

PATHOLOGY AND INTERVENTION
IN MUSCULOSKELETAL REHABILITATION

THIS PAGE INTENTIONALLY LEFT BLANK

PATHOLOGY
AND INTERVENTION
IN MUSCULOSKELETAL
REHABILITATION
Editors
David J. Magee, PT, PhD Professor and Associate Dean
Department of Physical Therapy
Faculty of Rehabilitation Medicine
University of Alberta
Edmonton, Alberta, Canada
James E. Zachazewski, PT, OPT, SCS, ATC Clinical Director
Physical Therapy
Massachusetts General Hospital
Boston, Massachusetts
William S. Quillen, PT, PhD, SCS, FACSM Professor
Associate Dean, College of Medicine
Director, School of Physical Therapy and Rehabilitation Sciences
University of South Florida
Tampa, Florida
Editorial Consultant
Bev Evjen Swift Current, Saskatchewan, Canada
ELSEVIER
SAUNDERS ELSEVIER
11830 Westline Indusu-ial Drive St. Louis, Missouri 63146
PATHOLOGY AND INTERVENTION IN MUSCULOSKELETAL REHABILITATION ISBN: 978- 1-4160-0251-2
Copyright © 2009 by Saunders, an imprint of Elsevier Inc. Photo Copyright © 2009 for Chapter 8 and Chapter 14, will be retained by Diane Lee Photo Copyright © 2009 for Chapter 8 and Chapter 14, will be retained by Linda-Joy Lee
All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Permissions may be sought directly from Elsevier's Rights Department: phone: (+ 1) 215
239 3804 (US) or (+44) 1865 843830 (UK); fax: (+44) 1865 853333; e-mail: [email protected]. You may also complete your request on-line via the Elsevier website at http://www.elsevier.com/permissions.
Notice Neither the Publisher nor the Authors assume any responsibility for any loss or injury and/or damage to persons or property arising out of or related to any use of the material contained in this book. It is the responsibility of the treating practitioner, relying on independent expertise and knowledge of the patient, to determine the best treatment and method of application for tile patient.
ISBN-13: 978-1-4160-0251-2
ISBN-I0: 1-4160-0251-0
Vice President and Publisher: Linda Duncan Acquisitions Editor: Kathy Falk Developmental Editor: Sarah Vales Publishing Services Manager: Julie Eddy Project Manager: Rich Barber Designel': Julia Dummitt
Printed in the United States
Last digit is the print number: 9 8 7 6 5 4 3 2 1
The Publisher
Working together to grow libraries in developing countries
www.elsevier.com I www.bookaid.org I www.sabre.org
ELSEVIER �,?e?n�t��� Sabre Foundation
INJURI{S TO T"{ M{NIS(US AND
ARTI(ULAR (ARTlLAG{ David J. Mayman and Thomas J. Gill
Introduction
Injuries to the articular cartilage and the meniscus of the
knee are common. They can be caused by work activities
and athletic injuries as well as act ivities of daily living and
degeneration. They can occur as isolated injuries or in combination with injury to ligaments and other knee structures .
Meniscal tears and chondral injuries can cause s ignificant clinical symptoms of pain, swelling, loss of motion, and
locking, often requiring surgical intervention. Arthroscopic
treatment of meniscal tears has become one of the most common procedures in the United States .l
To evaluate and treat these injuries , the clinician must
have an understanding of the anatomy, h istology, and fu nction of the meniscus and articular cartilage . This chapter
reviews the anatomy and histology of both the art icular cartilage and the meniscal cartilage and the s igns and symp
toms of injuries to these structures; diag nostic studies and treatment alternatives are then discussed .
Meniscus
Anatomy
The meniscus was first described by Bland -Sutton2 i n 1 897
as "the fu nctionless remnants of intra-articular leg musc1es ." Since that time, the meniscal anatomy h as been stud
ied extensively . From a gross anatomical perspective , the menisci are two fibrocartilaginous structures that h ave
strong bony attachments to the anterior and posterior tibial
plateau .
In the C-shaped medial meniscus, the anteroposterior
dime nsion of the posterior horn is larger than the antero
posterior dimension of the anterior horn . Some variation
is seen in the bony attachments of the medial meniscus.
Bedet and Fowler3 h ave described four types of anterior
horn meniscal attachments, three of which attached to bone. The type four var iant h ad no firm bony attachment ,
but this type was found i n only one of 34 specimens . A s imilar attachme nt was described by Nelson and LaPrade;4 1 4%
of their specimens h ad no direct bony attachment of the anterior horn . The remainder of the medial meniscus is attached to the knee joint capsule . The capsular attachment
of the meniscus to the t ibia is called the coronary ligament. The posterior bony attachment consiste ntly l ies anterior to
the tibial insert io n of the posterior cruciate l igament. John
son et al .5 studied the s ur face area of t11e meniscal bony
attachments and found that the anterior horn of the medial meniscus has the largest footprint (61.4 mm2 ), and the
posterior horn o f the lateral meniscus h as the smallest
(28 . 5 mm2) (Figure 1 7- 1 ) .
The lateral meniscus , which is more semic ircular in shape, also has anterior and posterior bony attachments .
The lateral meniscus covers a larger area of the t ibial art icu
lar sur face than the medial meniscus . A lateral d isc-shaped or discoid meniscus that covers the ent ire t ibial articular
surface has been reported in 3 .5% to 5% of cases 6 Discoid
menisci are the result of a developmental anomaly and
may have a familial p attern; they are rarely fou nd medially,
are generally thicker than normal, and lack normal poster ior attachments . The bony attachment s ites of the normally shaped lateral meniscus, the anterior and posterior horns, are much closer together in the lateral meniscus t1un
in the medial meniscus . The anterior horn attaches just
adj acent to the anterior cruciate l igament (ACL). The bony
attachment site of the posterior horn is located behind the
tibial spines and anterior to the i nsertion s ite of t11e medial
579
580 C HAPTER 1 7 • Injuries to the Meniscus and Articular Cartilage
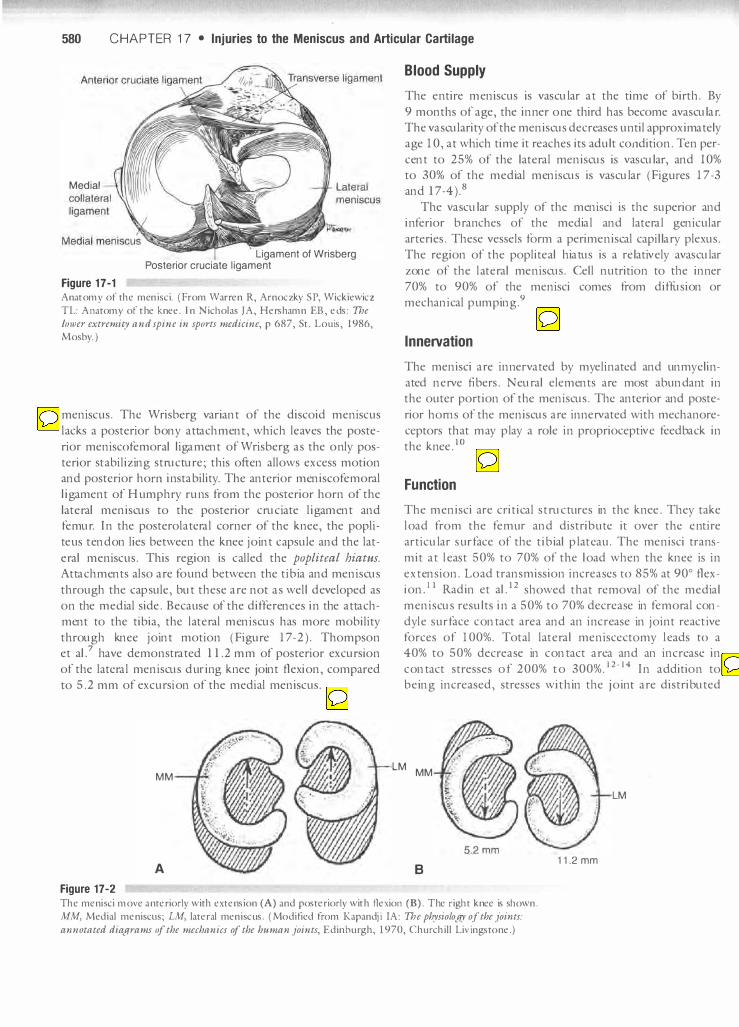
Medial
Figure 17-1
Ligament of Wrisberg Posterior cruciate ligament
Anatomy of th e meni sci. ( From Warren R, Arnoczky S P, Wicki ewicz
TL: Anatomy of the knee. In Nicholas JA, Hershamn EE, eds: The
IOlJler extremity and spine in sports medicine, p 687, St. Louis, 1986, Mosby. )
meniscus . The Wrisberg variant of the discoid meniscus
lacks a posterior bony attachment, which leaves the poste
rior meniscofemoral ligament of Wrisberg as the o nly pos
terior st abilizing structure; this often allows excess motion and posterior horn i nstability . The anterior meniscofemoral
ligament of H umphry runs from the posterior horn of the
lateral meniscus to the posterior cruciate ligament and femur. I n the posterolateral corner of the k nee, the popli
te us tendon lies between the knee joint capsule and the lat
eral meniscus . This region is called the popliteal hiatus. Attachments also are fo und between the tibia and meniscus
through the capsule, but these are not as well developed as
o n the medial side . Because of the differences i n the attachment to the tibia, the lateral meniscus has more mobility
through knee joint motion ( Figure 17-2). Thompson et al? have demonstrated 11.2 mm of posterior excursion
of the lateral meniscus d uring k nee joint flexion, compared
to 5.2 mm of excursion of the medial meniscus .
MM
A
Figure 17-2
Blood Supply
The e ntire meniscus is vascular at the time of birth . By
9 months of age, the inner o ne third has become avascular. The vascularity of the meniscus decreases until approximately age 10, at which time it reaches its adult condition . Ten per
cent to 25% of the lateral meniscus is vascular, and 10% to 30% of the medial meniscus is vascular (Figures 17-3 and 17-4).8
The vascular s upply of the menisci is the superior and i nferior branches of the medial and lateral genicular
arteries . These vessels form a perime niscal capillary plexus .
The region of the popliteal hiatus is a relatively avascular
zone of the l ateral me niscus . Cell nutrition to the inner
70% to 90% of the menisci comes from diffusion or mechanical p umping .9
Innervation
The menisci are innervated by myelinated and unmyelin
ated nerve fibers . Neural elements are most abundant in the outer portion of the meniscus . The anterior and poste
rior horns of the meniscus are innervated with mechanore
ceptors that may play a role i n proprioceptive feedback in
the k nee .lo
Function
The menisci are critical structures in the k nee . They take
load from the femur and distrib ute it over the e ntire
articular s urface of the tibial plateau. The me nisci trans
mit at least 50% to 70% of the load when the knee is i n
extension . Load transmission i ncreases to 85% at 90° flex
ion .11 Radin et al .12 showed that removal of the medial meniscus results i n a 50% to 70% decrease in femoral con
dyle s urface contact area and an i ncrease in joint reactive
forces of 100%. Total lateral me niscectomy leads to a 40% to 50% decrease in contact area and an increase in
contact stresses of 200% to 300%. ]2· 14 I n additio n to being increased, stresses within the joint are distributed
LM MM
B
LM
11.2 mm
Th e meni sci move anteriorly with extension (A) and posteriorly with flexion (B). The right knee is shown . MM, M edial meni sclls; LM, lateral meni scus. ( Modified from Kapandji IA: The physiology of the joints:
annotated diagl·ams of the mechanics of the human joints, Edinburgh, 1 970, Churchi l l Livingstone.)

