
National Communication Framework and Plan forInfant and Young Child Feeding in
Bangladesh
Institute of Public Health Nutrition (IPHN)Directorate General of Health ServicesMinistry of Health and Family Welfare

National Communication Framework and Plan forInfant and Young Child Feeding in
Bangladesh

Message
MinisterMinistry of Health and Family WelfareGovernment of the People’s Republic of Bangladesh
I am delighted to see the Institute of Public Health Nutrition (IPHN), onbehalf of the Ministry of Health and Family Welfare, has developed theNational Communication Framework and Plan on Infant and Young ChildFeeding (IYCF). This is a key step toward a comprehensive programimplementation. I do believe the IYCF communication plan will guide usfor detailing communication activities, their implementation andmonitoring.
The health and nutritional well being of a population is both an outcomeand indicator of national development. About one fifth of all under fivechild death is preventable through optimal IYCF alone. IYCF not onlyprevents child mortality and morbidity but can help a lot in realizing othermillennium development goals. I am pleased to note that the 55th WorldHealth Assembly adopted the Global Strategy on infant and young childfeeding. Accordingly the Ministry of Health and Family Welfare ofBangladesh already published the national strategy on IYCF.
IYCF should be a multi-sectoral program and I would like to call upon mycolleagues in different ministries, professional bodies, NGOs, anddevelopment partners to invest their full capacity to implement thecommunication activities. Doctors, nurses, nutritionists and other staff inhealth, population and nutrition sector should play the key role in IYCF.
ii

I appreciate the contribution of the stakeholders of the variousorganization for preparing the communication framework and plan andUNICEF Alive and Thrive for its technical and financial support. DirectorIPHN and her colleagues deserve special mention for hard work forpreparing the communication plan.
Joy Bangla, Joy Bangabandhu
Long Live Bangladesh
Prof. Dr. A.F.M. Ruhal Haque, MP
iii
Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
Message
Advisor toThe Hon’ble Prime Minister of the People’s Republic of BangladeshMinistries of Health and Family Welfare and Social Welfare
Appropriate Infant and Young Child Feeding (IYCF) is essential to realizesurvival and development of children. We appreciate that promotion ofIYCF is an affordable and sustainable child survival and developmentintervention. It is encouraging that a national communication frameworkand plan has been prepared in accordance with the directives of nationalIYCF strategy to ensure coordinated implementation.
The consequences of inappropriate feeding practices in early childhoodare major obstacles to our efforts towards sustainable socio-economicdevelopment and poverty reduction. In addition, the MillenniumDevelopment Goals (MDGs) will not be achieved without action toreduce the rate of malnutrition in infants and young children. Appropriatefeeding contributes directly to achievement of MDG 1 (eradicate extremepoverty and hunger) and MDG 4 (reduce child mortality).
I have full confidence that if the comprehensive actions identified inNational Communication Plan and fully implemented, children inBangladesh will be better protected from the scourge of malnutrition.
I congratulate the members of the technical group for preparing thecommunication plan and I believe that its implementation will bring forthchanges in the arena of child feeding practice that will lead to betternourishment of our children.
Prof. Dr. Syed Modasser Ali
iv

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
Message
State MinisterMinistry of Health and Family WelfareGovernment of the People’s Republic of Bangladesh
Inappropriate Infant and Young Child Feeding (IYCF) practices areamong the most serious obstacles to maintaining adequate nutritionalstatus, and contribute to under nutrition in children. In Bangladeshalmost one half of children under five years are victims of under-nutrition.IYCF not only prevents child mortality and morbidity but can help a lot inrealizing their millenium development goals. Malnourished children whosurvive are more frequently sick and suffer the lifelong consequences ofimpaired physical and intellectual development.
One of the most important goals of the Health, Nutrition and PopulationSector Programme is to improve the nutritional status of children andwomen. There is evidence that the feeding practices of infants andyoung children, particularly breastfeeding and complementary feeding,are not optimal in Bangladesh and are contributing to the high levels ofmalnutrition.
I hope that implementation of the national communication plan on IYCFwill make significant changes in the field of child feeding leading tohealthy generation.
Joy Bangla, Joy Bangabandhu
Dr. Capt. (Rtd.) Mozibur Rahman Fakir, MP
v

vi
Message
SecretaryMinistry of Health and Family WelfareGovernment of the People’s Republic of Bangladesh
The correction of inappropriate child feeding practices can preventmalnutrition and its consequences, including developmental delays,impaired educational ability, a lifetime of poor health, increased risk ofchronic disease and early death.
Behaviour change will focus on the actions that need to be taken by amother, her family, her employer, community and many others in supportof breastfeeding and complementary feeding practices that will bestserve the nutritional needs of infants and young children. Due attentionmust be given to interpersonal communication, particularly behaviourchange counselling, to effectively changing Infant and Young ChildFeeding (IYCF) practices.
The national communication framework and plan on IYCF describesessential interventions to protect, promote and support appropriate infantand child feeding. Guided by this document, the government willcoordinate all actions to improve infant and young child feeding practicesin Bangladesh.
Md. Humayun Kabir

Message
Director GeneralDirectorate General of Health ServicesMinistry of Health and Family WelfareGovernment of the People’s Republic of Bangladesh
I am pleased to know that a National Communication Framework andPlan for Infant and Young Child Feeding has been prepared inconcurrence with the National Plan of Action and National Strategy forInfant and Young Child Feeding to improve feeding practices.
We need to improve Infant and Young Child Feeding (IYCF) in childrenless than 2 years of age in order to increase exclusive breastfeeding tosix months and reduce under-nutrition (stunting, wasting, under-weightand anemia). This would support achievement of MDG 1 (to reducepoverty and child under-nutrition) and MDG 4 (to reduce neonatal andunder-five mortality). Since child under-nutrion results from acombination of inadequate nutritional intake and infections, and sincecomplementary feedings are a major source of pathogens leading todiarrhoea, handwashing before feeding young children is an importantbehaviour promoted as part of IYCF.
Infant and young child feeding requires both advocacy and behaviourchange. Advocacy is needed to keep infant and young child feeding highon the public health agenda and obtain proactive support for infant andyoung child feeding among leaders at all levels, including local elites,religious leaders, government officials and political leaders.
vii

Behaviour change will focus on the actions that need to be taken by amother, her family, her employer, community and many others in supportof breastfeeding and complementary feeding practices that will bestserve the nutritional needs of infants and young children. Due attentionmust be given to interpersonal communication, particularly behaviourchange counseling, to effectively changing Infant and Young ChildFeeding (IYCF) practices.
I appreciate IPHN, development partners including UNICEF and Aliveand Thrive, and other stakeholders in preparing the framework and plan.The challenge before us now is implementation of the plan and I callupon all stakeholders and partners for their continued support in thisrespect. Guided by this document, the Government will co-ordinate allcommunication actions to improve infant and young child feeding inBangladesh.
Prof. Dr. Shah Monir Hossain
viii

Acknowledgement
The role of breastfeeding and appropriate complementary feeding in thegood physical and mental health and development of children goeswithout saying. During early stage of childhood, vitamin and mineraldeficiencies caused by malnutrition impair the immune system and inhibitthe cognitive and physical development. Bangladesh has made someprogress in overcoming these deficiencies but much remains to be done.The Government of Bangladesh has taken several important steps toaddress IYCF problems. As part of the effort to tackle infant and youngchild nutrition in Bangladesh, the National Strategy for Infant and YoungChild Feeding has been developed and are being implemented throughan approved action plan. The overall goal of the National IYCF Strategyis to improve nutritional status, growth and development, health, andsurvival of infants and young children in Bangladesh through optimalIYCF practices.
The National IYCF strategy aims to create an environment to improveIYCF practices by addressing barriers regarding knowledge andpractices on infant and young child feeding. With that aim acommunication framework and plan has been developed to bringsustainable changes in generating the demand for infant and young childfeeding services and setting the stage where individual behaviourchange is supported by community members, basic health and socialservices and effective policies in several sectors.
The communication plan has been developed through a participatoryprocess involving different stakeholders, and a synthesis of past and newformative research, national and district level information and twoworkshops organized by IPHN. The communication plan outlines the role
ix

of communication for accelerating action to improve IYCF practices thatare proven to play major role in enhancing the health, nutrition, anddevelopment of infants and young children.
Success of the implementation of the communication will depend greatlyon the valuable support of the stakeholders who have helped us to comethis far.
Prof. Dr. Fatima Parveen ChowdhuryDirector, IPHN and Line Director MicronutrientsMinistry of Health and Family Welfare
x

