
Fundamentals of Deployment
Randy D. Kearns MSA, DHA(c), CEM
Clinical Instructor, Department of Surgery
University of North Carolina, School of Medicine
February 2009
W’s
• Who:
– Randy Kearns
• What
– Fundamentals of Deployment for EMS Systems
• Why
– Why is this important to me?
– New sense of urgency to be efficient .
Disclaimer
• UNC
– Researcher‐NC Burn Disaster Program
• NCOEMS
• ASPR
• FEMA (Reservist)
– Branch Director w/ Specialty: ES Branch

Who cares? Who is our audience?
• Public Safety Model
• Business Model
• Hospital Based Model
What do they want? and,
What do they need?
Overview
• System status management, dynamic versus static deployment (SSM)
• Call timeline gap analysis, event chain performance improvement, (patient) throughput measurements (ToT)– Time on task factors, choke points, etc.
• Unit hour utilization and the relevant variables (UHU)• Demand analysis versus "waiting‐line analysis/measurement"
(also referred to in the statistical world as Markov Chain)• Stand ready costs• Unit hour costs and how it relates to fees for service/costs for
services• Risk versus Utilization situations and relative costs• Measuring fixed costs versus variable costs

In a word, deployment is based on. . .
Utilization of
Positioning of
Cost of
Determining the need for
Definitions
• System Status Management
– The Strategy of Ambulance Placement
Deployment
• Static
– Examples
• Dynamic
– Examples
Static
• What influences selection for a base location?
– Data
– Availability of the land?
– Price of the land?
– Political influence?
– Do you redeploy ambulances when there is a call in an adjacent location?
Dynamic
• What data do you use?
• What time blocks do you move?
• How does staffing mirror demand?
• What process do you have in place to redeploy units?

Utilization of
Positioning of
Cost of
Determining the need for
Time on Task (ToT)
• Pre‐call
• Call to 9‐1‐1 or similar answering point
• PAI and Dispatch (queue)
• Chute Time
• Response Time
• On scene Time
• Transport Time
• Arrival and ready for service
Response Times
• Average
• Fractal
• (probably best but both are acceptable)

Unit Hours – Unit Hour Utilization (UHU)
• 1 ambulance, 24 hours / day, 365 days/ year
• 1 x 24 x 365 = 8760 unit hours
• (17,520 worked hours)
• If there is one call per hour then there will be a utilization of 1.0 UHU 24/24 = 1.
• 2 calls per 24 hr shift = 0.083 UHU (2/24 = 0.083)
• 8 calls per 24 hr shift = 0.333 UHU (8/24 = 0.333)
UHU Cont.
• 4 calls per 8 hr shift = 0.500 UHU (4/8 = 0.500)
• 6 calls per 8 hr shift = 0.750 UHU (6/8 = 0.750)
• 8 calls per 8 hr shift = 1.000 UHU (8/8 = 1.000)
• 4 calls per 12 hr shift = 0.333 UHU (4/12 = 0.333)
• 6 calls per 12 hr shift = 0.500 UHU (6/12 = 0.500)
• 8 calls per 12 hr shift = 0.667 UHU (8/12 = 0.667)

UHU Cont.
• Time on Task issues
• Choke Points
Utilization of
Positioning of
Cost of
Determining the need for
Unit Hour Costs (Direct Costs)• 1 ambulance, 24 hours / day, 365 days/ year
• 1 x 24 x 365 = 8760 unit hours
• (17,520 worked hours)
• If the average hourly rate is $15.00 per hour, then the salary for the unit is $15.00 x 17,520 = $262,800.
• If the benefits represent 25%, then the benefit value is $65,700
• If the supplies represent 30% of the value of the employee costs then; $140,786
• If the mileage (vehicle component is 30% of the total) then the vehicle component is: $234,643
• $703,929 / 8760 = $80.36 (significantly short of total costs per unit hour)

Medicare Source – Calculating Costs– Components
• National Uniform Base Rate – NUBR
• Relative Value Unit – RVU
• Geographic Adjustment Factor (GAF [GPCI])
• Loaded Mileage – LM
• Mileage Rate – MR
• Point of Pick up modification – POP
• Additional Payments for certain specified periods
– (NUBR x RVU x 0.7 x GAF) + (NUBR x RVU x 0.3) = Xb
– (LM x MR x POP) = Xm
Understanding Costs• Direct
• Indirect 20%
– (Public Safety Argument versus Business Model)
• Public Safety Includes Stand Ready Costs
• Business Model based solely on ability to generate revenue
• Public Safety Approach, add to costs, but also add to value. Such as specialty teams, QRV, etc.
Stand ready costs
• Typically measured poorly
– (piece of mind)