Injuries to the Meniscus and Articular Cartilage • CHAPTER 17 581
figure 17-3 Blood supply of the meniscus. Staining studies demonstrate vascular
network within the meniscus that is critical for potential for healing. ( From Arnoczky SP, Warren RF: Microvascu lature of the human meniscus, Am J Sports Med ]0:90, 1982.)
unevenly, resulting in increased compressive and shear forces across the joint.
The meniscus plays an important role in shock absorption.IS Compression studies using bovine menisci have demonstrated that articular cartilage is approximately twice as stiff as meniscal fibrocartilage.
The menisci also can play a large role in joint stability.16 Medial meniscectomy in a knee with an intact ACL does not affect knee stability; however, medial meniscectomy in an ACL-deficient knee results in an increase in anterior tibial translation of up to 58% at 90° flexion. Allen et al. J 7
showed that the resultant force in the medial meniscus of an ACL-deficient knee increased 52% in full extension and 197% at 60° flexion under a 134 newton (N) load.
figure 17-4 Schematic of meniscus demon strating three zones with varying degrees of
vascularity and potential for healing.
(From Insal l IN, Scott WN: Surgery of
the knee, cd 3, p 476, New York, 2001, Churchill Livingstone . )
Zone: Red-red
Shoemaker and Markolf18 demonstrated that the posterior horn of the medial meniscus is the most important structure in the knee for resisting an anterior tibial force applied to an ACL-deficient knee.
The inner two thirds of the menisci are important for shock absorption and for increasing joint contact surface area, and therefore for reducing contact stresses. The peripheral ring of the menisci is important for load transmission, shock absorption, and knee stability.
Functions of the Menisci
• Load sharing
• Reducing joint contact stresses (by increasing contact surface
area)
• Shock absorption
• Passive joint stabilization
• Limiting extremes of flexion and extension
• Proprioception
Epidemiology
The mean annual incidence of meniscal tears is 60 to 70 per 100,000/9,20 and the ratio of males to females varies from 2.5:1 to 4:1. Approximately one third of all meniscal tears are associated with a tear in the ACL.21 The peak incidence of meniscal tears associated with ACL injury occurs at 2 1 to
30 years of age in males and at 11 to 20 years of age in females. A traumatic cause is more likely in younger patients, whereas older patients are more likely to have degenerative meniscal tears.
Patients with an acute ACL injury are more likely to have a lateral meruscal tear than a medial meniscal tear.22 Patients with chronic ACL-deficient knees, on the other hand, are more likely to develop a medial meniscal tear; the role of the medial
Red-white White-white
Meniscus: Peripheral Central (free edge)
Vascularity: Excellent Variable Poor
582 CHAPTER 1 7 • Injuries to the Meniscus and Articular Cartilage
meniscus as an anteroposterior joint stabilizer in ACL-deficient knees is thought to be the reason for this phenomenon.
Diagnosis of Meniscal Tears
Meniscal tears can be diagnosed through a combination of a careful history, a thorough physical examination, and the appropriate diagnostic tests.
History
Younger patients usually have a history of a weight-bearing, twisting, or hyperflexion injury. These patients usually present with acute joint line pain and swelling. Loss of extension with a mechanical block (locking) suggests a displaced bucket handle tear and usually reg uires acute surgical treatment.
Patients may complain of catching, popping, or locking. These symptoms occur with meniscal tears, but they also may be symptoms of chondral injury or patellofemoral chondrosis. Degenerative tears of the meniscus usually occur in patients over 40 years of age. These tears frequently present with a traumatic history of swelling and joint line pain, and they often are associated with some degree of chondral damage.
Physical Examination
Whenever the clinician suspects meniscal pathology, a complete physical examination of the low back and lower extremity must be performed.
Examination of the knee should begin with inspection of tlle skin and surrounding tissues. Quadriceps atrophy should be assessed. The knee should be examined for evideIlCe of an effusion. Range of motion should be assessed and compared to the opposite side. The ligamentous structures should be tested. The joint should be palpated to assess for joint line tenderness, tenderness at ligamentous insertion points, and tenderness in the region of the pes anserine bursa. The patellofemoral region also should be palpated.
Numerous special tests have been used to assess for meniscal pathology. Taken in isolation, the various physical examination tests for meniscal tears do not have high sensitivities, specificities, or positive predictive values. These tests include joint line palpation, the flexion McMurray test, and Apley's grind test. These tests have been shown to have mixed results. Evans et al.23 looked at the flexion McMurray test to determine intraobserver reliability and accuracy. They found that a medially based "thud" with rotation and flexion was the only McMurray sign to correlate with meniscal pathology. This finding had 98% specificity but only 15% sensitivity for medial meniscal tears23 Weinstabl et a1.24 found that joint line tenderness was the best clinical sign of a meniscal tear, with a sensitivity of 74% and a 50% positive predictive
value. The presence of an ACL injury makes joint line tenderness less helpful. Shelbourne et al25 showed an accuracy of 54.9% for medial meniscal tears and 53.2% for lateral meniscal tears. Terry et a1.26 examined the accuracy of a thorough history, physical examination, and plain radiographs to predict meniscal pathology preoperatively. The overall clinical evaluation had a sensitivity of 95%, a specificity of 72%, and a positive predictive value of 85% for tears of the medial meniscus; it had a sensitivity of 88%, a specificity of 92%, and a positive predictive value of 58% for tears of the lateral meniscus. All tears were confirmed arthroscopically.26
Diagnosis of Meniscal Pathology
• History of twisting while weight bearing
• History of hyperflexion of the knee
• Joint line tenderness
• Minimal to moderate synovial swelling
• Pain or forced flexion
• Limited extension with spring block end feel
• MagnetiC resonance imaging
• High level of suspicion
Diagnostic Studies
Several types of imaging shlclies can be used as an adjunct to the history and physical examination. Radiographs, arthrography, magnetic resonance imaging (MRl), and arthroscopy have all been used to help define meniscal pathology.
Radiography Plain radiographic films should be obtained in the evaluation of all knee pathology. A standard knee series should include a posteroanterior/anteroposterior (PA/ AP) weight-bearing view in 30° flexion, a true lateral view, and a tangential image, such as a Merchant or skyline view (Figure 17-5). These images will not confirm the diagnosis of a meniscal tear, but tlley are still important. Plain radiographic films can be used to assess tlle knee for joint space narrowing, osteophyte formation, subchondral cysts, and subchondral sclerosis, all findings of osteoarthritis of tlle knee. Early degenerative changes are better seen on PAl AP views in 30° flexion, because degenerative changes usually are more severe on the posterior femoral condyles tllan on the dis�al femur27,28 Non-weight-bearing radiographic films are not useful for determining joint space narrowing. The tangential view is best for assessing the patellofemoral joint, which can be a cause of medial or lateral knee pain. Plain radiographic films can also help determine whether any otller bony pathology is present. If any question arises about lower limb alignment, 3-foot ( 1.0 m) standing films should be obtained to determine the anatomical and mechanical axis of the lower extremity.

Injuries to the Meniscus and Articular Cartilage • CHAPTER 1 7 583
Figure 17-5 Standard radiographic views. A, AP weight-bearing view of the knee showing medial joint space loss. B, Lateral radiograph of the knee. C, Tangential view of the pate l lofemoral joint.
Standard Knee Radiographic Films
• PAIAP weight-bearing view in 30° flexion
• Lateral view
• Merchant or skyline view
Magnetic Resonance Imaging MRI has proven to be a great advance in the diagnosis of knee pathology, but the scans must be read in the context of the patient 's history and the phy sical examination find
ings. Some of the advantages of MRI are (1) it allows the
clinician to see the ligamentous and cartilaginous structures in the knee; ( 2 ) it does not require the use of ionizing radi
ation ; and (3) it is noninvasive. Disadvantages of MRI include (1) a relatively high cost; ( 2 ) the amount of time
required to obtain the scan; and (3) the tight space in which the patient must lie unless an open magnet machine
is u sed. Normal menisci appear as low signal intensity on all
image sequences.
Based on its MRI appearance, the m eniscus tear/injury can be categorized according to a four grade system
(Figure 1 7-6) . Grade 0 represents a normal meniscus .
Grade I and grade I I show some degree of intrameniscal signal, but the signal does not abut the free edge of the
meniscus . With grade I I I m enisci, the intrameniscal signal exits t hrough the articular surface of the meniscus . The
grade I I I pattern is consistent with a m eniscal tear.29
MRI i s a power ful tool in the diagnosis of meniscal
pathology. Several studies have shown meniscal tears on
MRI scans of asymptomatic patients . Boden et a1 . 30 studied
74 asymptomatic patients . Sixty -three were under age 45,
and eight of these (13%) were found to have meniscal tears .

584 CHAPTE R 1 7 • Injuries to the Meniscus and Articular Cartilage
Figure 17-6 Categorization of menisci according to magnetic re sonance imaging ( M RI) results. A, Grade 0: N ormal meniscu s. B, Grade I: M ild intrameniscal signaL C, Grade I I : I ntrameniscal signa l . D, Grade I I I : Complex tear of the medial me niscus.
Eleven patients were over age 45, and four (36%) had positive findings on MRl.30 LaPrade et al.31 found MRl scans to be positive in 5.6% of knees in asymptomatic patients 18 to 39 years of age who had normal physical examination findings.3J
Arthroscopy Arthroscopy is the gold standard for the diagnosis of men iscal tears. Arthroscopic examination allows direct visualization of the tibial and femoral articular surfaces of the
meniscus and the meniscocapsular junction. It also allows visualization of the lateral meniscus at the popliteal hiatus and probing to determine whether hypermobility is present.
Classification of Meniscal Tears
Meruscal tears can be classified as oblique, vertical longitudinal, radial (or transverse), horizontal cleavage, or complex (Figure 17-7). Several authors have evaluated the incidence of these tear patterns. Metcalf et al. 32 determined