CONTENTS
Acronymes xii
I. Background 1
II. Rationale for the Communication Framework and Plan 3
III. Communication Approaches 4
IV. Communication Objectives 4
V. Barriers and Facilitators 7
VI. Participant Groups for Communication 10
VII. Communication Channels and Media 13
VIII. Key Messages 14
IX. Implementation Plan 21
X. Monitoring and Evaluation Indicators for IYCF Communication 31
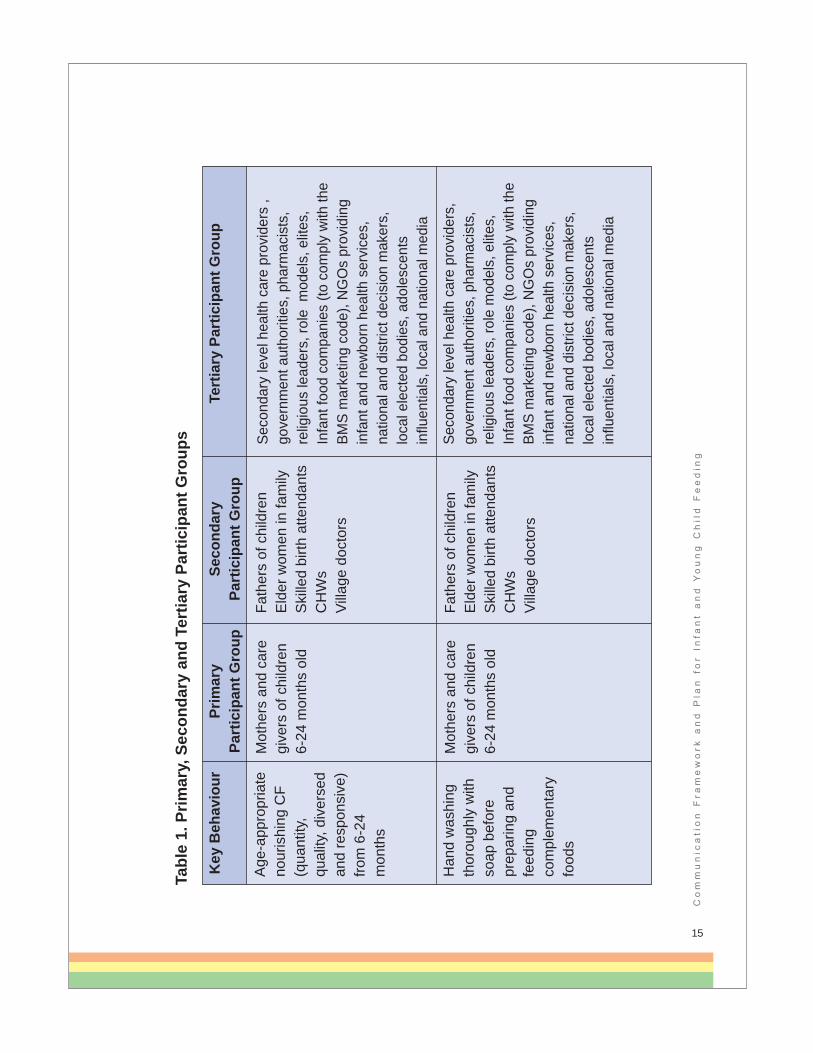
Table 1. Primary, Secondary and Tertiary Participant Groups 11
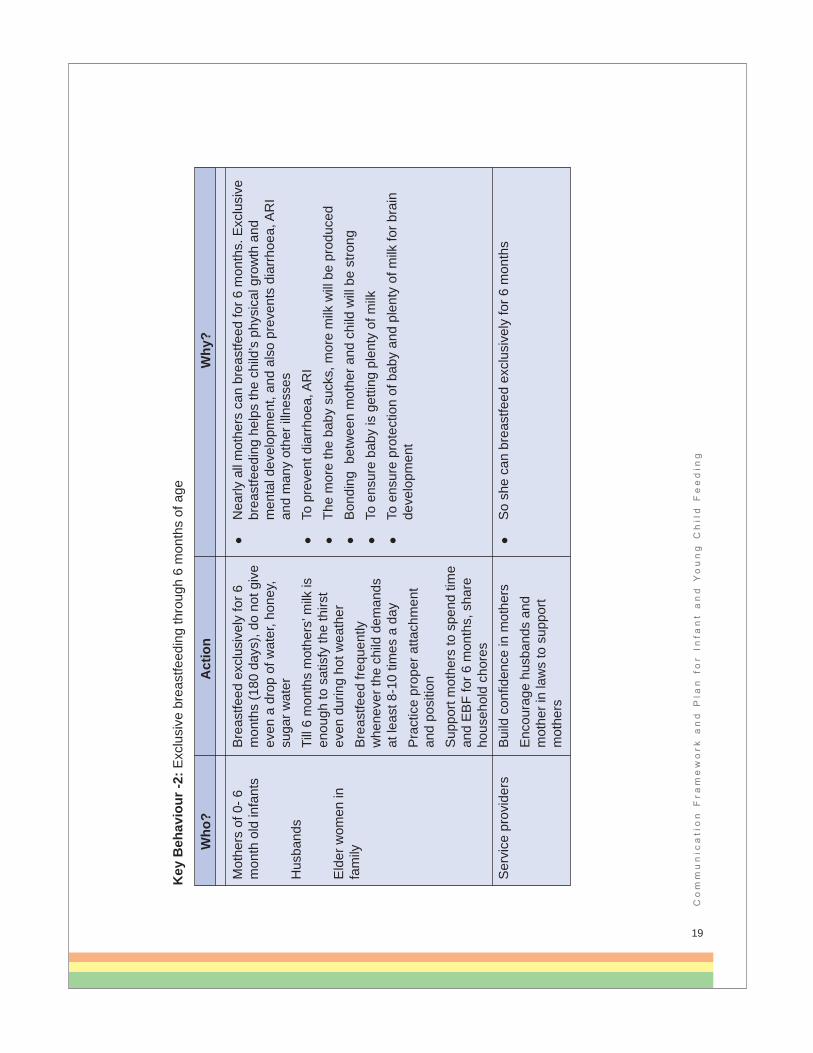
Table 2. Key Messages for Four IYCF Behaviours 15
Table 3. Stakeholders for National IYCF Communication Frameworkand Plan 22
Table 4. Action Plan for Implementation of Communication Activities 24
Table 5. Monitoring and Evaluation Indicators for IYCFCommunication Activities 32
xi

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
AcronymsANC Antenatal CareARI Acute Respiratory InfectionsBCC Behaviour Change CommunicationBBF Bangladesh Breastfeeding Foundation BDHS Bangladesh Demographic and Health SurveyBGMEA Bangladesh Garment Manufacturers and Exporters
Association BKMEA Bangladesh Knitwear Manufacturers and Exporters
AssociationBNFE Bureau of Non-Formal Education BNNC Bangladesh National Nutrition CouncilBTMA Bangladesh Textile Mills AssociationBPA Bangladesh Pediatric AssociationCF Complementary FeedingCHV Community Health VolunteerCHW Community Health WorkerCNO Community Nutrition Organiser CNP Community Nutrition PromoterCSR Corporate Social ResponsibilityDC Deputy CommissionerDDCC District Development Coordination Committee DEO District Education OfficerDGFP Directorate General of Family PlanningDGHS Directorate General of Health ServicesDPEO District Primary Education OfficerEBF Exclusive Breastfeeding EI Early InitiationENC Essential Newborn CareFWA Family Welfare Assistant
xii

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
FWV Family Welfare VisitorGOB Government of BangladeshHMIS Health Management Information SystemHW Hand WashingIMCI Integrated Management of Childhood IllnessIPHN Institute of Public Health Nutrition IYCF Infant and Young Child Feeding MNH Maternal and Neonatal Health MNCH Maternal, Neonatal and Child Health MNCS Maternal, Neonatal and Child Survival MOA Ministry of AgricultureMORA Ministry of Religious AffairsMOHFW Ministry of Health and Family WelfareMOI Ministry of Information MOLGRD Ministry of Local Government and Rural DevelopmentMOPME Ministry of Primary and Mass Education MOWCA Ministry of Women and Children AffairsMOSW Ministry of Social WelfareNCTB National Curriculum and Textbook BoardOGSB Obstetric & Gynaecological Society of BangladeshPNC Post Natal CareSACMO Sub-Assistant Community Medical OfficerSBA Skilled Birth AttendantTBA Traditional Birth AttendantWHO World Health Organization
xiii

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
x

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
Communication Framework and Planfor IYCF The Communication Framework and Plan is a component of the NationalIYCF Strategy and its goal is to contribute to the reduction of under-nutrition and death caused by sub-optimal infant and young child feedingpractices. In Bangladesh, as in many other countries, socialcommunication plays a significant role in achieving programmeobjectives. This communication framework and plan outlines the role ofcommunication in demand creation for basic services and in theadoption of key life-saving behaviours and bringing about social normschange related to IYCF. The plan sets out actions for reaching mothersand families through interpersonal and mass media channels andcreating an enabling environment for them to adopt healthy behavioursthrough social actions and supportive policies. This plan has beenprepared for 2010-2013 and will be reviewed and extended up to 2016to fit the national Health, Population and Nutrition Sector Strategy Planfor the period of 2011-2016.
In order to implement systematic multi-channel communication activities,a national communication framework and plan has been developedthrough a participatory process which involved different stakeholders.Main objective of the communication framework and plan is to createdemand for early initiation of breastfeeding, exclusive breastfeeding andquality complementary feeding for infant and young children. Thecontents of this document are based on a synthesis of past and newformative research, national and district level information and data, andtwo workshops organized by IPHN in March and April 2010 that wereattended by over 50 persons from 25 organizations.
Communication interventions are meant to be dynamic and take intoaccount the lessons learned from the field and the evolving socio-economic and programme contexts. It is a continued process. Thereforethis communication framework and plan will be adjusted to reflect what islearned during the testing and implementation phases.
1

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
I. Background Epidemiological evidence indicates that the following IYCF practices willhave substantial impacts on health and nutrition indicators in Bangladesh(Lancet 2008, BDHS 2007, WHO/PAHO 2003, and National IYCFStrategy 2007):
Initiation of breastfeeding immediately (within one hour) after birthand no pre/post-lacteal foods
Exclusive Breastfeeding from birth through 6 months
Timely initiation of semi-solid complementary feeding and givingrecommended amounts of solid or semi-solid foods to children from6-24 months in addition to continued breastfeeding for at least 24months
Assuring the quality of complementary foods through: adequatedensity of energy and nutrients, use of diverse types of foodsespecially animal foods, feeding fortified foods, or supplementation1
Reducing pathogens in complementary foods through handwashingwith soap before preparing and feeding children under two years.
In Bangladesh, current IYCF patterns fall short of these practicesresulting in nutritional deficits and increased infections leading to growthfailure, stunting, anaemia, cognitive damage and increased neonatal,infant and child morbidity and mortality. These five sets of behaviours aretop priorities for the national IYCF communication plan. Other WHOrecommended behaviours are already widely practiced in Bangladeshaccording to the available research and do not require special focus. Forexample, initiation of breastfeeding, continuation of breastfeeding to atleast 2 years, on demand feeding and frequency of complementaryfeeding do not present a serious problem at present.
2
1 1IPHN 2007: National Strategy for Anaemia Prevention and Control in Bangladesh: page 48

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
Past experience has shown that a lack of focus on a few prioritybehaviours and messages leads to limited achievement of programmeobjectives. The proposed communication framework and plan isselective and aims to address all the above mentioned behaviours. Inthe past, IYCF programmes addressed the barriers and motivations ofmothers and other family members inadequately. Insufficient coveragewith short duration programmes that did not use multiple channels ofcommunication further reduced the possibility of behaviour change on alarge scale. Currently Bangladesh offers an effective set ofcommunication channels and there are several options for reaching keyparticipant groups (target audiences). Recent formative researchconducted as a part of communication plan preparation has alsoidentified barriers and facilitators in the local context of Bangladesh. Thiscommunication framework and plan takes advantage of the newunderstanding of programme options and the availability of newtechnologies and communication channels.
The Government of Bangladesh (GOB) has taken several importantsteps to address IYCF problems. The overall goal of the National IYCFStrategy (2007) is to improve nutritional status, growth and development,health, and survival of infants and young children in Bangladesh throughoptimal IYCF practices. The specific objectives of the National Strategyare to:
Increase the national percentage of newborns who are breastfedwithin one hour of birth from 24% to 50%
Increase the national percentage of infants aged less than 6 monthswho are exclusively breastfed from 42% to 60%
Maintain the national percentage of children aged 20-23 months whoare still breastfed at 90%
Increase the percentage of children aged 6-9 months who arebreastfed and receive appropriate complementary foods to 50%
3

