Download - Intestinal Obstraction Maj


1. Introduction
2. Definition
3. Classification
4. Causes of intestinal obstruction
5. Anatomy & physiology
6. Pathophysiology , s&s
7. Diagnostic test
8. Complication
9. Treatment
10. Nursing interventions
11. Patients health education
12. reference

The bowel, or intestine, is the part of the
digestive tract that absorbs nutrients from
foods we eat. The residue of digested food
passes through the bowel and is excreted during
elimination, the final stage of digestion. This
process can be interrupted or halted by the
presence of a bowel obstruction,

The term intestinal obstruction refers
to any form of impedance to the
normal passage of the bowel
contents through the small or large
intestine.
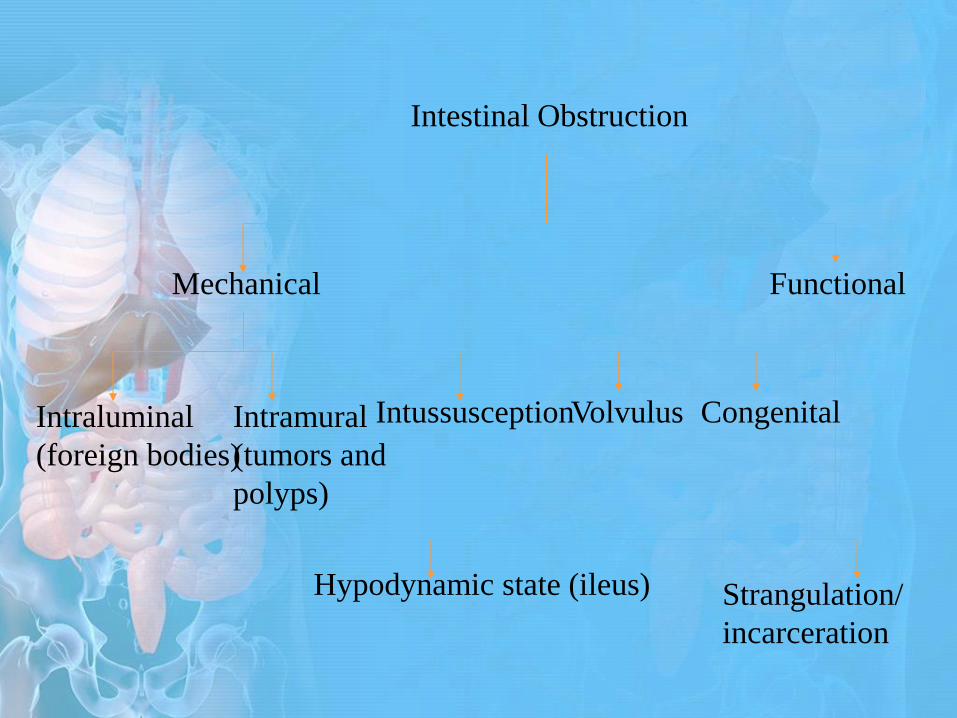
Intestinal Obstruction
Mechanical Functional
Intraluminal
(foreign bodies)
Intramural
(tumors and
polyps)
Intussusception Volvulus
Hypodynamic state (ileus) Strangulation/
incarceration
Congenital
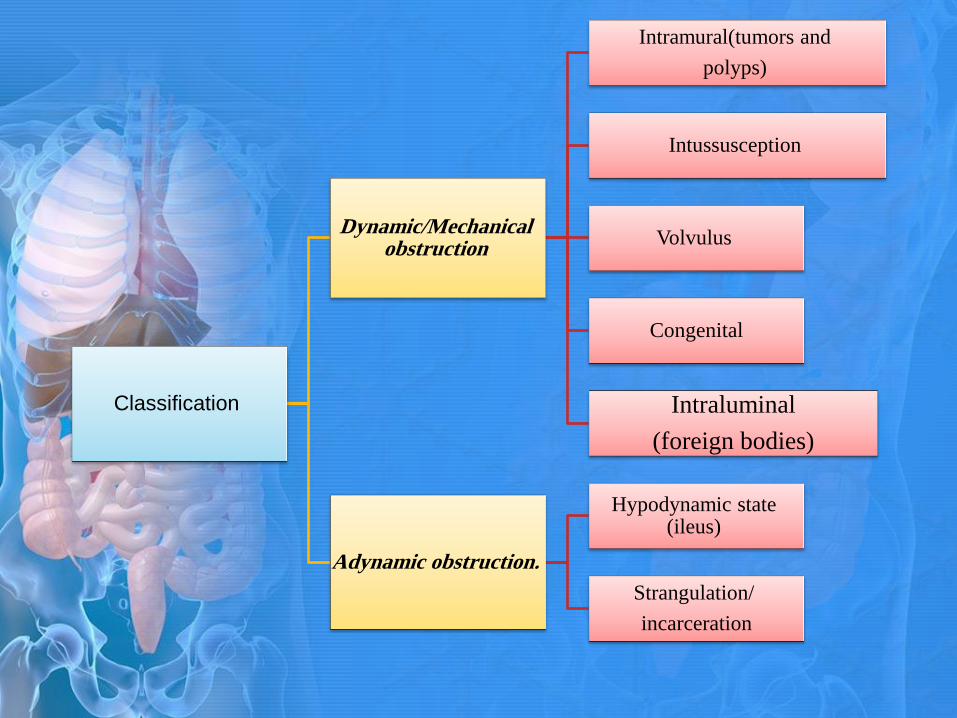
Classification
Dynamic/Mechanical obstruction
Intramural(tumors and
polyps)
Intussusception
Volvulus
Congenital
Intraluminal
(foreign bodies)
Adynamic obstruction.
Hypodynamic state (ileus)
Strangulation/
incarceration

