
K A N G A R O O M OT H E R C A R E F O U N DAT I O N
NEWSLETTERJJ çà¢à¢é „æx¢¢ïÐÝ}¢ì JJ
|¢¢Ú¼è² ÜU¢æx¢¢L }¢¢¼ë „æx¢¢ïÐÝ „æSƒ¢Ý}¢ì
Volume III | March 2016
JJ }¢¢¼ë±ÿ¢:SƒH}¢ì ݱ…¢¼çà¢à¢¢ï: Ÿ¢ïD Sƒ¢Ý}¢ì JJ

OUR INSPIRATION TO PRACTICE KMCB/O SARITHA • D.O.B – 26-07-2-12
GA : 28 WKS • BW : TWIN 1 -650gms • TWIN 2-1.1Kg
MOTHER , FATHER& GRAND MOTHER GIVING KMC FOR TRIPLETS
B/O NAGAMANI • GA: 28 WKS • BW: TRIPLET 1- 1.3Kg , TRIPLET 2- 1.2 Kg , TIPLET 3- 1.1 Kg
B/O ANITHA ,28 WK GA • BW: 800gms B/O RENUKA, 30Wks • BW: 1kg
B/O SUNITHA • GA :- 30WKS • BW: 1 Kg
Continued on back inner cover
1
3
5
7
2
4
6
8

NEWSLETTER | Kangaroo Mother Care Foundation 1
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
From the heart of the Editors
Dear Readers
We are very happy to place this news letter, the first in this new year 2016 and the third of the
series, for your valuable consideration with all the best wishes and request for your increasing
support to spread the theme of Kangaroo Mother Care all over the country through increasing
awareness, improving the quality of practice, promoting research studies relevant to our
country and ultimately making KMC a part of the routine care of all our newborns in all the
settings, which is our noble mission.
In this issue we are presenting to you a success story of the KMC in a district hospital of a
deprived section of Telengana. Against many odds and challenges, a KMC ward has been
created in a small hospital and shown a path to be emulated by others.
In another write up, how KMC is being promoted as a useful modality of transport of weak and
sick newborns in South Africa, has been briefly but effectively narrated. Another interesting
story from USA tells us the systematic approach and effort taken to promote KMC in a unit
from developed countries
A brief note about our activities since launching of KMCF has been reported. We have many
such heart warming and interesting items to present. Due to constraint of space we have
to halt for the time being. Your response as well as active participation through write ups is
eagerly awaited. That will give us a useful feedback for improving and spreading KMC in our
country much better and much faster and help to save many more precious tiny tots.
Please do not forget to see our logo!
Dr. Shashi N Vani Dr. Nikhil M [email protected] [email protected].: 98252 86088 Mob.: 98253 28749

2 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
Kangaroo Mother Care at SCNU NalgondaDr. Damera Yadaiah, Nodal Officer, SCNU, Nalgonda, Telengana
A twelve bedded New born unit of Nalgonda called as NICU, established on March 8th -2008 at District Head quarters, Hospital, Nalgonda.
Unit was established purely on the local interest of DCH’s, Dr.Venkateshwarulu and Medical superintendent Dr. K. Suresh Kumar to improve the survival of new born at Nalgonda district. In earlier days, to refer any sick new born, Niloufer hospital, Hyderabad was the referral centre which is located 125 km away from DH, Nalgonda.
To meet the needs of the babies delivered in and around DH, NLG, the twelve bedded NICU was established. The unit was maintained purely on the voluntary donations given by good Samaritans who got discharged from this unit. Regular auditing was conducted for all the donations received; all the audit records were maintained.
UNICEF started establishing SCNU all over developing countries including India, in order to reduce NMR. First SCNU was started by UNICEF at Bhopal in 2010 April in our country. But, off the record, NICU, Nalgonda was working since 2008. We take pride in saying that ours is the first Neonatal unit of 250 bedded District hospital in the country, which was upgraded on August 15th-2012 with 20 beds with all the facilities.
As more and more preterm and LBW babies survived, we were not able to accommodate all sick LBW babies within the 20 bedded unit. Then, KMC was introduced in 2013, April, as it is a low cost, holistic and safe and effective method to survive preterm and LBW babies. We have been supported by Dr.Srinivas Murki,
Fernandez hospital, Hyderabad, in convincing our SCNU staff regarding important benefits of KMC.
We converted a long corridor of SCNU into a 4 bedded KMC unit, later upgraded to 8 bedded within the limited resources. Initially, we have done KMC for LBW babies like 2.0 kg, 2.1kg babies. But, now, we can’t accommodate babies >1800gms.
Now, we are giving KMC for babies <1800gms and 1200gms as two subsets. Though KMC can be done for term babies, we can’t practice at our unit because of limited resources. Till date, we have given KMC for 500 babies. We are extremely happy to witness the improved survival of preterm, ELBW and VLBW babies and we are following up of the babies who have been discharged with us, and we have very few readmissions with minimum sepsis. We are proud to say, we feed our babies with EBM and Breast milk only.
Average weight gain of our babies is 16mg/kg/day. We have prepared a folder and one small case record, scoring system with codes of KMC to meet the needs of our unit. We have not only been practicing just in the unit, but, we are counseling and encouraging mothers to practice KMC even after going home. We are discharging babies in the KMC position also. We have made our handout in the local Telugu language which contains:
• What is KMC?
• KMC for whom, and when, why and duration of KMC
• Benefits of KMC to baby, mother and community

NEWSLETTER | Kangaroo Mother Care Foundation 3
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
We read out the handout and take the consent from the mother before putting on KMC. We practice KMC not just with mother but also with the other family members when mother is not available.
We have presented papers at state and National NEOCON conferences and won gold medal and best paper awards.
We are glad to say that, Dr. V.K. Bhutani, from Stanford medical school and Dr. John from Harward Medical School visited our unit on May 6th of 2015 and appreciated the work done by the unit and they are interested in doing the project with SCNU Nalgonda On “KMC with CTM Versus Ventilators in the survival of new borns.”
KMC unit at Nalgonda was established on our own with the interest of our staff; we have not been supported by any apex institutions. We feel we will do a better work if we have adequate support from the government of India.
We have created one video to answer all the queries of the mother regarding KMC in the
local language, and we show breast feeding video’s daily along with other entertainment programmes. At times when KMC ward is over loaded, we have eight bedded KMC ward, six semi reclining chairs to keep tiny babies at the side of the warmer at NICU. We also have facility of eight stainless steel chairs for KMC during the time of over loading.
We have started training staff nurses from smaller hospitals like six NBSU›s in practicing KMC and Essential New Born Care. Now, we are practicing KMC at New born stabilization units also
We are concentrating and doing KMC in the post natal ward, strengthening Domiciliary KMC’s and follow up.
We sincerely believe, practicing KMC is very holistic, safe, low cost, easy and effective method to improve the survival of preterm and LBW babies. We suggest all New born units across the country should start practicing KMC, the more humanized care.
Thank you.
1%
3%
6%
20%
70%19
20

