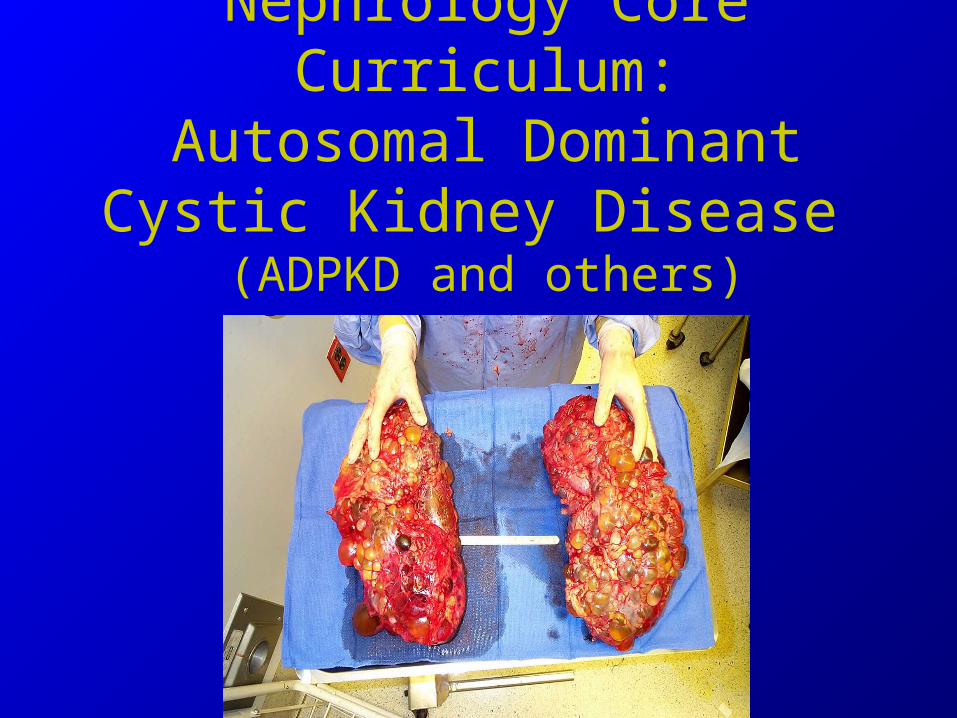
Nephrology Core Curriculum:Autosomal Dominant Cystic
Kidney Disease (ADPKD and others)

Inherited Kidney DiseasesBackground
• Dominant inherited polycystic diseases– ADPKD– Tuberous sclerosis– von Hippel-Lindau disease
• Recessive inherited polycystic diseases– ARPKD
• As would be expected with recessive, onset early in life with ESRD in youth
• Always associated with congenital hepatic fibrosis

Tuberous Sclerosis
• Hereditary disease with hamartomas in multiple organ systems– Autosomal dominant with high penetrance, but
extreme phenotypic variability

