PAEDIATRICTUBERCULOSIS
Sam Walters
Imperial NHS Trust
LONDON


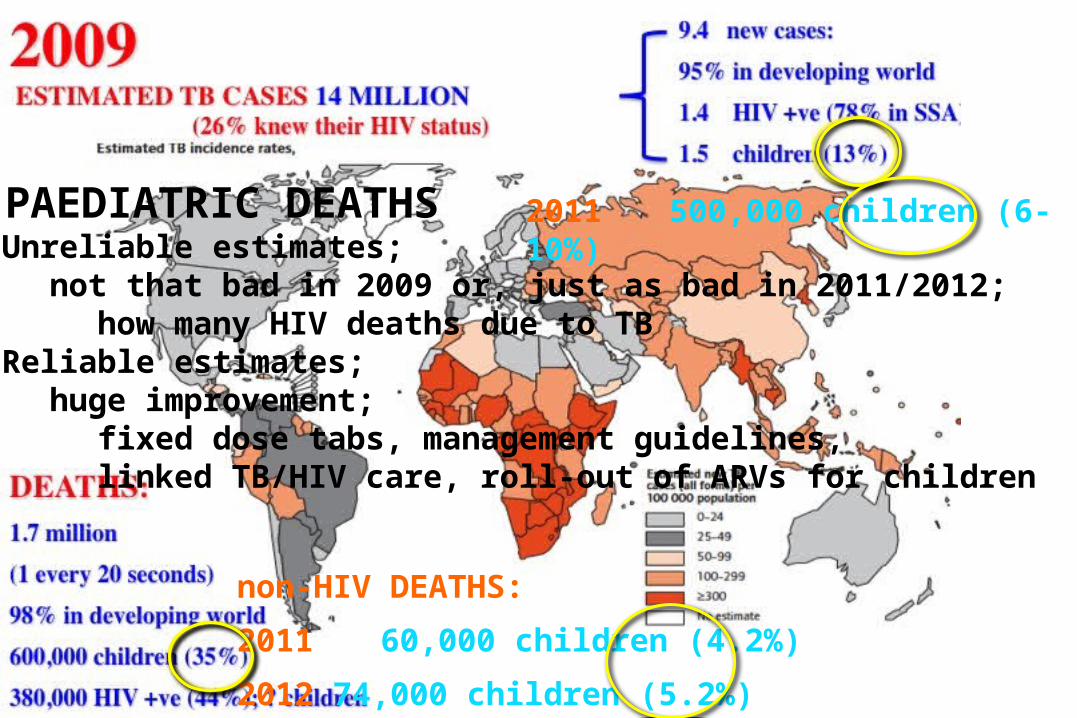
2011 ESTIMATED TB CASES 12 MILLION
8.7 million new cases:
500,000 children (6-8%)
DEATHS: 1.43 million
60,000 children (4.2%)
[2012; 74,000 children (5.2%)]
* Up to 40% of cases in high
incidence countries are children

2011 500,000 children (6-10%)
non-HIV DEATHS:
2011 60,000 children (4.2%)
2012 74,000 children (5.2%)
2011 500,000 children (6-10%)
non-HIV DEATHS:
2011 60,000 children (4.2%)
2012 74,000 children (5.2%)
? PAEDIATRIC DEATHSUnreliable estimates;
not that bad in 2009 or, just as bad in 2011/2012;how many HIV deaths due to TB
Reliable estimates;huge improvement;
fixed dose tabs, management guidelines, linked TB/HIV care, roll-out of ARVs for children

2011 500,000 children (6-10%)
non-HIV DEATHS:
2011 60,000 children (4.2%)
2012 74,000 children (5.2%)
? PAEDIATRIC DEATHSUnreliable estimates;
not that bad in 2009 or, just as bad in 2011/2012;how many HIV deaths due to TB
Reliable estimates;huge improvement;
fixed dose tabs, management guidelines, linked TB/HIV care, roll-out of ARVs for children
Children now firmly placed on global TB agenda

PAEDIATRIC TUBERCULOSIS
Clinical Presentation

Clinical Presentation
-18 month girl
-previously well, no family history of TB
-3 weeks cough and unwell
-admitted to hospital
-low grade fever, normal examination
-appropriate investigations: all negative, Mantoux; 2mm
-gastric aspirates x 3; negative AFB
-X-ray patchy consolidation;
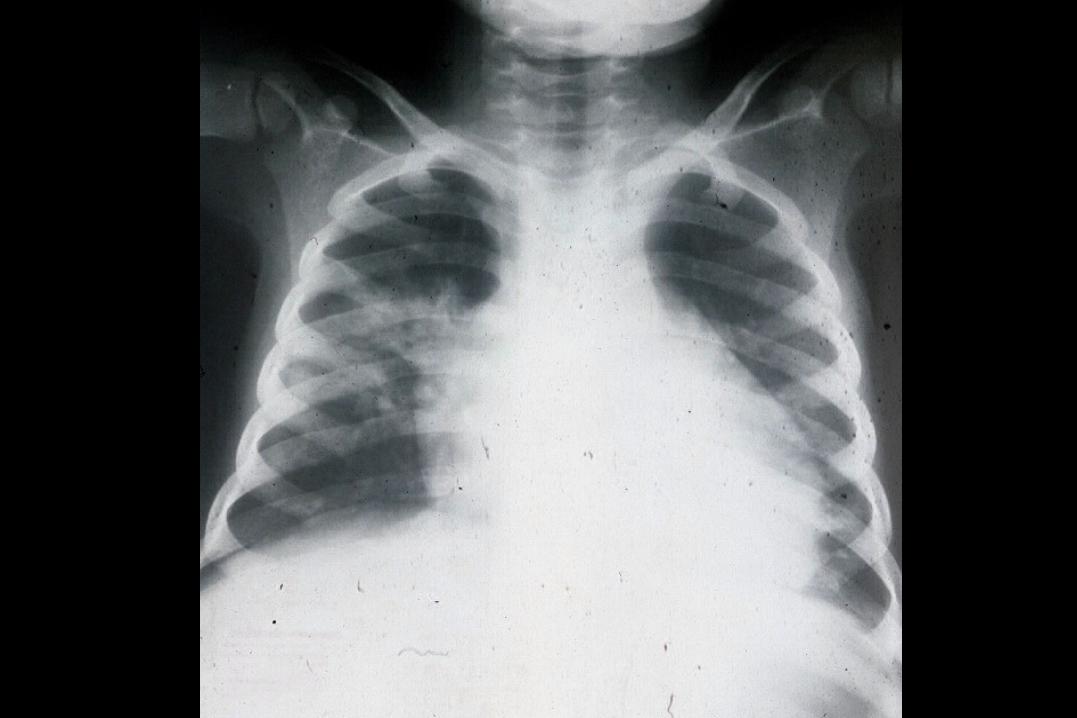

