
Paraproteins and Renal Disease

CASE 1
M RFMrs RFPhone referral from Wagga Wagga
Recent onset nephrotic syndromesAlb 18 g/l , 8 g/day proteinuria, no haematuriaNo other symptoms
Type II DM 4 yrsType II DM – 4 yrsNo known retinopathyNo macrovascular disease
What would you do?y

Renal Biopsy - H&Ep y

Renal Biopsy – Congo Redp y g

Renal Biopsy - EMp y

Renal Biopsy - EMp y

Case 1
What further investigations do you want?
What would you tell her about her prognosis/
What would you do next?

Case 1
IgG λ BJP 0.31 g/dayNormal serum Normal bone marrow
E h lEcho normal
Referred haematologyGSF stimulated stem cell mobilisationHigh dose mephalanAutologous stem cell transplant
CASE 2
Mrs WH 62 yoMrs WH 62 yo Known myeloma – 12 months
IgG λ 40 % plasma cells Rx prednisone / pamidronateIgG λ, 40 % plasma cells. Rx prednisone / pamidronate
Referred with rising creatinine 100 160 umol/lReferred with rising creatinine – 100 – 160 umol/lProteinuria – 1.2 g.dayParaprotein – 0 4 g/dayParaprotein – 0.4 g/day
What is you differential diagnosis?What is you differential diagnosis?
What would you do next?What would you do next?

Biopsy – Case 2p y

Case 2
DiagnosisPamidronate induced FSGS
Medication ceasedMedication ceasedResolution albuminuria over 4 monthsC ti i t bl t 140 150 l/lCreatinine stable at 140-150 umol/l
CASE 3
Mrs RB 66 yoIgA myeloma diagnosed 04/2002g y g
80% plasma cells, IgA 40-60 g/lλ light chain BJP, 1 g/day
PCAB and plasmapheresisSCT 11/2002
8% plasma cells, IgA 20 g/l
R/o retroperitoneal Leiomyoma – 05/2003

Case 3Commenced Thalidomide / Prednisone 09/03
Presented with R LL Pneumonia and ARF in Melbourne 07/2005
Prior to this IgA levels and BJP excretion were stable
TransferredParaprotein levels unchangedParaprotein levels unchangedDialysed?? Obstruction → stented → no changeg
What would you do next?

Case 3 renal Biopsyp y

Case 3 Renal Biopsyp y
Case 3
Commenced haemodialysisSubsequent change to PDq g
W i l / i f tiWorsening myeloma / infections Deceased 2 years later