4 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
21
22
23
24
25

NEWSLETTER | Kangaroo Mother Care Foundation 5
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
PROVIDING FRUITS & SNACKS TO MOTHERS
MOTHERS BEING SHOWN DOING HOUSEHOLD CHORES
• Practising KMC is Our Passion
• KMC is Baby’s Right Mother’s Delight
• We witnessed better outcomes in LBW & Pre-term Babies by Practising KMC
• KMC is Holistic, Humanized, Cost Free Strategy in Developing Countries where need is Great Resources are Scarce.
26
27
28
29
6 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
What is safe transfer???
What is safe transfer???
Inter-facility KMC ....Saving babies
Vanessa Booysen National Newborn Care Lead Facilitator
LINC University of Limpopo
REFERRING STAFF RECEIVING STAFF
Doctor's duties: Doctor's duties:* calls NICU at next LOC *Determine the most appropriate bed availabil ity and
* Discusses patient details with receiving doctor *Inform the referring doctor* Inform parents of tranfer including information pertaining to: *Inform the transport team
Reason for transport, medical condition, implications
* Direct the ambulance to the hospital where a bed is available
When transport will occur* Will advise the ambulance service of the clinical issues and the level of care that the neonate requires.
Length of time transport will take
Mode of travel
* Prepare patient documentation and referral letter yes no
Nursing manager's duties: Nursing manager's duties:* Staff and family members who may accompany the newborn during transport
* Will notify their admitting department of the newborn’s admission and name of the responsible doctor.
* Visiting hours and telephone number of the receiving hospital
* Will notify the receiving hospital of the time of departure and estimated time of arrival.
* Provide labelled samples to the ambulance team of: neonate stable neonate unstable * Will call parents to notify them of the newborn’s arrival at the receiving centre.
- Maternal blood sample (clotted) - Unpreserved placenta if available
* Collate all documentation (see below)
Tic Mothers Antenatal record (BANC booking card)
Newborns Road To Health booklet with HIV status
Nursing notes
Doctor’s notes/consultation and transfer summary
Relevant lab reports and x-rays
Medicine Drug Chart
Documentation/information to accompany the patient will be prepared by the referring staff and should include (when available) a legible copy of the following:
Algorithm 1: Referral and Transfer of patients
neonate managed by referring doctor
till bed becomes
available
receiving doctor directs the
ambulance to a hospital where a bed is available
OR
neonatally trained paramedic
dispatched to referral hospital
neonate trasferred in KMC if possible
by ambulance staff
