Joop van den Bergh
ASBMR 2017: ten topics for clinicians

Netherlands:3 young investigator awards1 late breaking abstract
Fractures and fracture risk

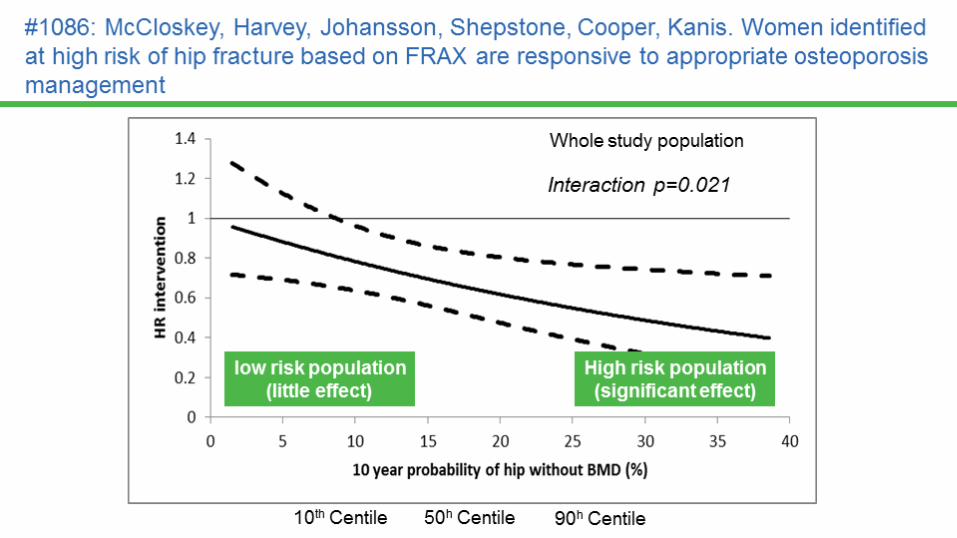
[1086] Women Identified at High Risk of Hip Fracture based on
FRAX are Responsive to Appropriate Osteoporosis Management:
Results from the SCOOP Study of Population Screening
The recently completed primary-care based SCOOP screening study targeted treatment to those at highest hip fracture risk using FRAX.
Congress Highlights ASBMR 2017 Annual Meeting
• To examine the impact of the screening intervention on hip fracture risk according to baseline FRAX hip fracture probability
BACKGROUND
Fx: fracture; BMD bone mineral density
EUGENE MCCLOSKEY, CENTRE FOR METABOLIC BONE DISEASES, UNIVERSITY OF SHEFFIELD, UK

[1125] Longitudinal 5-year changes in bone density and
microarchitecture after Roux-En-Y Gastric Bypass
• RYGB leads to substantial postoperative bone loss, but it is unknown whether accelerated bone loss is sustained beyond 2 years.
• To evaluate longitudinal changes in BMD and bone microarchitecture in the 5 years after RYGB
BACKGROUND
• Prospective 5-year longitudinal study
• 21 adults (17F, 4M; mean age 51 ± 14 years)
• Severe obesity (BMI 45 ± 7 kg/m2), mean weight loss 33 kg, stable after 2 yearsSTUDY
• DXA lumbar spine, total hip, and 1/3 radius• QCT at L1-L2• HRpQCT to assess bone microarchitecture of the distal radius and tibia
ANALYSIS
RYGB: Roux-en-Y Gastric Bypass; DXA: dual X-ray absorptiometry; BMI: body mass index; QCT: quantitative computer tomography; L: lumbar; HR-pQCT: high resolution peripheral quantitative computer tomography
ELAINE YU, MASSACHUSETTS GENERAL HOSPITAL

[1055] Fracture Risk Among 122,205 Cancer Patients: A Population-Based Cohort Study from Manitoba, Canada
• Prior studies have assessed osteoporosis-related fracture risk among patients with breast or prostate cancer
• Data are limited on occurrence of fractures and their risk factors for other cancers
Congress Highlights ASBMR 2017 Annual Meeting
To estimate fracture risk for different cancers and determine predictors of fracture risk among cancer patients
BACKGROUND
• Identification of cancer cases and matched controls, covariates and fracture events through population-based administrative data from Manitoba Canada
• Case definitions for clinical vertebral, forearm, and humerus fractures (“major fractures” [MF])
• Fracture incidence rates and incidence rate ratios (IRRs)• Competing risk time-to-event analysis (competing event=death)
METHODS
MF: major fracture
WILLIAM LESLIE, UNIVERSITY OF MANITOBA, CANADA
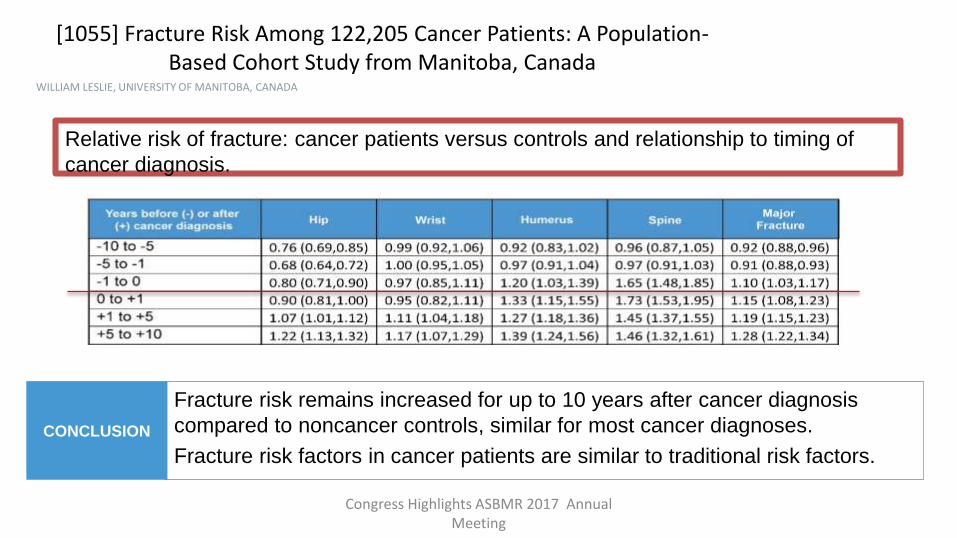
[1055] Fracture Risk Among 122,205 Cancer Patients: A Population-Based Cohort Study from Manitoba, Canada
Congress Highlights ASBMR 2017 Annual Meeting
WILLIAM LESLIE, UNIVERSITY OF MANITOBA, CANADA
Fracture risk remains increased for up to 10 years after cancer diagnosis
compared to noncancer controls, similar for most cancer diagnoses.
Fracture risk factors in cancer patients are similar to traditional risk factors.
CONCLUSION
Relative risk of fracture: cancer patients versus controls and relationship to timing of
cancer diagnosis.

