
Naviga&ngtheGray:ClinicalDecision-MakingwithFamiliesandtheirChildrenwithMedicalComplexityintheFaceof
Uncertainty
EmilyGoodwinMD,AssistantProfessorofPediatrics,Children’sMercyHospital,UniversityofMissouri,KansasCitySchoolofMedicine,KansasMO
KathleenHuthMDMMSc,InstructorofPediatrics,BostonChildren’sHospitalandHarvardMedicalSchool,BostonMA
NancyMurphy,MD,ProfessorandChief,DivisionofPediatricPMR,UniversityofUtahHealthSciencesCenter,SaltLakeCityUT
AACPDMIC27;Cincinna&2018

FINANCIAL DISCLOSURE AACPDM 72nd Annual Mee8ng October 9-13, 2018 Speaker Names: Emily Goodwin MD Kathleen Huth, MD, FRCPC, MMSC Nancy Murphy MD 1. Disclosure of Relevant Financial Relationships We have no financial relationships to disclose. 2. Disclosure of Off-Label and/or investigative uses: We will not discuss off label use and/or investigational use in our presentation.
AACPDMIC27;Cincinna&2018

Learningobjec&ves
1. Describetheimportanceandlimita&onsofevidence-basedprac&ceinthecareofCMCandneurodevelopmentaldisabili&es.
2. Demonstrateanapproachtograyscalethinkingappliedtocommonclinicalissuesthroughcase-baseddiscussions.
3. Applythe4basicprinciplesofhealthcareethicstochallengingdiagnos&candtreatmentdecisions,inpartnershipswithfamilies.
4. UsetheICFframeworktoguideclinicaldecision-makingforCMCandtheirfamilies,understandingtheimportanceofgoal-directedcare.
AACPDMIC27;Cincinna&2018

Course Overview
1. Defini&onsandapplica&onsofgrayscaledecision-making2. HowdowebestfeedaCMC?
Evidence,goalsofcare,anddecision-making.
3. HowdowebestmanagepaininaCMCandquadriplegicCP?Evidence,goalsofcare,anddecision-making.
4. Applyingtheprinciplesinterac&vely(3casestoconsider)5. Q&A
AACPDMIC27;Cincinna&2018
Naviga&ngtheGray:Defini&ons,FrameworksandApplica&ons
NancyMurphy,MDProfessorandChief,DivisionofPediatricPMR
UniversityofUtah,SaltLakeCityUT
AACPDMIC27;Cincinna&2018

Framingthedecisions
Grayscalethinking
• Easierorharder• Fasterorslower• Closerorfurther• Be`erorworse• Moreorless
Blackorwhitethinking• Rightorwrong• Goodorbad• Alwaysornever• Perfectordisastrous• Allornothing
AACPDMIC27;Cincinna&2018

Consideryourrecentclinicaldecisions
• ConvertGTtoGJ,orreviseaslippedfundoplica&on?• Systemicorintrathecalbaclofen?• Spinalfusionforadvancedscoliosiswithgoalofcomfort?• Where’sthelinesbetweenmedicalneglect-medicaliza&on-medicalchildabuse?
• Otherexamples?
AACPDMIC27;Cincinna&2018

AACPDMIC27;Cincinna&2018

AACPDMIC27;Cincinna&2018

AACPDMIC27;Cincinna&2018
Evidence
• Givesusconfidenceinourclinicaldecisionmaking• Armswithagreattoolsaseducators• Protectsusfrompayerdenials;empowersustomakeappeals• Protectsusfromli&ga&onshouldtherebeanadverseoutcome• Increasesadherencewithinterven&onswhenfamiliesarewell-informed
• It’sthe“goldstandard.”
AACPDMIC27;Cincinna&2018

h`ps://pct.libguides.com/EBM/levels-of-evidence.AccessedAugust19,2018.
AACPDMIC27;Cincinna&2018

Evidence-basedprac&ce
• EBPistheintegra&onofclinicalexper&se,pa&entvalues,andthebestresearchevidenceintothedecisionmakingprocessforpa&entcare.
• Clinicalexper&seisgroundedincumulatedexperience,educa&onandclinicalskills.
• Thepa&entbringstotheencounterhisorherownpersonalpreferencesanduniqueconcerns,expecta&ons,andvalues.
• Thebestresearchevidenceisusuallyfoundinclinicallyrelevantresearchthathasbeenconductedusingsoundmethodology.
h`p://guides.mclibrary.duke.edu/c.php?g=158201&p=1036021.AccessedAugust19,2018.AACPDMIC27;Cincinna&2018

