Download - Nov7 - Simulated 1& 2

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 1/51

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 2/51
GOODAFTERNOON!!!!
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 3/51
Clean-Catch (Midstream) Specimen
perennial area is washed
Mild antiseptic/liquid soap
midstream ur ine is collected 30 ml
avoid collecting initial & last f e w dr ops
send specimen laboratory or within 2 hour s
Collecting Urine Specimens

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 4/51
Ster ile Specimen f r om Indwelling Catheter
a. Fr om a closed system Method
² clamp drainage tubing about 4µbelow junction of drainage tubing and
catheter for 10-30 minutes ² Clean specimen collection port with
alcohol or antiseptic solution
² Collect 3-10 ml of urine with asterile syringe
² For self-sealing catheter, insert needle
slowly at 450 angle taking care not topuncture the other side of the tubing
Collecting Urine SpecimensCollecting Urine Specimens
b. Open-System Method
-Place line saver under tubing at
junction of catheter and drainagetubing
-Disinfect the junction before andafter the collection
-Hold the disconnected tube(catheter and drainage tubing)
1.5-2 inches from each other
-Do not allow the catheter tip totouch container

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 5/51
24-Hour Ur ine Collection.
Ur ine passed in a 24-hour per iod is collected
Measures the amount of certain chemicals the kidneys clean f r om the body.
To see if too little or too much ur ine is pr oduced. Decide on the day and time-usually started in the
morning
Discar d the fir st voided ur ine
Collect all the subsequent ur ine passed
At the 24th hour, collect the last sample Ur ine should be k ept cool, ref r igerated
Specimen sent to the laboratory within 2 hour s af ter collection
Collecting Urine Specimens

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 6/51
IntravenousIntravenous pyelogrampyelogram(IVP)(IVP)
Visualization of the Urinary system
K idney
Urethers
Bladders
Aka
Intravenous pyelography (IVP).
Urography.Pyelography.
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 7/51
IntravenousIntravenous pyelogrampyelogram(IVP)(IVP)
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 8/51
IntravenousIntravenous pyelogrampyelogram(IVP)(IVP)
ydetect problems:
kidney stones enlarged prostate
tumors in the kUB
surgery on the urinary tract

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 9/51
IntravenousIntravenous pyelogrampyelogram(IVP)(IVP)
y Preparation:
Enema( aperients) 24 hours
NPO 6
² 8 hoursRemove : jewelry, dentures, eye glasses and any
metal objects or clothing
y Patient wears cotton examination gown.
y Bladder emptied immediately before examination.
y Site: median cubital vein : 20 gauge

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 10/51
point of comparison«point of comparison«
- inflammation of RenalPelvis/ Renal Parenchyma
- s/sx:
cystitis s/sx
pain: flank pain ² T12 & L3
Costovertebral TendernessFever: High
CYSTITIS PYELONEPRHRITIS
- inflammation of theUrinary Bladder
- s/sx:
Dysuria
Freqyuency
Urgency
NoctoriaPyuria : cloudy.foul odor
Pain : suprapubic/hypogastric
Fever: Low Grade

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 11/51
y Furniture:
sturdy & stable
straight back seat firm should be NO lower
shallow than the knee height
sofas & chairs - 17 inches off the ground
heavy rocking chair with arm rest
clear plastic chair protector for upholstered
chairs
Parkinson·s Disease