Injuries to the Meniscus and Articular Cartilage • C HA PTER 1 7 585
Figure 17-7 Types of meniscal tears.
Oblique (Parrot-beak) tear
Transverse tear Vertical tear Flap tear
Peripheral tear Vertical longitudinal (Bucket-handle) tear
Discoid meniscus; degeneration and tear
Complex tear
that 81% of tears were oblique or vertical longitudinal. As patients get older, the incidence of complex tears increases. Most meniscal pathology is found in the posterior horns.
Oblique tears are most commonly found at the junction of the posterior and middle thirds of the meniscus. These tears are commonly calJed "flap" or "parrot beak" tears (Figure 17-8).
Vertical longitudinal tears, also called "bucket handle" tears, occur most often in young patients. These tears are commonly associated with ACL tears. Binfield et al.33
showed a 9% incidence of bucket handle tears of the medial
Figure 17-8 Arthroscopic view of an oblique (parrot beak) tear of the men iscu s. Symptoms like l y result from the flap getting
caught in the joint and pulling on the meniscocapsular junction. This also could lead to propagation of the tear.
meniscus in ACL-deficient knees. Bucket handle tears occur more often in the medial meniscus, probably because of its more rigid attachments and susceptibility to shear forces. The study by Binfield et al.33 evaluated knees that, on average, had suffered an ACL injury 23.3 months earlier. This interval is sufficient from the time or original injury for knee instability to generate medial meniscal tears. Vertical longitudinal tears occur most often in the posterior horn of the meniscus and can involve the entire meniscus (Figure 17-9).
Bucket handle tears are unstable and, if large enough, can dislocate into the intracondylar region, causing a
586 CHAPTER 1 7 • Injuries to the Meniscus and Articular Cartilage
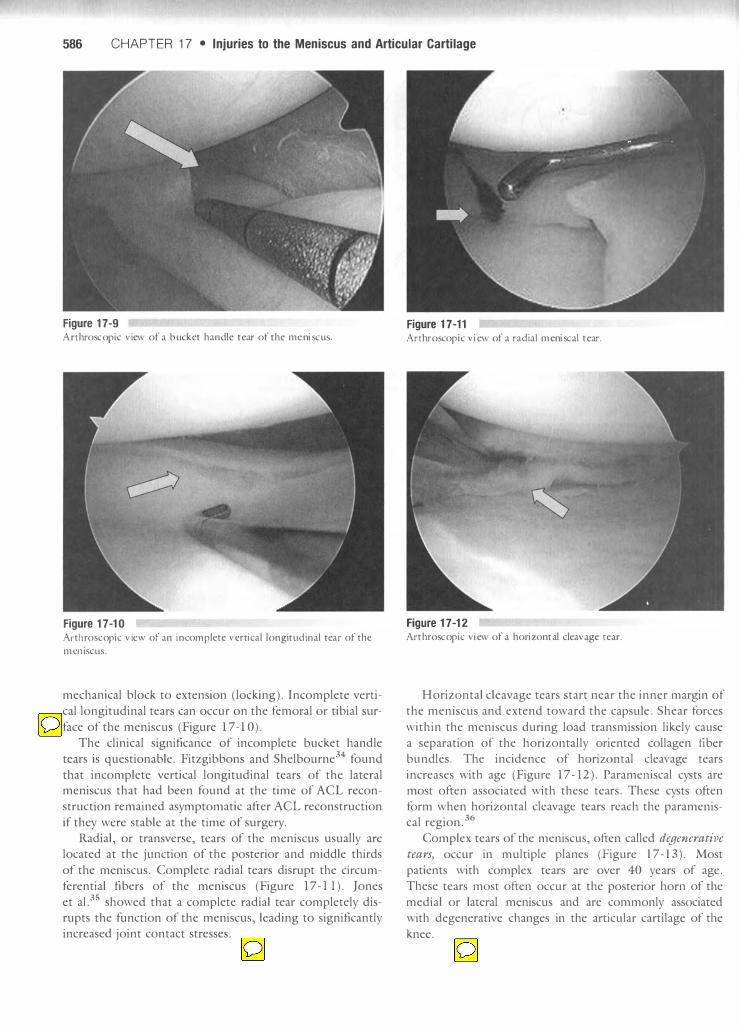
Figure 17-9 Arthroscopic view of a bucket handle tear of the meniscus.
Figure 17-10 Arthro scopic view of an i n complete vertical longitudinal tear of the
meniscus.
mechanical block to extension (locking ). Incomplete verti
cal longitudinal tears can occur on the femoral or tibial sur
face of the meniscus (Figure 1 7- 1 0).
The clinical significance of incomplete bucket handle
tears is questionable. Fitzgibbons and Shelbourne34 found
that incomplete vertical longitudinal tears of the lateral meniscus that had been found at the time of ACL recon
struction remained asymptomatic after ACL reconstruction
if they were stable at the time of surgery.
Radial, or transverse, tears of the meniscus usually are located at the junction of the posterior and middle thirds
of the meniscus. Complete radial tears disrupt the circum
ferential fibers of the meniscus (Figure 17-11) . Jones
et a1.35 showed that a complete radial tear completely disrupts the function of the meniscus, leading to significantly increased joint contact stresses.
Figure 17-11 Arthroscopic view of a radial meniscal tear.
Figure 17-12 Arthroscopic view of a horizontal cleavage tear.
Horizontal cleavage tears start near the inner margin of
the meniscus and extend toward the capsule . Shear forces
within the meniscus during load transmission likely cause
a separation of the horizontally oriented collagen flber bundles . The incidence of horizontal cleavage tears
increases with age (Figure 1 7-12 ). Parameniscal cysts are
most often associated with these tears . These cysts often form when horizontal cleavage tears reach the parameniscal region .36
Complex tears of the meniscus, often called degenerative tears) occur in multiple planes (Figure 17- 13 ) . Most
patients with complex tears are over 40 years of age. These tears most often occur at the posterior horn of the medial or lateral meniscus and are commonly associated
with degenerative changes in the articular cartilage of the
knee.

Injuries to the Meniscus and Articular Cartilage • CHAPTER 1 7 587
Figure 17-13 Arthroscopic view of a complex meniscal tear. Note the shredding of
the meniscus.
Treatment of Meniscal Tears
Indications for Surgical Treatment
Not all meniscal tears require surgical intervention. Before
deciding on surgery for meniscal pathology, the clinician
must exclude other causes of knee pain, such as degenerative
chondral changes. For surgery to be considered, symptoms of meniscal injury should limit activities of daily living, work, or sports. Some meniscal tears heal spontaneously; therefore
a trial of conservative management, with activity modifica
tion and rehabilitation, should be attempted before surgical intervention . Henning et a1.37 showed that some tears heal
spontaneously or remain asymptomatic, including short ver
tical tears (less than 10 mm), stable vertical longitudinal
tears, partial thickness tears (less than 50% of meniscal depth ) on the ti bial or femoral surfaces, and small radial tears
(less than 3 mm ) .
Indications for Meniscal Surgery
• Symptoms limit activities of daily living, work, or sports
• Conservative treatment has not improved symptoms
If the meniscal injury is associated with an ACL injury,
the timing of surgery usually is dictated by the acute rehabilitation after the ACL injury. Factors such as swelling and range of motion dictate the timing of ACL reconstruc
tion. Meniscal pathology usually can be addressed at the
time of ACL reconstruction. If a displaced bucket handle meniscal tear is limiting recovery of extension after an
ACL injury, the meniscal tear should be dealt with on an
urgent basis to allow the patient to regain full extension
before proceeding with ACL reconstruction.
Surgical Intervention
Surgeons should develop a standard approach to knee arthros
copy. A diagnostic arthroscopy of the entire knee should be
performed as the initial portion of all knee arthroscopies. This
diagnostic arthroscopy can be performed in a n umber of ways,
but each surgeon should choose one routine and stick to it to
avoid missing pathology. The final decision as to whether the
meniscal tear should be repaired or excised should be made after the diagnostic arthroscopy. Most meniscal tears are not
amenable to repair. These tears usually require partial menis
cectomy to relieve the patient's pain and mechanical symp
toms. When a partial meniscectomy is performed, as much of the functioning meniscus as possible is left, to maximize
the function of the remaining meniscus and minimize the
effect on joint biomechanics.
Indications for meniscal repair can be divided into patient factors and meniscal factors. Patient factors include the
chronicity of symptoms, the patient's ability to tolerate the
longer rehabilitation required after repair, and the risk of failure of the repair. The patient's age also should be factored
into the equation, because younger patients are likely to have
a greater chance of progression to arthritis after meniscect
omy. Meniscal factors that are favorable for repair include a
complete vertical tear longer than 10 mm, a tear within the
peripheral 10% to 30% or within 3 to 4 mm of the menisco
capsular junction (red-red zone), an unstable tear that can be
displaced by probing, a tear without secondary degeneration
or deformity, and tears in stable knees or associated with concomitant ligamentous reconstruction.30 If both patient
and meniscal factors indicate that the tear is amenable to surgical repair, then repair should be performed.
As previously mentioned, some meniscal tears heal spon
taneously or remain asymptomatic . If one of these tears is
seen at the time of diagnostic arthroscopy and the knee is
stable or is undergoing ACL reconstruction, the meniscus
can be left alone, or trephination (surgical excision of a circular piece of tissue ) and rasping can be performed without surgical stabilization.37 Weiss et al .38 reviewed 52 patients with stable vertical longitudinal meniscal tears (less than 3 mm of displacement with probing ) and performed repeat
arthroscopy. Complete healing was noted in 65% of these
patients. Only six patients required further treatment, and
four of those had suffered a new traumatic event.38
Meniscal Resection Total meniscectomy used to be a very common procedure.
Fairbank39 first described the damaging effects of total
meniscectomy in 1948. As long-term results became available, the progression to osteoarthritis was noted; conse
quently, total meniscectomy has become a very uncommon
procedure.40,41 With arthroscopic techniques, partial menis
cectomy has become feasible (Figure 17-14). When meniscal repair is not indicated, surgeons now
perform a partial meniscectomy. Metcalf et al.32 established

588 CHAPTER 1 7 • Injuries to the Meniscus and Articular Cartilage
Figure 17-1 4 Artshroscopic view of a partial meniscectomy.
guidelines for meniscal resection. All mobile fragments of
the meniscus that can be pulled past the inner margin of the meniscus into the center of the joint should be
resected. The remaining meniscal rim should be smoothed to remove any sudden changes in contour that may lead to
further tearing. A perfectly smootll rim is not necessary. A probe should be used to gain information about me sta
bility or mobility of tile remaining meniscus. The menisco
capsular junction and tile meniscal rim should be retained, if at all possible, to preserve tile load transmission proper
ties of the meniscus. Motorized and manual instruments
should be used. Manual instruments are more accurate,
and motorized shavers can remove loose debris and smoom
frayed edges.
Partial Meniscectomy Studies on the short-term outcome of partial meniscectomy have shown 80% to 90% good results at less man 2-year follow -up.42 A number of long -term follow-up studies have shown progression of artllritis radiographically after partial
meniscectomy. Fauno and Nielsen43 found tllat Witll 8 years
of follow-up, radiographic changes occurred in 53% of
knees that had undergone partial meniscectomy, compared
to 27% of untreated, contralateral knees. Schimmer et al .44
found good or excellent results in 9 1. 7% of partial meniscectomies at 4 years, but this dropped to 78. 1% at 1 2 years.
Articular cartilage damage associated with tile meniscal tear had the greatest impact on tile long-term outcome. Sixty
two percent of patients who had articular cartilage damage
at the time of me index operation had a good or excellent
result at fmal follow-up. In patients Witll no articular carti
lage damage, 94. 8% had good or excellent results.44
Postoperative Rehabilitation. Rehabilitation after
partial meniscectomy usually is uneventful. Postoperatively,
rehabilitation focuses on pain control, joint mobilization
and range of motion (ROM ), gait training, minimization
of effusion, regaining full strength, and a progressive return
to preinjury or preoperative activity. These goals can be
achieved eimer in a formal rehabilitation setting or wim home treatment. Icing and elevation can help minimize
pain and ef fusion in tile knee. ROM exercises can be started
immediately after surgery. Patients may bear weight as tolerated. Quadriceps strengthening exercises can begin
immediately after surgery. Patients should avoid twisting and repetitive inlpact activities for 4 to 6 weeks after
surgery.
Meniscal Cysts As mentioned, meniscal cysts occur most often with hori
zontal cleavage tears. These cysts usually can be decom
pressed at me time of partial meniscectomy from within the joint. Metcalf et al . 32 showed that meniscal cysts rarely recur if the meniscal pamology is dealt with appropriately. The results of arthroscopic decompression of cysts range
from 90% to 100% withom recurrence. If the cyst is not
easily identified from within the joint, a needle can be
passed percutaneously through the cyst into tile joint and
the location of me cyst identified arthroscopically. The cyst
men can usually be decompressed by probing or shaving
from wimin me joint.45,46 If the cyst cannot be decompressed arthroscopically, an open cyst excision should be
performed.
Meniscal Repair Some meniscal tears can heal without fixation. As previ
ously mentioned, meniscal tears that can be left to heal
Witllout fixation include vertical longitlldinal tears less than
10 mm long, incomplete tears, and stable tears that move
less man 3 mm wim probing .34 In such cases, me surgeon
can attempt to enhance tile healing response with abrasion of the synovial surfaces and meniscal trephination 47 Synovial abrasion causes a vascular pannus that migrates into
the tear and helps produce a healing response. Meniscal trephination is a variation of creating vascular access chan
nels. Horizontally oriented holes are made using a spinal
needle tllrough me peripheral vascularized region of the
meniscus. Fox et al.48 showed a 90% success rate in healing incomplete tears wim trephination .
When a meniscal tear is found to be amenable to repair
and tile patient understands the risks of meniscal repair
and tile rehabilitation required (described later in this chapter ), a series of steps must taken to maximize tile chances of
success of tile repair. First, the meniscal bed must be
prepared. Loose edges of the tear should be debrided.
The torn meniscal edges should be abraded with a rasp or
shaver. Rasping of the synovial fringe is also helpful in cre
ating a synovial pannus that can creep into the tear and aid
the healing response. Tears that extend into the avascular
zone have a lower healing rate. Some think that this can
be improved somewhat with trephination.

