Download - In The name of God

In The name of God

Diabetes epidemiology: Reflecting your clinic?

Question #1
• Approximately what percentage of your T2 diabetes patients are obese (>30 kg/m2)*?
1. <10%
2. 25%
3. 50%
4. 75%
5. >90%
*WHO Diabetes Fact Sheet No. 311. September 2006

Epidemiological transition” in newly industrialised nations
Cockram CS 2000. HKMJ; 6 (1): 43-52Mohan et al 2007. Indian J Med Res; 125: 217-230
Adapted from IDF Diabetes Atlas 4th ed., 2009
Aging population
Dietary changes Reduced physical activity
UrbanisationUnhealthy lifestyle choices

Urbanisation, Western dietary habits linked to obesity rates
• Emergence of obesity linked to lifestyle changes associated with urbanisation, modernisation
• Population adopts Western dietary habits, decreased physical activity etc.
Chiarelli and Marcovecchio 2008. EJE; 159: S67-S74Yach et al 2006. Nature Medicine; 12(1): 62-66
19702000

Methods:
• Conducted in 2007
• 5,287 Iranian citizens included
• Sample size aged 15–64 years
Results:
• Diabetes 8.7%8.7%
• Hypertension 26.6%26.6%
• Obesity 22.3%22.3%
• Central obesity 53.6%53.6%
FemaleFemale
Male
Prevalence of Diabetes and its risk factors in Iran
Esteghamati A, et al. Third national surveillance of risk factors of non-communicable diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemia. BMC Public Health. 2009 May 29;9:167
2.5 million Iranian2.5 million Iranian

Obesity contributes to increase in prevalence of T2DM
• Obesity• 2-fold increase in the
odds of developing diabetes for 40-55 yr age group over a 30 year period
• Physical inactivity
• Increase in the number of individuals > 65 years
Fox CS et al. The Framingham Offspring Study. Circulation 2006;113:2914–8
Normal weight Overweight Obese
1970s 1980s 1990s0
5
10
15
20
8 y
ear
rate
(%
)
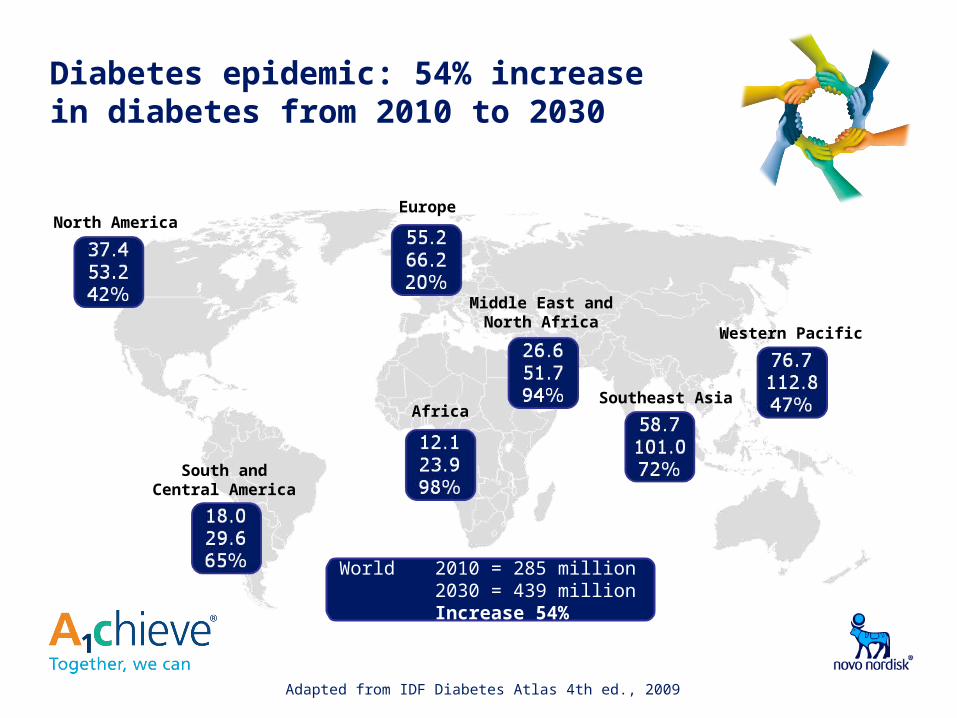
Diabetes epidemic: 54% increase in diabetes from 2010 to 2030
Adapted from IDF Diabetes Atlas 4th ed., 2009
World 2010 = 285 million2030 = 439 million
Increase 54%
North AmericaEurope
Middle East and North Africa
Africa
South and Central America
Western Pacific
Southeast Asia

Diabetes: from the globe to your clinic• Assume you are a physician in the
Asia/Western Pacific region, where the diabetes prevalence level is approximately 5-7%
• If you oversee a group of 200 patients, then:
• 14 will have diabetes (7%)
• 11 of these 14 remain undiagnosed (75%)
• Screen for high risk groups
• Only 2 of these people are undergoing optimal treatment
• Only 1 of these people have their diabetes properly controlled
IDF Diabetes Atlas 4th ed., 2009Asia-Pacific Type 2 Diabetes Policy Group. Practical Targets and
Treatments 4th Ed. 2005.