Tuberous SclerosisClinical Features
• Hamartomas– Benign tumors resulting from
disordered cell migration• Skin
– Facial angiofibromas (adenoma sebaceum)
– Fibrous forehead plaques– Ungual fibromas– Shagreen patches-
lumbosacral palpable lesions
– Hypomelanotic macules- earliest and most common skin lesions, occurring in 90% of cases
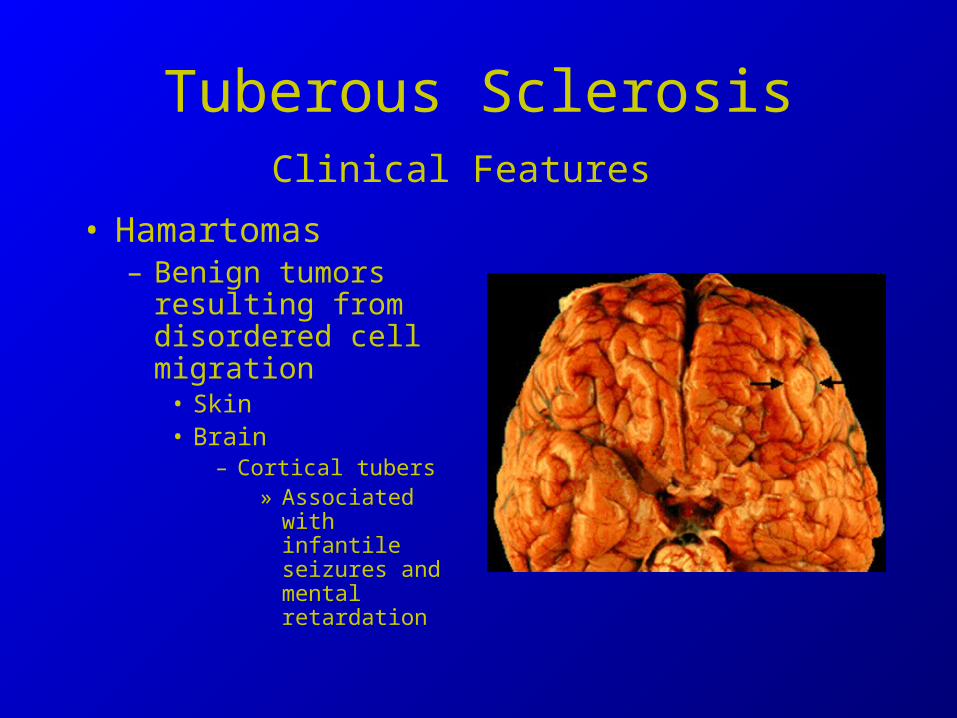
Tuberous SclerosisClinical Features
• Hamartomas– Benign tumors
resulting from disordered cell migration
• Skin • Brain
– Cortical tubers» Associated with
infantile seizures and mental retardation
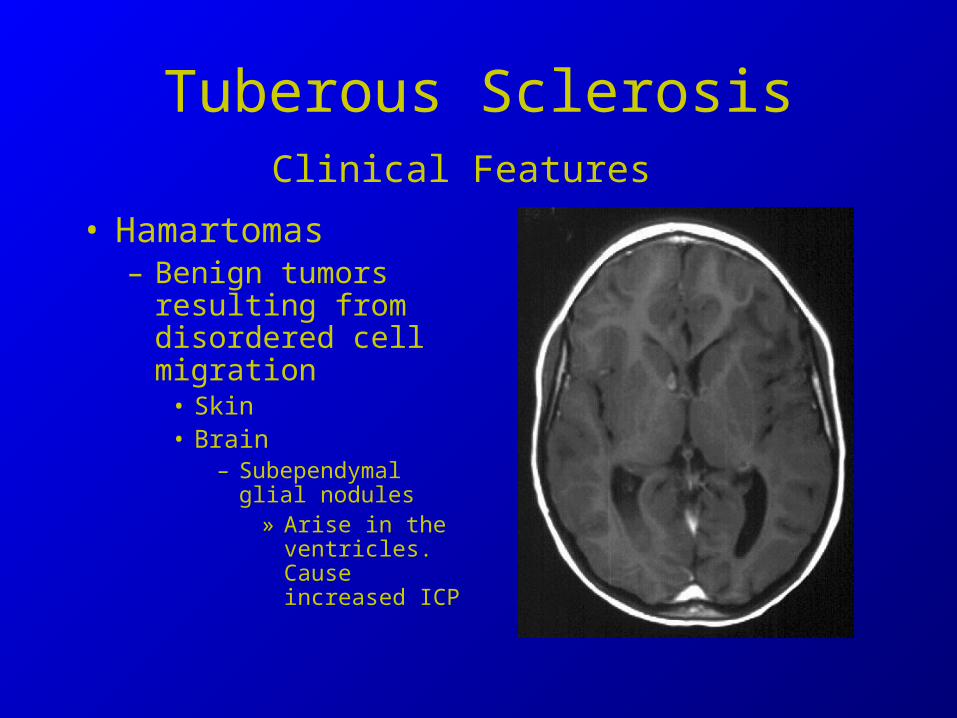
Tuberous SclerosisClinical Features
• Hamartomas– Benign tumors
resulting from disordered cell migration
• Skin • Brain
– Subependymal glial nodules
» Arise in the ventricles. Cause increased ICP

Tuberous SclerosisClinical Features
• Hamartomas– Other organs affected:
• Skin
• Brain
• Retina
• Heart- cardiac rhabdomyomas
• Kidneys
• Liver
• Lungs
• Bone

