
Course IC-99 – Cross-Linking – Vinciguerra - 1
XXIX Congress of The ESCRS
17 - 21 September, 2011 Vienna, Austria
Course IC-99
Successful Cross-Linking: Patient Selection, Management
of Complications, Long-Term Follow-Up, and
Understanding Corneal Response to Treatment
Senior Instructor: Paolo Vinciguerra, MD
Associate Instructors:
Theo Seiler, MD Fabrizio I. Camesasca, MD
Scipione Rossi, MD Elena Albè, MD
20 September 2011
14.30 – 16.30
Room 2

Course IC-99 – Cross-Linking – Vinciguerra - 2
INDEX
I. Patient Selection Elena Albè, MD
Page 3
II. Surgical Technique Fabrizio I. Camesasca, MD
Page 8
III. Topo-aberrometric, refractive and pachymetric analysis of Keratoconics eyes undergoing CXL Paolo Vinciguerra, MD
Page 11
IV. Corneal Cross-Linking for Ectasia After Excimer Laser Refractive Surgery: One-Year Results Paolo Vinciguerra, MD
Page 23
V. Complication and failure rates after corneal crosslinking Theo Seiler, MD
Page 29
VI. Pediatric Patients: Two Years Results Elena Albè, MD
Page 34
VII. Evaluation of Crystalline Lens Opacity Induced by Corneal Cross-Linking with Scheimpflug Imaging Fabrizio I. Camesasca, MD
Page 37
VIII. Anterior and Posterior Corneal Surface Scipione Rossi, MD
Page 40
ADDRESSES……………………………………………………………………………….. Page 45 Special thanks to Pietro Rosetta, MD Ophthalmology Dept. – Istituto Clinico Humanitas

Course IC-99 – Cross-Linking – Vinciguerra - 3
I. Patient selection
Collagen Cross Linking
TRADITIONAL USE
PROGRESSIVE CORNEA ECTASIA
• Keratoconus
• Pellucid Marginal Degeneration
• Post iatrogenic ectasia
RECENTLY…
• CXL and corneal infection
• CXL with INTACTS
• CXL and PTK
1. How to diagnose ectasia2. How to assess progression of
ectasiain KC, PMD, ectatic corneas
3. Inclusion CXL criteria4. Exclusion CXL criteria
Collagen Cross Linkingin progressive corneal ectasia
AIM
1.Corneal Topography2.Corneal Tomography3.Endothelial Microscopy
Collagen Cross Linkingin progressive corneal ectasia
METHODS
1. HOW TO DIAGNOSE ECTASIA
ectasia or pseudo‐ectasia?
Risk Factor or Hot Spots: Risk Factor or Hot Spots: RED on RED
Coincidence of hot spots: Coincidence of hot spots:
Maximum curvature Maximum curvature –– max ant.& post. max ant.& post. elevation elevation -- minimum minimum pachymetrypachymetry
Interlocking relationships on Holladay Report
ECTASIAECTASIA RED on RED
TANGENTIAL TANGENTIAL MAP MAP
SteepestSteepestpointpointREDRED
PACHYMETRY PACHYMETRY MAPMAP
ThinnestThinnestpointpointREDRED
ELEVATION ELEVATION MAPMAP
MostMost ElevatedElevatedpointpointREDRED
PSEUDOECTASIAPSEUDOECTASIA RED on BLUE
TANGENTIAL TANGENTIAL MAPMAP
FlattestFlattestpointpointBLUEBLUE
PACHYMETRY PACHYMETRY MAPMAP
ThickestThickestpointpointBLUEBLUE
ELEVATION ELEVATION MAPMAP
LessLess elevatedelevatedpointpointBLUEBLUE

Course IC-99 – Cross-Linking – Vinciguerra - 4
1. HOW TO DIAGNOSE ECTASIA
ectasia or pseudo‐ectasia?
Coincidence and displacement of Coincidence and displacement of maximum ant.& post. Elevationmaximum ant.& post. Elevation
Anterior elevation values > 12-15 µ
Posterior elevation values > 20 µ
Eccentricity of thinnest pointEccentricity of thinnest point
Map patterns (eccentric, asymmetric Map patterns (eccentric, asymmetric pattern/hot spots)pattern/hot spots)
Interlocking relationships on Holladay Report
BLUE on BLUEBLUE on BLUERED on RED on RED on REDRED on RED BLUEBLUE
Thinnest point located centrally
Thicker nasally and superiorly
Flatter nasally
Pachymetrygradient is predictable
Map patterns
BLUE on BLUEHolladay reportNormal cornea
+1,75 –6.75@170
ASTIGMATISM: tipical pattern ! BLUE on BLUE
IRREGULAR ASTIGMATISM BLUE on BLUE
PSEUDOECTASIAPSEUDOECTASIA
CicatrixCicatrixPerforatingPerforating woundswoundsHostHost--donordonor interfaceinterface
Highest curvature does not correspond
to thinnest cornea
Post refractive ablation
RED on BLUE

Course IC-99 – Cross-Linking – Vinciguerra - 5
ECTASIAECTASIACorneal thinning corresponds to
highest curvature point
SteepestSteepest, , thinnestthinnest, , mostmostelevatedelevated pointspointscoincidencecoincidence
BFS
HYPERCURVATUREHYPERCURVATURE
PELLUCID MARGINAL DEGENERATION
RED on RED
POST LASIK ECTASIA RED on RED
TAKE HOME MESSAGE 1. HOW TO DIAGNOSE ECTASIA
• Interlocking relationships are a safer and more sensitive tool for ectasia diagnosis than single maps
• ECTATIC CORNEA •• RED RED on REDRED
• NON ECTATIC CORNEA •• BLUE BLUE on BLUEBLUE
Slit lamp: subjective but not repeatable
Endothelium and Vogt striae: late changes
Confocal microscopy: not sensitive
Refraction: HOA, and LOA
Ectasia outside the pupillary area does not change refraction : false negative
Progression of myopia: false positive
2. HOW TO ASSESS ECTASIA PROGRESSION
These are not reliable indicators of ectasia progression
How can progression be monitored?
Follow up with DIFFERENTIAL MAPS Curvature: Tangential map
Elevation: Elevation Maps
Thickness: Pachymetry Map
…… MethodMethod : : toto evaluateevaluate changechange
ABSOLUTEABSOLUTE
VALUEVALUEPATTERNPATTERN

Course IC-99 – Cross-Linking – Vinciguerra - 6
When differential maps are notavailable we should compare
pattern & absolute value & indices
200155,22D
200558,10D
When differential maps are notavailable we should compare
pattern & absolute value & indices
TANGENTIAL MAPPattern change
Increased cone area
Absolute keratometrychange
11 months
O month
3.16 D
63,12 D
59,97 D
B B prepre
ELEVATION INCREASE ABSOLUTE VALUE
AA--BB
ANTERIOR ELEVATION MAP
A postA post
PATTERN VARIATION
INCREASE IN ELEVATION
POSTERIOR ELEVATION MAP
B B prepre AA--BBA postA post
PATTERN VARIATION
THICKNESS REDUCTION
PACHYMETRY MAP
B B prepre AA--BBA postA post

Course IC-99 – Cross-Linking – Vinciguerra - 7
TAKE HOME MESSAGE 2Only progression indicates ectasia
• Single topographic map is not a safe diagnostic instrument
• Differential maps allow soon progression assessment
• Differential maps allow earlier ectasia diagnosis in border‐line cases
• Early diagnosis is important for successful application of cross linking
WHAT TO DO IN CASE OF DOUBTFUL WHAT TO DO IN CASE OF DOUBTFUL ECTASIA? ECTASIA?
FALSE POSITIVE = WARPAGEFALSE POSITIVE = WARPAGE
OSV 0.8 +3.25 (-3.25)180 OSV 0.7 +2.0(-3.25)170 OSV 1.0 +2.0(-3.25)170
+49.80 +50.07 +45.59
2005 2006 2009
OSV 0.8 -1.00(-1.00)0 OSV 0.8 -2.00(-1.50)170 OSV 0.8 -1.50(-1.25)170
OSV 0.8 -2.00(-1.50)170 OSV 0.6 -2.00(-1.50)170
2/2005 07/2005 2/2006
05/2007 09/2008
False warpage: Progression of kc
SUSPECT KERATOCONUS RED on RED
WHAT TO DO IN CASE OF WHAT TO DO IN CASE OF DOUBTFUL ECTASIA? DOUBTFUL ECTASIA?
TOPO AND TOMOGRAPHIC INDICESTOPO AND TOMOGRAPHIC INDICES Corneal Navigator OPDCorneal Navigator OPD
BelinBelin AmbrosioAmbrosio Indices PENTACAMIndices PENTACAM
Corneal Hysteresis ORACorneal Hysteresis ORA
KERATOCONUS
NORMAL
ORACORNEAL NAVIGATOR
BELIN /AMBROSIO INDICES
BFSBFS
EnhancedEnhancedBFSBFS
DifferenceDifferenceElevation Elevation
MapsMaps
<6<6 >12>1266--1212

Course IC-99 – Cross-Linking – Vinciguerra - 8
TAKE HOME MESSAGE TAKE HOME MESSAGE EARLY DIAGNOSES IS IMPORTANT!
Avoid PK, DALK.
Soon CXL.
Preserve best VA .
Preserve good CL tolerance.
3. CXL TO TREAT OR NOT TO TREATINCLUSION CRITERIA
Ectatic corneal disease
Ectasia progression documented by serial differential corneal topographies and optical pachymetries
pt’age over 9 years
signed informed consent
Adequate corneal thickness
CORNEAL THICKNESS at its thinnest point
at least 400μin degenerative ectaticcorneal diseases
At least 380μin most severe cases
Expansion technique
At least 350μ in post refractive ectasia
…REMEMBER
First stages KC and pediatric patients havebetter topographical and visual recovery.
CL tolerance
CCT/Kmax
Kmax 87,44D Kmax 46,47D
CCT 332µin botheyes
1° Pt KC 2° Pt post LASIK ectasia
4. EXCLUSION CRITERIA
ABSOLUTE
Loss endothelial cell count
Severe corneal opacities
pregnant or nursing ♀
RELATIVE
history HSV,HZV
severe eye dryness
corneal infections
autoimmune diseases
previous ocular surgery
poor compliant pt
Thank you for your attention !
Elena AlbéIstituto Clinico Humanitas