Monoclonal Plasma Cell Diseases and Renal Disease
Wh t th di i l d?What are the diseases involved?
Why the different phenotypes?Why the different phenotypes?
Why can Cast Nephropathy develop with stable y p p y pparaprotein level?
What to do?What to do?
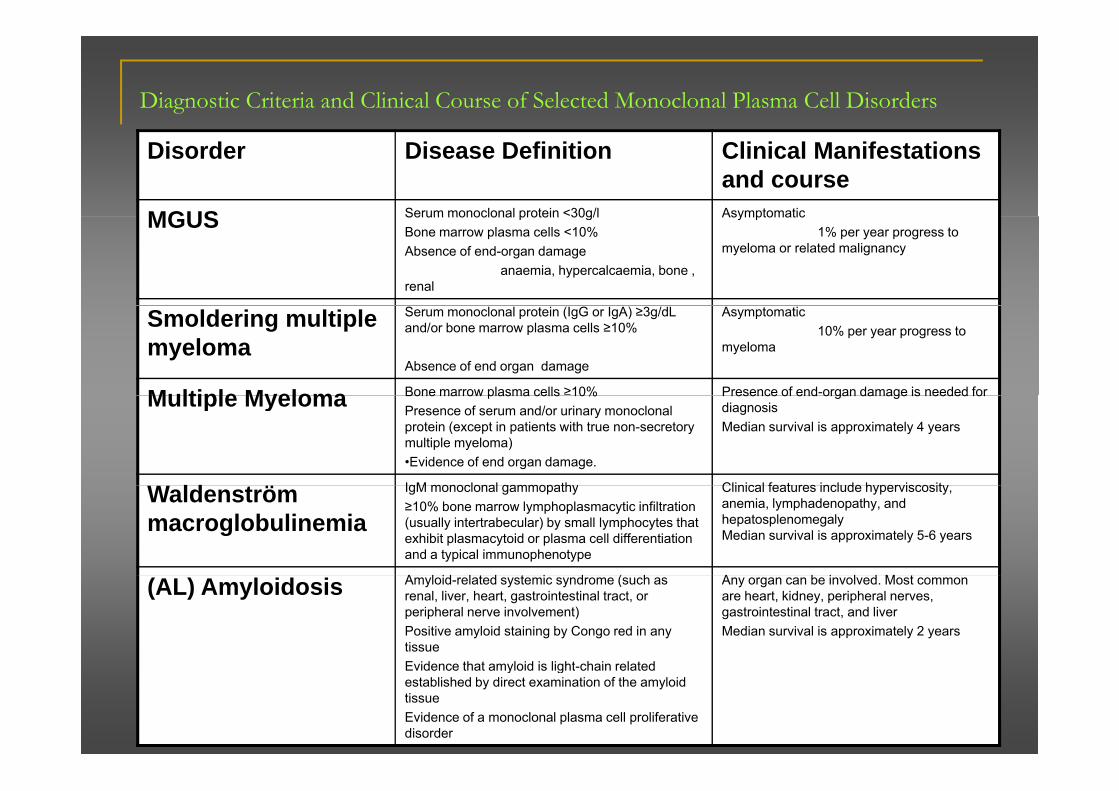
Diagnostic Criteria and Clinical Course of Selected Monoclonal Plasma Cell Disorders
Disorder Disease Definition Clinical Manifestations and course
MGUS Serum monoclonal protein <30g/l AsymptomaticMGUS Serum monoclonal protein 30g/lBone marrow plasma cells <10%Absence of end-organ damage
anaemia, hypercalcaemia, bone , renal
Asymptomatic1% per year progress to
myeloma or related malignancy
Smoldering multiple myeloma
Serum monoclonal protein (IgG or IgA) ≥3g/dL and/or bone marrow plasma cells ≥10%
Absence of end organ damage
Asymptomatic10% per year progress to
myeloma
Multiple Myeloma Bone marrow plasma cells ≥10% Presence of end-organ damage is needed forMultiple Myeloma Bone marrow plasma cells 10%Presence of serum and/or urinary monoclonal protein (except in patients with true non-secretory multiple myeloma)•Evidence of end organ damage.
Presence of end organ damage is needed for diagnosisMedian survival is approximately 4 years
W ld ö IgM monoclonal gammopathy Clinical features include hyperviscosityWaldenström macroglobulinemia
IgM monoclonal gammopathy≥10% bone marrow lymphoplasmacytic infiltration (usually intertrabecular) by small lymphocytes that exhibit plasmacytoid or plasma cell differentiation and a typical immunophenotype
Clinical features include hyperviscosity, anemia, lymphadenopathy, and hepatosplenomegalyMedian survival is approximately 5-6 years
A l id l t d t i d ( h A b i l d M t(AL) Amyloidosis Amyloid-related systemic syndrome (such as renal, liver, heart, gastrointestinal tract, or peripheral nerve involvement)Positive amyloid staining by Congo red in any tissueEvidence that amyloid is light chain related
Any organ can be involved. Most common are heart, kidney, peripheral nerves, gastrointestinal tract, and liverMedian survival is approximately 2 years
Evidence that amyloid is light-chain related established by direct examination of the amyloid tissueEvidence of a monoclonal plasma cell proliferative disorder

Paraproteinaemic Renal Diseasep
Li ht Ch i OthLight Chainmore common
Otherrare
AL AmyloidML(H) CDD
AH AmyloidMH CDD( )
Cast NephropathyProximal Tubulopathy
Immunotactoid GN*Type 1 Cryoglobulinaemic GNProximal Tubulopathy Type 1 Cryoglobulinaemic GNGN with monoclonal depositsWaldenstromsWaldenstroms
* Fibrillary GN