-Rx. 3 different antibiotic courses over 3 weeks
-gradual improvement; afebrile, less cough, looking well
-discharged home, no ∆
-6 weeks later out-patient review
-completely well, thriving, no cough
-gastric aspirates x 3; negative culture

-Rx. 3 different antibiotic courses over 3 weeks
-gradual improvement; afebrile, less cough, looking well
-continued improvement, discharged home, no ∆
-6 weeks later out-patient review
-completely well, thriving, no cough
-gastric aspirates x 3; negative culture
“Grandfather admitted to local hospital with pulmonary TB”
-repeat Mantoux; now 22 mm
-TB treatment commenced
PAEDIATRIC TB
Primary TB in children;
-spontaneous recovery is usual

CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
INFECTION ≠ DISEASE
NATURALHISTORY

CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELLCHILD
‘LIFELONG’IMMUNITY(live MTB)
Successfulimmuneresponse
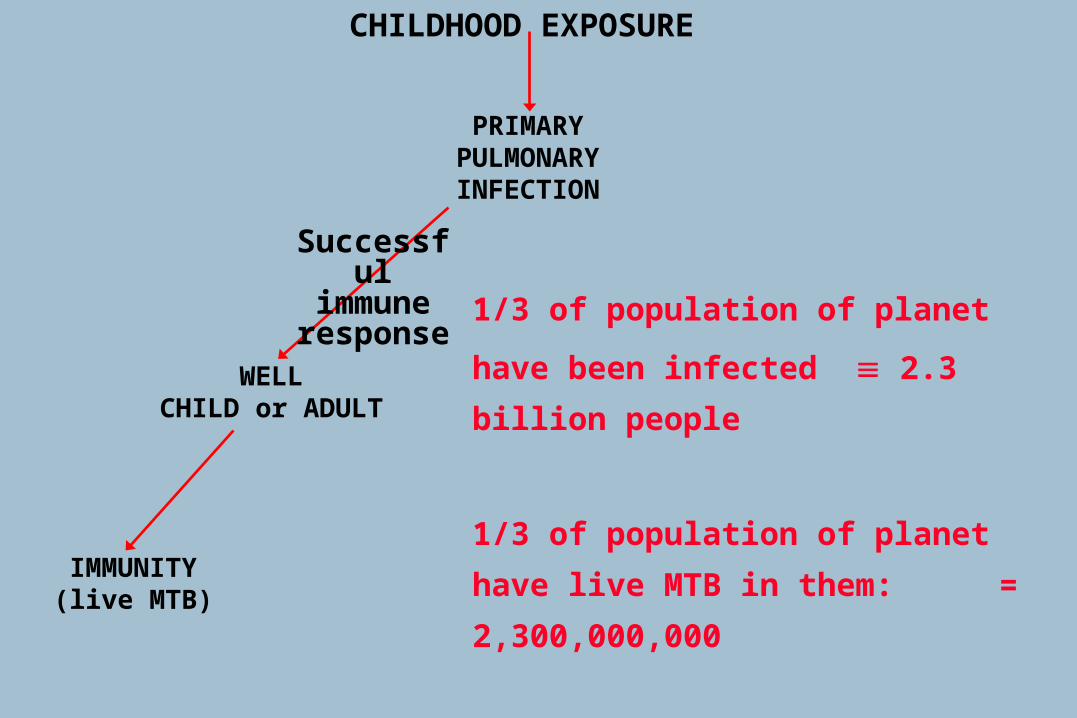
CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELLCHILD or ADULT
IMMUNITY(live MTB)
Successfulimmuneresponse 1/3 of population of planet
have been infected 2.3 billion people
1/3 of population of planet have live MTB
in them: = 2,300,000,000
Tuberculosis cases: = 12,000,000

CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELL CHILD or ADULT
IMMUNITY(live MTB)
Successfulimmuneresponse
LATE REACTIVATION, RE-INFECTION
‘Immunosuppression’;age, malnutrition, infection, HIV

CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELLADULT
IMMUNITY(live MTB)
Successfulimmuneresponse
LATE REACTIVATION OFADULT CAVITATING
PULMONARY DISEASE
FORMS CAVITY

CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELLADULT
IMMUNITY(live MTB)
Successfulimmuneresponse
LATE REACTIVATION OF PULMONARY DISEASE
ADULT DISEASE
FORMS CAVITY
TRANSMISSION
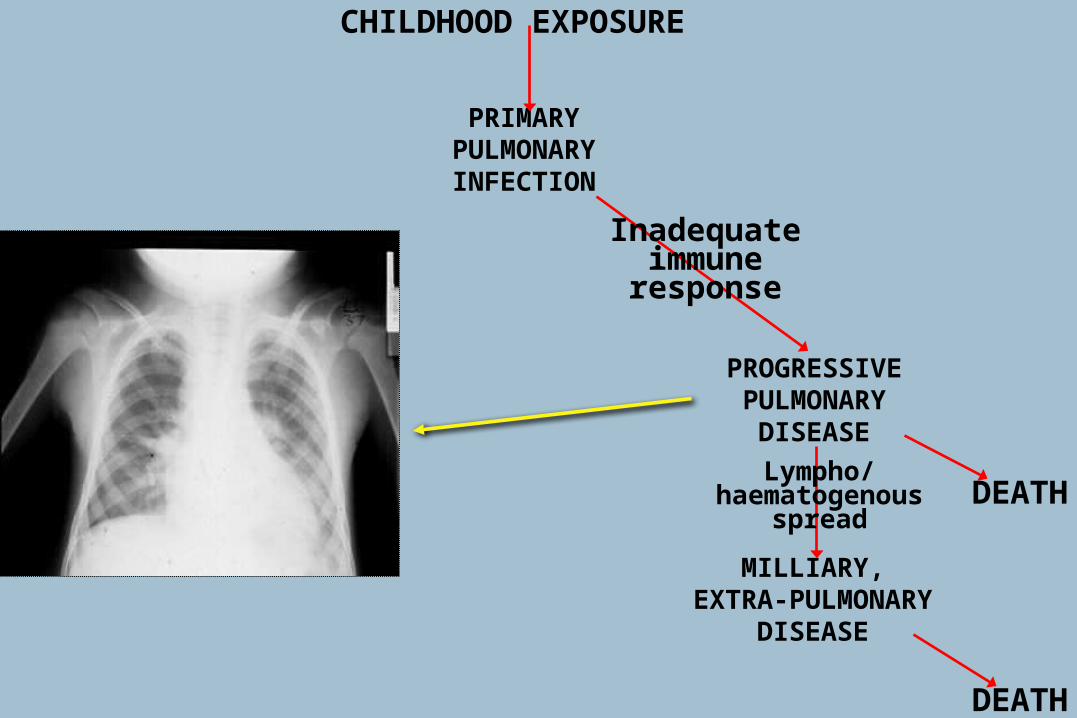
CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
PROGRESSIVEPULMONARY
DISEASE
MILLIARY,EXTRA-PULMONARY
DISEASE
DEATH
DEATH
Inadequateimmuneresponse
Lympho/haematogenous
spread

