesandselectedbibliography
Bonner,M.Coughlan,J.andParker,R.(1992).Introducing Total Quality Management in an Area Health Board.Canterbury,NewZealand:CanterburyAreaHealthBoard.
Cartwright,R.(1988).The Report of the Committee of Inquiry into Allegations Concerning the Treatment of Cervical Cancer at National Women’s Hospital and into other Related Matters. Auckland:GovernmentPrintingOffice.
Cull,H.(2001).Review of Processes Concerning Adverse Medical Events.Wellington:NewZealandMinistry of Health.
Duffy,A.P.,Barrett,D.K.andDuggan,M.A.(2001).Report of the Ministerial Inquiry into the Under-Reporting of Cervical Smear Abnormalities in the Gisborne Region.Auckland:MinistryofHealth.
Health and Disability Commissioner (2002). Southland District Health Board Mental Health Services, February–March 2001: A Report by the Health and Disability Commissioner.Auckland:Healthand Disabilities Commission. Available at: http://www.hdc.org.nz/files/pagepublications/other_southlandreport.pdfAccessedon14November,2004.
Health and Disability Commissioner (200�). Commissioner Announces Independent Inquiry into Southland District Health Board.Auckland:HealthandDisabilitiesCommission.Availableat:http://www.hdc.org.nz/publications.php?publication=151,Accessedon3March,2006.
Health and Disability Commissioner (2002). Wide Ranging Recommendations on Southland DHB Mental Health Service.Auckland:HealthandDisabilitiesCommission.Availableat:http://www.hdc.org.nz/publications.php?publication=149Accessedon3March,2006.
Health and Disability Commissioner (2003). Disciplinary Proceedings to be Issued against Southland health Professionals in Burton Case.Auckland:HealthandDisabilitiesCommission. Availableat:http://www.hdc.org.nz/publications.php?publication=148Accessedon3March,2006.
Malcolm,L.andWright,L.(2002).ImportantProgressinBuildingaQualityCultureinourHealthSystem. Health and Hospital,March-April:12-13.
Paul,C.(2000)InternalandExternalMoralityofMedicine:LessonsfromNewZealand.British Medical Journal, 320(7233): 499–503.
Reason,J.(2000).HumanErrorModelsandManagement.British Medical Journal,320:768.
9 WinnipegHealthSciencesCentre,Canada
ThissectionconcernscarethatwasprovidedattheWinnipegHealthSciencesCentre(theCentre)in1994.Twelvechildrendiedbetween14Marchand21DecemberduringorshortlyafterhavingundergonecardiacsurgeryattheCentre.Therewasahighdegreeofconcerninthemassmedia,mainlyasaconsequenceofactionsbytheparentsofthechildrenwhodied.
TheInquestthatwassubsequentlyconductedfoundthatcarehadbeenseriouslydeficient.ThefollowingistakenmainlyfromtheInquestReport.

�27
9.1 Context
The Centre had been operating a small but apparently satisfactory paediatric cardiac surgery program(theProgram)forseveralyears.However,itwassuspendedforashorttimein1993duetothelossofkeystaffincludingthreecardiologists.
Inearly1994,theProgramwasreactivatedfollowingtherecruitmentofanewsurgeon(DrOdim)asheadoftheteam,andanewdirectorofpaediatriccardiology.Concernswereexpressedatthetimeastowhethertherestartwaspremature,butthereweresomecentrewidefinancialpressuresthatmayhaveinfluencedthedecision.TheInquestwaslatertoconcludethatthereweresignificantproblemsincludinginadequaterecruitmentprocessesthatfailedtotakeaccountofalackofexperienceamongthenewrecruits,andunclearlinesofauthority.Intotal,theinquiryteamwastoconcludethat“…theProgramcontinuallyundertookcasesthatwerebeyondtheskillandexperienceofthesurgeonandtheteam.”
Childdeathsin1994
InadequatelyexplaineddeathsbegantooccuralmostimmediatelyaftertheProgramwasreactivated.Thefirstof12deathsoccurredon15March1994andthelaston21December1994–afterwhichtheProgram’soperationwassuspended.Moreover,therewasavarietyofother events including unusually high levels of post-operative complications that gave rise to concern.Onlythedeathsweresubsequentlysubjectedtorigorousinvestigation.
TheInquestwastoconcludethat,ofthe12deaths,fivewerepreventableandfourwerepossiblypreventable.Theevidencewasinsufficienttoreachaconclusionontwodeaths,andonewasjudgednottohavebeenpreventable.Theyoungestchildwastwodaysofage,andtheoldestchildwasjustoverfouryearsofage.
ConcernsinsidetheCentre
Twogroupsofstaffwereconcernedabouttheperformanceofthenewsurgeonalmostimmediatelyafterhebeganwork.Nurses(andparticularlythoseinoperatingroomsandintensivecareunits)madeavarietyofattemptstointervene,butwerelargelyignoredasdescribedbelow.
Perhapsmoreimportantinsomerespects,anaesthetistsbegantoexpressconcerns.InMay1994(followingthedeathofthefifthofthe12children),themembersoftheSectionofPaediatricCardiac Anaesthesia unanimously agreed to refuse to participate in any further paediatric open-heartcasesuntilareviewhadbeenundertaken.Itisarareeventinmosthealthsystemsforanydoctortoexpressformalconcernsaboutanotherdoctor,andthefactthattherewasconcertedaction by the anaesthetists should have been an event that no one could reasonably ignore.
Formalinternalandexternalreviews
ThereactionoftheCentrewastodoonlywhatwasnecessarytoreducethelevelofconcern.Theanaesthetists’minimumdemandswereaccepted:aninternalreviewcommitteewouldbeappointedandtheProgramwouldrestrictitselftolowriskcasesduringthereviewperiod.Casesthatcouldnotawaittheoutcomeofthereviewwerethereforetransferredtopaediatriccardiacsurgicalfacilitiesinotherprovinces.However,duringthisperiodofreducedservices,twomorechildrendiedfollowingsurgeryattheCentre.
�28 Patient Safety: a comparative analysis of eight Inquiries in six countries
Inspiteoftheevidencethatwassubsequentlyshowntobeoverwhelming,thereviewcommitteeconcludedtheproblemswereanormalconsequenceofhavingarelativelynewteam,andthattheteam had resolved the causes. It therefore recommended that the Program return to full service in September1994.Fromthatpointuntil21December1994,fivemorechildrendied.
Afterthedeathofthetwelfthchild,theCentredeterminedthatnofurtherpaediatriccardiacpatientsbereferredforsurgerytothePaediatricCardiacSurgicalProgramuntilareviewcouldbecompleted by an external team. The team presented its report to the Centre in early February �995. It expressed serious concerns that needed to be addressed and advised that the Centre should suspend the Program for a further six months.
ArelativelyneutralpressreleasewasissuedasacompromisebetweenthereviewteamandtheCentre’smanagement.Itmightnothaveresultedinanysignificantpublicinterestifithadnotstimulated some of the parents into action. They might have been less angry if there had been any kindofadmissionofpossibleerroronthepartoftheCentre,orevenasympatheticexpressionofregret.Asitwas,theparentshadbeentreatedpoorly(involvinglittlemorethanstatementsthat‘surgeryisalwaysrisky’and‘theCentrehasanenviablereputation’)andweredeterminedtobeheard.Withtheassistanceofthemassmedia,theymountedahighprofilecampaignforapublicinquiry–andmoreorlessachievedwhattheydemanded.
9.2 TheInquiry
9.2.1 TheInquest(1995-1998)
On5March1995,theChiefMedicalExaminerfortheProvinceofManitobaorderedanInquestintothe deaths of the �2 children. He directed that one Inquest be convened to investigate all the �994 deaths.TheMinisterofJusticedeclinedtoappointapublicinquiry,indicatingthatthemattermightbe reconsidered once the Inquest had reported.
InquestsinManitobaaregovernedbystatute,andtoacertainextentbycommonlaw.Theyarepresided over by judges of the Provincial Court of Manitoba. Their primary role is to determine theidentityofthedeceased,thefactssurroundingthedeath,howthedeceasedcametodie,andwhetherthedeathwaspreventable.Additionally,anInquestismandatedtoinquireintowhetheranyof the policies or programs of an institution or government should be changed in order to prevent a repeat of such a death.
The Inquest commenced hearings in December �995 and completed them in September �998. ItsfinalreportwasissuednearlyfouryearsafterthedecisionwasannouncedtoundertaketheInquest.Some83witnessestestifiedduringmorethan285daysofhearings.Nearly50,000pagesoftranscriptevidencewereproduced,and10,000pagesofmaterialwerefiledasexhibitsintheseproceedings.ThevolumeofevidencewassimilartothecombinedtotalforthetwomainInquiriesoverBristol,andfarexceededthevolumesoftheMacarthurHealthServiceandCeljeInquiries.
9.2.2 ConclusionsoftheInquiry
TheJudgesaidinhispreamblethateachchildhaddiedunderdifferentcircumstances,buttherewerecommoncausesforthemostpart.Thisledhimtothegeneralconclusionthatacombinationof many serious organisational and personnel problems experienced by the Centre’s Paediatric Cardiac Surgery Program during �993 and �994 had contributed to the deaths of most of the children.Inshort,theProgram“…didnotprovidethestandardofhealthcarethatitwasmandatedtoprovideandwhichparentsbelieved,andhadarighttoexpect,thattheirchildrenwouldreceive.”

�29
Thecentralfinding:systemicproblemsleadingtopoorcare
ItwasconcludedthatsomeoftheproblemsthattheProgramfacedrelatedtotheabilitiesandconductofspecificindividuals.However,themoreimportantconclusionwasthatmostoftheproblems“…werelargelysystemicinnature.”TheyrelatedtothestructureoftheCentreand,inparticular,tohospitalpoliciesandproceduresgoverningstaffing,leadership,teamwork,communication,decisionmakingandqualityassurance.“Weaknessesinalloftheseareasledtoproblemsintheproceduresandoutcomesoftheprogram.Asafurtherresultofsystemicfailures,theissuessurroundingtheabilitiesandconductofcertainteammembers,andtheperformanceofthesurgicalteamitself,werenotdealtwithinatimelyoreffectivemanner.”
ReplacementofProgramstaff
The evidence suggests that the loss of and failure to replace professional medical staff meant that the Centre could not continue to provide the level of service that it had previously provided. TheimpactontheProgramofthelossofmedicalstaffwasnotappreciatedbytheheadsoftheresponsible departments.
TheCentre’sprocessofrecruitmentofnewstaffwasflawedinmanyways.First,thoseresponsibleforstaffreplacementsin1993and1994wereslowtobegintheprocessofrecruitment,tooktoolongtofindcapablereplacementsoncetheydidbegin,reliedoninadequateprofessionalstaffrecruitmentprocesses,andfailedtotakeappropriatestepstoaddresscaseloadandotherProgramissueswhenpositionswereleftvacantforextendedperiods of time.
Second,therewasconfusionastowhowasontheformalsearchcommitteeestablishedtofindreplacements.Severalseniorstaffclaimedtheybelievedotherswereresponsible.
Third,therewerenodocumentsestablishingaformalsearchcommittee,nominuteswerekeptofanyformalcommitteemeetings,andnocriteriaexistedforthecandidatesthatweresought.Therewerenoformalratingsofcandidatesagainstspecificcriteria.
Fourth,noseriousattemptsweremadetoassessthecompetenceofcandidatesinanobjectiveway.Inthecaseofthenewsurgicalteamleader,DrOdim,theCentrereliedalmostexclusivelyonhiscurriculumvitaeandbriefandinformalinterviews.NooneattheCentreactuallysawhimperformasurgicalprocedureorspokewithanyoneathispreviousplaceofemployment(andwherehehadmostrecentlytrained).TheassessmentofDrOdim’soperatingroomskillsappearstohavebeenmadelargelyonthebasisofwhathetoldthem,wherehehadtrained,whathiscurriculumvitaestated,andcommentsfrompeoplewhohadnotobservedhiminsurgeryorhadhadnoinvolvementwithhimforthreeyearsormore.NoconsiderationwasgiventoassessinghisabilitytodevelopandworkwithasurgicalteamlikethatattheCentre.
TheInquestReportemphasisedtheimportanceofsurgicalability.“Itseemslogicaltothinkthatwhenhiringasurgeon,oneofthemostimportantareastoinvestigateisthatoftheindividual’ssurgicalskillsandability.Onecanproperlyassumethatanytrainedsurgeonhasbeencertifiedasbeingcapableofperformingthesurgicalproceduresassociatedwiththefieldofspecialtyforwhichheorsheisbeinghired.However,suchcertificationdoesnotprovideinformationonthelevelofskillandabilitythatthepersonbringstotheposition.Thatcanbestbedeterminedbyobservingthecandidatewhileheorsheactuallyperformssurgeryandbyinterviewingthosewhohaverecentlyobservedthecandidateinsurgeryandhavethecapabilitiesthemselvestomakejudgementsaboutthelevelofskillofthecandidate.ThoseattheCentreresponsibleforrecruiting Dr Odim did none of those things.”

