
Francesco NEGRO

Steatosis and Chronic Hepatitis C:
liaisons dangéreuses?
Francesco NegroFrancesco NegroUnité de ViropathologieUnité de Viropathologie
Centre Médical UniversitaireCentre Médical Universitaire
GenèveGenève
Paris, January 22, 2007Paris, January 22, 2007
Occurrence and severity of steatosis is associated with genotype 3
MIHM et al, 1997; RUBBIA-BRANDT et al, 2000; ADINOLFI et al, 2001KUMAR et al, 2002; MONTO et al, 2002; POYNARD et al, 2003
HOFER et al, 2002; WESTIN et al, 2002
The score of steatosis correlates with the level of HCV RNA in serum and liver, but only in patients with genotype 3
RUBBIA-BRANDT et al, 2000; ADINOLFI et al, 2001
Virological response to IFN- is associated with the disappearance of the steatosis, which recurs at the time of virological relapse
RUBBIA-BRANDT et al, 2001; KUMAR et al, 2002; POYNARD et al, 2003
HCV-induced (i.e. viral ) steatosis

Severity of steatosis and HCV genotype
The HCV-MAID study (n = 3,068)
0
10
20
30
40
50
60
1 2 3 4
st 0 st 1 st 2 st 3
P = <0.001
LEANDRO et al, Gastroenterology 2006;130:1636-1642

n Serum HCV RNA
Liver (+) HCV RNA
Liver (-) HCV RNA
All patients 70 0.24 0.26a 0.36b
Only steatotic 28 0.24 0.34 0.49b
Only genotype 1 29 0.45 0.27 0.32
Only genotype 3 24 0.48 0.37 0.64b
a P <0.05 ; b P <0.01
Steatosis score and HCV RNA levels
70 immunocompetent chronic hepatitis C cases
RUBBIA-BRANDT et al, J Hepatol 2000;33:106-115

Expression of liver steatosis in HCV infection
and pattern of response to -interferon
Liver steatosis in a patient with recurrent hepatitis C after LT, before -IFN therapy (1a),at the time of virological response (1b) and on occasion of the biochemical and
virological relapse after the end of treatment (1c)
RUBBIA-BRANDT et al, J Hepatol 2001; 35: 307

Serum lipid profile changes in HCV
In chronic hepatitis C, Apolipoprotein B levels:– are inversely correlated with steatosis score– revert to normal upon response to therapy
HCV type 3a lowers serum cholesterol levels: HCV 1 HCV 3 HCV 4 P 188 ± 36 147 ± 42 172 ± 35 <0.01
Hypocholesterolemia in genotype 3a: – returns to normal in sustained virological responders– is not shared by other HCV genotypes
HOFER et al, Am J Gastroenterol 2002;97:2880
SERFATY et al, J Hepatol 2001;34:428

HCV core protein transgenic mouseHCV core protein transgenic mouse
MTP
intracytoplasmicTG storage
STEATOSIS
HCV coreprotein
VLDLassembly
impairedVLDL secretion
TG Apo B
PERLEMUTER et al, FASEB J 2002;16:185

Intrahepatic MTP mRNA levels are inversely correlated with steatosis
scores
MIRANDOLA et al, Gastroenterology 2006;130:1661-9
steatosis score
Intr
ah
epati
c M
TP m
RN
A levels
P = 0.0017