Injuries to the Meniscus and Articular Cartilage • CHAPTE R 1 7 589
Open Repair Techniques. Open meniscal repair was
first repor ted by Annandale49 in 1 88 5 . Meniscal repair did not become widely used until it was popularized by
De Haven50 and Wir th .51 Open meniscal repair currently
is most useful with multiple-ligament injuries in which the collateral ligament injuries may require open repair or tibial
plateau fractures require open reduction and internal fixa
tion . With open repair, the meniscus can be sutured directly. The success rate for open meniscal repair is high in multiple-ligament injuries, likely because of tlle periph
eral nature of the tears and the acuteness of the injury
and the ensuing hemarthrosis . Rockborn and Gillquist52
reported a 7 1 % success rate in a 1 3-year follow-up of
patients with open meniscal repairs. Some surgeons still
advocate open meniscal repair, suggesting tlut meniscal
preparation and suturing are more readily achieved with
an open approach and that the incisions do not need to
be much larger than with inside -out ar throscopic repairs . Arthroscopic Repair. Arthroscopy allows evaluation
and treatment of meniscal tears that are not possible with open techniques . Three basic suturing techniques have been used wIth ar throscopic procedures : the inside-out
technique, the outside-in technique, and the all-inside
technique . Arthroscopic repairs also can be performed
using bioabsorbable implants and suture anchors .
Inside-Out Technique. The inside -out technique was
first popularized by Henning et al . 37 in tlle early 1 980s .
This technique uses double-armed sutures witll long needles, which are positioned through ar throscopically
directed cannulas . Skin incisions are then made between
the two needles . Soft tissues are dissected down to the cap
sule, with care taken that no neurovascular str uctures are
trapped between the sutures, and tlle sutures are then tied,
reducing the meniscus . A significant advantage of this tech
nique is that it allows accurate suture placement in the
meniscus . The main disadvantage of this technique is the
risk to neurovascular structures and the need for incisions between tlle sutures .
When this technique is performed on the medial side of the knee, branches of the saphenous nerve are most com
monly injured . 53 Injuries to the saphenous nerve can cause localized numbness or a painful neuroma . The standard
medial incision is a vertical incision approximately 3 cm
( 1 .2 inches ) long that star ts just above the joint line and
runs distally. The incision is made witll the knee in 90° flexion . The in frapatellar branch of the saphenous nerve runs
approximately 1 cm (0 .5 inch ) proximal to the joint line . The saphenous nerve usually lies below tlle subcutaneous
fat on tlle deep fascia covering the sar torius muscle . Keeping the knee in 90° flexion allows the sar torius and
saphenous nerve to fall posteriorly. Once the subcutaneous
tissue has been bluntly dissected down to the sar torius fas
cia , the fascia is opened in the direction of i ts fibers and a
plane is dissected down to tlle knee joint capsule. A retrac
tor can then be placed in tllis plane, protecting the
saphenous nerve . The needles can be visualized as they pass
tllrough the capsule .
On the lateral side of the knee, tlle peroneal nerve is
most at risk . The popliteal ar tery and tibial nerve are at risk
as the sutures move more posteriorly. The lateral capsule
should be exposed before needles are inser ted from within
tlle knee joint. An incision is made on the lateral side of
the knee just posterior to the fibular collateral ligament. Again , dissection is performed with the knee in 90° flexion .
The peroneal nerve is protected by finding tlle interval between the biceps femoris and the iliotibial band and
retracting the biceps and peroneal nerve posteriorly. The
lateral gastrocnemius muscle is found and its fascia is
divided in the direction of i ts fibers. Fibers of the lateral
head of the gastrocnemius are dissected off of the posterior
capsule . A retractor then can be placed posteriorly in tlle
knee to protect the neurovascular structures. Once this dis
section has been per formed , needles can be safely passed from inside the knee and retrieved as they exit the capsule , without risk of neurovascular injury.
After tlle appropriate exposure and neurovascular pro
tection have been obtained , attention can be returned
to the meniscal pathology. The menisca I bed is prepared (Figure 1 7- 1 5 ), and sutures tllen can be passed through
the meniscus , exiting tlle knee joint capsule . The sutures
should be passed in a ver tical mattress pattern for maximum
strength ; ideally, tlley should be placed at 2 to 3 mm intervals (Figure 1 7- 1 6 ) .54
Outside-In Technique. The outside-in technique was
developed as an attempt to avoid the neurovascular compli
cations that can occur with the inside-out technique . The
outside-in technique uses a spinal needle passed percutane
ously through tlle subcutaneous tissue , through the menis
cal tear, into the knee joint. A suture tllen is passed into tlle
join t through the needle and brought out through the
anterior portal . A knot is tied in the free end of the suture ,
Figure 17-15 Arthroscopic view of a bleeding edge in the red zone of the men isclls.
590 CHAPTER 1 7 • Injuries to the Meniscus and Articular Cartilage
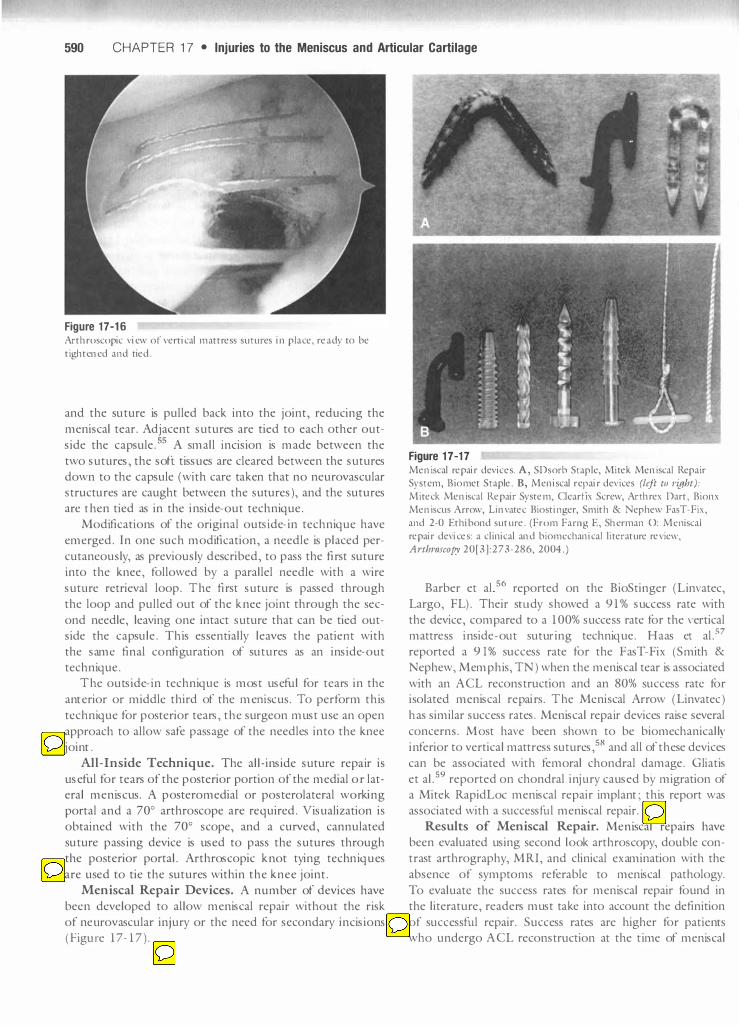
Figure 17-16 Arthroscopic view of vertical mattress sutures in place, ready to be tightened and tied .
and the suture is pulled back into the joint, reducing the
meniscal tear. Adjacent sutures are tied to each other out
side the capsule. 55 A small incision is made between the
two sutures, the soft tissues are cleared between the sutures down to the capsule (with care taken that no neurovascular structures are caught between the sutures ), and the sutures are then tied as in the inside-out technique.
Modifications of the original outside-in technique have
emerged. In one such modification, a needle is placed per
cutaneously, as previously described, to pass the first suture into the knee, followed by a parallel needle with a wire
suture retrieval loop. The first suture is passed through
the loop and pulled out of the knee joint through the sec
ond needle, leaving one intact suture that can be tied outside the capsule. This essentially leaves the patient with
the same final configuration of sutures as an inside-out technique.
The outside-in technique is most useful for tears in the
anterior or middle third of the meruscus. To perform this
technique for posterior tears, the surgeon must use an open
approach to allow safe passage of the needles into the knee joint .
All-Inside Technique. The all-inside suture repffir i s
useful for tears of the posterior portion of the medial or lateral meniscus. A posteromedial or posterolateral working
portal and a 700 arthroscope are required. Visualization is
obtained with the 700 scope, and a curved, cannulated
suture passing device is used to pass the sutures through the posterior portal. Arthroscopic knot tying techniques
are used to tie the sutures within the knee joint.
Meniscal Repair Devices. A nu mber of devices have
been developed to allow meniscal repair without the risk
of ne urovascular injury or the need for secondary incisions ( Figu re 1 7- 1 7 ).
Figure 17-17 Meniscal repair d evic es. A, SDsorb Staple, Mitek Meniscal Repair System, B iomet Staple. B, M eniscal repair d evices (left to t'ight):
Miteck Meniscal Repair System, Clearfix Screw, Arthrex Dart, Bionx Meniscus Arrow, Li nvatec Biostinger, Smith & N ephew FasT-Fix,
and 2-0 Ethibond suture. (From Farng E, Sherman 0: Mcniscal repair d evices: a c l inical and biomcchanical li terature review, Arthroscopy 20[3] :273-286, 2004 . )
Barber et al S6 reported on the BioStinger (Linvatec,
Largo, FL). Their sUldy showed a 9 1 % success rate with
the device, compared to a 1 00% success rate for the vertical mattress inside -ollt suturing technique. Haas et al.57
reported a 91% success rate for the FasT-Fix (S mith &
Nephew, Memphis, TN ) when the meniscal tear is associated
with an ACL reconstruction and an 80% success rate for i solated meniscal repffirs. The Meniscal Arrow (Linvatec )
has similar success rates. Meniscal repffir devices raise several
concerns. Most have been shown to be biomechanically
inferior to vertical mattress sutures,58 and all of these devices
can be associated with femoral chondral damage. Gliatis
et a I. 59 reported on chondral injury caused by migration of a Mitek RapidLoc meniscal repair implant ; this report was associated with a sllccessful meniscal repair.
Results of Meniscal Repair. Meniscal repairs have been evaluated using second look arthroscopy, double con
trast arthrography, M R I, and clinical examination with the
absence of sy mptoms referable to meniscal pathology.
To evaluate the success rates for meniscal repair found in the literature, readers must take into account the definition
of successful repair. Success rates are higher for patients who undergo ACL reconstruction at the time of meniscal