Tuberous SclerosisClinical Features
• Hamartomas– Benign tumors resulting from disordered cell migration
• Kidneys– Present in 50% of cases
– #1 lesion is angiomyolipomas
» Benign lesion made of adipose tissue, smooth muscle cells, and arterial vessels
» Fat content makes them easy to diagnose by CT scan
» Bleeding is a risk if >4cm, esp during pregnancy
– Renal cysts (unrelated to angiomyolipomas) also occur in 30% of patients

Tuberous SclerosisDiagnosis
• No definitive features
• Made by combination of major and minor features– Require at least two features

Tuberous SclerosisManagement
• No specific therapy
• Consensus conference– Evaluated every 1 to 3 years with renal US, CT
or MRI of the brain– One chest radiograph in adult women
• Surgical resection for CNS lesions causing hydrocephalus
Von Hippel-Lindau Disease
• Autosomal dominant disease with high penetrance– Development of benign and malignant tumors
in multiple organs• Type I - NO pheos
• Type II- Pheos (runs in 7-20% of families)

Von-Hippel-Lindau DiseaseClinical Features
• Potential Sites-
– Central nervous system, eyes, kidneys, adrenal glands, pancreas, and epididymis are commonly affected
• Usual lesions– CNS hemangioblastomas
• In the cerebellum, spinal cord and brainstem. No supratentorial lesions
• Benign, but mass effects cause difficulties
– Recur after surgery

Von-Hippel-Lindau DiseaseClinical Features
• Usual lesions– Retinal
hemangioblastomas• In 50% of cases
• Multiple or bilateral
• Red “dots” on retina that slowly enlarge
• Regular ophtho eval important
– Laser tx
Von-Hippel-Lindau DiseaseClinical Features
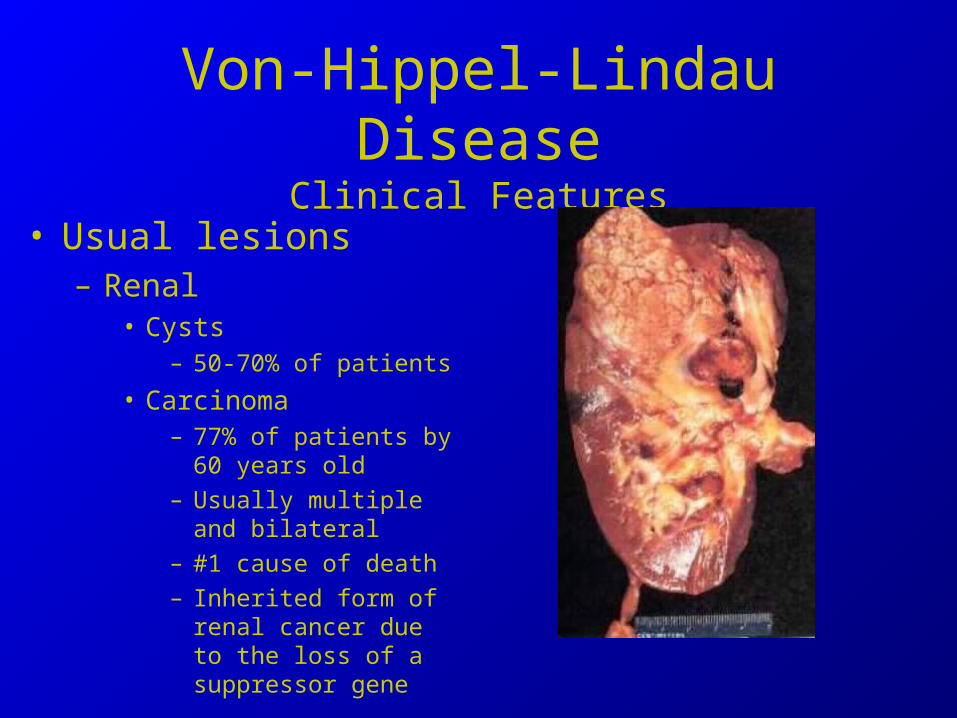
• Usual lesions– Renal
• Cysts– 50-70% of patients
• Carcinoma– 77% of patients by 60 years
old
– Usually multiple and bilateral
– #1 cause of death
– Inherited form of renal cancer due to the loss of a suppressor gene

Von-Hippel-Lindau DiseaseClinical Features
• Usual lesions– Pancreas
• Cysts in 30% of patients
• Likely to cause confusion with ADPKD