Paediatric TB: Adult TB: 104-106 bacteria >109 bacteria
-difficulty in confirming diagnosis-difficulty in detecting resistance
-? emergence of resistance
PAUCI-BACILLARY TBImplications of bacterial load:

Paediatric TB: Adult TB: 104-106 bacteria >109 bacteria
-difficulty in confirming diagnosis-difficulty in detecting resistance
-? emergence of resistance- infectivity
PAUCI-BACILLARY TBImplications of bacterial load:

Paediatric TB: Adult TB: 104-106 bacteria >109 bacteria
-difficulty in confirming diagnosis-difficulty in detecting resistance
-? emergence of resistance- infectivity-not part of immediate public health problem
PAUCI-BACILLARY TBImplications of bacterial load:

Paediatric TB: Adult TB: 104-106 bacteria >109 bacteria
-difficulty in confirming diagnosis-difficulty in detecting resistance
-? emergence of resistance- infectivity-not part of immediate public health problem
PAUCI-BACILLARY TBImplications of bacterial load:

CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELL CHILD
IMMUNITY( live MTB)
LATEREACTIVATION
Any Organ e.g. Bone, Kidney
PROGRESSIVEPULMONARY
DISEASE
MILLIARY,EXTRAPULMONARY
DISEASE
Inadequateimmuneresponse
Successfulimmune response Lympho/
haematogenousspread

CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELLCHILD
‘LIFELONG’IMMUNITY
(lesions sterilised)
PROGRESSIVEPULMONARY
DISEASE
MILLIARY,EXTRAPULMONARY
DISEASE
Inadequateimmuneresponse
Successfulimmune response Lympho/
haematogenousspread
Treatment
Treatment

CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELLCHILD
LIFELONGIMMUNITY(live MTB)
Successfulimmuneresponse
PROGRESSIVEPULMONARY
DISEASE
MILLIARY,EXTRA-PULMONARY
DISEASE
DEATH
DEATH
Inadequateimmuneresponse
Lympho/haematogenous
spread
HOSTImmunosuppressionGenetics ?Age esp. young children
ORGANISMInfecting dose -smear +ve, log phase -smear -ve / culture +ve, ? dormantMTB strain differences
? WHICH PATHWAY

AGE WHEN INFECTED PUERTO RICAN data SOUTH AFRICAN data
ADOLESCENT 15% 5 – 10%
5 yr - ADOLESCENT 5 – 10%
5 – 10 yr 2%
3 – 5yr 5%
1 – 5 yr 24%
1 – 2 yr 30%
< 1 yr 43% 50%
Age related risk of progression to disease:Adult 5 – 10%/lifetime (HIV 10%/yr)
Risk is life long, but concentrated in first 12-24 months after infection (approximately 80% of risk)
Undisputed ↑risk
Disputed ↑risk

CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELLCHILD
IMMUNITYSterile lesions
PROGRESSIVEPULMONARY
DISEASE
MILLIARY,EXTRAPULMONARY
DISEASE
Inadequateimmuneresponse
Successfulimmune response,
Lympho/haematogenous
spread Treatment
Treatment Successfulimmuneresponse

ISONIAZID
RIFAMPICIN
PYRAZINAMIDE
(Ethambutol)
Triple therapy: the Big Three (+ one)

September 2009
Probably correct dose but taken 40 yrs!

PAEDIATRIC DRUG DOSES
ISONIAZID 10-15 mg/kg/day
RIFAMPICIN 15 mg/kg/day
PYRAZINAMIDE 30-40 mg/kg/day
ETHAMBUTOL ?20 mg/kg/day
* Not CNS
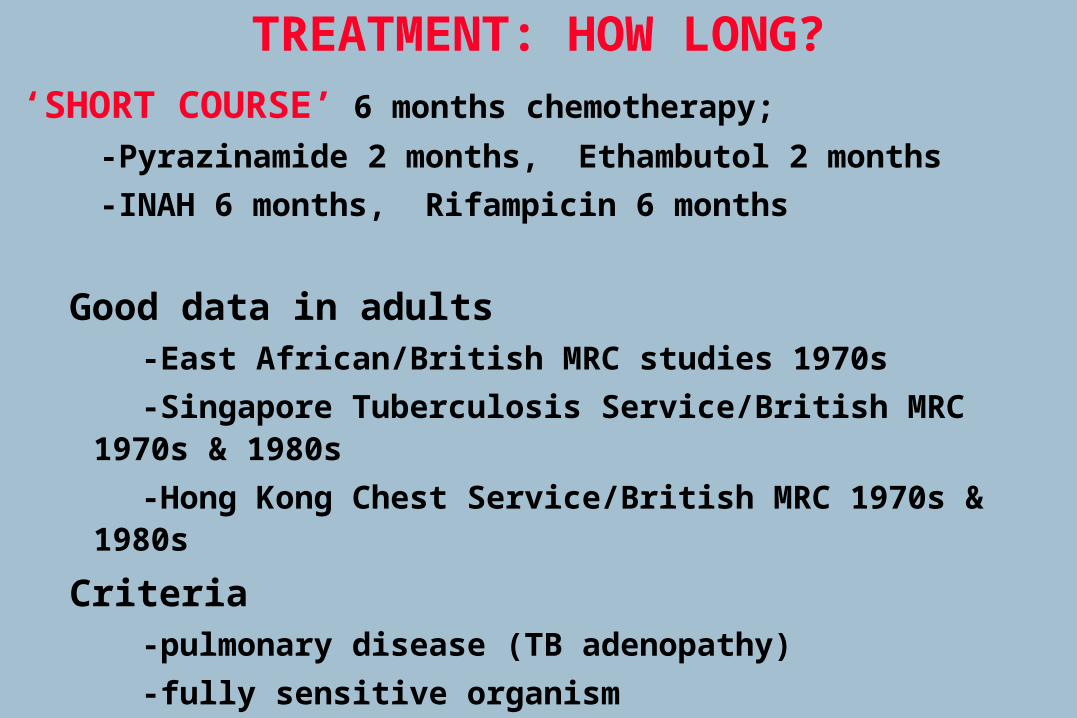
‘SHORT COURSE’ 6 months chemotherapy;
-Pyrazinamide 2 months, Ethambutol 2 months
-INAH 6 months, Rifampicin 6 months
Good data in adults-East African/British MRC studies 1970s
-Singapore Tuberculosis Service/British MRC 1970s & 1980s
-Hong Kong Chest Service/British MRC 1970s & 1980s
Criteria-pulmonary disease (TB adenopathy)
-fully sensitive organism
TREATMENT: HOW LONG?