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 12/51
LowLow purinepurine diet««diet««
- indicated for gout, ur ic acid kidney stones and ur ic acid retention
- pur pose is to decrease the amount of pur ine
FOODS:
AVOID organ meats, fish, lobster s dr iedpeas and beans, nuts, oatmeal, whole wheat
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 13/51
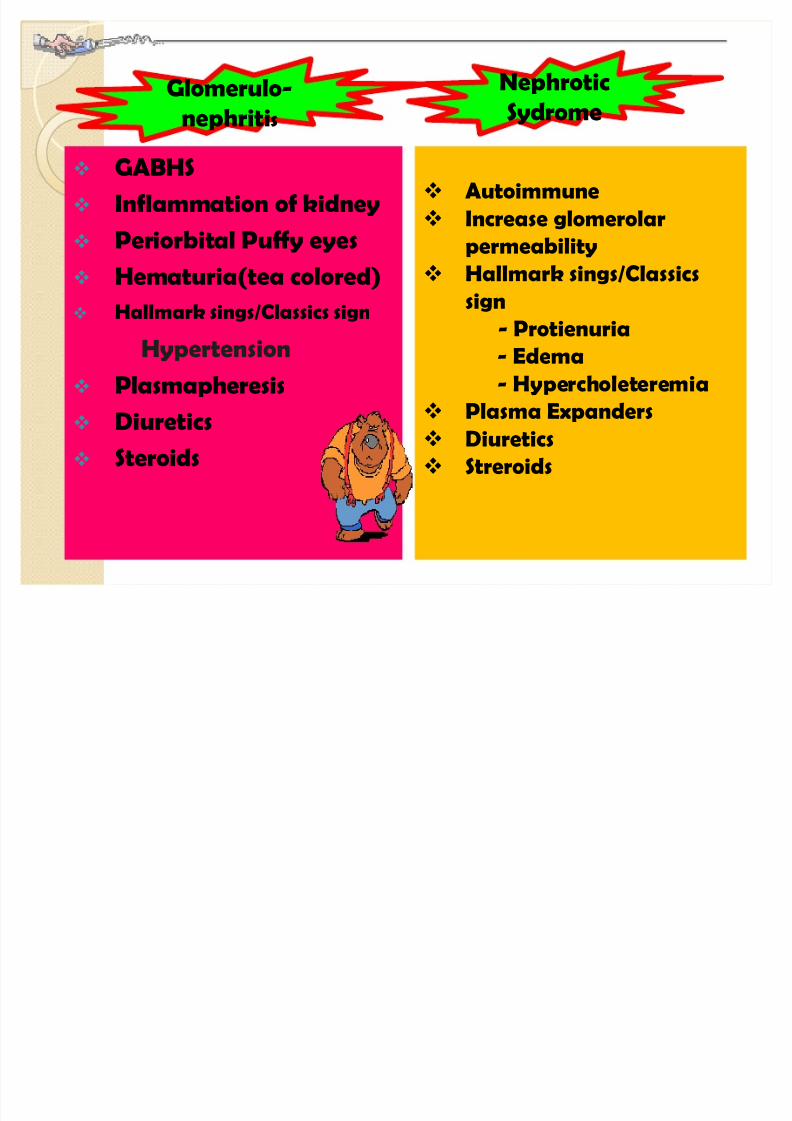
GABHS
Inflammation of kidney
Periorbital Puffy eyes
Hematuria(tea colored) Hallmark sings/Classics sign
Hypertension
Plasmapheresis
Diuretics
Steroids
Autoimmune
Increase glomerolar
permeability
Hallmark sings/Classicssign
- Protienuria
- Edema
- Hypercholeteremia
Plasma Expanders Diuretics
Streroids
Glomerulo-
nephritis
Nephrotic
Sydrome