Receiving hospital called for a neonatal transfer
ill neonate identified for referral
bed available at receiving hospital
transport ambulance contacted
stabilize if possible
COMMUNICATION communication
communications • On call staff
• Ambumedics
• Referral hospital
• Staff : doctors / nurses
• Follow - up
DOCUMENTATION TO ACCOMPANY BABY
• Mom: BANC Card • Baby: RTHC • NOTES
– Nursing – Doctors
• Medicine chart • Relevant blood results
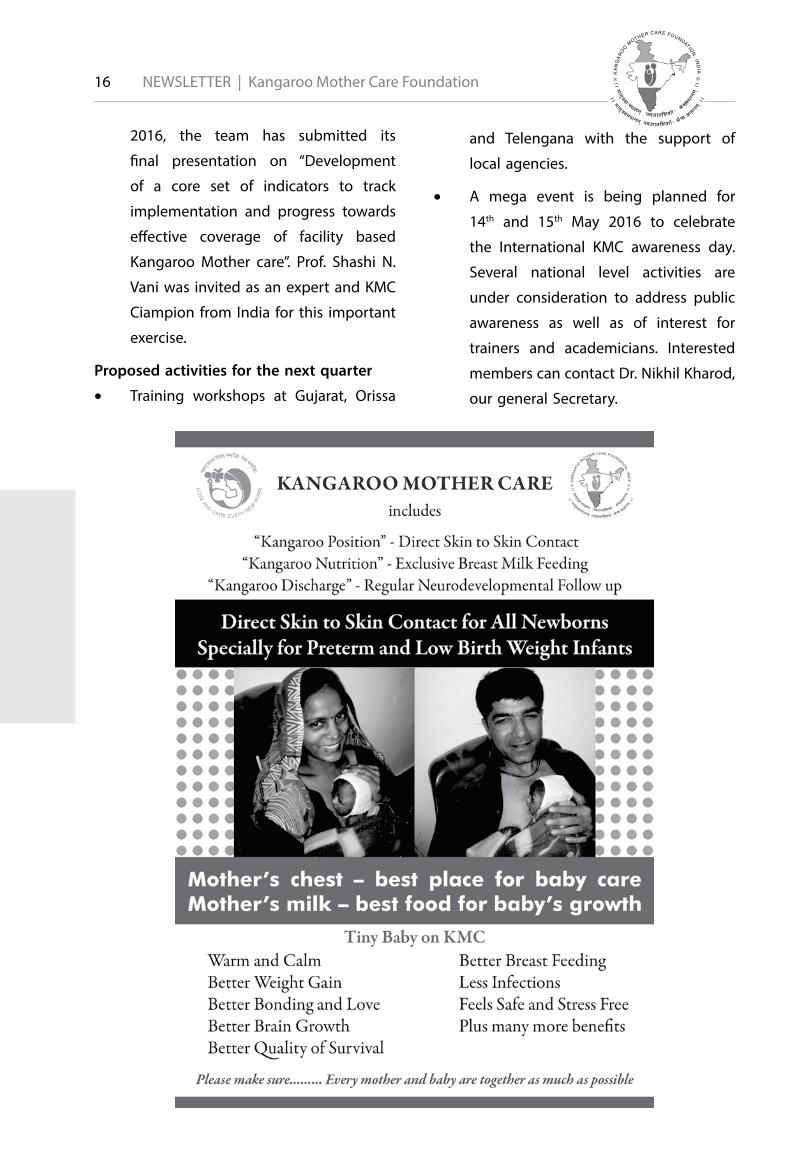
Bogota Declaration - 1989
Kangaroo Mother Care is a Basic Right of the newborn, and should be an
integral part of the management of low birth weight and full term newborns,
in all settings and at all levels of care
in all countries.
INTERNATIONAL KMC FOUDATION
1 4
2 5
3 6
NEWSLETTER | Kangaroo Mother Care Foundation 7
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
...AT ALL LEVELS
...IN ALL SETTINGS
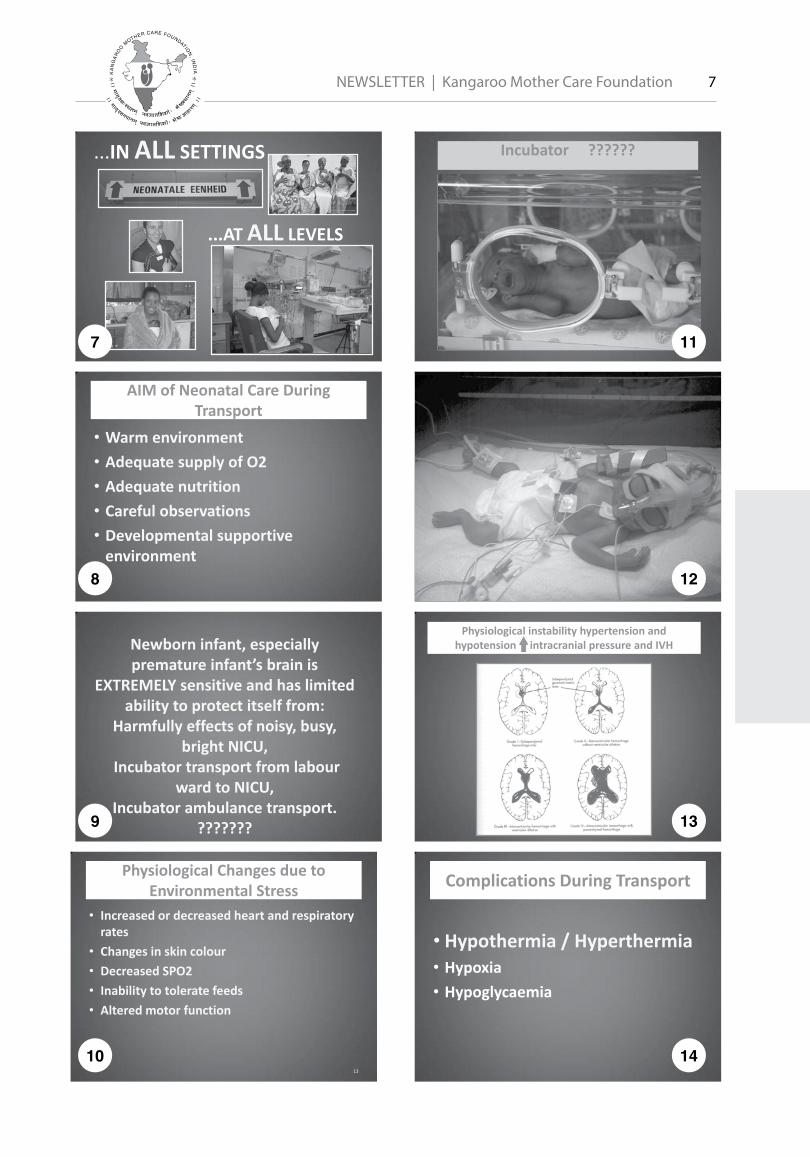
AIM of Neonatal Care During Transport
• Warm environment • Adequate supply of O2 • Adequate nutrition • Careful observations • Developmental supportive
environment
Newborn infant, especially premature infant’s brain is
EXTREMELY sensitive and has limited ability to protect itself from:
Harmfully effects of noisy, busy, bright NICU,
Incubator transport from labour ward to NICU,
Incubator ambulance transport. ???????
Physiological Changes due to
Environmental Stress • Increased or decreased heart and respiratory
rates • Changes in skin colour • Decreased SPO2 • Inability to tolerate feeds • Altered motor function
13
Incubator ??????
Physiological instability hypertension and hypotension intracranial pressure and IVH
Complications During Transport
• Hypothermia / Hyperthermia • Hypoxia • Hypoglycaemia
7
8
9
10
11
12
13
14
8 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
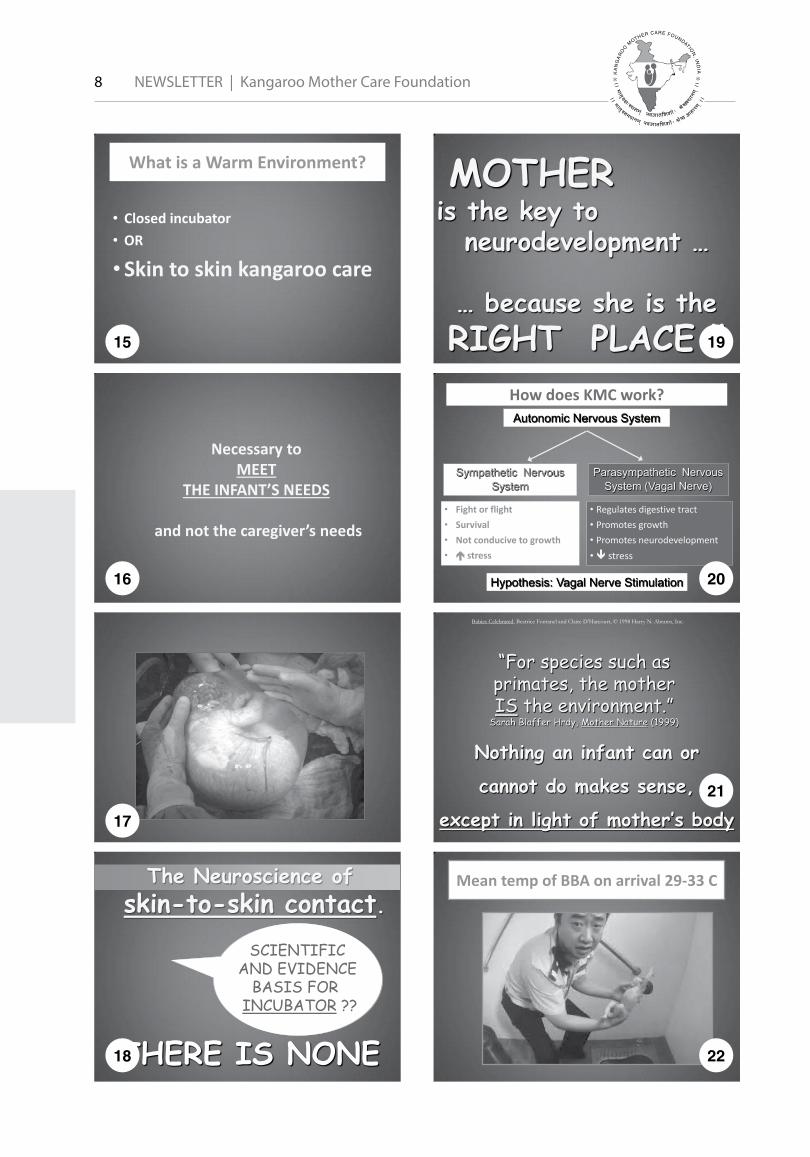
What is a Warm Environment?
• Closed incubator • OR
• Skin to skin kangaroo care
Necessary to MEET
THE INFANT’S NEEDS
and not the caregiver’s needs
The Neuroscience of skin-to-skin contact.
THERE IS NONE
SCIENTIFIC AND EVIDENCE
BASIS FOR INCUBATOR ??
MOTHER is the key to
neurodevelopment …
… because she is the RIGHT PLACE !!
How does KMC work? Autonomic Nervous System
• Regulates digestive tract • Promotes growth • Promotes neurodevelopment • stress
• Fight or flight • Survival • Not conducive to growth • stress
Sympathetic Nervous System
Parasympathetic Nervous System (Vagal Nerve)
Hypothesis: Vagal Nerve Stimulation
“For species such as primates, the mother IS the environment.”
Sarah Blaffer Hrdy, Mother Nature (1999)
Babies Celebrated, Beatrice Fontanel and Claire D’Harcourt, © 1998 Harry N. Abrams, Inc.
Nothing an infant can or
cannot do makes sense,
except in light of mother’s body
Mean temp of BBA on arrival 29-33 C
15
16
17
18
19
20
21
22