�30 Patient Safety: a comparative analysis of eight Inquiries in six countries
Itwasfurtherpointedoutthat,hadtheCentreconsultedwiththesurgeonwhohadsupervisedDrOdimduringhismostrecentmedicaltraining,theywouldhavelearnedfromhimthatDrOdimwasnotreadyforthepositionheundertookattheCentre.TheInquestteambelievedthisshouldhaveledtoreconsiderationofhissuitability.Atleast,theCentrewouldhavebeenable“…toputintoplacemeasurestomonitorandassistOdim,aswellasensurethathislackofexperienceandneedfor assistance in some technical areas did not compromise patient care.”
Unclearlinesofauthority
The Inquest established that the ultimate responsibility for paediatric cardiac surgery at the Centre wasjointlyheldbytheheadsoftheDepartmentsofSurgeryandPaediatrics.Theresponsibilityofthetwodepartmentalheadswasinfactdemonstratedwhenitwasnecessarytoobtaintheirjointagreement to a reduction in services in May �994 and a suspension of the services in December 2004.
However,thelinesofauthorityandconsequentlytheresponsibilitywereunclearandconfusingtovirtuallyallCentrestaffduring1994.TheconfusionwasinpartduetothefactthatthePaediatricCardiacSurgeryProgramwasmultidisciplinaryinthatitrequiredcliniciansfromavarietyofdepartments(nursing,perfusion,surgery,cardiology,anaesthesia,paediatrics,intensivecare,neonatologyandpathology)toworktogether.Thusthereweremanyopportunitiestoclaimsomeoneelsewasincharge.Moreover,thedistinctionwasunclearbetweenresponsibilityforservicesandresponsibilityfortheworkofspecificclinicians.Thiswasthecasewithregardtodeterminingwhowasresponsibleformonitoringtheperformanceofthesurgeon.
Theproblemswereexacerbatedbyprevious(andlargelyad hoc) arrangements regarding supervision.Forexample,themedicaldirectoroftheCentrehadprovideddaytodaymanagementandmonitoringofthesurgicalaspectsoftheProgram.ThiswasdespitethefactthatthesurgeonwasformallyresponsibletothesectionheadofCardiovascularThoracicSurgery.Inaddition,manyCentre staff believed that the head of Paediatric Surgery had some responsibility for monitoring thePaediatricCardiacSurgeryProgrambyvirtueofhistitle.Hedid,infact,haveverylittlesuchauthority.Theconfusionwascompoundedwiththerecruitmentofnewstaffwhowereseldomtoldpreciselyabouttheirresponsibilities.Onenewmemberofstaffwasassumedtohavetakenovertheresponsibilitiesformonitoringsurgicaloutcomesofhispredecessorbutwasinfactneveraskedtodo this.
TheInquestrecommendedthatanyfutureprogrammusthaveclearwrittenlinesofauthorityandresponsibility. Efforts must be made to ensure that program members understand these lines of authority. This is of particular importance in a multidisciplinary program.
Individuals’responsibilities
Twoofthedoctors–theheadofthesurgicalteam(DrOdim)andtheactingmedicaldirector(DrGiddins)wereconcludedtohavefailedintheirdutieswithregardtomonitoringandrespondingsuitably to the poor surgical results in the Program.
Inaddition,DrOdimfailedtobehonestabouthisexperience,attemptedproceduresthatwerenotsupportedbytheevidence,andfailedtolistentoandtakenoteofadvicefromothermembersofthesurgical team. Dr Giddins not only referred patients to Dr Odim but also reassured parents of those patientsthatDrOdimwascapableofperforminganyandalloftheproceduresrequiredforhispatients.Thereforehehadaresponsibilitytoensurethattheassuranceshewasgivingwerejustified.

�3�
Misusingtheconceptofthe‘learningcurve’
Theevidencesuggeststhatpoorperformancewasrecognisedandthenjustifiedonthegroundsthatallsurgeonsmustgothroughalearningprocess.NoactionwasconsiderednecessarybecauseDrOdimwasonalearningcurvethatwouldensurebetterperformanceinfuture.
TheInquestconcededthattherearelearningcurvesinsurgery.However,thisshouldhavebeen recognised by providing additional supervision at the start rather than used as an excuse forpoorcareoroptimismunfoundedinperformancemonitoring.TheInquestwasparticularlycritical of the tendency on the part of some staff of the Centre to justify inaction on the grounds that there had been ‘similar results’ at the start of Dr Odim’s predecessor: that there had been a sharp learning curve before and therefore it could be expected again.
TheInqueststressedtheneedtotakethreestepsbeforethestartupoftheProgramin1994.First,aneffortshouldhavebeenmadetoensureanexperiencedpersonwasinapositionofauthorityintheProgramtoprovideguidance.Second,thoseinchargeoftheProgramoughttohavebeencarefultoensurethatthenewsurgeonandtherestartedProgramwerecloselymonitoredatleastthroughoutthefirstyear.Third,initialpatientselectionoughttohavebeenrestrictedtothosecasesthatpromisedthebestresultswhileindividualandteamexperiencewasgained.
Theevidencesuggeststhatthesestepswerenottaken.Itwasclearthat“…thoseinchargeoftheProgramactedonthebasisthatpoorsurgicalresultswouldsimplyimproveovertime.Thatwassimplynotappropriate.”
Managementandsupervision
TheheadsoftheDepartmentsofPaediatricsandSurgeryfailedtomanagestaffingmattersadequately. They did not address the underlying issues that led to the departure of previous staff,butrathersimplyreplacedthemwithlessexperiencedstaff.ThiswasinspiteofthefactthatthedepartingstaffhadrepeatedlycomplainedofalackofsupportfromtheCentre,andtheconsequentinadequatestandardsoftheworkbeingundertaken.
ItwasacceptedthatthedepartmentalheadsmighthavedistractedtosomeextentbybudgetaryandadministrativechangesundertakenattheCentreduring1993-1994.However,ifthisweretrueitshouldhavebeenrecognised,andthedepartmentalheadsshouldconsequentlyhaveconsidered delaying the Program’s restart.
Thedepartmentalheadswerealsojudgedtohavefailedtoensuretherewasaproperorientationforthenewstaff.Nordidtheyensuretherewaseitherformalorinformalmentoringofnewstaff.“Inthecaseofayoungsurgeoninhisfirstappointmentfollowinghisresidency,morecarefulconsiderationoughttohavebeengiventothefactthathewasfacinganentirelydifferentexperiencefromwhathehadfacedasasurgicalresident.”
InadequateattentionwaspaidtobuildingandmentoringthePaediatricCardiacSurgeryteamasawhole.Withoutleadership,theproblemsthataroseintheearlyoperationsrapidlyledtounresolved–andintheendunresolvable–conflicts.TheoperatingroomandICUstaffwerenotproperlypreparedforDrOdim’sparticularapproachtosurgeryandpost-operativecare,whileDrOdim often made assumptions based on his limited experience at other institutions. This led to increased friction and mistrust.

�32 Patient Safety: a comparative analysis of eight Inquiries in six countries
ThelackofsupervisionmeantthattheProgramwascharacterisedbypoorcaseselectionin1994.TheProgramundertookcasesthatwerebeyondtheskillandexperienceofthesurgeonandtheteam.
Poorteamwork
TheInquestconcludedthatpoorteamworkwasafeatureofmuchoftheCentre’soperations.Thetwodoctorsmostinvolved,DrOdimandDrGiddins,werebothresponsibleforaportionofthepoorteamwork.Thereportsaidthatthey“…didnottakeappropriatestepstoestablishandmaintainopenandongoinglinesofcommunicationwithotherrelatedmedicalservicesinthehospital,suchas nursing and anaesthesia.”
DrOdimwasparticularlyatfault.Heusedtechniquesandapproacheswithwhichotherteammemberswerenotfamiliarandforwhichthesurgeondidnotpreparethem.Heerroneouslyassumedthateveryoneknewwhathewastalkingabout.Insomecases,therewasalackofconsultationandbriefingbeforetheteamundertookcomplicatedprocedures.OneexamplewasNorwoodprocedures,whereDrOdimfailedtogivesufficientadvicetotheneonatalintensivecareunit.
Amongtheirrecommendations,theInquestteamemphasisedtheneedforprotocolstobedevelopedthatinvolvedallinvolvedclinicians.Theyshouldspecificallyaddresstheneedsofnewortemporarystaff.Thepurposesshouldbebothprovisionofinformation,andbuildingthetrustandtheopencommunicationonwhichallteamsdepend.
Inanaddendum,theReportprovidesmoredetailsaboutteambuildingprocesses.Inthespecificcontextofsurgery,adescriptionisprovidedofprocessesthatmustincludeallplayers.Thereshouldbepre-operativebriefingsessionsthatfocusontheplanfortheoperation,anddiscussionofcontingencies.
Thereshouldbemoreuseofstandardoperatingprocedures,thedevelopmentofleadershipskills,theprovisionforteamdevelopmentandmaintenanceprocessesthatemphasiseteamcommunication,clarityinthedecisionmakingprocess,aprocessofconflictresolution,post-operativedebriefingsessionsforalloperationsregardlessofoutcomes,andastressmanagementcomponent.
Emphasis is given to training that focuses on the development of behavioural strategies to manageerror.Itshouldbespecificallydesignedtodecreaseorreducetheprobabilityoferrorsoccurring,correcterrorsbeforetheyhaveanimpact,andcontainordecreasetheseverityoftheconsequences of those errors that have been made.
Teamsshouldlearntoaddressdaytodayissues,andparticularlythoserelatingtocommunicationanddecisionmakingthatarisebetweendifferentmembersoftheteam(suchasbetweendoctorandnurse or surgeon and anaesthetist). There should be training in crisis management that includes the useofsimulationsofcriticalincidents,inordertoprovideparticipantswithpredeterminedresponses.
Itisnoted,however,thathealthworkersnotonlyneedtolearnhowtoworktogetherduringcrises.Itismoreimportanttoworkasateamundernormalcircumstances,whennothinggoeswrong.Teamsthatnormallyworkwelltogetherwillprobablymakefewererrorsandencounterfewerproblems.Whenseriousproblemsarise,theteamwillhavealreadydealtwithanyinterpersonalandorganisationaldifficulties.
Trainingtomanageerrormustbeincludedintheearliesttrainingofdoctors,nursesandotherhealthcareworkers.Ifthisisnotthecase,itwillcontinuetobedifficulttomovefromdoctor-dominatedtoteam-basedcare.Tobeeffective,thevalueofqualityassurance,riskmanagementandteam

�33
performance must become embedded in the culture of each health care organisation. This willrequireactivepromotionbyseniorstaffresponsiblefortrainingandevaluation,andtheythemselveswillconsequentlyneedadditionaltraining.Nomatterhowtrainingisdelivered,itmust be an ongoing process: repetition and reinforcement are vital if the desired outcomes are tobeachieved.Theremustbecontinuingprograms,bothformalandinformal.
Finally,theInqueststressedthatteamworkisthekeytoimprovement,andthatthefocusmustbe on changing the culture of health care organisations. It is particularly important that medical professionalsdealinmoreappropriatewayswithpatientsandtheirfamilies,andthatdoctorsandlaymanagers“…shouldceasetotreatnursesasunder-trainedsubordinateswhoseconcerns can be readily dismissed as emotional responses to tragic outcomes.”
Inappropriatestaffinglevels
ItwasnotedthatallsmallsurgicalunitslikethatattheCentrearelikelytohaveproblemsofstaffingfromtimetotime.Thisisyetanotherreasonforavoidinglowvolumeprocedureswheretherearesignificantcomplexities.Abalancehastobestruckbetweenexcessiveworkloads,andensuringeachteammemberisinvolvedinasufficientnumberofcasestomaintainanappropriateskilllevel.Stepsshouldthereforehavebeentakentolimitthenumberofpatientsand select the mix more carefully.
The departmental heads responsible for the Program failed fully to recognise the implications ofonlyonecardiologistbeingattheCentreformostof1994.Anothererrorwascreatingthesituationwheretherewasonlyonesurgeonwhowasonconstantcall.StaffshortagesintheDepartmentofPathologyalsocontributedtothefactthatautopsyreportswerenotcompletedina timely manner.
TheevidencesuggestedthatanappropriatebalancehadnotbeenstruckbetweenthenumberofanaesthetistsprovidinganaestheticcaretotheProgramandthenumberofcasesinwhicheachanaesthetistparticipated.Putanotherway,toomanydifferentanaesthetistswereinvolvedgiventhelowtotalvolume.Theneedtohaveenoughcasestodevelopandmaintainskilllevelsis the same for an anaesthetist as for a surgeon. The Inquest recommended several obvious stepsthatneededtobetakeninfuturetoensureanadequatelevelandmixofstaffatalltimes.
Poortreatmentofnurses
Itwasconcludedthat,becausenursingoccupiedasubservientpositionwithintheCentre,issuesraisedbynurseswerenotalwaystreatedappropriately.Throughout1994,theexperiencesand observations of the nursing staff involved in the Program led them to voice serious and legitimateconcerns.Theymadebothinformalcomplaints,and“…madeproperandappropriateuseofexistingchannelstovoicetheirconcerns.”Foravarietyofreasons,theirconcernswerenotaddressed.Indeed,thereceptiontheyweregivenledsomenursestosilencethemselves.Italsoleftthemfrustratedanddistraught,andmanypaidaheavyemotionalprice.BythetimetheProgramended,atleastonenursewasonthevergeoftakingherconcernsoutsidetheCentre,atgreatrisktoherpositionandcareer.
Thenurseswerenevertreatedasfullandequalmembersofthesurgicalprogram,despitethefactthatthiswasthestatedintentoftheadministrativechangesthattheProgramunderwentinJune1994.Intensivecareunitnurses,forexample,wereneverproperlyinvolvedinthereviewteamthatassessedtheProgramduring1994,andnursesingeneralwerenotproperlyinvolvedintheexternalreviewthatprecededtheInquest.