Course IC-99 – Cross-Linking – Vinciguerra - 9
II. Surgical Technique
Organized Surgical Approach
• Check‐List
•Eye
•Patient data
•Activities by:
•Attending physician
•Nurse
•Surgeon
•Alert
• Same‐day control of clinical situation
• Antipain meds 30 min before CXL
Surgical Approach ‐ Sterility Day Surgery
Sterile conditions in the operating suite
Preop disinfection
Scrub
Surgical gown and gloves
Disposable medication
Single‐set surgical instruments
Patient draping
Rama P et al. J Cataract Refract Surg 2009; Apr
Preoperative Medications
2% Pilocarpine drops
pilocarpine reduces the thermal and photochemical
Ultraviolet A (UVA) light irradiation potentially
harmful to the lens and retina
amount of light rays reaching the retina is
proportional to the square of the pupil diameter
i.e., 6 mm pupil = 36 units, 4 mm pupil = 16
units, 2 mm pupil = 4 units
Topical anesthesia with two applications of 4%
lidocaine drops and oxybuprocaine hydrochloride 0.2%
Available UVA Devices
UV light from a solid‐state UVA source
UV‐X ™ System Peschke Meditrade GmbH, Huenenberg,
Switzerland
The UV‐X ™ System was developed by
Theo Seiler, MD and Eberhard Spoerl,
PhD (Zuerich / Dresden).
It consists of a radiator which
emits highly homogenized UV‐light
at 365 nm and a table mount.
irradiance of 3 mW/cm2 or 5.4 J/ cm2
Available UVA Devices
UV light from a solid‐state UVA source
VEGA CBM X Linker, Oofta HT, Montegiorgio, Italy
diode UV‐A emitting source with a wavelight of 370 nm,
with diaphragm, fixation point, double light aiming
system, LCD camera
Standard Surgical Procedure
• Corneal epithelium is abraded in a central, 9‐mm
diameter area with an Amoils brush.
• Photosensitizing riboflavin 0.1% solution ( 10 mg
riboflavin‐5‐phosphate in 20% dextran‐T‐500 10 ml
solution) is applied onto the cornea every minute
for 30 minutes to achieve adequate penetration of
the solution
• Using a slit lamp with the blue filter, presence of
riboflavin in the anterior chamber is confirmed
before UV irradiation

Course IC-99 – Cross-Linking – Vinciguerra - 10
Surgical Procedure• A calibrated UVA meter (LaserMate‐Q; Laser 2000,
Wessling, Germany) used before treatment to check the
irradiance at a 1.0 cm distance. Laser 370±5 nm, Power
3 mW/cm2 (= 5.4 j/cm2)
• UV source exposition for 30 minutes
• leave untreated zone of at least 1.5 mm from the limbus
(stem cells protection)
● Do not shorten treatment time
● Do not use home‐made solutions
● Surface must remain moist to avoid haze formation
• Riboflavin solution is applied again, but only once every
5 minutes
• Focusing is very important: out‐of‐focus can result in
dangerous or ineffective dosage
Postoperative Medication
• Cyclopentolate 2% eyedrops
• Levofloxacin eyedrops
• Soft bandage contact lens until re‐
epithelialization is complete.
• Topical levofloxacin 4 times daily for 7 days
• Dexamethasone 21‐phosphate 0.15% drops 3 times
daily for 20 days
• 0.15 % sodium hyaluronate drops 6 times daily for
45 days
• Oral aminoacid supplement
Postoperative Period
• 1, 3, 6, 12 month‐controls
• Complete ophthalmological examination
• Corneal topography
• Pentacam
• Haze monitoring
• 0.15 % sodium hyaluronate drops
• CL use is allowed one month after surgery
if corneal epithelium appears healthy and
regular
Good Medical Practice
• Accurate preoperative patient information
(i.e., course of visual acuity)
• Standardized informed consent
• In Italy, one IC for the whole nation,
approved by the national
ophthalmological society (SOI)
• Documenting ectasia progression over at
least 6 month‐period:
• Corneal topography
• Pentacam
Good Medical Practice
• Documenting Surgery
• Surgical logbook
• Surgical report
• Use of product adhesive labels (i.e,
riboflavin)
• Documenting follow‐up:
•Visual Acuity
•Corneal topography
•Pentacam
Thank you for your attention !

Course IC-99 – Cross-Linking – Vinciguerra - 11
III. Topo-aberrometric, refractive and pachymetric analysis
of Keratoconics eyes undergoing CXL
Part 1
Cross‐linking (CXL) tecnique2% Pilocarpine drops (protection of lens and retina)
The light reaching the internal structures of the eye is decreased by the square of the reduction of the pupil diameter
(For example : a 6‐mm pupil = 36 units, a 4‐mm pupil = 16 units, 2‐mm pupill = 4 units)
Antipain meds 30 min before CXL.
Oxybuprocaine hydrochloride 0.2% + Lidocaine 5 min before CXL.
Cross‐linking (CXL) tecnique Laser test ((UVA meter)
Laser 370±5 nm
Power 3 mW/cm2 (= 5.4 j/cm2)
Calibration should be extremely precise: +/‐0.1 mW/cm2
Focusing is very important
out‐of‐focus can result in dangerous or ineffective dosage
Diaphragm adjusts size of treatment area
Laser plus camera enabling monitoring of focus, beam size and corneal surface
Monitor with view of cornea,beam, and treatment time

Course IC-99 – Cross-Linking – Vinciguerra - 12
Cross‐linking (CXL) tecnique
● A 9‐mm Ø central epithelial abrasion with Amoils brush
● Riboflavin 0.1% solution, 2 drops every minute for 30 minutes (commercially available®)● Do not be tempted to shorten treatment time
● Do not use home‐made solutions
● Surface must remain moist to avoid haze formation
● Riboflavin absorption check (anterior chamber flare)
● UVA irradiation, leaving an untreated zone of at least 1.5 mm from the limbus (stem cells protection)
● Riboflavine again, 1 drop every 2‐3 minutes during treatment
Cross‐linking (CXL) tecnique
At the end of treatment
● Cyclopentolate 0.5%
● Hyaluronic acid + antibiotics (till re‐epithelization)
● Bandage contact lens
545 treated eyes Preop.evaluated eyes:344 28 pediatric; 21 ectatic (lasik,prk,intacs); 3 PMD
Demographic
age@OP average 30 years (from 10 to 67)
sex female 27,1% or 95 eyes
male 72,4% or 254 eyes
pre SR equiv: mean ‐3,95 D ± 4,35 D (from ‐24,75 to 5,50)
pre SR sph: mean ‐2,49 D ± 4,20 D (from ‐23,00 to 6,00)
pre SR cyl: mean ‐2,92 D ± 1,97 D (from ‐10,00 to 0,00)
9%5%5%5%
21%22%
25%
42 %50%
51%50%
74%
59%
66%
75%79%
0%
10%
20%
30%
40%
50%
60%
70%
80%
<=1D
<=2D
<=4D
<=5D
pre op (351)
1 y (170)
2 y (40)
3 y (19)
month(eyes)
Defocus equivalent‐%
12%8%
3%5%
23%
26%
10%5%
27%
21%
20%
21%
13%
19%
28%
5%
16%
20%
38%
63%
0%
10%
20%
30%
40%
50%
60%
70%
lost 1 unchanged gained 1 gained 2 gained > 2
6 (200)
12 (168)
24 (40)
36 (19)
month(eyes)
Change in BSCVA ‐ %“Safety”
7% 6% 5%
10%
14%12%
9%
25%25%
23%
27%
47%
41%
42%44%
63%
0%
10%
20%
30%
40%
50%
60%
70%
Vin
cig
ue
rra
Pa
olo
+- 0,25 +- 0,5 +- 1,0 +- 2,0
pre op (351)
1 y (170)
2 y (41)
3 y (19)
month (eyes)
Refractive outcomerefractive variation / preop

Course IC-99 – Cross-Linking – Vinciguerra - 13
8%
14%18%
21%
10%
16%
30%
5%
14%
23%
13%
42%
13%15%
13%16%
55%
29%28%
16%
0%
10%
20%
30%
40%
50%
60%
1,0 0,9 0,8 0,7 0,6 or worse
1 m (280)
1 y (170)
2 y (40)
3 y (19)
month(eyes)
BSCVA ‐ %
BSCVA over time
0,62 0,64
0,42 0,42
0,490,52
0,580,63
36170202160281351 40 190,0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1,0
pre op 1 m 3 m 6 m 1 y 1,5 y 2 y 3 y
Vin
cigu
erra
Pao
lo
Achieved Correction SEQ over time“STABILITY”
-1,96-2,90
-2,88-3,28
-3,95-4,00
-4,50-3,95
1940351 281 160 202 170 35-10,00
-8,00
-6,00
-4,00
-2,00
0,00
2,00
pre op 1 m 3 m 6 m 1 y 1,5 y 2 y 3 y
Vin
cigu
erra
Pao
lo
Diopters
Normalized Double Angle Minus Cyl - Scatter Plot (351 eyes)
-5
-4
-3
-2
-1
-0
-1
-2
-3
-4
-5
-5 -4 -3 -2 -1 -0 -1 -2 -3 -4 -5
Mean Cyl -2,92 @ 0,0°
Vinciguerra Paolo
0°
45°
90°
135°
177.7°‐2.163 yrs post cxl
2°‐1.762 yrs poscxl
179.9°‐1.651 yr post cxl
0°‐2.92Pre cxl
@Meancyl
2,92
1,651,76
2,16
0
0,5
1
1,5
2
2,5
3
mean cyl (-)
pre cxl
1 yr post cxl
2 yrs post cxl
3 yrs post cxl
Dio
pte
r
PentacamChamber volume mm3
PRE PRE 224,17224,17±± 37.3 mm37.3 mm33
POSTPOST 3 m3 m 223.,37 223.,37 ±± 27 mm27 mm33
POST 6 m 221,17POST 6 m 221,17±±45.39mm45.39mm33
POST 12 m 238,50 POST 12 m 238,50 ±± 30 mm30 mm33
POST 24 m 236,29POST 24 m 236,29 ±± 26.3626.36 mmmm33
POST 36 m 239,05POST 36 m 239,05±± 17,3 mm17,3 mm33
mm
mm
33
mos
Anterior chamber dept mm3PRE PRE 3,45 3,45 ±± 0,24 mm0,24 mm33
POSTPOST 3 m 3 m 3,3,47 47 ±± 0,27 mm0,27 mm33
POST 6 m 3.45 POST 6 m 3.45 ±± 0.30 mm0.30 mm33
POST 12 m POST 12 m 3,3,53 53 ±± 0,19 mm0,19 mm33
POST 24 m 3.49 POST 24 m 3.49 ±± 0.21 mm0.21 mm33
POST 36 m 3,51 POST 36 m 3,51 ±± 0,2 mm0,2 mm33
mm
mm
33
mos

