HPV
Molecular
Pa Po Va virus
Molecular
Oncogenesis
Nam Hoon Cho, M.D.
Yonsei Univ Coll Med, Dept of Pathology

Presentation FlowHPV testing guideline: pros and cons
HC-2
Genotyping
HPV genome new highlight-HPV genome new highlight-
E6-E6AP-PDZ binding
E1^E4 and E2^E5
Controversial issue in cytopathology
What is phenotype with ASCUS?
CIN 2 from the viewpoint of HPV
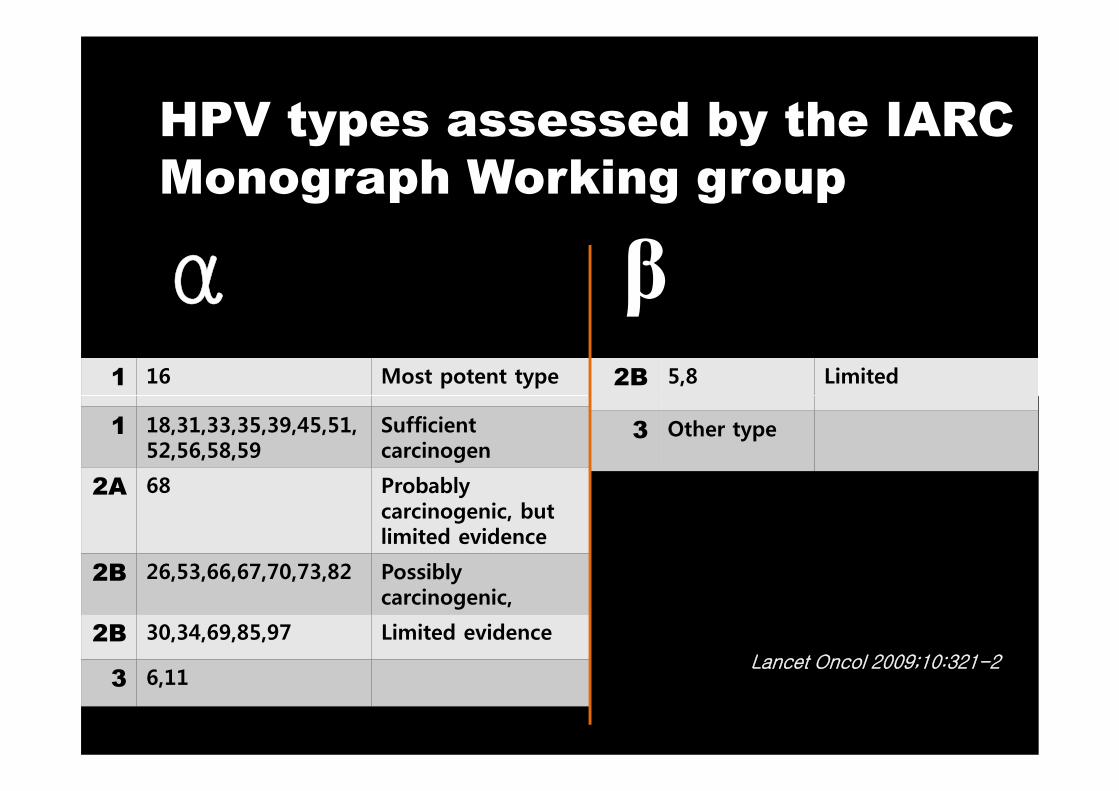
HPV types assessed by the IARC
Monograph Working group
α β1 16 Most potent type 2B 5,8 Limited
1 18,31,33,35,39,45,51,52,56,58,59
Sufficient carcinogen
2A 68 Probably carcinogenic, but limited evidence
2B 26,53,66,67,70,73,82 Possibly carcinogenic,
2B 30,34,69,85,97 Limited evidence
3 6,11
3 Other type
Lancet Oncol 2009;10:321-2
HPV types assessed by the IARC
Monograph Working group
α β1 16 Most potent type 2B 5,8 Limited
HPV 58 PPV for CIN 3+= 54.9% (An HJ et al. Cancer 2003; 97:1672)
HPV frequency: 16/18/58/39,52,56,51 (Cho et al. Am J Obstet Gynecol 2003; 188:56)
1 18,31,33,35,39,45,51,52,56,58,59
Sufficient carcinogen
2A 68 Probably carcinogenic, but limited evidence
2B 26,53,66,67,70,73,82 Possibly carcinogenic,
2B 30,34,69,85,97 Limited evidence
3 6,11
3 Other type
Lancet Oncol 2009;10:321-2
(Cho et al. Am J Obstet Gynecol 2003; 188:56)
HPV with no CIN: 37.2%(Hwang et al. Gynecol Oncol 2003; 90:51)
HPV in Korean commercial sex workers:47% (16, 51) (Choi et al. J Med Virol 2003; 71:440)
HPV multiple infection in 9.1% and OR 31.8 folds for CIN 3+ (Lee et al Cancer Lett 2003;198:187)
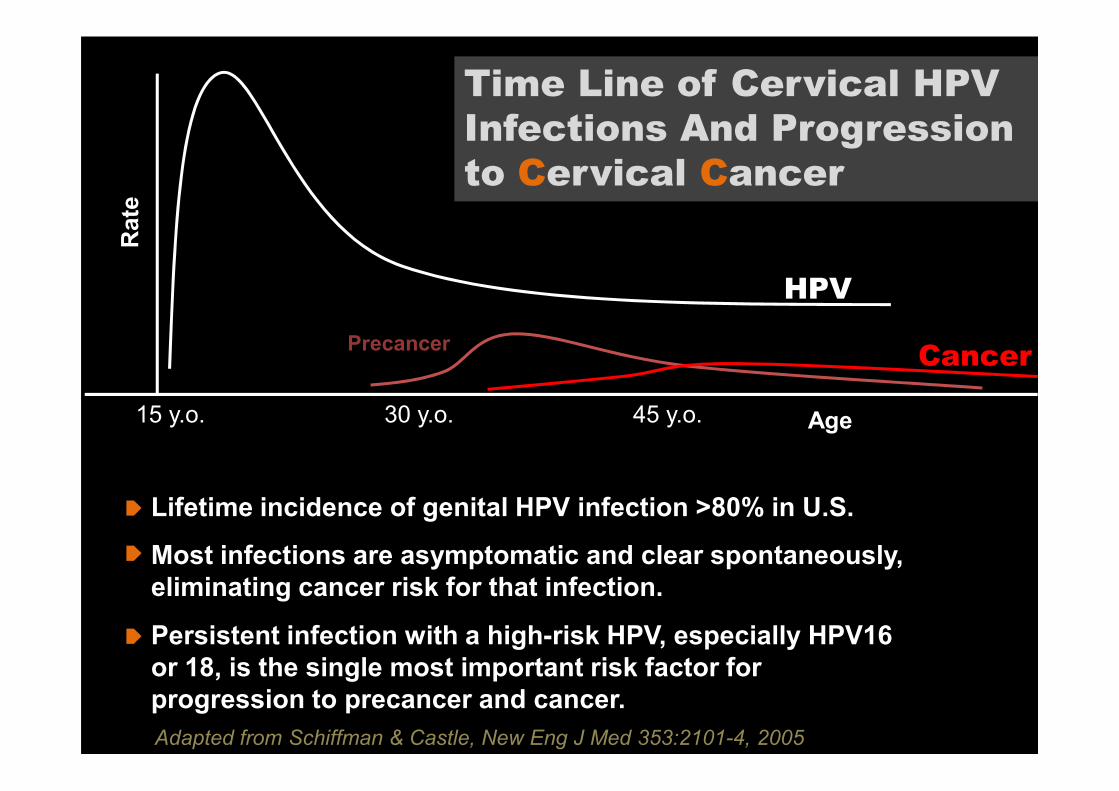
Time Line of Cervical HPV
Infections And Progression
to Cervical Cancer
HPV
PrecancerCancer
Rate
15 y.o. 30 y.o. 45 y.o. Age
Adapted from Schiffman & Castle, New Eng J Med 353:2101-4, 2005
Lifetime incidence of genital HPV infection >80% in U.S.
Most infections are asymptomatic and clear spontaneously,
eliminating cancer risk for that infection.
Persistent infection with a high-risk HPV, especially HPV16
or 18, is the single most important risk factor for
progression to precancer and cancer.
