

STREPTOCOCCUS
&
ENTEROCOCCUS

REVIEW
Bacterial Cell Morphology • Gram Stain • Cytoplasmic (plasma) membrane • Cell wall structure • Bacterial cell shapes


Common Cell Membrane

Gram-Positive Cell Wall

Gram-Negative
Gram-Positive
Peptidoglycan
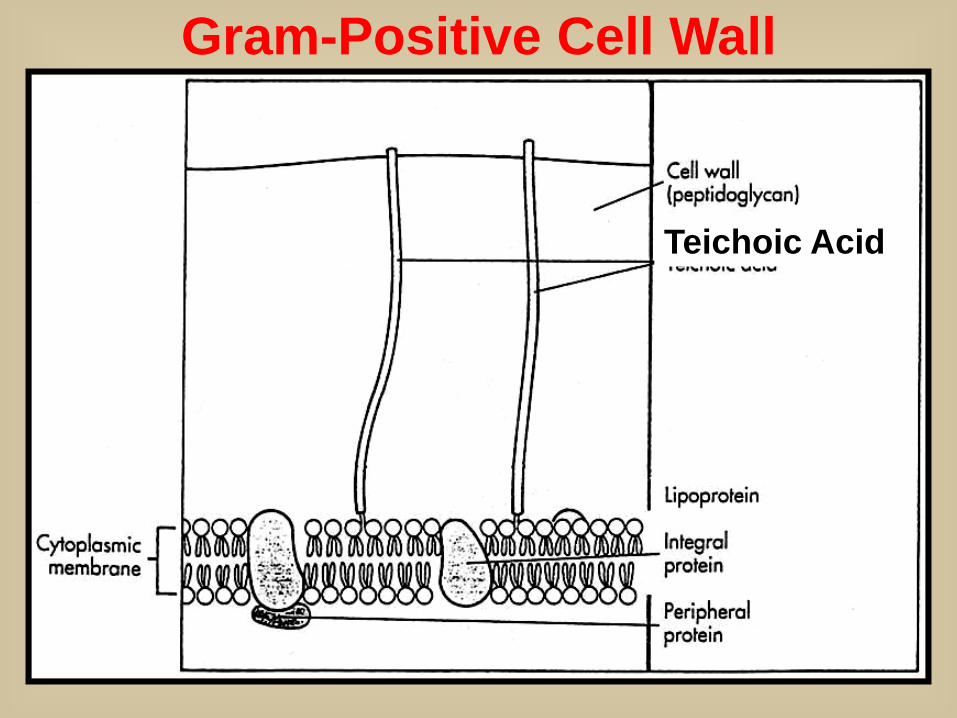
Teichoic Acid
Gram-Positive Cell Wall
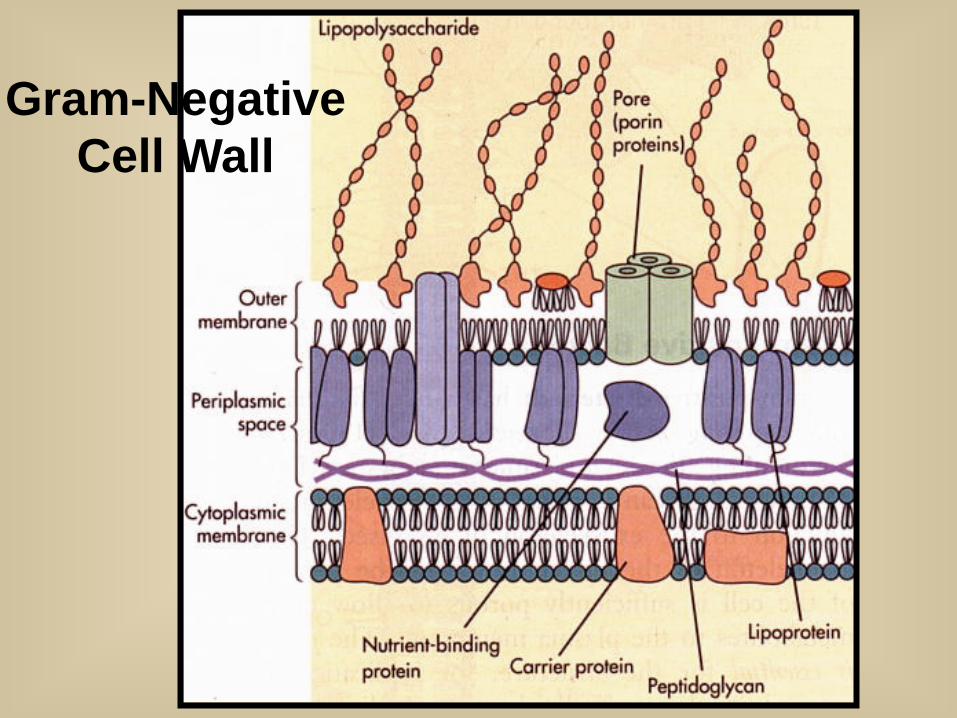
Gram-Negative Cell Wall

