
Blood, Vol 70, No 1 (July), 1987: pp 69-76 69
Immunological Specificity and Mechanism of Action of
IgG Lupus Anticoagulants
By Vittorio Pengo, Perumal Thiagarajan. Sandor S. Shapiro, and Marilyn J. Heine
Although observations have implied that lupus anticoagu-
lants have immunologic specificity toward anionic phos-
pholipids. this assumption has been directly demonstrated
in only one patient with a monoclonal 1gM paraprotein. We
tested the generality of this hypothesis directly by isolating
five lgG lupus anticoagulants from patients with lupuslike
syndromes and/or thrombosis. lgG lupus anticoagulant
fractions were isolated free of other plasma proteins and
free of contaminating phospholipid by adsorption to and
elution from cardiolipin-cholesterol-dicetyl phosphate
liposomes. followed by chromatography on protein A-
Sepharose. Cardiolipin liposomes. but not phosphatidyl-
choline liposomes, were capable of removing all, or nearly
all. lupus anticoagulant activity from patient plasma. The
affinity-purified lgG preparations reacted with cardiolipin,
L UPUS ANTICOAGULANTS are acquired inhibitors
of coagulation tests that occur in systemic lupus ery-
thematosus (SLE), in various other clinical settings, and in
apparently normal persons.’
Because the lupus anticoagulant effect is noted in all
phospholipid-dependent coagulation tests2�6 and because of
the correlation between the presence of lupus anticoagulants
and reactivity against cardiolipin in solid-phase immunoas-
says,7�” lupus anticoagulants have been widely assumed to be
antibodies reactive against anionic phospholipids. Actually,
the immunologic nature and mechanism of action of the
Iupus anticoagulant effect have only been demonstrated in
one patient.’2 In 1980, our laboratory’2 clarified the mecha-
nism ofaction ofan 1gM A paraprotein with lupus anticoagu-
lant activity. The purified paraprotein showed immunologic
reactivity against the anionic phospholipids phosphatidylser-
me, phosphatidylinositol, and phosphatidic acid, but did not
react with the neutral phospholipids phosphatidylcholine or
phosphatidylethanolamine. This protein inhibited the bind-
ing of prothrombin and factor X to phospholipid micelles,
thereby accounting for the prolongation of phospholipid-
dependent coagulation tests.
Since this initial work, it has been widely assumed,
although not rigorously demonstrated, that all lupus antico-
agulant activity is due to the same mechanism. However,
other authors have stressed the heterogeneity of the lupus
anticoagulant patient population, as well as the apparent
variability in the response of lupus anticoagulant tests to the
presence of platelets,’3 to argue against a common mecha-
nism ofaction. Interestingly, neither the original patient, nor
four other 1gM lupus anticoagulants we subsequently stud-
ied, nor 1gM lupus anticoagulants reported by others,’4”5
have been associated with thrombosis. Most lupus anticoagu-
lants, on the other hand, occur in a setting of polyclonal
increases in immunoglobulins and are associated with a high
incidence of thrombosis.”62’ To assess whether there is
indeed a general mechanism for the lupus anticoagulant
effect, a technique for isolating lupus anticoagulants from
plasma of patients without monoclonal paraproteins is neces-
sary. The preparation must be a pure immunoglobulin free of
contaminating phospholipid. We developed a technique that
phosphatidylserine. phosphatidylinositol. and phosphatidic
acid, but not with phosphatidylcholine or phosphatidyl-
ethanolamine. and inhibited calcium-dependent binding of
prothrombin and of factor X to phosphatidylserine-coated
and to cardiolipin-coated surfaces. F(ab’)2 fragments
retained Iupus anticoagulant activity and bound to cardioli-
pin in an enzyme-linked immunosorbent assay (ELISA).
Anticardiolipin and lupus anticoagulant activity were bothpresent in acidic fractions on isoelectric focusing. These
data strongly suggest that most, if not all, lupus anticoagu-
lants are antibodies that have immunologic specificity
towards anionic phospholipids. thereby blocking the calci-
um-mediated binding of vitamin K-dependent coagulation
factors to coagulation-active phospholipid surfaces.
S 1987 by Grune & Stratton, Inc.
uses affinity purification on cardiolipin liposomes followed
by protein A-Sepharose chromatography to prepare phos-
pholipid-free purified lupus anticoagulants. We isolated five
IgG lupus anticoagulants, four from patients with a history
of thrombosis, and examined the immunologic nature of their
interaction with phospholipids and the mechanism of their
inhibition of phospholipid-dependent coagulation tests.
MATERIALS AND METHODS
Human thrombin was a gift from Dr John Fenton, New York
State Department of Health Laboratories, Albany. Pepsin waspurchased from Worthington Biochemical, Freehold, Ni. Protein
A-Sepharose, Sephacryl G-75 (Superfine) and Sephacryl 5-300
were obtained from Pharmacia Fine Chemicals, Piscataway, NJ.
Ampholines were purchased from LKB, Bromma, Sweden. Phos-phatidylserine, phosphatidylinositol, phosphatidylethanolamine,
phosphatidic acid, and phosphatidylcholine were obtained from
Supelco, Bellafonte, PA. Cardiolipin, dicetyl phosphate, cholesterol,alkaline phosphatase-labeled goat antibodies to human lgG. human1gM, and rabbit IgG, as well as p-nitrophenyl phosphate and bovineserum albumin (BSA) (fraction V) were purchased from SigmaChemical, St Louis. The purity of phospholipids was checked by
thin-layer chromatography.2’ Russell viper venom was obtained
from Burroughs Wellcome, Raleigh, NC, and Thrombofax waspurchased from Ortho Diagnostic Systems, Raritan, NJ. Antisera tohuman IgG, IgA, and 1gM were obtained from Meloy Laboratories,
From the Cardeza Foundation for Hematologic Research.
Department of Medicine, Jefferson Medical College of Thomas
Jefferson University, Philadelphia.Submitted December 5. 1986; accepted February 1 1. 1987.Supported in part by Grants No. HL-09163. AG-04861 (5.5.5.).
HL-27278 (P. T.), and T32-AM-07084 (M.J.H.)from the National
Institutes ofHealth; an Established Investigator Award (84-190); a
grant-in-aid from the American Heart Association (P. T.); and the
Sheryl N. Hirsch Award ofthe Lupus Foundation of Philadelphia
(5.5.5.). V.P. is a Visiting Research Fellow from the Cardiology
Department. University ofPadua. Italy.Address reprint requests to Dr Sandor S. Shapiro. Cardeza
Foundation, Jefferson Medical College. 1015 Walnut St. Philadel-
phia, PA 19107.© 1987 by Grune & Stratton. Inc.
