
Manuscript Accepted Early View Article
Page 1 of 12
Early View Article: Online published version of an accepted article before publication in the
final form.
Journal Name: Journal of Case Reports and Images in Medicine
Type of Article: Case Report
Title: Case Report of Hyperthyroidism associated with an increased risk for infection
Authors: Andrew Dookhan, Hiren Patel, Mihir Patel, Kaival Patel, James Bass, Abhinav
Sinha
doi: To be assigned
Early view version published: June 4, 2016
How to cite the article: Dookhan A, Patel H, Patel M, Patel K, Bass J, Sinha A. Case
Report of Hyperthyroidism associated with an increased risk for infection. Journal of Case
Reports and Images in Medicine. Forthcoming 2016.
Disclaimer: This manuscript has been accepted for publication. This is a pdf file of the
Early View Article. The Early View Article is an online published version of an accepted
article before publication in the final form. The proof of this manuscript will be sent to the
authors for corrections after which this manuscript will undergo content check,
copyediting/proofreading and content formatting to conform to journal’s requirements.
Please note that during the above publication processes errors in content or presentation
may be discovered which will be rectified during manuscript processing. These errors may
affect the contents of this manuscript and final published version of this manuscript may
be extensively different in content and layout than this Early View Article.
Manuscript Accepted Early View Article
Page 2 of 12
TYPE OF ARTICLE: Case Report 1
2
TITLE: Case Report of Hyperthyroidism associated with an increased risk for 3
infection 4
5
AUTHORS: 6
Andrew Dookhan1, 7
Hiren Patel2, 8
Mihir Patel3, 9
Kaival Patel4, 10
James Bass5, 11
Abhinav Sinha6 12
13
AFFILIATIONS: 14
1MS-IV at Spartan Health Sciences University - [email protected] 15
2MS-IV at Spartan Health Sciences University - [email protected] 16
3MS-IV at Spartan Health Sciences University - [email protected] 17
4MS-III at Spartan Health Sciences University - [email protected] 18
5MS-III at Spartan Health Sciences University - [email protected] 19
6MD – Chief Director of Medicine at North Vista Hospital - [email protected] 20
21
CORRESPONDING AUTHOR DETAILS 22
Andrew Dookhan 23
197 Tysen Street, Staten Island, NY 10301, 718-501-5568 24
Email: [email protected] 25
26
Short Running Title: Hyperthyroidism and its association for an increased infection 27
risk 28
29
Guarantor of Submission : The corresponding author is the guarantor of 30
submission. 31
32
Manuscript Accepted Early View Article
Page 3 of 12
TITLE: Case Report of Hyperthyroidism associated with an increased risk for 33
infection 34
35
ABSTRACT 36
37
Introduction 38
Infection risk associated with hyperthyroidism although not uncommon, may present 39
with increased mortality if left untreated. 40
The role of hyperthyroidism and its risk for infection is primarily due to the 41
hypermetabolic effect on the body. Modification to the sympathetic nervous system 42
produces a downregulation of the neutrophil response towards the sites of 43
inflammation and/or infection. Consequently, remarkably increasing the risk for 44
complications of infections to occur i.e.: bacterial pneumonia. 45