Poor glucose control is associated with increased risk of complications
Stroke
Retinopathy and blindness
Heart disease
Kidney disease
Neuropathy
Diabetic foot disease
Peripheral vascular disease
Erectile dysfunction
International Diabetes Federation. Diabetes Atlas, 2006

Prevalence of Retinopathy and NeuropathyRetinopathy and Neuropathy in Type 2 diabetic patients in Iran compared to other countries
Study Location
Prevalence of Retinopathy (%)
Qazvin 51.1
Isfahan 45.4
Germany 16.1
Australia 21.9
Egypt 32.1
Study location
Prevalence of Neuropathy (%)
Isfahan 75.1
Islamshahr 33.3
Diabetes Atlas, 3rd edition, International diabetes federation, 2006
France 28.8
Australia 13.1
Egypt 21.9
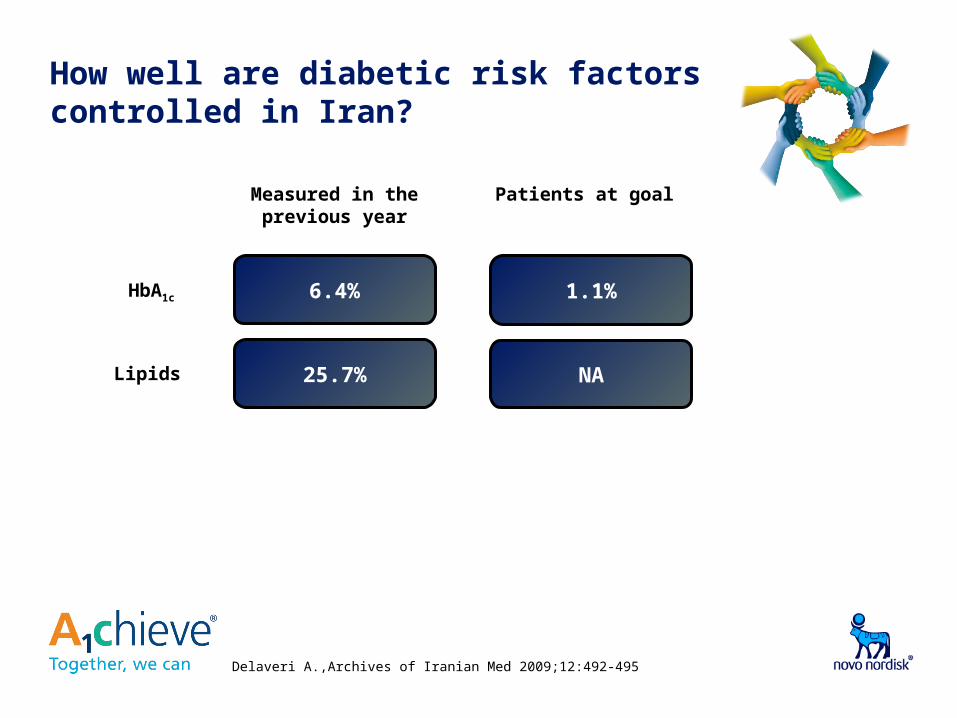
How well are diabetic risk factors controlled in Iran?
6.4% 1.1%
25.7% NA
HbA1c
Measured in the previous year
Patients at goal
Lipids
Delaveri A.,Archives of Iranian Med 2009;12:492-495

Question #3• What do you think is the greatest obstacle to
improving diabetes care in Iran?
1. Lack of infrastructure/healthcare training
2. Patient compliance towards diet and exercise
3. Physician attitude
4. Resistance of patients to medication
5. Difficulty managing diabetic complications
6. Other
Question #4
• Approximately what percentage of patients do you treat with insulin?
1. 5%
2. 10%
3. 15%
4. 20%
5. >20%

Antidiabetic treatment use: OHA’s favoured, insulin used infrequently
International Diabetes Federation. Diabetes Atlas. 2006: 273-287.
Suboptimal care results in diabetic complications
• Assume you are a physician overseeing a group of approximately 50 patients diagnosed with diabetes
• If your clinic is in Iran:• 38 patients will have suboptimal control of
HbA1c
• Approximately 4 patients (8%) will be treated with insulin; 28 patients will be treated with OADs only and 18 patients will be treated with diet only
• 6 patients (11.3%) will suffer from renal failure as a complication of their diabetes
IDF Diabetes Atlas 4th ed., 2009Novo Nordisk. Changing Diabetes Barometer. 2009
International Diabetes Federation. Diabetes Atlas. 2006: 273-287.