�34 Patient Safety: a comparative analysis of eight Inquiries in six countries
OneofthestatedgoalsoftheCentre’sreorganisationin1994wastostrengthenthenurses’roles.However,itimplicitlydevaluednurses:thereorganisationwasactuallydrivenbyaconcerntocutcostsprimarilybyreducingstaff,andthemajorityofthereductionswereinnursing.
Theconcernsexpressedbysomeofthecardiacsurgicalnursesweredismissedonthegroundsthattheyreflected“…aninabilitytodealemotionallywiththedeathsofsomeofthepatients.”Furthermore,anyconcernsovermedicalissuesthatthenursesexpressedwererejectedonthegroundsthattheydidnothave“…anyproperbasis,clearlystemmingfromtheviewthatthenursesdidnothavethepropertrainingandexperiencetoholdorexpresssuchaview.”
Inaddition,whiletheCentre’sdoctorshadarepresentativeontheCentre’sBoardofDirectors,nursesdidnot.Thisreflectedtheimplicationthatthenurses“…lackedavisionofthelargerpicture”.
Wenoteinpassingthatthisisinconsistentwithmostoftheavailableevidence.Itsuggestsnursestendtohavemuchbroaderviewsofthepatientinrelationtofamilyandcommunity,andagreaterappreciationoftheneedtoseeboththeclinicalandthefinancialdimensionsofcare.
The Inquest Report argued that the role of nurses has traditionally been subordinate to that of doctors.“Whiletheyarenolongerexplicitlytoldtobesilent,itisclearthatlegitimatewarningsandconcernsraisedbynurseswerenotalwaystreatedwiththesamerespectorseriousnessasthoseraisedbydoctors.”Theattemptedsilencingofmembersofthenursingprofession,andfailuretoaccepttheirlegitimateconcerns,meantthatseriousproblemswerenotrecognisedoraddressedina timely manner.
TheInquestmadeseveralrecommendations.First,itwasnecessarytoputinplacestructuresthatensurethatstaffcanmaketheirconcernsknownwithoutfearofreprisal.Thisappliedparticularlytonursing.
Second,thestructureoftheCentreshouldbeadjustedtoensurethatthepositionofnursingdidnot continue to be a subservient one. The Nursing Council of the Centre should contain members selected by the nurses themselves. It should have representation on the Centre’s governing body andberesponsibleformonitoring,evaluating,andmakingrecommendationspertainingtothenursingcare.Itshouldalsoserveasavehiclethroughwhichnursescouldreportincidents,issues,andconcernswithoutriskofprofessionalreprisal.
Third,theCentreshouldestablishaclearpolicyonhowstaffshouldreportconcernsaboutrisksforpatients.Thispolicymustensurethatthereisnorisktothepersonwhoismakingthereport.Itshouldbecleartoeverystaffmembertowhomtheyaretopresentsuchreports.TheProvinceofManitobashouldconsiderpassingwhistleblowinglegislationtoprotectnursesandotherprofessionals from reprisals stemming from their disclosure of information arising from a legitimately and reasonably held concern over the medical treatment of patients.
Poortreatmentofthefamilies
Themostimportantproblemforparentswasthattheirchildrenweregivenpoorcareasnotedabove.However,theInquestnotedotheraspectsinwhichtheyweretreatedpoorly.
Inparticular,therewereweaknessesintheprocessofinformedconsent.Parentswerenotasfullyinformedastheywereentitledtobewhenaskedtogiveconsenttosurgeryontheirchildren.Mostwitnessesacceptedthatpatientsandfamilymembersgrantingconsentonbehalfofapatientareentitledtoknowtherisksbeforetheygivetheirconsenttosurgery.However,therewascleardisagreement over the methods and content of information to be shared.

�35
Severalmedicalwitnessesarguedthatdeclaringone’smedicalexperienceisnotarequirementforinformedconsent.Ontheotherhand,mostparentsfeltstronglythattheyshouldhavebeenprovidedwithmoreinformationabouttheProgramandaboutthesurgeon’sexperience.
ManyCentrestaffseemedtobelieveitwassufficienttodescribethesurgeonashighlytrained,or‘oneofthebest’,andtostatethattheCentre’sprogramwas‘ascapableasanywhereelse’.TheyarguedthatitwouldhavebeeninappropriatetotellthefamiliesthatDrOdimhadnotperformedanyoftheproceduresheproposedin1994withoutsupervision.TheInquestsaidtheywereconcernedastothelogicofdoingtheformerwhilenotfeelingobligatedtodothelatter.
Somewitnessesfeltthatthepatientorparentisowedthetruthifaquestionaboutpreviousexperienceisasked,butthatadoctorcanremainsilentonthesamepointifthepatientorparentdoesnotask.TheInquestarguedthat,whiletheobligationtotellthetruthisobvious,itseemsillogicalthatsomewouldseetheobligationtobetruthfulasnotencompassinganobligationtodisclosearelevantfact.Whileitmightnotbenecessarytodiscloseasurgeon’sabundantexperienceatperformingaparticularprocedure,asurgeon’slackofexperienceisclearlyafactthatisrelevanttothequestionofwhetherornotsomeonewouldbewillingtoentrusthislife,orthelifeofhisorherchild,tothatsurgeon.Forthatreasonalone,suchinformationoughttohavebeendisclosedwithoutprompting.
Arelatedconcernwasthatinformationprovidedaboutsurgicalriskwasmisleading.TheriskfactorsthatwerecitedtoparentsfortheproceduresundertakenbyDrOdimin1994werenotbasedontherealityoftheCentre’ssituationatthetime.Inmanycasestheindicationsthatweregiventotheparentswerereflectiveofprofessionwiderisk,ratherthanthelevelofriskfortheprocedure at the Centre.
Informationsuchastherelativeinexperienceofthesurgeon,andthefactthathewouldbeperformingtheprocedureinanunsupervisedsettingforthefirsttimeinhiscareer,wasnotfactoredintotheriskassessmentsharedwiththefamilies.Thisinformationshouldhavebeenincludedwhendeterminingwhattosaytoparentsregardingtherisklevelassociatedwiththeoperationontheirchild.TheInquestReportarguedthatalltheavailabledataclearlysuggestedariskfactorattachedtoasurgeon’sexperience.Thefactthatitisclearlyhigherwithinexperienceoughttohavebeendisclosedtotheparents,alongwithanindicationastowhatwasapplicablewithDrOdim.Thestateofexperienceandleveloffunctioningofthesurgicalteamshouldalsohavebeentakenintoaccount.
Furthermore,allparentswhosechildrenunderwentoperationsafter17May1994shouldhavebeeninformedabouttheanaesthetists’withdrawalofserviceonthatdate.Parentswereentitledtobeinformedofthedecisiontoperformonlylowriskproceduresthereafter.Theyshouldalsohavebeenmadeawareoftheexternalreviewandallowedtoreaditsreport.TheyshouldhavebeencontactedandinformedofthedecisiontosuspendthePrograminFebruary1995,beforethatdecisionwasmadepublic.
The Inquest recommended that the Department of Health of Manitoba should prepare and distributewidelyapatients’rightshandbookthatincludesdetailedadviceoninformedconsent.Thehandbookshouldclearlyindicatepatients’rightsincludingthoseofbeingfullyinformedbeforegivingconsenttomedicaltreatment,ofasurgeon’sexperienceinperformingaparticularprocedure(andtheexperienceoftheCentreandthesurgicalteam),asecondopinion,andoutof province referral in certain circumstances.

�36 Patient Safety: a comparative analysis of eight Inquiries in six countries
TheCentrewasfurtheradvisedtoreviewallitspoliciesoncommunicationwithfamilies.Thereshould be a requirement for medical staff to be forthright and truthful in disclosing all relevant information to the patient or representative before the procedure in question.
Inadequatesupportforthefamilies’legalcosts
The families involved in the Inquest experienced serious problems in meeting the costs associated withhavinglegalcounsel.Allfamilieshadgoodreasonstoparticipateintheproceedingsbutitslengthmeantthatthelesswealthycouldnotaffordtodoso.
TheInquestteamarguedthatthefamilieswereentitledtohavealltheirlegalcostspaid.Intheevent,somefamiliesobtainedreimbursementfromthegovernment.However,itwasunfairforfamiliestohavetotakestepstopersuadethegovernmenttoprovidethemwithfinancialassistanceforlegalcostsonacasebycasebasis.Familiesthatwerebestabletodevelopandmarshalprivateorpublicsupportstoodinapotentiallymorefavourablepositionthandidthosewhosepoliticalcontactsorinfluencewereless.TheReportconsequentlyrecommendedthatthegovernmentshouldestablisha policy for the routine payment for counsel for families granted standing at inquests.
MonitoringwithintheCentre
TheformalandinformalmonitoringofissuesattheCentrefailedtoidentifytheproblemswiththePaediatricCardiacSurgeryPrograminatimelyfashion.Asnotedelsewhere,theresponsibledepartmentalheads,thecardiologistandthesurgeondidnotadequatelymonitorsurgicalperformance either on a case by case or collective basis. Nor did these doctors appreciate the significanceofthepoorlevelofcommunicationandthepoorinterpersonalrelationshipsbetweenthesurgeonandothers.Thedepartmentalheadswerealsoslowtorespondeffectivelytoconcernsthatwereraisedbyprogramstaff.
Likemanyothermanagers,theyignoredpertinentinformationthatwasbroughttotheirattentionand,atbest,simplytoleratedthebearersofbadnews.Theresponsibilityfordealingwiththisinformationwasneverclearlydelineated.
Therewasnotrackingofcommonindicatorsthatmightpointtomattersofconcern,suchasthedurationofcardiopulmonarybypasstimes,thedurationoftotalcirculatoryarresttimes,thevolumeofbloodloss,thenumberofunitsofbloodandbloodcomponentstransfused.TherewerenoplanstodevelopsuchadatabaseatthetimethattheProgramwassuspended.NorwasthereanyattempttocollectdatafromtheProgramandcomparetheresultsoftheCentre’sprogramwithanyothers,asonebasisforevaluationoftheProgram’sperformance.
Therewasnodebriefingsettinginwhichmembersofthesurgicalteamcoulddebateanddiscusspre-operativeissues,intra-operativecare(includingsurgicalproceduresandpost-operativecare)andoutcomes.Routineroundswerementionedasapossiblesettingforsuchdiscussions,buttheywereclearlyintendedasteachingandlearningopportunitiesforstaffintheCentregenerallyandwereopentoindividualsnotinvolvedinthecase,suchasmedicalstudents.Theroundswerenotintendedasaforumforafullandfrankdiscussionofthedetailsofeachprocedure.Inthemedicalcultureofthetime,theroundsdidnotprovideanappropriateforumfordiscussionofrelatedconcerns,suchascommunicationbetweenvariousclinicalprofessions.
ThemedicalcultureoftheCentrereflectedtheconceptofthesurgeonasthesupremeandinfalliblecaptainoftheship.Thismeantthatwhatshouldhavebeenthecollectiveconcernabouttheteam’sabilitytohandlecertaincasesturnedintohighlychargedconflictscentringonthesurgeon.Onceframedinthatmanner,itbecamedifficulttohaveopendiscussionsorsuccessfullyresolvetheissues.

�37
Despiteformalpolicies,theuseofincidentreportswasnotanengrainedelementoftheCentre’sculture.Centrestaffobservedmanyseriousandalarmingeventsin1994.Indeed,manystaffmembersbegankeepingprivateaccountsoftheseevents.However,onlyoneincidentreportwasfiledforthecasesunderreviewduringtheentireyear.
Problemsandcomplicationsduringoperationswereoftennotcharted,recordedorreportedtotheStandardsCommittee.TheCommitteestructurewassimplynotcapableofaddressingandevaluatingimportantquestionsinatimelyfashion.Theprocessdidnot,inmostinstances,begintoreviewadeathuntilanautopsyhadbeencompleted.
Finally,DrOdim’smembershiponthepanelofsurgeonsthatreviewedeachsurgicaldeathfortheCentrehadthepotentialforaseriousconflictofinterest.Thiswasyetanothermanifestationofa‘clubculture’wheremembersshouldneverbequestionedandnonmembershadnostanding at all.
MonitoringoutsidetheCentre
InManitoba,theOfficeoftheChiefMedicalExaminer(CME)hasaprimaryresponsibilityforinvestigationofpatientharm.ItfailedtoidentifytheproblemswiththeProgram,mainlybecauseof over reliance on information provided by the surgeon alone.
Inmostcases,theCMEinvestigationteamwaitedforthefinalautopsyreport–whichwasnotavailabletotheCMEinatimelymanner.Itdidnottracksurgicaldeathsbyprogram,andconsequentlywasunabletoidentifytrendsintheProgram.
Moreover,manyrelevantmatterswerenevercommunicatedtotheCME–suchastheanaesthetists’withdrawalofservice.Inmostcases,theCMEsimplyreadthemedicalrecordsandspokewiththesurgeonconcerned.Evenacursorydiscussionwiththenursesandtheanaesthetistswouldhaverevealedsignificantunderlyingconcerns.
Intheautopsies,overreliancewasplacedontheinformationthatwasobtainedfromthesurgeon.TheInquestReportarguedthat,sinceinformationastowhathappenedduringsurgeryisvitaltotheconclusionstobedrawnbythepathologist,agreaterattemptmustbemadetogather such information from as many of the people involved in the proceeding as possible. To relyexclusivelyontheonepartywhomightbemostresponsibleforthefataloutcomeseemedunwise.ItwasalsoinappropriatetohavetheautopsiesinCMEcasesinvolvingsurgicaldeathsperformedbythestaffoftheCentreinwhichtheoperationtookplace.ThebetterpracticewouldbetohaveautopsiesinCMEcasesperformedbyapathologistnotaffiliatedwiththeCentreinordertoovercomeanyappearanceofapotentialconflictofinterest.
The Inquest Report recommended many changes in the methods of operation of the CME Office.Theyincludeddevelopmentofaprotocolrequiringhospitalstoinformitofsignificantchangesinthedeliveryofmedicalservices,maintenanceofadatabaseofhospitaldeathstotrackinhospitaldeathsandcausesofdeathonaweeklyandmonthlybasis,andtheconductofinterviewsofnursingandmedicalstaffinvolvedinthepatient’scare.
9.3 RecommendationsoftheInquiry
Overall,theInquestmade36recommendationspertainingtokeyareasoftheCentre’soperations. The recommendations relate to: the loss and recruitment of staff; unclear lines ofauthority;themisuseoftheconceptofa’learningcurve’;inappropriatestaffinglevels;thetreatment of nurses and of families; monitoring of issues and problems; human and medical error; and the future of Pediatric Cardiac Surgery in Manitoba.

