
1
Identification of Priority Policy Research
Questions in the area of Access to and Use of
Medicines in EMRO Countries:
Focusing on Iran, Pakistan and Lebanon
Project team for the Eastern Mediterranean Region:
Arash Rashidian1, Shehla Zaidi
2, Samer Jabbour
3, Fatemeh
Soleymani1, Nader Jahanmehr
1
1 Tehran University of Medical Sciences
2 Aga Khan University Karachi
3 American University of Beirut
Funded by:
The Alliance for Health Policy and Systems Research
Access to Medicines Policy Research
July 2011

2
Identification of Priority Policy Research Questions in the
area of Access to and Use of Medicines in EMRO Countries:
Focusing on Iran, Pakistan and Lebanon
Country specific teams:
Iran: Arash Rashidian, Nader Jahanmehr, Fatemeh
Soleymani, Rasoul Dinarvand
Pakistan: Shehla Zaidi, Noureen Nishtar
Lebanon: Samer Jabbour, Rouham Yamout and colleagues

3
Contents 1
Abstract ..............................................................................................................................10
Executive summary..........................................................................................................12
Background and objectives .............................................................................................16
Goal, purpose and objectives .....................................................................................18
General Objective: ........................................................................................................18
Objectives: .....................................................................................................................18
Methods ..............................................................................................................................20
Literature reviews .........................................................................................................20
Search strategy – regional literature .....................................................................20
Search for Iranian literature in Farsi (Persian) .....................................................23
Previous research priority setting in Iran ..............................................................24
Search Strategy and literature review - Pakistan ................................................24
Search strategy and literature review - Lebanon ................................................28
Inclusion process and criteria and data extraction .................................................31
Data extraction tool ..................................................................................................32
Qualitative interviews ..................................................................................................34
Key informant interviews – Iran and the region ..................................................34
Key informant Interviews - Pakistan......................................................................37
Key informant interviews - Lebanon ......................................................................38
Consensus development ..............................................................................................42
Consensus development - Iran ...............................................................................42
Consensus development - Pakistan .......................................................................45
Consensus development and priority research questions - Lebanon ...............46
Results – literature review – country cases studies ...................................................50
Literature review - Iran ...............................................................................................52
Literature review, papers locally published in Iran and grey literature ...........52
Literature review, papers published from Iran in international journals .........58
Literature review - Pakistan ........................................................................................64
RATIONAL USE OF MEDICINES IN PAKISTAN ......................................................64
AFFORDABILITY & FINANCING ...............................................................................69
RELIABLE HEALTH SYSTEMS ...................................................................................71

4
Regulation: Licensing, Registration, Pricing, and Quality Control ....................80
Literature review - Lebanon ........................................................................................85
Journal articles ...........................................................................................................85
Published and unpublished documents and gray literature ...............................88
Research questions emanating from the literature review ................................91
Results - Literature on access to medicines issues in the EMR area .......................93
Producing the evidence: number and geographical distribution of countries of
origins of the identified publications ..........................................................................93
Countries of focus and ATM issues of focus .............................................................96
Limitations of the regional literature review .......................................................... 104
Access to medicine as a research priority: still a Cinderella topic? ....................... 106
Policy maker attention to ATM research ................................................................. 106
Researcher and research funder attention to ATM research ............................... 108
Results – qualitative interviews ................................................................................... 114
Key informant interviews, Iran and the region ..................................................... 114
Key informant interviews, Pakistan ......................................................................... 130
Key informant interviews, Lebanon ......................................................................... 135
Policy concerns ........................................................................................................ 135
General points .......................................................................................................... 135
Thematic analysis .................................................................................................... 137
Research questions emanating from key informant interviews ...................... 140
Results – qualitative interviews, EMRO region ...................................................... 141
Priority research areas for ATM – findings and consensus ...................................... 142
Consensus development on research priorities - Iran.......................................... 142
Consensus development on research priorities - Pakistan .................................. 147
Consensus development on research priorities - Lebanon .................................. 159
Conclusions ...................................................................................................................... 160
Acknowledgements ........................................................................................................ 163
References – regional study ......................................................................................... 164
Reference list. List of EMR region literature on ATM issues ................................ 170
References: list of Journal articles – Lebanon ....................................................... 188
Pakistan references .................................................................................................... 191
Appendices ...................................................................................................................... 196

5
Pharmaceutical system in Iran ................................................................................. 196
Pakistan country profile ............................................................................................. 207
Key informant interview rsources ............................................................................ 209
Interview guide for regional experts .................................................................... 209
Interview guide in Farsi .......................................................................................... 213
Interviewee invitation letter for regional experts .............................................. 217
Thematic framework – in Farsi ............................................................................. 218
Appendix : Search strategies for Lebanon .......................................................... 222
Interview guide (modified after the guide provided by Dr. Arash Rashidian et
al) ............................................................................................................................... 225
Access to Medicines list of research priority topics by the level of barriers to
ATM ............................................................................................................................... 228
Research questions emanating from literature review - Lebanon...................... 239
Research questions emanating From key informant interviews - Lebanon ...... 242

6
Table of figures
Figure 1. Improving Access to Essential Medicines: A Framework for Collective
Action in Line with Millennium Development Goals* ...................................... 20
Figure 3. Research Study Selection Diagram - Pakistan .................................... 26
Figure 2. Mapping of key stakeholders in Pakistan .......................................... 37
Figure 4: Flow chart of search strategies in electronic databases for ATM ....... 51
Figure 5. ATM issue categorization for papers published in Iran's journals. ..... 54
Figure 6. Growth in ADR reporting in Iran. Figure reproduced using Cheraghali
et al 2003 data. ................................................................................................ 57
Figure 7. An increasing trend: ATM papers on Iran published in local Farsi
(Persian) journals and international English language journals. ....................... 59
Figure 8. Percentage of patients receiving antibiotics. ..................................... 65
Figure 9. Number of medicines per prescription .............................................. 67
Figure 10. Percentage of patients receiving injections ..................................... 68
Figure 11. Share of Total Pharmaceutical Expenditure in Total Health
Expenditure ..................................................................................................... 69
Figure 12. Share of Public and Private Sectors in Total Pharmaceutical
Expenditure ..................................................................................................... 70
Figure 13. Distribution of the country of origin of publications for access to
medicines issues in the EMR ............................................................................ 94
Figure 14. The number of ATM publications per year. Note that 2011 covers
only the first half of this year. .......................................................................... 95
Figure 15. The number of publications discussing AT issues in EMR's low and
middle countries .............................................................................................. 97
Figure 16. Proportion of publications discussing each ATM issue in EMR
countries .......................................................................................................... 97

7
Figure 17. Distribution of ATM issues discussed, and the level of barriers
considered in publications: Iran, Jordan, Lebanon, Pakistan and Sudan. ....... 100
Figure 18. Medicines affordability in Iran, in comparison with other countries
(source: WHO, the World Medicines Situation Report – 2011). ..................... 108
Figure 19. The percentage of prescriptions containing antimicrobials or
injectable medicines. Source: The National Committee of Rational Drug Use in
Iran 2010........................................................................................................ 198
Figure 20. Items per prescription in 2006 – a provincial comparison. ............ 199
Figure 21. National trend in mean items per prescription. 1998-2010 ........... 199
Figure 22. The first pharmacy established in Birjand in 1933, eastern Iran. The
pharmacy is still active. Photo © Arash Rashidian, 2010. ............................... 206

8
Table of tables
Table 1. Search strategy for regional literature ................................................ 22
Table 2. Data extraction tool ............................................................................ 33
Table 3. Key informants' matrix: The interviewees are selected from the
following categories in Iran and in the region. ................................................. 35
Table 4. The main categories for the identification of research priorities ........ 44
Table 5. An example of the consensus development tool ................................ 44
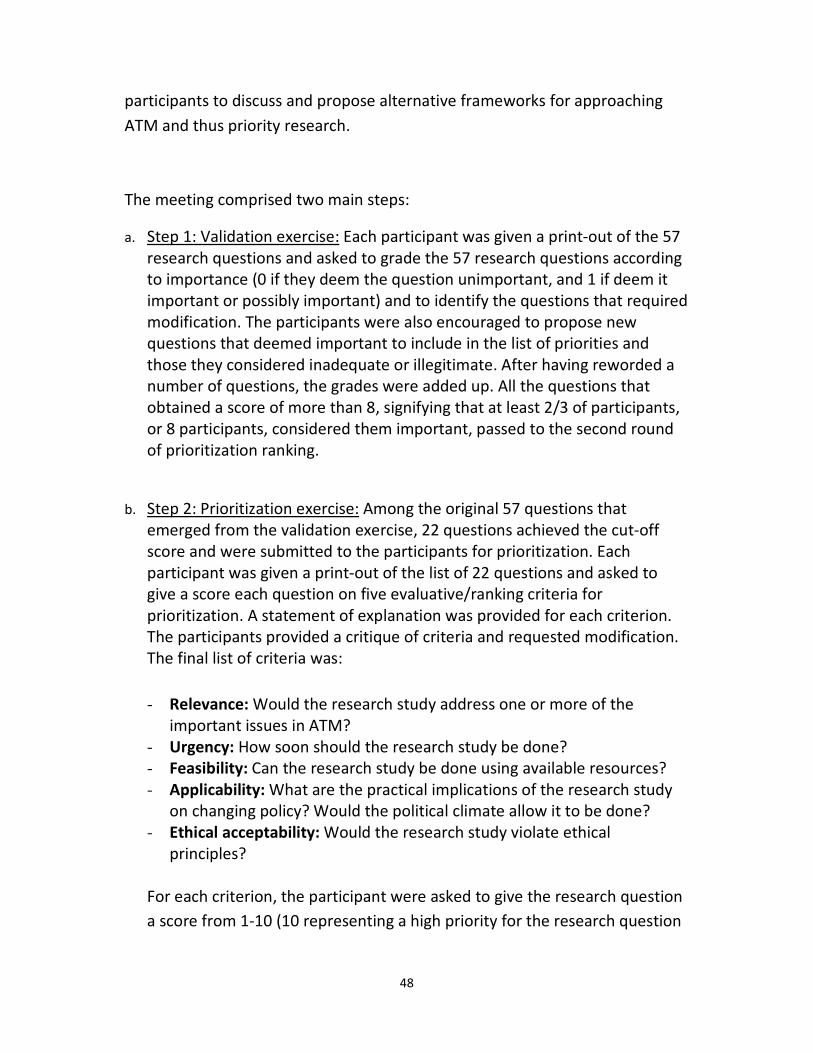
Table 6. Distribution of papers published annually in Iran's Farsi (Persian)
language scientific journals and the categorization of ATM issues and levels of
barriers discussed. ........................................................................................... 55
Table 7. Provincial or national distribution of issues covered in papers
published in Iran's Farsi (Persian) language scientific journals and the
categorization of ATM issues and levels of barriers discussed. ........................ 56
Table 8. Annual a growth in the number of ATM papers from Iran in
international literature, and the distribution of issues covered and the levels of
barriers discussed ............................................................................................ 60
Table 9. A more detailed analysis of research papers published on ATM in Iran
in local and international literature ................................................................. 61
Table 10. Level of Dissatisfaction with Public Sector and Underlying Reasons . 71
Table 11. Medicine Availability at Public Facilities and Private Pharmacies ..... 72
Table 12. 171717
Availability of Medicines in Percentage of BHUs and RHCs ....... 72
Table 13. Availability of Different Medicines in THQHs and DHQHs ................. 74
Table 14. Median MPRs for innovator brands and lowest priced generics in the
public (procurement only) and private sector (patient price only) ................... 75
Table 15. Availability of Essential Drugs and Vaccines: Comparison between
Contracted and Non-Contracted BHUs ............................................................ 77
Table 16. Areas Covered by National Medicines Policy .................................... 80

9
Table 17. ATM issues discussed each year in EMR publications ....................... 98
Table 18. The level of barriers studied in EMR publications each year ............. 99
Table 19. Ten agreed criteria for research priority setting (Pharmaceutical
Sector Research Network). ............................................................................ 110
Table 20. Twenty high priority research topics for pharmaceutical sector,
developed by the Pharmaceutical Sector Research Network. ........................ 112
Table 21. Conceptual thematic framework from Iran and regional data –
qualitative analyses and policy concerns ....................................................... 115
Table 22. Iran ATM research priorities. The results of the consensus
development meeting .................................................................................... 143
10
Abstract
Background
The provision of reliable access to affordable, appropriate and high-quality
medicines is a key component of a functioning health system. Access to
medicines needs to be fully integrated with health financing, human resource
planning, service delivery, information and governance systems. We aimed to
identify the policy concerns and related policy research questions in the field
of access to and use of medicines in low and middles income countries (LMICs)
within the Eastern Mediterranean Region (EMR) of the WHO, while focusing on
such issues in Iran, Lebanon and Pakistan.
Methods
Three closely linked teams conducted the studies. The teams conducted
systematic search strategies of international databases, country specific
databases and also search the grey literature to identify country specific and
regional literature on ATM.
A total of seventy key informant interviews were conducted. The interviews
were recorded and transcribed and were subsequently analyzed using
conceptual frameworks developed based on the ATM concepts and regional
and country level concerns.
Consensus development approaches used formal consensus development
methods (in two countries) and focus group discussions (in one country) for
the identification of the research priorities. Then the final outcomes of
different studies (three country case studies and regional study) were collated
with each other.
Main findings
Almost 80% of AT research in the region is originating from the region. While
there is a wide variation in the number of publications originating from
different countries. Conceptual frameworks of policy concerns and research
priority lists for use in the region were developed. The main concerns of the
key informants were around the affordability and financing aspects of access

11
to medicines, followed by issues of availability and rational use of medicines.
The key informants paid attention to all levels of barriers to access: the
household level, providers (public or private sector), health system, other
sectors and cross border issues. The identified previous research on the issue,
however, did not reflect that. ATM research in the region is heavily biased
towards RUD.
Conclusions
The picture of research on the ATM in the region is better than what had been
reported in recent publications. There is a growing trend, over the years, of
more and better quality studies from the region appearing in international
journals.
The majority of policy concerns were not addressed by published research. The
study clearly indicates that there is dire need for further research on financing
and affordability aspects of ATM in the region. Also cross-border issues and
other sectors roles on access to medicines in the region has not explored
widely. It seems that many household (demand side) studies in the region
remain of poor quality and limited methods. Together, these main areas
should provide the main aspects of access to medicines research in the region.
12
Executive summary
The provision of reliable access to affordable, appropriate and high-quality
medicines is a key component of a functioning health system. Access to
medicines needs to be fully integrated with health financing, human resource
planning, service delivery, information and governance systems. As part of the
Access to Medicines Policy Research project, funded by the WHO's Alliance for
Health Policy and Systems Research, studies are conducted in order to increase
access to and improve the use of medicines in low and middle income
countries, particularly for the poor (MDG 8). In this study we aimed to identify
the policy concerns and related policy research questions in the field of access
to and use of medicines in low and middles income countries (LMICs) within
the Eastern Mediterranean Region (EMR) of the WHO, while focusing on such
issues in Iran, Lebanon and Pakistan.
This is the first study conducted in this region that has collated published
literature and summarized the main policy concerns to identify ATM research
priorities. In this study we used an extensive search of local and regional
literature, interviews with key informants, analysis of previous priority setting
exercises and consensus development approaches to identify the main
research priorities for ATM research. We developed detailed maps of research
on the issue, conceptual frameworks of policy concerns and issues, and
identified lists of ATM research priorities for the countries of focus and the
region as a whole.
Three closely linked teams based at the Tehran University of Medical sciences
(Iran), the American University of Beirut (Lebanon) and the Aga Khan
University Karachi (Pakistan) conducted the studies. The teams conducted
systematic search strategies of international databases, country specific
databases and also search the grey literature to identify country specific and
regional literature on ATM. Then they collated essential data from the studies
13
using purposefully defined data extraction forms. The teams used the
conceptual framework developed by the WHO and the AHPSR for ATM for data
extraction and analysis. Additional to this an analysis of previous research
priority setting exercises was conducted in one country to see how much
attention has been devoted in the past to research priorities relevant to ATM
issues.
The teams conducted a total of seventy key informant interviews across the
region. The interviews were conducted following a pre-defined semi-
structured interview guide. The interviews were recorded and transcribed and
were subsequently analyzed using conceptual frameworks developed based on
the ATM concepts and regional and country level concerns.
Consensus development approaches followed different approaches. In two
countries formal consensus development methods (albeit with variation in
tools deployed) were used. In one country a focus group discussion approach
was followed for identification of the research priorities. Then the final
outcomes of different studies (three country case studies and regional study)
were collated with each other in one report.
The main concerns of the key informants were around the affordability and
financing aspects of access to medicines, followed by issues of availability and
rational use of medicines. The key informants paid attention to all levels of
barriers to access: the household level, providers (public or private sector),
health system, other sectors and cross border issues. The identified previous
research on the issue, however, did not reflect that.
The results of the study indicate that ATM research in the region is heavily
biased towards RUD. RUD research has been mainly in the shape of
prescription audits, the majority of it showing there are important problems in
prescriptions. In recent years there is shift towards interventional studies
assessing the impact of interventions on improving prescribing outcomes.
There are two important patterns to note in here. First, the RUD research,
although forming the majority of ATM research is yet to show a substantial
effect in improving drug utilization patterns. The prescribing problems of focus
in ten years ago remain unresolved today, if not joined by new challenges (e.g.
non-generic prescribing). Second, it seems a change in research strategies is

14
required and future studies should focus on interventional issues. Fortunately
there is a move in that direction. Also further demand side (why public still
sees fascinated with antibiotics) and health systems angle (what are the
financial and organizational barriers to improving prescribing patterns)
research will be required.
This study clearly indicates that there is dire need for further research on
financing and affordability aspects of ATM in the region. This should be given
paramount attention in future research funding and calls for proposals. Also
cross-border issues and other sectors roles on access to medicines in the
region has not explored widely. It seems that many household (demand side)
studies in the region remain of poor quality and limited methods. Together,
these main areas should provide the main aspects of access to medicines
research in the region.
This is in no way indicating that further RUD or studies of health systems and
availability access are not needed. Or that the barriers at the levels of
providers and health systems are exhaustively identified. Rather it seems that
individual researchers and available funding route are giving attention to these
issues at the moment, which should continue while further resources should
be mobilized for studies related to the relatively ignored aspects of ATM
research in the region.
Almost 80% of AT research in the region is originating from the region.
However, there is a wide variation in the number of publications originating
from different countries. Certain countries (e.g. Somalia), or certain areas of
other countries, do not appear in the literature.
The picture of research on the ATM in the region is better than what had been
reported in recent publications that had not followed extensive
methodologies. There is a growing trend, over the years, of more and better
quality studies from the region appearing in international journals. Still, a
concurrent trend will be required to ensure the local audience of such research
(i.e. practitioners, policy makers and media) remains informed of the new
development as a result of ATM research in countries in the region. An active
knowledge translation approach will be essential.

15
Finally, the key informant interviews clearly demonstrate that the majority of
policy concerns were not addressed by published research. There was a
mismatch between the concerns and research, and hence the outcomes of this
study can contribute to developing a research agenda for improving access to
and appropriate use of medicines in the region and the three countries of
focus.
16
Background and objectives
The provision of reliable access to affordable, appropriate and high-quality
medicines is a key component of a functioning health system1. Access to
medicines needs to be fully integrated with health financing, human resource
planning, service delivery, information and governance systems.
Prescribing costs have been growing 6-8% per year in the global context (Le
Grand et al, 1999). In Australia in one year prescribing costs rose more than
23% (Beilby and Silagy, 1997), and in the USA the prescribing expenditure
increased thirteen-fold in only thirty years from 1960-1990 (Pippalla et al,
1995). GP prescribing amounts to over 10% of total Britain's NHS spending and
it is estimated that about 75% of visits to office-based doctors end up in
prescribing. Therefore, focusing on quality and cost of prescribing is important
and vital.
The WHO refers to the ideal state of prescribing, distribution and use of drugs
as ‘rational drug use’ and has provided this definition:
The rational use of drugs requires that patients receive medications
appropriate to their clinical needs, in doses that meet their own
individual requirements for an adequate period of time, and at the
lowest cost to them and their community; WHO conference of experts
Nairobi 1985.
Irrational use of drugs (including not using medicines when needed) occurs for
a variety of reasons. Appropriately prescribed medicines may be used
inappropriately. Patients may not use the specified doses of medicines in
appropriate intervals or for prescribed durations. In many LMICs countries
pharmacies dispense a range of drugs without physician (or other clinician)
prescription. It is also part of another problem which is self-medication. In
1 WHO 2007 Framework for Action for Strengthening Health Systems: Everybody's Business -
http://www.who.int/healthsystems/topics/en/index.htm

17
countries where the medicines market is not adequately regulated, patients
may decide on what they need and obtain it freely from dispensers. The
problem of irrational use of drugs may be the result of system failure.
Inadequate financial support for patients with chronic or serious infectious
diseases and substantial co-payments put disadvantaged groups in
unfavourable situation in terms of access to drugs. Also lack of availability of
medicines and the problem of counterfeit drugs complicate the picture in
LMIC. We may also add the issues of low uptake of clinical practice guidelines,
limited use of local formularies, weak implementation of essential drug
programmes and a variety of other issues to the picture.
Access to and appropriate use of medicines is often poor in low and middle
income countries (LMICs). WHO estimates that the average availability of
essential drugs in LMICs is 35% in public sector facilities and 66% in the private
sector.2 Medicines account for a high proportion of health spending in LMICs,
between 20% – 60% (developed country spending is around 18%).3 Moreover,
between 50% - 90% of expenditure on medicines in LMICs is out-of-pocket.4
This inequitable mode of financing creates significant access barriers for the
poor and/or may lead to catastrophic household expenditures. The poor as
well as other population groups often rely on the private informal sector for
medicines, particularly in rural areas. Over and inappropriate prescription and
dispensing of medicines are prevalent5.
Despite some progress in some areas - such as price and availability -6 , data on
access to and use of medicines is often weak. Even where data are available,
there is limited contextual evidence and analysis to assist in interpretation or
in the development of policy options to improve access to medicines in
different health systems and country settings, especially for LMICs. Health
2 MDG Gap Taskforce Report (2008): Delivering on the Global Partnership for Achieving he Millennium Development Goals.
3 Cameron et al (2009): Medicines prices, availability and affordability in 36 developing and middle income countries: a
secondary analysis.. Lancet 2009; 373: 240–49 4 WHO (2004)::WHO Medicines Strategy: 2004 – 2007. Countries at the Core’
5 WHO (2008): Medicines use in primary care in developing and transitional countries: fact book summarising results from
studies reported between 1990 and 2006. 6 Data on medicines prices, availability and affordability from WHO-HAI medicines price and availability surveys is now
available for more than 36 countries. See: Cameron, A et al (200): Medicine prices, availability, and affordability in 36 developing and middle-income countries: a secondary analysis. Lancet 2009; 373: 240–49

18
Systems Research (HSR) is essential to understanding, planning, monitoring
and evaluating the interaction of health system components in delivering
health outcomes efficiently. The importance of health systems research was
confirmed by the High Level Forum task team report at the Global Ministerial
Forum on Research for Health in Bamako in 2008.7 The application of HSR tools
and methods in the field of Access to Medicines will help understand the
weaknesses of this building block and generate and use adequate evidence to
formulate policies.
Goal, purpose and objectives
The goal of the Access to Medicines Policy Research project is to increase
access to and improve the use of medicines in low and middle income
countries, particularly for the poor (MDG 8).
The purpose of this project is to increase the use of evidence in policies to
improve access to and use of medicines in LMICs, focusing on EMRO region as
well as country specific issues in Iran, Pakistan and Lebanon.
General Objective:
Identification of policy concerns and related policy research questions in the
field of access to and use of medicines.
Objectives:
• Identify to the extent possible, regional level policy concerns related
to access to and use of medicines, as perceived by policy makers, civil
society organizations and patients and communities
• Identify and rank, to the extent possible, related policy research
questions in the field of access to and use of medicines in EMRO
region as a whole and in Iran, Pakistan and Lebanon specifically.
7 WHO (2009): Scaling up Research and Learning for Health Systems: Now is the Time.

19

20
Methods
The WHO Framework for Access to Medicine (WHO 2002) was used as the basis for data collection and synthesis. Under this framework accessibility has been defined as having four parameters: that the available medicines are effective and of consistently good quality, that there is no financial obstacle to a patient receiving it, and that required knowledge and guidance are available for proper use of these medicines Any isolated effort to improve one
part may be effective for that part but it would not improve the overall situation.
Figure 1. Improving Access to Essential Medicines: A Framework for Collective Action in Line with Millennium Development Goals*
*Source: Richard Laing, Improving Access to Child Health Medicines, Review and
Discussion Paper, WHO Regional and Country Child Health Advisers, Geneva, 2002
Literature reviews
Search strategy – regional literature
For the extraction of research priorities of barriers to drug access in the EMRO
region, we employed two sets of search strategies: general search for regional
literature, and specific searches for the three countries (Iran, Pakistan and
Lebanon).
1. Rational
Drug Use
4. Reliable
Health Systems
2. Affordable
Prices
3. Sustainable
Financing
ACCES

21
General regional search
In Latin sector two major electronic databases- PubMed and SSCI and SCI (ISI
Thompson) - were systematically searched, using a search strategy that we
carefully designed and tested (Table 1).
The PubMed electronic search identified the sixteen low and middle income
countries (according to the World Bank categories) of the WHO's Eastern
Mediterranean Region. The country specific searches were conduced both in
affiliations as well as the titles and abstracts of the papers.
The specific ATM terms were developed in two brainstorming meetings and
then were used for devising the search strategy. The search strategy was applied
and tested in a number of limited searches. Then a full search was conducted
and compared against a country specific list of entries. The results of the
assessment was used to revised and conduct the final search (Table 1).
The main terms selected for this study were drug, medicine, medication and
pharmaceutical and their variations are suitably linked with the terms: use,
access, availability, affordability, utilization, pricing, licensing etc and their
variations. Also certain specific terms were included in the search on their own
(e.g. pharmacy, prescribing). Early searches were conducted in January 2011
and were updated in June 2011.
Moreover, we hand-searched the Journal of Southern Medicine, yielding three
relevant articles. We also looked for relevant WHO reports (regional and
global), and especially the WHO reports of the World Medicine Situation in
2011 were used in this study.

22
Table 1. Search strategy for regional literature Pubmed example:
#1- ((((((((((((((((iran[Affiliation]) OR pakistan[Affiliation]) OR lebanon[Affiliation]) OR
Egypt[Affiliation]) OR Afghanistan[Affiliation]) OR Sudan[Affiliation]) OR Yemen[Affiliation])
OR Jordan[Affiliation]) OR Tunisia[Affiliation]) OR Morocco[Affiliation]) OR Syria[Affiliation])
OR Palestine[Affiliation]) OR Iraq [Affiliation]) OR Djibouti[Affiliation]) OR Libya$[Affiliation])
OR Somalia[Affiliation])
#2- ((((((((((((((((((((middle east[Title/Abstract]) OR Iran[Title/Abstract]) OR
Tehran[Title/Abstract]) OR low income countries[Title/Abstract]) OR middle income
countries[Title/Abstract]) OR Pakistan[Title/Abstract]) OR Lebanon[Title/Abstract]) OR
Egypt[Title/Abstract]) OR Afghanistan[Title/Abstract]) OR Sudan[Title/Abstract]) OR
Yemen[Title/Abstract]) OR Jordan[Title/Abstract]) OR Tunisia[Title/Abstract]) OR
Morocco[Title/Abstract]) OR EMRO[Title/Abstract]) OR Syria[Title/Abstract]) OR
Palestine[Title/Abstract]) OR eastern Mediterranean[Title/Abstract]) OR Iraq
[Title/Abstract]) OR Djibouti[Title/Abstract]) OR Libya$[Title/Abstract]) OR
Somalia[Title/Abstract])
#3- (#1) OR (#2)
#4- ((((drug$[Title/Abstract]) OR medicines[Title/Abstract]) OR medication$[Title/Abstract])
OR pharmac$[Title/Abstract])
#5- ((((((((((((((((((use[Title/Abstract]) OR access[Title/Abstract]) OR available[Title/Abstract])
OR availability[Title/Abstract]) OR affordable[Title/Abstract]) OR
affordability[Title/Abstract]) OR utilisation[Title/Abstract]) OR utilization[Title/Abstract]) OR
essential [Title/Abstract]) OR counterfeit$[Title/Abstract]) OR price[Title/Abstract]) OR
pricing[Title/Abstract]) OR licensing[Title/Abstract]) OR licencing[Title/Abstract]) OR
labeling[Title/Abstract]) OR labelling[Title/Abstract]) OR formularies[Title/Abstract]) OR
generic[Title/Abstract])
#6- ((((((((prescription$ [Title/Abstract]) OR prescrib$ [Title/Abstract]) OR "drug
policy"[Title/Abstract]) OR "pharmaceutical policy"[Title/Abstract]) OR
formulary[Title/Abstract]) OR pharmacy[Title/Abstract]) OR pharmacies[Title/Abstract]) OR
pharmacist$[Title/Abstract])
#7- (#3) AND (#6)
#8- (#3) AND (#4) AND (#5)
#9- (#7) OR (#8)
23
Search for Iranian literature in Farsi (Persian)
We used the general regional search strategy for retrieving Iran's literature in
English. This is restrictive, as there are Iranian publications in English indexed
in other databases. However it provided a comparative coverage of Iran's
literature, in the context of regional publications.
We searched for scientific publications in Farsi languages using the following
approaches:
1. Systematic searches in specifically designed electronic databases, including
IranMedex and the SID.
2. Searching the grey literature, including student dissertations (at two major
academic libraries) and review of the documents and records of Iran's Ministry
of Health and Medical Education.
The Persian resources – IranMedex and SID – are not yet suitable for systematic
searches as the one described in Table 1. Hence we conducted a very simple and
sensitive search (that is we searched for the word 'medicine' دارو in the title).
Over 700 papers were identified. After reviewing the titles and abstracts, 34
related publications considered relevant and of them were retrieved for full text
assessment and data extraction.
We also searched Farsi theses and dissertations in the libraries of two major
schools: the School of Pharmacy and the School of Public Health of the Tehran
University of Medical Sciences, which yielded eight relevant theses. By hand-
searching in documents and records in the Iranian Ministry of Health we found
150 records and five articles entered final analysis.

24
Previous research priority setting in Iran
We also searched for, and conceptually analyzed some previous research
priority activities in the country. We used this to see how much attention has
been devoted in the past to ATM, and to identify potential topics for research
priority.
Search Strategy and literature review - Pakistan
Desk Review: This involved published studies, unpublished studies and grey
literature such as commissioned reports and surveys. A total of 11706 titles
were yielded using the electronic search and reference from bibliographies.
These were sifted by 2 researchers for identification of relevant studies. A total
of 184 studies were shortlisted. Abstracts and report summaries of 184 studies
were reviewed and a total of 96 studies were further short-listed. The full text
of all these 96 studies, including articles, reports, presentations and books was
then reviewed and 92 studies were selected and uploaded into EndNote
In addition 19 policy documents were also included through a system involving
online search as well as opinion taken from experts. Identification and access
to other policy documents that are not in public domain were sought during
stakeholder interviews. Data from each reviewed study and policy documents
was systematically extracted and analyzed using grids based on the WHO
Access to Medicines Framework under the four domains of rational use,
affordability, financing, and reliable health systems. Details of search strategy
and analysis of desk review is presented in Annex.
The scope of the search includes identification of relevant research, policy and
programmatic documents. A systematic wide scoped search was conducted
looking into published and unpublished documents. This primarily involved a
desk review but was assisted by key informant interviews.
Sources included a range of both peer reviewed electronic databases such as
Pubmed, Cochrane, Cinahl as well other unpublished databases such as
WHOLIS, ELDIS and Google Scholar. We also reviewed bibliographies of all
selected articles. A combination of search terms was applied to yield a
sufficiently large number of studies for detailed analysis. Search terms were
carefully selected, keeping in mind the objective of the study. Five sets of

25
search terms were used Drugs Pakistan; Drugs Pakistan Affordability; Drugs
Pakistan Rational Use; Drugs Pakistan Financing; and Drugs Pakistan Health
System.
The following inclusion criteria were applied:
1. Studies reporting on Pakistan, whether Pakistan only studies or multiple
country studies inclusive of Pakistan.
2. Studies published 1990 onwards.
3. Studies on bio-efficacy of drugs were excluded.
4. Commentary articles were excluded with inclusion restricted to primary
research, systemic reviews and reviews supported by research data.
A total of 11706 titles were yielded using the electronic search and reference
from bibliographies. These were sifted by 2 researchers for identification of
relevant studies. A total of 184 studies were shortlisted. Abstracts and report
summaries of 184 studies were reviewed and a total of 96 studies were further
short-listed. The full text of all these 96 studies, including articles, reports and
books was then reviewed, of which 4 were found to be irrelevant and a total of
92 studies were selected and uploaded into EndNote (List attached). Diagram 1
shows the study identification process and yielded results.

26
Figure 2. Research Study Selection Diagram - Pakistan
Policy and Programmatic Documents: For policy and programmatic documents
an online search was conducted as well as opinion taken from experts. Online
search was conducted of websites of the Ministry of health, provincial
Departments of Health, WHO Pakistan, WHO-EMRO and Pakistan Consumer
Protection Network on Rational Use of Drugs and Google Scholar. These
yielded a total of 15 documents. Identification and access to other policy
documents that are not in public domain were sought during stakeholder
interviews and yielded another 4 policy documents. Presently we have a total
of 19 policy documents (List attached).
Data Extraction Strategy: Data from each reviewed study and policy
documents was systematically extracted and analyzed. The WHO access to
medicines framework identifying type and level of barrier to access to
medicines (WHO 2004)i was used as a guideline for extraction of data. Findings
from were categorized under four grids as under:
11706 titles yielded in
the initial search
Stage 1
184 abstracts were
shortlisted and reviewed n=
184
120 were excluded:
duplicates,
commentaries, drug
efficacy studies
Stage 2
96 abstracts were
shortlisted, reviewed and
screened
Stage 3
n=
96
4 were excluded:
because those were
irrelevant
Full texts of 92
publications were
reviewed &
Stage 4
n=
92

27
1. Rationale Use of Drugs in Pakistan
2. Reliable Health System in Pakistan
3. Sustainable Financing of Drugs in Pakistan
4. Affordability of Drugs in Pakistan
Each grid in turn slotted information on:
• study title,
• author,
• study year,
• source,
• type of publication,
• level of barrier,
• methodology,
• key findings,
• identified issues & challenges (See attached).
During review of study, notable findings were highlighted. Findings from each
study were categorized into the relevant grid/s and within each grid into the
relevant sections. A narrative synthesis is also provided on barriers to access
based on the systematic organization of retrieved information.
All the above mentioned documents were analyzed systematically using
different grids employing World Health Organization Access to Medicines
Framework for Essential Medicines for this purpose8.
8 WHO Policy Perspectives on Medicines, March 2004. Equitable access to essential medicines: a framework for
collective action

28
Search strategy and literature review - Lebanon
The research team has developed a multi-pronged and comprehensive search
strategy to identify published journal articles and documents as well as
unpublished (gray) documents. The strategy focuses on identifying publications
and documents in several categories (listed below). Documents within each of
the following categories were sought. Documents were considered of interest
to this research if they focused on issues of ATM, discussed ATM in one or
more part of the document, or discussed issues of direct relevance to ATM.
− Peer-reviewed journal articles identified through a search of multiple
databases.
− Documents of the Lebanese parliament, the Government of Lebanon, the
MoPH, of ministries and of governmental agencies other than MoPH
− Publications and documents of the WHO, WHO/EMRO in Cairo or WHO
country office in Lebanon
− Publications and documents of other international agencies (e.g. UNDP,
UNICEF, World Bank)
− Books on devoted to one or more aspects of ATM in the Arab world, MENA,
EMR or Lebanon
− Books on health systems or public health in the Arab world, EMR, MENA, or
Lebanon where ATM is discussed
− Reports and studies about the pharmaceutical industry or market in
Lebanon
− Other publications, for example as identified by key informants.
In addition to improving our understanding the issues of and surrounding ATM
in Lebanon, the purpose of the search strategy was to create a mini-library of
documents of interest to ATM which can aid future research on ATM in
Lebanon.
Journal articles
The TUMS-based research team was responsible for identifying ATM-specific
journal articles from EMR countries and has followed a consistent search

29
strategy in PubMed to identify journal articles published in English for each
country (see the PubMed search strategy for Lebanon in Appendix 1-A).9 As
this did not seem to represent the body of potentially-relevant literature on
ATM in Lebanon, the Lebanon team felt the need to expand the search
strategy and use multiple databases to retrieve a larger number of articles.
Although it was obvious that this approach might reduce the specificity of the
search strategy, the rationale was that the conceptual framework of ATM, for
example according to WHO 2004, is quite broad and encompassing and many
articles, even if not specific to ATM, can enlighten a better understanding of
the health system issues of direct relevance to ATM. The research team
developed an expanded MeSH terms/keyword list to capture more domains of
the ATM framework (according to WHO 2004) and conducted a systematic
review using the following electronic databases: PUBMED/MEDLINE, EMBASE,
SCIRUS, IMEMR (WHO EMRO’s Index Medicus for the Eastern Mediterranean
Region), and Google Scholar. We reviewed abstracts and excluded irrelevant
articles. For Google Scholar, we searched the first 13 pages of around 36,000
articles obtained. For each step of literature search we retained articles that
have not been found during a previous search to avoid redundancy in the list.
In addition to the aforementioned search strategy, we attempted to identify
additional journal articles by searching the following national resources: The
National Health Information Library, supported by the WHO country office in
Lebanon, and the online database of the Lebanese Corner at the Saab Medical
Library of the American University of Beirut, a resource on all health-related
publications concerning Lebanon.
Document review
To identify documents, whether published or unpublished, of interest to ATM
we carried out a multi-pronged strategy. We searched websites (e.g. MOPH,
WHO-EMRO), databases (WHO Medicines Bookshelf version 6 [2010],
Lebanese Corner at the Saab Medical Library of the American University of
Beirut), and other national resources (e.g. the National Health Information
9 The regional search strategy was later revised. The final regional search strategy can be identified in Table 1.

30
Library of the WHO country office in Lebanon). This led us to identify only a
limited number of documents. In addition, we asked key informants to supply
us with any documents of potential interest to ATM. Key informants supplied
the research team with a large number of documents covering a broad range
of topics.

31
Inclusion process and criteria and data extraction
Papers published from 2000 onward were considered for further analysis. All
the titles and the abstracts of the identified papers via the search were
reviewed by one investigator. To insure accuracy, two separated samples of
the papers were reviewed by two authors and disagreements were discussed
and clarified.
Inclusion and exclusion of the papers followed the following criteria:
• Studies that were directly relevant to access to medicine concepts were
included. For example, for RUD studies, we focused on studies that
assessed the RUD in a certain setting, or the studies that have sought to
improve use of medicines specifically. However, studies of improving
clinical care (which might have involved prescribing issues) were not
included; a clinical practice guideline development project may not be
included. Although prescribing is part of the majority of the guidelines,
the purpose of a CPG is not prescribing per se, rather it is improving
quality of care. This criterion was required to ensure we remained
focused on ATM issues. The same logic was applied to the search results.
• Studies of drug resistance that did not elaborate on health system or
access to medicines implications of it were not included.
• Studies of herbal medicines alone were not included.
• Studies of drug abuse were not included.
• Contraceptive medicines use studies that were focused on family
planning issues were excluded.
• Letters to editors and abstract only publications were not included
• Studies focusing only on education methods and curriculum
development for pharmacy issues were not included.

32
After agreeing on inclusion of a study, the full texts of the studies were
retrieved as far as possible. All the identified studies were assessed to extract
the data required by the data extraction tool (Table 2). We extracted data on
title, authors, the year of publication, country of origin, countries of focus,
research design and sample, a summary of main findings, ATM issues
considered in the study, levels of barrier studies, and the research topics
recommended by the authors.
Data extraction tool
Then we collated the extracted data to develop a map of the literature as
pertaining to the study questions. We also used the research topics
recommended by the studies to identify the research priorities, and the maps
for focusing on what topics have been regularly researched in the region and
what topics remain in the Cinderella.

33
Table 2. Data extraction tool
number First
author title year
country (ies) in origin
Country (ies) in focus
Barriers to ATM
discussed? Y/N
Research design
and sample
Main findings
Issues considered (Y/N)
Level of barrier studied (Y/N)
Research topics recommended
affo
rda
bility
Su
sta
ina
ble
finan
cin
g
RU
D
Hea
lth s
yste
m a
nd
ava
ilab
ility
Ho
use
hold
& c
om
mu
nity
He
alth
serv
ice p
ub
lic o
r priv
ate
Natio
na
l He
alth
se
cto
r
Natio
na
l beyond
he
alth
se
cto
r
Cro
ss b
ord
er is
sue
s

34
Qualitative interviews
Key informant interviews – Iran and the region
Participants: We interviewed a purposeful sample of twenty participants. We
selected the sample purposefully. A list of stakeholders was developed in a two
step consultative process. A matrix was developed to categorize the
organizational background and settings from which the stakeholders would be
selected. These included WHO regional office, the ministries of health and their
entities, civil society organizations (as patient representatives), medical
associations (as clinician representatives), pharmacists associations (as
pharmacist representatives), research institutions, development partners etc (see
Table 3. Key informants' matrix: The interviewees are selected from the
following categories in Iran and in the region.). The participants were invited
by telephone calls or emails, explaining the objectives of the study and
introducing the investigators. The time, location and mode of the interviews
(telephone or face-to-face) were mutually agreed. The interviewees were paid
no honorarium.

35
Table 3. Key informants' matrix: The interviewees are selected from the following categories in Iran and in the region.
WHO and
other
sectors
Pharmaceutical
companies
Insurance
organizations
PHC
networks/
public
provision
of health
services
Ministry
of Health
Academics
in relevant
disciplines
Clinicians
/medical
institutions
Pharmacies
And
distribution
Patient
representatives
Interviewees
codes
* * KI10 * * KI15
* * * KI9
* * KI17 * * KI13 * KI3
* KI11
* KI1
* * KI2
* * KI4
* KI5
* KI6
* KI7
* KI8
* KI12
* KI14
* KI16
* K18
* K19
* K20

36
A semi structured questionnaire was developed using the general ATM structure
developed by the WHO and the Alliance. We updated this structure to form
broad questions. Then the structure was discussed in a meeting of investigators.
We then presented the interview structure to a meeting with regional
investigators and study advisers. In the end a three part interview guide was
developed (see Appendices). We shared the tool with colleagues in Pakistan and
Lebanon.
The first part was the introductory and intended to capture the general aspects of
the interviewees' background as educational level, affiliations and experiences.
The second was an open question about issues regarding access to medicines.
This part was meant to investigate the interviewees' personal opinions about the
access and use of medicines concepts. In the third part of the guide – which was
the main part – the interviewees were asked about different level of access
according to each component of the WHO/ATM framework (individual,
household and community level, health service delivery level- both public and
private services delivery channels, health sector policy, beyond the health
sector).
Interview analysis was done manually and the WHO 2002 Access to Medicine
Framework was taken as the conceptual framework for analysis.
Interviews:
Thirty individuals were invited to interviews and twenty three agreed to
participate. In the end twenty face-to-face and telephone interviews were
conducted in late 2010 and early 2011 (three other interviews did not in the end
result in mutually convenient time set ups for the interviews). Interviews, except
one, were tape recorded and transcribed, each interview lasting 30–45 min. Six
participants were female and 14 were male. We used thematic content analysis
approaches to analyze the data.

37
Key informant Interviews - Pakistan
21 in-depth interviews were conducted involving a diverse range of
stakeholders. Purposive sampling was done and the list of stakeholders was
developed in a 2 step consultative process. In a meeting of regional partners
at Tehran University a matrix was developed mapping major organizational
backgrounds for stakeholder selection across all the three participating EMRO
countries. These included MO and its entities, CSOs (as patients’
representatives), medical associations (as clinician representatives),
pharmacists associations (as pharmacists representatives), industry, research
institutions, development partners etc (see attached stakeholder matrix).
These would be consistent for all 3 countries but identification of specific
names and exact numbers would be done by country team. Subsequently a
meeting was held of Pakistan team with WHO Pakistan for identification of
specific interviewees under each organizational category.
Ethical approval was obtained prior to interviews. Written informed consent
was obtained from each interviewee and written project information and
contact details of investigators were provided. Written assurance was also
given of confidentiality of interviewee identity in making reference to
interview results. Interviews were conducted in Islamabad, Karachi and Lahore.
Interviews notes were taken by a two member team and transcribed and
compared between note takers on same day. Interview analysis was done
manually and the WHO 2002 Access to Medicine Framework was taken as the
conceptual framework for analysis.
Figure 3. Mapping of key stakeholders in Pakistan

38
Key informant interviews - Lebanon
The research team conducted in-depth interviews with 29 key informants
whose work directly concern ATM to solicit their views on the most important
policy and research issues concerning ATM.
Inclusion criteria
We initially identified 15 key informants as the target for interviews but ended
up conducting interviews with 29 informants, following the advice provided by
other informants. Although saturation in responses was reached after the first
15 interviews, the later set of interviews were useful in addressing specific
issues and in clarifying particular questions in ATM. We identified informants
whose work encompasses the various domains of ATM. In many cases,
informants served in multiple roles. For example, some informants served in
professional associations or NGOs but were also practitioners of medicine,
pharmacy or nursing. Some practitioners were also educators in their fields. A
key strategy in identification of key informants was to ensure diversity of
n= 184
39
professional backgrounds, fields of work, and perspectives. Informants came
from the public sector, the private sector, professional associations, civil
society groups/NGOs and consumer groups, and from among practitioners.
Appendix 2 presents the complete list of informants
Conduct of key informant interviews
Key informants identified based on the aforementioned criteria were called by
telephone or contacted by email to explore their interest in participating in the
study. If they expressed interest, we sent the consent form (Appendix 3) by
email, fax or delivered it in person and the WHO-2004 paper explaining the
ATM framework. On the interview day, informants were asked to go over the
consent document and encouraged to seek any clarification from the
investigator. Informants were then asked to complete the informed consent
document if they voluntarily agree to participate. Interviews were recorded on
a digital recorder and later transcribed. One to three members of the research
team conducted the interviews which lasted from 30 minutes to 90 minutes,
depending on informant’s time availability.
Informants were told that the interviewers would be exploring ATM in
Lebanon according to the WHO-2004 framework and that there will be an
attempt to cover the four domains of the ATM framework but that the
interview can expand well beyond that. For informants who seemed unfamiliar
with the terminology of ATM and the various domains of ATM framework, the
researcher briefly reviewed the WHO-2004 framework prior to the start of the
interview. It was felt that this allowed interviews to be more focused and allow
more productive use of time. The informants did not seem biased in particular
directions by this approach.
The interviews used loosely the ‘Semi-structured interview guide’ developed
by the research team at TUMS (Appendix 4). The researchers felt that the
interview guide, although comprehensive and useful, did not allow for the
flexibility and fluidity that informants demanded. Consequently, the interviews

40
were largely based on asking the informants about their views of which are the
most important policy concerns, and corresponding research questions, in
ATM and then moved to explore the ATM issues more in-depth using the leads
provided by the informants, the WHO 2004 framework and the semi-
structured interview guide. This method gave the informants the needed space
to move about the ATM sphere freely and gave the researchers the needed
structure to explore ATM issues from various angles.
The initial objective was to elicit from each informant a list of policy research
questions and priorities in the area of ATM. However, this proved difficult as
informants commonly focused on the policy aspect of ATM issues rather than
on identification of related research questions. In some cases, prodding by the
interviewing researcher proved useful in identifying specific research
questions. In other cases, this proved difficult and it became clear to the
researchers that they would need to identify research questions based on the
policy concerns expressed by informants.
Privacy and confidentiality
Several measures were taken to ensure the privacy and confidentiality of
informants. Consent forms lacked any personal identifiers. During the recoded
interviews, informants were asked not to provide any identifiers, such as
names or names of the institution or their positions. If such information was
provided, it was not transcribed or deleted from transcription. The recordings
were downloaded to a password-protected computer immediately after the
interviews and deleted from the digital voice recorder. Only one person of the
research team had access to the recording. Once successfully transcribed and
checked by the PI, the digital recordings were permanently removed from
computers. The consent documents are locked in a safe place with access
restricted only to the PI. All those documents will be permanently destroyed
once the study report is submitted and the articles and papers published.

41

42
Consensus development
Consensus development - Iran
The results of the qualitative study and literature search were used to
identify a set of potential research priority topics.
All the interviewees were invited to attend the consensus development
meeting. The meeting was conducted following a nominal group
technique approach. First a brief overview of the study and the step that
had been followed was presented in the meeting. Then the participants
were invited to offer their views on the main ATM concerns and issues.
The potential priority topics for research had been categorised under the
main themes developed from the qualitative phase of the study based on
the general categorization of the ATM by the WHO (

43
Table 4). Under each main theme a set of topics were offered to the
participants. After a brief discussion of the topics, they were invited to
vote on the importance of the topic as an ATM research topic relevant to
that category. The voting was in private and on previously prepared
table that allowed the participants to select from 1 (no priority) to 9
(maximum priority) for each potential research topic (Table 5). Voting for
each category was conducted separate from the other categories.