In most patients with genotype non-3 who do not drink alcohol:
Steatosis occurrence and severity is not (or only partially) modified by antiviral treatment
KUMAR et al, 2002; POYNARD et al, 2003
Steatosis score correlates with body mass index rather than with HCV RNA replication
ADINOLFI et al, 2001
Metabolic steatosis in chronic hepatitis C
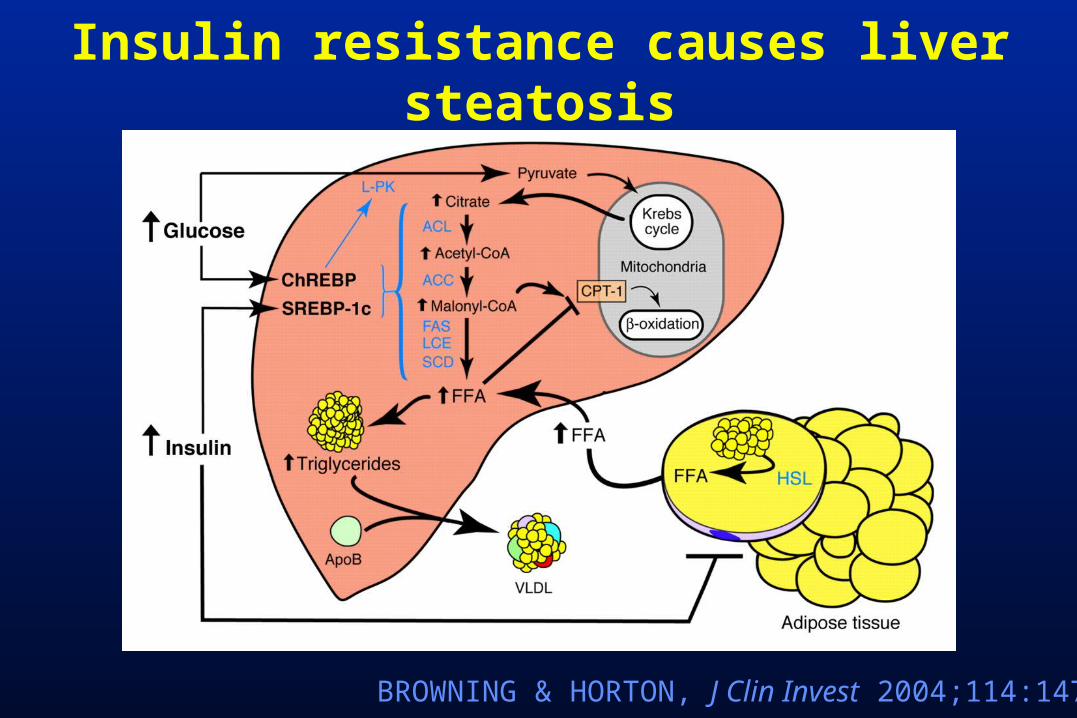
Insulin resistance causes liver steatosis
BROWNING & HORTON, J Clin Invest 2004;114:147

Risk factors for steatosis in 44 non-3a, alcohol abstinent chronic hepatitis C
patients
BMI >25
HOMA >2
no risk factors
BMI >25 / HOMA >2
MUZZI et al, J Hepatol 2005;42:41-46
30%20%
18%
32%

Mechanisms of steatosis in hepatitis C
Steatosis in hepatitis C is multifactorial:
viral steatosis:•correlates with viral replication level•responsive to antivirals•likely due to impaired lipoprotein secretion
metabolic steatosis:•mostly unaffected by antivirals•associated with BMI/insulin resistance
other causes (genetic?)

Steatosis as a factorof liver disease
progression

Natural History of HCV Liver DiseaseNatural History of HCV Liver Disease
~70%
2 – 30% / 20 yrs
2 - 4% / yr
Liver failure
(2 – 5% / yr)
Factors associated with an accelerated fibrosis progression
in chronic hepatitis C
Age at infectionSex
HIV CoinfectionHBV Coinfection
ImmunosuppressionLiver disease activity
OverweightAlcohol abuse
SteatosisSmoking
Iron overloadInsulin resistance