‘SHORT COURSE’ Criteria-pulmonary disease (TB adenopathy)
-fully sensitive organism (usually unknown in paediatrics)
- mostly adult data
HOW LONG TO TREAT CHILDREN?
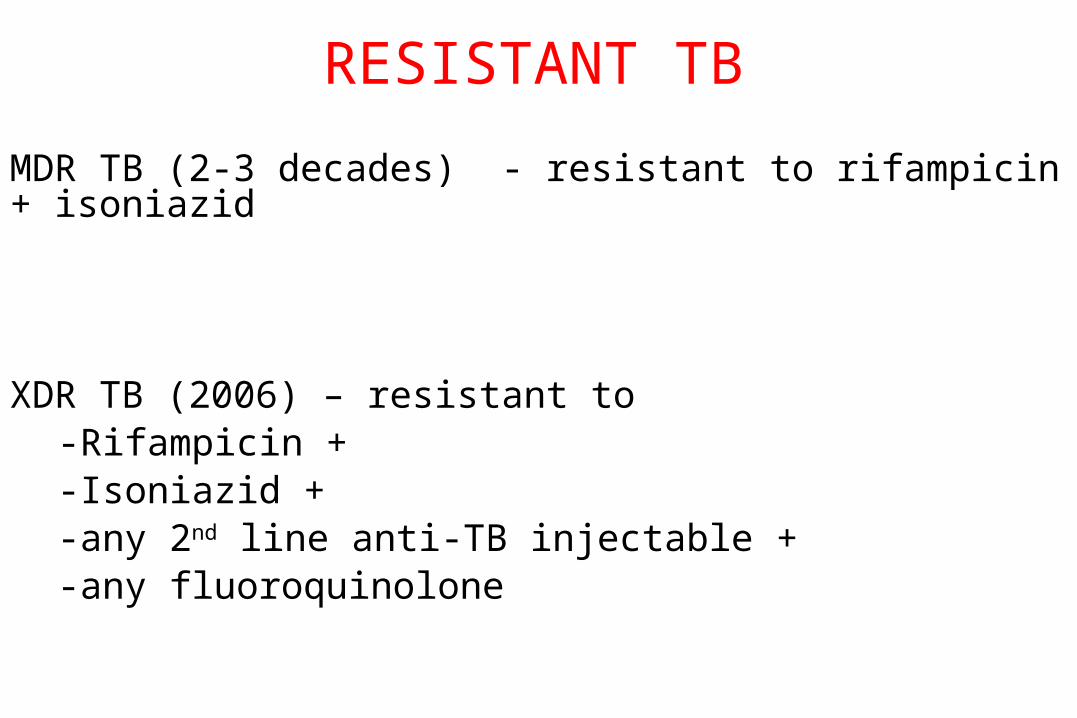
RESISTANT TB
MDR TB (2-3 decades) - resistant to rifampicin + isoniazid
XDR TB (2006) – resistant to -Rifampicin +-Isoniazid +-any 2nd line anti-TB injectable +-any fluoroquinolone
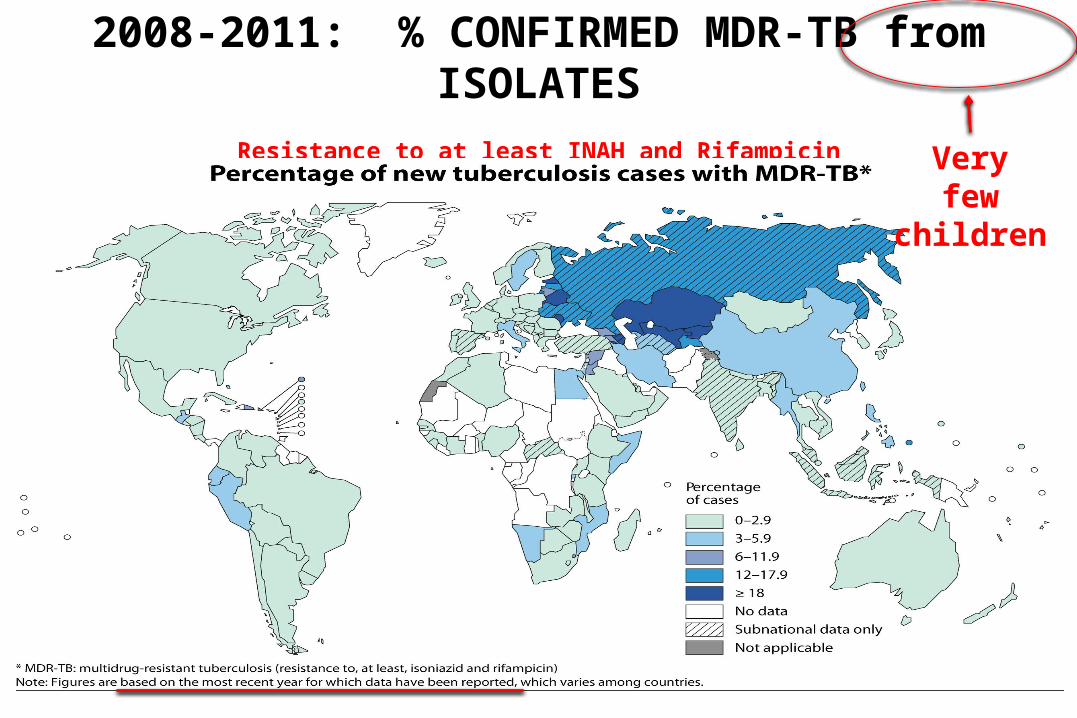
2008-2011: % CONFIRMED MDR-TB from ISOLATES
Resistance to at least INAH and Rifampicin(2010 global prevalence; 650,000 cases)
Very few children
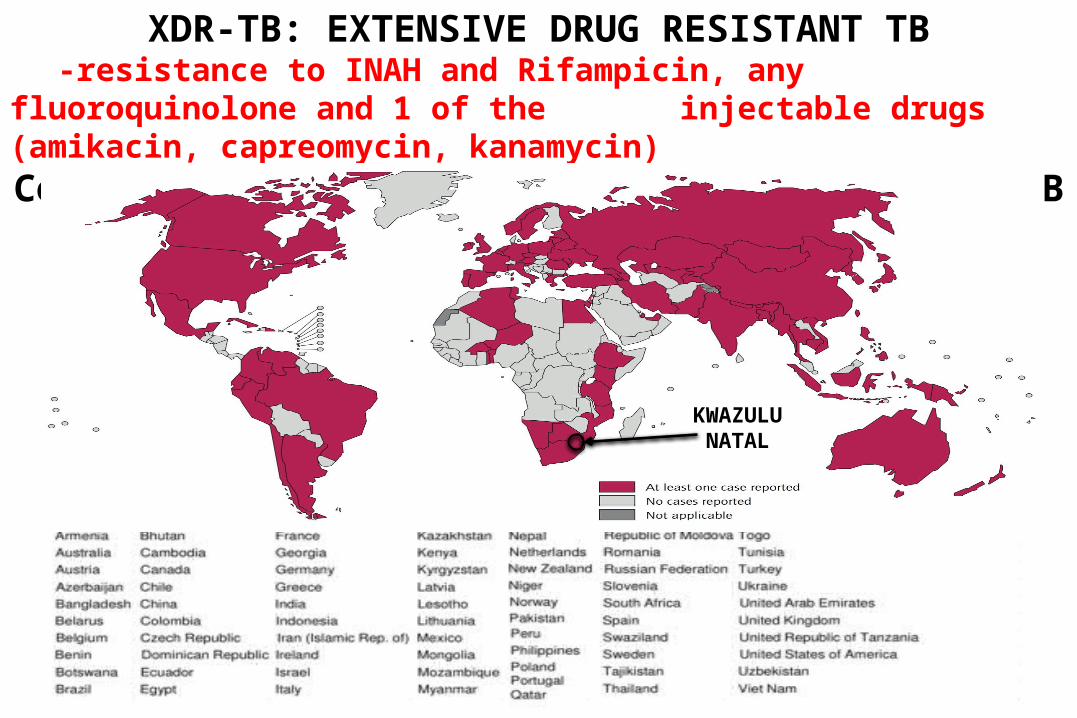
XDR-TB: EXTENSIVE DRUG RESISTANT TB-resistance to INAH and Rifampicin, any fluoroquinolone and 1 of the
injectable drugs (amikacin, capreomycin, kanamycin)Countries that had reported at least one XDR-TB case by Oct 2012
KWAZULUNATAL

