Medical roboticsDesign
J. Gangloff – B. Bayle, University of Strasbourg
Medical robotics - Design B. Bayle, University of Strasbourg
2/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion

Medical robotics - Design B. Bayle, University of Strasbourg
3/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion

Medical robotics - Design B. Bayle, University of Strasbourg
4/46
Introduction
How can robotics help surgery ?

Medical robotics - Design B. Bayle, University of Strasbourg
5/46
Introduction
How can robotics help surgery ?
Accurate positioning using preoperative or peroperative registration
Accurate path following (bone milling, skin harvesting)
Solving the hand-eye coordination problem
Real-time integration of operative data (motion compensation)
Constraining the instrument position in a safe area
Heavy tools manipulation (gamma source for radiotherapy)
Hand tremor compensation
Motion scaling (microsurgery)
Operations in hazardous environment (interventional radiology)
Long distance surgery ?
Medical robotics - Design B. Bayle, University of Strasbourg
6/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion
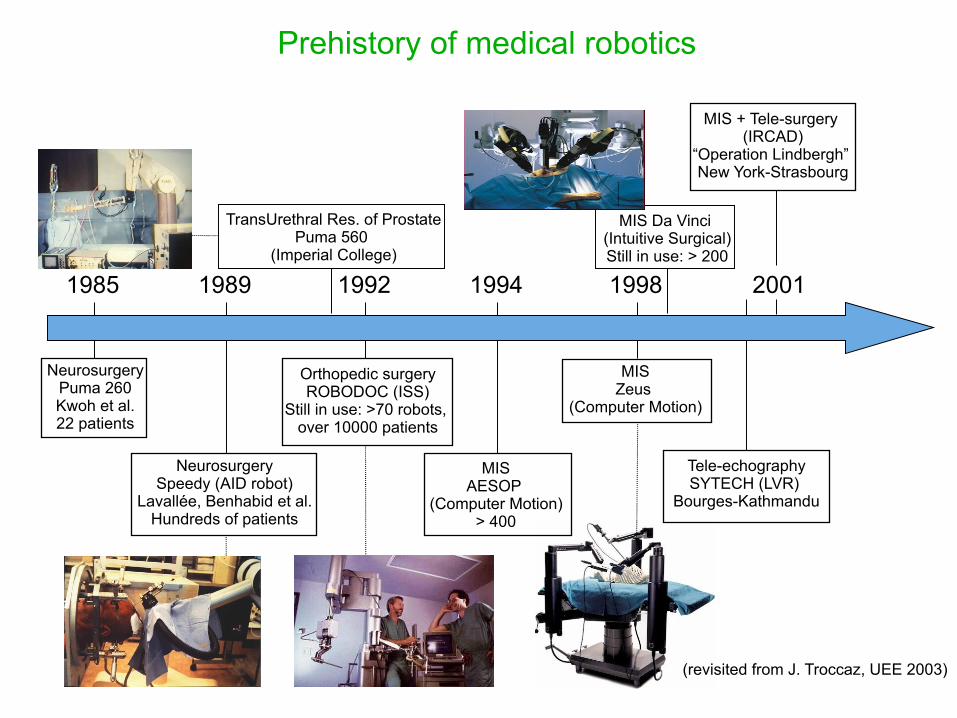
1985 1989 1992 1994 1998 2001
NeurosurgeryPuma 260Kwoh et al.22 patients
NeurosurgerySpeedy (AID robot)
Lavallée, Benhabid et al.Hundreds of patients
Orthopedic surgeryROBODOC (ISS)
Still in use: >70 robots, over 10000 patients
MISAESOP
(Computer Motion)> 400
MISZeus
(Computer Motion)
MIS + Tele-surgery (IRCAD)
“Operation Lindbergh” New York-Strasbourg
MIS Da Vinci (Intuitive Surgical)Still in use: > 200
TransUrethral Res. of Prostate Puma 560
(Imperial College)
(revisited from J. Troccaz, UEE 2003)
Tele-echographySYTECH (LVR)
Bourges-Kathmandu
Prehistory of medical robotics

Medical robotics - Design B. Bayle, University of Strasbourg
8/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion

Medical robotics - Design B. Bayle, University of Strasbourg
9/46
Medical robot design workflow
Analysis
Description of the manual procedure
Which improvements expected from the robot ?
(real benefits for the patient/surgeon/hospital/society ? If no, give up)
Can the technology state of the Art address the problem ?
Robotic design
Specifications with medical staff
Derive robotic specifications
Architecture synthesis, CAD design, 3D simulations
First prototype → surgeons corrections → next prototype ...
… Iterate until you find the best compromise
10/46
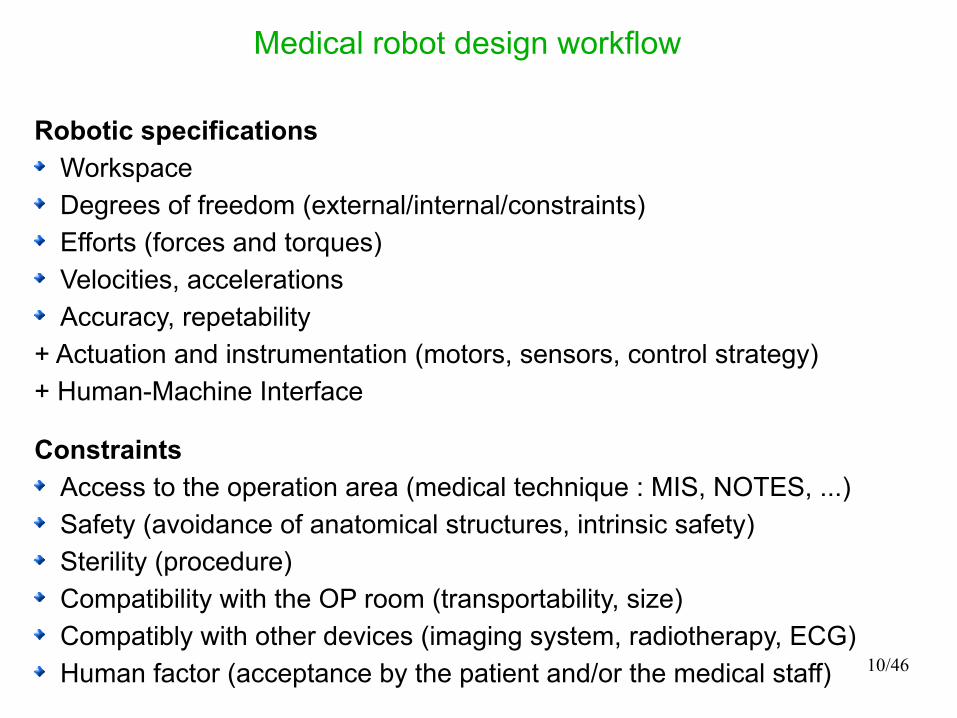
Medical robot design workflow
Robotic specifications
Workspace
Degrees of freedom (external/internal/constraints)
Efforts (forces and torques)
Velocities, accelerations
Accuracy, repetability
+ Actuation and instrumentation (motors, sensors, control strategy)
+ Human-Machine Interface
Constraints
Access to the operation area (medical technique : MIS, NOTES, ...)
Safety (avoidance of anatomical structures, intrinsic safety)
Sterility (procedure)
Compatibility with the OP room (transportability, size)
Compatibly with other devices (imaging system, radiotherapy, ECG)
Human factor (acceptance by the patient and/or the medical staff)