Impact of steatosis on liver fibrosis progression in chronic hepatitis C
A retrospective study on repeated liver biopsies
FARTOUX et al, Hepatology 2005;41:82-87
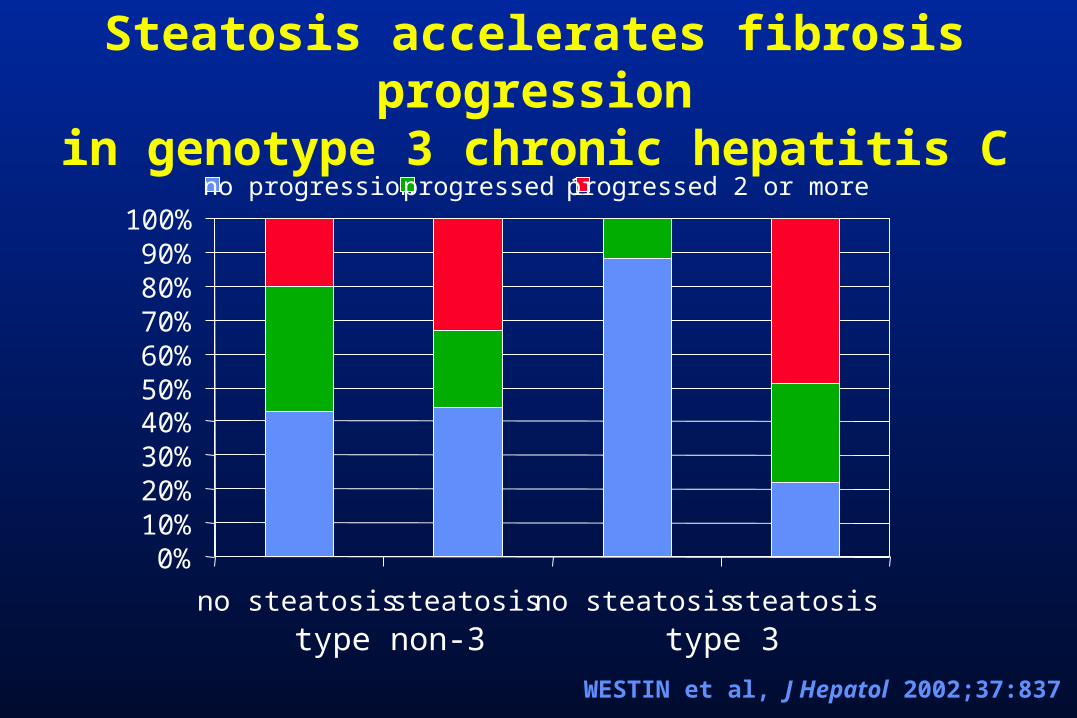
0%10%20%30%40%50%60%70%80%90%
100%
no steatosis steatosis no steatosis steatosis
no progression progressed 1 progressed 2 or more
type non-3 type 3
Steatosis accelerates fibrosis progression
in genotype 3 chronic hepatitis C
WESTIN et al, J Hepatol 2002;37:837
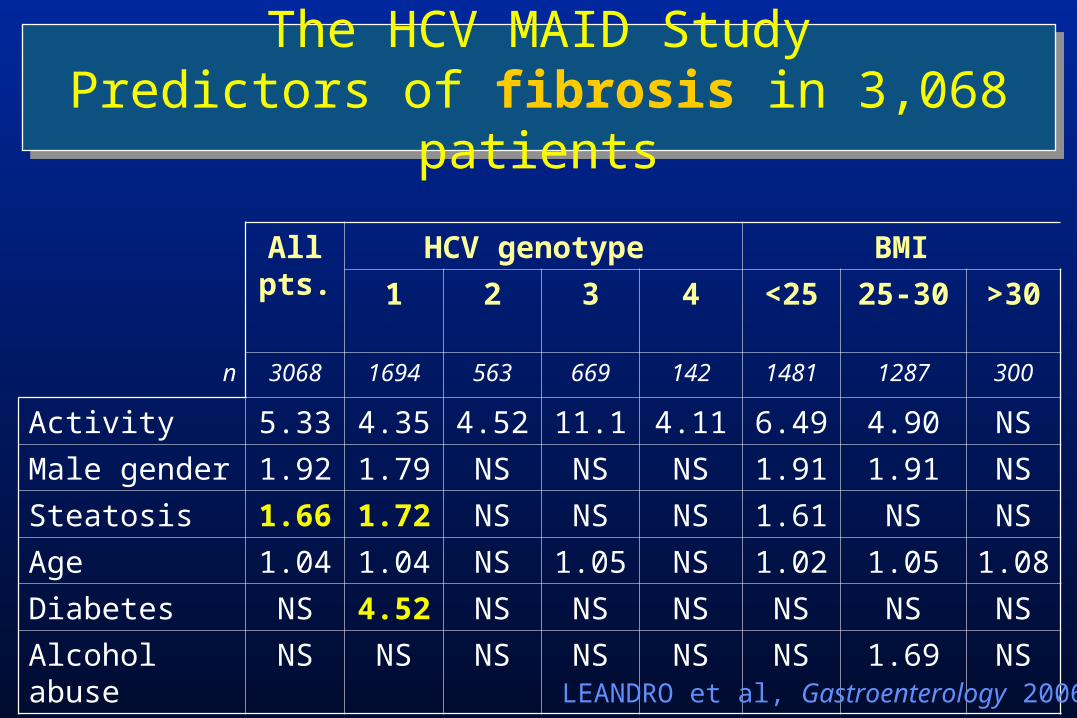
The HCV MAID StudyPredictors of fibrosis in 3,068
patients
All pts.
HCV genotype BMI
1 2 3 4 <25 25-30 >30
n 3068 1694 563 669 142 1481 1287 300
Activity 5.33 4.35 4.52 11.1 4.11 6.49 4.90 NS
Male gender 1.92 1.79 NS NS NS 1.91 1.91 NS
Steatosis 1.66 1.72 NS NS NS 1.61 NS NS
Age 1.04 1.04 NS 1.05 NS 1.02 1.05 1.08
Diabetes NS 4.52 NS NS NS NS NS NS
Alcohol abuse
NS NS NS NS NS NS 1.69 NSLEANDRO et al, Gastroenterology 2006
By MV, the HOMA insulin resistance index (but not steatosis) is a factor independently associated with fibrosis (P<0.001) and its progression rate (P=0.03)
HUI et al, Gastroenterology 2003
Insulin resistance and/or diabetes are associated with severity of fibrosis
RATZIU et al, 2003; HUI et al, 2003; FARTOUX et al, 2005MUZZI et al, 2005; LEANDRO et al, 2006
Fibrogenesis in Chronic Hepatitis C:Fibrogenesis in Chronic Hepatitis C:Steatosis or Insulin Resistance?Steatosis or Insulin Resistance?
Association between diabetes and hepatocellular carcinoma
A systematic review of epidemiologic evidence
• Diabetes significantly associated with HCC:– In 9 of 13 case-control studies (OR 2.5, 95% CI 1.8 - 3.5)– In 7 of 13 cohort studies (risk ratio 2.5, 95% CI 1.9 - 3.2)
• Association independent of alcohol or viral hepatitis (in 10 studies that examined these factors)
EL-SERAG et al, Clin Gastroenterol Hepatol 2006;4:369-380