TUGELA FERRY (KZN, SOUTH AFRICA)

-544 TB patients
-221 MDR TB
-53 XDR TB (55% primary infection)
-44 HIV tested; ALL +ve
-52 died within 25 days diagnosis
transmission
mortality
association with HIV
Must have spread to children but no data; culture negative or not public health threat!
TUGELA FERRY (KZN, SOUTH AFRICA)2005 - 2006

MDR and XDR TB
HOW MANY ARE CHILDREN?
Not an immediate public health threat but many will be infectious in the future.

2nd line drugs with anti-TB activityStreptomycin CycloserineAmikacin RifabutinCapreomycin RifapentineCiprofloxacin EthionamideOfloxacin ProthionamideSparfloxacin ClofazamineThiacetazone LinezolidPAS ClarithromycinIFN TNF
2nd line for good reasons- limited paediatric data- complex drug interactions-↑toxicities,↓tolerability
Promising new drugs;
Moxifloxacin PA 824 (Nitroimidazol-oxazine)
TMC-207 (Bedaquiline) Sirturo™ (metronidazole
class)

EXTRA PULMONARY DISEASE (paucity of data)(2 months intensive treatment)
Joint / bone
-? 9-12 months
CNS
-12 months at least, ? 18-24 months if tuberculomata
-steroids for 1 month
-4th drug initially ethambutol
But why should it take longer to sterilise extrapulmonary lesions?
HIV
-?12 months (relapse with same organism: SA children treated for 6/12)
TREATMENT sensitive MTB: HOW LONG?
PAEDIATRIC TB
ADHERENCE
If you don’t take the
drugs,
the drugs won’t work.

HEPATITIS
-rare in children
-usually with predisposing co-morbidity e.g. HIV, viral hepatitis
? Only routinely measure LFTs at start of therapy
BUT with newer ↑in recommended doses need to be vigilant
DRUG TOXICITY
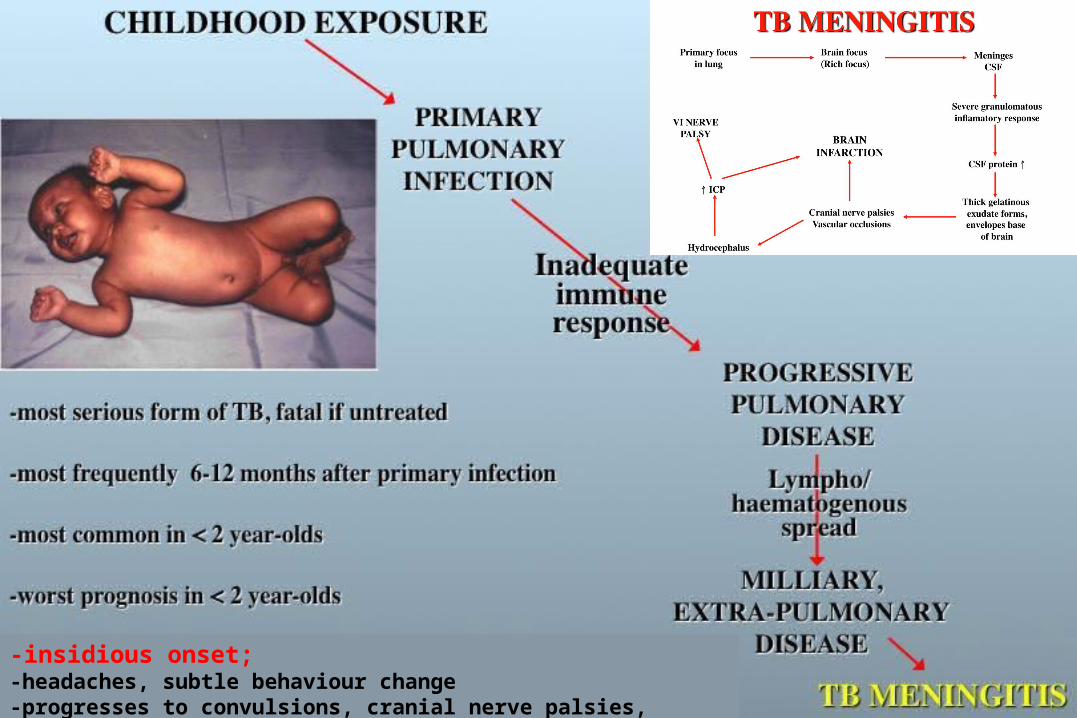
-insidious onset;-headaches, subtle behaviour change-progresses to convulsions, cranial nerve palsies, hemiplegia, coma, DEATH

TB MENINGITIS DIAGNOSISCSF (textbook description)
-lymphocytes, low sugar, high protein, AFB visible
But, Mycobacteria don’t read textbooks
Early disease;
-often polymorphs
-protein can be normal initially
-sugar can be normal initially
Usually -no visible organisms

