
Engaging Citizens and Engaging Citizens and Consumers in Setting Consumers in Setting
Health PrioritiesHealth Priorities
Susan Dorr Goold MD, MHSA, MASusan Dorr Goold MD, MHSA, MA
Associate Professor of Internal MedicineAssociate Professor of Internal Medicine
Director, Bioethics ProgramDirector, Bioethics Program

AcknowledgmentsAcknowledgments
Marion Danis, MD – Department of Clinical Bioethics, Marion Danis, MD – Department of Clinical Bioethics, Warren Magnuson Clinical Center, National Institutes Warren Magnuson Clinical Center, National Institutes of Healthof Health
Health Media Research Lab, UM Comprehensive Health Media Research Lab, UM Comprehensive Cancer CenterCancer Center
Matt Davis, MD, and Jeannie Thrall, Pediatrics; Matt Davis, MD, and Jeannie Thrall, Pediatrics; Andrea Biddle, UNC; Ellen Benavides and John Klein, Andrea Biddle, UNC; Ellen Benavides and John Klein, Cirdan, Minnesota; Marge Ginsburg, Sacramento Cirdan, Minnesota; Marge Ginsburg, Sacramento Health Decisions; Nancy Baum; Stephanie Marion-Health Decisions; Nancy Baum; Stephanie Marion-LandaisLandais
Picker-Commonwealth Scholars Program, Robert Picker-Commonwealth Scholars Program, Robert Wood Johnson Foundation, Allina Foundation, Wood Johnson Foundation, Allina Foundation, California Healthcare Foundation, UM Biotechnology California Healthcare Foundation, UM Biotechnology Development FundDevelopment Fund

DisclosureDisclosure
As one of the inventors of CHAT, I, As one of the inventors of CHAT, I, the University of Michigan, and the the University of Michigan, and the NIH benefit from royalties received NIH benefit from royalties received from licensed uses of CHATfrom licensed uses of CHAT

Public FrustrationPublic Frustration
Purchasers search for ways to Purchasers search for ways to contain costscontain costs
Patients and citizens have lost Patients and citizens have lost power and control over healthcare power and control over healthcare decisionsdecisions
How do we make allocation How do we make allocation decisions more patient-centered?decisions more patient-centered?

The ProblemThe Problem
Healthcare allocation decisions are Healthcare allocation decisions are politically, emotionally, intellectually politically, emotionally, intellectually and morally difficultand morally difficult

Consumer Sovereignty ModelConsumer Sovereignty ModelChoiceChoice
Informed, prudent and imaginative consumers Informed, prudent and imaginative consumers choose from several diverse alternative health choose from several diverse alternative health insurance plans according to their own values insurance plans according to their own values and preferencesand preferences Variations: Variations: Consumer cost-sharing, consumer-Consumer cost-sharing, consumer-
directed health benefit plansdirected health benefit plans
Like market allocation of other resources, this Like market allocation of other resources, this system would fairly distribute goods according system would fairly distribute goods according to individual differences in how they value to individual differences in how they value various types and features of health insurancevarious types and features of health insurance
Citizen Involvement Citizen Involvement VoiceVoice
Healthcare priority setting should Healthcare priority setting should reflect values and preferences of reflect values and preferences of populationpopulation
Population affected by decisions Population affected by decisions should be involved in decision makingshould be involved in decision making
Allocation decisions self-imposed, Allocation decisions self-imposed, consent via participationconsent via participation

Obstacles for Both ModelsObstacles for Both Models
Issues lack salience for the wellIssues lack salience for the well Consumers not well-informed Consumers not well-informed
– Issues complex, technical, intimidating, Issues complex, technical, intimidating, frightening frightening
– Information needs are voluminousInformation needs are voluminous– Need imaginationNeed imagination
Purchaser is not consumerPurchaser is not consumer Accountability to purchasersAccountability to purchasers
How involve citizenry - what methodHow involve citizenry - what method
CHATCHATChoosing Healthplans All TogetherChoosing Healthplans All Together©©
Simulation exercise Simulation exercise Participants design a hypothetical health benefits Participants design a hypothetical health benefits
package, making trade-offs between competing needs for package, making trade-offs between competing needs for limited resourceslimited resources
Group product Group product group deliberation group deliberation Overcome apathy, perceived irrelevance, and complexity, Overcome apathy, perceived irrelevance, and complexity,
and moderate individual self-interestand moderate individual self-interest GoalsGoals
What health insurance features/benefits do What health insurance features/benefits do citizens/consumers prefer?citizens/consumers prefer?
What reasons or values do citizens/consumers use to What reasons or values do citizens/consumers use to justify tradeoffs?justify tradeoffs?
Can CHAT be a “just enough” process for setting Can CHAT be a “just enough” process for setting healthcare priorities?healthcare priorities?