0006-4971/87/7001-0008$3.00/0
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

70 PENGO ET AL
Springfield. VA. Standard laboratory chemicals were supplied byFisher Scientific, Fair Lawn, NJ. Carrier-free 1251 was obtained fromCambridge Nuclear, Billenica, MA.
JgG Purification
Lupus anticoagulant plasma was clotted by incubation with 2
U/mL of human thrombin for 2 hours at 37#{176}.Fibnin was removed bycentnifugation at 4#{176}Cfor 10 minutes at 14,000 g. y-Globulins wereprecipitated from the supernatant serum by addition at 4#{176}Cof an
equal volume of saturated ammonium sulphate. After 25 minutes of
stirring, the precipitate was recovered by centnifugation in the coldfor 10 minutes at 14,000 g. The precipitate was dissolved in
approximately one-seventh the original plasma volume, using Tnis-buffered saline (TBS: 0.02 mol/L of Tnis, 0. 1 5 mol/L of NaCI, pH
7.4), and applied to a 2.5 x 90-cm column of Sephacryl 5-300equilibrated with TBS. Fractions of 2.5 mL were collected and testedqualitatively for IgG, 1gM. and IgA by Ouchterlony double diffusion
and for lupus anticoagulant activity by their ability to prolong thedilute Russell viper venom time (RVVT) of normal plasma.23’�4
Fractions containing lupus anticoagulant activity were pooled and
applied to a I x 5-cm column of protein A-Sepharose equilibratedwith TBS. The lupus anticoagulant activity, in every case, wasretained on the column and was eluted using a buffer consisting of
0.1 mol/L of glycine, 0.5 mol/L of NaCl, pH 3, and immediatelyneutralized with I mol/L of Tnis buffer, pH 8.4. Eluates were
dialyzed against TBS before being tested for lupus anticoagulantactivity. Control lgG was prepared from normal plasma in anidentical manner. IgG prepared in this manner is free of other
immunoglobulins and shows no bands other than IgG on sodiumdodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE)
after staining with Coomassie blue.
F(ab’)2 Preparation
After dialysis against acetate buffer (0.2 mol/L of Na acetate, 0.2mol/L of NaCI, pH 4), purified IgG (2 to 3 mg/mL) was incubated
at 37#{176}Cfor 20 hours with freshly prepared pepsin at a weight ratio of50: 1 25 At the end of the 20-hour incubation, no intact IgG wasdetectable by SDS-PAGE. The reaction was stopped by adding solid
Tnis (5 to 10 mg). The digested material was dialyzed against TBSand applied to a 1 x 5-cm protein A-Sepharose column. Theflowthrough, containing the F(ab’)2 fragments, was concentrated by
Amicon ultrafiltration using PM-l0 membranes (Amicon, Lexing-ton, MA) and tested for lupus anticoagulant and anticardiolipinactivities. The protein A-Sephanose flowthrough was free of whole
IgG and Fe-fragments, as judged by SDS-PAGE and by doublediffusion against antiserum to human IgG (Fe-specific).
ELISA for Anticardiolipin Antibodies
One microgram of cardiolipin in 25 j�L of ethanol was added toeach well of a 96-well microtiter plate (Falcon #391 1, BectonDickinson, Oxnard, CA) and evaporated under a stream of nitrogenfor 20 minutes, after which the wells were washed twice with I 00 �zL
of phosphate-buffered saline (PBS: 8 g/L of NaCI, 0.2 g/L ofKH,P04. 2.9 g/L of Na2HPO4 . l2H20, 0.2 g/L of KCI, pH 7.4).All subsequent steps were carried out at room temperature. One
hundred microliters of 10% fetal calfserum (FCS) in PBS was thenadded to each well and incubated for 2 hours to block nonspecific
binding. After the plates were washed six times with PBS, 100 j.tL of
plasma diluted in PBS containing 10% FCS was added to each well
and incubated for I hour. The wells were washed six times with PBS,after which 100 �.iL of a 1:1000 dilution of alkaline phosphatase-
labeled goat anti-human IgG or goat anti-human 1gM was added
and incubated for I hour. The plates were then washed six times
more in PBS, and 100 �iL of freshly prepared p-nitrophenyl phos-
phate solution (1 mg/mL in 10% diethanolamine buffer, pH 9.8)was added to each well. After I -hour incubation, the absorbance was
measured at 405 nm, using a Titertek Multiscan plate reader (FlowLaboratories, McLean, VA). In experiments using F(ab’)2, 100 �zL
of a 1:400 dilution of rabbit anti-human F(ab’)2 (Jackson Laborato-
nies, Avondale, PA) was used as a second antibody, and alkalinephosphatase-labeled goat anti-rabbit IgG was used as the developingantibody.
The ELISA assay for antibody activity against other phospholi-pids was performed in a similar manner, except that: (a) Two
micrograms of phosphatidylsenine, phosphatidylinositol, phospha-tidic acid, phosphatidylethanolamine, or phosphatidylcholine in 10
�L ofchloroform was added to each well ofa 96-well microtiter platecontaining 30 zL of ethanol; (b) when phospholipid reactivity of
eluates from cardiolipin liposomes was studied, 100 �iL-aliquots ofeluate were used; and (c) the reaction was stopped after I 5 minutes.
Isoelectric Focusing
Forty grams of Sephadex G-75 was washed and prepared asdescribed by the manufacturer, and finally suspended in 90 mL of
d#{231}ionized water. To the Sephadex was added: 2.5 mL of Ampholine,
pH 5 to 7; 2.5 mL of Ampholine. pH 7 to 9; and S mL of purified
patient IgG (10 mg/mL in 1% glycine). After gentle stirring, the
mixture was poured into a 10 x 20-cm glass tray, and excess waterwas evaporated under a stream of air. Focusing was performed at10#{176}for 1 5 hours at 8 W constant power. The gel was then cut into six
fractions. A small amount of each fraction was resuspended in
deionized water for pH measurement; the remainder ofeach fractionwas resuspended in 5 mL ofTBS in a small column, and the proteinswere eluted by washing the column with 5 mL of TBS. Column
eluates were dialyzed against TBS and tested for lupus anticoagu-lant and anticardiolipin activities.
Analytical isoelectnic focusing was performed in an LKB Multi-phor apparatus on 5% polyacrylamide gels containing 2.2% (wt/vol)Ampholine, pH 5.5 to 8.5. Purified IgG or liposome eluates weredialyzed against deionized water, applied to the gel, and run at 50mA with a constant power of 25 W. The gels were fixed for I hour in
a solution of 5% tnichloroacetic acid and 5% sulfosalicylic acid and
stained using the Bio-Rad silver-staining kit (Bio-Rad Laboratories,
Richmond, CA).