Insulin resistance and activation of hepatic stellate
cellsProduction of CTGF
hyperglycemia hyperinsulinemia
PARADIS et al, Hepatology 2001;34:738-744
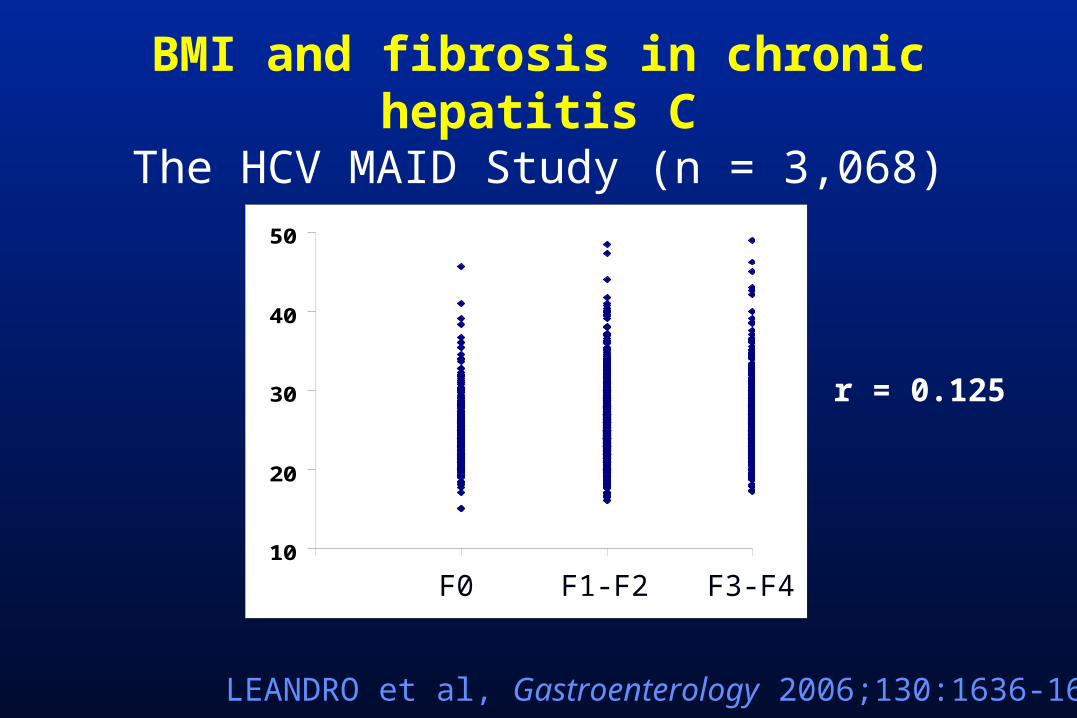
BMI and fibrosis in chronic hepatitis C
The HCV MAID Study (n = 3,068)
r = 0.125
LEANDRO et al, Gastroenterology 2006;130:1636-1642
10
20
30
40
50
0 1 2 3F0 F1-F2 F3-F4F