Versions/DerivativesVersions/Derivatives Board game (paper version)Board game (paper version) Software Software
Group exercise - same time/place, Group exercise - same time/place, laptopslaptops
Content (financials, benefit options) Content (financials, benefit options) can be altered using Planner software can be altered using Planner software and Survey Editorand Survey Editor
Automated data collectionAutomated data collection Web CHAT (2005)Web CHAT (2005)

The ExerciseThe Exercise Each round of playEach round of play
Choose healthplan benefitsChoose healthplan benefits Experience “health events”Experience “health events” Reflect out loudReflect out loud
4 Rounds of play4 Rounds of play Individual- choose benefits for self and Individual- choose benefits for self and
familyfamily Groups of 3-choose for “neighborhood”Groups of 3-choose for “neighborhood” Entire group-choose for communityEntire group-choose for community Individual-choose for self and familyIndividual-choose for self and family
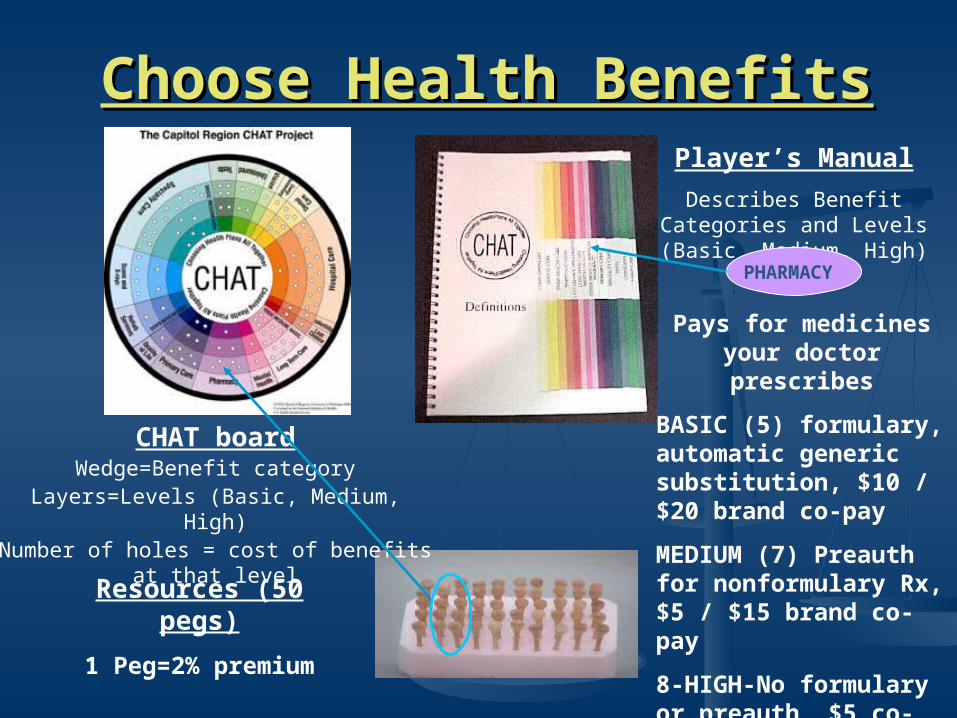
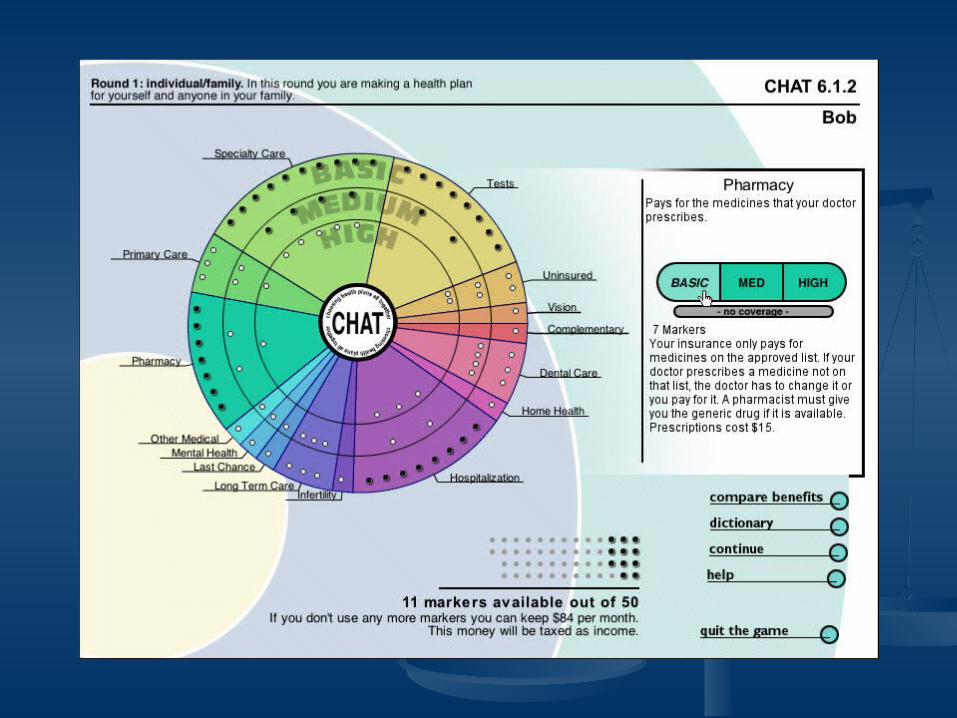
Choose Health BenefitsChoose Health Benefits
CHAT boardWedge=Benefit category
Layers=Levels (Basic, Medium, High)Number of holes = cost of benefits at that level
Resources (50 pegs)
1 Peg=2% premium
Player’s Manual
Describes Benefit Categories and Levels (Basic, Medium, High)
PHARMACY
Pays for medicines your doctor prescribes
BASIC (5) formulary, automatic generic substitution, $10 / $20 brand co-pay
MEDIUM (7) Preauth for nonformulary Rx, $5 / $15 brand co-pay
8-HIGH-No formulary or preauth, $5 co-pay