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 14/51

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 15/51
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 16/51
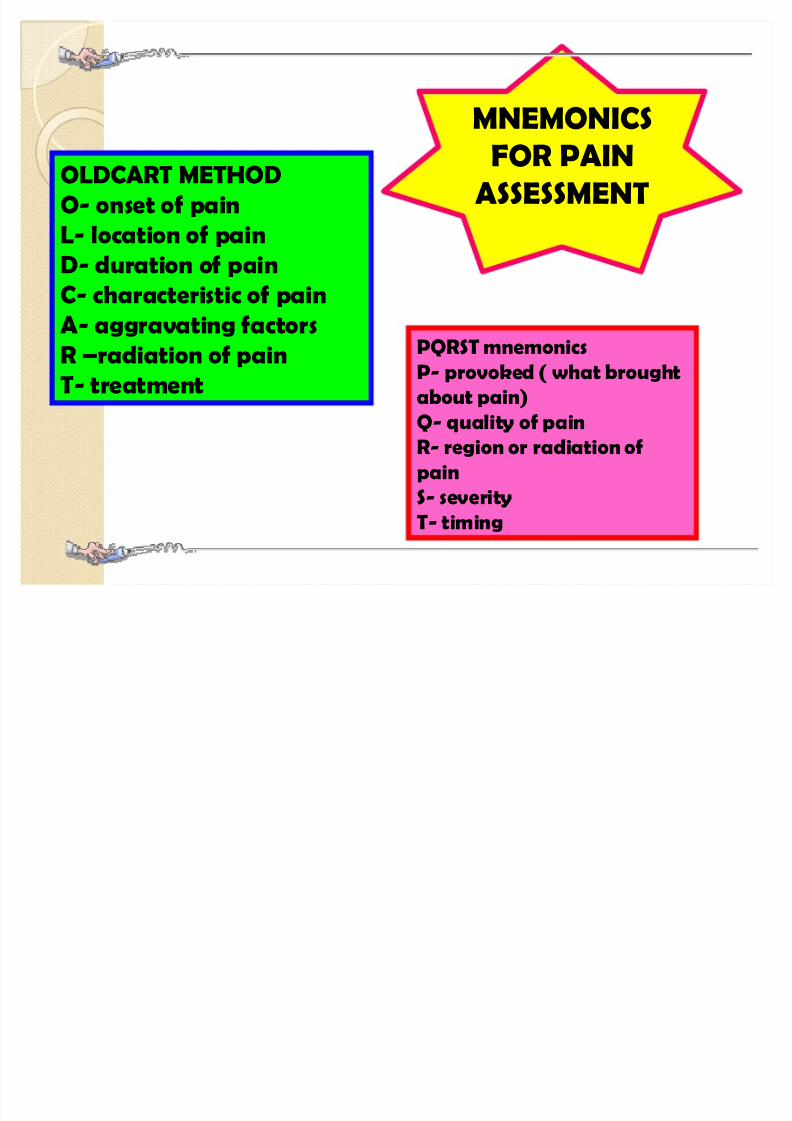
OLDCART METHOD
O- onset of pain
L- location of pain
D- duration of pain
C- characteristic of pain
A- aggravating factors
R ²radiation of pain
T- treatment
PQRST mnemonics
P- provoked ( what brought
about pain)
Q- quality of painR- region or radiation of
pain
S- severity
T- timing
MNEMONICS
FOR PAIN
ASSESSMENT

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 17/51
Pulmonary Wedge PressurePulmonary Wedge Pressureak a:ak a:Pulmonary capillary wedge pressurePulmonary capillary wedge pressure (PCWP)(PCWP)
Pulmonary artery occlusion pressurePulmonary artery occlusion pressure ( PAOP)( PAOP)
y Catheter Swan-Ganz
y Indication - Diagnose the severity of left ventricular failure
- Check if Left Ventricle is over stretched, under
stretched or appropriately stretched
- Quantify the degree of mitral valve stenosis
- Physician can calculate the dose of diuretic drugs
- Evaluating pulmonary hypertension
- diagnosis of acute respiratory distress syndrome
Normal PAWP : 8-12 mmHg
Above 20 mmHg : Acute Pulmonary edema

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 18/51
Pulmonary Wedge PressurePulmonary Wedge Pressureak a:ak a:Pulmonary capillary wedge pressurePulmonary capillary wedge pressure (PCWP)(PCWP)
Pulmonary artery occlusion pressurePulmonary artery occlusion pressure ( PAOP)( PAOP)
y Catheter Swan-Ganz
y Indication - Diagnose the severity of left ventricular failure
- Check if Left Ventricle is over stretched, under
stretched or appropriately stretched
- Quantify the degree of mitral valve stenosis
- Physician can calculate the dose of diuretic drugs
- Evaluating pulmonary hypertension
- diagnosis of acute respiratory distress syndrome
Normal PAWP : 8-12 mmHg
Above 20 mmHg : Acute Pulmonary edema

