
Impact of Maternal Education and Health Related Behaviors on Infant
and Child Survival in Pakistan
G. Mustafa ZahidUniversity of Western Ontario
London, Ontario

Research Question
What is the nature of the association between mother’s schooling and child mortality on the one hand, and between the health seeking behavior of the mother and child mortality on the other hand?

Introduction
The level of infant and child mortality is widely used not only as a demographic measure, but also as an important indicator of the level of the health in a society and of its living standard.
Women are known and considered all over the world as the first providers of health care in the home. Mother’s behavior has a great impact on health and survival of children through curative means when the child is sick, whether the mother uses modern medicine or traditional practices.

Introduction (contd. i)
Prenatal visits enable mothers to obtain health information on prevention as well as specific medical attention which results in low morbidity and mortality in developing countries. Therefore, the mother’s behavior in seeking health either as a preventive or curative treatment is an important factor in determining child survivorship through the child’s health and nutritional status, as well as through her own health.

Introduction (contd. ii)
Women are expected by policy makers and society in general to implement the child survival revolution by:
1. Bringing children to be immunized four times during the first year of life;
2. Procuring or producing oral re-hydration solutions and administering them to a sick child many times over the course of each day of every bout of diarrhea;
3. Breastfeeding their babies on demand until the child is six months to two years old and processing and feeding proper weaning foods in frequent meals to small children at the appropriate ages;
4. Bringing children under age five to a weight surveillance program monthly.

What is Health Seeking behavior
Health seeking behavior includes consulting a physician during the prenatal (for mother’s immunization against tetanus), ante-natal (place of delivery and help at delivery) and postnatal (immunization of the child) period, especially when disease symptoms are aparent.

Previous Studies
Bicego and Boerma, 1993; Rajna et al., 1998; Caldwell, 1979 ,1987, 1990, 1994; Desai and Alva, 1998; Hobcraft et al., 1984; Martin et al., 1983; Sathar, 1985; D’Souza and Bhuiya, 1982; Streatfield, 1992.

Theoretical Framework
Socio-economic determinants
Maternalfactors
EnvironmentalContamination
Nutrientdeficiency
Injury
Healthy Sick
GrowthFaltering
MortalityPersonalIllnessControl
Treatment
Prevention
Source: Mosley and Chen 1984, PDR Supplement 10: 25-45

Objectives
To examine the pattern of health seeking behavior of mothers and its effects on childhood mortality.
To examine and compare the effects of socio-economic factors through demographic and health seeking behavior especially education of mother on childhood mortality.

Source of Data and Method of Analysis
Data derive all its variables under study from the Pakistan Demographic and Health Survey (PDHS) of 1990-91, a nationally representative survey covering all four provinces of the country, the first and up till now the latest survey undertaken by Macro International in conjunction with the National Institute of Population Studies (NIPS).

Continued (methods)
The dependent variable is the survival times of the children during neonatal, infant and childhood ages. Since many children have not completed the event at the date of survey these observations were considered as censored. Cox’s proportional hazard model is appropriate for the analysis of data that includes censored observations. Unlike parametric models, the proportional hazard model does not make any assumption on the distribution of the timing function and thus appropriate for events whose empirical distribution of the timing function is unknown.

1) Summary Results: NeonatalCovariates Regression Coefficients Exp (β)
Age of mother at Birth
15-19 0.000 1.000
20-29 -0.104** 0.901
30-49 -0.092** 0.912
Birth Order
1 0.000 1.000
2-3 0.436*** 1.547
4+ 0.381** 1.464
Immunization
No 0.000 1.000
Incomplete -1.863** 0.155
Complete -3.906*** 0.020
Ever-breastfed
Yes 0.000 1.000
No 2.302*** 10.045
Antenatal Care
Doctor/ LHV / Nurse 0.000 1.000
Traditional 0.351*** 1.421
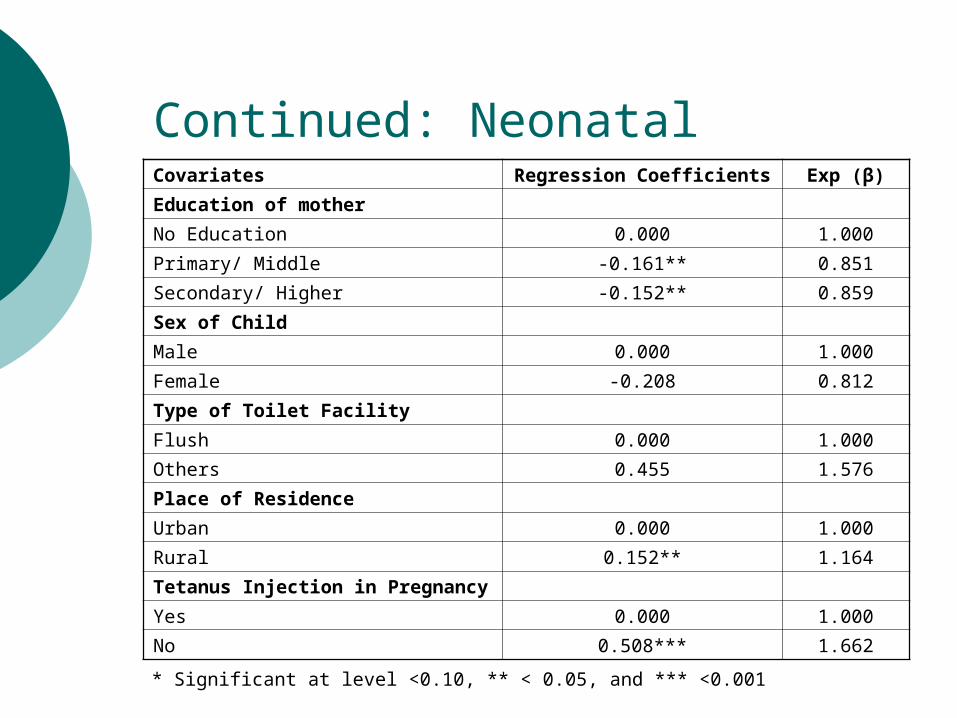
Continued: NeonatalCovariates Regression Coefficients Exp (β)
Education of mother
No Education 0.000 1.000
Primary/ Middle -0.161** 0.851
Secondary/ Higher -0.152** 0.859
Sex of Child
Male 0.000 1.000
Female -0.208 0.812
Type of Toilet Facility
Flush 0.000 1.000
Others 0.455 1.576
Place of Residence
Urban 0.000 1.000
Rural 0.152** 1.164
Tetanus Injection in Pregnancy
Yes 0.000 1.000
No 0.508*** 1.662 * Significant at level <0.10, ** < 0.05, and *** <0.001