Course IC-99 – Cross-Linking – Vinciguerra - 14
THINNEST POINT PRE 429 ± 48.15 µm POST 3 m 401 ± 59.03 µm POST 6 m 417 ± 64.03 µm POST 12 m 429 ± 45,10 µm POST 24 m 428 ±35.6 µm POST 36 m 429 ± 33.03 µm
Result pentacam‐‐pachymetry
micron
Result pentacam‐‐pachymetry PUPIL CENTER
PRE 440 ± 45,18 µm POST 3 m 410 ± 60,98 µm POST 6 m 435 ± 59,17 µm POST 12 m 432 ± 31,51 µm POST 24 m 438 ± 29.12 µm Post 36 m 439 ± 34 µm
440
410
435432
438 439
395
400
405
410
415
420
425
430
435
440
pupil center
pre op
3 mos post cxl
6 mos pos cxl
12 mos post cxl
24 mos pos cxl
36 mos post cxl
micron
PentacamCentral corneal thickness µm
micron
351PRE
170POST 12 m
40POST 24 m
19POST 36 m
ACP 44.75 43.6 42.08 40,5
CYL 2,57 1.98 1.75 1,68
CVP 73.14 60.12 57 55
SDP 4.12 2.7 2.5 1,9
AA% 85,68 82.75 80.03 78,2
CEI 0,37 0.1 0.09 0,06
LogMAR 0,17 0.1 0.14 0,09
DSI 8,7 5.9 5.5 4,9
SRI 1.34 1.22 1.21 1,19
SRC 1,19 1.10 1.07 1,02
SAI 1,88 1.3 1.26 1,26
IAI 5,86 0.56 0.58 0,58
OSI 7,18 4.2 3.95 3,94
CSI 0.9 0.02 0.03 0,02
KCI 8,9 0.25 0.24 0.23
KPI 0,43 0.27 0.28 0.25
EDP 2,67 2.40 2.45 2.39
EDD 10.01 6.5 5.1 4,9
OPD
OPD
CO
RN
EA
L N
AV
IGA
TO
RC
OR
NE
AL
NA
VIG
AT
OR
KL
YC
E IN
DE
XE
SK
LY
CE
IND
EX
ES
IMPROVED
UNCHANGED
WORSED
N =
1,26
0,58
isv iva ki cki iha ihd rmin
PRE CXL
77,4 0,78 1,13 1,02 19,12 0,08 6,57
POST 3 mos
79,0 0,8 1,17 1,12 19,1 0,065 6,66
POST6 mos
86 1,19 1,07 0,89 19,6 0,075 6,67
POST 1 yrs
61,27 0,76 1,09 1,01 14,56 0,04 6,89
POST2 yrs
59.07 0.55 1.03 1.02 13.12 0.023 5.9
POST 3 yrs
52,9 0.38 0.76 0.87 11.5 0.020 5.6
Indici di Ambrosio
Topo classifier map
GRAFICA Klyce classification
Le Le classiclassi di di probabilitprobabilitàà sonosono ottenuteottenute da da unauna correlazionecorrelazione tratra indiciindicicheratometricicheratometrici e le e le corrispondenticorrispondenti patologiepatologie o o distrofiedistrofie cornealicorneali, e , e sonosonobasatebasate sullesulle deviazionideviazioni standardstandard provenientiprovenienti dalladalla reterete neuraleneurale NidekNidek..
Course IC-99 – Cross-Linking – Vinciguerra - 15
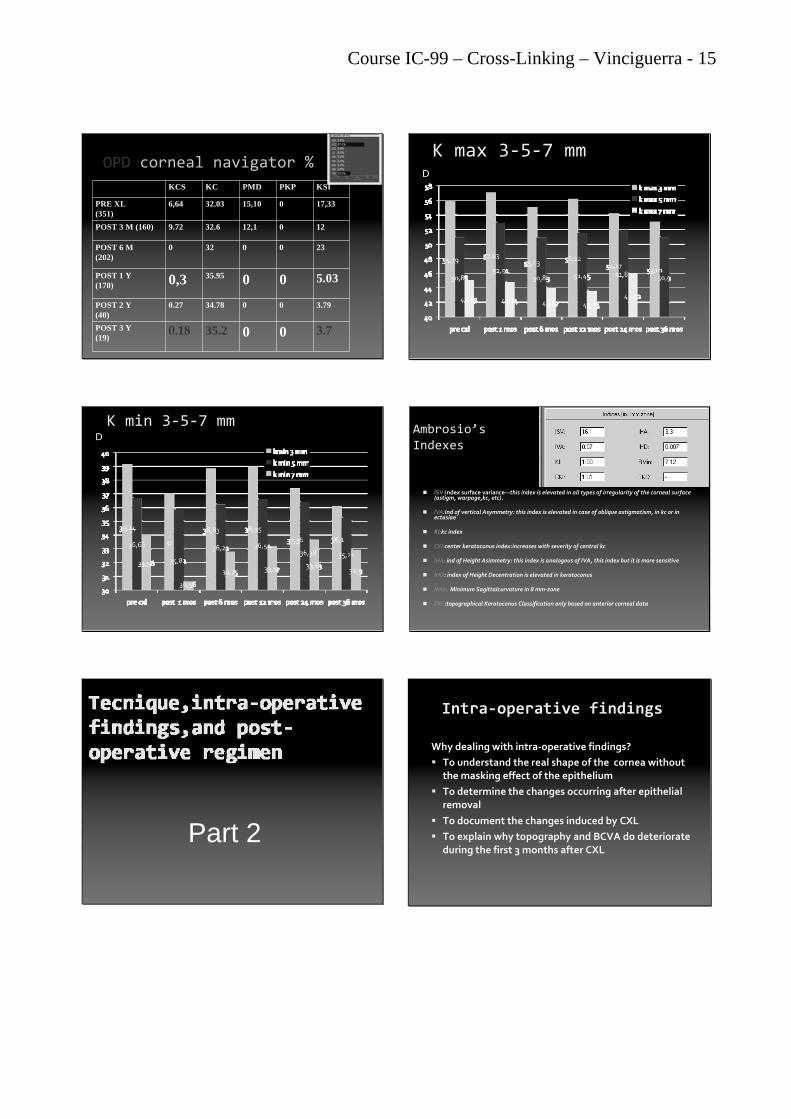
OPD corneal navigator %
KCS KC PMD PKP KSI
PRE XL(351)
6,64 32.03 15,10 0 17,33
POST 3 M (160) 9.72 32.6 12,1 0 12
POST 6 M(202)
0 32 0 0 23
POST 1 Y(170) 0,3 35.95 0 0 5.03
POST 2 Y(40)
0.27 34.78 0 0 3.79
POST 3 Y(19)
0.18 35.2 0 0 3.7
K max 3‐5‐7 mmD
K min 3‐5‐7 mmD
Ambrosio’sIndexes
ISV:index surface variance—this index is elevated in all types of irregularity of the corneal surface (astigm, warpage,kc, etc).
IVA:Ind of vertical Asymmetry: this index is elevated in case of oblique astigmatism, in kc or in ectasiae
KI:kc index
CKI:center keratoconus index:increases with severity of central kc
IHA: ind of Height Asimmetry: this index is analogous of IVA, this index but it is more sensitive
IHD: index of Height Decentration is elevated in keratoconus
Rmin: Minimum Sagittalcurvature in 8 mm‐zone
TKC:topographical Keratoconus Classification only based on anterior corneal data
Part 2
Intra‐operative findings
Why dealing with intra‐operative findings?
To understand the real shape of the cornea without the masking effect of the epithelium
To determine the changes occurring after epithelial removal
To document the changes induced by CXL
To explain why topography and BCVA do deteriorate during the first 3 months after CXL

Course IC-99 – Cross-Linking – Vinciguerra - 16
PRE sine epithelium
PRE con
PRE with epithelium
POST sine
Note the increased power and diameter of the cone and the flattening of the surrounding area
PRE sine epithelium
PRE con
PRE with epithelium
POST sine epithelium
Note the decreased power and diameter of the cone and the steepening of the surrounding
area immediately after CXL
1 month post CXL
7 days post CXL
PRE with epithelium
At 7 days cone looks steeper, larger
At 1 mos cone even steeper, larger
Now first signs of
flattening/shrinkage
PRE with epithelium
3 mos after CXL
Why these late cone changes? The epithelium in a keratoconic cornea is arranged according to the law of surface tension: thinner at the apex and thicker at the edge of the cone
This masks the real ( keratoconic) shape of the stroma
Why these late cone changes?
After any epithelial abrasion, the physiological rearrangement of the layers takes weeks to complete
Only when the epithelium is back to normal, and its masking function is re‐established, does the flattening effect of CXL begin to appear ( at about 3 mos)

Course IC-99 – Cross-Linking – Vinciguerra - 17
Other intra‐operative findigs
Apparent corneal thinning
Biomechanical changes
BSCVA is better even if there is an apparent corneal thinning
474 µ -176 µ +94 µ
1 mos post cxl
0,6 +7,00 ‐1,00@90
pre cxl
0,8 – 1,25@94
6 mos post cxl0,9 nat
1 mos post cxl
0,6 +7,00 ‐1,00@90
pre cxl
0,8 – 1,25@94
6 mos post cxl0,9 nat
+28 µ + 23 µ (-5 µ) +28 µ (-14 µ)
Differential elevation anterior map: -14 µ
Reduction of the elevation anterior of the keratoconus overtime
1 mos post cxl
0,6 +7,00 ‐1,00@90
pre cxl
0,8 – 1,25@946 mos post cxl0,9 nat
+63.5 D + +58 D (-5.4 D) +53.9(-9.6 D)
Reduction of the area/power of the keratoconus overtime
Differential tangential map: -9.6 D
Pachymetry distribution 6 mos after CXL
1 mos post cxl
0,6 +7,00 ‐1,00@90
pre cxl
0,8 – 1,25@94
6 mos post cxl0,9 nat
- 44.20 % -38.4 % (+ 5.8 %) -21.4 % (+ 22.8%)
+22.8%
Differential Pachymetry relative map
Apparent corneal thinning
“Thinning” is only temporary because:
Riboflavine solution contain dextrane that together with the exposure to air of the denuded cornea dehydrates the stroma
Collagen fibers and lamellae are packed by CXL
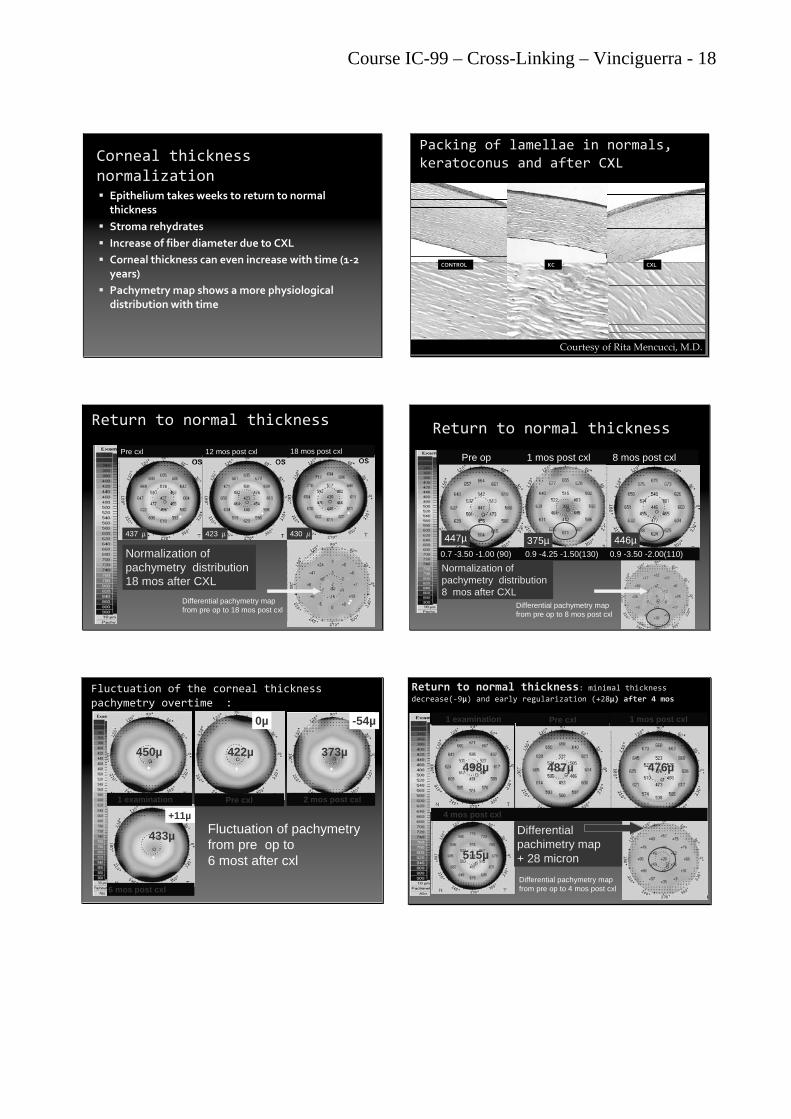
Course IC-99 – Cross-Linking – Vinciguerra - 18
Corneal thickness normalization Epithelium takes weeks to return to normal
thickness
Stroma rehydrates
Increase of fiber diameter due to CXL
Corneal thickness can even increase with time (1‐2 years)
Pachymetrymap shows a more physiological distribution with time
Courtesy of Rita Mencucci, M.D.
CONTROL KC CXL
Packing of lamellae in normals, keratoconus and after CXL
Return to normal thickness
Pre cxl 12 mos post cxl 18 mos post cxl
430 μ437 μ 423 μ
Normalization of pachymetry distribution 18 mos after CXL
Differential pachymetry mapfrom pre op to 18 mos post cxl
0.7 -3.50 -1.00 (90) 0.9 -4.25 -1.50(130) 0.9 -3.50 -2.00(110)
Pre op 1 mos post cxl 8 mos post cxl
447µ 375µ 446µ
Normalization of pachymetry distribution 8 mos after CXL
Return to normal thickness
Differential pachymetry mapfrom pre op to 8 mos post cxl
Fluctuation of the corneal thickness pachymetry overtime :
+11µ
433µ
450µ 422µ
0µ
373µ
Pre cxl
6 mos post cxl
1 examination
-54µ
2 mos post cxl
Fluctuation of pachymetryfrom pre op to6 most after cxl
Return to normal thickness: minimal thickness decrease(‐9µ) and early regularization (+28µ) after 4 mos
1 examination Pre cxl 1 mos post cxl
4 mos post cxl
498µ 476µ
515µ
487µ
Differentialpachimetry map+ 28 micron
Differential pachymetry mapfrom pre op to 4 mos post cxl