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 19/51
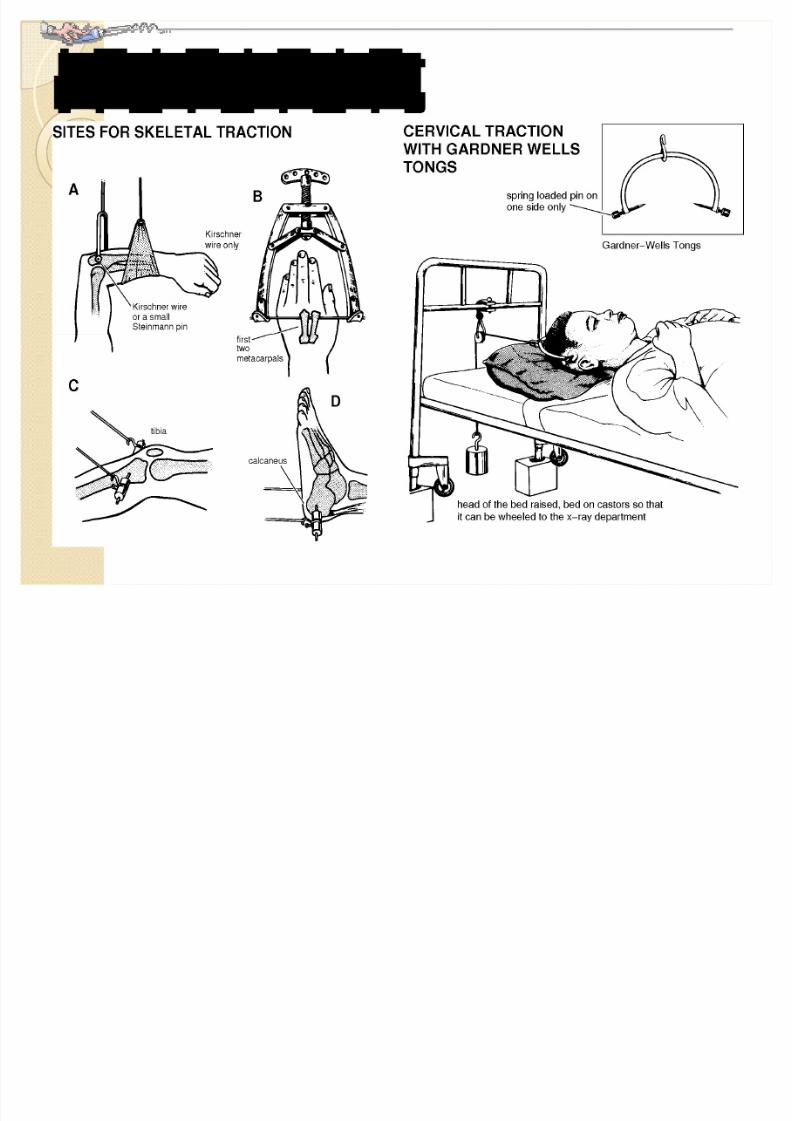
sk eletal tractionsk eletal traction

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 20/51
Thomas splint

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 21/51
y Dribbling, Difficulty starting urine stream
y Retention
y Inability to void after alcohol & cold
exposurey Frequency
y Urgency
y Small less forceful urine
y Nocturia
y Elevated WBC, and BUN
y Prostate specific antigen (PSA)

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 22/51

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 23/51
y ASYMPTOMATIC for 5 or more years after
y Early symptoms resemble a FLULIK E illness
y MALIGNANCIES: Kaposi·s sarcoma, skin cancer
y laboratory tests
- Enzyme-linked immunosorbent assay (ELISA)- Western Blot
- Rapid HIV tests (30 minutestest)

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 24/51
Pregnancy Induced HypertensionPregnancy Induced Hypertension
TypesTypes BPBP ProteinuriaProteinuria EdemaEdema Other S/Other S/SxSx
MildMild140/90140/90
(increase(increaseof 30/15)of 30/15)
1+ to 2+1+ to 2+Slight inSlight in
upperupperextermitiesextermities
Wt gainWt gain
22ndnd tri 2 lbs/weektri 2 lbs/week33rdrd tri 1 lb/weektri 1 lb/week
SevereSevere160/110160/110
3 to 4 +3 to 4 +PulmonaryPulmonaryPeripheralPeripheral
EdemaEdema
EpigastricEpigastric PainPain
Hepatic DysfunctionHepatic Dysfunction
OliguriaOliguria<500ml/24<500ml/24
Eclam psiaEclam psia
upup 4+4+--samesame-- CONVULSIONCONVULSION
COMACOMA

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 25/51
Anorexia Nervosa Bulimia Nervosa
15% loss of BW
BMI<17.5 kg/mStrict dieters
Indulges in strenous exercises
Pre-occupation with foods
Amenorrhea for 3 cycles
binge-purge
Russel·s sign
Teeth missing lower incisors
Abusive of laxative, enema,
diuretics
Rectal bleeding/constipation
Do·s
Small frequent feedings
Monitor I&O, weight gain
Stay with client during meal
or atleast 1 hr after
Accompany to the bathroom
Don·ts
Express feeling of
shock/disgust
Don·t compare with others
Don·t allow long time meals
(set 30 mins. meal time)