44
Table 4. The main categories for the identification of research priorities
1- National pharmaceutical policies (stewardship and governance)
2- Financing, insurance and financial coverage
3- Pharmaceuticals' production (or import) and distribution
4- Other sectors' policies and players at national and international level
5- Household access to medicine and utilization
6- Health care provider behaviour (including physicians, pharmacists …)
Table 5. An example of the consensus development tool
Please express your opinion about the priority of each issue as a research topic by
ticking a number from 1 (no priority) to 9 (maximum priority)
Code Topic Priority of research on the topic
No priority Maximum priority
1 1 2 3 4 5 6 7 8 9
2 1 2 3 4 5 6 7 8 9
3 1 2 3 4 5 6 7 8 9
For the analysis of the findings, we calculated the mean (standard error)
of the scores for each topic to observe the distribution of the responses.
We then grouped the score into three groups: 1-3 (“low importance”), 4-6
(“medium importance”) and 7-9 (“high importance”). For each category
of issues (
45
Table 4), we identified the topics as “high importance” if 70 per cent of
the respondents scored the topic as high importance.
Consensus development - Pakistan
A consultative process was taken for identification of policy and research
concerns. A Roundtable with stakeholders was held on 12th May at AKU
Karachi involving 25 stakeholders from different entities attended the meeting
including country Investigators from Iran and Lebanon as well as focal person
for ATM project from Alliance HSPR, WHO Geneva. The Roundtable was
chaired by Secretary Health, Sindh, Pakistan. The roundtable took a
consultative process to identify emerging policy concerns and research
questions. It involved presentation of scope and objectives of ATM
prioritization project being carries out globally, brief overviews of findings from
Iran and Lebanon and detailed presentation on Pakistan findings. Following the
presentation, policy concerns were collectively identified and a list of research
questions generated for further action. Written comments were further invited
post Roundtable through an email listing for improvement of data and
incorporation of needed research areas.

46
Consensus development and priority research questions - Lebanon
Two researchers (SJ and RY) reviewed the literature, both journal articles and
documents, to identify ATM areas that have been covered in prior research
and to retrieve new policy-relevant research questions. When a research
question was explicitly expressed, it was added unmodified to the list of
research questions. When a research question was not explicitly expressed but
could be inferred from policy concerns about ATM appearing in the literature,
the two researchers developed the corresponding research questions(s) and
modified the question(s) until a consensus is reached about the wording of
research questions. Identified research questions were categorized in one of
the four domains as per the WHO 2004 framework. An additional category
comprised research questions encompassing cross-cutting and general issues.
The research questions emanating from the literature review are listed in
Appendix 6-A.
Similarly, the transcribed interviews were analyzed to identify policy concerns
and research questions. Just as the case for literature review, when a research
question was explicitly expressed, it was added unmodified to the list of
research questions. When a research question was not explicitly expressed but
could be inferred from policy concerns about ATM stated by the informants,
the researchers developed the corresponding research questions(s). The first
step was to list all possible questions emerging from the analysis of all
transcripts. This exercise was performed by two research assistants. In the
second step, a third researcher reviewed the list of questions, merged similar
questions, and excluded the research questions that seemed incoherent.
During these two steps, identified research questions were categorized in one
of five categories corresponding to the four domains of ATM as presented in
the WHO-2004 framework, and one general cross cutting category
encompassing such research questions that pertain to all the four aspects such
as corruption, governance, or free market. We included a research question,
where expressed explicitly or inferred implicitly from a policy concern, even if
such a question was cited only once by one informant during the two steps of
identification. This process was meant to allow the inclusion of as many
47
research questions as possible. The research questions emanating from the
analysis of KII are listed in Appendix 6-B.
The principal investigator then reviewed all research questions that have
emerged from literature review and key informant interviews, and
consolidated and shortened the research questions, excluding those deemed
redundant, inadequate, or not corresponding to the domain of ATM. In the
final step, two researchers reviewed all research questions and reached
consensus about the research questions in their final reworded and merged
form. This resulted in a list of 57 questions (Appendix 6-C) which were to be
submitted to the validation-prioritization meeting.
All key informants were invited to participate in the validation-prioritization
meeting. Key informants unable to participate were asked to recommend
representatives of their institutions/organizations if possible. The final list of
participants is presented in Appendix 2. Both the participants and the
researchers felt that the number of participants was adequate and allowed for
engagement in discussions and for completing the prioritization tasks within
the allotted time of three hours.
The objectives of the validation-prioritization meeting were to review the
research questions that have emerged from literature review and key
informant interviews, remove the questions that were not thought to be
priorities, modify questions as needed and rank questions according to pre-
specified evaluative criteria.
Although the research questions from literature review and key informant
interviews had been categorized thematically in the previous step (see 3.3.
above), the 57 questions were presented to the participants in one list. The
rationale behind this was to avoid force-fitting the questions into pre-defined
categories, i.e. according to the WHO 2004 framework, and allow the
48
participants to discuss and propose alternative frameworks for approaching
ATM and thus priority research.
The meeting comprised two main steps:
a. Step 1: Validation exercise: Each participant was given a print-out of the 57
research questions and asked to grade the 57 research questions according
to importance (0 if they deem the question unimportant, and 1 if deem it
important or possibly important) and to identify the questions that required
modification. The participants were also encouraged to propose new
questions that deemed important to include in the list of priorities and
those they considered inadequate or illegitimate. After having reworded a
number of questions, the grades were added up. All the questions that
obtained a score of more than 8, signifying that at least 2/3 of participants,
or 8 participants, considered them important, passed to the second round
of prioritization ranking.
b. Step 2: Prioritization exercise: Among the original 57 questions that
emerged from the validation exercise, 22 questions achieved the cut-off
score and were submitted to the participants for prioritization. Each
participant was given a print-out of the list of 22 questions and asked to
give a score each question on five evaluative/ranking criteria for
prioritization. A statement of explanation was provided for each criterion.
The participants provided a critique of criteria and requested modification.
The final list of criteria was:
- Relevance: Would the research study address one or more of the
important issues in ATM?
- Urgency: How soon should the research study be done?
- Feasibility: Can the research study be done using available resources?
- Applicability: What are the practical implications of the research study
on changing policy? Would the political climate allow it to be done?
- Ethical acceptability: Would the research study violate ethical
principles?
For each criterion, the participant were asked to give the research question
a score from 1-10 (10 representing a high priority for the research question

49
on the concerned ranking criterion). The final list of 22 questions ranked
according to these criteria is presented in Appendix 6-D.

50
Results – literature review – country cases studies
Figure 4 provides the details of the search strategy and the number of
papers retrieved at each stage of the search. Search in the Social
Sciences Citation Index and Science Citation Index electronic databases
was very similar to the Pubmed search, the only difference was that
countries in this database searched in the address rather than the
affiliation, and the other terms was limited to the topic. This search
yielded 3393 publications and records.
All the records from the searches were included in the Endnote software,
then merged together. After review all titles of publications, 597 records
were selected then by review the abstract of remaining records ,110
relevant studied were selected. Finally we omitted articles that was
published before 2000. Finally 91 articles were selected to review their
full text.

51
Figure 4: Flow chart of search strategies in electronic databases for ATM
Article titles considered (n=4086) (a) ISI search result (total n=3393)
(b) PubMed search result (total n=693) Search date: 2 nov 2010
Abstracts considered (n=874) (a) ISI abstracts (n=433)
(b) PubMed abstracts (n=198)
Not likely to be relevant by title and therefore excluded (n=3455)
(a) n=2960 (b) n=495
Select of related Articles for read in full text (n=88) (a) ISI or (b) PubMed
Articles read in full text (n=75) Articles read in abstract (n=13 , because of
don’t access to full text)
(a) ISI or (b) PubMed
Not likely to be relevant after examination of the abstract and therefore excluded (n=786)
(a) ISI or (b) PubMed
Article titles considered (n=1311) New result (n=1311-693=669)
- PubMed search result Search update: 21 june 2011
Abstracts considered (n=224) - PubMed abstracts
Select of related Articles for read in full text (n=123) - PubMed
Articles read in full text (n=37) Articles read in abstract (n=86, because of
don’t access to full text)
- PubMed
Not likely to be relevant by title and
therefore excluded (n=445)
Not likely to be relevant after examination of the abstract
and therefore excluded (n=786)
Articles identified (n=211)
Primary search (n=88)
Update search (n=123)
Articles included after final
assessment of inclusion and
exclusion criteria (n=151)
Primary search (n=88)

52
Literature review - Iran
Literature review, papers locally published in Iran and grey literature
Sensitive searches of the databases and websites, revealed 1755 potentially
relevant titles. we then screened the titles and abstracts to identify potentially
relevant articles. Also a Ministry of Health and Medical Education collection of
150 grey literature and published magazine articles were reviewed. We
included articles published from 2001 (1380- Iran's calendar) onward.
As a result the full texts of 46 papers were fully assessed, and 39 papers were
included in the study. As demonstrated in the

53
Figure 5, the majority of these papers (i.e. 79%) discussed the rational use of
medicines, inclusively or in conjunction with other issues. Also most papers
were focused on health service provider level.

54
Figure 5. ATM issue categorization for papers published in Iran's journals.
The included studies came from 18 different provinces (out of 30), and the
majority were from Tehran province (eight studies). Seven studies were
national studies, and two papers reviewed previous research (Table 6 ). We
observed no particular trend in the number of publications each year, or the
focus of the publications in Farsi papers. As we'll demonstrate later on, it
seems that the growth in the number of research outputs from Iran on ATM
has consolidated in English language publications in international journals.
Table 7 demonstrates that not all provinces have been covered by such
studies. Still the focus of attention of ATM issues shows no pattern or
significant geographical variation in the country.
0
5
10
15
20
25
30
35
Papers published in Persian (Farsi) language
research journals
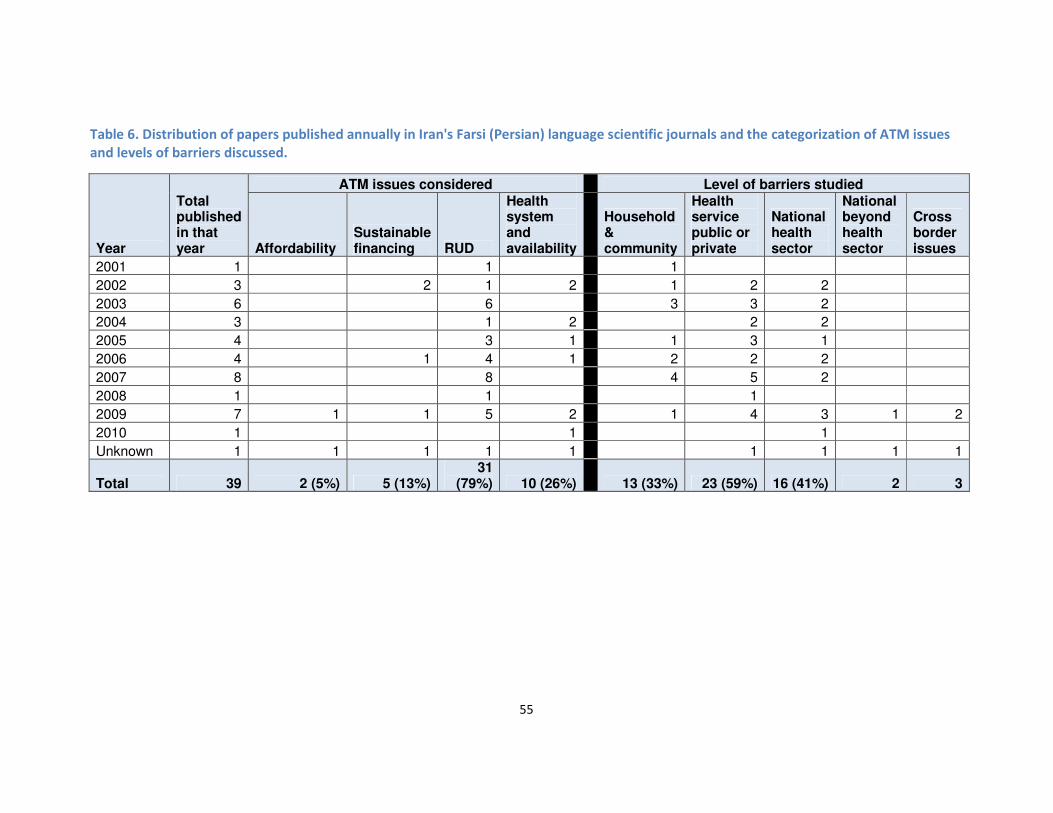
55
Table 6. Distribution of papers published annually in Iran's Farsi (Persian) language scientific journals and the categorization of ATM issues
and levels of barriers discussed.
Year
Total published in that year
ATM issues considered Level of barriers studied
Affordability Sustainable financing RUD
Health system and availability
Household & community
Health service public or private
National health sector
National beyond health sector
Cross border issues
2001 1 1 1
2002 3 2 1 2 1 2 2
2003 6 6 3 3 2
2004 3 1 2 2 2
2005 4 3 1 1 3 1
2006 4 1 4 1 2 2 2
2007 8 8 4 5 2
2008 1 1 1
2009 7 1 1 5 2 1 4 3 1 2
2010 1 1 1
Unknown 1 1 1 1 1 1 1 1 1
Total 39 2 (5%) 5 (13%) 31
(79%) 10 (26%)
13 (33%) 23 (59%) 16 (41%) 2 3
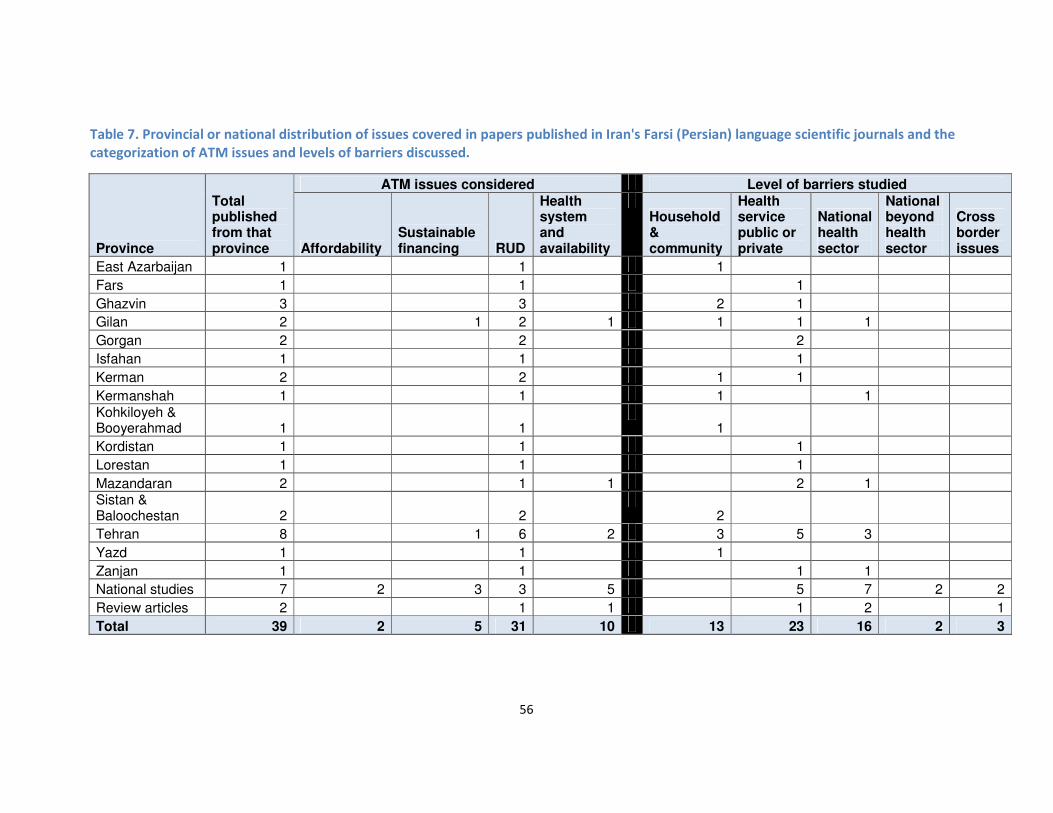
56
Table 7. Provincial or national distribution of issues covered in papers published in Iran's Farsi (Persian) language scientific journals and the
categorization of ATM issues and levels of barriers discussed.
Province
Total published from that province
ATM issues considered Level of barriers studied
Affordability Sustainable financing RUD
Health system and availability
Household & community
Health service public or private
National health sector
National beyond health sector
Cross border issues
East Azarbaijan 1 1 1
Fars 1 1 1
Ghazvin 3 3 2 1
Gilan 2 1 2 1 1 1 1
Gorgan 2 2 2
Isfahan 1 1 1
Kerman 2 2 1 1
Kermanshah 1 1 1 1 Kohkiloyeh & Booyerahmad 1 1
1
Kordistan 1 1 1
Lorestan 1 1 1
Mazandaran 2 1 1 2 1 Sistan & Baloochestan 2 2
2
Tehran 8 1 6 2 3 5 3
Yazd 1 1 1
Zanjan 1 1 1 1
National studies 7 2 3 3 5 5 7 2 2
Review articles 2 1 1 1 2 1
Total 39 2 5 31 10 13 23 16 2 3

57
Although it seems that studies are more concerned with rational use of drugs
at the level of provider (usually measuring mean number of items per
prescription, or proportion prescriptions containing antibiotics), there are signs
that health system level issues are gaining further attention in the country. A
good example of such focus on Adverse Drug Reaction (ADR) reporting system
has been presented in Cheraghali et al 2003.1 We produced using their data to
demonstrate that a move in the right direction is happening (Figure 6).
Figure 6. Growth in ADR reporting in Iran. Figure reproduced using Cheraghali
et al 2003 data.
570620
11631210
1675
0
200
400
600
800
1000
1200
1400
1600
1800
ADRs reported in Iran to the Ministry of
Health and Medical Education 1998-2002

58
Literature review, papers published from Iran in international journals
We also used our international literature search of regional reports, to retrieve
studies published from Iran (see search strategy - Table 1). The analysis of the
data suggests an increasing trend in the number of research output relevant to
ATM issues from Iran (Figure 7). In the period of coverage of our study (i.e. 2001
onward), the first identified paper has been published in 2004, and since then
the number of studies has been growing. Still the absolute majority of the
studies focus on RUD alone or in combination with other ATM issues (Table 8).
In that sense, there is no observable difference between papers published
within or outside Iran. However, there are considerably more papers focusing
on affordability issues (Table 8). This is in line with the increasing cost of
medicines in the country, and national policies that involves gradual move
away from the generic prescribing policy.
59
Figure 7. An increasing trend: ATM papers on Iran published in local Farsi (Persian) journals and international English language journals.
20012002200320042005200620072008200920102011 -
first halfunkown
grand
total
Total 13658710718105180
English papers 000243261195042
Farsi papers 13634481710139
0
10
20
30
40
50
60
70
80
90
An increasing trend: ATM papers on Iran published in
local Farsi (Persian) journals and International English
language journals
Total
English papers
Farsi papers

60
Table 8. Annual a growth in the number of ATM papers from Iran in international literature, and the distribution of issues covered and the
levels of barriers discussed
Year
ATM issues considered Level of barriers studied
Affordability Sustainable financing RUD
Health system and availability
Household & community
Health service public or private
National health sector
National beyond health sector
Cross border issues
2004 1 1 1 1 1 1
2005 1 3 1 3 1 1
2006 3 2 2 3 1
2007 1 1 2 2 2 3 1
2008 1 7 2 7 4
2009 2 1 9 3 3 7 5 1
2010 1 1 8 4 1 7 4 1 1
2011 1 1 4 3 4 3 2 2
Total 8 (19%) 4 (10%) 37
(88%) 16 (38%)
9 (21%) 34 (81%) 22 (52%) 6 (14%) 3 (7%)
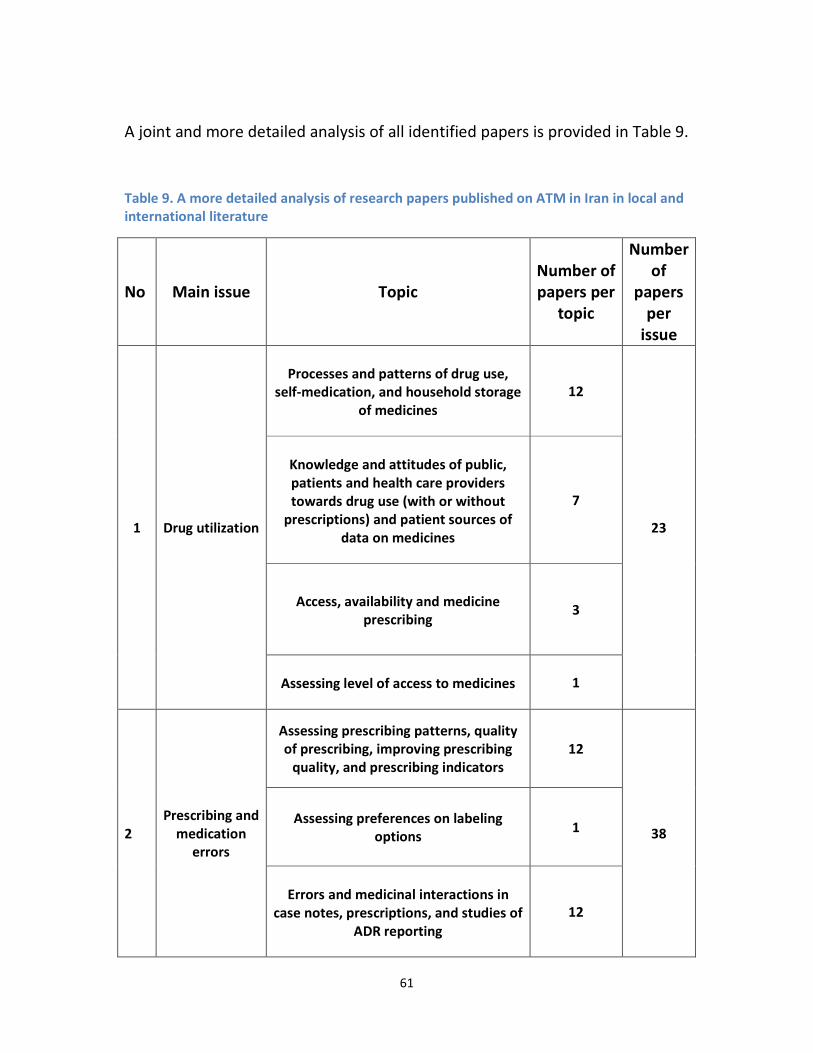
61
A joint and more detailed analysis of all identified papers is provided in Table 9.
Table 9. A more detailed analysis of research papers published on ATM in Iran in local and
international literature
No Main issue Topic Number of
papers per
topic
Number
of
papers
per
issue
1 Drug utilization
Processes and patterns of drug use,
self-medication, and household storage
of medicines
12
23
Knowledge and attitudes of public,
patients and health care providers
towards drug use (with or without
prescriptions) and patient sources of
data on medicines
7
Access, availability and medicine
prescribing
3
Assessing level of access to medicines
1
2
Prescribing and
medication
errors
Assessing prescribing patterns, quality
of prescribing, improving prescribing
quality, and prescribing indicators
12
38 Assessing preferences on labeling
options 1
Errors and medicinal interactions in
case notes, prescriptions, and studies of
ADR reporting
12
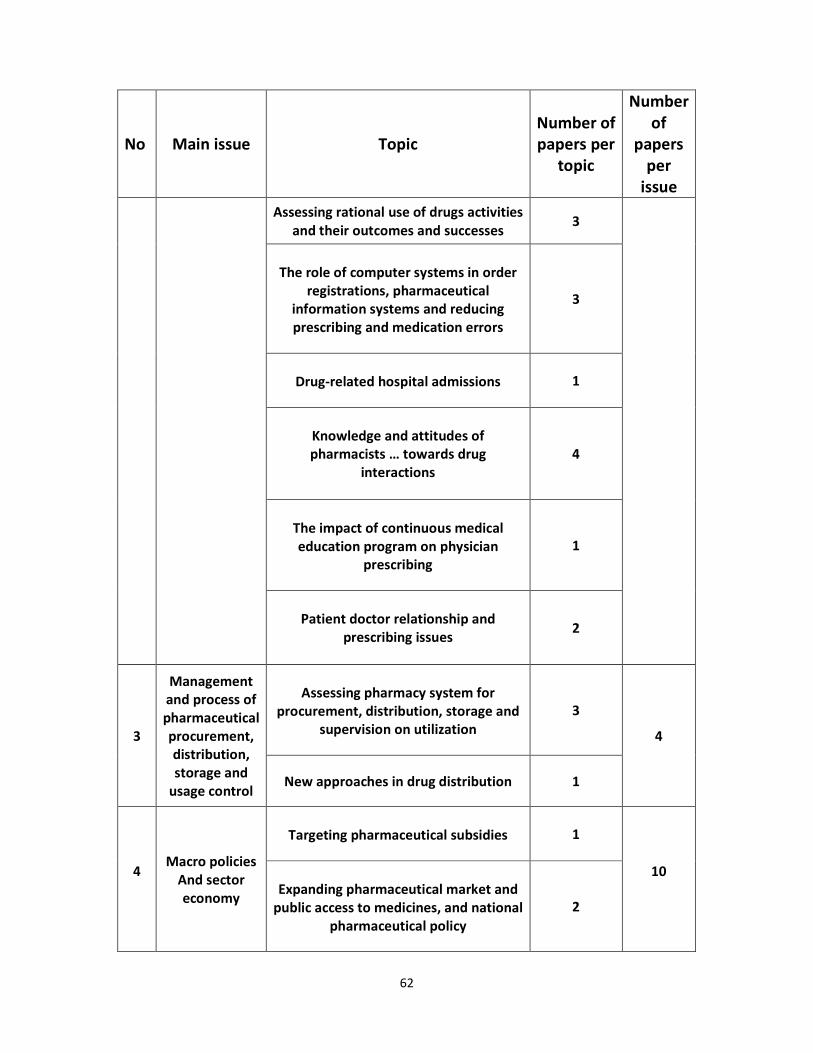
62
No Main issue Topic Number of
papers per
topic
Number
of
papers
per
issue
Assessing rational use of drugs activities
and their outcomes and successes 3
The role of computer systems in order
registrations, pharmaceutical
information systems and reducing
prescribing and medication errors
3
Drug-related hospital admissions
1
Knowledge and attitudes of
pharmacists … towards drug
interactions
4
The impact of continuous medical
education program on physician
prescribing
1
Patient doctor relationship and
prescribing issues
2
3
Management
and process of
pharmaceutical
procurement,
distribution,
storage and
usage control
Assessing pharmacy system for
procurement, distribution, storage and
supervision on utilization
3
4
New approaches in drug distribution 1
4
Macro policies
And sector
economy
Targeting pharmaceutical subsidies
1
10
Expanding pharmaceutical market and
public access to medicines, and national
pharmaceutical policy
2
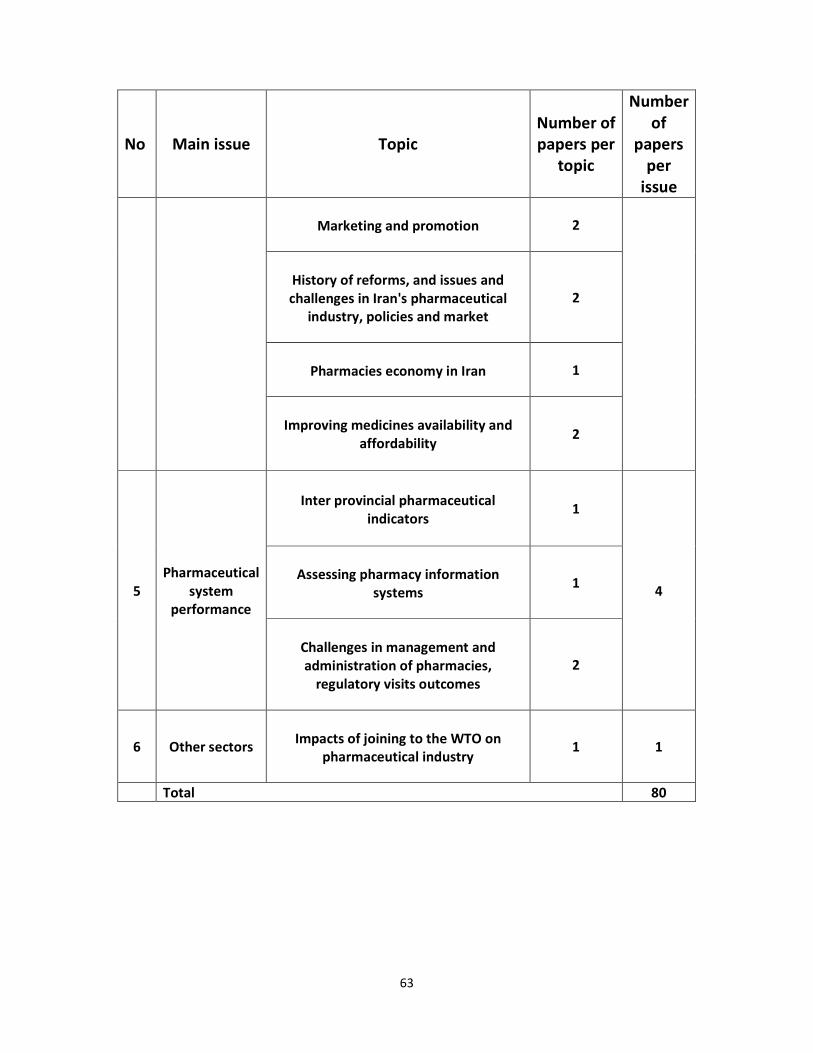
63
No Main issue Topic Number of
papers per
topic
Number
of
papers
per
issue
Marketing and promotion
2
History of reforms, and issues and
challenges in Iran's pharmaceutical
industry, policies and market
2
Pharmacies economy in Iran
1
Improving medicines availability and
affordability
2
5
Pharmaceutical
system
performance
Inter provincial pharmaceutical
indicators
1
4
Assessing pharmacy information
systems
1
Challenges in management and
administration of pharmacies,
regulatory visits outcomes
2
6 Other sectors
Impacts of joining to the WTO on
pharmaceutical industry
1 1
Total 80

64
Literature review - Pakistan
RATIONAL USE OF MEDICINES IN PAKISTAN
Irrational drug prescribing, dispensing and self-medication continue to be a major problem in Pakistan. Although a national essential drug list exists it is poorly enforced across the health sector. Irrational prescription is due to high level of prescription by non-qualified practitioners and self medication, frequently inappropriate prescription particularly by qualified providers, particularly high use of injectables, and resulting issues of polypharmacy, unnecessary expenditure, drug resistance, and contributing to high prevalence of Hepatitis B and C in the country.
National Essential Drug List: Essential medicines as defined by WHO are those that satisfy the health care needs of majority of the population. Through 1970s and 1980s the Essential Medicines Program of WHO Pakistan promoted this concept to redress imbalance in selection of drugs. The National Essential Drug List (EDL) of Pakistan was first prepared in 1994 in consultation with relevant experts and using WHO’s model list of Essential Medicines as a template. The list was subsequently reviewed in 1995, 2000 and 2003 and the present list is the fourth revision containing 335 medicines (MOH 2007). Development of EDL is a function of the Federal Ministry of Health (MOH) while compliance and adherence rests with the provincial Departments of Health (DOH). Procurement of drugs in DOHs is based on EDL although non-EDL purchasing has been reported (details in supply side issues). Compliance and adherence to EDL varies from poor to good in different parts of Pakistan 2-4. In a baseline survey in three provinces of Pakistan, it was found out that EDL is only available in one out of five public sector facilities 2. Compliance with EDL in terms of prescriptions was found to be 50% at public sector facilities in one survey 4 and 80% in a survey of three public sector teaching hospitals 3.
Frequent prescription by non-qualified prescribers: Prescription by non-qualified practitioners as well as self medication is common in Pakistan, however there are few studies that capture the magnitude of self medication and hardly any literature on quacks. In a survey of 500 households examining health seeking behavior for childhood illnesses, self-medication was given to 51.3% children (Haider &Thaver, 1995). These mostly comprised of analgesics/antipyretics (25%), anti-diarrheals/ anti-emetics (11%) and antibiotics (11%) while 34% were unidentified drugs (34%). Infants were self medicated particularly during diarrheal episodes, which is a dangerous trend as improper management has resulted in childhood diarrhea being the number two cause of death in children under five 5. A study on youth reported frequent prescription and consumption by college students on medical student’s advice or self prescription 6. 55.3% of medical students prescribe medicines independently and most are likely to belong to 1st and 3rd year of medical college while a third of non-medical students report self prescription 6. Another study pointed out that most potent drugs like antibiotics, psychotropic, narcotics, anti-cancers and hormones are being misused by un-trained doctors or by quacks or through self medication due to lack of co-ordination among the relevant professionals 4. High level of inappropriate prescription by qualified providers: Drug prescription even amongst qualified providers is also frequently irrational. Both general practitioners & public sector physicians have been found to excessively prescribe anti-bacterials, anti-amoebics and anti-diarrhoeals in the case of ARI, diarrhea and fever in children while ORS has been inadequately prescribed (Siddiqi 2002). 30% of prescriptions sent to pharmacies lack a
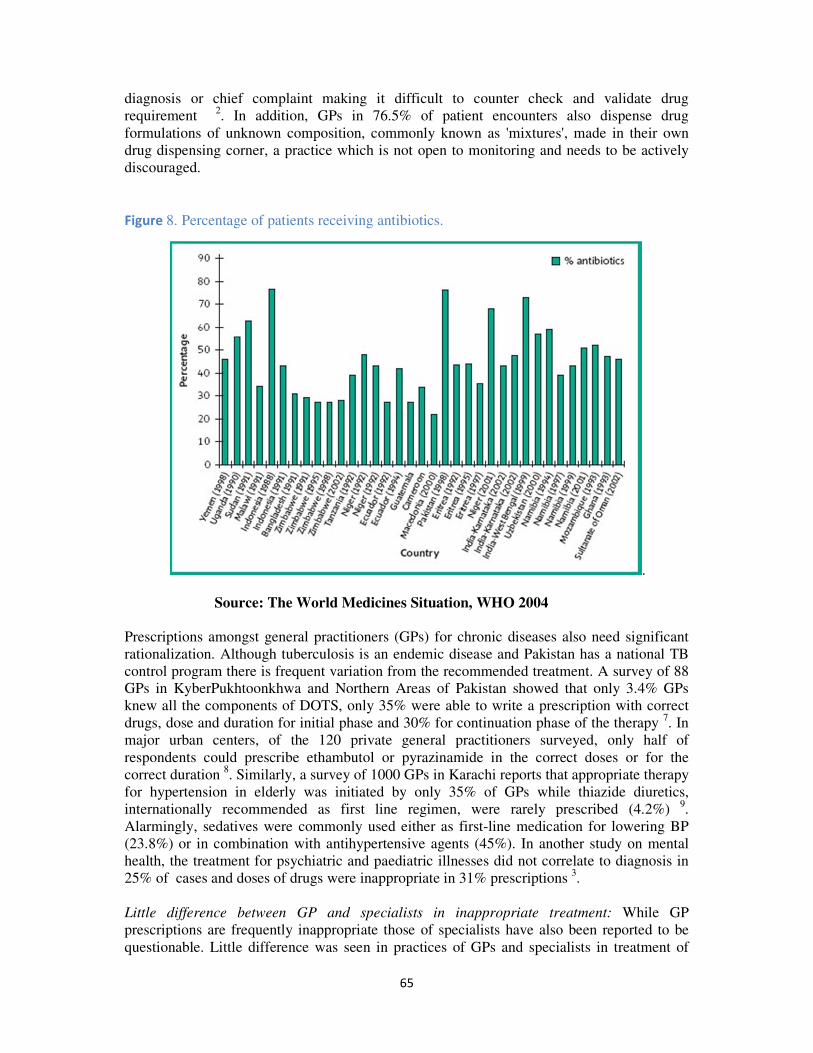
65
diagnosis or chief complaint making it difficult to counter check and validate drug requirement 2. In addition, GPs in 76.5% of patient encounters also dispense drug formulations of unknown composition, commonly known as 'mixtures', made in their own drug dispensing corner, a practice which is not open to monitoring and needs to be actively discouraged.
Figure 8. Percentage of patients receiving antibiotics.
.
Source: The World Medicines Situation, WHO 2004 Prescriptions amongst general practitioners (GPs) for chronic diseases also need significant rationalization. Although tuberculosis is an endemic disease and Pakistan has a national TB control program there is frequent variation from the recommended treatment. A survey of 88 GPs in KyberPukhtoonkhwa and Northern Areas of Pakistan showed that only 3.4% GPs knew all the components of DOTS, only 35% were able to write a prescription with correct drugs, dose and duration for initial phase and 30% for continuation phase of the therapy 7. In major urban centers, of the 120 private general practitioners surveyed, only half of respondents could prescribe ethambutol or pyrazinamide in the correct doses or for the correct duration 8. Similarly, a survey of 1000 GPs in Karachi reports that appropriate therapy for hypertension in elderly was initiated by only 35% of GPs while thiazide diuretics, internationally recommended as first line regimen, were rarely prescribed (4.2%) 9. Alarmingly, sedatives were commonly used either as first-line medication for lowering BP (23.8%) or in combination with antihypertensive agents (45%). In another study on mental health, the treatment for psychiatric and paediatric illnesses did not correlate to diagnosis in 25% of cases and doses of drugs were inappropriate in 31% prescriptions 3.
Little difference between GP and specialists in inappropriate treatment: While GP prescriptions are frequently inappropriate those of specialists have also been reported to be questionable. Little difference was seen in practices of GPs and specialists in treatment of

66
childhood diarrhea. It was observed that only 17.7% of GPs and 14.3% of pediatricians prescribed ORS in all of their encounters while instructions for preparing ORS were given in only 6% of encounters by GPs and 8.4% of encounters by pediatricians (Nizami et al 1996). A significant difference was observed only in higher prescription of anti-diarrhoeals by GPs over pediatricians (P < 0.01) while there was no significant difference in antibacterial amongst GPs and pediatricians (P <0.16).
High number of drugs per prescription: The average number of drugs prescribed per patient is 3 or more in Pakistan as compared to an average of 2-3 in LMICs, and over 70% of patients are prescribed antibiotics 10. A survey of 10 health care facilities from each province were selected keeping appropriate representation from first level health facilities, district health facilities and tertiary care hospitals, found out that average prescribed number of drugs per patient was 2.77 (Range: 0-7) and would be higher if drugs per prescription rather than drugs per patient were to be computed (Hafeez et al 2004). Drugs prescribed at BHus and RHCs is high at 2.75 medicines per prescription and close to the average of 2.79 prescribed at Teaching Hospitals 2. In a randomized survey of prescriptions of 354 (specialists), practicing in private facilities, there was an average of 4.51 medicines prescribed per prescription with over prescriptions of antimicrobials, vitamins/minerals and injections were overprescribed 4.

67
Figure 9. Number of medicines per prescription
Source: The World Medicines Situation, WHO 2004.
High use of injections: Overuse of drugs also translates into a high rate of injection usage. Pakistan is globally one of countries with the highest rate of injection usage with over 60% of patient encounter involving an injection (WHO 2004). This translates into 13 injections per person per year (DAWN 2009). Studies in Pakistan show that up to 90% of injections are estimated to be unnecessary 10. A cross-sectional survey of general practitioners in urban and rural areas of Murree showed that 80% of the general practitioners give injections to every patient (Janjua 2003). 53% of GPs in rural areas and 28% in urban areas preferred injection as an essential component of treatment 11. When comparing public and private healthcare providers, in Attock district, over 48% of GP prescriptions had at least one injectable drug compared with 22.0% by public providers ( p < 0.0001) 12. Asides from polypharmacy issues, high injection use raises grave risks of spread of blood borne diseases such as Heptatis B, C and HIV. GPs largely make use of unsafe practices with most surveyed GPs using multi dose vials for medications and none of the practitioners used separate syringes for drawing and injecting. There was also seen to be insufficient numbers of sharp material disposal boxes, which were not available in 86% of the facilities. Moreover, 79% of the injection providers were never vaccinated for Hepatitis B 13.

68
Figure 10. Percentage of patients receiving injections
Higher rate of irrational use amongst GPs over public sector: In a survey in 114 health facilities, including 62 public sector and 52 private sector facilities, it was found that the mean number of drugs per prescription was 4.1 (SE: +/- 0.06) for general practitioners and 2.7 (SE:+/- 0.04) for public providers (p < 0.0001) 14. Prescription rate was particularly higher for antibiotics (62%) and injections (48%) amongst GPs as compared to public sector with rates of 54% and 22% respectively (p < 0.0001). Similarly more than 11% of GP prescriptions had an intravenous infusion compared with 1% for public providers (p < 0.001). General practitioners were also found to prescribe anti-diarrheals more frequently than doctors working in the public sector (p < 0.01) (Siddiqi et al 2002). However, many public sector physicians also practice as general practitioners during evening hours and it is uncertain whether the relative edge of prescriptions within public sector facilities is maintained during switch to general practice. Drug resistance: Antimicrobial resistance and containment often results from irrational drug use 15. High level of resistance has been found to ampicillin, cotrimoxazole, chloramphenicol and erythromycin in a large study of 9209 individuals in Karachi 16. The results are alarming as these are the frontline antibiotics for control of infections. The study also found that these drugs had been frequently used by the individuals in the four weeks preceding the resistance survey. It is expected that resistance to front line anti-malarials, anti-tuberculous therapy and HIV retroviral therapy is also present in Pakistan however surveillance of resistance is a major challenge and there is need for robust information in this area.

69
AFFORDABILITY & FINANCING
Total financing to health sector is inadequate: In Pakistan 2.4% of GDP is spent on health with total health expenditure being extremely low at $15/capita/ year. National Health Accounts analyzing 2005-06 data shows that of the total health expenditure, that only 32% is spent by public sector including the Ministry of Health, para-statal organizations and facilities of Armed Forces Federal Bureau of Statistics 17. Private health expenditure is responsible for the major share 64% of total health expenditure of which 97.5% comes from out of pocket spending by households with very few covered by pre-payment schemes 17. International development partners have a marginal contribution of 1.9% of total health expenditures. Medicine expenditure is low and responsible for shortages: Overall, an estimated 47% of the total health expenditure in Pakistan is spent on medicines (WHO 2004). The public sector is responsible for only 27% of medicine expenditure while private health expenditure on medicine comprises nearly three-fourth with the burden borne by households through out of pocket payments (WHO 2004). 43% of private sector users pay for medicines within the facility while 60% pay for medicines at outside pharmacies/ drug stores. Spending in the public sector on medicines is clearly inadequate and a major contributor to drug shortages as shown in later sections. WHO predicts that governments spending less than US$2 per person per year on essential drugs are likely to face shortages in the public sector forcing patients and their families to purchase from the private sector 18. The MOH in Pakistan spends $3 per capita on health (NHA 2009) and available evidence shows that the Ministry of Health’s operational budget is mainly taken up by salaries with a 30-20% spent on non-salary expenditures including medicines 19-21.
Figure 11. Share of Total Pharmaceutical Expenditure in Total Health Expenditure

70
Figure 12. Share of Public and Private Sectors in Total Pharmaceutical Expenditure
Out of pocket medicine expenditure at public and private sector facilities: A synthesis of national evidence shows that out of pocket expenditure at public sector facilities consists largely of payments for medicines bought outside the facility by nearly two-thirds of users. Mean cost of medicines outside is Rs. 252 in private and Rs. 198 in public facilities 22. With lack of specific financing schemes such as prepayment schemes for risk-pooling or commodity vouchers, the poor and sick are vulnerable to prescription practices of health staff and the pharmaceutical market 23. A study reported that low income users of obstetric care at a government hospital in Karachi spent 44% of the direct medical expenses on drugs
24. Expenditure estimation for out-patient diabetes care at three facilities including a NGO, private sector and government health facility in Karachi found that 46% of the total out of pocket expenditure is on drugs 25. A population based study on 2675 households in Karachi reported that 54% of patient expenditure on hypertension control at outpatient cares across is spent on purchase of medicines (Zaidi et al 2008). The high share of expenditure consumed by medicines is one of the major reasons underlying patient non-compliance with chronic care therapy. Available studies examining non-compliance report that in at least 33.5% of psychiatric patients and 41% of tuberculosis patients unaffordability of drugs was the primary reason for non-compliance (Rizwan 2005; Ahmed 2009). The above findings highlight that sufficient financial access to even generic equivalents needs to be guaranteed for the poor while use of originator brands needs to be substantially rationalized. Medicine prices of public sector procurement: The Median Price Ratio (MPR) gives an indication of country price to international reference price with a ratio of 1 or below considered to be efficient. The public sector procurement of generics medicines is at an acceptable Median Price Ratio of 0.6 however that for originator brands is substantially high with a MPR of 7.0 as compared to international average of 3.0. This shows that generics in the public sector are purchased at acceptable prices however it does not give an indication of quality of medicines. At the same time the gap between generics and originator brands is extremely high and needs to be reduced through both price regulation and rational selection.

71
Medicine prices in private sector: In the private retail sector, Median Price Ratios of drugs are substantially higher in private retail outlets than those observed in public sector procurement both in Pakistan and most LMICs with the exception being countries such as Kuwait where because of pricing regulations there is little price differential between originator brands and generics. In Pakistan basic generic medicines in private retail outlets have a MPR range of 1.2-7.3 and originator brands for basic therapy have a range between 0.8-15.8. Specific medicines suffer from excessive prices and need to be targeted for regulatory action and cautious prescription Affordability Indexes and Studies: A price and availability survey by the World Health Organization and Health Action International studied the affordability of 29 important medicines in 36 countries including Pakistan 26. The affordability of treatment was estimated as the number of days’ wages the lowest paid government worker would be required to pay to purchase a standard one-month medicine therapy for a chronic illness or for one episode of acute illness. A treatment requiring more than one day’s wage is considered unaffordable. In the public sector in Pakistan, like most of other countries, medicines are generally provided free of charge however given frequent non-availability of medicines, patients were commonly forced to seek supply from private retail pharmacies. Medicine therapy for acute respiratory infection was affordable given a range of 0.3-1 days wage, therapy for chronic illness such as hypertension, depression, diabetes, epilepsy, arthritis and peptic ulcer was unaffordable even with use of low priced generics (WHO-EMRO 2008). Affordability of chronic conditions with low priced generics was 1.7-7.7 while with originator brand was the range was much higher from 1.9-36.4 (WHO-EMRO 2008).
RELIABLE HEALTH SYSTEMS
1.Public Health Care System
Public sector facilities provide medicines free of charge. There are more than 10000 health public sector facilities ranging from 5798 Basic Health Units (BHUs), 581 Rural Health Centres (RHCs), 947 Tehsil HeadQuarter and District HeadQuarter Hospitals (THQH/ DHQH), and 29 Teaching Hospitals 27. Supply of medicines to primary and secondary facilities is based on essential drug list for each tier of health facility and inlcude approximately 70-80 drugs for BHUs, 100-120 for RHCs and 300 for District Hospitals. Tertiary facilities, including Teaching Hospitals, procure medicines independently based both on the National EDL as well as recommendations of the hospital drug procurement committee. Low utilization of public sector facilities: Overall utilization of public sector is low with 21% of the population utilizing public sector while the rest utilize a primarily fee based private 28. Low utilization is consistent across both rural and urban areas with respectively 36% and 22% of households utilizing the public sector 27. There is particularly low utilization of primary care tiers of the health systems, with 1 visit/capita/ year to a PHC facility, while there is heavy utilization of tertiary hopsitals. Amongst users of public sector facilities, 40% are dissatisfied with services provided with lack of medicine availability being the most frequent reason for dissatisfaction 29.
Table 10. Level of Dissatisfaction with Public Sector and Underlying Reasons
Percentage dissatisfied with service 40

72
Reason for dissatisfaction
No doctor 12
No trained staff 20
No medicine available 23
Long waiting 13
Staff not helpful 14
Treatment unsuccessful 11
Source: PSLM 2004/05.
Availability of medicines in public sector facilities: Availability of even essential recommended generics is extremely low in public sector facilities with a 3.3.% median availability and is much lower than the range of 29-54% found in LMICs while originator brand medicines are generally not available in public sector facilities in Pakistan as well as other LMICs 26. Availability in public sector is lower than that in private sector as discussed in a following section. Availability of medicines for acute care range between 30-67% while availability of essential chronic care drugs for management of cardiovascular disease, diabetes, chronic respiratory disease, glaucoma and palliative cancer therapy ranges between 3-57% 30.
Table 11. Medicine Availability at Public Facilities and Private Pharmacies
0% beclomethasone inhaler, Carbamazepine, Hydrochlorothiazide, Indinavir,
Losartan, Lovastatin, nevirapine, Nifedipine retard, phenytoin, zidovudine
1-10% Acyclovir, fluconazole, fluoxetine, fluphenazineinj, ranitidine, salbutamol inhaler, Sulfadoxine/Pyrimethamine
11-40% Amitriptyline , ceftriaxone inj , Co-trimoxazole, susp, Diclofenac ,
Glibenclamide, Omeprazole
41-50% Ciprofloxacin
51-60% Captopril, diazepam
61-80% Amoxicillin, atenolol, metformin
>80% None
Source: Pakistan: Medicine Prices, Availability, affordability & price components, WHO/HAI Report 2008 There is lack of comprehensive assessments of drug availability across the country giving details by drug type and by primary and secondary tiers. Available information from one province, the province of Sindh, shows that there was not a single BHUS or RHC maintaining a full stock of mandated drugs 31. Stock outs were comparatively higher in BHUs as compared to RHCs. BHUs had 10-25% availability of antibiotics in BHUs, followed by 25-50% availability of iron tablets, anti-malarials and anti-tuberculosis drugs and 50-80% availability of anti-pyretics while in RHCs there was
Table 12. 171717Availability of Medicines in Percentage of BHUs and RHCs
Medicines Availability of Medicines in
%age BHUs
Availability of Medicines in
%age RHCs
Antibiotics <25% <25%

73
Analgesics
Paracetamol 70%
Antituberculosis
Streptomicin, Isoniazid
Pyrazinamide, Ethambutol
<50% >80%
Rifampicin <50% 50-80%
Antimalarials
Fansidar <50%
Chloroquin <50% 50-80%
Obsterics
Oxytocin <25%
Source: NPPI Baseline Survey, Sindh 2009, One UN Program in Pakistan, NMNCH
Program, & Department of Health Government. Medicine availability in THQs and DHQs, particularly of emergency medicines, is also sub-optimal. Asides from dexamethasone, the availability of emergency medicines ranges between 30-50%, and is even lower for certain basic drugs such as Calcium Gluconate and Magnesium Sulphate 32. Availability of basic obstetric care medicines was also very poor with 45-60% availability of ergometrine and oxytocin and 0% of mesoprostol. Availability of antibiotics was comparatively better however only 1 antibiotic had 100% availability with availability of others ranging between 25-80%.