46
Case Report 47
A 34-year-old Caucasian female presented to the ER complaining of tachycardia, 48
isolated systolic hypertension, tremors, dyspnea, fever, chills, and productive cough 49
with yellow-brown sputum for 5 days. 50
She reported several similar episodes have occurred in the past. A clinical diagnosis 51
of Hyperthyroidism with thyroid storm induced pneumonia was made by the 52
physician and the patient was admitted to the ICU for treatment and close 53
monitoring. 54
Urinary antigen testing detected a positive result for Streptococcus pneumoniae or 55
pneumococcal pneumonia to confirm the pneumonia and treatment was initiated. 56
57
Conclusion 58
The role of hyperthyroidism and its risk for infection causes devastating infectious 59
complications, such as pneumonia, an example that this patient experienced along 60
with having similar episodes in the past but without causality to account for why they 61
are recurrent. Clinical suspicion for diagnosing hyperthyroidism will vastly aid in the 62
management of patient’s more effectively and hopefully avoid any infectious 63
complication that may result. It is entirely important that these patients should be 64

Manuscript Accepted Early View Article
Page 4 of 12
closely monitored to help prevent any further complications that may present upon 65
admission. 66
67
Keywords: Hyperthyroidism, Infection, Pneumonia, Thyroid storm 68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
Manuscript Accepted Early View Article
Page 5 of 12
TITLE: Case Report of Hyperthyroidism associated with increased risk for infection 97
98
INTRODUCTION 99
Hyperthyroidism can be defined as an overactive thyroid, a condition in which your 100
thyroid gland produces too much of the hormone thyroxine (T4). An overactive 101
thyroid increases the basal metabolic rate and increased sympathetic nervous 102
system activity in the human body. Changes in the sympathetic nervous system 103
cause a downstream of effects, an example being a rare complication of thyroid 104
storm with increased infection risk. It manifests itself as a state of exaggerated 105
hyperthyroidism accompanied by systemic organ decompensation. The etiology of 106
thyroid storm can range from poorly controlled to precipitant such as infection, 107
surgery, diabetic ketoacidosis, etc. Increased infection risk is a serious complication 108
these patients face because they are at a higher risk than the normal average 109
person due to the lapse of neutrophil attraction towards sites of inflammation and/or 110
infection. This occurs because hyperthyroidism causes a hypermetabolic effect 111
causing a downregulation of neutrophil response to sites of infection, resulting in 112
complications such as bacterial pneumonia. 113
114
CASE REPORT 115
A 34-year-old Caucasian female presented to the ER complaining of tachycardia, 116
isolated systolic hypertension (148/82), tremors, dyspnea (respiratory rate of 28), 117
fever (102.4), chills, and productive cough with yellow-brown sputum for 5 days. She 118
reported several similar episodes have occurred in the past. Also, the patient stated 119
that she had persistent symptoms of anxiety and myalgia as well, especially for the 120