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 26/51
SpinaSpina BifidaBifida

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 27/51
IV Therapy
Phlebitis
Inflammatory response to damage to
the intimal layer of the vein caused by
mechanical or physiochemical forces.
S/sx of infection
A palpable venous cord indicates
advanced stage of phlebitis. When identified,remove the PIV .
Phlebitis Scale
0 = No Symptoms
1 = Erythema
2 = Pain
3 = Streak Formation, venous
cord
4 = Purulent Drainage,
palpable venous cord
Infiltration
Inadvertant administration of
medication or solution into tissue
surrounding the vein. It¶s called
Extravasion if vesicant medication isadministered into the surrounding
tissue.
Infiltration: Most commonly identified
complication of PIV therapy with a
reported incidence of 23% to 78%.
.
Infiltration Scale
0 = No Symptoms
1 = Some Edema, Cool
2 = 1-6 inch Edema, Cool,Pain
3 = > 6 inch edema, pain,
numb
4 = Pitting Edema,
Circulatory impairment
The difference
between Phlebitis
and Infiltration

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 28/51

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 29/51
«just remember this«just remember this
r ADiAtIoN SaFeTy- Label potentially radioactive material
- Limit time spent near the source 30 mins/day
- Distance from the source 6 feet away
- Shield Device Lead Apron
- Room Private Room
- Dislodge Implant
1. Long handle forceps2. place in lead lined container
3. report
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 30/51
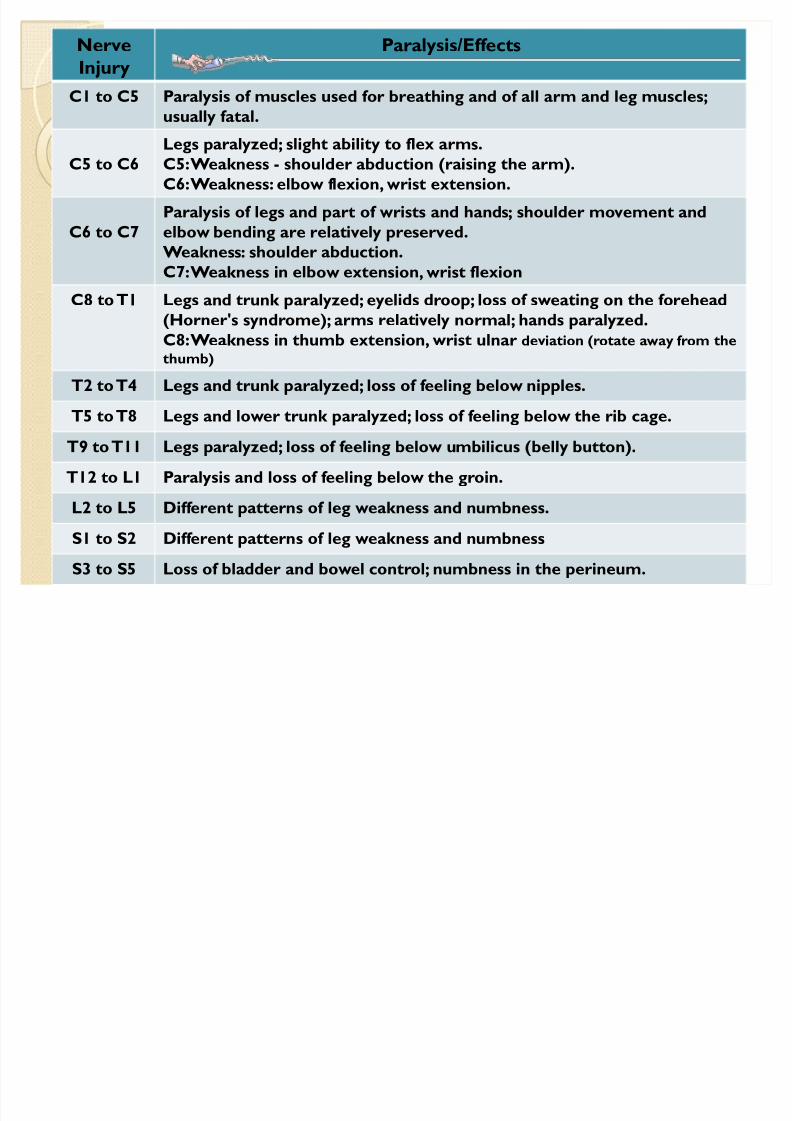
Nerve
Injury
Paralysis/Eff ects
C1 to C5 Paralysis of muscles used for breathing and of all arm and leg muscles;
usually f atal.
C5 to C6Legs paralyzed; slight ability to f lex arms.C5: Weak ness - shoulder abduction (raising the arm).
C6: Weak ness: elbow f lexion, wr ist extension.
C6 to C7
Paralysis of legs and part of wr ists and hands; shoulder movement and
elbow bending are relatively preserved.
Weak ness: shoulder abduction.
C7: Weak ness in elbow extension, wr ist f lexionC8 to T1 Legs and tr unk paralyzed; eyelids dr oop; loss of sweating on the forehead
(Horner's syndr ome); arms relatively normal; hands paralyzed.
C8: Weak ness in thumb extension, wr ist ulnar deviation (r otate a way f r om the
thumb)
T2 to T4 Legs and tr unk paralyzed; loss of f eeling below nipples.
T5 to T8 Legs and lower tr unk paralyzed; loss of f eeling below the r ib cage.
T9 to T11 Legs paralyzed; loss of f eeling below umbilicus (belly button).
T12 to L1 Paralysis and loss of f eeling below the gr oin.
L2 to L5 Diff erent patterns of leg weak ness and numbness.
S1 to S2 Diff erent patterns of leg weak ness and numbness
S3 to S5 Loss of bladder and bowel contr ol; numbness in the per ineum.