NEWSLETTER | Kangaroo Mother Care Foundation 9
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
• SUBJECT: GUIDELINES FOR THE TRANSPORTING OF INFANTS IN
KMC Kangaroo Mother Care, Skin to Skin POSITION EMS Maternal Health Circular No. 1 of 2013 KMC correctly done is an alternative, safe and efficient mode of transport for
all infants but especially for the VLBW (very low birth weight) infant. As a province we have decided that infants will no longer routinely be transported in a transport incubator, either for down- or up referral.
IT IS COMPULSORY THAT ALL BABIES MUST BE TRANSPORTED SKIN TO SKIN IN KMC POSITION BY THE MOTHER or family member or EMS.
Exceptional conditions where the baby can be transported in a transport incubator:
An Intubated and ventilated baby where monitoring of this baby might be a challenge, and there might be a risk of extubating the baby.
Special conditions that the MO motivates for incubator transport eg. Abdominal wall defects like Exsomphalos, Gastrochesis etc.
Control Center/Room Responsibilities:
The following criteria must be adhered to when a call for BBA is received:
• The EMS CONTROL CENTRE call receiver must
immediately advise the caller that the baby is put naked on his stomach against the mother’s naked chest, thus skin to skin. The baby’s arms are bent so that his hands are in front of his face. Place a warm a cap on the baby’s head. Turn the babies head to the side and make sure that his airway is open. Cover the mother and baby with a blanket while waiting for the ambulance.
BBA Skin to skin Kangaroo Mother Care
• KMC is the early, prolonged and
continuous skin-to- skin contact between a
mother and her newborn infant
Call center operators were trained in HBB
All Ambulances must have a KMC kit:
• A woolen cap (Ante-natal clinics to assist in
educating mothers in KMC) • A see through plastic bag – 30cm X 20cm.( Please
note that the baby is put FEET FIRST into the plastic bag with the Baby’s HEAD OUTSIDE THE BAG) ILCOR GUIDELINE
• A KMC wrap or draw sheet to tie the baby to the mother
• Infant stick-on under armpit thermometers (Traxit)
WET RESUSCITATION • STABILIZATION OF PREM
– Babies (< 2 kg) – Wrap in food-grade, heat-resistant
plastic bags/wraps without drying infant, HAT !
23
24
25
26
27
28
29
30

10 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
Support from Health Staff (facility and
community based) • Explain the concept of KMC to the mother
and demonstrate how it is done • Explain the benefits of KMC • Integrate family members like father,
grandmother, aunts, or other person, depending on the cultural set up • Help the mothers with any problems related
to positioning, feeding
LOADING/ POSITIONING INTO KMC
• Hand hygiene • Secure mother to seat or stretcher
• Secure infant to BARE CHEST of MOTHER, father, granny, EMS
• Secure lines and tubes to prevent dislodgement. Stick onto shoulder of person holding baby.
• Tie KMC Wrap around mother and baby • Infants Airway open • Hat on head
Putting baby skin to skin for transport
• Temp Regulation better on HIGHER part of chest
• Place baby BETWEEN breasts
Breast Thermography
Putting baby skin to skin for transport
• Chin of Mother/ Father/ EMS must touch the head of baby
• Baby’s head in a sniffing position to keep airway open at all times
Putting baby skin to skin for transport
Tie baby line from ear to nose • Take wrap under mothers arms. • Tie tight. Baby says “UUHH”! • Tie knot at the back of baby’s head • Tie the binder firmly enough so that the baby will not slide out • Make sure that the tight part of the cloth is across the baby’s chest • The baby’s abdomen should not be constricted • Baby should have enough room for abdominal breathing
Putting baby skin to skin for transport
• Examples of different binders :
31
32
33
34
35
36
37
38

NEWSLETTER | Kangaroo Mother Care Foundation 11
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
Putting baby skin to skin for transport
Mother positioned in semi fowlers position Sontheimer, D; 2002
Mother with infant at arrival after kangaroo transport in an ambulance
over a long distance (400 km, 5 hours).
Mother with infant after kangaroo transport (40 minutes). An additional blanket is placed on top of
the mother and infant.
Father and infant after kangaroo transport (back transfer, day 32, 1580 g,
90 km, 80 minutes).
Mother with infant during kangaroo transport in a helicopter (back transfer
after abdominal surgery).
39
40
41
42
43
44
45
46

12 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
EMS Responsibilities during Transport
• a) Secure the mother onto the ambulance stretcher. • b) The neonate needs ongoing observation for the entire
duration of transport. • The AMB 2 as well as the Neonatal Transport Observation
chart, has to be completed by the attending EMS crew/Prof Nurse for all babies transported during the first 28 days after birth, until arrival at the referral hospital. (Eventually this form will be filled out in Triplicate.)
• Newborn babies and premature babies cannot maintain their blood sugar especially if they are cold, and therefore they need to be kept warm and get breast milk early. Either by suckling on the mothers breast, or drops of breastmilk in a syringe.
Baby Weight Temp before transfer
Temp @ receiving site
Time of Transport
1 3.0kg 35.2 35.6 30 min 2 2.0kg 37.0 37.1 23 min 3 1.0kg 34.0 37.0 27 min 4 1.0kg 36.0 37.0 1hr 30 min 5 3.0kg 35.4 36.6 1hr 10 min 6 3.0kg 36.3 36.3 5 min 7 2.8kg NO Hat 36.5 36.0 40 min 8 2.4kg 37.0 37.0 35 min 9 2.9kg 36.0 36.1 35 min
10 Prem 35.7 36.5 1hr 10 min 11 Prem 35.7 36.5 1hr 5 min 12 3.2kg
KMC done and baby suckling on breast on
route
33.3 36.1 45 min
KMC: Benefits in the ambulance for the Baby
• Improved cardiac & respiratory stability • Good temperature regulation • Decreased energy expenditure • Neurological protection (from stress)
–Improved neurodevelopment –Organized electrical brain activity
Physiological stability
In KMC: • Normal cycling • Non-chaotic pattern
48 hour baseline chaotic pattern of activity and quiet HR & RR
Pre-KC KMC
“For species such as primates, the mother IS the environment.”
Sarah Blaffer Hrdy, Mother Nature (1999)
Babies Celebrated, Beatrice Fontanel and Claire D’Harcourt, © 1998 Harry N. Abrams, Inc.
Nothing an infant can or
cannot do makes sense,
except in light of mother’s body
KMC for transfers and at discharge
KMC IS GOOD FOR:
• BABIES
• MOTHERS
• HEALTHSERVICE
• EMS
HUMANITY FIRST TECHNOLOGY SECOND
SKIN-TO-SKIN CONTACT
47
48
49
50
51
52
53
54
NEWSLETTER | Kangaroo Mother Care Foundation 13
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
Florence Nightingale
• Put the patient in the
best environment for nature to act upon him
Incubator ??????
Implementation
Everybody is in favour of progress, Nobody likes change !
Who will climb on board ????
To Dr Nils Bergman and Elise van Rooyen for igniting the passion and fire in
me towards KMC and sharing their expertise and slides with me
55
56
57
58
59
60
14 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
Printing and distribution of KMC education
charts
• Gujarati (5000) and English (3000)
• Distributed free of cost all over Gujarat
and different states of India through
various training workshops, KMC
promotion programs, CMEs of different
professional bodies and voluntary
health care organizations to doctors,
nurses, consultants, and community
health workers of all cadres in urban as
well as rural and tribal areas
• Charts are being prepared in other
languages including Hindi, Oriya and
Telugu.
Quarterly Newsletter
• The first issue was released formally on
the day of launching KMCF by the Hon.
Minster of Health for Gujarat, Shri Nitin
Patel.
• Second one was released in month of
Nov. 15 and the third is the current
one.
• This quarterly news letter is being
distributed free of cost to academic
institutions like medical and nursing
colleges and schools, KMC champions
all over the country departments of
health and family welfare of Gujarat
and India and NH missions of different
states. Gradually the scope of content
and number of copies for distribution
Activities of Kangaroo Mother Care Foundation in year 2015
(After launching on 2nd August 2015)
are being increased..
• News letter covers articles related to
different aspects of KMC including
general information, experiences of
different institutions and individual
workers, research articles, recent
developments, events and various
community experiences also.
• It carries one section in local language.
So far it has been in Gujarati. In future
we plan to include articles from other
languages also.
Training Activities of KMCF
• Following KMC training workshops
have been conducted with the support
of KMCF
• A) At Ahmedabad, following the
launching of KMCF during the world
breast feeding promotion week, for
doctors, nurses, faculty members of
nursing colleges, schools, ANM training
centers, trainers of AWWs and ASHA
workers and others ( About 400)
• B) At Bhubaneshwar, Orissa as a pre
conference activity of NNF annual
convention
• C) At Rajkot, Gujarat as a preconference
workshop of Annual conference of AOP
Gujarat
• Dr. Shashi N. Vani as one of the chief
faculty member at Full day CME