Von-Hippel-Lindau DiseaseDiagnosis
• Positive family history, plus a single hemangioblastoma or visceral lesion
• No family history, two or more hemangioblastomas or one and a visceral lesion
• Direct mutation analysis is now possible
• Distinguish from ADPKD– Both with kidney cysts
– ADPKD with rare panc and freq hepatic
– VHL with rare hepatic and freq panc• Suspect in any patient with kidney
and pancreas cysts without liver cysts

Von-Hippel-Lindau DiseaseManagement
• Regular screening program– Annual physical and
ophtho
– Annual MRI of CNS
– Annual abdominal imaging• Either US,CT,MRI
– If positive family history,• Periodic metanephrines
screening for pheo

ADPKDEpidemiology
• Prevalence approximately 1:400 to 1:1000 in people of European descent– 600,000 Americans with the
disease– More than CF, muscular
dystrophy, hemophilia, Down’s syndrome and sickle cell anemia– COMBINED
– Frequency in Non-Europeans unknown
• 4% of ESRD patients• Common in cats
ADPKDGenetics
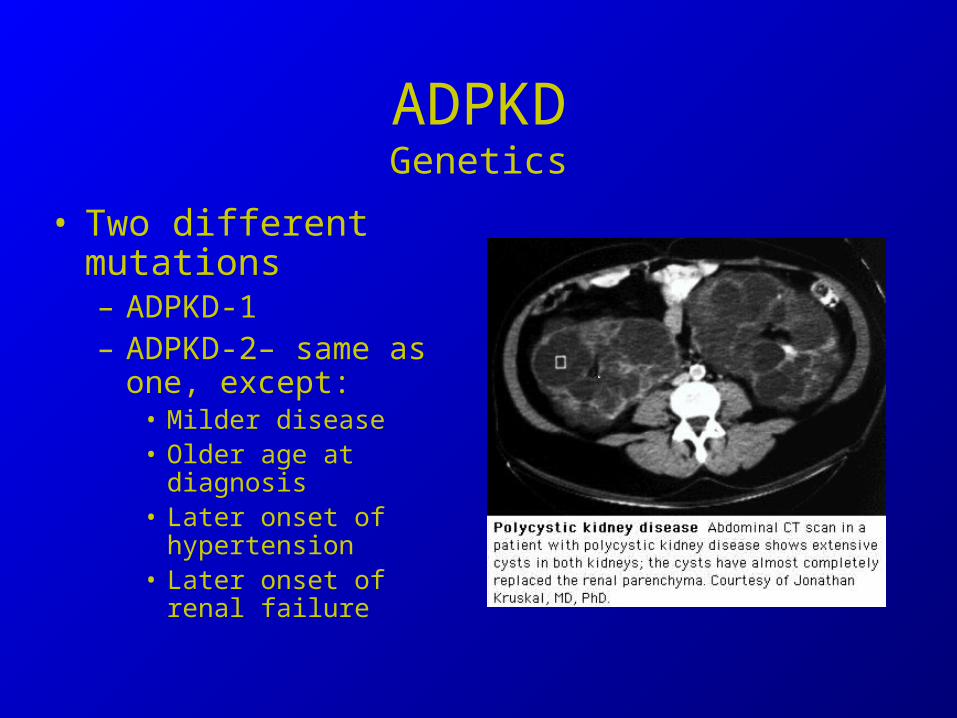
• Two different mutations– ADPKD-1– ADPKD-2– same as
one, except:• Milder disease• Older age at diagnosis• Later onset of
hypertension• Later onset of renal
failure

ADPKDGenetics
• Only 1-2% of tubules affected– Two-hit hypothesis– genetic abnormality not sufficient,
requires an additional insult to manifest• (argument for aggressive treatment of ADPKD patients)
• Cysts begin as focal dilatations of tubular segments
• Not just impermeable cul-de-sacs. They collect and store urine from more proximal nephron segments
– Synthesize and transport proteins, hormones, and cytokines