Incidence of Monoclonal Gammopathy Related Renal Disease
Varies depending on definitionsIn myeloma patients renal insufficiency is noted inIn myeloma patients, renal insufficiency is noted in 18% to 56%
At t l i l t i i i t lAt autopsy, renal involvement is seen in approximately 50% of patients with multiple myeloma
Light chain cast nephropathy (29%-32%)g p p y ( )AL amyloidosis (5%-11%)LCDD (3%-5%)
Acute tubular necrosisCommon findingCan occur alone or in conjunction with other pathologiesCan occur alone or in conjunction with other pathologies
Incidence of Monoclonal Gammopathy Related Renal Disease
Less is kno n abo t the incidence of monoclonalLess is known about the incidence of monoclonal gammopathy related kidney disease in patients without myelomay
In patients who have significant proteinuria or renal i ffi i ti l bi thinsufficiency warranting a renal biopsy, more than half have a monoclonal gammopathy-related kidney disease
Cryoglobulinemic glomerulonephritis – 16.5%LCDD – 11.6%Light chain cast nephropathy 10 7%Light chain cast nephropathy – 10.7%AL amyloidosis – 10.7%Light heavy chain deposition disease – 4.1%g y p
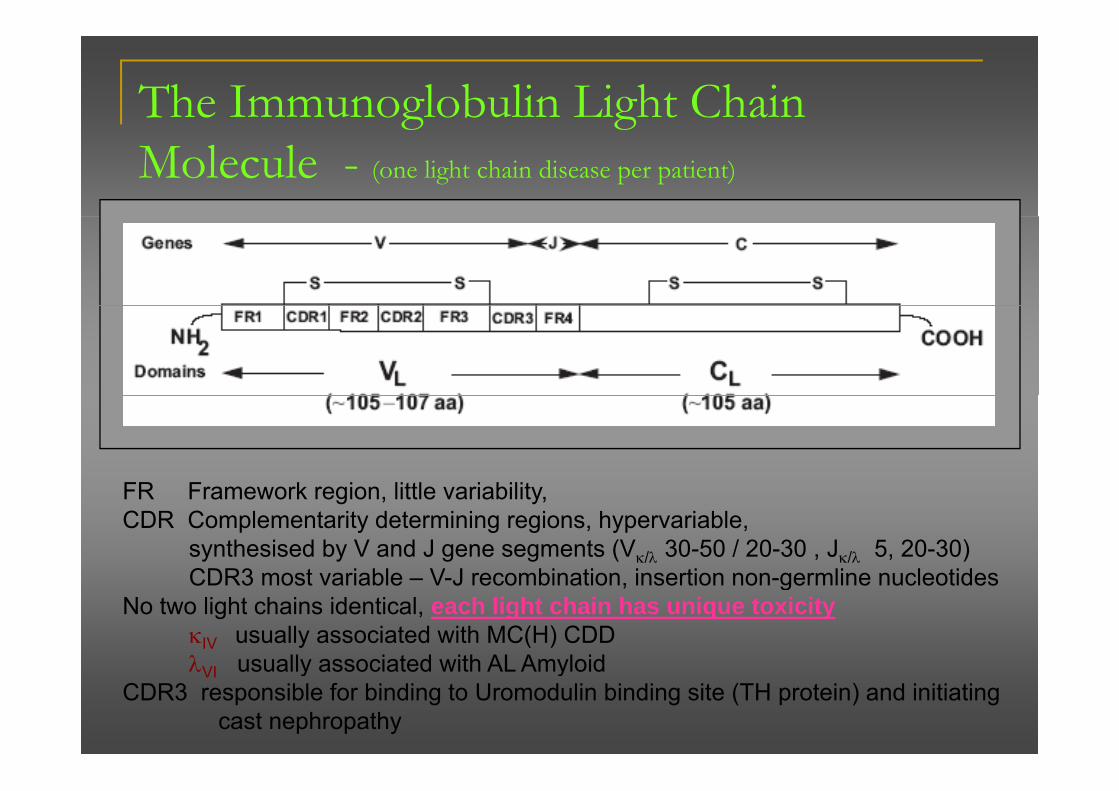
The Immunoglobulin Light Chain g gMolecule - (one light chain disease per patient)
FR F k i littl i bilitFR Framework region, little variability, CDR Complementarity determining regions, hypervariable,
synthesised by V and J gene segments (Vκ/λ 30-50 / 20-30 , Jκ/λ 5, 20-30)CDR3 most variable V J recombination insertion non germline nucleotidesCDR3 most variable – V-J recombination, insertion non-germline nucleotides
No two light chains identical, each light chain has unique toxicityκIV usually associated with MC(H) CDDλ usually associated with AL AmyloidλVI usually associated with AL Amyloid
CDR3 responsible for binding to Uromodulin binding site (TH protein) and initiating cast nephropathy
Renal Handling of Immunoglobulin Light g g gChains
Potential interaction every segment of nephrony g pFreely filtered at glomerulusPresented to proximal tubulePresented to proximal tubule
Endocytosed after binding to megalin-cubulin complexDegraded in lysosomes and aa returned to circulation
If endocytic uptake saturated then light chains appear in tubular fluid of distal nephron segments
Present in urine = BJP

