
Lung Scan &
Rdn. Venography
Jiraporn Sriprapaporn, M.D.
Nuclear Medicine,
Siriraj Hospital
Last updated on 21 JAN 2017
Copy Right By J Sriprapaporn

Contents
Anatomy
Physiology
Mechanism
Technique
Indications
Interpretation
Radionuclide venography
V/Q Lung scans

Respiratory System
Perfusion lung scan Tc-99m MAA
Ventilation lung scan
Xe-133, Tc-99m aerosol, Technegas
Anatomy
Right lung & left lung
Bronchopulmonary segments
(artery, vein, & bronchus)
Right Lung: 3 lobes; RUL,RML, & RLL
Left Lung: 2 lobes; LUL (Lingular segments) & LLL
Adults: Pulmonary arterioles 280 million
(Children adult number ~ 8 yr)

Bronchopulmonary Segments
http://www.anatomychartee.us/anatomy-lung-segments-diagram-system/lung-segmental-anatomy/
http://radiologykey.com/pulmonary-scintigraphy/

Blood Supply
2 Systems:
Pulmonary arteries: 95%
Bronchial arteries: 5%

Physiology
AIR Respiratory tract: trachea bronchi bronchioles alveoli
Function: Gas exchange
Distribution of Q & V from apex to base is not uniform in the upright position (gravity effect)
Gravity effects the distribution of both Q & V (affects perfusion > ventilation)

Effects of Gravity (Upright Position)
APEX VENTILATION PERFUSION V/Q RATIO
BASE 1.5-2 folds 3-5 folds

Pathophysiology
Ventilation abnormality redistribution of
pulmonary perfusion
Hypoventilation reflex vasoconstriction hypoperfusion
Acute hypoperfusion rarely produces
hypoventilation or minimal; not clinically significant

Lung Scan
PERFUSION LUNG SCAN (Q)
Tc-99m MAA
VENTILATION LUNG SCAN (V)
Xe-133, Xe-127, Kr- 81m
Tc-99m DTPA/ phytate aerosol
Technegas

Indications of V/Q Lung Scan
Acute pulmonary embolism*
Pulmonary hypertension
Right-to-left shunt
Prior to thoracic surgery

Pulmonary Embolism
Most important complication of DVT
Symptomatic, fatal*
Asymptomatic (silent)
Origin: Leg DVT (70-80%)

DIAGNOSIS OF PULMONARY EMBOLISM
Clinicals : Inaccurate Lab tests : D-dimer Arterial Blood Gases: Hypoxemia, A-A gradient ECG : Classic S1Q3T3 pattern CXR : Normal or mild abn (*R/O other
diseases) V/Q lung scan : V/Q mismatched
defects Pulmonary Angiography*** Gold
standard Pulmonary CTA Others: MRI


Perfusion Lung Scan: Principle
Tracer: Tc-99m MAA, particle size=20-40 u
Mechanism: Capillary blockade in proportion to regional blood flow
Number of particles: minimum 100,000; optimal 200,000-600,000
Less than 1/1000 capillaries are blocked
Biological T1/2 = 2-4 hr Reticuloendothelial (RE) system
Defects from PE
// bronchopulmonary
segments
Essentials Nucl Med

Reduced Number of Particles Injected
Pediatric patients
Patients with suspected or known Rt-to-Lt
shunt
Patients with pulmonary hypertension
Patients with prior pneumonectomy
Patients with single lung transplant

Perfusion Lung Scan: Techniques
Radiopharm: Tc-99m MAA Dose 3-5 mCi for adults IV injection in supine
position Do not draw blood into
syringe; “hot spots” in Q scan
Imaging techniques Static planar images 6-8
views, 500 kcts SPECT imaging

Ventilation Lung Scan: Principle
Particle size: Smaller go deeper!
Tracers
Inert gas: 133Xe, 127Xe, 81mKr
Aerosol*: 99mTc-DTPA/ phytate [Tc-99m
aerosol particle size = 0.5-3 um]
Technegas: particle size = 0.02-0.2 um

Ventilation Agents
Xe-133 Xe-127 Kr-81m Tc-99m radioaerosol
Technegas/ Pertechnegas
T1/2 5.3d 36.4d 13s 6h 6h
energy 80 203 190 140 140
Status Gas Gas Gas Aerosol (0.5-3 um)
Gas-like (0.02-0.2 um)
Cost Low High High Low High
Before/After Q scan
B A A B B
Multiple V N N Y Y Y

Ventilation Lung Scan: Techniques
Patient preparation: None
Techniques:
Inhalation, upright position is preferred.
Needs patient’s cooperation

Xe-133 Ventilation Lung Scan
Single view-3 phases: Washin-Equilibrium-Washout

Radio-aerosol Ventilation Lung Scan
O2
• Imaging of multiple views
• Relatively large particles central
airway deposition !