Adhesions
the most common
cause of small bowel
obstruction.
Intussusceptions
One part of the
intestine slips into
another part located
below it.

Volvulus
-Bowel twists and turns on itself.
Strangulated Hernia
-Protrusion of intestine through a weakened area in the
abdominal muscle or wall.
Tumor
-a tumor that exists within the wall of the intestine or
a tumor outside the intestine causes pressure on the
wall of the intestine.
Impaction of stool
Foreign bodies

paralytic /Functional obstruction:
Failure of peristalsis to move intestinal
contents: due to neurologic or
muscular impairment.
• in which The intestinal muscles cannot
propel(push) the contents along the
bowel.

Causes;
Abdominal surgery and trauma.
Spinal injuries
Peritonitis
Vascular insufficiency
muscular dystrophy,



H+
K+
CL- K+
metabolic
alkalosis.


•Dehydration
•Ischemic bowel disease
•Intestinal perforation
•Peritonitis
•sepsis

:
In most cases the patient is kept NPO.
NG tube to decompressed , which relieves
symptoms and may resolve the obstruction.
I.V solution with electrolytes is initiated to
correct the fluid and electrolyte imbalance.
IV antibiotics .

The surgical treatment of intestinal obstruction
depends largely on the cause of the
obstruction.
In the most common causes of obstruction, such as
hernia and adhesions, the surgical procedure involves
repairing the hernia or dividing the adhesion to which
the intestine is attached.