Gram-Negative Cell Wall




Genus Streptococcus
Commensals or Parasites of man & animals or
Saprophytes of decaying matter
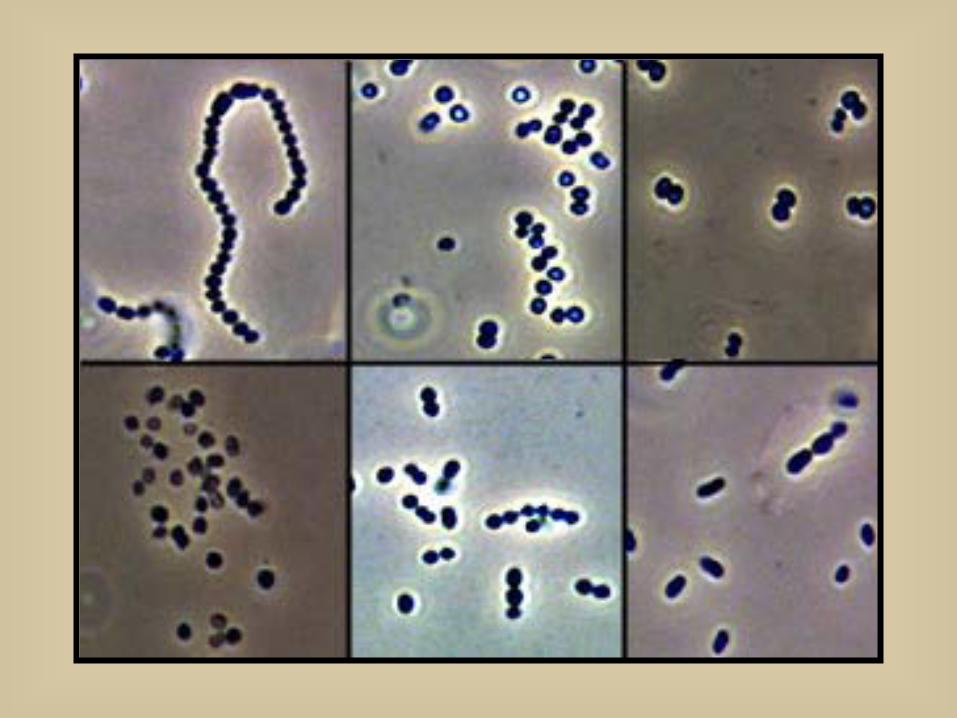
Morphology
Gram-Positive Cocci in Pairs or Chains

Gram-Positive Streptococcus

Genus Streptococcus
Physiology & Metabolism Facultative Anaerobes Fastidious Growth Requirements Fermentative Metabolism of Carbohydrates:
Lactic acid, ethanol, acetate endproducts produced; No gas
Catalase Negative (2H2O2 ---> O2 + 2H2O) Separation of streptococci from staphylococci Oxidase Negative (oxidoreductase oxidizes substrate w/ O2)
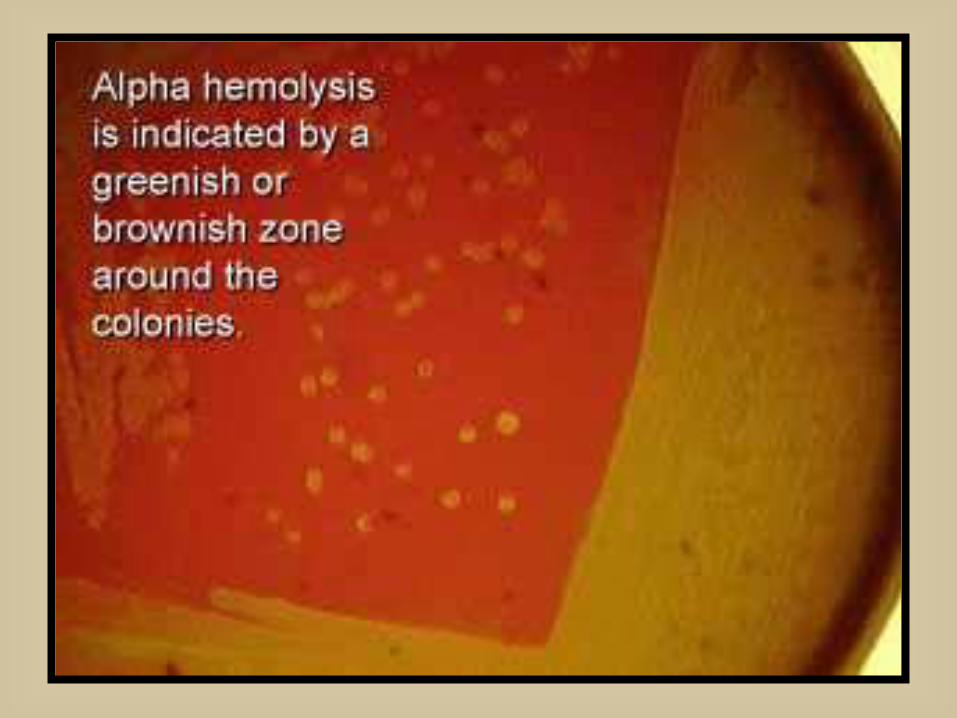
Beta, Alpha, or Gamma Hemolysis on blood agar



Genus Streptococcus
Rebecca Lancefield Developed useful serogrouping system
Classification of beta-hemolytic streptococci by group-specific cell wall carbohydrate (CHO) antigen
As of 1992, Serogroups A to H and K to V
Groups A, B, C, D, and G are most comonly associated with human disease
Viridans streptococci and Streptococcus pneumoniae have no group-specific antigen