�38 Patient Safety: a comparative analysis of eight Inquiries in six countries
MostoftheInquest’srecommendationswereaddressed,insitu,intheprevioussections.Theissueofhowhealthservicescanrespondtohumanandmedicalerroristakenupinthediscussionsectionbelow.
9.4 Discussion
Thisfinalinquiryreflectsmanyofthesameconcerns,andindeedthesamepatientgroup,asthefirstinquiry,Bristol,reviewedinthismongraph.Thesimilaritydoesnotendwiththetypeofoperation,ortheriskfactorsinvolved.InbothManitobaandBristol(andmanyoftheotherinquiriesconsidered)thelengthoftimeduringwhichconcernswereraisedwithinthehospital,thecombinationofinternalandexternalformalandinformalreviews,alongwiththeoutsidepressureoffamiliesandtheroleofthemediainpushingforaformalinquiry,allformafamiliarpattern.
IndiscussingtheManitobaInquiry,wewouldliketoconsiderindetailtheimplicationsofthesectionoftheInquestReportwhichcontainsadetailedreviewofthemanagementoferrors.Reflectiononthecauseandmanagementoferrorsisafundamentalthreadinalltheinquiriesreviewed.ThesectionintheManitobareportappearsasaconsequenceofthegeneralrulesoninquests.Judgesarerequiredtoassessresponsibilitybutarenotallowedtomakefinaldecisionsonculpability.Theyhavenochoicebuttodetermineifchangesareneededinthewaythatinstitutionsandorganisationsgoabouttheiractivities,soastopreventsuchdeathsfromrecurring.
MuchofthetextoftheReportisadaptedfromstandardsourcesoferrormanagement,andthereforeonlyabriefsummaryisneededhere.Firstlyitisnoted,thehealthcaresystem,likemanyothersystems,isdrivenlargelybyhumans,andhumansmakeerrorsofmanykinds:inthedesignand construction of a system; the design and construction of technologies used in the system; the maintenance of technologies; planning and execution; and so on.
Errorisahumanreality.Itisappropriatetostrivetoreducethefrequencyatwhicherrorsaremade,butunrealistictobelievetheycanbeeliminated.Itisimpossibletodesignasystemthatiserrorfree,andunwisetoassumeeveryonewillfollowtherules.
Itisthereforenecessarytomanageerrorfromthestart,andthiscaninvolvetwomaintypesofapproaches.First,wecanseektoidentifythepersonwhocommittedtheerrorinordertoholdhimorherresponsible(toassignblame).Theotherwayisanalysetheerrorinordertolearnfromitandtoimprovethingssoastoreducetheprobabilitythattheerrorwillnotbemadeagain.
Blamingpeoplefortheiractions,suchasthosetypesoferrorthatinvolveviolationsofexistingstandardsorrules,isamajorfocusofthecourtsystem.Legalblamingisanormalandnecessarywayofaddressingerrorsthatviolaterulesorstandards.However,becauseinquestsarenotabletomakefindingsofculpability,theobligationofaninquestoughtthereforetobetofocusondiscussingerrorinthecontextofwhatcanbelearnedfromit.Forthesamereason,hospitalsneedtoapproachthe issue of error from a learning perspective.
Therefore a process must be put into place that emphasises the need to gather and consider all of therelevantfactsinanhonestandcandidmanner,withoutregardtoanyindividualorinstitutionalconsequencesthatmightflowfromtheerrors.Forthattohappen,considerationmustobviouslybegiventobalancingtheissueofconfidentialityandprotectionofinformantsfromliabilityfordescribingwhathappened,withtheequallystrongneedforpatientsandtheirfamiliestobeinformedastowhatreallyhappened.

�39
Unfortunately,theidentificationoferrorsisoftendifficultincomplicatedsystemslikehealthcare.TheInquestReportsaysthaterrorfinding“…isoftenhinderedbyforcesthatexistwithinthemedicalcommunity.Theseforcesseektominimisetheappearanceoferrorswhentheyoccur.This may arise from the fact that the current culture of medicine reinforces the belief that medical personnelmustperformwithouterror.Alltoooften,themakingofanerrorinmedicineisequatedwithamoralfailingorisregardedasasignofignoranceorincompetence.Toadmittoerror,ortoimplythatacolleague’sactionswereinerror,istoraiseseriousquestionsaboutsomeone’scompetence,andhencelegitimacyandauthoritywithinthehealth-caresystem.Oneoftheaimsof this Report is to contribute to increasing openness about the existence of human error in the medical community.”
Errors are unplanned events that could or do lead to negative consequences. Humans commit errors,notbecauseofanymoralfailing,butbecausehumansareflawedbeings,workinginflawedsystemsthattogethercontributetothecommissionoferrors.Thereisahierarchyoferrors:thosethatgiverisetosimpleincidents;thosethatevolveintomoreseriouseventswiththe potential for harm to a patient (critical incidents); and those that evolve into events that cause actualharm(adverseoutcomesinthewordsoftheReport,andinpatientsafetyparlance).
Itisessentialtohaveanerrormanagementprocessthatidentifiesallthreetypesoferrors.However,simpleandcriticalincidentsareinfactseldommanaged.Thismightbebecausetheydidnotproducenegativeresults.However,theyareimportantbecausetheyareevidenceofthepotentialforharm.TheInquestconcludedthattherewerenoprocessesinplacethattookaccountofthemanysimpleandcriticalerrorsthat,ifnotedandaddressed,wouldhavereducedtheactualharm.Therewasnoearlywarningsystem.
Afundamentalreasonforabsenceofsuchasystemwasbecausetherewasareluctancetodiscusserrorsinasettingwhereeveryonemightcontributeinanopenway.TheReportsaystherewasnoprocess“…thatallowedteammemberstocomfortablyandcollectivelyassessand evaluate the events that occurred in the operating room in a manner that contributed to improvementsinthewaythatthepatientsweretreated.”Everyhospitalneedstoensurethereisaprocesswherebymembersofsurgicalteamsandprogramscanlearnfromthemistakesthattheywillinevitablymake.
TheInquestproposedelementsofsuchaprocess,withparticularreferencetohumanfactorsanalysisasitoriginatedintheaviationindustry.“Studiesofairdisasterssuggestedthatthemajorityofaccidentsdidnotresultfromtechnologicalfaultsoralackoftechnicalskills.Instead,thestudiessuggestedthatinadditiontoanunderlyingflawedsystem,thecontributingfactorsortriggersforthedisasterlaywithintheareatermedhumanfactors.Thisisthescientificdisciplineconcernedwithinteractionsamonghumansandotherpartsofasystemincarryingoutapurposefulactivity.Humanfactorsincludeleadership,teamwork,communicationanddecisionmaking.”Itisequallyrelevanttohealthcare.“Leadership,teamwork,communicationanddecisionmakingarerecurringthemesinthisReport.Theyarenotsideissues,notmattersofmerepersonalitydifference,butcentralissues.Wheretheseissueswerenotresolved,theyoften led to tragic results.”
Humanfactoranalystssuggestthattheerrors,incidents,criticalincidentsandaccidentsthatarise from human behaviour can best be addressed in a systematic fashion through programs ofqualityassuranceanderrorandriskmanagement.Theseprogramsneedtoaddressthebehaviourofpeoplewhomightappeartoperformatlessthananoptimallevel.Moreimportantly,theprogramsmustaddresswhataretermed‘systemicissues’–thatis,problemsthatliewithinthewholeofthehospitaloreventhehealthcaresystemitself.

�40 Patient Safety: a comparative analysis of eight Inquiries in six countries
9.5 Afootnote:implementationofrecommendations
AReviewandImplementationCommitteewasestablishedin2000bytheMinisterofHealth,Manitoba,toensurechangesrecommendedbytheInquestandotherreviewprocesseswereactuallyimplemented.ThefirstannualreportoftheCommitteemadethefollowingpoints.
First,theCommitteereiteratedakeyfeatureofthecontext:thatthehealthcaresystemishighlycomplicated.Althoughtherearelargenumbersofhighlyknowledgeableandcommittedhealthprofessionals,itisfarfromeasytomakesomekindsofchanges.
Second,themainimprovementshadbeenmadeinafewareas.Theyincludedanimprovedpolicyoninformedconsentthatcouldbecomeamodelforotherhospitals,theestablishmentofaNursingPracticeCouncilattheCentre,andtheestablishmentofanewcriticalincidentreportingpolicyattheCentre.Minorimprovementshadalsobeenmadewithregardtoaccountability,riskmanagement,qualityassuranceandthehandlingofpatientcomplaints.
Third,ideashadbeendevelopedbutimplementationhadnotyetbeguninseveralotherareas.TheyincludedcollaborationbetweenManitobaHealthandtheCollegeofPhysiciansandSurgeonstodevelopmethodsofprofilingofdoctors,developmentofapolicyframeworkforinternaldisclosurepoliciesasaguideforindividualhealthcarefacilities,anddevelopmentofaguidetohealthservicesin Manitoba for the general public.
Finally,theCommitteerecommendedadditionalactionsbetakeninotherareas.TheyincludedincreasingthepublicprofileoftheCollegeofPhysiciansandSurgeons(withemphasisonincreasingtheawarenessoftheCollege’scomplaintprocesses),acknowledging(formally,culturallyandoperationally)theroleandskillsofnurses,andchangingcultureswithinhealthcaresystems.TheCommitteesaidthatthemostimportantaspectsofculturewere“…tobemoreopenandacceptingofprocessesthatcatchmistakesearly,andindealingwithmistakesaslearningexperiences.”However,itnotedthat“…changesincultureandattitudestakeyears,notmonths,and are the responsibility of health care professionals and the general public.”
9.6 Referencesandselectedbibliography
Krever,H.(1997).Report of the Commission of Inquiry on the Blood System in Canada.Ottawa:Health Canada.
Manitoba Health (200�). Report of the Review and Implementation Committee for the Report of the Manitoba Pediatric Cardiac Surgery Inquest May 2001. Available at: http://www.gov.mb.ca/health/cardiacAccessedon3March,2006.
Manitoba Health (2002). Progress report for the period June 1, 2001 – June 1, 2002 of Recommendations from the Report of the Review and Implementation Committee for the Report of the Pediatric Cardiac Surgery Inquest. Available at: http://www.gov.mb.ca/health/documents/pediatric.pdfAccessedon3March,2006.
Sibbald,B.(1998).WhyDid12InfantsDie?Winnipeg’sEndlessInquestSeeksAnswers.Canadian Medial Association Journal,158:783-789.
Sinclair,C.M.(2000).The Report of the Manitoba Paediatric Cardiac Surgery Inquest: an Inquiry into Twelve Deaths at the Winnipeg Health Sciences Centre in 1994.Winnipeg:ProvincialCourtofManitoba. Available at: http://www.pediatriccardiacinquest.mb.ca/Accessedon3March,2006.