TECHNEGAS

Technegas Ventilation Scan
• Ultrafine particles
• Ideal for ventilation lung SPECT

Figure 1. Normal V/Q SPECT. using Technegas and Tc-99 m MAA are aligned and displayed in transverse, coronal and sagittal planes
Roach PJ, et al SNM08
V/Q SPECT

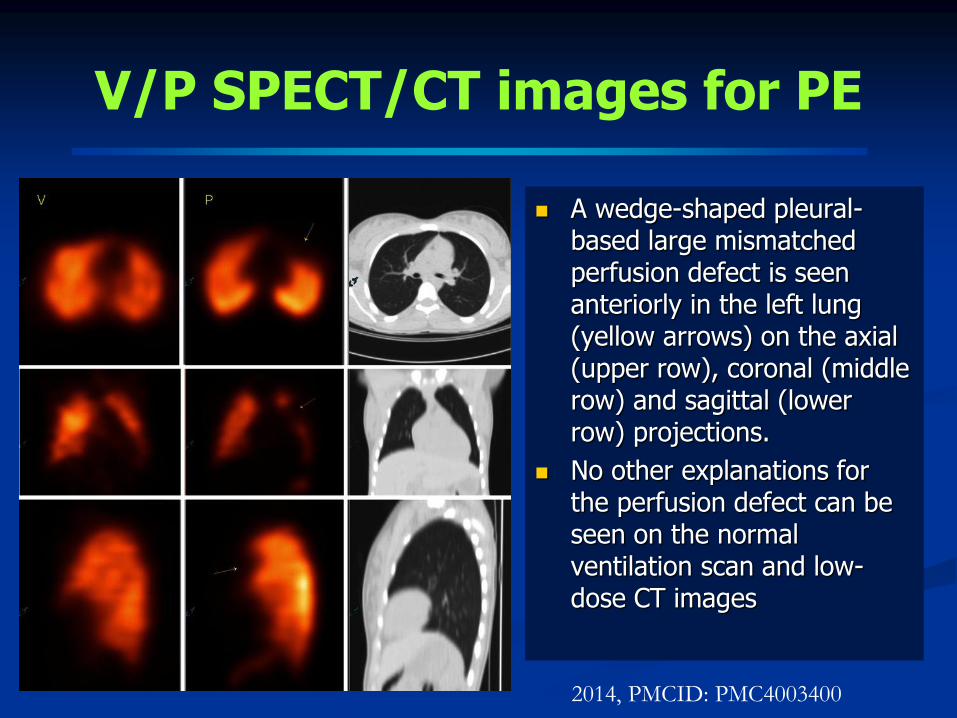
V/P SPECT/CT images
A wedge-shaped pleural-based large mismatched perfusion defect is seen anteriorly in the left lung (yellow arrows) on the axial (upper row), coronal (middle row) and sagittal (lower row) projections.
No other explanations for the perfusion defect can be seen on the normal ventilation scan and low-dose CT images
2014, PMCID: PMC4003400