74
Table 13. Availability of Different Medicines in THQHs and DHQHs
Availability in % THQs Availability in % DHQs
Emergency Medicines
Diazepam and Frusemide 50% 50%
Dexamethasone 80% 86%
Cagluconate and
Magnesium Sulphare
20% 3%
Insulin and Adrenaline 30-40% 30-40%
Antibiotics
Cloxacillin 80% 25%
Amoxacillin 56% 100%
Metronidazole 100% 73.3%
Ciprofloxacillin 40% 60%
Obstetric Medicines
Ergometrine 60% 46%
Oxytocin 60% 56%
Misoprostol 0% 0%
Source: NPPI Baseline Survey, Sindh 2009, One UN Program in Pakistan, NMNCH
Program, & Department of Health Government. . Shortage of medicines for, at least for obstetric care, has also been reported by other studies. Essential low cost drugs such as iron tablets, folate tablets, broad spectrum antibiotics and oxytocin were largely unavailable at primary and secondary health facilities 33. while Magnesium Sulfate needed for basic emergency obstetric care services was only sporadically available or completely unavailable 34
Procurement and Supply of Drugs: Procurement of drugs is based on an essential list of medicines specific for each facility tier, however procurement in practice has also frequently involved purchasing of other drugs not on the list. Although a computerized Health Management Information System (HMIS) exists there is little link between case volume and morbidity generated by HMIS reports and the process of forecasting and budgeting. Purchasing is done on the basis of cheapest tender submitted by any licensed drug production company. This has often been criticized as resulting in a low quality threshold as company registration is used as the only quality criteria and with presence of 500-650 licensed production companies in Pakistan, it does not serve to discriminate on quality aspects. The onwards supply chain essentially relies on manual record keeping and although a computerized drug logistics management systems is in place for the GFATM it is yet to be applied to the public sector.
Existing public sector procurement practice has resulted in curtailing drug expenditure. A median price ratio (MPR) compares local price to international price and a MPR of greater than 2.5 indicates excessive medicine prices. Generics purchased by public sector are either below or equal to the international price index however branded drugs have been bought up to 3.5 times the international reference prices 26. The price index of public sector, for both generics and branded drugs, is more efficient than that of the private sector in Pakistan. Whether efficiency has been achieved as a result of quality compromise, needs serious exploration. Anecdotal evidence highlights institutionalized malpractices in procurements

75
where standard mark-ups are charged as a result of collusion between public entities and production companies (N2 35.
Table 14. Median MPRs for innovator brands and lowest priced generics in the public (procurement only) and private sector (patient price only)
Median Price Ration (MPR) to Reference
Price (MSH, 2003)
Reference
Price
Sector Type and No.
of Medicines
Median MPR
(25% - 75%
IQR)
Minimum
MPR
Maximum
MPR
MSH, 2003
Public Brand (n=2) 2.24 (1.60-2.87) 0.96 3.51
Lowest Priced Generic (n=14)
0.57 (0.38-0.74) 0.24 1.04
Private Brand (n=23) 3.36 (2.20-5.88) 0.72 26.20
Lowest Priced Generic (n=21)
2.26 (1.15-3.60) 0.20 7.02
Source: Synthesis report of medicine price surveys undertaken in selected countries ,WHO-EMRO 2008. Procurement has traditionally been done at the provincial level with supply onwards to different districts however as a result of devolution to district level under the Local Governance Ordinance of 2001 drug budgeting, procurement and management took place at the district level for a stretch of nearly ten years. With lapse of the ordinance in 2010, it is uncertain whether there will be a shift back to centralized procurement and supply. As yet there has been no study to assess the relative performance of district versus provincial based drug management.
Issues related to drug storage & dispensation: A survey of first level care facilities, district hospitals and tertiary hospitals conducted as part of Emergency Drug Supply Project in NWFP, Punjab and Balochistan, highlighted issues related to drug storage and dispensation2; 36. Dispensing time on average is merely half a minute which is inadequate for good dispensing while communication with patients was poor and is a cause for concern given low awareness level of patients. Preparation of prescriptions by dispensers is often unhygienic, prone to mistakes and every one in five prescription is dispensed without validation. Preparation of drugs, labeling of drugs and record keeping were also inadequate. Storage issues were also examined at public sector facilities. It was found that while stock auditing was satisfactory at majority of sites, presence of essential drug list was seen in only 1 facility, storage conditions including temperature maintenance, hygiene and pest control was unsatisfactory at majority of places, and actual store capacity was not known by 97% of storekeepers. Store keepers lacked both pre-service and in-service training on proper stock handling. Another study reports labeling and storage of anesthetic medications across 58 operation rooms. Only 15% of operating rooms were compliant with proper drug labeling 36.
2. New Modalities of Health Care Provision – Contracting out of Health Facilities

76
The Government of Pakistan launched a country wide program known as the People’s Primary Healthcare Initiative (PPHI) involving contracting the management of BHUs for improved service delivery. Out-sourcing of BHUs has been done to the National Rural Support Program (NRSP) and the initiative is administratively housed under and financially assisted by the Federal Ministry of Industries. It is an example of contracting-in through management contracts and involves outsourcing the operation budget of BHUs by the department of health to the contractor accompanied with financial and administrative powers for flexible usage of budget and staffing to improve BHU utilization. Overall, 2391 BHUs and 701 other health facilities including dispensaries and MCH centers have been contracted out over 127 districts including 36 in Punjab, 23 Sindh, 30 in Balochistan, 31 in NWFP and 7 in Gilgit-Baltistan. Further experiments with alternative financing models are underway with performance based contacting out, contacting in and competitive voucher schemes being rolled out in the province of Sindh with Norwegian government and One UN Program assistance. Availability of medicines at contracted BHUs:A study to evaluate the pilot of BHU contracting in Rahim Yar district of Pakistan was conducted using intervention and control districts. Although it found mixed result with improvements in curative care and under performance in preventive and promotive care, drug availability was improved in contracted BHUs. Users reported 30% availability of medicines in contracted BHUs as compared to only 7% in non-contracted37. A national third party evaluation has been recently conducted which confirms that there have been improvements in essential drugs availability. Overall 22.5% of contracted BHUs were in the highly satisfactory category for drug availability as compared to only 8.3% of non contracted BHUs, while close to 87% of non-contracted BHUs fell in the unsatisfactory or highly unsatisfactory category compared to 57% of contracted BHUs. Greatest improvement with contracting was seen in Sindh and least in Khyber Pukhtunkhwa. A breakdown of results by essential drugs shows that highest improvement was in availability of amoxicillin, oral pills and chloroquin, with little change seen in availability of iron/ folic acid and IV infusions.

77
Table 15. Availability of Essential Drugs and Vaccines: Comparison between Contracted and Non-Contracted BHUs
Source: Third-Party Evaluation of the PPHI in Pakistan Volume 1 – Draft One for comments - 14 December 2010
Source: Third-Party Evaluation of the PPHI in Pakistan
Procurement and Supply in Contracted BHUs: The contracted BHUs have a more expanded list of approved drugs - 117 drugs as compared to 70-80 drugs at non-contracted BHUs – with some drugs falling outside the national EDL. Procurement and supply of drugs in the

78
case of contracted BHUs is centralized at the provincial level. Some adaptation of public sector purchasing rules has been done for procurement and purchase not necessarily bound by cheapest tender in an attempt to improve drug quality. Although availability has been proven to be higher, there are concerns over presence of inappropriate drugs at BHUs not required for first level primary care. Standardized and clear selection and procurement systems are needed across all provinces. 3. Essential Medicine Management during Emergencies In Pakistan, areas affected by the earthquake in 2005 and floods in 2010 are being supported for drug supply through the WHO and international NGOs. Assessment of essential medicines management in disaster hit areas in Pakistan showed that a steady supply of medicines without stock-outs was seen in 56 first-level care government facilities of calamity hit area 38. WHO has been assisting in the procurement and supply of drugs to in disaster areas and has outlined modalities for acceptance of donated medicines, assisted in speedy procurement, developed tools for forecasting, designed customized kits and implemented a computerized logistic support system for assisting in sustained supply and inventory control. Due to lack of WHO certified production units in Pakistan, drugs are procured internationally. A computerized Disease Early Warning System provides alert on diseases meeting in disaster areas for timely provision of essential and life saving drugs. Large international NGOs have also been directly procuring and dispensing drugs through their health delivery network. The most notable amongst the INGOs is Merlin which is providing services to a population of 2 million though 100 government health facilities.
4. Private Sector Market
Composition of private sector: In Pakistan, 79% of the population utilizes the private health sector 22. Private providers largely rely on private pharmacies and medical stores for provision and dispensing of medicines to patients with few large hospitals maintaining own chain of selection and supply of medicines. Of the total expenditure on medicines, private health expenditure on medicine comprises nearly three-fourth with the burden borne by households through out of pocket payments (Lancet 2009). The private sector comprises a wide mix of providers including at least 20,000 registered general practice clinics, 340 dispensaries, 300 MCH centers and 450 laboratories/ diagnostic centres, however actual numbers are probably much higher as all cadres of government health staff also maintain private practice 27. There are also 500 small to medium sized hospitals and although large regular hospitals are much fewer in number (WHO-EMRO 2011) they include some of the longest established philanthropic hospitals that continue to be heavily utilized (Rahman 2008). In addition there are 1800 local NGOs providing health care services including few large national NGOs and several small-medium scaled NGOs. Beside the allopathic sector, there are at least 52,600 registered unani medical practitioners providing non-allopathic remedies. Private pharmacies/ medical stores: Pharmacies and medical stores are an important source of care as there is little restriction on drug sales and patients frequently resort to self medication. Although there are no national figures for self medication, available studies indicate 6-51% depending on the contextual setting (Thaver & Haider 1995; Sturn 1997), and figures are nearly two decades old and require updating. There are 45000-50000 pharmacies and medical stores in Pakistan (Butt et al 2005), one of the highest numbers in LMICs.

79
Many drug sellers have minimal formal education and little or no professional training; of those with training, most were absent from pharmacies (Rabbani et al 2001) a practice also observed in other developing countries. While there are regulatory checks on drug quality at retail outlets there is little regulation of quality of retail outlet. A cross-sectional survey of 311 pharmacies /medical stores in Rawalpindi showed that the proportion of pharmacies meeting licensing requirements was only 19.3% [95% C.I: 15.1, 24.2] 39. Qualified staff was present in only 22% of pharmacies. Only 10% had a temperature monitoring device and only 4% had an alternative power supply for refrigerators as a back-up for frequent power outages.
Availability of medicines in private sector: In private retail pharmacies medicine availability is higher than public sector both for generics and originator brands. Availability of originator brands exceeds that of low cost generics with respective figures of 59% for originator brands and under 30% for low priced generics. There is excess availability of originator brands in the private sector, exceeding the 23-47% range found in LMICs while low priced generics needs to be increased as it falls much below the 50-75% availability figures for LMICs. The originator brand versus generic imbalance is influenced by local regulations on production of medicines as well as demand, marketing by industry and demand of health care providers and patients. Marketing of Drugs to Health Providers: Malpractices in the distribution chain are evident in the area of marketing, where members of the industry collude with health providers in order to promote the use of medicines, products, and technologies without regard for cost, quality or appropriateness of use (Nishtar 2010). Health care facilities whether in the public and private sector, with extremely few exceptions, do not place any restriction on industry representatives to health providers. Pakistan Medical and Dental Council’s ordinance on relationship between the industry and registered doctors and dentists is vague at best. It does not prohibit the receiving of gifts, inducements, or promotional aids by registered practitioners from pharmaceutical industry provided it does not compromise professional integrity 40 Visit by industry representative for many general practitioners is alarmingly often the only source of treatment information, underscoring the lack of in-service training, however information provided is questionable. A study found that 18% of sales advertisements had unjustified or misleading claims 41. Another study involved promotional brochures claiming that full prescribing information was available on request. When doctors requested information from a mix of 45 multinational and local companies 26% letters received a response and only 15% of responses met the WHO criteria for optimal drug information 42. 5. Trained Human Resource: Inadequate supply and use of pharmacists: Pharmacists in developing countries are still underutilized and their role as health care professionals is not deemed important by either the community or other health care providers (Azhar et al 2009). There is inadequate supply of pharmacists with a total of 28 pharmacy institutions but only 8102 pharmacists in the country as compared to 110,000 doctors. This provides a ratio of 0.9 pharmacists: 10000 population as opposed to a recommended ratio of 1 pharmacist: 2000 population (WHO-EMRO 2009). Among the total number of pharmacists in Pakistan, approximately 55% are engaged in the production of pharmaceuticals – 15% of them working at the federal and provincial drug control authority and hospital pharmacy level – with another 15% in sales and marketing of pharmaceuticals, 10% in community pharmacy, and the rest 5% in teaching and research
80
(Azhar et al 2009). Particularly acute shortage of pharmacists is seen in the areas of drug procurement, management and dispensing across both the public and private sectors. Within the public sector, the post of pharmacist is only seen in district and teaching hospitals, however numbers are meager with for example only 1 pharmacist posted in Civil Hospital Karachi a large teaching hospital with an OPD of 800 patients/ day and 1500 beds. Although elsewhere in the world the role of pharmacists is recognized in community pharmacies, hospital and drug regulatory authorities, the health care system of Pakistan has yet to recognize this role. Regulation of pharmacy practice: There are legal provision requiring pharmacists to be registered and requiring private pharmacies to be licensed however National Good Pharmacy Practice Guidelines have not been made public by the government 43. A Pharmacy Council has been recently formed under the Pharmacy Council Act 2009 to regulate the practice of pharmacy. Specific functions include developing and overseeing standards for conduct of pharmacists and allied staff, standard of teaching and accreditation of pharmacy degrees, maintaining registers of qualified pharmacists and pharmacy technicians, and training programs, and organization of continuing training courses. The Pharmacy Council is currently functional however its functions are limited to the relatively low numbers of pharmacists in the country and has no control over the vast number of medical stores in the country manned by those holding no training or qualification in pharmacy.
Regulation: Licensing, Registration, Pricing, and Quality Control
Drug Policy & Acts: Access to essential medicines/technologies as part of the fulfillment of the right to health, is recognized in the national constitution. Regulation of the pharmaceutical sector had traditionally been by the Drug Act 1940 and the Pharmacy Act 1967. In 1972 the Generic Drug Act was introduced but had to be revoked in the wake of strong opposition by the commercial sector and the medical community 35. The Drug Act 1976 currently regulates the pharmaceutical sector and is a comprehensive document setting out extensive stipulations for industry licensing, drug registration, quality control etc. However implementation of the act is loosely monitored and creates space for abuse. Furthermore, it has not been updated since the declaration of the World Trade Organization’s (WTO) statutes and Pakistan’s Patent Ordinance 2000. A National Medicines Policy was also formed in 1993, updated in 1997 and is currently again in the process of update. At present there is no strategic plan for implementation of National Medicine Policy. Issuance of Statutory Regulatory Orders further creates confusion and unevenness in the application of policies. In response to quality concerns over drugs in the market, the Federal Cabinet has approved the establishment of an independent Drug Regulatory Authority (DRA), however its constitution has not taken place so far.
Table 16. Areas Covered by National Medicines Policy
Selection of essential medicines Yes
Medicines financing NO
Medicines Pricing Yes
Procurement Yes
Distribution Yes

81
Regulation Yes
Pharmacovigilance Yes
Rational use of medicines Yes
Human resource development Yes
Research Yes
Monitoring and evaluation Yes
Traditional Medicine Yes
Source: Pharmaceutical Country Profile. Pakistan. Ministry of Health. 2010
Regulatory Functions & Organizational Structure: The federally based Ministry of Health (MOH) is responsible for licensing of drug production companies, registration of drugs and pricing while the function of quality control lies with the provincial Departments of Health (DOH). Each function has detailed and well developed guidelines given by the Drug Act 1976.
Source: Ministry of Health Pakistan
Drug Production: Pakistan meets 70% of its domestic demand of medicines from local production and 30% through imports (MOH 2011). Although at the time of independence in

82
1947, there was hardly any pharmaceutical industry in the country there are currently 30 multinational and 411 local units involved in pharmaceutical manufacturing 44. However, share of market both in terms of number of medicines manufactured and revenues, is almost evenly divided between the few multinationals and large number of local companies. The local market for pharmaceuticals in Pakistan has been expanding at a rate of around 10-15% over the last few years. The value of pharmaceuticals sold in Pakistan exceeded US$1.4 billion, which equates to per capita consumption of less than US$ 10 per year while it is expected to exceed US$2.3 billion by 2012 45. The Pakistan pharmaceutical industry has a small share of the international market with an export turnover of US$ 400 Million and accounts for 1% of the exports 45. However there is wide variation in quality of drugs manufactured with existence of both sophisticated manufacturing units having well developed quality monitoring mechanisms as well as low cost units having non-existent quality assurance systems 35. There is lack of local production of WHO certified drugs which are mandated for usage in donor funded programs such as GFATM and also required for use by international NGOs serving mainstream and refugee populations. So far industry has not shown interest in investing in quality assurance for WHO or FDA certification, and quality measures are up to interest and motivation of individual production units. Drug Licensing: In Pakistan, there are legal provisions requiring manufacturers to be licensed and requiring manufacturers to comply with Good Manufacturing Practices 43. Drug Act 1976 provides a system for licensing of each manufacturing unit. The Licensing Board at the MOH examines and approveslayout plans of new manufacturing units, inspects units through panel of experts and processes applications for renewal of licenses. However there is wide variation in terms of quality of registered production units. At present there is no WHO certified nor FDA approved manufacturing facility in the country. In the process of manufacturing, very few manufacturers in Pakistan comply at best, only with minimal quality standards and the barest minimum current Goods Manufacturing Practices (GMP) stipulated criteria raising quality concerns. These entities find compliance with regulations costly and try to influence regulators to get their products registered, speed up approval processes, get favorable prices or to have their drugs included in the formularies of various hospitals and institutions 35. Drug Registration: The Drug Registration Board processes application for registration of any new pharmaceutical item including new molecules, new dosages of approved molecules as well as different brands of approved molecules under the Drug Act 1976, the de-registration process is also a function of the board. Registration can be made on basis of proven efficacy in any country and does not require bio-equivalency results from Pakistan. Cost effectiveness studies are also not required for registration of products. At present there are 1100-1200 registered molecules and approximately 76000-88000 registered products which is one of the highest across LMICs. This is due to a high number of drug registrations for example there are seven forms of Acetaminophen in the market being sold under different brands, dosages and prices. Another underlying reason is that there is no systematic system of de-registration of old and superfluous products. With record keeping still manual it is difficult to access and review data of the numerous registered products. Pricing & Issue of Orphan Drugs: In Pakistan, there are regulatory provisions affecting pricing of medicines targeted at manufacturers, wholesalers and retailers. Pricing is fixed at the MOH with the standard practice of pricing based on reported price of raw material, other input and overhead costs. This also creates opportunity for collusion to obtain high prices 35. As yet there has been no move towards a clear pricing formula. By law, wholesalers can

83
markup goods by maximum 2% of the final price and retail markup for locally produced medicines is 15% of the final price. Regulations exist mandating that retail medicine price information should be publicly accessible and the information is made publically available through the Official Gazette Notification and printed on each medicine box. The capacity of inspectors to comprehensively monitor prices and ensure adherence to officially set prices is limited and there is no official data on levels of adherence 46. The MOH has consistently provided measures for low pricing tax breaks as well as price control. There is tax exemption on import of raw material and equipment for basic manufacturing of drugs and is of considerable importance given that there is little production of raw material with most being imported in large quantities from different countries. In addition, medicines are exempted from the general sales tax on commodities. Moreover, full import tariff exemptions are provided for UN partners and for HIV/AIDS medicines when procured by a donor funded program 46. Asides from tax breaks, there is flat price control is in place since the last 10 years in which prices of all pharmaceutical products have been frozen. The only attempt at partial price de-regulation attempt led to several fold increase in price of drugs and had to be rescinded. The issue of Orphan Drugs: While price control is well intentioned it has also contributed to the issue of ‘Orphan Drugs’ by which essential low cost drugs have disappeared from the market due to lack of profit margins. The list is alarming and includes basic essentials such as phenytoin, thiazide, adrenaline, thyroxine, primaquin, folic acid to name a few. Action by the MOH to enforce production of ‘orphan drugs’ has usually been counter productive leading to sub-standard production. Reliance is often on import of ‘orphan drugs’ to plug in chronic shortages. The MOH has not yet explored the potential of various approaches of differential pricing to control prices of drugs on the National EDL. Differential pricing is expected in the new National Drug Policy currently under development.
Quality Control: The quality of drugs on the market is an important public health concern in many countries. In Pakistan the quality monitoring of products on the market is done by the provincial governments while registration authority, as earlier mentioned, rests with the federal government. Quality control in Pakistan follows the traditional approach of being a government dominated function relying on monitoring and punitive action. There has been little attempt for more participatory regulation of drug quality that could result in more buying in from industry, distributors ns retailers. The basic functions for quality monitoring include sampling and testing of drugs being sold at retail outlets, inspection of drug storage and inspection of drug transportation. Investigation reports for sub-standard drugs, misbranded or adulterated drugs are sent to Federal Licensing and registration Boards and through them to all the provincial governments for ensuring effective recall of drugs. 7 laboratories exist in Pakistan for Quality Control testing, however reportedly only 3 have required capacity. The federal Drugs Testing Laboratory is located at Karachi and an Appellate Laboratory for re-testing is in Islamabad. The Provincial Governments have their own Drug Testing laboratories at Peshawar, Quetta, Lahore and Karachi. In the past 2 years, 60,000 samples were taken for quality control testing of which 1,194 failed to meet the quality standards, however results are not publicly made available 43 Issues of counterfeit medicines: According to WHO, 25% of all medicines in developing countries are counterfeit with prevalence far higher in certain countries. Counterfeit medicines constitute between 40-50% of total supply in Nigeria and Pakistan 47.Counterfeit

84
medicines result in either under-dosage or even active harm causing injury or death. It also undermines the incentives of registered pharmaceutical producers to invest in quality control. Report from pharmaceutical manufacturers of the European Union and another from US Trade Office have alleged that the Pakistani market has almost 50% spurious drugs 48. Counterfeit medicines can get access into the medicines chain either through regulated or unregulated channels. The latter include manufacturing of spurious drugs by unlicensed manufacturers and smuggling. Both spurious as well as sub-standard medicines can also get access into the market through regulated channels. For example, when licensed manufacturers use substandard raw material and/or fail to comply with stipulated manufacturing practices, quality may be detrimentally affected. Similarly, official channels of trade can involve trade of counterfeit medicine inadvertently or intentionally and it is reported that 6-10% of cross border trade in medicines in developing countries comprises of counterfeit medicines (Nishtar 2010).
Research fund tax: A Central Research Fund is maintained by the MOH for investigation, evaluation or development of a drugs and its use is governed by detailed guidelines given by the Drug Research rules 1978. Every pharmaceutical manufacturer is supposed to contribute 1% of gross profit, before deduction of income tax, towards the Central Research Fund 46 An Expert Committee is responsible for fund allocation to individuals and/ or Institutions, which are engaged in research in the field of pharmacy and medicine however to date there has been little utilization of research funds.

85
Literature review - Lebanon
Here a review of what has been written (both journal articles and documents).
You can build on the paragraphs you had previously. It just needs to be a more
formal review.
Journal articles
Using the expanded search strategy, a total of 44 journal articles were identified
as relevant to ATM (Appendix 5-A). No articles specifically discussed the issue
of access and no articles examined ATM in a comprehensive manner that
includes the four domains of the WHO 2004 framework.
As common in ATM research globally, the area of rational selection and use has
received attention from researchers in Lebanon. Saab et al (2001) described that
“In 1966, Lebanon had around 19,000 drug formulations registered in the
Ministry of Public Health. The government decreased that number to 5400 in
1992 through numerous interventions.” They described the process of
development of a list of essential drugs for primary care by an ad hoc committee
set up by the Lebanese government.
Several studies have looked at prescribing behaviors, in general or for specific
conditions. In a university health center, Hamadeh et al (2001) studied
prescribing practices and found low rate of generic and essential drug
prescribing and frequent prescribing in respiratory or ear infections (about 50%
of encounters). Bizri et al (2002) reviewed available data at the time on patterns
of antibiotic prescribing in ambulatory care. In a four-country (Lebanon,
Morocco, Spain and USA) study of medical management of menopause, Sievert
et al (2008) reported that physicians were generally well informed and that
prescription patterns and perceived benefits of hormone therapy appeared to
reflect local medical culture rather than simply physician characteristics. El
Sayed et al (2009) described that pediatricians prescribed antibiotics to infants
at least once in 21.4% of cases diagnosed as the common cold and 45.5% of

86
cases of acute bronchiolitis. Antibiotics misuse was more common among
infants born to mothers with lower educational levels. Pediatricians tend to
prescribe antibiotics in dispensaries more often than in private clinics. Abi Risk
et al (2010) reported that primary care physicians prescribed antibiotics for
pharyngitis at high rates (42% with 68% in winter and 38% in summer) and “No
physician used all the criteria in the score adopted by the CDC to decide on the
prescription of antibiotic or throat culture.”
Prescribing practices in hospital settings appear largely adequate. Azzam et al
(2002) reported that antimicrobial prophylaxis for surgical procedures was
appropriate. Kanafani et al (2005) found that antibiotic prescribing for acute
cholecystitis was erratic and costly in the absence of international guidelines on
appropriate use. Nassar et al (2008) found high rates of appropriate prescribing
among obstetricians for a specific indication. The area of management of post-
operative pain was, however, sub-optimal as reported by Madi-Jebara et al
(2008).
Several studies described development of practice guidelines and other
interventions to improve prescribing practices for managing specific conditions.
Azar (2000) proposed practice guidelines for managing hypertension in
diabetics. El-Hajj Fuleihan et al (2002) proposed guidelines for managing
osteoporosis. These guidelines were updated in 2008 (El-Hajj Fuleihan et 2008).
Riachy et al (2010) reported that an intervention using clinical guidelines aimed
at improving the use of nebulizers in a university hospital did not succeed in
lowering inappropriate prescriptions. Zgheib et al (2011) describe the
introduction of “rational prescribing” sessions, using team-based learning
format, to medical students at AUB.
Several studies have looked into medication use patterns. Naja et al (2000)
carried out a first pharmaco-epidemiological study on benzodiazepine
consumption, as such medicines were often available without a prescription at
the time. Benzodiazepine use during the past month was found in 9.6% of
subjects and described as “particularly high”. Benzodiazepine dependence was
found in 50.2% of users. Makhlouf Obermeyer et al (2002) analyzed medication

87
use in the 1999 National Household Health Expenditures and Utilization Survey
and found that education and employment were associated with lower rates of
medication use while higher socioeconomic status was associated with higher
use rates. The researchers highlighted three areas for further research and
interventions: the higher use of antibiotics in rural areas, the greater use of
psychotropics by women, and the possible obstacles to obtaining needed
medications for those with lower incomes. Among elderly Lebanese, Saab et al
(2006) documented that about 60% were taking at least one inappropriate
medication and identified correlates of inappropriate use. Soldberg (2008)
reported increasing use of medication to treat mental health challenges which
may be related to Lebanon’s recent history of conflict. In a multi-country study
involving Lebanon, Scicluna et al (2009) documented the highest rates of self-
medication in Lebanon (37%). Lebanon had the highest percentage (60%) of
people keeping antibiotics at home. There was a significant association between
antibiotic hoarders and intended users of antibiotics for self-medication.
Because irrational use of medicines is common, several studies have reported on
consequences. As antibiotics are accessible without a prescription, several
studies have documented the consequences in terms of microbial resistance
(Araj 1994; Araj 1999; Araj & Kanj 2000), including in specific conditions such
as tuberculosis (Hamze et al 1997; Araj et al 2006), haemophilus influenzae
(Santanam et al 1990) and streptococcus pneumonia (Araj 1999; Harakeh 2006;
Uwaydah et al 2006).
Major et al (1998) studied the incidence of drug-related hospitalization in a
tertiary medical center and its association with self-medicating behavior. They
found that among adults and children admitted, 10.2% and 7.9% had drug-
related illnesses, respectively. Adverse drug reactions accounted for 7.0% and
5.7% and therapeutic failures for 3.2% and 2.2% of adult and pediatric
admissions, respectively. Self-medication was commonly practiced (52.6% of
adults and 41.6% of children). Interestingly, female sex increased the risk of
adverse drug reaction in adults, whereas self-medication decreased the risk. In
children, the risk of adverse drug reaction was increased in lower
socioeconomic groups. Kassab et al (2005) reported the first-year results of a

88
national system of adverse drug reactions. They found that antimicrobial agents
were the most common drugs involved in such reactions (43%).
Articles concerning the health and supply systems highlighted a few interesting
aspects. Kyriacos et al (2008) studied the quality of amoxicillin formulations in
Lebanon, Jordan, Egypt and Saudi Arabia and found that 56% of amoxicillin
capsules did not meet the United States Pharmacopeia (USP) requirements.
They identified several factors that might jeopardize the quality status of
medicines: lack of effective quality assurance system during manufacture in
both Arab and export countries, and uncontrolled storage conditions, especially
unsuitable pharmacy premises. Use of substandard antibiotic preparations
increases the risk of therapeutic failure and the emergence of drug-resistant
microorganisms.
The practice of pharmacy received important attention. Dib et al (1998)
described pharmacy practice and outlined the challenges. Bou Antoun and
Salameh (2006) carried out a survey among community and pharmaceutical
company pharmacists in Lebanon to evaluate their satisfaction with professional
status and willingness to work as clinical pharmacists. The first group was more
satisfied and more willing to engage in clinical pharmacy. Salameh et al (2007)
carried out a survey of a pharmacist and a nurse in each of 59 hospitals in two
regions of Lebanon on the drug circuit starting from prescription to
administration. There were gaps in all hospitals that could lead to drug errors.
Salameh et al (2008) noted that clinical pharmacy is not professionally applied
in Lebanese hospitals despite the accreditation requirements and showed that
the majority of physicians and nurses thought that interventions by clinical
pharmacists would be beneficial. Khachan et al (2010) described pharmacy
education in Lebanon but did not describe aspects relevant to ATM.
Published and unpublished documents and gray literature
Using the previously discussed search strategy and supplemented with
documents provided by key informants, the research team has assembled a
library of documents of direct relevance to ATM (Appendix 5-B). It is beyond

89
the scope of this report to review all such documents. Therefore we focus in this
section on observations about key aspects of the ATM situation in Lebanon.
These observations supplement the evidence-based review of research published
in peer reviewed journal articles (see section 5.1.1. above) and can inform the
agenda for essential research on ATM.
Expenditures on medicines (ATM) are an important concern in Lebanon.
Different resources estimate that medicines account for 25% of total health
expenditures (Hamra et al 2009; Chebaro 2010). Reported market sales in 2007
exceeded USD900 million (Ammar 2009, p. 102). The Lebanese
pharmaceutical market is expected to reach USD1.1 billion in 2015 (Chebaro
2010). This means that Lebanon, with a population of a little more than four
million, comes third in the region after such populous countries as Egypt and
Saudi Arabia in terms of the bill for medicines. About 80% of medicines are
sold in pharmacies, 14% consumed in hospitals and 6% purchased directly by
the MOPH (Ammar 2009, p. 103).
An important proportion of spending on medicines is out-of-pocket (OOP),
accounting for 67.8% of total spending on medicines (rate calculated from
Table IV-2, Ammar 2009, p. 104) and for 31.01% of total household spending
on health in 2005 (which increased from 25.35% in 1998) (Ammar 2009, p.
104). Between 1998 and 2005, while spending on medicines by
“intermediaries” increased by 34.2%, household spending on medicines
increased only by 0.7% indicating that “cheaper sources of supply have become
available for at least a part of the population” (Ammar 2009, p. 104). In 2005,
household annual spending on medicines was estimated between USD100 and
USD 125 per capita (Ammar 2009, p. 102; Hamra et al 2009). However, there
are indications that this figure is underestimated (Hamra et al 2009).
Lebanon is the leading importer of pharmaceuticals in the region. There are
between 85 and 142 agents (importers) (Chebaro 2010; Hamra et al 2009) who
import some 5,995 drugs from more than 558 factories in 32 countries
constituting between 92% and 94% of the products available in the market
(Hamra et al 2009; Chebaro 2010). Among all registered medicines in 2008,

90
79.42% came from European countries, 9.59% from Arab countries, 5.75%
from USA and 5.24% from other countries (Ammar 2009, p. 102). The local
pharmaceutical manufacturing industry is still small but is expanding. In 2010,
medicines manufactured by seven local factories made up from 6 to 9% of all
medicines consumed (Hamra et al 2009; Chebaro 2010).
Prices of medicines are a major concern. In a study of prices of 32 medicines
based on an international standardized methodology, Karam (2004) found that
the public sector purchases medicines at reasonable prices for poor patients and
provides medicines for free in public health facilities but availability in the
public sector is “very low” and “poor patients are forced to buy expensive
medicines from private pharmacies.” In the private sector, availability is very
good but that “almost all the surveyed medicines are over-priced if compared
with the international reference price and the prices of innovator brands are up
to 5 times more expensive than the prices of their generic equivalents.” Chebaro
(2010) notes that the Lebanese spend three to six times more on the prices of the
essential medicines they need than they should. Karam (2004) also notes that a
“big part of price problem is the current price structure including profit margins,
expenses and fees as well as the incremental calculation method.” Hamra et al
(2009) note that the profit component of prices designated for pharmacies is
considerable, reaching 22.5% of the original price, which encourage
pharmacists to promote for more expensive products. High rates of importation
from European countries and USA (over 85% according to Ammar 2009, p.
102) contribute to the high prices of medicines.
A major contribution to the medicines situation is low rates of generic
prescribing. Karam (2004) notes that Lebanon is a “brand name” country. She
notes that “innovator brands drugs are possibly used more extensively as there
are “no incentives to prescribe and sell generic equivalents.” Ammar (2009, p.
104) attributes this to “absence of any framework for medical prescription
accountability”. The well-known oversupply of physicians, especially
specialists, and pharmacists in Lebanon contributes to high rates of prescribing
and dispending of branded medicines. Hamra et al (2009) note that pharmacists
are not allowed to substitute a prescribed product with a cheaper or generic one.

91
Almost all publications acknowledge the role of aggressive promotion by
pharmaceutical firms and the incentives for physicians to prescribe branded
medicines. For example, physicians commonly reply on pharmaceutical
companies to finance their continuous education by sponsoring their trips to
international conferences (Chebaro 2010). The heavy promotion of brands
creates trade name affinity, discouraging doctors from prescribing generics
(Hamra et al 2009). The MOPH has proposed a code of ethics for promotion of
pharmaceutical products and has recently revised it and re-circulated it to
stakeholders but this document has not been formally adopted by any
stakeholder yet.
At the policy level, Hamra et al (2009) note that Lebanon lacks a “modern
medicine regulatory authority structure in place or a national medicine policy or
policy document that lays out a vision for the future of the sector and that
defines political, technical, economic and health related parameters that form
the framework for pharmaceutical legislation”. While there is large political
interest in the pharmaceutical sector, there is “insufficient will and
commitment” to carry out reform.
There are common media reports of corruption in the medicines sector but there
are no studies that document or measure the level of such corruption. In their
study of governance in the public pharmaceutical sector, Hamra et al (2009)
evaluated vulnerability to corruption of the policy, structures, and procedures in
place at the time of the survey. They found that “the area of medicine
distribution received the highest score and is minimally vulnerable to
corruption; medicines registration, inspection, and procurement are marginally
vulnerable to corruption; and the promotion and selection functions had the
lowest scores and are moderately vulnerable to corruption.”
Research questions emanating from the literature review
It is apparent from the aforementioned literature review that there is important
evidence for policy action to improve ATM. Nevertheless, the review indicates

92
that evidence is lacking in many key areas. The research questions that emanate
from the literature review are provided in Appendix 6-A.

93
Results - Literature on access to medicines issues in the EMR area
We found several comparative studies that used data from EMR or
discussed issues relevant to EMR countries. These are included in the
analyses and data provided in different tables and figures. We also
identified a further twelve international studies that although had no
specific mention of the EMR countries, had important implications
about access to medicines in low and middle income countries of the
region.49-51
{Vreeman 2006}52-59
Among these twelve studies, eight
had been published in 2011 alone. We used these studies to discuss
and highlight some of the identified issues.
Six papers identified via international databases were in languages
other than English. Five papers published in French (2 each from
Tunisia and Morocco and one from Lebanon) and one in Czech
(about Yemen).60-65
We used the abstracts of these studies to include
and categorize them according to the issues and levels of barriers
discussed in the studies.
Producing the evidence: number and geographical distribution of countries
of origins of the identified publications
In total, 151 articles were identified that focused entirely, or in some parts of
the reports on ATM issues in one or more of EMR countries. Most of these
articles (125, 83%) were originated (as the corresponding author's address)
from EMR countries in that sense the majority of evidence on ATM in the EMR
region is homegrown. There is a wide variety in the number of publications per
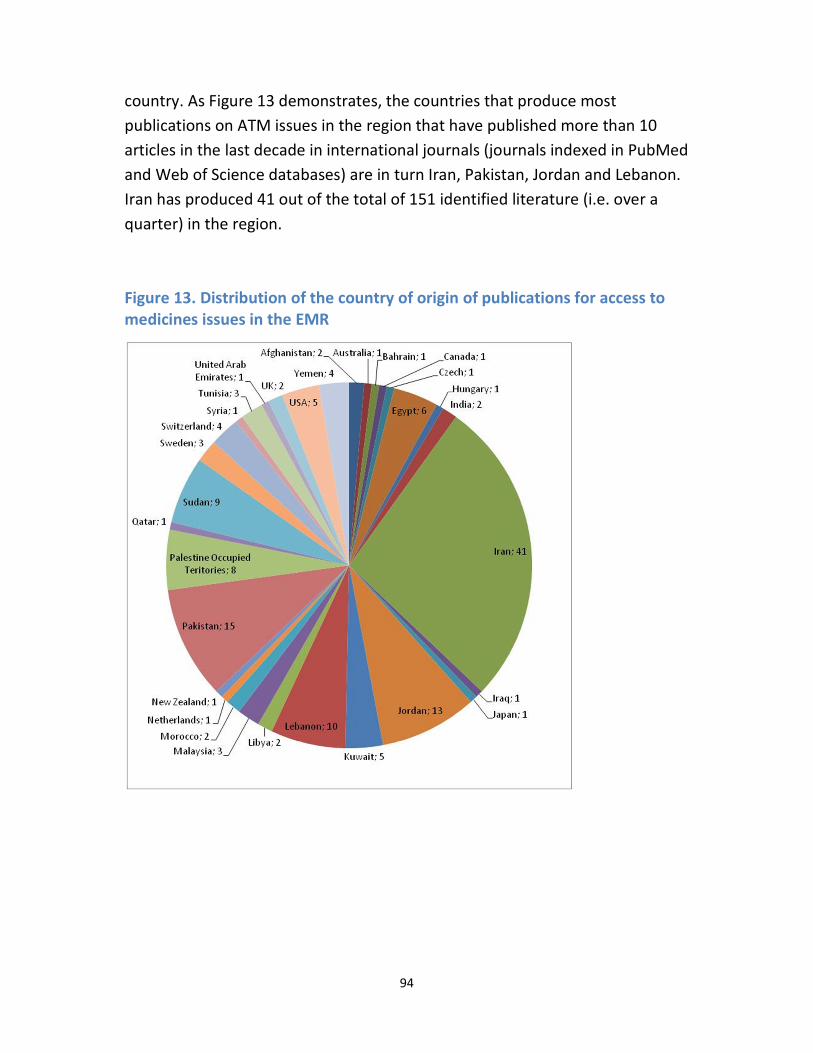
94
country. As Figure 13 demonstrates, the countries that produce most
publications on ATM issues in the region that have published more than 10
articles in the last decade in international journals (journals indexed in PubMed
and Web of Science databases) are in turn Iran, Pakistan, Jordan and Lebanon.
Iran has produced 41 out of the total of 151 identified literature (i.e. over a
quarter) in the region.
Figure 13. Distribution of the country of origin of publications for access to
medicines issues in the EMR

95
The number of publications for some countries is proportionately very low. For
example, if we had excluded the studies from Egypt that were published
because of the presence of WHO regional office in Cairo, then very few studies
from Egypt would have remained in our sample. This is indeed very surprising
given that Egypt is one of the most populous countries in the region, and it
enjoys an expanded academic sector.
EMR The last decade demonstrates a relatively steady growth in the number of
publications per year on ATM in the EMR. This is a good sign that with further
development of health systems in the issue, the number of publications are
growing (see Figure 14). While in the first three years of this period we
observed only about ten publications from the region, the last three years
demonstrates there over 80 studies published. Most of this increase in the
number of publications per year
Figure 14. The number of ATM publications per year. Note that 2011 covers
only the first half of this year.
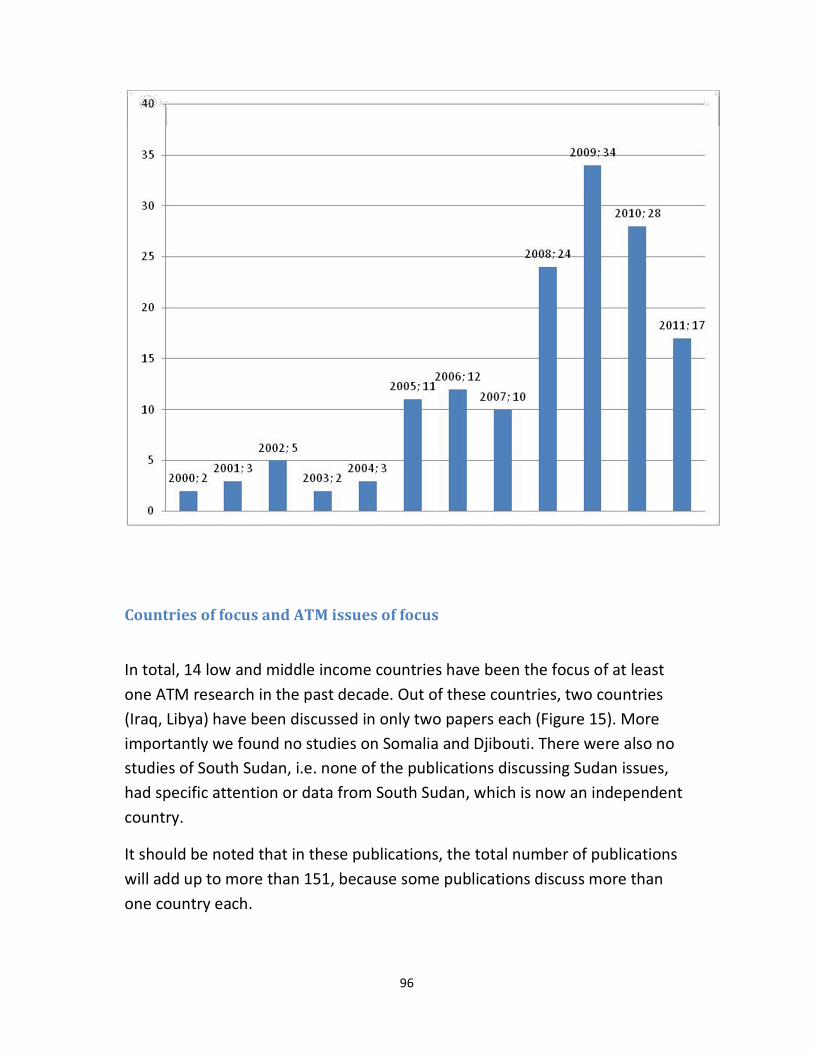
96
Countries of focus and ATM issues of focus
In total, 14 low and middle income countries have been the focus of at least
one ATM research in the past decade. Out of these countries, two countries
(Iraq, Libya) have been discussed in only two papers each (Figure 15). More
importantly we found no studies on Somalia and Djibouti. There were also no
studies of South Sudan, i.e. none of the publications discussing Sudan issues,
had specific attention or data from South Sudan, which is now an independent
country.
It should be noted that in these publications, the total number of publications
will add up to more than 151, because some publications discuss more than
one country each.