Dutch awardees

Screening for atypical femur fractures using extended femur scans by DXA
Denise van de Laarschot, Sandra Smits, Sanne Buitendijk, Merel Stegenga,
M. Carola Zillikens. Bone Center, Erasmus MC, Netherlands
• to evaluate the potential of extended femur scans by DXA as a screening tool forincomplete AFFs in all consecutive patients undergoing DXA
• who had used bisphosphonates or denosumab at any given moment in the previous year
• Beaking = a localized periosteal or endosteal thickening of the lateral cortex
Journal of Bone and Mineral Research, Vol. 32, No. 8, August 2017, pp 1632–1639
Young Investigator Award

Journal of Bone and Mineral Research, Vol. 32, No. 8, August 2017, pp 1632–1639

Journal of Bone and Mineral Research, Vol. 32, No. 8, August 2017, pp 1632–1639
• Beaking was detected in 12 out of 282 patients (4.3%)
• In 9 patients (3.2%) beaking corresponded with the radiological presence of incomplete AFFs
• 4 already had an X-ray made because of a previous complete AFF of the other leg
• 5 patients (1.8%) were newly diagnosed with six yet unknown incomplete AFFs
• The positive predictive value of beaking on extended femur scan was 83.3% in our study.
Journal of Bone and Mineral Research, Vol. 32, No. 8, August 2017, pp 1632–1639

Negligible Long-Term Effects on Bone Density after Four years of Treatment with TwoIntensive Combination Strategies, including initially High dose Prednisolone, in Early
Rheumatoid Arthritis patients: The COBRA-light Trial.
Merel JJ Lucassen, Marieke M ter Wee, Nicole PC Konijn, Debby den Uyl, Maarten Boers, Willem F Lems
• changes in bone mineral density (BMD) after four years in early RA patients initially randomized to one yearof COBRA or COBRA-light therapy
• (COBRA)-light therapy (methotrexate and initially 30mg/day prednisolone)
• non-inferior to
• COBRA therapy (methotrexate, sulfasalazine and initially 60mg/day prednisolone) in
• the first year of treatment of early rheumatoid arthritis (RA) patients
Young Investigator Award

4-year follow-up
COBRA-light COBRA
• Total Hip -3.3% (-1.7%) -1.7% (0.5%)
• Femoral Neck -3.7% (-1.0%) -3.0% (-0.6%)
• Lumbar spine -0.5% (-1.0%) -1.0% (0.0%)
Conclusion: in modern management of RA, one year of (initially high) glucocorticoid treatment has negligible long-term effects on bone.