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
In addition to the National IYCF Strategy, the National Neonatal HealthStrategy (2009) is also supportive of IYCF. It states,
"All birth attendants and providers must know about the benefits ofbreastfeeding and should be trained on breastfeeding counseling andtechniques. They should promote initiation of breastfeeding immediatelyafter birth and no later than one hour, counsel for exclusivebreastfeeding for six months and encourage compliance to breastfeedingthrough advocacy and health education of family and mothers. Allfacilities should provide environment conducive for breastfeeding.Additional efforts to raise motivation and practice for immediate initiationand continuation of breastfeeding for mothers with caesarean sectionsshould be in place. Feeding should be as frequent as the babydemands, without any pre-lacteals (plain water, sugar water, honey etc.)"
National IMCI guidelines and protocols also contain sections related toassessing and counseling on breastfeeding and complementary feeding.
II Rationale for the CommunicationFramework and PlanThe national IYCF programme aims to create an environment to improveIYCF practices by addressing barriers regarding knowledge andpractices on infant and young child feeding. Thus a communicationframework and plan has been prepared to bring sustainable changes ingenerating demand for infant and young child feeding services andsetting the stage where individual behaviour change is supported bycommunity members, basic health and social services and effectivepolicies in several sectors. As stated earlier the plan will be extended toalign with the Health, Population and Nutrition Sector Strategy Plan for2011-2016.
4

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
III Communication ApproachesCommunication is a systematic, planned and evidence based strategicprocess that is intrinsically linked to programme elements. It usesconsultation and participation of children, family members, communitypeople, opinion leaders and networks; privileges local contexts, andrelies on a mix of communication tools, channels and approaches topromote positive and measurable behaviour and social change. In orderto achieve desired behavioural and social change objectives the IYCFframework and plan uses a mix of three key approaches. All theapproaches complement each other, thus implementation of theseapproaches is continuous and simultaneous.
Advocacy - helps garner political support to help shape and implementpolicies and ensure adequate allocation of resources. Advocacy ensuresthat the perspectives, concerns and voices of women and men from allsegments of the population including marginalized groups, are heard andreflected in upstream policy dialogue, decision making and interventions.
Communication for Social Change - engages, motivates andempowers communities and networks to influence or reinforce socialnorms and cultural practices to create an enabling environment thatsupports long-term sustainable social change for infant and young childfeeding practices.
Behaviour Change Communication (BCC) - uses a combination ofstrategies including social marketing and participatory communication tohelp inform, influence and support individuals, families, communitygroups and opinion leaders for the adoption and sustained practice andsupport of desired IYCF behaviours.
5

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
IV. Communication Objectives The IYCF framework and plan has been prepared for 2010-2013. Thefollowing communication objectives have been identified for advocacy,communication for social change, and behaviour change related topriority topics in IYCF.
Advocacy Objectives:
By the end of 2013,
50% of government authorities (all directors and programmemanagers from DGHS and DGFP) and development partners aresensitized about National IYCF Strategy and initiate allocation ofresources for implementing relevant sections of the action plan andgive additional support for mainstreaming IYCF into health, familyplanning, education, agriculture, food security and nutrition sectorprogrammes
DGFP and DGHS add counseling and support to mothers forappropriate IYCF in job descriptions of health providers, particularlythose who provide services on ANC, PNC, ENC, FP, immunizationsand management of childhood illnesses; and HMIS indicators forappropriate IYCF are added and reviewed regularly by relevanthealth and family planning staff
Policy makers agree that government medical and nursing collegeswill be teaching about how to provide practical support to mothers
50% of monthly District Development Coordination Committee(DDCC) review meetings cover topics related to IYCF, including theimportance of maternal and child nutrition and reporting of IYCFprogress made in various sectors in programme areas
National school curriculum for classes 6-10 include the importance ofmaternal and child nutrition and appropriate IYCF
At least 20% of business corporations; and BTMA, BGMA, BKMAmembers; the national forum for CSR; consumers associations; and
6

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
chamber of commerce members are sensitized about the impact ofchildhood nutrition and IYCF on adult labour productivity and at least40% of these are promoting appropriate IYCF among their workersand communities in which they operate
Handwashing linked to complementary feeding addressed in nationalhygiene promotion strategy and active plans
Reporters and gatekeepers from 50% of national media outlets (print,broadcast, radio and web) producing increased coverage on IYCFpractices and impact on child mortality, nutrition, health anddevelopment outcomes in order to remove barriers and increasesupport and resources for IYCF services among policy and decisionmakers.
Communication for Social Change Objectives:
By the end of 2013,
50% of trained health service providers (doctors, nurses, villagedoctors, pharmacists, CHWs) in programme areas support mothersto practice priority IYCF behaviours (EI, EBF, CF and hand washing)
At least 30% of religious leaders in programme areas coming incontact with pragnent women or their family members promotepriority IYCF practices during their regular and special prayers andceremonies
25% of communities in programme areas have more than onecommunity leader e.g. teachers, elites, union parishad members,woman leaders and others, promote emphasis behaviours of IYCFamong all family members
25% of communities in programme areas have adolescent groupsactively promoting priority IYCF practices
At least 50% of existing community groups and associations inprogramme areas support emphasis IYCF behaviours
At least 3 soap manufacturers agree to include handwashing linkedto complementary feeding messages in their advertising campaigns
7

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
Behaviour Change Objectives:
By the end of 2013,
Mothers initiated breastfeeding immediately (within one hour) of birthincreased from 43% to 65%2
At least 65% of birth attendants (SBA, TBA, family members)reached through the IYCF initiative put infant to mother's breastimmediately (within one hour) of birth
Mothers exclusively breastfeeding their infants 0-6 months of ageincreased from 43% to 60%
An additional 10% mothers and caregivers over baseline feed animalfoods to children 6-24 months of age
50% of mothers and caregivers in programme areas feed age-appropriate quantity of diversed solid or semi-solid atleast once dailyfamily food (atleast 4 food groups) to 6-24 month old children
10% of additional mothers and caregivers wash their handsthoroughly with soap before food preparation and feeding of children6-24 months of age
50% family members and birth attendants prevent giving pre andpost lacteals within first 3 days after birth and continue exclusivebreastfeeding
Atleast 50% family planning workers promoting LAM as acontraception method
8
2 BDHS 2007. However, the Multiple Indicator Cluster Survey 2009 indicates 50% early initiation rate

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
V. Barriers and FacilitatorsThe IYCF communication famework and plan focuses on four themeswith the greatest public health impact according to studies and surveysin Bangladesh and the region:
1) Timely initiation of breastfeeding immediately after birth and on pre-post lacteals foods
2) Exclusive breastfeeding through 6 months of age
3) Age-appropriate nourishing complementary feeding (quantity,quality, diversed and responsive from 6-24 month old children
4) Handwashing linked to complementary feeding for 6-24 month oldchildren thoroughly with soap before preparing and feedingcomplementary foods
Factors that facilitate the adoption of emphasis behaviours form the mainfocus of the communication plan. The following facilitating factors wereidentified through qualitative research methods such as observations,focus groups, in-depth interviews, semi-structured interviews and Trialsof Improved Practices (TIPs). This has helped to narrow down the focuson the plan on certain groups of individuals, to identify effective channelsof communication for reaching them and to formulate effective messagesand strategies.
1) Timely initiation of breastfeeding immediately after birth and nopre-post lacteals foods
Key factors to facilitate adoption of behaviours:
- Mothers and family members learn about the importanceduring pregnancy or earlier
- At delivery, mothers receive support and help to place thenewborn on the breast for immediate breastfeeding
9
Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
- Elder female family members support timely initiation ofbreastfeeding and no pre/post lacteals foods
- Reduction in unnecessary C-sections, and appropriate support,if C-section is essential
- Decisions made about timely initiation and no pre-lactealsduring pregnancy
Main barriers: Poor understanding about adequacy of colostrum,danger of pre-post-lacteals and no skilled support given to mothers onposition, attachment, expression of breast milk and feeding of smallnewborns.
Exclusive breastfeeding through six months of age
Key factors to facilitate adoption of behaviours:
- Mother's and family members' confidence in the sufficiency ofher milk for six months
- Mother knows how to assess if milk supply is sufficient and notinterpret infant's crying as a cue that BF is not sufficient(learning to take cues from infant correctly)
- Mother knows correct position and attachment skills so infantcan withdraw as much milk as s/he needs
- Mother knows how to prevent a decline in milk supply, how toincrease milk supply and how to manually express breastmilk
- Family members are supportive and husband does not bringbreastmilk substitutes
- Mother and family members know the dangers of artificialpowdered milk and use of bottle, nipples and pacifiers
- Health workers and 'village doctors' reassure, support and buildconfidence in mother's ability to EBF for six months; anddoctors do not recommend breastmilk substitutes
10

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
Main barriers: Perception of insufficient milk supply, lack of skills andstrategies to increase and maintain supply for six months, inadequatesupport from family and doctors/health workers.
Age-appropriate nourishing complementary feeding (quantity, quality,diversed and responsive) from 6-24 months
Key factors to facilitate adoption of behaviours:
- Mother's confidence that she can motivate her child to eat therequired amounts (e.g. responsive feeding, supervised self-feeding and learning to act on child's cues for readiness to eat)
- Mothers’ and family members' knowledge of quantities (volumeand consistency) of food required for normal braindevelopment and growth
- Family members support and encourage mother to spend timeto feed child appropriately in sickness/when healthy
- Health workers (including 'village doctors') encourage mothersto feed young children appropriately
- Benefits that are of interest for mothers are reinforcedfrequently: 'develops child's brain' and 'protection fromillnesses', 'child likes to eat this way' and 'likes these foods';'convenient to feed child using family foods'
- Animal food encouraged by and brought by husband anddoctors
Main barriers: Perception of poor appetite among children 6-24 months,inadequate knowledge on amounts/consistency/diversity/use of animalfoods, little support for skills and strategies to increase child's interestand ability to consume needed CF.
11