Medical robotics - Design B. Bayle, University of Strasbourg
11/46
Medical robot design workflow
Choices
Architecture: type synthesis (serial or parallel + joint arrangement)
Singularities
Joint limits
Actuators (DC, DC brushless, piezo, pneumatic, ...)
Sensors (absolute/incremental encoders, force sensors, acceleration sensors, visual sensors, …)
Materials (metal, biocompatible material, …)
Control strategy (robustness, predictive or repetitive control)
Human-machine interface (mouse/keyboard, touchscreen, voice recognition, gaze tracking, joysticks/haptic interface)
Medical robotics - Design B. Bayle, University of Strasbourg
12/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion

Medical robotics - Design B. Bayle, University of Strasbourg
13/46
Environmental constraints : Minimally Invasive Surgery
Widely used technique in abdominal surgery and also now in cardiac surgery
Difficulties :3 hands are necessaryMonocular visionPosition of the surgeonHand-eye coordination (fulcrum effect)No force feedback + friction at the trocartLoss of mobility due to the trocarLimited workspaceVisual field occlusionsPhysiological motionsCritical areas

Medical robotics - Design B. Bayle, University of Strasbourg
14/46
Environmental constraints : coronary artery anastomosis
Medical specificationsØ 2 mm, 10 to 20 stitching pointsØ suturing thread : 0.1 mmStitching force: up to 1NResolution: better than 0.1 mmTask : stitching + knot tying
graft
Suture of a graft on a coronary artery
Difficulties Accurate force-controlled motionSoft-tissue interactionPhysiological motionsComplex geometry of the working area+ all the difficulties linked to MIS if it is done this way

Medical robotics - Design B. Bayle, University of Strasbourg
15/46
Environmental constraints : interventional radiology
Interventional radiology Biopsy, tumor ablation,stents Image-guided needle or catheter insertion
(CT, MRI) High doses of radiation
Difficulties Mental registration of the needle position with respect to the patient anatomy, Accurate control of the insertion force during the crossing of tissues of various stiffness Physiological motion compensation Critical areas avoidance
Medical robotics - Design B. Bayle, University of Strasbourg
16/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion

҉ Robotics Basics
Actuator = motor
Axis = joint
Body = link
End effector
Base
҉ Robotics Basics
11
22
11
22
11
22
11
22
11
22
11
22 1122
11
22
11 22
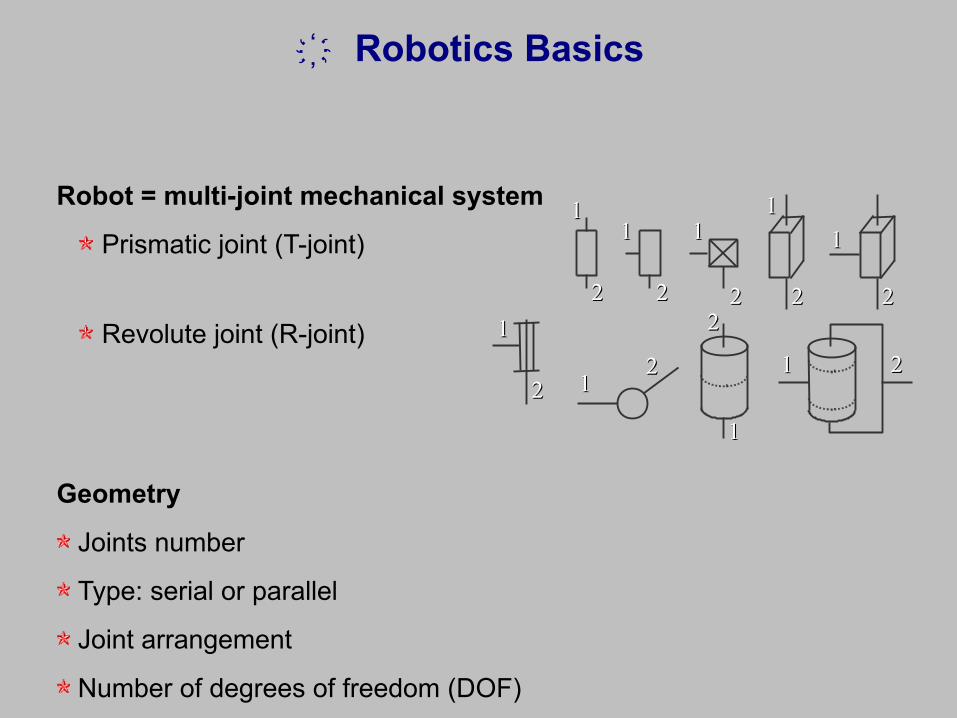
Robot = multi-joint mechanical system
Prismatic joint (T-joint)
Revolute joint (R-joint)
Geometry
Joints number
Type: serial or parallel
Joint arrangement
Number of degrees of freedom (DOF)