97
Figure 15. The number of publications discussing AT issues in EMR's low and
middle countries
It is important also to see what are the ATM issues of focus in the published
literature. We noted the issues of focus for each identified publication, using
the WHO categorization of issues into: affordability (25 publications), financing
(18 publications), rational use of drugs (106 publications), and health system
and availability (63 publications) (Figure 16; Table 17). If a publication was
discussing more than one issue, we noted as many issues as applied to that
publication.
Figure 16. Proportion of publications discussing each ATM issue in EMR
countries

98
Table 17. ATM issues discussed each year in EMR publications
Affordability Sustainable financing RUD
Health system and availability
2000 2 1
2001 1 1 2
2002 1 1 5
2003 1 2
2004 2 1 2 2
2005 10 1
2006 2 8 5
2007 1 1 8 6
2008 4 5 16 9
2009 7 7 20 15
2010 4 20 10
2011 3 3 13 10
Total 25 18 106 63
Also it is visible that despite the importance of cross border issues and the role
of sectors beyond the health sector in facilitating or impeding access to
medicines, scarce attention is devoted to those issues (Table 18). The majority
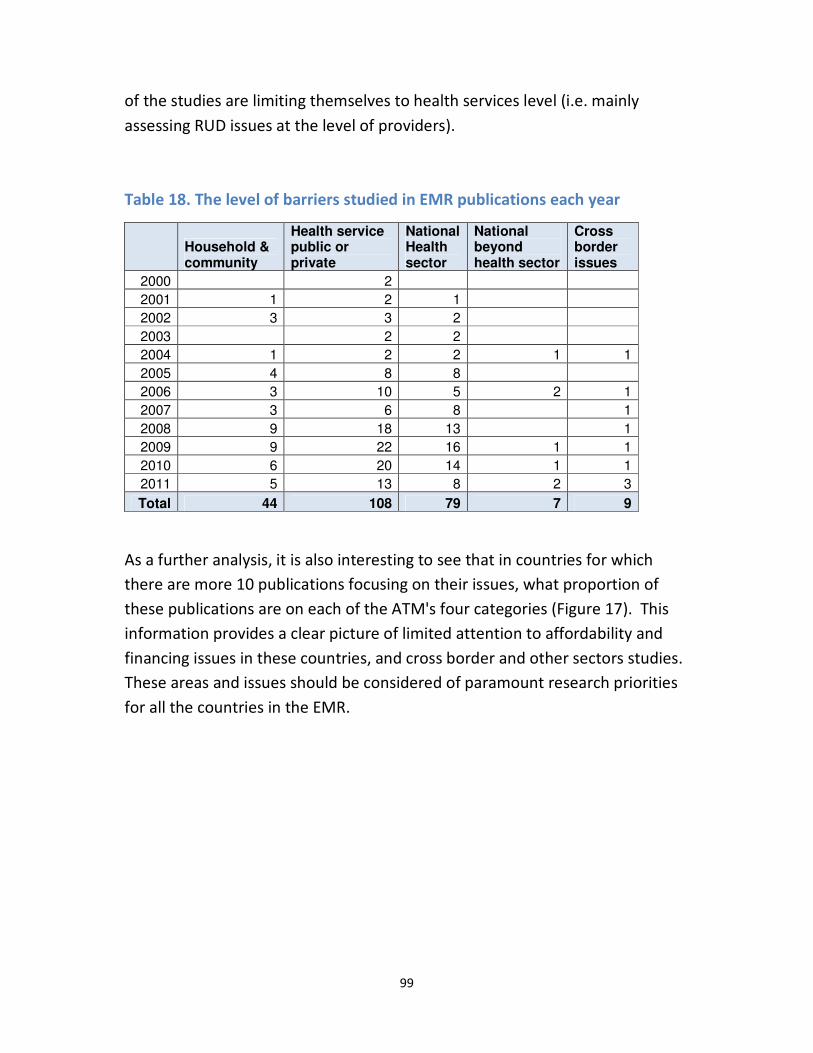
99
of the studies are limiting themselves to health services level (i.e. mainly
assessing RUD issues at the level of providers).
Table 18. The level of barriers studied in EMR publications each year
Household & community
Health service public or private
National Health sector
National beyond health sector
Cross border issues
2000 2
2001 1 2 1
2002 3 3 2
2003 2 2
2004 1 2 2 1 1
2005 4 8 8
2006 3 10 5 2 1
2007 3 6 8 1
2008 9 18 13 1
2009 9 22 16 1 1
2010 6 20 14 1 1
2011 5 13 8 2 3
Total 44 108 79 7 9
As a further analysis, it is also interesting to see that in countries for which
there are more 10 publications focusing on their issues, what proportion of
these publications are on each of the ATM's four categories (Figure 17). This
information provides a clear picture of limited attention to affordability and
financing issues in these countries, and cross border and other sectors studies.
These areas and issues should be considered of paramount research priorities
for all the countries in the EMR.
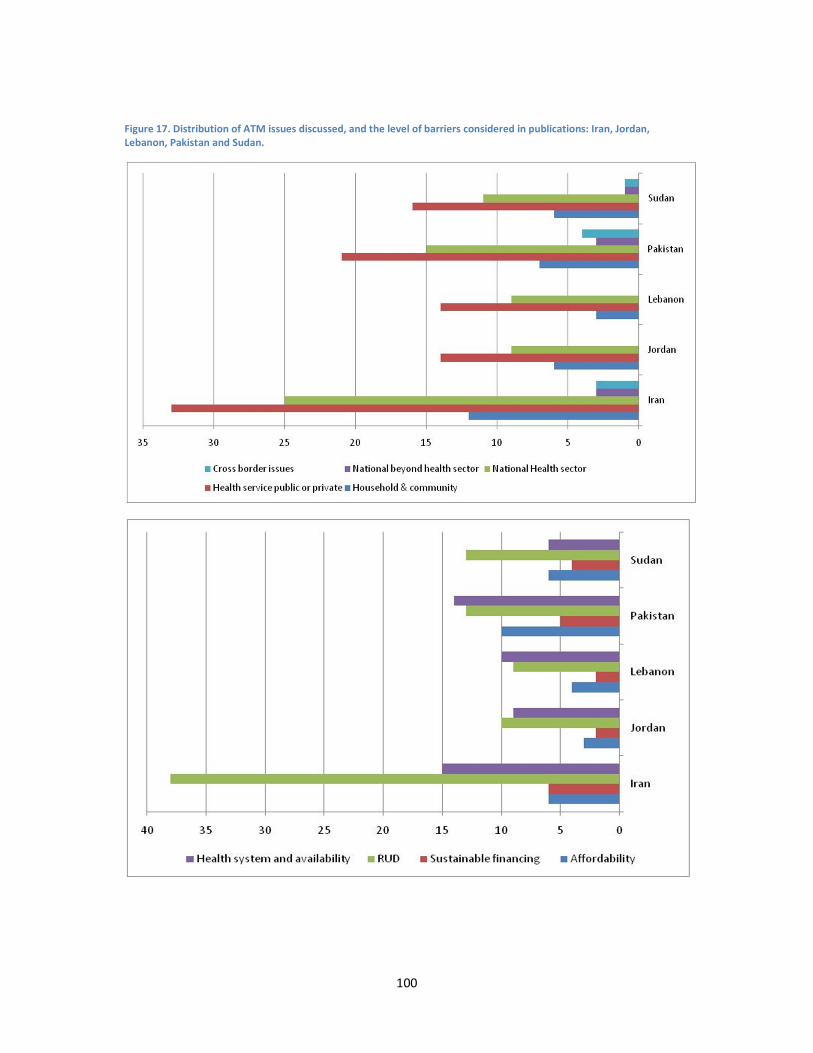
100
Figure 17. Distribution of ATM issues discussed, and the level of barriers considered in publications: Iran, Jordan,
Lebanon, Pakistan and Sudan.

101
Lack of attention to financing and affordability aspects of ATM in EMR studies
is despite the fact that several studies have demonstrated the importance of
these aspects. In an international study using household survey data from
World Health Surveys, it was clear that affordability is a major barrier to access
at the level of household. The study concluded that between 41% and 56% of
households in LMICs spent almost all of health care expenditures on
medicines.66 The study called for expanded benefit packages and further
coverage of medicines in insurance plans in low and lower middle income
countries. Whether or not this will be taken up in the region is another matter.
As reported by Zafar Mirza, among low and middle income countries in the
region, Jordan, Iran, Egypt, Morocco and Tunisia have health care insurance
systems developed and established by the government 67. These schemes have
various successes and limitations which may impede access to medicines. For
other LMICs in the region, without such nationally funded programs, adopting
Wagner et al's advice may be more difficult.
Another study that used a small dataset from Pakistan observed that 45% of
households' out of pocket health care expenditure was for obtaining
medicines.68
Also others assessed the effects of expenditure on medicines on
impoverishing household in developing world.69
They used data from three
countries in the region (among other countries). As an example the study
noted the strong impoverishing effects of using originator brand glybenclamide
instead of generic products in Yemen. Another study focused on the impact of
GIPAP program (that provides free of charge drugs for CML patients) on access
to iminitab for these patients in poor countries. 70
Data from Pakistan and
Sudan was included in the study (among other countries), which in general
suggested that GIPAP had been helpful in improving patient access and health
outcomes.
Another issue for both affordability as well as financing of medicines in LMICs,
is the pricing aspects of medicine. Wagner et al noted that there an array of
reasons and manifestations of price differences for medicines in different
countries. Despite the importance of the issue they noted that literature from

102
developing countries has showed very little attention to pricing issues.49 on the
positive side, Thatte et al provide a useful coverage of procedures for
medicines approval, entry to market decisions and pricing in Pakistan and
three other countries from South East Asia and Western Pacific regions of the
WHO 71
. Obviously this is not the only study from the region on the issue (there
are country specific publications), but very few have looked at the issue
critically in the region.
Other sectors (other than health care sector) effects on access to medicines
are barely considered in publications from the region. A secondary analysis
tried to link data on duration of untreated psychosis with GDP per capita (as an
indicator of country's macroeconomic situation).72 Although it did not include
any ATM study from EMR, it used data from three studies of duration of
untreated psychosis from Egypt, Iran and Pakistan. The general finding of the
study was that lower GDP per capita was correlated with longer duration of
untreated psychosis in low and middle income countries.
Despite the fact many studies assessed health systems and availability aspects
of ATM, there are very few studies that discuss important policy directions on
ATM. For example we did not find any study that had assessed the impact of
essential drug lists initiatives on access to medicines in a country. This is
despite the fact that according to Mirza (2008), by that time all the low and
middle income countries in the EMR region, except Libya and Lebanon, had a
policy of essential drug lists in place.67 Other reports published in 2010 suggest
that now also Libya has a national essential medicines list.73
A study not
specific to EMR countries provides a summary of available evidence on
different interventions for improving access to essential medicines in primary
care settings.74
Fortunately, further attention has been devoted to studies on availability of
medicines than to affordability and financing. An international comparative
study provides a good summary of the picture.75
It identified while in the public

103
sectors of South-East Asia, the Americas and the Eastern Mediterranean
regions, medicines for acute conditions were more available compared with
medicines for chronic diseases, in the European and the Western Pacific
regions medicines for chronic conditions were more available.
We found many studies of RUD issues (Table 17), including several studies that
focused on adverse drug reaction reporting in several countries (see also the
sections relevant to the three country case studies). Still, an eye-opening
international study suggests still along way is ahead of the countries until such
programs are implemented effectively. The study assessed the ADR repots for
artimisin based anti-malaria treatments at global level.76 It concluded that the
ADR systems in countries prone to malaria were extremely weak. In the EMR
region the situation was similar: only three countries in the region (Iran,
Morocco, Tunisia) had ever reported an ADR for such medicines, and the
number of ADRs reported was very small compared to what should be
expected. This is despite the fact the three countries mentioned in the study
are not those with high burden of malaria in the region, while for countries
with hyper- and meso- endemic malaria problems they did not find a single
report of ADR for artimisin based medicines. The same goes with other aspects
of quality of prescribing care in the region. A systematic review of studies of
pharmacy service quality included two papers from Alexandria in Egypt.77
The
studies demonstrated low quality of service and room for improvement in
provision of care at the pharmacies. Similar problems were reported in several
other studies. It is also important to consider the strong and weak aspects of
presence of private sector in health care systems in the region, as there is
evidence from low and middle income countries that private sector performs
as good as the public sector in terms of availability of medicines and quality of
services and responsiveness.54
In a way, maybe it is safe to conclude that even RUD studies have not been
that effective in improving access, or tackling the main issues. Still, the region
should move towards more interventional studies linked with RUD issues in
which the effects if different interventions in improving rational use of

104
medicines are assessed. There are signs, at least in some countries, that a
move in that direction is shaping.78-82
Limitations of the regional literature review
The bibliographic research in which we have used the affiliations of
the corresponding author as the identifying reason for the authors
country of origin has indeed several limitations. For example, it may
be a team work, in which authors from different countries
contribute. Also several identified studies were from research
students attending high-income countries institutions and then
running research on their own countries. Many such students are
also funded by their own countries. On the other hand, there are
studies conducted by foreign missions based in a country, and
although the address of the foreign mission is from that country, the
study cannot be strictly considered as home grown. Despite such
limitations, for the purposes we followed in this study, the
bibliographic search can be useful and informative.
We conducted systematic searches of the main international
databases for identifying ATM papers published on or from low and
middle income countries in the EMR. Although we conducted the
search meticulously and tried to ensure that we did not miss relevant
papers, the search should not be considered exhaustive. There may
be further papers published from these countries and not indexed in
the databases we systematically searched. It is highly possible that if
e.g. Scopus or Embase databases had been published, or databases
more attentive to French language publications, there should have
been further papers identified from the region. Despite these

105
limitations, we believe our main and general findings from the
literature search remain valid, as it provides an explicit and
comparable platform to assess between country and regional
variations in ATM research and to identify the research gaps in the
region.

106
Access to medicine as a research priority: still a Cinderella topic?
It is safe to assume that certain aspects of aspect to medicine are still an
'orphan' research topic in the region. We use part of our case study in Iran to
demonstrate it further. Before doing so, it is important to highlight that our
findings demonstrated that the status of ATM studies in the EMR is not as bas
it had been presented in a previous study.83
Ritz et al 2010 provide a
bibliographic analysis of access to medicine literature and tries to provide a
picture of the number and distribution of publications from different regions
and countries. Our findings demonstrate that Ritz et al work has important
factual errors in its analysis and results. It underestimates the number of
papers produced from the EMR region by a wide margin, and certain countries
are altogether excluded from their findings.
Policy maker attention to ATM research
Another reason for limited attention to ATM research, may be due to the
perceived level of availability of medicines. For example in Iran it is generally
considered that medicines availability is high, and with a well spread health
systems in the country, they are also widely distributed to the remote areas of
the country. The exception to this may be highly specialized or expensive
cancer treatments which are offered via limited outlets in the country, and the
most of these outlets are located in Tehran or other metropolitan areas. Hence
the issues of ATM may not be considered as major research issues. There are
valid reasons for this: the success of the generic production of medicines in
Iran, relative low price of medicines in the country, and the wide spread
coverage of health care insurance in the country. See also

107
Figure 18.

108
Figure 18. Medicines affordability in Iran, in comparison with other countries
(source: WHO, the World Medicines Situation Report – 2011).
Researcher and research funder attention to ATM research
The regional review demonstrates that in the EMR region the comparative
level of attention to ATM issues by Iranian scholars is relatively higher. Our
search indicates that a large proportion of ATM research in the region has
been conducted by Iranians. This is interesting and encouraging. However if we
put in the context, then the ATM issues are not given a priority attention in
Iran. The fact is that the research output of Iran is the highest in the region in
general. The high proportion of papers from the country may just be the by-
product of the level of research activity, and not because a serious attention is

109
paid to the issue by researchers or research funding bodies. We will discuss
this further later on.
A demonstration of this is the way the formal research priority outputs are
presented. Assessing to relatively recent research priority setting exercises,
one for the pharmaceutical sector research (Pharmaceutical Sector Research
Network) (

110
Table 20), and the other for the School of Pharmacy of the Tehran University of
Medical Sciences are demonstration of lack of research institutions attention
to ATM.
The Pharmaceutical Sector Research Network conducted a consensus
development exercise in which they first agreed on the criteria for priority
setting (Table 19), and then voted on the different pharmaceutical main
categories. As it can be observed in Table 1, apart from the first issue (burden
of the disease) the remaining criteria are tuned towards innovation or market
aspects of pharmaceutical research. This is a clear attention to only limited
aspects of ATM.
Table 19. Ten agreed criteria for research priority setting (Pharmaceutical
Sector Research Network).
Ten agreed criteria for research priority setting (Pharmaceutical Sector Research Network)
Rank Criterion Score
1 Disease burden 7.86
2 Innovation 7.41
3 Network members capacity 7.05
4 Applicability of the output 6.64
5 Increase in monetary value of local market sale 6.59
6 Total monetary value of local market sale 6.59
7 Existing technological capacity 6.50
8 Existing internal resources 5.95

111
9 Expanding the status of pharmaceutical research 5.23
10 Increase in total volume of sale 5.09
The Pharmaceutical Sector Research Network final research priority list was
clearly targeted at innovative research that could result in production (re-
production) of innovative or expensive medicinal products, for use in the
country as well as future export and market expansion. This direction of
attention is in-line with the interests of the majority of high rank research
institutions in the country.

112
Table 20. Twenty high priority research topics for pharmaceutical sector, developed by the
Pharmaceutical Sector Research Network.
Twenty high priority research topics for pharmaceutical sector, developed by the Pharmaceutical
Sector Research Network*
Lipid modifying agents
Agents acting on the renin-angiotensin system
Antineoplastic agents
Beta blocking agents
Analgesics
Drugs used in diabetes
Antihistamines for systemic use
Anti-inflammatory and antirheumatic products
Antibacterials for systemic use
Antihypertensives
Drugs for functional gastrointestinal disorders
Antiepileptics
Cardiac therapy
Calcium channel blockers
Psychoanaleptics
Anti-parkinson drugs
Anti-acne preparations 17
Drugs for acid related disorders
Diuretics
Vaccines
* unpublished data. Provided to us courtesy of Prof Kebriaeezadeh.
The research priority list of the School of Pharmacy provided a similar picture.
Only two or 3 topics for a list of over 80 research priority areas are directly
relevant to ATM issues: i.e. 'Drug Utilization Review and Drug Utilization
Evaluation'; 'phamacovigilance for adverse reactions to medicines' and a third
broad areas titled as 'social pharmacy, pharmacoeconomics and rational use of
drugs'.
This is, however, about to change in major schools of pharmacy in Iran.
Departments of Phamacoeconomics and Pharmaceutical Managements are
being established. A couple of universities now offer (from three years ago)
PhDs in Phamacoeconomics and Pharmaceutical Managements, and a few
researchers have started establishing their careers around ATM research areas.
The reality is that the capacity for health policy and systems research in the
country is expanding and not just pharmacy related disciplines, but also health
economics, health policy, epidemiology and other disciplines are giving more
and more attention to these issues.

113

114
Results – qualitative interviews
Key informant interviews, Iran and the region
We invited thirty to interviews and conducted twenty interviews. Fourteen
respondents were male and six female. The distribution of their backgrounds is
presented in Table 3. The interviewees represented all the main stakeholders
relevant to ATM issues, including pharmaceutical and physician providers,
policy makers, industry, patient representatives, distribution chains, insurance
organizations, and sectors beyond health care.
As a result of analyzing the interviews, we identified 90 sub-themes or
important ATM policy and practice issues. Examples of concerns relevant to
each main category of the themes are provided in Table 21. The quotes have
been translated from Farsi to English. The quotes are not meant to be
representative, rather they provide a glimpse of rich discussions and issues
raised by the participants.
In practice it was very difficult to keep the focus of interviewees on research
priorities. They discussed policy concerns and barriers to ATM. In terms of the
main concerns, as we can now clearly see, the AT concerns are largely different
from the majority of issues covered by research projects so far. While RUD
remains a big policy concern, it is not the biggest issue to deal with. There are
many more concerns that needs to be tackled, for the perspective of the key
informants, to reduce barriers to access and appropriate use of medicines.

115
Table 21. Conceptual thematic framework from Iran and regional data – qualitative analyses and policy concerns
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
"We cannot ignore educational problems. Our education
system is not perfect."(KI3)
"I believe we do not have a serious and strong policy to
support research and development in drug production and
the margin of benefit for importing drug is higher, and this is
why we she drug imports are increasing."(KI4)
"The biggest problem is questioning the generic strategy in
the country."(KI4)
"Ministry of Health and health system decision makers should
consult the experts before making decisions … [such as]
Thalassemia Society, physician societies, Cancer Society,
scientific societies or senior and established physicians …
many decisions are without using expert opinions."(KI5)
"The main responsible organization has to be the Ministry of
Health and the Food and Drug Organization, and all other
1. Public-private health system mix
2. decentralization
3. Pharmaceutical policy
formulation/evaluation &
promotion
4. Pharmaceutical regulatory function
and enforcement
5. Human resources for the
pharmaceutical sector
6. Human resources for policy
planning
7. Health facilities (hospitals, clinics)
8. Family physicians/referral system
1. Health sector
organization

116
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
inter-sectoral organizations should act on that basis. I
personally think that inert-sectoral organizations should not
act like an ectopic [unit] in vital issues such as
medicines…"(KI8)
"Some people say we need to give monetary issues to the
Ministry of Commerce, and the Ministry of Health focuses on
quality control. Even before the revolution that we think the
structure was different, at that time for medicines pricing,
the ministries of commerce and health representatives were
present."(KI15)
"Access to medicines should be approached from a health
system perspective." (KI18)
"Each company that intends to import a medicine, they need
to get the Article 20 Commission's approval. … this takes
time, they need to have full documentation … then there are
monetary issues, nowadays opening an LC with a bank is
difficult."(KI2)
"National formulary is the first hurdle. If the medicine is not
listed, it cannot be imported."(KI2)
1. National drug policy
2. National drug formulary
3. Pricing
4. Labelling
5. Licensing/regulations on import
medicines
6. Generic versus brands
7. Quality assurance( GMP)
8. Quality control/ Drug quality
2. Health
sector
pharmaceutical
policies

117
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
" 'Single item importers' are an issue in Iran. They bring
medicines that are listed on Iran's national formulary.
Physicians decide they need a drug for their patients and
'single item importers' deliver." (KI2)
"At the moment we at the Ministry of Health set the
[medicines'] price, while insurance organizations are best
suited to do that. I mean it is the insurance organization that
can bargain with the producer, importer to reduce the prices
…"(KI3)
"Sometimes in meetings they [industry] mention it, in the end
the difference in cost of substance of 96% purity and 99%
purity, for the one with 99%, the price may triple, and that 2-
3 per cent impurity may cause the majority of adverse
reactions, most problems that people suffer from it."(KI17)
"… because of weakness in our insurance system, they keep
down the medicines' prices at the company, and [the
company] in turn will buy cheap ingredients. Medicines price
in Iran, part of it is from outside via 'single item' importing
which are very expensive, the ones that have to be of good
quality are very very cheap and lacks quality …"(KI11)
9. Post marketing surveillance
10. Adverse drug reactions
11. Audit –Drug utilization review
12. Medication errors
13. Essential drug list
14. Vertical programmes(malaria, HIV,
tuberculosis)
15. Conflict of interests providers and
pharmaceutical company
16. Regulations on drug promotion
and advertisement in the society
17. Drug share in health expenditures
18. Public and private health system
interactions

118
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
"We have the problem of medicines, as they are cheap, being
smuggled to the neighboring countries… "(KI12)
"Our first statement is this: if the quality of a medicine is bad,
and the price is low, that's no use to us because we need to
pay the price later."(KI16)
" … the issues is that do countries have essential package of
services at the primary care level … is there a clear essential
medicines list … if that essential package is there … how are
those being financed … in Pakistan .. there is a clear lack of
access to medicines …[due to] insurance issues, lack of
government funding …"(KI18)
"… in Afghanistan the medicines are available, but the
medicines that are of good quality , that are effective … that
is the problem. ."(KI19)
KI1. "Financial [limitations] has resulted in insurance
organizations, including both basic and complementary
insurance, do not make contracts with all existing
pharmacies. This has important access implications."(KI1)
"Pharmacies have contracts with insurance organizations and
1- Health system financing, national
health budgets, social health
protection
2- Universal coverage
3- Social welfare and social protection
policies
3. Health
system
financing /
insurance
system

119
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
should be reimbursed by them. Sometimes the insurance
companies do not pay pharmacies for 6-9 months. A
pharmacy has 20 million Tomans [~20 thousand US$] with
the insurance organization and may not dispense a patient's
prescription …"(KI2)
"Our insurance system is unhealthy …"(KI3)
"Should we include expensive and unaffordable-for-all
medicines in the national formulary or no? If we say it should
be included, then many people cannot afford it, and naturally
some people will be deprived of it. If we say it they should
not be included, then some people say that we could afford
it, why shouldn't we get it?"(KI4)
"60% of our patients [thalassemia] are covered by the
Medical Services Insurance Organization, they have lots of
problem. Their coverage is less than Social Security Insurance
Organization."(KI5)
"Most of our patients [thalassemia] are from low
socioeconomic groups. They problems in paying for their
medical costs."(KI5)
4- List of medicines under coverage
5- Cost coverage – financial protection
6- High expenditure disease groups
cost coverage
7- Cost coverage for other target
groups
8- National subsidy and benefit
distribution

120
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
"Certain private insurances, or insurances provided by the
banks offer full coverage for the insured … even plastic
surgery … others don’t. Even the coinsurance level differs,
some at 10%, others 20% or 30%. Hence we do not see the
equity we expect to see between insurance packages. While
most probably the premium they [users] pay is not that
different."(KI6)
"At least we need to have a database of all diabetic patients.
… If the insurance organization and the Ministry of Health
who is responsible for it have the data, a lot or repetitions
will disappear and many costs will reduce and can be used to
cover other expenditures …" (KI7)
"All medicines are now [covered by insurance] … some are
covered 90% of cost, other insurance [organizations] may pay
all of it, or are covered via separate subsidies. 300 million US$
is just the subsidy paid for special diseases of hemophilia,
thalassemia, MS."(KI9)
"We need to look at the large picture, and see if there is a
disease that each year 50 people suffer from it and die, is it
ok to spend 10, 20 million dollars on it, or should we keep
that to vaccinate 1-2 million children. Which one is our
121
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
priority?"(KI17)
"As for insurance coverage, I think we need to compare
ourselves with other countries. Our insurance coverage is not
bad."(KI14)
"evidence from both low income countries and middle
income countries in the region, particularly middle income
countries suggest people pay substantial costs for medicines
out of their own pockets for life saving drugs … these are the
gaps that exist between policy and practice"(KI18)
"… in Afghanistan the policy is to keep primary health care
drugs free of charge … in secondary care NGOs charge people
… the Ministry of Public Health policy is that secondary care
treatment in public hospitals is free of charge but the
majority of doctors do not admit patients until they get paid
by the patient."(KI19)
" We need to pay attention to health insurance and coverage
as it could lead to over prescribing and polypharmacy. This is
a very clear case in Palestine. More research is needed in the
area of insurance coverage in relation to rational use."(KI20)

122
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
"Right now not all medicines can be distributed everywhere.
Some medicines are just for certain pharmacies. E.g. some
people may have to travel to Tehran for certain medicines, as
they are not available in provincial cities."(KI2)
"Drug distribution in slow. Pharmacies have to stock a lot of
medicines. … and in the end they stock high usage medicines,
and not necessarily essential medicines."(KI3)
"Subsidized medicines are the same story, because we have
not used proper technology … patient has to go to a certain
pharmacy once or twice a month, because we say that
medicine is in short supply, is expensive, is subsidized [by the
government] …using IT and modern distribution systems we
could have get it to the patient where she lives …"(KI3)
"The laws are [part of the problem]. E.g. for opioids … and
end stage cancer patient has to travel to the center [to get it]
…"(KI3)
"In distribution system, sometimes no medicine reaches an
area. Recently following a lot of lobbying I though medicine
problems are resolved. But yesterday I saw a letter that
claimed in their city there no Desferal and no Desfonac."(KI5)
1- Private –sector drug distribution
systems
2- Governmental /public distribution
systems
3- Drug availability in the
market(pharmacies)
4- Informal distribution network
5- Geographical distribution
(pharmacy, health facility, hospital
drugs,…)
6- Drug distribution in the hospital
7- Prescriptions' drug distribution
without prescription
8- Drug distribution in the health
facility
9- Drug's import
10- Counterfeits
11- Corruption
12- Drug's export
13- Trained human resources delivery
14- Technical capacity of distribution
staff/well trained manager
15- Monitoring and evaluation
16- Marketing
4. Drug
Distribution
system

123
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
"[From the pharmacy point of view] we have problem at the
distribution system. The pharmacy cannot be sure whether a
medicine gets more expensive or cheaper. It does not how
much they can stock and for how long the drug is easily
available. … sometimes you have to stock medicine instead of
the distributors."(KI6)
"There was a time that we had a critical situation, if you
remember we were suffering, and our people were suffering
because of medicines scarcity, I mean there always was a
long list of medicines in short supply."(KI9)
"We have good competition in distribution [system]. In fact
there is no monopoly. There are almost tens of distribution
companies, provincial companies, national companies who
distribute medicines [registered] with the Ministry of
Health…".(KI9)
"Another problem of distribution companies is that we have
lots of distribution companies and some of the do not have
the minimum standards for keeping medicines."(KI10)
"we, in the pharmaceutical sector, gave permission of
17- Competition
18- Distribution generic drugs

124
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
accessing medicines via emergency center [single item
importers] , it affected quality, and the medicines were
bought from distributer before the quality was assessed in a
laboratory."(KI13)
"… [in Afghanistan] some medicines samples are assessed
and then it becomes possible they have not be assessed by
specialized laboratories … around the country in different
areas there are low quality medicines, expired medicines
around"(KI19)
"… unfortunately in Afghanistan, access to medicines, but low
quality medicines, is very easy. People when they go to
pharmacies even outside the pharmacies … in groceries …
they can get it [without prescriptions]. ."(KI19)
"In our country inappropriate use of medicines, is more deep-
rooted than many other countries. If you ask doctors why
they prescribe such medicines, they respond that because of
patients' request."(KI3)
"Whoever prescribes the medicines, also sets public
preferences [that is] … the medical society influences
[people], people alone are not that influential."(KI4)
1- Demand for medicines and health
care services
2- Public knowledge and awareness
3- Self medication
4- Affordability ,Out-of-pocket ,price
of medicines
5- Drug promotion in the community
6- Specific groups( geriatrics,
5. Individual,
household
and
community
level

125
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
"For certain internally produced drugs, the users do not have
enough trust in local products, sometimes because they
cannot see the quality."(KI6)
"Sometimes [people] believe foreign products are better than
domestic products."(KI6)
"Physician has to send him [patients] to other physicians to
give him consultation. The patient might say I would not get
insulin, and the physician will back down and we will be away
from our aim of treating the patient."(KI7)
"Access can be viewed from different angles. In terms of
availability, we have no access problem … but whether
people can afford it is another matter."(KI10)
"There are other diseases not considered by the Ministry of
Health as 'special disease',10
while the disease are really
special and their medicines are expensive."(KI14)
"I think [household] out-of-pocket [expenditure] is important,
pediatrics,)
7- Chronic disease
8- Socio-cultural constrains
9- Stigmas and cultural barriers to seek
treatment
10
'Special disease' is a certain category in Iran health system, based on a parliamentary law, that includes thalassemia, hemophilia, and kidney replacement therapies. These diseases receive a substantial amount of subsidies to cover the costs of the required expensive treatments.

126
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
but the cultural issues are more important. If the demand
reduces and becomes more rational, access will
improve."(KI14)
"… our problem is that [in Afghanistan] people who have low
education level, when they get the medicine do not know
how to use it, and those that give them the medicines, do not
teach them how to use it."(KI19)
"We do not have standards for the required number of
[pharmacist] providers, have copied other countries, or have
lowered standards based on the number of pharmacists. We
need to define evidence base geographical access standards
…."(KI1)
"If a pharmacist just thinks of money, she would not care
what the patients get, will give them whatever they want,
even without prescription, if they pay."(KI2)
"Pharmaceutical companies should not be allowed to serve
doctors … to keep medical society away from the low of
financial links with pharmaceutical producers and
importers."(KI4)
1- Induced Demand for medicines and
health care services
2- Rational drug use/ Evidence based
medicine
3- Payment methods
4- Pharmacy
5- Role of medicines' Income in
hospital/clinics' income
6- Drug safety and medication errors
7- Fee splitting
8- OTC drugs
9- Traditional and herbal drugs
10- Consultant pharmacist, clinical
pharmacy
11- Chronic disease
6. Health care
providers

127
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
"The set so many laws for OTCs but the pharmacies dispense
whatever they want to people."(KI11)
"A very important role that pharmacies can play is to correct
costumer drug utilization culture. Many people when they
visit a pharmacy may be looking for more expensive and
trendier medicines. … the pharmacists … can guide people
…"(KI12).
"For example, does the Ministry of Commerce has enough
expertise for market control? … or does is look at it
[pharmacy] like a general shop or outlet? This is a specialized
issues and should be outside the Ministry of Commerce."(KI1)
"Each company that intends to import a medicine … there are
monetary issues, nowadays opening an LC with a bank is
difficult."(KI2)
"Scientific societies are influential in adding a medicine to the
national list, and with the relations they have with companies
and can heavily promote a drug. For example if a company
collaborates with the neurology society and introduce its
drug, and the medicine becomes the best seller in Iran, you
know how much it will sell. The can increase or decrease drug
1- Ministry of finance
2- Standard organization
3- The medical council – medical
societies
4- Pharmacists association
5- Ministry of commerce
6- Ministry of industries
7- charities
8- WHO guidelines
9- WTO agreements
10- Gavi
11- World Bank - UNICEF
12- Global Fund – other UN agencies
13- International NGOs
14- SWAp
7. Policies
beyond the
health
sector

128
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
sale, bankrupt a company …"(KI2)
"If a drug needs to be imported in an emergency, its import
should register with us, and another time with [Ministry of]
Commerce, and once with the Customs."(KI3)
"If the Ministry of Commerce comes and opens an office in
Foods and Drugs [Organization] and do the works from there
… is better than we send people in the [Ministry of]
Commerce's loop … when we move around people between
different ministries, different organizations … this puts an
expense on the person or company … the company will not
pay out of pocket … public have to pay more in the end from
their pocket as insurance budget is limited."(KI17)
"… we have problems in making regulations within the sector,
not much problem with the Ministry of Commerce but within
the Ministry of Health …"(KI10)
"… I want to see to what level exists a governmental
commitment to access to essential medicines … most
countries in the region that have committed themselves to
strategic plans [they do better]… "(KI18)
15- Philanthropic organizations – Bill &
Melinda Gates
16- Roll Back Malaria
17- PEPFAR / USAID
18- EU / JICA / DfID / …

129
Examples of verbatim quotes and policy concerns Sub-themes Main theme
and issue
"… there are signs that some importers of medicines [to
Afghanistan] change of the label of the expired drugs they
import from Pakistan, India or China."(KI19)
"Cross-border smuggling of medicines is a major issue in
Afghanistan."(KI19)
"In Palestine, the stewardship and governance are well
organized with coordination between the Ministry of Health
and the union of Pharmacists. However, other challenges
related to Israeli Occupation manifested in controlling the
boarders, affecting supply chain, delays, controlling which
types to import and all quality control tests. The same could
be extrapolated to other countries in the region with war like
conditions."(KI20)

Key informant interviews, Pakistan
Access and Magnitude of the issue: All stakeholders were unanimously of the
opinion that access to medicines was a major issue in Pakistan. There was divided
opinion on extent of work done in this area with close to half of the opinion that
some work had been done on this area but major work needed to be done while
others opinion that substantially little work had been done so far.
Only 3 respondents identified access as involving elements of quality, affordable
prices and availability at nearest access while others mainly tended to identify
with one aspect either physical availability, quality or affordability.
Main Barrier to Access: Weak regulation, supply side issues and irrational
prescription of drugs were identified as the main barriers to access. Although
open end in-depth interviews precludes computing of quantitative frequency,
broadly most stakeholders identified weak regulation is the main barrier, followed
closely by irrational prescription while a variety of supply side issues was the third
common response. Weak regulation covered a range of issues including low
quality threshold for registration, weak enforcement of existing regulations, flat
price control leading to drug disappearances from the market, and corruption
nexus at the level of licensing, registration and quality control. Supply side issues
cited included inappropriate procurement of drugs, lack of pharmacists rile in
supply management, and poor management of drug availability at public sector
facilities. Irrational use responses involved inappropriate prescription by
providers, undue influence of medical specialists in procurement and nexus
between providers and industry.
Rational Use: “Essential generics don’t have star status like new brand drugs..”
(Intw: 21)

131
There was unanimous opinion that prescribing practices need improvement from
specialists down to dispenser level. With more than 70% of health care provide by
private providers there was felt to be a huge role o f the private retail market and
dominance of well promoted products. Essential drugs have been around for a
long time and don’t have the same prestige as new brand products. A number of
factors were cited for market dominance over drug usage. A foremost one was
the open access of doctors to industry representatives and entrenched practices
of receiving incentives at all levels of the medial profession. Others included lack
of institutionalization of pharmacists role in selection of drugs at health care
facilities with much left in the hand of doctors or civil servants. Yet another factor
cited was weak pre-service training and almost a complete lack of in-service
training on standard therapy. Formularies are absence at all levels of the health
system and there is as a result little concept of referral to formularies for
appropriate drug use.
Wide Variation in Registered Products: “There is an open access policy in Pakistan
for drug registration..” (Intw: 4)
All stakeholders expressed grave concerns over registration of too many products
and wide variation in quality of registered drugs, however there were slightly
differing perceptions over underlying reasons. Acknowledgement of wide quality
variation in products was also acknowledged by industry which felt that presently
the onus was on individual companies who felt that the low threshold was a
disincentive advantage to those manufacturers who invested in quality.
Some stakeholders cited weak technical management and planning by Ministry of
Health and others were wont to blame this on a nexus between industry and
technical registration staff. Respondents reported that there were close to 88000
products, exact number was not available even with MOH and there is lack of
national formulary. Registration does not look into cost effectiveness,
comparative cost analysis over other products, local bio-equivalency is not
required and scrutiny of submitted bio-equivalence is variable. Registration
system is still manual making it difficult to manage the data and there are few
132
attempts at de-registration. Staff managing registration has not received targeted
training for registration nor been exposed to drug registration best practices in
other countries. Stakeholders also expressed concerns at opportunity for
corruptions in the registration process due to the loosely managed system of
registration. Lack of an independent drug regulatory board was felt to enhance
undue political influence over registration with swings of high and low corruption
taking place according to the leadership in place.
Flat Price Control & Issue of Orphan Drugs: The issue of critical shortages of
essential drugs was felt to be of high concern across all stakeholders. Basic drugs
such as phenytoin, phenobarbitone, thyroxine, thiazide, folic acid have been
missing from the market. On the part of the industry the major underlying factor
was flat price control in place over drugs leading to disincentive to produce low
cost drugs. Political sensitivities of the MOH and fear of public outcry leads to
reluctance to deregulate prices. Forced production by Ministry leads to sub-
standard methods Experts also pointed to cross border traffic of drugs to regional
counties offering better prices. A suggestion was put forward to move to regional
basket of drugs to avoid drug shortages. There was much interest in exploring
different formulas for pricing to encourage rational use and increase access.
There was also demand that pricing deliberation should be made more
participatory with greater inclusion of provincial implementors.
Procurement: Quality of drugs at public sector facilities was generally felt to be
suspect was due to weak discrimination during procurement. The practice of
going for the cheapest tender was felt to allow companies with low quality drugs
to be eligible for tenders. At least one province has shown interest in tightening
the threshold for tenders. From the industry many of the better quality producers
stayed away from public sector tenders due to uncertainty over payments and
preference of favorites and rent seeking in public sector. Moreover although

133
public sector had a generic procurement policy with provincially pre-approved
tenders at an annual rate contract, in practice district health managers were
reported to often purchase drugs not on the national EDL and inclusion of other
suppliers. Forecasting was another area for improvement with current practice
relying on incremental increase in inventory rather than scientifically being
forecasting on scientific forecasting based on morbidity data and patient volume
statistics, while in case of hospitals procurement was also excessively dominated
by specialists. Some stakeholder pointed to marginal involvement of pharmacists
in procurement- some of the larger teaching hospitals having only 1 pharmacist
for 1000 beds - while others felt that drug selection was an area that could be
taken care off by medical doctors. Another area of concern was frequent shortage
of drugs, with stakeholders divided over whether this was an issue of inadequate
funds or lack of aggressive management of stock. In contrast NGOs were felt to be
more scientific in procurement based on morbidity reports, a stronger check on
drug quality with discrimination on quality parameters and avoidance of stock-
outs through bumper stocks.
Supply chain & Stock-outs: “We have always focused on macro-economic policies
but attention to service delivery level; has been lacking …there lies the
gap”(Interview 5)
Respondents felt that drug supply chain was an area that would not get
highlighted due to attention spotlight usually on registration and pricing, however
needs practical attention and may be more amendable to quick wins rather than
larger contentious issues. Vertical program often due to centralized procurement
were wont to end up with stock outs while the mainstream government health
facilities faced stock outs due to lack of scientific forecasting, more a problem of
management of funds rather than non-availability of funds. Logistics management
systems were no in place and where developed were being applied only to donor
funded programs with little roll out to the mainstream public health care sector.
Drug storage and dispensing were also felt to have received little technical input.
Professional staff has not been inducted for handling drug distribution and

134
storage nor is there a practice of staff training and capacity building. Junior staff
does dispensing with only secondary school qualification raising grave issues of
quality.
Post Devolution Prospects: While respondents saw partial devolution as an
opportunity for increased implementer feedback on drug regulation there was
concern by nearly all stakeholders on total devolution of drug regulation to
provinces. The latter was viewed as creating inequities in terms of physical
availability, quality and pricing within country population. Respondents expressed
concern that if medicine is registered in one province but not another then
patients in one province can be deprived of the drug. This can create legal
implications by compromising right of patient access to drugs and furthermore
not all provinces have even capacity to register and test drugs putting in question
their regulatory role. Similarly the same drug will be registered cross-province
movement of drugs with low availability in provinces with higher prices.
Respondents cited example of OECD countries where drug regulation is a
centralized function but autonomous function and current situation in Pakistan
can be improved by an autonomous regulatory body with adequate stakeholder
representation.
Key Researchable Areas: Stakeholders identified the following key areas for
research feeding into practice:
- how to increase compliance with standard therapy amongst providers and
patients;
- how can awareness of patients and end users be increased for rational drug
use;
- what are the underlying factors behind poor availability of medicines at
public sector facilities;
- what measures are needed to improve quality control of drugs;
- what measures are needed to address issue of orphan drugs.
135
Key informant interviews, Lebanon
Policy concerns
The transcriptions of interviews with key informants provide for a rich material
for understanding the various concerns regarding ATM. As expected, concerns
reflect the positions and interests of stakeholders; different stakeholders have
varying and sometimes opposing concerns. It is an important exercise, indeed a
research question, to map out the ATM concerns in relation to stakeholder
positions and interests. However, as this is beyond the scope of this report, we
focus in this section on highlighting a few general points which are of particular
relevance to a future agenda of ATM research in Lebanon and then move to
provide a thematic analysis using the WHO 2004 ATM framework.
General points
The concept of ATM. All informants identified the situation of medicines are a
challenge of profound public health dimensions. However, very few informants
expressed and voiced this challenge in terms of “access”. Access therefore was
not prioritized as a concept in the interviews. While many informants highlighted
important and specific challenges that limit ATM such as high prices of medicines
in the private sector or interrupted supplies in the public sector, very few
informants explicitly expressed such concerns in terms to equity, which lies at the
heart of the concept of access. Equity did not come up as a central theme in the
discussions of ATM.
The approach to ATM. Most informants identified concerns with ATM that impact
people and patients. However, only a few informants stressed the need to make

136
the perspectives of people and patients the central aspect of approaching the
subject of ATM. One informant brought up the concern that the WHO 2004
framework for ATM focuses on the policy level and is directed to policymakers
and suggested alternatively the use of the framework of Frost and Reich (2009)
which approaches ATM from the perspective of users by focusing on attributes
that concern them directly: availability, affordability and acceptability. This
informants wondered how the ATM research agenda would be different if ATM is
approached from the perspective of health as a basic human right to all.
The importance of the political and economic context to understanding and
improving ATM. Irrespective of the sometimes-opposing positions of different
informants, the majority of informants emphasized that ATM must be understood
in relation to the political set-up and the economic free market and the
prominent role of special interests and confessional parties. Medicines in Lebanon
are treated as consumption goods rather than as public goods and are submitted
to free market laws and profit making. Several informants were quick to highlight
that they don’t see improvements in the ATM situation, or the point of carrying
out research on ATM, unless the political governance are first addressed as the
broader governance framework directly impacts and determines governance of
medicines.
The party(ies) which are most responsible for ensuring ATM. Informants
pinpointed to the fragmentation in the governance, financing, and supply of
medicines. Almost all informants stress the need for a stronger role for the state
and especially the MOPH. The MOPH already plays a key role, seen for example in
policy development and regulation or in supply such as through the YMCA-
administered program to ensure availability of medicines for chronic conditions in
PHC centers and in dispensaries or through the free provision of expensive
medicines for conditions such as HIV/AIDS, multiple sclerosis and cancer.

137
However, the role of the MOPH is undermined by powerful interests. How to
strengthen the role of the MOPH in improving ATM within the current political
set-up remains an open question.
The important role of non-state parties in improving the ATM situation.
Informants have acknowledged that the CSOs and NGOs have played an
important role in ensuring access, for example through the dispensaries and
through health NGOs, and this role must continue even as they stress the priority
of strengthening the role of the MOPH in ATM. However, informants also see the
need for more supervision and better coordination of the contributions of CSOs
and NGOs in order to make their contributions more effective.
The role of practitioners and their professional associations. Informants have
acknowledged the important role of practitioners and professional associations.
These can do much more to improve access but must be protected and given the
mandate to play such a role.
Thematic analysis
Here we summarize some of the recurrent concerns expressed by key informants
using the WHO’s 2004 ATM framework.
Financing: Of the four areas, concerns were expressed the least often in this area.
Spending on medicines, as a proportion of total health expenditures, is much
higher than in many other high middle-income countries and is unacceptably
high. Out-of-pocket expenditures for medicines are the primary source of
financing posing a challenge to access. There is significant fragmentation of

138
financing as seen for example in the absence of a common medicines financing
framework for all six social insurance organizations.
Affordable prices: The prices of medicines, and consequently affordability,
indicate that there are major challenges. Prices are much higher than would be
expected, and are much higher than prevailing prices in other countries in the
region. The free market logic cannot alone explain this situation. Presumed open
competition has not led to reducing prices of medicines. The regulations
stipulating that new imported medicines must be cheaper than medicines of the
same compound that exist in the market, has not led to need reductions in the
prices of medicines.
Rational selection and use: This is a key ATM challenge. There are almost 7200
medicine formulations on the market of which almost 5900 are registered by the
MOPH. This well exceeds the needs of the country, leads to wastage and over-
spending on advertisements and creates the opportunities for corruption. An
essential medicines list has not been updated in many years. However, even if
such a list were to be updated and provided, its impact is not clear in the absence
of strong governance, regulatory capacity, and implementing and sanctioning
bodies. For example, even the NSSF does not have an essential medicines list.
Medicines are neither rationally prescribed nor rationally dispensed. Physicians’
prescribing practices are unduly influenced by pharmaceutical promotions and
self-interest. There is no prescribing accountability. Many physicians draw their
knowledge from pharmaceutical companies’ prospectors, and they depend on
them to acquire continuous learning as alternative systems, either supported by
public funds or by professional associations are very weak. Clinical practice
139
guidelines are very few. The over-supply of physicians and pharmacists tends to
increase irrational prescribing and dispensing of medicines.
Rational use of medicines by the public is also a major problem. There is common
misconception about generics and the superiority of medicines from expensive
sources such as manufacturers in Europe. Some informants felt that cultural
particularities in Lebanon encourage use of branded medicines; other informants
disagrees stating that irrational use is more related to the lack of a strong
governance and the nature of the political and health system. Many people
purchase medicines without prescriptions or consume medicines prescribed by
the multiple providers, especially specialists, they might seek for consultation.
Health and supply systems: Supply systems are reasonably well developed in
Lebanon especially that much of such services are in the private sector and are
for-profit. Informants did not think of important concerns about inadequate
storage, or inadequate transportation of medicines. However, they expressed
serious concerns about the quality of medicines on the market and the presence
of counterfeit drugs. The closure of the central laboratory is a major impediment
to improve quality of medicines. Some medicines that have been withdrawn from
the market in North America or Europe may remain on the market in Lebanon for
a while. There are regular interruptions in the supply of medicines supported by
the MOPH, especially expensive medicines for conditions such as HIV/AIDS,
multiple sclerosis and cancer. The problem is less pronounced in the supply of
medicines for chronic conditions through the program administered by YMCA.
Geographical access of the population to health care and medicines is not usually
seen as a major problem. However, much of the dispensing of medicines in
dispensaries and PHC centers is not necessarily well linked to provision of care
and users may get their medicines in these outlets but have their actual care
elsewhere, especially by private providers.
140
Research questions emanating from key informant interviews
Appendix 6-B presents the list of research questions that emerged from the KII.