ADPKDDiagnosis
• Ultrasound– Insert Australian ultrasound study– Age adjusted criteria
• 18-29yo, at least 2 cysts• 30-59yo, at least 2 cysts in each kidney• >60yo, four cysts in each kidney
– For r/o diagnosis of ADPKD in patient at risk, no age at which 100% of gene carriers have detectable cysts
• US can only prove ADPKD, it cannot r/o• 2 studies in families with gene linkage
analysis showed no false negatives after age 30 yo (but only two families)
– Can’t just screen parents• 10% of ADPKD patients are new mutations

ADPKDGenetics
• Genetic tests by linkage analysis only– No direct mutation analysis– Requires at least two related family members with the
disease. – Expensive ($1000s)– Only utility is for donor screening
• Other reported uses include family planning decisions and prenatal diagnosis
– Athena diagnostics launched a molecular test based on direct mutation analysis
• Detects only 50% of PKD-1 and 75% of PKD-2 mutations• (takes 4 weeks and $2600 by credit card)
ADPKDSigns and Symptoms
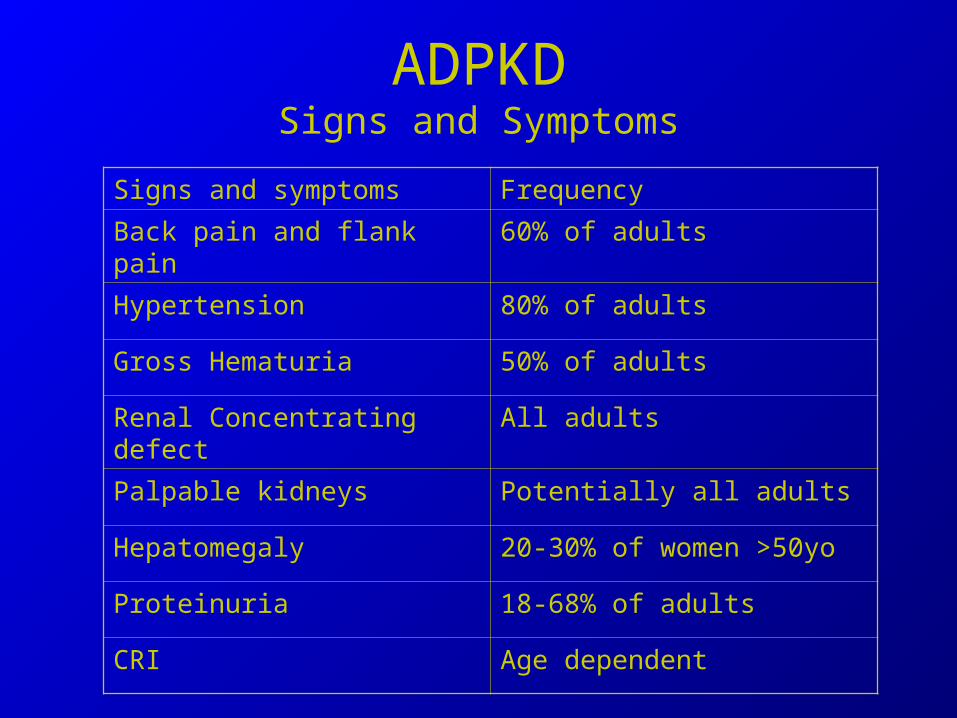
Signs and symptoms Frequency
Back pain and flank pain 60% of adults
Hypertension 80% of adults
Gross Hematuria 50% of adults
Renal Concentrating defect All adults
Palpable kidneys Potentially all adults
Hepatomegaly 20-30% of women >50yo
Proteinuria 18-68% of adults
CRI Age dependent

ADPKDSigns and Symptoms
• Back pain– Chronic- Likely the result of stretching of the renal
capsule by the enlarging cysts• Tylenol• Physical measures- ice massage and heating packs• TENS• Autonomic plexus blockade• Decompression of cysts
– Usually laproscopic. Can drain one or hundreds of cysts– Immediate pain relief in 90%. Persistent relief at 3 years in 25-
60% of patients– Some bp improvement.

