
Kristen K. Reynolds, PhDAssociate Medical Director, VP Laboratory Operations
Copyright 2010 PGXL Laboratories LLC, Louisville KYAll materials herein are the exclusive property of PGXL Laboratories

Enabling Personalized Medicine
IntuitiveMedicine
PrecisionMedicine

~60% of meds in top 20 list causing ADRs are linked to a genetic variation
~122 drugs have FDA box warnings related to genetics

Applications of pharmacogenomics• Individualizing drug therapy selection
• Predicting adverse reactions, dosing, response
• Identify increased sensitivity to drug interactions

CYP2D6
DRD2
5-HTT
5-HTR2A
SSRI
SNRI
TCA
FGA
SGA
MetabolismClearance
PDResponse
PK
UMs
EMs
PMs X
Dependent on drug concentration, receptor expression and affinity
CYP2D6 and psychotropic receptor variantsalter drug dose and/or selection
Ramey-Hartung, El-Mallakh, Reynolds. Clin Lab Med 2008;28:627-43.

Clinical Applications of Pharmacogenetic Information
• Anti-coagulation– Warfarin– Clopidogrel
• Psychiatry– Anti-depressants
• Oncology– Thiopurines– Tamoxifen– EGFRi’s
• Pain management– Codeine– Methadone
• Epilepsy– Phenytoin– Carbamazepine
• Diabetes– Glipizide

Application of Pharmacogenomics to warfarin therapy

The Problem
Reynolds et al. Pers Med 2007;4(1):11-31.

Reynolds et al. Pers Med 2007;4(1):11-31.

• 40% of population have deficient CYP2C9
• > 70% of population have decreased VKOR and are more sensitive to warfarin
Genetics of Warfarin metabolism and response

0 3 6 9 12 15 18 21 24 27 30
Ti me (days)
0. 00
0. 60
1. 20
1. 80
2. 40
3. 00
S-W
arfa
rin
(mg/
L) CYP2C9*1/*3
CYP2C9*1/*1
CYP2C9*1/*2
Accumulation
Steady-State
Linder et al. J Thrombosis & Thrombolysis 2002;14:227-232
CYP2C9 status increases magnitude of accumulation/unit dose as well as time to achieve steady-state

VKORC1 -1639 G>A genotype dictates S-warfarin therapeutic concentration
Dose2.7 ± 1.2 mg
Dose4.2 ± 2.2 mg
Dose6.7 ± 3.3 mg
All within INR 2-3
Zhu Y et al. Clin Chem 2007;53(7):1199-1205.

• Calculation of estimated maintenance dose• Modeling of individualized response to dose changes• Guidance for:
Monitoring strategy Dosing modifications Transition: induction to maintenance therapy
PerMIT:Warfarin©
Powered by PGXL Laboratories

All; 66 y/o, female, 130 lbs


No Loading Dose
PerMIT-guided Loading Dose

Concentration/Response Time Profile
Genotype: CYP2C9*1*2 // VKORC1 GGEstimated Maintenance dose: 6.3 mg/d (5.7 – 7.0)Time to Steady-State: 11 to 15 daysTarget therapeutic concentration: 0.8 mg/L
. . . . . . 6 mg/d. . . . . . . 10, 10, 8, 6 mg/d
Linder MW et al. 2011 (unpublished results)
CONFIDENTIAL

Application of Pharmacogenomics to Anti-platelet therapy

CYP2C19 - Plavix
• Clopidogrel (Plavix) is a pro-drug which is converted to an active metabolite by CYP2C19
• Active metabolite is what elicits the desired antiplatelet response
• ~ 30% of patients have deficiency in CYP2C19

Influence of CYP2C19 on Clopidogrel Response

New Draft Report
CONFIDENTIAL COPYRIGHT PGXL LABORATORIES 2012
THERAPEUTIC IMPLICATIONS1 Gene Phenotype Avoid Alternative Consideration Adjust Dosage Adjustment X CYP2C19 *2/*2
Poor Metabolizer
Clopidogrel*
Prasugrel Imipramine† Sertraline†
30% 50%
*Lack of efficacy due to failure to produce active metabolite; †Increased risk of adverse events due to diminished drug clearance.
CYP2C19 Poor Metabolizer (PM): This patient’s genotype is consistent with significantly reduced CYP2C19 enzymatic activity. PMs are at increased risk of drug-induced side effects due to diminished drug elimination of active drugs. Patients with no CYP2C19 function (PMs) taking clopidogrel lack adequate antiplatelet response and remain at risk for cardiovascular events, including thrombosis, myocardial infarction, stroke, and death.