Course IC-99 – Cross-Linking – Vinciguerra - 19
Normalization of pachymetrydistribution 1 year after CXL
Pre‐CXL relative pachymetry Post‐ CXL relative pachymetry
Normalization of pachymetry distributiononly 3 mos after cxl
-8 % at only 3 mos post cxl!!
Pre cxl 3 mos post cxl
Biomechanical properties of cornea (ORA)
Biomechanical improvement immediately after CXL
CRFCRF Corneal ResistanceCorneal Resistance FactorFactor
9,05 9,42
14,15
0
2
4
6
8
10
12
14
16
CRF
StatisticalStatistical significancesignificance pp<0.05<0.05
PRE XLWITH EPI
PRE XLWout EPI
POST XLWout EPI
RESULTS RESULTS CHCH Corneal HysteresisCorneal Hysteresis
9,68 10,32
15,18
0
2
4
6
8
10
12
14
16
CH
StatisticalStatistical significancesignificance pp<0.05<0.05
PRE XLWITH EPI
PRE XLWout EPI
POST XLWout EPI
Reduction of the area/power of the keratoconus overtime
1°examination pre cxl 1 mos post‐op 3 mos post
6 mos post 12 mos post 24 mos post
+3.65 D -6.18 D
-5.17 D -6.08 D -6.61 D
-4.15 D
pt n° 138 Differential map from pre cxl to 24 mos post cxl
Cxl over time: from keratoconus toirregular astigmatism
1.0 -2.25@7 0,9 -0,75 -2.00@20 0,9 -2,50@156 mos post cxl (-0,14 D) 1 yrs post cxl (-3,42 D)
Pre cxl (44,57 D) 1 mos post cxl (+1,02 D) 3 mos post cxl (-0,37 D)
0,9 con -2,50 @15 1.0 con -2.00@10
DifferentialTangential map
from pre op to 1yrs post cxl-3,42 D

Course IC-99 – Cross-Linking – Vinciguerra - 20
BSCVA is better with minimal decrease of the curvature
3 mos post cxl
0.4 -3.00 sph
8 mos post cx
0.9 +0.75 33.00(115)
Pre cxl
0.4 -3.00 sph
1 mos post cxl
0.4 -3.00 sph
52,9 D 55,0 (+2,1) D 51,8 (-0,9) D 52,4 (-0,5) D
Differential tangential map: only – 0,5 D!!!
pt n° 154
( Differential Tru net power map +1.1D )
Curvature reduction ofkeratoconus post Cxl over time
0.2 -23sf -3.50 @55 0,4 -15,25 (-5,25)50 0.5 con -16sf -4.50@40
Differentialaxial map-11,23D
Pre cxl 6 mos post cxl 1 yrs post cxl
54,42 D 46,59 D 43,19 D
Reduction of the TRUE NET power of the keratoconus
overtime
Pre op cxl 1 mos post cxl 3 mos post cxl 6 mos post cxl
12 mos post cxl 24 mos post cxl
Differential map from pre op cxl to 2 yrs post cxlpt n° 75
49.3 D 48.8 D 46.0 D 46.3 D
46.8 D 46.1 D
Coma reduction overtime
Pre op cxl 1 mos post cxl 3 mos post cxl
6 mos post 12 mos post cxl 24 mos post cxl
coma reduction of the 44.57 %
1.685 µ 1.096 µ 1.029 µ
1.079 µ 1.013 µ 0.934 µ
pt n° 75
Reduction of elevation anterior map overtime of the keratoconus
Pre cxl 3 mos post cxl 6 mos post cxl 1 yrs post cxl
DifferentialElevation anterior
map-8 micron
Reduction of elevation posterior mapover time of the keratoconus
Pre cxl 3 mos post cxl 6 mos post cxl
DifferentialElevation
posterior map-19+ micron
pt n° 250

Course IC-99 – Cross-Linking – Vinciguerra - 21
Reduction of elevation anterior map overtime of the keratoconus
DifferentialElevation
anterior map-13 micron
Pre cxl 3 mos post cxl 6 mos post cxl
pt n° 250
Reduction of pachimetry map over time of the keratoconus post cxl with expansion (<400 µ)
385µ 272µ 287µ 275µ
Pre cxl 1 mos post cxl 3 mos post cxl 9 mos post cxl
0.3 +2.50 (-4.25)80 0.3 -2.00 (-5.00) 80 0.4 -1.50 (-4.50)80 0.6 -1.50 (-4.50)80
-110 µDifferential pachimetry map
pt n° 305
Pre cxl 1 mos post cxl 3 mos post cxl 9 mos post cxl
0.3 +2.50 (-4.25)80 0.3 -2.00 (-5.00) 80 0.4 -1.50 (-4.50)80 0.6 -1.50 (-4.50)80
62.81 D 68.47 D 59.69 D 59.77 D
Reduction of area/power over time ofthe keratoconus post cxl with expansion
pt n° 305
-5.99D of flattening
Lasik : zo ricentrata molto visibile con
riduzione dell’ametropia
PRE PRE cxlcxl 4 4 mosmos post post cxlcxlKmax 39.0.2 D Kmax 33.12 D
0,7 +3.50 -2.00 (80) 1,0 +3.50 sph
1 32
Pentacam Nucleus Staging
0
Precxl
Post cxl1yrs
Post cxl2yrs
Post cxl3yrs (19)
0 0 0 0
Staging example
Cirrus vs Pentacam
Cirrus
Pentacam
1 mos after cxlSame patient
328μ in cornea
315μ in cornea

Course IC-99 – Cross-Linking – Vinciguerra - 22
Transition line of keratoconuspost cxl over time
1 mos post cxl 2 mos post cxl
3 mos post cxl 6 mos post cxl
256μ in cornea
260μ in cornea 308μ in cornea
328μ in cornea
Transition line of keratoconus post cxlover time
in different pts
2 yrs post cxl
3 yrs post cxl3,5 yrs post cxl
1 yrs post cxl
340μ in cornea
404μ in cornea
292μ in cornea
328μ in cornea
keratoconus
Keratoconus is a degenerative disorder of the eyein wich structural changes within the cornea cause it to thin and change to a more conical shape thanits normal gradual curve.
The exact cause of the kc is uncertain, but hasbeen associated with detrimental enzyme activitywithin the cornea and with disorder of thyroid(altered value of T3, T4, FTSH) and hipofisy.
Total 91 asintomatic pts
•65, 9% male (18,3 % alterated value)
•34,1 % female (16,12 % with alterated value)
• Patologies checked:• Struma plurinodulare
• Tiroidite cronica su base autoimmunitaria
• Tiroidite cronica con noduli solidi
• Iperplasia nodulare dx/sx
• Tiroidite (assenza di noduli)
• Noduli isoecogeni
Study
•FT3‐ pg/ml (tri‐iodo‐tironina)= 1%
•FT4 ng/dl (tiroxina) = 1%
•TSHmicro U/L (thyroid stimulating hormone) = 4,39%
•Ab HTG Ul/ml =5,49%
•HTG ng/ml (normal value)
•Ab Rec TSH U/L (value normal)
•AbTPOUI/ml = 8,79%
conclusions
Thank you for your attention

Course IC-99 – Cross-Linking – Vinciguerra - 23
IV. Corneal Cross-Linking for Ectasia After Excimer Laser Refractive Surgery:
One-Year Results
CausesCauses of Ectasiaof Ectasia
Flap thicker than planned
Insufficient bed thickness
LASIK flap cuts 200 million stromal fibers
(PRK 5 millions)
Interface infiammation/infection, S.O.S. etc.
Pre‐operative overlook of risk factors
[email protected]@camesasca.com
• Patients that underwent refractive surgery
• After looking for a permanent solution for an
unpleasant situation, such as high myopia…
•…find themselves with an even worst life quality !
• Instability and an apparently endless progression of
bad visual acuity, heading towards PK…
• Often these patients come to our office when CXL is
not anymore possible, due to extreme corneal thinning
• Astonished and diffident patients …
CrossCross‐‐LinkingLinking and Ectasia and Ectasia After After RefractiveRefractive SurgerySurgery
[email protected]@camesasca.com

Course IC-99 – Cross-Linking – Vinciguerra - 24
A A GrowingGrowing PhenomenonPhenomenon ?? Effects are visible only over the long period
Inefficient interpretation of topographymaps
Unsufficient use of pachymetric mapsduring patient evaluation
Wide‐diameter flap e O.Z. (large pupil) sever a larger number of fibers
[email protected]@camesasca.com
Materials And MethodsMaterials And Methods
INCLUSION CRITERIA
corneal thickness of at least 350μm, at thinnest point
Age: 30 to 59
Signed informed consent.
Ectatic cornea (post‐LASIK, post‐PRK)
EXCLUSION CRITERIA
history of HSV, HZV
severe eye dryness
corneal infections
corneal opacities
autoimmune diseases
poorly compliant pt
pt wearing RGP CL 4 weeks before baseline examination.
[email protected]@camesasca.com
CORNEAL THICKNESS CORNEAL THICKNESS at its thinnest pointat its thinnest point
at least 400μ in degenerative ectaticcorneal diseases
At least 340μ in most severe cases
Expansion technique
At least 300μ in post refractive ectasia
[email protected]@camesasca.com
MaterialsMaterials And And MethodsMethods
13 eyes with ectasia after refractive surgery 3 prk 10 lasik
9 patients: 6 women, 3 men, mean age 42.2 years
pre SR equiv: mean ‐4,13 D ± 5,24 D (from ‐18,50 to 5,50)
pre SR sph: mean ‐2,97 D ± 4,68 D (from ‐16,00 to 6,00)
pre SR cyl: mean ‐2,32 D ± 2,06 D (from ‐8,75 to 0,00)
Ectasia progression documented in the last 6 months by:
differential topography
Scheimpflug optical pachimetry
Minimal corneal thickness: 350 µm
MEAN CCT 412 microns
Follow up: 1, 3, 6 and 12 months.
[email protected]@camesasca.com
28%
19%
5%
11%
28%
44%
20%
28%
13%15%
22% 22%
13%
30%
11%
6%
13%
25%22%
0%
10%
20%
30%
40%
50%
60%
70%
lost 1 unchanged gained 1 gained 2 gained > 2
1 (18)
3 (16)
6 (20)
12 (18)
month(eyes)
Change in BSCVA ‐ %“Safety”
[email protected]@camesasca.com
BSCVA over TIMEBSCVA over Time
0,77
0,610,680,67
0,480,48
30 18 16 20 18 50,0
0,2
0,4
0,6
0,8
1,0
1,2
1,4
pre op 1 m 3 m 6 m 1 y 1,5 y
Vin
cigu
erra
Pao
lo