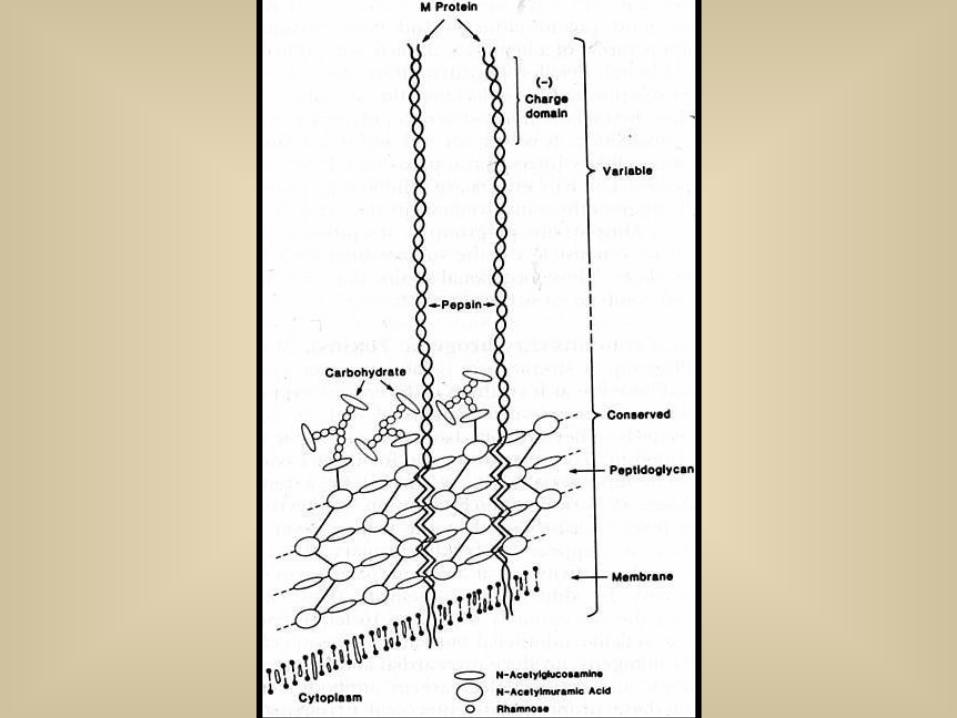
Antigenic Structure Streptococcus pyogenes (Group A)
Lancefield Group-specific antigen (C polysaccharide) Complex polysaccharide in cell wall
Proteins: Two major classes, M & T antigens Two minor classes, R & F
M-Protein: Type-specific antigen Fimbriae-like, hairy extensions
Resistant to heat and acid Trypsin Sensitive
Specific adherence by lipoteichoic acid and M-protein • (LTA-M) complexes
Antigenic Structure Streptococcus pyogenes (Group A)
Lancefield Group-specific antigen (C polysaccharide) Complex polysaccharide in cell wall
Proteins: Two major classes, M & T antigens Two minor classes, R & F
M-Protein: Type-specific antigen Fimbriae-like, hairy extensions
Resistant to heat and acid Trypsin Sensitive
Specific adherence by lipoteichoic acid and M-protein (LTA-M) complexes
T Antigens (not virulence factor) Resistant to trypsin, heat and acid; Adjunct to M-typing; Routine surveillance
Others

Antigenic Structure (cont.) Streptococcus pyogenes (Group A)
Capsular Polysaccharide: Hyaluronic acid
Not present in all strains Same as host hyaluronic acid (cartilage,skin etc) Nonimmunogenic Antiphagocytic Hyaluronidase (cell wall division) during late growth
Lipoteichoic Acid

Lancefield Serogroup Classification of Beta-Hemolytic Streptococci Important in
Human Disease
Group A Streptococci: Streptococcus pyogenes
• One of Most Important Human Pathogens
• Suppurative Diseases: Pharyngitis; Scarlet Fever; Cutaneous & Soft Tissue Infections Systemic Disease
• Non-Suppurative Sequelae:ARF,RHD,AG

Streptococcus pyogenes
(Phase Contrast)
Lancefield Serogroup Classification of Beta-Hemolytic Streptococci Important in
Human Disease (cont.)
Group B Streptococci: Streptococcus agalactiae
•Neonatal disease & obstetric complications
•Systemic, Cutaneous, UTI's

Streptococcus agalactiae

Lancefield Classification of Beta-Hemolytic Streptococci (cont.)
Group C Streptococci: Pharyngitis
Group G Streptococci: S.anginosus-milleri grp; Streptococcus spp.
Pharyngitis Non-Lancefield Group Streptococci
Viridans Streptococci Dental Caries: Streptococcus mutans Streptococcus sanguis; Streptococcus salivarius; Streptococcus mitis
Streptococcus pneumoniae
Enterococcus & Group D Streptococci Genitourinary Tract Infections (UTIs) Endocarditis