Application of Pharmacogenetics to Pain Management

CYP2D6 - Opioids
• Hydrocodone• Oxycodone• Methadone• Others…
• Propoxyphene• Tramadol• Codeine
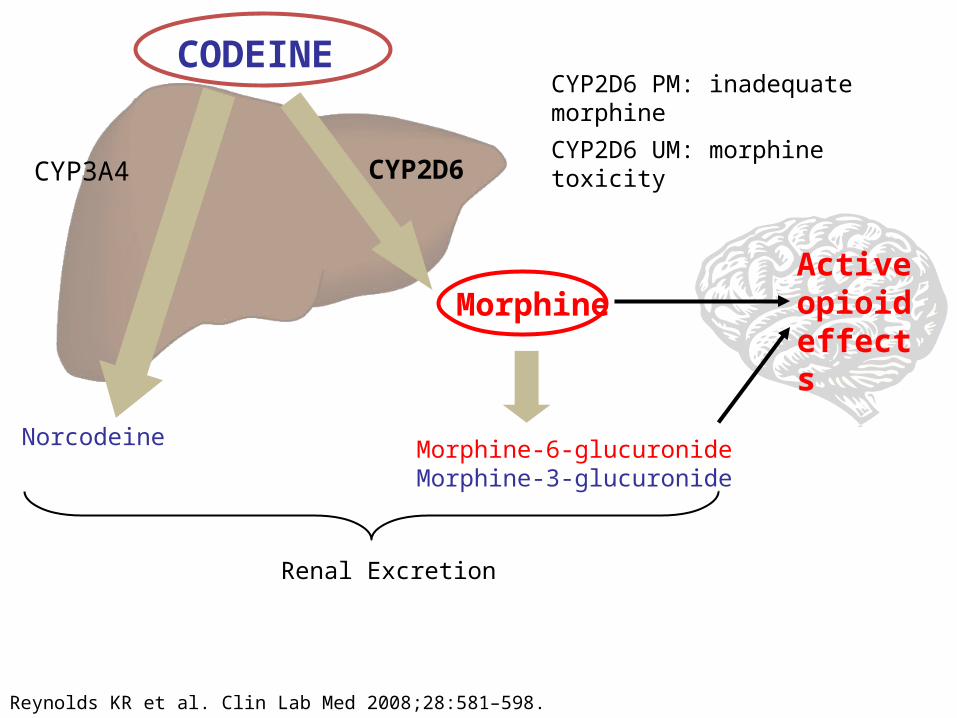
CODEINE
CYP3A4 CYP2D6
Norcodeine
Morphine
Morphine-6-glucuronide Morphine-3-glucuronide
Active opioid effects
Renal Excretion
Reynolds KR et al. Clin Lab Med 2008;28:581–598.
CYP2D6 PM: inadequate morphine
CYP2D6 UM: morphine toxicity

• Decreased drug metabolism = lack of efficacy– Poor pain control– Mis-interpretation of drug seeking behavior
• Ultra-rapid drug metabolism = possible side effects– Over-production of active compound– Mis-interpretation of over-compliance– Possible lower doses required
Effects of CYP2D6

CYP2D6 Variants
Extensive Metabolizers (EM) 55 – 60 % of population
Intermediate Metabolizers (IM) 25 – 30% of population
Poor Metabolizers (PM) 7 – 10 % of population
Ultra-rapid Metabolizers (UM) 1 – 3 % of population

Application of Pharmacogenomics to behavioral health

28
CASE: Depression/ADHD• 51 y/o male• Problematic Polypharmacy (Atomoxetine, Topiramate,
Oxcarbazapine, Aripaprazole,Valproic acid)• Genotyping results

29
Relevance to case (drugs affected)
MedicationPGx Gene PM Effect
atomoxetine CYP2D6Reduced clearance. Half life ~ 5 times longer
aripiprazole CYP2D680% increase in exposure, half-life twice as long

• Adjust dosage based on PK• Goal to achieve
normalized exposure and ADR risk
• Adjust monitoring expectations for SS delay
• Allow for adequate “wash-out” period
How to apply PGx to atomoxetine therapy?
0 24 48 72 96 120 144 168 192 216 240 264
Time (hrs)
0
300
600
900
1200
1500
Pla
sm
a a
tom
oxetine (ng/m
L)
SS; EM SS ; P M
PM 2 0 mg q 1 2 h
EM
PM 1 0 mg q 1 2 h