Local insulin usage: human insulin preferred vs. analogues in Iran
0
20
40
60
80
100
Iran
Analogue Insulins
Human Insulins
Insu
lin U
sag
e (
%) • Prevalence of Diabetes in
Iran in 2007 was 8.7%*
• In Iran, insulin is prescribed to less than 7.5% of diabetic patients
• Uncontrolled blood sugar = increased risk of complications
99%
1%
*Esteghamati A, et al. Third national surveillance of risk factors of non-communicable diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and Dyslipidemia. BMC Public Health 2009, 9:167** National Pharmaceutics Statistics, Ministry of Health, 2009,Iran
**

Question #5
• Which of the following factors do you feel is most important to improving diabetes care in your region in the future?
1. Diabetes prevention via education programmes
2. Patient lifestyle changes (diet and exercise)
3. Treatment advances/new drugs
4. Improved training for clinicians
5. Political will/government investment in diabetes care
6. Other

Age atdiagnosis
First majorcomplications
*Average risk reduction
Better treatment extends and improves lives
First minorcomplications
Baseline (HbA1c = 7.0%)EarlierDiagnosis +EnhancedTreatment
69-71
71”Mr. Lee"
Age at diabetes diagnosis 52
65-6852
25-40%* 25-65%*
71 years
52 66-68
68 years
Baseline(HbA1c =9.1%)”Mr. Kim"
Age at diabetes diagnosis 52
60-62
UKPDS Risk Engine: modelled data based on newly diagnosed cohort at age 52
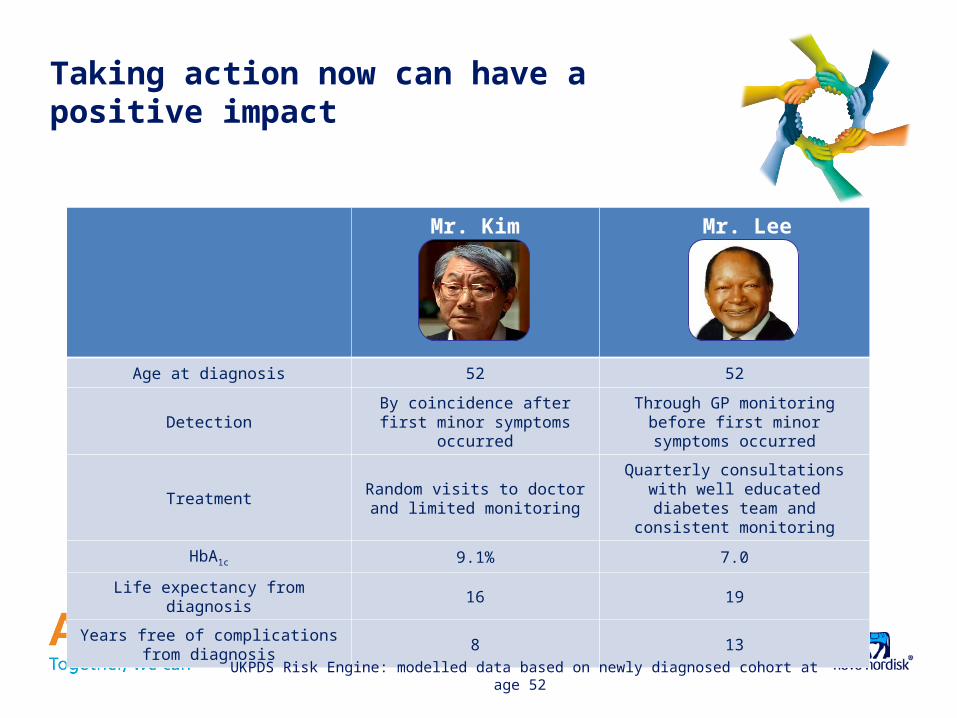
Taking action now can have a positive impact
Mr. Kim Mr. Lee
Age at diagnosis 52 52
DetectionBy coincidence after first minor symptoms occurred
Through GP monitoring before first minor symptoms occurred
TreatmentRandom visits to doctor and
limited monitoring
Quarterly consultations with well educated diabetes team
and consistent monitoring
HbA1c 9.1% 7.0
Life expectancy from diagnosis 16 19
Years free of complications from diagnosis
8 13
UKPDS Risk Engine: modelled data based on newly diagnosed cohort at age 52