Omental macrophages are associated with liver necroinflammation
CANCELLO et al, Diabetes 2006;55:1554-1561
Intrahepatic necroinflammation
P<0.05
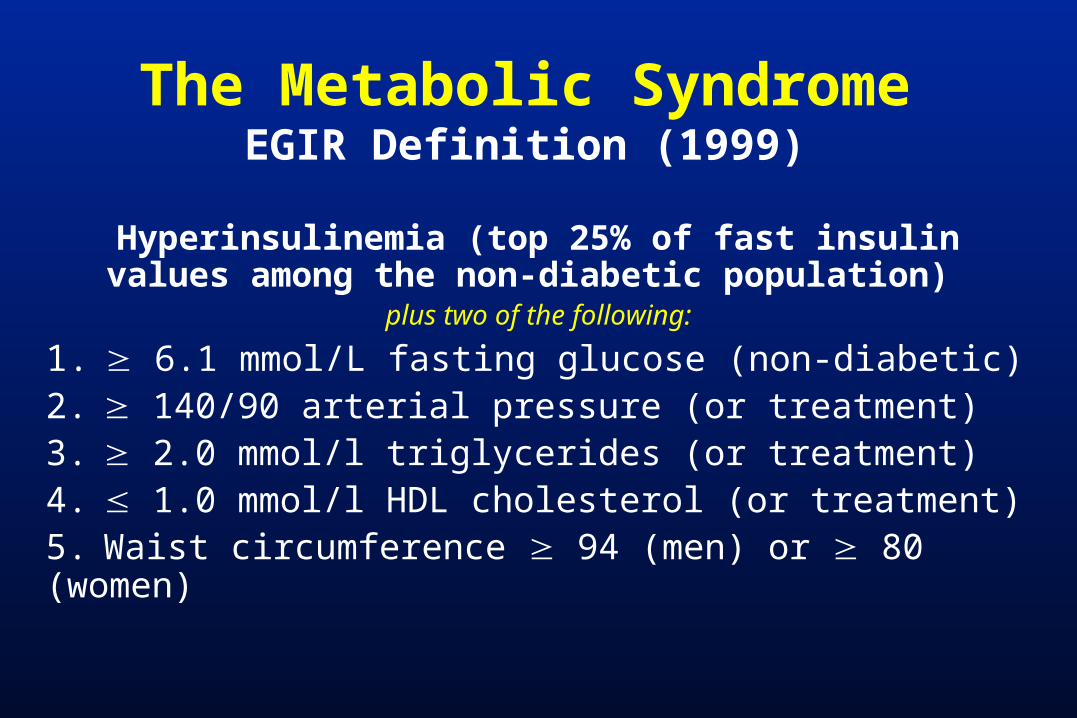
The Metabolic SyndromeEGIR Definition (1999)
Hyperinsulinemia (top 25% of fast insulin values among the non-diabetic population)
plus two of the following:
1. 6.1 mmol/L fasting glucose (non-diabetic)2. 140/90 arterial pressure (or treatment)3. 2.0 mmol/l triglycerides (or treatment)4. 1.0 mmol/l HDL cholesterol (or treatment)5. Waist circumference 94 (men) or 80 (women)