past 2 weeks. Nothing alleviated or persisted the patient’s symptoms. She denied 121
any medication use, recent travel, contact with those whom are sick, rhinorrhea, 122
nausea, rash, urinary/bowel changes, sleep disturbance, recent infection, and 123
dizziness. Physical exam revealed bilateral expiratory wheezing along with a normal 124
S1/S2, no murmur, rub, and gallop present on arrival. 125
Chest radiograph and echocardiogram were ordered initially. The results revealed 126
left lower lobe opacification with pleural effusions consistent of a lobar pneumonia 127
and revealed a mild systolic ejection murmur, respectively. 128
Manuscript Accepted Early View Article
Page 6 of 12
A clinical diagnosis of Hyperthyroidism with thyroid storm induced pneumonia was 129
made and the patient was admitted to the ICU for treatment and close monitoring. 130
131
Treatment regimen consisted of: 132
• Rocephin – 1g IM once every 24 hours 133
• Zithromax – 500mg by mouth once then 250mg by mouth once a day for 4 134
days. 135
• Tamiflu – 75mg by mouth once a day for 10 days (ICU prophylaxis due to 136
another patient whom acquired H1N1 influenza) 137
• Methimazole – 15mg by mouth three times a day 138
• Propranolol - 5mg IV 139
• Atrovent HFA – 2 puffs by mouth every six hours or as needed. 140
• IV steroids – 125mg IV for three days 141
142
Day 1 to day 3 of hospitalization, following the results of radiology and the 143
echocardiogram, the patient experienced a change in consciousness and was 144
placed on mechanical ventilation due to high risk of aspiration potentially worsening 145
the pneumonia. Additional tests were ordered to confirm the physician’s clinical 146
diagnostic suspicion: CBC with diff. (complete blood count with differential), CMP 147
(comprehensive metabolic panel), TFTs (thyroid functioning tests), sputum gram 148
stain, urinalysis, and blood cultures. 149
Result findings proved to have a decreased TSH (<0.07 µU/mL; Normal: 0.5-5.0 150
µU/mL) and an increased T3 (490 ng/dL; Normal: 115-190 ng/dL) and free T4 level 151
(33.5 µg/dL; Normal: 5-12 µg/dL). It is also noted that within the CBC differential, the 152
absolute neutrophil count was 1.13 (ANC normal range: 1.5-8.0 or 1,500- 153
8,000/mm3). 154
Sputum gram stain was inconclusive due to lack of specimen gathered from patient. 155
Urinary antigen testing detected a positive for Streptococcus pneumoniae and 156
treatment remained the same but route of administration changed from by mouth to 157
either IV or IM. 158
Day 2 of hospitalization, the patient’s vitals were unstable exhibiting hyperpyrexia 159
(101.6) but blood pressure was managed within normal limits. The patient was 160
Manuscript Accepted Early View Article
Page 7 of 12
closely monitored and remained on mechanical ventilation as she was in and out of 161
consciousness. Medication regimen remained the same. 162
Day 3 of hospitalization, the patient’s body temperature fell slightly above normal 163
limits. Blood pressure was still controlled and was within normal limits. Mechanical 164
ventilation was still in place but ordered for extubation the following day pending 165
patient stability and new radiographs and labs were to be drawn. 166
Day 4 of hospitalization. Patient’s vitals were within normal limits and new 167