Evidencebasedprac&ce
h`p://guides.mclibrary.duke.edu/c.php?g=158201&p=1036021.AccessedAugust19,2018.AACPDMIC27;Cincinna&2018
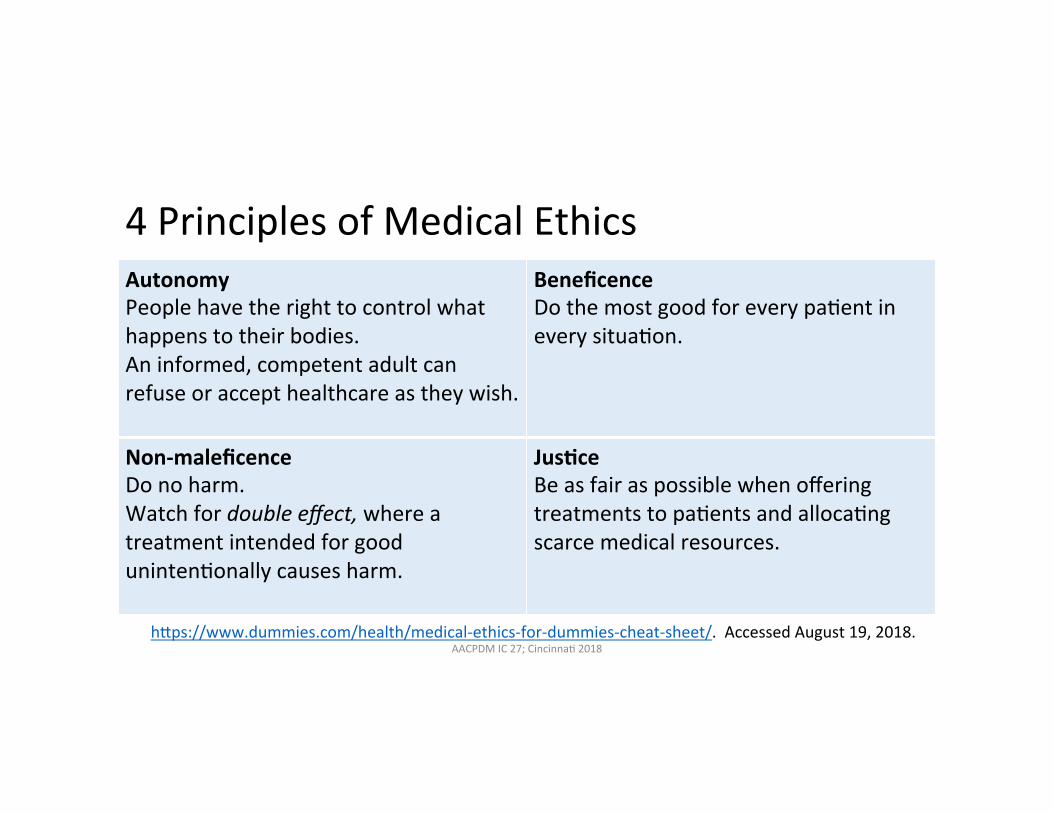
4PrinciplesofMedicalEthicsAutonomyPeoplehavetherighttocontrolwhathappenstotheirbodies.Aninformed,competentadultcanrefuseoraccepthealthcareastheywish.
BeneficenceDothemostgoodforeverypa&entineverysitua&on.
Non-maleficenceDonoharm.Watchfordoubleeffect,whereatreatmentintendedforgooduninten&onallycausesharm.
JusCceBeasfairaspossiblewhenofferingtreatmentstopa&entsandalloca&ngscarcemedicalresources.
h`ps://www.dummies.com/health/medical-ethics-for-dummies-cheat-sheet/.AccessedAugust19,2018.AACPDMIC27;Cincinna&2018
Afunc&onalapproachtocare Goal-directedmedicalplanofcareCarecoordina&onFamilysupports
AACPDMIC27;Cincinna&2018
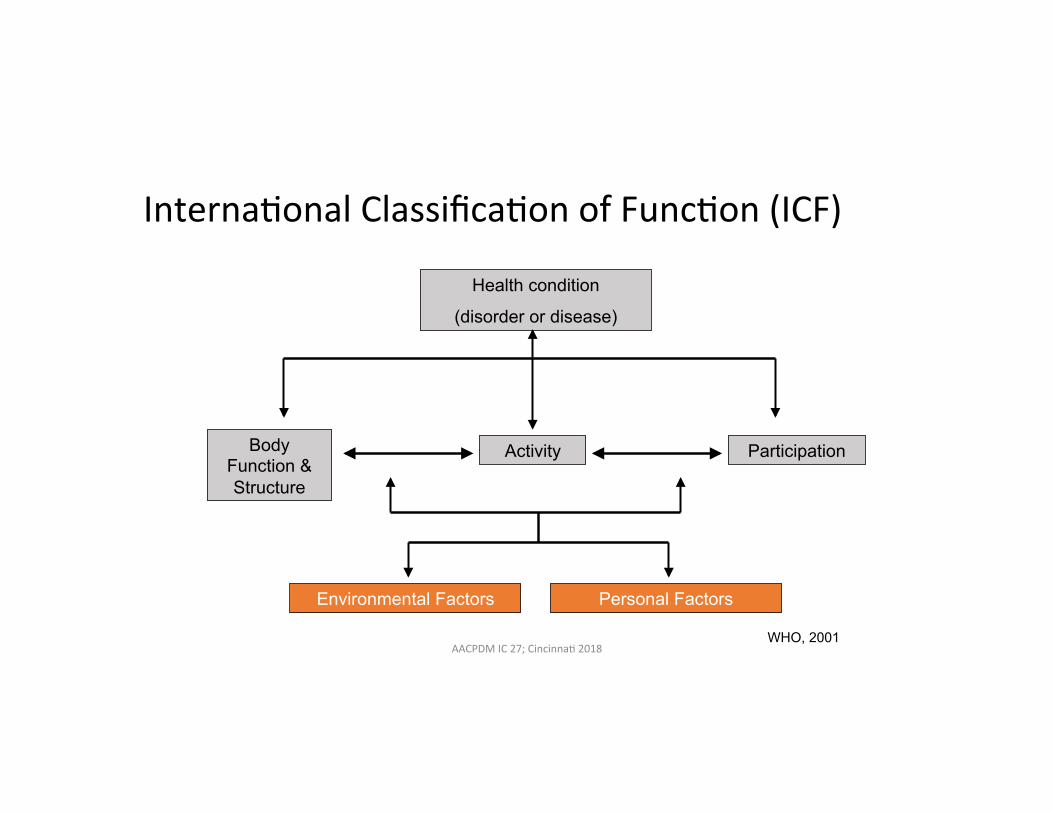
WHO, 2001
Interna&onalClassifica&onofFunc&on(ICF)
Body Function & Structure
Health condition
(disorder or disease)
Activity Participation
Environmental Factors Personal Factors
AACPDMIC27;Cincinna&2018