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
4) Hand washing thoroughly with soap before preparing andfeeding complementary feeding children 6-24 months
Key factors to facilitate adoption of behaviours:
- Availability of soap and water
- Supportive family members
- Role models
- Local leaders encourage this behavior
Main barriers: Inadequate understanding of dangers of contaminatedCF, few role models.
VI. Participant Groups forCommunication Participant groups (audiences) analysis is an important component fordesigning the communication plan. Primary participant group is the directbeneficiary in this communication. Secondary and tertiary participantgroups play the direct and the indirect role as influencers for primaryparticipant groups. Programmes, many times, design and implementinterventions for the primary participant groups and less emphasis isgiven on the secondary and tertiary groups. Communication activities,therefore, need to focus on the behaviours of those who need to practicethe desired behaviours e.g. mothers, but also those who directly andindirectly influence mothers/caregivers and others or enable them topractice the desired behaviours. Current thinking calls for activeparticipation also by secondary and tertiary participant groups rather thantreating them as passive audiences or recipients of information.
The main categories of participant groups (audiences) for IYCF are:
- Primary participant groups are usually pregnant women,mothers and caregivers of children <2 years of age. Other
12

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
care providers such as skilled birth attendants, who need toplace the newboarn on the mother’s breast immediatly afterbirth, can also be primary participant group. Attendants whoneed to place the baby on the breast immediately after birth.
- Secondary participant groups are usually husbands and olderfemale family members and service providers.
- Tertiary participant groups are community leaders andmanagers or those who can mobilize or allocate resources andinvolve in making policies on various sectors. These sectorsare health, education, food security and agriculture, livelihoodsand poverty reduction, local government, gender equity andadvancement of women, religious and educational institutions,medical associations. Also others who can influence primary orsecondary participant groups or who can remove barriers andcreate an enabling environment.
The following table describes the primary, secondary and tertiaryparticipant groups for each of the IYCF key behaviours.
13

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
14
Key
Beh
avio
ur
Tim
ely
initi
atio
n of
bre
astfe
edin
g im
med
iate
ly
(with
in o
ne
hour
) afte
r birt
h an
d no
pre
-pos
t la
ctea
ls fo
ods
Exc
lusi
ve
brea
stfe
edin
g th
roug
h 6
mon
ths
of a
ge
Prim
ary
Pa
rtic
ipan
t Gro
up
Pre
gnan
t wom
en
Lact
atin
g m
othe
rs
Mot
hers
of 0
-6
mon
th o
ld in
fant
s
Seco
ndar
y Pa
rtic
ipan
t Gro
up
Ski
lled
birth
atte
ndan
tsE
lder
wom
en in
fam
ily
Eld
er w
omen
in fa
mily
Hus
band
sS
kille
d bi
rth a
ttend
ants
C
HW
s Vi
llage
doc
tors
Hom
eopa
ths
Tert
iary
Par
ticip
ant G
roup
Em
ploy
ers
of w
omen
, mat
erna
l and
ne
onat
al h
ealth
exp
erts
, gov
ernm
ent
auth
oriti
es (n
atio
nal
/dis
trict
/upa
zila
/com
mun
ity le
vels
), lo
cal e
lect
ed b
odie
s, re
ligio
us le
ader
s,
priv
ate
doct
ors
and
prof
essi
onal
as
soci
atio
ns, N
GO
s pr
ovid
ing
mat
erna
l and
new
born
hea
lth c
are
serv
ices
Sec
onda
ry le
vel h
ealth
car
e pr
ovid
ers,
go
vern
men
t aut
horit
ies,
pha
rmac
ists
, re
ligio
us le
ader
s, ro
le m
odel
s, e
lites
, In
fant
food
com
pani
es (t
o co
mpl
y w
ith
the
BM
S m
arke
ting
code
), N
GO
s pr
ovid
ing
mat
erna
l and
new
born
he
alth
car
e se
rvic
es, n
atio
nal a
nd
dist
rict d
ecis
ion
mak
ers,
loca
l ele
cted
bo
dies
, inf
luen
tials
, loc
al a
nd n
atio
nal
med
ia
Tabl
e 1.
Prim
ary,
Sec
onda
ry a
nd T
ertia
ry P
artic
ipan
t Gro
ups
Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
15
Key
Beh
avio
ur
Age
-app
ropr
iate
no
uris
hing
CF
(qua
ntity
, qu
ality
, div
erse
d an
d re
spon
sive
) fro
m 6
-24
mon
ths
Han
d w
ashi
ng
thor
ough
ly w
ith
soap
bef
ore
prep
arin
g an
d fe
edin
g co
mpl
emen
tary
fo
ods
Prim
ary
Pa
rtic
ipan
t Gro
up
Mot
hers
and
car
e gi
vers
of c
hild
ren
6-24
mon
ths
old
Mot
hers
and
car
e gi
vers
of c
hild
ren
6-24
mon
ths
old
Seco
ndar
y Pa
rtic
ipan
t Gro
up
Fath
ers
of c
hild
ren
Eld
er w
omen
in fa
mily
Ski
lled
birth
atte
ndan
ts
CH
Ws
Villa
ge d
octo
rs
Fath
ers
of c
hild
ren
Eld
er w
omen
in fa
mily
Ski
lled
birth
atte
ndan
ts
CH
Ws
Villa
ge d
octo
rs
Tert
iary
Par
ticip
ant G
roup
Seco
ndar
y le
vel h
ealth
car
e pr
ovid
ers
, go
vern
men
t aut
horit
ies,
pha
rmac
ists
, re
ligio
us le
ader
s, ro
le m
odel
s, e
lites
, In
fant
food
com
pani
es (t
o co
mpl
y w
ith th
e BM
S m
arke
ting
code
), N
GO
s pr
ovid
ing
infa
nt a
nd n
ewbo
rn h
ealth
ser
vice
s,
natio
nal a
nd d
istri
ct d
ecis
ion
mak
ers,
lo
cal e
lect
ed b
odie
s, a
dole
scen
ts
influ
entia
ls, l
ocal
and
nat
iona
l med
ia
Seco
ndar
y le
vel h
ealth
car
e pr
ovid
ers,
go
vern
men
t aut
horit
ies,
pha
rmac
ists
, re
ligio
us le
ader
s, ro
le m
odel
s, e
lites
, In
fant
food
com
pani
es (t
o co
mpl
y w
ith th
e BM
S m
arke
ting
code
), N
GO
s pr
ovid
ing
infa
nt a
nd n
ewbo
rn h
ealth
ser
vice
s,
natio
nal a
nd d
istri
ct d
ecis
ion
mak
ers,
lo
cal e
lect
ed b
odie
s, a
dole
scen
ts
influ
entia
ls, l
ocal
and
nat
iona
l med
ia
Tabl
e 1.
Prim
ary,
Sec
onda
ry a
nd T
ertia
ry P
artic
ipan
t Gro
ups

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
VII. Communication Channels andMedia Media and channels of communication were identified through nationalsurveys and in-depth formative research. For mothers, direct andfrequent interpersonal communication will be conducted through trainedcommunity health volunteers (CHVs) and health workers or CHWsincluding 'village doctors' and skilled birth attendants. Simple practicalsolutions to address critical IYCF problems will be emphasized, e.g.position and attachment, how to express breastmilk, how (and howmuch) to mix and feed complementary foods in a responsive manner.Also included are how to assess and prevent insufficient milk and how toassess appetite problems and prevent poor appetite in children of 6-24months. CHVs and CHWs require not only practical hands-on trainingbut ongoing support and motivation through a 'PerformanceImprovement Cycle' that includes supportive supervision, monthlymeetings and reviews to discuss field difficulties, incentives/rewards/recognition, and accountability through monitoring data anddiscussion/feedback of monitoring results. The tools for generating goodperformance for IYCF support in communities on a sustained basis arebeing field tested.
Secondary and tertiary participant groups and women in urban areas canbe reached on a larger scale through electronic media. TV, in particular,has been found to penetrate almost all regions of Bangladesh. TV spots,e.g. through BTV, at prime time, drama serials and films and particularlyduring major sports events and national holidays. 'Meena'films/spots/storybooks through BTV and other private channels, schools,mobile film units have wide coverage. Journalist trainings andfellowships, news editor and director engagement, earned mediaoutreach, building media champions, and TV debates will be used totarget the opinion shapers - in order to create a supportive environmentfor IYCF. Other channels include tea stall sessions, courtyard meetings,community events such as Friday prayers, 'melas'/fairs; schoolmanagement committee meetings and adolescent group activities; adult
16

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
non-formal education learning centers; high school curriculum. Mobilephone 'hot lines' will be used for counseling and problem-solving (e.g.Grameenphone).
Special events and forums for medical professionals and medical/nursingcollege curricula have been identified as key for a sustainable strategy.Billboards, wall paintings, tin boards, digital boards, interactive theaters,mobile vans, film shows, school-based events etc. have also beenrecommended but in a selected and targeted way due to their limitedcoverage. As the communication campaign gets underway, the planinvolves monitoring and assessment of the effectiveness of eachchannel, reviewing results, and making adjustments as necessary.Throughout the implementation period, the media plan will be shaped formaximum reach and impact.
VIII. Key Messages Message development workshops with stakeholders and findings offormative research form the basis of key messages in this section(Table-2). Stakeholders worked together and agreed to use thesemessages in the interest of a harmonized national communication plan.
17