141
Results – qualitative interviews, EMRO region

142
Priority research areas for ATM – findings and consensus
Consensus development on research priorities - Iran
A total of 125 potential research topics were presented to the consensus
development meeting. The participants further added 15 new potential topics
during the discussions that took place in the meeting.
As explained in the methods, the topics were categorized under the six main
themes. In the end twenty priority topics were selected by the participants. Three
topics appeared twice in the results (i.e. under two different main themes). Hence
seventeen unique research topics were identified in this process (Table 22).
Under one theme (beyond the health sector), no agreement on a topic as a
research priority issue was observed. This is despite the fact that this area was
considered a major policy concern in qualitative interviews. This may reflect the
nature of the health system in Iran, in which the majority of decisions are taken
within the sector, and hence the impact of issues from outside is not seen as
important. It may also be the result of a lack of useful input from the interviews
and literature and hence resulting in a situation in which the proposed topics did
not deemed priorities.
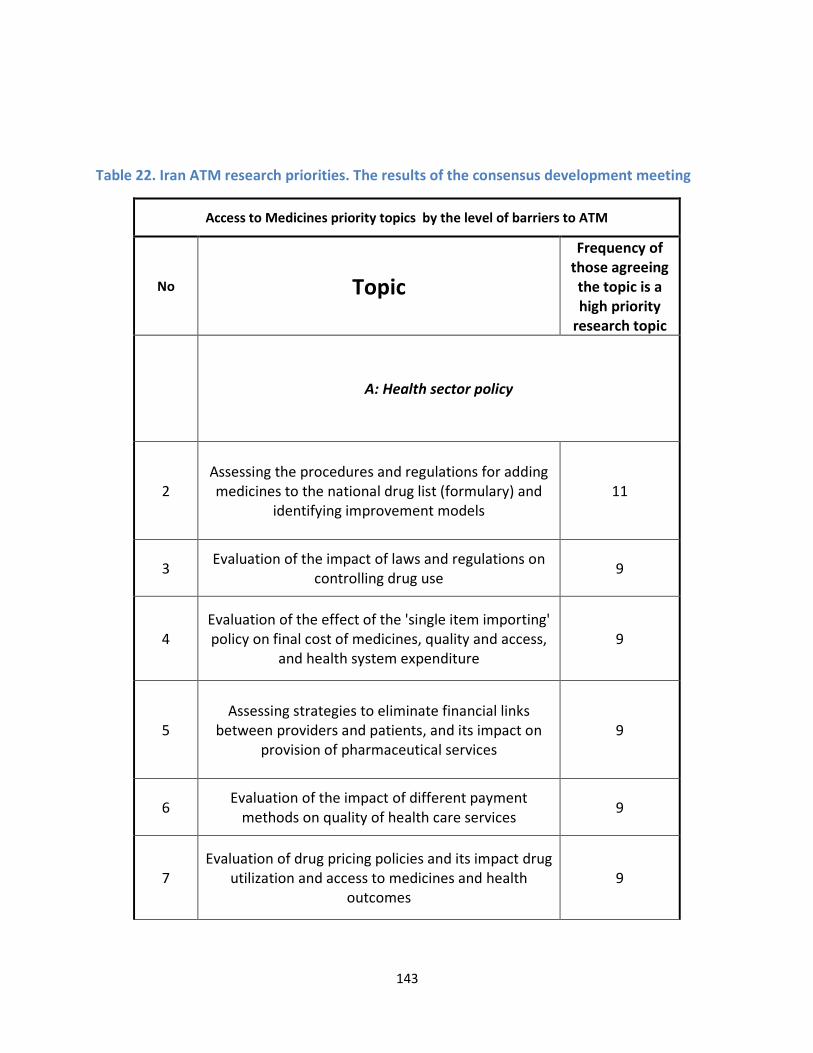
143
Table 22. Iran ATM research priorities. The results of the consensus development meeting
Access to Medicines priority topics by the level of barriers to ATM
No Topic
Frequency of
those agreeing
the topic is a
high priority
research topic
A: Health sector policy
2
Assessing the procedures and regulations for adding
medicines to the national drug list (formulary) and
identifying improvement models
11
3 Evaluation of the impact of laws and regulations on
controlling drug use 9
4
Evaluation of the effect of the 'single item importing'
policy on final cost of medicines, quality and access,
and health system expenditure 9
5
Assessing strategies to eliminate financial links
between providers and patients, and its impact on
provision of pharmaceutical services
9
6 Evaluation of the impact of different payment
methods on quality of health care services 9
7
Evaluation of drug pricing policies and its impact drug
utilization and access to medicines and health
outcomes
9

144
Access to Medicines priority topics by the level of barriers to ATM
No Topic
Frequency of
those agreeing
the topic is a
high priority
research topic
8
Evaluation of pharmaceutical policies,regulatory
function and enforcement for traditional and herbal
medicines
8
9
Evaluation of pharmaceutical policies and procedures,
and the applications of post marketing surveillance
reports
8
B: Health system financing/insurance system
34
Evaluation of the process of adding medicines to the
insurance organizations' list of medicines covered
11
35 Evaluation of the impact of different payment
methods on quality of health care services 9
36
Evaluation of drug pricing policies and its impact drug
utilization and access to medicines and health
outcomes
9
37
Evaluation of the effect of free medicine provision in
SSIO11 (and charity) owned facilities on drug usage
patterns and access to medicines
9
38
Evaluation the relationship between pharmaceutical
pricing policies and costs and benefits of
pharmaceutical companies
8
11
Social Security Insurance Organization, a major social insurance organization in Iran

145
Access to Medicines priority topics by the level of barriers to ATM
No Topic
Frequency of
those agreeing
the topic is a
high priority
research topic
39
Assessing strategies to eliminate financial links
between providers and patients, and its impact on
provision of pharmaceutical services
8
C: Drug production and distribution system in the country
44
Evaluation of the extent and effects of drug
promotions activities of the industry and its impact
on prescribing behavior of providers
9
45
Evaluation of the effect of the 'single item importing'
policy on final cost of medicines, quality and access,
and health system expenditure 9
46
Evaluation of the impact of regulatory function providing
financial incentives for pharmacists' that provide
appropriate pharmacy services on increasing quality and
improving rational drug use indicators
8
47 Evaluation the role of pharmaceutical companies on
prescribing and drug use patterns 8
D: Beyond the health sector
No agreement was made for this domain
E: Individual, household and community level
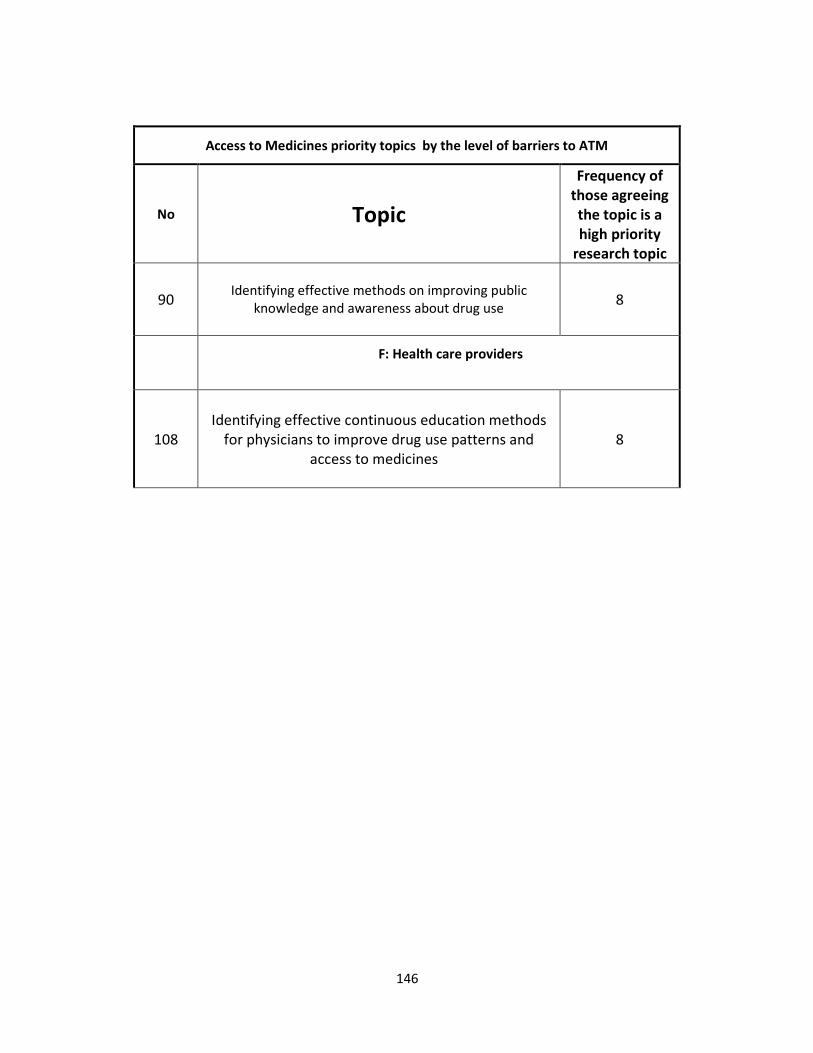
146
Access to Medicines priority topics by the level of barriers to ATM
No Topic
Frequency of
those agreeing
the topic is a
high priority
research topic
90
Identifying effective methods on improving public
knowledge and awareness about drug use
8
F: Health care providers
108
Identifying effective continuous education methods
for physicians to improve drug use patterns and
access to medicines
8

147
Consensus development on research priorities - Pakistan
Policy Concerns: The following were the policy concerns prioritized through the
Roundtable discussion.
Rational Use
� Unnecessary, and often inappropriate prescriptions, by medical
practitioners
� Large and unregulated private sector with reportedly high utilization levels
of informal providers and quacks
� Underutilized role of pharmacists in health service delivery
� Little presence of therapeutic protocols & formularies
� No restriction of type of prescriptions by level of health care
� Open access of industry to health care providers
Financing & Affordability
� Burden of medicine payment mainly on households
� Chronic care therapy unaffordable with both generics and originator bands
� Inadequate operational budget for medicine in public sector
� Existing budget in public sector need to be more efficiently managed
� Contracting out of BHUs has resulted in better availability of drugs
� Need to explore new financing mechanisms for health service delivery that
can improve access to drugs
Supply Side Issues
� Low availability of medicines in public sector at all tiers of health
system
� Low quality threshold for procurement in public sector
� Information on pricing fixed by MOH is not readily available for
procurement
� Lack of bumper stocks & advance forecasting based on morbidity
pattern
� Outdated logistics management systems
� Drug storage and dispensing poor across public and private sector
� Lack of sufficient number of pharmacists across public and private
sector

148
� Too many drug stores o proper regulation
� Black-marketing practices in private retail market due to collusion
Registration
� Too many registered products
� Low quality threshold for registration
� No WHO or FDA certified production unit in the country
� Need for regular review of EDL
� Little utilization of Central Research Funds despite need for evidence
Pricing
� Clear cut pricing formula needed
� Flat price control is counter productive
� Low priced essential drugs, even life saving ones, are chronically short in
the market
� Wide gap between prices of generics and originator brands
� Uneven regional pricing contributes to cross border supply resulting in
stock-outs
Quality Assurance
• Lack of incentives to produce quality drugs
� Continuous capacity building of for quality surveillance
� Government dominance and punitive measures not enough for quality
improvement
Decentralization
• Need for independent drug regulation authority with greater
representation of provinces
• Total devolution of drug regulation can potentially have negative
consequences on drug availability and cost across provinces
Research Concerns: The following were the research priorities identified
collectively through the Roundtable discussion
• Impact of decentralization on
– Prices

149
– Availability
– Overall access
• Regulations exist in Pakistan but need to be implemented : research into
implementation gap for existing medicines policies (determinants, reasons)
• Investigating the success and failures (and reasons) of the essential
medicines programme in the past 20+ years in Pakistan
• Human resources:
– The role of pharmacists at decision making level on medicines
policies
– Credibility of health professionals and the issue of trust
• Pricing policies
– Deregulation or price regulation? Which regulation mechanism
– How to improve access to orphan medicines
– Monitor price in the actual market to inform pricing regulations
- Lack of medicine unit cost estimation
• Role of private sector
– Informal / shadow pharmacies: prominent role that need to be
investigated
– Regulated private sectors
– Traditional healers
• Documentation of quality – post-marketing surveillance system
• Transparency of information, availability in public domain:
– Research into a health /medicines information system
• Registered medicines (and unregistered)
• Human resources
• Prices
– Routine monitoring of relevant indicators on medicines access
– Integrated HMIS
• Medicines policies part of an overall health policy – Research needs to feed
national health policy
• Harmonization and Alignment –
• Access to research – feedback on research made – Need for a wider
research network, continuous culture of research
• Consumer perspective

150
– Health seeking preferences
– Other
In Pakistan there has been considerable work in terms of Policy Acts, legislations,
and detailed regulatory and operative guidelines for the pharmaceutical sector.
From 1960s onwards to date Pakistan has introduced at least 16 documented
regulations for enhancement of access to medicines, including an abortive
attempt to bring into place the Generic Drug Policy Act, however gaps exist
between policy and practice. This is due to weak implementation, absence of
monitoring framework, as well as a traditional tilt of policies towards punitive
action by government rather than co-option of other stakeholders towards more
participatory regulation.
There is dire need for update of policies in line with on ground evidence and
infusion of new strategies involving an innovative mix of measures.
PRIORITY POLICY CONCERNS FOR INCREASING ACCESS TO MEDICINES:
Using the WHO’s Access to Essential Medicines Framework (Laing 2002) we came
up with the following policy concerns.
Rational Use: Medical practitioners, including both GPs and specialists, often
prescribe unnecessary number of medications with average for Pakistan being
>3 medicines per prescription as compared to 2-3 in LMICs and injection usage
rate one of the highest in the world. Pakistan was one of the first countries in
which the Essential Medicine Program of WHO was started back in the 1970s and
a National EDL comprising of 335 medicines is in place, however rational drug use
continues to be a major issue. There is unnecessary prescription of antibiotics,
vitamins and painkillers, preference for higher line therapy over standard therapy,
sub-optimal knowledge of standard therapy for endemic diseases even amongst
licensed practitioners. Apart from medical practitioners, population in Pakistan
frequently utilizes quacks and informal providers who are not only unqualified to
prescribe but alarmingly also dispense their own medication mixtures. Rate of
injection usage in Pakistan is one the highest in the world at 13 injections/person/
capita and is driven by quacks as well as qualified medical practitioners. With
largely unrestricted access to drugs in pharmacies and medical stores, there is
also considerable self medication and although its prevalence has not been
comprehensively assess, indicative figures are of 30-55%. Drug resistance to first

151
line antibiotics has been established at least in urban Pakistan while there is also
high prevalence of Hepatitis B and C diseases as a result of injection usage across
Pakistan.
There are several contributing reasons for irrational drug use requiring
integrated action at multiple tiers of the health systems. Standard therapies are
poorly enforced in the medical sector with prescribing practices influenced by
peer modeling on specialists, patients demand for quick treatment and
information by industry. Industry representatives have unrestricted access to
medical practitioners and reported nexus of industry and practitioners has been a
long-standing concern in Pakistan. Moreover over 79% of the population utilizes
the private sector which also comprises of both licensed providers as well as
quacks and informal providers, and continues to be loosely regulated. Although
there are successful examples of large CSOs franchising with GPs for appropriate
treatment these have yet to be replicated on a large scale. There is also
unrestricted access to drugs in retail outlets and an unnecessarily high number of
drug stores most of which do not meet appropriate dispensing requirements.
Financing & Affordability: 63% of total drug expenditure is borne by households,
one of the highest in developing countries, as opposed to only 18% in OECD
countries and leads to non-compliance with chronic care treatment and risk of
catastrophic expenditure. The public sector in Pakistan spends merely $5 per
capita when compared with other countries with similar income levels. Spending
by public sector is only 34% of total health expenditure and of that less than 25%
is spent on non-salary items including medicines. Patients incur costs for
medicines at both public and private sector facilities with drug shortages in public
sector forcing patients to private retail pharmacies. Patient spending on
medicines at public sector facilities is considerable at Rs198 on medicines / visit
versus Rs258 per visit at private sector facilities. At present there are no pre paid
schemes and commodity vouchers to ensure patient compliance with therapy and
protect households against catastrophic expenditure
There is wide gap between prices of generics and originator brands in Pakistan.
Certain medicines have very high prices several fold those of international
reference prices. Unaffordability of medicines has been documented as one of the
primary reasons for loose compliance with chronic care therapy. Medicine

152
therapy for chronic care is clearly unaffordable even with use of low cost
generics (MPR of 1.7-7.7) while it can be dangerously expensive with originator
brands (MPR of 1.9-36.4).
Reliable Health Systems: Policy concerns within this area are further sub-divided
into:
Supply Side Issues: In Pakistan availability of essential generics is extremely low
in public sector 3.3% in public sector compared to 29-54% in LMICs. only 21% of
the population utilizes the public sector facilities, despite provision of free
services, with medicine non-availability reported by users as one of the primary
reasons for dissatisfaction with public sector services. Amongst medicines, there
is relatively better availability of acute illness drugs 30-60%), much lower for
chronic care (1-57%), while that of emergency life medicines is alarmingly low (30-
50%). Reasons for frequent drug stock-outs have not been properly investigated
but are attributed to a combination of low budget, lack of rational procurement
and delayed release of funds.
There has been limited attention to management of drugs supply in the public
sector with issues of low quality and logistics management. Generic
procurement and cheapest tender practice in the public sector has managed to
secure efficient prices for drugs however lack of a quality threshold raises
widespread concerns over quality of drugs. Companies better known for quality
are hesitant to apply for public sector tenders due to fears of delayed payments,
rent seeking and government preference for favored suppliers. Lack of scientific
forecasting, budgeting and procurement results in areas of inefficiency and
inappropriate drug selection. Over the last decade, drug management has been
devolved to districts however there is little assessment of its impact on drug
quality and availability. Additionally manual logistic management systems and
poor storage facilities are key issues needing attention and while new systems are
in place for GFATM supported TB and malaria programs these need to be rolled
out to the mainstream public sector.
Improvement in drug availability has been seen in contracted Basic Health Units
with need for attention to alternative financing mechanisms for improving drug
availability. Only 8.3% falling in unsatisfactory category as compared to 87% of

153
those directly managed by the Department of Health, however quality,
appropriateness of drugs and storage have not been assessed. New financing
mechanisms can potentially improve drug access for the poor and need to be
aggressively explored.
Private retail outlets are the predominant means to supply to both private and
public sector patients however the existence of close to 80,000 drug stores, one
of the highest in developing countries, defeats attempts at regulation. Most of
these are drug stores rather than pharmacies, are manned by untrained persons
rather than pharmacists, and only a fifth of all retail outlets meet licensing
requirements. Disappearance of certain drugs from the market drugs is common
and is due to withholding by and black-marketing by wholesalers and distributors.
There is shortage of trained human resource across public and private sector for
drug procurement, management and dispensation. As opposed to WHO’s
recommended ratio of 1:2000 pharmacists per population, Pakistan has only 0.9
pharmacists per 100000 population, of which 70% are engaged in industry with a
very small core serving in health service delivery. Role of pharmacists is also not
institutionalized with selection and procurement dominated by medical doctors
while dispensing is done by junior untrained staff.
Regulation & Production: Pakistan produces 70% of consumed medicines
however close to 50% of the market belongs to multinationals and is far from
achieving self-sufficiency in production. Local production units number up to 414
but vary widely from well equipped units to those with questionable quality of
drugs putting into question licensing and quality assurance practices. Self-
sufficiency in tem of raw material production is yet to be achieved with
dependence essentially on imports. Although TRIPS has afforded certain new
opportunities there has been little use of patents and local companies need
assistance in deciphering legalities of patents on offer.
Pakistan has 76000-88000 registered drugs, one of the highest numbers in
LMICs, with many being unnecessary drugs having marginal therapeutic effect
over each other or multiple variations of the same drug available at different
prices and quality. Although Pakistan has detailed guidelines on licensing of drug
production units and registration of drugs however implementation has been

154
questionable with existing practice encouraging a market monopoly with loose
control. This results in irrational prescription, unnecessary drug expenditure and
weakens monitoring of quality assurance. Reliance on a traditional manual
registrations system makes it difficult to strategically plan and review drug
registrations while there has also been little utilization of the Central Research
Fund in bioequivalence and comparative cost analysis. There are wide
discrepancies in terms of quality of registered products with little incentive for
more sophisticated production units to invest in quality control. The Supreme
Court and Cabinet have recommended Creation of an autonomous Drug
Registration Authority to counter poor drug quality but still needs to be put into
practice.
Counterfeit medicines are common in Pakistan and need new modalities of
control. Traditional market monitoring systems is government dominated,
punitive and there are widespread concerns of nexus between laboratories,
inspectors, suppliers and industry. More participatory and incentive based
policies need to be implemented.
Price of standard chronic care therapy is unaffordable across generics and
originator brands and excessive prices are in place for certain medicines in
general. Pricing is based on input costs but lack of a clear pricing formula creates
opportunity for collusion and inefficient market spending on products. A flat price
control is in practice and although well intentioned has resulted in disappearance
of low cost essential medicines, even life saving drugs, from the market, little
impact on high priced items, and a general disincentive to producers.
Greater participation of implementers is needed in regulation however move to
totally devolve drug registration to provinces as part of ongoing devolution of
Ministry of Health may have serious repercussions. Regulatory capacity of
provinces is very uneven at present. Moreover total devolvement can result in
creation of potential inequities across the country with differential drug
availability and prices across provinces as well as cross provincial trafficking in
drugs. Institutional realignments need to be directed towards creation of an
autonomous drug regulation authority but built along more participatory lines.

155
RESEARCH NEEDS FOR ADDRESSING POLICY CONCERNS:
There is high need for evidence generation to assist action on prioritized policy
concerns. So far research in the pharmaceutical area in Pakistan has not been
from a comprehensive health systems perspective with the result that existing
research is small scale, mostly confined to rational prescription while areas such
as policy, supply side and financing have largely been overlooked. There is need
for collation of best practice from other countries, routine monitoring surveys to
assess policy impact, operational pilots for testing out new financing and supply
side strategies, formative research on health seeking and affordability, and
increased pharmaco-vigilance studies. For achieving this, an expanded range of
researchers needs to be involved including policy analysts, financing specialists,
health systems specialists in addition to pharma experts.
Key research priorities were identified through the consensus building exercise
and salient features are given as follows:
Continuous surveillance is needed into effect of national policies on medicine
availability, prices and affordability covering both the market and the public
sector. It is internationally recommended that such surveys should be repeated
periodically every two years however there has been no updating of information
since the last WHO global survey in 2004. District level information is also need to
assess impact of Local government Ordinance as well as Devolution of federal
Ministry of Health on access to medicines. Accompanying this there is also high
need for policy analysis research as to explore reasons underlying gap between
policy regulations and actual practice.
Pricing policies require examination to improve access to essential generics
particularly for standard chronic care therapy and contain prices of excessively
priced originator brands. There is need to move away from flat price control to
exploring optimal mix of pricing regulations based on lessons learnt from other
countries. There is also need to monitor price in the actual market to inform
pricing regulations and production of disaggregated information by prices fixed by
MOH, prices at retail pharmacies, and prices for public sector procurement.

156
Bottlenecks faced by the Essential Medicines Programme in Pakistan need to be
examined to reduce the gap between policy and practise. This would required
identification of constraints and opportunities at different health systems level.
Compilation of lessons learnt from other LMICs is needed for promotion of
generics at policy level, supply side level, individual provider levels and consumer
level.
Examination of alternative financing mechanisms is required to reduce medicine
expenditure borne by households particularly on chronic care therapy, and
supplement public sector provision. Possible mechanisms include franchising
with GPs, contracting with NGOs, commodity vouchers, health equity funds and
pre-payment schemes, to supplement public sector provision. As a first step
operational research pilots and compilation of best practise lessons are needed to
inform decision-making on best-suited financing mechanisms for Pakistan’s
context. Unit cost estimation of standard therapies will also be needed to roll out
financing support platforms for drugs.
Standardised mapping and assessment surveys of private sector are required
including of qualified providers, informal providers, shadow pharmacies, and
traditional healers. Information is needed on adequate licensing, prescription
practises, dispensation practises, medicine charges, and patient satisfaction.
Qualitative information is also needed on sources of information, openness to
regulation, and expressed information needs of private sector.
Formative research is needed into consumer demand, health-seeking
preferences, willingness to pay, and enhancing patient role in accountability.
Credibility of health professionals and the issue of trust is also an area that needs
to be explored.
Finally operation research is also needed into improving logistics and human
resource management in the public sector for improving drug access. Areas t be
looked into include scientific budgeting, forecasting and procurement, integrated
HMIS for drugs, institutionalization of pharmacists and increasing supply,
monitoring of quality storage, and routine monitoring of access to health
facilities.

157
CONCLUSION
Pakistan has relatively well documented policy and operative guidelines however
there is gap between policy and actual practice. There is tremendous need for
both standard assessment surveys to assess policy impacts as well exploratory
research to identify major constraints.
Priority areas as identified through this exploratory study and consensus building
exercise include
• Continuous surveillance of impact of policies on availability, price and
affordability
• Identification, regulation and monitoring of standard chronic care therapies
that would particularly benefit from reduced pricing and wider availability.
• Optimal mix of pricing regulations to reduce expenditure burden on
households.
• Tighter regulatory control to cut down on unnecessary medicines having
marginal therapeutic effect over each other.
• Market vigilance for spurious drugs and participatory strategies to counter
spurious drugs
• Multi-tiered health system measures for promotion of generics
• Operation pilots on alternative financing mechanisms to supplement public
sector through a range of commodity voucher, GP contracting, pre-payment
schemes, equity funds for increasing drug availability and affordability
• Mapping of private sector and exploring support needs for rational use
• Consumer health seeking preferences and participation in accountability
mechanisms
• Improvement of logistics and human resource management in public sector
for drug access
Pharmaceutical policy and research need to be centrally placed within larger
health systems related initiatives, reviews and policy updates. This needs to be
accompanied by sustained dialogue and interaction between entities including
public health sector, pharmacists association, medical doctors association, local
governments, industry, researchers and development partners. Adequate steps
also need to be taken to ensure access to research, feedback on research and a
continuous culture of research feeding into evidence based policies.

158

159
Consensus development on research priorities - Lebanon
As discussed under “Methods”, the researchers combined the research questions
emanating from the literature review and from the KII into one list. The
researchers aimed to reduce the large volume of questions and produce a list of
around 50-60 questions. As a result, a list of 57 questions was generated and
submitted to the validation and prioritization meeting (Appendix 6-C). While
questions were initially categorized according to four domains of the WHO 2004
ATM framework, it was decided to remove the categories and just provide a
single list. The rationale for this approach was to avoid imposing categories on
participants as they prioritized questions in the validation-prioritization meeting.
Furthermore, the researchers hoped that this would allow discussions among
participants to suggest whether the WHO 2004 framework was appropriate or
whether there are alternative frameworks that need to be considered.
After the first round we retained the 22 questions deemed important by at least
two thirds of the participants. Those questions were submitted to the ranking
exercise. The participants were asked to rate each question for a scale from 1 to
10 by each of five criteria. We then added up the scores of all 12 participants.
Appendix 6-D shows the rank of the 22 questions. The five questions that receive
the highest scores are (in descending order):
1. Assessment of quality of medicines on the market and role of counterfeit
medicines and black market.
2. A study of attitudes of physicians and of the public towards generic substitution
and the opportunities for implementing relevant policies
3. Is access to medicines a priority for policymakers, for professional associations,
and for consumer advocates?
4. Evaluation of the role of civil society organizations and non-governmental
organizations in improving access to medicines especially for the poor, vulnerable
groups and hard-to-reach populations.
5. What happens at the dispensary? Dispensing medicines or delivering primary
health care? Adherence to generics in PHC and dispensaries.

160
Conclusions
The provision of reliable access to affordable, appropriate and high-quality
medicines is a key component of a functioning health system. Access to medicines
needs to be fully integrated with health financing, human resource planning,
service delivery, information and governance systems. This is the first study
conducted in this region that has collated published literature and summarized
the main policy concerns to identify ATM research priorities. In this study we used
an extensive search of local and regional literature, interviews with key
informants, analysis of previous priority setting exercises and consensus
development approaches to identify the main research priorities for ATM
research. We developed detailed maps of research on the issue, conceptual
frameworks of policy concerns and issues, and identified lists of ATM research
priorities for the countries of focus and the region as a whole.
The main concerns of the key informants were around the affordability and
financing aspects of access to medicines, followed by issues of availability and
rational use of medicines. The key informants paid attention to all levels of
barriers to access: the household level, providers (public or private sector), health
system, other sectors and cross border issues. The identified previous research on
the issue, however, did not reflect that.
The results of the study indicate that ATM research in the region is heavily biased
towards RUD. RUD research has been mainly in the shape of prescription audits,
the majority of it showing there are important problems in prescriptions. In
recent years there is shift towards interventional studies assessing the impact of
interventions on improving prescribing outcomes. There are two important
patterns to note in here. First, the RUD research, although forming the majority of
ATM research is yet to show a substantial effect in improving drug utilization
patterns. The prescribing problems of focus in ten years ago remain unresolved
today, if not joined by new challenges (e.g. non-generic prescribing). Second, it
seems a change in research strategies is required and future studies should focus
161
on interventional issues. Fortunately there is a move in that direction. Also further
demand side (why public still sees fascinated with antibiotics) and health systems
angle (what are the financial and organizational barriers to improving prescribing
patterns) research will be required.
This study clearly indicates that there is dire need for further research on
financing and affordability aspects of ATM in the region. This should be given
paramount attention in future research funding and calls for proposals. Also
cross-border issues and other sectors roles on access to medicines in the region
has not explored widely. It seems that many household (demand side) studies in
the region remain of poor quality and limited methods. Together, these main
areas should provide the main aspects of access to medicines research in the
region.
This is in no way indicating that further RUD or studies of health systems and
availability access are not needed. Or that the barriers at the levels of providers
and health systems are exhaustively identified. Rather it seems that individual
researchers and available funding route are giving attention to these issues at the
moment, which should continue while further resources should be mobilized for
studies related to the relatively ignored aspects of ATM research in the region.
Almost 80% of AT research in the region is originating from the region. However,
there is a wide variation in the number of publications originating from different
countries. Certain countries (e.g. Somalia), or certain areas of other countries, do
not appear in the literature.
The picture of research on the ATM in the region is better than what had been
reported in recent publications that had not followed extensive methodologies.
There is a growing trend, over the years, of more and better quality studies from
the region appearing in international journals. Still, a concurrent trend will be
required to ensure the local audience of such research (i.e. practitioners, policy
makers and media) remains informed of the new development as a result of ATM

162
research in countries in the region. An active knowledge translation approach will
be essential.
Finally, the key informant interviews clearly demonstrate that the majority of
policy concerns were not addressed by published research. There was a mismatch
between the concerns and research, and hence the outcomes of this study can
contribute to developing a research agenda for improving access to and
appropriate use of medicines in the region and the three countries of focus.

163
Acknowledgements
The study is funded by the Alliance for Health Policy and Systems Research
(AHPSR). AHPSR works within the Health Systems Strengthening cluster of WHO
HQ. It aims at promoting the generation and use of health policy and systems
research as a means to improve the health systems of developing countries. The
Access to Medicines (ATM) Policy research is a new program of work,
implemented by the AHPSR and funded by the UK Department for International
Development (DfID). The program aims at improving the availability and use of
evidence on access to medicines in Low and Middle Income countries.
The investigators thank the AHPSR for its support and guidance, especially Dr
Abdul Ghaffar, Dr Maryam Bigdeli and Maryse Coutty and their colleagues for thei
excellent support. Especially we would like to thank Maryam Bigdeli for he hands-
on support and for attending our workshop and focus group discussion in Karachi.
The authors also thank the research ethics committees in the three universities
and the research governance bodies. The authors are indebted to the
interviewees and the consensus development participants for their valuable input
and time. The teams received advice and support from different individuals in the
three countries. They would also thank Prof Soonman Kwon who attended the
workshop in Tehran as a resource person.
The views expressed in the document are those of the individual authors and do
not necessarily reflect the views of their respective organizations or the funding
body.
164
References – regional study
1. Cheraghali AM, Soleymani F, Shalviri G. Promoting rational use activities in Iran: a successful
trend. Essential Drugs Monitor 2003;33:10-11.
2. DFID W. EDSP Baseline Survey Report. Prescription, dispensing and storage practices in the
provinces of NWFP, Baluchistan and Punjab in collaboration with Network for Consumer
Protection, 2002.
3. Najmi MH, Hafiz RA, Khan I, Fazli FR. Prescribing practices: an overview of three teaching
hospitals in Pakistan. J Pak Med Assoc 1998;48(3):73-7.
4. Das N. Prescribing Practices of Consultants at Karachi Pakistan. . JPMA 2001.
5. Haider S, Thaver IH. Self medication or self care: implication for primary health care
strategies. J Pak Med Assoc 1995;45(11):297-8.
6. Zafar SN, Syed R, Waqar S, Irani FA, Saleem S. Prescription of medicines by medical students
of Karachi, Pakistan: a cross-sectional study. BMC Public Health 2008;8:162.
7. Shehzadi R, Irfan M, Zohra T, Khan JA, Hussain SF. Knowledge regarding management of
tuberculosis among general practitioners in northern areas of Pakistan. J Pak Med Assoc
2005;55(4):174-6.
8. Khan J, Malik A, Hussain H, Ali NK, Akbani F, Hussain SJ, et al. Tuberculosis diagnosis and
treatment practices of private physicians in Karachi, Pakistan. East Mediterr Health J
2003;9(4):769-75.
9. Jafar TH, Jessani S, Jafary FH, Ishaq M, Orakzai R, Orakzai S, et al. General practitioners'
approach to hypertension in urban Pakistan: disturbing trends in practice. Circulation
2005;111(10):1278-83.
10. WHO. The World Medicines Situation., 2004.
11. Janjua NZ. Injection practices and sharp waste disposal by general practitioners of Murree,
Pakistan. J Pak Med Assoc 2003;53(3):107-11.
12. Siddiqi S, Hamid S, Rafique G, Chaudhry SA, Ali N, Shahab S, et al. Prescription practices of
public and private health care providers in Attock District of Pakistan. Int J Health Plann
Manage 2002;17(1):23-40.
13. Samad L. SIGN Rapid Assessment Survey Northern Areas, Pakistan 2001.
14. Siddiqui S, Hussein K, Manasia R, Samad A, Salahuddin N, Zafar A, et al. Impact of antibiotic
restriction on broad spectrum antibiotic usage in the ICU of a developing country. J Pak
Med Assoc 2007;57(10):484-7.
15. WHO-EMRO. The Work of WHO in the Eastern Mediterranean Region, Annual Report of the
Regional Director, 1 January - 31 December 2000, 2000.

165
16. Sturm AW, van der Pol R, Smits AJ, van Hellemondt FM, Mouton SW, Jamil B, et al. Over-
the-counter availability of antimicrobial agents, self-medication and patterns of
resistance in Karachi, Pakistan. J Antimicrob Chemother 1997;39(4):543-7.
17. Pakistan Go. National Health Accounts for Pakistan, Islamabad, . 2009.
18. Laing R. Improving Access to Child Health Medicines Review and Discussion Paper prepared
for WHO Regional and Country Child Health Advisers Geneva, 2002.
19. Bank. W. The World Bank Country data, Pakistan. Washington., 2008.
20. World Bank SAR. Sindh: Health Policy Note, 2005.
21. World Bank SAR. Health and Population Policy Note for Pakistan, 2007.
22. Bank W. Delivering Better Health Services to Pakistan's poor, 2010.
23. WHO. Regional Office for Eastern Mediterranean Technical discussion on Medicine prices
and access to medicines in the Eastern Mediterranean Region. WHO Regional Office for
the Eastern Mediterranean. Accessed on 17th February 2010. , 2007.
24. Kadir MM, Khan A, Sadruddin S, Luby SP. Out-of-pocket expenses borne by the users of
obstetric services at government hospitals in Karachi, Pakistan. J Pak Med Assoc
2000;50(12):412-5.
25. Khowaja LA, Khuwaja AK, Cosgrove P. Cost of diabetes care in out-patient clinics of Karachi,
Pakistan. BMC Health Serv Res 2007;7:189.
26. WHO HAI. Medicine prices, availability, affordability and price components, A synthesis
report of medicine. Price surveys undertaken in selected countries of the WHO Eastern
Mediterranean Region, . 2008.
27. EMRO W-. Regional Health Systems Observatory- EMRO, 2011.
28. Pakistan FBoSGo. Pakistan social and living standards measurement survey-pslm-2006-07,
2006-07.
29. Pakistan FBoSGo. Pakistan social and living standards mearurement survey-pslm-2004-05
2004-05
30. Mendis S, Fukino K, Cameron A, Laing R, Filipe A, Jr., Khatib O, et al. The availability and
affordability of selected essential medicines for chronic diseases in six low- and middle-
income countries. Bull World Health Organ 2007;85(4):279-88.
31. Associates WBaA. Evaluation of quality of care in public sector in Sindh., 2008.
32. Norway-Pakistan Partnership Initiative OUPiPMMoH, Government of Sindh. Baseline survey
of key indicators in Sindh 2009, . , 2009.
33. Fikree FF, Mir AM, Haq IU. She may reach a facility but will still die! An analysis of quality of
public sector maternal health services, District Multan, Pakistan. J Pak Med Assoc
2006;56(4):156-63.
34. Meyer J. Emergency Obstetric Care:Critical Need among Populations Affected by Conflict.
Reproductive Health Response in Conflict Consortium.

166
http://womensrefugeecommission.org/docs/emoc.pdf Accessed on 19th February 2011, 2004.
35. Oxford. SN. Choked pipes, 2010.
36. Imran M, Khan FA, Abbasi S. Standards for labelling and storage of anaesthetic medications-
-an audit. J Pak Med Assoc 2009;59(12):825-8.
37. Loevinsohn B, Haq IU, Couffinhal A, Pande A. Contracting-in management to strengthen
publicly financed primary health services--the experience of Punjab, Pakistan. Health
Policy 2009;91(1):17-23.
38. S.K.S Bukhari JARHQ, Jooma 1 R., Bile K.M, et al. Essential medicines management during
emergencies in Pakistan. EMHJ 2010;Vol. 16.
39. Butt ZA, Gilani AH, Nanan D, Sheikh AL, White F. Quality of pharmacies in Pakistan: a cross-
sectional survey. Int J Qual Health Care 2005;17(4):307-13.
40. PMDC. PMDC Ordinance 1962. Available at
http://www.pmdc.org.pk/AboutUs/tabid/72/Default.aspx. Accessed on 20th June 2011,
2011.
41. Rohra DK, Gilani AH, Memon IK, Perven G, Khan MT, Zafar H, et al. Critical evaluation of the
claims made by pharmaceutical companies in drug promotional material in Pakistan. J
Pharm Pharm Sci 2006;9(1):50-9.
42. Hafeez A, Mirza Z. Responses from pharmaceutical companies to doctors' requests for more
drug information in Pakistan: postal survey. BMJ 1999;319(7209):547.
43. Pakistan M. Pharmaceutical Country Profile. Pakistan. 2010.
44. Pakistan Go. Ministry of Health of Pakistan, Islamabad. Accessed on 20 th June
2011.http://202.83.164.26/wps/portal/Moh, 2011.
45. PPMA. http://www.ppma.org.pk/PPMAIndustry.aspx 2007.
46. Protection. TNfC. Prices, availability and affordability of medicines in Pakistan., 2006.
47. London. IPN. Julian Morris and Philip Stevens. Counterfeit medicines in less developed
countries. Problems and solutions.. Accessed on 18th February 2011., 2006.
48. Nishtar S. Pharmaceuticals--strategic considerations in health reforms in Pakistan. J Pak
Med Assoc 2006;56(12 Suppl 4):S100-11.
49. Wagner JL, McCarthy E. International differences in drug prices. Annu Rev Public Health
2004;25:475-95.
50. Vasan A, Hoos D, Mukherjee JS, Farmer PE, Rosenfield AG, Perriens JH. The pricing and
procurement of antiretroviral drugs: an observational study of data from the Global
Fund. Bull World Health Organ 2006;84(5):393-8.
51. Hogerzeil HV, Samson M, Casanovas JV, Rahmani-Ocora L. Is access to essential medicines
as part of the fulfilment of the right to health enforceable through the courts? Lancet
2006;368(9532):305-11.
52. Suh GH. High medicine prices and poor affordability. Curr Opin Psychiatry 2011;24(4):341-5.
167
53. Kishore SP, Vedanthan R, Fuster V. Promoting global cardiovascular health ensuring access
to essential cardiovascular medicines in low- and middle-income countries. J Am Coll
Cardiol 2011;57(20):1980-7.
54. Berendes S, Heywood P, Oliver S, Garner P. Quality of private and public ambulatory health
care in low and middle income countries: systematic review of comparative studies.
PLoS Med 2011;8(4):e1000433.
55. Faden L, Vialle-Valentin C, Ross-Degnan D, Wagner A. Active pharmaceutical management
strategies of health insurance systems to improve cost-effective use of medicines in low-
and middle-income countries: a systematic review of current evidence. Health Policy
2011;100(2-3):134-43.
56. Renaud-Thery F, Avila-Figueroa C, Stover J, Thierry S, Vitoria M, Habiyambere V, et al.
Utilization patterns and projected demand of antiretroviral drugs in low- and middle-
income countries. AIDS Res Treat 2011;2011:749041.
57. Machado M, O'Brodovich R, Krahn M, Einarson TR. International drug price comparisons:
quality assessment. Rev Panam Salud Publica 2011;29(1):46-51.
58. Hoen E, Berger J, Calmy A, Moon S. Driving a decade of change: HIV/AIDS, patents and
access to medicines for all. J Int AIDS Soc 2011;14:15.
59. Wagner AK, Graves AJ, Reiss SK, Lecates R, Zhang F, Ross-Degnan D. Access to care and
medicines, burden of health care expenditures, and risk protection: results from the
World Health Survey. Health Policy 2011;100(2-3):151-8.
60. Salameh P, Najjar Aad M, Semaan M, El Hawzi R, Bechara M, El Kadi B, et al. [Drug circuit in
Lebanese hospitals]. Rev Epidemiol Sante Publique 2007;55(4):308-13.
61. Ben Abdelaziz A, Harrabi I, Rahmani S, Gaha R, Ghannem H. Circulation of pharmaceutical
information among general practioners in the region of Sousse (Tunisia). Therapie
2002;57(3):229-35.
62. Belkacem A. [Profile of prescription of psychotropic drugs in a National Fund of Social
Foresight Organisation in Morocco]. Encephale 2006;32(3 Pt 1):335-40.
63. Soussi-Tanani D, Alaoui K, Belaiche A, Hassar M, Cherrah Y. [Consumption analyze of the
antihypertensive drugs in Morocco: period 1991-2005]. Therapie 2008;63(2):129-33.
64. Hachfi W, Kaabia N, Bougmiza I, Bellazreg F, Hattab Z, Ben Lasfar N, et al. [Prescribing
practices of fluoroquinolones in Tunisia]. Rev Med Liege 2011;66(4):205-8.
65. Alwarafi A, Hartlova S. [The Yemen health service and possibilities of cooperation with the
Czech Republic in the area of pharmacy]. Ceska Slov Farm 2001;50(3):120-3.
66. Wagner AK, Graves AJ, Reiss SK, Lecates R, Zhang F, Ross-Degnan D. Access to care and
medicines, burden of health care expenditures, and risk protection: Results from the
World Health Survey. Health Policy 2010.
168
67. Mirza Z. Thirty years of essential medicines in primary health care. East Mediterr Health J
2008;14 Suppl:S74-81.
68. Vialle-Valentin CE, Ross-Degnan D, Ntaganira J, Wagner AK. Medicines coverage and
community-based health insurance in low-income countries. Health Res Policy Syst
2008;6:11.
69. Niens LM, Cameron A, Van de Poel E, Ewen M, Brouwer WB, Laing R. Quantifying the
impoverishing effects of purchasing medicines: a cross-country comparison of the
affordability of medicines in the developing world. PLoS Med 2010;7(8).
70. Kanavos P, Vandoros S, Garcia-Gonzalez P. Benefits of global partnerships to facilitate
access to medicines in developing countries: a multi-country analysis of patients and
patient outcomes in GIPAP. Global Health 2009;5:19.
71. Thatte U, Hussain S, de Rosas-Valera M, Malik MA. Evidence-based decision on medical
technologies in Asia Pacific: experiences from India, Malaysia, Philippines, and Pakistan.
Value Health 2009;12 Suppl 3:S18-25.
72. Large M, Farooq S, Nielssen O, Slade T. Relationship between gross domestic product and
duration of untreated psychosis in low- and middle-income countries. Br J Psychiatry
2008;193(4):272-8.
73. Mustafa AA, Kowalski SR. A comparative analysis of the Libyan national essential medicines
list and the WHO model list of essential medicines. Libyan J Med 2010;5.
74. Nunan M, Duke T. Effectiveness of pharmacy interventions in improving availability of
essential medicines at the primary healthcare level. Trop Med Int Health
2011;16(5):647-58.
75. Cameron A, Roubos I, Ewen M, Mantel-Teeuwisse AK, Leufkens HG, Laing RO. Differences in
the availability of medicines for chronic and acute conditions in the public and private
sectors of developing countries. Bull World Health Organ 2011;89(6):412-21.
76. Kuemmerle A, Dodoo AN, Olsson S, Van Erps J, Burri C, Lalvani PS. Assessment of global
reporting of adverse drug reactions for anti-malarials, including artemisinin-based
combination therapy, to the WHO Programme for International Drug Monitoring. Malar
J 2011;10:57.
77. Smith F. The quality of private pharmacy services in low and middle-income countries: a
systematic review. Pharm World Sci 2009;31(3):351-61.
78. Imran M, Khan FA, Abbasi S. Standards for labelling and storage of anaesthetic medications
- an audit. JPMA Journal of the Pakistan Medical Association 2009;59(12):825-28.
79. Khalili H, Dashti-Khavidaki S, Talasaz AHH, Tabeefar H, Hendoiee N. Descriptive Analysis of a
Clinical Pharmacy Intervention to Improve the Appropriate Use of Stress Ulcer
Prophylaxis in a Hospital Infectious Disease Ward. Journal of Managed Care Pharmacy
2010;16(2):114-21.
169
80. Khalili H, Dashti-Khavidaki S, Talasaz AH, Mahmoudi L, Eslami K, Tabeefar H. Is deep vein
thrombosis prophylaxis appropriate in the medical wards? A clinical pharmacists'
intervention study. Pharm World Sci 2010;32(5):594-600.
81. Gariani A, Rahbar M, Ghafourian T, Maleki N, Garjani A, Salimnejad M, et al. Relationship of
pharmacist interaction with patient knowledge of dispensed drugs and patient
satisfaction. Eastern Mediterranean Health Journal 2009;15(4):934-43.
82. Ehsani A, Esmaily N, Noormohammadpour P, Toosi S, Hosseinpour A, Hosseini M, et al. The
comparison between the efficacy of high dose acyclovir and erythromycin on the period
and signs of pitiriasis rosea. Indian J Dermatol 2010;55(3):246-8.
83. Ritz LS, Adam T, Laing R. A bibliometric study of publication patterns in access to medicines
research in developing countries. Southern Medical Review 2010;3(1):2-6.
84. Basmenji K. Pharmaceuticals in Iran: an overview. Archives of Iranian Medicine
2004;7(2):158-64.
85. Davari M, Walley T, Haycox A. Pharmaceutical policy and market in Iran: past experiences
and future challenges. Journal of Pharmaceutical Health Services Research 2011;2:47-52.
86. Zargarzadeh AH, Minaeiyan M, Torabi A. Prescription and nonprescription drug use in
Isfahan, Iran: An observational, cross-sectional study. Current Therapeutic Research-
Clinical and Experimental 2008;69(1):76-87.