High imminent vertebral fracture risk
in smokers and COPD patients with a
prevalent or incident vertebral fracture
Mayke van Dort Piet GeusensAnnemariek Driessen
Lisette RommeFrank Smeenk
Emiel WoutersJoop van den Bergh
The Netherlands
Young Investigator Award
Incidence of VFs
One year Three year0
20
40
60
80
100
None
1 VF
Subjects (%)with
incident VFs
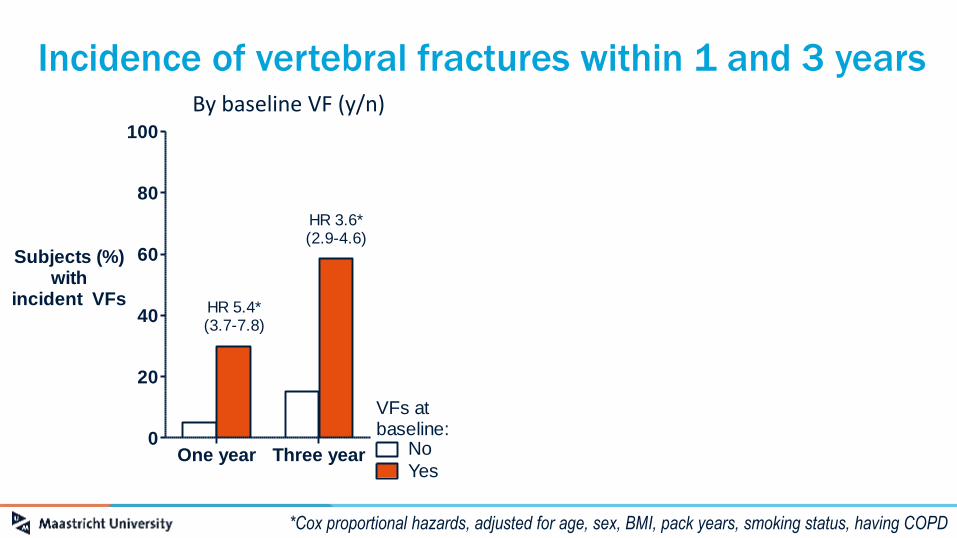
HR 3.6*(2.9-4.6)
HR 5.4*(3.7-7.8)
VFs atbaseline:
Incidence of vertebral fractures within 1 and 3 years
*Cox proportional hazards, adjusted for age, sex, BMI, pack years, smoking status, having COPD
By baseline VF (y/n)
No
Yes
Incidence of VFs
One year Three year0
20
40
60
80
100
None
1 VF
Subjects (%)with
incident VFs
HR 3.6*(2.9-4.6)
HR 5.4*(3.7-7.8)
VFs atbaseline:
Incidence of VFs
One year Three year0
20
40
60
80
100
None
1 VF
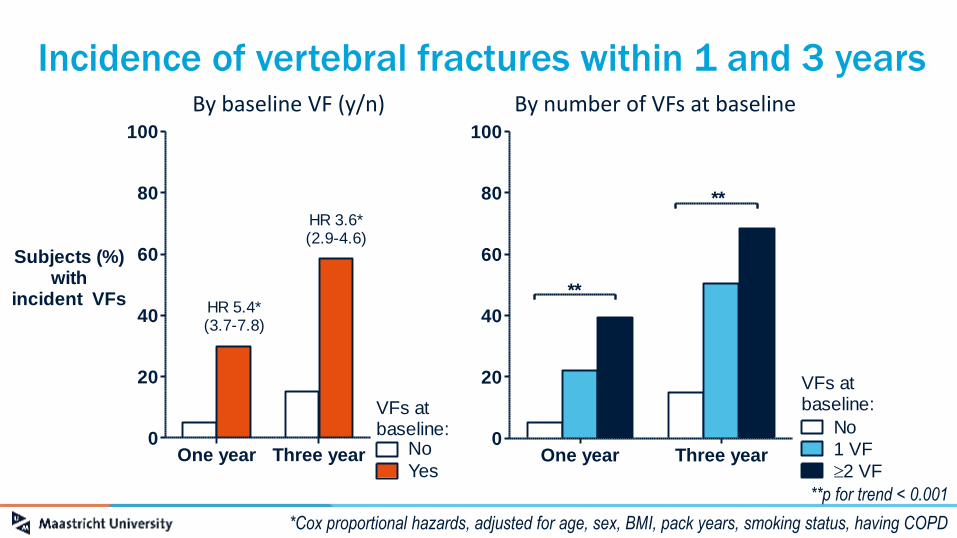
**p for trend <0.001
Subjects (%)with
incident VFs
2 VF
**
**
VFs atbaseline:
By number of VFs at baseline
Incidence of vertebral fractures within 1 and 3 years
*Cox proportional hazards, adjusted for age, sex, BMI, pack years, smoking status, having COPD
By baseline VF (y/n)
**p for trend < 0.001
No
Yes

Incidence of VFs
One year Three year0
20
40
60
80
100
None
Grade 1
**p for trend <0.001
Subjects (%)with
incident VFs
Grade 2Grade 3
**
**
Severity atbaseline:
By severity of VFs at baseline
Incidence of vertebral fractures within 1 and 3 years
*Cox proportional hazards, adjusted for age, sex, BMI, pack years, smoking status, having COPD
**p for trend < 0.001
Incidence of VFs
One year Three year0
20
40
60
80
100
None
1 VF
Subjects (%)with
incident VFs
HR 3.6*(2.9-4.6)
HR 5.4*(3.7-7.8)
VFs atbaseline:
By baseline VF (y/n)
No
Yes
Mortality after a recent clinical fracture before and after the introduction of a Fracture Liaison Service
Caroline Wyers, PhD
ASBMR – September 11, 2017
Lisanne VrankenJohanna H Driessen
Irma JA de BruinPiet PM Geusens
Robert Y van der VeldeHeinrich MJ JanzingSjoerd Kaarsemaker
John A EismanJoop PW van den Bergh
LB-1160

HR*: 0.8095% CI: 0.72-0.90
Post
Pre
Mortality: Pre vs. Post FLS
* adjusted for age, sex and fracture type
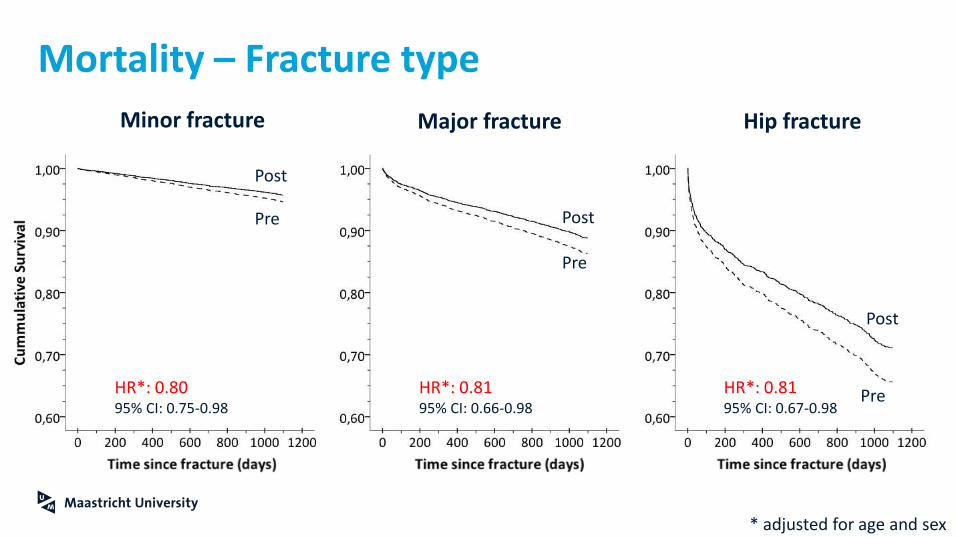
Mortality – Fracture type
Minor fracture Major fracture Hip fracture
* adjusted for age and sex
HR*: 0.8195% CI: 0.67-0.98
Post
PreHR*: 0.8195% CI: 0.66-0.98
Post
Pre
HR*: 0.8095% CI: 0.75-0.98
Post
Pre