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 31/51
Br onchial Hygiene Therapy (BHT)Br onchial Hygiene Therapy (BHT)

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 32/51

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 33/51
Chest physiotherapy
y Percussion is carried out by cupping the hands and
lightly str iking the chest wall; 3 to 5 minutes;
percussion over chest drainage tubes, the sternum,
spine, liver, kidneys, spleen, or breasts is avoided
y Vibration is the technique of applying manual
compression and tremor to the chest wall during
the exhalation phase of respiration; helps toincrease the velocity of the air expired from the
small airways, thus freeing the mucus.
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 34/51
«tractions & pins«tractions & pins

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 35/51
BMI BMI vsvs Weight to Height TableWeight to Height Table

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 36/51
BMIBMI
y Imper ial BMI Formula
The imperial bmi formula accepts weight measurements in pounds& height measurements in either inches or feet.1 foot = 12 inchesinches² = inches * inches
y Metr ic Imper ial BMI Formula
The metric bmi formula accepts weight measurements inkilograms & height measurements in either cm's or meters.
1 meter = 100cmsmeters² = meters * meters
Imperial BMI ( lbs/inches ) = (weight in pounds * 703 )height in inches
Metric BMI ( kg/m ) = weight in kilograms
height in meters
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 37/51
EnteralEnteral Nutr itionNutr ition
y pr ovides liquefied f eeding into the
gastr ointestinal tract via a tube
y for patient who have a functioning GI tract but cannot
ingest food by MOUTH
y Feeding tubes:
- short-term: nasogastric tube
- long-term: esophagostomy, gastrostomy,
enterostomy tube
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 38/51
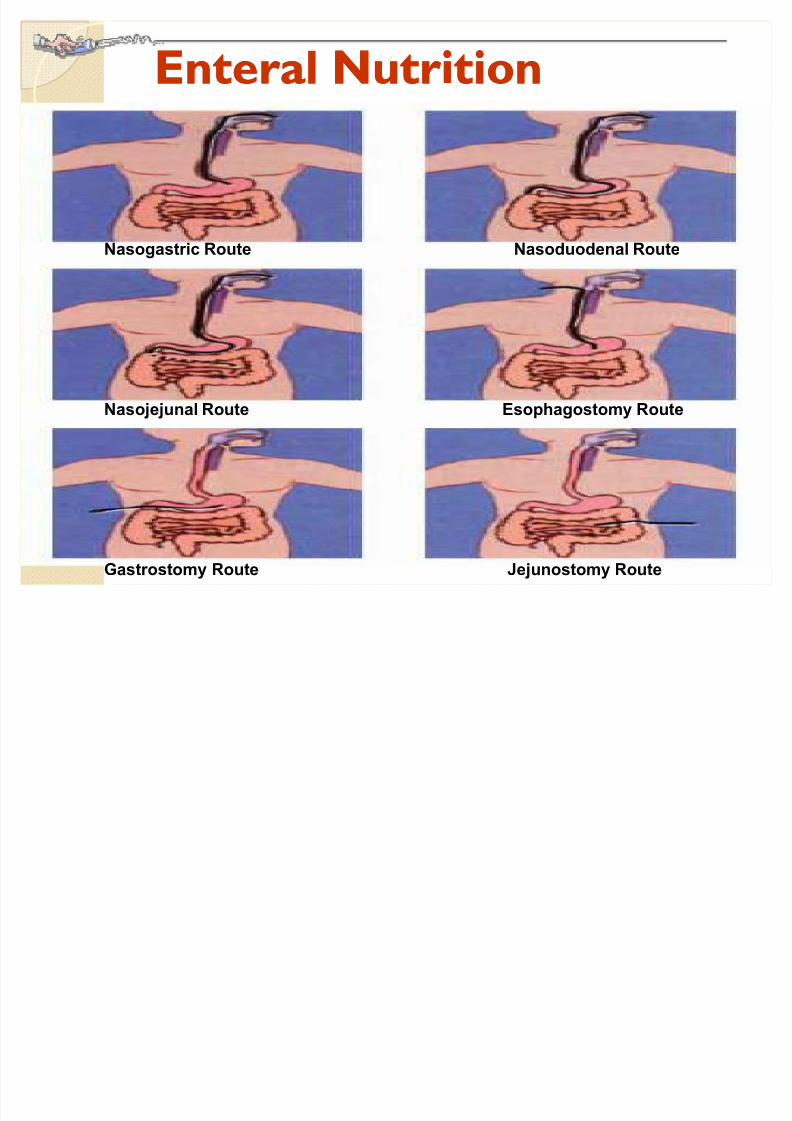
Enteral Nutr itionEnteral Nutr ition
Nasogastric Route Nasoduodenal Route
Nasojejunal Route Esophagostomy Route
Gastrostomy Route Jejunostomy Route

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 39/51
Nasogastr ic Tubey Insertion:
- NEX
- High Fowler·s position- Sips of water and advance tube as client swallows- Do not force the tube!