Major Human Diseases of Beta-Hemolytic Streptococci
Group A Streptococcus (S. pyogenes): Diverse group of acute suppurative (pus-forming) & nonsuppurative diseases
Suppurative Streptococcal Diseases Pharyngitis (& tonsilitis):
Scarlet fever: Complication of streptococcal pharyngitis when infecting strain is lysogenized; Frequently develop scarletina rash on upper chest spreading to extremities
Cutaneous & Soft Tissue Infxns. Pyoderma (Impetigo: contagious pyoderma with superficial yellow weeping lesions) Erysipelas: Acute superficial cellulitis of skin with lymphatic involvement; face and lower extremities, skin and subcutaneous tissues
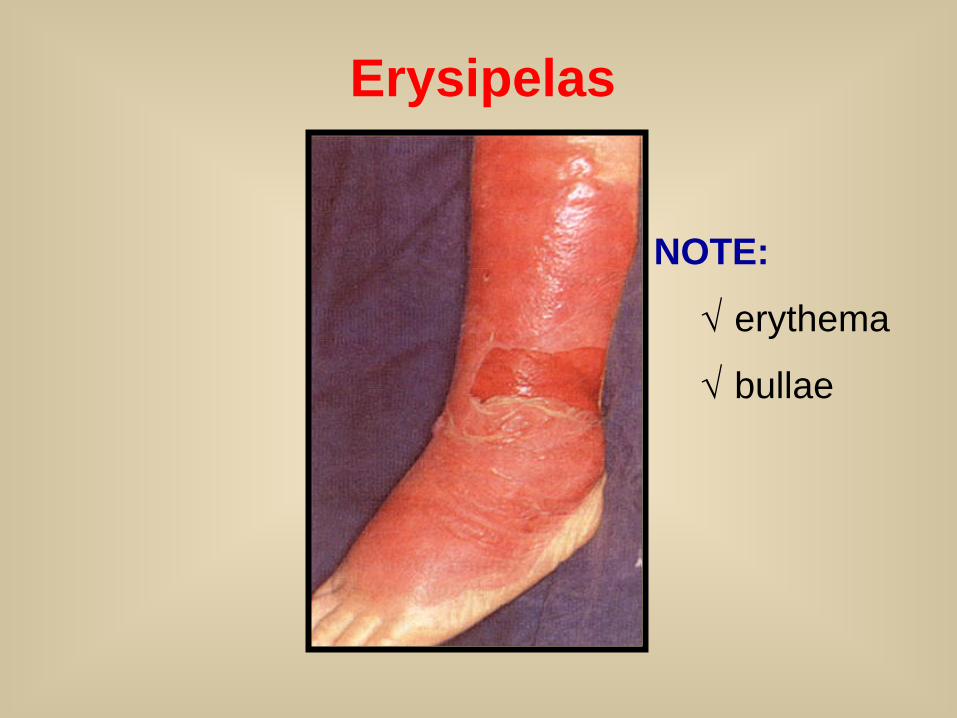
Erysipelas
NOTE:
√ erythema
√ bullae

Major Human Diseases of Beta-Hemolytic Streptococci (cont.)
Group A Streptococcus (S. pyogenes)
Suppurative Streptococcal Diseases Cutaneous & Soft Tissue Infxns(cont.)
Cellulitis: Involvement of deeper subcutaneous tissues; Deeper invasion with systemic symptoms
Necrotizing fasciitis: (a.k.a., “flesh-eating bacteria”): Infection deep in subcutaneous tissues that spreads along fascial planes, destroying muscle and fat; Initially cellulitis followed by bullae (fluid filled blisters; bulla is singular), gangrene, systemic toxicity, multiorgan failure and mortality in more than 50% of patients
Wound Infections

Suppurative Streptococcal Diseases Group A Streptococcus (cont.)
Other Suppurative Diseases Puerperal & neonatal sepsis Lymphangitis: Inflammation of lymphatic vessel(s) Pneumonia
Systemic Disease
Streptococcal Toxic Shock Syndrome (TSS): Multisystem toxicity following soft tissue infection progressing to shock and organ failure (not to be confused with Staphylococcal Toxic Shock Syndrome where hyperabsorbent tampons have been identified as an important risk factor)
Bacteremia

Group A Streptococcal Diseases (cont.)
Nonsuppurative Sequelae Post-infection complications of Group A streptococcal disease; Serious complications in pre-antibiotic era; still important in developing countries Acute rheumatic fever (ARF):
Inflammation of heart, joints, blood vessels, sub-cutaneous tissues
Rheumatic heart disease (RHD): Chronic, progressive heart valve damage
Acute glomerulonephritis (AG): Acute inflammation of renal (kidney) glomeruli
Foodborne Disease
Epidemiology of Acute Streptococcal Infection
• Predilection for upper respiratory tract or skin
•Group A commonly colonize oropharynx of healthy children
• M-types of strains colonizing throat differ from those on skin
• Rapidly killed after phagocytosis, but cell walls not digested and may lead to chronic inflammatory lesions
Pharyngitis transmitted by droplets from respiratory secretions • Crowding increases risk (e.g., classrooms, day care facilities)
Pyoderma transmitted by direct contact with infectious lesions

Nonsuppurative Sequelae of Acute Group A Streptococcal Infection
Acute Rheumatic Fever (ARF) Inflammatory reaction characterized by arthritis, carditis, chorea (disorder of CNS with involuntary spastic movements), erythema marginatum (skin redness with defined margin), or subcutaneous nodules Within 2-3 weeks following pharyngitis • Epidemic pharyngitis: ARF in as many as 3% • Sporadic pharyngitis: ARF in 1 per 1000
Morbidity & mortality linked to subsequent disease of heart valve (Rheumatic Heart Disease)
Poorly understood pathogenesis with several proposed theories including cross-reactivity of heart tissues & strep AGNs •?? (Type ?? hypersensitivity, exotoxins, direct invasion) II