Interpretation of Lung Scan
1. Pretest clinical probability
2. Perfusion lung Scan (Q)
3. Ventilation lung Scan (V)
4. CXR (within 24 hrs)
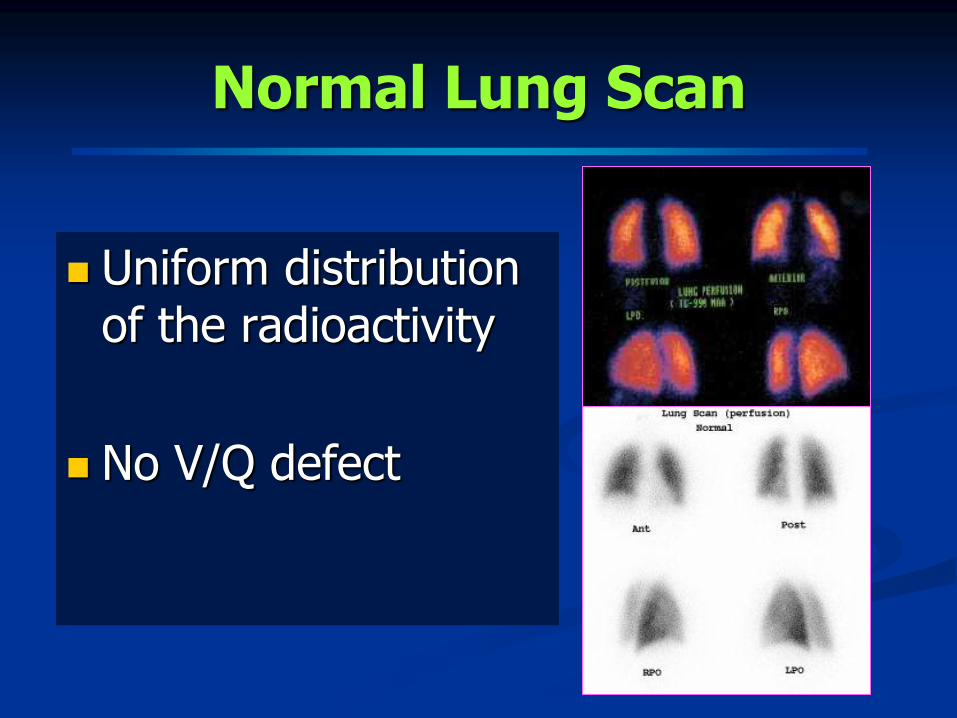
Normal Lung Scan
Uniform distribution of the radioactivity
No V/Q defect

1. Nonuniform distribution
2. Perfusion and/ or ventilation defect
Nonsegmental defect
Segmental defect: wedged-shaped & pleural-based defect Large defect: > 75% of segment
Moderate defect: 25-75% of segment
Small defect: < 25% of segment
Abnormal Lung Scan

V/Q Match vs Mismatch
V/Q matched defect: Abn both Q & V
V/Q mismatch defect: Abn Q, Normal V
Pulmonary Embolism

Segmental Non-segmental
Pulmonary embolism
Pulmonary infarct
Tumors
Pleural effusion
Cardiomegaly
Mediastinal or hilar adenopathy
Pneumonia
Bullae
Metal artifacts

Non-PE Diseases/Conditions
Findings:
Patchy distribution
Nonsegmental defect
Matched V/Q defect(s)
Abnormal CXR finding corresponding to the area of V/Q defect
Causes
COPD
Blebs, bullae
Pulmonary edema, CHF
Pleural effusion
Asthma
Pulmonary trauma
Mucous plug
Bronchogenic CA
Pneumonia

V/Q Matched Abnormalities

V/Q Mismatches: Causes
Acute PE
Previous PE
Bronchogenic carcinoma
Vasculitis
Previous radiation therapy
Pulmonary vasc anormalies

Typical Scintigraphic Findings For PE
Multiple segmental perfusion defects
Normal ventilation
Usually normal CXR
“Mismatched V/Q defects”
V/P SPECT/CT images for PE
A wedge-shaped pleural-based large mismatched perfusion defect is seen anteriorly in the left lung (yellow arrows) on the axial (upper row), coronal (middle row) and sagittal (lower row) projections.
No other explanations for the perfusion defect can be seen on the normal ventilation scan and low-dose CT images
2014, PMCID: PMC4003400

Interpretation of Acute PE
PIOPED
Modified PIOPED II
Perfusion-only modified PIOPED II
Perfusion-only PISAPED
PIOPED " The Prospective Investigation of Pulmonary Embolism Diagnosis "

PIOPED
" The Prospective Investigation of Pulmonary Embolism Diagnosis “
Used pulmonary angiogram as a gold standard.
The criteria were developed in late 1983
The largest study of accuracy of lung scan in the Dx of acute PE
6 medical centers in U.S.A.
PIOPED II CTA PIOPED III MRA
PIOPED I V/Q Lung scan

“PIOPED CRITERIA” for Interpretation of Acute PE
Normal Exclude significant PE !, with an incidence of 2% to 4% &
the chance of significant morbidity or mortality from PE is < 1%.
Very low probability
Low probability
Intermediate
High probability: > 2 large segmental mismatched V/Q defects,
negative CXR