Course IC-99 – Cross-Linking – Vinciguerra - 25
Achieved Correction SEQ over Time 'STABILITY'
-2,60-2,49-2,06-2,94-2,98
-4,13
30 18 16 20 18 5-10,00
-8,00
-6,00
-4,00
-2,00
0,00
2,00
pre op 1 m 3 m 6 m 1 y 1,5 y
Vin
cigu
erra
Pao
lo
Achieved Correction over time ‐SE ‐ “STABILITY”
UCVA: unchanged
preop BSCVA 0.75
12 mos: 0.9 (p<.05), SE: reduced at 6 mos (p> .05)
6 mos: Subjective UCVA improvement
6 to 12 mos continuous improvement in BSCVA.
3 mos postoperatively:
Klyce CVP, LogMAR and SRC indexes increased (p<.05)
SDP index decreased (p<.05).
6 mos postoperatively:
Ambrosio IVA index increased
KCI index, on the opposite, was significatively decreased
12 mos :
mean corneal coma, SA and high order astigmatism were decreased (p> .05)
CrossCross‐‐LinkingLinking and Ectasia and Ectasia AfterAfter RefractiveRefractive SurgerySurgery
ResultsResults
[email protected]@camesasca.com
Indexes of Indexes of
AmbrosioAmbrosio
ISV:index surface variance—this index is elevated in all types of irregularity of the corneal surface (astigm, warpage,kc, etc).
IVA:Ind of vertical Asymmetry: this index is elevated in case of oblique astigmatism, in kc or in ectasiae
KI:kc index
CKI:center keratoconus index:increases with severity of central kc
IHA: ind of Height Asimmetry: this index is analogous of IVA, this index but it is more sensitive
IHD: index of Height Decentration is elevated in keratoconus
Rmin: Minimum Sagittalcurvature in 8 mm‐zone
TKC:topographical Keratoconus Classification only based on anterior corneal [email protected]@camesasca.com
PentacamPentacam OpticalOpticalPachymetryPachymetry
PUPIL CENTER PRE 437 ± 45,28 µm POST 3 m 404 ± 64,89 µm POST 6 m 426 ± 64,25 µm POST 12 m 432 ± 31,51 µm
THINNEST POINT PRE 427 ± 47,33 µm POST 3 m 389 ± 66,42 µm POST 6 m 413 ± 66,01 µm POST 12 m 422 ± 43,61 µm
µm
[email protected]@camesasca.com
Optical Pachymetry with Pentacam
3 mos
• Mean central pupil pachymetry and mean pachymetry at
the thinnest corneal point were decreased (p< .05)
• total corneal volume at was decreased (p< .05)
• Corneal thickness at 0 and 2 mm: decreased (‐9,0%)
(p<.01)
CrossCross‐‐LinkingLinking and Ectasia and Ectasia AfterAfter RefractiveRefractive SurgerySurgery
ResultsResults
[email protected]@camesasca.com
PREPRE
PPostost 4 m 4 m
At 4 months the STEEPEST POINTcurvature value is greatly reduced
Post-lasik-5.99D of flattening

Course IC-99 – Cross-Linking – Vinciguerra - 26
20012001Case 13. 35 35 y.o.y.o. woman, woman, PhysicianPhysician
VOD 20/VOD 20/2020 ––4.00 D4.00 D
VOS 20/VOS 20/2020 ––4.00 D4.00 D
2001, OU 2001, OU successfulsuccessful LASIKLASIK
AllAll wentwent wellwell forfor twotwo yearsyears, , thenthen……
Progressive Progressive decreasedecrease in VA, in VA, withwith returnreturn totospectaclespectacle useuse..
[email protected]@camesasca.com
20032003
20052005
VOD 20/25 VOD 20/25 ––0.75 0.75 ––1.00 (65)1.00 (65)
VOS 20/35 VOS 20/35 ––1.50 1.50 ––3.25 (110)3.25 (110)
PentacamPentacam:: 2nd 2nd orderorder topographicaltopographical astigmatismastigmatism
NormalNormal pachimetrypachimetry
OD 12 OD 12 mumu suspectsuspect elevationelevation on on altimetricaltimetric mapmap
ContactContact lenslens correctioncorrection
[email protected]@camesasca.com
20052005
[email protected]@camesasca.com
20082008
VOD 20/30 –3.00 –3.75 (80)
VOS 20/40 –2.75 –3.75 (95)
OO apparent central cornealthinning
LAC withdrawal
Pentacam
OPD
[email protected]@camesasca.com
20082008
[email protected]@camesasca.com
LE, 2005 vs. 2008LE, 2005 vs. 2008
[email protected]@camesasca.com

Course IC-99 – Cross-Linking – Vinciguerra - 27
20082008LELE 404 404 μμ
+19 mu +29 mu
RE, 2008 vs. 2005RE, 2008 vs. 2005
[email protected]@camesasca.com
20082008RERE 435 435 μμ
+14 mu +30 mu
…Patient Selection !……PatientPatient SelectionSelection !!
LELE
RERE
[email protected]@camesasca.com
LE, CXL 10.14.08: 3 mos post CXLLE, CXL 10.14.08: 3 mos post CXL
Note central flattening
[email protected]@camesasca.com
CrossCross‐‐LinkingLinking and Ectasia and Ectasia
After After RefractiveRefractive SurgerySurgery
Case 13. LE, 04.03.2005, first examination, four years after LASIK for ‐4.00 –0.50 (125). BSCVA is 20/35 with ‐1.50 ‐3.25 (110).
LE, 09.03.2008, immediately before cross‐linking, BSCVA is 20/50 with ‐2.75 ‐6.00 (95). Note worsening of ectasia.
LE, 04.07.2009, 6 months after cross‐linking, BSCVA is 20/30 with ‐2.50 ‐4.00 (105). Note central flattening.
[email protected]@camesasca.com

Course IC-99 – Cross-Linking – Vinciguerra - 28
Upper right, LE 04.03.2005, first examination, the cross indicates a central point with 43.01 D of curvature. Upper left, LE 09.03.2008, immediately before cross‐linking, the same, cross‐marked, point now has 47.17 D of curvature. Differential map showing that the progression of ectasia was of 4.15 D.
Upper right, 09.03.2008, immediately before cross‐linking, the cross is on the central point with 47.17 D of curvature. Upper left, 04.07.2009, 6 months after cross‐linking, the same, cross‐marked, point now has 43.90 D of curvature. Differential map
shows that ectasia regressed of 3.27 [email protected]@camesasca.com
CrossCross‐‐LinkingLinking and Ectasia and Ectasia
AfterAfter RefractiveRefractive SurgerySurgery
ConclusionsConclusions 11
Perform regular topo‐ and tomographicexaminations using differential maps
Always suspect that a LASIK patient may develop ectasia at some future point
Perform CXL early, before cornea becomes too thin, with greatest refractive changes
[email protected]@camesasca.com
ConclusionsConclusions 22
No complications
All patients display stability
OZ apparently recentered
Mild reduction of refractive error
Improvement continues long after CXL
Corneas thinner than 400 μ are still treatable
Paolo Vinciguerra [email protected]@camesasca.com

Course IC-99 – Cross-Linking – Vinciguerra - 29
Reprinted with permission from Elsevier

Course IC-99 – Cross-Linking – Vinciguerra - 30

Course IC-99 – Cross-Linking – Vinciguerra - 31

Course IC-99 – Cross-Linking – Vinciguerra - 32

Course IC-99 – Cross-Linking – Vinciguerra - 33

Course IC-99 – Cross-Linking – Vinciguerra - 34
VI. Pediatric Patients: Two Years Results
AFTER 4 MONTHS…
-186 MICRON!!!!!!
PROGRESSION OF KCPROGRESSION OF KC
PZ 12 years
NO CXL
NO CL fitting
ExpulsiveExpulsive ChoroidalChoroidal HemorrageHemorrage 22‐‐3%3%
WoundWound leakleak or or dehiscencedehiscence 22‐‐10%10%
InadvertentInadvertent lenslens loss 1loss 1‐‐2%2%
CornealCorneal ulcerulcer and/or and/or infectioninfection 44‐‐9 %9 %
EndophthalmitisEndophthalmitis 2%2%
New New onsetonset glaucoma 5glaucoma 5‐‐9%9%
CataractCataract 22‐‐7%7%
RetinalRetinal DetachmentDetachment 33‐‐5%5%
PhthisisPhthisis 44‐‐13%13%
PK PK ComplicationsComplicationsin in PediatricsPediatrics
Stulting RD et al: Penetrating keratoplasty in children, Ophthalmology 91:1222-1230, 1984
Demographic
number of eyes : 57 stage II KC(Amsler‐Krumeich Classif)
Age average 14 years (from 9 to 18)
female 22,8% or 13 eyes
male 77,2% or 44 eyes
pre SR equiv:
mean ‐3,17 D ± 3,74 D (from ‐13,75 to 2,00)
KC progression documented by serial
differential corneal topographies and optical pachymetries.
Controlateral not‐treated eyes stage I‐II used as control.
PATIENT'S AGE DISTRIBUTION
3% 8%5%
10%
13%
17%14%
22%
5% 3% 9101112131415161718
2% Pilocarpine drops and antipain meds 30 min before CXL.
Oxybuprocaine hydrochloride 0.2% 5 min before CXL.
LASER TEST UVA meter Laser 370±5 nm
Power 3 mW/cm2 (= 5.4 j/cm2)
RICROLIN riboflavin 0.1% solutioninstillation each minute for 30 min
Riboflavin check absorption in anterior chamber (flare).
UVA Light Corneal irradiation CBM CSO 7.5 mm Ø.
RICROLIN instillation 6 times of 5 min each
Bandage soft CL application and levofloxacin eyedrops