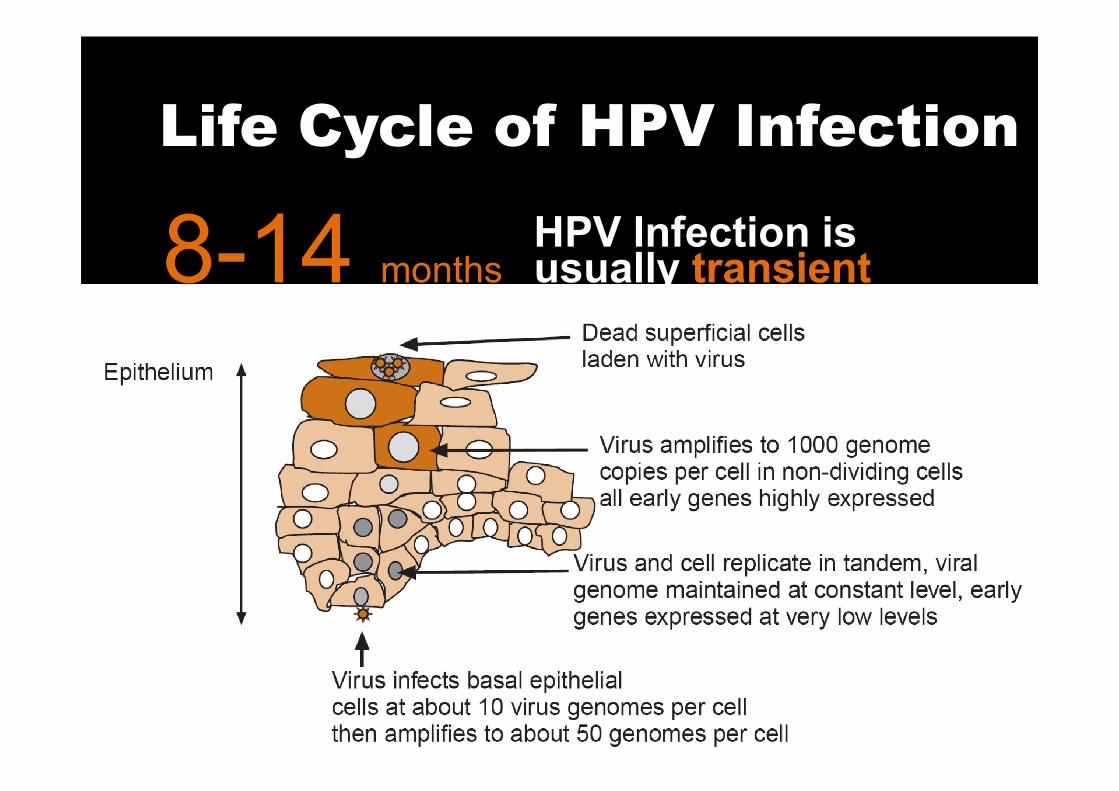
Life Cycle of HPV Infection
HPV Infection is usually transient8-14 months
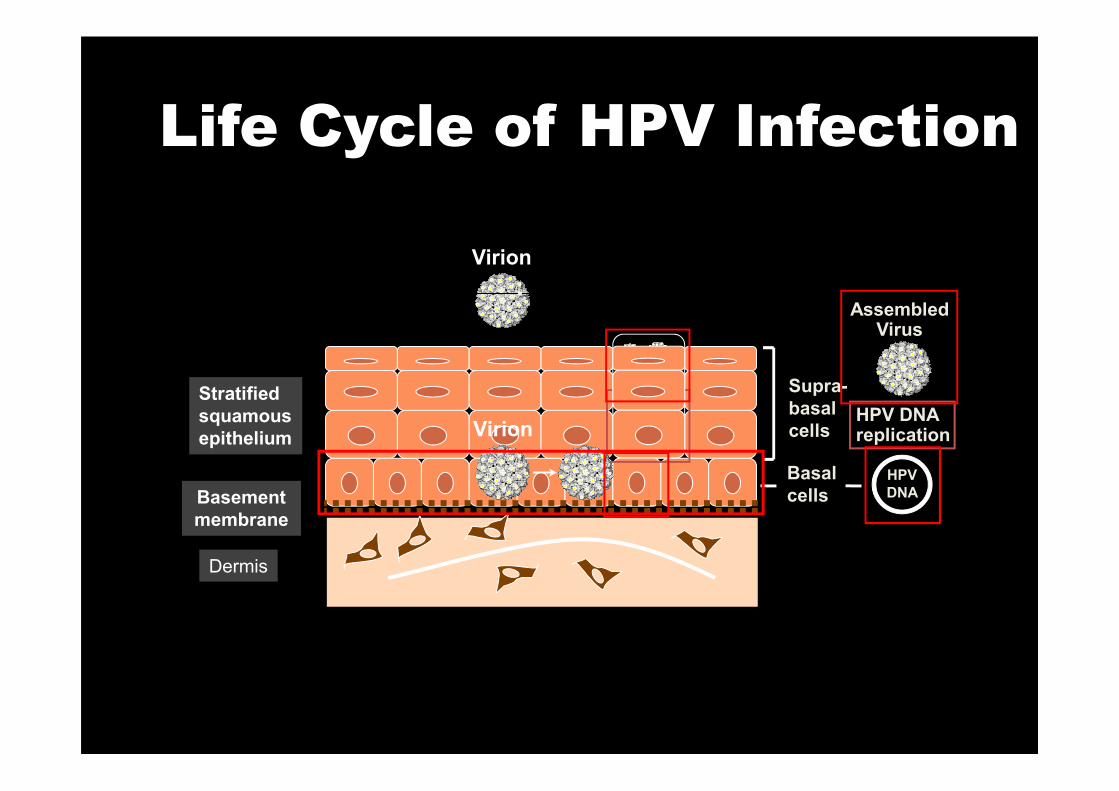
Life Cycle of HPV Infection
Stratified
Virion
Supra-
AssembledVirus
Basement
membrane
Dermis
Stratified
squamous
epithelium Virion
Supra-
basal
cells
Basal
cellsHPV
DNA
HPV DNAreplication
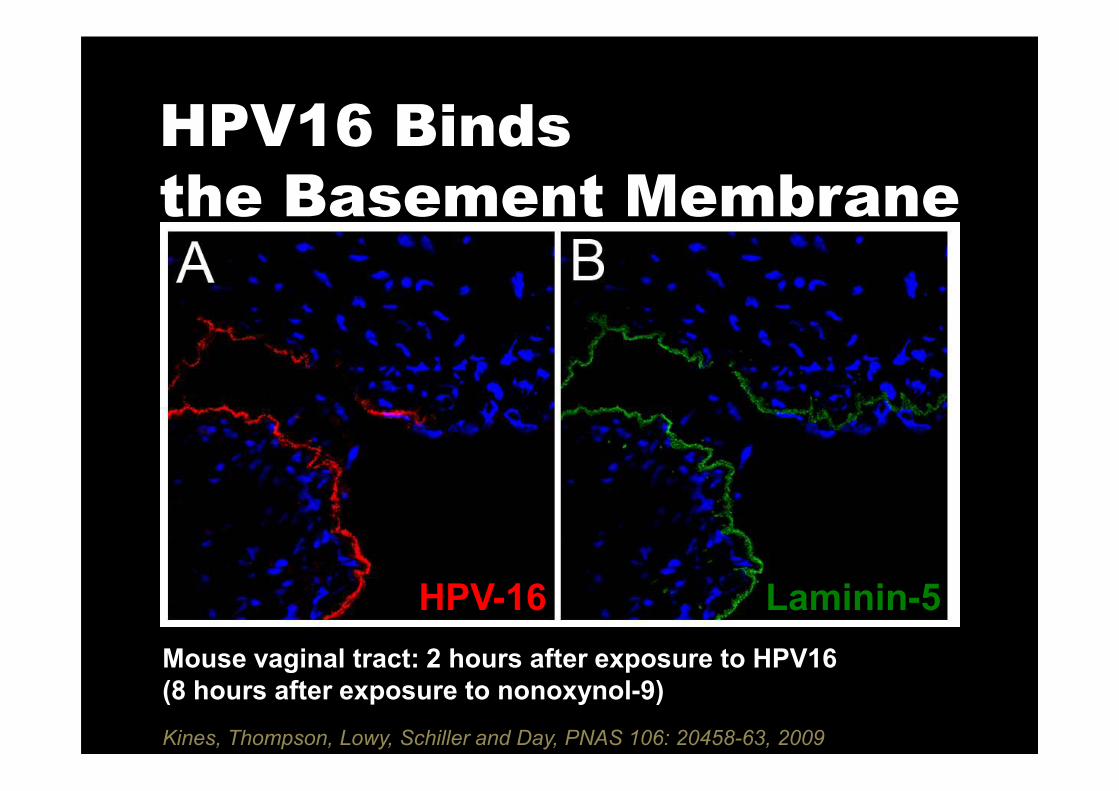
HPV16 Binds
the Basement Membrane
HPV-16 Laminin-5
Mouse vaginal tract: 2 hours after exposure to HPV16
(8 hours after exposure to nonoxynol-9)
Kines, Thompson, Lowy, Schiller and Day, PNAS 106: 20458-63, 2009
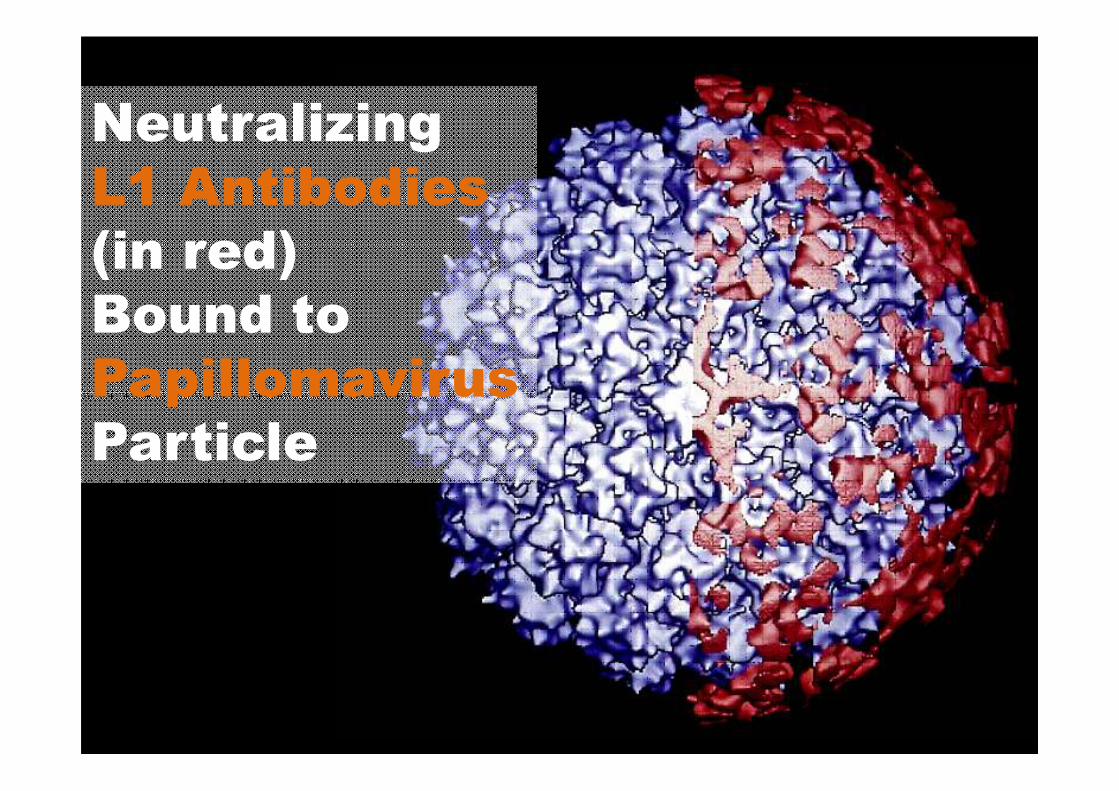
Neutralizing
L1 Antibodies
(in red)
Bound to
PapillomavirusPapillomavirus
Particle

VLP Vaccination Induces High
Titer Antibodies that Prevent
Basement Membrane BindingDay et al, Cell Host Microbe 8: 260-70, 2010
Virion
No Infection
Basement
membrane
Dermis
Stratified
squamous
epithelium
Virion
STOP
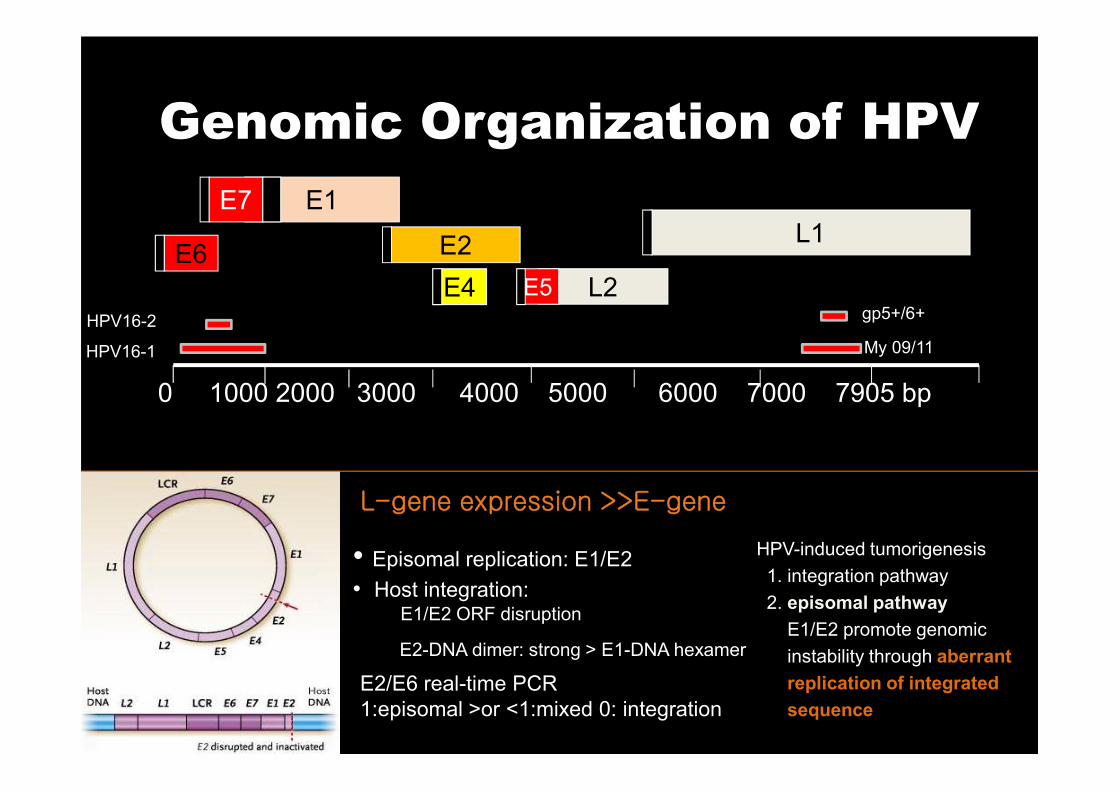
0 1000 2000 3000 4000 5000 6000 7000 7905 bp
E6
E1E7
E2
E4 L2E5
L1
My 09/11
gp5+/6+
HPV16-1
HPV16-2
Genomic Organization of HPV
• Episomal replication: E1/E2• Host integration:
E1/E2 ORF disruption
E2-DNA dimer: strong > E1-DNA hexamer
E2/E6 real-time PCR
1:episomal >or <1:mixed 0: integration