UM IM PMCODEINEAMITRIPTYLINECLOMIPRAMINEOXYCODONERISPERIDONEZUCLOPENTHIXOL
PROPAFENONERISPERIDONEVENLAFAXINE
CODEINEAMITRYPTYLINEOXYCODONERISPERIDONETAMOXIFENTRAMADOLVENLAFAXINE
Medications to avoid by CYP2D6 phenotype

RESULTS THERAPEUTIC IMPLICATIONS1 Gene Phenotype Avoid Alternative Consideration Adjust Dosage Adjustment X CYP2D6 *4/*4
Poor Metabolizer
Codeine* Hydrocodone* Oxycodone* Tramadol* Amitriptyline† Venlafaxine† Risperidone† Tamoxifen*
Morphine, non-opioid Hydromorphone, non-opioid Oxymorphone, non-opioid Consider active drug, non-opioid Citalopram, sertraline Citalopram, sertraline Quetiapine, olanzapine, clozapine Anastrozole, exemestane, letrozole
Aripiprazole† Clomipramine† Doxepin† Flecainide† Haloperidol† Imipramine† Nortriptyline† Propaphenone† Metoprolol† Zuclopenthixol
10 mg/day maximum 50% 60% 50% 50% 70% 60% 70% 75%, or atenolol, bisoprolol, carvedilol 50%, or flupenthixol, quetiapine, olanzapine, clozapine
*Lack of efficacy due to failure to produce active metabolite; †Increased risk of adverse events due to diminished drug clearance.
CYP2D6 Poor Metabolizer (PM): This patient’s genotype is consistent with a lack of CYP2D6 enzymatic activity. PMs are at increased risk of drug-induced side effects due to diminished drug elimination of active drugs or lack of therapeutic effect resulting from failure to generate the active form of the drug, as is the case with pro-drugs.
New Draft Report
CONFIDENTIAL COPYRIGHT PGXL LABORATORIES 2012

Fundamental Principles• Genetic variability in drug metabolism significantly increases risk of
ADRs and non-response• Genetic variation can be managed:
• Poor Metabolizers• Decreased maintenance dosing (20 – 70% )• Increased pro-drug dosing• Allow longer time to reach Steady-State• Allow longer time between medication changes• Increased observation • Choose alternative medication
• Rapid metabolizers• Increased dosages (50 – 200%)• Decreased pro-drug dosages

CYP2C9 CELECOXIB CELEBREXIBUPROFEN ADVIL, MOTRINNAPROXEN ALEVEGLYBURIDE DIABETAGLIPIZIDE GLUCOTROLTOLBUTAMIDE ORINASEGLIMEPIRIDE AMARYLPHENYTOIN DILANTINFLUVASTATIN LESCOLLOSARTAN COZAAR CYP2C9/VKORC1WARFARIN COUMADIN
CYP2C19
CLOPIDOGREL PLAVIXCITALOPRAM CELEXAESCITALOPRAM VARIOUS BRANDSIMIPRAMINE TOFRANILSERTRALINE ZOLOFTOMEPRAZOLE PRILOSECESOMEPRAZOLE NEXIUMPANTOPRAZOLE PROTONIXRABEPRAZOLE ACIPHEXLANSOPRAZOLE PREVACIDDIAZEPAM VALIUMNELFINAVIR VIRACEPT
Medications and metabolic pathways

Medications and CYP2D6 pathwayPain Management Psychiatry
Codeine Various brands Amitriptyline Various brandsOxycodone Oxycontin, various Clomipramine AnanfranilHydrocodone Various brands Desipramine NorpraminDextromethorphan Various brands Doxepin SinequanTramadol Ultram, various Imipramine Tofranil Nortriptyline Pamelor, AventylCardiology Fluoxetine ProzacCarvedilol Coreg Paroxetine PaxilMetoprolol Toprol-XL Venlafaxine EffexorPropanolol Inderal, various Risperidone RisperidolPropafenone Rythmol Aripiprazole AbilifyFlecainide Tambocor Zuclopenthixol Various brands Maprotoline LudiomilOther Duloxetine CymbaltaLoratadine Claritin Donepezil Aricept Tamoxifen Various brands