Course IC-99 – Cross-Linking – Vinciguerra - 35
SAFETY:ENDOTHELIAL CELL COUNT
32013089
3189
1500
1700
1900
2100
2300
2500
2700
2900
3100
3300
3500
PRE 6m 24m
ECC cell/mm2
p>0.05
0,25
0,320,35
0,380,35
0,00
0,05
0,10
0,15
0,20
0,25
0,30
0,35
0,40
0,45
PRE 1m 3m 12m 24m
UCVA
p<0.05
0,570,63
0,670,72 0,7
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
PRE 1 3 12 24
BSCVA
p<0.05
UCVAUCVA
BSCVABSCVA
p<0.05
p<0.05
,PRE 1m 3m 12m 24m
Change in BSCVA% SAFETY
6%
3%
11%
34%
17%16%
31%
34%
32%
9%
14%
11%13%
21%
26%
50%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
lost 1 unchanged gained 1 gained 2 gained > 2
1 6 12 24month(eyes)
CORRECTIONsphere and cylinder
P>0.05
1,98
3,37
2,27
2,9
0,62
2,38
3,56
2,25
3,24 3
3,44
3,32
0
0,5
1
1,5
2
2,5
3
3,5
4
PRE 1m 3m 6 m 12 m 24 m
Dio
pte
rs
SPHERE
CYLINDER
p<0.05
P>0.05
SEQ correction over timeSTABILITY
-1,88
-3,10-5,10-4,89
-2,84
-5,03-3,17
257 32 19 29 19 6-12,00
-10,00
-8,00
-6,00
-4,00
-2,00
0,00
2,00
4,00
pre op 1 m 3 m 6 m 1 y 1,5 y 2 y
COMA REDUCTION
POST 2Y
PRE
RESULTS
PENTACAM TOMOGRAPHY
494,15
471,15414,64
420,36
463,80
447,00
459,83
435,00
522,00
481,00
0,00
100,00
200,00
300,00
400,00
500,00
600,00
Pupil Center Pachimetry
Thinnest Point Pachimetry
p<0.05
p<0.05
p>0.05
p>0.05
20082008 20102010 FASTER RECOVER
PEDs /ADULTs1 year
instead of 2
reductionequalityincrease
PRE XL Treat PED Eye
POST XL 6 m PED Eye
POST XL 2y PED Eye
PRE XL ADULT Eye
POST XL 6m ADULT Eye
POST XL2y ADULT Eye
ACP 50,86 49,27 49,08 50,75 52,01 49,01CYL 6,05 6,05 5,57 4,38 4,59 4,5CVP 100,99 99,04 99,37 106,42 108,02 97,02SDP 4,97 4,78 4,8 5,24 5,31 4,82CEI 1,05 0,9 0,84 1,19 1,21 1,02LogMAR 0,29 0,28 0,27 0,28 0,29 0,26DSI 11,1 11,2 12,05 12,87 12,92 12,61SRI 1,66 1,67 1,58 1,53 1,54 1,52SRC 1,46 1,48 1,44 1,53 1,55 1,5SAI 2,68 2,61 2,58 3,25 3,28 3,21IAI 0,63 0,63 0,62 0,63 0,64 0,63OSI 8,87 8,81 8,51 10,29 10,32 10,27CSI 3,21 2,68 2,45 3,45 3,62 3,15KCI 0,79 0,75 0,74 0,92 0,89 0,86KPI 0,41 0,4 0,39 0,46 0,48 0,43EDP 3,69 3,88 3,64 4,18 4,32 4,13EDD 14,88 14,49 13,59 17,01 17,52 16,75
OPDOPD CORNEAL NAVIGATORCORNEAL NAVIGATORKLYCE INDEXESKLYCE INDEXES
EQUAL BEHAVIOUR PEDs /ADULTs

Course IC-99 – Cross-Linking – Vinciguerra - 36
RESULTSTOPOGRAPHY
47,01
53,05
43,59
45,8
51,84
42,24
45,36
50,93
41,458
40
50
60
SIMK flat SIMK steep Min K
PRE
12m
24m
p<0.05
p<0.05
KERATOCONUS IRREGULAR ASTIGMATISM
PRE ODV 1.0 con -2.25@7
8 months post cxlODV 1.0 con -2.00@10
pre cxl 1 m post cxl
6 m post cxl 12 m post cxl
0.7 ‐13.25(‐8.00)0
0.7 ‐12.00(‐4.00)0 0.8 ‐6.25 (‐6.00)130
0.7 ‐12.00(‐4.00)0
DifferentialInstantaneusmap-5.48D
59.08D 56.65D
53.87D 53.60D
Only after 1 mos!!Reduction of the area/power of the keratoconusovertime
Evaluation pachymetry map over time in Pediatric cxl
Contenuta perdita di
Spessore post cxl
‐46 micron
post 1 yr!!
pre cxl 1 m post cxl
6 m post cxl 12 m post cxl
pre cxl 1 m post cxl
6 m post cxl 12 m post cxl
Only after 1 month
Reduction of the true net power of the keratoconusovertime
pre cxl 1 m post cxl 7 m post cxl
0.6 ‐8.00(‐4.00)0 0.9 ‐4.25(‐4.75)250.7 ‐7.00(‐4.00)0
Differentialaxial map-6.23D
Only after 1 month
57.95D 52.48D 51.72D
Reduction of the area/power of the keratoconusovertime
Conclusions
CXL is indicated in PEDs with progressive KC.
CXL appears to be effective in improving UCVA and BSCVA by reducing corneal asimmetry and cornealwavefront aberrations at two years follow‐up.
CXL is a safe treatment for KC, with faster reepithelialization and faster recovery of CCT in pediatric pt.
Careful screening and closer followup needed in pediatricage to avoid faster and more dramatic progression of the disease.
Thank you for your attention !
Elena AlbéIstituto Clinico Humanitas

Course IC-99 – Cross-Linking – Vinciguerra - 37
VII. Evaluation of Crystalline Lens Opacity Induced by Corneal Cross-Linking
with Scheimpflug Imaging
[email protected]@camesasca.com
EvaluationEvaluation of of CrystallineCrystalline LensLens OpacityOpacityInducedInduced byby CornealCorneal CrossCross--LinkingLinking withwith
ScheimpflugScheimpflug ImagingImaging
FI Camesasca, P Vinciguerra, S FI Camesasca, P Vinciguerra, S TrazzaTrazza
Department of OphthalmologyDepartment of Ophthalmology
IRCCS IRCCS IstitutoIstituto ClinicoClinico HumanitasHumanitas
RozzanoRozzano, Milano, Italy, Milano, Italy
Chairman: Prof. P. VinciguerraChairman: Prof. P. Vinciguerra
I have no financial interest to discloseI have no financial interest to disclose
[email protected]@camesasca.com
•• CornealCorneal CrossCross--linkinglinking (CXL):(CXL):•• stabilizesstabilizes progressive progressive keratoconuskeratoconus
•• inhibitsinhibits some some physiopathologicalphysiopathological mechanismmechanism ofof
cornealcorneal ectasia ectasia
•• increasesincreases biomechanicalbiomechanical strenghtstrenght ofof cornea cornea ofof
300%300%
•• preventsprevents PKPK
((WollensakWollensak G, Am J G, Am J OphthalmolOphthalmol 2003)2003)
ScheimpflugScheimpflug, Cristalline , Cristalline LensLens andand
CornealCorneal CrossCross--LinkingLinking
[email protected]@camesasca.com
•• ObjectiveObjective evaluationevaluation ofof crystallinecrystalline lenslens opacityopacity::•• ComplexComplex
•• LOCS III, LOCS III, AgeAge--RelatedRelated EyeEye DiseaseDisease StudyStudy
•• ClinicalClinical measurementmeasurement: : subjectivesubjective
ScheimpflugScheimpflug, Cristalline , Cristalline LensLensand and CornealCorneal CrossCross--LinkingLinking
(McCarty CA, Dev Ophthalmol 2002)
[email protected]@camesasca.com
•• OculusOculus PentacamPentacam HR Software (HR Software (OculusOculus
OptikgerOptikgeräätete, , WetzlarWetzlar, Germania) , Germania) •• information information fromfrom the the anterioranterior cornealcorneal surfacesurface
toto the the posteriorposterior crystallinecrystalline capsulecapsule
•• objectiveobjective system system measuringmeasuring densitometrydensitometry
•• full full scanscan toto reconstructreconstruct the the lenslens
ScheimpflugScheimpflug, Cristalline , Cristalline LensLensand and CornealCorneal CrossCross--LinkingLinking
[email protected]@camesasca.com
ScheimpflugScheimpflug, , LensLens andandCrossCross--LinkingLinking
PentacamPentacam software software evaluatesevaluates::•• volumevolume•• 3D 3D opticaloptical densitydensity•• meanmean opticaloptical density density
DensitometryDensitometry Software :Software :•• comparescompares density density withwith anan advancedadvanced nomogramnomogram•• assignesassignes a a lenslens density density gradegrade•• quantifiesquantifies density and area density and area ofof lenslens opacificationopacification
Measures the lens density in an objective, reppoducible and accurate way
[email protected]@camesasca.com
UV UV raysrays: a : a wellwell--knownknown etiologicaletiological agentagent ofof cataractcataract
The The ocularocular structurestructure mostmost exposedexposed toto UV UV raysrays duringduringcrosscross--linkinglinking, , afterafter the the cornealcorneal endotheliumendothelium, , isis the the crystallinecrystalline lenslens
Ectasia Ectasia patientspatients are are oftenoften veryvery youngyoung::•• progressive progressive keratoconuskeratoconus•• ectasia ectasia followingfollowing refractiverefractive surgerysurgery
ScheimpflugScheimpflug, , LensLens andandCrossCross--LinkingLinking