Nonsuppurative Sequelae of Acute Group A Streptococcal Infection (cont.)
Acute Glomerulonephritis Follows either respiratory (pharyngitis) or cutaneous (pyoderma) streptococcal infection Associated with well-defined group of M-types Incidence varies from <1% to 10-15% Most often seen in children manifesting as dark, smoky urine with RBC's, RBC casts, white blood cells, depressed serum complement, decreased glomerular filtration rate Latent period: 1-2 weeks after skin infection and 2-3 weeks after pharyngitis
Granular accumulations of immunoglobulin due to deposition of immune complexes within the kidney (Type ?? Hypersensitivity) III


Determinants of Pathogenicity Cellular Virulence Factors
Capsule Antiphagocytic; Nonspecific adherence Hyaluronic acid (polysaccharide) mimics animal tissue
Lipoteichoic Acid Cytotoxic for wide variety of cells Adherence: Complexes with M protein (LTA-M) and binds to fibronectin on epithelial cells
M-Protein LTA-M protein is adhesin Antiphagocytic Inhibits alternate C’ pathway and opsonization
M-like Proteins: bind IgM and IgG F Protein: mediates adherence

Extracellular Virulence Factors Exotoxins:
Streptolysin O (SLO): Hemolytic and Cytolytic Prototype of oxygen-labile and thiol-activated cytolytic exotoxins (e.g., Streptococcus, Bacillus, Clostridium, Listeria)
Lytic for variety of cells: bind to cholesterol-containing membranes and form arc- or ring- shaped oligomers that make cell leaky (RBC's, WBC’s, PMN's, platelets, etc.)
Causes sub-surface hemolysis on BAP
Stimulate release of lysosomal enzymes
SLO titer indicates recent infection (300-500 in pediatric populations)

Extracellellular Virulence Factors (cont.)
Exotoxins (cont.):
Streptolysin S (SLS): Hemolytic and Cytolytic
Oxygen stable, non-antigenic
Lytic for red and white blood cells and wall-less forms (protoplast, L- forms)
Causes surface hemolysis on BAP Lysogeny: Lysogenized bacteriophages play key role in directing synthesis of various Group A streptococcal enzymes and toxins
• Pyrogenic Exotoxin (erythrogenic toxin)
• Phage-associated muralysins (lyse cell walls) produced by both Groups A and C
Extracellular Virulence Factors (cont.)
Exotoxins (cont): Pyrogenic (Erythrogenic) Exotoxins (Types A, B &C)
Produced by more than 90% of Grp A strep Lysogeny: Structural gene is carried by temperate bacteriophage, as is the case with diphtheria toxin
Mediate pyrogenicity (fever)
Causes scarlet fever (scarletiniform) rash
Increase susceptibility to endotoxic shock Type C toxin increases permeability of blood-brain barrier
Enhance DTH
Mitogenic for T lymphocytes (cause cell division), myocardial and hepatic necrosis, decrease in antibody synthesis
Immunomodulators (superantigens): stimulate T cells to release cytokines
Cardiohepatic toxin

Extracellular Virulence Factors (cont.)
Enzymes:
Nucleases: Four antigenic types (A,B,C,D) Facilitate liquefication of pus generating growth substrates Nucleases A, C have DNase activity Nucleases B, D also have RNase activity
Streptokinases: Two different forms Lyse blood clots: catalyze conversion of plasminogen to plasmin, leading to digestion of fibrin
C5a Peptidase: destroys C’ chemotactic signals (C5a) Hyaluronidase: hydrolyzes hyaluronic acid Others: Proteinase, NADase, ATPase, phosphatase, etc.

Lab Identification of S. pyogenes (Group A)
• Primary culture by pour or streak plate
• Domed,grayish/opalescent colonies
• Encapsulated cells produce mucoid colonies
Beta-hemolytic • Zone several times greater than diameter of colony

TSA
S. pyogenes

Lab Identification of S. pyogenes (Group A) (cont.)
Catalase Negative: Differentiates from Staphylococcus
Bacitracin test: presumptively distinguishing between Group A beta-hemolytic streptococci (bacitracin POS) and other beta-hemolytic streptococci that are isolated from pharyngeal swabs (95% sensitivity for Grp A strep)
Rapid Identification Tests: Based on extraction of Group A carbohydrate directly from throat swabs
• ELISA, Coagglutination, Fluorescent Antibody


Group B Streptococcus
Streptococcus agalactiae

Group B Streptococcal Infections

Grp B Streptococcal Infections (cont.)

Age-Specific Attack Rates of Group B Streptococcal Disease

Epidemiology of Neonatal Group B Streptococcal Disease

Group B Streptococcus S. agalactiae
Diagnostic Laboratory Tests • CAMP factor positive
• Hippurase positive

CAMP Factor Test S. aureus
(Spingomyelinase C) Group B
Streptococcus (CAMP Factor)
Group A Streptococcus
Enhanced Zone of
Hemolysis

Hippurase NEG

Hippurase POS
Grp B Streptococci
and
Campylobacter


Streptococcus pneumoniae
• Commonly referred to as pneumococcus
• Formerly Diplococcus pneumoniae

Streptococcus pneumoniae Infections

Epidemiology (cont.) Pneumococcal Infections (cont.)