Behandeling
• Denosumab
• Abaloparatide
• Teriparatide
• Romosozumab

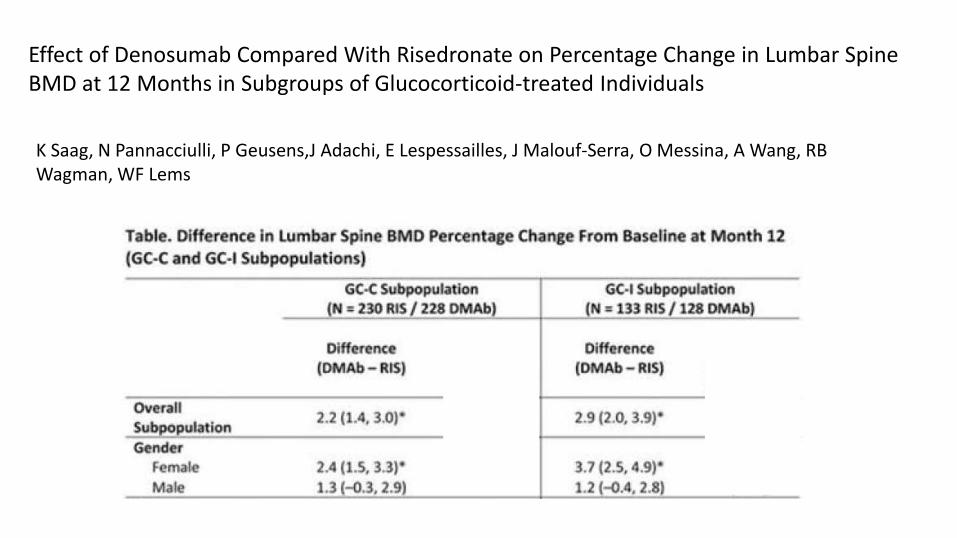
Effect of Denosumab Compared With Risedronate on Percentage Change in Lumbar SpineBMD at 12 Months in Subgroups of Glucocorticoid-treated Individuals
K Saag, N Pannacciulli, P Geusens,J Adachi, E Lespessailles, J Malouf-Serra, O Messina, A Wang, RB Wagman, WF Lems

