Download - Hypernatraemia

HYPERNATRAEMIAQusyairi
Defined as serum sodium >145mmol/L
Normal range: 135-145 mmol/L

Outline
Definition
Causes
Signs & symptoms
Investigation
Managements

Definition Serum [Na+](mmol/l)
Mild Hypernatremia 146 - 149
Moderate Hypernatraemia
150 - 169
Severe Hypernatraemia
≥ 170
Introduction
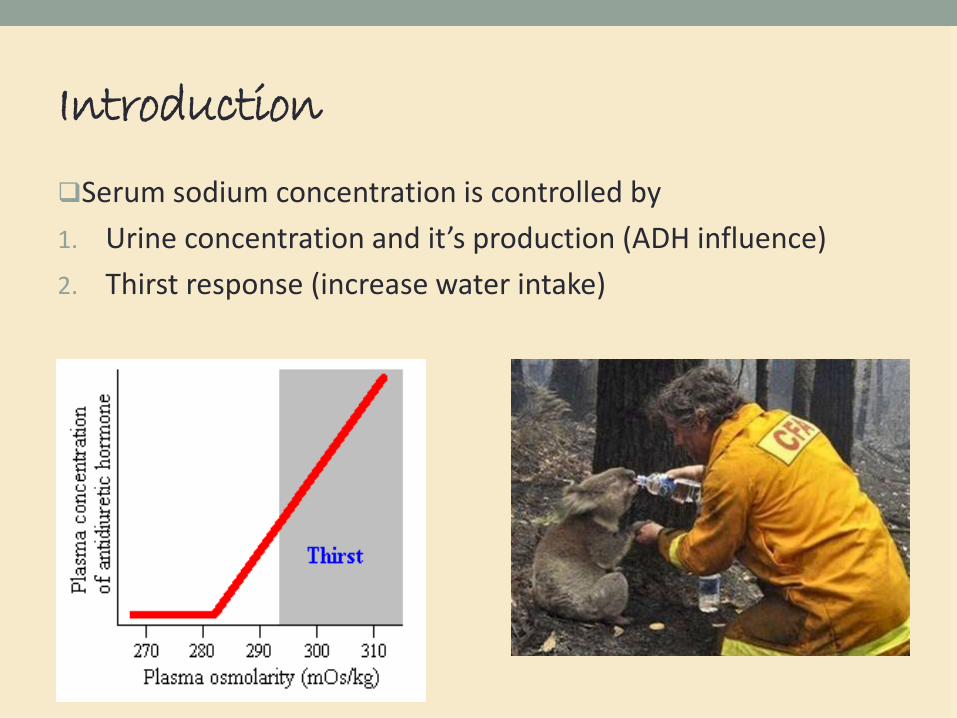
Serum sodium concentration is controlled by
1. Urine concentration and it’s production (ADH influence)
2. Thirst response (increase water intake)

