
Exercise Treatment of Non-Accident Exercise Treatment of Non-Accident Related Chronic Ankle Instability in Related Chronic Ankle Instability in
Ehlers-Danlos SyndromeEhlers-Danlos Syndrome
Alberto Friedmann, MSAlberto Friedmann, MS
American College of Sport MedicineAmerican College of Sport Medicine

Ankle Injuries in Sport:
• Common
• Debilitating
• Poorly Rehabilitated
• Reocurring
• Functional Instability

Chronic instability is not limited to injuries:
Genetic and neuromuscular disorders result in instability without trauma.
Hereditary Disorders of Connective Tissue (HDCT)
• Ehlers-Danlos Syndrome
• Marfan’s Syndrome
• Osteogenesis Imperfecta
• Benign Hypermobility Syndrome (Mild EDS Hypermobility – Type III)

Hereditary Disorders of Connective Tissue:
•Result of defective collagen (glue)
•Elastin and collagen are weak
•Tissue is frail and lax
•Fibrillins are weak and tear

Up to 70% show the same symptoms as those with frequent ankle sprains.

“Hypermobility is defined as an abnormally increased range of joint motion due to excessive laxity of the constraining soft tissues” (Everman, 1998).
Clinical Maneuver Unable to perform (0 points)
Able to Perform (1 Point)
Apposition of Thumb to ForearmRightLeft
00
11
Extension of fifth finger beyond 90 degreesRightLeft
00
11
Extension of elbow beyond 10 degreesRightLeft
00
11
Extension of knee beyond 10 degreesRightLeft
00
11
Forward flexion of trunk, legs straight, palms touching the floor
0 1
Total Beighton Score (0-9)

Functional Ankle Instability
Inability to use the ankle for daily activity:
• Walking
• Standing
• Bathing
• Getting out of a chair
• Basic balancing
Functional instability of the ankle is the most common residual disabilities after an acute ankle sprain.

Ankle Rehabilitative Therapies
• Strengthening (pronation)
• Balance
• Proprioception
• Caused by nerve-fiber damage
• Traditionally low in hypermobile subjects
“Recent studies have demonstrated reduced proprioceptive sensation in the joints of subjects who have hypermobility syndrome. Such findings have led to speculation that impaired sensory feedback contributes to excessive joint trauma in effected individuals” (Everman, 1998).

Most common trauma:
•Talofibular Joint
•Calcaneofibular Joint
Other trauma – often seen in hypermobile subjects:
• Talocrural Joint
• Talocalcaneal Joint
• Talocaneonavicular Joint
• Calcaneocuboid Joint

Traditional rehabilitation therapies:
• Balance Boards
• Theraband resistance
• Open and Closed Kinetic Chain
• Peroneal reaction treatment
• Joint proprioception treatment

Traditional means of rehabilitaion:
• Resistance training
• Reactive Neuromuscular training
• Proprioceptive training
Study purpose was to determine the effects of exercise on non-accident-related chronic ankle instability, particularly in subjects who have Ehlers-Danlos Syndrome or Benign Hypermobility Syndrome. The study looked at multi-range stability in the talocrural, talocalcaneal, talocaneonavicular and calcaneocuboid joints .

Hindfoot
Midfoot
Talocrural
Tibiofibular
Talocalcanear (Subtalar)
Talocalcaneonavicular
Cuneonavicular
Cuboideonavicular
Intercuneiform
Cuneocuboid
Calcaneocuboid

Participants:
• Direct Observation
• Volunteers
• Hypermobility Syndrome
• Five or higher on Beighton’s Scale
• 18-older
• No recent ankle trauma
• No severe ankle trauma
Procedures:
• Eight-Week Exercise Program
• Three days of exercise per week
• Traditional Rehabilitation Therapies
• Resistance Training
• Reactive Neuromuscular
• Proprioception/Balance
• Active stabilization exercises

Measures:
•Range of Motion
•Functional Strength
•Stability
•Proprioception
•Neurological Reflex
•Study start, after four weeks, study end (total of three measures)

Range of Motion:
• Standard Goniometer
• Anatomical Neutral
• Dorsiflexion – 200
• Plantar Flexion – 500
• Inversion – 50
• Eversion - 50

Monthly Training Regimen
Exercise Mon. Tue. Wed. Thur. Friday Sat. Sun.
Resistance Training X X X
Reactive Neuromuscular Training X X
Proprioception Exercises X X
Active Stabilization Exercises X

Resistance ExercisesResistance Exercises
• Leg Press
• Calf Raise
• Knee Extensor
• Knee Flexor
• Two sets of 12 repetitions at 60% max.
• Resistance increased by 10% at week four
• Third set added at week seven