Severe rebound-associated vertebral fractures afterdenosumab discontinuation
• These 9 cases are unusual and disturbing for several reasons
• All VFs were spontaneous and most patients had a high number of VFs(mean = 5.5) in a short period of time.
• Their VFs occurred rapidly after last denosumab injection (9 to 16 months)
Lamy et al. JCEM October 6, 2016
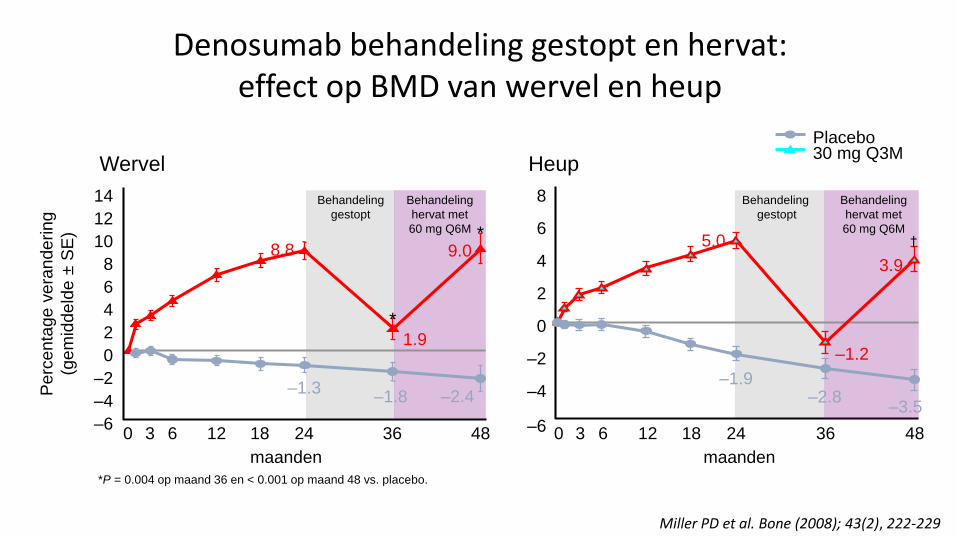
Denosumab behandeling gestopt en hervat:effect op BMD van wervel en heup
Behandeling
hervat met
60 mg Q6M
–2.4–1.8
Behandeling
gestopt
9.0
1.9
0 3 6 12 18 24 36 48–6
–2
0
2
4
6
8
10
12
14
–4
8.8
–1.3
*
*
–6
–4
–2
0
2
4
6
8
0 3 6 12 18 24 36 48
Behandeling
hervat met
60 mg Q6M
Behandeling
gestopt
–2.8–3.5
–1.2
3.9
5.0
–1.9
†
maanden maanden
Perc
enta
ge v
era
ndering
(gem
iddeld
e ±
SE
)
Wervel Heup
Placebo30 mg Q3M
*P = 0.004 op maand 36 en < 0.001 op maand 48 vs. placebo.
Miller PD et al. Bone (2008); 43(2), 222-229
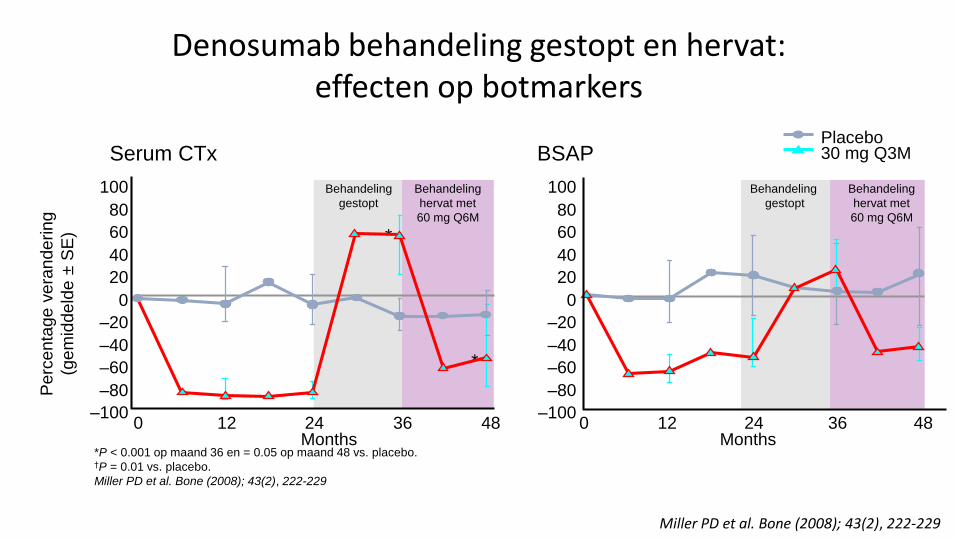
Denosumab behandeling gestopt en hervat:effecten op botmarkers
–100
–80
–60
–40
–20
0
20
40
60
80
100
–100
80
100
Placebo30 mg Q3M
0 12 24 36 48 0 12 24 36 48Months Months
*
*
–80
–60
–40
–20
0
20
40
60
Serum CTx BSAP
*P < 0.001 op maand 36 en = 0.05 op maand 48 vs. placebo.†P = 0.01 vs. placebo.
Miller PD et al. Bone (2008); 43(2), 222-229
Behandeling
hervat met
60 mg Q6M
Behandeling
gestopt
Behandeling
hervat met
60 mg Q6M
Behandeling
gestopt
Perc
enta
ge v
era
ndering
(gem
iddeld
e ±
SE
)
Miller PD et al. Bone (2008); 43(2), 222-229

Discontinuation of Denosumab therapy for osteoporosis: A systematic review and position statement by ECTS
• Based on current data, denosumab should not be stopped without considering alternative treatment in order to prevent rapid BMD loss anda potential rebound in vertebral fracture risk.
• Re-evaluation after 5 years of denosumab treatment– high fracture risk should either continue denosumab therapy for up to 10 years
– or be switched to an alternative treatment
– low risk: bisphosphonate therapy should be considered to reduce or prevent the rebound increase in bone turnover.
E. Tsourdi et al. / Bone 105 (2017) 11–17

LB abstract - Disco Dmab study
24 mnd
BP
Behandeling
• Denosumab
• Abaloparatide
• Teriparatide
• Romosozumab