0 1000 2000 3000 4000 5000 6000 7000 7905 bp
HPV-induced tumorigenesis
1. integration pathway
2. episomal pathway
E1/E2 promote genomic
instability through aberrant
replication of integrated
sequence
L-gene expression >>E-gene
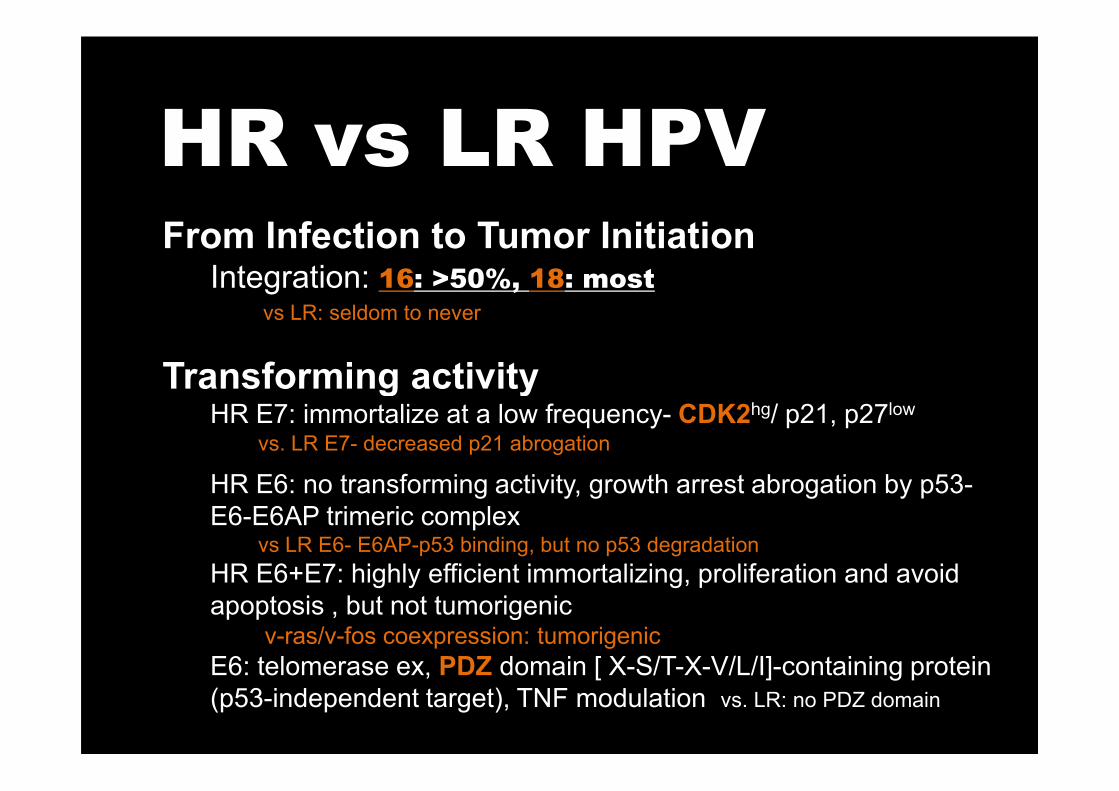
HR vs LR HPVFrom Infection to Tumor InitiationIntegration: 16: >50%, 18: most
vs LR: seldom to never
Transforming activityTransforming activityHR E7: immortalize at a low frequency- CDK2hg/ p21, p27low
vs. LR E7- decreased p21 abrogation
HR E6: no transforming activity, growth arrest abrogation by p53-
E6-E6AP trimeric complex vs LR E6- E6AP-p53 binding, but no p53 degradation
HR E6+E7: highly efficient immortalizing, proliferation and avoid
apoptosis , but not tumorigenicv-ras/v-fos coexpression: tumorigenic
E6: telomerase ex, PDZ domain [ X-S/T-X-V/L/I]-containing protein
(p53-independent target), TNF modulation vs. LR: no PDZ domain
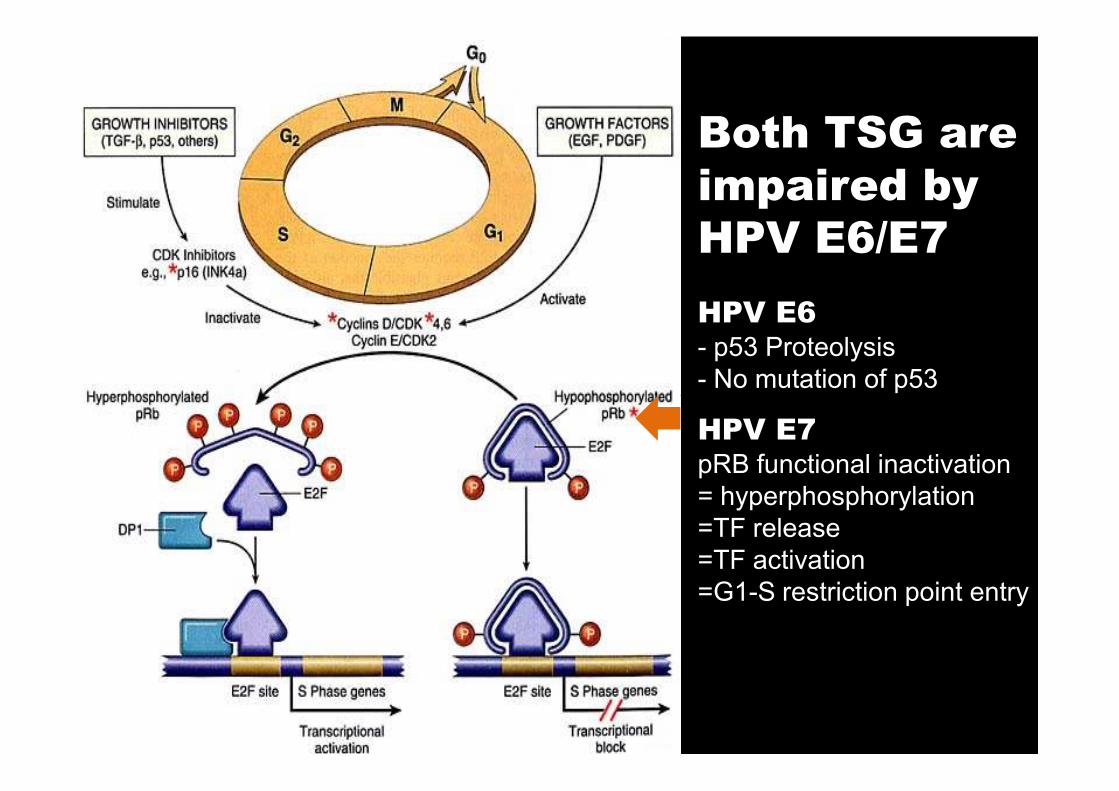
HPV E6- p53 Proteolysis
- No mutation of p53
Both TSG are
impaired by
HPV E6/E7
HPV E7pRB functional inactivation
= hyperphosphorylation
=TF release
=TF activation
=G1-S restriction point entry

E6 and PDZ domain
PDZ-domain protein: scaffolding protein
cell polarity, cell junction
E6 HR/E6AP-PDZ binding induce loss of cell polarity, EMT,
and carcinogenesis.