Risk and Service Availability
• How do you place resources when the services are seldom utilized?
QRV
QRV

Determining the need for
Utilization of
Positioning of
Cost of
Statistics
• Mean – mathematical average
– (problem is outliers will skew the results)
• Median – middle value of a set of values
• Range – high and low
Prediction Models
• Demand analysis versus "waiting‐line analysis/measurement" (one approach is referred to in the statistical world as Markov Chain Monte Carlo Methods)
• Demand analysis
• Common approach
• Easier to Understand
• Less precise
• Waiting‐line analysis
• Common business model
o (such as fast food)
• More difficult, generally need statistical expertise
• More precise
Demand AnalysisApr-
May05
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23Total
Monday 1 2 0 1 0 1 2 6 11 3 13 8 17 12 9 13 6 5 5 5 2 2 1 1 126Monday
0 1 0 2 0 0 0 2 6 12 12 8 10 16 14 7 4 4 0 8 6 3 2 0 117
Monday1 0 0 0 0 1 0 1 1 3 9 8 8 9 11 11 3 4 2 7 3 0 0 0 82
Monday2 0 0 0 0 0 3 2 6 11 9 11 10 16 16 8 5 6 3 5 2 7 0 1 123
Monday0 0 1 0 0 0 0 2 5 8 7 8 7 9 6 5 8 2 6 3 3 1 0 1 82
Monday1 1 0 0 0 0 0 2 0 7 5 8 5 3 5 4 5 1 6 5 0 0 0 0 58
Monday 0 1 1 0 0 0 0 9 2 0 2 2 4 1 4 2 3 2 5 9 1 0 2 1 51
Total 5 5 2 3 0 2 5 24 31 44 57 53 61 66 65 50 34 24 27 42 17 13 5 4 639
Avg # 0.71 0.71 0.29 0.43 0.00 0.29 0.71 3.43 4.43 6.29 8.14 7.57 8.71 9.43 9.29 7.14 4.86 3.43 3.86 6.00 2.43 1.86 0.71 0.57
Apr-May-06
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23TotalMonday
0 1 0 1 0 0 0 1 6 8 11 9 11 8 14 5 8 3 6 4 5 3 2 2 108Monday
2 1 1 1 3 2 1 4 10 10 13 14 12 12 9 8 5 2 4 1 2 7 3 2 129
Monday0 1 0 1 0 0 3 8 9 10 13 9 16 11 10 8 8 8 3 1 2 2 2 5 130
Monday0 0 2 1 0 2 1 3 2 10 3 7 10 11 11 6 3 5 3 0 4 3 1 2 90
1 1 0 0 1 0 2 4 4 8 9 8 11 10 12 6 4 1 3 2 2 2 0 0 91Monday
0 3 1 1 0 1 1 0 1 4 4 3 2 3 7 2 1 0 4 0 3 3 2 3 49Monday
1 1 1 1 1 2 0 3 2 1 3 3 3 5 3 1 2 1 4 4 1 4 0 1 48
Total 4 8 5 6 5 7 8 23 34 51 56 53 65 60 66 36 31 20 27 12 19 24 10 15 645
Avg # 0.57 1.14 0.71 0.86 0.71 1.00 1.14 3.29 4.86 7.29 8.00 7.57 9.29 8.57 9.43 5.14 4.43 2.86 3.86 1.71 2.71 3.43 1.43 2.14

