
Paediatric Abdominal Trauma
LA HodsdonOct 09
UPDATE ON BURNS MANAGEMENT IN CHILDRENUPDATE ON BURNS MANAGEMENT IN CHILDREN

Considerations
• Incidence• Type• Anatomical Considerations• History & Examination• Diagnostic Modalities• Suggested Investigative Approaches

Incidence:
• Abdominal Trauma:
– 8-10% admissions to Paediatric Trauma Centres– 3rd most frequent cause of death ()– MOST COMMON UNRECOGNIZED FATAL INJURY– NAI – 5% admitted with Abdominal Trauma

Type of Injury:
• Blunt Abdominal Trauma:
– 85% of paeds abdo trauma (US/UK)– > 50 due to MVA’s– Other common causes bicycles, sports, falls, NAI
• RSA ?% Penetrating Trauma – Likely to be >15%

Anatomical Considerations:
• Solid Organs: proportionally larger & more anterior
• Kidneys: larger, more mobile +/- foetal lobulations
• Subcutaneous Fat: ↓• Abdominal Musculature: ↓• AP Diameter: ↓• Flexible Cartilaginous Ribcage
• Increased Solid Organ Injury– Both Blunt & Penetrating Injury
• GIT Trauma not uncommon– Duodenal & Small Bowel haematomas &
perforation– Pancreatic injuries– Mesenteric lacerations

History & Examination:
• Age dependant
• Often difficult for kids to localise / verbalise
• FEAR– Often hard to reassure– Fear of unknown / vague concepts– Separation– Fear of Medical Personnel
• Haemodynamically stable child- who is alert and co-operative- able to communicate effectively
history and examination approach reliability rates of adults

2004 Poletti et al:Awake, haemodynamically stable (adults): abdo pain, tenderness & peritoneal signs more reliable physical signs & can be found in 90%
BUT significant injuries can be missed No physical signs ≠ exclude intra-abdominal injury 7.1% pts with normal physical examination = intra-
abdominal injuries on CT
Multiple small studies suggest normal examination excludes the need for therapeutic surgery
Plain X-Rays
• Free Air– Gastric, duodenal bulb & colonic perforation– Only 25-33% of jejunal & ileal perforations have FA– Better viewed on CT
• Foreign Bodies
• Projectory Paths

FAST
• Advantages:– Rapid ID of Intraperitoneal Haemorrhage– Non Invasive– Portable – Rapid (5min FAST)– Widespread (US) therefore not rely on
Radiologists– Serial examinations possible– No side effects

FAST
• Disadvantages:– Not able to image extent of organ damage– Not able to visualise retroperitoneum– Operator dependant– Patient dependent– Can’t differentiate blood from ascites– Can’t pick up contained bleeding

FAST in ABDO Trauma
• Most studies: – sensitivity for haemoperitonium 86-89%– Depends on required end point (Intra-abdominal
Injury / Intra-abdominal Injury requiring ø / Potentially Fatal intra-abdominal Injury)
• Ollerton et al: U/S & Trauma Management– Changed Mx decisions 32.8% of time– ↓ CT (4734%) & ↓ DPL (91%)
• Branay et al: U/S key pathway– ↓CT (5626%) & ↓DPL (17-4%)
FAST: Reliability in Kids:• Holmes: 224 kids (mean age 9 yrs)
– Prospective– Hypotension (13): 100% sens, 100% spec– All Patients (244): 82% sens, 95% spec
• Soudack: 313 kids (2months – 17yrs)– Retrospective– 275 Negative FASTs– 73 of Negative FASTs had abdominal signs & CTs:
• 3 Positive – Parenchymal Injuries, none requiring ø
– 92.5% sens, 97.% spec
CT Scan• Advantages
– Define extent of injury & organ involvement– Non Invasive– Most Accurate S/I for Solid Organ injury– Evaluates retroperitoneum
• 3 Contrast Studies have 97% sens, 98% spec• Velmahos et al achieved similar rates with IVI
contrast alone.