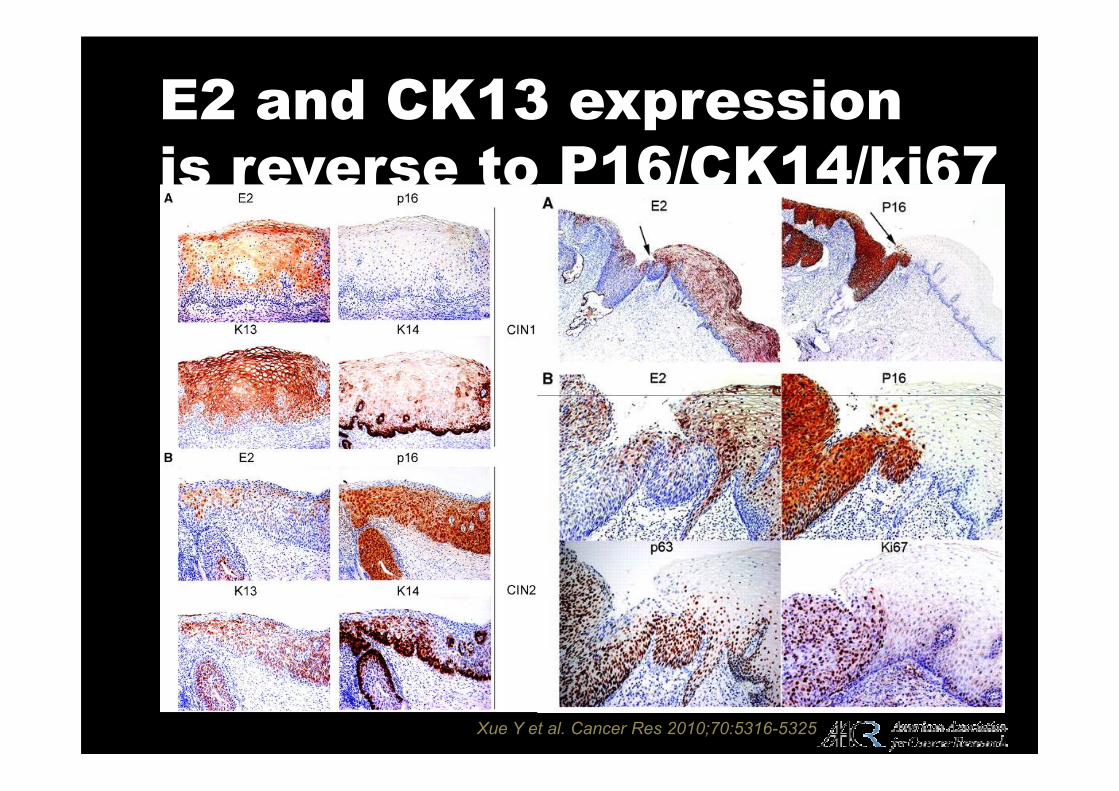
E2 and CK13 expression
is reverse to P16/CK14/ki67
Xue Y et al. Cancer Res 2010;70:5316-5325

E1^E4 (amino-terminal E1 ORF splicing to E4 ORF)E4
Long-acting multitasking
role of E4 genome
Most divergent domain in sequence according
to HPV types
L1
N terminal: Binding to cytokeratin and concomitant
destabilization of cytokeratin network
Body: cell cycle arrest at G2/M checkpoint
L1 protein encoding
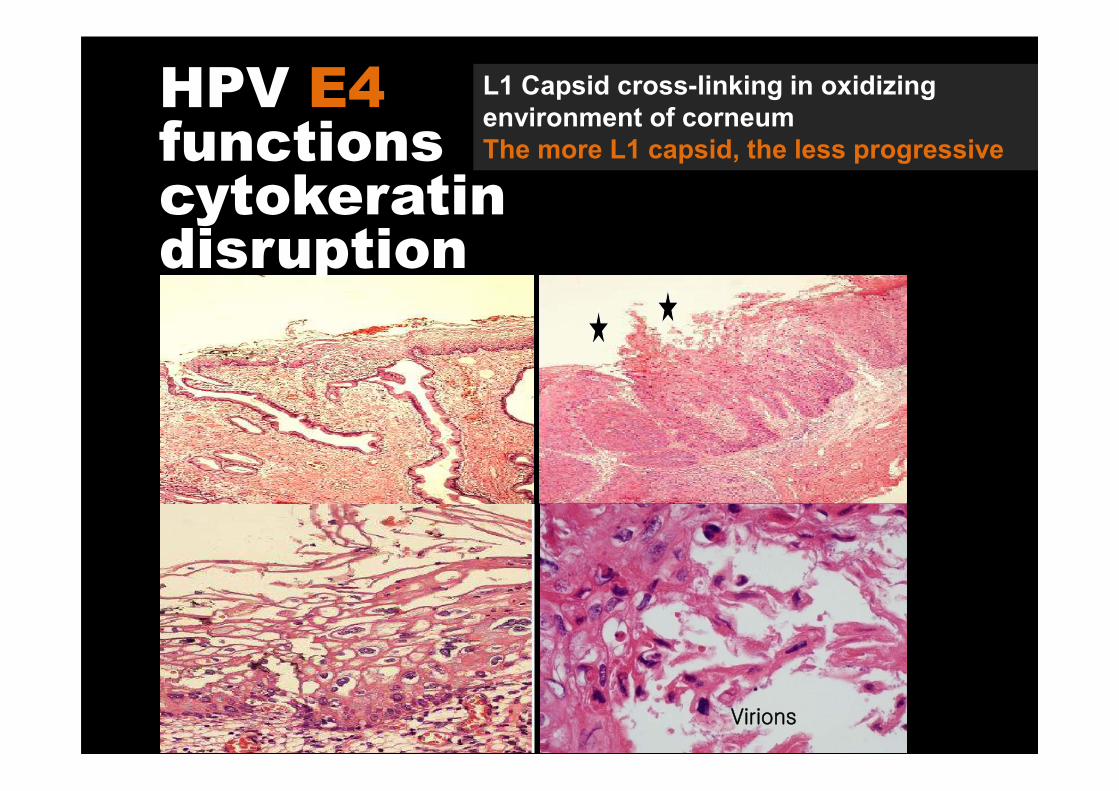
HPV E4functions cytokeratindisruption
L1 Capsid cross-linking in oxidizing
environment of corneum
The more L1 capsid, the less progressive
Virions
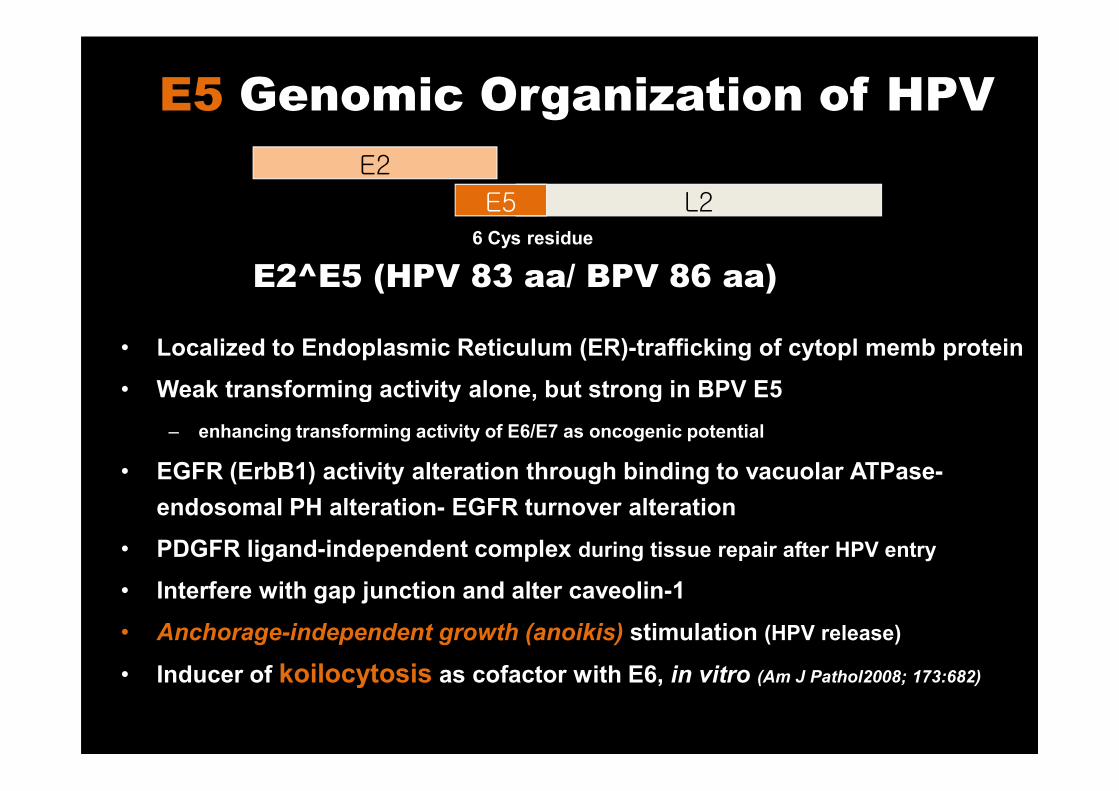
E5 Genomic Organization of HPV
E2
L2E56 Cys residue
• Localized to Endoplasmic Reticulum (ER)-trafficking of cytopl memb protein
• Weak transforming activity alone, but strong in BPV E5
E2^E5 (HPV 83 aa/ BPV 86 aa)
• Weak transforming activity alone, but strong in BPV E5
– enhancing transforming activity of E6/E7 as oncogenic potential
• EGFR (ErbB1) activity alteration through binding to vacuolar ATPase-
endosomal PH alteration- EGFR turnover alteration
• PDGFR ligand-independent complex during tissue repair after HPV entry
• Interfere with gap junction and alter caveolin-1
• Anchorage-independent growth (anoikis) stimulation (HPV release)
• Inducer of koilocytosis as cofactor with E6, in vitro (Am J Pathol2008; 173:682)
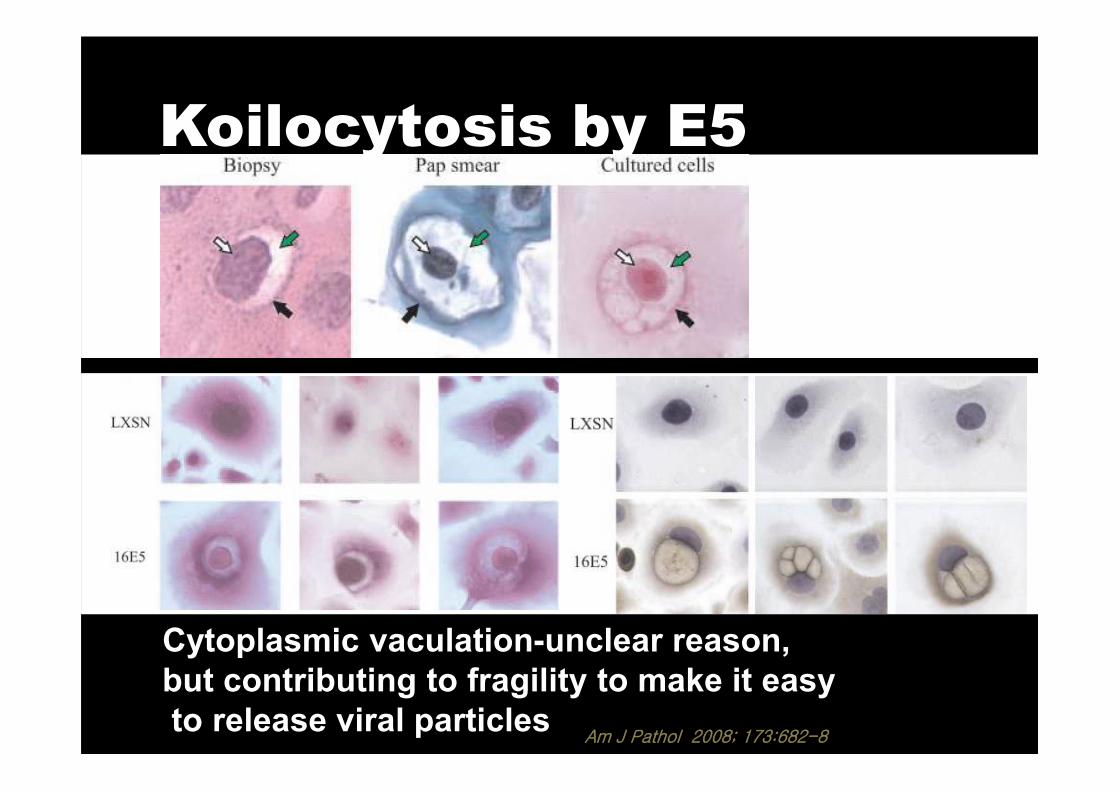
Koilocytosis by E5
Cytoplasmic vaculation-unclear reason,
but contributing to fragility to make it easy
to release viral particlesAm J Pathol 2008; 173:682-8
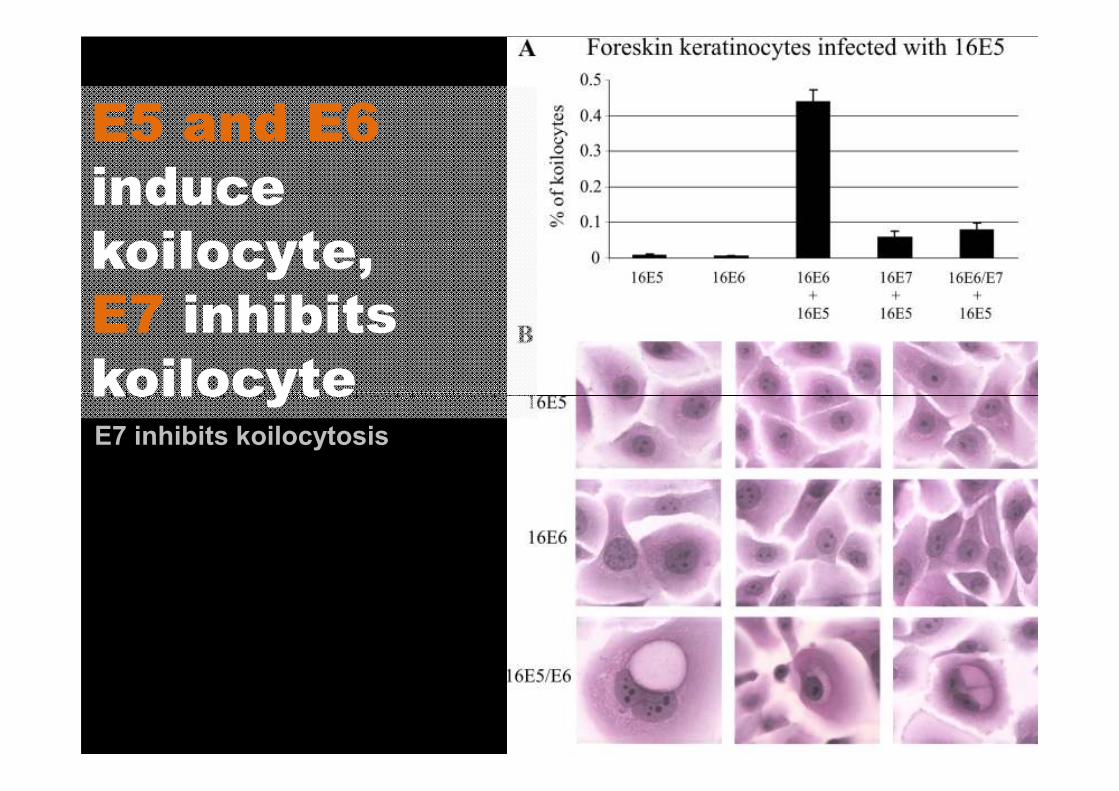
E5 and E6
induce
koilocyte,
E7 inhibits
koilocyteE7 inhibits koilocytosis
koilocyte
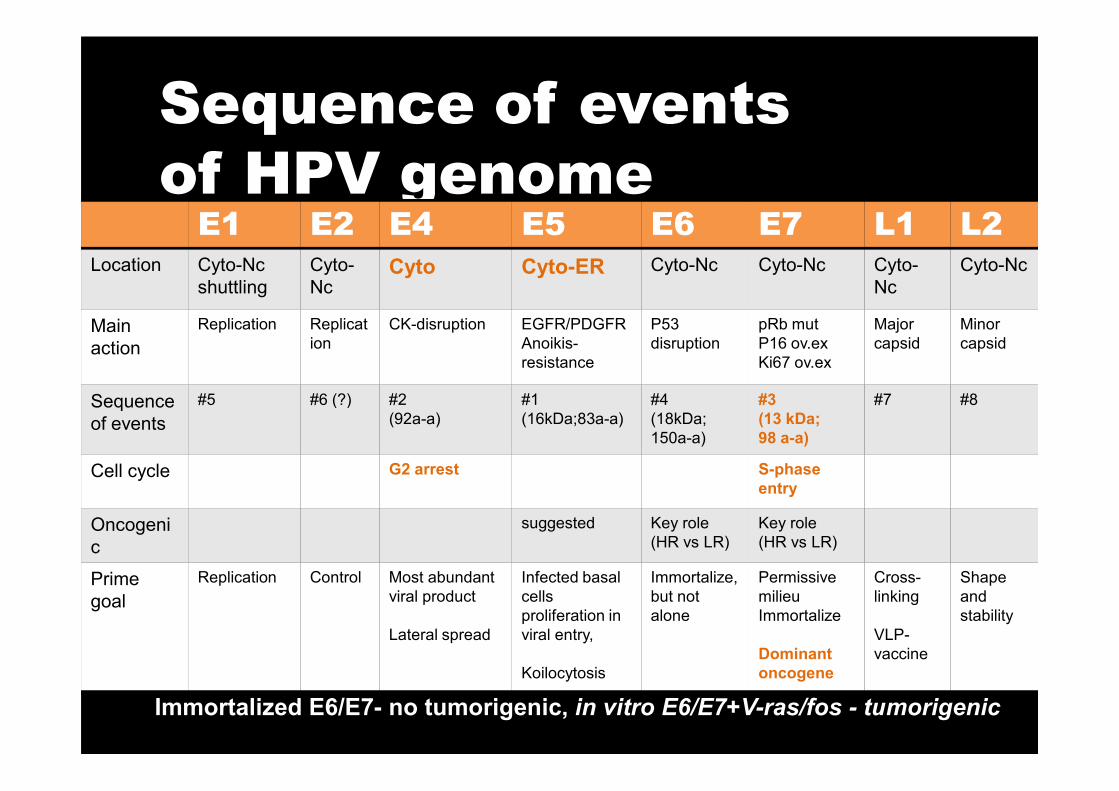
Sequence of events
of HPV genomeE1 E2 E4 E5 E6 E7 L1 L2
Location Cyto-Nc
shuttling
Cyto-