Factors associated with an accelerated fibrosis progression
in chronic hepatitis C
Age at infectionSex
HIV CoinfectionHBV Coinfection
ImmunosuppressionLiver disease activity
OverweightAlcohol abuse
SteatosisSmoking
Iron overloadInsulin resistance
Metabolic syndrome
Steatosis as a factorof poor response to
interferon-
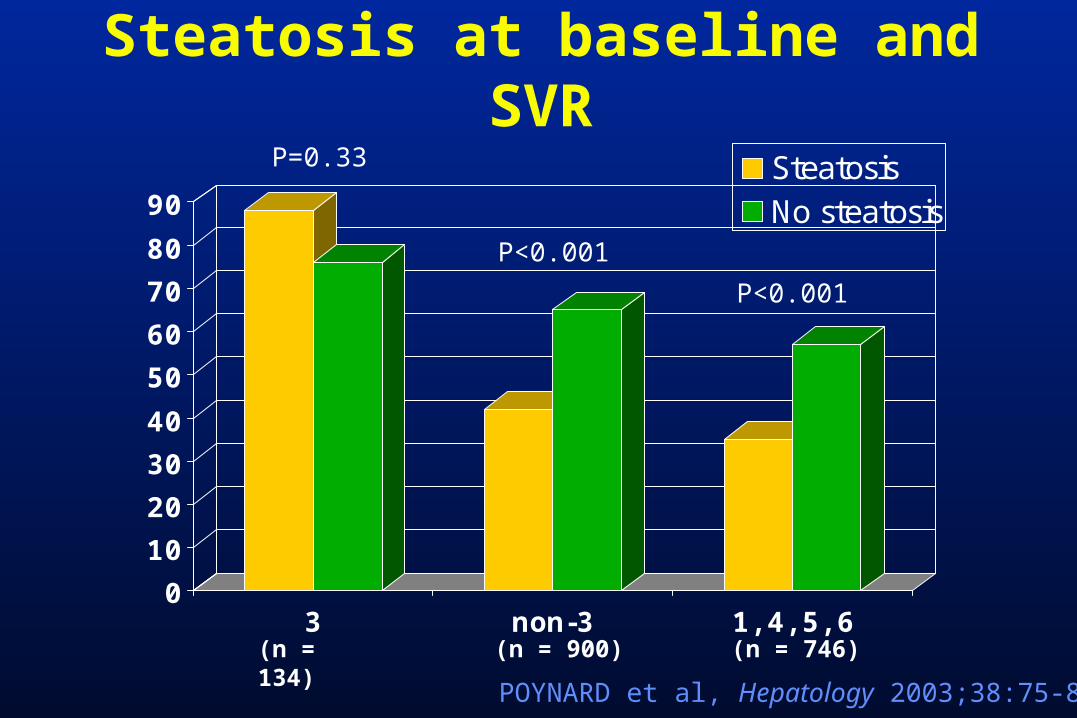
Steatosis at baseline and SVR
POYNARD et al, Hepatology 2003;38:75-85
0
10
20
30
40
50
60
70
80
90
3 non-3 1, 4, 5, 6
SteatosisNo steatosis
P=0.33
P<0.001
P<0.001
(n = 134) (n = 746)(n = 900)

Steatosis and SVR in HCV genotype 2 and 3 patients
0
20
40
60
80
100
0 <5% 6-32% 33-66% >66%
ZEUZEM et al, J Hepatol 2004;40:993-999
% S
VR
severity of steatosis
In HCV patients with virally-induced steatosis:
high serum HCV RNA
high steatosis score

Insulin resistance decreases SVR in chronic hepatitis C
ROMERO-GOMEZ et al, Gastroenterology 2005;128:636-641

HCV genotype 1, intrahepatic SOCS-3 and response to IFN-
therapy
WALSH et al, Gut 2006