Immunoaffinity Purification ofAnticardiolipin Antibodies
Liposomes were prepared essentially according to the method of
Kinsky.” A mixture of cardiolipin, cholesterol and dicetyl phosphate(molar ratio I 0: 1 5:2) in chloroform was dried in a stream of nitrogen
in a 25-mL glass tube. The lipids were resuspended in 1 mL of 0.15
mol/L of NaCl by vigorous agitation, using a vortex mixer. Afterresuspension, the concentration of phospholipids was 5.3 to 5.9mg/mL. Ten milliliters each of saline and plasma were added to I
mL of liposome suspension. and the mixture was incubated at 4#{176}Cfor 30 minutes. After centnifugation at 27,000 g for 10 minutes at4#{176}C,the precipitate was washed three times with 0. 1 5 mol/L ofNaCl. The precipitate was resuspended by vigorous agitation in 2
mL of 3 mol/L of NaCI, following which the suspension was addedto a separatory funnel containing 10 mL of ethyl ether.27 Aftersettling, the clear aqueous layer was removed from the bottom of the
funnel, centrifuged, and dialyzed in the cold against three changes ofTBS. The dialyzed eluate was tested for lupus anticoagulant activity
by the dilute RVVT, for immunoglobulin class by Ouchterlonydouble diffusion, and for reactivity against phospholipids byenzyme-linked immunosorbent assay (ELISA). The eluate wasfurther purified by protein A-Sepharose column chromatography, as
previously described, and retested for purity and for biological
activities.
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

MECHANISM OF LUPUS ANTICOAGULANTS 71
Labeling ofCardiolipin with !25J
Cardiolipin was radioiodinated directly by the chloramine-T
method, as described by Antonov and colleagues.28 Thin-layer
chromatography demonstrated that -60% of the added radioactivity
had been incorporated into cardiolipin. Most of the remainder
traveled with the solvent front. Labeled cardiolipin had the samemobility as standard cardiolipin. The spot containing the radioactive
cardiolipin was extracted from the silica gel plate as described
previously.22 When re-run on thin-layer chromatography, this
extracted labeled material showed a single spot with the mobility of
standard cardiolipin; no radioactivity was present in the solvent
front. On the basis of phosphorus content,29 the specific radioactivityof ‘25I-cardiolipin was calculated as 26 mCi/mmol.
Coagulation Studies and Assessment of Lupus
Anticoagulant Activity
Venous blood was collected in one-tenth volume of 3.8% tnisodium
citrate, and plasma was obtained by centnifugation in the cold at
2,300 g for 15 minutes. Routine coagulation studies were performed
as previously described.’2 Lupus anticoagulant activity of patient
plasma was assessed by the dilute RVVT, as previously
described.23’24 In our laboratory, the dilute RVVT of normal plasmais 25.6 ± 2.6 seconds ( ± 2 SD). Patients were not considered to have
lupus anticoagulants unless their dilute RVVT was >30 seconds andwas not corrected by addition of an equal volume of normal plasma.
The anticoagulant activity of IgG or of F(ab’)2 was measured in the
dilute RVVT by adding 200 �L of the dialyzed test material, instead
of the usual 100 ML, to this system. Addition of 200 �tL of TBS aloneto normal plasma gives a dilute RVVT of 27 to 30 seconds.
Prothrombin and Factor X Binding to Phospholipid
Prothrombin was purified from normal plasma by a slight modifi-cationt#{176}of the method of Morrison and Esnouf,3’ and labeled with1251 by the lodogen method32 to a specific activity of 231 Ci/mmol.
Factor X was purified according to the method of Miletich andco-workers,3’ with some modifications described previously,’2 and
labeled with 1251 by the lodogen method to a specific activity of 60Ci/mmol. Two micrograms of phospholipid was added to each well
of a microtiter plate and dried and washed as described above. Two
hundred microliters of TBS containing I mg/mL of BSA was thenadded, to block nonspecific binding, and the plates were incubatedfor I hour. After plates were washed once with TBS, 150 �zL of TBS
containing I mg/mL of BSA and 2 mmol/L ofcalcium was added,
followed immediately by 50 �L of immunoaffinity-punified IgG (134
zg/mL) or control IgG ( I 50 �.�g/mL) in TBS. The plates wereincubated for 1 hour at room temperature, after which 10 ML of
labeled prothrombin (I .4 x 106 cpm) or factor X (I .7 x 106 cpm)was added. After 10-minute incubation at room temperature, the
wells were aspirated dry, and the bottoms of the wells were punched
out and counted in an Isodyne ‘y-counter (Model 1 185, GD. Searle,
Chicago). Maximum binding of prothrombin was determined by
addition of TBS-albumin-calcium buffer alone, in the absence of any
IgG. As a control, prothrombin and factor X binding were measuredin the presence of 2 mmol/L of EDTA and were 3% and I 1% of
maximum binding, respectively. Residual binding, measured in the
presence of a 50-fold excess of cold prothrombin or factor X, wassubtracted from total binding, to give “specific” binding.
Patients
Patient no. I. The patient was a 35-year-old man with a 10-yearhistory of a manic-depressive illness for which he had been treated
with lithium, chlorpromazine, and other tnicyclic antidepressants.
He had not received any medication except lithium in the 6 months
prior to study. He had had several episodes of deep vein thrombosis
as well as at least one probable pulmonary embolism. He had a
normal platelet count, and his serological test for syphilis (RPR) was
negative. At the time of the study, he was receiving warfanin.
Patient no. 2. The patient was a 39-year-old woman with SLE of
8-year duration who had end-stage renal disease and was onhemodialysis. She had had a cerebrovascular accident at the age of
35, and also had a history of possible pulmonary emboli. She had
occlusion of arteniovenous shunts in the forearm on at least two
occasions. Her platelet count was in the low-normal range. She had a
false-positive serological test for syphilis (RPR) at the time of
diagnosis, but not at the time of study, when she was receiving 20 mg
of prednisone every other day.Patient no. 3. The patient was a 32-year-old woman with a
history of three spontaneous abortions, after which she delivered a
full-term live baby while on steroid therapy. She had a normal
platelet count. She had had a false-positive serology (RPR) since her
teens, but had no other signs of SLE.Patient no. 4. The patient was a 49-year-old man with a 10-year
history of SLE. He had an acute episode of right ileofemoral arterial
occlusion I year earlier, at which time a lupus anticoagulant was
discovered. He had a normal platelet count and a negative serologi-
cal test for syphilis (RPR).Patient no. 5. The patient was a 58-year-old woman with renal
disease and possible SLE. She had no history of thromboembolic
phenomena. She had a normal platelet count and a false-positive
serology (RPR). At the time ofthe study, she was receiving 20 mg of
prednisone daily.