S. pneumoniae
• Diplococcus

S. pneumoniae: lancet-shaped diplococcus

S. pneumoniae Virulence Factors

S. pneumoniae Seasonal Incidence

Comparison of Morbidity & Mortality
for Bacterial Meningitis

Genetic Variation (Mutation)

Beginning of Molecular Genetics

Transformation (In vivo) (Griffith)

Streptococcus pneumoniae
Diagnostic Laboratory Tests • Optochin sensitivity (Taxo P disc)
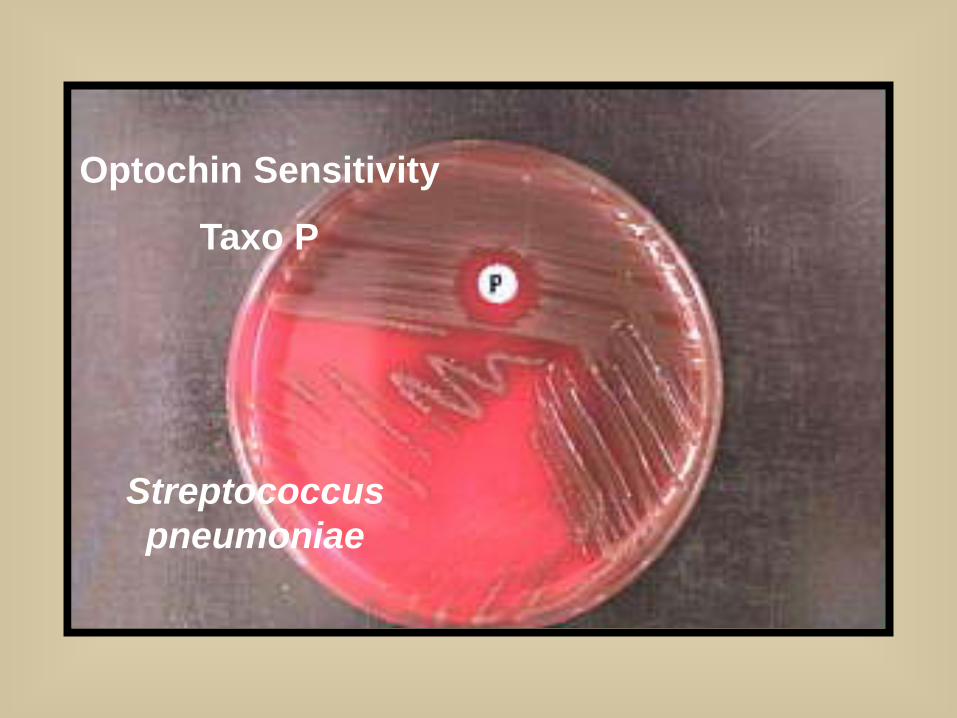
Optochin Sensitivity
Taxo P
Streptococcus pneumoniae


Enterococcus faecalis Enterococcus faecium
• GI tract of humans and animals
• Group D carbohydrate cell wall antigen
• Formerly Streptococcus

Enterococcal Infections

Enterococcal Infections (cont.)

Important nosocomial pathogen
Vancomycin resistant Enterococcus (VRE)

Enterococcus
Diagnostic Laboratory Tests • Resistant to bile
• Esculin hydrolysis
• BEA media

Bile Esculin Agar
POS
Enterococcus
Group D Streptococcus
Bile Esculin Agar
NEG

Esculin Bile
Assay


REVIEW

Lancefield Serogroup Classification of Beta-Hemolytic Streptococci Important in
Human Disease
Group A Streptococci: Streptococcus pyogenes
One of Most Important Human Pathogens Suppurative Diseases: Pharyngitis; Scarlet Fever;
Cutaneous & Soft Tissue Infections; Systemic Disease
Non-Suppurative Sequelae:ARF,RHD,AG Group B Streptococci:
Streptococcus agalactiae Systemic, Cutaneous, UTI's Neonatal disease Obstetric Complications REVIEW

Nonsuppurative Sequelae of Acute Group A Streptococcal Infection
Acute Rheumatic Fever (ARF) Inflammatory reaction characterized by arthritis, carditis, chorea (disorder of CNS with involuntary spastic movements), erythema marginatum (skin redness with defined margin), or subcutaneous nodules Within 2-3 weeks following pharyngitis • Epidemic pharyngitis: ARF in as many as 3% • Sporadic pharyngitis: ARF in 1 per 1000
Morbidity & mortality linked to subsequent disease of heart valve (Rheumatic Heart Disease)
Poorly understood pathogenesis with several proposed theories including cross-reactivity of heart tissues & strep AGNs •?? (Type ?? hypersensitivity, exotoxins, direct invasion) II REVIEW

Nonsuppurative Sequelae of Acute Group A Streptococcal Infection (cont.)
Acute Glomerulonephritis Follows either respiratory (pharyngitis) or cutaneous (pyoderma) streptococcal infection Associated with well-defined group of M-types Incidence varies from <1% to 10-15% Most often seen in children manifesting as dark, smoky urine with RBC's, RBC casts, white blood cells, depressed serum complement, decreased glomerular filtration rate Latent period: 1-2 weeks after skin infection and 2-3 weeks after pharyngitis
Granular accumulations of immunoglobulin due to deposition of immune complexes within the kidney (Type ?? Hypersensitivity) III REVIEW