ChildrenwithMedicalComplexity(CMC)
• CMCareasubsetofthe18%ofallUSchildrenwhohavespecialhealthcareneeds
• CMChavethehighestdegreeofmedicalfragilityandmostintensivehealthcareneeds
• Onenwithtechnology-dependenciesandhighpsychosocialcomplexity
• Lessthan1%ofallUSchildren
AACPDMIC27;Cincinna&2018

ExamplesofCMC
• Perinatalcondi&onsandprematurity• Congenitalanomaliesandchromosomaldisorders• Chroniclungdisease• Neurologicimpairments• Technologydependencies• Progressiveneuromusculardisorders• Metaboliccondi&ons• Childrenwhohistoricallywouldnothavesurvivedwiththeircondi&ons
AACPDMIC27;Cincinna&2018

Lessthan1%ofallUSchildren…
• Accountfor1/3ofallpediatrichealthcarecosts• 5%ofCMCaccountfor50%ofthetotalspend• Accountfor42%ofallUSpediatrichospitaliza&ons,and71%ofthe30-dayunplannedhospitalreadmissions
• Childrenwithneurologicimpairmentsaccountfornearly30%ofhospitalchargeswithinchildren’shospitals
• Howcanprovidersnavigatethegraywiththesechildrenandfamilies?
AACPDMIC27;Cincinna&2018

AACPDMIC27;Cincinna&2018

ToolsforNaviga&ngtheGray
1. Useevidence-basedprac&cetoguideclinicaldecisionmaking.2. Whenevidenceislacking,applythe4principlesofmedicalethicsin
discussionsanddecisionsofgoal-directedcare.3. Takeafunc&onalapproachtocare,alwayswithclearlystatedgoals.4. Promotehealthcarevaluebypartneringwithpa&ents,parentsand
providerstoensurethebestoutcomesatthelowestmostappropriatecost.
AACPDMIC27;Cincinna&2018


Case:FeedingSafetyinaCMC
KathleenHuth,MD,FRCPC,MMSCPhysician,ComplexCareService
InstructorinPediatricsBostonChildren'sHospitalandHarvardMedicalSchool
AACPDMIC27;Cincinna&2018

Case: Feeding safety in a CMC
• 2andahalfyearoldgirlwithspas&cquadriplegia,GMFCSIII• Chroniclungdiseaseofprematurity,inhaledbudesonidedaily• Twohospitaliza&onsforpneumoniainthepastyear• Sialorrheamanagedwithglycopyrrolate• Weightz-score-2.5• Meal&mesareprolongedandasourceofstressforthefamily.• Parentsdescribeoccasionaldribblingoffoodfromherlips.• Lotsofanxietyaroundthepossibilityofrequiringenteralgastrostomytubefeeds.
AACPDMIC27;Cincinna&2018

How would you evaluate feeding safety in this child? A. Clinicalfeedingevalua&onB. VideofluoroscopicswallowingstudyC. Fiberop&cendoscopicexamina&onofswallowingD. Noneoftheabove
AACPDMIC27;Cincinna&2018