ADPKDSigns and Symptoms
• Hypertension– Occurs well before renal insufficiency
• 40% by 18-24yo
• 54% by 24-30yo
• 65-80% > 30yo
– Hypertension correlates with renal size• Mechanism clearly complex– but demonstrated to
have hyperplasia of renin producing cells and increased renin levels

ADPKDSigns and Symptoms
• Gross hematuria– Painless or associated with dull colicky pain– 40-50% of patients experience at least one
episode• In 20% of patients it is how ADPKD is discovered
– Last 2-7days and cease spontaneously– Can be seen on CT with contrast- high density
cyst without enhancement after administration of contrast

ADPKDSigns and Symptoms
• Renal concentrating defect• Palpable kidneys- exam is poor at
estimating size• Palpable hepatomegaly
– 20-30% of patients older than 50
• UTI– Must use lipophilic agents to treat
• Cipro, Clindamycin, Emycin, and Bactrim

ADPKDManifestations
Not just a renal process, it is a basement membrane abnormality that affects multiple sites
Manifestation Frequency
Renal Cysts 100% by 30 yo
Nephromegaly 95% by 30 yo
Decreased concentrating ability All adults
Hypertension 65-80% of adults
Extra-renal
Liver cysts 75% by age 60yo
Pancreatic cysts 9% after age 30yo
Seminal vesicle and prostate
cysts
60% and 11% at 40yo
Arachnoid cysts 5-8%
MVP 25%
Intracranial Aneurysms 2-3%
Abdominal Wall Hernia 45% with ESRD
ADPKDSigns and Symptoms
• Nephrolithiasis– 20-36%– Stone composition
• Higher uric acid than general population--- 50%• Remainder CaOx
– Due to metabolic factors and urine stasis associated with distorted renal architecture
• 50% have hypocitraturia
– Can use lithotripsy

ADPKDSigns and Symptoms
• Renal Cell Cancer– No increased risk– Presence should raise the suspicion of a
misdiagnosis• Consider Von Hippel Lindau disease, esp. if familial
cancers

ADPKDUrinary findings
• Microscopic hematuria 23%• Pyuria up to 45%• Dipstick Proteinuria 34-68%
– Nephrotic range proteinuria does not occur with ADPKD alone
– Only 18% with > 300mg/day proteinuria
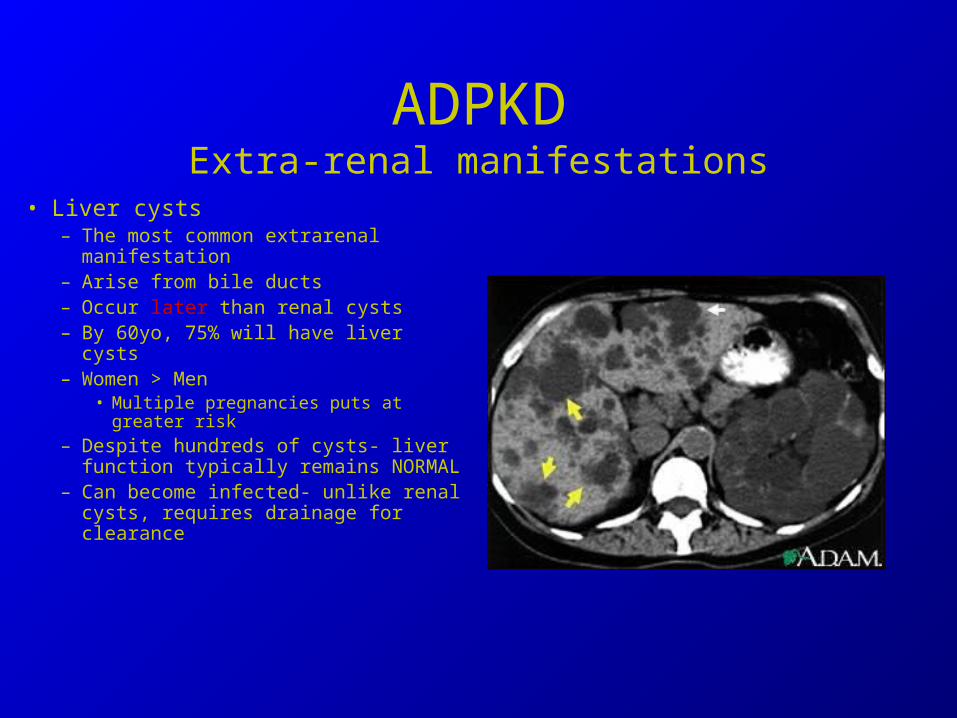
ADPKDExtra-renal manifestations
• Liver cysts– The most common extrarenal
manifestation– Arise from bile ducts– Occur later than renal cysts– By 60yo, 75% will have liver cysts– Women > Men
• Multiple pregnancies puts at greater risk
– Despite hundreds of cysts- liver function typically remains NORMAL
– Can become infected- unlike renal cysts, requires drainage for clearance