Determinants of Pathogenicity Cellular Virulence Factors
Capsule Antiphagocytic; Nonspecific adherence Hyaluronic acid (polysaccharide) mimics animal tissue
Lipoteichoic Acid Cytotoxic for wide variety of cells Adherence: Complexes with M protein (LTA-M) and binds to fibronectin on epithelial cells
M-Protein LTA-M protein is adhesin Antiphagocytic Inhibits alternate C’ pathway and opsonization
M-like Proteins: bind IgM and IgG F Protein: mediates adherence REVIEW
Extracellular Virulence Factors Exotoxins:
Streptolysin O (SLO): Hemolytic and Cytolytic Prototype of oxygen-labile and thiol-activated cytolytic exotoxins (e.g., Streptococcus, Bacillus, Clostridium, Listeria)
Lytic for variety of cells: bind to cholesterol-containing membranes and form arc- or ring- shaped oligomers that make cell leaky (RBC's, WBC’s, PMN's, platelets, etc.)
Causes sub-surface hemolysis on BAP
Stimulate release of lysosomal enzymes
SLO titer indicates recent infection (300-500 in pediatric populations) REVIEW

Extracellellular Virulence Factors (cont.)
Exotoxins (cont.):
Streptolysin S (SLS): Hemolytic and Cytolytic
Oxygen stable, non-antigenic
Lytic for red and white blood cells and wall-less forms (protoplast, L- forms)
Causes surface hemolysis on BAP
REVIEW

Extracellular Virulence Factors (cont.)
Exotoxins (cont): Pyrogenic (Erythrogenic) Exotoxins (Types A, B &C)
Produced by more than 90% of Grp A strep Lysogeny: Structural gene is carried by temperate bacteriophage, as is the case with diphtheria toxin
Mediate pyrogenicity (fever)
Causes scarlet fever (scarletiniform) rash
Increase susceptibility to endotoxic shock Type C toxin increases permeability of blood-brain barrier
Enhance DTH
Mitogenic for T lymphocytes (cause cell division), myocardial and hepatic necrosis, decrease in antibody synthesis
Immunomodulators (superantigens): stimulate T cells to release cytokines
Cardiohepatic toxin REVIEW

Extracellular Virulence Factors (cont.)
Enzymes:
Nucleases: Four antigenic types (A,B,C,D) Facilitate liquefication of pus generating growth substrates Nucleases A, C have DNase activity Nucleases B, D also have RNase activity
Streptokinases: Two different forms Lyse blood clots: catalyze conversion of plasminogen to plasmin, leading to digestion of fibrin
C5a Peptidase: destroys C’ chemotactic signals (C5a) Hyaluronidase: hydrolyzes hyaluronic acid Others: Proteinase, NADase, ATPase, phosphatase, etc.
REVIEW

Epidemiology of Neonatal Group B Streptococcal Disease
REVIEW
REVIEW

Streptococcus pneumoniae Infections
REVIEW
Infections from endogenous spread from naso- or orapharynx
Pneumonia; sinusitis; otitis media; bacteremia; meningitis
Colonization highest in children
Antecedent viral respiratory tract disease increases risk
Most common in cold months
Polyvalent vaccine available (newly available for children)
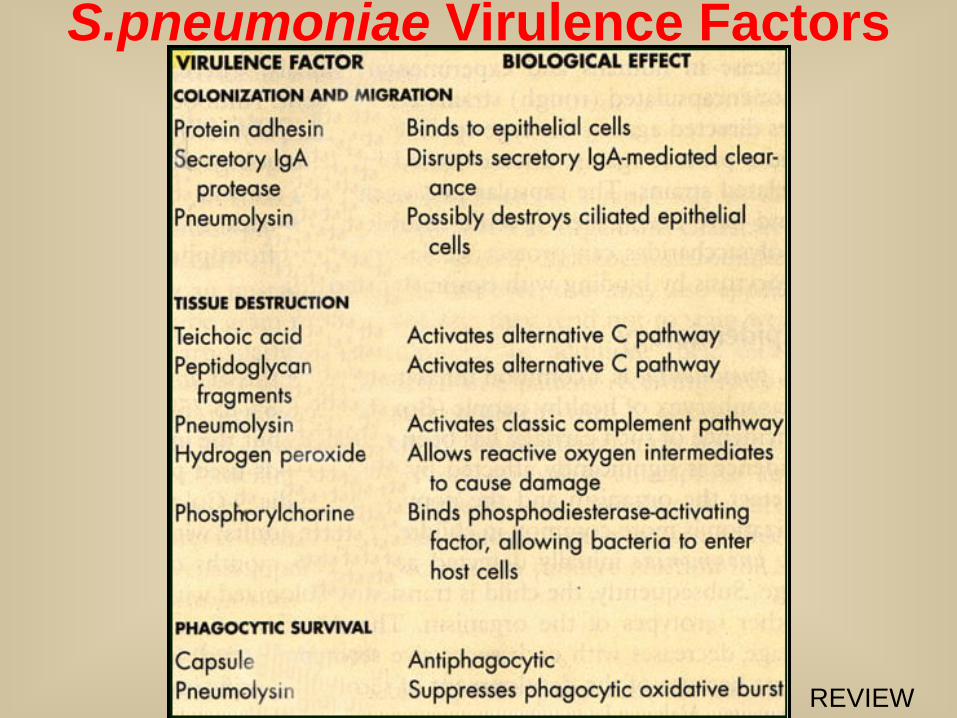
S.pneumoniae Virulence Factors
REVIEW