radiographs and labs were taken. Extubation was unremarkable. Physical exam 168
revealed decreased bilateral expiratory wheezing. Result findings of chest 169
radiographs proved to show diminished right lower lobe opacification and no pleural 170
effusions present. Lab results improved but the patient to still had a decreased TSH 171
(<0.33 µU/mL; Normal: 0.5-5.0 µU/mL) and an increased T3 (244 ng/dL; Normal: 172
115-190 ng/dL) and free T4 level (18 µg/dL; Normal: 5-12 µg/dL). CBC differential 173
was unremarkable. The patient was scheduled for discharge within the next 24 hours 174
along with a management plan for the hyperthyroidism. 175
Day 5 of hospitalization, the patient was discharged and discharge plan consisted of: 176
• Cefuroxime sodium – 250mg by mouth twice a day for ten days 177
• Salbutamol – 2mg by mouth four times a day for 14 days 178
• Methimazole – 15mg by mouth three times a day for 14 days 179
• Tamiflu – 75mg by mouth once a day for 5 days 180
• Rest and hydration 181
182
The patient chose to arrange follow-up appointments with the attending physician 183
within the next two weeks at their outpatient office and adjust treatment regimen as 184
needed to manage the hyperthyroidism. 185
186
DISCUSSION 187
Hyperthyroidism with thyroid storm is a rare clinical case and may present with 188
overwhelming complications. This should be overseen as mortality rates from thyroid 189
storm alone ranges from 20-50% and complications such as infections i.e.: 190
pneumonia, increases the risk furthermore. Due of the potentially high mortality rate, 191
early diagnosis and treatment of thyroid storm is of the utmost importance [1]. 192
Manuscript Accepted Early View Article
Page 8 of 12
Patients experiencing a thyroid storm are at a higher infection risk due to the fact that 193
an overactive metabolic state acts as a catalyst to delay the neutrophil response 194
towards sites of infection. Consequences of this physiologic process may lead to 195
neutropenia (low white blood cell count in blood) where the body lacks its defense 196
mechanism to fight infection. In a similar prospective and observational study 197
conducted, all patients enrolled had an absolute neutrophil count (ANC) below 198
2 × 109/L, documented in at least 3 consecutive occasions within the last 3 months 199
[2]. This process increases susceptibility to infections i.e.: bacterial pneumonia, 200
especially seen in this patient with a noted lower than normal absolute neutrophil 201
count (ANC). The incidence of absolute neutropenia in hyperthyroid patients varied 202
from less than 5% to 18% [3]. 203
It should also be stated that the patient experienced similar episodes in the past. It 204
cannot be coincidental but only fortifying the support a correlation between 205
hyperthyroidism and infection risk does indeed exist. Several reported documents 206
continue to prove a relationship between severe hyperthyroid states and infection 207
acquisition whether it is either bacterial or viral [4,5,6]. Severe complications, fatal if 208
not treated, may arise if a patient presents with symptoms of a thyroid storm and 209
should be a diagnostic clue to expeditiously admit them to the ICU where they will be 210