NEWSLETTER | Kangaroo Mother Care Foundation 15
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
for nurses on Essential Newborn
Care including KMC in NNF national
convention at Bhubaneshwar
• Dr. Nikhil Kharod as the faculty for IYCF
training including KMC in district of
Anand for AWW workers ( 5 sessions)
• Dr. Deepa Banker during world breast
feeding promotion week for the
urban health workers of Ahmedabad
Municipal Corporation
Public Awareness Programs for KMC
• Dr. Parag Dagli, Dr. Ashish Mehta, Dr.
Abhishek Bansal, Dr. Anuj Grover, Dr.
Viren Doshi and Dr. Shashi N. Vani
included KMC in different public
functions.
Health Education Exhibition on KMC
• Nursing School of P S Medical College
arranged an excellent exhibition on
KMC with attractive models, charts and
other visuals and arranged for guided
tour of the exhibition with explanatory
remarks for public visitors at
Ahmedabad management association
hall.
International Activities
• Dr. Shashi N. Vani Invited as a keynote
speaker at KMCF conference of South
Africa at Port Elizabeth, near Cape
Town in Nov. 2015 her presentation
on recent study on Home based KMC
in Gujarat was very well accepted and
appreciated.
• She also participated as faculty in
workshop on Helping Babies Breath
during the same conference..
• Dr. Narendra Vani and Dr. Shashi Vani
had a formal meeting and discussion
with the trustees of KMCF South
Africa Several innovative projects were
discussed..
• The next International Conference
of KMC is scheduled at Trieste, Italy
from 14th to 17th Nov. coinciding with
the international prematurity day on
17th Nov. This meeting also marks
the completion of 20 years after the
first International meeting of KMC
during1996. Dr. Shashi N. vani was
invited to attend the first meeting and
she presented her first study paper on
KMC which was conducted as a part
of multi centric study. In the meeting
of 2016 trustees of KMCF Dr. Shashi
N.Vani and Dr. Deepa Banker have been
invited to attend and also participate
in the pre-conference workshop as
faculty members to present on gains
and challenges of KMC in India. .
Dr. Rekha Udani from Mumbai, our
national advisor, has also been invited
for this workshop and conference. Dr.
Udani is a member of the advisory
committee of International network
of Kangaroo Mother Care , who are
the main organizers of these biannual
conferences.
• Save the Newborn Lives (SNL) invited
experts and KMC champions from
different countries for meetings at
Washington D.C., USA and Kigali,
Rewanda in the years 2014 and
2015. Recently, in month of Feb.
16 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
2016, the team has submitted its
final presentation on “Development
of a core set of indicators to track
implementation and progress towards
effective coverage of facility based
Kangaroo Mother care”. Prof. Shashi N.
Vani was invited as an expert and KMC
Ciampion from India for this important
exercise.
Proposed activities for the next quarter
• Training workshops at Gujarat, Orissa
and Telengana with the support of
local agencies.
• A mega event is being planned for
14th and 15th May 2016 to celebrate
the International KMC awareness day.
Several national level activities are
under consideration to address public
awareness as well as of interest for
trainers and academicians. Interested
members can contact Dr. Nikhil Kharod,
our general Secretary.

NEWSLETTER | Kangaroo Mother Care Foundation 17
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
Neonatal intensive care units (NICUs) are intense environments in which staff work diligently to protect and strengthen fragile infants who are receiving complex medical care and encountering a variety of stressors.
Many premature infants live inside an isolette—an incubator with armholes so that the baby can be reached without significantly disturbing the controlled environment that includes endotracheal tubes, umbilical arterial or venous lines, and cardiac and temperature monitors.
Within this environment, unless great care is taken, such simple tasks as positioning the infant, changing his or her diaper, and checking his or her temperature can cause bradycardia (abnormally slow heart action), dangerous oxygen desaturation, and oral aversion.
An unfortunate result of this protective environment is that it creates barriers to touch for infants and parents. Bonding, attachment, even breast milk production are affected by the stress of an infant’s residence in the NICU.
“Kangaroo care” (KC) is the practice of holding an infant who is wearing only a diaper skin-to-skin, typically chest-to-chest, with his or her parents. The intervention has been shown by many studies (see “Resources”) to help mitigate stress and bonding issues.
The literature also documents the challenges, however, of adapting NICU culture to the demands of KC implementation. It can take
3 or even 4 people to successfully prepare and transfer an infant from isolette to parent, from bed to skin position. For staff, this can mean that family members are in the NICU for hours—as opposed to minutes in times past—with the potential disruption to NICU operations that that entails.
Thus, while the benefits of KC are well-documented, implementing it presents a variety of challenges. The following is an account—from conception through results and lessons learned—of our experiences with KC at Niswonger Children’s Hospital in Johnson City, Tennessee, where I am a physical therapist (PT) in the NICU and am a member of an interdisciplinary developmental care team that also has implemented safe sleep, “save the septum,” and head positioning initiatives in the NICU.
Jumping Into Kangaroo CarePTs and their NICU colleagues promote a practice that benefits premature infants and their parents.
By Karen Speropulos, PT, MPT, PCSNovember 2015