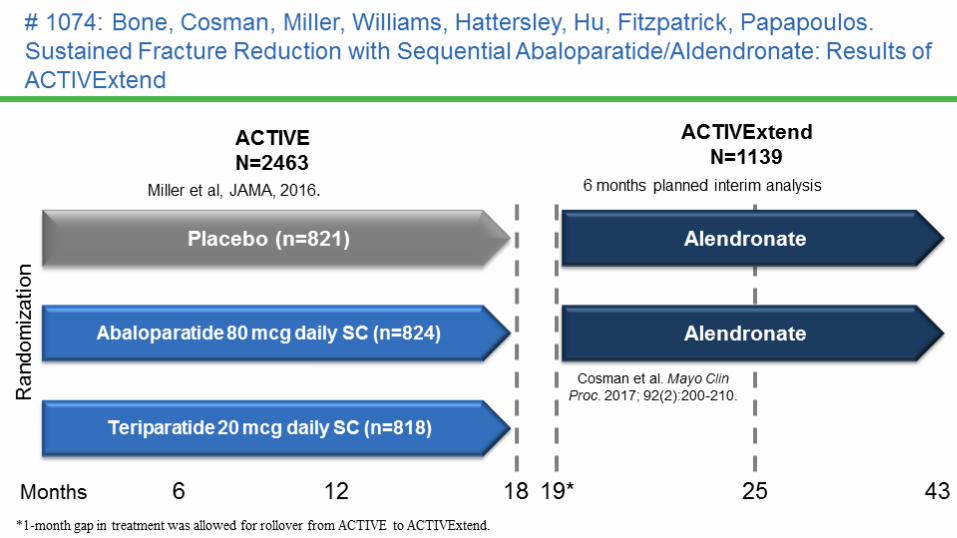
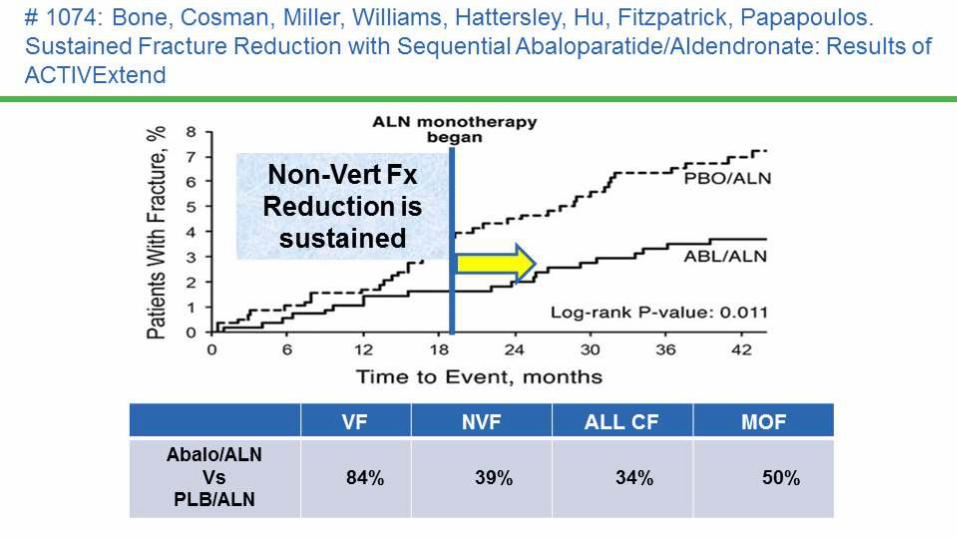
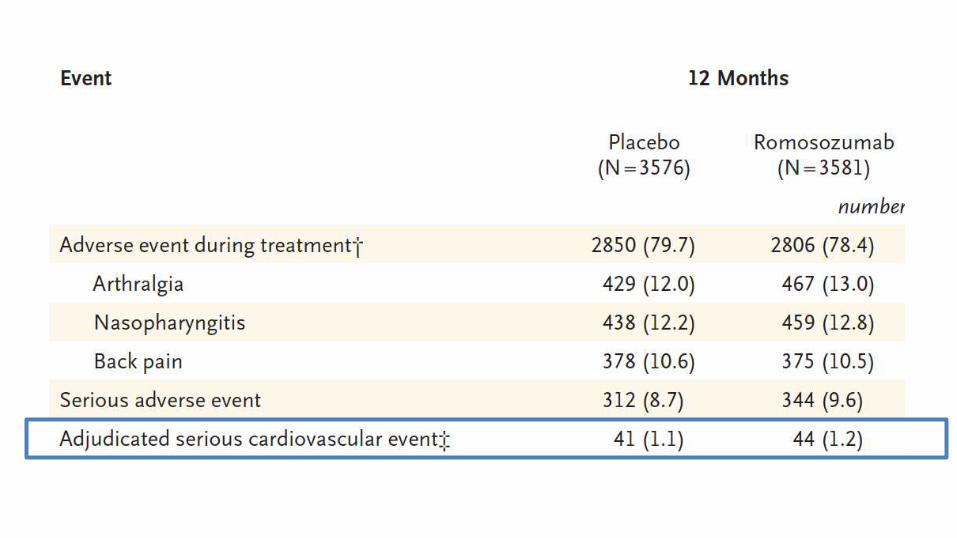
JAMA. 2016;316:722-733