Clinical features
Affects all ages
• Tremulousness
• Irritability
• Ataxia
• Spasticity
• Mental confusion
• Shortness of breath
• Vomiting
• Coma
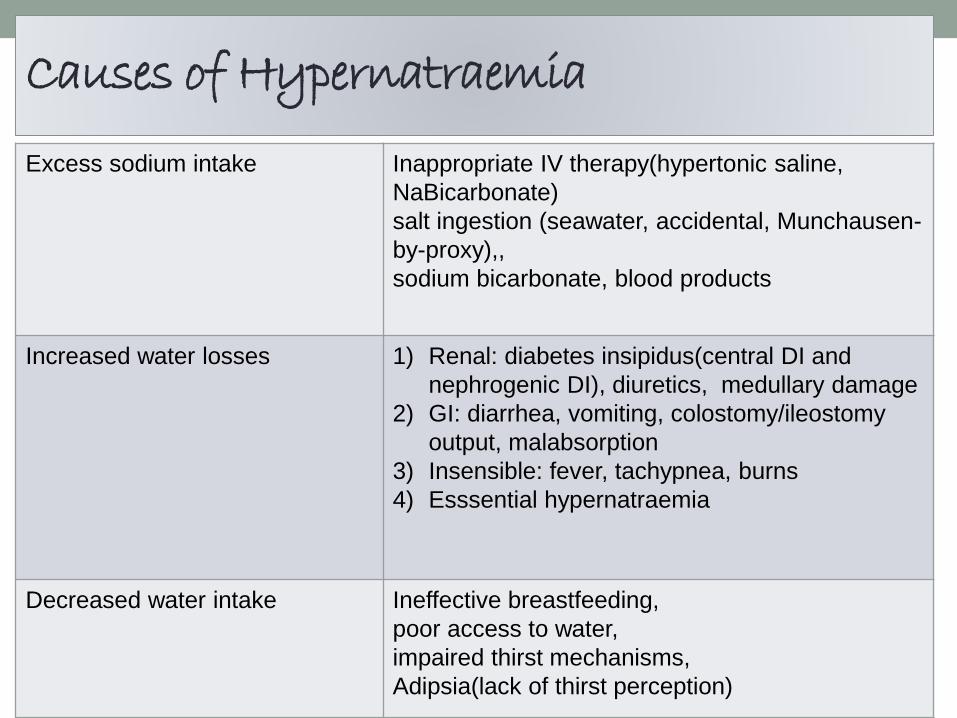
Causes of Hypernatraemia
Excess sodium intake Inappropriate IV therapy(hypertonic saline,
NaBicarbonate)
salt ingestion (seawater, accidental, Munchausen-
by-proxy),,
sodium bicarbonate, blood products
Increased water losses 1) Renal: diabetes insipidus(central DI and
nephrogenic DI), diuretics, medullary damage
2) GI: diarrhea, vomiting, colostomy/ileostomy
output, malabsorption
3) Insensible: fever, tachypnea, burns
4) Esssential hypernatraemia
Decreased water intake Ineffective breastfeeding,
poor access to water,
impaired thirst mechanisms,
Adipsia(lack of thirst perception)
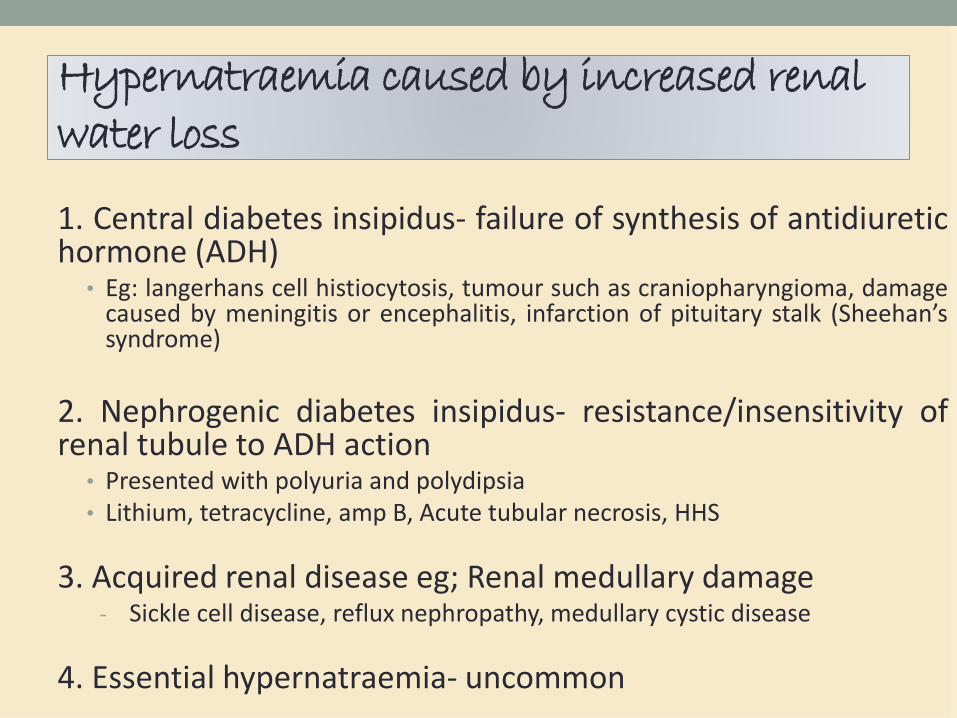
Hypernatraemia caused by increased renal water loss
1. Central diabetes insipidus- failure of synthesis of antidiuretichormone (ADH)
• Eg: langerhans cell histiocytosis, tumour such as craniopharyngioma, damagecaused by meningitis or encephalitis, infarction of pituitary stalk (Sheehan’ssyndrome)