under close observation, as it is the standard of care in an acute intervention setting 211
[7]. 212
The role of hyperthyroidism and its risk for infection is primarily due to the 213
hypermetabolic effect on the body. The increased sympathetic response causes a 214
downward regulation of neutrophil response to areas of inflammation and/or 215
infection. Devastating infectious complications such as pneumonia is an example 216
that this patient experienced along with having similar episodes in the past but 217
without causality to account for why were are recurrent. A comparable analysis by 218
Rosenthal et al, exhibited similar findings [8]. 219
Through the metabolic process of hyperthyroidism, it can be noted that it indeed 220
does play a part to increase infection risk particularly since the patient had recurrent 221
bouts of pneumonia. A similar case report by Lum et al, had related findings where 222
streptococcus pneumoniae was diagnosed in a patient with characteristics of 223
hyperthyroidism via sputum gram stain [9]. Clinical diagnosis can either be confirmed 224
Manuscript Accepted Early View Article
Page 9 of 12
via sputum gram stain, blood cultures, and/or urinary antigen testing. Urinary antigen 225
testing has been proven to be a more favorable confirmatory test due to its rapid 226
success and minimum invasiveness compared to a bronchoalveolar lavage [10]. 227
Clinical suspicion for diagnosing hyperthyroidism will vastly aid in the management 228
of patient’s more effectively and hopefully avoid any infectious complication that may 229
result. It is entirely important that these patients should be closely monitored to help 230
prevent any further complications that may present upon admission. 231
232
CONCLUSION 233
Thyroid storm is a rare and life- threatening endocrinologic emergency that may be 234
precipitated by trauma, surgery, systemic illness, particularly infection and sepsis [5]. 235
Prompt recognition and immediate treatment is vital to limit the concurrent morbidity 236
and mortality associated with this condition. 237
238
CONFLICT OF INTEREST 239
The authors declare no conflict of interest. 240
241
AUTHOR’S CONTRIBUTIONS 242
Andrew Dookhan 243
Group 1 – Substantial contributions to conception and design, acquisition and 244
analysis of data 245
Group 2 – Drafting the article, revising it critically for important intellectual content 246
Group 3 – Final approval of the version to be published 247
248
Hiren Patel 249
Group 1 – Substantial contributions to conception and design, acquisition and 250
analysis of data 251
Group 2 – Drafting the article, revising it critically for important intellectual content 252
Group 3 – Final approval of the version to be published 253
254
255
256
Manuscript Accepted Early View Article
Page 10 of 12
Mihir Patel 257
Group 1 – Substantial contributions to conception and design, acquisition and 258
analysis of data 259
Group 2 – Drafting the article, revising it critically for important intellectual content 260
Group 3 – Final approval of the version to be published 261
262
Kaival Patel 263
Group 1 – Substantial contributions to conception and design, acquisition and 264
analysis of data 265
Group 2 – Drafting the article, revising it critically for important intellectual content 266