ADPKDExtra-renal manifestations
Cystic• Other cysts
– Pancreas- 9% of patients >30 yo– Ovaries No increase (12%)– Seminal vesicles 60%
• No signif
– Prostate 11%– Arachnoid cysts 8%

ADPKDExtra-renal manifestations
Non-Cystic• Mitral valve prolapse 25%• LVH• Intracranial Aneurysm• Colonic divertics
– Increased in ADPKD ESRD patients, but not pre-ESRD
• Abdominal wall hernias, up to 45%– Not associated with renal size or volume
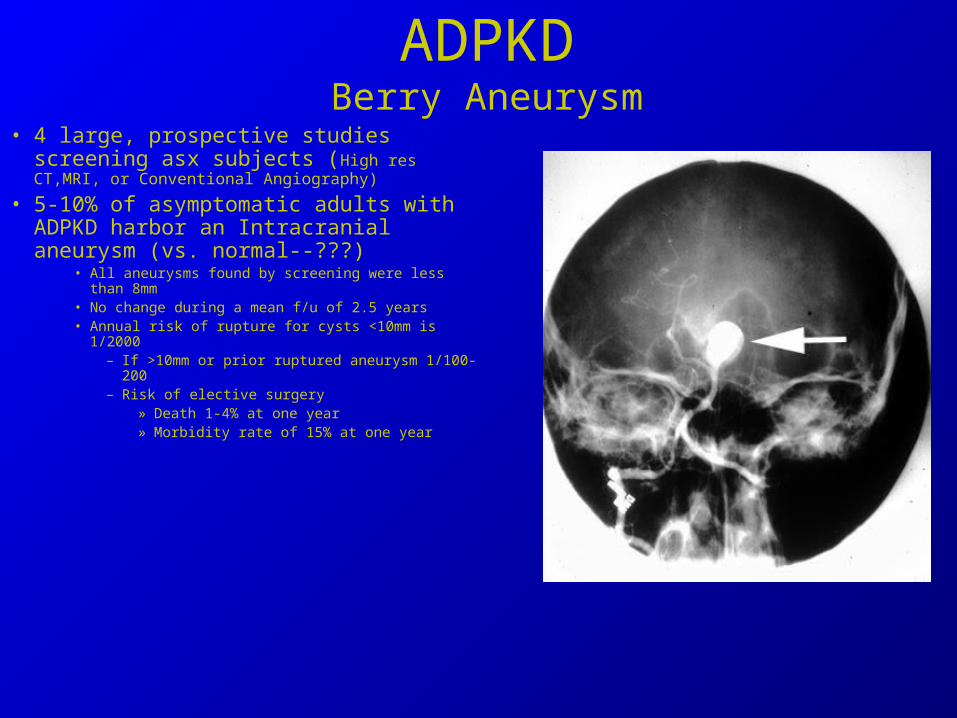
ADPKDBerry Aneurysm
• 4 large, prospective studies screening asx subjects (High res CT,MRI, or Conventional Angiography)
• 5-10% of asymptomatic adults with ADPKD harbor an Intracranial aneurysm (vs. normal--???)
• All aneurysms found by screening were less than 8mm• No change during a mean f/u of 2.5 years• Annual risk of rupture for cysts <10mm is 1/2000
– If >10mm or prior ruptured aneurysm 1/100-200– Risk of elective surgery
» Death 1-4% at one year» Morbidity rate of 15% at one year

ADPKDBerry Aneurysm
• Sawyer’s rule of 20s
– 1/20 chance of having an asx aneurysm (5-10%)– 1/200 chance of rupture if >10mm– 1/2000 chance of rupture if <10mm– 20% chance of complications with surgery
• 1-4% death + 15 % morbidity at one year
– 20% of aneurysms multiple
ADPKDSubarachnoid Hemorrhage
• Familial clustering of aneurysm rupture– Occurs in the general population
as well– 5% of ADPKD, but 22% if + fhx
• 20-30% with have multiple aneurysms
• 10% who have one aneurysm rupture will have a second rupture