18 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
Identifying a Priority
Niswonger is part of the Mountain States Health Alliance, which consists of 13 hospitals that serve a total of 29 counties in Tennessee, Virginia, Kentucky, and North By Karen Speropulos, PT, MPT, PCS November 2015 Carolina. The alliance’s integrated health care
and Training,” a fact sheet produced by APTA’s Section on Pediatrics:
• Develop and implement a plan to prevent neurobehavioral disorganization and complications from prematurity in multiple systems.
• Design, implement, and evaluate the efficacy of intervention plans in collaboration with the family and medical team.
• Incorporate evidence-based literature into neonatal practice.
KC is a proven, evidence-supported activity that positively affects outcomes of infants in the NICU. (See “Benefits of Kangaroo Care.”) Among its many benefits, it helps infants reach physical therapy goals related to neurobehavioral organization. In order to increase the frequency of KC and bring about positive change for infants and families, PTs in NICUs must collaborate closely with the entire medical team.
Examining the Evidence
Once the developmental care team identified KC as an area of emphasis, a literature review was conducted to provide team members with evidence-based knowledge. Raquel submitted a request to our medical library for a PubMed search of the terms “kangaroo care” and “skin-to-skin care.” The search was limited to articles written in English in the past 5 years. It produced a list of 254 articles which was shared with all team members via email.
Each member then chose 5-12 articles of interest to read and share with the others. For example, the team dietician selected articles related to breastfeeding and breast milk
Prizes awarded to parents on International Kangaroo Care Day.
delivery system includes primary/preventive care centers and numerous outpatient care sites.
Our 36-bed level III NICU—primarily an open-bay layout, with 7 additional private-care rooms—is overseen by the developmental care team mentioned previously, which in turn is led by Raquel Keithley, PT, DPT, PCS, and includes, besides me, several nurses, a speech-language pathologist, a dietitian, and a nurse practitioner. We meet monthly to identify care strategies that we believe could be improved, and to implement necessary changes. In February of this year, we determined that KC should be emphasized within the NICU. Because of the strong link between KC and breastfeeding, a NICU lactation consultant was added to the care team for this project.
In our role as neonatal PTs, Raquel and I focused on the following responsibilities, as outlined in “Neonatal Physical Therapist Practice: Roles

NEWSLETTER | Kangaroo Mother Care Foundation 19
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
production. We did not review all 254 articles. Once the team had thoroughly reviewed the presented literature, we considered the reasons that KC had not been occurring with sufficient frequency in our NICU.
We determined that barriers to KC in Niswonger’s NICU included:
• Lack of staff knowledge of its benefits,
• Lack of sufficient equipment, and insufficient familiarity with the equipment,
• Lack of interest in and knowledge of KC among family members, and
• Lack of staff motivation to attempt transfer of medically fragile infants from isolette to skin-to-skin position.
Many of the barriers to KC identified by our team were among those noted in the literature. One study (see “Strand” in “Resources”) cited the benefit of educating staff by teaching theory and providing guidelines, as opposed to overwhelming them with literature. The developmental team adopted this practical approach. Our team’s goal was to minutely absorb the literature, but when it came to encouraging care providers to implement KC, we focused on the benefits and the steps needed. Our overarching goal was to change the frequency of skin-to-skin care in our NICU from occasional to an “always event” and standard of care.
Developing a PlanHaving identified KC as our area of focus during that February meeting, the team set a goal of implementing changes during the week leading up to May 15, which is International Kangaroo Care Awareness Day. This gave us only 3 months to prepare and
carry out our plan.
We reviewed several helpful Internet sites for implementation ideas. The March of Dimes’ Close to Me NICU family support program provided valuable information on equipment and tools, as well as practical information for staff. The “Kangaroo Challenge” issued by Toronto’s Sunnybrook Health Sciences Centre, meanwhile, inspired our own “kangaroo-a-thon.”
We first needed to determine the current frequency of KC within our NICU. All we had to go on initially were the anecdotal observations of team members. So, we conducted a baseline audit. Over the course of an entire week, we recorded only 5 hours of KC being done. Determining that setting a numeric goal would be a good platform for monitoring and implementing change, we set our sights on 100 hours of KC to be completed in the week leading up to May 15. Dubbing it a kangaroo-athon, with associated visuals and prizes, would make this shift in care fun for both staff and families, we hoped.
The neonatal nurse practitioner on our team developed KC guidelines, including eligibility criteria, transferring procedures, when/why to terminate KC, and how to document it. Once these guidelines were approved by the NICU leadership, they were distributed to current staff and added to orientation for new staff.
Recognizing the need for additional equipment to support KC, the team submitted a request to the Mountain States Foundation, a local hospital-affiliated organization created to advance quality health care in our region. We received $2,000 to purchase extra-large zero-gravity chairs for the comfort of parents.