Injuries to the Meniscus and Articular Cartilage • CHAPTER 1 7 591
repair than for patients who have isolated meniscal repairs.
When meniscal repair success rates are evaluated, patients
who had concomitant ACL reconstruction must be
grouped separately and the length of follow-up must be
critically evaluated. Studjes have been published on the
short -term results of meruscal repair, but success rates
decline if patients are followed for longer than 2 years.
Albrecht -Olsen et al60 reviewed 27 patients at a median
3-year tallow-up, using a clinical examination to determine success. They showed a 63% success rate, and all knees were
stable. Buseck and Noyes61 reviewed 66 repairs associated
with ACL reconstruct ion. All patients underwent second
look arthroscopy. Eighty percent were completely healed,
1 4% were partially healed, and 6% failed. Ninety -eight percent of tears in the outer one third healed. Cannon and
Vittori62 looked at stable knees and knees that underwent ACL reconstruction at the time of meruscal repair. Of the
stable knees , 50% healed, whereas 90% of the knees that
underwent concomitant ACL reconstruction healed. Healing was con firmed with arthroscopy or an arthrogram.
Rubman et al 63 evaluated 198 meniscal tears that
extended into the avascular (white ) zone. Clinical examina
tion showed that 80% of these patients had no symptoms
referable to meniscal pathology. Second look arthroscopy
was performed in the 20% who had symptoms. Of the
39 knees that underwent second look arthroscopy , only
two tears were healed. Thirteen tears were partially healed, and 24 had fa jled . In the entire group, 9 1 repairs were evaluated arthroscopically. Of these menisci , 2 5% were healed,
Table 1 7-1
Rehabilitation Protocol After Meniscal Repair
Weeks 1 -2 Weeks 3-4 Weeks 5-6
Brace Immobil ized Immobilized No brace
Weight NWB PWE WE as bearing tolerated
R.1nge of 0°_900 00_900 00- 1 200 motion
Exercises Isometric Isometric Begin closed Quad Quad chain Exercises Exercises exercises
• Quadsets • Quad sets • SLR • SLR
Manual Patellar Patellar and Patellar and therapy mobilization joint joint
mobilization mobilization Passive ROM Passive ROM to 900 to 1 200
38% were partially healed, and 36% failed. Seventy-three
percent of the patients with unhealed menisci had symptoms referable to the tibiofemoral joint.
Indicators of Successful Meniscal Repairs
• Repairs are done at the same time as ACL reconstruction
• Lateral meniscal repairs are more successful than medial
meniscal repairs
• Tear is in the peripheral one third of the meniscus
• A functioning meniscus is present
Postoperative Rehabilitation. Rehabilitation after
meniscal repair depends on whether ACL reconstruction
was per formed at the same time. Although many protocols exjst, the principles of rehabibtation include an irutial period
of non-weight-bearing and limitation of flexion. Standard meniscal repair guidebnes are presented in Table 1 7- 1.
If ACL reconstruction is per formed concomitantly with the meniscal repair, more aggressive ROM exercises should
be performed. Flexion should be limited to 90° for tlle first
4 to 6 weeks. Arnoczky et al.64 showed that the meniscus is
subject only to small amounts of motion and stress between
1 5° and 60° flexion. After 6 weeks, more aggressive closed
bnetic chain activities can be started. Return to pivoting sports should not be allowed before 6 months.
Complications of Meniscal Repair. The most common complication of meniscal repair is failure of healing
Weeks 7-8 Weeks 9 - 1 6 Weeks 1 7-20 Weeks 2 1 -24
No brace No brace No brace No brace
WE as WE as WE as WE as tolerated tolerated tolerated tolerated
Full ROM Full ROM Full ROM Full ROM
Closed chain Closed chain Running, Cutting exerCises exerCises straight
Hamstrings Hamstrings Stationary Stationary
bike bike Stair climber
Patellar and joint mobil ization
NWB, Non- weight-bearing; PWB, partial weight bearing; WB, weight bearing; ROM, range of motion.

592 C HA PTER 1 7 • Injuries to the Meniscus and Articular Cartilage
and the need for subsequent partial meniscectomy. Other complications specifically associated with meniscal repair include injury to the saphenous nerve or vein, injury to the peroneal or tibial nerve, and injury to the popliteal artery or vein. Loss of motion after repair also can be associated with meniscal repairs.53,65,66 Deep vein thrombosis, pain, infection, and hemarthrosis can occur but are not seen at a higher rate than with partial meniscectomy. Shelbourne and Johnson67 reported a 25% incidence of stiffness when ACL reconstruction is performed at the same time as repair of a locked bucket handle meniscal tear. Meniscal repair performed at the same time as ACL reconstruction does appear to be a risk factor for postoperative stiffuess; however, meniscal healing rates are higher when meniscal repair and ACL reconstruction are performed at the same time.
Complications of Meniscal Surgery
• Nerve injury (saphenous, peroneal, tibial)
• Vascular injury (saphenous, popliteal)
• Loss of range of motion (stiffness)
• Deep vein thrombosis
• Pain
• Infection
• Hemarthrosis
Meniscal Transplantation Transplantation of the meniscus was first described by Milachowski et al.68 in 1 989. The experience with human meniscal transplantation was preceded by clinical studies in animals and cadavers. Cadaveric models have shown decreased contact pressures and increased contact surface areas after meniscal transplantation. Both the anterior and posterior horns of the meniscus must be securely attached in their anatomical positions to gain these biomechanical advantages. When both anterior and posterior attachments are released, the decrease in contact stresses is completely lost. If one attachment site is lost, some biomechanical benefit is obtained, but it is significantly reduced.69
Arnoczky et al?O transplanted cryopreserved medial meniscal allografts in 1 4 dogs. These menisci healed to tl1e capsule by fibrovascular scar. At 3 months they maintained a normal gross appearance. Histological studies showed that the transplanted menisci maintained a normal cellular distribution. Jackson et al 71 used a goat model to compare autograft to fresh allograft and cryopreserved allograft. At 6
months, the implanted menisci appeared very similar histologically to the controls. A slight decrease was seen in the cellularity in tl1e central portions of tl1e menisci. Peripheral vascularity was almost normal. The water content of the meniscus was increased and tl1e proteoglycan content was decreased compared to controls. In another study, Fabriciani et al. 72 demonstrated little difference between cryopreserved and deep-frozen meniscal transplants. Their study showed
nearly complete remodeling at 6 and 1 2 months. Debeer et al.73 showed tlut 95% of the dem .. ,),ribonucleic acid (DNA) in a human transplanted meniscus was identical to that of the recipient at 1 year, which indicated that the host bad repopulated the meniscal cells.
Indications for Meniscal Transplantation. The ideal patient for meniscal transplantation is one who previously bas undergone complete or near complete meniscectomy and has joint line pain, early chondral damage, a stable knee, and normal lower limb alignment. Meniscal transplantation can be considered at the same time as ACL reconstruction in an ACL-deficient knee. If axial malalignment is present, tibial or femoral osteotomy should be considered to correct it. Meniscal transplantation is contraindicated in patients with advanced chondral changes.74 At tl1is point, no evidence supports meniscal transplantation in asymptomatic patients who have undergone complete or near complete meniscectomy. As longer term results become available, the indications may expand to cover asymptomatic young patients with complete meniscectomies.
Indications for Meniscal Transplantation
• Previous complete or near complete meniscectomy
• Joint line pain
• Early chondral damage
• Stable knee
• Normal lower limb alignment
Graft Sizing. Graft SIZIng is extremely important. To obtain the beneficial biomechanical effects of meniscal transplantation, tl1e transplanted meniscus should vary less than 5% from the original meniscus. Various studies have used computed tomography (CT) scans, MRI, and plain radiography for meniscal allograft sizing. A study by Shaffer et al.74 showed that MRI was accurate to within 5 mm of width and length measurements in 84% of cases, compared to 79% of cases measured with plain radiographs. Most tissue banks use plain radiographs for allograft sizing.75
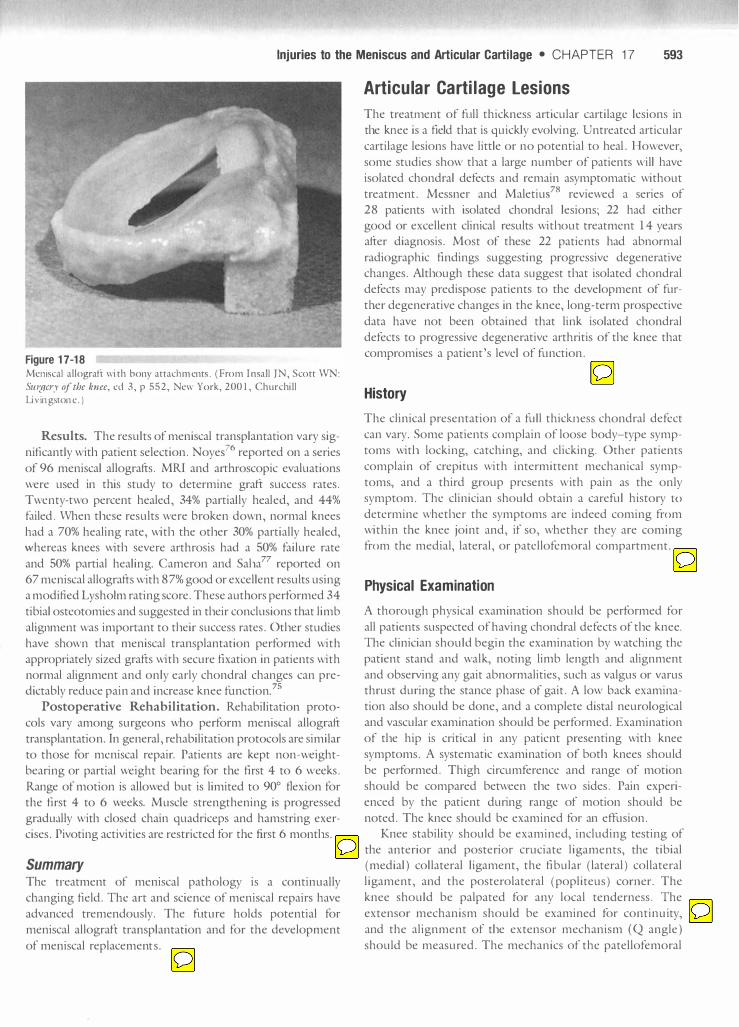
Surgical Technique. The insertion of meniscal allografts has been described using an open technique with collateral ligan1ent detachment, an open technique without collateral ligament detachment, and an arthroscopically assisted technique. The results of meniscal transplantation seem to depend on patient selection, graft sizing, and secure graft fixation more than surgical technique. As described previously, to increase the contact surface area and reduce contact stresses, the surgeon must securely fix tl1e anterior and posterior horns. Soft tissue fixation, fixation with bone plugs, and fixation with a bony bridge inserted into a trough in the tibial plateau have been described as techniques for secure anterior and posterior horn fixation (Figure 1 7- 1 8 ) .
Injuries to the Meniscus and Articular Cartilage • CHAPTER 17 593
Figure 17-18 Meniscal a l lograft with bony attach ments. ( From I n saJl IN, Scott WN: Stt1lJcry of the knee, cd 3, p 552, New York, 200 1 , Churchill Livingstone . )
Results. The results of meniscal transplantation vary significantly witl1 patient selection. Noyel6 reported on a series of 96 meniscal allografts. MRI and ariliroscopic evaluations were used in mis study to determine graft success rates. Twenty-two percent healed, 34% partially healed, and 44%
failed. When tl1ese results were broken down, normal knees had a 70% healing rate, witl1 the otl1er 30% partially healed, whereas knees witl1 severe arthrosis had a 50% failure rate and 50% partial healing. Cameron and Salla77 reported on 67 meniscal allografts with 87% good or excellent results using a modified LyshoLm rating score. These aumors performed 34
tibial osteotomies and suggested in tl1eir conclusions mat limb alignment was important to tl1eir success rates. Otl1er studies have shown tl1at meniscal transplantation performed with appropriately sized grafts witll secure fixation in patients with normal alignment and only early chondral changes can predictably reduce pain and increase knee function?5
Postoperative Rehabilitation. Rehabilitation protocols vary among surgeons who perform meniscal allograft transplantation. In general, rehabilitation protocols are similar to those for meniscal repair. Patients are kept non-weightbearing or partial weight bearing for me first 4 to 6 weeks. Range of motion is allowed but is limited to 90° flexion for the first 4 to 6 weeks. Muscle strengthening is progressed gradually witl1 closed chain quadriceps and hamstring exercises. Pivoting activities are restricted for me first 6 montl1s.
Summary The U'eatment of meniscal pathology is a continually changing field. The art and science of meniscal repairs have advanced tremendously. The future holds potential for meniscal allograft transplantation and for me development of meniscal replacements.
Articular Cartilage lesions
The treaU11ent of full thickness articular cartilage lesions in tl1e knee is a field tl1at is quickly evolving. Untreated articular cartilage lesions have little or no potential to heal . However, some studies show tl1at a large number of patients will have isolated chondral defects and remain asymptomatic without treatment. Messner and Maletiul8 reviewed a series of 28 patients with isolated chondral lesions; 22 had either good or excellent clinical results witl10ut treatment 1 4 years after diagnosis. Most of mese 22 patients had abnormal radiographic findings suggesting progressive degenerative changes. Altl10ugh mese data suggest tl1at isolated chondral defects may predispose patients to the development of furmer degenerative changes in the knee, long-term prospective data have not been obtained that link isolated chondral defects to progressive degenerative arthritis of tl1e knee that compromises a patient's level of function.
History
The clinical presentation of a full thickness chondral defect can vary. Some patients complain of loose body-type symptoms witl1 locking, catching, and clicking. Other patients complain of crepitus with intermittent mechanical symptoms, and a third group presents with pain as the only symptom. The clinician should obtain a careful history to
determine whetl1er the symptoms are indeed coming from within me knee joint and, if so, whether they are coming from me medial, lateral, or patellofemoral compartment.
Physical Examination
A thorough physical examination should be performed for all patients suspected of having chondral defects of tl1e knee. The clinician should begin the examination by watching the patient stand and walk, noting limb lengtl1 and alignment and observing any gait abnormalities, such as valgus or varus thrust during me stance phase of gait. A low back examination also should be done, and a complete distal neurological and vascular examination should be performed. Examination of tl1e hip is critical in any patient presenting witl1 knee symptoms. A systematic examination of botl1 knees should be performed. Thigh circumference and range of motion should be compared between tl1e two sides. Pain experienced by me patient during range of motion should be noted. The knee should be examined for an effusion.
Knee stability should be examined, including testing of the anterior and posterior cruciate ligaments, the tibial (medial) collateral ligament, the fi bular (lateral) collateral ligament, and the posterolateral (popliteus) corner. The knee should be palpated for any local tenderness. The extensor mechanism should be examined for continuity, and the alignment of tl1e extensor mechanism (Q angle) should be measured. The mechanics of the patellofemoral