CT Scan
• Disadvantages– Time consuming & unable to monitor patients– Requires IVI Contrast– Requires Sedation in most kids– Can’t visualise pancreas, diaphragm, small bowel
or mesentery– Radiation Dose – Brenner et al
1 yr old child: lethal malignancy risk of 1 abdominal CT was ± 1 in 550

CT Scan in Kids
• High Sensitivity & Specificity for the solid organ pattern common in kids
• Radiation dose and need for sedation major drawback in kids, so CT scans should be considered not just ordered as ‘routine’

DPL
Rapidly reveals/excludes the abdomen as the source of hypotension
AdvantagesMay detect Bowel Injury (GIT matter)
DisadvantagesInvasive with complication rate of 0.3%Operator dependantComparatively time consuming (vs. FAST)
Widespread replacement by FAST

Other Diagnostic Modalities
• Local Wound Exploration:– Bedside surgical exploration of tract– Determine whether Peritoneal Violation has taken
place– Patient Factors
• Contrast Studies• Angiography• ERCP• Laparoscopy

Management Questions:Blunt Abdominal Trauma
– Trauma vs. Medical component– Single vs. Multisystem trauma– Emergency Laparotomy vs. Dx workup– Single vs. Multiple Intraperitoneal Injury– Expectant vs. Necessary Laparotomy
Paediatric patients tolerate expectant management better than adults.
If paediatric patient is stable and adequate monitoring is available: normally follow expectant management.



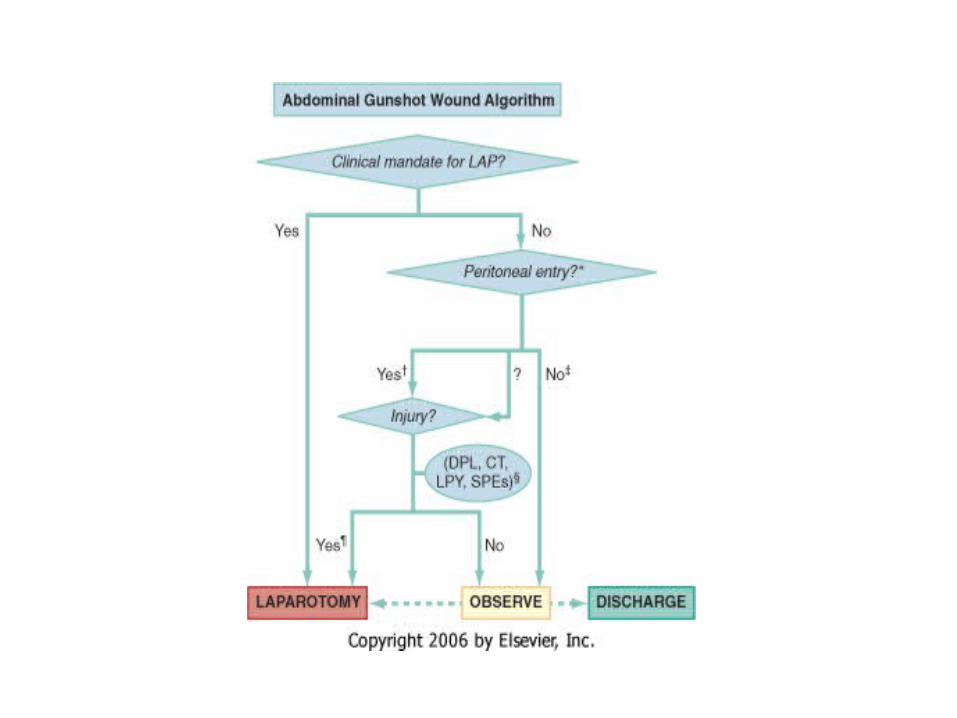
Management Questions:Penetrating Trauma
• Trauma vs. Medical component• Single vs. Multisystem trauma• Emergency Laparotomy required?• Peritoneal Violation?• Intraperitoneal Injury?
Stab Wounds – 70% have peritoneal violation but only 25-33% of those require surgery.
Expectant: Shaftan 1960’s



Operative vs. Non-operative Management.
Successful: mod – high grade liver / spleen trauma
Failures considerable morbidity / mortality Balance between avoiding unnecessary
laparotomy & preventing significant morbidity or mortality by waiting too long.
Requirements: Patient – alert & co-operative, mild-mod MOAInstitution - experienced nursing staff, trauma
surgeons, radiologists & facilities for urgent laparotomy

• Pitfalls:1) Hollow Viscera Injuries: missed2) Increased use of blood products 3) Approach will fail if haemorrhage ≠ respond to Rx
angiography + embolization or not abate from solid organs.
Time from injury operation: increase morbidity and mortality.
Resources:
Advances in Abdominal Trauma; J.L . Isenhour, MD, J Marx, MD; Emerg Med Clin N Am 25 (2007) 713–733
Pediatric Major Trauma: An Approach to Evaluation and Management; J.T. Avarello, MD, FAAP, R.M. Cantor, MD, FAAP, FACEP; Emerg Med Clin N Am 25 (2007) 803–836
Rosen’s Emergency Medicine Emergency Medicine Manual, 6th Ed; O.John Ma & Davis
M Kline Oxford Handbook of Trauma for Southern Africa; A Nicol
& E Steyn