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
18
Pre
gnan
t w
oman
and
la
ctat
ing
mot
her
Oth
er fa
mily
m
embe
rs
Eld
er w
oman
in
fam
ily
M
othe
r’s m
ilk is
the
only
food
for t
he b
aby
A
ny o
ther
pro
duct
will
incr
ease
cha
nces
of d
eath
and
di
arrh
oea
Th
e so
oner
you
put
the
baby
to b
reas
t the
soo
ner
mot
her’s
milk
will
flow
M
othe
r’s m
ilk is
the
only
food
for t
he b
aby
An
y ot
her p
rodu
ct w
ill in
crea
se c
hanc
es o
f dea
th a
nd d
iarrh
oea
Th
e so
oner
you
put
the
baby
to b
reas
t the
soo
ner
mot
her’s
milk
will
flow
Ski
lled
birth
at
tend
ant
Teac
her,
Imam
Doc
tor,
nurs
e an
d m
edic
al
prof
essi
onal
s
Hea
lth a
nd fa
mily
pl
anni
ng o
ffici
als
Hel
p to
put
the
baby
to th
e m
othe
r bre
ast
imm
edia
tely
afte
r birt
h
Tell
the
mot
her,
fath
er, g
rand
mot
her,
elde
rly
wom
an, o
f you
r loc
ality
to p
lace
the
baby
to
mot
her’s
bre
ast i
mm
edia
tely
afte
r birt
h
Hel
p th
e m
othe
r who
just
del
iver
ed to
put
th
e ba
by to
the
mot
her’s
bre
ast
In a
ll A
NC
ses
sion
s, e
nsur
e ea
rly
initi
atio
n m
essa
ges
are
give
n
R
emem
ber m
othe
r’s m
ilk is
the
only
food
for t
he b
aby
E
arly
initi
atio
n ca
n sa
ve th
e ba
by’s
life
P
rogr
amm
e w
ill a
chie
ve re
sults
in re
duci
ng n
eona
tal a
nd
child
mor
talit
y
Mot
her’s
milk
sav
es a
chi
ld’s
life
Hel
ps th
e ba
by to
be
inte
llige
nt
M
othe
rs’ m
ilk p
rote
cts
the
baby
from
dis
ease
s
Your
adv
ice
and
supp
ort c
an s
ave
a ch
ild’s
life
P
rogr
amm
e w
ill a
chie
ve re
sults
in re
duci
ng n
eona
tal a
nd
child
mor
talit
y
Tabl
e 2.
Key
Mes
sage
s fo
r Fou
r IYC
F B
ehav
iour
s
Who
?A
ctio
nW
hy?
Key
Beh
avio
ur -1
: Tim
ely
initi
atio
n of
bre
astfe
edin
g im
med
iate
ly (w
ithin
one
hou
r) af
ter b
irth
and
no p
re-p
ost l
acte
als
food
s
Put
yo
ur
baby
to
br
east
im
med
iate
ly a
fter b
irth
Hel
p to
pu
t th
e ba
by
to
the
mot
her
brea
st im
med
iate
ly a
fter
birth
Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
19
Mot
hers
of 0
- 6
mon
th o
ld in
fant
s
Hus
band
s
Eld
er w
omen
in
fam
ily
Ser
vice
pro
vide
rs
Bre
astfe
ed e
xclu
sive
ly fo
r 6
mon
ths
(180
day
s), d
o no
t giv
e ev
en a
dro
p of
wat
er, h
oney
, su
gar w
ater
Ti
ll 6
mon
ths
mot
hers
’ milk
is
enou
gh to
sat
isfy
the
thirs
t ev
en d
urin
g ho
t wea
ther
Bre
astfe
ed fr
eque
ntly
w
hene
ver t
he c
hild
dem
ands
at
leas
t 8-1
0 tim
es a
day
Pra
ctic
e pr
oper
atta
chm
ent
and
posi
tion
Sup
port
mot
hers
to s
pend
tim
e an
d E
BF
for 6
mon
ths,
sha
re
hous
ehol
d ch
ores
Bui
ld c
onfid
ence
in m
othe
rsE
ncou
rage
hus
band
s an
d m
othe
r in
law
s to
sup
port
mot
hers
N
early
all
mot
hers
can
bre
astfe
ed fo
r 6 m
onth
s. E
xclu
sive
br
east
feed
ing
help
s th
e ch
ild’s
phy
sica
l gro
wth
and
m
enta
l dev
elop
men
t, an
d al
so p
reve
nts
diar
rhoe
a, A
RI
and
man
y ot
her i
llnes
ses
To
pre
vent
dia
rrho
ea, A
RI
Th
e m
ore
the
baby
suc
ks, m
ore
milk
will
be
prod
uced
B
ondi
ng b
etw
een
mot
her a
nd c
hild
will
be
stro
ng
To
ens
ure
baby
is g
ettin
g pl
enty
of m
ilk
To e
nsur
e pr
otec
tion
of b
aby
and
plen
ty o
f milk
for b
rain
de
velo
pmen
t
S
o sh
e ca
n br
east
feed
exc
lusi
vely
for 6
mon
ths
Who
?A
ctio
nW
hy?
Key
Beh
avio
ur -2
: Exc
lusi
ve b
reas
tfeed
ing
thro
ugh
6 m
onth
s of
age

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
20
Villa
ge d
octo
rsP
harm
acis
tsM
edic
al
prac
titio
ners
Nur
ses
Pol
icy
mak
ers
from
Hea
lth a
nd
Oth
er s
ecto
rs
Sup
port
mot
hers
in E
BF
for 6
m
onth
s by
bui
ldin
g co
nfid
ence
D
o no
t pre
scrib
e or
re
com
men
d B
MS
or o
ther
fo
ods
befo
re 6
mon
ths
Pro
vide
app
ropr
iate
sup
port
whe
n a
brea
stfe
edin
g m
othe
r ne
eds
help
D
o no
t acc
ept g
ifts
and
ince
ntiv
es fr
om B
MS
co
mpa
nies
, fol
low
oth
er
prov
isio
ns o
f nat
iona
l Cod
e of
m
arke
ting
for B
MS
Giv
e pr
iorit
y to
IYC
F an
d is
sue
Gov
ernm
ent O
rder
and
C
ircul
ars
(e.g
. all
heal
th
wor
kers
com
ing
in c
onta
ct w
ith
mot
hers
)
�
For t
he b
enef
it of
you
r com
mun
ity’s
chi
ldre
n�
To a
void
bre
akin
g th
e la
w, a
nd to
avo
id ta
rnis
hing
you
r im
age
�
The
child
ren
of th
e na
tion
will
be
heal
thy
�
To m
aint
ain
your
eth
ical
sta
ndar
ds, a
void
pen
altie
s fo
r vi
olat
ing
the
Cod
e, a
nd p
reve
nt ta
rnis
hing
you
r im
age
�
Chi
ld s
urvi
val g
oals
will
be
achi
eved
and
the
coun
try’s
ec
onom
y w
ill b
e he
lped
Who
?A
ctio
nW
hy?
Key
Beh
avio
ur -2
: Exc
lusi
ve b
reas
tfeed
ing
thro
ugh
6 m
onth
s of
age

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
21
Mot
hers
and
ca
regi
vers
Fath
ers
of c
hild
ren
Eld
er w
omen
in
fam
ily
�
For p
hysi
cal g
row
th a
nd m
enta
l dev
elop
men
t�
Fam
ily fo
od is
imm
edia
tely
ava
ilabl
e, n
ouris
hing
and
ch
eap
�
Liqu
id fo
ods
fill u
p st
omac
h on
ly�
Chi
ld w
ill g
row
wel
l, pl
ay a
nd s
leep
wel
l. C
hild
will
be
safe
fro
m il
lnes
s, a
nd c
hild
’s b
rain
will
dev
elop
�
Your
chi
ld w
ill b
e in
telli
gent
and
chi
ld w
ill li
ke it
Hea
lth, F
amily
P
lann
ing
and
Nut
ritio
n w
orke
rsC
omm
unity
Hea
lth
Wor
kers
(g
over
nmen
t and
no
n-go
vern
men
t)
Sho
w m
othe
rs h
ow to
giv
e ag
e-ap
prop
riate
CF
(qua
ntity
an
d ty
pes
of fo
ods)
Iden
tify
6-24
mon
th c
hild
ren,
pr
ovid
e tim
ely
coun
selin
g/de
mon
stra
tion
at 6
, 9,
12,
18
mon
th t
o fe
ed
appr
opria
te C
F
�
To s
uppo
rt m
othe
rs a
nd re
min
d th
em h
ow to
feed
eno
ugh
of g
ood
food
to c
hild
�
To fu
lfill
your
job
resp
onsi
bilit
y, g
et re
war
ds/re
cogn
ition
, re
spec
t fro
m c
omm
unity
and
sup
port
mot
hers
for h
ealth
y ch
ildre
n
Who
?A
ctio
nW
hy?
Key
Beh
avio
ur -3
: A
ge-a
ppro
pria
te n
ouris
hing
CF
(qua
ntity
, qua
lity,
div
erse
d an
d re
spon
sive
) fro
m 6
-24
mon
ths
Sta
rt se
mi-s
olid
(not
liqu
id)
mas
hed
fam
ily fo
ods
twic
e a
day
afte
r 6 m
onth
sC
aref
ully
sel
ect a
ppro
pria
te
fam
ily fo
od. N
o ne
ed o
f spe
cial
co
okin
g/fo
ods
A ch
ild s
houl
d ea
t 2-5
bat
is
(bow
l)* a
day
in a
dditi
on to
br
east
feed
ing,
plu
s 1-
2 nu
tritio
us s
nack
sFe
ed o
ne p
iece
of m
eat o
r fis
h or
egg
at l
east
onc
e ev
ery
day
*Bow
l siz
e : 2
50 m
l

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
22
DP
EO
DE
Os
Ado
lesc
ents
Rel
igio
us le
ader
sC
omm
unity
lead
ers
Sec
y. M
OH
&FW
Oth
er o
ffici
als
(e.g
.Dep
uty
Com
mis
sion
er)
Trad
eB
usin
ess
pers
ons
and
CE
Os
Enc
oura
ge te
ache
rs to
talk
w
ith p
aren
ts a
bout
impo
rtanc
e of
app
ropr
iate
food
and
fe
edin
g pr
actic
es fo
r bra
in
deve
lopm
ent o
f chi
ld n
utrit
ion
and
IYC
FP
rom
ote
IYC
F m
essa
ges
durin
g re
gula
r and
spe
cial
pr
ayer
s an
d ce
rom
onie
s m
eetin
gs w
ith th
e co
mm
unity
R
eque
st th
e co
rpor
ate
sect
or
to s
tart
or e
nhan
ce C
SR
ac
tiviti
es o
n ap
prop
riate
CF
Pro
mot
e an
d pr
ovid
e su
ppor
t fo
r app
ropr
iate
CF
amon
g yo
ur
wor
kers
’ chi
ldre
n
�
To b
enef
it co
mm
unity
with
hea
lthy
and
inte
llige
nt c
hild
ren,
to
get
ext
ra re
spec
t fro
m th
e co
mm
unity
, and
to g
et m
ore
inte
llige
nt c
hild
ren
in s
choo
l
�
To s
prea
d re
ligio
us m
essa
ges
abou
t BF
for 2
yea
rs. T
o de
mon
stra
te c
omm
itmen
t to
the
com
mun
ity b
y re
ligio
us
lead
ers
of M
uslim
, Hin
du, B
uddh
ist a
nd C
hris
tian
Com
mun
ity�
For b
enef
its fo
r hea
lth a
nd a
dult
labo
ur p
rodu
ctiv
ity�
Age
-app
ropr
iate
nou
rishi
ng C
F is
cru
cial
for t
he p
hysi
cal
grow
th a
nd m
enta
l dev
elop
men
t of t
he c
hild
. It i
s an
es
sent
ial m
ulti-
sect
oral
issu
e
�
To e
nsur
e cu
rren
t and
futu
re p
rodu
ctiv
ity in
the
labo
ur
forc
e. C
ompa
nies
will
nee
d to
spe
nd le
ss m
oney
on
heal
th c
are
and
wor
kers
will
be
happ
ier a
nd le
ss a
bsen
t
Who
?A
ctio
nW
hy?
Key
Beh
avio
ur -3
: A
ge-a
ppro
pria
te n
ouris
hing
CF
(qua
ntity
, qua
lity,
div
erse
d an
d re
spon
sive
) fro
m 6
-24
mon
ths