Behandeling
• Denosumab
• Abaloparatide
• Teriparatide
• Romosozumab

Lancet
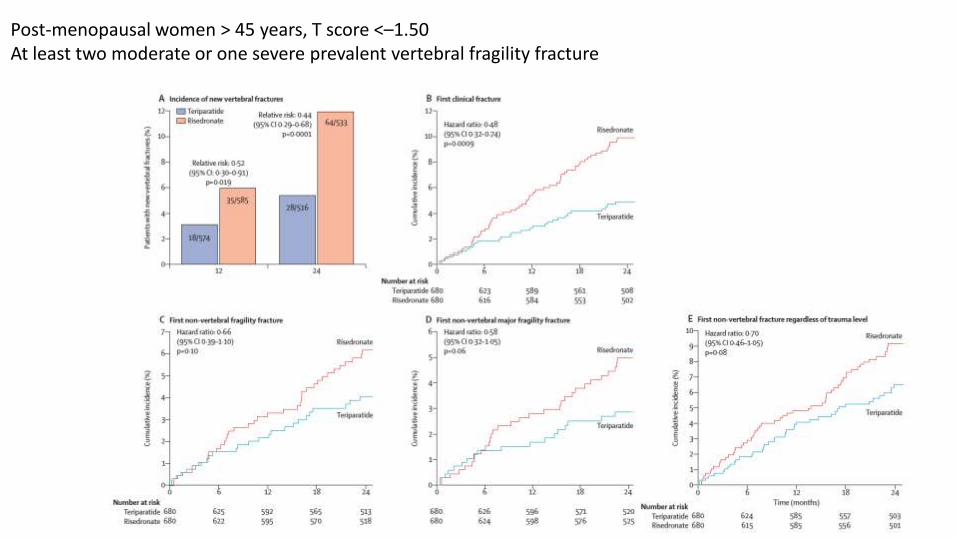
Post-menopausal women > 45 years, T score <–1.50 At least two moderate or one severe prevalent vertebral fragility fracture
Behandeling
• Denosumab
• Abaloparatide
• Teriparatide
• Romosozumab
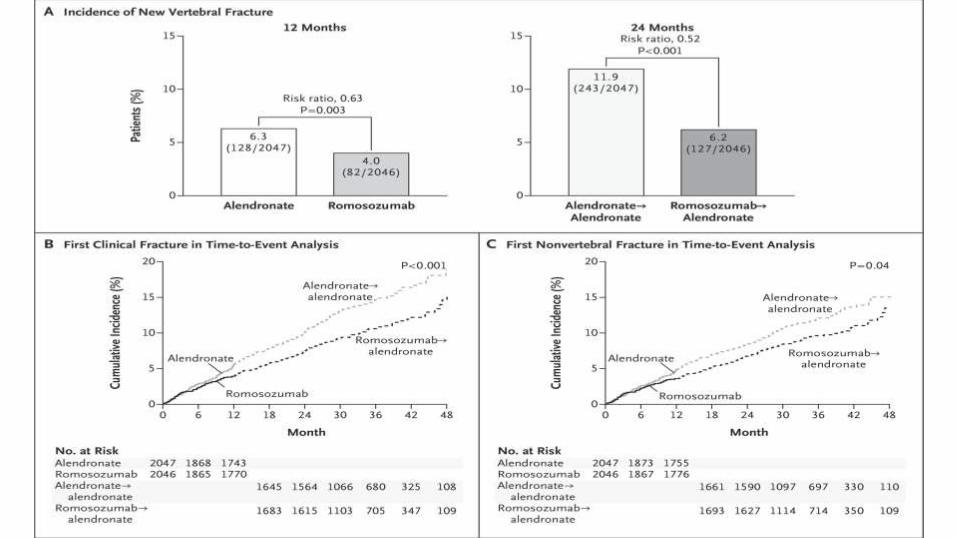
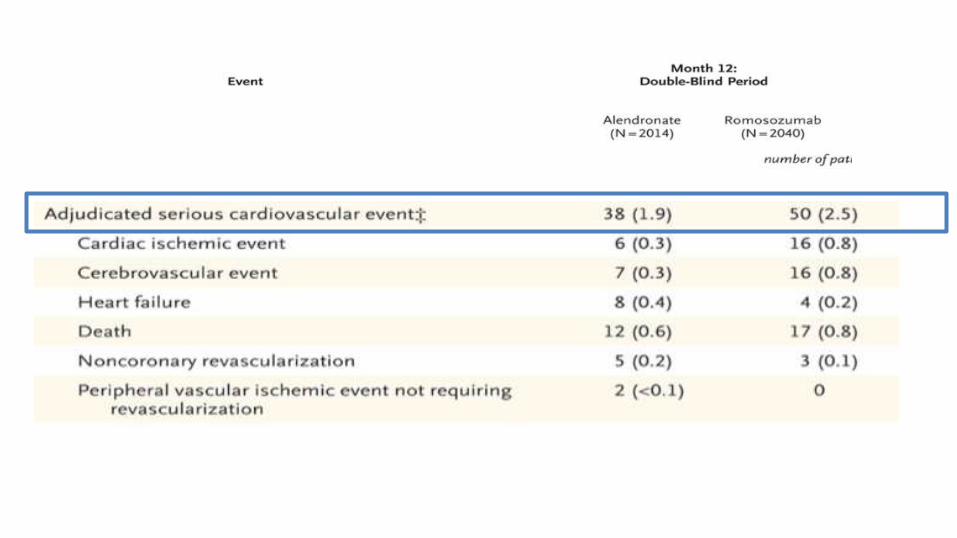
Original Article
Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis
Kenneth G. Saag, M.D., Jeffrey Petersen, M.D., Maria Luisa Brandi, M.D., Andrew C. Karaplis, M.D., Ph.D., Mattias Lorentzon, M.D., Ph.D., Thierry Thomas, M.D., Ph.D., Judy Maddox, D.O., Michelle Fan, Ph.D., Paul D. Meisner, Pharm.D., and Andreas
Grauer, M.D.
N Engl J MedVolume 377(15):1417-1427
October 12, 2017
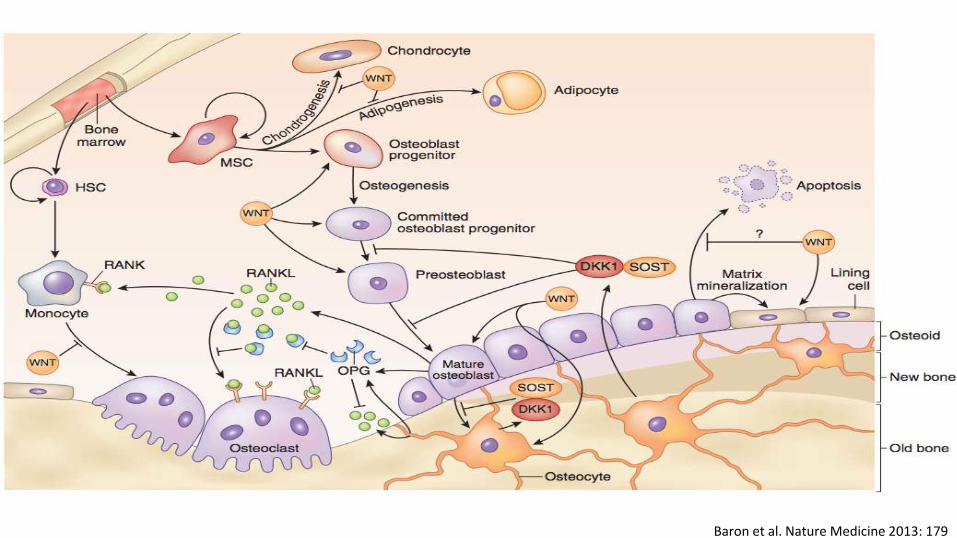
Baron et al. Nature Medicine 2013: 179