Reactive Neuromuscular Reactive Neuromuscular TrainingTraining
Used resistance tubing:
• Uniplanar Anterior Weight Shift
• Uniplanar Posterior Weight Shift
• Uniplanar Medial Weight Shift
• Uniplanar Lateral Weight Shift
Proprioceptive ExercisesProprioceptive Exercises
One-foot standing balance
One-foot standing balance with hip flexion
One-foot standing balance using weights in diagonal pattern
One-foot standing balance while playing catch
Exercises on balance board
Active Stabilization Active Stabilization ExercisesExercises
Used a step-stool measuring 16” x 16” x 8” (40.6cm x 40.6cm x 20.3cm
• Forward step-up on stool
• Lateral step-up on stool
• Two-foot hop-up on stool
• Two-foot lateral hop-up on stool
• One-foot hop-up on stool
• One-foot lateral hop-up on stool
• Two-foot jump-over stool
• Two-foot lateral jump-over stool
• One-foot jump-over stool
• One-foot lateral jump-over stool

FunctionalityFunctionality
Measured on a scale 0-15:
• 0 Non functional
• 0-4 Functionally Poor
• 5-9 Functionally Fair
• 10-15 Functional
Plantar Flexion
Dorsiflexion
Inversion
Eversion

FunctionalityFunctionality
After four weeks:After four weeks: Overall increase in functional strengthOverall increase in functional strength Decrease in painDecrease in pain Decrease in joint poppingDecrease in joint popping
After eight weeks:After eight weeks: All participants fully functional in all testsAll participants fully functional in all tests Virtual elimination of painVirtual elimination of pain Elimination of joint poppingElimination of joint popping

Quality of LifeQuality of LifeFunctional StrengthFunctional Strength
Less = lower exercise = atrophy = less functionalityLess = lower exercise = atrophy = less functionality
More = more exercise = hypertrophy = more functionality = Independence= Higher Quality of LifeMore = more exercise = hypertrophy = more functionality = Independence= Higher Quality of Life

Quality of LifeQuality of Life
PainPain
More = depression = unwillingness to exercise = atrophy = more painMore = depression = unwillingness to exercise = atrophy = more pain
Less = Better outlook = social activities = social exercise = Less Less = Better outlook = social activities = social exercise = Less medication = Higher Quality of Lifemedication = Higher Quality of Life