Reference list. List of EMR region literature on ATM issues
First author Title Year Country of
origin
Country (ies) in
focus
Abdo-Rabbo, A Prescribing rationality and availability of antimalarial drugs
in Hajjah, Yemen 2003 Yemen Yemen
Abi Rizk, G
Determinants of antibiotic use and throat culture in
managing pharyngitis among primary health care physicians
in Beirut
2010 Lebanon Lebanon
Abu Rumman, K Training on the Practical Approach to Lung Health: effect on
drug prescribing in PHC settings in Jordan 2009 Jordan Jordan
Aburuz, S. M. Comprehensive assessment of treatment related problems
in hospitalized medicine patients in Jordan 2011 Jordan Jordan
Ahmed, A. M Drug use practices at pediatric hospitals of Khartoum State,
Sudan 2010 Sudan Sudan
Al Seyed prospective study on antibiotic misuse among infants with
upper respiratory infections 2009 Lebanon Lebanon
Al-Abbadi, I One-Year Assessment of Joint Procurement of
Pharmaceuticals in the Public Health Sector in Jordan. 2009 Jordan Jordan
Al-Azzam, S. I. Self-medication with antibiotics in Jordanian population 2007 Jordan Jordan

171
First author Title Year Country of
origin
Country (ies) in
focus
Al-Bakri, A. G
Community consumption of antibacterial drugs within the
Jordanian population: sources, patterns and
appropriateness
2005 Jordan Jordan
Albsoul-Younes,
A
Abuse and misuse of prescription and nonprescription drugs
sold in community pharmacies in Jordan 2010 Jordan Jordan
Al-Faham, Z The sale of antibiotics without prescription in pharmacies in
Damascus, Syria 2011 Syria Syria
Ali, G. K How to establish a successful revolving drug fund: the
experience of Khartoum state in the Sudan 2009 Sudan Sudan
Ali, G. K. A prescription for improvement: A short survey to identify
reasons behind public sector pharmacists' migration 2006 Sudan Sudan
Ali, G. K. M. Accessibility of medicines and primary health care: The
impact of the revolving drug fund in Khartoum State 2009 Sudan Sudan
Ali, O QUALITY OF CEFTRIAXONE IN PAKISTAN: REALITY AND
RESONANCE 2009 Pakistan Pakistan
Al-Niemat, S. I
Drug use evaluation of antibiotics prescribed in a Jordanian
hospital outpatient and emergency clinics using WHO
prescribing indicators
2008 Jordan Jordan

172
First author Title Year Country of
origin
Country (ies) in
focus
Altaf, A The cost of unsafe injections in pakistan and challenges for
prevention program 2006 Pakistan Pakistan
Al-Taiar, A
Who develops severe malaria? Impact of access to
healthcare, socio-economic and environmental factors on
children in Yemen: a case-control study
2008 Yemen Yemen
Alwarafi, A The Yemen health service and possibilities of cooperation
with the Czech Republic in the area of pharmacy 2001 Czech Yemen
Ameli, O.
Contracting for health services: effects of utilization and
quality on the costs of the Basic Package of Health Services
in Afghanistan
2008 Afghanistan Afghanistan
Amin, M. E Sources of drug information for patients with chronic
conditions in Alexandria, Egypt. 2011 Egypt Egypt
Awad Drug-use practices in teaching hospitals of Khartoum State,
Sudan
2006 Sudan Sudan
Awad, A Self-medication practices with antibiotics and antimalarials
among Sudanese undergraduate university students 2007 Kuwait Sudan
Awad, A Medical doctors' perceptions and expectations of the role
of hospital pharmacists in Sudan 2007 Kuwait Sudan

173
First author Title Year Country of
origin
Country (ies) in
focus
Awad, A Self-medication with Antibiotics and Antimalarials in the
community of Khartoum State, Sudan 2005 Kuwait Sudan
Awad, A. A. I Drug use practices in teaching hospitals of Khartoum State,
Sudan 2009 Kuwait Sudan
Azhar The role of pharmacists in developing countries: the current
scenario in Pakistan
2009 Malaysia Pakistan
Azhar, S.
A survey evaluating nurses' perception and expectations
towards the role of pharmacist in Pakistan's healthcare
system
2011 Malaysia Pakistan
Azoulay, L Inappropriate medication prescribing in community-
dwelling elderly people living in Iran 2005 Canada Iran
Babar Social pharmacy strengthening clinical pharmacy: why
pharmaceutical policy research is needed in Pakistan? 2008 NewZealand Pakistan
Baniasadi Developing an Adverse Drug Reaction Reporting System at a
Teaching Hospital 2008 Iran Iran
Bashrahil, K. A Antimalarial drugs: availability and mode of prescribing in
Mukalla, Yemen 2010 Yemen Yemen
Basmenji PHARMACEUTICALS IN Iran: AN OVERVIEW 2004 Iran Iran
Belkacem, A. Profile of prescription of psychotropic drugs in a National
Fund of Social Foresight Organisation in Morocco 2006 Morocco Morocco

174
First author Title Year Country of
origin
Country (ies) in
focus
Ben Abdelaziz,
A.
[Circulation of pharmaceutical information among general
practitioners in the region of Sousse (Tunisia)] 2002 Tunisia Tunisia
Ben Salem, K Essential drugs: availability and prescription in Monastir
(Tunisia) health district 2000 Tunisia Tunisia
Bodenschatz, C Injection prescribing patterns in public health care facilities
in Egypt. 2009 Egypt Egypt
Bukhari Essential medicines management during emergencies in
Pakistan 2010 Pakistan Pakistan
Butt, Z. A Quality of pharmacies in Pakistan: a cross-sectional survey 2005 Pakistan Pakistan
Cameron
Differences in the availability of medicines for chronic and
acute conditions in the public and private sectors of
developing countries
2011 Switzerland
mentions Iran,
Jordan, Lebanon,
Morocco,
Pakistan, Sudan,
Syria, Tunisia,
Yemen
Cameron, A., M
Medicine prices, availability, and affordability in 36
developing and middle-income countries: a secondary
analysis
2009
World Health
Organization,
Geneva,
Switzerland
mentions Jordan,
Lebanon,
Pakistan, Sudan,
Syria, Tunisia,
Yemen, UAE,
Kuwait
Cheraghali, A. M Improving availability and affordability of plasma-derived
medicines 2010 Iran Iran

175
First author Title Year Country of
origin
Country (ies) in
focus
Cheraghali, A. M Economical impact of plasma fractionation project in Iran
on affordability of plasma-derived medicines 2009 Iran Iran
Cheraghali, A. M Availability of blood components and plasma derived
medicines in Iran 2007 Iran Iran
Cheraghali, A. M Evaluation of availability, accessibility and prescribing
pattern of medicines in the Islamic Republic of Iran 2004 Iran Iran
Cheraghali, A. M Availability, affordability, and prescribing pattern of
medicines in Sudan 2009 Iran sudan
Das, N. Prescribing practices of consultants at Karachi, Pakistan 2001 Pakistan Pakistan
Dashti-
Khavidaki, S
Clinical pharmacy services in an Iranian teaching hospital: a
descriptive study 2009 Iran Iran
Davari Pharmaceutical policy and market in Iran: past experiences
and future challenges 2011 Iran Iran
Dinarvand, R
New National Drug Policy in Iran leading to Expanded
Pharmaceutical Market and Extended Access of Public to
Medicines
2009 Iran Iran
Ebrahimzadeh,
M. A
Utilization pattern of antibiotics in different wards of
specialized Sari Emam University Hospital in Iran 2008 Iran Iran
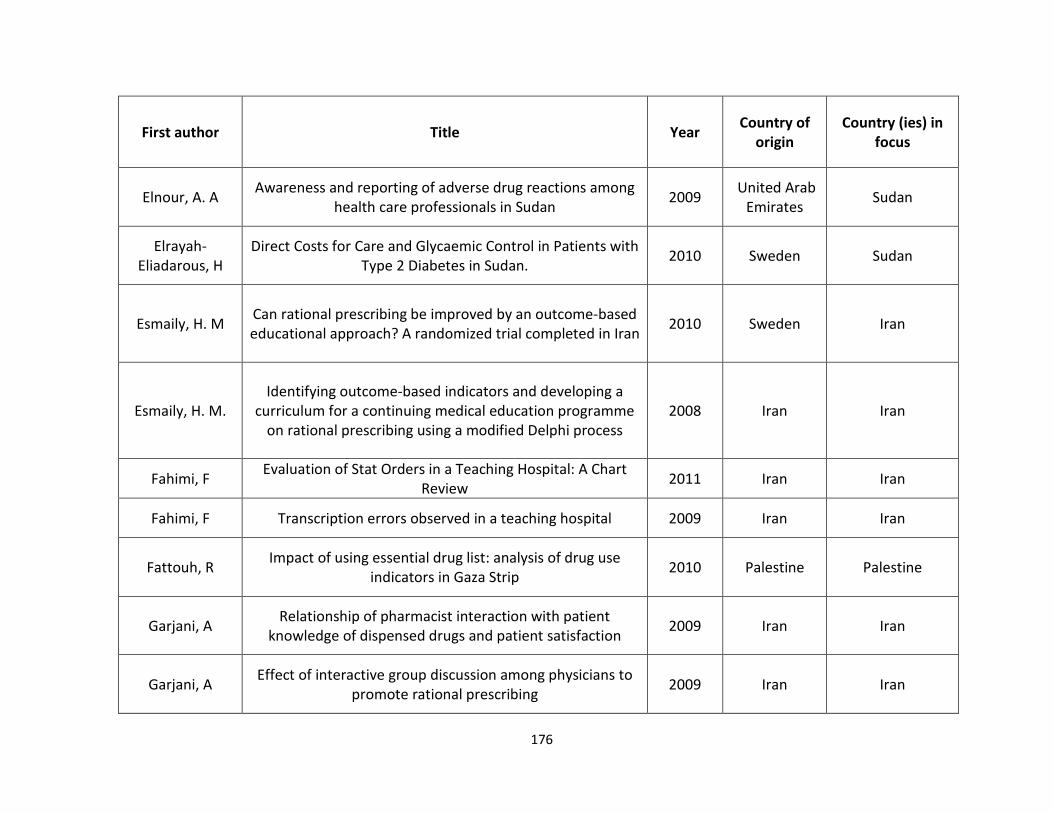
176
First author Title Year Country of
origin
Country (ies) in
focus
Elnour, A. A Awareness and reporting of adverse drug reactions among
health care professionals in Sudan 2009
United Arab
Emirates Sudan
Elrayah-
Eliadarous, H
Direct Costs for Care and Glycaemic Control in Patients with
Type 2 Diabetes in Sudan. 2010 Sweden Sudan
Esmaily, H. M Can rational prescribing be improved by an outcome-based
educational approach? A randomized trial completed in Iran 2010 Sweden Iran
Esmaily, H. M.
Identifying outcome-based indicators and developing a
curriculum for a continuing medical education programme
on rational prescribing using a modified Delphi process
2008 Iran Iran
Fahimi, F Evaluation of Stat Orders in a Teaching Hospital: A Chart
Review 2011 Iran Iran
Fahimi, F Transcription errors observed in a teaching hospital 2009 Iran Iran
Fattouh, R Impact of using essential drug list: analysis of drug use
indicators in Gaza Strip 2010 Palestine Palestine
Garjani, A Relationship of pharmacist interaction with patient
knowledge of dispensed drugs and patient satisfaction 2009 Iran Iran
Garjani, A Effect of interactive group discussion among physicians to
promote rational prescribing 2009 Iran Iran

177
First author Title Year Country of
origin
Country (ies) in
focus
Gelders Price, availability and affordability An international
comparison of chronic disease medicines 2006 Egypt
mentions Jordan,
Lebanon,
Morocco,
Ghadimi, H General practitioners' prescribing patterns for the elderly in
a province of Iran 2011 Sweden Iran
Hachfi, W Prescribing practices of fluoroquinolones in Tunisia 2011 Tunisia Tunisia
Hafeez, A Prescription and dispensing practices in public sector health
facilities in Pakistan: survey report 2004 Pakistan Pakistan
Hajebi, G
A Survey of Knowledge, Attitude and Practice of Nurses
towards
Pharamacovigilance in Taleqani Hospital
2010 Iran Iran
Hamidi, S Implementing an essential medicines list: effects on pricing
and utilization in West Bank, Palestine 2008 Palestine Palestine
Harper
Afghanistan pharmaceutical
sector development: problems and
prospects
2011 Hungary Afghanistan
Hassan, N. A
The impact of problem-based pharmacotherapy training on
the competence of rational prescribing of Yemen
undergraduate students
2000 Yemen Yemen

178
First author Title Year Country of
origin
Country (ies) in
focus
Hosseini SAR Counterfeit medicines: Report of a cross-sectional
retrospective study in Iran 2010 Iran Iran
Imran, M. Standards for labelling and storage of anaesthetic
medications--an audit. 2009 Pakistan Pakistan
JANJUA Injection use in two districts of Pakistan: implications for
disease prevention 2005 pakistan Pakistan
Kanavos, P
Benefits of global partnerships to facilitate access to
medicines in developing countries: a multi-country analysis
of patients and patient outcomes in GIPAP
2009 UK mentions
Pakistan, Sudan
Kassab, I Setup of a national system of adverse drug reaction
reporting in Lebanon: results of the first year of activity 2005 Lebanon Lebanon
Khalili, H Anticoagulant utilization evaluation in a teaching hospital: a
prospective study. 2010 Iran Iran
Khalili, H Is deep vein thrombosis prophylaxis appropriate in the
medical wards? A clinical pharmacists' intervention study 2010 Iran Iran
Khalili, H
Descriptive analysis of a clinical pharmacy intervention to
improve the appropriate use of stress ulcer prophylaxis in a
hospital infectious disease ward
2010 Iran Iran
Khan, M. S Common trend of antibiotics usage in a tertiary care
hospital of Peshawar, Pakistan 2010 Pakistan Pakistan

179
First author Title Year Country of
origin
Country (ies) in
focus
Khawaja, M. R Prescription pattern of benzodiazepines for inpatients at a
tertiary care university hospital in Pakistan 2005 Pakistan Pakistan
Khdour, M. R Extent and nature of unlicensed and off-label medicine use
in hospitalised children in Palestine 2011 Palestine Palestine
Kheir Pharmacy Education and Practice in 13 Middle Eastern
Countries 2008 Qatar
focuses on Arab
speaking
countries
Khowaja, K., R A systematic approach of tracking and reporting medication
errors at a tertiary care university hospital, Karachi, Pakistan 2008 Pakistan Pakistan
Kuemmerle
Assessment of global reporting of adverse drug reactions
for anti-malarials, including artemisininbased combination
therapy, to the WHO Programme for International Drug
monitoring
2011 USA mentions Iran,
Morocco, Tunisia
Large, M., S Relationship between gross domestic product and duration
of untreated psychosis in low- and middle-income countries 2008 Australia
mentions Egypt,
Iran, Pakistan
Lowe Legislation, regulation, and consolidation in the retail
pharmacy sector in low-income countries 2009 USA
mentions
Pakistan,
Lebanon

180
First author Title Year Country of
origin
Country (ies) in
focus
Makhlouf
Obermeyer, C
Medication use, gender, and socio-economic status in
Lebanon: analysis of a national survey 2002 Switerland Lebanon
Mannan, A. A Antimalarial prescribing and dispensing practices in health
centres of Khartoum state, 2003-04 2009 Sudan Sudan
Mashayekhi, S.
O
Study of awareness among pregnant women of the effects
of drugs on the fetus and mother in Iran 2009 Iran Iran
Mendis, S., K
The availability and affordability of selected essential
medicines for chronic diseases in six low- and middle-
income countries
2007 Switzerland mentions
Pakistan
Mirza, Z. Thirty years of essential medicines in primary health care 2008 Egypt mentions EMR
Mohagheghi, M.
A
Community-based outpatient practice of antibiotics use in
Tehran 2005 Iran Iran
Mustafa, A. A
A comparative analysis of the Libyan national essential
medicines list and the WHO model list of essential
medicines
2010 libya libya
Mustafa, A. A A need for the standardization of the pharmaceutical sector
in Libya 2010 libya libya
Nader, F Patient sources for drug information in Iran: A
questionnaire-based survey 2008 Iran Iran
Namazi, S A Drug Utilization Research on Aminophylline/Theophylline
in Ali-Asghar Hospital, Shiraz, Southern Iran 2010 Iran Iran
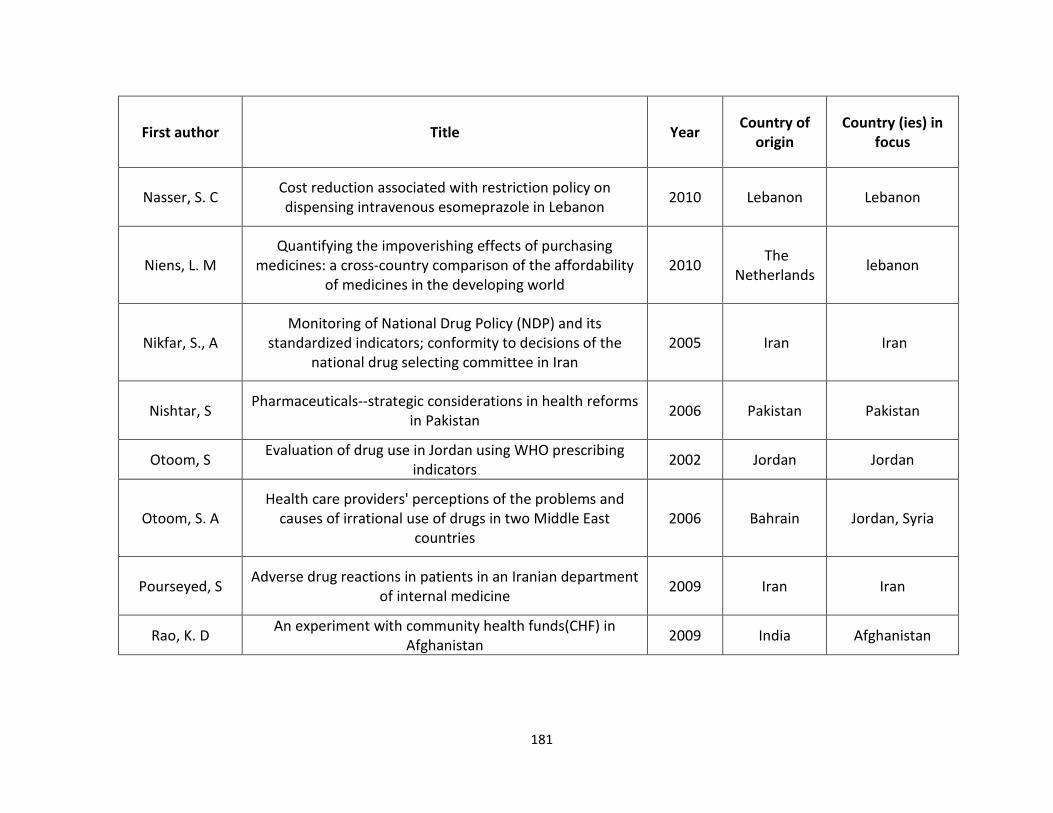
181
First author Title Year Country of
origin
Country (ies) in
focus
Nasser, S. C Cost reduction associated with restriction policy on
dispensing intravenous esomeprazole in Lebanon 2010 Lebanon Lebanon
Niens, L. M
Quantifying the impoverishing effects of purchasing
medicines: a cross-country comparison of the affordability
of medicines in the developing world
2010 The
Netherlands lebanon
Nikfar, S., A
Monitoring of National Drug Policy (NDP) and its
standardized indicators; conformity to decisions of the
national drug selecting committee in Iran
2005 Iran Iran
Nishtar, S Pharmaceuticals--strategic considerations in health reforms
in Pakistan 2006 Pakistan Pakistan
Otoom, S Evaluation of drug use in Jordan using WHO prescribing
indicators 2002 Jordan Jordan
Otoom, S. A
Health care providers' perceptions of the problems and
causes of irrational use of drugs in two Middle East
countries
2006 Bahrain Jordan, Syria
Pourseyed, S Adverse drug reactions in patients in an Iranian department
of internal medicine 2009 Iran Iran
Rao, K. D An experiment with community health funds(CHF) in
Afghanistan 2009 India Afghanistan

182
First author Title Year Country of
origin
Country (ies) in
focus
Raoof
Awareness and Use of Benzodiazepines in Healthy
Volunteers and Ambulatory Patients Visiting a Tertiary Care
Hospital: A Cross Sectional Survey
2008 Pakistan Pakistan
Rickrode, G. A Internal reporting system to improve a pharmacy's
medication distribution process 2007 Lebanon Lebanon
Ritz A bibliometric study of publication patterns in access to
medicines research in developing countries 2010 USA mentions EMR
Saab, B. R List of essential drugs for primary care in Lebanon 2001 Lebanon Lebanon
Saab, Y. B Inappropriate medication use in elderly lebanese
outpatients: prevalence and risk factors 2006 Lebanon Lebanon
Sabawoon, W Delay in the treatment of pulmonary tuberculosis: a report
from Afghanistan 2011 Japan Afghanistan
Sabzghabaee, A.
M
The design and equipments of hospital pharmacies in
Isfahan, Iran 2010 Iran Iran
Sahebi, L Self-medication and storage of drugs at home among the
clients of drugstores in Tabriz 2009 Iran Iran
Salameh, P Drug circuit in Lebanese hospitals 2007 Lebanon Lebanon
Salameh, P Pharmacy manpower in Lebanon: An exploratory look at
work-related satisfaction 2007 Lebanon Lebanon

183
First author Title Year Country of
origin
Country (ies) in
focus
Salameh, P. R Clinical pharmacy in Lebanon: a pilot study regarding health
care professionals' opinion 2006 Lebanon Lebanon
Sallam, S. A Pharmacoepidemiological study of self-medication in adults
attending pharmacies in Alexandria, Egypt. 2009 Egypt Egypt
Sarahroodi, S Antibiotics Self-Medication among Southern Iranian
University Students. 2010 Iran Iran
Sawair, F. A Assessment of Self-Medication of Antibiotics in a Jordanian
Population 2009 Jordan Jordan
Sawalha, A. F Analysis of prescriptions dispensed at community
pharmacies in Nablus, Palestine 2010 Palestine Palestine
Sawalha, A. F Self-therapy practices among university students in
Palestine: focus on herbal remedies 2008 Palestine Palestine
Sedighi, B. Evaluation of self-medication prevalence, diagnosis and
prescription in migraine in Kerman, Iran 2006 Iran Iran
Sepehri, G The quality of prescribing in general practice in Kerman,
Iran 2005 Iran Iran
Sepehri, G The patterns of antihypertensive drug prescription by
cardiologists in Kerman province of Iran 2008 Iran Iran

184
First author Title Year Country of
origin
Country (ies) in
focus
Sepehri, G.
Pattern of drug prescription and utilization among Bam
residents during the first six months after the 2003 Bam
earthquake
2006 Iran Iran
Shabila
Iraqi health system in kurdistan region: medical
professionals’ perspectives on challenges and priorities for
improvement
2010 Iraq Iraq
Sharrad, A. K Consumer perception on generic medicines in Basrah, Iraq:
preliminary findings from a qualitative study 2011 malaysia Iraq
Siddiqi, S Prescription practices of public and private health care
providers in Attock District of Pakistan 2002 Pakistan Pakistan
Smith, F The quality of private pharmacy services in low and middle-
income countries: a systematic review 2009 UK mentions Egypt
Soleymani, F Challenges and Achievements of Promoting Rational Use of
Drugs in Iran 2009 Iran Iran
Soussi-Tanani, D Consumption analyze of the antihypertensive drugs in
Morocco: period 1991-2005 2008 Morocco Morocco
Sweileh, W. M Storage, utilization and cost of drug products in Palestinian
households 2010 Palestine Palestine
Sweileh, W. M Extent of potential drug interactions among patients
receiving anti-hypertensive medications 2005 Palestine Palestine
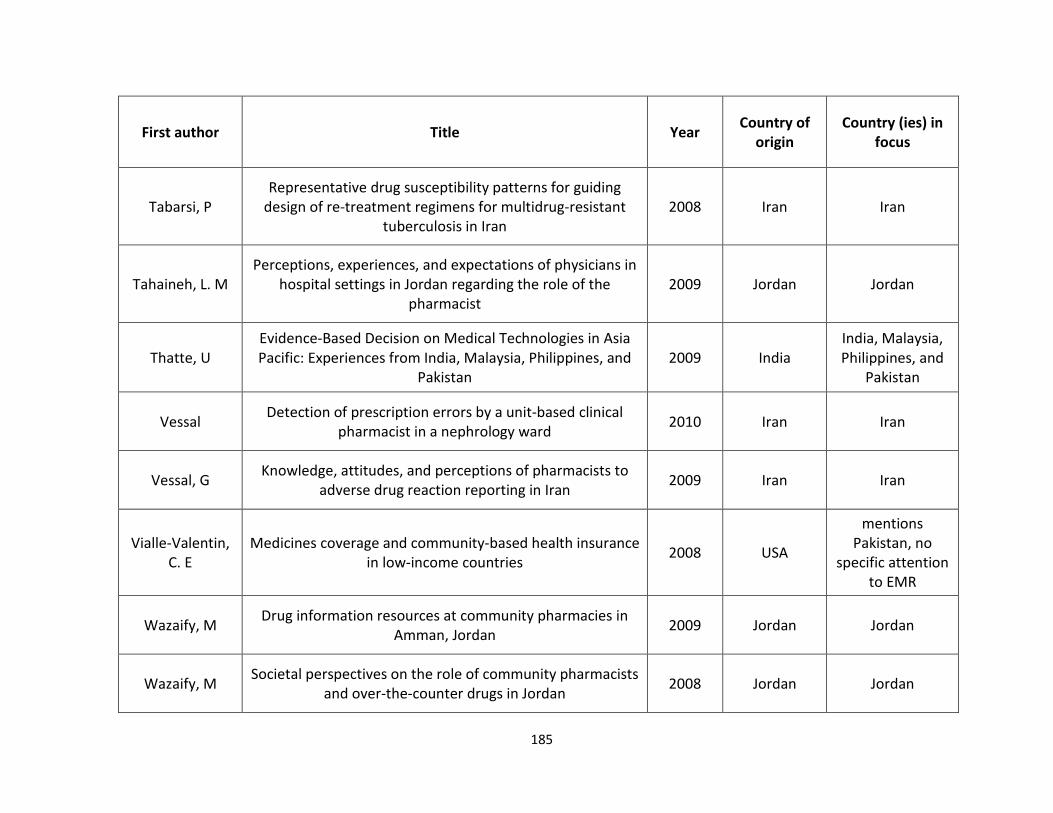
185
First author Title Year Country of
origin
Country (ies) in
focus
Tabarsi, P
Representative drug susceptibility patterns for guiding
design of re-treatment regimens for multidrug-resistant
tuberculosis in Iran
2008 Iran Iran
Tahaineh, L. M
Perceptions, experiences, and expectations of physicians in
hospital settings in Jordan regarding the role of the
pharmacist
2009 Jordan Jordan
Thatte, U
Evidence-Based Decision on Medical Technologies in Asia
Pacific: Experiences from India, Malaysia, Philippines, and
Pakistan
2009 India
India, Malaysia,
Philippines, and
Pakistan
Vessal Detection of prescription errors by a unit-based clinical
pharmacist in a nephrology ward 2010 Iran Iran
Vessal, G Knowledge, attitudes, and perceptions of pharmacists to
adverse drug reaction reporting in Iran 2009 Iran Iran
Vialle-Valentin,
C. E
Medicines coverage and community-based health insurance
in low-income countries 2008 USA
mentions
Pakistan, no
specific attention
to EMR
Wazaify, M Drug information resources at community pharmacies in
Amman, Jordan 2009 Jordan Jordan
Wazaify, M Societal perspectives on the role of community pharmacists
and over-the-counter drugs in Jordan 2008 Jordan Jordan

186
First author Title Year Country of
origin
Country (ies) in
focus
Wells, W. A Size and Usage Patterns of Private TB Drug Markets in the
High Burden Countries 2011 USA
mentions
Pakistan
WHO/HAI Medicine prices, availability, affordability and price
components 2008 Egypt
mentions Jordan,
Lebanon,
Morocco, Egypt,
Pakistan, Sudan,
Syria, Tunisia,
Yemen
Wright, K
Afghanistan: an assessment of the status of health care and
pharmacy mentoring efforts in an Afghan National Army
hospital
2003 Afghanistan Afghanistan
Yousef, A. M Self-medication patterns in Amman, Jordan 2008 Jordan Jordan
Yousif, E Deficiencies in medical prescriptions in a Sudanese hospital 2006 Sudan Sudan
Yousif, M. A In-home drug storage and utilization habits: a Sudanese
study 2002 Sudan Sudan
Yousif, M. A Investigation of medication prescribing errors in Wad
Medani, Gezira, Sudan 2011 Sudan Sudan
Zafar S. N. Prescription of medicines by medical students of Karachi,
Pakistan: a cross-sectional study
2008 Pakistan Pakistan

187
First author Title Year Country of
origin
Country (ies) in
focus
Zaid, A. N Appropriate use of oral drops: perception of health
professionals and assessment of package insert information 2010 Palestine Palestine
Zargarzadeh H Prescription and nonprescription drug use in Isfahan, Iran:
An observational, cross-sectional study 2008 Iran Iran
Zargarzadeh H Drug-related hospital admissions in a generic
pharmaceutical system
2007 Iran Iran
Zargarzadeh, A.
H
Design and test of preference for a new prescription
medication label 2011 Iran Iran

188
References: list of Journal articles – Lebanon
Author(s) Title of journal article Journal issue
Salameh P, Hamdan I.
Pharmacy manpower in Lebanon: An exploratory look at work-related satisfaction.
Res Social Adm Pharm. 2007 Sep;3(3):336-50.
Kyriacos S, Quality of amoxicillin formulations in some Arab countries.
J Clin Pharm Ther. 2008 Aug;33(4):375-9.
Araj GF, Nationwide study of drug resistance among acid-fast bacilli positive pulmonary tuberculosis cases in
Lebanon.
Int J Tuberc Lung Dis. 2006 Jan;10(1):63-7.
Araj GF, Comparative study of antituberculous drug resistance among Mycobacterium tuberculosis
isolates recovered at the American University of Beirut Medical Center: 1996-1998 vs 1994-1995.
J Med Liban. 2000 Jan-Feb;48(1):18-22.
Araj GF, Drug-resistant Streptococcus pneumoniae in the Lebanon: implications for presumptive therapy.
Int J Antimicrob Agents. 1999 Aug;12(4):349-54.
Araj GF, . Antifungal susceptibility of Candida isolates at the American University of Beirut Medical Center.
Int J Antimicrob Agents. 1998 Nov;10(4):291-6.
El Accaoui R, A review of the off-label use of recombinant activated factor VII in a developing country tertiary
care center.
Blood Coagul Fibrinolysis. 2006 Nov;17(8):647-50.
Ghosn Z.
Crackdown on pharmacies in Lebanon spurs blame game.
Nat Med. 2010 Apr;16(4):359.
Hamadeh GN, Common prescriptions in ambulatory care in Lebanon.
Ann Pharmacother. 2001 May;35(5):636-40.
Hamze MM, Araj GF.
Drug resistance among Mycobacterium tuberculosis isolates in Lebanon.
Int J Tuberc Lung Dis. 1997 Aug;1(4):314-8.
Kassab IA, [Setup of a national system of adverse drug reaction reporting in Lebanon: results of the first year of
activity].
Therapie. 2005 Nov-Dec;60(6):583-7.
Major S, Drug-related hospitalization at a tertiary teaching center in Lebanon: incidence, associations, and
relation to self-medicating behavior.
Clin Pharmacol Ther. 1998 Oct;64(4):450-61.
Major S. Drug related illness leading to hospitalization at the American University of Beirut-Medical Center.
J Med Liban. 1997 Dec;45(4):245

189
Makhlouf Obermeyer C,
Medication use, gender, and socio-economic status in Lebanon: analysis of a national survey.
J Med Liban. 2002 Sep-Dec;50(5-6):216-25.
Saab BR, List of essential drugs for primary care in Lebanon. J Med Liban. 2001 Sep-Oct;49(5):265-73.
Saab YB, Inappropriate medication use in elderly Lebanese outpatients: prevalence and risk factors.
Drugs Aging. 2006;23(9):743-52.
Santanam P, Prevalence of antimicrobial resistance in Haemophilus influenzae in Greece, Israel, Lebanon
and Morocco.
Eur J Clin Microbiol Infect Dis. 1990 Nov;9(11):818-20.
Solberg KE.
Lebanese turn to drugs to treat mental-health problems.
Lancet. 2008 Sep 27;372(9644):1137-8.
Abi Rizk, G, Determinants of antibiotic use and throat culture in managing pharyngitis among primary health care
physicians in Beirut.
J Med Liban. 2010 Oct-Dec;58(4):217-21.
Riachy DM, [Application of a hospital audit to the use of nebulizers: the Case of the Hôtel-Dieu de France-
Lebanon].
Rev Mal Respir. 2010 Nov;27(9):1049-54. Epub 2010 Oct 28. French.
Zgheib NK, Using Team-based Learning to Teach Clinical Pharmacology in Medical School: Student
Satisfaction and Improved Performance.
J Clin Pharmacol. 2010 Jul 29. [Epub ahead of print]
Nassar AH, Prescribing practices among Lebanese obstetricians for prenatal corticosteroids to enhance fetal lung
maturity.
Int J Gynaecol Obstet. 2009 Feb;104(2):144-5. Epub 2008 Nov 28.
El Sayed MF Prospective study on antibiotics misuse among infants with upper respiratory infections.
Eur J Pediatr. 2009 Jun;168(6):667-72. Epub 2008 Sep 2.
Sievert LL, The medical management of menopause: a four-country comparison care in urban areas.
Maturitas. 2008 Jan 20;59(1):7-21. Epub 2008 Jan 4.
Salameh P, [Drug circuit in Lebanese hospitals]. Rev Epidemiol Sante Publique. 2007 Aug;55(4):308-13.
Nassar AH, Gynecologists' attitudes towards hormone therapy in the post "Women's Health Initiative" study era.
Maturitas. 2005 Sep 16;52(1):18-25.
Kanafani ZA, Antibiotic use in acute cholecystitis: practice patterns in the absence of evidence-based
guidelines.
J Infect. 2005 Aug;51(2):128-34. Epub 2005 Jan 20.
Bizri AR
The current status of antibiotic prescribing in ambulatory care the Lebanese experience.
J Med Liban. 2002 Sep-Dec;50(5-6):211-5.

190
Naja WJ, A general population survey on patterns of benzodiazepine use and dependence in Lebanon.
Acta Psychiatr Scand. 2000 Dec;102(6):429-31.
El-Hajj Fuleihan G, First update of the Lebanese guidelines for osteoporosis assessment and treatment.
J Clin Densitom. 2008 Jul-Sep;11(3):383-96. Epub 2008 May 2.
Naccache N, . Pain management and health care policy. J Med Liban. 2008 Apr-Jun;56(2):105-11.
Azar S. A practical guideline for management of hypertension in patients with diabetes.
J Med Liban. 2000 Nov-Dec;48(6):392-5.
Fuleihan Gel-H, Lebanese guidelines for osteoporosis assessment and treatment: who to test? What measures to use?
When to treat?
J Med Liban. 2002 Sep-Dec;50(5-6):211-5.
Azzam R, Survey of antimicrobial prophylaxis for surgical procedures in Lebanese hospitals.
East Mediterr Health J. 2009 Nov-Dec;15(6):1553-63.
Bou Antoun RB, Salameh P.
[Satisfaction of pharmacists in Lebanon and the prospect for clinical pharmacy].
J Med Liban. 2006 Jan-Mar;54(1):2-8.
Salameh PR, [Clinical pharmacy in lebanon: a pilot study regarding health care professionals' opinion].
Am J Health Syst Pharm. 2004 Apr 15;61(8):794-5.
Dib JG, Saade S, Merhi F.
Pharmacy practice in Lebanon. Am J Health Syst Pharm. 1998 Sep 1;55(17):1826-7.
Scicluna E.A., Self-medication with antibiotics in the ambulatory care setting within the Euro-Mediterranean region;
results from the ARMed project
Journal of Infection and Public Health 2009 2:4 (189-197)
Araj G.F., Kanj S.S.
Current status and changing trends of antimicrobial resistance in Lebanon
Journal Medical Libanais 2000 48:4 (221-226)
Araj G.F. Antimicrobial resistance in Lebanon Enfermedades Infecciosas y Microbiologia 1999 19:4 (197-198)
Araj G.F., Antimicrobial susceptibility patterns of bacterial isolates at the American University Medical Center
in Lebanon
Diagnostic Microbiology and Infectious Disease 1994 20:3 (151-158)
Khachan V Pharmacy education in Lebanon Currents in Pharmacy Teaching and Learning Volume 2, Issue 3, July 2010, Pages 186-191
Uwaydah M Penicillin-resistant Streptococcus pneumoniae in Lebanon: the first nationwide study
International Journal of Antimicrobial Agents, Volume 27, Issue 3, March 2006, Pages 242-246
Steve Harakeh Antimicrobial-resistance of Streptococcus pneumoniae isolated from the Lebanese
environment
Marine Environmental Research Volume 62, Issue 3, September 2006, Pages 181-193. Volume 62,
Issue 3, September 2006, Pages 181-193

Pakistan references
• Azhar, S., et al.2009. The role of pharmacists in developing countries: the current scenario in Pakistan. Hum Resour Health, 7: p. 54.
• Bukhari,S.K., Jooma 1 R., Bile K.M, et al. 2010. Essential medicines management during emergencies in Pakistan. EMHJ, Vol. 16.
• Butt, Z.A., et al. 2005. Quality of pharmacies in Pakistan: a cross-sectional survey. Int J Qual
Health Care, 17(4): p. 307-13.
• Cameron, A., et al. 2009. Medicine prices, availability, and affordability in 36 developing and middle-income countries: a secondary analysis. Lancet, 373(9659): p. 240-9.
• Das, N., Khan, A. N., Badini, Z. A., Baloch, H. & Parakash, J. 2001. Prescribing practices of consultants at Karachi, Pakistan. J Pak Med Assoc, 51, 74-7.
• DAWN, 2008. Shunning injections. Accessed on May 3rd, 2011. Accessed at http://archives.dawn.com/2008/09/01/ed.htm#2
• DFID. 2002. Prescription, dispensing and storage practices in the provinces of NWFP,
Baluchistan and Punjab in collaboration with Network for Consumer Protection. EDSP Baseline Survey Report.
• Drugs Control Organization; Ministry of Health of Pakistan, Islamabad. Website available at: http://www.dcomoh.gov.pk/, Accessed on 21-06-2011
• Fikree, F.F., Mir A.M., and Haq, I.U., 2006. She may reach a facility but will still die! An analysis of quality of public sector maternal health services, District Multan, Pakistan. J Pak Med
Assoc, 56(4): p. 156-63.
• Hafeez, A., et al., 2004. Prescription and dispensing practices in public sector health facilities in Pakistan: survey report. J Pak Med Assoc,. 54(4): p. 187-91.
• Hafeez, A. and Mirza Z.,1999. Responses from pharmaceutical companies to doctors' requests for more drug information in Pakistan: postal survey. BMJ,. 319(7209): p. 547.
• Haider, S. and Thaver I.H., 1995. Self medication or self care: implication for primary health care strategies. J Pak Med Assoc, 45(11): p. 297-8.
• Imran, M., Khan, F.A., and Abbasi, S. 2009. Standards for labelling and storage of anaesthetic medications--an audit. J Pak Med Assoc, 59(12): p. 825-8.
• Jafar, T.H., et al. 2005. General practitioners' approach to hypertension in urban Pakistan: disturbing trends in practice. Circulation, 111(10): p. 1278-83.

192
• Janjua, N.Z., 2003. Injection practices and sharp waste disposal by general practitioners of Murree, Pakistan. J Pak Med Assoc, 53(3): p. 107-11.
• Janjua, N.Z., et al. 2006, Pattern of health care utilization and determinants of care-seeking from GPs in two districts of Pakistan. Southeast Asian J Trop Med Public Health,. 37(6): p. 1242-53.
• Kadir, M.M., et al., 2000. Out-of-pocket expenses borne by the users of obstetric services at government hospitals in Karachi, Pakistan. J Pak Med Assoc, 50(12): p. 412-5.
• Khan, J., et al., 2003. Tuberculosis diagnosis and treatment practices of private physicians in Karachi, Pakistan. East Mediterr Health J,. 9(4): p. 769-75.
• Khowaja, L.A., Khuwaja A.K., and Cosgrove P., Cost of diabetes care in out-patient clinics of Karachi, Pakistan. BMC Health Serv Res, 2007. 7: p. 189.
• Laing, R. 2002. Improving Access to Child Health Medicines Review and Discussion Paper
prepared for WHO Regional and Country Child Health Advisers Geneva. Accessed online at www.unmillenniumproject.org/documents/tf05atemapr18.pdf. Accessed on Feb 5th 2011.
• Leslie, T., et al., 2009. Epidemic of Plasmodium falciparum malaria involving substandard antimalarial drugs, Pakistan, 2003. Emerg Infect Dis,. 15(11): p. 1753-9.
• Loevinsohn, B., et al. 2009. Contracting-in management to strengthen publicly financed primary health services--the experience of Punjab, Pakistan. Health Policy,. 91(1): p. 17-23.
• MDG Gap Taskforce Report 2008: Delivering on the Global Partnership for Achieving he
Millennium Development Goals. United Nations, Office for Outer Space Affairs. 2008. Accessed online at www.un.org/en/development/desa/news/.../mdg-gap-2008.shtml. Accessed on April 8th 2011.
• Mendis, S., et al., 2007. The availability and affordability of selected essential medicines for chronic diseases in six low- and middle-income countries. Bull World Health Organ, 85(4): p. 279-88.
• Meyer, J. 2004. Emergency Obstetric Care: Critical Need among Populations Affected by
Conflict. Reproductive Health Response in Conflict Consortium. Accessed online at www.rhrc.org/resources/gbv/bib/index.cfm?category=prot. Accessed on March 15th 2011.
• Morris, J. and Stevens, P, 2006. Counterfeit medicines in less developed countries: Problems
and solutions, London, International Policy Network, Accessed online at http://www.fightingdiseases.org/pdf/ipn_counterfeit.pdf. Accessed on June 2nd, 2011.
• MOH.2007. National Essential Medicine List of Pakistan. Ministry of Healh. Government of Pakistan. 2007.
http://apps.who.int/medicinedocs/documents/s17119e/s17119e.pdf.Accessed on 18th February, 2011.
193
• MOH. 2010. Pharmaceutical Country Profile Pakistan. Accessed online at http://www.who.int/medicines/areas/coordination/pakistan.pdf. Accessed on March 25th 2011.
• MOH. 2011. Ministry of Health of Pakistan, Islamabad. http://202.83.164.26/wps/portal/Moh.
2011 [cited; Available from: http://202.83.164.26/wps/portal/Moh. Accessed on June 20 th 2011.
• Pharmacy Act 1967, Ministry of Health. Government of Pakistan, http://www.dcomoh.gov.pk/regulations/pharmacyact1967.php. Accessed on 18th February 2011.
• PMDC 2010. Pakistan Medical and Dental Council (Physician-Pharmaceutical Industry
Relationship Ethical Standards), Regulations 2010. Ministry of Health, Government of Pakistan
http://202.83.164.27/wps/portal/Moh/!ut/p/c0/04_SB8K8xLLM9MSSzPy8xBz9CP0os_hQN68AZ3dnIwN_Qz8DAyPXQGczU08jA29nM_2CbEdFAHXcy38!/?WCM_GLOBAL_CONTEXT=/wps/wcm/connect/MohCL/ministry/news/pharma+physician+relation+guidlines, Accessed on Feb 18th 2011.
• Najmi, M.H., et al., 1998. Prescribing practices: an overview of three teaching hospitals in Pakistan. J Pak Med Assoc, 48(3): p. 73-7.
• Nishtar, S., 2006. Pharmaceuticals--strategic considerations in health reforms in Pakistan. J Pak
Med Assoc, 56(12 Suppl 4): p. S100-11.
• Nishtar, S., 2006.The Gateway Paper--health service delivery outside of the public sector in Pakistan. J Pak Med Assoc, 56(12 Suppl 4): p. S66-77.
• Nizami, S.Q., I.A. Khan, and Z.A. Bhutta, 1996 Drug prescribing practices of general practitioners and paediatricians for childhood diarrhoea in Karachi, Pakistan. Soc Sci Med,. 42(8): p. 1133-9.
• Nishtar S. 2010. Choked pipes Oxford University Press. 2010.
• NHA. 2009. National Health Accounts for Pakistan. Federal Bureau of Statistics 2009 Islamabad. Accessed online at http://www.statpak.gov.pk/depts/fbs/publications/publications.html. Accessed on April 24 th 2011.
• NPPI. 2009. Baseline survey of key indicators in Sindh 2009. Norway-Pakistan Partnership Initiative, One UN Programme in Pakistan & MNCH & Ministry of Health, Government of Sindh.
• PMDC. PMDC Ordinance 1962. Available at
http://www.pmdc.org.pk/AboutUs/tabid/72/Default.aspx. Accessed on June 20th 2011.
• . PPHI. 2010. Third-Party Evaluation of the PPHI in Pakistan. TRF/SOSEC/ HLSP.2010

194
• PPMA. 2007. Available at http://www.ppma.org.pk/PPMAIndustry.aspx. Accessed on June 20th, 2011
• PRB. 2010. World Population Report. Population Reference Bureau. Washington DC 2010. Accessed at http://www.prb.org/Publications/Datasheets/2010/2010wpds.aspx. Accessed online on 20th June, 2011
• PSLM. 2005. Pakistan social and living standards measurement survey 2004-05 Federal
Bureau of Statistics, Islamabad. 2005. Accessed online at http://www.statpak.gov.pk/fbs/content/pakistan-social-and-living-standards-mearurement-survey-pslm-2004-05. Accessed on June 15th 2011
• PSML. 2007. Pakistan social and living standards measurement survey. Federal Bureau of
Statistics. Islamabad 2006-2007. Islamabad. Accessed online at http://www.statpak.gov.pk/fbs/content/pakistan-social-and-living-standards-measurement-survey-pslm-2005-06-national-provincial. Accessed on June 20th.
• Rabbani F, et al. 2001. Behind The Counter: Pharmacies and Dispensing Patterns of Pharmacy Attendants in Karachi. JPMA. 2001; 51 (4). 149-153.
• Rohra, D.K., et al. 2006. Critical evaluation of the claims made by pharmaceutical companies in drug promotional material in Pakistan. J Pharm Sci, 9(1): p. 50-9.
• Samad, L. 2001. SIGN Rapid Assessment Survey Northern Areas, Pakistan Accessed online at. http://www.google.com/search?sourceid=navclient&ie=UTF-8&rlz=1T4WZPA_enPK414PK416&q=Lubna+Samad+Injections+pakistan. Accessed on May 12th 2011.
• Shehzadi, R., et al. 2005.Knowledge regarding management of tuberculosis among general practitioners in northern areas of Pakistan. J Pak Med Assoc, 55(4): p. 174-6.
• Siddiqi, S., et al., 2002. Prescription practices of public and private health care providers in Attock District of Pakistan. Int J Health Plann Manage, 17(1): p. 23-40.
• Siddiqui, S., et al., 2007. Impact of antibiotic restriction on broad spectrum antibiotic usage in the ICU of a developing country. J Pak Med Assoc, 57(10): p. 484-7.
• Sturm, A.W., et al., 1997 Over-the-counter availability of antimicrobial agents, self-medication and patterns of resistance in Karachi, Pakistan. J Antimicrob Chemother,. 39(4): p. 543-7..
• WHO-EMRO. 2000. The Work of WHO in the Eastern Mediterranean Region, Annual Report of
the Regional Director, 1 January - 31 December 2000. World Health Organization, Accessed online at www.emro.who.int/rd/annualreports/2000/. Accessed on April 2nd 2011.
• WHO, 2004 a. WHO Medicines Strategy: 2004 – 2007. Countries at the Core’. Accessed online at whqlibdoc.who.int/hq/2004/WHO_EDM_2004.5.pdf.. Accessed on March 4th, 2011.

195
• WHO. 2004 b. The World Medicines Situation. World Health Organization. Accessed online at www.searo.who.int/LinkFiles/Reports_World_Medicines_Situation.pdf. Accessed on February 5th 2011.
• WHO/ Heartfile/ MOH. 2004. National Action Plan for Prevention and Control of Non-
Communicable Diseases and Health Promotion in Pakistan. A Public private partnership in
health. 2004. World Health Organization,
• WHO/HAI. 2006. Prices, availability and affordability of medicines in Pakistan. Accessed at
www.thenetwork.org.pk. Accessed on April 26th, 2011.
• WHO. 2007. Framework for Action for Strengthening Health Systems: Everybody's Business - http://www.who.int/healthsystems/topics/en/index.htm. Accessed online on Feb 3rd, 2011.
• WHO- EMRO. 2007a. Regional Health Systems Observatory- EMRO.2007.Health Systems Profile- Pakistan... WHO- EMRO. 2007. Accessed online at http://gis.emro.who.int/HealthSystemObservatory/PDF/Pakistan/Exec%20summary.pdf. Accessed on Feb 2nd, 2011.
• WHO- EMRO 2007b. Regional Office for Eastern Mediterranean Technical discussion on
Medicine prices and access to medicines in the Eastern Mediterranean Region. World Health Organization. Regional Office for the Eastern Mediterranean. Accessed online at http://www.emro.who.int/edb/media/pdf/EMRC54TECHDISC01en.pdf. Accessed on February 17th 2010.
• WHO, H.A.I. 2008. Medicine prices, availability, affordability and price components, A synthesis
report of medicine. Price surveys undertaken in selected countries of the WHO Eastern
Mediterranean Region. World Health Organization. 2008.. Accessed online at http://apps.who.int/medicinedocs/en/m/abstract/Js16180e/. Accessed online on Feb 2nd 2011.
• WHO (2009): Scaling up Research and Learning for Health Systems: Now is the Time. Accessed online at www.who.int/alliance-hpsr/alliancehpsr_task_force_report_research.pdf. Accessed on March, 4th 2011.
• WHO-EMRO, 2011. Regional Health Systems Observatory- EMRO. World Health Organization. 2011. Accessed online at gis.emro.who.int/healthsystemobservatory/main/Forms/main.aspx. Accessed online on May 2nd, 2011.
• World Bank. 2005. Sindh: Health Policy Note. World Bank., South Asia Region 2005.
• World Bank. 2007. Health and Population Policy Note for Pakistan. World Bank South Asia Region.2007.
• World Bank. 2008. Evaluation of quality of care in public sector in Sindh, Pakistan / Islamabad
Report, 2008.World Bank Islamabad. 2008.
• World Bank. 2008. Health Policy Note, Northern Areas. World Bank South Asia Region. 2008.