NcCyto Cyto-ER Cyto-Nc Cyto-Nc Cyto-
Nc
Cyto-Nc
Main
action
Replication Replicat
ion
CK-disruption EGFR/PDGFR
Anoikis-
resistance
P53
disruption
pRb mut
P16 ov.ex
Ki67 ov.ex
Major
capsid
Minor
capsid
Sequence #5 #6 (?) #2 #1 #4 #3 #7 #8Sequence
of events
#5 #6 (?) #2
(92a-a)
#1
(16kDa;83a-a)
#4
(18kDa;
150a-a)
#3
(13 kDa;
98 a-a)
#7 #8
Cell cycle G2 arrest S-phase
entry
Oncogeni
c
suggested Key role
(HR vs LR)
Key role
(HR vs LR)
Prime
goal
Replication Control Most abundant
viral product
Lateral spread
Infected basal
cells
proliferation in
viral entry,
Koilocytosis
Immortalize,
but not
alone
Permissive
milieu
Immortalize
Dominant
oncogene
Cross-
linking
VLP-
vaccine
Shape
and
stability
Immortalized E6/E7- no tumorigenic, in vitro E6/E7+V-ras/fos - tumorigenic
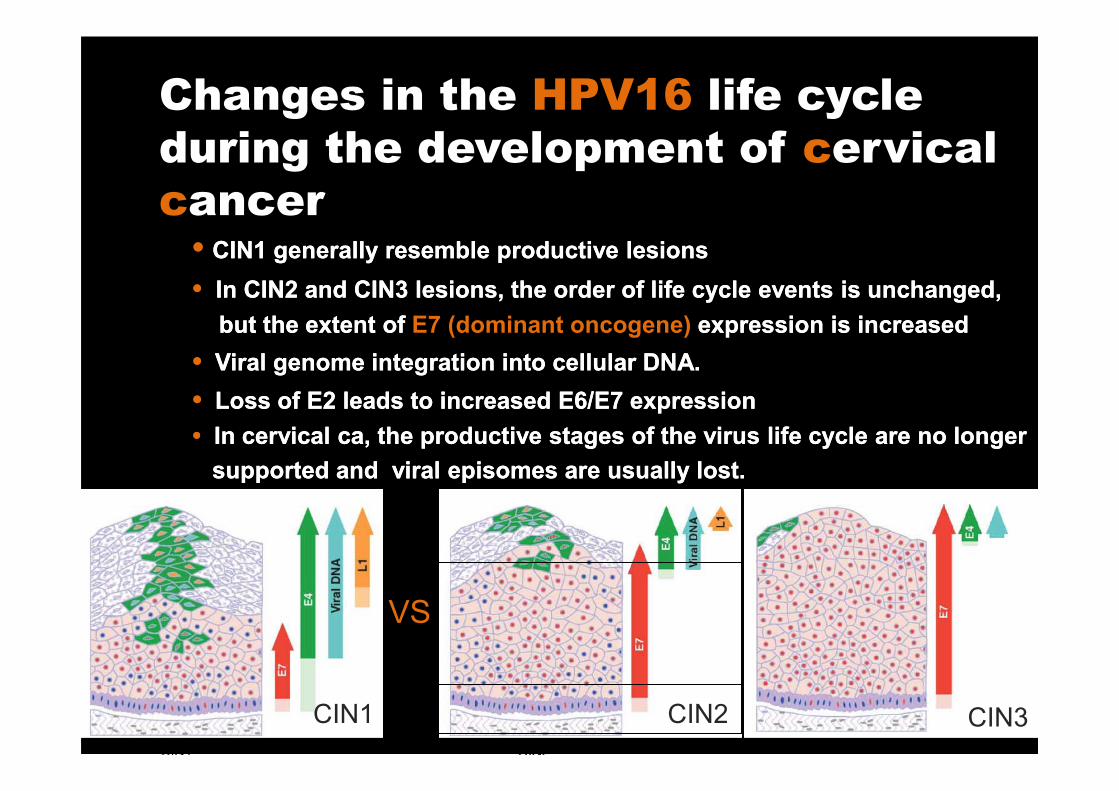
Changes in the HPV16 life cycle
during the development of cervical
cancer•• CIN1 generally resemble productive lesionsCIN1 generally resemble productive lesions
•• In CIN2 and CIN3 lesions, the order of life cycle events is unchanged, In CIN2 and CIN3 lesions, the order of life cycle events is unchanged,
but the extent of but the extent of E7 (dominant oncogene) expression is increasedexpression is increased
•• Viral genome integration into cellular DNA. Viral genome integration into cellular DNA.
•• Loss of E2 leads to increased E6/E7 expressionLoss of E2 leads to increased E6/E7 expression
CIN1 CIN2 CIN3
VS
•• Loss of E2 leads to increased E6/E7 expressionLoss of E2 leads to increased E6/E7 expression
• • In cervical ca, the productive stages of the virus life cycle are no longer In cervical ca, the productive stages of the virus life cycle are no longer
supported and viral supported and viral episomesepisomes are usually lost. are usually lost.
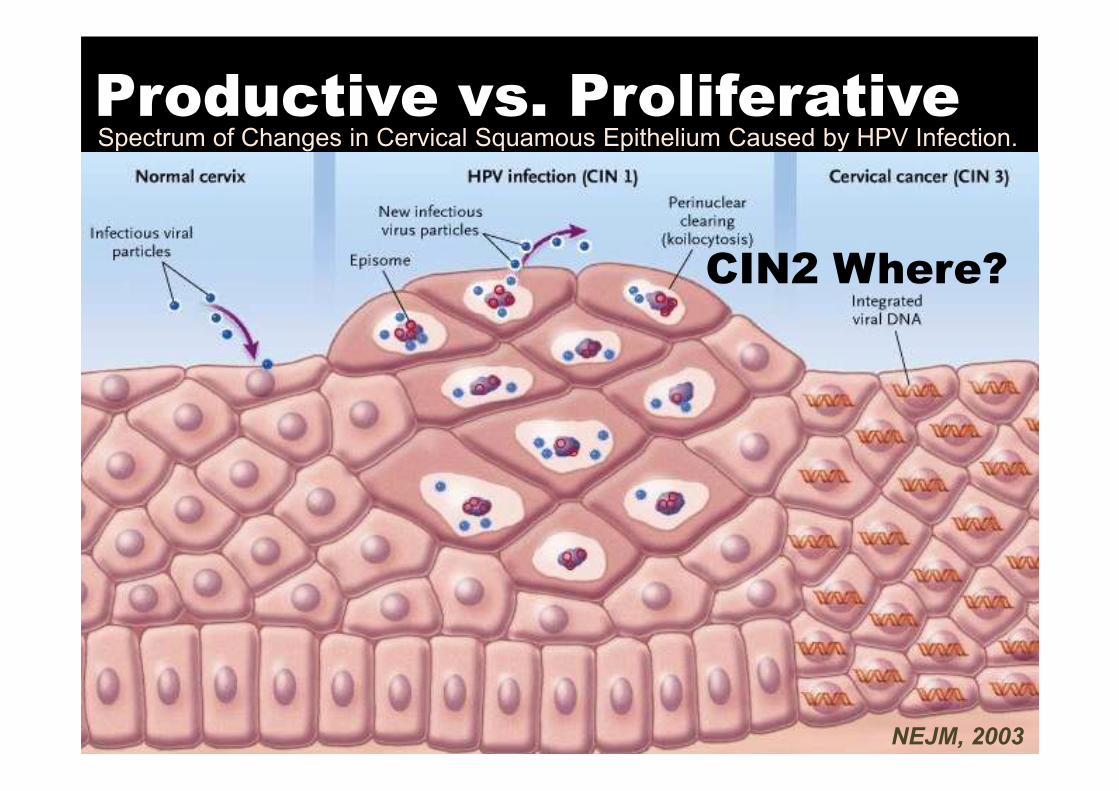
Productive vs. Proliferative
CIN2 Where?