Pathogenesis of Cast formationg

Mechanisms of renal Injuryj y
Tubular preccipitationTubular preccipitationLight chain cast nephropathy
DepositionAmyloidAmyloidMonoclonal immunoglobulin deposition diseaseFanconi
HyperviscosityHyperviscosityWaldenstromsElevated serum Ig
IgM > 30 g/l/IgA > 60 g/l
IgG > 40g/lGlomerular
Amyloid MIDD MPGN immune complexAmyloid, MIDD, MPGN, immune complexPamidronate MCN, FSGS
TubularATN and ATINATN and ATIN
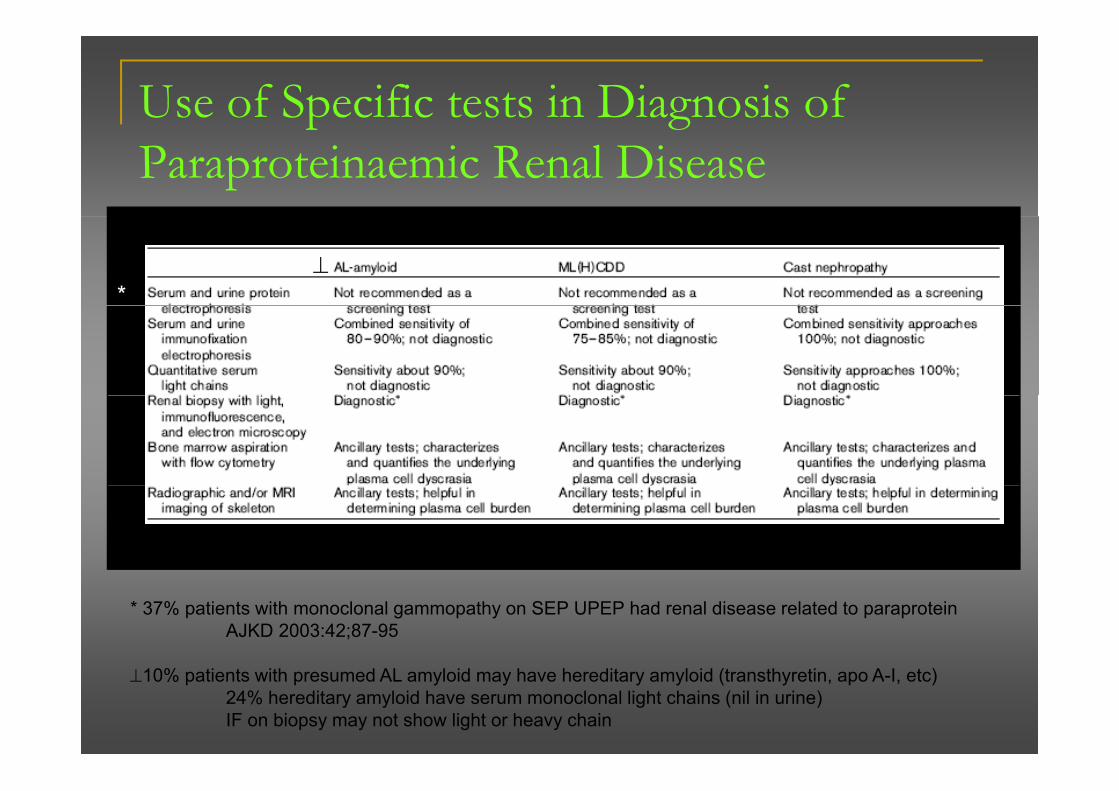
Use of Specific tests in Diagnosis of p gParaproteinaemic Renal Disease
*⊥
*
* 37% patients with monoclonal gammopathy on SEP UPEP had renal disease related to paraproteinAJKD 2003:42;87-95
⊥10% patients with presumed AL amyloid may have hereditary amyloid (transthyretin, apo A-I, etc)24% hereditary amyloid have serum monoclonal light chains (nil in urine)IF on biopsy may not show light or heavy chain

Case 1 – Al Amyloid - clinicaly
%75% nephrotic proteinuria>20 g/d in ∼ 30%Albumin (dipstix) +ve
ExtrarenalCardiac
CCF and conductionAlbumin (dipstix) +ve50% CKDHypotension
CCF and conduction defects
NeurologicalHypotensionOften ACEi intolerantOrthostatic
Peripheral and autonomicLiver
H t lVolume and neuropathy
Light chainL bd > k (3 1)
HepatomegalySoft tissue
Carpal tunnellLambda > kappa (3:1)Vλv1
Carpal tunnellTongue enlargement

Case 1 – Al Amyloid - prognosisy p g
18% progress to ESRDMedian time from diagnosis to ESRD 14 monthsgMedian dialysis survival 8 months
Median survival overall18-24 months

Case 1 – Al Amyloid - therapyy pyConventional - Melphalan plus high dose steroid
33% haematologic responseLow treatment related mortalityOption for non-transplant patients
HDCT with Autologous Stem Cell TxHDCT with Autologous Stem Cell Tx8 prospective, selected trials. 1 retrospective case control40% complete responseOrgan response follows hematologic responseOrgan response follows hematologic responseLong-term survival in organ responders
In ESRDStem cell can be performed
Response similar to non-ESRDHigher morbidityResponders have undergone renal Tx
Newer drugsNewer drugsThalidomide and dexamethasone
19% haematologic response, 26% organ respone65% treatment toxicity65% treatment toxicity
Lenalidomide and dexamethasone