196
• World Bank / Rahman, F. 2008. .Building upon successful Philanthropic models in the Health Sector of Pakistan. World Bank 2008.
• World Bank. 2010. Delivering Better Health Services to Pakistan's poor. World Bank Islamabad 2010.
• World Bank. 2011. Capitalizing on the Demographic Transition: Tackling Non-communicable Diseases in South Asia, 2011. Accessed at siteresources.worldbank.org/SOUTHASIAEXT/.../NCDs_South_Asia_ .... Accessed on March 24th 2011.
• Zafar, S.N.a, et al. 2008. Self-medication amongst university students of Karachi: prevalence, knowledge and attitudes. J Pak Med Assoc, 58(4): p. 214-7.
• Zafar, S.N.b, et al. 2008. Prescription of medicines by medical students of Karachi, Pakistan: a cross-sectional study. BMC Public Health, 8: p. 162.
• Zaidi S et al. 2008. Utilization and Expenditure on Ambulatory Care for Hypertension Control Findings from Low Income Urban Population. Department of Community Health Sciences. Aga Khan University. Poster Presentation (Unpublished).
Appendices
Pharmaceutical system in Iran
A couple of valuable resources have summarized succinctly the progress in Iran's
pharmaceutical industry and sector over the last half a century, by Basmenji
(2004) and Davari et al (2011) 84-85
. Here we provide a summary of those two
papers, updated with other resources and info relevant to the issue.
Iran with a population of almost 75 million is one of the most populous counties in
the region. The share of health system from GDP is estimated at about 6 percent
(the estimates range from 5.6% to 7.4%), and Ministry of Health and Medical
Education is responsible for providing healthcare services all over the country, and

197
one of the most duties of it, is to ensure the efficacy and cost effectiveness of
health care services.
Medicines as an essential part of health care services are important and having
access to them is one of the most important duties of policy makers. Access to
medicines reflects the strengths and weaknesses of health system governance,
prioritization of equity in policymaking, and the role of primary health care in the
health system and it is closely linked with professional practice too. Regarding to
have an efficient system in ATM, some plans like implementing of rational drug
use committees, adverse drug monitoring and pharmacovigilance center, national
drug formulary committee were implemented and promoted specially in last two
decades.
Irrational drug use and self-medication continue to be a major problem in Iran.
Although national committee of rational drug use in the ministry of health and it's
branches in the 44 universities all over the country have developed some strategies
adopted from WHO for improving and promoting RUD, still there is inappropriate
drug use particularly high use of injectables, antimicrobials, and resulting issues of
polypharmacy, unnecessary expenditure, drug resistance.
The average number of drugs prescribed per patient is 3 or more in Iran and over
50% of patients are prescribed antibiotics.(FSoleymani, M Valadkhani, R Dinarvand.Challenges
and Achivements of Promoting Rational Use of Drugs in Iran.Iranian J of Public Health, Vol 38, Sppl.1, 2009,pp
166-168
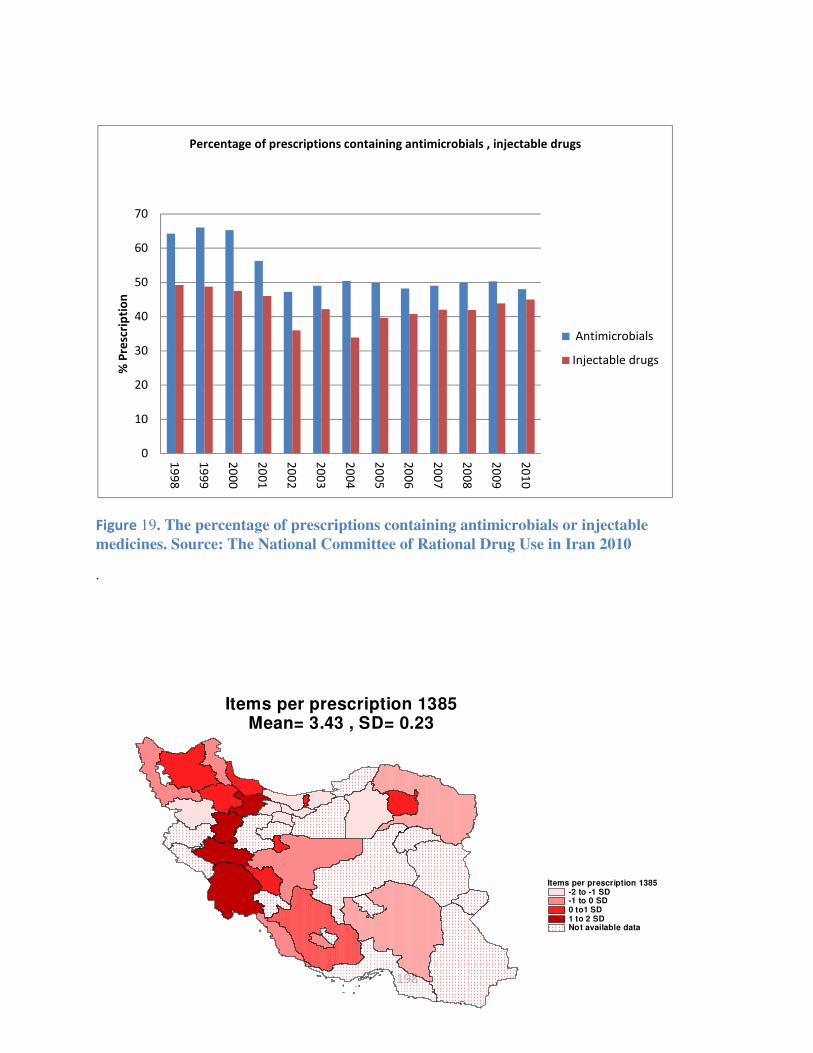
198
Figure 19. The percentage of prescriptions containing antimicrobials or injectable
medicines. Source: The National Committee of Rational Drug Use in Iran 2010
.
0
10
20
30
40
50
60
70
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
% P
resc
rip
tio
n
Percentage of prescriptions containing antimicrobials , injectable drugs
Antimicrobials
Injectable drugs
Items per prescription 1385-2 to -1 SD-1 to 0 SD0 to1 SD1 to 2 SDNot available data
Items per prescription 1385Mean= 3.43 , SD= 0.23

199
Figure 20. Items per prescription in 2006 – a provincial comparison.
Figure 21. National trend in mean items per prescription. 1998-2010
The history of medicines goes back a hundred years to the establishment of the first modern drugstores in Tehran by foreign missionaries.84 Alongside that development,
European academicians started teaching sessions on pharmacology in the Polytechnic School in Tehran
(Dar-ol-Fonoun).84 However, the real start for modern medicines in Iran goes back to the establishment of the first modern School of Pharmacy in Tehran in 193612 85. By 1946, some simple dosage forms were produced, but the first modern pharmaceutical factory was established in 1953. The first supervising law on the regulation of pharmaceuticals, foods and drinks and cosmetics was passed in 1955.(Lotfi K.Iran's drug industry in the past 80 years(part 1). Chemistry and development.2000;4:6-11) From 1964, the government encouraged foreign investment in Iran, so that many European and American pharmaceutical companies established local subsidiaries which imported the ingredients and completed final production in Iran. Forty-one pharmaceutical factories were operating in Iran by 1979, most of which were branches of the foreign companies and there were around 4000 different
12
Others have noted the date as 1934 84. Basmenji K. Pharmaceuticals in Iran: an overview. Archives of Iranian Medicine 2004;7(2):158-64.
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Mean item per prescription
Mean item per prescription

200
pharmaceutical products available on the Iranian market – 70% of which were exclusively license from foreign companies.85
) jphs_42 47
After the Islamic revolution in 1979, all the foreign owned factories were
nationalised produced medicines under generic names. (Siyamak-Nejad F. Generic scheme: a
revolution in the Iranian pharmaceutical sector. Razi. 1989; 1(2): 1–3) .The war with Iraq from 1980
onwards caused scarcity of medicines, particularly in the early years of the war.
This disruption to the supply of medicines was difficult for both patients and the
government. This was because the domestic factories were unable to meet the war
need for pharmaceuticals and the government had financial difficulties limiting
importation of foreign products. Patients were faced therefore with a limited range
and unreliable supply of pharmaceuticals. In response, the idea of a ' Generic
Scheme' came about in late 1980. The elements of this scheme were government
support for domestic manufacture, a national list of essential drugs, a commitment
to promote equity of access to good quality essential drugs at a reasonable and
regulated price, and the manufacture and prescribing of all drugs by international
non-proprietary names (INN).85s_42
Since the end of the war with Iraq in 1988, the pharmaceutical industries were able
to meet 86% of demand and eight new pharmaceutical companies had been
established.(Montaseri A, Bahaane-ye B. Gozareshe Saazmaan-e Behdaasht-eJahaani [In the reason of the
Report of theWorld Health Organization].Daaroo wa Darman [Drugs and Therapeutics] 1986; 3:
3–4.) , and the share was increased to 95% of the pharmaceutical market in the 2008
year. (Food and Drug Department. Iranian Drugs Statistics Letter [CD].2009.Tehran: Chemi Darou Co.)
The state was the main owner of the pharmaceutical factories and its first priorities
in the early years of the Generic Scheme were to simply ensure availability of
commonly used drugs. Government management of the industry was heavy
handed; every single activity in pharmaceutical factories needed to get the
agreement from the government: purchasing raw materials, pricing, marketing, etc.
On the positive side, factories had access to subsidized foreign currency to allow
them to import raw materials, machinery parts and other relevant materials based
on their capability and share of the production. This helped keep the price of the
medicines low and stable.852
201
Another important reform was establishing a centralized national distribution
system, in which six state-owned firms wholly administrated the country's
centralized medicines distribution. This and the low prices enhanced access to
essential medicines across the country significantly. (Montaseri A, Bahaane-ye B. Gozareshe
Saazmaan-e Behdaasht-eJahaani [In the reason of the Report of theWorld Health Organization].Daaroo wa Darman
[Drugs and Therapeutics] 1986; 3:3–4.)
In the beginning of 1990s, the pharmaceutical system faced new challenges to
those of the 1980s. From the consumers' perspective, there was poor availability of
some newer imported drugs, rarely access to more than a limited range of drugs,
and even poor packaging of the domestic product which undermined patients trust
in its quality. From the industry perspective, the lack of market competition and
guaranteed price regardless of quality led to unfair profit, and the bureaucratic
barriers were major disincentives to innovation and change hindering development
and growth.
From 1989, as a part of broader economic and social development programme in
Iran, some market-oriented reforms were started in the pharmaceutical industries.
The first was to transfer the state owned pharmaceutical industries to the private
and semi-private sectors, which started from 1989 and was completed by 1994.
The government started to reduce the supply of subsidized currency to the factories
from 1989 and introduced a new pricing system, allowing gradual increases in
prices to reflect true production costs. Importation regulations were eased, and it
fell to factories rather than the government to ensure quality and price of raw
materials. Factories were allowed to use brand names for their products, and
previous central controls on production were removed; industry was encouraged to
export surpluses.
In this period, the government faced greater demand for foreign and new medicines
from both the population and physicians. As a response to this pressure, import and
export regulations became much freer than before, with import licences easily
obtained even for drugs already manufactured in Iran. This led to a wider
availability of drugs and a competitive market, such that formal rationing of drugs
was no longer considered necessary and therefore ceased.85

202
Mainly from Davari et al:85
The first modem School of Pharmacy in Iran was established in Tehran in 1936,
and then later also in Tabriz in 1949 and Esfahan in 1956. Production of some
simple dosage forms was under way by 1946, but the first modern pharmaceutical
factory was not established until 1953.13 The first law regulating pharmaceuticals,
foods and drinks was passed in 1955. From 1964, the government encouraged
foreign investment in Iran, so that many European and American pharmaceutical
companies established local subsidiaries which imported the ingredients and
completed final production in Iran. Cheap labour and the large and expanding
market made such investment attractive, and these foreign companies were also
allowed to import their other non pharmaceutical products for industrial or
domestic use, e.g. washing powder. Forty-one pharmaceutical factories were
operating in Iran by 1979, most of which were branches of the foreign companies
and there were around 4000 different pharmaceutical products available on the
Iranian market – 70% of which were exclusively license from foreign companies.
There was no regulation of the extensive promotional activities of companies or of
prescribing. The lack of an effective national systematic distribution for
pharmaceutical products caused problems with inequality of access across the
country.
After the Islamic revolution in 1979, all the foreign owned factories were
nationalised. They continued production but now produced medicines under
generic rather than branded names. The war with Iraq from 1980 onwards caused
13
Others have argued the fist modern factory was built three years later in 1335 Iranian calendar (i.e. 1956)

203
scarcity of medicines, particularly in the early years of the war. This disruption to
the supply of medicines was difficult for both patients and the government. This
was because the domestic factories were unable to meet the war need for
pharmaceuticals and the government had financial difficulties limiting importation
of foreign products. Patients were faced therefore with a limited range and
unreliable supply of pharmaceuticals. In response, the idea of a ' Generic Scheme'
came about in late 1980. The elements of this scheme were government support for
domestic manufacture, a national list of essential drugs, a commitment to promote
equity of access to good quality essential drugs at a reasonable and regulated price,
and the manufacture and prescribing of all drugs by international non-proprietary
names (INN). Some drugs not manufactured in Iran were designated by the Iranian
Food and Drug Department as essential and could be only imported by two state
owned companies, and prescribed by brand name. These rationalisation measures
reduced the numbers of drug available (only around 1000 of the previously
available drugs were included in the Iranian Drugs List – the other 3000 drugs
were considered ' me-too' drugs, or simple duplication, and unnecessary) while
increasing supply and often dramatically reducing the price; e.g. the price of a
Mebendazole tablet decreased to one-eleventh of its previous level.
The young pharmaceutical industry struggled at first to meet these expectations,
but by 1988 it was able to meet 86% of demand and eight new pharmaceutical
companies had been established. By early 2008, this share increased to 95% of the
pharmaceutical market. However, there was a shortage of newer and more difficult
to manufacture drugs.

204
The state was the main owner of the pharmaceutical factories and its first priorities
in the early years of the Generic Scheme were to simply ensure availability of
commonly used drugs. Government management of the industry was heavy
handed; every single activity in pharmaceutical factories needed to get the
agreement from the government: purchasing raw materials, pricing, marketing, etc.
On the positive side, factories had access to subsidized foreign currency to allow
them to import raw materials, machinery parts and other relevant materials based
on their capability and share of the production. This helped keep the price of the
medicines low and stable.
Another important reform was establishing a centralized national distribution
system, in which six delivery companies delivered the pharmaceutical products to
all pharmacies across the country. This and the low prices enhanced access to
essential medicines across the country significantly.
In the beginning of 1990s, the pharmaceutical system faced new challenges to
those of the 1980s. From the consumers' perspective, there was poor availability of
some newer imported drugs, rarely access to more than a limited range of drugs,
and even poor packaging of the domestic product which undermined patients trust
in its quality. From the industry perspective, the lack of market competition and
guaranteed price regardless of quality led to unfair profit, and the bureaucratic
barriers were major disincentives to innovation and change hindering development
and growth.

205
From 1989, as a part of broader economic and social development programme in
Iran, some market-oriented reforms were started in the pharmaceutical industries.
The first was to transfer the state owned pharmaceutical industries to the private
and semi-private sectors, which started from 1989 and was completed by 1994.
The government started to reduce the supply of subsidized currency to the factories
from 1989 and introduced a new pricing system, allowing gradual increases in
prices to reflect true production costs. Importation regulations were eased, and it
fell to factories rather than the government to ensure quality and price of raw
materials. Factories were allowed to use brand names for their products, and
previous central controls on production were removed; industry was encouraged to
export surpluses.
In this period, the government faced greater demand for foreign and new medicines
from both the population and physicians. As a response to this pressure, import and
export regulations became much freer than before, with import licences easily
obtained even for drugs already manufactured in Iran. This led to a wider
availability of drugs and a competitive market, such that formal rationing of drugs
was no longer considered necessary and therefore ceased.
So, after more than 29 years of implementation of the Generic Drug Scheme in
Iran, and despite its major achievements, drug policy makers in Iran are moving
towards a freer competitive market with brand name prescribing and looser
pricing.

206
Figure 22. The first pharmacy established in Birjand in 1933, eastern Iran. The pharmacy is still
active. Photo © Arash Rashidian, 2010.

207
Pakistan country profile
Pakistan is situated in the North-Western part of South Asia, with about 185 million people and annual population growth rate is 1.9%. It is bordered by China on the northeast side, India on the eastern side, Iran and Afghanistan on the western side and the Arabian Sea on its south. The GNP per capita is $1200 and 1% is spent on health.
Life expectancy in Pakistan is 63 for males and 65 for females. Maternal mortality ratio is 276, infant mortality rate is 74 and under five mortality rate is 98 (PDHS 2006-07). Total fertility rate in Pakistan is 4.1, 3.3 in urban and 4.5% in rural areas and CPR is 30%, whereas unmet need of contraception is 25%. (PDHS 2006-7). At the same time Non Communicable Disease burden in Pakistan is also high and accounts for 59% of the forgone DALYs while the remaining 41% disease burden is due to communicable diseases and maternal, child care and nutritional issues (World Bank 2011). In recent years natural disasters have also had a detrimental effect on health status. 75,000 people died in the 2005 earthquake and 1,810 in the 2010 floods but asides from fatality these disasters resulted in widespread communicable diseases and destroyed the health care infrastructure and peoples’ livelihoods in affected areas. Health care provision in Pakistan comprises private and public services. Although the public sector has a well developed infrastructure of primary, secondary and tertiary facilities as well as an outreach Lady Health Worker Program, public sector is under-utilized and serves 21% of the population (WHO-EMRO 2011). The private sector serving nearly 79% of the population is

208
primarily a fee for service system and covers the range of health care provision from commercial private sector, CSOs, philanthropic institutions and traditional faith healers. Under Pakistan’s constitution, health is primarily the responsibility of the provincial government, except in the federally administrated areas. Ministry of Health (MOH) at the Federal level has played the major role in developing national policies and strategies, hosts 11 vertical programs and also the Drug Control Organization. Under a recent constitutional amendment the Federal MOH along with a number of other ministries is to be devolved to the provinces in 2011 with retaining of a minimalist MOH under the Cabinet Division. Areas and functions to be devolved to provinces are as yet unclear.

209
Key informant interview rsources
Interview guide for regional experts
Identification of Priority Policy Research Questions in the area of Access to and
Use of Medicines in EMRO Countries
Introduce yourself to the interviewee. Give a summarizing statement about the project and the
purpose of the interviews. Clarify that the interview will be tape-recorded. Ask for consent to
record.
• Ask the interviewee to briefly introduce himself/herself.
1-How do you define 'access and use of medicines'? What are the different aspects of it?
2- Thinking of access and use of medicines, in your view what are the roles of issues and
aspects such as affordability to pay, insurance coverage, governmental expenditure on
drugs, drug quality, rational drug use and/or health system financing in 'access and use of
medicines'?
(note to the interviewer: you may need to ask about issues one by one.)
3- How do you think of the health system's performance in this region (i.e. EMRO
countries – especially LMICs) or your country about different aspects of access to
medicine?
4-What are the challenges in access and use of medicine at the level of health sector policy
(stewardship and governance function)?
(examples of governance issues may include: national drug lists, pricing, import or production
regulation, generic or branding policy, subsidizing, quality control, pharmaceuticals share of
total health expenditure …)
210
A. How much do we know about these topics in the region or your country? Is there enough
research evidence in the region in this field? Do you know about any published or
unpublished reports, articles or ongoing research, and which ones do you recommended as
useful research?
B. What is the priority of research for these issues? What questions remain and for what
questions more research is required?
5- Thinking of access and use of medicines, what are the challenges in your country or
other countries in the region in terms of health insurance systems or general revenue
financing in securing access to medicines?
(Including insurance coverage, decision to allocate governmental revenues, the decisions to
cover medicines, depth of coverage, entitlements, medicines' pricing …)
A. How much do we know about these topics in the region or your country? Is there
enough research evidence in the region in this field? Do you know about any published
or unpublished reports, articles or ongoing research, and which ones do you
recommended as useful research?
B. What is the priority of research for these issues? What questions remain and for what
questions more research is required?
6- What is your view about the challenges in production, procurement and supply chain for
access to medicine and what factors may improve it?
(Factors influencing public and private sectors, drug pricing, pharmacies' geographical
distribution and geographical access and use of medicines, healthcare networks, hospital
pharmacies, ..)
A. How much do we know about these topics in the region or your country? Is there enough
research evidence in the region in this field? Do you know about any published or
unpublished reports, articles or ongoing research, and which ones do you recommended as
useful research?
B. What is the priority of research for these issues? What questions remain and for what
questions more research is required?
7- Thinking of the role of other sectors in access and use of medicines, what are the
challenges at the national and international level?
211
(e.g. think of the positive or negative roles that they followings may have: ministries of finance,
commerce and industry; authorities that issue standards, medical councils or unions,
pharmaceutical societies, NGOs, patient groups, medical societies, WTO, WHO, donors in this
region or your country …)
A. How much do we know about these topics in the region or your country? Is there enough
research evidence in the region in this field? Do you know about any published or
unpublished reports, articles or ongoing research, and which ones do you recommended as
useful research?
B. What is the priority of research for these issues? What questions remain and for what
questions more research is required?
8- What do you think the factors that affect access to medicine at the individual, household
and community levels?
(e.g. demand for medicines, care-seeking behaviour, knowledge and preferences of users, beliefs,
socio-cultural constraints, financial barriers for individuals, households and communities)
A. How much do we know about these topics in the region or your country? Is there enough
research evidence in the region in this field? Do you know about any published or
unpublished reports, articles or ongoing research, and which ones do you recommended as
useful research?
B. What is the priority of research for these issues? What questions remain and for what
questions more research is required?
9- What are the barrier and challenges in access and use of medicines related to providers
(physicians, pharmacist...) behaviour?
(e.g. induced demand, rational drug use, reimbursement methods, retailing behaviour, generic
substitution policy, pharmacy revenue, OTCs, herbal medicines, drug counterfeits and fraud …)
A. How much do we know about these topics in the region or your country? Is there enough
research evidence in the region in this field? Do you know about any published or
unpublished reports, articles or ongoing research, and which ones do you recommended as
useful research?
B. What is the priority of research for these issues? What questions remain and for what
questions more research is required?
10- Is there anything else to add? Are there other research priorities you may propose?

212
Thank you.

213
Interview guide in Farsi
م ��ا� � �� :��ح����� راه
� او������ � � � �� داروه� %$وه#� در ز� �&�در (#�ر و � )'� د
� �ور�
*� � �)�+� و ����� (,�+�
��ح �2�1 ����� �0 ��ا� ����� ���* �)�ر در ا�/�ا ه�ف از ا-�ا�
(�;> �4ف و �;:� 9�2 8 داد* �� ��د. د��0* (6� ��ح ��5 �� ��34م
) �/=� � ن ��د. @? < ا�< �&� زه �� د ��� � در ا�/�ا �
� (�2* ��ت و � ن :�رت �6� و (#�ر� ا�� و زه در �'�C ز�
1�40/� �� ��د. / �E ��ح ��ا� �D* ��دار� �2 F ����ت ���G ا
� �� ��H�9ت ��1�2 �� دارو ه5/ � و � �I;H �) ���K > ''Lص �0وه
���/NOاران MK دارو ��رد ا�/4د* ا � � � *�D F و ��)�C ��دم
.�� � ��اه
(P5 ر9�� ��ا� 1�9 :�ا
� �� دارو Q �5 و از .1�&�� و ا�+د� ��رد �Q �-�2 د�I�R ��ر
ا��؟
G � ,�ا@� در • �2= �� ��=/� ��ا� ����� �0: %�T �OU=< ا)
�W+� .� �زار، ��2 � دا�R، �2ز��Z- Cا, ��، .. و X �* ا�ر* (
�T �OU=< � 2( � ��2ارد د��O در ��ال % � Q ه� ،��� �� *� ��%
.(� ا�� @ < - ا�ر* (
�G [ ا�+د� G � �2ان %�دا�� ��ا� دا .2 ���� � M��% ، رو و�ا
Gم �;�� در ^ � �� و � 2� < ��'( � F��_ � 4 � دارو و )
� �� دارو" دار�؟�&�� در ��34م "د�- �Q دارو
• ��=/� ��ا� ����� T :�0=< ا) *� ��% �bزم ��د ا-Fا� ,�ق -�ا0
���.(
3. 8(��/NOار� در �دارو�� ��ا� � c/5 (��2 � و �(� �) (;ن
� ه� D �Q& �� دارو �)�ح �(#�ر �Q ��اC و � �5�&�6� -�3 د
� �� �N0ار�، �eز واردات (�Rd ورود �� ,�3�� دارو��، I ��؟ �
�c3 دارو از ،�Gرت ( 4 ،�� ��2 �، ��ح ژ��f، �2ز�C �را
(... ��;� � ���ت �Fه
ان ا��؟ ��� •�� � دردر ا�� ز��� دا�� روز ���ط ���ر � ا� از� ��&% $#وه� ! � ا��؟ در ��� ار�
��پ ��0/.�ت ��پ ! � ، و �� ت، �*�( ه� ��� )ارش

214
و�2د دارد � �5 در ��12ن و �� در �4ل ا12ا�%�� � �% ��� ؟�6�� �ن ��!� و � ام را
ز��� ؟� � ا� > ا;�م $#وه� در �4ل 1:�4او/���89 •� ��ا?��% ��<% ��� � و ا��؟ ه�> $#وه�% ���= ���ز�
��ع $#وه�%��8 ���= �% ��ا�� �@� ��!� ؟�
4. R�H f� ان� H �� (#�ر �م � �� اG� �� دارو ، �&�در ز� � د
رو��؟ �6� رو��2N0 � hار در Gم �;�� � Q �Q�#3 و �5
(... �/� I M��% انF � ،�ا �� � M��% �� c ��2)
ان ا��؟ ��� •�� � در در ا�� ز��� دا�� روز ���ط ���ر � ا� از� ��&% $#وه� ! � ا��؟ در ��� ار�
��پ ��0/.�ت ��پ ! � ، و �� ت، �*�( ه� ��� )ارشو�2د دارد � �5 در ��12ن و �� در �4ل ا12ا�%�� �
�% ��� ؟�6�� �ن ��!� و � ام را
ز��� ؟� � ا� �ل 1:�4> ا;�م $#وه� در 4او/���89 •� ��ا?��% ��<% ��� � و ه�> $#وه�% ���= ���ز ا��؟�
��ع $#وه�%��8 ���= �% ��ا�� �@� ��!� ؟�
� ,�ا� � ��2 � و �2ز�C دارو در (#�ر در .5�&���اC ����ط �� د
5� �Q �5 و Q� � � �)�ح ��j�, >در ا� ��&�6� ��ا� ��Dد د
� و ��(� �� �؟:��� MK �� ارN0� h2 Rا��H) �� I ،�ه� دو�/
دارو، �2ز��Z- Cا, �� دارو��، ��=� �Dا�� و در�ن، داروه�
�U5 f2 ،�/� ا� ...)� �ر
ان ا��؟ ��� •�� � در در ا�� ز��� دا�� روز ���ط ���ر � ا� از� ��&% $#وه� ! � ا��؟ در ��� ار�
��پ ��0/.�ت ��پ ! � ، و �� ت�(، �* ه� ��� )ارشو�2د دارد � �5 در ��12ن و �� در �4ل ا12ا�%�� �
�% ��� ؟�6�� �ن ��!� و � ام را
ز��� ؟� � ا� > ا;�م $#وه� در �4ل 1:�4او/���89 •� ��ا?��% ��<% ��� � و ه�> $#وه�% ���= ���ز ا��؟�
��!� ؟ ��ع $#وه�%��8 ���= �% ��ا�� �@� �
6. MK �Oد� �� *O�;��، ه� ���h �� در (�� �� دارو در �&��ح د
��6 3#�Q �Q � �66kو و � < ارو���5 �'M رو ا��؟�6)
�ارد، Gم /��، وزارت اI/�د، اوزارت : �C، وزارت �زر0
�، اl�< ه� دارو�ز� و دارو�زان، �ز�ن=�F%دم�� �د، هm

215
>�lا>�lران، ا� � �نهز�� ،���n ��6H �ه �66k< ا � �ه
� �WTO وWHO(
ان ا��؟ ��� •�� � در در ا�� ز��� دا�� روز ���ط ���ر � ا� از� ��&% $#وه� ! � ا��؟ در ��� ار�
��پ ��0/.�ت ��پ ! � ، و �� ت، �*�( ه� ��� )ارشو�2د دارد � �5 در ��12ن و �� در �4ل ا12ا�%�� �
�% ��� ؟�6�� �ن ��!� و � ام را
ز��� ؟� � ا� > ا;�م $#وه� در �4ل 1:�4او/���89 •� ��ا?��% ��<% ��� � و ه�> $#وه�% ���= ���ز ا��؟�
��ع $#وه�%��8 ���= �% ��ا�� �@� ��!� ؟�
7. Q5� �� �� ��&��ار R و �#=;2� در ار�2ط � د� 8(�دارو در
�؟�� �(,�ه o 2'9 و ���ف ���ت �;�� و دارو، 0jه� �)�ح �
��، ��د در����H(�2ان %�دا�� ،
ان ا��؟ ��� •�� � در در ا�� ز��� دا�� روز ���ط ���ر � ا� از� ��&% $#وه� ! � ا��؟ در ��� ار�
��پ��0/.�ت ��پ ! � ، و �� ت، �*�( ه� ��� )ارشو�2د دارد � �5 در ��12ن و �� در �4ل ا12ا�%�� �
�% ��� ؟�6�� �ن ��!� و � ام را
ز��� ؟� � ا� > ا;�م $#وه� در �4ل 1:�4او/���89 •� ��ا?��% ��<% ��� � و ه�> $#وه�% ���= ���ز ا��؟�
��ع $#وه�%��8 ���= �% ��ا�� �@� ��!� ؟�
� دارو ����ط �� H�6=�د 5� �Q�R و �#=;2� در .8�&�ار�2ط � د
�0ن ���ت (%F�=ن، دارو�زان ...) �)�ح �� ���؟ ارا�� (
� دارو، روش'( � F��_ ،�-ه� %�دا�� �� ارا��(2'9� ا�'�
� و اI/�د دارو��، _��F ژ��f و دارو� ? % �U5 �0ن، )
� و 0 ه�) �ر-�، IQق دارو، دارو� ��ون �U5، داروه�/ �
ان ا��؟ ��� �� � در ���ر در ا�� ز��� دا�� روز ���ط ��� � ا� از� ��&% $#وه� ! � ا��؟ در ��� ار�
و ��پ �� � ��0/.�ت ��پ ! � ، و �� ت، �*�( ه� )ارشو�2د دارد � �5 در ��12ن �ن ��!� �� در �4ل ا12ا�%
�% ��� ؟�6�� و � ام را

216
ز��� ؟� � ا� ا;�م $#وه� در �4ل 1:�4> او/���89� ��ا?��% ��<% ��� � و ه�> $#وه�% ���= ���ز ا��؟�
��ع $#وه�%��8 ���= �% ��ا�� �@� ��!� ؟�
� �� دارو .9�&���ال و زه� %$وه#� �j در ار�2ط � ��اC د
د��O� و-�د دارد (� در ا�< ����� �< �� jن ا�ر* =�دم؟

217
Interviewee invitation letter for regional experts
Subject: interview on research priorities on access to medicines
Dear Dr ,
Hope this email finds you well.
We are conducting a regional EMRO study to identify priority research areas relevant to 'access
and use of medicines' (ATM) in the region. The study team includes Shehla Zaidi (Pakistan) and
Samer Jabbour (Lebanon) as well as other collaborators.
The study is funded by the Alliance for Health Policy and Systems Research, which is a
partnership working within the HSS cluster in WHO and is part of a global research agenda by
the Alliance. The findings of the study will influence research funding decisions for ATM
research at the Alliance as well as other agencies. As such, it is very important to ensure an
accurate picture of research priority areas is identified.
The study involves a systematic search of literature from the region, as well as qualitative
interviews with experts and key individuals.
For the interviews, we would like to invite you to spare a few minutes of your time (about 30-45
minutes). As you are a knowledgeable person on the issues and wider health system aspects of
access to medicines, it will be great if you agree with this. Your contribution will be gratefully
acknowledged in the reports.
I do hope you find this request agreeable. The interview guide is attached to this email.
For conducting the interview there are three options. I'll be happy to go along whichever you
find more convenient.
1. Telephone interview.
2. Recording your responses to the question using an electronic tape recorder and sending
us the files.
3. Written responses to the questions. This is not the ideal choice as we would like to
receive your detailed responses to the questions. Typing down responses may be time
consuming for you
I am happy to provide any further information regarding this research, which we hope will
provide useful information to researchers and policy makers in the region and worldwide, with
a new vision86
of the pharmaceutical sector as a core component of a responsive health system.
With warm regards

218
Thematic framework – in Farsi
� او������ � � � ه� %$وه#� در ز� �&�در (#�ر داروو ا�/4د* از د
� و � )'� �ور�
�� #��% c هر �4/��
ز�� ���9ع ���9ع�/NOار� . 1-1 �: (;ن
ز����� ه� ��1�2 در Gم ��;�
�s �� ارز��� H�6=�د > �Iاt 6�2 / ���� �vارا
�e و ��� ز ��2 �ز��
/ �5 �و� ا � ��2 دارو�ز
�� / دو�/:��� MK �2ان
� F)�w زدا� ��;�352 ;ت و ا�=ت Gم
(*O (� �ر�/ن، در��اد* / Gم ار-ع / � �=�F%
�3 ���� ر�F� در - �5 �و� ا��;�Gم
�/NOار� . 1-2 �: اH�ل (;ن� �)�
) ��/NOار� (;ن دارو� �NDP( � ورود �� ,�3�� دارو�
�� I�ارN0 P5Q��- labeling دارو
�eز / 2 c G وارداتf�� o ژ���� /
�Gرت ( 4 )GMP( &ل ( 4 � / ( 4 � دارو)
Gرت %x از ورود �� �زار (PMS(
F0ار��ه� و �H ��hارض ) �/���اADR(
� �)ه� دارو�) F��_ 6=�د�H �� رتGaudit – drug
utilization review( ����) ��� essentialداروه� ا
drugs( ،R��� ه� H��د� ارا�� ���� (��
�bر�، ا��ز ...)ه� دارو�� و ارا�� ار�2ط ��(�
�0ن ) Gرت �� t 6�2 در -�+�
�c3 دارو ��;� � ���ت �Fاز ه

219
�� و دو�/:��� MK ;ت�2+ Gم � �� ا� ��� M��% �
��;� (#�ر���ت > �2��;�Gم ���
��;�� ���ت O@ M��% انF �)universal coverage(
�/�z M��% /�ا �� � M��% �� c ��2 M��% م ��رد;Iا
�/� I M��% انF � � �F%�ه �ه �ر� � �و�$* ��ا M��%–
�0و* ه� ه�ف� �2ز�C �را
'M �2ز�C دارو در (#�ر �:��� MK M'�)��� / ��� دو�/� ه� دو�/
دارو�� ه – ,�ا@� در �زار�زار � * –�2ز�X C � ر}� (�Zز* ه
(... �2ز��Z- Cا, �� دارو��، ��=� �Dا�� �U5 f2 ،�/�- و در�ن، داروه� � �ر
ا� ...)'M –�2ز�C ��ون �U5 دارو� �U5 ا�
| % �U5 ���Q �2ز�C در � �ر�/ن
���ت او� � �2ز�C دارو در ��=�2 c G واردات –واردات �داروو I P6'2Qق �
C�2ز� ���Q د در5,- corruption ��وج دارو –:درات
� ��jزش د��*5 �و� ا C�2ز� C�2ز� ���Q *~� �5 �و� ا–
C�2ز� ������ ���=� ه� –Gرت و ارز� �
�5 �2H;ا� � �زار��
��Iد رEا� f�� �2ز�C ژ
�ار� 8(�,�ه o 2'9 و ���ف ���ت �;�� و و -�+� دارو
����H � 0jه� ��د در�
I �� دارو – �2ان %�دا�� c '/5� t 6�2 در -�+�
�ان –�0و* ه� ه�ف k� –ا�4ل – زن �< �رور�
>�F� �ه �ر� � � در�,� –اo ه O �#=;ت ,�ه
در�ن �0ن ���ت 2'9� ا�'�� H�6=�د ارا�� (

220
� دارو'( � F��_ – �� � /�� ��اه�
�0نه� %�دا�� �� ارا��روش ) �� و اI/�د دارو�? % �U5
��jاز دارو در در �� ��jدر M'*O � �ر�/ن / در�
�� و �)ه� دارو� ا��� _��F ژ��f و دارو� �ر-
*� –ار�2ط دارو�� و ارا�� (fee splitting
�U5 دارو� ��ون �� و 0 ه/ � داروه�
�� –�#ور* دارو� دارو�ز� �� �O و -�+�
>�F� �ه �ر� � (�� 8�� و 6#K رج� > �
�66kا C� وزارت :
� وزارت �زر0 وزارت اI/�د
�ارد �ز�ن/� ا�ز�ن �=�F% مG
اl�< ه� دارو�ز� و دارو�زان mده� ��دم�ز�ن >�lرانا� � �ه >�lا���n ��6H �ه
International NGOs SWAp WHOراه �ه� �2WTOا,'ت
Gavi Global Fund World Bank Philanthropic organizations – Bill & Melinda Gates Roll Back Malaria PEPFAR / UNAID EU / JICA / DfID / …

221
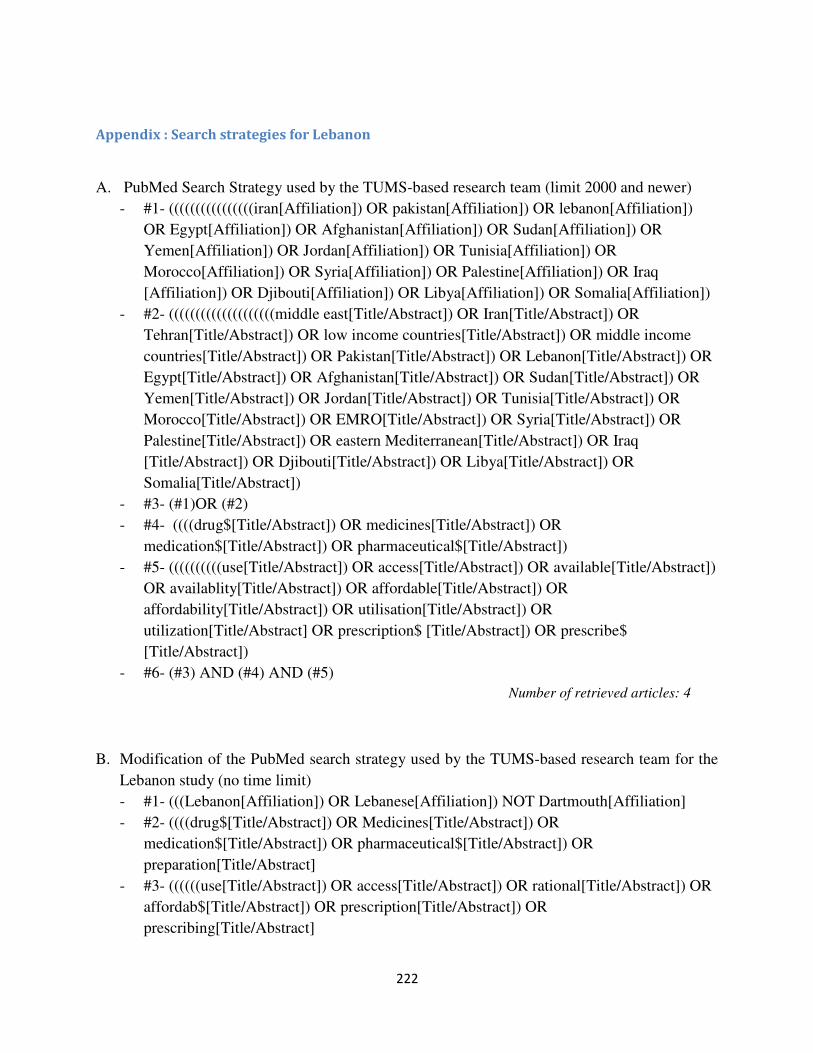
222
Appendix : Search strategies for Lebanon
A. PubMed Search Strategy used by the TUMS-based research team (limit 2000 and newer)
- #1- ((((((((((((((((iran[Affiliation]) OR pakistan[Affiliation]) OR lebanon[Affiliation])
OR Egypt[Affiliation]) OR Afghanistan[Affiliation]) OR Sudan[Affiliation]) OR
Yemen[Affiliation]) OR Jordan[Affiliation]) OR Tunisia[Affiliation]) OR
Morocco[Affiliation]) OR Syria[Affiliation]) OR Palestine[Affiliation]) OR Iraq
[Affiliation]) OR Djibouti[Affiliation]) OR Libya[Affiliation]) OR Somalia[Affiliation])
- #2- ((((((((((((((((((((middle east[Title/Abstract]) OR Iran[Title/Abstract]) OR
Tehran[Title/Abstract]) OR low income countries[Title/Abstract]) OR middle income
countries[Title/Abstract]) OR Pakistan[Title/Abstract]) OR Lebanon[Title/Abstract]) OR
Egypt[Title/Abstract]) OR Afghanistan[Title/Abstract]) OR Sudan[Title/Abstract]) OR
Yemen[Title/Abstract]) OR Jordan[Title/Abstract]) OR Tunisia[Title/Abstract]) OR
Morocco[Title/Abstract]) OR EMRO[Title/Abstract]) OR Syria[Title/Abstract]) OR
Palestine[Title/Abstract]) OR eastern Mediterranean[Title/Abstract]) OR Iraq
[Title/Abstract]) OR Djibouti[Title/Abstract]) OR Libya[Title/Abstract]) OR
Somalia[Title/Abstract])
- #3- (#1)OR (#2)
- #4- ((((drug$[Title/Abstract]) OR medicines[Title/Abstract]) OR
medication$[Title/Abstract]) OR pharmaceutical$[Title/Abstract])
- #5- ((((((((((use[Title/Abstract]) OR access[Title/Abstract]) OR available[Title/Abstract])
OR availablity[Title/Abstract]) OR affordable[Title/Abstract]) OR
affordability[Title/Abstract]) OR utilisation[Title/Abstract]) OR
utilization[Title/Abstract] OR prescription$ [Title/Abstract]) OR prescribe$
[Title/Abstract])
- #6- (#3) AND (#4) AND (#5)
Number of retrieved articles: 4
B. Modification of the PubMed search strategy used by the TUMS-based research team for the
Lebanon study (no time limit)
- #1- (((Lebanon[Affiliation]) OR Lebanese[Affiliation]) NOT Dartmouth[Affiliation]
- #2- ((((drug$[Title/Abstract]) OR Medicines[Title/Abstract]) OR
medication$[Title/Abstract]) OR pharmaceutical$[Title/Abstract]) OR
preparation[Title/Abstract]
- #3- ((((((use[Title/Abstract]) OR access[Title/Abstract]) OR rational[Title/Abstract]) OR
affordab$[Title/Abstract]) OR prescription[Title/Abstract]) OR
prescribing[Title/Abstract]
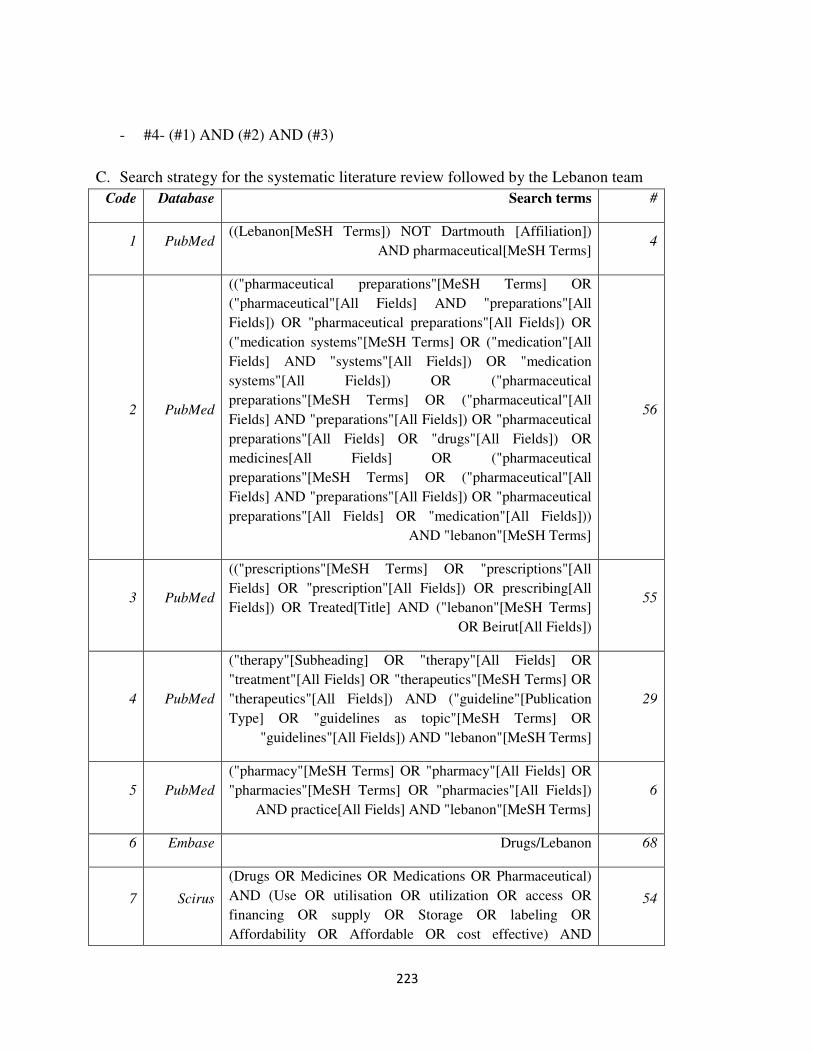
223
- #4- (#1) AND (#2) AND (#3)
C. Search strategy for the systematic literature review followed by the Lebanon team
Code Database Search terms #
1 PubMed ((Lebanon[MeSH Terms]) NOT Dartmouth [Affiliation])
AND pharmaceutical[MeSH Terms] 4
2 PubMed
(("pharmaceutical preparations"[MeSH Terms] OR
("pharmaceutical"[All Fields] AND "preparations"[All
Fields]) OR "pharmaceutical preparations"[All Fields]) OR
("medication systems"[MeSH Terms] OR ("medication"[All
Fields] AND "systems"[All Fields]) OR "medication
systems"[All Fields]) OR ("pharmaceutical
preparations"[MeSH Terms] OR ("pharmaceutical"[All
Fields] AND "preparations"[All Fields]) OR "pharmaceutical
preparations"[All Fields] OR "drugs"[All Fields]) OR
medicines[All Fields] OR ("pharmaceutical
preparations"[MeSH Terms] OR ("pharmaceutical"[All
Fields] AND "preparations"[All Fields]) OR "pharmaceutical
preparations"[All Fields] OR "medication"[All Fields]))
AND "lebanon"[MeSH Terms]
56
3 PubMed
(("prescriptions"[MeSH Terms] OR "prescriptions"[All
Fields] OR "prescription"[All Fields]) OR prescribing[All
Fields]) OR Treated[Title] AND ("lebanon"[MeSH Terms]
OR Beirut[All Fields])
55
4 PubMed
("therapy"[Subheading] OR "therapy"[All Fields] OR
"treatment"[All Fields] OR "therapeutics"[MeSH Terms] OR
"therapeutics"[All Fields]) AND ("guideline"[Publication
Type] OR "guidelines as topic"[MeSH Terms] OR
"guidelines"[All Fields]) AND "lebanon"[MeSH Terms]
29
5 PubMed
("pharmacy"[MeSH Terms] OR "pharmacy"[All Fields] OR
"pharmacies"[MeSH Terms] OR "pharmacies"[All Fields])
AND practice[All Fields] AND "lebanon"[MeSH Terms]
6
6 Embase Drugs/Lebanon 68
7 Scirus
(Drugs OR Medicines OR Medications OR Pharmaceutical)
AND (Use OR utilisation OR utilization OR access OR
financing OR supply OR Storage OR labeling OR
Affordability OR Affordable OR cost effective) AND
54
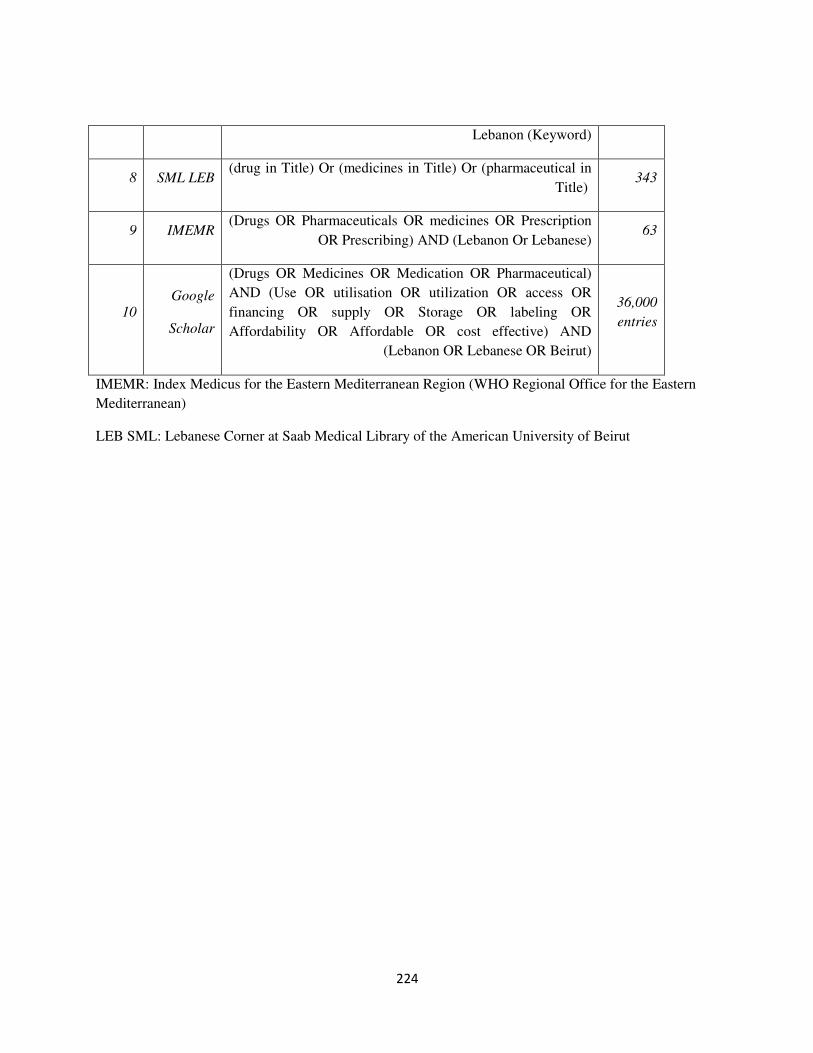
224
Lebanon (Keyword)
8 SML LEB (drug in Title) Or (medicines in Title) Or (pharmaceutical in
Title) 343
9 IMEMR (Drugs OR Pharmaceuticals OR medicines OR Prescription
OR Prescribing) AND (Lebanon Or Lebanese) 63
10
Scholar
(Drugs OR Medicines OR Medication OR Pharmaceutical)
AND (Use OR utilisation OR utilization OR access OR
financing OR supply OR Storage OR labeling OR
Affordability OR Affordable OR cost effective) AND
(Lebanon OR Lebanese OR Beirut)
36,000
entries
IMEMR: Index Medicus for the Eastern Mediterranean Region (WHO Regional Office for the Eastern
Mediterranean)
LEB SML: Lebanese Corner at Saab Medical Library of the American University of Beirut

225
Interview guide (modified after the guide provided by Dr. Arash Rashidian et al)
Introduce yourself to the informant. Give a summarizing statement about the project and the purpose of
the interviews. Clarify that the interview will be digitally-recorded and transcribed without identifying
information. Review the consent document and ask for consent prior to proceeding. Ask the informant not
to provide any identifying information during the interview.
1-How do you define 'access to medicines'? What are the different dimensions of such access?
2- In your view what are the key issues relating to access to medicines in Lebanon (if not mentioned
by the informant, the interviewer can explore issues such as affordability to pay, insurance
coverage, drug quality, rational drug use and/or health system financing in 'access to medicines')?
(note to the interviewer: you may need to ask about issues one by one.)
• If the informant seems well knowledgeable about the key issues, explore the policy concerns
and corresponding research questions under each key issue. Then use a snow-bowling
technique to explore other issues that come up in the discussion and identify relevant policy
concerns and research questions.
• If the informants seems uncomfortable with the opening questions or does not appear
knowledgeable about the issues, please to ask specific questions as below.
3-What do you think of the health system performance in Lebanon in relation to access to
medicines?
• How much do we know about this area in Lebanon? Is there enough research evidence in Lebanon in this area? Do you know about any published or unpublished reports, articles or ongoing research in this area? What questions remain and for what questions more research is required? In which areas do you think research would be most useful? What are the priorities for research in this area?
4-What are the challenges in access to medicine at the level of health sector policy (stewardship and
governance function)?
(examples of governance issues may include: national drug list, pricing, import or production regulation,
generic or brand policy, subsidizing, quality control, pharmaceuticals share of total health expenditure
…)
• How much do we know about this area in Lebanon? Is there enough research evidence in Lebanon in this area? Do you know about any published or unpublished reports, articles or ongoing research in

226
this area? What questions remain and for what questions more research is required? In which areas do you think research would be most useful? What are the priorities for research in this area?
5- What are the challenges in Lebanon's health insurance system in securing access to medicines?
(Including insurance coverage, the decisions to cover medicines, depth of coverage…)
• How much do we know about this area in Lebanon? Is there enough research evidence in Lebanon in this area? Do you know about any published or unpublished reports, articles or ongoing research in this area? What questions remain and for what questions more research is required? In which areas do you think research would be most useful? What are the priorities for research in this area?
6- What are the challenges in production, procurement and supply chain for access to medicine?
What factors may improve this system? (Factors influencing public and private sectors, drug pricing,
pharmacies' geographical distribution and geographical access to medicines, healthcare networks,
hospital pharmacies, ..)
• How much do we know about this area in Lebanon? Is there enough research evidence in Lebanon in this area? Do you know about any published or unpublished reports, articles or ongoing research in this area? What questions remain and for what questions more research is required? In which areas do you think research would be most useful? What are the priorities for research in this area?
7- Thinking of the role of other sectors in access to medicines, what are the challenges at the
national and international level? (e.g. think of the positive or negative roles that the following may
have: ministries of finance, commerce and industry; authorities that issue standards, medical councils or
unions, pharmaceutical societies, NGOs, patient groups, medical societies, WTO, WHO, donors in your
country …)
• How much do we know about this area in Lebanon? Is there enough research evidence in Lebanon in this area? Do you know about any published or unpublished reports, articles or ongoing research in this area? What questions remain and for what questions more research is required? In which areas do you think research would be most useful? What are the priorities for research in this area?
8- What do you think are the factors that affect access to medicine at the individual, household and
community levels? (e.g. demand for medicines, care-seeking behaviour, knowledge and preferences of
users, beliefs, socio-cultural constraints, financial barriers for individuals, households and communities)
• How much do we know about this area in Lebanon? Is there enough research evidence in Lebanon in this area? Do you know about any published or unpublished reports, articles or ongoing research in this area? What questions remain and for what questions more research is required? In which areas do you think research would be most useful? What are the priorities for research in this area?
9- What are the barriers and challenges in access to medicines related to provider (physicians,
pharmacist...) behaviors? (e.g. induced demand, rational drug use, reimbursement methods, retailing
behaviour, generic substitution policy, pharmacy revenue, OTCs, herbal medicines, drug counterfeits and
fraud …)

227
• How much do we know about this area in Lebanon? Is there enough research evidence in Lebanon in this area? Do you know about any published or unpublished reports, articles or ongoing research in this area? What questions remain and for what questions more research is required? In which areas do you think research would be most useful? What are the priorities for research in this area?
10- Is there anything else you would like to add? Are there other research priorities you would like
to propose?
Thank you very much for your participation in this study.