As shown in Table I , all five patients had a prolonged dilute
RVVT, which did not normalize on addition of an equal volume of
normal plasma. Four of the five patients had a prolonged activated
partial thromboplastin time (APTT), whereas only one (patient no.
1, receiving warfarin) had a prolonged prothrombin time (PT).
RESULTS
Immunoglobulin Nature ofthe Lupus Anticoagulant and
Anticardiolipin Activities
Lupus anticoagulant activity in all five patients gel-
filtered on Sephacryl 5-300 in the IgG peak. Three patients
(patients no. I, 3, and 5) had, in addition, a very small
amount of inhibitory activity associated with the 1gM peak.
The maximum prolongation of the dilute RVVT in 1gM
fractions was 2 seconds, whereas the maximum prolongation
in the IgG peak was I 3 to 14 seconds. No prolongation of the
RVVT was observed in any of the Sephacryl 5-300 fractions
of control plasma. The IgG peaks were further purified by
chromatography on protein A-Sepharose. Glycine eluates of
the protein A-Sepharose columns contained the inhibitory
activity, whereas the flowthrough fractions had no lupus
anticoagulant activity.
IgG anticardiolipin activity was detected in all five patient
Table 1 . Screening Coagulation Tests
Patient
1 2 3 4 5 Normal
APTT (s) 90.0 27.0 42.6 38.4 42.0 23-36
PT(s) 23.2 11.7 13.2 12.2 12.0 11.5-13.5
Dilute RVVT (5)
Patient 38.2 33.4 34.0 36.5 46.3 23-28.2
Patent+normal(1:1) 36.6 30.4 29.9 32.0 42.7 23-28.2
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom
A
K
./
/
.,.
I
7
45
40
61
I-> 35>
30
10
�o84
z
a 06z
z� 04
0
0
4
U 02
C0NTR0,�,,
- -
�
�-�4 ! I I
0 2.0 4.0 6.0 80 10.0
F(ob’)2 or IgG CONCENTRATION (A2ao)
B
C0NTR0L�
72 PENGO ET AL
After protein A-Sepharose chromatography.
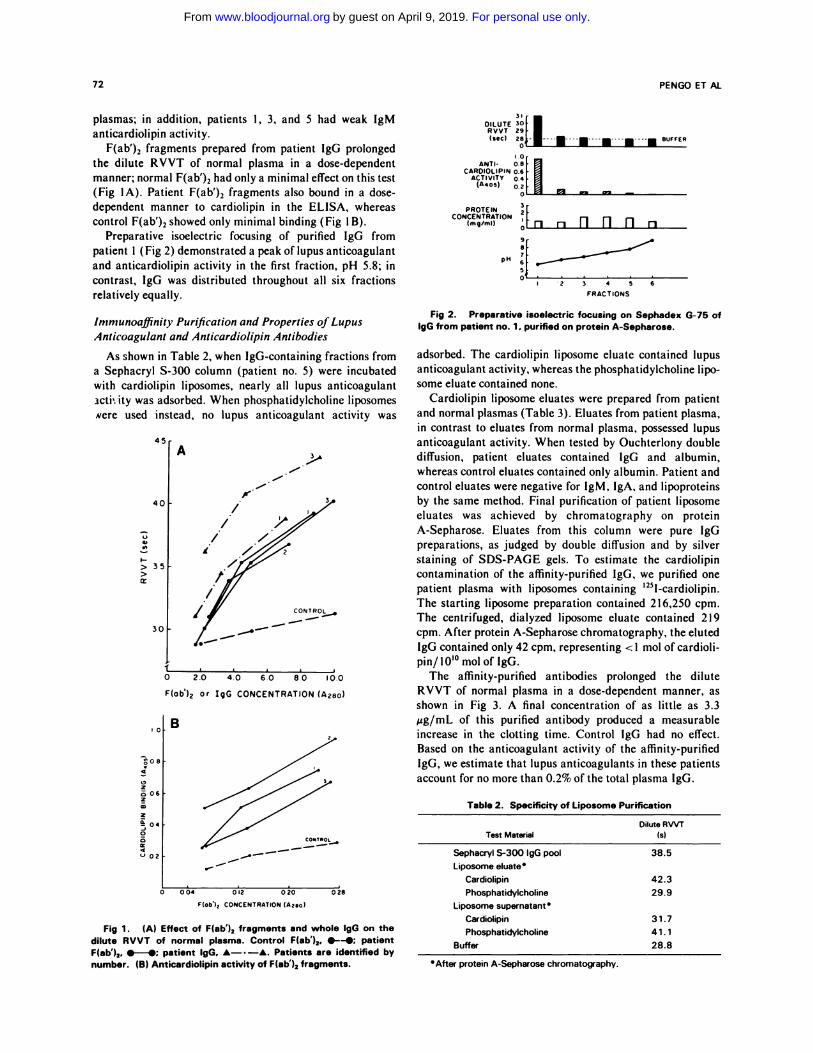
plasmas; in addition, patients I , 3, and 5 had weak 1gM
anticardiolipin activity.
F(ab’), fragments prepared from patient IgG prolonged
the dilute RVVT of normal plasma in a dose-dependent
manner; normal F(ab’)2 had only a minimal effect on this test
(Fig IA). Patient F(ab’)2 fragments also bound in a dose-
dependent manner to cardiolipin in the ELISA, whereas
control F(ab’)2 showed only minimal binding (Fig 1 B).