Ventilation, Perfusion, and Radiographic Interpretive Criteria for PE
(SNM guideline v4, 2012)
PIOPED Modified PIOPED II
High LR [> 80% risk]
- >2 large mismatched (V:Q)
segmental defects*
High LR [85-90% risk]
- > 2 large mismatched (V:Q) segmental defects*
Borderline high LR
- 2 large mismatched (V:Q)
segmental defects*
Intermediate LR [20-80% risk]
- 2 moderate or 1 large mismatched
(V:Q) defect*
- Difficult to categorize as high or low
Nondiagnostic [20-80% risk]
- All other findings
Borderline low LR
- 1 matched (V:Q) defect, CXR-negative
Low LR [< 20% risk]
- Nonsegmental perfusion defects†
- Q defect substantially < CXR defect
- Matched (V:Q) defects, CXR-negative
- Any number of small Q defects*
Very low LR [< 10 % risk]
- Nonsegmental†
- Q defect < CXR lesion
- 1–3 small segmental*defects
- Solitary matched (V:Q:CXR) defect (#1 segment) in mid
or upper lung
- Stripe sign‡
- Solitary large pleural effusion§
- > 2 matched (V:Q) defects, regionally normal CXR
Normal
- No Q defects
Normal
- No Q defects
*Or equivalent where large segmental defect, >75% of segment, equals 1 segmental equivalent; moderate defect, 25%–75% of segment, equals 0.5 segmental equivalent; small defect, < 25%, is not counted.

Very Low Probability
• Nonsegmental defects*
• Q defect < CXR lesion
• 1-3 small segmental defects
• Single triple matched defect (V, Q, CXR) in mid or upper zone
• Stripe sign
• Solitary large pleural effusion
• ≥2 matched defects, normal CXR
< 10% chance for
PE

"Stripe Sign" = A thin line (stripe) of activity (perfusion) at the pleural surface of a Q defect.
The finding is associated is likely related to spared perfusion in the cortex of the lung [Sostman HD, Gottschalk A. Radiology 1992 ]
"Stripe Sign" is suggested to indicate very low probability = 7% of lung zones with the stripe sign had PE present on PAG in the PIOPED study [Gottschalk A, et al. J Nucl Med 1993]
STRIPE SIGN

PPV of V/Q Lung Scan in Diagnosis of PE
Clinical Probability
Scan Category 80-100% 20-79% 0-19%
High 95% 85% 83%
Intermediate 71% 29% 14%
Low 43% 16% 4%
Normal/NN 0% 7% 2%
[PIOPED JAMA 1990, Sostman HD Radiology 1994]

Comparison of Interpretive Schema for Acute Pulmonary Emboli
Method Sensitivity (%) Specificity (%)
PIOPED 41 97
Modified PIOPED II 85 93
PISAPED 80-86 93-97
MDCT 83 96
Essentials in NM
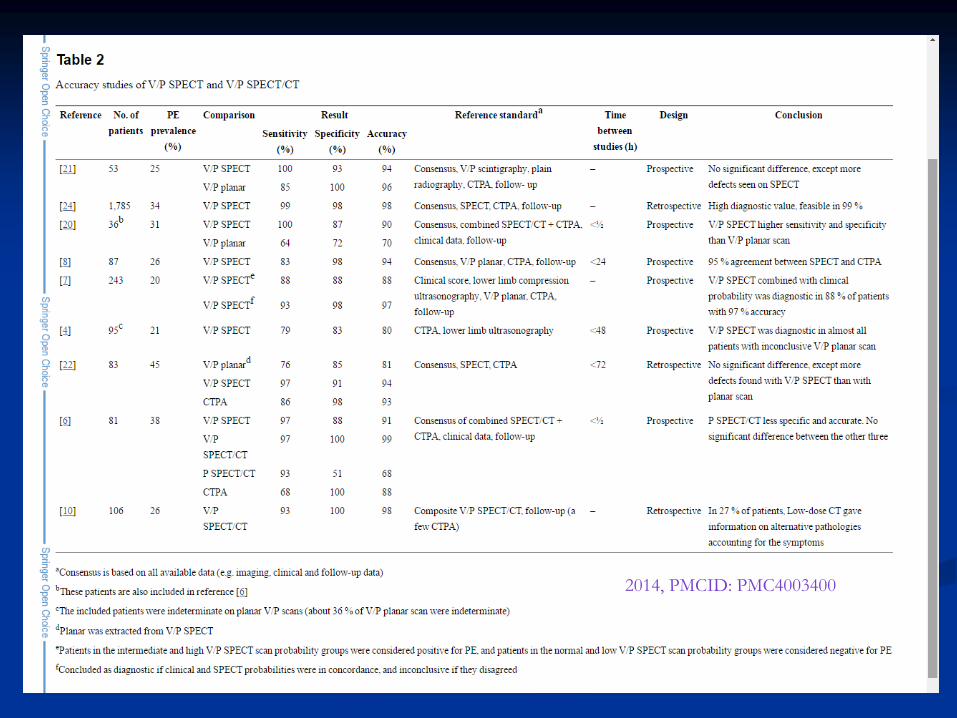
2014, PMCID: PMC4003400