Access to Medicines list of research priority topics by the level of barriers to
ATM
Access to Medicines list of research priority topics by the level of barriers to ATM – for Iran
Topic
Frequency of
those agreeing
the topic is a
high priority
research topic
A: Health sector policy
Assessing the procedures and regulations for adding medicines to the national
drug list (formulary) and identifying improvement models 11
Evaluation of the impact of laws and regulations on controlling drug use 9
Evaluation of the effect of the 'single item importing' policy on final cost of
medicines, quality and access, and health system expenditure 9
Assessing strategies to eliminate financial links between providers and patients,
and its impact on provision of pharmaceutical services
9
Evaluation of the impact of different payment methods on quality of health care
services 9
Evaluation of drug pricing policies and its impact drug utilization and access to
medicines and health outcomes 9
Evaluation of pharmaceutical policies,regulatory function and enforcement for
traditional and herbal medicines
8
Evaluation of pharmaceutical policies and procedures, and the applications of post
marketing surveillance reports 8
Evaluation of pharmaceutical policies,regulatory function and enforcement for
drug promotion 7

229
Evaluation of the impact of pharmaceutical policies,regulatory function and
enforcement on private sector presence in the market and competitiveness of
different pharmaceutical functions 7
Evaluation of the effects of privatization of distribution system on quality and
quantity of medicines 7
Evaluation of the impact drug registration and regulations for adding medicines
to the national drug list (formulary) on drug use patterns and access to medicines 7
Evaluation of the efficacy of pharmaceutical regulatory function and
enforcement 7
Evaluation of the effect of family physicians and referral system on drug use
patterns and access to medicines 7
Identifying the effectiveness of post marketing surveillance and ADR on drug
quality 7
The impact of governments national policy of re-directing governmental subsidies
on pharmaceutical system and households' access to medicines 7
Assessing the policy of cost-plus and reference based pricing methods in the
country 7
Evaluation of the effect of generic and brand system in the country 7
Assessing the methods of using research result on decision making in
pharmaceutical sector 6
Assessing the methods for improving production and distribution of
pharmaceutical sector in the country 6
Assessing the effect of decentralization and privatization on pharmaceutical
sector on access to medicines 6
Assessing the relationship between different pricing approaches and the
pharmaceutical companies' margins of benefit 5
Identifying the methods for evaluation of the top managers in the pharmaceutical
planning and decision makers 5

230
Assessing the methods for distribution systems of human resources for the
pharmaceutical sector 5
Evaluation the effect of sanction on the quality, distribution and cost of drug
production 5
Assessing the impact of the policy of allowing the retailers and distributers to use
a certain percentage their total sale of medicines as the benefit on
pharmaceutical sector behavior 5
Improvement of pharmaceutical policies on assessing the ADR reports on
decision making in the pharmaceutical sector 5
Assessing the methods of health system financing, national health
budgets, public funding for medicines 4
The impact of mandatory 'in-house pharmacist' policy for food and cosmetic
industry on quality of industry products 3
The effect of using a specialist committee to develop a well-defined
pharmaceutical distribution system adapted to country socioeconomic and
cultural characteristics
2
Evaluation of the role of nanotechnology on pharmaceutical care system 0
B: Health system financing/insurance system
Evaluation of the process of adding medicines to the insurance organizations' list
of medicines covered 11
Evaluation of the impact of different payment methods on quality of health care
services 9
Evaluation of drug pricing policies and its impact drug utilization and access to
medicines and health outcomes 9
Evaluation of the effect of free medicine provision in SSIO14
(and charity) owned
facilities on drug usage patterns and access to medicines 9
14
Social Security Insurance Organization, a major social insurance organization in Iran
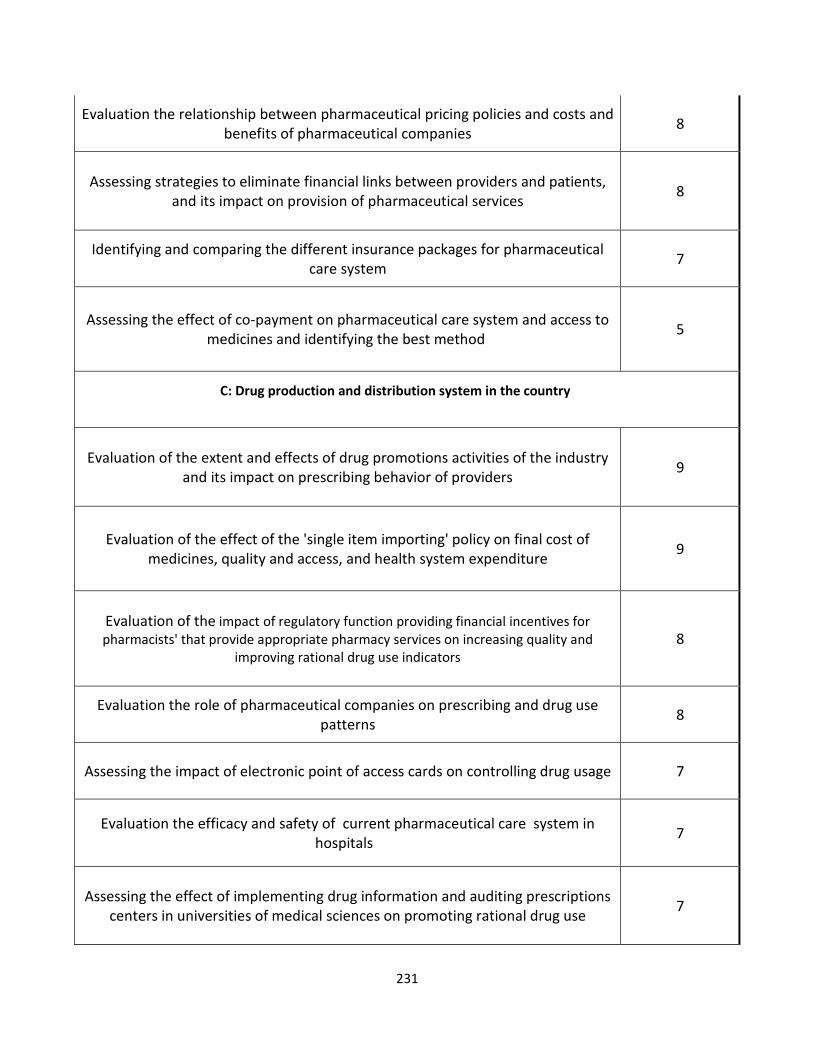
231
Evaluation the relationship between pharmaceutical pricing policies and costs and
benefits of pharmaceutical companies 8
Assessing strategies to eliminate financial links between providers and patients,
and its impact on provision of pharmaceutical services
8
Identifying and comparing the different insurance packages for pharmaceutical
care system 7
Assessing the effect of co-payment on pharmaceutical care system and access to
medicines and identifying the best method 5
C: Drug production and distribution system in the country
Evaluation of the extent and effects of drug promotions activities of the industry
and its impact on prescribing behavior of providers
9
Evaluation of the effect of the 'single item importing' policy on final cost of
medicines, quality and access, and health system expenditure 9
Evaluation of the impact of regulatory function providing financial incentives for
pharmacists' that provide appropriate pharmacy services on increasing quality and
improving rational drug use indicators 8
Evaluation the role of pharmaceutical companies on prescribing and drug use
patterns 8
Assessing the impact of electronic point of access cards on controlling drug usage 7
Evaluation the efficacy and safety of current pharmaceutical care system in
hospitals 7
Assessing the effect of implementing drug information and auditing prescriptions
centers in universities of medical sciences on promoting rational drug use 7

232
Evaluation the effect of implementing computerized system for registering the
prescriptions order on decreasing the medication errors 7
Evaluation the role of pharmacist on pharmaceutical care 7
Assessing the improvement methods for drug production and distribution in the
country 7
Evaluation the raw materials and drug registry system on quality and cost of drug
and time of access 7
Assessing and comparing the current drug distribution systems and designing a
national model adjusted to the cultural, political and socio economical
environment
6
Assessing the relation between the number of pharmacists and the quality of
pharmaceutical care in the hospitals 6
Evaluation and improving the methods of data gathering and registering in drug
production and distribution system 6
Evaluation of the effect of free medicine provision in SSIO15
(and charity) owned
facilities on drug usage patterns and access to medicines 6
The effectiveness of continuing outreach visits by health network pharmacists on
training of CHWs and their (limited) prescribing behavior 5
Evaluation of the effect of family physicians and referral system on drug use
patterns and access to medicines 5
Evaluation of health care providers ideas and problems about pharmaceutical
care system by pharmacists and pharmacies in hospitals 4
Assessing the effect of access to databases and drug information systems on
accuracy and speed of pharmaceutical care in the pharmacy 4
Identifying the methods for evaluating the managers in the drug production and
distribution system 4
15
Social Security Insurance Organization, a major social insurance organization in Iran

233
Assessing the effect of privatization on the quality and quantity of drug
distribution system 4
Assessing the methods of health system financing, national health budgets,
public funding for medicines 4
Determining the WHO drug use indicators in pharmacies for implementing
strategies to promote rational drug use 3
Identifying the relationship methods between pharmaceutical industry, pharmacy
faculties and research centers and the methods for improving them 3
Assessing the methods for human resources distribution on pharmaceutical care
system and identifying the best methods 3
Evaluation the effect of sanction on the quality, distribution and cost of drug
production 3
Evaluation of the role of nanotechnology on pharmaceutical care system 0
D: Beyond the health sector
Assessing the role of pharmaceutical companies on drug prescribing patterns 7
Assessing the role of NGO's and scientific associations on access to medicines
and drug use pattern 6
Evaluation the raw materials and drug registry system on quality and cost of drug
and time of access 6
Evaluation of the effect of free medicine provision in SSIO16
(and charity) owned
facilities on drug usage patterns and access to medicines 5
Evaluation the impact of drug promotion on drug use patterns 5
16
Social Security Insurance Organization, a major social insurance organization in Iran

234
Evaluation the effect of sanction on the quality, distribution and cost of drug
production 5
Assessing the methods and impact of relationship between pharmaceutical
companies and scientific associations 4
Identifying the relationship methods between pharmaceutical industry, pharmacy
faculties and research centers and the methods for improving them 4
Evaluation and improvement the methods of inter sector corporations 4
Assessing the effect of decentralization and privatization on ATM 4
Assessing the methods and impact of relationship between pharmaceutical
companies and patients' associations 3
Assessing the effect of privatization on the quality and quantity of drug
distribution system 2
E: Individual, household and community level
Identifying effective methods on improving public knowledge and awareness about drug
use
8
Assessing the role of medical group and patient education on improving self
medication in geriatrics 7
Assessing the observance of patient rights in pharmaceutical care sectors and
the methods for improving it 6
Assessing strategies to eliminate financial links between providers and patients,
and its impact on provision of pharmaceutical services
6
Evaluation the effect of pregnant women knowledge on drug use pattern by them
during pregnancy 5
Assessing the effectiveness of educational interventions on drug use patterns by
pregnant women 5
Assessing the impact of patient education about pharmacists' role on rational
drug use 5
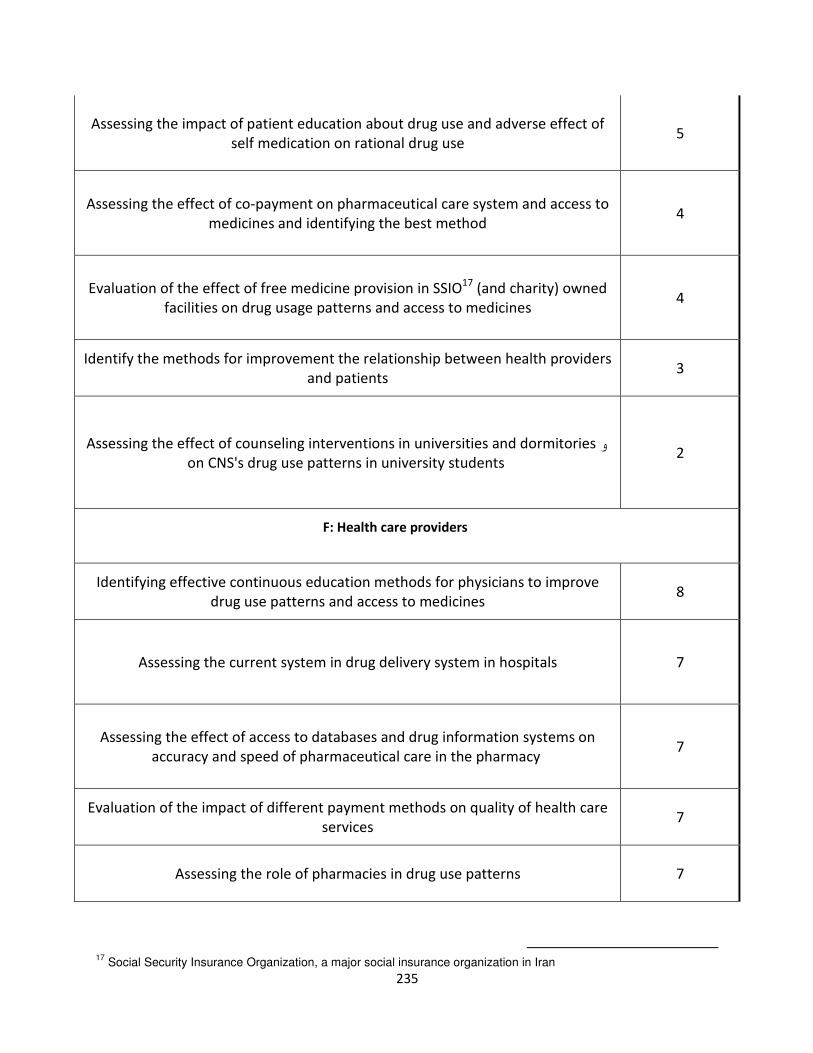
235
Assessing the impact of patient education about drug use and adverse effect of
self medication on rational drug use 5
Assessing the effect of co-payment on pharmaceutical care system and access to
medicines and identifying the best method 4
Evaluation of the effect of free medicine provision in SSIO17
(and charity) owned
facilities on drug usage patterns and access to medicines 4
Identify the methods for improvement the relationship between health providers
and patients 3
Assessing the effect of counseling interventions in universities and dormitoriesو
on CNS's drug use patterns in university students 2
F: Health care providers
Identifying effective continuous education methods for physicians to improve
drug use patterns and access to medicines 8
Assessing the current system in drug delivery system in hospitals 7
Assessing the effect of access to databases and drug information systems on
accuracy and speed of pharmaceutical care in the pharmacy 7
Evaluation of the impact of different payment methods on quality of health care
services 7
Assessing the role of pharmacies in drug use patterns 7
17
Social Security Insurance Organization, a major social insurance organization in Iran

236
Evaluation of the impact of regulatory function providing financial incentives for
pharmacists' that provide appropriate pharmacy services on increasing quality and
improving rational drug use indicators
6
Assessing strategies to eliminate financial links between providers and patients,
and its impact on provision of pharmaceutical services 6
Identifying the effectiveness of PMS and ADR on drug Quality 6
Assessing the role of medical group and patient education on improving self
medication in geriatrics 5
Evaluation of the effect of educational strategies on improving NSAIDs prescribing
patterns by general practitioners 5
Revisiting the role of pharmacists in pharmacies 5
Assessing the impact of patient education about pharmacists' role on rational
drug use 5
Identify the methods for improvement the relationship between health providers
and patients 5
Assessing the role of family physicians and referral system on ATM and drug use
patterns 5
Assessing the impact of patient education on pharmacist role in the rational drug
use process 4
Assessing the relation between drug interactions in prescriptions and
demographic factor of physicians such as gender 4

237
Determining the WHO drug use indicators in pharmacies for implementing
strategies to promote rational drug use 4
Assessing the effect of implementing drug information and auditing prescriptions
centers in universities of medical sciences on promoting rational drug use 3
Assessing the effect of access to databases and drug information systems on
accuracy and speed of pharmaceutical care in the pharmacy 3
Assessing the observance of patient rights in pharmaceutical care sectors and
the methods for improving it 3
Assessing the quality of pharmaceutical care and the methods for improvement 2ا
Evaluation of health care providers ideas and problems about pharmaceutical
care system by pharmacists and pharmacies in hospitals 1
Other topics proposed by the participants
Assessing the impact and methods of delegating hospital pharmacies to the
private sector and comparing with governmental sector
Evaluation the impact of implementing electronic prescribing system on drug
and patient safety
Assessing the approaches used for provision of expensive medicines for certain
high costs diseases on access to medicines

238
Assessing the policies and regulations for issuing permissions to establish a
pharmacy (certificate of need) on access to medicines
Assessing the current situation on counterfeit drug and fraud
Evaluation of the effect of pharmaceutical regulatory function and enforcement
on controlling counterfeit drug and fraud
Assessing the effect of biosemiolars on ATM
Evaluation the drug prescribing patterns
Evaluation of the effect of the 'single item importing' policy on drug distribution
system
Assessing the impact of relationship between pharmaceutical companies and
providers
Evaluation of the presence and impact of conflict of interest in pharmaceutical
and the other part of health sector
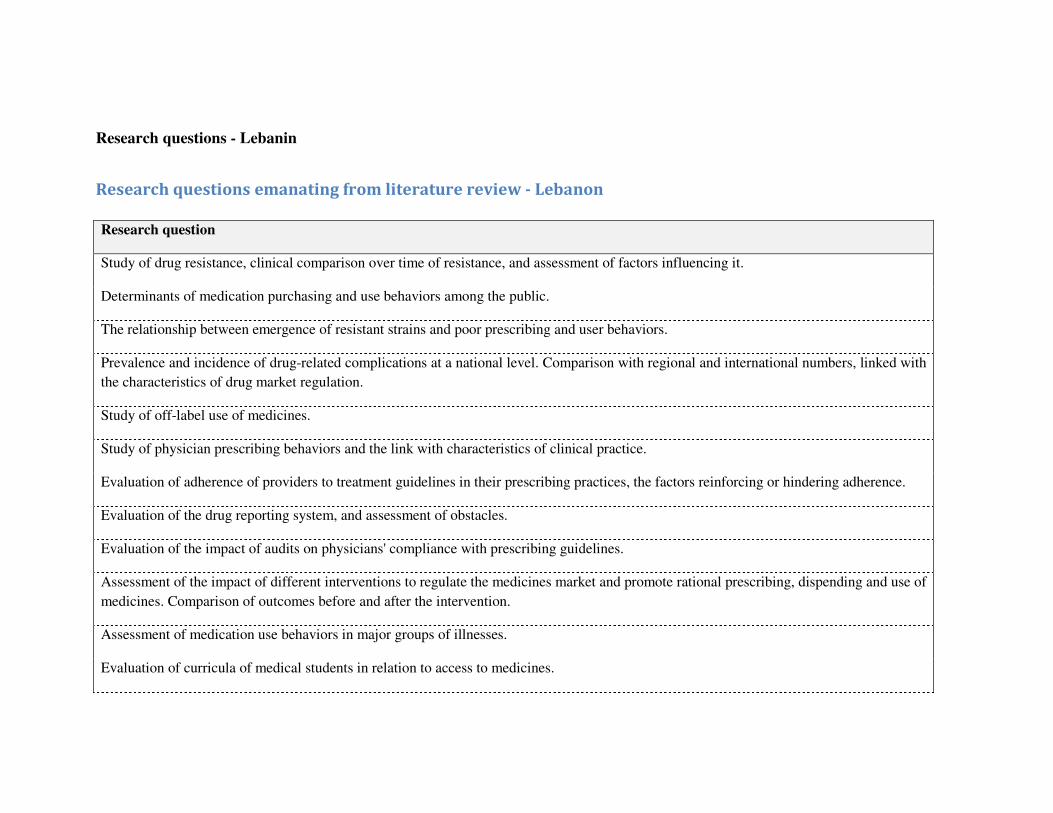
Research questions - Lebanin
Research questions emanating from literature review - Lebanon
Research question
Study of drug resistance, clinical comparison over time of resistance, and assessment of factors influencing it.
Determinants of medication purchasing and use behaviors among the public.
The relationship between emergence of resistant strains and poor prescribing and user behaviors.
Prevalence and incidence of drug-related complications at a national level. Comparison with regional and international numbers, linked with
the characteristics of drug market regulation.
Study of off-label use of medicines.
Study of physician prescribing behaviors and the link with characteristics of clinical practice.
Evaluation of adherence of providers to treatment guidelines in their prescribing practices, the factors reinforcing or hindering adherence.
Evaluation of the drug reporting system, and assessment of obstacles.
Evaluation of the impact of audits on physicians' compliance with prescribing guidelines.
Assessment of the impact of different interventions to regulate the medicines market and promote rational prescribing, dispending and use of
medicines. Comparison of outcomes before and after the intervention.
Assessment of medication use behaviors in major groups of illnesses.
Evaluation of curricula of medical students in relation to access to medicines.

240
What is the link between prescribing legislation and use patterns of psychotropic drugs and narcotics
Determinants of medicines use behaviors. How does family income influence medicines use?
Assessment of quality control of medicines in the market.
Are counterfeit drugs an important issues in the Lebanese market? Tracing the path of entry of counterfeit drugs.
Evaluation of cost effectiveness of generic vs. branded medicines
Study of prescribing behaviors and determinants of non-compliance with evidence-based guidelines
The influence of cultural factors on prescribing and use behaviors
Evaluation of regulatory laws in prescription
Comparative studies between generic and brand drugs in the goal of advertising for the use of generics and optimize cost effectiveness of
medication
Determinants of patterns of self-medication
Evaluation of guidelines in terms of cost effectiveness of different treatment strategies
Assess the perceptions of pharmacists regarding access to medicines
Assessment of population needs for medicines through epidemiologic studies
Evaluation of budget allocation for medicines and assessment of impact on ATM
Comparative studies of prices of medicines and of expenditures on medicines with other countries in the region and with countries of similar
level and level of development
Study of the processes for selection and registration of medicines, and the factors influencing these processes
In relation to the import of medicines, assess the cost-effectiveness of the import of medicines. Are the alternatives valid?
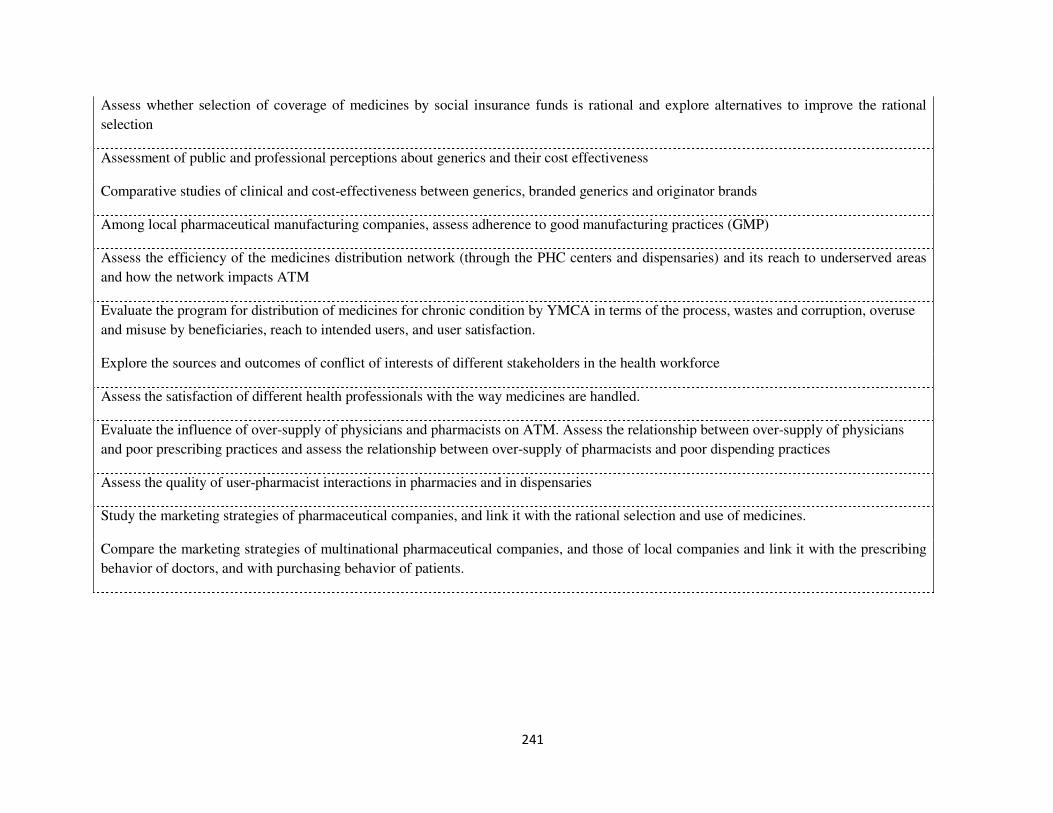
241
Assess whether selection of coverage of medicines by social insurance funds is rational and explore alternatives to improve the rational
selection
Assessment of public and professional perceptions about generics and their cost effectiveness
Comparative studies of clinical and cost-effectiveness between generics, branded generics and originator brands
Among local pharmaceutical manufacturing companies, assess adherence to good manufacturing practices (GMP)
Assess the efficiency of the medicines distribution network (through the PHC centers and dispensaries) and its reach to underserved areas
and how the network impacts ATM
Evaluate the program for distribution of medicines for chronic condition by YMCA in terms of the process, wastes and corruption, overuse
and misuse by beneficiaries, reach to intended users, and user satisfaction.
Explore the sources and outcomes of conflict of interests of different stakeholders in the health workforce
Assess the satisfaction of different health professionals with the way medicines are handled.
Evaluate the influence of over-supply of physicians and pharmacists on ATM. Assess the relationship between over-supply of physicians
and poor prescribing practices and assess the relationship between over-supply of pharmacists and poor dispending practices
Assess the quality of user-pharmacist interactions in pharmacies and in dispensaries
Study the marketing strategies of pharmaceutical companies, and link it with the rational selection and use of medicines.
Compare the marketing strategies of multinational pharmaceutical companies, and those of local companies and link it with the prescribing
behavior of doctors, and with purchasing behavior of patients.

242
Research questions emanating From key informant interviews - Lebanon
Rational Use
Explore perceptions of providers and patients about the use of generic drugs
Explore the drug seeking/purchasing behavior. Compare and contrast between different Lebanese communities, SES categories
Study the existing data to pinpoint trends of drug purchasing behavior
Assessment of Prescribing behavior of providers and its determinants
What are the factors that interplay the physicians’ prescribing behavior?
Drug purchasing behavior and its determinants and factors
Need assessment to guide rational selection
Assessment of central control of prescriptions, dispensing and promotion of medicines
Production of treatment guidelines to guide selection of drugs
Assessment of abidance to guidelines
Explore the factors influencing the misuse of Antibiotics/ antidepressants / sedatives, etc
What should a unified structured prescription form include and how it can be applied and monitored?
Cost analysis of the unified prescribing form
What are the barriers faced by NSSF to reinforce RU and how they can be overcome?
What are the possible mechanisms that can be used to control dispensing of drugs?
How can we control the aggressive marketing of drugs
explore the pharmaceutical companies marketing and its influence over access to medicines
Do doctors and hospitals follow the guidelines? And how this can be ensured?
Explore the appropriate mechanism to implementation generic substitution
Settle the standards of update the essential drug list?
Factors that affect the population’s basic drug knowledge in Lebanon?
Explore the methods of increasing providers and patients' awareness regarding drug rational use
How can international guidelines be adapted for management of diseases and prescriptions?
Explore the abidance to the code of ethics and professionalism among physicians
Why do people take medications without consulting a physician? And how this can be overcome?
Explore self-medication and factors leading to it
To what extent drug representatives stick to codes of ethics?
knowledge of doctors about law related to prescriptions?
explore barriers of doctors' knowledge and abidance by the prescription laws.
Explore the household pattern of drug usage
What are the guidelines for substitution of drugs by generics and how they can be implemented and monitored?
Assess factors influencing follow up on patients taking chronic medications?
Affordability
Study the cost effectiveness of Are generics cost effective?
How can we ensure sustainability of high quality services regarding education and drugs?
Assess processes and explore ways of improvement of medicines price control
Price analysis of imported and locally manufactured drugs, especially chronic medication.
Assess processes of better pricing tenders just like the army to help get discounts for the MOH on big drug quantities
Settle guidelines for fair pricing
Pricing studies: Price structure in origin country.
Assess transparency in pricing mechanisms
Trace the sources of price increase
Study the Lebanese drug market
Anticipate the influence of the generic drugs on the cost of essential medicines
243
Pharmaco-economic study (multidisciplinary): is the pricing good? Should have multiplicity of choice or a standard list?
Anticipate the change in the need for free or subsidized drugs and explore the ways of securing the growing need
Assessment of barriers against increase % of generics in the market?
Assess the relationship b/w the affordability/prices and the rational use of drugs?
Comparing with other countries in the regions, authentification of documents,
Assess the abidance of pharmacies by the law or regulations concerning pricing of drugs including discounts
Explore the patterns of marketing generics as trade?
Assess time trends in drug bills considering that the bill is increasing in spite of the introduction of generic drugs
Assess the relationship b/w the price of drugs and the profit of pharmacists
Anticipate the measures to be taken to increase the competition and decrease monopoly
Explore the possibility to have locally manufactured drugs to eventually decrease the prices?
Assess the benefits of the economic exchange policy with other Arab countries?
Retrieve the standards and qualifications of factories and raw materials and apply to local factories
Explore way of encouraging and improving local/national production?
Compare the compliance of insured versus non insured people to few indicator expensive drugs
What causes prices’ fluctuation? How it can be controlled?
Assess the drug bill of tertiary care and compare with international standards
Comparative prevalence of chronic diseases, recurrent expenses on health, by income
Exploration of speculation b/w Lebanese agents and the manufacturer
Assess critically governmental purchasing chronic drugs policies through YMCA with focus on protectionist policy to emphasize the local industry
Financing
Review eligibility criteria for coverage by MOH and NSSF to ensure that only people in need are covered
Assess patients' satisfaction when using reimbursed drugs from NSSF and other insurance schemes
Census of insurance and NSFF coverage in Lebanon in sight of planning better drug budget
Assess the compliance of insurance companies to cancer drugs coverage during the whole treatment period
Assess the part of donation in the drug market, and plan for measures to face the currently ongoing decreasing
donations for drugs
Compare accessibility between the army, NSSF, and MOH?
What is the most effective national insurance model and what are possible ways to implement among other
national insurance organizations?
Explore way of collaboration b/w the private and public sector, in terms of insurance
Explore possibilities of expanding NSSF to cover child vaccination, dental care and psychotherapy?
Explore the MOH coverage by eligible patients
People perception about cheaper drugs from PHC centers and dispensaries
Compare treatment cost by diseases b/w users of private versus public sectors
244
Explore the justifiability of the high budget of cancer treatment on MOH
Set quality control guidelines on the MOH expenses on cancer drugs
Assess abuse of insurances, and explore ways to avoid it.
Assess the reasons of the high OOP in Lebanon and explore ways of its reduction
Supply
What is named generic, list of generics and their category
Draft national guidelines for management of certain diseases to base the essential drug list on (to ensure cost
effectiveness)
Assess the marketing of generics, the patterns of marketing generics as trade?
What is the list of drugs that a pharmacist can prescribe without a physician’s order
Study the market of antibiotics and sedatives in sight of self-medication and lack of prescription?
Study the drug market in general,
Are pharmacists aware of the law related to prescriptions? If they are, why they do not apply it?
Explore ways of introducing and ensuring sustainability of high quality services in pharmacies regarding
education and drugs
Retrieve the standards of reliable quality-control in the national control lab?
Assessment of the quality of drugs entering Lebanon
Retrieve and adopt standards for classifying products as pharmaceuticals
Study counterfeit and non-regulated drug market
Exploring the legislations specific to registering or allowing drugs in Lebanon on possible pitfalls
Establishment of a pharmaco-vigilance system
Set mechanisms to determine appropriate quota of drugs to be allowed in Lebanon
Assess monitoring and evaluation of drug distribution in dispensaries
Establish a database of the cases covered and people using private insurances
Prioritizing exercise of the recommendations of WHO
Evaluation of the effectiveness of the WHO recommendations
Accreditation of dispensaries, and PHC centers run by NGOs
245
Evaluation of the equipment and presence of specialized doctors in dispensaries far from Beirut
Assess duplication and explore ways to avoid it (in dispensaries)
List of all drugs on the Lebanese market including donations and those distributed by dispensaries
Patients perceptions of access to dispensaries
Set standard for transportation and storage of drugs and ways of control
How can MOH monitor the chain of supply that includes pharmacists, wholesalers and importer
How can we ensure that all products including locally manufactured and imported generics and generics have
bioequivalence?
Assessment of the influence of political power and its influence over the effectiveness of the central lab work
Assessment of the registration process from the perspective of importers and companies?
Assess the effectiveness of health system when based on primary health care and explores ways of application
how can this be applied?
How to control and monitor clinical trials done on patients through agreements between doctors and drug
companies?
Assess emergency preparedness of dispensaries
What are generics supervised by original countries and subject to control lab and how they can be prioritized?
General
The status of corruption and its influence over the drug market
Assess the morbidity trends and health seeking behavior trends in Lebanon in sight of informing policy, selection,
guidelines, and eligibility criteria
What are the criteria for registering a medicine? Are they online with international standards?
The status of conflict of interests and its influence on the drug access
Explore people's voices, and their needs as they state them
Settle indicators to raise accountability in selection and delivery of medicines
Explore the mechanisms of influence of magnetic card to rationalize utilization
What is the part of each element of the framework in shaping drug accessibility?
Assess the causes of drug monopolies

246
How can we draft a national health policy without the influence of politicians
What are the economic, social, political, and sectarian determinants of access to medicine in Lebanon?
Assess the effectiveness of possible collaboration of MOH, pharmacists and NGOs with educational institutions
regarding drugs.
How continuous education of physicians can be ensured without the interference of drug companies?
How can people’s awareness on their health rights be raised?
What are the laws regarding drugs in Lebanon and what are the physicians and pharmacists views on it?

247
Research questions submitted to the validation-prioritization exercise - Lebanon
1. Is access to medicines a priority for policymakers, for professional associations, and for consumer
advocates?
2. Assessment of quality of pharmacy services at the different levels of the health system (public as well as
private pharmacies, different geographical areas).
3. Current and future projection of health needs assessment at the population level to guide rational selection
of medicines.
4. Assessment of adherence of pharmaceutical manufacturing to good manufacturing practices (GMP)
5. Evaluation of the current procedures of inspection and quality control of pharmaceutical products.
6. Assess the impact of the good governance for medicines (GGM) program on access to medicines
7. Assess the perceptions and current practices of different members of the health care team (physicians, nurses
pharmacists, community educators) in facilitating or impeding rational use of medicines at the community level.
8. Evaluate the process of registration and pricing of medicines and compare between Lebanon and other
countries in the region.
9. The equity dimension: Assessment of patterns of use and access to medicines between different
socioeconomic groups including insured vs. un-insured population groups.
10. Public and professional perceptions of ATM as part of the right to health.
11. Exploration of the political economy (e.g. influence of special interests, different power relations and
sectarian politics) of the situation of medicines and the role of corruption
12. Assessment of options for cost-savings such as through introducing a unified list of medicines (formularies)
and improving prescribing behaviors for different social insurance organizations and joint procurement of
medicines by NGOs and assess the impact on affordability.
13. The cost savings of developing a system for coding of pharmaceutical products according to international
guidelines for coding of consumer products.
14. Evaluation of the role of civil society organizations and non-governmental organizations in improving
access to medicines especially for the poor, vulnerable groups and hard-to-reach populations.
15. Evaluation of the impact of electronic health information system and electronic card on improving
efficiency, reducing potential corruption, and improving access to medicines
16. Study of consumer behaviors such as purchasing patterns, intake patterns, selection patterns, and home
storage and use of medicines
248
17. Prescribing behaviors of physicians, and adherence to international prescribing indicators, and explanatory
factors of such behaviors
18. Barriers to development of a national policy for medicines
19. Mapping the capacity of researchers and research institutions to carry out essential research on access to
medicines
20. What happens at the dispensary? Dispensing medicines or delivering primary health care? Adherence to
generics in PHC and dispensaries
21. Consumer satisfaction with medicines services at different points of service in the health system (both
public and private)
22. Price analysis and surveillance and monitoring of prices of medicines in Lebanon compared with prices in
other countries in the region.
23. A study of the lost value of medicines purchases due to various factors in the medicines supply chain (higher
than needed procurement prices, poor distribution, irrational prescribing, irrational use)
24. The patterns of use of supplements for medicinal purposes by the public and corresponding physician
prescribing
25. Sources of information for physicians and their influences on their prescribing behaviors
26. A study of attitudes of physicians and of the public towards generic substitution and the opportunities for
implementing relevant policies
27. Assess the coverage of medicines by private insurers and practices in sustaining medicines coverage in the
event of emergence of a costly disease.
28. Assess the impact of medicines donations on access to medicines and the supply system
29. Feasibility of pharmaco-vigilance studies
30. Exploring conflict of interest in both the public and private sector and its impact on access to medicines
31. Cultural factors influencing consumers’ preferences for originator brands vs. generics
32. Developing and testing a framework for physician prescribing accountability (which has three components:
scientific, ethical, and regulatory)
33. Consumers’ unmet needs due to current restrictions on access to medicines (e.g. narcotics and pain control)
34. Impact of irregularity in medicines supply (e.g. through MOPH central pharmacy, or YMCA) on adherence
to medicines and on proxy health outcomes
35. Rational selection and use of medicines in hospitals and potential for savings for smaller and medium size
hospitals from adherence to formularies

249
36. Assessment of quality of medicines on the market and role of counterfeit medicines and black market.
37. The proportion of emergency room visits and hospitalizations that results of irrational prescribing or
irrational use of medicines
38. Impact of delay in reimbursement by NSSF on ATM among NSSF beneficiaries on finances of families and
on increasing rates of hospitalization. What are the equity dimensions for such delays (among low and middle
income households)? How do NSSF beneficiaries solve their medicines needs?
39. The impact of the institutional policy framework (e.g. at the hospital level) in influencing prescribing
behaviors
40. Assessment of barriers to adoption of code of ethics for drug promotion proposed by the Ministry of Public
Health among different stakeholders.
41. The impact of developing disease management protocols (e.g. for management of hypertension) and
prescribing guidelines (which drugs to start with, which ones to add) for improving the rational use of medicines.
42. Impact of audits on physicians’ prescribing behaviors.
43. Developing and testing different incentive structures to improve physician prescribing behaviors
44. The impact of social networks (e.g. access to specialists among family and friends) on irrational use of
medicines
45. Who are the users of dispensaries and PHC network? Are they the poor and low income household? How
important are the medicines to their use of these dispensaries and PHC network?
46. Assessment of the availability and affordability of medicines in dispensaries and PHC network.
47. Challenges facing pharmaceutical manufacturing and options for reform.
48. Assessment of sustainability of access to medicines during emergencies
49. Differentials in access to medicines vs. access to health services.
50. The potential role of professional associations (physicians, pharmacists, nurses) working together to
improve rational prescribing, dispending and use.
51. The role of medical education and residency training on developing irrational prescribing behaviors.
52. Obstacles to and opportunities for empowering consumers to improve their access to medicines.
53. The impact of alternative administrative structures (e.g. a separate drug agency similar to Jordan FDA
within MOPH or independent) on improving registration, pricing and monitoring of medicines.
54. Pharmacoeconomic studies on various pharmaceuticals

250
55. Change in availability of medicines due to fluctuating currency exchange rates and the impact on adherence
to medical therapy.
56. Study of access to medicines among special populations such as those supported by the MOPH (for cancer,
HIV…), refugees, and Bedouins.
57. Reasons for professional perception of low quality of generics or low-priced branded generics

251
Research questions submitted to the ranking exercise and the results of ranking according to five
evaluative criteria - Lebanon
1= Urgency, 2= Feasibility, 3= Applicability, 4= Ethical acceptability, 5=Relevance, T=Total score
Possible score for each criterion = 0-10 (10 being most important)
Total score = the combined score from all evaluative criteria

252
Research question 1 2 3 4 5 T
Assessment of quality of medicines on the market and role of counterfeit medicines and black market. 112 63 62 88 103 340
A study of attitudes of physicians and of the public towards generic substitution and the opportunities for
implementing relevant policies 90 80 74 83 92 336
Is access to medicines a priority for policymakers, for professional associations, and for consumer advocates? 88 75 77 102 81 321
Evaluation of the role of civil society organizations and non-governmental organizations in improving access to
medicines especially for the poor, vulnerable groups and hard-to-reach populations. 92 71 76 106 82 321
What happens at the dispensary? Dispensing medicines or delivering primary health care? Adherence to generics in
PHC and dispensaries 98 70 65 87 87 320
The potential role of professional associations (physicians, pharmacists, nurses) working together to improve rational
prescribing, dispending and use. 85 87 73 97 73 318
The equity dimension: Assessment of patterns of use and access to medicines between different socioeconomic
groups including insured vs. un-insured population groups. 97 77 64 103 79 317
Prescribing behaviors of physicians, and adherence to international prescribing indicators, and explanatory factors of
such behaviors 93 65 64 85 91 313
The role of medical education and residency training on developing irrational prescribing behaviors. 91 68 65 99 84 308
Assessment of sustainability of access to medicines during emergencies 85 70 68 99 85 308
Reasons for professional perception of low quality of generics or low-priced branded generics. 95 70 68 90 74 307
Impact of delay in reimbursement by NSSF on ATM among NSSF beneficiaries on finances of families and on
increasing rates of hospitalization. What are the equity dimensions for such delays (among low and middle income 108 59 50 75 89 306

253
households)? How do NSSF beneficiaries solve their medicines needs?
Developing and testing different incentive structures to improve physician prescribing behaviors 95 61 61 76 81 298
Barriers to development of a national policy for medicines 94 63 63 87 77 297
Evaluation of the current procedures of inspection and quality control of pharmaceutical products. 87 65 58 98 84 294
The impact of developing disease management protocols (e.g. for management of hypertension) and prescribing
guidelines (which drugs to start with, which ones to add) for improving the rational use of medicines. 73 72 66 93 83 294
Impact of irregularity in medicines supply (e.g. through MOPH central pharmacy, or YMCA) on adherence to
medicines and on proxy health outcomes 75 73 63 83 72 283
Developing and testing a framework for physician prescribing accountability (which has three components:
scientific, ethical, and regulatory) 77 67 64 82 69 277
Evaluation of the impact of electronic health information system and electronic card on improving efficiency,
reducing potential corruption, and improving access to medicines 81 65 52 88 78 276
Assessment of barriers to adoption of code of ethics for drug promotion proposed by the Ministry of Public Health
among different stakeholders. 77 59 54 88 69 259
Assessment of options for cost-savings such as through introducing a unified list of medicines (formularies) and
improving prescribing behaviors for different social insurance organizations and joint procurement of medicines by
NGOs and assess the impact on affordability.
77 60 61 77 52 250
Current and future projection of health needs assessment at the population level to guide rational selection of
medicines. 67 51 47 73 84 249