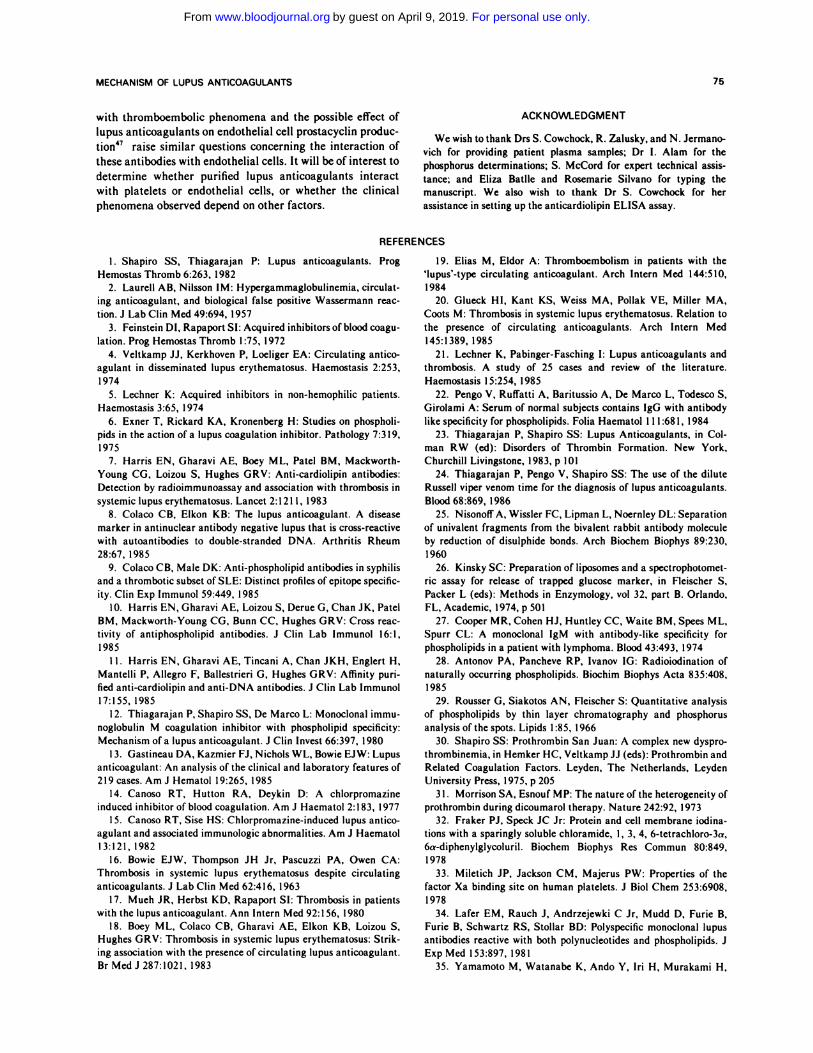
Preparative isoelectnic focusing of purified IgG from
patient 1 (Fig 2) demonstrated a peak of lupus anticoagulant
and anticardiolipin activity in the first fraction, pH 5.8; in
contrast, IgG was distributed throughout all six fractions
relatively equally.
Immunoaffinity Purification and Properties of Lupus
Anticoagulant and Anticardiolipin Antibodies
As shown in Table 2, when IgG-containing fractions from
a Sephacryl 5-300 column (patient no. 5) were incubated
with cardiolipin liposomes, nearly all lupus anticoagulant
icti� ity was adsorbed. When phosphatidylcholine liposomes
were used instead, no lupus anticoagulant activity was
004 012 020 028
F(ob’)2 CONCENTRATION (42101
Fig 1 . (A) Effect of F(ab’), fragments and whole lgG on the
dilute RVVT of normal plasma. Control F(ab’),. --; patientF(ab’),. #{149}-#{149};patient lgG. A- . -A. Patients are identified bynumber. (B) Anticardiolipin activity of F(ab’), fragments.
DILUTE �I�_I___I__�I___I___U.___M�______BUFFER
I .0
ANTI’ 0.8CARDIOLIPIN 0.6
ACTIVITY 04(A405) 0.2
3PROTEIN 21
CONCENTRATION1mg/mi) �Fn ri 11 ri ii �
pH
‘2 3 45 6
FRACTIONS
Fig 2. Preparative isoelectric focusing on Sephadex G-75 oflgG from patient no. 1 . purified on protein A-Sepharose.
adsorbed. The cardiolipin liposome eluate contained lupus
anticoagulant activity, whereas the phosphatidylcholine lipo-
some eluate contained none.
Cardiolipin liposome eluates were prepared from patient
and normal plasmas (Table 3). Eluates from patient plasma,
in contrast to eluates from normal plasma, possessed lupus
anticoagulant activity. When tested by Ouchterlony double
diffusion, patient eluates contained IgG and albumin,
whereas control eluates contained only albumin. Patient and
control eluates were negative for 1gM, IgA, and lipoproteins
by the same method. Final purification of patient liposome
eluates was achieved by chromatography on protein
A-Sepharose. Eluates from this column were pure IgG
preparations, as judged by double diffusion and by silver
staining of SDS-PAGE gels. To estimate the cardiolipin
contamination of the affinity-purified IgG, we purified one
patient plasma with liposomes containing ‘25I-cardiolipin.
The starting liposome preparation contained 216,250 cpm.
The centrifuged, dialyzed liposome eluate contained 219
cpm. After protein A-Sepharose chromatography, the eluted
IgG contained only 42 cpm, representing < I mol of cardioli-
pin/10’#{176}mol of IgG.
The affinity-purified antibodies prolonged the dilute
RVVT of normal plasma in a dose-dependent manner, as
shown in Fig 3. A final concentration of as little as 3.3
sg/mL of this purified antibody produced a measurable
increase in the clotting time. Control IgG had no effect.
Based on the anticoagulant activity of the affinity-purified
IgG, we estimate that lupus anticoagulants in these patients
account for no more than 0.2% of the total plasma IgG.
Table 2. SpecifIcity of Liposo me Purification
Test MaterialDilute RVVT
(s)
Sephacryl S-300 lgG pool
Liposome eluate
Cardiolipin
Phosphatidylcholine
Liposome supernatant
Cardiolipin
Phosphatidylcholine
Buffer
38.5
42.3
29.9
31.7
41.1
28.8
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

08
0
06
04
02
45
40
IMMUNOAFFINITY-PURIF,(0 PT
35
30 CONTROL (gO
IO 20 30 40 50 60
(gO CONCENTRATION (ug/mll
pH 8.5
MECHANISM OF LUPUS ANTICOAGULANTS 73
Fig 3. Effect of affinity-purified patient lgG and control lgG onthe dilute Russell viper venom time (RVVT) of normal plasma.
Table 3. Lupus Anticoagulant Activity of Liposome Eluates From
Patient and Normal Plasma
Patient
A2�Eluate
Dilute RVVT(Eluate/Buffer. s)
1 0.237 34.4/27.9
2 0.991 38.8/27.9
3 0.291 36.9/28.4
A 0.044 26.9/27.8
B 0.114 29.4/28.4
With the ELISA test system, the cardiolipin liposome
eluates reacted with cardiolipin and, as shown for patient I in
Fig 4, also reacted with phosphatidylserine, phosphatidylino-
sitol, and phosphatidic acid, but not with phosphatidyletha-
nolamine, phosphatidylcholine, or dicetyl phosphate. Identi-
cal results were obtained in all four patients tested (patients
no. 1, 2, 3, and 5). Normal IgG, at approximately the same
concentration as in patient eluates, showed no reactivity
against any phospholipids. In addition, liposome eluates from
normal plasma contained only trace amounts of protein and
showed little or no reactivity.