V/Q Lung Scan Classification
High Prob
Nondiagnostic
Very low prob
Normal

Management Guideline
Normal Rule out clinically significant PE
Very-low probability Find out other causes of
symptoms.
Nondiagnostic Cannot rule out PE and needs
further investigations such as ultrasound for DVT.
High prob The patient can be treated for PE.
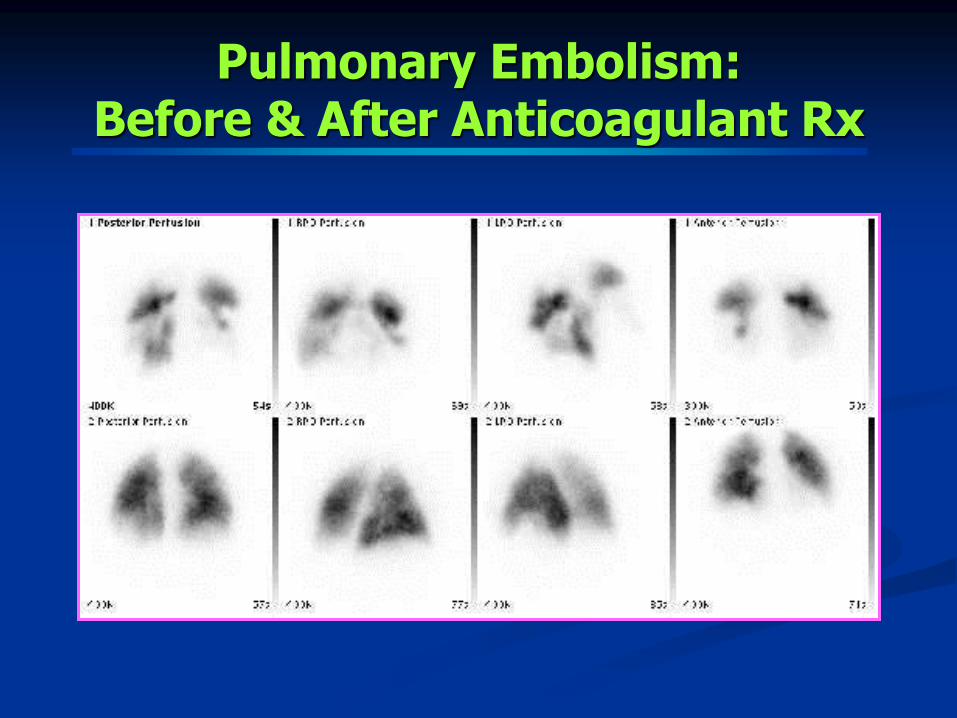
Pulmonary Embolism: Before & After Anticoagulant Rx

Acute Pulmonary Embolism
Perfusion-Ventilation lung scan ***
Multiple segmental V/Q mismatched defects , no radiographic abnormality
Increasing no. of defects increasing specificity
Pulmonary angiography is the original gold standard, now usually being replaced with CTPA.
V/Q scan cannot DDx acute from chronic PE, so F/U scan to evaluate the lung status post Rx *** (Baseline for the new episode, if any)

V/Q Lung Scan for Dx PE
Advantages
Simple, noninvasive, safe, and economical
High specificity (98%) esp. increasing no. of defects
The usefulness is well documented.
Disadvantages
Not widely available
Minimal radiation
Low sensitivity (41%)
Limitation in abn CXR
V/Q scan cannot DDx acute from chronic PE need F/U scan


Applications for Non-embolic Lung Disorders
Rt-to-Lt shunt
Intracardiac shunt
Intrapulmonary shunt
Evaluate lung function prior thoracic surgery eg. lung cancer
Quantitative lung function study

Right-to-left Shunt Systemic Circulation

Presence of Tc-99m MAA in the systemic circulation; brain & kidneys
Technique: Limited MAA particles.
Lung Scan in Rt-to-Lt Shunt

Prior Thoracic Surgery
Quantitative lung function study
To evaluate regional lung function and predict residual lung function post surgical resection
Lung cancer
Other lung diseases


