
Multitarget Stool DNA Testing for Colorectal-Cancer Screening
NEJM April 3, 2014 Vol 3
Imperiale, T.F. et alPresented by Melissa Spera, MD
Background• Colon cancer is a major cause of death in the
US• Simple, non invasive screening with high
sensitivity could improve outcomes• Colorectal cancer arises from genetic and
epigenetic alterations• These changes are the basis for analyzing stool
to identify tumor specific changes

Background
• Previous stool DNA tests had low sensitivity for detecting advanced carcinomas
• Moderate sensitivity for colorectal cancers• Advances have since been made• Previously evaluation of the stool DNA test
was performed on archived specimens with a diagnosis

Primary Aim
• To determine the performance characteristics of the DNA test in the detection of colorectal cancer.

Secondary Aim
• To compare the performance of the stool DNA test to the commercially available fecal immunochemical test (FIT) for human hemoglobin in the detection of both colorectal cancer and advanced precancerous lesions

Methods-Study Design
• Cross sectional study• Participants enrolled from Jun 2011-Nov 2012• From 90 sites in the US and Canada• Private Practice and academic settings• Study design by the authors• Funded by Exact Sciences• Health Decisions-gathered/monitored data

Methods-Study Population
• Asymptomatic people-ages 50-84 years old• Average risk for colorectal cancer• Scheduled for a colonoscopy• Enrollment weighted towards people > 65• Many were excluded

Methods-Clinical Procedures
• Participants provided stool specimen• screening colonoscopy w/in 90 days• Required to describe:• the extent of examination• cecal visualization• quality of prep • Size and location of lesion
Methods-Clinical Procedures
• The most advanced lesion present and its location were used to categorize participants
• If two similar lesions found, the larger lesion was the index lesion

Methods-Clinical Procedure
• Proximal Colon- the splenic flexure and all colon proximal to it, insertion depth > 60cm, or the phrase “right colon” was used
• Distal Colon-all other segments than above, insertion depth < 60cm or the phrase “left colon” was used

Methods-Clinical Procedures
• All biopsies and surgical specimens were evaluated at the lab typically used by the institution
• Concerning lesions were re reviewed• Disagreements were resolved by a consensus
of at least 2 pathologists

Methods-Lab Procedures
• 3 labs processed all stool samples • Exact Sciences (Madison, WI) *Funded Study*• Mayo Medical Lab (Rochester, Mn)• Molecular Pathology Lab Network (Knoxville,
Tn)• Labs were blinded to clinical information• The same stool sample was used for both tests

Multitarget stool DNA test
• Molecular assays for• Aberrantly methylated BMP3• NDRG4 promoter regions• Mutant KRAS• B actin(reference gene for human DNAquality)• IC assay for human hemoglobin

FIT(Fecal Immunochemical Test)
• Performed according to manufacturer instructions
• All samples sent to a single, blinded lab• Samples with > 100ng of hemoglobin per
milliliter were considered to be positive

Statistical Analysis
• Study designed to have a power of 90%• Hypothesis: DNA test would have sensitivity
of 65% or more to detect CR cancer• 2nd Hypothesis: R/O a 5% non inferiority
margin for sensitivity for detection of CR cancer with the DNA test compared with FIT