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
23
Mot
hers
, ca
regi
vers
, fam
ily
mem
bers
Rel
igio
us le
ader
s C
omm
unity
le
ader
s
Uni
on P
aris
had
mem
ber
Loca
l G
over
nmen
t R
ural
D
evel
opm
ent
Min
istry
�
To k
eep
child
’s fo
od s
afe
from
illn
ess,
and
pre
vent
un
der-
nutri
tion
and
brai
n da
mag
e�
To p
rote
ct y
our c
hild
from
dia
rrho
ea a
nd d
ysen
tery
�
Bec
ause
you
r acc
epta
nce
will
incr
ease
in s
ocie
ty fo
r pr
otec
ting
the
mos
t vul
nera
ble
mem
bers
(you
ng c
hild
ren)
of
the
com
mun
ity
�
Beca
use
mal
e m
embe
rs g
athe
r tog
ethe
r and
list
en to
you
and
th
ey c
an s
uppo
rt m
othe
rs to
kee
p ch
ildre
n sa
fe fr
om il
lnes
s�
To d
emon
stra
te y
our c
omm
itmen
t to
the
com
mun
ity�
You
can
incr
ease
the
invo
lvem
ent o
f man
y co
mm
unity
le
ader
s to
pro
tect
you
ng c
hild
ren
from
illn
ess/
mal
nutri
tion
�
To re
min
d m
embe
rs th
eir r
espo
nsib
ility
tow
ards
thei
r co
mm
uniti
es b
y en
cour
agin
g ha
ndw
ashi
ng b
efor
e fe
edin
g yo
ung
child
ren
�
So
that
uni
on p
aris
hads
will
be
activ
e an
d ac
tiviti
es w
ill
mov
e fo
rwar
d to
pro
tect
you
ng c
hild
ren
from
illn
ess
and
mal
nutri
tion
�
To p
rote
ct c
hild
hea
lth a
nd n
utrit
ion
for t
he fu
ture
de
velo
pmen
t of t
he lo
cal c
omm
uniti
es
Who
?A
ctio
nW
hy?
Key
Beh
avio
ur -4
: Han
d w
ashi
ng th
orou
ghly
with
soa
p be
fore
pre
parin
g an
d fe
edin
g co
mpl
emen
tary
food
s
Bef
ore
prep
arin
g fo
od a
nd
befo
re fe
edin
g in
fant
s an
d yo
ung
child
ren
was
h bo
th
hand
s w
ith s
oap
and
wat
erW
hen
your
chi
ld le
arns
to e
at
on it
s ow
n w
ash
his/
her h
ands
w
ith s
oap
and
wat
erD
iscu
ss th
e im
porta
nce
of
hand
was
hing
bef
ore
prep
arin
g an
d fe
edin
g ch
ildre
n un
der 2
in
regu
lar w
eekl
y pr
ayer
sD
iscu
ss th
e im
porta
nce
of
hand
was
hing
bef
ore
prep
arin
g an
d fe
edin
g ch
ildre
n in
di
ffere
nt p
ublic
aw
aren
ess
prog
ram
mes
Incl
ude
the
impo
rtanc
e of
ha
ndw
ashi
ng in
you
r mon
thly
m
eetin
g ag
enda
Issu
e pr
ovid
e G
over
nmen
t O
rder
and
Circ
ular
s to
incl
ude
hand
was
hing
issu
e in
the
mon
thly
wor
kpla
n ac
tiviti
es o
f U
nion
Par
isha
d

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
IX. Implementation PlanInstitute of Public Health Nutrition of Directorate General of HealthServices, Ministry of Health and Family Welfare is the main coordinatingbody for the implementation of national IYCF strategy and itscommunication plan. The communication framework and plan isdesigned to be implemented in collaboration with partners in thegovernment, development organizations, NGOs and private sectors. Thelist of stakeholders is presented in Table 3 below.
The implementation is planned as a concerted effort of variousstakeholders. Government will work together with donors, developmentpartners and other key entities to ensure a harmonized and unifiedimplementation approach. This will be done through ensuring allocationof resources, using a common logo and branding of the campaign.
The IYCF communication plan will be implemented in phases to cover allthe 64 districts. GOB with support of the several partner agencies isimplementing some components of IYCF communication interventions aspart of their maternal, neonatal and child health and nutritionprogrammes. Table 4 indicates the action plan with targets and timelineof activities.
24

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
25
Tim
ely
initi
atio
n of
br
east
feed
ing
imm
edia
tely
(with
in o
ne
hour
) afte
r birt
h an
d no
pr
e-po
st la
ctea
ls fo
ods
MO
HFW
- D
GFP
, DG
HS
, IP
HN
,NN
P, B
NN
C, B
BF
MO
I M
OR
A M
OS
W
MO
E -N
CTB
BPA
Nat
iona
l Neo
nato
logy
Fo
rum
Don
ors
and
deve
lopm
ent
partn
ers
: WH
O, U
NIC
EF
A&
T, U
SA
ID, G
TZ, D
FID
, C
IDA
, JIC
A, W
FP, F
AO
M
edia
Par
tner
s N
ewsp
aper
s &
priv
ate
TV
and
Rad
io C
hann
els
All
NG
Os
Wor
king
in
Rel
ated
Fie
ld
Excl
usiv
e br
east
feed
ing
thro
ugh
6 m
onth
s of
ag
e
MO
HFW
- D
GFP
, DG
HS
, IP
HN
, NN
P, B
NN
C, B
BF
MO
I M
OR
A M
O L
GE
RD
MO
SW
Min
istry
of H
ome
Affa
irsM
OE
Don
ors
and
deve
lopm
ent
partn
ers
: WH
O, U
NIC
EF,
A
&T,
US
AID
, GTZ
, DFI
D,
CID
A, J
ICA
, WFP
, FA
OM
edia
Par
tner
s N
ewsp
aper
s &
priv
ate
TV
and
Rad
io C
hann
els
Em
ploy
ers,
Gar
men
ts a
nd
othe
rs
Age
-app
ropr
iate
no
uris
hing
CF
(qua
ntity
, qu
ality
, div
erse
d an
d re
spon
sive
) fro
m 6
-24
mon
ths
MO
HFW
-DG
FP, D
GH
S,
IPH
N, N
NP,
BN
NC
MO
I M
OR
A D
G-A
EM
OP
ME
-- D
G-D
PE
, DG
- B
NFE
MO
SW
M
OE
- N
CTB
Don
ors
and
deve
lopm
ent
partn
ers
: WH
O, U
NIC
EF,
A
&T,
US
AID
, GTZ
, DFI
D,
CID
A, J
ICA
, WFP
, FA
OM
edia
Par
tner
s N
ewsp
aper
s &
priv
ate
TV
and
Rad
io C
hann
els
Wom
en le
ader
s (M
P,
UC
,UP
-C)
Han
d w
ashi
ng
thor
ough
ly w
ith s
oap
befo
re p
repa
ring
and
feed
ing
com
plem
enta
ry
food
sM
OH
FW-D
GFP
, DG
HS
, IP
HN
NN
P, B
NN
C
Min
istry
of A
gric
ultu
reM
OI
MO
RA
MO
LG
ER
D
MO
SW
M
OW
CA
Don
ors
and
deve
lopm
ent
partn
ers
: WH
O, U
NIC
EF,
A
&T,
US
AID
, GTZ
, DFI
D,
CID
A, J
ICA
, WFP
, FA
OM
edia
Par
tner
s N
ewsp
aper
s &
priv
ate
TV
and
Rad
io C
hann
els
Isla
mic
Fou
ndat
ion
Tabl
e 3.
Sta
keho
lder
s fo
r Nat
iona
l IYC
F C
omm
unic
atio
n Fr
amew
ork
and
Plan

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
26
Ban
glad
esh
Per
inat
al
Soc
iety
OG
SB
All
Bab
y Fo
rmul
a M
aker
s
BTR
C a
nd a
ll ot
her T
elco
an
d N
okia
NG
Os
& IN
GO
s: B
RA
C,
SC
US
SC
UK
, Pla
n B
angl
ades
h, C
are,
C
once
rn W
orld
wid
e an
d ot
hers
Nat
iona
l Neo
nato
logy
Fo
rum
Ban
glad
esh
Per
inat
al
Soc
iety
OG
SB
BPA
NG
Os
& IN
GO
s: B
RA
C,
SC
US
SC
UK
, Pla
n B
angl
ades
h, C
are,
C
once
rn W
orld
wid
e an
d ot
hers
A
ll B
aby
Form
ula
Mak
ers
Priv
ate
sect
or, T
elco
, foo
d co
mpa
nies
DG
-TV,
Bet
ar
Ans
ar -V
DP
Shi
shu
Aca
dem
y
BPA
NG
Os
& IN
GO
s: B
RA
C,
SC
US
SC
UK
, Pla
n B
angl
ades
h, C
are,
C
once
rn W
orld
wid
e an
d ot
hers
Priv
ate
sect
or, f
ood
com
pani
es
Pub
lic P
rivat
e P
artn
ersh
ip
(PP
P)
Priv
ate
sect
or, s
oap
man
ufac
ture
r P
ublic
Priv
ate
Par
tner
ship
(P
PP
)N
GO
s &
ING
Os:
BR
AC
, S
C-U
S S
C-U
K, P
lan
Ban
glad
esh,
Car
e,
Con
cern
Wor
ldw
ide
and
othe
rs
Tabl
e 3.
Sta
keho
lder
s fo
r Nat
iona
l IYC
F C
omm
unic
atio
n Fr
amew
ork
and
Plan