20 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
We purchased a large number of “KangaROO Kuddlers”—soft, lightweight cotton wraps designed to fit snugly around the parent and baby—to enhance positioning during KC. We bought hand-held mirrors to help parents’ view their infant against their chest. We also purchased charms in the shape of a kangaroo as keepsakes for families of their first KC experience.
The developmental care team posted and populated bulletin boards around the unit to educate families, visitors, and staff about the use and benefits of KC. On 2 of the boards we also posted research highlights on the benefits of KC. The most centrally located bulletin board served as a game board for the kangaroo-a-thon, with 100 spaces to be filled with cartoon stickers of kangaroos. It would serve as a visual reminder of our goal and our progress toward 100 hours of KC in 1 week.
The developmental care team used small personal donations to purchase prizes for families participating in KC—40 plushtoy kangaroos, 15 kangaroo charm bracelets, and 50 infant onesies imprinted with our hospital logo and the phrase “I’ve Been Roo’d!”
Physicians and nurse practitioners contributed funds to purchase spa and restaurant gift certificates for staff assisting in getting KC for infants. Their names were entered into drawings that encouraged participation and awareness of KC efforts throughout the NICU.
Each time a NICU staff member assisted with KC—whether for his or her own assigned patient or by helping another team member—he or she filled out a ballot. On the ballot were KC-related questions regarding such matters as whether an assistant was needed
to perform the transfer, how much respiratory support the infant needed, and the amount of time the family spent in KC. The care also had to be properly documented on the infant’s chart—including information about length of time, method, and baby’s tolerance—in order for providers to be eligible for prizes.
Prior to KC week, we monitored the amount of KC that was occurring, to serve as baseline information. This would be our basis for comparison with the week of the kangaroo-a-thon, allowing us to assess how successfully our education and promotion of KC had increased its practice in the NICU. The charge nurse for each shift collected this information.
Finally, in preparation for the week leading up to International Kangaroo Care Awareness Day, the developmental care team posted information on various social media websites and on our hospital website about the benefits of KC. We entered a contest sponsored by Nurtured By Design, designers of ergonomic devices for babies, and received honorable mention for our submitted photo. Further publicity came when a local news station ran a Mother’s Day story about 1 family’s experience of KC while in our ICU.
Implementing Kangaroo Care
Prior to and beginning at the start of the day shift on Mother’s Day, Sunday, May 10, we took the following steps:
• Emails were sent to NICU staff about the benefits of KC.
• Short quotes and brief facts about KC’s benefits were placed in prominent locations around the unit.
• The 3 bulletin boards were populated and
NEWSLETTER | Kangaroo Mother Care Foundation 21
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
placed in the NCU 1 week before KC week to help build awareness. Again, 2 of the boards included research results and the other illustrated the kangaroo-a-thon.
• Plush kangaroos and a brief handout about KC were distributed to all parents in the NICU at the beginning of the week as a “kick off,” to raise awareness and encourage KC.
• Ballots were collected and tallied at the end of each shift, and the game board was constantly updated with the number of KC hours completed. One small kangaroo sticker was placed on the game board for each hour of KC, to serve as visual encouragement and a challenge to families and staff to reach the 100-hour goal.
• PTs and other developmental care team members saw to it that new equipment purchased for KC was available and used correctly.
At the end of the week, on International Kangaroo Care Awareness Day, the onesies with the hospital logo and the phrase “I’ve Been Roo’d” were given to all participating families in the NICU. The 15 families with the most KC time also received a kangaroo bracelet charm. The 3 staff members who participated in the most KC time were given incentives.
Seeing the ResultsThrough the first 6 days of the KC promotion, 68 hours of KC had been logged in the NICU. The game board was not complete. We had started the kangaroo-a-thon on Mother’s Day, a Sunday, and had planned to conclude on Friday, which was International Kangaroo
Care Awareness Day. This plan excluded some weekend staff, as well as families visiting over the weekend. When we realized we had not met our goal and had excluded some people, we decided to extend game board eligibility over the weekend.
We concluded our data collection at the end of the Sunday night shift on May 17 with the game board complete—and then some. Over the course of those 8 days, 110.5 hours of KC time had been completed—a 20-fold increase from the 5.5 hours recorded during the observation week.
We were pleased with the number and the wide variety of family members and staff who participated in KC during the week
of the kangaroo-a-thon. Our hope was that this exposure and experience would increase the likelihood that both families and caregivers would revisit KC many times over.
Reviewing the PositivesThe developmental team was gratified by the increased use of KC by families. We noted that bedside registered nurses now were encouraging parents to plan for KC during their next visit when they called to check on their infant. Non-bedside staff were quick to help secure needed equipment. Family members were asking about KC more frequently.
Simply seeing another parent hold his or her child skin-to-skin encourages other parents to ask questions about holding their own infant this way. One NICU nurse commented, “One thing that has helped is, parents are more aware, and thus are asking for KC more frequently.”
During KC week, a mother commented, “I’m an educated woman, and I know that
22 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
kangaroo care is a good thing, but I won’t ask for it, because the nurses are so busy! But I love that they are actively making plans to help me hold my baby.”
Finding Room for ImprovementWe identified some factors that inhibit KC in our NICU. We learned, for example, that KC can be difficult in the open-bay area for logistical reasons—including the fact that, per current policy, the unit is closed to family members during new-patient admissions and procedures. The unit manager acknowledged the need to reconsider this. One possible solution would be to allow parents to continue KC with their infants behind a screen while other activities are being conducted in the wider openbay area.
Also, data revealed that significantly fewer KC hours were occurring during the night shift. The team was unable to pinpoint the reason, but we discussed some possibilities. The absence of a representative from the developmental care team during the night shift may have been a factor. (The 1 night shift nurse on the developmental care team did not work during the week of the kangaroo-a-thon.) Another possibility is that parents simply are tired and not as interested in KC during the evening hours. The team continues to consider how to best to address the culture of night shift regarding KC.
Onesies that had not been distributed during KC week were displayed and made available in the ensuing weeks for families that chose to engage in KC. The garments’ presence also encouraged families to ask about KC, and reminded participants to continue this effective intervention. The bulletin boards remained on display for several weeks, as well.
PTs in our NICU now regularly include KC education and discussion as part of their intervention with families.
Starting a Kangaroo Care ProgramOur developmental care team has a few recommendations, based on our experiences, for other facilities interested in starting a similar program:
• Give yourself more than the 3 months we gave ourselves to prepare for and roll out your KC event.
• Survey NICU staff. Ask whether they have any personal hesitations about KC, and if they see any environmental or equipment barriers to KC at your facility.
• Focus on staff education on KC, with an emphasis on practicality.
• Plan to have PTs and other developmental care team members available during both day and night shifts to ensure KC continuity, and sufficient assistance with complex patient transfers.
• Be certain to obtain accurate and complete baseline data, in order to truly discern the project’s impact and develop appropriate follow-up plans.
We also recommend a longer period for the kangaroo-a-thon itself. While 1 week was enough time to prove that our unit is capable of markedly increasing KC hours, it was not long enough to definitively change behaviors. Several weeks later, it seemed that staff and families had largely returned to old habits of less time in KC. One month to 6 weeks might be a better time frame within which to promote lasting adaptation of this practice.
It is vitally important to involve representatives from all care disciplines, including therapists, nurses, nurse leaders, respiratory therapists,
NEWSLETTER | Kangaroo Mother Care Foundation 23
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
dieticians, nurse practitioners, and physicians. Such a multidisciplinary approach better ensures encouragement of KC across the spectrum, as well as better problem-solving during complex isolette-to-skin transfers.
Looking ahead to next year, our unit is considering a partnership with the March of Dimes Close to Me program, which takes a formalized approach to KC equipment acquisition and nursing education.
Karen Speropulos, PT, MPT, PCS, is a NICU PT and developmental care team member at Niswonger Children’s Hospital in Johnson City, Tennessee. Also contributing to the article was Raquel Keithley, PT, DPT, PCS.
Resources
Bloch-Salisbury E, Zuzate I, Indic P, et al. Kangaroo care: Cardiorespiratory relationships between infant and caregiver. Early Hum Dev. 2014; 90(12):843-850.
Conde-Agudelo A, Diaz-Rosello JL. Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane Database Syst Rev. Apr 22;4:CD002771.
Cooper L, Morrill A, Russell RB, et al. Close to me: enhancing kangaroo care practice for NICU staff and parents. Adv Neonatal Care. 2014;14(6): 410-423.
Engler AJ, Ludinton-Hoe SM, Cusson RM, et al. Kangaroo care: national survey of practice, knowledge, barriers, and perceptions. MCN Am J Matern Child Nurs. 2002;27:146-153.
Feldman R, Eidelman A. Skin-to-skin contact (kangaroo care) accelerates autonomic and neurobehavioural maturation in preterm infants. Dev Med Child Neurol. 2003;4:274-281.
Head LM, The effect of kangaroo care
on neurodevelopmental outcomes in preterm infants. J Perinat Neonatal Nurs. 2014;4:290-299. Heidarzadeh M, Hosseini MB, Ershadmanesh M, et al. The effect of kangaroo mother care (KMC) on breast feeding at the time of NICU discharge. Iran Red Crescent Med J. 2013;15(4):302-306.
Strand H, Blomqvist YT, Gradin M, et al. Kangaroo mother care in the neonatal intensive care unit: staff attitudes and beliefs and opportunities for parents. Foundation ACTA Paediatrica. 2014;103: 373-378.
Benefits of Kangaroo Care
For the baby:
• Stabilization of the heart rate
• Improved (more regular) breathing pattern
• Faster weight gain
• Decreased crying
• More successful breastfeeding episodes
• Earlier hospital discharge
• Improved oxygen saturation levels
• Improved sleep-wake cycle
For the parent:• Improved bonding, feelings of closeness
with baby
• Increased breast milk supply
• Increased confidence in ability to care for baby
• Increased sense of control
Furthermore, the evidence suggests that KC positively affects body systems that PTs always must consider.
Per Bloch-Salisbury et al in the Resources box on page 30, there is evidence of improved regularity and stabilization in the infant’s cardiovascular system, and of a decreased
24 NEWSLETTER | Kangaroo Mother Care Foundation
KA
NG
AR
OO
MOTHER CARE FOUNDATIO
N, IN
DIA
JJ }¢¢¼ ë±ÿ¢:S‰¢H}¢ ì ݱÁ¢¢¼çà¢à¢¢ï :
Ÿ¢ ïD
S‰¢¢Ý
}¢ì J
J
JJ }¢ ¢¼ ëS¼ÝТÝ}¢ ì ݱÁ¢ ¢¼çà¢à¢ ¢ ï : Ÿ¢ ïD ¥
¢ã
¢Ú}¢ ì J
J
✻ ✻
need for oxygen supplementation in the pulmonary system.
Per Head, there is evidence of a positive if indirect effect on the infant’s neuromuscular system, in that KC can improve general organization by enhancing the baby’s deep-sleep cycle.
Per Feldman and Eidelman, there is evidence that infants experience decreased stress during KC, which helps their neuromuscular system.
Per Conde-Agudelo and Diaz-Rosello, there is evidence of a positive if indirect effect on the
infant’s musculoskeletal system due to the promotion of neonatal flexion while parent and baby are in skin-to-skin position. Overall, these researchers say, the infant benefits from decreased risk of infection, improved likelihood of breastfeeding, and better parent-child bonding.
PT in Motion, APTA’s official member magazine, is the successor to PT—Magazine of Physical Therapy, which published 1993-2009. All links within articles reflect the URLs at the time of publication and may have expired.