Case 3: Cast Nephropathy - clinicalp p y
M lik l ith hi h P iMore likely with higher tumour burdenARF 10 15 with ESKD
PrognosisRecovery 26-58%
HypercalcaemiaARF, 10-15 with ESKD> 75% sub-nephrotic proteinuria
HypercalcaemiaLower creatinine
Recovery affects survivalproteinuriaPrecipitating
Dehydration
Response to chemotherapy also affects survival
DehydrationHypercalcaemiaNSAIDsIV contrastInfection
Case 3: Cast Nephropathy - Rxp p y
R t l / f iRestore volume / perfusionRemove toxinsReduce light chain levels
ChemotherapypyThalidomide plus dexamethasoneBortezomib plus dexamentasone
Plasma exchange (controversial)Efficacy in 2 older studies
fMore recent study no benefit on overall survivalStandard treatment in hyperviscosity (Waldenstroms)

Management of ESKDg
Survival significant diminished in patients withSurvival significant diminished in patients with dysproteinaemia and ESKD
Median survivalMedian survival4 years LCDD2 years AL amyloid2 years AL amyloid1 year MM

THERAPY – ML(H) CDD( )
1/3 have myeloma, rest plasma cell dyscrasia
Similar trials / consideration to AL amyloid
Recurrence in transplants (AJKD 2004:43;147-153)pMedian graft survival 37.4 monthsMedian patient survival 6.1 yearsMedian patient survival 6.1 years