Enrollment and Outcomes.
Imperiale TF et al. N Engl J Med 2014;370:1287-1297

Sensitivity and Specificity of the Multitarget Stool DNA Test and the Fecal Immunochemical Test (FIT) for the Most Advanced Findings on Colonoscopy.
Imperiale TF et al. N Engl J Med 2014;370:1287-1297
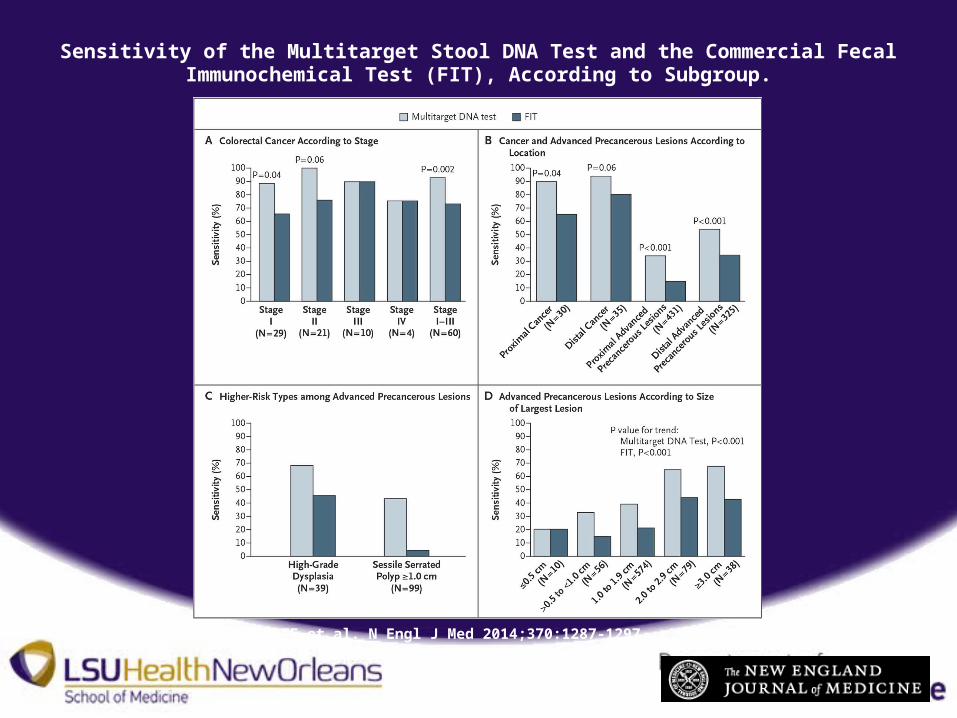
Sensitivity of the Multitarget Stool DNA Test and the Commercial Fecal Immunochemical Test (FIT), According to Subgroup.
Imperiale TF et al. N Engl J Med 2014;370:1287-1297

Numbers of Persons Who Would Need to Be Screened with Colonoscopy, Multitarget DNA Test, and FIT to Detect One Colorectal Cancer and One Advanced Precancerous Lesion.
Imperiale TF et al. N Engl J Med 2014;370:1287-1297

Extrapolation of Findings to an Expanded Population of 10,000 Persons at Average Risk for Colorectal Cancer Undergoing Screening with Colonoscopy, Multitarget Stool DNA Test, and
FIT.
Imperiale TF et al. N Engl J Med 2014;370:1287-1297

Discussion
• Sensitivity of DNA test exceeded FIT by 20%• Difference attributed to the DNA markers and
algorithm components of the test• Both tests hemoglobin component were =• FIT was more specific in detecting CRC by 6-8%

Sensitivity
• Most important characteristic for screening tests
• Primary role to rule out cancer• DNA test exceeded that of FIT in sensitivity• A negative result on DNA testing reduced the
chance of having CRC to a greater extent than a negative result on FIT

Specificity
• Also very important• Affects the number of people who have a
positive result• A majority of the number with a false positive
would be due to the low prevalence of cancer• The specificity of FIT was superior to the DNA
test
Specificity and false positivity
• Specificity of FIT 94.9-96.4% • False positivity of FIT 3.6%-5.1%• Specificity of DNA test 86.6-89.8%• False positivity of DNA test 10.2-13.4%

Two points regarding the specificity of DNA testing
• The analysis of specificity included those with non advanced adenomas
• These could cause a positive DNA test• But a negative colonoscopy• Among patients with a negative colonoscopy
the specificity was 90%• FIT was still superior at > 96%

Second point
• Specificity correlated inversely with age• Among patients with findings other than
advanced neoplasia:• Specificity of 91.5% for ages 50-64 yo• Specificity of 83.7% for ages 65 yo and older• But patients 50-64 yo with a negative
colonoscopy the specificity was 94% and similar to that of FIT

Second point
• Age related variation in specificity could be due to missed lesions on colonoscopy
• These are more prevalent among those over 70
• This could also be due to age related DNA methylation

Conclusions
• In asymptomatic persons at average risk for colorectal cancer, multitarget stool DNA testing detected significantly more cancers with a higher sensitivity than did FIT but had more false positive results and a lower specificity.