҉ Robotics Basics
Workspace = reachable volume for the end effector. Depend on :
Robot geometry
Links lengths
Joints limits
Medical robotics - Design B. Bayle, University of Strasbourg
20/46
Which architecture ?
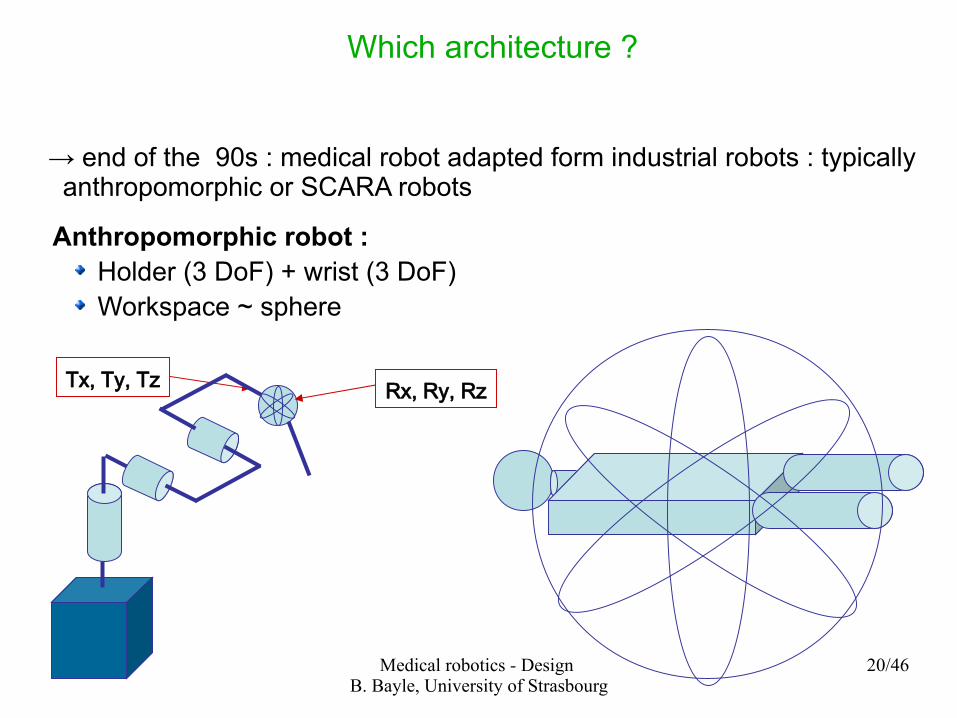
→ end of the 90s : medical robot adapted form industrial robots : typically anthropomorphic or SCARA robots
Anthropomorphic robot :Holder (3 DoF) + wrist (3 DoF)Workspace ~ sphere
Tx, Ty, Tz Rx, Ry, Rz
21/46
Which architecture ?
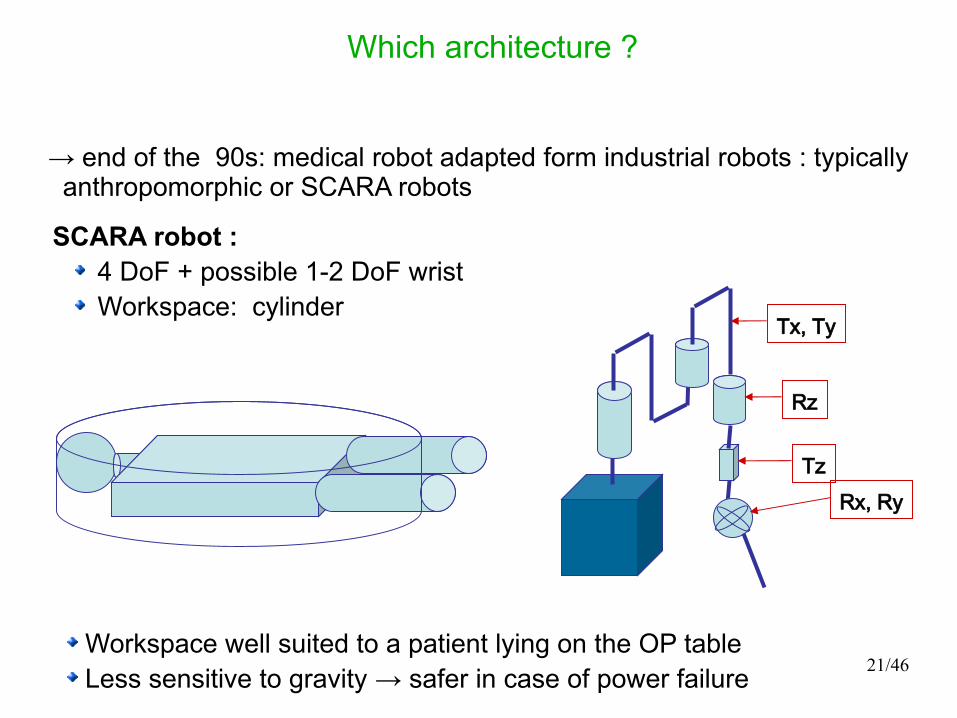
→ end of the 90s: medical robot adapted form industrial robots : typically anthropomorphic or SCARA robots
SCARA robot :4 DoF + possible 1-2 DoF wristWorkspace: cylinder
Tx, Ty
Tz
Rz
Rx, Ry
Workspace well suited to a patient lying on the OP table Less sensitive to gravity → safer in case of power failure
22/46
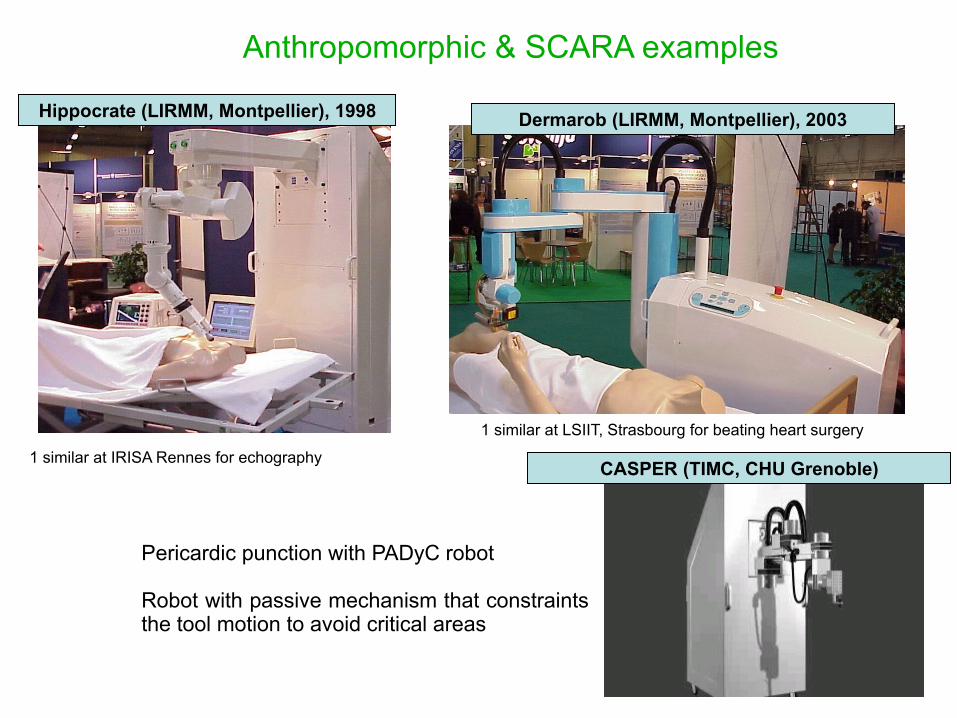
Anthropomorphic & SCARA examples
Hippocrate (LIRMM, Montpellier), 1998 Dermarob (LIRMM, Montpellier), 2003
1 similar at IRISA Rennes for echography
1 similar at LSIIT, Strasbourg for beating heart surgery
CASPER (TIMC, CHU Grenoble)
Pericardic punction with PADyC robot
Robot with passive mechanism that constraints the tool motion to avoid critical areas