Analytical isoelectric focusing of affinity-purified, phos-
pholipid-free IgG from patients no. 2 and 3 (Fig 5) showed
several bands ofacidic p1; in contrast, the bulk ofnormal IgG
focused in the alkaline range.
Inhibition ofProthrombin and Factor X Binding to
Phosphatidylserine-coated Surfaces
The calcium ion-dependent binding of ‘25I-prothrombin to
phospholipid-coated surfaces was studied in microtiter
plates. As expected, prothrombin bound to phosphatidyl-
serine-coated wells ( 136 to 205 fmol/well, in eight expeni-
ments), and, to a much lesser extent, to cardiolipin-coated
wells (27 and 44 fmol/well, in two experiments). In contrast,
prothrombin binding to phosphatidylcholine-coated wells
was only 6.2 and 7.0 fmol/well in two experiments, a figure
similar to the value obtained for nonspecific binding to
phosphatidylsenine-coated wells in the presence of EDTA (6
to 9 fmol/well). As shown in Fig 6A, immunoaffinity-
purified patient IgG inhibited the binding of prothrombin to
phosphatidylsenine-coated wells by 73% and 66%, respec-
PATIENT ELUATE CONTROL ELUATE CONTROL (gO
fT�:�T..: �
�----�-�.I 8 I 4 12 8 I 4 I � I B I 4 I 2
DILUTIONS OF ELUATE
Fig 4. Antiphospholipid activity (ELISA) of cardiolipin lipo-
some eluates. Because control eluates contained essentially nolgG. reactivity of purified normal lgG is also shown.
tively. Purified IgG from patient no. I (not shown in Fig 6),
tested only at a much lower protein concentration (23
�zg/mL), inhibited prothrombin binding by 25.5%. Binding
of factor X was also inhibited by patient IgG, although to a
slightly lesser extent than prothrombin (Fig 6B). Three
control IgG preparations showed no inhibition of prothrom-
bin or factor X binding. Binding to cardiolipin-coated wells
was also inhibited by patient eluates.
DISCUSSION
Although earlier observations implied that lupus anticoag-
ulants have as their locus of action the negatively charged
phospholipids,”3’56’34 this assumption has been directly dem-
onstrated in only one patient.’2 On the basis of this case, the
correlation that has been observed between the presence of
anticardiolipin activity and lupus anticoagulant activity,7�”
as well as some more recently described absorption studies,35
all lupus anticoagulants have been widely assumed to operate
by the same mechanism. We tested the generality of this
hypothesis directly in five patients with lupuslike syndromes
and/or thrombosis, whose lupus anticoagulants were largely
IgG.
pH 5.5
I 2 3
Fig 5. Analytical isoelectric focusing of normal IgG (lane 1 ) andimmunoaffinity-purifled lgG from patients no. 2 and 5 (lanes 2 and3).
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

80
60
20
23
BUFFER PATIENTS
80
60
40
20
I z
BUFFER PATIENTS
120A cardiolipin liposome eluates invariably contain significant
- amounts of albumin, a further purification step by protein‘00 - - - A-Sepharose chromatography was added.
0
Using these preparations, we were able to obtain a gooddose-response relationship between lupus anticoagulant
activity and IgG concentration and to detect lupus anticoag-
ulant activity at IgG concentrations as low as 3 �ig/mL.
Thus, the dilute RVVT, as normally performed on plasma,
can detect lupus anticoagulants at plasma concentrations of
-
�I�1I:!:::::!1 r-i
- .� � �CONTROLS EDTA
�l0�ig/mL.
The mechanism of prolongation of phospholipid-depen-
dent coagulation tests in the patients we studied is similar to
that of the patient previously reported.’2 Our data clearly
show inhibition by patient affinity-purified IgG of prothrom-
bin binding to phosphatidylserine surfaces and, to a lesser
120 B extent, a similar inhibition of factor X binding. The reason
for this difference in inhibition is not presently known. Our
100 data further indicate that prothrombin can bind to cardioli-
pin surfaces, although to a much lesser extent than to
phosphatidylserine surfaces, and that this binding is also
inhibited by the affinity-purified IgG.
Although all six lupus anticoagulants we studied in this
and the previous’2 report are clearly antibodies with anionic
phospholipid specificity, these anticoagulants probably rep-
resent only a subpopulation of antibodies to anionic phos-
pholipids. Several studies suggest that there may be more
than one type of anticardiolipin antibody,’#{176}’38�#{176}and we have
0
CONTROLS EDTA
studied patients with true-positive and false-positive serolog-
ies whose anticardiolipin antibodies did not possess lupus
anticoagulant activity. Furthermore, the presence of severalFig 6. Effect of affinity-purified antibodies on binding of
1’l-prothrombin (A) and 1’l-factor X (B) to phosphatidylserine-
coated wells. Patients are identified by number. Controls arepurified normal lgG at the same concentration as affinity-purifiedpatient lgG.
We demonstrated that both lupus anticoagulant and anti-
cardiolipin activities are mediated by the F(ab’)2 portion of
IgG and therefore are immunologic in nature. We demon-
strated that all, or nearly all, lupus anticoagulant activity can
be adsorbed on cardiolipin-containing liposomes, but not on
phosphatidylcholine-containing liposomes. We further dem-
distinct bands on isoelectric focusing of the affinity-purified
IgG preparations from our patients raises the possibility that. . . . . . .
not all affinity-purified IgG anticardiohpin antibodies pos-
sess lupus anticoagulant activity.
In addition to anticardiolipin antibodies, other phenomena
have been correlated with the presence of a lupus anticoagu-
lant, including biologic false-positive serology,”3’�#{176}’4’ throm-
bocytopenia,7’2#{176} a history of recurrent abortions,4253 and a
high incidence of thromboembolic phenomena.’7’42’43 Three
of our patients had false-positive serologies, and only 1 may
have had thrombocytopenia, whereas 4 of the 5 had either a
history of thrombosis or of recurrent abortion. Because this is
onstrated that with a combination of cardiolipin-liposome
adsorption, high molanity NaC1 and ether elution, and
protein A-Sepharose chromatography, it is possible to obtain
pure, phospholipid-free, IgG fractions from patient plasma
that interact with anionic but not neutral phospholipids and
also act as lupus anticoagulants. Recently, Harris and asso-
ciates” reported a cardiolipin liposome purification proce-
a highly selected group, no conclusions can be drawn con-
cerning incidence of these clinical findings. Because all
patients had anticardiolipin antibodies, it is surprising that
two had negative serologies. Even a high concentration (56
.�g/mL) of affinity-purified IgG from one patient did not
produce a positive RPR serology, suggesting that antibody
concentration alone may not explain this observation. In this
dune using I mol/L of sodium iodide as the elutant. We connection, it is of interest that the two patients with positive
previously used sodium iodide as an elutant from phospha-
tidic acid36 and phosphatidylsenine37 liposomes, but found
serologies at the time of our study had some 1gM lupus
anticoagulant and 1gM anticardiolipin activity. Because
that these preparations were heavily contaminated with many flocculation tests are more sensitive to 1gM than to
phospholipid, making some subsequent testing procedures
difficult to evaluate. For example, the presence of free and
IgG antibodies,54 a biologic false-positive serology may
correlate better with levels of 1gM than of IgG anticardioli-
IgG-bound phospholipid in the liposome eluates interfered
with coagulation tests and was capable of producing spurious
results on isoelectric focusing. For this reason, we developed
pin antibodies.