ADPKDBerry Aneurysm
• Screening recommendations– Risk benefit ratio against routine screening of asx patients– Screen
• Prior rupture• Positive Family history• High risk occupation- Air Line Pilots etc• Prior to a surgery with hemodynamic instability associated with hypertension (KI, 1994 IC
aneurysms in ADPKD)• Neurologic symptoms suggestive of an aneurysm• ** Trash indication**
– Patient’s who need screening for peace of mind

ADPKDBerry Aneurysm
• Questions to answer if you screen anyway– How often?
• Does a negative screen you will never develop cysts?• At what age will you develop cysts?• Are you born with cysts and the remain stable for life, or do they enlarge?
– Serial MRAs show stability for at least 30 months– No de novo aneurysms over an 8 year period– Stable for 2.5 – 5 years, otherwise no data
– General recommendation are q5-10 years– Note
• ADPKD patients have more CVAs than subarachnoids• ADPKD patients have more hemorrhagic strokes than subarachnoids

ADPKDPregnancy with normal renal function
235 women with 605 pregnancies• ADPKD has no impact on fertility• Rate of live birth unchanged
– 77% vs. 82% of normals
• Fetal complication rate- unchanged• Maternal complications INCREASED (35% vs 19%)
– New or worsening hypertension– Pre-eclampsia– Edema
• No impact on renal function– Except if FOUR or more pregnancies and hypertensive

ADPKDESRD
• 50% at 60 years, 75% at 70 years at ESRD• Negative prognostic factors:
– HTN • Reviewed 1215 subjects• Median renal survival 14 years longer if not hypertensive by age 35 years old
– LVH– Male– Younger age at diagnosis-
• -difference of ten years to ESRD between onset <30 vs >30yo
– 3+ pregnancies, UTIs (in men)– Episodes of gross hematuria, H/o hypertension in parent– If you have HTN, hematuria, and diagnosis before age 30 years old– 100% ESRD by 48 yo
ADPKDModifier Genes
• ACE sub-type– 2 studies show impact, 2 don’t
• Sickle cell trait– Likely accelerates

ADPKDTreatment
• HTN– MDRD had 200 patients with ADPKD
• No protective effect over a mean 2.2 years– ? Disease already too far advanced
– Progression is slowed in animal models– Use of ACE-I
• No evidence that hemodynamics plays an important role in progression– Can perform unilateral nephrectomy without accelerating the disease process– Proteinuria always less than nephrotic range– However ultimate progression of disease is due to fibrosis and ACE-Is selectively
block
– Use of amiloride• Shown to block Na entry into cysts and halt cyst enlargement in animal
models

ADPKDTreatment
• Protein restriction– MDRD- no protective effect on moderate or severe restriction
• Cyst decompression– Pain management tool. No evidence for delayed disease progression
• Animal models• Protein restriction beneficial• Soy protein supplementation beneficial• Flaxseed beneficial• Statins beneficial • Alkalinization- helps in rats, but not mice
– Thought is that the 2nd ammonia genesis by the kidney in order to compensate leads to tubular damage

ADPKDCounseling and Screening
• Newly diagnosed patients should be informed about ADPKD, it’s hereditary nature, and that children have a 50% chance of inheriting the gene
• Before screening, subjects should be “informed of the consequences of diagnostic screening, particularly regarding insurability.”– My practice--Screening offers no benefit
• A negative US doesn’t r/o disease• A positive US will not lead to a change in therapy, but it will make the
person uninsurable and potentially unemployable• Gene linkage can be performed if potential donation is considered
-remember it costs approximately $2600

Acquired Cystic Kidney Disease
• Development of multiple, bilateral cysts in kidneys of patients with chronic renal disease due to causes other than cystic kidney disease– 10-20% of pre-dialysis patients– Increases with dialysis, 50% of patients on HD
x 3 years with cysts– Major determinant is the duration of renal
insufficiency
Acquired Cystic Kidney Disease• Cysts are usually less than 0.5 cm
– Occasionally reach 2-3cm
• Affect both the cortex and medulla• Result of a failure to clear unknown “mytogenic and
cystogenic” substances due to renal insufficiency– Lesions regress with transplantation
• Concern is transition to cancer– Men 7x more than women– Some recommend screening starting at 3years with annual
US– Given shortened lifespan with ESRD, others refute