0.571.140.710.860.711.001.143.294.867.298.007.579.298.579.435.144.432.863.861.712.713.431.432.14
Mean for May 06
0 1 1 1 0 1 1 3 4 8 9 8 11 10 10 6 4 2 4 1 2 3 2 2
Median for May 06
3 2 1 1 1 1 2 4 5 11 11 11 11 11 11 10 7 5 5 5 4 4 3 3
Staffing for May 06
0.61.10.70.90.71.01.13.34.97.38.07.69.38.69.45.14.42.93.91.72.73.41.42.10 1 1 1 0 1 1 3 4 8 9 8 11 10 10 6 4 2 4 1 2 3 2 23 2 1 1 1 1 2 4 5 11 11 11 11 11 11 10 7 5 5 5 4 4 3 3
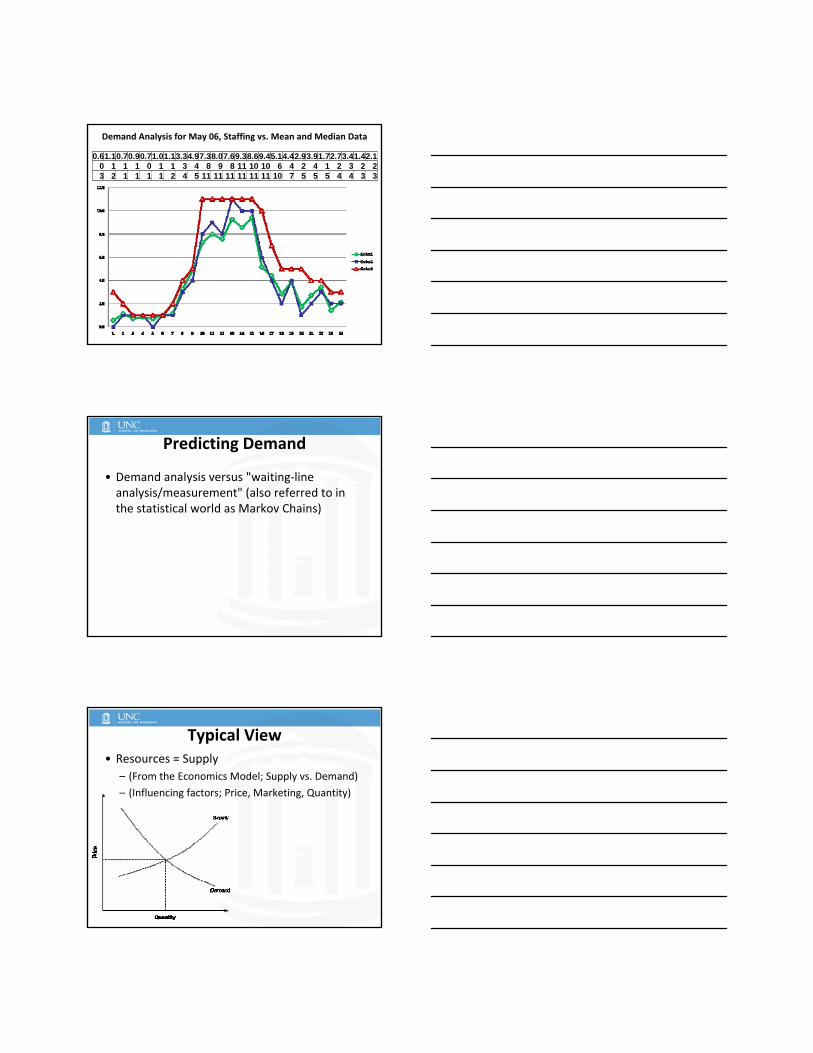
Demand Analysis for May 06, Staffing vs. Mean and Median Data
Predicting Demand
• Demand analysis versus "waiting‐line analysis/measurement" (also referred to in the statistical world as Markov Chains)
Typical View• Resources = Supply
– (From the Economics Model; Supply vs. Demand)
– (Influencing factors; Price, Marketing, Quantity)
Waiting Line Analysis
• Queue
– A single waiting line
• (order in which customers are served)
• Waiting line system consists of:
– Arrivals
– Servers
– Waiting line structures
Waiting Line Analysis components:
• Calling Population
• Arrival rate
– (must be less than service rate or system never clears out)
• Service time