Spectrum of Changes in Cervical Squamous Epithelium Caused by HPV Infection.
NEJM, 2003
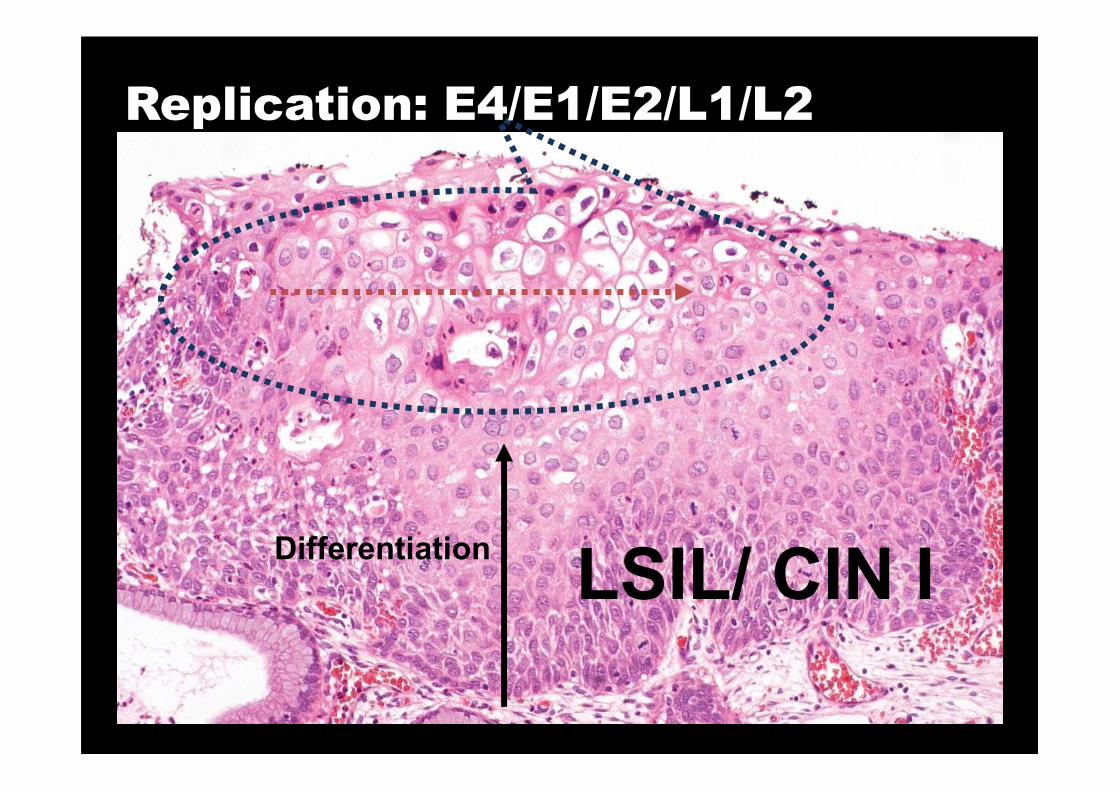
Replication: E4/E1/E2/L1/L2
Differentiation
LSIL/ CIN I
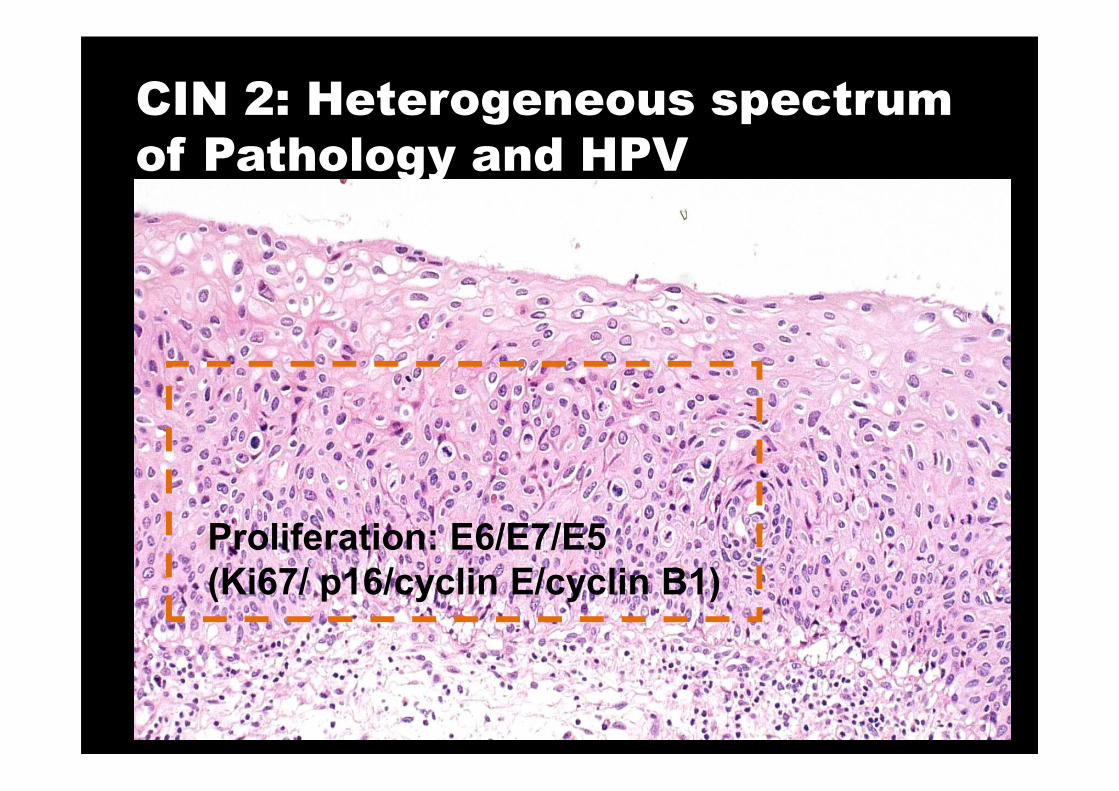
CIN 2: Heterogeneous spectrum
of Pathology and HPV
Proliferation: E6/E7/E5
(Ki67/ p16/cyclin E/cyclin B1)
Take Home Message
• E1^E4, E2^E5 splicing genome
– Multitasking crucial roles from entry to exit
– Phenotypically meaningful sign of – Phenotypically meaningful sign of
koilocytes and ruffled surface
• LSIL vs. HSIL completely two different
entity- CIN2 should be included in HSIL,
or overlapped with CIN 3
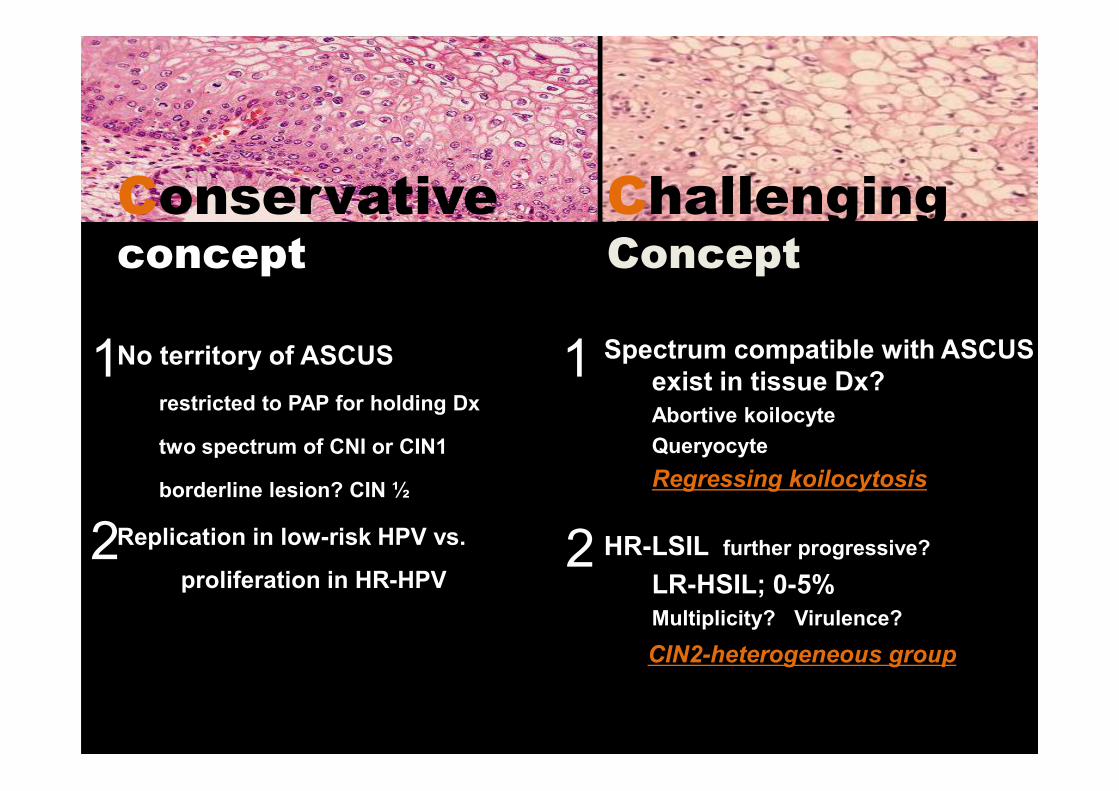
No territory of ASCUS
restricted to PAP for holding Dx
Spectrum compatible with ASCUS
exist in tissue Dx?
Conservativeconcept
Challenging Concept
1 1restricted to PAP for holding Dx
two spectrum of CNI or CIN1
borderline lesion? CIN ½
Replication in low-risk HPV vs.
proliferation in HR-HPV
exist in tissue Dx?
Abortive koilocyte
Queryocyte
Regressing koilocytosis
HR-LSIL further progressive?
LR-HSIL; 0-5%
Multiplicity? Virulence?
CIN2-heterogeneous group
2 2

Revisited ConceptASCUS cells caused by incomplete E4/E5 activity
Abortive koilocyte
Queryocyte
Regressing koilocyte : not enough cleared by immune sys
1
2 HR-LSIL
Need to monitor carefully, but no overconcern!