Comparison of Morbidity & Mortality
for Bacterial Meningitis
REVIEW
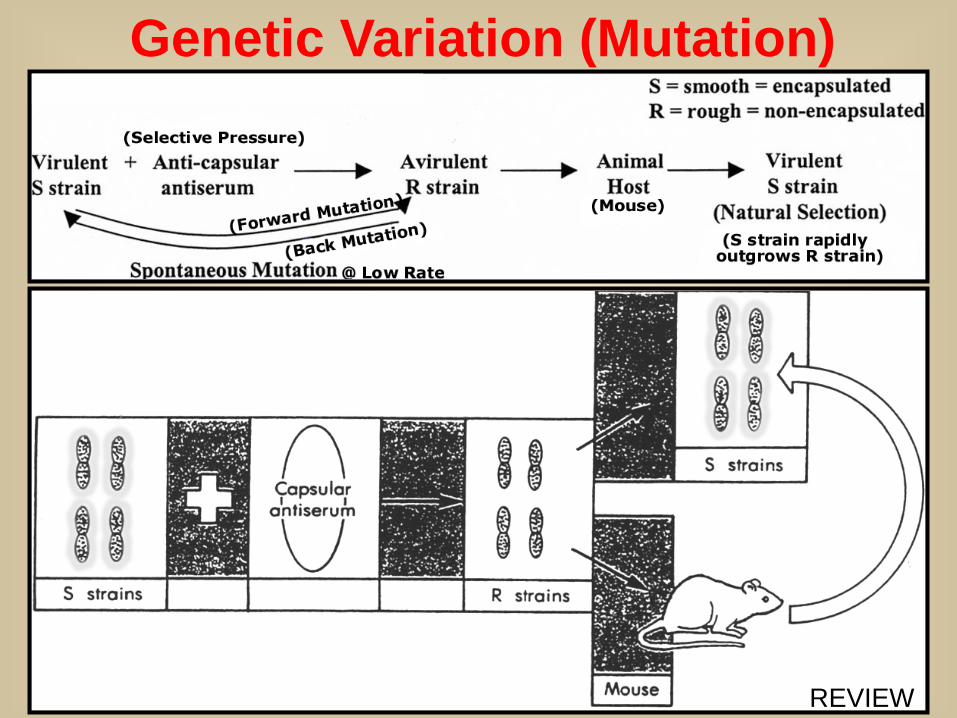
Genetic Variation (Mutation)
REVIEW

Beginning of Molecular Genetics
REVIEW
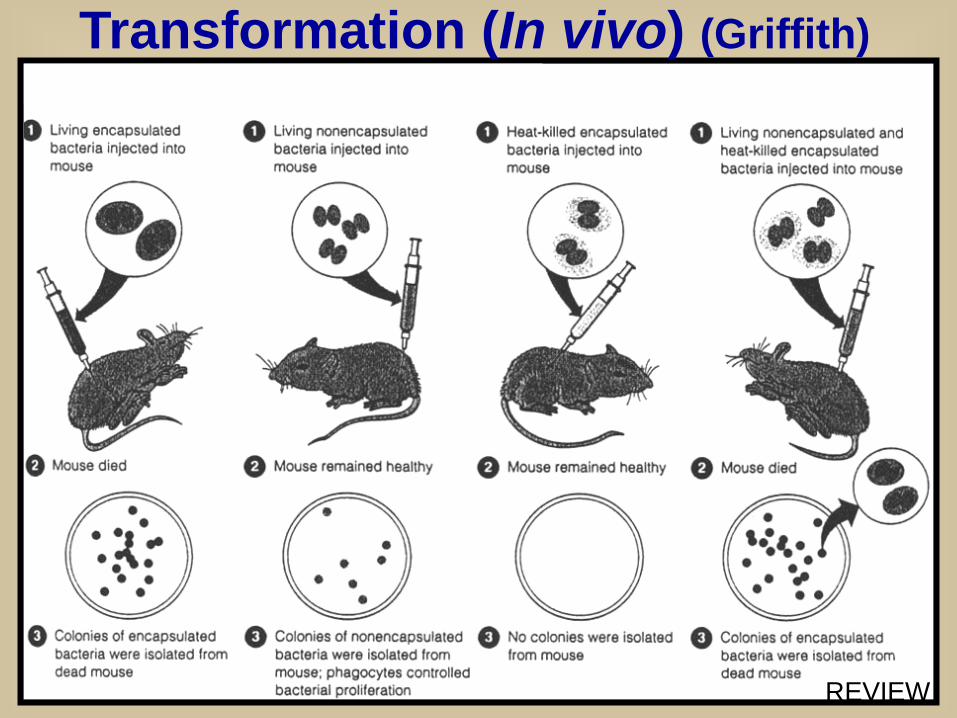
Transformation (In vivo) (Griffith)
REVIEW
Enterococcal Infections
REVIEW
Group D cell wall antigen
Enterococcus faecalis; Enterococcus faecium
GI tract of humans and animals
UTI most common; wound infections; bacteremia; endocarditis
Most infections from endogenous source
Prolonged hospitalization and broad-spectrum antibiotics increase risk
Antibiotic resistance (VRE)