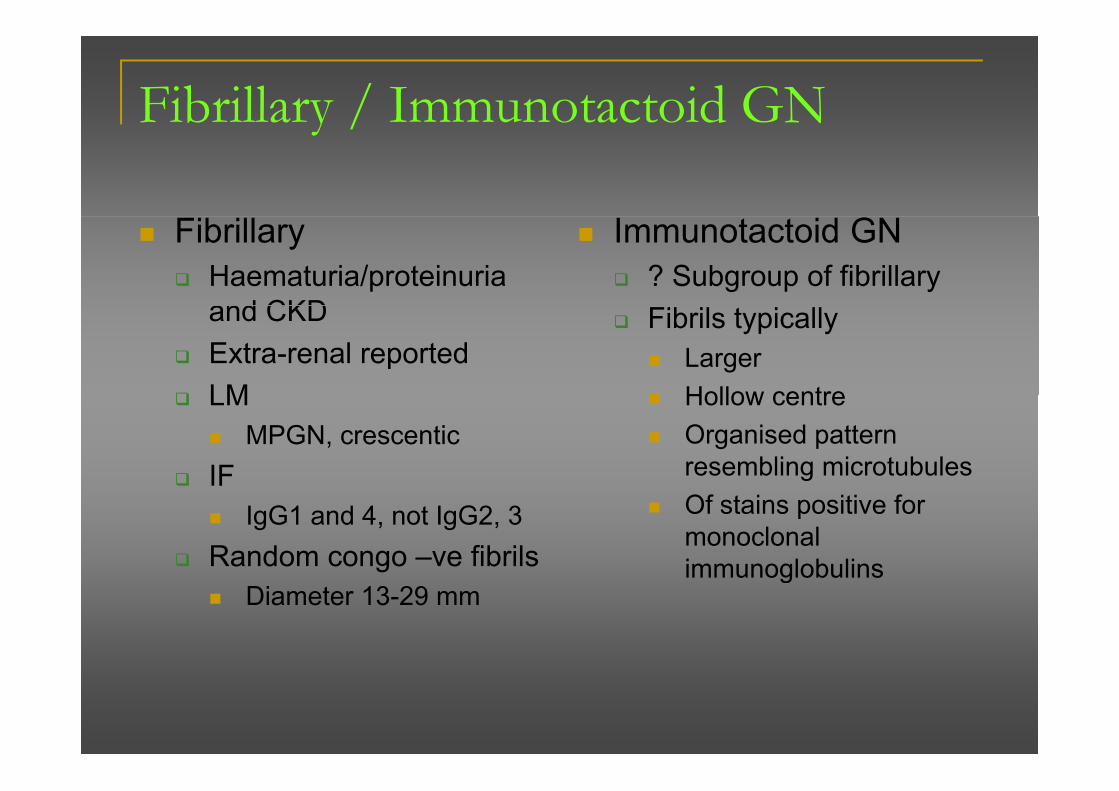
Fibrillary / Immunotactoid GNy /
Fibrillary Haematuria/proteinuria and CKD
Immunotactoid GN? Subgroup of fibrillary
and CKDExtra-renal reportedLM
Fibrils typically LargerHollow centreLM
MPGN, crescenticIF
Hollow centreOrganised pattern resembling microtubulesIF
IgG1 and 4, not IgG2, 3Random congo –ve fibrils
Of stains positive for monoclonal immunoglobulins
Diameter 13-29 mmimmunoglobulins
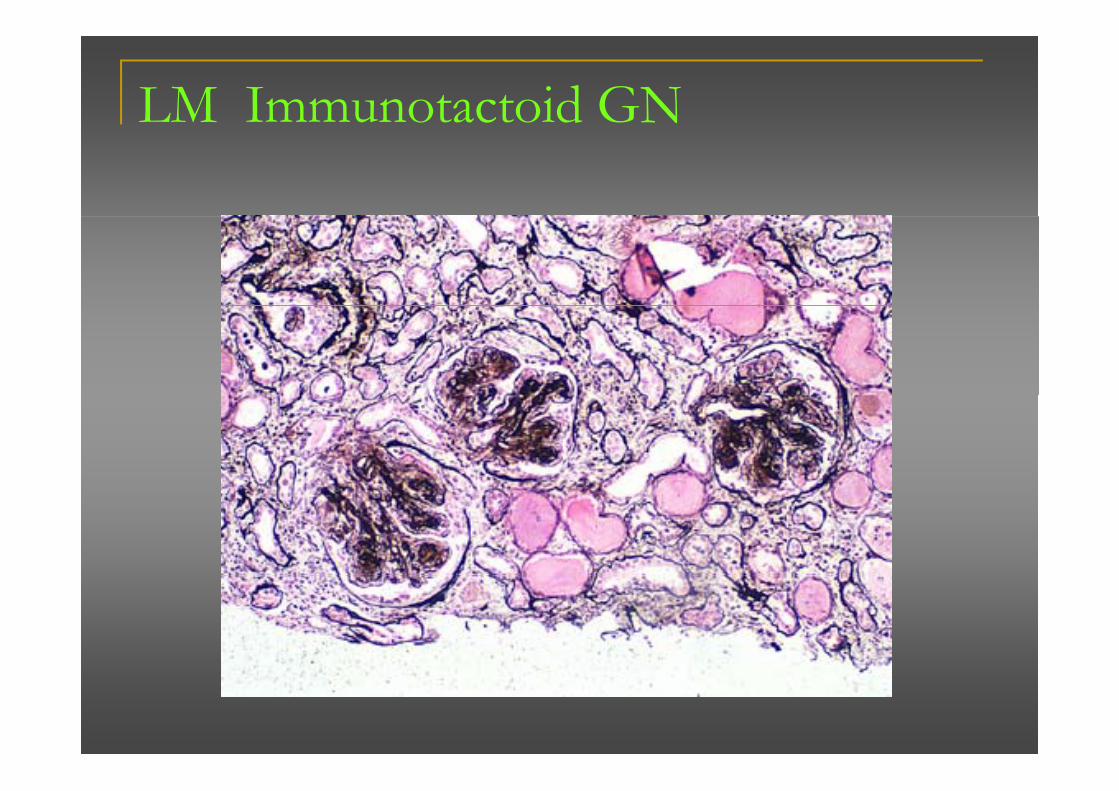
LM Immunotactoid GN

EM – Fibrillary and Immunotactoid GNy
Fibrillary GN Immunotactoid GN

AA Amyloid

Underlying Disorders and Treatment in 374 Patients with AA Amyloidosis
Lachmann H et al. N Engl J Med 2007;356:2361-2371

Changes in Amyloid Burden from Baseline to Most Recent Follow-up in 221 Patients and Changes in Amyloid Burden and Renal Function during Follow-up in 178 Patients with a
B li C ti i Cl f M Th 20 l Mi tBaseline Creatinine Clearance of More Than 20 ml per Minute
Lachmann H et al. N Engl J Med 2007;356:2361-2371

Regression of AA Amyloid Deposits in a Patient with Familial Mediterranean FeverMediterranean Fever
Lachmann H et al. N Engl J Med 2007;356:2361-2371