LR-HSIL
Occur rarely in single, but often combined, need to be further studied
CIN2
definitely heterogeneous in HPV life cycle to manifest combined
productive and proliferative phase
2
3
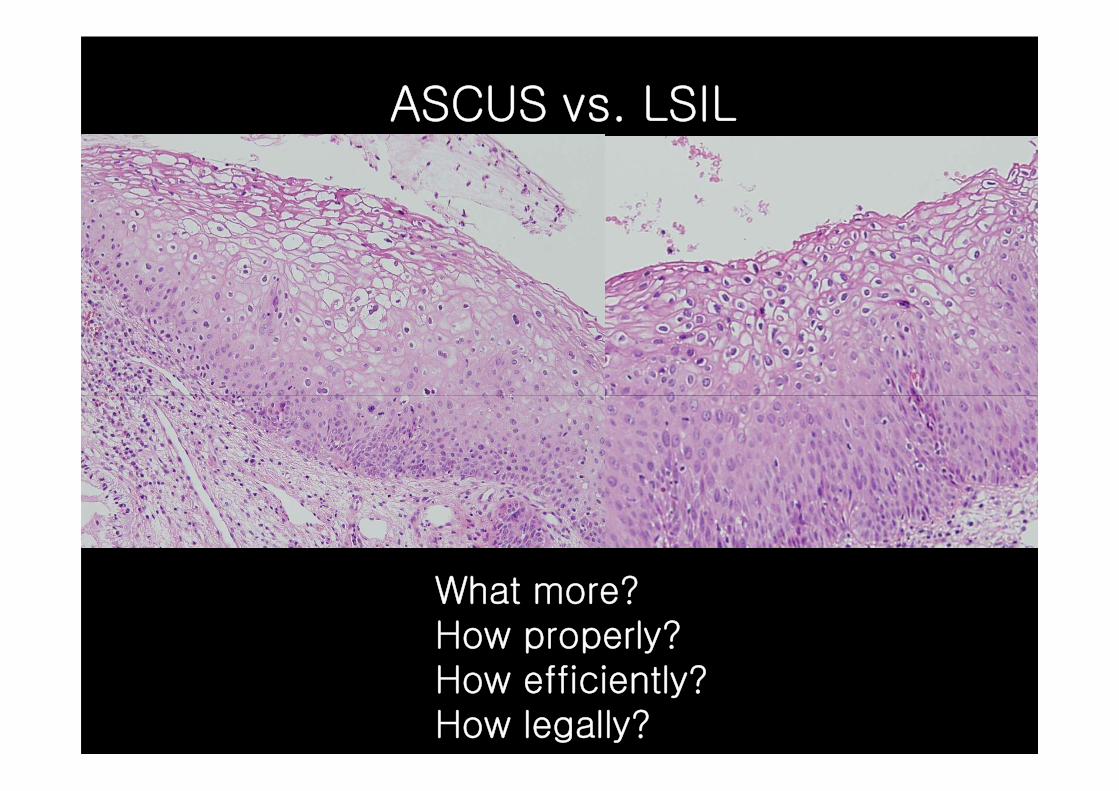
ASCUS vs. LSIL
What more? How properly? How efficiently?How legally?

Performance characteristicsDesignation Probes/primers
Reaction
product
Analytical
sensitivity, fg
detectable
types
Hybridi
zation
HC2 HPV DNA
assay
Mixture of
RNA probes
DNA/RNA
hybrids25–75 13
PCRMY09/11 Dot blot Degenerate primer 450 bp 0.1–100 39
PCR PGMY09/11 Mixture of 450 bp 0.1 27
PCR PGMY09/11
reverse LBA
Mixture of
consensus primers450 bp 0.1 27
PCR GP5+/GP6+ EIA
ELISA systemConsensus primers 150 bp 0.5–10 20
PCRGP5+/6+ reverse
LBAConsensus primers 150 bp 0.5–10 37
PCRSPF-PCR reverse
LiPA
Mixture of
consensus primers65 bp 0.1–10 43
Iftner T, et al. J Natl Cancer Inst Monogr. 2003;(31):80-8.
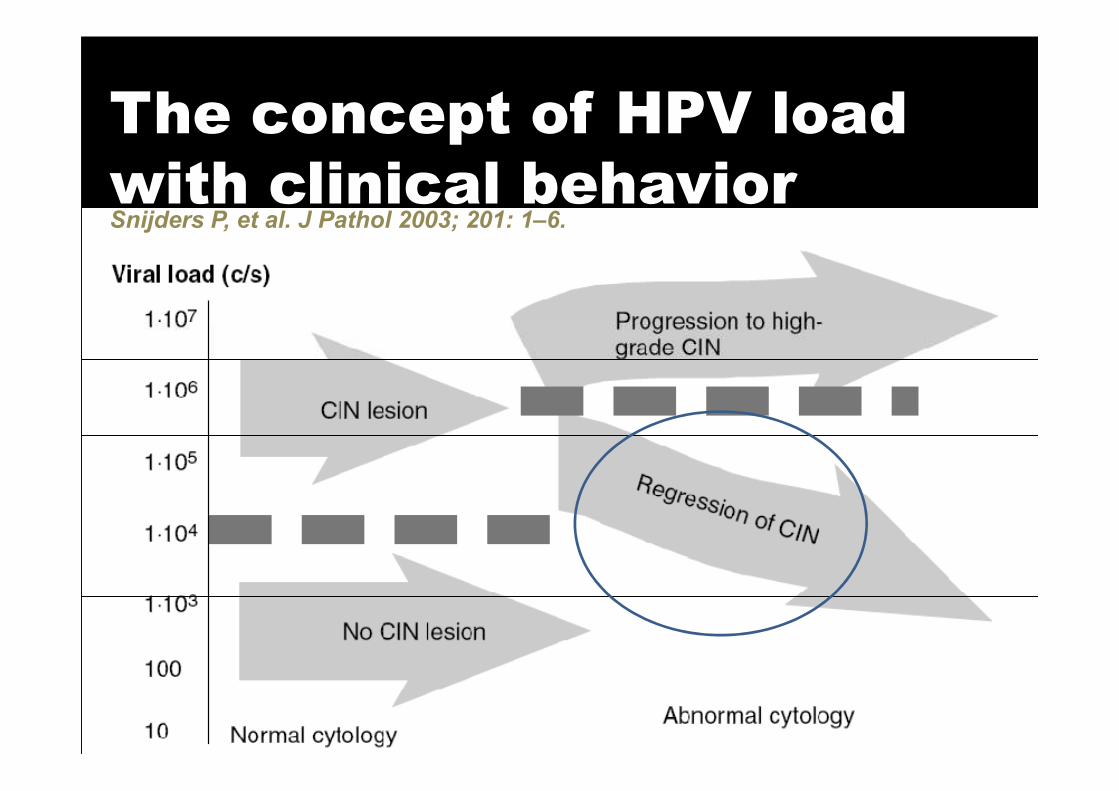
The concept of HPV load
with clinical behaviorSnijders P, et al. J Pathol 2003; 201: 1–6.
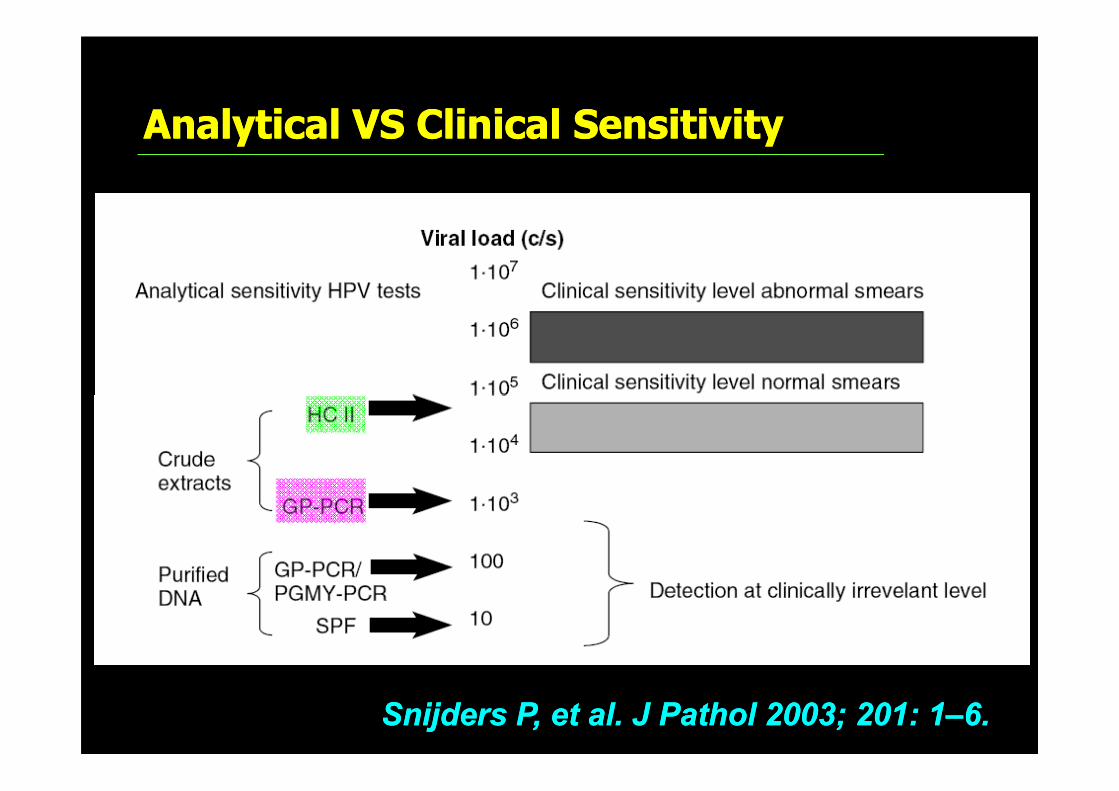
Analytical VS Clinical SensitivityAnalytical VS Clinical Sensitivity
SnijdersSnijders P, et al. J P, et al. J PatholPathol 2003; 201: 12003; 201: 1––6.6.