Insulin resistance in HCV infection:
additional, direct role of HCV 1b 3a GFP Huh-7
IRS-1
-Actin
IRS-2
1b 3a GFP Huh-7
SOCS-7
-Actin
PAZIENZA et al, Hepatology 2007
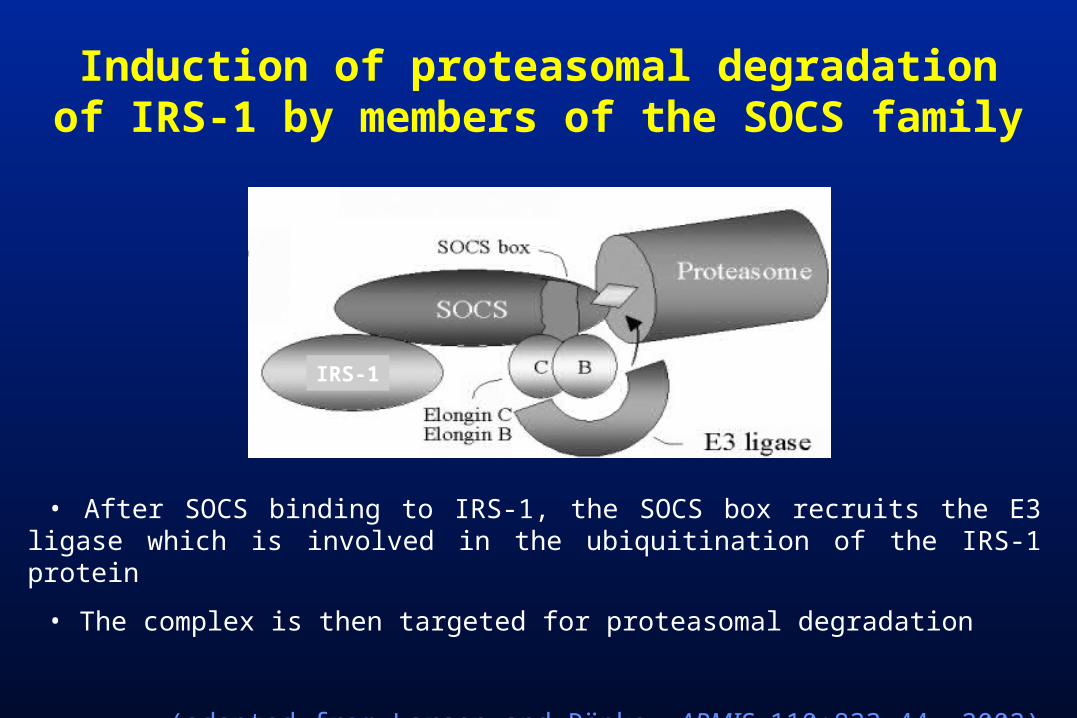
• After SOCS binding to IRS-1, the SOCS box recruits the E3 ligase which is involved in the ubiquitination of the IRS-1 protein
• The complex is then targeted for proteasomal degradation
(adapted from Larsen and Röpke, APMIS 110:833-44, 2002)
IRS-1
Induction of proteasomal degradationof IRS-1 by members of the SOCS family
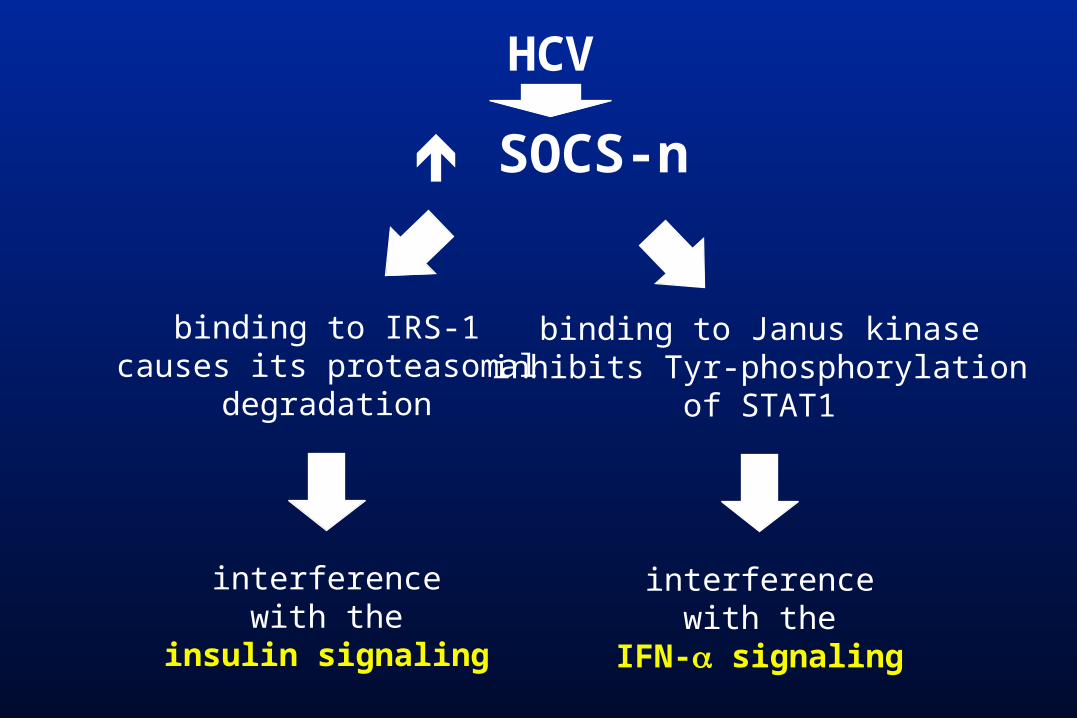
binding to IRS-1causes its proteasomal
degradation