Course IC-99 – Cross-Linking – Vinciguerra - 38
•• 18 18 eyeseyes ofof 18 18 patientspatients withwith progressive progressive keratoconuskeratoconus, , documenteddocumented
•• CXL CXL performedperformed betweenbetween AprilApril and and JuneJune 20062006
•• meanmean patientpatient ageage: 34.9 : 34.9 ±± 6.5 6.5 yrsyrs ((rangerange: 26 : 26 toto 50)50)
•• CXL: CXL: wellwell--establishedestablished and and describeddescribed techniquetechnique
•• PreoperativelyPreoperatively and 1, 2, 3 and 1, 2, 3 yearsyears postoperativelypostoperatively
[email protected]@camesasca.com
MaterialsMaterials e e MethodsMethods
Vinciguerra P, Ophthalmology 2009
ScheimpflugScheimpflug, , LensLens andandCrossCross--LinkingLinking
••EvaluationEvaluation ::
•• complete complete ophthalmologicalophthalmological examinationexamination
•• endothelialendothelial cellcell countscounts
•• cornealcorneal topographytopography
•• aberrometryaberrometry
•• centralcentral pachimetrypachimetry and /or topo/and /or topo/tomographytomography withwith ScheimpflugScheimpflug system system
((PentacamPentacam))
•• ScheimpflugScheimpflug system system usedused forfor the the objectiveobjective evaluationevaluation ofof lenslens transparencytransparency
•• lenslens opacitiesopacities gradedgraded withwith a system a system rangingranging fromfrom 0 0 toto 33
[email protected]@camesasca.com
MaterialsMaterials e e MethodsMethods
Vinciguerra P, Ophthalmology 2009
ScheimpflugScheimpflug, , LensLens andandCrossCross--LinkingLinking
•• InclusionInclusion criteriacriteria
••Progressive Progressive keratoconuskeratoconus ((seriesseries ofof topotopo--tomographiestomographies))
••AgeAge aboveabove 1818
•• ExclusionExclusion criteriacriteria::
•• cornealcorneal thicknessthickness < 400 < 400 mumu at at thinnestthinnest pointpoint
•• historyhistory ofof herpeticherpetic keratitiskeratitis
••SvereSvere dry dry eyeeye
•• ConcurrentConcurrent cornealcorneal infectionsinfections
•• CornealCorneal opacitiesopacities
•• ConcomitantConcomitant autoimmune autoimmune diseasedisease
[email protected]@camesasca.com
MaterialsMaterials e e MethodsMethods
Vinciguerra P, Ophthalmology 2009
ScheimpflugScheimpflug, , LensLens andandCrossCross--LinkingLinking
[email protected]@camesasca.com
The The PentacamPentacam--basedbased lenslensopacityopacity evaluationevaluation system on system on
providesprovides gradesgrades rangingrangingfromfrom 0 0 toto 33
ScheimpflugScheimpflug, , LensLens andandCrossCross--LinkingLinkingMaterialsMaterials and and MethodsMethods
1 32
Pentacam Nucleus Staging
0
StagingStaging exampleexample
Time Interval
Preoperative
1 year 2 years 3 years
Crystalline lens opacity (mean)
0.18 ± 0.39(0 -1)
0.21 ±0.53
(0 -2)
0.04 ±0.20(0 -1)
0.17 ± 0.39 (0 -1)
[email protected]@camesasca.com
MeanMean UCVA and BSCVA:UCVA and BSCVA:
preoperativepreoperative :180/20 and 20/40:180/20 and 20/40
3 3 yearsyears afterafter CXL: 20/50 and 20/25 (p<.05)CXL: 20/50 and 20/25 (p<.05)
SE: SE: reductionreduction ofof 0.96 D 0.96 D
MeanMean simulatedsimulated keratometrykeratometry: : reducedreduced (p<.05)(p<.05)
EndotelialEndotelial CellCell CountsCounts : : unchangedunchanged ((p=p=.13). .13).
LensLens transparencytransparency::
measuredmeasured withwith the the ScheimpflugScheimpflug system, system, threethree yearsyears afterafter CXL CXL
remainedremained unchangedunchanged
LensLens alwaysalways transparenttransparent
ScheimpflugScheimpflug, , LensLens andandCrossCross--LinkingLinking
ResultsResults

Course IC-99 – Cross-Linking – Vinciguerra - 39
[email protected]@camesasca.com
22.34 ±9.38
(9.4 –41.6)
18.19 ±6.32
(8.2 –32.2)
ns18.4 ±3.92
(11.4 –26.3)
24.99 ± 7.9(13.7 – 37.6)
Min (%)(mean ± SD)(range: min to max)
22.34 ±9.38
(9.4 –41.6)
ns18.19 ±6.32
(8.2 –32.2)
ns18.4 ±3.92
(11.4 –26.3)
24.99 ± 7.9(13.7 – 37.6)
Max (%)(mean ± SD)(range: min to max)
3.10 ±2.29
(0.6 –7.8)
ns2.12 ±1.31
(0.3 –4.8)
ns1.93 ±0.60
(0.9 –2.9)
3.14 ± 1.21(1.3 – 5.2)
ST Dev (%)(mean ± SD)(range: min to max)
10.41 ±2.44
(7.8 –17.2)
ns9.90 ±1.64
(87.4 –14.7)
ns10.48 ±
1.79(8.30 –13.7)
11.51 ± 1.70(8.50 – 17.2)
Average opacity (%)(mean ± SD)(range: min to max)
0 -1ns0 -1ns0 -20 -1Crystalline lens opacity grading scale value (range: min to max)
0.17 ±0.39
ns0.04 ±0.20
ns0.21 ±0.53
0.18 ± 0.39Crystalline lens density (mean ± SD)
3 yearsp2 yearsp1 yearPreoperativeTime Interval
[email protected]@camesasca.com
Young Young meanmean ageage ofof the the studystudy cohortcohort: : completelycompletely
transparenttransparent lenslens
LensLens persistentlypersistently trasparenttrasparent 36 36 monthsmonths afterafter CXL: CXL:
the procedure the procedure diddid notnot induce induce anyany lenslens changechange
measurablemeasurable withwith PentacamPentacam and the and the dedicateddedicated
densitometrydensitometry softwaresoftware
Grewal DS, Ophthalmology 2009
ScheimpflugScheimpflug, , LensLens andandCrossCross--LinkingLinking
ConclusionsConclusions
[email protected]@camesasca.com
PentacamPentacam dedicateddedicated software can software can measuremeasure lenslens density in density in
anan accurate, accurate, objectiveobjective and and reproduciblereproducible wayway
AfterAfter CXL, CXL, wewe diddid notnot observeobserve anyany side side effecteffect involvinginvolving
the the lenslens or the or the cornealcorneal endotheliumendothelium at at anyany timetime intervalinterval..
Grewal DS, Ophthalmology 2009
ScheimpflugScheimpflug, , LensLens andandCrossCross--LinkingLinking
ConclusionsConclusions

Course IC-99 – Cross-Linking – Vinciguerra - 40
VIII. Anterior and Posterior Corneal Surface
Scipione Rossi,MDDirector of Ocular Microsurgey Unit
San Carlo Hospital-IDIRome, Italy
POSTERIOR CORNEAL HIGH-ORDER ABERRATIONS
AFTER CORNEAL CROSS LINKING
To evaluate the posterior corneal surface high-order aberrations (HOAs) outcomes 4 years after corneal collagen cross-linking
(CXL) in eyes with progressive keratoconus
OBJECTIVE
WHY POSTERIOR CORNEAL SURFACE?
The cornea does not exhibit uniform biomechanical strength
– The collagen fibrils of the anterior lamellae are smaller (50 µm to 100 µm) and more densely packed and interweave.
– the posterior lamellae are larger and more loosely packed and do not interweave
– This lamellae arrangement allows for the cornea to be divided into strong and weak zones, both anterior-posterior and peripheral-central.
the posterior corneal surface is a “weak zone”
IN NORMAL EYES:
Marshall J.ESCRS ,2007.
STRONG CORNEA
160 µm
1. the posterior corneal surface, its elevation and curvature have been shown to be screening factors for keratoconus
• For cut-off of 35 µm, sensitivity 93% & specificity 95%,
2. Mean posterior corneal elevation significantly higher compared to mean anterior corneal in keratoconus eyes
Nilforoushan MR, Speaker M, Marmor M, Abramson J, Tullo W, Morschauser D, Latkany R. Comparative evaluation of refractive surgery candidates with Placido topography, Orbscan II, Pentacam, and wavefront analysis. J Cataract Refract Surg 2008; 34: 623–631.Schlegel Z, Hoang-Xuan T, Gatinel D.Comparison of and correlation between anterior and posterior corneal elevation maps in normal eyes and Keratoconus suspecteyes. J Cataract Refract Surg 2008; 34:789–795De Sanctis U, Loiacono C, Richiardi L,Turco D, Mutani B, Grignolo FM. Sensitivity and specificity of posterior corneal elevation measured by Pentacam in discriminating keratoconus/subclinical keratoconus.Ophthalmology 2008; 115: 1534–1539..Tomidokoro A, Oshika T, Amano S, HigakiS, Maeda N, Miyata K. Changes in anterior and posterior corneal curvatures in
keratoconus. Ophthalmology 2000; 107: 1328–1332.Dubbleman M, Sicam VADP, Van der Heijde RGL. The contribution of the posterior corneal surface to the coma aberration of the human cornea. J Vision 2007; 7:1–8.
IN KERATOCONIC EYES:the posterior corneal surface is a “critical zone”
POSTERIOR CORNEAL ELEVATION
Table 1. The sensitivity and specificity of different posterior corneal elevation levels to distinguish between keratoconic eyes and controls.
Keratoconus Controls
Cut-off point (µm) Sensitivity Specificity
10 100 0
15 100 12.3
20 100 53.4
25 100 66.2
30 96.4 84.5
35 93.2 94.9
40 89.0 98.9.
45 86.2 100
posterior elevation optimal cutoff point to discriminate
keratoconus and keratoconus suspect versus normal corneas
35 µm
Rao SN, Raviv T, Majmudar PA, Epstein RJ. Role of Orbscan II in screening keratoconus suspects before refractive corneal surgery. Ophthalmology 2002; 109:1642–1646
Course IC-99 – Cross-Linking – Vinciguerra - 41
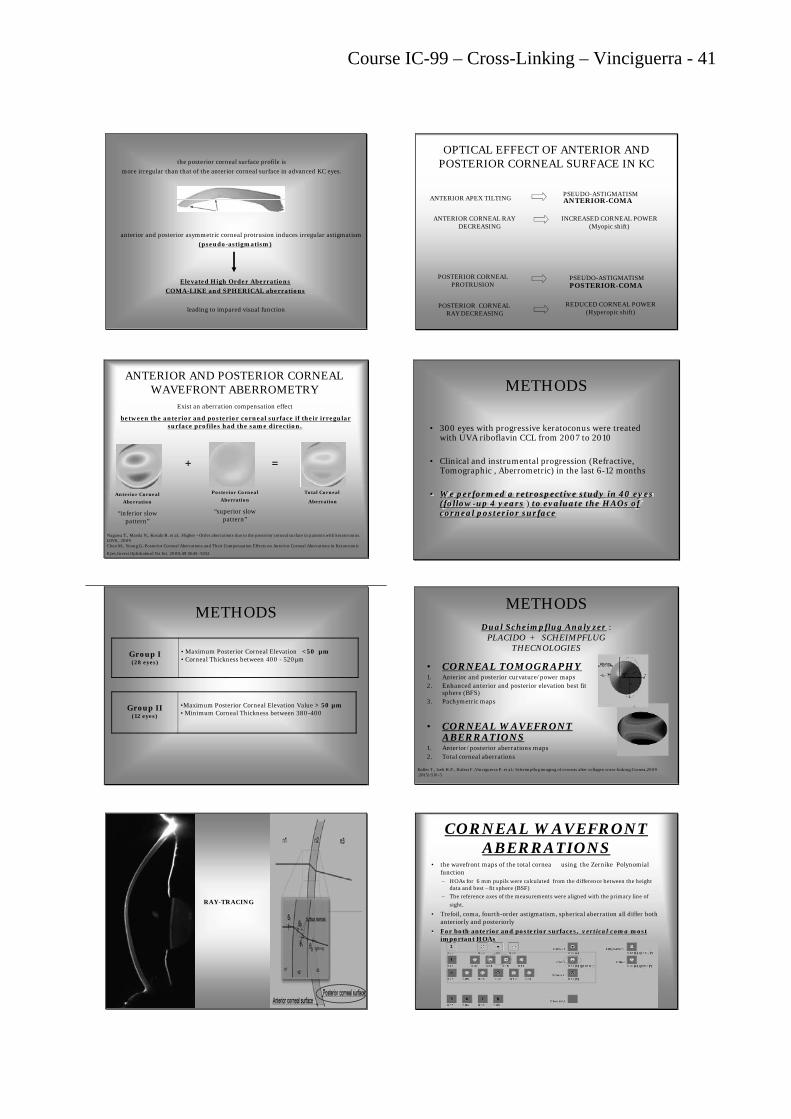
the posterior corneal surface profile is
more irregular than that of the anterior corneal surface in advanced KC eyes.
anterior and posterior asymmetric corneal protrusion induces irregular astigmatism
(pseudo-astigmatism)
Elevated High Order Aberrations
COMA-LIKE and SPHERICAL aberrations
leading to impared visual function
OPTICAL EFFECT OF ANTERIOR AND POSTERIOR CORNEAL SURFACE IN KC
ANTERIOR APEX TILTING ANTERIOR-COMAPSEUDO-ASTIGMATISM
ANTERIOR CORNEAL RAY DECREASING
INCREASED CORNEAL POWER(Myopic shift)
POSTERIOR CORNEAL PROTRUSION
REDUCED CORNEAL POWER(Hyperopic shift)
POSTERIOR CORNEAL RAY DECREASING
PSEUDO-ASTIGMATISMPOSTERIOR-COMA
Anterior Corneal
Aberration
“inferior slow pattern”
Posterior Corneal
Aberration
“superior slow pattern”
Total Corneal
Aberration
+ =
Nagawa T., Maeda N., Kosaki R. et al.: Higher –Order aberrations due to the posterior corneal surface in patients with keratoconus. IOVS., 2009Chen M., Yoong.G.:Posterior Corneal Aberrations and Their Compensation Effects on Anterior Corneal Aberrations in Keratoconic
Eyes.Invest Ophthalmol Vis Sci. 2008;49:5645–5652
ANTERIOR AND POSTERIOR CORNEAL WAVEFRONT ABERROMETRY
Exist an aberration compensation effect
between the anterior and posterior corneal surface if their irregular surface profiles had the same direction.
METHODS
• 300 eyes with progressive keratoconus were treated with UVA riboflavin CCL from 2007 to 2010
• Clinical and instrumental progression (Refractive, Tomographic , Aberrometric) in the last 6-12 months
• We performed a retrospective study in 40 eyes (follow-up 4 years ) to evaluate the HAOs of corneal posterior surface
METHODS
Group I (28 eyes)
• Maximum Posterior Corneal Elevation <50 µm• Corneal Thickness between 400 - 520µm
Group II (12 eyes)
•Maximum Posterior Corneal Elevation Value > 50 µm• Minimum Corneal Thickness between 380-400
• CORNEAL TOMOGRAPHY1. Anterior and posterior curvature/power maps2. Enhanced anterior and posterior elevation best fit
sphere (BFS)3. Pachymetric maps
• CORNEAL WAVEFRONT ABERRATIONS
1. Anterior/posterior aberrations maps2. Total corneal aberrations
Koller T., Iseli H.P., Hafezi F.,Vinciguerra P. et al.: Scheimpflug imaging of corneas after collagen cross-linking.Cornea,2009 ;28(5):510-5
Dual Scheimpflug Analyzer :PLACIDO + SCHEIMPFLUG
THECNOLOGIES
METHODS
RAY-TRACING
CORNEAL WAVEFRONT ABERRATIONS
• the wavefront maps of the total cornea using the Zernike Polynomial function – HOAs for 6 mm pupils were calculated from the difference between the height
data and best –fit sphere (BSF)
– The reference axes of the measurements were aligned with the primary line of
sight.
• Trefoil, coma, fourth-order astigmatism, spherical aberration all differ both anteriorly and posteriorly
• For both anterior and posterior surfaces, vertical coma most important HOAs