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
27
SN
Act
iviti
es
Key
Ta
rget
s R
espo
nsib
ilitie
s 20
10
2011
20
12
2013
beha
viou
rs
Rev
iew
exi
stin
g tra
inin
g an
d ot
her m
ater
ials
and
in
corp
orat
e va
rious
IYC
F re
late
d co
mm
unic
atio
n co
nten
t for
diff
eren
t pa
rtici
pant
gro
ups
Trai
ning
and
orie
ntat
ion
of
gove
rnm
ent,
NG
O, p
rivat
e co
mm
unity
wor
kers
ser
vice
pr
ovid
ers
and
skille
d bi
rth
atte
ndan
ts o
n in
clud
ing
coun
selin
g ho
me
visi
ts,
cour
tyar
d se
ssio
nsO
rient
atio
n of
vill
age
doct
ors
and
phar
mac
ists
Orie
ntat
ion
of re
ligio
us
lead
ers
for d
isse
min
atio
n of
IY
CF
mes
sage
s du
ring
relig
ious
occ
asio
ns a
nd
wee
kly
pray
ers
Hea
lth a
nd fa
mily
pla
nnin
g
prog
ram
mes
impl
emen
t co
unse
ling
(with
de
mon
stra
tion)
am
ong
preg
nant
wom
en a
nd
mot
hers
and
fam
ilies
th
roug
h ho
me
visi
ts
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
BF(
EI,E
BF)
CF,
HW
CF
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
40 d
istri
cts
40 d
istri
cts
40 d
istri
cts
40 d
istri
cts
40 d
istri
cts
DG
HS,
IPH
N,
UN
ICEF
, DG
FP,
NN
P, B
BF,
SCF-
USA
, USA
ID,
BRAC
(A&T
), ot
her N
GO
s
IPH
N, U
NIC
EF,
N
IPO
RT,
BH
E,
IEM
, NN
P, B
BF,
S
CF-
US
A, B
RA
C
(A&
T)
IPHN
, UNI
CEF,
IEM
, BH
E, B
RAC
(A&T
)IP
HN
, UN
ICE
F,
IEM
, BR
AC
(A&
T)
IPH
N, U
NIC
EF,
IE
M, B
HE
, NN
P,
BB
F, S
CF-
US
A,
BR
AC
(A&
T),
PLAN
-Ban
glad
esh
othe
r NG
Os
11. 2. 3. 4. 5.
23
41
23
4X
XX
XX
X
XX
XX
XX
XX
XX
XX
XX
X
XX
XX
XX
X
XX
XX
XX
XX
Tabl
e 4.
Act
ion
Plan
for I
mpl
emen
tatio
n of
Com
mun
icat
ion
Act
iviti
es

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
28
TV s
pots
at p
rime
time
and
mob
ile fi
lm s
how
s
Rad
io s
pots
for n
atio
nal
and
Com
mun
ity R
adio
Visu
al re
min
der I
EC
m
ater
ials
or j
ob a
ids
for
heal
th p
rovi
ders
and
co
mm
unity
wor
kers
M
eena
pro
duct
ion
and
view
ing
of a
nim
ated
film
s
Tea
stal
l vie
win
g of
TV
Cs
and
docu
men
tarie
s in
DV
D
play
ers,
foru
ms
for m
othe
r, fa
ther
, mot
her i
n la
w a
nd
com
mun
ity p
eopl
eTe
levi
sion
pro
gram
me
once
a w
eek
targ
eted
to
war
ds a
dole
scen
ts a
nd
youn
g m
othe
rs a
nd
fam
ilies
BF
(EI,E
BF)
C
F, H
WC
FB
F (E
I,EB
F)
CF,
HW
CF
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
FB
F (E
I,EB
F)
CF,
HW
CF
BF
(EI,E
BF)
C
F, H
WC
F
IPH
N, A
&T,
MO
I
A&
T, U
NIC
EF,
M
OI
IPH
N, U
NIC
EF,
A
&T,
US
AID
, N
GO
s
UN
ICE
F, A
&T
and
DM
C
IPH
N, U
NIC
EF,
IE
M, B
HE
, NN
P,
BR
AC
, (A
&T)
, N
GO
s
IPH
N, M
OI,
Pla
n–B
angl
ades
h,
US
AID
16. 8.7. 9. 10
.
11.
23
41
23
4X
XX
XX
XX
XX
XX
XX
XX
XX
XX
XX
XX
Tabl
e 4.
Act
ion
Plan
for I
mpl
emen
tatio
n of
Com
mun
icat
ion
Act
iviti
es
XX
XX
XX
XX
XX
XX
XX
X
XX
XX
X
3 at
leas
t ai
red
natio
nally
3 at
leas
t ai
red
natio
nally
As
need
ed
3 ai
red
natio
nally
40 d
istri
cts
At l
east
8
epis
odes
an
nual
ly
SN
Act
iviti
es
Key
Ta
rget
s R
espo
nsib
ilitie
s 20
10
2011
20
12
2013
beha
viou
rs

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
29
SN
Act
iviti
es
Key
Ta
rget
s R
espo
nsib
ilitie
s 20
10
2011
20
12
2013
beha
viou
rs
Laun
ch o
f com
mun
icat
ion
ca
mpa
ign
for p
ublic
and
pr
ivat
e se
ctor
, pre
ss
brie
fing
of J
ourn
alis
ts,
succ
ess
stor
ies
diss
emin
ated
and
repe
ated
Bui
ld c
apac
ity o
f ad
oles
cent
net
wor
ks fo
r so
cial
act
ion
initi
ativ
eS
choo
l/col
lege
deb
ates
an
d qu
iz p
rogr
amm
es
Adv
ocac
y m
eetin
g in
7
divi
sion
s w
ith d
iffer
ent
sect
ors
of G
OB
, NG
O,
priv
ate
sect
or a
nd lo
cal
Mem
bers
of P
arlia
men
t an
d in
fluen
tials
In
tera
ctiv
e dr
ama
seria
ls
on ra
dio
an T
V
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
FB
F (E
I,EB
F)
CF,
HW
CF
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
At l
east
2
As
need
ed
At l
east
5
per y
ear
Ann
ually
in
7 D
ivis
ions
13 e
piso
des
As
need
ed
IPH
N, U
NIC
EF,
D
MC
, PIB
, DM
C,
A&
T
CM
ES
, BR
AC
(A
&T)
, oth
er
NG
Os
IPH
N, U
NIC
EF,
IEM
, BH
E,
Seco
ndar
y Ed
ucat
ion,
SC
F-U
SA, U
SAID
, BR
AC (A
&T),
othe
r NG
Os
IPH
N, U
NIC
EF,
A
&T
and
othe
rs
impl
emen
ting
Par
tner
s
IPH
N, U
NIC
EF,
M
OI
112
.
13.
14.
15.
16.
23
41
23
4X
XX
XX
XX
XX
XX
XX
X
XX
XX
XX
X
XX
XX
XX
XX
XX
XX
X
Tabl
e 4.
Act
ion
Plan
for I
mpl
emen
tatio
n of
Com
mun
icat
ion
Act
iviti
es

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
30
SN
Act
iviti
es
Key
Ta
rget
s R
espo
nsib
ilitie
s 20
10
2011
20
12
2013
beha
viou
rs
Dev
elop
and
pro
duce
co
mm
unic
atio
n gu
idel
ines
, m
odul
es a
nd m
ater
ials
, as
requ
ired
Nat
iona
l con
sulta
tions
for
tech
nica
l, po
licy
and
prog
ram
me
upda
tes
Adv
ocac
y m
eetin
gs w
ith
GO
B, d
onor
s, p
artn
ers
and
othe
r inf
luen
tial g
roup
s su
ch
as p
arlia
men
taria
ns, m
edia
pe
rson
nel
IYC
F tra
inin
g an
d m
edia
en
gage
men
t pro
gram
me
for
natio
nal h
ealth
and
oth
er
jour
nalis
ts, e
dito
rs a
nd n
ews
dire
ctor
s an
d up
date
sA
rticl
es p
ublis
hed
in m
ost
wel
l circ
ulat
ed n
atio
nal a
nd
regi
onal
dai
lies
Advo
cacy
ana
lysi
s (p
rofil
es)
activ
ities
/eve
nts
and
mat
eria
ls
in c
olla
bora
tion
with
med
ia
e.g.
Wor
ld B
reas
tfeed
ing
Wee
k, H
andw
ashi
ng W
eek
and
othe
r eve
nts
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
FB
F (E
I,EB
F)
CF,
HW
CF
2 pe
r yea
r
At l
east
3
per y
ear
4 wor
ksho
ps
per y
ear
At l
east
8
per y
ear
At l
east
4
activ
ities
an
d 2
mat
eria
ls
per y
ear
IPH
N, U
NIC
EF,
A
&T
and
othe
rs
IPH
N, U
NIC
EF,
an
d m
ultip
le A
&T
impl
emen
ting
partn
ers
IPH
N, U
NIC
EF,
A
&T
and
mul
ti im
plem
entin
g pa
rtner
s
IPH
N, U
NIC
EF,
A
&T
and
US
AID
IPH
N, A
&T
IPH
N, A
&T,
U
NIC
EF,
US
AID
(F
AN
TA 2
), im
plem
entin
g pa
rtner
s
1
18.
17.
19.
20.
21.
22.
23
41
23
4
XX
XX
XX
XX
XX
X
XX
XX
XX
XX
XX
XX
XX
XX
XX
XX
XX
X
Tabl
e 4.
Act
ion
Plan
for I
mpl
emen
tatio
n of
Com
mun
icat
ion
Act
iviti
es

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
31
SN
Act
iviti
es
Key
Ta
rget
s R
espo
nsib
ilitie
s 20
10
2011
20
12
2013
beha
viou
rs
Incl
usio
n of
IYC
F co
nten
t in
non-
form
al a
nd fo
rmal
sc
hool
edu
catio
n cu
rric
ulum
and
orie
ntat
ion
of fa
cilit
ator
sW
orks
hop
for M
essa
ges
and
mat
eria
ls
deve
lopm
ent,
revi
ew a
nd
upda
ting
Wor
ksho
ps a
nd fo
llow
up
for p
re-s
ervi
ce tr
aini
ng in
m
edic
al a
nd n
ursi
ng
colle
ges
Orie
ntat
ion
of u
nion
/u
pazi
la p
aris
hads
/loca
l le
ader
s to
incr
ease
sup
port
for I
YC
F Fo
rmat
ive
rese
arch
, te
stin
g, m
onito
ring,
le
arni
ng a
nd e
valu
atio
n:
base
line
surv
eys,
m
onito
ring
and
qual
ity
asse
ssm
ents
, ana
lysi
s an
d re
view
/revi
sion
, qua
litat
ive
stud
ies
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
BF
(EI,E
BF)
C
F, H
WC
F
2 se
ts o
f m
ater
ials
At l
east
1
per y
ear
At l
east
2 To
T
per y
ear
In 4
0 fo
cus
dist
ricts
In a
t lea
st
10 f
ocus
di
stric
ts
IPH
N, N
CTB
, BN
FE, A
& T
, U
NIC
EF,
IPH
N, U
NIC
EF,
A&T
IPH
N, C
ontin
uous
M
edic
al E
duca
tion
BPA,
NN
F, O
GSB
, A&
T
IPH
N, U
NIC
EF,
NG
Os,
Min
. Loc
al
Gov
t., B
RAC
(A
&T)
IPH
N, U
NIC
EF,
A&T,
IFPR
I, ot
her
NG
Os
123
.
24.
25.
26.
27.
23
41
23
4
XX
XX
XX
XX
XX
X
XX
XX
XX
XX
XX
XX
X
Tabl
e 4.
Act
ion
Plan
for I
mpl
emen
tatio
n of
Com
mun
icat
ion
Act
iviti
es