23/46
Dermarob 1998-2003, LIRMM Montpellier
Skin repair surgery for severe-burn patients 2 stages procedure :
skin harvestinggrafting
Issues : important efforts and accuracy Constraints : constant skin thickness, avoid holes Automated harvesting
24/46
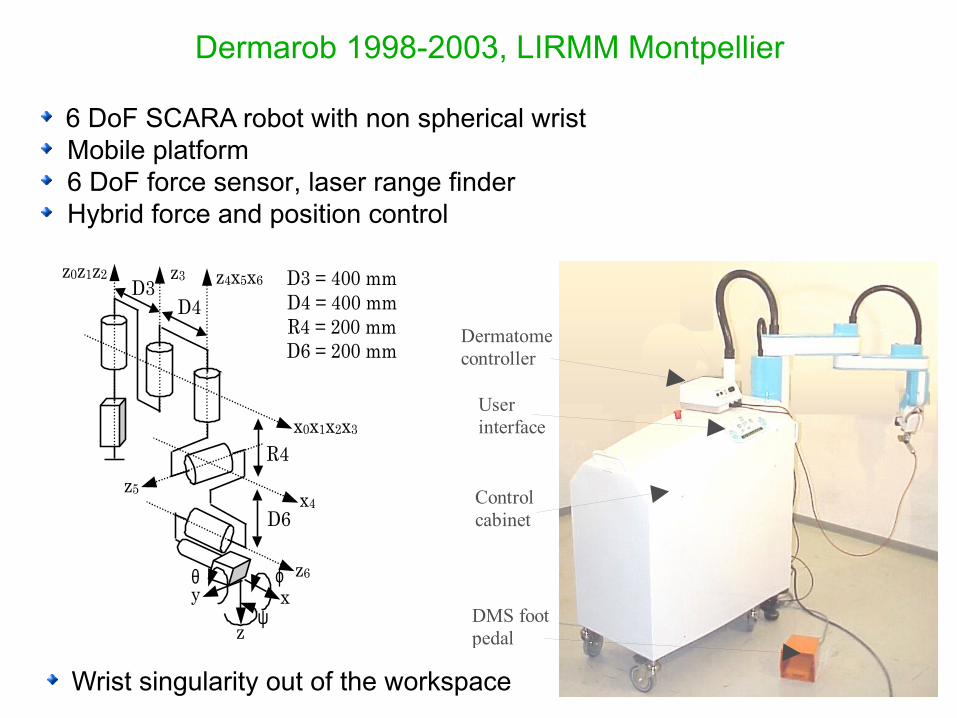
v
DMS footpedal
Userinterface
Dermatomecontroller
Controlcabinet
6 DoF SCARA robot with non spherical wrist Mobile platform 6 DoF force sensor, laser range finder Hybrid force and position control
z0z1z2 z3 z4x5x6
z6
z5
x0x1x2x3
D3D4
D6x4
R4
z
y xϕθ
ψ
D3 = 400 mmD4 = 400 mmR4 = 200 mmD6 = 200 mm
Wrist singularity out of the workspace
Dermarob 1998-2003, LIRMM Montpellier

25/46
Parallel robot example
Stiffness, accuracy, acceleration, lightweight, load/weight ratio Complex model, singularities, small workspace
… traditional architecture of haptic interfaces
Surgiscope, ISIS

Medical robotics - Design B. Bayle, University of Strasbourg
26/46
Which architecture ?
2000 → now : medical robot designed for specific tasks
Frequent properties :
Number of DoF limited to the task achievement
Often : fixed point (environmental) constraint (trocar, needle)
Often : tool raw positioning
Very often : tool orientation with spherical workspace
Sometimes : tool translation or translation+rotation

Medical robotics - Design B. Bayle, University of Strasbourg
27/46
First problem : going through the trocarRemote Center of Motion architectures (RCM)
Surgical tasks with fixed point constraint : Minimally Invasive Surgery (MIS) Echography Percutaneous needle insertion