What is the evidence? Whereisitmissingorconflic&ng?
h`p://guides.mclibrary.duke.edu/c.php?g=158201&p=1036021.AccessedAugust19,2018.AACPDMIC27;Cincinna&2018

Clinical feeding evalua8on
• DiagnosCcaccuracyoftheclinicalfeedingevaluaConindetecCngaspiraConinchildren:asystemaCcreview.
• Calvoetal.,DevMedChildNeurol2016
• Sixstudiesexaminingthediagnos&caccuracyofCFEusingVFSSand/orFEESasagoldstandard
• Methodswerevariedandconsideredlowquality• CFEstriallingliquidconsistenciesmightprovidebe`eraccuracyes&matesthanCFEstriallingsolidsexclusively
• “cri&callackofevidence”ontheaccuracyofCFEindetec&ngoropharyngealaspira&on
AACPDMIC27;Cincinna&2018

Videofluoroscopic swallow study (VFSS) Advantages Disadvantages
Visualizeoral,pharyngealandupperesophagealphasesofswallowing
Contrastmedium—issuestolera&ngit,whetherthereisconcordancewithtypicallyconsumedliquids
Assessanatomyandphysiology Radia&onexposure
Canseetheeffectoftherapeu&cmaneuvers
Ques&onablegeneralizabilityofjudgmentsbasedononeperiodof&me
Arvedsonetal.Instrumentalassessmentofpediatricdysphagia.SeminSpeechLang2017
AACPDMIC27;Cincinna&2018

VFSS
• InfantvideofluoroscopicswallowstudytesCng,swallowingintervenCons,andfutureacuterespiratoryillness
• Coonetal.,HospPediatr2016
• 576infantsweretestedwithaVFSSintheirfirstyearoflife,receivingatotalof1051VFSSsintheirfirst3yearsoflife.
• Morethan60%ofinfantsreceivedafeedinginterven&on.• thickeningfeeds,NG/NJfeeds,gastrictubeplacement,fundoplica&on
• Primaryoutcome:EDvisitorhospitaladmissionforacuterespiratoryillness(ARI),occurringbetweenthefirstVFSSandthirdbirthday.
• Thickening/nasaltubefeedings,comparedwithnointerven&on,werenotassociatedwithadecreasedriskofsubsequentARI.
• Exceptforinfantswithsilentaspira&onwhoreceivedthickenedfeedings
AACPDMIC27;Cincinna&2018

Fiberop8c endoscopic evalua8on of swallowing (FEES)
Advantages Disadvantages
Noradia&on Cannotassessoralphaseofswallowing
Canbedoneatthebedside Maynottoleratecamerainser&on
Canassesssecre&onmanagement LessavailablethanVFSS
Evaluateconcernsrelatedtoupperairwayobstruc&onorvocalcordparesis.
Ques&onablegeneralizabilityofjudgmentsbasedononeperiodof&me
ArvedsonJC.Feedingchildrenwithcerebralpalsyandswallowingdifficul&es.EurJClinNutr.2013AACPDMIC27;Cincinna&2018

Arvedsonetal.Instrumentalassessmentofpediatricdysphagia.SeminSpeechLang2017AACPDMIC27;Cincinna&2018

Challenges with VFSS and FEES interpreta8on
Pisegnaetal.Parametersofinstrumentalswallowingevalua&ons:Describingadiagnos&cdilemma.Dysphagia2016AACPDMIC27;Cincinna&2018

Case con8nued: Feeding safety in a CMC
• Theyfamilymetwithadie&cianandhavebeensupplemen&ngcalorieswithanutri&onaldrink,thoughsheisnotconsistentlyachievinggoalintake.
• Atherfollow-upappointment,parentsnoteshesome&mesbecomescongestedandhas“gurgly”breathinganerdrinking.Youwitnessthisinyourclinic.
• Shehasgainedanaverageof4g/dayoverthepastmonth.• Shehasnormalvitalsignsandiswell-hydratedonexam.• Parentsreiteratetheirhopesthattubefeedscanbeavoided.
AACPDMIC27;Cincinna&2018

How would you provide nutri8onal support to this child? A. ArrangeregularfeedingtherapyB. RecommendthickeningherfeedsC. Nasogastrictubefeedsandini&ateevalua&onforgastrostomytube
AACPDMIC27;Cincinna&2018

What is the evidence? Whereisitmissingorconflic&ng?
h`p://guides.mclibrary.duke.edu/c.php?g=158201&p=1036021.AccessedAugust19,2018.AACPDMIC27;Cincinna&2018

Feeding interven8ons • FeedingintervenConsforchildrenwithcerebralpalsy:areviewoftheevidence
• Snideretal.,PhysOccupTherPediatr2011.
• Feedinginterven&onsincluded:oralsensorimotorfacilita&on,foodconsistency,posi&oning,oralappliances,andadap&veequipment.
• 21studieswereincludedinthefinalanalysis,• Outcomesmainlyfeedingsafetyandefficiency.1studyshowedheightandweightincrease.
• Sensorimotorinterven&onsprovidedregularlyoverweekstomonthsaswellasposi&oningtechniquesmayimproveoral-motorskills.
• Adjus&ngfoodconsistencymayalsohelpimprovefeedingperformance.• “currentlevelofevidenceispoor”,smallsamplesizes,limiteddatapar&cularlyformul&modalapproachesorlongtermoutcomes.
AACPDMIC27;Cincinna&2018
Oromotor therapy
• IntervenConsfororopharyngealdysphagiainchildrenwithneurologicalimpairment
• Morganetal.,CochraneDatabaseSystRev2012.
• Primaryoutcomes,whichwerephysiologicalfunc&onsoftheoropharyngealmechanismforswallowing,respiratoryinfec&onsanddietconsistency.
• 3studiesmetinclusioncriteria;evalua&ngoralsensorimotorinterven&onsandlipstrengtheningexercises
• Studiesaffectedbya`ri&on,detec&onbias,smallsamplesizes• “insufficienthigh-qualityevidence…toprovideconclusiveresultsabouttheeffec&venessofanypar&culartypeoforal-motortherapy.”
AACPDMIC27;Cincinna&2018

Thickened feeds
• Thickenedliquidsasatreatmentforchildrenwithdysphagiaandassociatedadverseeffects:asystemaCcreview
• Gosaetal.,InfantChildAdolesc2011
• 6studiesexaminedtheeffectsofthickenedliquidsonswallowingorpulmonaryoutcomesandreportedmixedfindings.
• 16studiesexaminedadverseeffects—amongpediatricpa&entswithGER,therewasnosignificantincreaseintherateofadverseeffectsfromtheuseofthickenedliquids.
• “insufficientevidencebaseforthispopulartreatmentop&on”
AACPDMIC27;Cincinna&2018

Tube feeding
• Gastrostomyfeedingincerebralpalsy:AsystemaCcreview.• SleighandBrocklehurst,ArchDisChild2004.
• Twocohortstudies,15caseseries,andeightcasereportsmetinclusioncriteria.• Weightgainresultedfromgastrostomyfeedinginmostcases.• Complica&onsreportedincludedincreasedGERandaspira&on.
• Gastrostomyfeedingversusoralfeedingaloneforchildrenwithcerebralpalsy.• Gantasalaetal.,CochraneDatabaseSystRev2013.
• NoRCTsiden&fied.• “considerableuncertaintyabouttheeffectsofgastrostomyforchildrenwithcerebralpalsyremains"
AACPDMIC27;Cincinna&2018

Gastrostomy tube: Exploring impact
• Commonconcerns• Missingmeal&mesocializa&onexperiences• Restrictedmobility/inabilitytoleavehome• Gtubesiteissues• Aytudesofothers• Sleepdisrup&on• “unnatural”
• Impactofgastrostomytubefeedingonthequalityoflifeofcarersofchildrenwithcerebralpalsy.
• Sullivanetal.,DevMedChildNeurol2004
• 12monthsanergastrostomy,significantimprovementsinsocialfunc&oning,mentalhealth,energy/vitality,andgeneralhealthpercep&onwerereported.
• Significantreduc&oninfeeding&mesandreducedconcernabouttheirchild'snutri&onalstatus.
AACPDMIC27;Cincinna&2018

4PrinciplesofMedicalEthics
AutonomyPa&ent/familyvaluesanddecision-makingaroundfeedingtheirchildanerbeinginformedoftherisks/benefits.
BeneficenceProvidingnutri&onalsupportinawaythatisposi&ve,func&onalforthefamily,andreducesstress.
Non-maleficencePreven&ng/mi&ga&ngriskofaspira&on
JusCceSelec&nginves&ga&onsbasedondiagnos&cyieldandtriallinginterven&onswithclearlyestablishedgoals
AACPDMIC27;Cincinna&2018
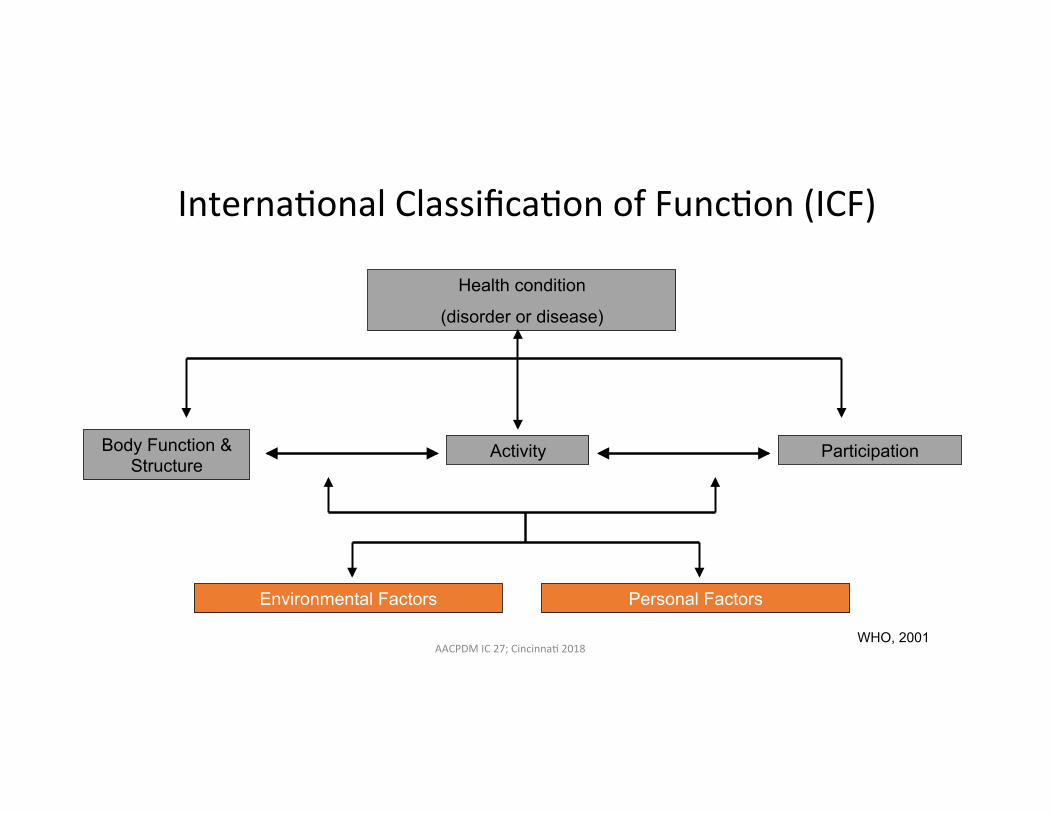
WHO, 2001
Interna&onalClassifica&onofFunc&on(ICF)
Body Function & Structure
Health condition
(disorder or disease)
Activity Participation
Environmental Factors Personal Factors
AACPDMIC27;Cincinna&2018
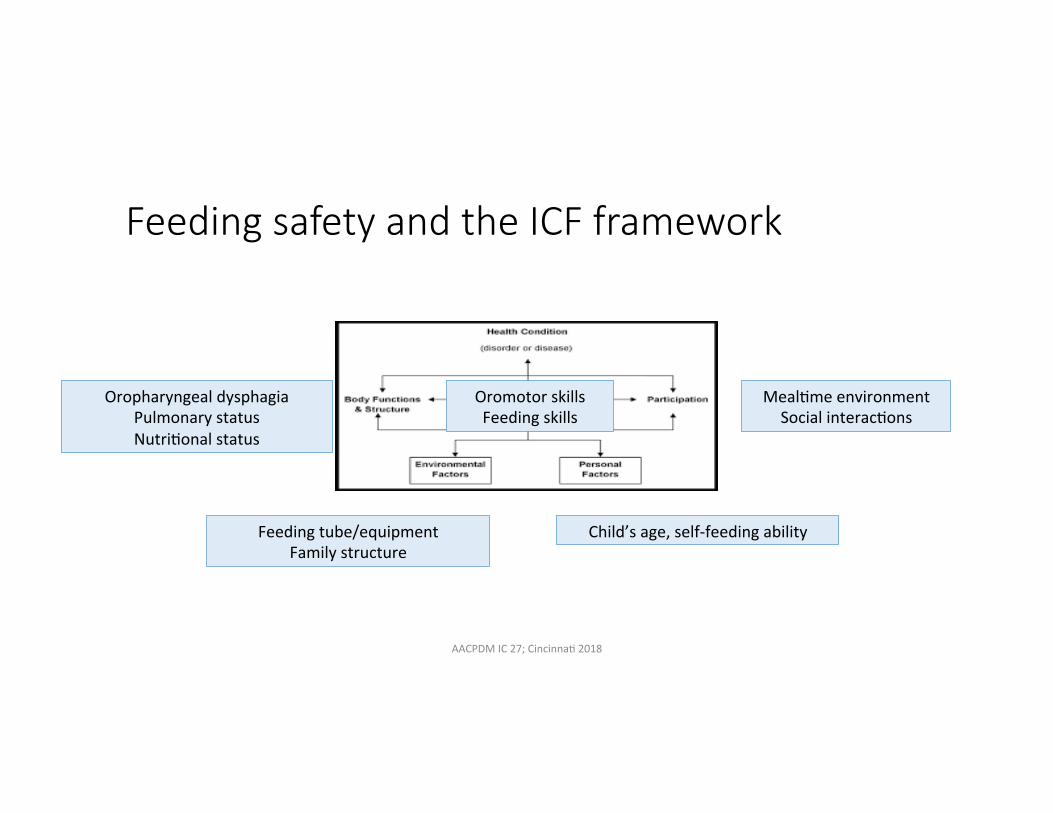
Feeding safety and the ICF framework
OropharyngealdysphagiaPulmonarystatusNutri&onalstatus
Feedingtube/equipmentFamilystructure
Meal&meenvironmentSocialinterac&ons
Child’sage,self-feedingability
OromotorskillsFeedingskills
AACPDMIC27;Cincinna&2018

A func8onal approach to feeding safety
• Interdisciplinaryteamapproachconsideringmul&plefactors• Pulmonarystatus,GIissues,Oralsensorimotorskills,Behaviouralissues,Familyinterac&ons
• Not”allornothing”• Oralskillsandaspira&onriskchangesdependingoncontextandover&me.Considerimpactoffa&gue,URTI,seizuredisorder,GERD,medica&onsthataffectsecre&ons,dentalhygiene,posture/tonemanagement
• Goalisn’tnecessarilytotaloralfeeding.Iden&fywhatfeedingispossible,withappropriateparametersandsupports
• Discusstheevidenceandlimita&onsofproposedevalua&onsandtreatment• Priori&zepulmonaryhealthandop&mizingnutri&onandhydra&onstatuswhileensuringalignmentwithfamilygoals.
ArvedsonJC.Feedingchildrenwithcerebralpalsyandswallowingdifficul&es.EurJClinNutr.2013AACPDMIC27;Cincinna&2018

Andrewetal.Feedingdifficul&esinchildrenwithcerebralpalsy.ArchDisChildEduc2012.AACPDMIC27;Cincinna&2018


Naviga&ngtheGray:CaseExampleChronicPain
AACPDMIC27;Cincinna&2018
EmilyJGoodwin,MD,FAAPClinicalAssistantProfessorChildren’sMercyHospital
UniversityofMissouriKansasCitySchoolofMedicine

Case: Chronic Pain • 12yofemalewithGMFCSVCerebralPalsy• SheisdependentonG-tubefornutri&on,hasosteopenia,cor&calvisualimpairment,scoliosiss/pspinalfusion,andspas&citymanagedbybaclofenpump.
• Shehasbeenhavingunexplainedepisodesofchronicpainnearlydailyforthepastfewmonths.
• Painbehaviors:inabilitytobeconsoled,tachycardia,moaning,restless,archesback.Occursmostevenings.
• Pa&entisnon-verbalandunabletousecommunica&ondevice.Nolongersiyngcomfortablyinherwheelchairandimpac&ngschoolandac&vi&esofdailyliving.Nooneissleeping.
• Examisunrevealing.X-rayimagingshowsbilateralcoxavalga,migra&onpercentage40%bilaterally,allspinalfusionhardwareintact,nofractures,mildtomoderatestool.
AACPDMIC27;Cincinna&2018

How would you approach treatment op8ons in addi8on to non-pharmacologic measures? A. FurtherDiagnos&cevalua&ons(x-rays,endoscopy,pHstudies,
assessbaclofenpump)B. Stepwiseempiricmedica&ontrials(H2antagonist,PPI,cons&pa&on
treatment,analgesics,gabapen&noids,opioids,adjustbaclofenpump,tricyclican&depressants,alphaagonists)
C. Offerproceduralinterven&ons(botulinumtoxin,phenol,surgicalop&onsforhipsubluxa&on)
D. Noneoftheabove
AACPDMIC27;Cincinna&2018

What is the evidence? Whereisitmissingorconflic&ng?
AACPDMIC27;Cincinna&2018

Case: Chronic Pain sources
Children(Basel).2018Jan;5(1):13.Publishedonline2018Jan18.doi:10.3390/children5010013AACPDMIC27;Cincinna&2018

Case: Chronic Pain • Iden&fica&onofsourceandtargetedtreatmentidealbutnotalwayspossible
• Nostandardapproach
• Empirictrialsnotwithoutadverseeffects • Pa&entandfamilyimpact/&me• Medica&onsideeffects
AACPDMIC27;Cincinna&2018
Hauer&Houtrow.PainAssessmentandTreatmentinChildrenwithSignificantImpairmentintheCentralNervousSystemPediatrics2017,139(6)
Oravaetal(2014).Chronicpainassessmenttoolboxforchildrenwithdisabili&es:Sec&on1.0:Toolboxbackground.Toronto,Ontario:HollandBloorviewKidsRehabilita&onHospital.Retrievedfrom:h`p://hollandbloorview.ca/toolbox
KingsnorthetalChronicPainAssessmentToolsforCerebralPalsy:ASystema&cReview.PediatricsOct2015,136(4)e947-e960;DOI:10.1542/peds.2015-0273