594 C HA PTER 1 7 • Injuries to the Meniscus and Articular Cartilage
ar ticulation should be exa mined, and the clinician should
observe for a J sign ( i . e ., deviation of the patella cephali
cally and la terally in the pattern of an upside-down J) , lat
eral tilt of the patella, lateral retinacular tightness, and
patellofemoral crepitation .
Diagnostic Imaging
Diagnostic imaging should begin with plain radiographic
fil ms. A standing PA flexion view should be included in
the standard knee series. A tangential view of the patellofe
moral joint (e .g., Merchant view ) should also be included .
These plain radiographic films can show joint space narrow
ing, osteochondral defects, and patellofemoral tilt or sub
luxation . However, isolated chondral defects often cannot be seen on plain radiographic films .
The i maging s tudy of choice for chondral defects is M R I because of its excellent sensitivity and specificity for this type of lesion. Bredella et al .79 reported on 1 30 patients under
going knee ar throscopy for suspected internal derange
ment. Of 86 ar throscopically proven abnormalities, 8 1
were detected with M R I . M R I done with a T 2-weighted, fast
spin-echo sequence with fat saturation had a sensitivity
of 94% and a specificity of 99% compared to ar throscopy (Figures 1 7- 1 9 and 1 7-20) .
Nonoperative Management
The goal of nonoperative management of chondral lesions
is to minimize symptoms and allow maximum activity .
Maintenance of range of motion, muscle s trength ening,
and a variety of therapeutic modalities to reduce pain and
Figure 17-19 T r we ighted MRl scan of a chondral defect ( outlined by lVhite dotted
line) of the p osterior condyle.
Figure 17-20 T I - weighted MR1 scan of a trochlear chondral defect (circled).
inflammation all can minimize sy mptoms . Orthotics, bracing, and gait tra ining can minimize the stresses on the
affected region of the joint. Weight loss in overweight
patients can dramatically improve sy mptoms by reducing
patellofemoral and tibiofemoral contact stresses.
Surgical Management
The ultimate goal of surgical treatment is restoration of the
microarchitecture of the articular car tilage, which allows
complete restoration of the biomechanical and physiologi
cal function of the knee. A number of techniques for car ti
lage repair and regeneration have been developed . The
following sections present a detailed look at each of these
modal ities and review the basic science, surgical techniques, and rehabilitation principles and results.
Abrasion Arthroplasty The idea of doing something to eburnated bone to cause a
reparative tissue response was first proposed by Pridie80 in
1959. He recom mended joint debridement, removal of
osteophytes, retention of the patella, shaving of fissured
articular car tilage, and drill ing of eburnated bone . He
described fibrous, reparative-type tissue filling and covering 0 .5 cm (0 .25 inch ) cortical drill holes through the femoral
condyle. Most of his poor results involved patients in
whom he also performed a patellectomy. Akeson et al.8 1
attempted to confirm Pridie's findings in laboratory ani
mals. They removed the ar ticular cartilage and subchondral
bone of dog femoral heads . At I-y ear follow-up, they con
cluded that excessive loading destroy ed the initial reparative
tissue . These results also showed that the proteoglycan con
centrations in the reparative tissue were less than half
that of nor mal ar ticular car tilage . Mitchell and Shepard82