CSF ABNORMALITIES IN MENINGITIS (%)Donald et al. 1987; J Trop Ped; 33: 213-216 Viral Neisseria Haemophilus Streptococcus Tuberculous
Investigation meningitis meningitidis influenzae pneumomiae meningitis
Cell count >500x106/l 12 81 74 70 3
Protein >0.8 g/l 7 83 84 97 76
Glucose< 2.2mmol/l 1 76 73 75 64
CSF/bloodglucose : <0.4 7 79 74 91 79
Organisms seenon microscopy 0 65 47 85 8
Number of cases 108 140 47 34 62
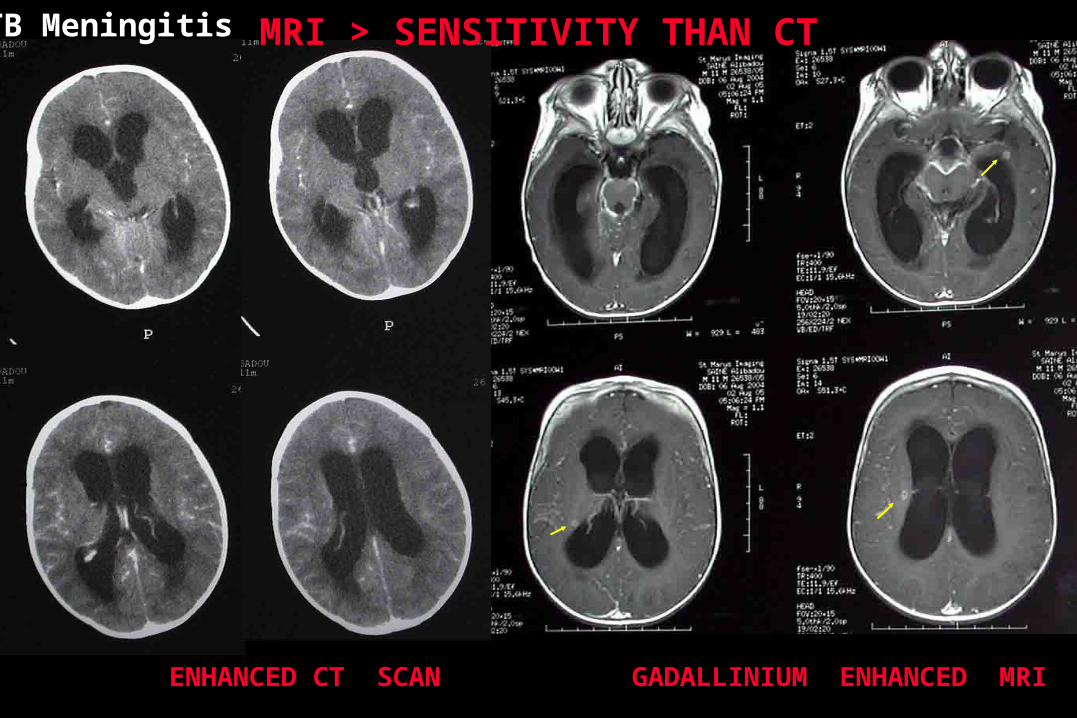
ENHANCED CT SCAN GADALLINIUM ENHANCED MRI
MRI > SENSITIVITY THAN CTTB Meningitis


MRI > SENSITIVITY THAN CT
ENHANCED CT SCAN GADALLINIUM ENHANCED MRI
Miliary TB, no meningitis

TB MENINGITIS TREATMENTTREATMENT
Anti TB drugs;
-duration
-sensitivity
-? CSF penetration
Adjunctive therapy;
-steroids
-SIADH
-acetazolamide
-surgeryHYDROCEPHALUS

DRUG TYPICAL
MIC mg/ml
PEAK LEVELS
SERUM mg/ml
PEAK LEVELS
CSF mg/ml
% PENETRATION
INAH 0.025-0.5 4.4 3.2 80
RIFAMPICIN 0.006-0.2 11.5 0.78 6.8
PYRAZINAMIDE 12.5 50 50 100
ETHAMBUTOL* 1 1.2-8 0.9-4.2 52-75
STREPTOMYCIN 2.1-10 30 2 6.6
MOXIFLOXACIN** 0.37 5.49 4.07 74
* poor penetration of ethambutol across non-inflamed meninges**Kanellakopoulou k et al. J Anti microb Chemo. 2008 61; 1328-31
CSF penetration of anti-TB drugs