The high correlation between lupus anticoagulants and
thrombocytopenia raises the question of the interaction of
the present liposome elution procedure. In addition, since lupus anticoagulants with platelets. The strong correlation
74 PENGO ET AL
‘3z02
0
Za:
a:#{176}‘U.
a:� 40
0320-I
20
a:000
H
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom
MECHANISM OF LUPUS ANTICOAGULANTS 75
with thromboembolic phenomena and the possible effect of
lupus anticoagulants on endothelial cell prostacyclin produc-
tion47 raise similar questions concerning the interaction of
these antibodies with endothelial cells. It will be of interest to
determine whether purified lupus anticoagulants interact
with platelets or endothelial cells, or whether the clinical
phenomena observed depend on other factors.
ACKNOWLEDGMENT
We wish to thank Drs S. Cowchock, R. Zalusky, and N. Jermano-vich for providing patient plasma samples; Dr I. Alam for the
phosphorus determinations; S. McCord for expert technical assis-
tance; and Eliza Batlle and Rosemanie Silvano for typing the
manuscript. We also wish to thank Dr S. Cowchock for herassistance in setting up the anticardiolipin ELISA assay.
REFERENCES
1 . Shapiro 55, Thiagarajan P: Lupus anticoagulants. Prog
Hemostas Thromb 6:263, 1982
2. Laurell AB, Nilsson IM: Hypergammaglobulinemia, circulat-ing anticoagulant, and biological false positive Wassermann reac-
tion. J Lab Clin Med 49:694, 1957
3. Feinstein DI, Rapaport SI: Acquired inhibitors of blood coagu-
lation. Prog Hemostas Thromb 1:75, 1972
4. Veltkamp ii, Kerkhoven P. Loeliger EA: Circulating antico-
agulant in disseminated lupus erythematosus. Haemostasis 2:253,I 974
5. Lechner K: Acquired inhibitors in non-hemophilic patients.
Haemostasis 3:65, 1974
6. Exner T, Rickard KA, Kronenberg H: Studies on phospholi-pids in the action of a lupus coagulation inhibitor. Pathology 7:3 19,
I975
7. Harris EN, Gharavi AE, Boey ML, Patel BM, Mackworth-
Young CG, Loizou 5, Hughes GRV: Anti-cardiolipin antibodies:Detection by radioimmunoassay and association with thrombosis in
systemic lupus erythematosus. Lancet 2:1211, 1983
8. Colaco CB, Elkon KB: The lupus anticoagulant. A disease
marker in antinuclear antibody negative lupus that is cross-reactivewith autoantibodies to double-stranded DNA. Arthritis Rheum
28:67, 1985
9. Colaco CB, Male DK: Anti-phospholipid antibodies in syphilisand a thrombotic subset of SLE: Distinct profiles of epitope specific-ity. Clin Exp Immunol 59:449, 1985
10. Harris EN, Gharavi AE, Loizou 5, Derue G, Chan JK, Patel
BM, Mackworth-Young CG, Bunn CC, Hughes GRV: Cross reac-tivity of antiphospholipid antibodies. J Clin Lab Immunol 16:1,
1985
I 1. Harris EN, Gharavi AE, Tincani A, Chan JKH, Englert H,
Mantelli P. Allegro F, Ballestnieni G, Hughes GRV: Affinity pun-fled anti-cardiolipin and anti-DNA antibodies. J Clin Lab Immunol
17:155, 1985
12. Thiagarajan P, Shapiro 55, Dc Marco L: Monoclonal immu-noglobulin M coagulation inhibitor with phospholipid specificity:Mechanism of a lupus anticoagulant. J Clin Invest 66:397, 1980
1 3. Gastineau DA, Kazmier FJ, Nichols WL, Bowie EJW: Lupus
anticoagulant: An analysis of the clinical and laboratory features of
219 cases. Am J Hematol 19:265, 198514. Canoso RT, Hutton RA, Deykin D: A chlorpromazine
induced inhibitor of blood coagulation. Am J Haematol 2:183, 1977
15. Canoso RT, Sise HS: Chlorpromazine-induced lupus
agulant and associated immunologic abnormalities. Am J Haematol13:121, 1982
16. Bowie EJW, Thompson JH ir, Pascuzzi PA, Owen CA:
Thrombosis in systemic lupus erythematosus despite circulatinganticoagulants. J Lab Clin Med 62:4 16, 1963
17. Much JR. Herbst KD, Rapaport SI: Thrombosis in patientswith the lupus anticoagulant. Ann Intern Med 92:156, 1980
18. Boey ML, Colaco CB, Gharavi AE, Elkon KB, Loizou 5,Hughes GRV: Thrombosis in systemic lupus erythematosus: Stnik-ing association with the presence of circulating lupus anticoagulant.Br Med J 287:1021, 1983
19. Elias M, Eldor A: Thromboembolism in patients with the‘lupus’-type circulating anticoagulant. Arch Intern Med 144:510,I 984
20. Glueck HI, Kant KS, Weiss MA, Pollak VE, Miller MA,
Coots M: Thrombosis in systemic lupus erythematosus. Relation to
the presence of circulating anticoagulants. Arch Intern Med
145:1389, 1985
21. Lechner K, Pabinger-Fasching I: Lupus anticoagulants and
thrombosis. A study of 25 cases and review of the literature.
Haemostasis I 5:254, 1985
22. Pengo V. Ruffatti A, Banitussio A, Dc Marco L, Todesco 5,
Girolami A: Serum of normal subjects contains IgG with antibody
like specificity for phospholipids. Folia Haematol 1 1 1 :68 1 , 1984
23. Thiagarajan P. Shapiro 55: Lupus Anticoagulants, in Col-
man RW (ed): Disorders of Thrombin Formation. New York,Churchill Livingstone, 1983, p 101
24. Thiagarajan P. Pengo V. Shapiro 55: The use of the dilute
Russell viper venom time for the diagnosis of lupus anticoagulants.