VENOUS SYSTEM
Leg Veins

Deep Vein Thrombosis
Incidence: 2.5 million in US Risks: Stasis Symptoms: Leg swelling/
pain/tender/warm/red Complication: most important
= pulmonary embolism Dx of DVT
Clinical Dx is unreliable Noninvasive tests Invasive tests
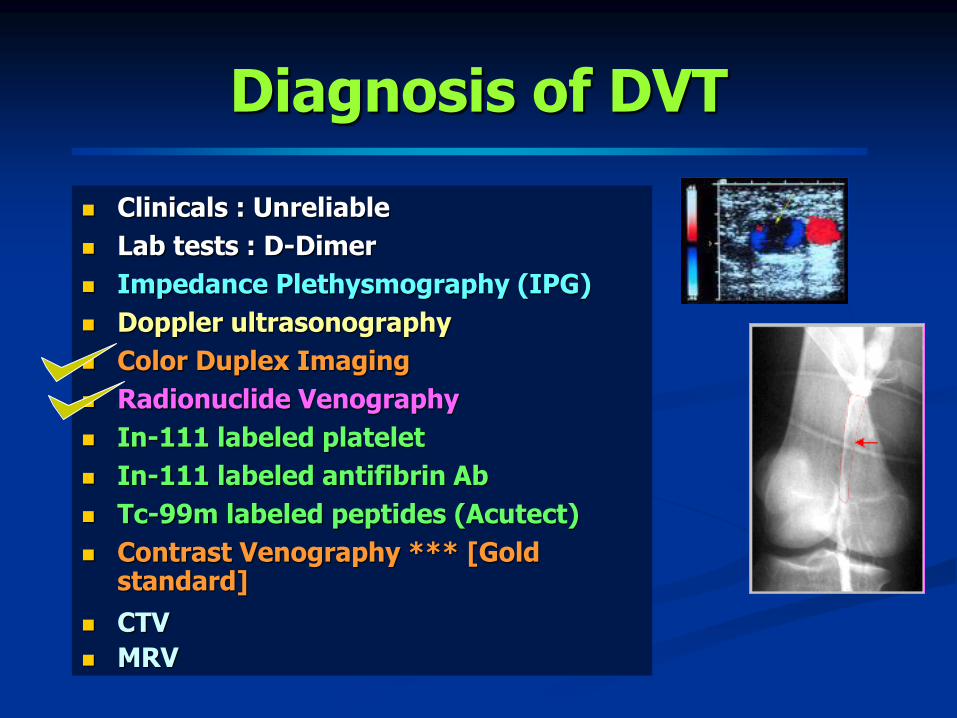
Diagnosis of DVT
Clinicals : Unreliable
Lab tests : D-Dimer
Impedance Plethysmography (IPG)
Doppler ultrasonography
Color Duplex Imaging
Radionuclide Venography
In-111 labeled platelet
In-111 labeled antifibrin Ab
Tc-99m labeled peptides (Acutect)
Contrast Venography *** [Gold standard]
CTV
MRV

Radionuclide Venography
Ascending Radionuclide Venography (RNV) Tc-99m phytate/ SC
Tc-99m MAA* (+Q scan)
Tc-99m labeled RBC Radionuclide Venography
Tc-99m labelled peptide venography

Ascending RNV
Principle: Direct injection of the radiotracer in to
foot veins
Mechanism: To evaluate venous flow; venous
occlusion or evidence of collateral circulation
Anatomy: calf veins*, popliteal vein, femoral, ext
iliac & common iliac, IVC
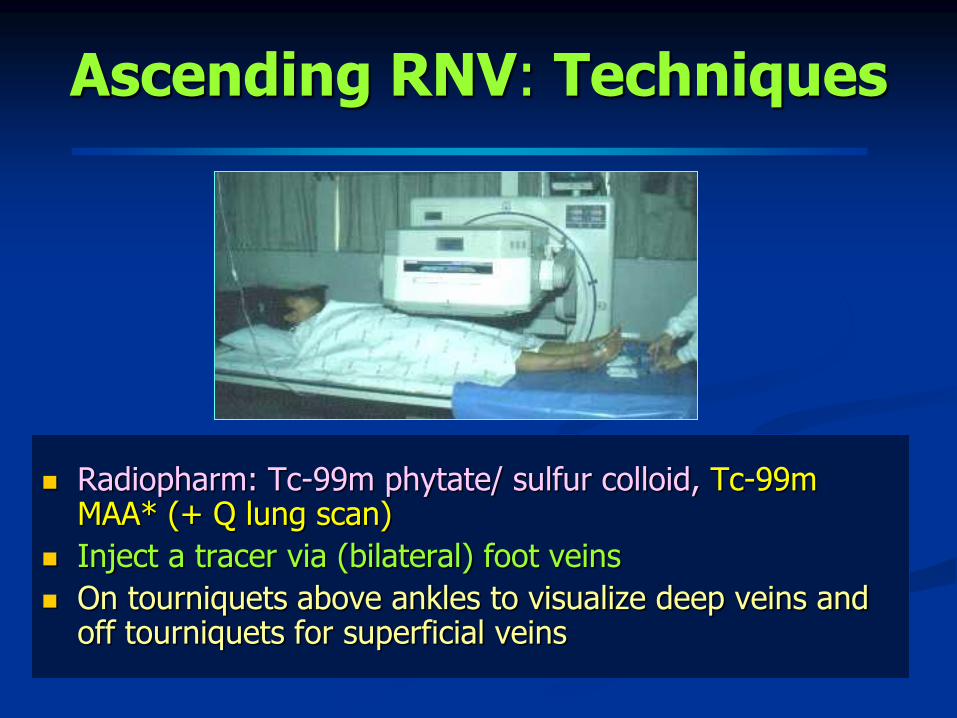
Ascending RNV: Techniques
Radiopharm: Tc-99m phytate/ sulfur colloid, Tc-99m MAA* (+ Q lung scan)
Inject a tracer via (bilateral) foot veins
On tourniquets above ankles to visualize deep veins and off tourniquets for superficial veins