? PAEDIATRIC CNS DRUG DOSES
ISONIAZID 15 mg/kg/day ?20 if < 10kg
RIFAMPICIN 15 mg/kg/day ?20 if < 10kg
PYRAZINAMIDE 30-40 mg/kg/day 40 if < 10kg
ETHAMBUTOL 20 mg/kg/day
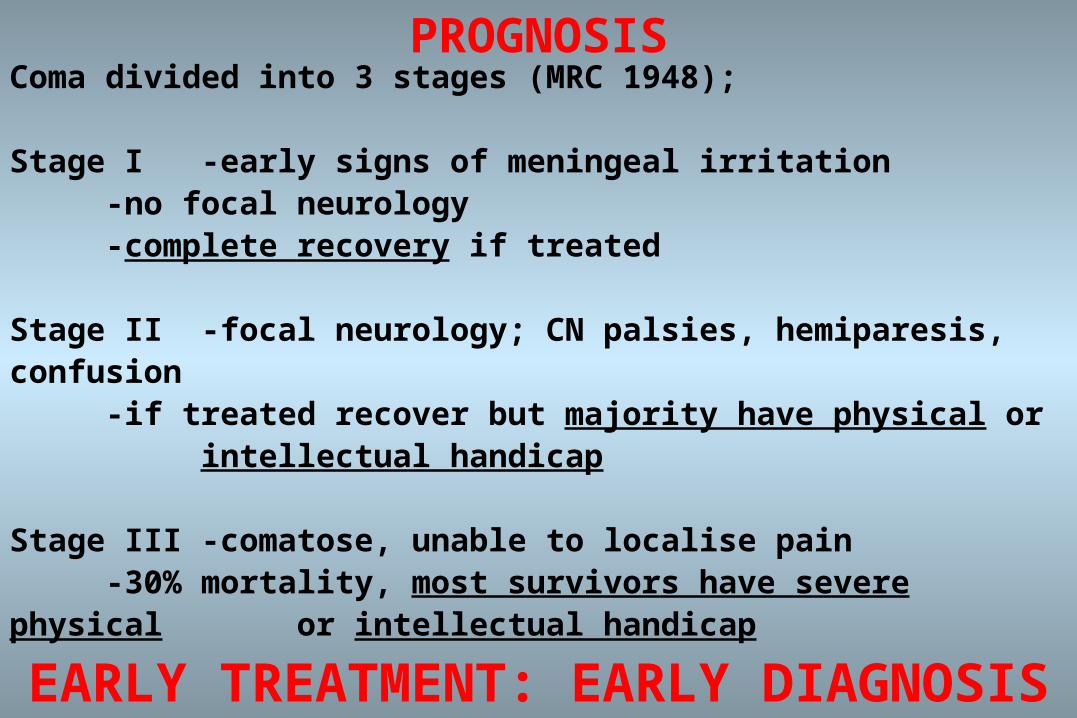
PROGNOSISComa divided into 3 stages (MRC 1948);
Stage I -early signs of meningeal irritation-no focal neurology-complete recovery if treated
Stage II -focal neurology; CN palsies, hemiparesis, confusion-if treated recover but majority have physical or
intellectual handicap
Stage III -comatose, unable to localise pain-30% mortality, most survivors have severe physical
or intellectual handicap
EARLY TREATMENT: EARLY DIAGNOSIS
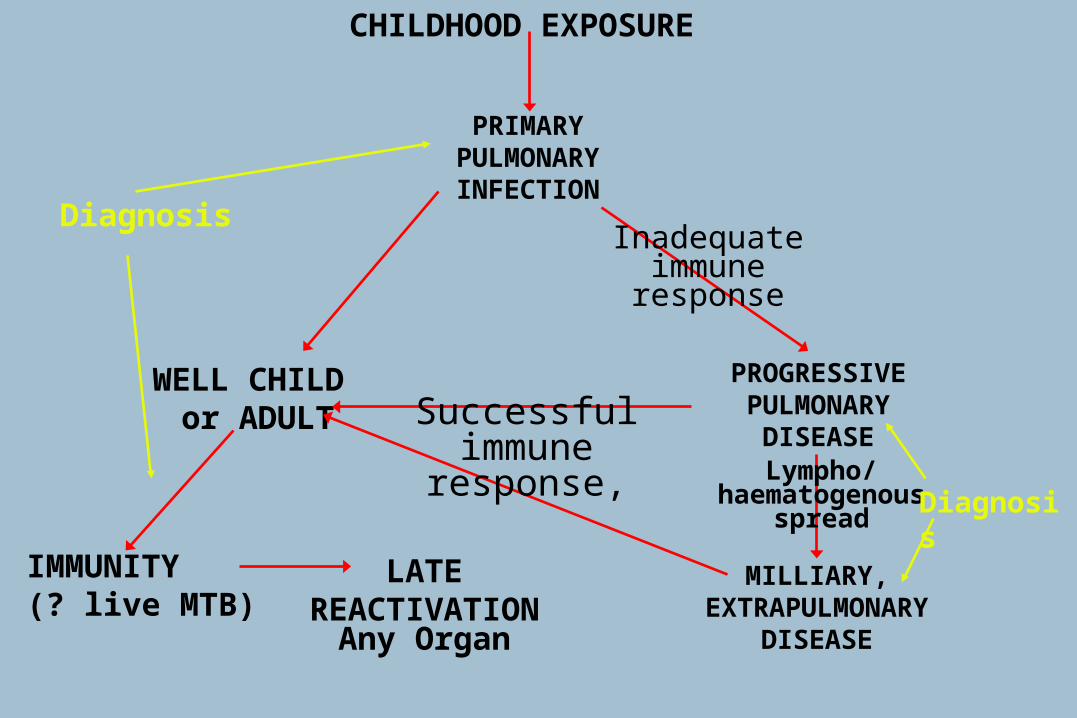
CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
WELL CHILD or ADULT
IMMUNITY(? live MTB)
LATEREACTIVATION
Any Organ
PROGRESSIVEPULMONARY
DISEASE
MILLIARY,EXTRAPULMONARY
DISEASE
Inadequateimmuneresponse
Successfulimmune response,
Lympho/haematogenous
spreadDiagnosis
Diagnosis

Difficulty in diagnosis–Primary TB
• Non-specific symptoms• Tuberculin reaction -ve• X-ray changes non-specific
–Progressive primary• Non-specific symptoms• Pauci-bacillary• Tuberculin reaction ve• X-ray changes non-specific
–Post-Primary, late reactivation (Adult)• Cavitating pulmonary disease (any organ
involved)• Tuberculin reaction +ve (usually)
PAEDIATRIC TUBERCULOSIS
Difficulty in diagnosis–Primary TB
• Non-specific symptoms• Tuberculin reaction -ve• X-ray changes non-specific
–Progressive primary• Non-specific symptoms• Pauci-bacillary• Tuberculin reaction ve• X-ray changes non-specific
–Post-Primary, late reactivation (Adult)• Cavitating pulmonary disease (any organ
involved)• Tuberculin reaction +ve (usually)
PAEDIATRIC TUBERCULOSIS
Easy for adult TB colleagues !

DIAGNOSIS OF TB IN CHILDREN
Microscopy / culture ‘gold standard’
(pauci-bacillary, prolonged culture)-respiratory secretions
-sputum (need > 5000/ ml to see AFB)-gastric washings > BAL-?induced sputum vs gastric washings**
-CSF, bone marrow, lymphoid tissue, etc.
Paediatric TB: 104-106 bacteria
**Induced sputum >> gastric lavage for microbiological confirmation of pulmonary tuberculosis in infants and young children: a prospective study. H J Zar et al. Lancet, 2005; 365:130-134
**Induced sputum or gastric lavage for community-based diagnosis of childhood pulmonary tuberculosis? Showed equivalence. M Hatherill, H J Zar et al. Arch Dis Child, 2009;94:195-201

Diagnostic testsImmunology
Host response
Tuberculin antigen-specific skin test (TST) production of IFN
Microbiology
Organism
smear culture DNA
Histology

TUBERCULIN SKIN TEST (used since 1890)-measures;
-degree of hypersensitivity to PPD
-does not measure; -immunity to tuberculosis
-time of infection
-presence or extent of disease
-poor specificity, does not distinguish between; -TB disease and TB infection
-BCG
-atypical mycobacteria
-poor sensitivity, can be falsely negative in;-early infection, disseminated disease
-other acute infections (measles, pertussis), live vaccines
-severe malnutrition
-immunocompromised
In children negative test does not exclude TB
Problems with SpecificityLow Sensitivity in young kids