Group 3 – Final approval of the version to be published 267
268
James Bass 269
Group 1 – Substantial contributions to conception and design, acquisition and 270
analysis of data 271
Group 2 – Drafting the article, revising it critically for important intellectual content 272
Group 3 – Final approval of the version to be published 273
Abhinav Sinha, MD 274
Group 1 – Substantial contributions to conception and design, acquisition and 275
analysis of data 276
Group 2 – Drafting the article, revising it critically for important intellectual content 277
Group 3 – Final approval of the version to be published 278
279
REFERENCES 280
1. Refener S, Arunachalam V, Ajluni R, Sil A. Thyroid Storm Precipitated by 281
Infection: An Atypical Case Involving Multisystem Organ Dysfunction. 282
Endocrinologist: March/April 2005 - Volume 15 - Issue 2 - pp 111-114. 283
CME Review Article #9 284
2. Kyritsi EM, Yiakoumis X, Pangalis GA, Pontikoglou C, Pyrovolaki K, et al. 285
High Frequency of Thyroid Disorders in Patients Presenting With Neutropenia 286
to an Outpatient Hematology Clinic STROBE-Compliant Article. Medicine 287
(Baltimore). 2015 Jun; 94(23). doi: 10.1097/MD.0000000000000886 288
Manuscript Accepted Early View Article
Page 11 of 12
3. Baidya A, Singha A, Bhattacharjee R, Dalal BS. Tuberculosis of the thyroid 289
gland: two case reports. Oxf Med Case Rep (2015) 2015 (4): 262-264. doi: 290
10.1093/omcr/omv028 291
4. Bahatoon SA. H1N1 infection-induced thyroid storm. Ann Thorac Med. 2010 292
Apr-Jun; 5(2): 110–112. doi: 10.4103/1817-1737.62475 293
5. Oguz A, Ersoy R, Guner R, Cakir B. Thyroid storm accompanied by H1N1 294
influenza infection. European Society of Endocrinology - Endocrine Abstracts 295
(2010) 22 P194. 296
6. Ford HC, Carter JM. The haematology of hyperthyroidism: abnormalities of 297
erythrocytes, leucocytes, thrombocytes and haemostasis. Postgraduate 298
Medical Journal (1988) – 64, 735-742. 299
7. Carroll R, Matfin G. Endocrine and metabolic emergencies: thyroid storm. 300
Ther Adv Endocrinol Metab. 2010 Jun; 1(3): 139–145. 301
doi: 10.1177/2042018810382481 302
8. Rosenthal MJ, Goodwin JS. A case of hyperthyroidism presenting as 303
recurrent pneumonia. West J Med. 1985 Apr; 142(4): 550–552. PMCID: 304
PMC1306097 305
9. Lum SA, Kaptein EM, Nicoloff JT. Influence of Nonthyroidal Illnesses on 306
Serum Thyroid Hormone Indices in Hyperthyroidism. West J Med. 1983 May; 307
138(5): 670–675. PMCID: PMC1010785 308
10. Couturier MR, Graf EH, Griffin AT. Urine antigen tests for the diagnosis of 309
respiratory infections: legionellosis, histoplasmosis, pneumococcal 310
pneumonia. Clin Lab Med. 2014 Jun;34(2):219-36. 311
doi:10.1016/j.cll.2014.02.002. Epub 2014 Apr 12. 312
313
FIGURE LEGENDS 314
315
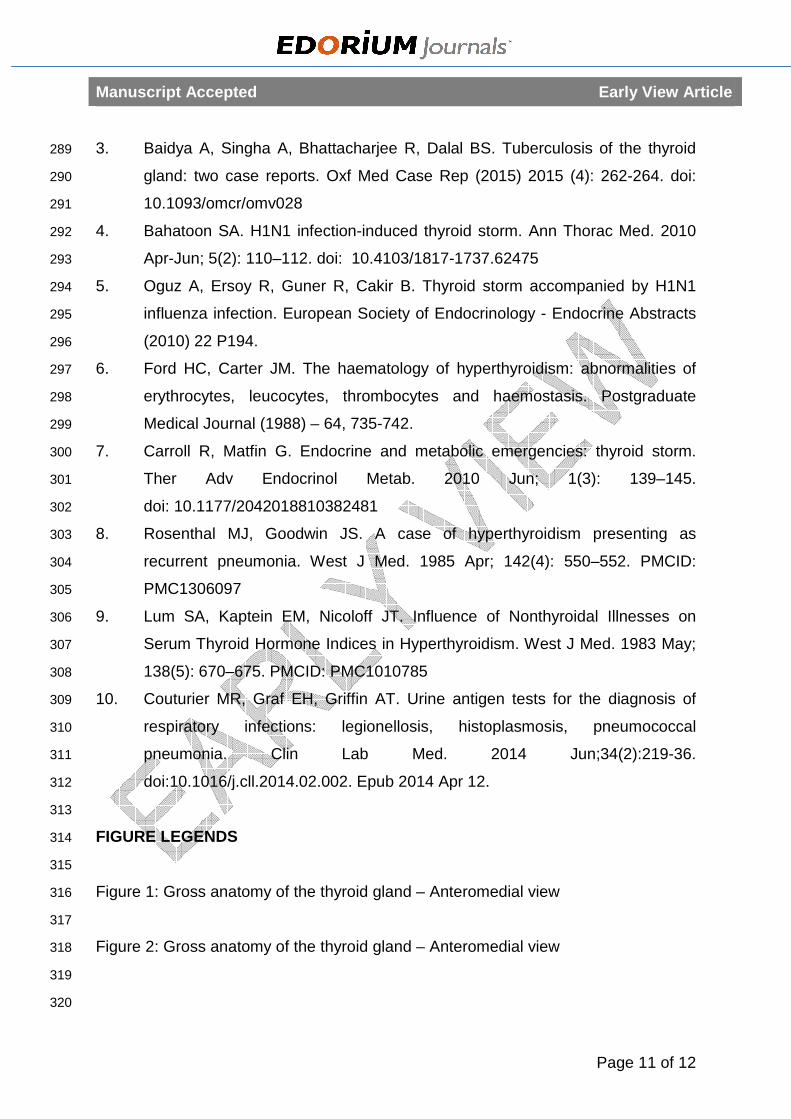
Figure 1: Gross anatomy of the thyroid gland – Anteromedial view 316
317
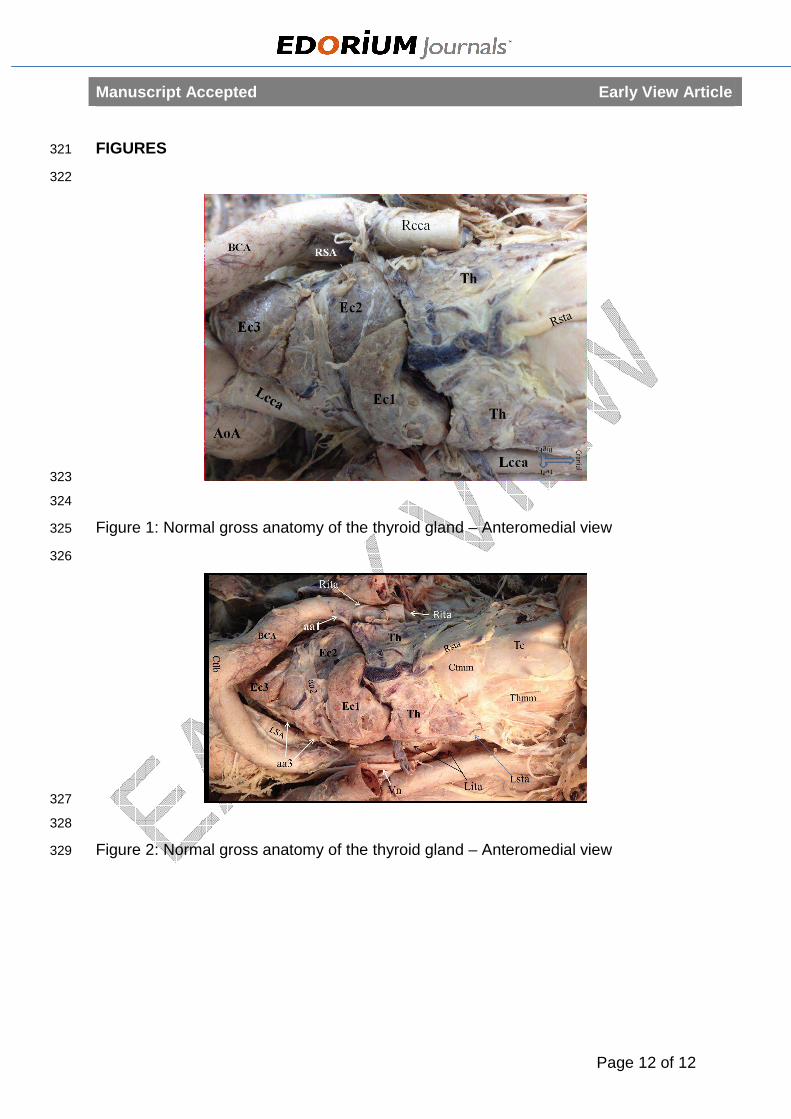
Figure 2: Gross anatomy of the thyroid gland – Anteromedial view 318
319
320
Manuscript Accepted Early View Article
Page 12 of 12
FIGURES 321
322
323
324
Figure 1: Normal gross anatomy of the thyroid gland – Anteromedial view 325
326
327
328
Figure 2: Normal gross anatomy of the thyroid gland – Anteromedial view 329