Ascending RNV: Interpretation
Bilateral comparison, on & off TQ
Normal: Good flow without signs of venous occlusion
Abnormal: Obliteration of flow, filling defect, asymmetric flow +/-collaterals

Normal Asc RNV
Whole-body Images
phytate
Multiple Static Images

Normal vs Abnormal RNV
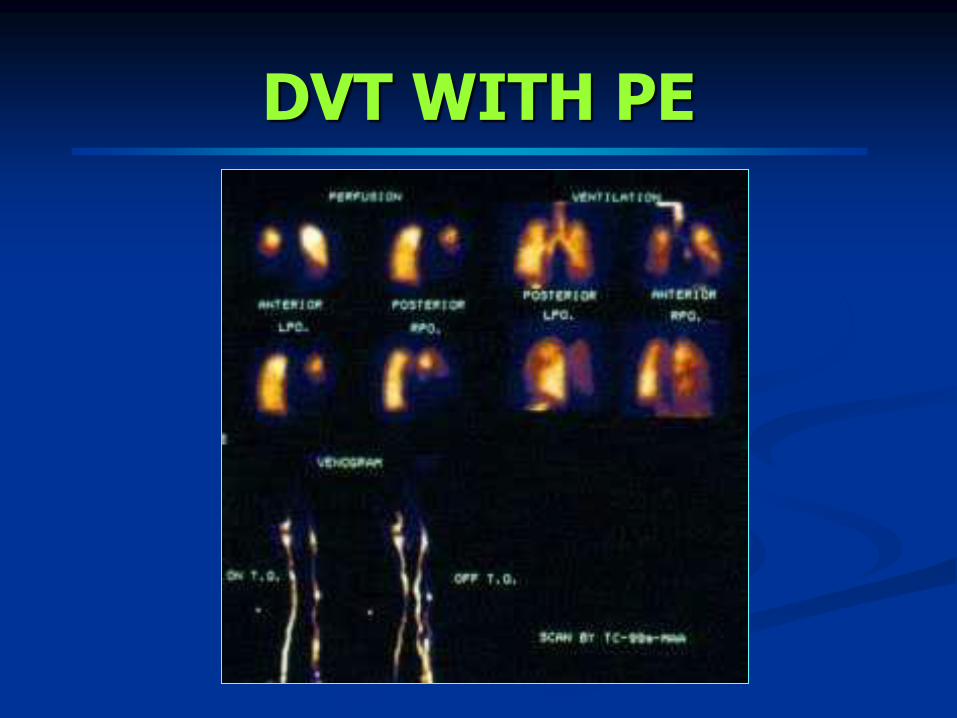
DVT WITH PE

Accuracy of Asc RNV
Authors Year No. (studies)
Sen (%)
Spec (%)
Corr (%)
Site of DVT
Webber (12) 1974 30 65 92 77 Overall Henkin (13) 1974 25 100 86 96 Proximal Van Kirk (14) 1976 19 100 95 95 Overall Vlahos (15) 1976 52 100 100 100 Pelvis 98 89 100 97 Thigh 98 92 97 95 Calf Ennis (16) 1977 154 90 89 95 Overall
Cordoba (17) 1977 44 100 80 94 Overall Ryo (18) 1977 47 89 66 89 Overall Gomes (19) 1982 51 88 65 67 Overall Mohamadiyeh(20) 1993 32 90 73 89 Proximal
Mangkharak 1998 72 88 96 90 Overall 55 95 97 96 Pelvic 72 95 100 90 Thigh 72 77 96 83 Calf
Mangkharak J, et al. J Med Assoc Thai 1998;81:432-441