IGRAs
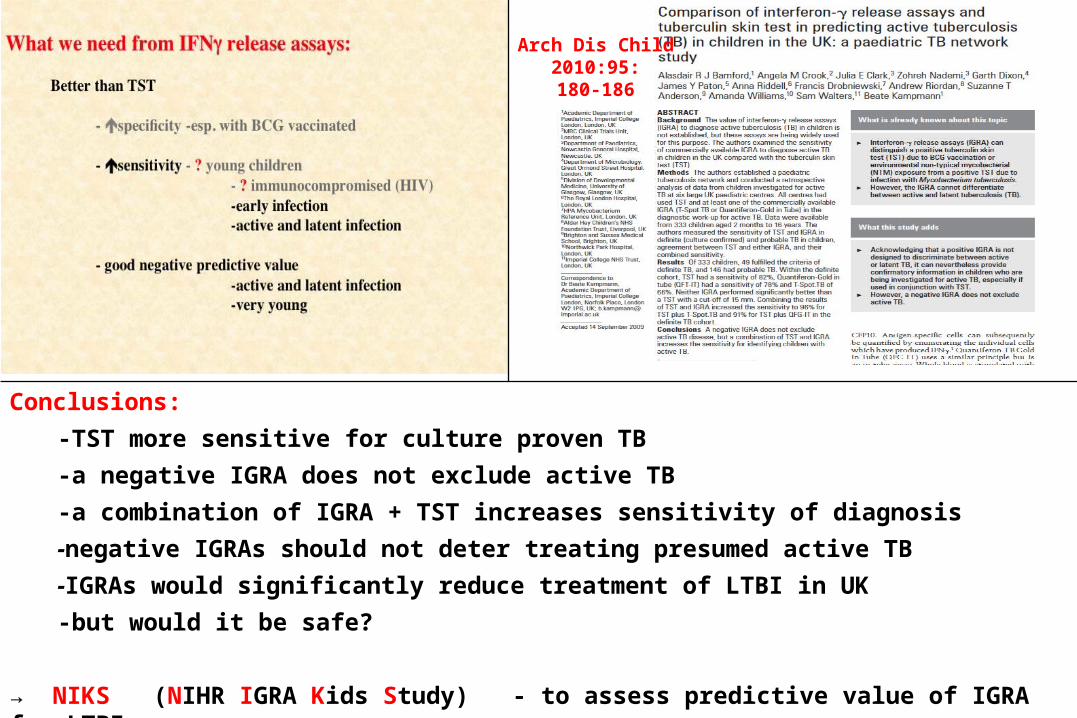
Arch Dis Child2010:95:180-186
Conclusions:
-TST more sensitive for culture proven TB
-a negative IGRA does not exclude active TB
-a combination of IGRA + TST increases sensitivity of diagnosis
-negative IGRAs should not deter treating presumed active TB
-IGRAs would significantly reduce treatment of LTBI in UK
-but would it be safe?
→ NIKS (NIHR IGRA Kids Study) - to assess predictive value of IGRA for LTBI

Aims of the project
1. To determine if it is safe to withhold chemoprophylaxis from children exposed to TB with negative IGRA but positive TST
Prospective cohort study
2. To link TB exposure, infection and outcome in children via a national contact tracing module, linked to TB register
Contact module
PI: Prof B Kampmann, Imperial College; study involves 11 NHS sites in the UK

Design
TB house-hold-exposed children
TST and IGRA at screening and 2 months later
TST+ve/IGRA-ve followed for 1-2 years
Primary endpoint: Development of active TB(? NICE: how safe are the guidelines)
Secondary endpoint: how concordant are TST and IGRA(? NICE: is the step-wise screening approach justified)
Target: 500, Currently: 489
Results for secondary endpoint available in early 2014, primary endpoint: 2015

Clinical; but TB can do anything!

DIAGNOSIS OF TB IN CHILDREN
Family history
Epidemiology
Trial of treatment
DIAGNOSIS OF TB IN CHILDREN
HIGH LEVEL OF SUSPICION
Ask yourself
“WHY ISN’T THIS TB?”
CHILDHOOD EXPOSURE
PRIMARYPULMONARYINFECTION
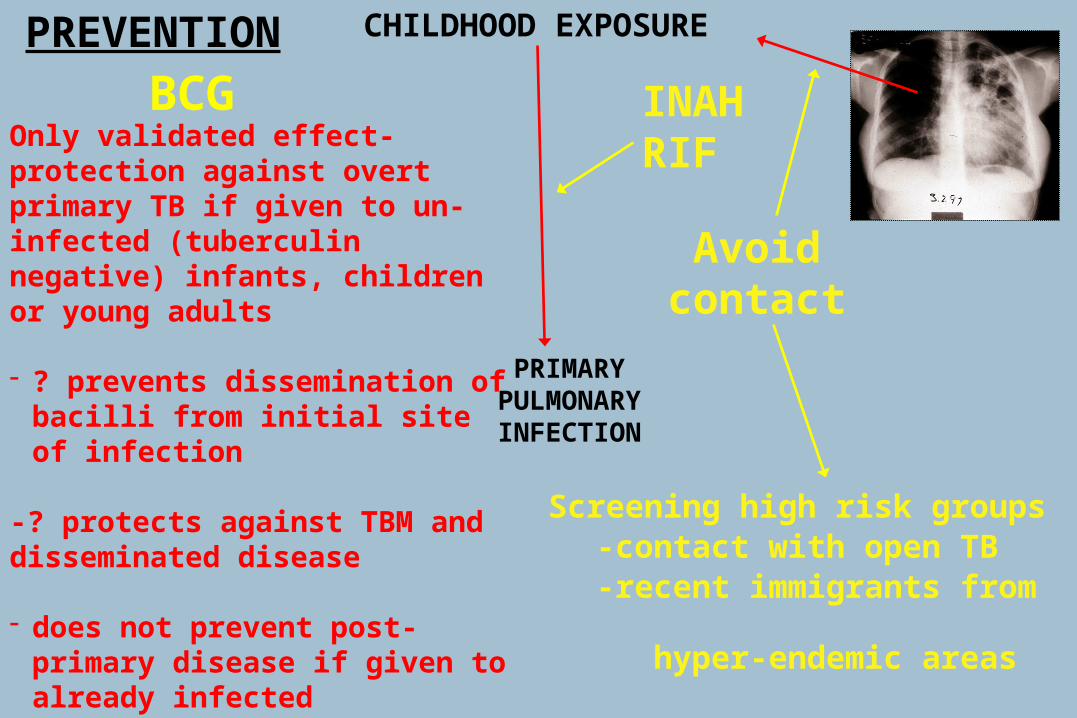
Only validated effect- protection against overt primary TB if given to un-infected (tuberculin negative) infants, children or young adults
- ? prevents dissemination of bacilli from initial site of infection
-? protects against TBM and disseminated disease
- does not prevent post-primary disease if given to already infected (tuberculin reactive) people
-can produce severe necrotising lesions
BCG
Avoidcontact
PREVENTION
Screening high risk groups-contact with open TB-recent immigrants
from hyper-endemic areas
INAHRIF

WISH-LISTBetter diagnostic tests
- differentiate between infection and disease
- global application- cheap, robust and simple
- monitor success of therapyBetter immunisationBetter treatments
- drugs/regimens- ? immunotherapy- ? other
Better delivery of healthcare
PAEDIATRIC TUBERCULOSIS
WISH-LISTMore data; better understandingBetter diagnostic tests
- differentiate between infection and disease
- global application- cheap, robust and simple
- monitor success of therapyBetter immunisationBetter treatments
- drugs- ? immunotherapy- ? other
Better delivery of healthcare
PAEDIATRIC TUBERCULOSIS
Better understandingMore dataMore research