Course IC-99 – Cross-Linking – Vinciguerra - 42
Correlation the mean RMS of coma like aberration to the Amsler-Krumeich classification :
Stage I
• Eccentric steeping• Myopia and astigmatism < 5.00 D•Mean central K readings < 48.00 D•RMS of coma-LIKE from 1,50 to 2,50 µm
Stage II
• Myopia and astigmatism from 5.00 to 8.00 D• Mean central K readings < 53.00 D•Absence of scarring • Minimum corneal thickness >400 µm•RMS of coma-LIKE from > 2,50 to ≥ 3.50 µm
Stage III
•Myopia and astigmatism from 8.00 to 10.00 D• Mean central K readings >53.00 D•Absence of scarring • Minimum corneal thickness 300 to 400 µm•RMS of coma-LIKE from 3,50 to ≤4,50 µm
Stage IV
• Refraction not measurable• Mean central K readings >55.00 D• Central corneal scarring• Minimum corneal thickness 200 µm•RMS of coma-LIKE from > 2,50 µm
Aliò J.L., Shabayek M.H.: corneal higher order aberration: a method to grade keratoconus. Journal of refractive surgery., 2006;22:539-545
RESULTS AFTER 4 YEARS
• UVA: 3 mW/cm2
• Exposure time: 30 min
• Depth: 300 mm
ORDER ABERRATIONPRE OPERATIVE
MEAN (µm)POST OPERATIVE
MEAN (µm)
Mean aberration coeficient 1.75 ( 0.48198) 1.8925 ( 0.62936)
3rd Coma 2,3597 ( 1.18623) 1,0233 ( 1.925109)
3rd Trefoil -0.0548 ( 0.35627) -0.0963 ( 0.51242)
4th High order astigmatism -0.0491 ( 0.48198) 0.1524 ( 0.77456)
4th Tetrafoil -0.0294( 0.60129) -0.0543 ( 0.52224)
4th Spherical Aberration 0.3513 ( 0.73449) 0.6033 ( 1.08027)
5th High order coma 0.0488 ( 0.28599) -0.0643 ( 0.38893)
5th High order trefoil -0.0035 ( 0.20314) -0.061 ( 0.23362)
5th Pentafoil -0.0121 ( 0.19826) -0.0234 ( 0.40602)
Summary of total HOA s mean before and 4 years after corneal CXL treatment (GroupI)
Coma aberration reduction was statistically significant
ORDER ABERRATIONPRE OPERATIVE
MEAN (µm)POST OPERATIVE
MEAN (µm)
Mean aberration coeficient 1.95 ( 0.56298) 2.0925 ( 0.7336)
3rd Coma 4,895 ( 1.14623) 3,082( 1.925109)
3rd Trefoil -0.0548 ( 0.25627) -0.5478 ( 0.36242)
4th High order astigmatism -0.1091 ( 0.58198) 0.5524 ( 0.25456)
4th Tetrafoil -0.0494( 0.30129) -0.0643 ( 0.53424)
4th Spherical Aberration 0.5513 ( 0.83449) 0.8033 ( 1.09127)
5th High order coma 0.0588 ( 0.68599) -0.0843 ( 0.38893)
5th High order trefoil -0.00345 ( 0.50314) -0.071 ( 0.22562)
5th Pentafoil -0.01521 ( 0.39826) -0.0634 ( 0.42302)
Summary of total HOA s mean before and 4 years after corneal CXL treatment (GroupII)
Coma and Trefoil aberrations reduction was statistically significant
GROUP I
(28 eyes)
GROUP II
(12 eyes)Pre-CXL 4 years
Post-CXL
Pre-CXL 4 years
Post-CXL
Anterior Elevation
(µm)12,10
0,043
8,98 0,023
24,3
0,087
20,4
0,045
Posterior elevation (µm)
23,8
0,072
28,8
0,064
57,1
0,052
50,2
0,087
Total
Corneal Wavefront (COMA-RMS)
2,35
0,012
1.83
0,015
4,59
0,032
3,13
0,043
Anterior
Corneal Wavefront
(COMA-RMS)
2,40
0,027
2,35
0,038
5,62
0,068
3,24
0,0027
Posterior
Corneal Wavefront
(COMA-RMS)
-0,50
0,015
-0,80
0,013
-1,02
0,020
-0,40
0,002
Pre germano
PosteriorElevation
BFS
Thinnest point 547
PRE-CXL
27 µm
AnteriorElevation
BFS 18 µm
18
GROUP I:
Pre germano)
PosteriorElevation
BFS 33 µm
4 years POST-CXL
Thinnest point 550
AnteriorElevation
BFS 14 µm
PRE-CXL
RMS Total COMA
2,35µm
RMS Anterior COMA
2,40 µm
≥
GROUP I:

Course IC-99 – Cross-Linking – Vinciguerra - 43
RMS Total COMA
1,83 µm
RMS Anterior COMA
2,35 µm
4 years POST-CXL
> >
GROUP I:
PRE-CXL
62 micron
PosteriorElevation
BFS
Thinnest point 376
AnteriorElevation
BFS 26 micron
GROUP II:
4 years POST-CXL
Thinnest point 385
AnteriorElevation
BFS
GROUP II:
24 micron 45 micron
PosteriorElevation
BFS
PRE-CXL
RMS Total COMA
4,59µm
RMS Anterior COMA
5,62 µm
>
GROUP II:
RMS Total COMA
3,13 µm
RMS Anterior COMA
3,24 µm
4 years POST-CXL
≥
GROUP II:
Outcomes:
• In the Group I after CXL
1. The total corneal HAOs aberrations decreasedsignificantly
2. The anterior corneal HAOs aberrations decreased
3. The posterior corneal HAOs aberration increased
Outcomes:
• In the Group II after CXL
1. The total corneal HAOs aberrations decreasedsignificantly
2. The anterior corneal HAOs aberrations decreased
3. The posterior corneal HAOs aberration decreased
What Happens after Cross Linking?CONCLUSION
Demarcation line
485µ
If we treat keratoconic cornea with high tickness(450/500μm) :
The 300 μm of anterior cornea are cross-linked andthe posterior cornea (weak cornea) continue ectasic evolution
with no evidence of anterior progression ?The cross-linked anterior lamellae produce an increase of post.
elevation due too biomecanical effects ( transport effect) ?

Course IC-99 – Cross-Linking – Vinciguerra - 44
What Happens after Cross Linking?
CONCLUSION:
Does the treatment in low pachimetry cornea ( around 400 ) allow the cross-linking in the posterior corneal stroma?
390 µm
CONCLUSION
• Total Corneal HAOs, especially coma-like aberrations, always decrease significantly
• The posterior surface HOAs are related with posterior elevation and initial pachimetry.
What Happens after Cross Linking regarding HAOs?
• We observe : in our series the age of the first Group waslower than the second one but this data are notsignificative (a few cases)
• We think that also the age play a role in changing the posterior HAOs aberrations after CXL
Now our goal is follows the posterior corneal elevation and HOAs in pediatric cases
FUTURE PLANNING
THANKS FOR YOUR ATTENTION
Course IC-99 – Cross-Linking – Vinciguerra - 45
Addresses
Paolo Vinciguerra, MD Chairman, Ophthalmology Dept. Istituto Clinico Humanitas Office: Via Ripamonti, 205 20100 Milano - Italy ph + 39 02 55211388 fax +39 02 57410355 [email protected] www.paolovinciguerra.com www.refractiveonline.it
Scipione Rossi, MD [email protected]
Fabrizio I. Camesasca, MD Ophthalmology Dept. Istituto Clinico Humanitas Office: P.za Maria Adelaide, 1 20129 Milano - Italy Ph +39 02 29529396 Fax +39 02 29529396 [email protected] www.camesasca.com
Theo Seiler, MD IROC AG Institute fur Refractive und Ophthalmo-Chirurgie Stockerstrasse, 37 CH-8002 Zurich Ph. +41 43 488 38 00 Fax + 41 43 488 38 09 [email protected] www.iroc.ch
Elena Albè, MD Ophthalmology Dept. Istituto Clinico Humanitas Via Manzoni, 56 20089 Milano - Italy Ph + 3902 8824 4680 Fax +3902 8224 4694 [email protected]