Medical robotics - Design B. Bayle, University of Strasbourg
28/46
First problem : going through the trocarRemote Center of Motion architectures in MIS
Da Vinci (Intuitive Surgical), 1999
ZEUS (Computer Motion), 1998ZEUS (Computer Motion), 1998
Active RCM
Passive RCM
29/46
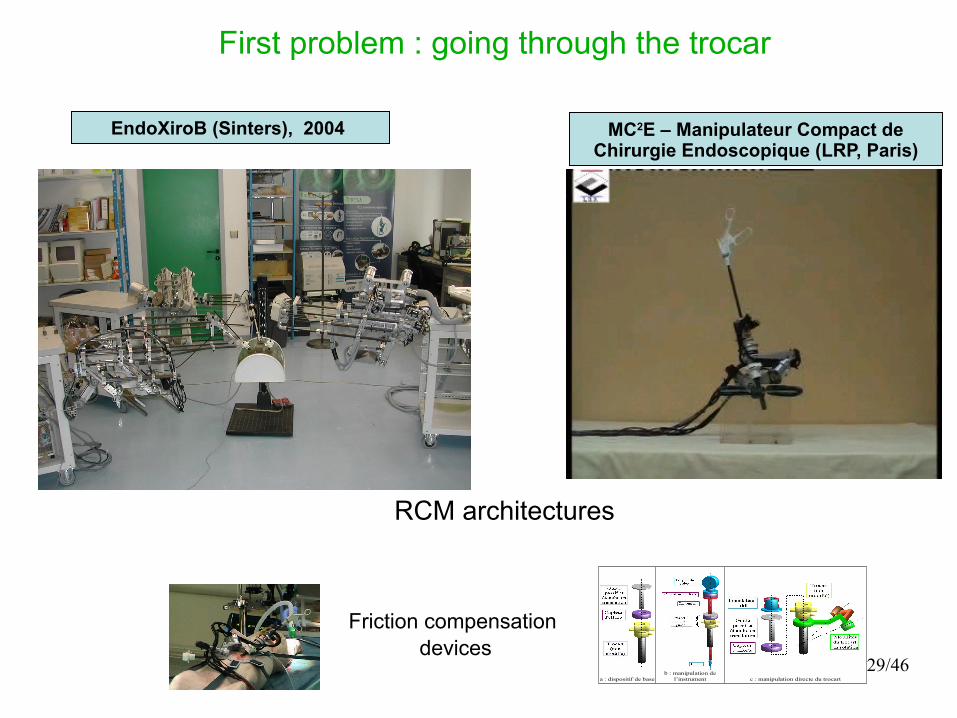
First problem : going through the trocar
MC2E – Manipulateur Compact de Chirurgie Endoscopique (LRP, Paris)
EndoXiroB (Sinters), 2004
RCM architectures
c : manipulation directe du trocart
b : manipulation de l’instrument
a : dispositif de base
Friction compensation devices
Medical robotics - Design B. Bayle, University of Strasbourg
30/46
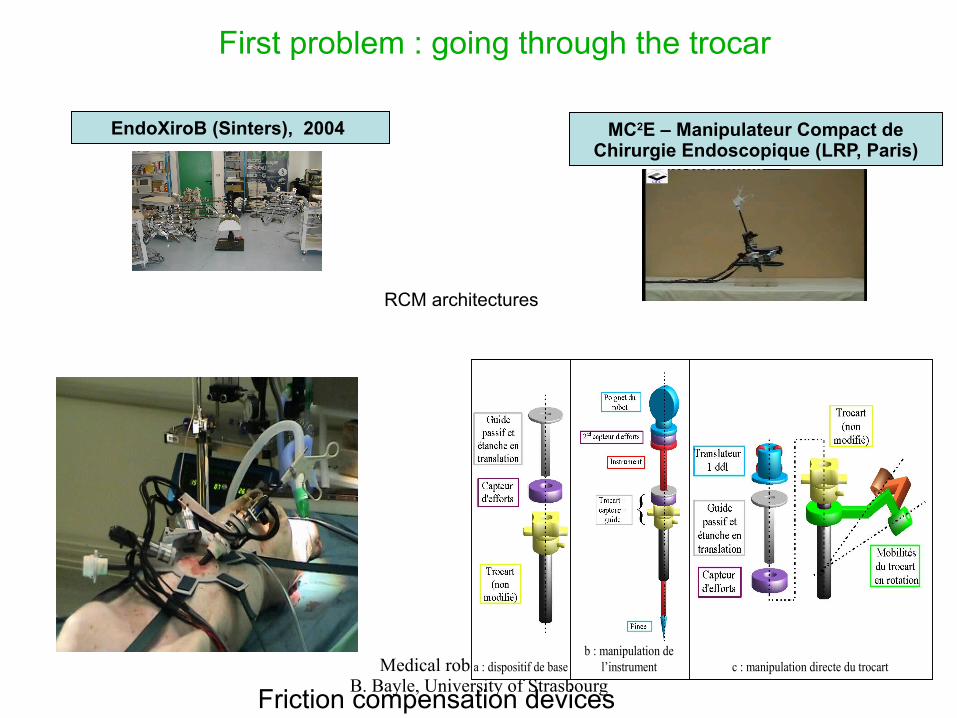
First problem : going through the trocar
MC2E – Manipulateur Compact de Chirurgie Endoscopique (LRP, Paris)
EndoXiroB (Sinters), 2004
RCM architectures
c : manipulation directe du trocart
b : manipulation de l’instrument
a : dispositif de base
Friction compensation devices
Medical robotics - Design B. Bayle, University of Strasbourg
31/46
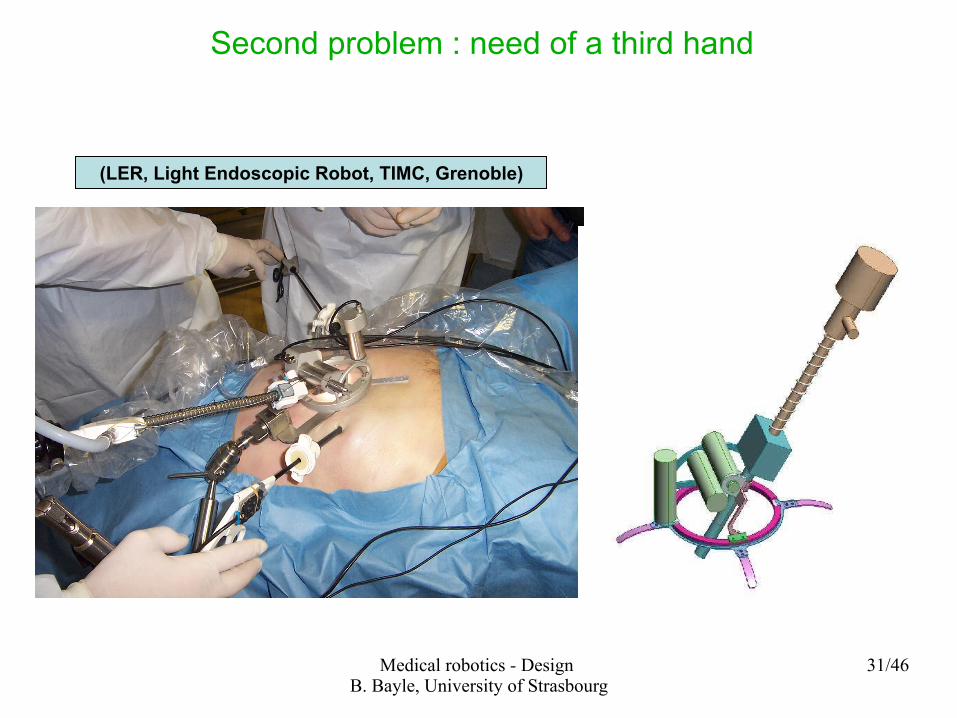
Second problem : need of a third hand
(LER, Light Endoscopic Robot, TIMC, Grenoble)
32/46
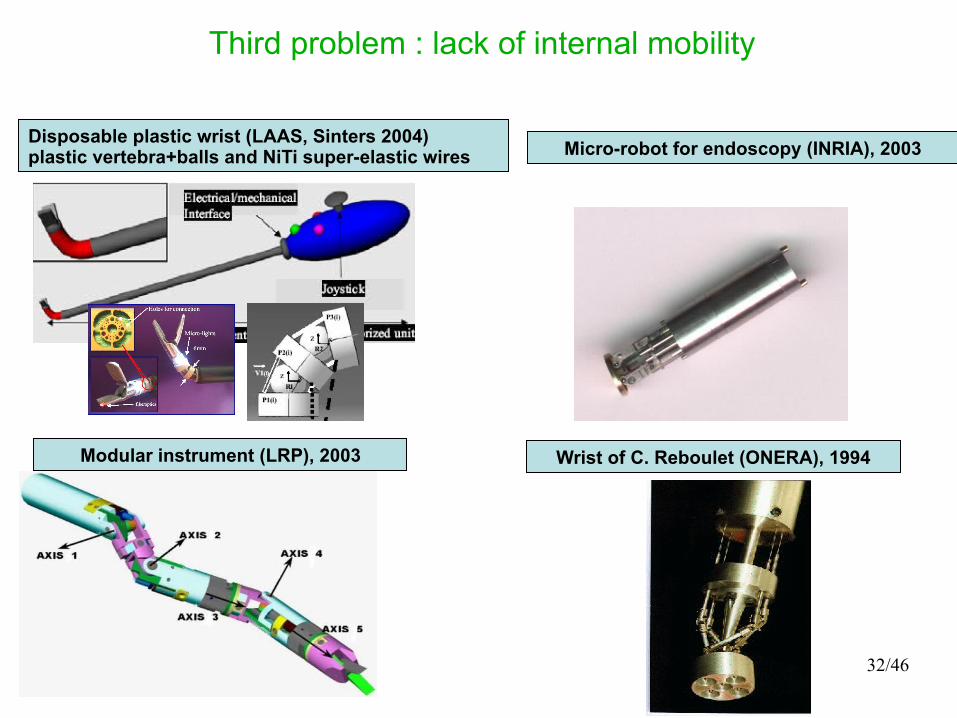
Third problem : lack of internal mobility
Disposable plastic wrist (LAAS, Sinters 2004)plastic vertebra+balls and NiTi super-elastic wires
Modular instrument (LRP), 2003
Micro-robot for endoscopy (INRIA), 2003
Wrist of C. Reboulet (ONERA), 1994
Medical robotics - Design B. Bayle, University of Strasbourg
33/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion

34/46
About safety
35/46
About safety
Problems
Robot shares its workspace with the medical staff and with the patient
Trial and error approach is not allowed
Sterility constraint
Compatibility with other medical devices
Some solutions
Intrinsically safe mechanical design : lightweight, limited power, slow motion, workspace suited to task, passive limits
Redundancy of sensors : incremental and absolute encoders, collision detectors, force sensors, hardware self-check sensors
High-quality software : fault tolerant programming language, redundancy of computers, quality certified programming
Safe human interface : simple to use, easy to understand, important function easily and quickly accessible

Medical robotics - Design B. Bayle, University of Strasbourg
36/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion
37/46
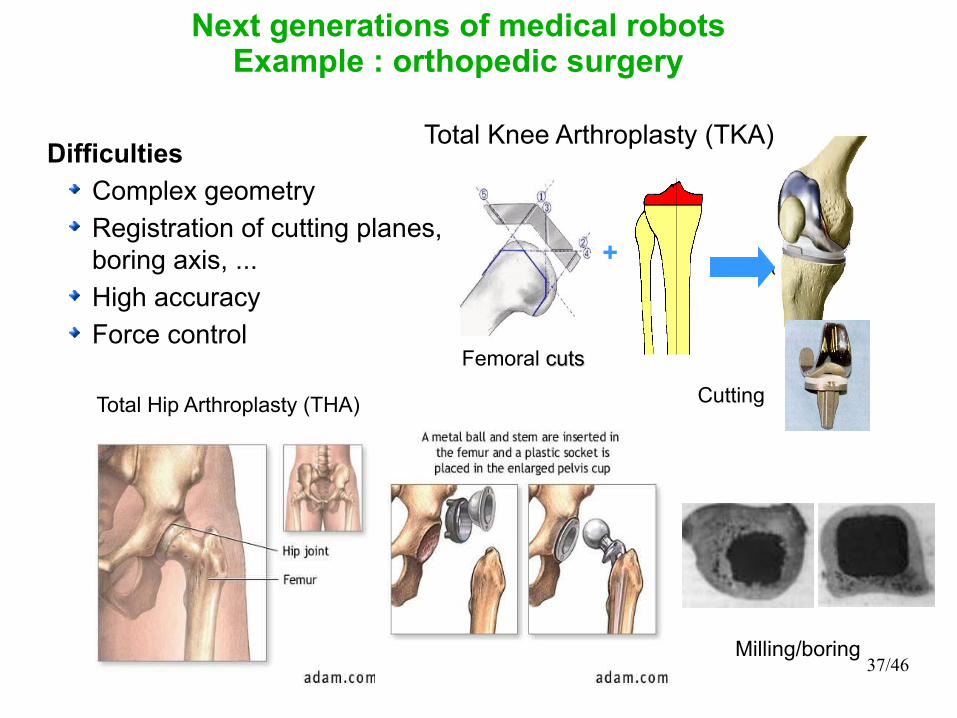
Difficulties
Complex geometry
Registration of cutting planes, boring axis, ...
High accuracy
Force control
Next generations of medical robotsExample : orthopedic surgery
Tibial cutTibial cut
Femoral cuts cuts
Total Knee Arthroplasty (TKA)
+
Total Hip Arthroplasty (THA)
Milling/boring
Cutting