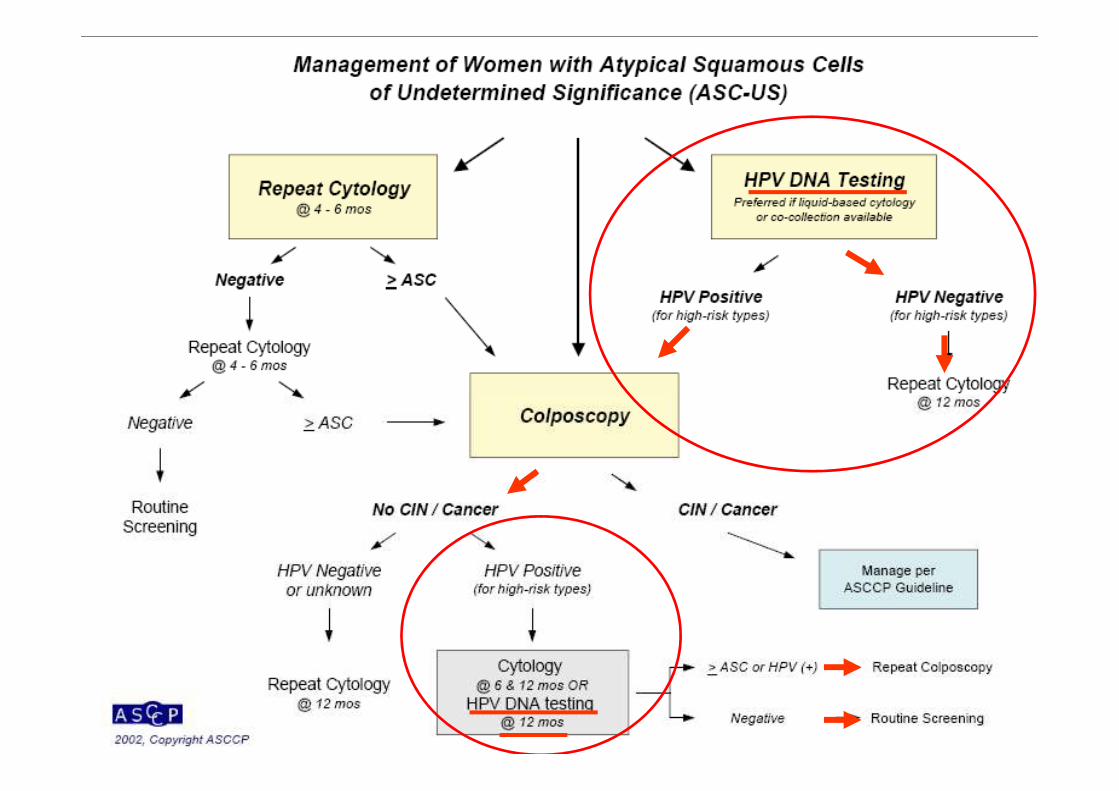
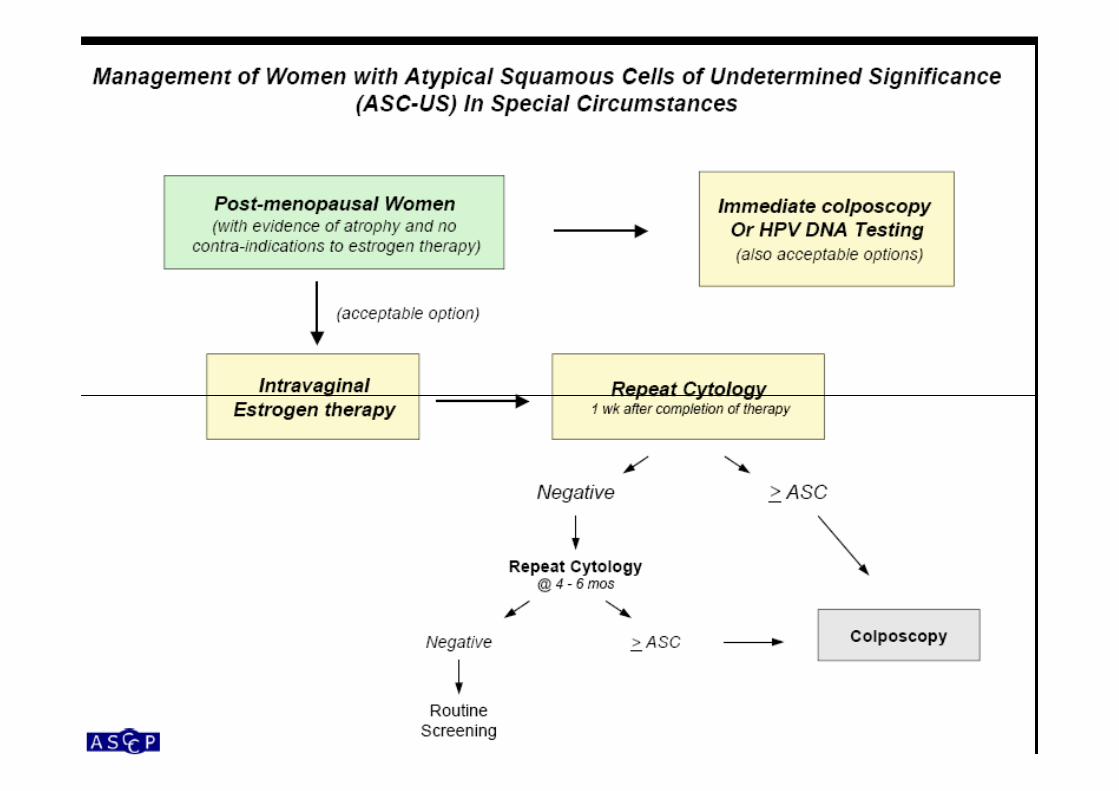

비정상비정상자궁경부자궁경부세포검사를세포검사를보인보인환자의환자의처치에처치에있어서있어서 HPV DNA testing HPV DNA testing
�� ASCASC--US/LSIL US/LSIL 환자의환자의처치처치및및추적추적검진검진
–– 고위험군고위험군 HPV DNA testing : HPV DNA testing : 연연 11회회시행시행 급여급여인정인정
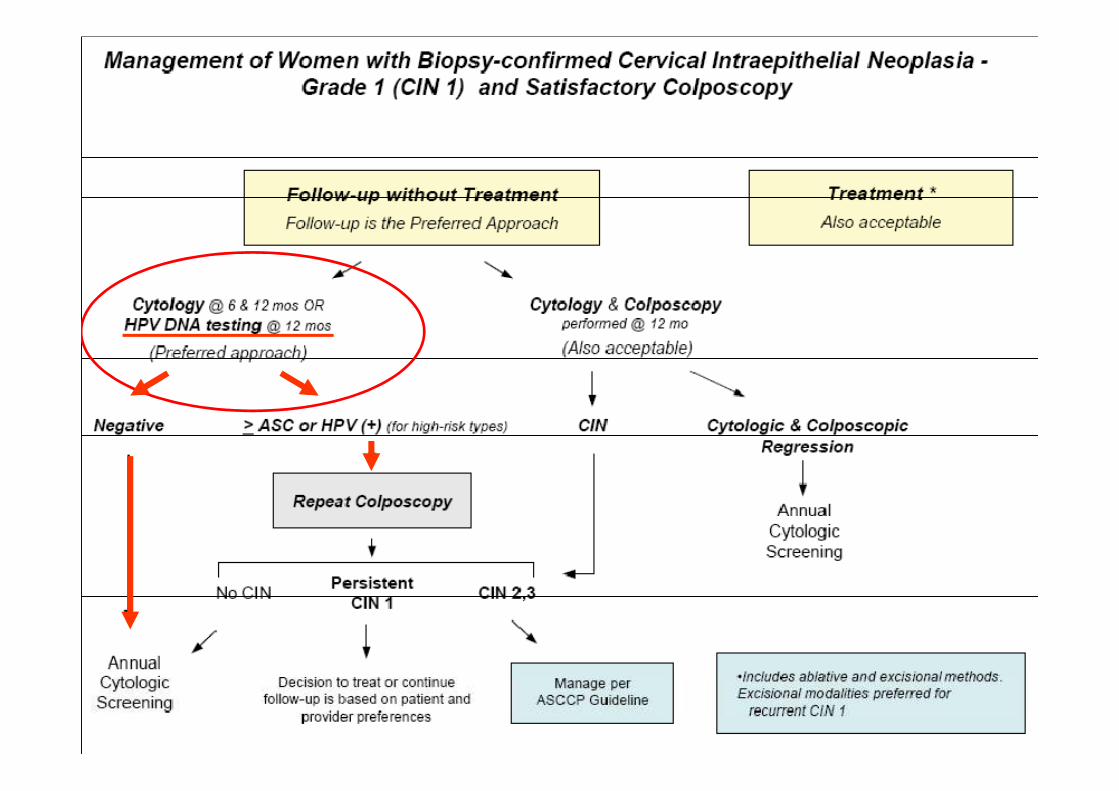
�� 조직검사상조직검사상 CIN 1CIN 1으로으로확진된확진된환자의환자의추적추적검진검진
–– 고위험군고위험군 HPV DNA testing : HPV DNA testing : 연연 11회회시행시행 급여급여인정인정
CIN II/III CIN II/III 환자의환자의치료치료전전,,후후검사로서검사로서HPV DNA testing HPV DNA testing
�� 고위험군고위험군 HPV DNA testing: HPV DNA testing:
–– 치료치료전전 11회회시행시행급여급여인정인정
–– 치료치료후후최소최소 66개월개월후후 11회회시행시행급여급여인정인정–– 치료치료후후최소최소 66개월개월후후 11회회시행시행급여급여인정인정
�� 치료치료후후시행한시행한고위험군고위험군 HPV DNA testingHPV DNA testing이이양성양성
–– 66--1212개월개월간격으로간격으로고위험군고위험군 HPV DNA testingHPV DNA testing을을
반복반복시행시행 급여급여인정인정
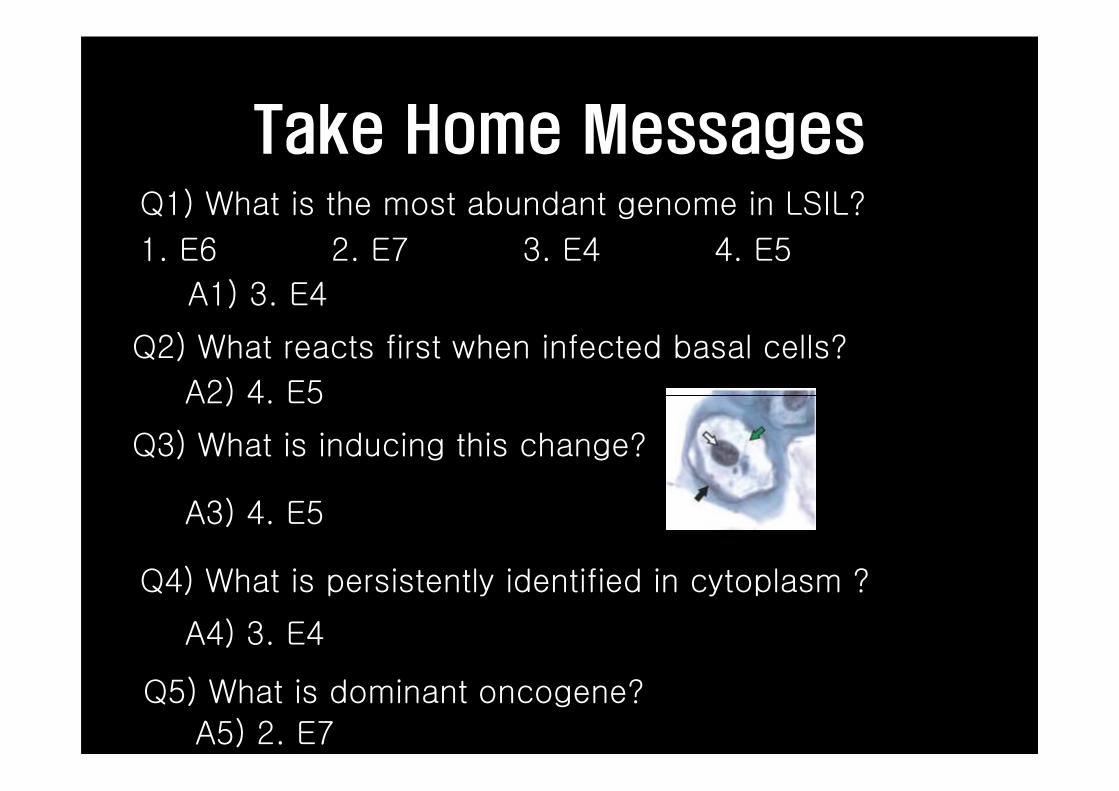
Take Home MessagesQ1) What is the most abundant genome in LSIL?
1. E6 2. E7 3. E4 4. E5
A1) 3. E4
Q2) What reacts first when infected basal cells?
A2) 4. E5A2) 4. E5
Q3) What is inducing this change?
A3) 4. E5
Q4) What is persistently identified in cytoplasm ?
A4) 3. E4
Q5) What is dominant oncogene?
A5) 2. E7
Despite the common notion that
cervical histology Is the golden standard,
cytology is an important indicator of
subsequent risk of CIN3+ within the
group of normal histology.
Cancer Res 2010; 70:8578-86
Thank youNam Hoon Cho, M.D.
Yonsei Univ Coll Med, Dept of Pathology
Thank you