interferencewith the
insulin signaling
binding to Janus kinaseinhibits Tyr-phosphorylation
of STAT1
interferencewith the
IFN- signaling
SOCS-n
HCV
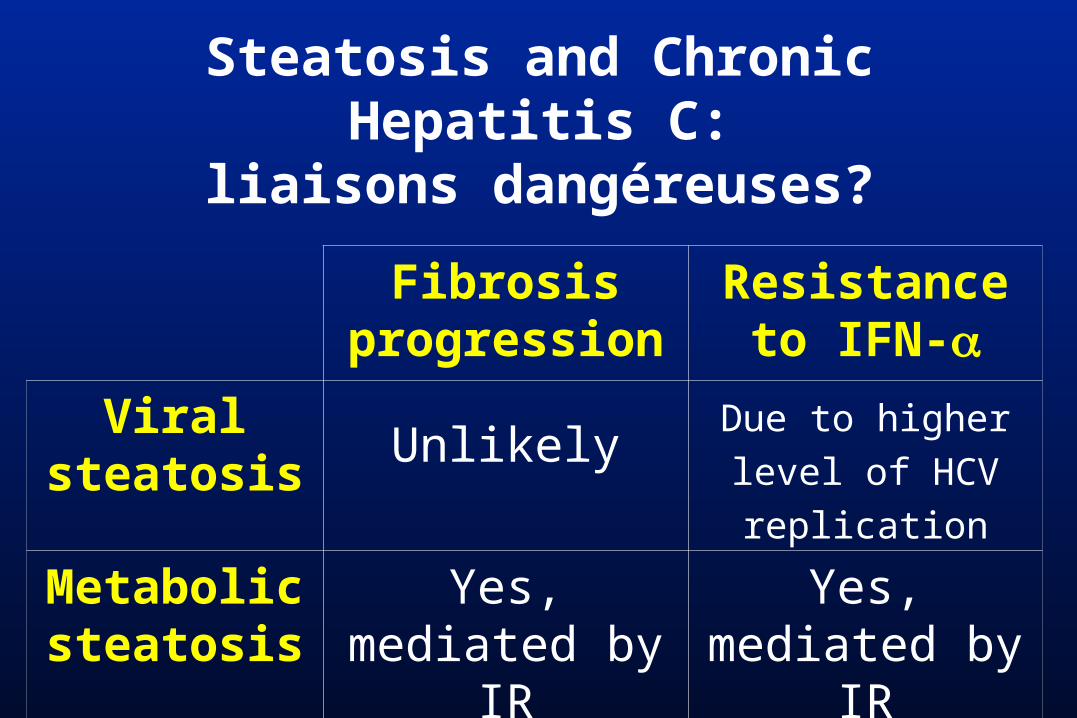
Steatosis and Chronic Hepatitis C:
liaisons dangéreuses?
Fibrosis progression
Resistance to IFN-
Viral steatosis
UnlikelyDue to higher level of HCV replication
Metabolic steatosis
Yes, mediated by IR
Yes, mediated by
IR

Increasing insulin sensitivity
in chronic hepatitis C patients• Increase physical activity
•Reduce body weight• Insulin sensitizers ??
–Metformin–Thiazolidindiones (pioglitazone, rosiglitazone…)
But the best solution is ……