38/46
ROBODOC (ISS), 1992ROBODOC (ISS), 1992
CASPAR (OrtoMaquet), 1997
CRIGOS (Helmholtz-Institute/TIMC), 1997
Table-mounted robots + navigation systems
ACROBOT (Imperial College/Acrobot Ltd), 2001
BRIGIT (MedTech, LIRMM), 2005
Next generations of medical robotsExample : orthopedic surgery
39/46
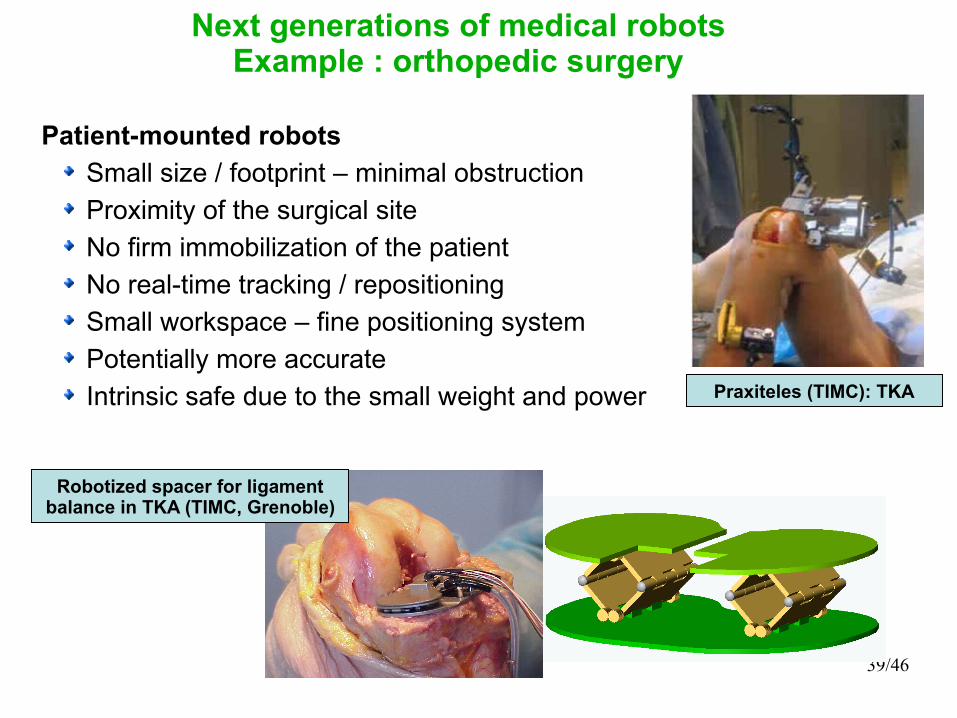
Praxiteles (TIMC): TKA
Patient-mounted robots
Small size / footprint – minimal obstruction
Proximity of the surgical site
No firm immobilization of the patient
No real-time tracking / repositioning
Small workspace – fine positioning system
Potentially more accurate
Intrinsic safe due to the small weight and power
Robotized spacer for ligament balance in TKA (TIMC, Grenoble)
Next generations of medical robotsExample : orthopedic surgery

40/46
Some trends
Technical challenges for new medical procedures
Diagnostic and therapy of smal intestine
Microsurgery
Neuroendoscopy for treatment of back pain
Totally endoscopic beating heart surgery
NOTES
Biomicromachines
Technical challenges to improve existing procedures
Smaller, simpler, smarter and cheaper robots
More integrated systems “plug and play”
More immersive human-machine interface
General trend : robots dedicated to the task
Medical robotics - Design B. Bayle, University of Strasbourg
41/46
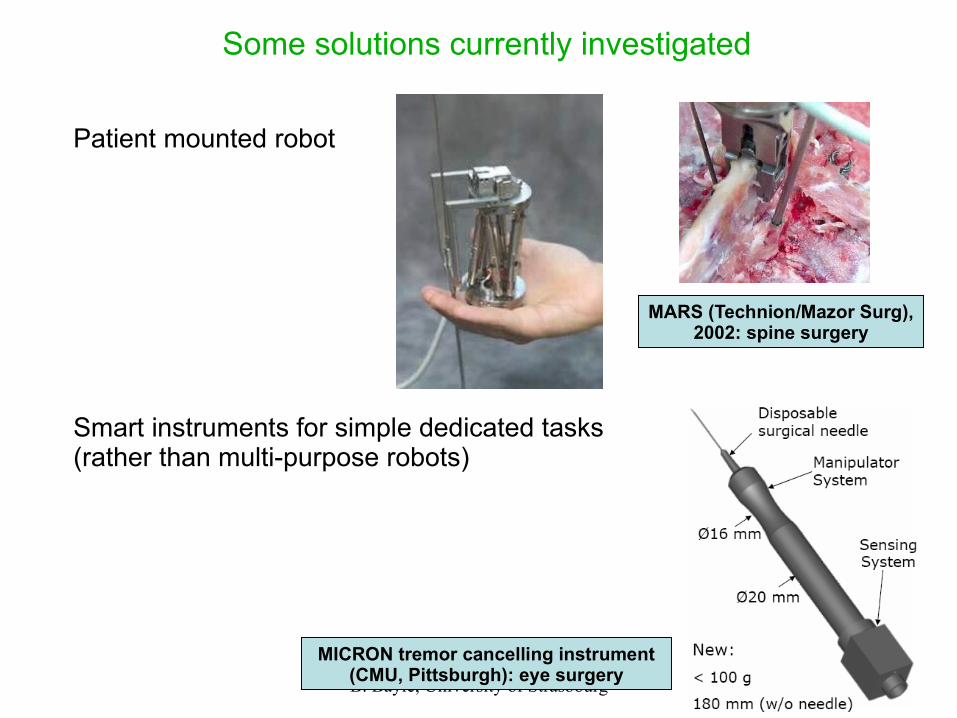
Some solutions currently investigated
MARS (Technion/Mazor Surg), 2002: spine surgery
Patient mounted robot
Smart instruments for simple dedicated tasks (rather than multi-purpose robots)
MICRON tremor cancelling instrument (CMU, Pittsburgh): eye surgery
Medical robotics - Design B. Bayle, University of Strasbourg
42/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion
Medical robotics - Design B. Bayle, University of Strasbourg
43/46
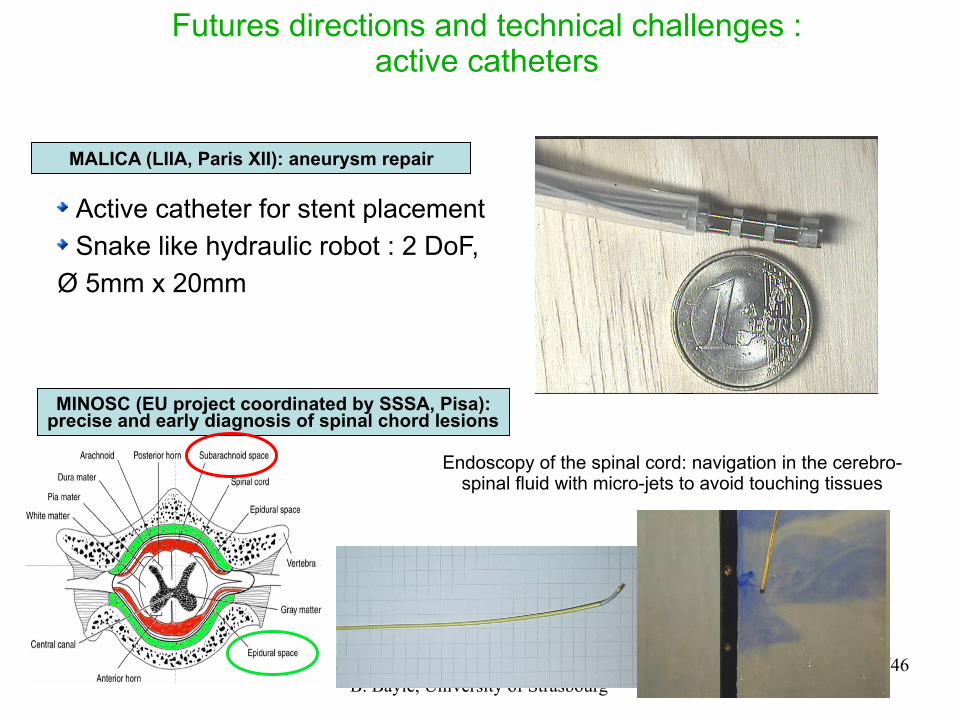
MALICA (LIIA, Paris XII): aneurysm repair
Active catheter for stent placement
Snake like hydraulic robot : 2 DoF,
Ø 5mm x 20mm
Futures directions and technical challenges :active catheters
MINOSC (EU project coordinated by SSSA, Pisa): precise and early diagnosis of spinal chord lesions
Endoscopy of the spinal cord: navigation in the cerebro-spinal fluid with micro-jets to avoid touching tissues