2. Nephrogenic diabetes insipidus- resistance/insensitivity ofrenal tubule to ADH action
• Presented with polyuria and polydipsia• Lithium, tetracycline, amp B, Acute tubular necrosis, HHS
3. Acquired renal disease eg; Renal medullary damage- Sickle cell disease, reflux nephropathy, medullary cystic disease
4. Essential hypernatraemia- uncommon
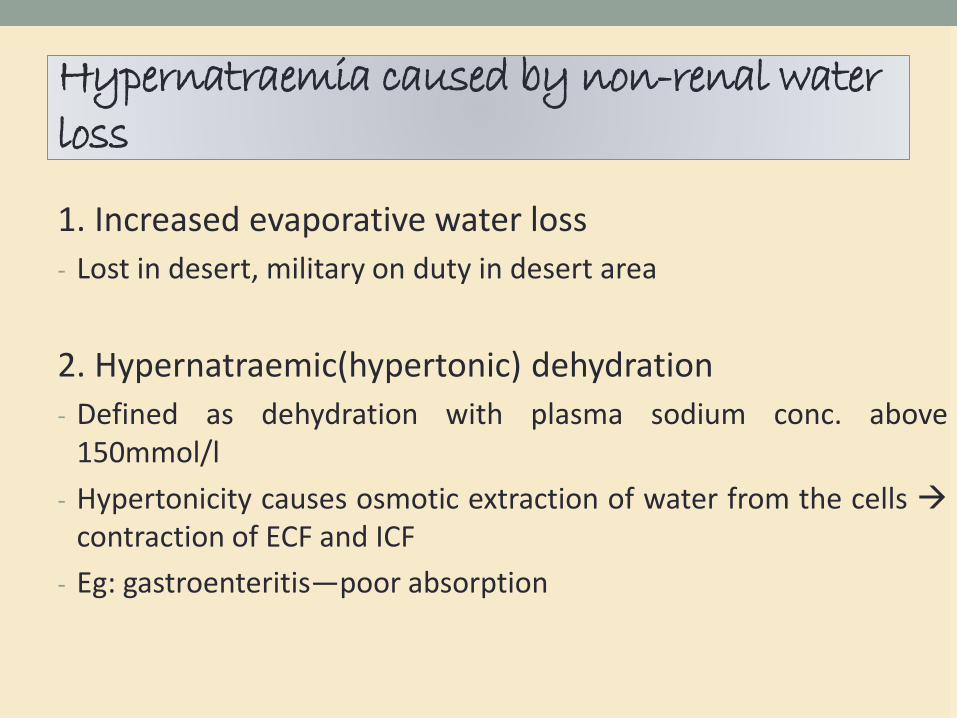
Hypernatraemia caused by non-renal water loss
1. Increased evaporative water loss
- Lost in desert, military on duty in desert area
2. Hypernatraemic(hypertonic) dehydration
- Defined as dehydration with plasma sodium conc. above150mmol/l
- Hypertonicity causes osmotic extraction of water from the cells contraction of ECF and ICF
- Eg: gastroenteritis—poor absorption
Hypernatraemia caused by non-renal water loss
3. Hypernatraemia caused by sodium excess:
a. Iatrogenic hyperNa
• Eg: result from the administration of repeated doses ofhypertonic Na bicarbonate to correct acidosis
b. Non-accidental salt poisoning
• Abuse:Adding salt in to the feed or directly into child’s mouth
c. Accidental salt poisoning
• Use of as anti-emetic as treatment
• Use of hypertonic saline to induce an abortion