9
11
13
15 16
14
12
10
Founder Trustees of KMCF India
Managing Trustee : Dr. Shashi N. Vani | Hon. Secretary: Dr. Nikhil M.KharodHon. Joint Secretaries: Dr. Parag Dagli | Hon. Joint Secretaries : Dr. Abhishek M. Bansal | Treasure: Dr. Viren S. Doshi
Trustees: Dr. K.M.Mehariya | Mr. Bharat Sarabhai Shah | Dr. Narendra T. Vani | Dr. Anuj J. GroverDr. Ravi kumar D. Parikh | Dr. Jatin Gunvantlal Mistri | Dr. Ashish Arunbhai Mehta | Dr. Deepa Alay Banker
Dr. Somsekhar Nimbalkar
Office: 10, Shamiana Apartment, 61, BMM Society, Ellisbridge, Ahmedabad - 380 006Administrative Wing: Department of Paediatrics, Pramukhswami Medical College, Gokal Nagar, Karamsad 388 325, Dist. Anand
Private Circulation Only
AN
AN
D P
RESS
, GA
MD
I-AN
AN
D
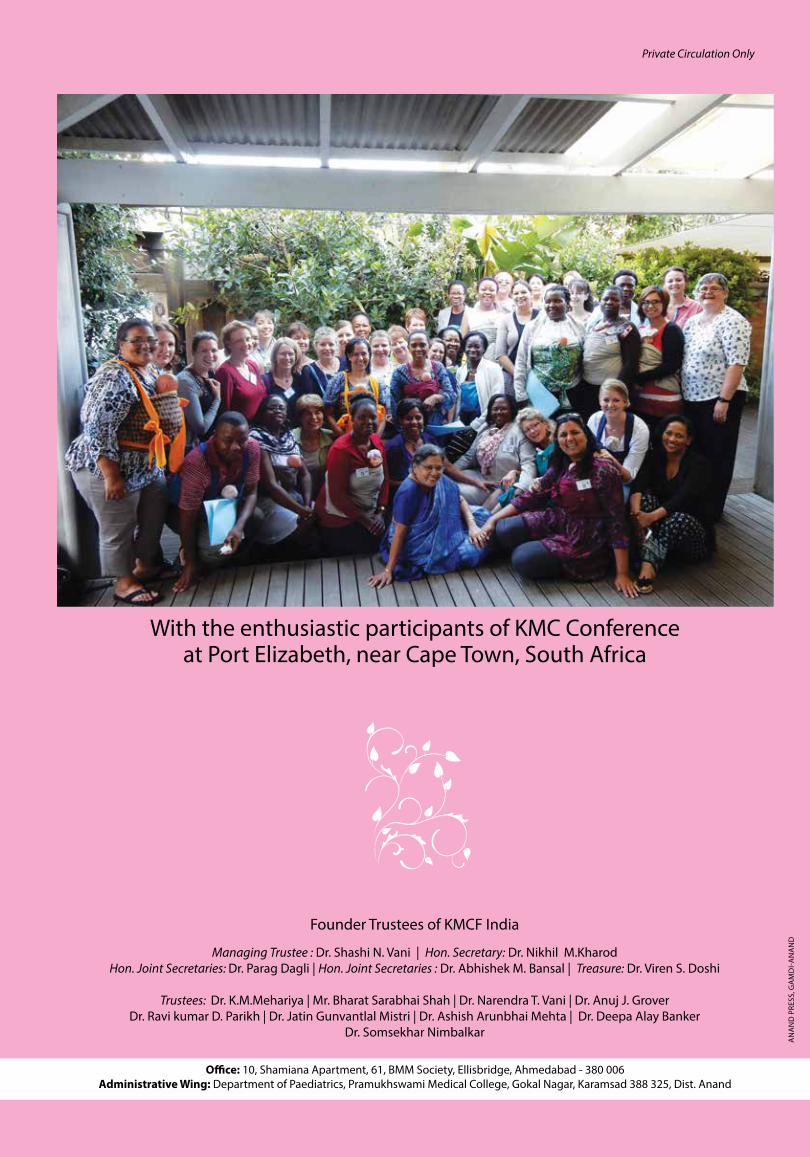
With the enthusiastic participants of KMC Conferenceat Port Elizabeth, near Cape Town, South Africa