Unadjusted Relative Risk of Death Associated with the Most Recent Median Annual SAA Concentration during Follow-up
Lachmann H et al N Engl J Med 2007;356:2361 2371Lachmann H et al. N Engl J Med 2007;356:2361-2371
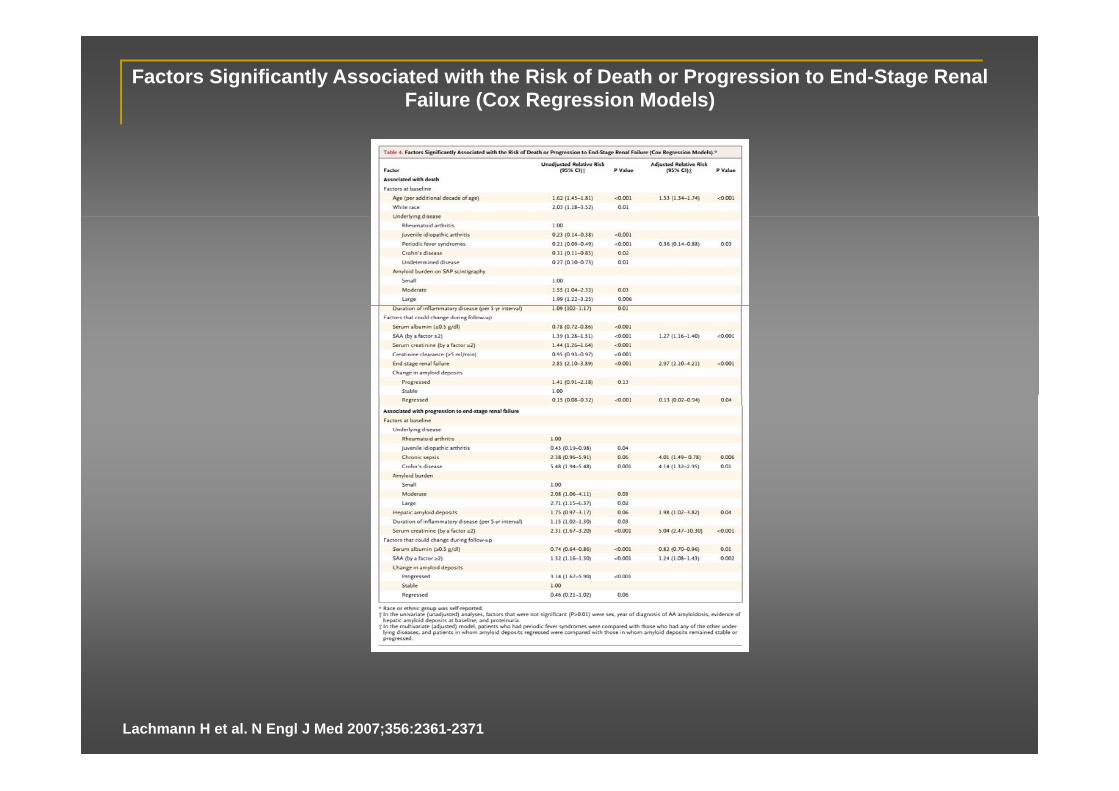
Factors Significantly Associated with the Risk of Death or Progression to End-Stage Renal Failure (Cox Regression Models)
Lachmann H et al. N Engl J Med 2007;356:2361-2371

Eprosidate in treatment of AA Amyloid
Dember L et al. N Engl J Med 2007;356:2349-2360

Baseline Demographic and Clinical Characteristics of Patients
Dember L et al. N Engl J Med 2007;356:2349-2360
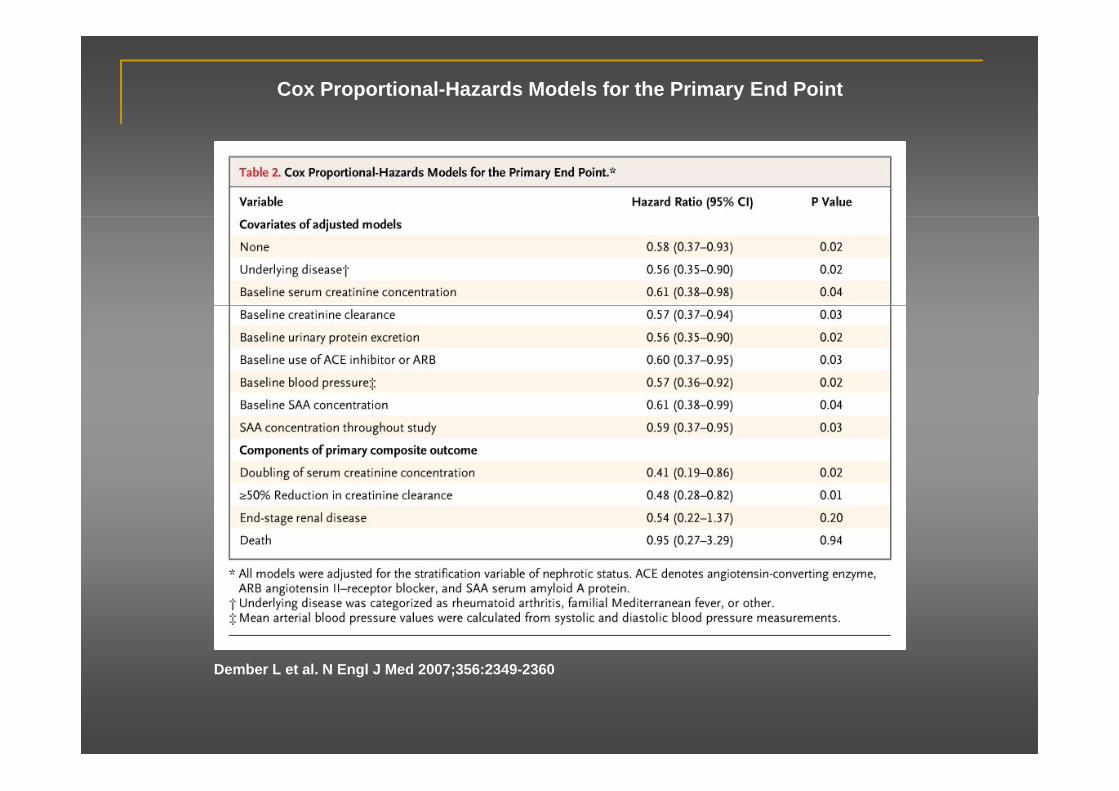
Cox Proportional-Hazards Models for the Primary End Point
D b L t l N E l J M d 2007 356 2349 2360Dember L et al. N Engl J Med 2007;356:2349-2360