Blood68:869, 1986
25. NisonoffA, Wissler FC, Lipman L, Noernley DL: Separation
of univalent fragments from the bivalent rabbit antibody molecule
by reduction of disulphide bonds. Arch Biochem Biophys 89:230,1960
26. Kinsky SC: Preparation of liposomes and a spectrophotomet-nc assay for release of trapped glucose marker, in Fleiseher 5,
Packer L (eds): Methods in Enzymology, vol 32, part B. Orlando,FL, Academic, 1974, p 501
27. Cooper MR, Cohen HJ, Huntley CC, Waite BM, Specs ML,
Spurn CL: A monoclonal 1gM with antibody-like specificity forphospholipids in a patient with lymphoma. Blood 43:493, 1974
28. Antonov PA, Pancheve RP, Ivanov IG: Radioiodination of
naturally occurring phospholipids. Biochim Biophys Acta 835:408,
I985
29. Rousser G, Siakotos AN, Fleischen 5: Quantitative analysis
of phospholipids by thin layer chromatography and phosphorus
analysis of the spots. Lipids 1 :85, 1966
30. Shapiro 55: Pnothnombin San Juan: A complex new dyspro-
thrombinemia, in Hemken HC, Veltkamp JJ (eds): Prothnombin andRelated Coagulation Factors. Leyden, The Netherlands, Leyden
University Press, 1975, p 205
3 1 . Morrison SA, Esnouf MP: The nature of the heterogeneity of
pnothrombin during dicoumanol therapy. Nature 242:92, 197332. Fraker PJ, Speck JC in: Protein and cell membrane iodina-
tions with a sparingly soluble chloramide, I , 3, 4, 6-tetnachloro-3a,6a-diphenylglycolunil. Biochem Biophys Res Commun 80:849,
197833. Miletich JP, Jackson CM, Majenus PW: Properties of the
factor Xa binding site on human platelets. J Biol Chem 253:6908,1978
34. Lafer EM, Rauch J, Andrzejewki C in, Mudd D, Funie B,Funie B, Schwartz RS, Stollan BD: Polyspecific monoclonal lupus
antibodies reactive with both polynucleotides and phospholipids. J
ExpMed 153:897, 1981
35. Yamamoto M, Watanabe K, Ando Y, In H, Murakami H,
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

76 PENGO ET AL
Sato K, Ikeda Y, Toyama K: Further evidences that lupus anticoag-
ulants are anti-phospholipid antibodies. Thromb Haemostas 54:276,
1985 (abstr)36. Thiagarajan P. Shapiro 55: Lupus anticoagulants are anti-
bodies reactive against phospholipids. Circulation 62:279, 1980
(abstr)
37. Shapiro SS, Thiagarajan P. McCord 5: The specificity of
lupus anticoagulants. Eur J Rheumatol Inflamm 7:16, 1984 (abstr)
38. Aho K: Studies of syphilitic antibodies. I. Antilipoidal anti-
bodies in various stages of syphilis. Br J Vener Dis 43:259, 1967
39. Aho K: Studies ofsyphilitic antibodies. II. Substances respon-
sible for biological false positive seroreactions. Br J Venen Dis 44:49,1967
40. Johansson EA, Lassus A: The occurrence of circulating
anticoagulants in patients with syphilitic and biologically false
positive antilipoidal antibodies. Ann Clin Res 6: 105, 1974
41. Schleider MA, Nachman RL, Jaffe EA, Coleman M: A
clinical study of the lupus anticoagulant. Blood 48:499, 1976
42. Nilsson IM, Astedt B, Hedner U, Berezin D: Intrauterine
death and circulating anticoagulant (“antithnomboplastin”). Acta
MedScand 197:153, 1975
43. Firkin BG, Howard MA, Radford N: Possible relationshipbetween lupus inhibitor and recurrent abortion in young women.
Lancet 2:366, 1980
44. Gabriel L, Samama M, Conard J, Honellou MH, Senvelle M:
Anticoagulant circulant antiprothombinase, thromboses Ct avonte-
ments spontanes, une nouvelle observation. Nouv Presse Med
9:2159, 1980
45. Soulien JP, Boffa MC: Avortements a repetition, thromboses
et anticoagulant circulant anti-thromboplastine: trois observations.
Nouv Presse Med 9:859, 1980
46. Cameras LO, Defreyn 0, Machin Si, Venmylen J, Deman R,
Spitz B, van Assche A: Arterial thrombosis, intrauterine death and
“lupus” anticoagulant: Detection of immunoglobulin interfering
with prostacyclin formation. Lancet I :244, 198147. Cameras LO, Vermylen JG: “Lupus” anticoagulant and
thrombosis-Possible role of inhibition of prostacyclin formation.
Thromb Haemostas 48:38, 1982
48. Dc Wolf F, Cameras LO, Moenman P. Venmylen J,
vanAssche A, Renaen M: Decidual vasculopathy and extensive
placental infarction in a patient with repeated thromboembolic
accidents, recurrent fetal loss and a lupus anticoagulant. Am J
Obstet Gynecol 142:829, 1982
49. Fanquhanson RG, Pearson JF, John L: Lupus anticoagulant
and pregnancy management. Lancet 2:228, 1984
50. Gardlund B: The lupus inhibitor in thromboembolic diseaseand intrauterine death in the absence of systemic lupus. Acta Med
Scand 215:293, 1984
51. Lubbe WF, Butler WS, Palmer SJ, Liggins GC: Lupus
anticoagulant in pregnancy. Br J Obstet Gynaecol 91:357, 1984
52. Reece EA, Romeno R, Clyne LP, Kniz NS, Hobbins JC:
Lupus-like anticoagulant in pregnancy. Lancet 1:344, 1984
53. Lockshin MD, Maurice L, Duzin MB, Goel 5, Qamar T,
Magid MS. Jovanovic L, Ferenc M: Antibody to cardiolipin as a
predictor of fetal distress or death in pregnant patients with systemic
lupus erythematosus. N Engl J Med 3 1 3: 1 52, 1985
54. Van Oss Ci: Antigen and Antibodies, in Milgnom F, Abeyou-
nis Ci, Kano K (eds): Principles of Immunological Diagnosis in
Medicine. Philadelphia, Lea & Febiger, 1973, p 14
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom
1987 70: 69-76
V Pengo, P Thiagarajan, SS Shapiro and MJ Heine anticoagulantsImmunological specificity and mechanism of action of IgG lupus
http://www.bloodjournal.org/content/70/1/69.full.htmlUpdated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom