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
32
SN
Act
iviti
es
Key
Ta
rget
s R
espo
nsib
ilitie
s 20
10
2011
20
12
2013
beha
viou
rs
Mon
itorin
g, le
arni
ng a
nd
eval
uatio
n: b
asel
ine
surv
eys,
mon
itorin
g an
d qu
ality
ass
essm
ents
, an
alys
is a
nd
revi
ew/re
visi
onR
evie
w o
f co
mm
unic
atio
n fra
mew
ork
and
plan
BF (E
I, EB
F)C
F, H
WC
FIn
focu
s di
stric
ts
1
IPH
N, A
& T
, U
NIC
EF,
NG
Os
IPH
N, U
NIC
EF,
A
& T
1
29.
30.
23
41
23
4
XX
XX
XX
XX
IPH
N, A
& T
,U
NIC
EF
BF (E
I, EB
F)C
F, H
WC
FR
evie
w o
f com
mun
icat
ion
fram
ewor
k an
d pl
an
28.
XX
Tabl
e 4.
Act
ion
Plan
for I
mpl
emen
tatio
n of
Com
mun
icat
ion
Act
iviti
es

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
X. Monitoring and Evaluation
Indicators for IYCF Communication
The achievement of this communication plan will depend on thefollowing processes that will be carefully monitored:
effective planning and timely implementation of activities;
use of a common, harmonized set of messages and approaches byvarious stakeholders covering all parts of the country for a sustainedperiod of time;
development and production of appropriate communication materialsfor different participant groups and channels;
use of mass media and IPC materials through multiple channels toachieve adequate intensity and saturation with key messages; and
an effective monitoring and evaluation plan is implemented andresults used for continuous fine-tuning of the strategy until changesin behaviour are documented.
The monitoring and evaluation plan for communication should be part ofthe total M&E plan for the IYCF programme. Government, stakeholdersand partners will jointly monitor the implementation of the IYCFprogramme. The IYCF programme will build the capacity of communities,service providers and project managers at all level to collect, synthesize,analyze and use data for making decisions about how to improve theimpact on behaviours through better reach/coverage, greater intensity,more channels, better comprehension, and timing/targeting of thecommunication activities. Reports on the processes and outputs will beroutinely discussed at national and district levels. A series of studiesmay be undertaken on various aspects of the plan including a post linestudy on KAP of IYCF to be conducted at the end of the campaign.
The monitoring and evaluation framework presented in Table 5 will befurther developed and finalised through a workshop.
33

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
34
Table 5. Monitoring and Evaluation Indicators for IYCF CommunicationActivities
By the end of 2013,
Mothers initiated breastfeedingimmediately (within 1 hour) ofbirth increased from 50% to 65%
At least 65% of birth attendants(SBA/TBA/midwife/familymember) reached through IYCFinitiative in programme areas putnewborns to mothers' breastimmediately (within 1 hour) ofbirth and no pre-post lactealsfoods
At least 50% of service providersinvolved in ANC/PNC/FP/IMCI/ENC/EPI in programme areaswho promote putting newbornsto mothers' breast immediately(within 1 hour) of birth and nopre-post lacteals foods
Optional:
At least 30% of religious leaderscoming in contact with pregnantwomen or their families activelypromote early initiation of BF andno pre-lacteals in programmeareas during their regular andspecial prayers and ceremonies
At least 50% of family planningworkers promoting LAM as acontraceptive method inprogramme areas
Key Behaviour 1 - Timely initiation of breastfeeding immediately afterbirth and no pre-post lacteal foods
% of newborns who were put tothe breast within 1 hour of birth
% of birth attendants (SBA/TBA/midwife/family member) putnewborns to mothers' breastwithin 1 hour of birth
% of service providers involvedin ANC/PNC/FP/IMCI/ENC/EPIput newborns to mothers' breastwithin 1 hour of birth and notgiving pre-lacteals foods
Optional:
% of religious leaders, coming incontact with pregnant women ortheir families who activelypromote early initiation and nopre-lacteals
% of family planning workerswho promote LAM as acontraceptive method
Communication Objectives Monitoring & Evaluation Indicators

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
35
By the end of 2013,
Mothers exclusively breastfeedingtheir infants 0-6 months of ageincreased from 43% to 60% inprogramme areas
At least 50% of communitieshave trained CHWs orvolunteers support mothers toexclusively breastfeed for 6months (including position,attachment, how to expressbreastmilk and how to assessand maintain milk supply, anddangers of BMS), in programmeareas
Optional:
At least 25% of communitieshave more than one communityleader or adolescent sensitizedand promotes exclusivebreastfeeding for 6 months anddiscourages BMS among familymembers in programme areas
Key Behaviour 2 - Exclusive breastfeeding through six months
% of mothers who areexclusively breastfeeding theirinfants 0-6 months of age
% of communities with trainedCHWs or volunteers who supportmothers to exclusivelybreastfeed for 6 months(including position, attachment,how to express breastmilk andhow to assess and maintain milksupply, and dangers of BMS)
Optional:
% of communities with morethan one community leader oradolescent who promotingexclusive breastfeeding for 6months and discourages BMSamong family members
Communication Objectives Monitoring & Evaluation Indicators

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
36
By the end of 2013,
At least 50% of mothers andcaregivers of 6-24 months of ageare consuming age-appropriatequantity of diversified (at least 4food groups) semi-solid or solidfamily foods in programme areas
At least 50% of communitieshave trained CHWs orvolunteers who support mothersto feed age-appropriate quantityof diversified (at least 4 foodgroups) semi-solid or solid familyfoods to children 6-24 months ofage in programme areas
An additional 10% of mothersand caregivers of 6-24 months ofage feed animal foods at leastonce daily in programme areas
Optional:
At least 50% of service providerssupport mothers to feed age-appropriate quantity of diversified(at least 4 food groups) semi-solid or solid family foods tochildren 6-24 months of age inprogramme areas
At least 50% of communities havemore than one community groupsor leaders or adolescents who aresensitized and promote feeding ofage-appropriate quantity ofdiversified (at least 4 food groups)semi-solid or solid family foods tochildren 6-24 months of age inprogramme areas
Key Behaviour 3 - Age appropriate nourishing & complementary feeding(quantity, quality, diversity and responsive) for children 6-24 months
% of children 6-24 months ofage who are consuming age-appropriate quantity of diversified(at least 4 food groups) semi-solid or solid family foods
% of communities that havetrained CHWs or volunteers whosupport mothers to feed age-appropriate quantity of diversified(at least 4 food groups) semi-solid or solid family foods tochildren 6-24 months of age
% of children 6-24 months ofage who are consuming animalfoods at least once daily
Optional:% of service providers whosupport mothers to feed age-appropriate quantity of diversified(at least 4 food groups) semi-solid or solid family foods tochildren 6-24 months of age
% of communities that havemore than one community leaderor adolescent promoting feedingof age-appropriate quantity ofdiversified (at least 4 foodgroups) semi-solid or solid familyfoods to children 6-24 months ofage
Communication Objective Monitoring & Evaluation Indicators

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
37
By the end of 2013,
An additional 10% of mothersand caregivers wash their handsthoroughly with soap before foodpreparation and feeding ofchildren 6-24 months of age inprogramme areas
Handwashing linked tocomplementary feedingaddressed in national hygienepromotion strategy and actionplans
Optional:
An additional 10% of householdsprocure and make handwashingmaterials (soap and water)available to mothers andcaregivers who prepare food andfeed children 6-24 months of agein programme areas
At least 3 soap manufacturersinclude handwashing linked tofeeding of young children inadvertising messages for soap
Key Behaviour 4 - Handwashing thoroughly with soap before preparingcomplementary foods and feeding complementary food
% of mothers and caregiverswho wash their hands thoroughlywith soap before foodpreparation and feeding ofchildren 6-24 months of age
Whether handwashing linked tocomplementary feeding isaddressed in national hygienepromotion strategy and actionplans
Optional:
% of households that procureand make handwashingmaterials (soap and water)available to mothers andcaregivers who prepare food andfeed children 6-24 months of age
Number of soap manufacturersthat include handwashing linkedto feeding of young children inadvertising messages for soap
Communication Objective Monitoring & Evaluation Indicators

Co
mm
un
ica
tio
n F
ram
ew
ork
an
d P
lan
fo
r In
fan
t a
nd
Yo
un
g C
hil
d F
ee
din
g
1. Proffesor Dr. Shah Monir Hossain,Director General of HealthServices
2. Professor Dr. M.Q.K. Talukder3. Professor Dr.T.A Chowdhury4. Professor Dr. Syeda Afroza5. Directorate General of Family Planning6. Directorate General of Health Services7. Institute of Public Health Nutrition8. Bureau of Health Education, DGHS9. National Nutrition Program10. Dhaka Shishu Hospital11. Bangladesh Breastfeeding Foundation 12. Dhaka Dental College & Hospital13. Directorate of Primary Education14. Bureau of Non Formal Education, MOPME15. National Curriculum and Text Book Board, MOPME16. Bangladesh Betar17. Bangladesh Television18. UNICEF19. United States Agency for International Development (USAID)20. Alive and Thrive21. BRAC22. AED/FANTA23. CARE Bangladesh24. Concern Worldwide25. Centre for Woman and Children Health 26. Helen Keller International27. International Centre for Diarrhoeal Disease Research, Bangladesh28. Plan Bangladesh29. Save the Children-USA30. Action Contre la Faim31. ASIATIC JWT32. Dhanshiri Communication
38
Names of individual participants and oganisations contributed indevelopment of Communication Framework and Plan for Infant andYoung Child Feeding (2010 - 2013)

N
Developed and Published by :
Institute of Public Health Nutrition (IPHN)
Directorate General of Health Services
Ministry of Health and Family Welfare, Bangladesh
Supported by:
UNICEF and Alive & Thrive, Bangladesh
October 2010
For more information contact:Director, IPHN &Line Director, MicronutrientsDirectorate General of Health ServicesMinistry of Health and Family WelfareTelephone : (88-02) 8821361e-mail: [email protected]