RNV-upper Extremities
Normal
Abnormal

Advantages & Disadvantages
Contrast Venography
Most reliable for Dx (gold
std.)
Need skilled team
Good anatomic visualization
(calf iliac veins & IVC)
More Invasive
Potential risks
Not suitable for frequent F/U
Not provide information about
associated PE
Radionuclide Venography
Reliable results esp. proximal
vein
Simpler
Poorer anatomic details
(good only for proximal v.)
Less invasive
Safe
More suitable for frequent F/U
Provide information about
associated PE (Tc-99m MAA)

Tc-99m labeled RBC Radionuclide Venography
Or blood-pool radionuclide venography
equilibrium stage
Inject the radiotracer via any vein
Need high-resolution collimator
Image quality depends on labeling efficiency
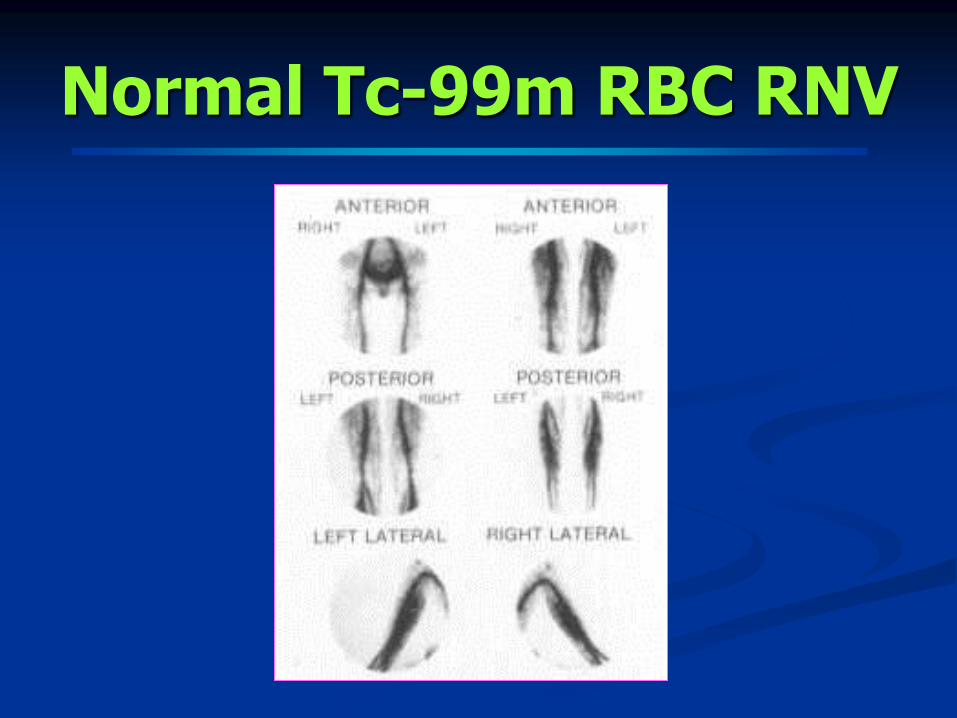
Normal Tc-99m RBC RNV

Tc-99m RBC RNV
Whole-body vs
multiple overlapping static images

Tc-99m Labeled RBC vs Ascending RNV
Advantages
Do not need foot vein access, easier
Possible less painful
Disadvantages
Image quality depends on labeling efficiency
Not direct evaluation of venous flow
Less anatomical details
Concomitant Q lung scan is impossible.
Both cannot DDx acute vs chronic DVT !

Summary
Diagnosis of Ac PE needs clinical and other diagnostic tests eg. venous US, VQ, CTA.
Lung and vascular scintigraphy has an important role in evaluation of patients with suspected PE &/or DVT in an appropriate setting esp. normal CXR, C/I for CTA.
Tc-99m MAA can be used to evaluate DVT & PE in the same setting.
It can be used not only for the diagnosis but also for the follow-up after treatment.

References
Essentials in Nuclear Medicine, 2013
The Requisites in Nuclear Medicine, 2014
Pulmonary embolism http://emedicine.medscape.com/article/300901-overview
Online Radiography Continuing Education for Radiologic X ray Technologist. https://www.ceessentials.net/article12.html
Lung scan guideline v 4.0: http://interactive.snm.org/DOCS/LUNG_SCINTIGRAPHY_V4_FINAL.PDF