Investigation
Urinalysis
Plasma osmolality
Blood urea serum electrolyte
#urine osmolality is low in diabetes insipidus
#plasma osmolality is high in hyperNa
#hypernatraemia

Treatment
• Depends on type of hydration, cause, and time period of development
• Target fall in serum Na conc of 10mmol/L/day except with long-standinghyperNa
• Long-standing hyperNa: to lower extracellular hypertonicity slowly inhypertonically-dehydrated patients eg; 0.5 mmol/hr
(prevent cerebral oedema)
• If acute eg: with accidental Na loading, do rapid correction (eg 1mmol/hr)
• Treat the aetiology!!!!!!
1. Water depletion
• Give water orally if tolerated
• If not, set up IV infusion of D5% or 0.45% NaCl
• Rate: hypertonicity should resolved slowly
- Plasma osmolality should not be corrected at a rategreater than 1mmol/L/hr
- Change in Na conc not exceed 1mmol/L/hr
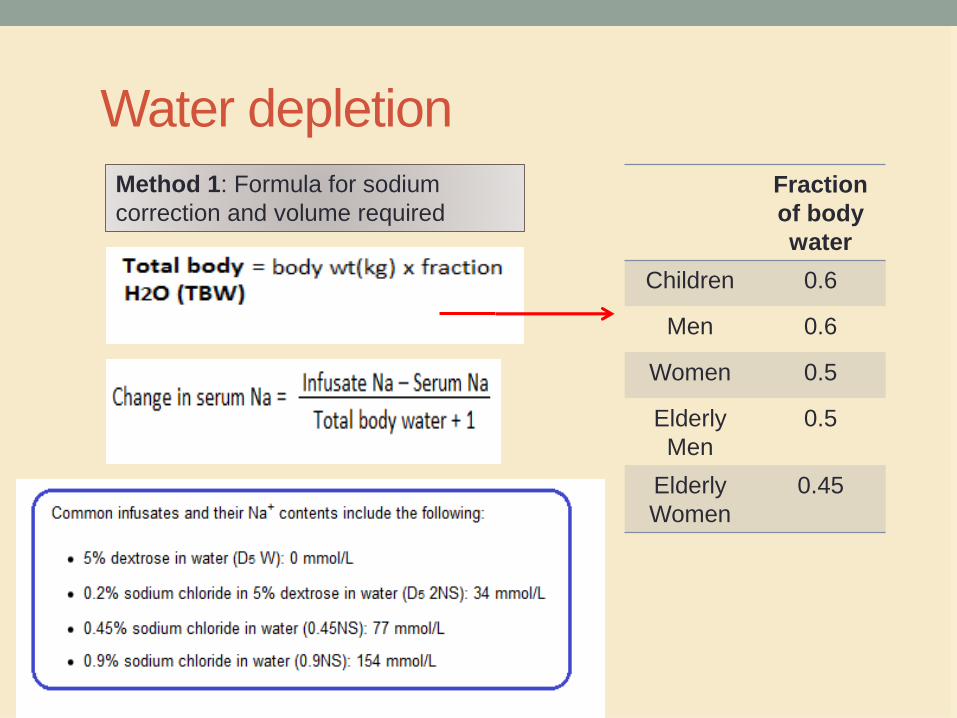
Water depletion
Fraction
of body
water
Children 0.6
Men 0.6
Women 0.5
Elderly
Men
0.5
Elderly
Women
0.45
Method 1: Formula for sodium
correction and volume required

Ongoing free water loss (urine from the electrolyte-
free water clearance (EFWC)):
EFWC = volume of urine (1 - ((urinary [Na+] +
urinary [K+] + urinary glucose/2)/ serum [Na+]))(Where volumes are in L and concentrations in mmol/L.)
Method 2: Calculation of
volume required

1. Water depletion
#Diabetes insipidus
- Central DI: desmopression through intranasal 5-10ugonce or twice daily or aqueous vasopressin SC 5-10 Utwice daily. SC/IV: 1-2 µg od/bd in acute care
- Nephrogenic DI: thiazide diuretic with or withoutprostaglandin synthetase inhibitors eg: indomethacin,or amiloride + modest Na restiction

2. Salt gain
• Aim: to remove sodium rapidly using a potent diuretic (IV
frusemide) + D5% infusion
• In severe and difficult cases dialysis may be necessary