�4�
�0 Additional bibliography
Inthisfinalsection,weprovidealistofpertinentpapersonthreerelatedareastotheinquirieswehavecoveredhere.Theseare:culture,systemschangeandsystemsapproaches;generalpapersoninquiries;andinquiriesintopre-meditatedinjurytopatients.Copiesofthesearewidelyavailableintheliterature,andthose from staff of the Centre for Clinical Governance Research can be obtained by contacting us.
Culture,systemschangeandsystemsapproaches
Alvesson,M.(2002).Understanding Organizational Culture. London: Sage Publications.
Braithwaite,J.(2005).AxiomsforGoverningHealthSystems.British Medical Journal,330(7498):�032.
Braithwaite,J.(2005a).Hunter-GathererHumanNatureandHealthSystemSafety:anEvolutionaryCleftStick?International Journal for Quality in Health Care, 17(6): 541-45.
Braithwaite,J.(inpress).AnalysingStructuralandCulturalChangeinAcuteSettingsUsingaGiddens-WeickParadigmaticApproach.Health Care Analysis 2006.
Braithwaite,J.(inpress).AnEmpiricalAssessmentofSocialStructuresandCulturalChangeinClinical Directorates. Health Care Analysis 2006.
Braithwaite,J.andWestbrook,M.T.(2004).ASurveyofStaffAttitudesandComparativeManagerialandNon-ManagerialViewsinaClinicalDirectorate.Health Services Management Research, �7(3): �4�-66.
Braithwaite,J.andWestbrook,M.T.(2005).RethinkingClinicalOrganizationalStructures:AnAttitudeSurveyofDoctors,NursesandAlliedHealthStaffinClinicalDirectorates. Journal of Health Services Research and Policy, �0(�): �0-7.
Braithwaite,J.,Westbrook,M.T.,Iedema,R.,Mallock,N.A.,Forsyth,R.andZhang,K.(2005).ATaleofTwoHospitals:AssessingCulturalLandscapesandCompositions. Social Science and Medicine,60(5):1149–62.
Hindle,D.,Braithwaite,J.andIedema,R.(2004).Patient Safety Research: A Review of the Literature.Kensington:CentreforClinicalGovernanceResearch,UNSW.
IedemaR.,JormC.,LongD.,BraithwaiteJ.,TravagliaJ.,WestbrookM.(2006).Turningthemedicalgazeinuponitself:rootcauseanalysisandtheinvestigationofclinicalerror.Social Science & Medicine,62(7):1605-1615.
Iedema,R.,Flabouris,A.,Grant,S.,Jorm,C.(2006).NarrativizingErrorsofCare:CriticalIncident Reporting in Clinical Care. Social Science & Medicine, 62(�): �34-44.
Iedema,R.,Meyerkort,S.andWhite,L.(2005.)EmergentModesofWorkandCommunitiesofPractice. Health Services Management Research, �8(�): �3-24.
Iedema,R.,Rhodes,C.andScheeres,S.(2005).PresencingIdentity:OrganizationalChangeand Immaterial Labor. Journal of Organizational Change Management, �8(4): 3�7-37.
Iedema,R.,Rhodes,C.andScheeres,S.(inpress).Surveillance,Resistance,Observance:TheEthicsandAestheticsofIdentity(at)Work.Organization Studies.

�42 Patient Safety: a comparative analysis of eight Inquiries in six countries
Martin,J.(2002).Organizational Culture: Mapping the Terrain.ThousandOaks,CA:SagePublications.
Schein,E.H.(2003).Organizational Culture and Leadership. (3rdEd)SanFrancisco,CA:Jossey-Bass.
Generalpapersoninquiries
Runciman,W.B.andMerry,A.(2003).ATragicDeath:ATimetoBlameoraTimetoLearn?Quality and Safety in Health Care, �2(4): 32�–322.
Smith R. (2000). Inquiring into Inquiries. British Medical Journal, 32�(7263): 7�5-�6.
Walshe,K.andOffen,N.(2001).AveryPublicFailure:LessonsforQualityImprovementinHealthcareOrganisationsfromtheBristolRoyalInfirmary.Quality in Health Care,10(3):250–256.
Walshe,K.andHiggins,J.(2002).TheUseandImpactofInquiriesintheNHS.British Medical Journal, 325(7369): 895–900.
Inquiriesintopre-meditatedinjurytopatients
Department of Health (�994). The Allitt Inquiry: Independent Inquiry Relating to Deaths and Injuries on the Children’s Ward at Grantham and Kesteven General Hospital during the Period February to April 1991. London: HMSO.
Smith,J.(2005).Shipman: The Final Report (The Sixth Report).London:TheCrown.
�� Appendix �: Summary of inquiries
Whatfollowsaresummariesoftheeightinquiriesintopatientsafetywedealwithinthisreport.Eachtableprovidesasummaryofthecontextwithinwhichthepatientsafetyissuesemerged,thefindingsofeachInquiryteam and some of the most relevant recommendations.
Theselectionoftheseinquirieswaspragmatic:itwaspartlyonthebasisoftheirprominence,andpartlyontheaccessibilityoftheinquiryreports.Achoicewasalsomadetoincludeinquiriesintoarangeofservicetypesandcountries.Inquiriesintohealthprofessionalswhocauseddeliberateharm,suchthoseofShipmanandAllitt,wereexcluded.Whiletheycanteachusaboutsystemicflaws,theywereoutsidethescopeofthestudy.
11.1 BristolRoyalInfirmary,UnitedKingdom
TheInquiryintotheBristolRoyalInfirmaryandtheBristolRoyalHospitalforSickChildrenhasoneofthehighestprofilesofinquiriesintopatientsafety.Table3outlinesthecontext,findingsandrecommendationsofthecase,whichrelatestotheoutcomesofpaediatricheartsurgeryattheBristol. One of the most important systemic issues arising from the Bristol case is that concerns aboutthesafetyofthepatientswereraisedbybothstaffandpatientsforaperiodofalmosttenyearsbeforeacomprehensivereviewwasundertaken.
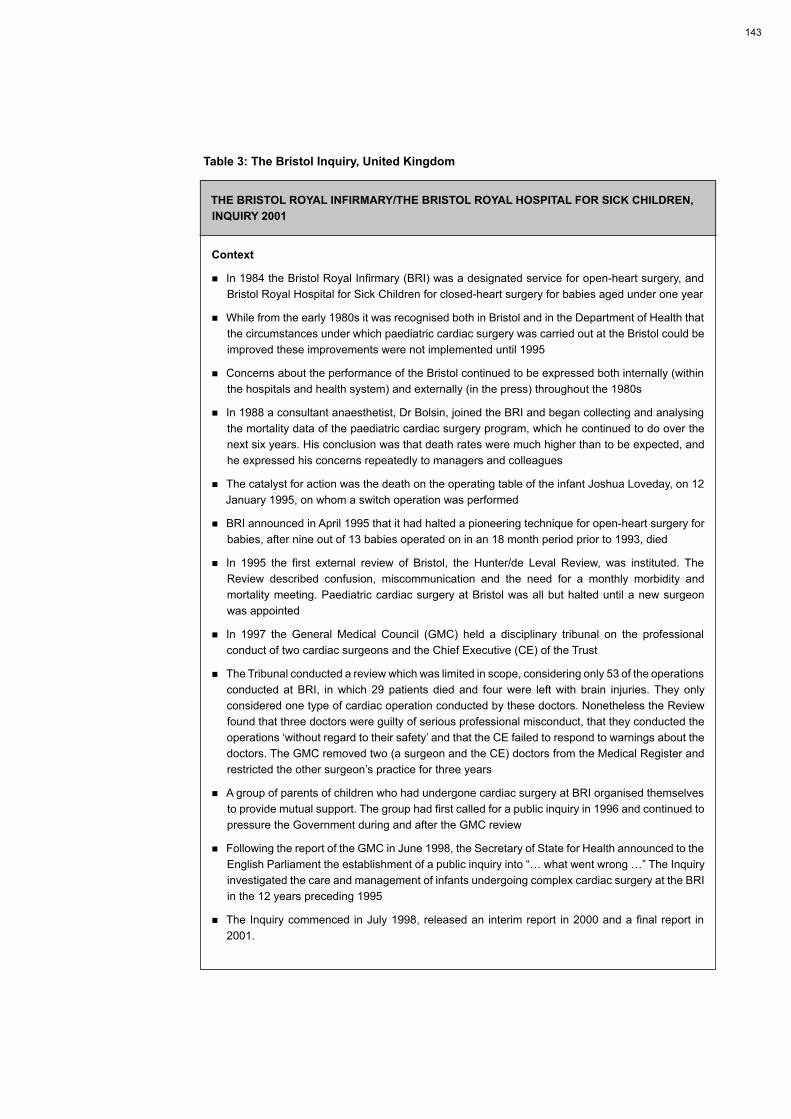
�43
Table3:TheBristolInquiry,UnitedKingdom
THEBRISTOLROyALINFIRMARy/THEBRISTOLROyALHOSPITALFORSICKCHILDREN,INQUIRy2001
Context
nIn1984theBristolRoyalInfirmary(BRI)wasadesignatedserviceforopen-heartsurgery,andBristolRoyalHospitalforSickChildrenforclosed-heartsurgeryforbabiesagedunderoneyear
nWhilefromtheearly1980sitwasrecognisedbothinBristolandintheDepartmentofHealththatthecircumstancesunderwhichpaediatriccardiacsurgerywascarriedoutattheBristolcouldbeimprovedtheseimprovementswerenotimplementeduntil1995
nConcernsabouttheperformanceoftheBristolcontinuedtobeexpressedbothinternally(withinthe hospitals and health system) and externally (in the press) throughout the �980s
nIn1988aconsultantanaesthetist,DrBolsin,joinedtheBRIandbegancollectingandanalysingthemortalitydataofthepaediatriccardiacsurgeryprogram,whichhecontinuedtodooverthenextsixyears.Hisconclusionwasthatdeathratesweremuchhigherthantobeexpected,andhe expressed his concerns repeatedly to managers and colleagues
nThecatalystforactionwasthedeathontheoperatingtableoftheinfantJoshuaLoveday,on12January1995,onwhomaswitchoperationwasperformed
nBRI announced in April �995 that it had halted a pioneering technique for open-heart surgery for babies,afternineoutof13babiesoperatedoninan18monthperiodpriorto1993,died
nIn 1995 the first external review of Bristol, the Hunter/de Leval Review, was instituted. TheReview described confusion, miscommunication and the need for a monthly morbidity andmortalitymeeting.PaediatriccardiacsurgeryatBristolwasallbuthalteduntilanewsurgeonwasappointed
nIn �997 the General Medical Council (GMC) held a disciplinary tribunal on the professional conductoftwocardiacsurgeonsandtheChiefExecutive(CE)oftheTrust
nTheTribunalconductedareviewwhichwaslimitedinscope,consideringonly53oftheoperationsconductedatBRI, inwhich29patients diedand fourwere leftwith brain injuries.Theyonlyconsideredonetypeofcardiacoperationconductedbythesedoctors.NonethelesstheReviewfoundthatthreedoctorswereguiltyofseriousprofessionalmisconduct,thattheyconductedtheoperations‘withoutregardtotheirsafety’andthattheCEfailedtorespondtowarningsaboutthedoctors.TheGMCremovedtwo(asurgeonandtheCE)doctorsfromtheMedicalRegisterandrestricted the other surgeon’s practice for three years
nAgroupofparentsofchildrenwhohadundergonecardiacsurgeryatBRIorganisedthemselvestoprovidemutualsupport.Thegrouphadfirstcalledforapublicinquiryin1996andcontinuedtopressuretheGovernmentduringandaftertheGMCreview
nFollowingthereportoftheGMCinJune1998,theSecretaryofStateforHealthannouncedtotheEnglishParliamenttheestablishmentofapublicinquiryinto“…whatwentwrong…”TheInquiryinvestigated the care and management of infants undergoing complex cardiac surgery at the BRI in the �2 years preceding �995
nTheInquirycommenced inJuly1998,releasedan interimreport in2000andafinalreport in200�.

�44 Patient Safety: a comparative analysis of eight Inquiries in six countries
Findings
nThe Inquiry found that the story of the paediatric cardiac surgical service in Bristolwas “not anaccountofbadpeople…peoplewhodidnotcare,norofpeoplewhowilfullyharmedpatients”
nTheInquiryconcludedthatthereasonsfortheproblemswere,forthemostpart,systemic“…productsofasystemthathadfundamentalweaknesses”
nKeyfindingsincluded:
– Whiletherewereconstantshortagesinthesupplyofstaff,under-fundingoftheservicewasnotthe cause of poor care
– TheNationalHealthService(NHS)hadmadeanerrorinapprovingthepaediatriccardiacservice,giventhattheaspirationsoftheservicewerenotmatchedbyitscapabilities
– TheserviceatBristolwaspoorlyorganisedandthephysicalenvironmentwasdangerous,withsurgeons in one hospital and paediatric cardiologists in another
– Therewasinequitabletreatmentofvariousstaff,withstronglinksbetweenseniormanagementand the ‘old guard’ of clinicians
– Thesurgeonslackedinsighttoseethattheywerefailingintheirduties
– Therewere inadequacies ateverypointof thecareprocess fromreferral throughtodiagnosis,surgery,andintensive care
– Therewasanabsenceofdefinedstandardsofcareforpaediatriccardiacsurgeryandforanyother specialty at Bristol
– Therewasafailuretoshareinformationwithparents,andwhattheyreceivedwasoftenpartial,confusing and unclear
– Therewasnostructureforthemonitoringoftheclinicalperformanceofhealthcareprofessionalsor of hospitals
– Therewaspoorteamworkbetweenprofessionals,attributedinparttothelackofeffectiveclinicalleadership,whichwasfoundtohaveaffectedboththeperformance,andoutcomes,ofcare
– Clinicians were actively involved in collecting and discussing data about adverse events, butdeniedanyadverseinferencesdrawnfromthatdata
– Themanagementculture includedapunitiveelement,whichhadresulted inanorganisationalenvironmentwherespeakingoutwasneitheracceptablenorsafe
– The NHSmanagement was considered to be poor; having devolved responsibility to HealthCareTrusts,ithadnotsubsequentlymonitoredtheimpactofthisprocessonthequalityofhealthcare
– TheBoardofManagementwereeitherpartofthe‘club’ortreatedasoutsiders,andwereunawareof,oruninvolvedin,thedailyoperationoftheservice
– Therewerepoorwaysofdealingwithpatients,whowereoftengiveninadequateorincompleteinformation,resultingintheirinabilitytogiveinformedconsent
nThecentralproblemwasdefinedasbeing’destructiveorganisationalcultures’
Recommendations
nChildrenandtheirhealthcareneedsweretobegivenhigherpriorityintheNHS
– According to the Inquiry’s recommendations, this would require: better coordination andintegration of services; the location of children’s acute hospital services in a children’s hospital; clear standards for the care of children; the publication of information about the quality and performance of children’s health care services; and specialist training of all health care staff workingwithchildren

�45
Recommendations(continued)
nPatientsintheirjourneythroughthehealthcaresystemwereentitledtobetreatedwithrespectandhonestyandtobeinvolved,whereverpossible,indecisionsabouttheircare
– Thiswastoachievedthroughthe:trainingofhealthcareprofessionalsincommunicationskills;freeandhonestexchangeofinformationbetweenparentsandprofessionals;establishmentof an integrated system of support and counselling for patients and carers; and upholding of therightofparents,ratherthanhealthcarestaff,todecidewhatinformationtheyrequire
nPatientswereentitledtoexpectthatboththeNHSandthehospitalinwhichtheyarecaredforwerewellled
– Inorder toachieve this, the Inquiry recommended that the:governmentestablisheffectivesystems to regulate the quality of health care; chief executives of health care organisations besupported in their tasks;managementboardsofhealthcareorganisationswere tobeselected and trained for leadership of health care at the local level; and quality of health care wastoberegulatedthroughbodiessuchastheNationalInstituteforClinicalExcellenceandthe Commission for Health Improvement
nPatientswereentitledtobecaredforbyhealthcareprofessionalswithrelevantanduptodateskillsandexpertise
– This would require: health care professionals to undertake training in communication,organisationalandteamworkskills;medical,nursingandmanagementschoolstodevelopjoint,multidisciplinary,courses;medicalschoolstoreviewtheircriteriaforapplicantstoensuregreaterdiversity;asystemofregulationcoveringtheeducation,registration,revalidationanddisciplineofhealthcareprofessionals;compulsorycontinuingprofessionaldevelopment,periodicappraisaland revalidation for health care professionals; positive incentives and training for senior clinicians totakeonseniormanagerialroles;propertraininganddirectsupervisionforsurgeonsandotherclinicians;permissiontobesoughtfromlocalethicscommitteebeforeneworuntriedproceduresweretobeattemptedonpatients;patientstobeinformedabouttheexperienceofsurgeonsorother clinicians before giving consent; and the employer to carry the primary responsibility for dealingwithpoorperformanceandmisconduct
nPatientswereentitledtocarethatwassafe
– Thecomponentsofsafecarewereconsideredtobemuchmorethantheactionsorcompetenceof health care professionals, and included the physical environment, equipment, workingarrangements,teamworkandgoodcommunication.Therecommendationsassociatedwithsafe care related to the: establishment of a safety culture and the removal of the existing culture of blame; creation of aNationalPatientSafetyAgency for the reporting, analysisanddisseminationofinformationaboutadverseevents,includingtheanalysisofpersistentcausesofunsafepractices;replacementofthesystemofclinicalnegligencewithsystemsforidentifying,analysing,learningfromandpreventingerrors;andintroductionofincentivesforthe reporting of sentinel events
nPatientsweretobeentitledtocareandtreatmentofanappropriatestandardinformedbycurrentknowledge
– Thereweretobeagreedandpublishedstandardsofclinicalcareforhealthcareprofessionalstofollow,sothatpatientsandthepublicknewwhattoexpect,andthereweretobestandardsforhospitalsasawhole,withhospitalsnotmeetingthesestandardsunabletoofferserviceswithintheNHS
nGenericstandardsweretobemetbyhealthcareinstitutions
– AllNHSservicesweretomeetaminimumsetofcapabilitiesrelatingtothestateofthebuildingsandequipment,thequalityofleadership,andtheorganisation’spoliciesandproceduresforensuring that care is safeandofgoodquality.Theserviceswere toperiodicallyundergoaprocessof revalidationby theCommission forHealth,whichwouldalsomonitorclinicalperformance at a national level

�46 Patient Safety: a comparative analysis of eight Inquiries in six countries
Recommendations(continued)
nThepublicwasentitledtoexpectthatmeansexistedforthemtobecomeinvolvedintheplanningofservices
– TheNHSwasto:takeaccountof,andrespondtotheinterestsandneedsofthepubliconadailybasis; involve patients in those processes designed to secure the competence of health care professionals; and embed the interest of patients into all their organisations and institutions. The Inquiry provided principles to facilitate this process.
11.2 CampbelltownandCamdenHospitals,Australia
Table4summarisestheoutcomesofinquiriesintoCampbelltownandCamdenHospitalsinsouthwestSydney.Followingthereportsinthemediaofwhistleblowernurses,thehospitalswerethesubjectoftwoinquiries.
ThefirstwasconductedbytheNSWHealthCareComplaintsCommission(HCCC)between2002and2003.Afterpolitical,mediaandpublicreactionstothefindingsofthatreport,aSpecialCommissionofInquirywasinstigatedbytheMinisterforHealth.ThisCommissionreportedin2004.Table 4 highlights recommendations from the second Inquiry.
Table4:TheCampbelltownandCamdenInquiry,Australia
THESPECIALCOMMISSIONOFINQUIRyINTOCAMDENANDCAMPBELLTOWNHOSPITALS,2004
Context
nTheCampbelltownandCamdenHospitalsarethemainhealthcareorganisationsintheMacarthurHealthServiceinsouthwestSydney
nPrior to2001 therewere fouryearsof informaland formal complaintsmadeaboutmedical care,mainlyfromnurses,attheCampbelltownandCamdenHospitals
nBy2002therumoursaboutinadequatecarehadbeenpickedupbythemedia,andwerefrontpagenews
nDuring November 2002 the Minister for Health heard formal complaints from nurses and directed the Health Care Complaints Commission (HCCC) to investigate them
nTheHCCC investigation lasted fromNovember2002 toDecember2003.A significant degreeofconcernwas expressed about the effectiveness of this investigation by a number of the partiesinvolved
nASpecialCommissionofInquirywasinitiatedinDecember2003.AnInterimReportwaspublishedon31March2004andafinalreportinJuly2004
Findings
nThe HCCC should have investigated all the allegations in relation to the individual professional conductoftherelevantpractitionersandsothestakeholders’misgivingsabouttheHCCCprocesswere,inbroadterms,vindicated
nMany of the adverse events could have been more appropriately handled through better internal hospitalprocedures,moreopendiscussionbetweenprofessionalcolleagues,andfullerdisclosuresto patients and families
nThestatutorypatientcarecomplaintssysteminNSWwasconsideredtobewelldesigned,anddidnotrequireanychanges,butstatutoryproceduresmustbefollowed

�47
Findings(continued)
nThe administrators at the hospitals did not deliberately attempt to cover up adverse events,clinicalincidents,ortostifleinvestigationofallegations
nThecomplaintssystemneeded to lookatbothsystemicand individual issues,butasystemsapproach did not exclude orthodox professional discipline procedures
nAfter the commencement of the Inquiry improvements had been made at various levels of the health service. These included the establishment of the Clinical Excellence Commission and the use of root cause analyses (RCAs) across the health system
Recommendations
nSeventeensuggestedchanges to thestatutorysystem including issuessuchasdefinitionsofunsatisfactory professional conduct, changes to theNursesAct, changes to theHealthCareComplaintsAct,andchangestotheHCCC’spower,proceduresandprocesses
nItwas recommended thatAreaHealthServices create policies consistentwith the principlesin outlined in the Report: open disclosure standards; best practice complaints handling; and a model for managing concerns about clinicians
nAllteamsconductingrootcauseanalyses(RCA)weretousetheModel for Managing Concerns about a Cliniciantodetermineifanindividualwastobereferredtoseniormanagersforreview
nAllteamsweretoconductRCAsofincidentswithaseverityassessmentcode(SAC)of1or2weretohavethesameprotectionasprovidedintheHealth Administration Act
nAreviewofRCAprocesswasrecommendedafterthreeyearstoensureabalanceofusefulnessoftheinformation,withtheprotectionprovidedtoparticipantsinRCAteams
nDocuments generated by RCAs were to be made available to the HCCC, when a relevantcomplaint wasmade – but these documentswere not to bemade admissible in a statutorydisciplinaryproceedingorelsewhere
11.3 CeljeHospital,Slovenia
TheCeljeHospitalInquiryprovidesinsightsintotheimpactonpatientsafetyofclinicalsupportservices,inthiscase,pathology.ItalsoallowsforreflectiononahospitalsystemoutsidethoseofEnglishspeakingcountries.AswithBristol,CeljeHospitalhadahistoryofadecadeofformalandinformalcomplaintsandmultiplereviewsbeforeanydirectactionwastaken.Table5providesthedetails.
Table5:TheCeljeHospitalInquiry,Slovenia
THECELjEHOSPITALINQUIRy,2003
Context
nSignificanterrorsmadeintheMorphologyandCytologyDepartmentatCeljeHospitalregardingthe examination of tissue specimens and reporting of the results
nThehospitalconducteditsowninquiryin1994,buttheerrorscontinued
nInJanuary2002,theMedicalDirectoroftheHospitaldeterminedthataformalinternalinquiryshouldtakeplaceandwrotetotheSlovenianMedicalChamberrequestingthatthisoccur
nInOctober2002aCommitteeof Inquirywasconvened,with thecollaborationof theMedicalChamber and the Slovenian Police
nThefinalreportwaspresentedtotheMinisterforHealthinMay2003

�48 Patient Safety: a comparative analysis of eight Inquiries in six countries
Findings
nTherewerelittlehospitaldataavailablebywhichtomonitorperformance
nTheHospital’slackofresourceswasusedtorationalisethelimitedmonitoringandmanagementofstaff
nPatient empowerment was considered to be unsatisfactory; patients who complained about thequalityoftheserviceoftenhadtheirpathologysamplesreturnedwiththesuggestionthattheyhavethemanalysedelsewhere
nNo one ever apologised to patients, even those who had been found to have been seriouslyharmed
nWhiletherehadbeennointentionalintenttoharmpatientsthereweremajorsystemicandculturalproblems. These included:
– Staffmemberswhofeltthatitwasneithertheirdutynorresponsibilitytomanagethepatientfromadmission to discharge
– Doctorswhobelievedthat theirworkshouldnotbesubject tooversightbyothers,andnurseswhofelttheydidnothavetheresponsibilitytocommentonerrorsmadebyseniordoctors
– An organisational culturewhich discouraged both the admission of errors and acceptance ofcomplaints
– Amedicalculture thatsupported thepracticeofnotwritingdownrulesandguidelines,so thatchangestoprocedureswheretransmittedalmostentirelyorally
– Almostacompleteabsenceofrecognitionthatclinicalworkrequiredcollectivemanagementonthe part of clinicians
Recommendations
nSignificantimprovementsinclinicalteamworkwereneeded
nAnincreasedunderstandingandrespectofdifferencesbetweenclinicalprofessionswasrequired
nForumsweretobedevelopedwheremultidisciplinaryteamswereabletodiscussmultidisciplinaryproblems
nAdmissionoferrorsweretobeseenasasignofstrengthonthepartofcliniciansandstaff
nThe patient was to be placed at the centre of care process, rather than the profession or theorganisation
nTheblamingofindividualsandthepracticeofpassingblamedownwardswastobeavoidedinplaceof a systems approach
nMoretrustandcommunicationwasrequiredbetweenmanagementandstaff
nGreaterusewastobemadeofclinicalpracticeguidelinesandclinicalpathways
nChangeswererequiredatalllevelsfromthegovernmenttohealthcareagenciesinordertoimprovethequalityofservicesprovided,withpatientstobethekeyplayersintheprocessofreform

�49
11.4 Glasgow’s,VictoriaInfirmary,Scotland
TheVictoriaInfirmary,Glasgow,providesanexampleofthreatstopatientsafetythatemanatefromthewiderhospitalenvironment.Thehealthcareassociatedinfection(HAI)inthiscasewassalmonella,buttheorganisationalissuesreflectthosethatoccurinresponsetoalltypesofHAIs.
Table6:TheVictoriaInfirmaryInquiry,Scotland
THEVICTORIAINFIRMARyINQUIRy,2003
Context
nTherewereoutbreaksofhealthcareassociatedinfection(HAI)thatoccurredoverseveralyearsacross Scotland
nActionsweredeemednecessary in thecaseof theVictoria Infirmarybecauseofwidespreadpublic concern and mass media interest
nTherewereoutbreaksofsalmonella infectionat theVictoria Infirmary,Glasgow, inDecember2001andJanuary2002
nThreepeoplediedandalargenumberwereinjuredorplacedatrisk
nAninquiryteamwasestablishedbyNHSScotlandunderthechairmanshipofDrBrianWattin2002
nAsaconsequenceofthatInquiry’sreport,theMinisterforHealthandCommunityCarecalledaconventionofexpertsandinterestedpeoplefromacrossScotlandandinternationally, inJune2002
Findings
nOne of the patients in the Infirmary was the likely source of the infection, having acquiredsalmonella enteritidis in the community before admission to hospital
nTherewasnoevidencethathospitalfoodcausedtheoutbreak
nTheexactrouteorroutesofcross-infectioncouldnotbeidentified
nThemainfindingwasthatwhiletheoutbreakofsalmonellainfectionwasunfortunatetherewasno evidence that the deaths could have been avoided
nTheInquiryarguedthatwhileitwaspossibletoreducethechancesofhospitalacquiredinfection,they could not be eliminated entirely
nTheInquiryalsofoundthattheVictoriaInfirmary(builtin1893)was“…nolongerfitforpurposeas a busy general hospital.”
nIthadsufferedfromaprolongedperiodofuncertaintyaboutitsfuturewithconsequentseriousunderinvestment in the fabric of the building
nTheHospitalhadalsofacedalongstandingseriesofdifficulties,whichhadbeenwellpublicised,inoftenhostilemediacoverage.Theabovefactorswereseentohavehadtwoconsequences:
– difficultiesinrecruitment(30%shortfallofthenursingestablishmentinthemedicalunitwheretheoutbreaksoccurred)withrelianceonbankandagencystafftofillthegaps,and
– aloweringofmoraleandthedevelopmentofa’siege’mentalityinsomeTruststaff

�50 Patient Safety: a comparative analysis of eight Inquiries in six countries
Recommendations
nIncreasedcompliancewithexistinginfectioncontrolrulesandguidelineswasrequiredfromallstaff
nRegularauditingofstaffcompliancewithhandwashingandfoodhandlingwastobeconducted
nOperatingprocedurescentredonissuessuchascleaningspecifications,dealingwithcontaminationanddecontaminationofstaff,staffuniforms,andthemovementofpatientsweretoberefined
nAllstaffandmanagersweretobemaderesponsibleandaccountableforhygieneissues
nInordertodealwithseriousHAIoutbreaksassoonastheyoccurred,eachhealthcareorganisationwastohave:
– adesignated,trained,infectioncontroldoctor
– an Infection Control Team (ICT)
– an infection ‘issue manager’
nEachNationalHealthTrustwastohavealeadInfectionControlNurse(ICN)
nA more systematic approach to reporting of infection control threats was needed, includingdocumentation of:
– contactandincidentswithinfectiousmaterials
– advice given and received about infection control from ICTs
– thescreeningofrelevantstaffincaseofoutbreaks
– theclassificationofincidentoutbreaks
nThelevelsofbasicwardequipmentweretomaintainedataleveltoreducethecommunaluseofsuch equipment
nThenumberofinfectioncontrolstaffweretobesufficienttoallowthemtohavedailycontactwithwards
nTeamworkandleadershiponinfectioncontrolissuesneededtobeimproved
nAcultureofopennessbetweentheScottishExecutive,theNHSandrelevantagenciesneededtobedeveloped
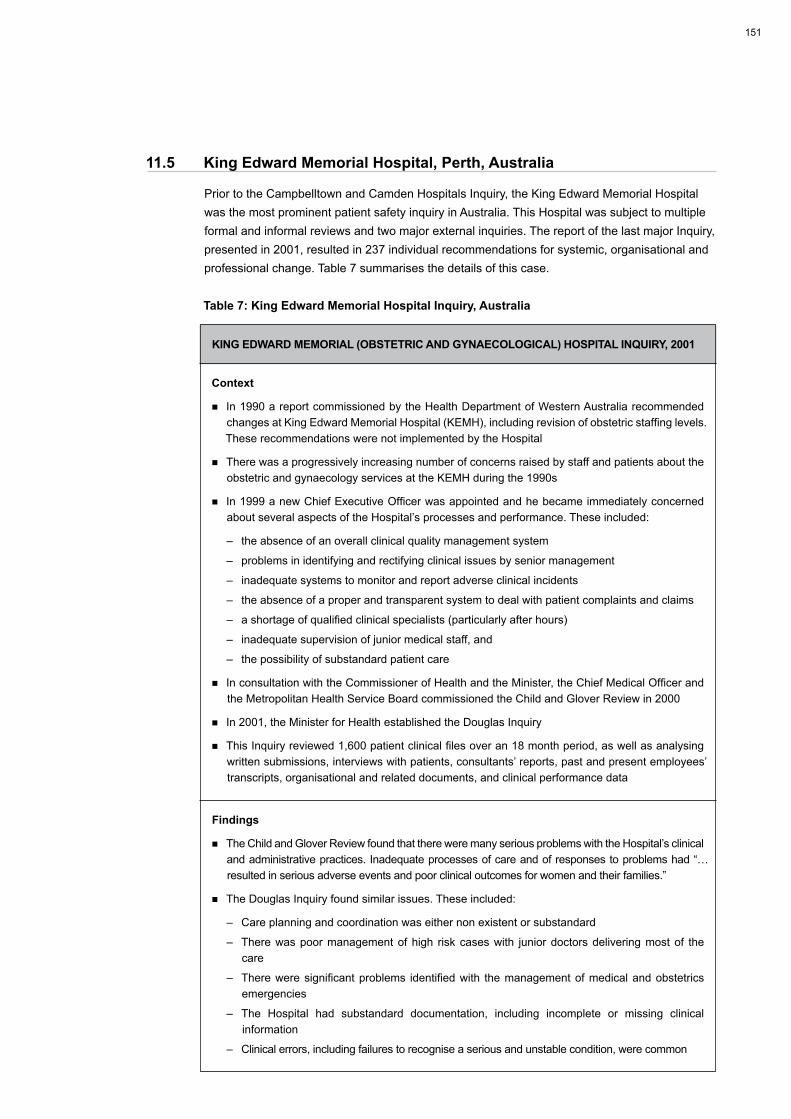
�5�
11.5 KingEdwardMemorialHospital,Perth,Australia
PriortotheCampbelltownandCamdenHospitalsInquiry,theKingEdwardMemorialHospitalwasthemostprominentpatientsafetyinquiryinAustralia.ThisHospitalwassubjecttomultipleformalandinformalreviewsandtwomajorexternalinquiries.ThereportofthelastmajorInquiry,presentedin2001,resultedin237individualrecommendationsforsystemic,organisationalandprofessional change. Table 7 summarises the details of this case.
Table7:KingEdwardMemorialHospitalInquiry,Australia
KINGEDWARDMEMORIAL(OBSTETRICANDGyNAECOLOGICAL)HOSPITALINQUIRy,2001
Context
nIn1990areportcommissionedbytheHealthDepartmentofWesternAustraliarecommendedchangesatKingEdwardMemorialHospital(KEMH),includingrevisionofobstetricstaffinglevels.TheserecommendationswerenotimplementedbytheHospital
nTherewasaprogressivelyincreasingnumberofconcernsraisedbystaffandpatientsabouttheobstetric and gynaecology services at the KEMH during the �990s
nIn1999anewChiefExecutiveOfficerwasappointedandhebecameimmediatelyconcernedabout several aspects of the Hospital’s processes and performance. These included:
– the absence of an overall clinical quality management system
– problems in identifying and rectifying clinical issues by senior management
– inadequate systems to monitor and report adverse clinical incidents
– theabsenceofaproperandtransparentsystemtodealwithpatientcomplaintsandclaims
– ashortageofqualifiedclinicalspecialists(particularlyafterhours)
– inadequatesupervisionofjuniormedicalstaff,and
– the possibility of substandard patient care
nInconsultationwiththeCommissionerofHealthandtheMinister,theChiefMedicalOfficerandtheMetropolitanHealthServiceBoardcommissionedtheChildandGloverReviewin2000
nIn2001,theMinisterforHealthestablishedtheDouglasInquiry
nThisInquiryreviewed1,600patientclinicalfilesoveran18monthperiod,aswellasanalysingwrittensubmissions,interviewswithpatients,consultants’reports,pastandpresentemployees’transcripts,organisationalandrelateddocuments,andclinicalperformancedata
Findings
nTheChildandGloverReviewfoundthatthereweremanyseriousproblemswiththeHospital’sclinicalandadministrativepractices.Inadequateprocessesofcareandofresponsestoproblemshad“…resultedinseriousadverseeventsandpoorclinicaloutcomesforwomenandtheirfamilies.”
nThe Douglas Inquiry found similar issues. These included:
– Careplanningandcoordinationwaseithernonexistentorsubstandard
– Therewaspoormanagementofhigh riskcaseswith juniordoctorsdeliveringmostof thecare
– Thereweresignificantproblems identifiedwith themanagementofmedicalandobstetricsemergencies
– The Hospital had substandard documentation, including incomplete or missing clinicalinformation
– Clinicalerrors,includingfailurestorecogniseaseriousandunstablecondition,werecommon

�52 Patient Safety: a comparative analysis of eight Inquiries in six countries
Findings(continued)
– Policyandguidelinedevelopment,deployment,compliancemonitoringandreview,werefoundtobelacking
– Therewereno formal systemsoraccountabilities for identifying, reviewingand responding toincidents and adverse events
– Where incidents were reported, there were significant delays between the time of a criticalincident and the lodging of a report
– Attimestherewasacompletelackofresponsetocriticalincidentsandadverseeventsonthepart of the Hospital management and clinicians
– The Hospital had failed to report several reportable deaths to the Coroner
– TheHospitalhadlongtermproblemswithstaffing
– Patients’ complaints of the poor treatment and poor communication by staff were poorlyhandled
– Therewasnohospitalwidequalityimprovementprogram
Recommendations
nAnevaluationofthestructure,roleandmanagementoftheHospitalwastobeconducted
nJuniordoctorsweretobesupervisedmoreeffectively,andafterhourscoverageofseniorstaffandtheavailabilityofbackupconsultantswastobeincreased
nClinicalguidelinesandguidelinesforclinicalcareplanningweretobeestablished
nA policy on how the hospital developed, deployed,monitored and reviewed clinical policies andguidelineswastobedeveloped
nTraining on a range of issues was to be conducted and monitored and postgraduate medicaleducation improved
nThegynaecologyserviceandtheAdultSpecialCareUnitweretobereviewed
nCarecoordinationandfollowupresponsesweretobeenhanced
nPatientsweretobeactivelyinvolvedindecisionmaking
nCommunicationwithpatientswastobeimproved
nDocumentationwastobestrengthenedandcomparativedataanalysiswastobeundertakenandpublished
nClinicalaccountabilitywastobeincreased
nAnincidentreportingsystemwastobeestablished,alongwithrelevantpoliciesandprocedures
nPoliciesandprocedureswerealsotobeestablishedfortheappointment,reappointment,supervisionand performance management of all clinicians and staff
nTheHospitalwastobereaccreditedbyanexternalbody
nTheClinicalGovernanceCommitteeoftheHospitalwastobeheldresponsibleforitsdecisionsandactions

�53
11.6 RoyalMelbourneHospital,Australia
TheInquiryintoRoyalMelbourneHospital,summarisedinTable8,offersinsightsintoanorganisation in some degree of turmoil. The Hospital had faced constant systemic and organisationalchange,ongoingshortagesofexperiencedstaff,andalackofmanagerialandclinical leadership. The Royal Melbourne Hospital Inquiry provides a supporting rationale for systemic approaches to patient safety.
Table8:TheRoyalMelbourneHospitalInquiry,Australia
THEROyALMELBOURNEHOSPITALINQUIRy,2003
Context
nIn2002,seriousallegationsweremadepublic concerning theconductofnursingstaffat theRoyal Melbourne Hospital (RMH)
nTheallegationsbecamethesubjectofseparateinvestigationsbytheVictorianCoronerandtheVictorianPolice
nThe Nurses Board of Victoria suspended the registration of two nurses but postponed itsinvestigations until the Coroner’s investigation had been completed
nThe Executive and Board of Melbourne Health conducted separate investigations into the allegations
nInviewof thehigh levelofpublicconcern, theMinister forHealth immediately requested theHealth Services Commissioner to conduct an independent inquiry
nItwastoaddressgeneralissues,ratherthantheparticularcomplaintsthatwerethesubjectoflegal proceedings. This Inquiry reported in 2002
Findings
nThe inquiry team concluded that the systemic, organisational and leadership changes thatoccurredbetween1995and2000inhospitalsacrossVictoriahadhadanadverseimpactonstaffmorale and standards
nTheresultantleadershipinstabilityduringthisperiodhadresultedin:alackofaccountability;afailuretoincludestaffindecisionmaking;alackofvision;andtoomuchfocusonfiscalmatters
nTheHospitalwasmarkedby:acultureofelitism;anattitudeofcomplacency;confusionoverresponsibilities;fragmentation;andalackofaccountability
nOperatingrulesandguidelineshadbeeninadequateinthepast,andwheretheyexistedtheyhadlowlevelsofcompliance
nTheHospital’squalityassuranceandimprovementprogramswerenoteffectivelyintegrated
nSomerelationshipsbetweenhealthprofessionalshaddeterioratedovertheyears,tothedetrimentof patient care
nThere had been a decline in the rigour of medication control and clinical document in the recent past
nTherewerenoestablishedsystemsforcollectingdataonsentineleventsoradverseoccurrencescreening
nThe organisational culture did not value or respond to complaints by staff
nResourceconstraintsinthe1990shadhadledtoacombinationoffactorswhichaffectednurses’work including: high workloads; exposure to stressful situations; poor roster and shiftworkarrangements; and reduction in staff support positions
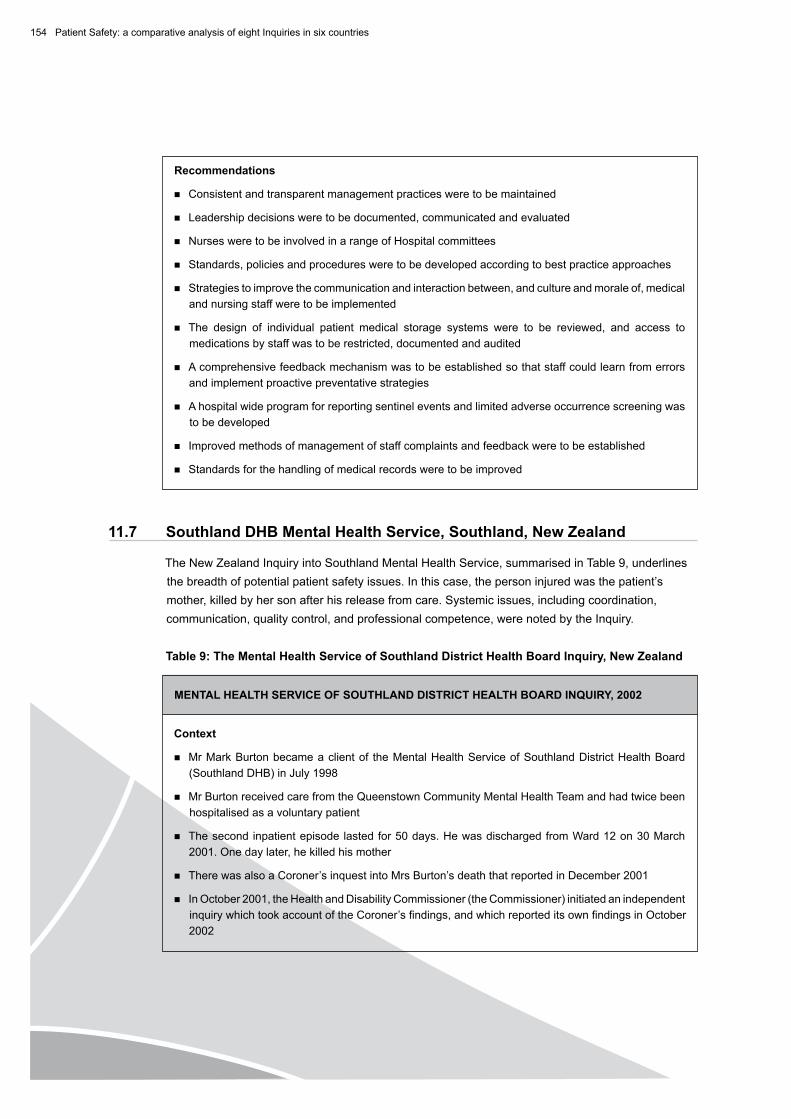
�54 Patient Safety: a comparative analysis of eight Inquiries in six countries
Recommendations
nConsistentandtransparentmanagementpracticesweretobemaintained
nLeadershipdecisionsweretobedocumented,communicatedandevaluated
nNursesweretobeinvolvedinarangeofHospitalcommittees
nStandards,policiesandproceduresweretobedevelopedaccordingtobestpracticeapproaches
nStrategiestoimprovethecommunicationandinteractionbetween,andcultureandmoraleof,medicalandnursingstaffweretobeimplemented
nThe design of individual patient medical storage systems were to be reviewed, and access tomedicationsbystaffwastoberestricted,documentedandaudited
nAcomprehensivefeedbackmechanismwastobeestablishedsothatstaffcouldlearnfromerrorsand implement proactive preventative strategies
nAhospitalwideprogramforreportingsentineleventsandlimitedadverseoccurrencescreeningwasto be developed
nImprovedmethodsofmanagementofstaffcomplaintsandfeedbackweretobeestablished
nStandardsforthehandlingofmedicalrecordsweretobeimproved
11.7 SouthlandDHBMentalHealthService,Southland,NewZealand
TheNewZealandInquiryintoSouthlandMentalHealthService,summarisedinTable9,underlinesthebreadthofpotentialpatientsafetyissues.Inthiscase,thepersoninjuredwasthepatient’smother,killedbyhersonafterhisreleasefromcare.Systemicissues,includingcoordination,communication,qualitycontrol,andprofessionalcompetence,werenotedbytheInquiry.
Table9:TheMentalHealthServiceofSouthlandDistrictHealthBoardInquiry,NewZealand
MENTALHEALTHSERVICEOFSOUTHLANDDISTRICTHEALTHBOARDINQUIRy,2002
Context
nMrMarkBurtonbecameaclientof theMentalHealthServiceofSouthlandDistrictHealthBoard(SouthlandDHB)inJuly1998
nMrBurtonreceivedcarefromtheQueenstownCommunityMentalHealthTeamandhadtwicebeenhospitalised as a voluntary patient
nThesecondinpatientepisodelastedfor50days.HewasdischargedfromWard12on30March2001.Onedaylater,hekilledhismother
nTherewasalsoaCoroner’sinquestintoMrsBurton’sdeaththatreportedinDecember2001
nInOctober2001,theHealthandDisabilityCommissioner(theCommissioner)initiatedanindependentinquirywhichtookaccountoftheCoroner’sfindings,andwhichreporteditsownfindingsinOctober2002

�55
Findings
nThe Commissioner concluded that no single act or single individual could be held to carry the primaryresponsibilityforthepoorcarebutthatthe“…overallpicture[was]oneofsloppycarethatwaslaxandlaissez-faire.”
nTherehadbeenmanydeficienciesintheclinicalcareofthepatientandthatwhileeachdeficitsingularly may not have been responsible for the outcome in total they resulted in poor care
nTherewereinadequatemonitoringandcontrolmechanismstoensurethatstaffpractisedsafely,thatincidentandriskmanagementstrategieswereputinplace,andthatpoliciesandprocedureswerefollowed
nCommunicationwiththeclient’sfamilyhadbeeninadequate
nDischargeplanninghadbeencareless,imprecise,lackingdetailandpoorlycoordinated
nThe lack of coordination between the inpatient and community care teams was considerednotable
nThe policy and procedural standards for the mental health service were considered to beinadequate
nCompliancewithincidentreportingruleswasalsoinadequate
nThestaffwerefoundtohavefailedtoworkasateamandhadbeenunabletocommunicateandcollaborate adequately
nTherewereindividualfindingsinrelationtoeachofthestaffinvolvedinthecase(doctors,nurses,social workers,mental health needs assessor, alcohol and drug services counsellor, patientservicemanager,clinicaldirectorandteamleader),aswellastothecorporateresponsibilityofthe Southland DHB
Recommendations
nAllstaffassociatedwiththecase,aswellastheDHB,wererequiredtoapologiseinwritingtothepatient’s family
nThetwodoctorsassociatedwiththecaseweretohavetheircompetencereviewedbytheMedicalCouncilofNewZealand
nAllotherstaffwererequiredtoreviewtheirpracticeinlightofthefindingsoftheInquiry
nCompetencereviewsofkeypersonnelweretobeconductedandperformancecriteriaestablishedfor each of their positions
nSpecificrecommendationsweremadetoaddresstheunderlying,systemiccausesofpoorcare,including the establishment of internal auditing and monitoring processes
nImmediateattentionwastobegiventopatientassessment,patientrecordsanddocumentation,incident reporting, risk assessment andmanagement, quality care and treatment, discharge,supervision,andfamilyandcarerparticipationinthecareofpatients
nAcultureofcontinuousqualityimprovementwastobeestablished,includingcontinuouscriticalappraisalandreflectionbyallstaffontheirownandjointpractice
nNursingstandardsandskillsformentalhealthnursingweretobeimproved
nStaffing structures and employment conditions were to be reviewed, including professionalsupportandpathways
nImprovementsweretobemadetothecommunicationandcoordinationprocessesandsystems

�56 Patient Safety: a comparative analysis of eight Inquiries in six countries
11.8 WinnipegHealthServicesCentre,Canada
Thefinalstudy,thatofWinnipegHealthServicesCentre,alsorelatestoapaediatriccardiacservice.LikeBristol,doctors,nursesandparentshadallraisedconcernsaboutpatientsafetyoveranextendedperiodoftimebeforeaninquirywasfinallyheld.ThesummaryisprovidedinTable10.
Table10:TheWinnipegHealthSciencesCentreInquiry,Canada
THEWINNIPEGHEALTHSCIENCESCENTREINQUIRy,1998
Context
nIn1994,subsequenttoashortsuspensionduetochangesinkeypersonnel,thepaediatriccardiacsurgeryprogramattheWinnipegHealthServicesCentrewasre-establishedaftertheemploymentofanewsurgeonasheadoftheteam,andanewdirectorofpaediatriccardiology
nInadequatelyexplaineddeathsbegantooccuralmostimmediatelyaftertheProgramwasreactivated.Thedeathscontinuedfrom15Marchto21December,1994
nIntotal,12childrendiedduringorshortlyafterhavingundergonecardiacsurgeryattheCentre.Thechildrenwereagedfromtwodaystofouryearsold
nTwogroupsofstaff (anaesthetistsandnurses) fromtheoperatingroomsand intensivecare,hadbeguntoexpressconcernsabouttheperformanceofthenewsurgeon,almostimmediatelyafterhisarrival at the Centre
nInMay 1994 (following the death of the fifth of the 12 children), themembers of theSection ofPaediatric Cardiac Anaesthesia at the Centre unanimously refused to take part in any furtherpaediatricopen-heartcasesuntilareviewofthecaseswasundertaken
nAninternalreviewcommitteewasappointed,andtheprogramwasaskedtoreduceitsprogramtolowriskcases.Duringtheperiodofreview,twomorechildrendied
nThereviewconcludedtheproblemswereanormalconsequenceofhavingarelativelynewteamand that the team had resolved the causes. It recommended that the program return to full service in September �994
nFromthattimeuntil21December1994,fivemorechildrendied
nThatreviewpresenteditsreporttothehospitalinearlyFebruary1995andadvisedthattheCentreshould suspend the program for a further six months
nThehighdegreeofconcerninthemassmediacontinued,mainlyasaconsequenceofactionsbytheparentsofthechildrenwhodied,whomountedahighprofilecampaignforapublicinquiry
nOn5March1995,theChiefMedicalExaminerfortheProvinceofManitobaorderedaninquestintothedeathsofthe12children,andtheInquestcontinuedhearingsuntilSeptember1998.Itreleasedits report four years after it had commenced hearings
Findings
nTheInquestfoundthatcarehadbeenseriouslydeficient;ofthe12deaths,fivewerepreventableandfourwerepossiblypreventable.Theevidencewasinsufficienttoreachaconclusionontwodeaths,andonewasjudgednottohavebeenpreventable
nThe Inquest also found that while some of the problems in the cardiac surgery program wereconsideredattributabletotheabilitiesandconductofspecificindividuals,mostoftheproblemswereconsidered to be systemic in nature

�57
Findings(continued)
nSystemsissueswhichhadbeenfoundtoeffecttheoutcomesoftheprogramincludedthehospitalpolicies and procedures governing: staffing; leadership; teamwork; communication; decisionmaking;andqualityassurance
nTherecruitmentprocessfornewsurgicalstaffwasseentobeflawed,withnoseriousattemptshaving been made to assess the competence of the candidates
nThe lines of authority and responsibility for the programwere felt to have been unclear andconfusing,resultinginopportunitiesforblameshiftingbetweenstaffandmanagement
nTherehadbeeninadequate,ad hoc supervision of clinical staff
nTwodoctors,theheadofthesurgicalteamandtheactingmedicaldirector,wereconsideredtohave failed in their duties
nThesurgeons’poorperformancehadbeenidentifiedbytheCentre,buthadsubsequentlybeenjustifiedonthebasisoftheir(thesurgeons’)learningcurve
nTheheadsof departmentshad failed tomanage staffingadequately andhadnot addressedunderlying issues which ultimately led to the loss of the program’s previous staff. Theysubsequentlyhiredlessexperienced,butavailable,clinicians
nPoorteamworkhadmarkedtheCentre’soperations,withinadequatecommunicationbetweenstaffaboutwhatwherecomplicatedprocedures
nNurseshadoccupiedsubservientpositionswithintheCentre,andasaresulttheirconcernswerenot treated appropriately
nTherehadbeenseriousweaknessesintheprocessofobtaininginformedconsentfromparents,includingparentsnotbeingfullyinformedeitherabouttherisksoftheprocedures,ortheskillsofthe surgeons
nTheOfficeoftheChiefMedicalExaminer,whichwasresponsiblefortheinvestigationofpatientharm,had:failedtoidentifytheproblemswiththeprogram;waitedtoolongforthefinalautopsyreports;nottrackedthesurgicaldeathsoftheprogram;andreliedtooheavilyontheinformationobtained from thesurgeons involved in thecase, rather thanseekingadvice froma rangeofexperts
Recommendations
nTheCentrewastoestablishatimelyrecruitmentprocess,overseenbyaformalsearchcommittee(includinginputfromnursingandrelatedstaff)whichallowedfortheobservationofapplicants’skillspriortohiring
nStandardoperatingproceduresandprotocolsweretobedeveloped
nA range of development programs and processes were recommended including those for:leadershipskills;teamdevelopment;teamcommunication;conflictresolution;andpost-operativedebriefingsessions
nStructuresweretobeputinplacewhichensuredthatallstaff,butinparticularnurses,couldvoicetheirconcernswithoutfearofreprisal
nAclearpolicywastobeestablishedonhowstaffcouldreportconcernsaboutrisksforpatients
nTheGovernmentwastoestablishapolicyfortheroutinepaymentoflegalcounselforfamiliesgranted standing at inquests
nChangestotheoperationoftheOfficeoftheChiefMedicalExaminerwerealsorecommended,includingthe:developmentofaprotocolrequiringhospitalstoinformitofsignificantchangesinthe delivery of service; maintenance of a database on numbers and causes of hospital deaths; andconductofinterviewswithnursingandmedicalstaffinvolvedinpatientcare.