2: Summary Results: InfantsCovariates Regression Coefficients Exp (β)
Age of mother at Birth
15-19 0.000 1.000
20-29 -0.085** 0.918
30-49 -0.723** 0.485
Birth Order
1 0.000 1.000
2-3 0.227*** 1.255
4+ 0.299** 1.349
Immunization
No 0.000 1.000
Incomplete -1.547** 0.213
Complete -1.208*** 0.299
Ever-breastfed
Yes 0.000 1.000
No 1.519*** 4.566
Antenatal Care
Doctor/ LHV / Nurse 0.000 1.000
Traditional 1.076*** 2.932

Continued: InfantsCovariates Regression Coefficients Exp (β)
Education of mother
No Education 0.000 1.000
Primary/ Middle -0.457* 0.633
Secondary/ Higher -0.398*** 0.672
Sex of Child
Male 0.000 1.000
Female -0.161 0.851
Type of Toilet Facility
Flush 0.000 1.000
Others 0.113** 1.120
Place of Residence
Urban 0.000 1.000
Rural 0.147** 1.158
Tetanus Injection in Pregnancy
Yes 0.000 1.000
No 0.498*** 1.645

3: Summary Results: ChildrenCovariates Regression Coefficients Exp (β)
Age of mother at Birth
15-19 0.000 1.000
20-29 -0.503*** 0.650
30-49 -0.643* 0.526
Birth Order
1 0.000 1.000
2-3 0.605** 1.831
4+ 1.118* 3.059
Immunization
No 0.000 1.000
Incomplete -0.659* 0.517
Complete -0.755*** 0.470
Ever-breastfed
Yes 0.000 1.000
No 1.015** 2.760
Antenatal Care
Doctor/ LHV / Nurse 0.000 1.000
Traditional 1.042** 2.835

Continued: ChildrenCovariates Regression Coefficients Exp (β)
Education of mother
No Education 0.000 1.000
Primary/ Middle -0.102*** 0.903
Secondary/ Higher -0.491*** 0.612
Sex of Child
Male 0.000 1.000
Female 0.072*** 1.075
Type of Toilet Facility
Flush 0.000 1.000
Others 0.687** 1.988
Place of Residence
Urban 0.000 1.000
Rural 0.127** 1.136
Tetanus Injection in Pregnancy
Yes 0.000 1.000
No 0.009 1.009

Conclusion
The highest mortality occurred among children born to mothers aged less than 20 years.
Neonatal and infant mortality is higher for males than for females; this relationship is then reversed for child mortality. This shows that there are some gender related differences in child rearing practices that favor boys over girls.
The high mortality of first and high order births may be related to the age of the mother at the child’s birth which is termed as high risk births for very young and older mothers.

Conclusion (continued)
The analysis identifies that the mothers who have a better perception of disease processes and an excellent aptitude to utilize modern health services are qualitatively distinct from those who do not.

Conclusion (continued)
Differences in infant and child mortality have also been observed according to the place of residence at the time of the survey. Mortality is higher in rural areas than in urban areas as expected. This finding might be due to factors including sanitation, water supply, and unequal distribution of health facilities between rural and urban areas of the country.

Conclusion (continued)
The important conclusion from this analysis of differentials in infant and child mortality is that mother’s education and age at birth are strongly correlated with lower neonatal and infant mortality.