Injuries to the Meniscus and Articular Cartilage • C HA PTER 1 7 595
studied rabbit knee joints. They found that after multiple
small holes were drilled into the subchondral bone, repara
tive tissue was stimulated to cover large areas of articular s ur
faces . The reparative tissue grew out f rom the drill holes and
then spread over the exposed bone. This tissue began to
fibrillate and break down within 1 y ear 82 These two studies
were the first to demonstrate that a fibrocartilaginous repair
tissue could be stimulated to form on large areas of articular surface. However, these studies also showed that this rep ara
tive tissue did not have the proteoglycan concentration of articular cartilage and that it started to break down quickly
with excessive loading.
Abrasion arthroplasty using motorized instrumentation
was introduced by Johnson83 in 198 1 . Whether the abra
sion should be int racortical or cancellous bone should be
exposed is the subject of debate. Hjertquist and Lemperg84
reported that cartilage tissue of mature appearance forms
only if the debridement is superficial enough to maintain a cortex .
Surgical Technique. The procedure introduced by
Johnson in 1981 is essentially an extension of that described
by Pridie . Along with debridement of the joint , a superficial
lay er of subchondral bone (1 to 3 mm deep ) is removed to
expose interosseous vessels. This theoretically results in a
hemorrhagic exudate that forms a fibrin clot and allows
fibrous repair tissue to form over the area of exposed bone.
Rehabilitation. Regeneration of articular cartilage benefits from motion and from limiting the compressive force on the articular cartilage from weight bearing. P at ient
adherence to a program of motion with limited or no
weight bearing is critical. To assist with this , the use of continuous passive motion (C P M ) often is considered. Weight
bearing often is restricted for up to 12 weeks, with daily CPM, especially in the early postoperative period. Active
and passive range of motion are encouraged throughout the postoperative course until weight bearing and strength training can begin.
Results. Eight knees were biopsied in Johnson 's original series.83 Of those eight biopsy specimens, only one showed
any type II collagen typical of hyaline cartilage. All other biopsy specimens showed a combination of type I and type
I I I collagen. Bert and Maschka85 reviewed a series of 59
patients who ullderwent abrasion arthroplasty with a mini
mum 5-y ear follow-up. Of the 59 patients , 1 5 h ad conver
sion to total knee arthroplasty. Biopsies were performed on
any remaining fibrous tissue. The fibrous tissue was stained
with safranin 0 to look for proteoglycan. The fibrous surf ace
did not stain , indicating the lack of proteoglycan.
Microfracture Microfracture cm be performed on the patellar, tibial, or
femoral articular surface. The general indication for micro
fracture is a full thickness chondral defect in either a
weight-bearing region or a region of contact between the
femur and patella. Microfracture can also be performed after
debridement of unstable chondral flaps. Contraindications
to microfracture include axial malalignment , partial thickness chondral defects , and a patient who is unable or unwilling to
comply with a strict postoperative rehabilitation protocol ,
including minimal weight bearing . Joint space n arrowing,
chronic lesions , and inability to use a C P M machine may affect the outcome but are not su-ict con u-aindications .
Surgical Technique. Microfracture can be performed arthroscopically with a combination of shavers , curets , and
picks. The technique h as been described by Steadman
et al .86 Three portals are made, allowing use of an inflow
canula, the arthroscope, and the working instruments. A diag
nostic arthroscopy is performed, and the full thickness chon
dral defect is identified. Any other work that needs to be
performed in the knee is completed before the microfracture
p rocedure is begun. The chondral defect is then inspected ,
and all cartilage remnants are debrided (Figure 17-21 ) .
The articular cartilage surrounding the defect is inspected and any loose, delaminated cartilage is removed.
A perpendicular edge of healthy cartilage is obtained ci rcumferentially around the lesion . The calcifi ed cartilage
lay er is removed , which care taken not to debride through the subchondral plate .
An arthroscopic awl with the appropriate angle then is used to create perforations in the subchond ral plate th at
are perpendicular to the surface. The awl allows the
surgeon to make holes (microfractu res ) in the subchondral
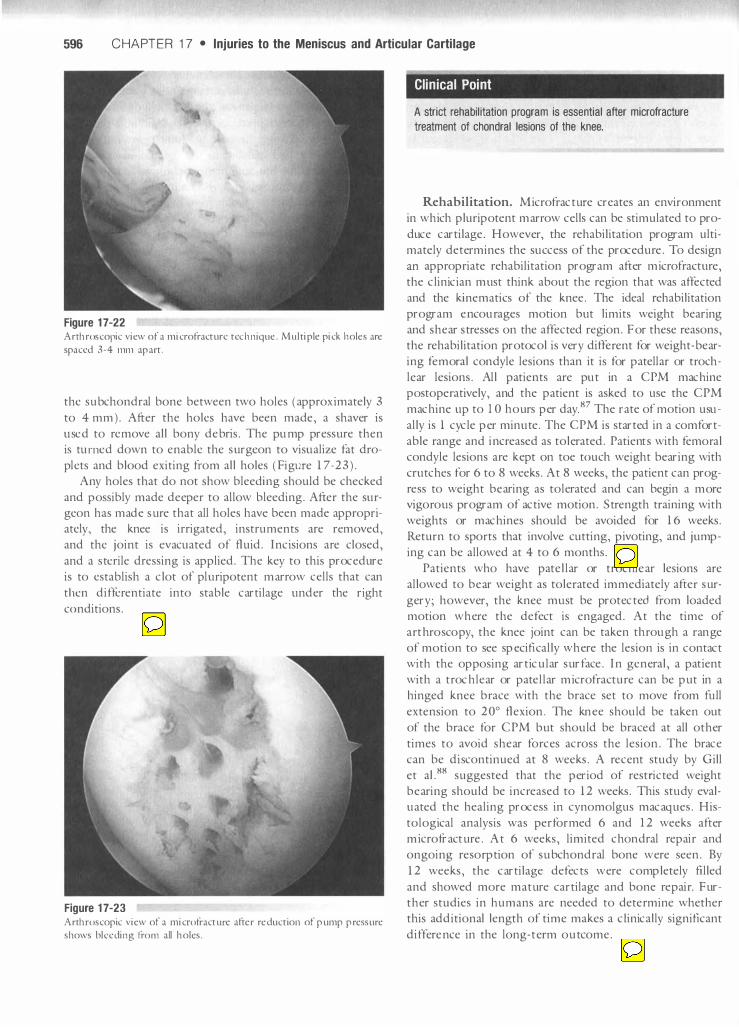
bone with control and without any worry of heat necrosis (Figure 17-22 ) . Attention fi rst is given to the periphery of
the lesion . Holes are made at 3 to 4 mm intervals around
the periphery and are approximately 3-4 mm deep. Once the holes have been made around the periphery, the remaining surface of the lesion is addressed . Holes should
be spaced as close together as possible without fracturing
Figure 17-21 Arthroscopic view of a chondral defect debrided to subchondral bone. The calcified cartilage layer has been removed .
596 C HA PTER 1 7 • Injuries to the Meniscus and Articular Cartilage
Figure 17-22 Arthroscopic view of a microfracture tech n ique. Multiple pick holes are
spaced 3-4 mm apart.
the subchondral bone between two holes (approximately 3
to 4 mm ). After the holes have been made, a shaver is
used to remove all bony debris. The pump pressure then is tu rned down to enable the s urgeon to visualize fat dro
plets and blood exiting fj·om all holes ( Figure 1 7-23 ) . Any holes that do not show bleecling should be checked
and possibly made deeper to allow bleeding. After the surgeon has made sure that all holes have been made appropriately, the knee is i rrigated, instruments are removed,
and the joint is evacuated of fluid. Incisions are closed,
and a sterile dressing is applied. The key to this procedure
is to establish a clot of pl uripotent marrow cells that can
t hen differentiate into stable cartilage under the right
conditions.
Figure 17-23 Arthroscopic view of a microfracture after reduction of pump pressure shows bleeding from all holes.
Clinical Point
A strict rehabilitation program is essential after microfracture
treatment of chondral lesions of the knee.
Rehabilitation. Microfracture creates an environment
in which pluripotent marrow cells can be stimulated to pro
duce cartilage. However, the rehabilitation program ultimately determines the success of the procedure. To design
an appropriate rehabilitation program after microf racture,
the clinician m ust think about the region that was affected
and the kinematics of the knee. The ideal rehabilitation
program encourages motion but limits weight bearing and shear stresses on the affected region. For these reasons, the rehabilitation protocol is very different for weight-bear
ing femoral condyle lesions than it is for patellar or troch lear lesions. All patients are put in a C PM machine postoperatively, and the patient is asked to use the C PM
machine up to 1 0 hours per day 87 The rate of motion usu
ally is 1 cycle per minute. The C PM is started in a comfort
able range and increased as tolerated. Patients with femoral condyle lesions are kept on toe touch weight bearing with
crutches for 6 to 8 weeks. At 8 weeks, the patient can prog
ress to weight bearing as tolerated and can begin a more vigoro us program of active motion. Strength training with
weights or machines should be avoided for 1 6 weeks.
Return to sports that involve cutting, pivoting, and jump
ing can be allowed at 4 to 6 months.
Patients who have patellar or trochlear lesions are
allowed to bear weight as tolerated immediately after sur
gery ; however, the knee must be protected from loaded motion where the defect is engaged. At the time of a rthrosco py, the knee joint can be taken th rough a range of motion to see specifically where the lesion is in contact with the opposing articular surface. In general, a patient
with a t rochlear or patellar microf racture can be put in a hinged knee b race with the brace set to move from full
extension to 20° flexion. The knee should be taken out
of the brace for C PM b ut should be braced at all other
times to avoid shear forces across the lesion. The brace
can be discontinued at 8 weeks. A recent study by Gill
et aL88 suggested that the period of restricted weight bearing should be increased to 1 2 weeks. This study evaluated the healing process in cynomolgus macaques. His
tological analysis was performed 6 and 1 2 weeks after
microfracture. At 6 weeks, limited chondral repai r and
ongoing resorption of subchond ral bone were seen. By
1 2 weeks, the cartilage defects were completely filled
and showed more mature cartilage and bone repai r. Further studies in humans are needed to dete rmine whether this additional length of time makes a clinically significant
difference in the long-term outcome.

Injuries to the Meniscus and Articular Cartilage • CHAPTER 1 7 597
Results. Steadman et al .89 looked at a series of 75
knees in 72 patients who underwent microfracture for full
thickness traumatic chondral defects. Follow-up was 7 to
17 years . Their three inclusion criteria were (1 ) a traumatic
full thickness chondral defect, (2 ) no meniscal or ligamen
tous injury, and (3) patient age under 45 years . Significant
improvements were found according to the Lysholm and
Tegner knee rating scales . At 7 years after surgery, 80% of
patients stated that they were better than before surgery . Some patients took u p to 2 years to obtain maximum
improvement. Kn utsen et a1 90 performed a randomized
clinical trial comparing microfracture and autologous chon
drocyte implantation (AC I ) for isolated chondral defects . Eighty patients were enrolled in the study. Microfracture
was performed on 40 patients, and AC I was performed
on the other 40. An independent observer performed the follow-up data collection at 1 2 and 24 months. Both
groups showed improvement . According to the Short
Form-36 (SF-36) outcome measurement tool, the microfracture group had a significantly greater improvement . Biopsy specimens were obtained from 84% of patients at
2 years. Hi�tological evaluation of repair tissues showed
no significant differences between the two groups . Interest
ingly, no association was found between the histological
specimens and the clinical outcome, according to the
Lysholm scale, t ile SF-36, and a visual analog scale.
Mosaicp/asty Autologous osteochondral grafting has shown great promise in that it is a means to transplant bone and hyaline car
tilage to a region of a chondral or osteochondral defect. Lane et al.9 1 showed that the hyaline cartilage remains via
ble 12 weeks after transfer . However, two problems were
encountered wi t il single plug osteochondral transfers :
donor site morbidity and s urface incongruity at the recipi
ent site . Mosaicplasty was developed in an attempt to mini
mize these problems. Mosaicplasty involves the transfer of multiple small osteochondral plugs to a region of chondral or osteochondral defects. The use of multiple small grafts allows for maintenance of donor site integrity and contouring of the new surface .
Surgical Technique. A utologous osteochondral
mosaicplasty involves harvesting and transferring small ,
cylindrical osteochondral grafts (2 .7 to 8 . 5 mm in diame
ter ) from the periphery of the femoral condyles at the level of the patellofemoral joint (Figure 1 7-24) . The cylindrical
grafts are then transplanted to prepared recipient sites in
the region of the chondral or osteochondral defect . Combination of different graft sizes allows for cover
age of approximately 80% of the lesion . The areas
between the osteochondral cylinders are filled with fibro
cartilage . At the time of the procedure , a diagnostic
arthroscopy is performed. The chondral or osteochondral
defect is identified and inspected . All loose cartilage frag
ments are debrided back to stable , normal articular
Figure 17-24 View of a graft donor site on the periphery of the bteral fe moral condyle.
cartilage . The defect then is sized to determine the num
ber and sizes of grafts needed . If the defect can be
accessed adeq uately arthroscopically, the procedure can
be performed arthroscopically . A mini arthrotomy may be
req uired . The grafts can be obtained from either the
medial or lateral peripheral margins of the femoral con
dyles at the level of the patellofemoral joint. The appropri
ate -sized tube chisel is introduced perpendicular to the
donor site, and the harvester is driven into the donor site. For chondral defects, a 1 5 -mm graft is taken. For osteo
chondral defects, a 2 5 -mm graft is obtained . The chisel is twisted to break the cancellous bone , and the graft is
removed. All grafts are harvested with a similar technique
(Fig ure 1 7- 2 5 ) .
Figure 17-25 Single osteochondral plug.
598 C HAPTER 1 7 • Injuries to the Meniscus and Articular Cartilage
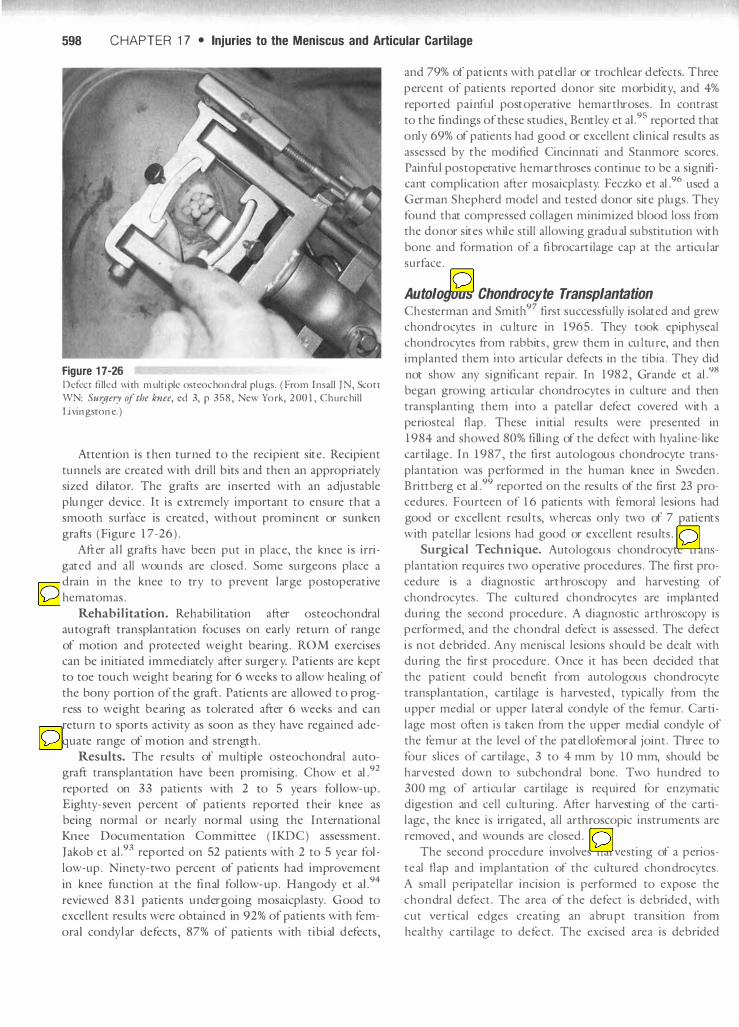
Figure 1 7-26 Defect fi lled with multiple osteochondral plugs. ( From I nsaU TN, Scott WN: Surgery of the knee, ed 3, p 358, New York, 2 00 1 , ChurchiU
Livingstone. )
Attention is then turned to the recipient site. Recipient
tunnels are created with drill bits and then an appropriately sized dilator. The grafts are inserted with an adjustable
plunger device . It is extremely important to ensure that a smooth surface is c reated , without prominent or sunken
grafts (Figure 1 7-26) .
After a l l grafts have been p ut in place, the knee is i rri
gated and a ll wounds are closed. Some surgeons place a drain in the knee to try to prevent large postoperative
hematomas.
Rehabilitation. Rehabilitation after osteochondral autograft transp lantation focuses on early return of range
of motion and p rotected weight bearing. R O M exercises can be initiated immediately after surgery. Patients are kept to toe touch weight bearing for 6 weeks to a llow healing of
the bony portion of the graft. Patients are allowed to p rog
ress to weight bearing as tolerated after 6 weeks and can
return to sports activity as soon as they have regained ade
quate range of motion and strength. Results. The results of m ultiple osteochondral auto
graft transplantation have been promising. Chow et a1.92
reported on 33 patients with 2 to 5 years fol low-up. Eighty -seven percent of patients reported their knee as being normal o r nearly normal using the International
Knee Documentation Committee ( IKDC ) assessment.
Jakob et a 1 .93 reported on 52 patients with 2 to 5 year fol
low-up. Ninety -two percent of patients had improvement
in knee function at the final fol low-up. Hangody et a1.94
reviewed 8 3 1 patients undergoing mosaicplasty. Good to excellent results were obtained in 92% of patients with fem
ora l condy lar defects , 87% of patients with tibial defects ,
and 79% of patients with patellar or trochlear defects. Three
percent of patients reported donor site morbidity, and 4%
reported painful postoperative hemarthroses. In contrast
to the findings ofthese studies , Bentley et a1.95 reported that
only 69% of patients had good or excellent c linical results as
assessed by the modified Cincinnati and Stanmore scores.
Painfu l postoperative hemarthroses continue to be a significant complication after mosaicplasty. Feczko et a1.96 used a German Shepherd model and tested donor site plugs . They
found that compressed collagen minimized blood loss from the donor sites while sti ll allowing gradual substiultion with
bone and formation of a fibrocartilage cap at tile articular
surface.
Autologous Chondrocyte Transplantation Chesterman and Smitl197 first successfully isolated and grew chondrocytes in culture in 1 965. They took epiphyseal
chondrocytes from rabbits , grew them in culture, and then implanted t llem into articular defects in tile tibia . They did
not show any significant repair. In 1982, Grande et a1Y8
began growing articular chondrocytes in culture and then
transplanting them into a pate llar defect covered with a
periosteal flap. These initial results were presented in
1 984 and showed 80% filling of the defect with hyaline- like
cartilage. In 1 987, the first autologous chondrocyte trans
plantation was performed in the h uman knee in Sweden . B ri ttberg et al.99 reported on the results of the first 23 procedures. Fourteen of 1 6 patients with femoral lesions had
good or excellent results, whereas only two of 7 patients
with patellar lesions had good or excellent results.
Surgical Technique. Autologous chondrocy te trans
plantation requires two operative procedures. The first pro
cedure is a diagnostic arthroscopy and harvesting of
chondrocytes. The cultu red chondrocytes are implanted
during tile second procedure. A diagnostic arthroscopy is performed, and the chondral defect is assessed. The defect
is not debrided. Any meniscal lesions should be dealt with during tile first procedure. Once it has been decided that the patient could benefit from autologous chondrocyte
transp lantation , cartilage is harvested , typically from the
upper medial or upper lateral condy le of tile femur. Carti
lage most often is taken from the upper medial condy le of
the femur at the leve l of the patellofemoral joint. Three to
four s lices of cartilage , 3 to 4 mm by 1 0 mm, should be
harvested down to subchondral bone. Two hundred to
300 mg of articular cartilage is req uired for enzymatic digestion and cell culturing . After harvesting of tile cartilage , the knee is irrigated, all arthroscopic instruments are
removed , and wounds are closed.
The second p rocedure involves harvesting of a perios
teal flap and implantation of the cultured chondrocytes .
A smal l peri patellar incision is performed to expose the
chondra l defect. The area of the defect is debrided , with
c ut vertical edges creating an abrupt transition from
healthy cartilage to de fect. The excised area is debrided