y Confirm placement of NGTy Monitor and recor d residual volume q4h by aspirating stomach content
with a syr inge.A residual volume of >100-150 ml indicates delayedgastr ic emptying. Notif y MD.
y Dur ing and af ter f eeding k eep HOB 30 degrees to prevent aspiration;For continuous f eedings, k eep the patient in a semi-Fowler·s position at all times
y Flush/Irr igate tube f eeding with 30-60ml of water q4h dur ing continuousf eeding, before and af ter each intermittent f eeding, before and af ter administer ing meds, af ter each time you check residual volume
y Feeding set changed q24h. y Bag r insed q4h.y Medications:
Liquid medications should be diluted with water
Mixing medications with the f eeding should be avoided
Avoid diluting capsules in water
She should consult with the pharmacist to coor dinate timing of meds

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 40/51
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 41/51

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 42/51
Digital Rectal ExamDigital Rectal Exam

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 43/51
Hodgkin·s DiseaseHodgkin·s Disease

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 44/51
Glasgow Coma ScaleGlasgow Coma Scale

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 45/51

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 46/51

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 47/51
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 48/51
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 49/51
Points for quick thinking«Points for quick thinking«Natremias
DhypErnatremiahydration
hypOnatremiaverload
I was taught that k alemias do the same as the prefix except for heartrate and ur ine output.
EX: HYPERkalemia: bradycardia, oliguria, restlessness,diarrhea,hyperglycemia,hyperreflexia, increased BP, peaked T waves
HYPOkalemia: tachycardia, polyuria, constipation, hypoglycemia
Calcemias do the opposite of the prefix
EX: HYPOcalcemia causes neuromuscular irritability
8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 50/51
««any question?««any question?

8/8/2019 Nov7 - Simulated 1& 2
http://slidepdf.com/reader/full/nov7-simulated-1-2 51/51