• In some instances, the portion of affected bowel may be
removed and an anastomosis performed.
• A colonoscopy may be performed to untwist and
decompress the bowel. A cecostomy, in which a surgical
opening is made into the cecum, may be performed for
patients who are poor surgical risks and urgently need
relief from the obstruction. The procedure provides an
outlet for releasing gas and a small amount of drainage.
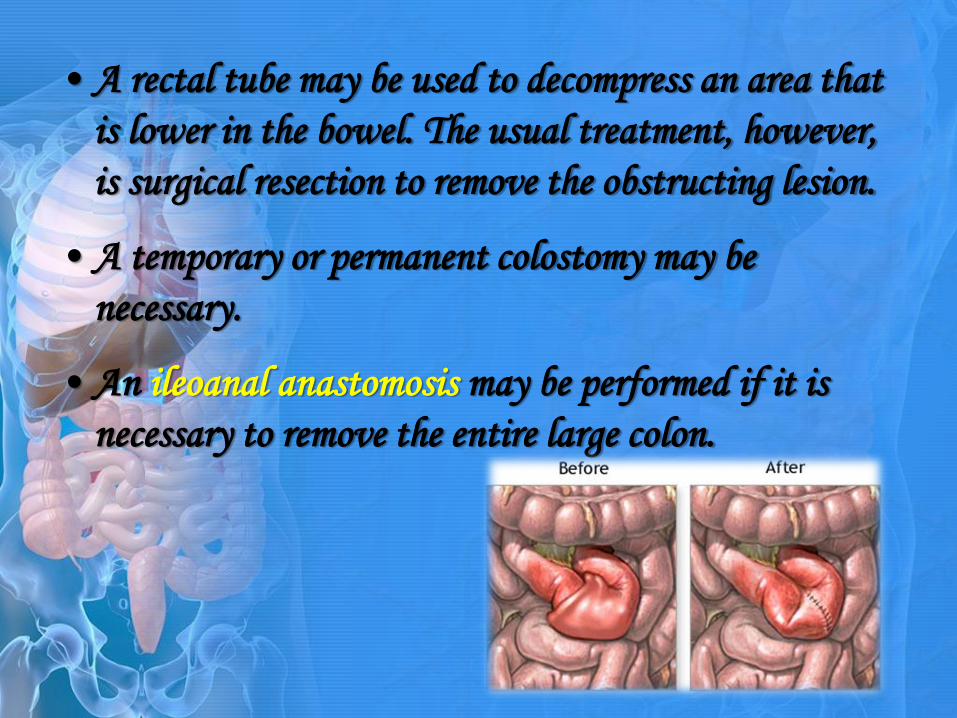
• A rectal tube may be used to decompress an area that
is lower in the bowel. The usual treatment, however,
is surgical resection to remove the obstructing lesion.
• A temporary or permanent colostomy may be
necessary.
• An ileoanal anastomosis may be performed if it is
necessary to remove the entire large colon.
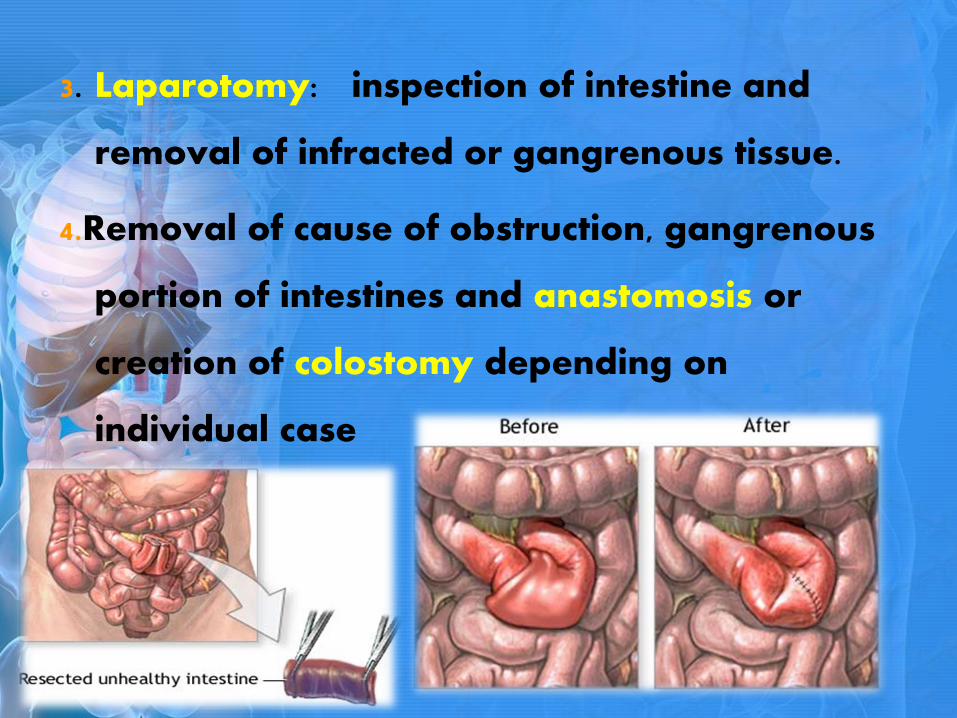
3. Laparotomy: inspection of intestine and
removal of infracted or gangrenous tissue.
4.Removal of cause of obstruction, gangrenous
portion of intestines and anastomosis or
creation of colostomy depending on
individual case


1. Assess the nature and location of the patient's
pain, the presence or absence of distention,
flatus, defecation, emesis, obstipation.
2. Listen for high-pitched bowel sounds,
peristaltic rushes, or absence of bowel sounds.
3. Assess vital signs.

1. Acute Pain related to obstruction, distention, and strangulation.
2. Risk for Deficient Fluid Volume related to impaired fluid
intake, vomiting, and diarrhea from intestinal obstruction.
3. Diarrhea/Constipation may be related to presence of
obstruction/changes in peristalsis, possibly evidenced by changes
in frequency and consistency or absence of stool, alterations in
bowel sounds, presence of pain, and cramping.
4. Ineffective Breathing Pattern related to abdominal distention,
interfering with normal lung expansion.
5. Risk for Injury related to complications and severity of illness.
6. Fear related to life-threatening symptoms of intestinal
obstruction.