Medical robotics - Design B. Bayle, University of Strasbourg
44/46
HeartLander (CMU, Pittsburgh)
Inchworm-like robot for beating heart surgery
Futures directions and technical challenges :intra-cavity mobile robots
The Endoscopy « Pill » M2A(Given Imaging), 2001
EMIL (SSSA, ARTS Lab., Pise)

Medical robotics - Design B. Bayle, University of Strasbourg
45/46
Outline
Introduction : how can robotics help surgery ?
Prehistory
Medical robot design workflow
Environmental constraints
Which architecture ?
About safety
Next generations of medical robots
Futures directions and technical challenges
Conclusion
Medical robotics - Design B. Bayle, University of Strasbourg
46/46
Conclusion
To be improved :
Benefits/(costs x complexity ) ratio should be increased
Technical staff in the OP room
Simpler training for the surgeons
Operation time should be at least similar than conventional operation
Reduce overall costs for the hospital (maintenance, training)
Long-term benefits should be proven
Installation and use should be simpler
Safety
► Still lot of work : improve interaction surgeons / engineers
Medical robotics - Design B. Bayle, University of Strasbourg
47/46
Examples
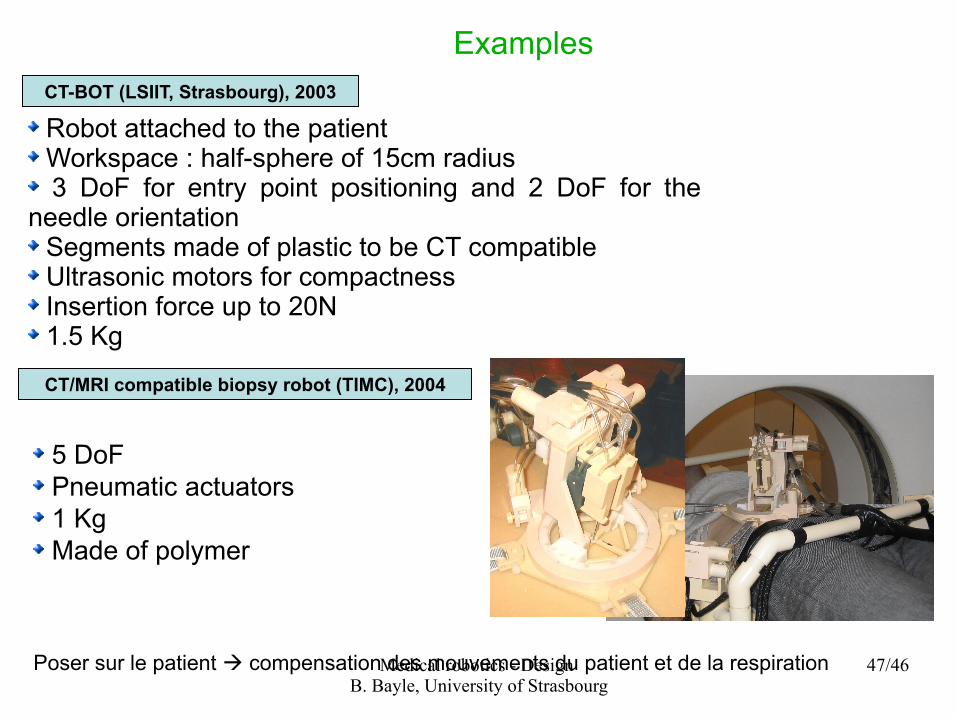
Robot attached to the patient Workspace : half-sphere of 15cm radius 3 DoF for entry point positioning and 2 DoF for the
needle orientation Segments made of plastic to be CT compatible Ultrasonic motors for compactness Insertion force up to 20N 1.5 Kg
CT-BOT (LSIIT, Strasbourg), 2003
CT/MRI compatible biopsy robot (TIMC), 2004
5 DoFPneumatic actuators1 KgMade of polymer
Poser sur le patient compensation des mouvements du patient et de la respiration