Suggested guidelines for pharmacologic management of recurrent pain behavior episodes.45,93–95,105–107.
Julie Hauer et al. Pediatrics 2017;139:e20171002
©2017 by American Academy of Pediatrics AACPDMIC27;Cincinna&2018

Case: Chronic Pain
• SurgicalInterven&ons• Nopreferredprocedurefornon-ambulatorypa&entswithpainfulchronicsubluxatedordislocatedhips(arthodesisnotrecommended,FHR,VO,THAareop&ons).Painreliefbetween88-93%,complica&onsbetween24-35%
AACPDMIC27;Cincinna&2018
KolmanSE,RuzbarskyJJ,SpiegelDA,BaldwinKD.SalvageOp&onsintheCerebralPalsyHip:ASystema&cReview.JPediatrOrthop.2016Sep;36(6):645-50

Case: Chronic Pain
• Limitedevidenceforuseofmanymedica&onsinchildrenfromchronicpain.NoRCTs
• Gabapen&noids(Gabapen&n,Pregabalin)• HauerJM1,SolodiukJC.Gabapen&nformanagementofrecurrentpainin22nonverbalchildrenwithsevereneurologicalimpairment:aretrospec&veanalysis.JPalliatMed.2015May;18(5):453-6.doi:10.1089/jpm.2014.0359.Epub2015Feb6.
• N=22,21(91%)hadsignificantdecreaseinsymptoms/painbehaviors• CooperetalAn&epilep&cdrugsforchronicnon-cancerpaininchildrenandadolescents.Cochranereview2017
• noevidencetosupportorrefutetheuseofan&epilep&cdrugstotreatchronicnon-cancerpaininchildrenandadolescents.
AACPDMIC27;Cincinna&2018

Evidencebasedprac&ce
h`p://guides.mclibrary.duke.edu/c.php?g=158201&p=1036021.AccessedAugust19,2018.
Hipsurgeryrecommendedbutunclearifthisis
THEsourceofpainbehaviors
Familywishestoavoidsurgery
Somemedica&onsfoundtobehelpful
AACPDMIC27;Cincinna&2018

ChronicPaintreatmentandMedicalEthicsAutonomyFamilyhopestoavoidanesthesiaandsurgery,valuesdecisionmakinganerbeinginformedofbenefitsandrisks
BeneficenceCana`empttotreatpainmedicallywithoutknowingsource
Non-maleficenceLimitedevidence(RCTs)forsomemedica&ons,mayhaveadverseeffects.Unknownifhipsaresourceofpainbehaviors,manysurgicalandanesthesiarisks
JusCceManytreatmentop&ons,cantrialsomesystema&callywithcleargoals(pa&entcomfort,par&cipa&on)
AACPDMIC27;Cincinna&2018

Afunc&onalapproachtocare Goal-directedmedicalplanofcareCarecoordina&onFamilysupports
AACPDMIC27;Cincinna&2018

Interna&onalClassifica&onofFunc&on(ICF)
Spasticity and Pain behaviores,
40% MP hips, near skeletal
maturity
Chronic Pain
Relies on wheelchair
Pain limits participation in
school and therapy
Wheelchair not fitting comfortably
Non-verbal, enjoys school and family time
AACPDMIC27;Cincinna&2018ICFWHOFramework

Case: Chronic Pain
• Mul&disciplinaryCareconferenceisheld• Unclearifhipsaresourceofpain• risksandbenefitsofsurgeryandproceduralinterven&onsandmedica&onsarediscussed
• Botulinumtoxintrialedwithoutimprovement• Gabapen&noidstrialedwithoutimprovement• Ul&matelytransi&onedtohomeboundschoolingwithcommunityac&vi&esini&atedtominimizepainwithtransfers
• Alpha2agonisttrialedandprovidesbenefitAACPDMIC27;Cincinna&2018


GrayscaleDecisionMakingInterac&veDiscussion
AACPDMIC27;Cincinna&2018
AutonomicDysfunc&onSpas&city&Dystonia ProgressiveNeuromuscularScoliosis

WhatistheEvidence?ApplyEthicalPrinciplesFunc&onalApproach
Interac&veDiscussion
AACPDMIC27;Cincinna&2018
AutonomicDysfunc&onSpas&city&Dystonia ProgressiveNeuromuscularScoliosis

Evidencebasedprac&ce
h`p://guides.mclibrary.duke.edu/c.php?g=158201&p=1036021.AccessedAugust19,2018.AACPDMIC27;Cincinna&2018
What’syourtreatmentplan?
Whatfactorsinfluenceyourdecisions?
AACPDMIC27;Cincinna&2018

Acknowledgements
SpecialthankstomembersoftheAACPDMComplexCareEduca&onsubcommi`eeontheComplexCareCommi`eefortheircontribu&ons
andassistancewiththispresenta&on
AACPDMIC27;Cincinna&2018

Thankyou.
AACPDMIC27;Cincinna&2018