Nursing Interventions
Achieving Pain Relief:
Administer prescribed analgesics.
Provide supportive care during NG intubation to
assist with discomfort.
To relieve air-fluid lock syndrome, turn the patient
from supine to prone position every 10 minutes
until enough flatus is passed to decompress the
abdomen.
A rectal tube may be indicated.
Maintaining Electrolyte and Fluid Balance:
Measure and record all intake and output.
Administer I.V. fluids and parenteral nutrition as
prescribed.
Monitor electrolytes, urinalysis, hemoglobin, and blood
cell counts, and report any abnormalities.
Monitor urine output to assess renal function and to
detect urine retention due to bladder compressions by
the distended intestine.
Monitor vital signs; a drop in BP may indicate
decreased circulatory volume due to blood loss from
strangulated hernia.
Maintaining Normal Bowel Elimination:
Collect stool samples to test for occult blood if
ordered.
Maintain adequate fluid balance.
Record amount and consistency of stools.
Maintain NG tube as prescribed to
decompress bowel.

Maintaining Proper Lung Ventilation:
Keep the patient in Fowler's position to
promote ventilation and relieve abdominal
distention.
Monitor ABG levels for oxygenation levels if
ordered.

Preventing Injury Due to Complications:
Prevent infarction by carefully assessing the
patient's status; pain that increases in intensity or
becomes localized or continuous may herald
strangulation.
Detect early signs of peritonitis to minimize this
complication.
Avoid enemas, which may distort an X-ray or make
a partial obstruction worse.
Observe for signs of shock.
Watch for signs of (metabolic alkalosis and
metabolic acidosis.


• When client is to be discharged from the hospital,
nursing care is still continued. With sufficient
support at home, most client recover gradually.
During home visits, the client’s physical status and
progress towards recovery is assessed. The client’s
understanding of therapeutic regimen is also assessed,
and previous teaching is reinforced.

•Instruct the significant others to take the following home
medication as ordered by the physician.
•Explain to the significant others the drug names as well as the
right route and dosage.
•Inform the significant others about the side effects that may
occur brought by the medication.
•Encourage the significant others to comply and follow religiously
the right timing in taking the medication.
•Confer with the patient’s family the need take precautions
regarding medication therapy, activity, and dietary restriction.
•Discuss with the patient’s family ways to cope with stressful
situations in positive manner.

• Instruct patient’s family to report for immediate
occurrence of signs and symptoms to a health care
professional.
•Reinforce and supplement patient’s family knowledge
about diagnosis, prognosis, and expected level of function.
•Provide patient’s family with specific directions about
when to call the physician and what complications require
prompt attention.
•Peer support and psychological counseling may be helpful
for some families.

•Once at home, patient may resume much of the normal activity
short of aggressive physical exercise.
•Walk short distances everyday and gradually increase activity.
•No lifting of a weight greater than 20 lbs (9kg) for 6 weeks.
Exercise should be started cautiously.
•Encourage to practice deep breathing exercise and range of
motion exercises up to the level of capability.

•Explain the need for rest periods both before and after
certain activities.
•Teach client the importance of stress management
through relaxation technique,
•Help improve patient’s self-concept by providing
positive feedback, emphasizing strengths and
encouraging social interaction and pursuit of interests.

•Explain to the significant others the need to continue
drug therapy
•Provide patient’s family with a list of medications,
with information on action, purpose and possible side
effects.
•Advise significant others to always comply with the
medications. Call the physician if there is a problem
taking them.
Hygiene
•Keep proper hygiene. Teach client’s family
the importance of hygiene like daily oral
care, bathing and changing clothes.
•Proper Wound care must be observed.

•Emphasize to the client’s family the importance of proper
nutrition, its need for early recovery. This can aid in
restoring body functioning.
•Provide dietary instructions to help patient’s family
identify and eliminate foods that is needed by the patient.

• Soft or low residue diet upon discharge; this should be
continued at home for approximately 2 weeks (this
includes breads, cereals, chicken, fish, and soup).
• Avoid large quantities of raw fruits and vegetables.
• After 2 weeks, gradually reintroduce your regular diet.
• Encourage to drink plenty of fluids.
• Take nutrition supplements

•Advise to visit or have her follow up check-up
with her attending physician.
•Advise to call and notify the attending physician
for any unusual ties that may occur
•Routinely, follow up check – up with patients
within two weeks. If there are staples that require
removal, postoperative problems, or wound issues, a
follow-up appointment will be scheduled sooner.

Smeltzer, S.C. & Bare, B.G. Brunner and Suddarth’s
Textbook of Medical Surgical Nursing. 12th Ed.
Philadelphia: Lippincott Company, 2010.
http:// www MedicinePlus.com
http://nanda-nursinginterventions.blogspot.com