Kaplan-Meier Estimates of Event-free Survival
Dember L et al. N Engl J Med 2007;356:2349-2360
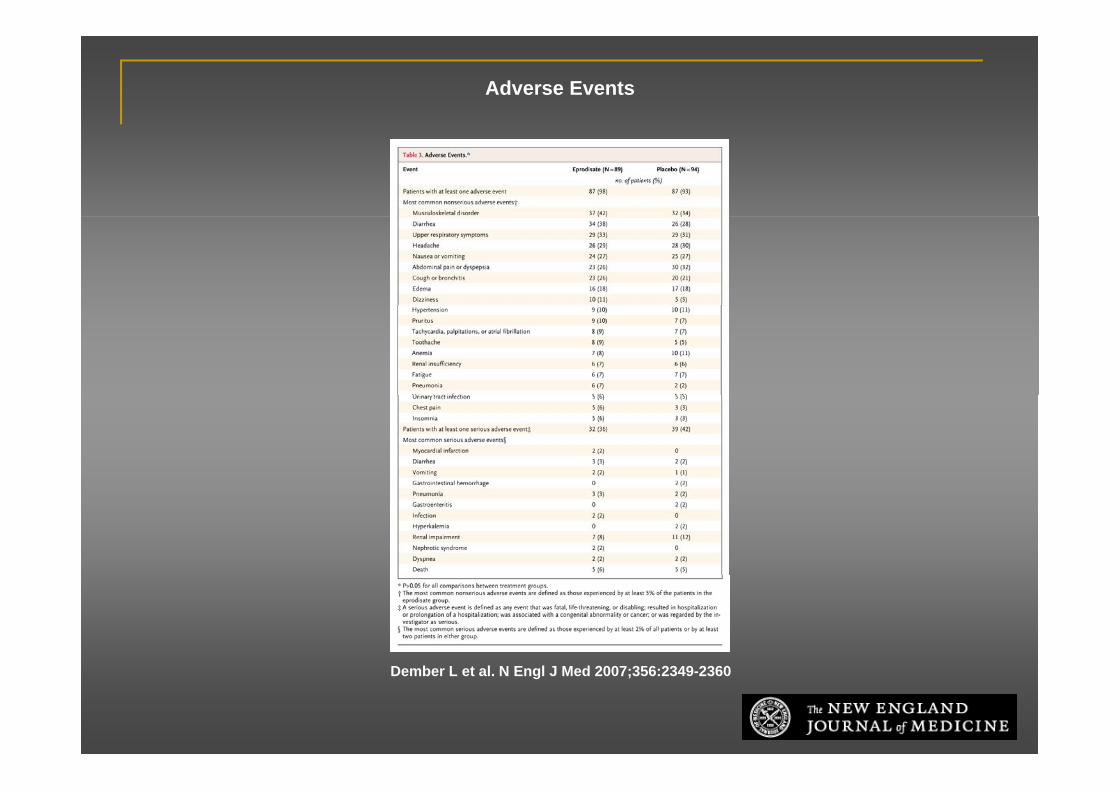
Adverse Events
Dember L et al. N Engl J Med 2007;356:2349-2360