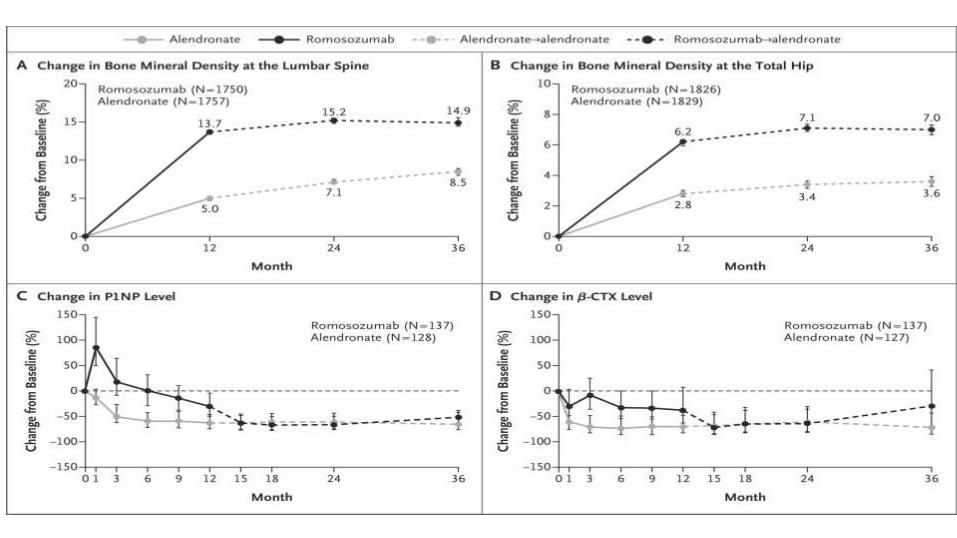
Saag KG et al. N Engl J Med 2017;377:1417-1427

Effect van medicatie in de primaire analyses van RCTs met fractuurpreventie als eindpunt*
Medicament Wervel-fracturen Niet wervel-fracturen Heupfracturen
Follow-up Relatief effect Relatief effect Relatief effect
Alendronaat 1-4 jaar 0.55 (0.45-0.67) 0.84 (0.74-0.94) 0.61 (0.4-0.92)
Risedronaat 2-3 jaar 0.63 (0.51-0.77) 0.80 (0.72-0.90) 0.74 (0.59-0.94)
Zoledronaat 3 jaar 0.30 (0.24-0.38) 0.75 (0.64-0.87) 0.59 (0.42-0.83)
Denosumab 3 jaar 0.32 (0.26-0.41) 0.80 (0.67-0.95) 0.60 (0.37-0.96)
Teriparatide 1.5 jaar 0.36 (0.28-0.47) 0.62 (0.48-0.82)
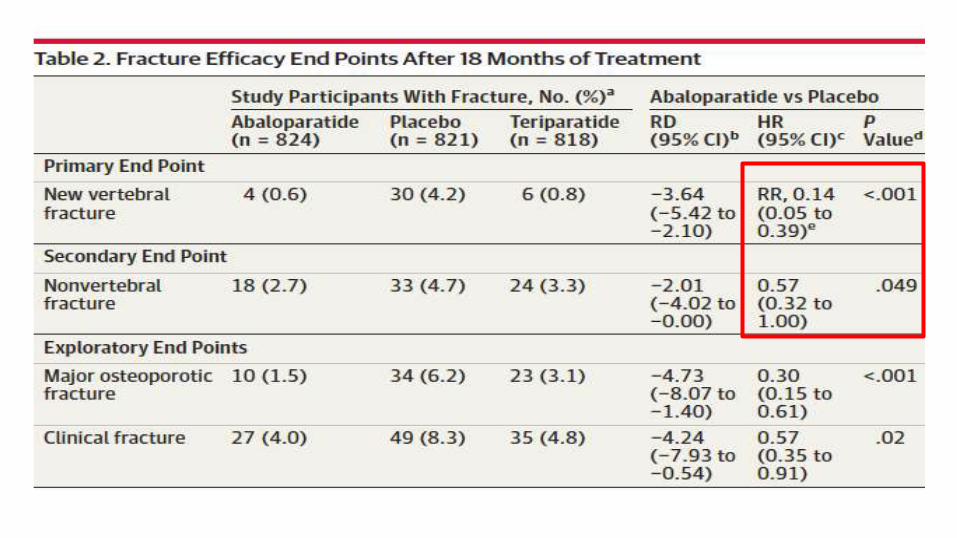
Abaloparatide 1.5 jaar 0.14 (0.05-0.39) 0.57 (0.32-1.00)
Romosozumab (plac) 1 jaar 0.27 (0.16-0.47)0.75 (0.53-1.05)
0.58 (0.37-0.89)*
Romosozumab (Aln) 2 jaar 0.52 (0.40-0.66) 0.81 (0.66-0.99) 0.62 (0.42-0.92)
Teriparatide (Ris) 2 jaar 0.44 (0.29-0.68)
* Cave: rebound wervelfracturen na staken therapie