Quality of LifeQuality of Life
ProprioceptionProprioceptionLess = Poor balance = unwillingness to exercise = Higher risk of injury = Less = Poor balance = unwillingness to exercise = Higher risk of injury =
Nerve fiber damage = Decreased proprioceptionNerve fiber damage = Decreased proprioception
More = Better balance = feeling of ability = exercise adherence = lower More = Better balance = feeling of ability = exercise adherence = lower risk of injury = Increased independence = Higher quality of liferisk of injury = Increased independence = Higher quality of life
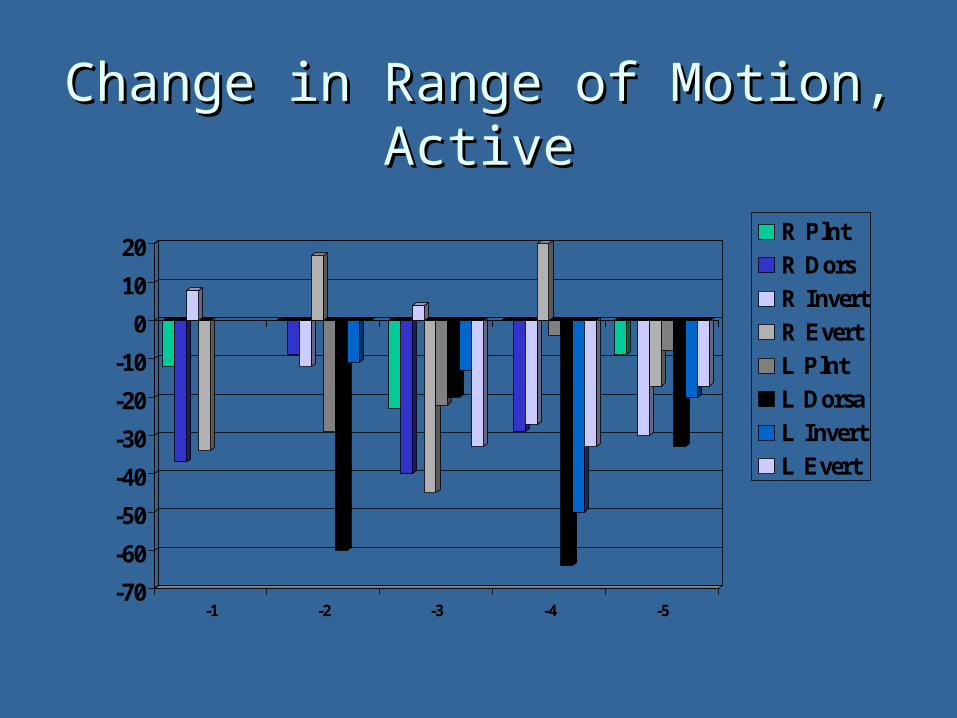
Change in Range of Motion, Change in Range of Motion, ActiveActive
-70
-60
-50
-40
-30
-20
-10
0
10
20
-1 -2 -3 -4 -5
R Plnt
R Dors
R Invert
R Evert
L Plnt
L Dorsa
L Invert
L Evert
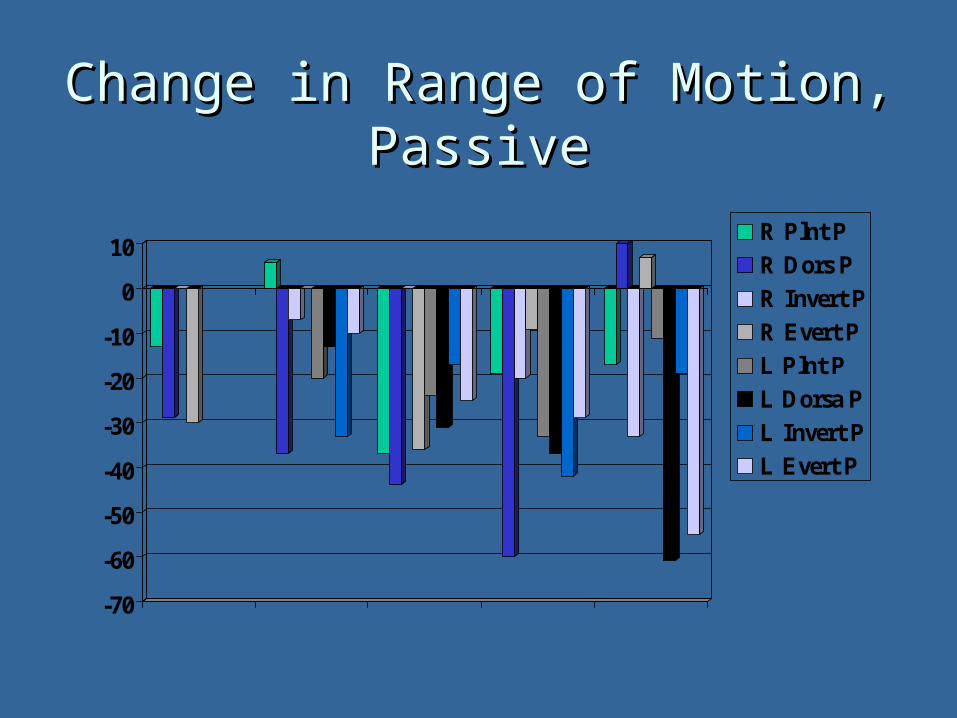
Change in Range of Motion, Change in Range of Motion, PassivePassive
-70
-60
-50
-40
-30
-20
-10
0
10 R Plnt P
R Dors P
R Invert P
R Evert P
L Plnt P
L Dorsa P
L Invert P
L Evert P

Overall Change in Range of Overall Change in Range of MotionMotion
-30
-25
-20
-15
-10
-5
0
Part. 1 Part. 2 Part. 3 Part. 4 Part. 5 1-5 Mean

Reduction in ROMReduction in ROM
Overall decrease in both passive and active indicates:
Hypertrophy in tendons and ligaments as well as muscle tissue.
Hypermobile joints can be strengthened and stabilized before laxity leads to injury.
Proper, supervised exercise is of benefit to this population

Inversion ChangesInversion Changes
Inversion injuries:
• Common
• Reoccur
• Difficult to rehabilitate

Participants showed:
Decreased Pain and Joint Popping
Decreased Range of Motion
Increased Balance and Proprioception
Increased Daily Functioning

ImplicationsImplications
Rehabilitation of other joints for this special population
Shoulder Capsule
Hip Socket
Interphalangeal Joints
Metacarpophalangeal Joints

ImplicationsImplications
EDS patients, and possibly patients with other hypermobility syndromes, could be treated in multiple joints prior to disruptive injuries or the need for surgery due to joint hyperlaxity.
Injury and surgery is more damaging and dangerous for this population than the average person.
ImplicationsImplications
Study participants showed primary gains during the initial four weeks of study intervention
Primary increases in range of motion occurred during the final four weeks of study intervention
Therefore, it is possible that a four-week intervention followed by maintenance would be as, if not more, successful

Future ResearchFuture Research
Studies involving a larger population and studies involving multiple-joint treatments
Long-term effects of exercise on children with Hereditary Disorders of Connective Tissue
Four-week versus Eight-week programs
Animal studies involving muscle, tendon and ligament tensile strength, elasticity and plasticity