Injuries to the Meniscus and Articular Cartilage • CHA PTER 1 7 599
down to subchond ral bone wi thout causing bleeding. If
bleeding occurs from the subchondral bone , it m ust be
stopped before implantation of the chondrocy tes. A sepa
rate incision is made to harvest the periosteal flap , which
usually is obtained from the upper medial tibia. The peri
osteal flap is sutured into the healthy cartilage surrounding the defect. The cambium layer of the flap m ust face
the subchondral bone of the defect. Sutures a re placed
at 5- to 6-mm intervals, and intervals between the sutures are sealed off with fibrin gl ue. An opening is left in the periosteal patch for injection of the chondrocy tes. After
injection of the cell s, closure of the periosteal patch i s
completed with sutures and fibrin glue (Figures 1 7-27
to 1 7-29 ) .
Rehabilitation. Rehabilitation after autologous chon
drocy te transplantation can be broken down into range of motion , CPM, weight bearing , strengthening, and func
tional training. Patients can begin working on range of motion immediately after surgery. Trochlear groove patients should not work on active extension for the first
4 weeks, because as active extension increases patellofe
moral contact stresses . C P M should be used as much as possible for the first 6 weeks. Most patients should be
non-weigh t-bearing for at least the first 2 weeks. Patients
then can progress to partial weight bearing. All patients
should be in a hinged knee brace that is locked in extension
for ambulation. Femoral condyle patients can progress to weight bearing as tolerated at 6 weeks. Trochlear patients
can progress to weight bearing as tolerated as soon as they
are comfortable as long as they are in the knee brace locked in extension. This keeps the patella out of the trochlear
groove and protects the repair. Strengthening can begin
Figure 17-27 Periosteal patch being sewn into place. (From I nsaJi IN, Scott WN: SUllferyofthe knee, ed 3, p 349, New York, 200 1 , Churchill Livingstone. )
Figure 17-28 Completion of the periosteal patch. ( From Insall IN, S cott WN:
SUllfcry of the knee, ed 3, p 349, New York, 200 1 , Churchill Livingstone. )
Figure 1 7-29 I njection of chondrocytes beneath the periosteal patch. (From Insall
IN, Scott WN : Surgery of the knee, ed 3, p 349, New York, 200 1 ,
Churchill Livingstone. )
Clinical Point
It is imperative that the surgeon inform the rehabilitation team of
the range of motion to prevent loading, as determined from
intraoperative viewing of the lesion during knee range of motion.
This allows optimum rehabilitation and protection of the repair.
in the first 2 weeks with isometric quad riceps sets and
straight leg raises. Closed chain activities can be started at
6 weeks. Positions that stress the region of chondrocy te
implantation should be avoided . For anterior femoral

600 CHAPTER 1 7 • Injuries to the Meniscus and Articular Cartilage
condyle lesions , loading in full extension should be
avoided . For posterior femoral condyle lesions , loacling in
flexion should be avoided . For trochlear lesions , deep
sq uats sho uld be avoided . Functional training can begin
between weeks 8 and 1 2 .
Positions to Avoid with Autologous Chondrocyte Transplantation
• Anterior femoral condyle lesions-avoid full extension
• Posterior femoral condyle lesions-avoid loaded flexion
• Trochlear lesions-avoid deep squats
Low impact activities , such as cycling, roller blading, and
skating, can be star ted 9 to 1 2 months after surgery . Repet itive impact loading , such as jogging and aerobics , can be started at 1 3 to 1 5 months, and h igh level sporting activ
ities can be star ted 1 6 to 1 8 months after surgery .
Results. The results of autologous chondrocyte trans
plantation have been q uite promising . Peterson et al .lOO
reported on 1 0 1 patients treated with ACI with 2 to 9 year
follow-up . Ninety -two percent of patients w ith isolated
femoral les ions had good or excel lent results . Sixty -five per
cent of pat ients with patellar defects had good to excellent results . Second look ar throscopy was performed in 5 3 patients . Of these, 26 had a hyperu"ophic response of the periosteum or graft. Seven of these 26 were symptomatic .
The incidence of graft failure was 7%. Peterson et al .l Ol fol
lowed a group of 61 patients treated for isolated femoral or
patellar defects for 5 to 1 1 years to determine t he d urability
of the repair t issue . At 2 years, 50 of 6 1 patients had good
to excellent results . At 5 to 1 1 year follow-up , 5 1 of 6 1
patients had good to excel lent results .
Several studies have been performed to eval uate the outcome of AC I compared to the outcomes w it h microfracture and mosaicplasty . Kn utsen et a1 .90 compared
ACI to microfracture in a randomized trial . Eighty
patients with a single c hondral defect in the femoral con
dyle were randomized to AC I or microfract ure . Indepen
dent observers performed follow-up examinations at 1 2
and 24 mont hs . Second look arthroscopy was performed
at 2 years . Histological evaluation was performed by a
pat hologist and a clin ical sc ient ist , both of whom were
blinded to each pat ient 'S treatment . Both groups showed improvement at 2 years , but the microfracture group had
slightly better improvement as measured by the SF -36.
B iopsy specimens were obtained from 84% of pat ients .
No histological d ifference was seen between the two
groups . Horas et al . 102 compared AC I to osteochondral
cyl inder transplantation . Forty patien ts with isolated fem
oral defects were randomized to AC I or osteochondral
cyl inder transplantation . Us ing Lysholm scores , recovery
from AC I was slower than recovery from osteochondral
cyl inder transplantation . After 2 years, clin ical results were equal between the two groups . Histomorphological exam
inat ion of the AC I patients showed a stable resurfac ing of the defect in all pat ients . T he tissue consisted mainly of
fibrocart ilage , w it h local ized areas of hyaline-l ike regener
at ive cartilage close to the s ubchondral bone . Examinat ion
of biops ies from the osteochondral cylinder transplanta
t ion showed remaining gaps between the graft and intact
articular cart ilage , but no histological difference was seen between the osteochondral transplan ts and the s urrounding original cartilage .
N umerous stuclies have shown that autologous chon drocyte transplantat ion provides good to excellent results
in 80% to 90% of patients with isolated chondral defects
of the femoral condyles . Results are less preclictable for
patellar or trochlear defects . Autologous chondrocyte
transplantation is one option in the treatment of chondral defects in the knee .
Summary
The treatment of chondral injuries has become an increas
ingly popular field . As outlined in th is chapter, a number
of different options are available to today 's ortllopedic sur
geon . The clifferent techniq ues have vary ing advantages
and clisadvantages . The rehabilitat ion team needs to under
stand t lle b iology of tlle repair technique, the biomechanics
of the knee , and how tlle locat ion of the chondral defect
affects the biomechanics in order to develop the best rehabilitat ion program and offer the best rehabilitation advice to each patient.
References
To enhance this text and add value for the reader, all refer
ences have been incorporated into a C D-ROM tllat is
provided with tllis text . The reader can view ·tlle reference
source and access it onl ine whenever poss ible . There are a
total of 1 02 references for t llis chapter .