Waiting Line Analysis components:
Source of Customers
Source of Customers
population we serve
Waiting line (or queue)
Waiting line (or queue)
Served Customers
Served Customers
EMS components9‐1‐1 decisions, response times, on scene times
Patients
Patients
Patients
Waiting Line Basic Structures:
• Channels (parallel servers)
– For us, it is the various ambulances/locations
• Phases (sequential servers customers must go through)
– For us, it includes 9‐1‐1 call center, response time, on scene time, transport time
• http://www.usfca.edu/~villegas/classes/984‐307/307ch16/sld001.htm
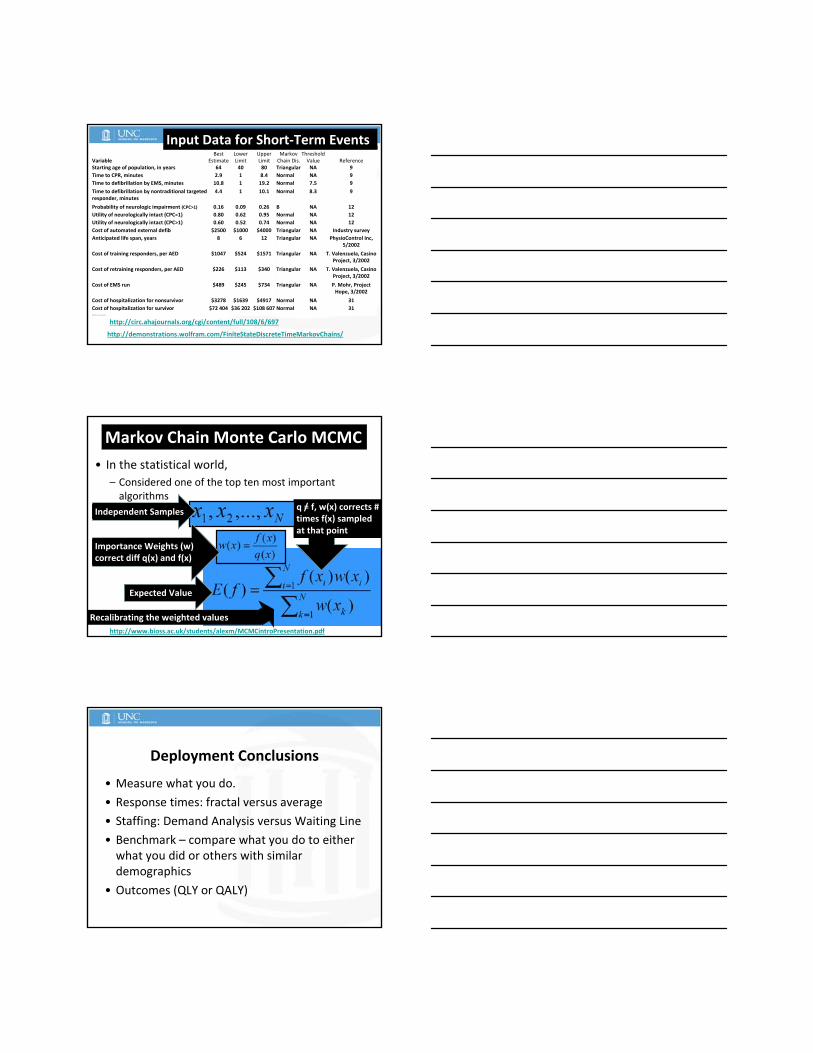
http://demonstrations.wolfram.com/FiniteStateDiscreteTimeMarkovChains/
http://circ.ahajournals.org/cgi/content/full/108/6/697
Variable Best
Estimate Lower Limit
Upper Limit
Markov Chain Dis.
Threshold Value Reference
Starting age of population, in years 64 40 80 Triangular NA 9
Time to CPR, minutes 2.9 1 8.4 Normal NA 9
Time to defibrillation by EMS, minutes 10.8 1 19.2 Normal 7.5 9
Time to defibrillation by nontraditional targeted responder, minutes
4.4 1 10.1 Normal 8.3 9
Probability of neurologic impairment (CPC>1) 0.16 0.09 0.26 B NA 12
Utility of neurologically intact (CPC=1) 0.80 0.62 0.95 Normal NA 12
Utility of neurologically intact (CPC>1) 0.60 0.52 0.74 Normal NA 12
Cost of automated external defib $2500 $1000 $4000 Triangular NA Industry survey
Anticipated life span, years 8 6 12 Triangular NA PhysioControl Inc, 5/2002
Cost of training responders, per AED $1047 $524 $1571 Triangular NA T. Valenzuela, Casino Project, 3/2002
Cost of retraining responders, per AED $226 $113 $340 Triangular NA T. Valenzuela, Casino Project, 3/2002
Cost of EMS run $489 $245 $734 Triangular NA P. Mohr, Project Hope, 3/2002
Cost of hospitalization for nonsurvivor $3278 $1639 $4917 Normal NA 31
Cost of hospitalization for survivor $72 404 $36 202 $108 607 Normal NA 31NA indicates not applicable.
Input Data for Short‐Term Events
• In the statistical world,
– Considered one of the top ten most important algorithms
http://www.bioss.ac.uk/students/alexm/MCMCintroPresentation.pdf
Markov Chain Monte Carlo MCMC
Expected Value
q = f, w(x) corrects # times f(x) sampled at that point
Recalibrating the weighted values
Expected ValueIndependent Samples /
Importance Weights (w) correct diff q(x) and f(x)
Deployment Conclusions
• Measure what you do.
• Response times: fractal versus average
• Staffing: Demand Analysis versus Waiting Line
• Benchmark – compare what you do to either what you did or others with similar demographics
• Outcomes (QLY or QALY)

Deployment Conclusions – cont.
• Have a plan, follow the plan.
• Process to hold calls or surge capacity to meet demand?
• How do we see ourselves?
• How do others see us?

Questions?
• 101‐87
• UNC over Duke