---Experience Health Events------Experience Health Events---
UNINSURED PEOPLE
Health Events
Players receive a “health event” through a “random” process
SPECIALTY CARE
VISION CARE

What we have learnedWhat we have learned What do they choose?What do they choose? Why do they choose the way they do?Why do they choose the way they do? What do they think of CHAT?What do they think of CHAT? >4000 have participated>4000 have participated
low-income uninsuredlow-income uninsured employeesemployees senior citizenssenior citizens adult disabled Medicaid enrolleesadult disabled Medicaid enrollees Californians (basic benefits package)Californians (basic benefits package) youth and young adults in S. Africayouth and young adults in S. Africa

CHAT is enjoyable and understandable, CHAT is enjoyable and understandable, even for those with little educationeven for those with little education
75% 80% 85% 90% 95% 100%
Informative
Easy to Do
Enjoyable
Understandable

Category Initial - Individual - Final Groups
Hospitalization 98.7 99.6 100
Pharmacy 93.1 96.1 100
Dental 96.1 93.0 100
Tests 81.1 88.1 91
Primary Care 81.4 86.4 95
Specialty 69.6 81.4 100
Vision 83.3 80.7 82
Mental Health 59.0 65.2 95
Home Health 58.4 64.2 86
Last Chance 49.8 59.1 73
Other 56.7 56.2 73
Uninsured 50.2 56.0 86
Long Term Care 53.3 55.7 86
Complementary 59.0 50.6 50
Infertility 18.4 13.7 9
Low-Income Uninsured (n=234 in 22 groups)
Danis M, Biddle AK, Goold SD. Insurance Benefit Preferences of the Low-Income Uninsured J Gen Int Med. 2002
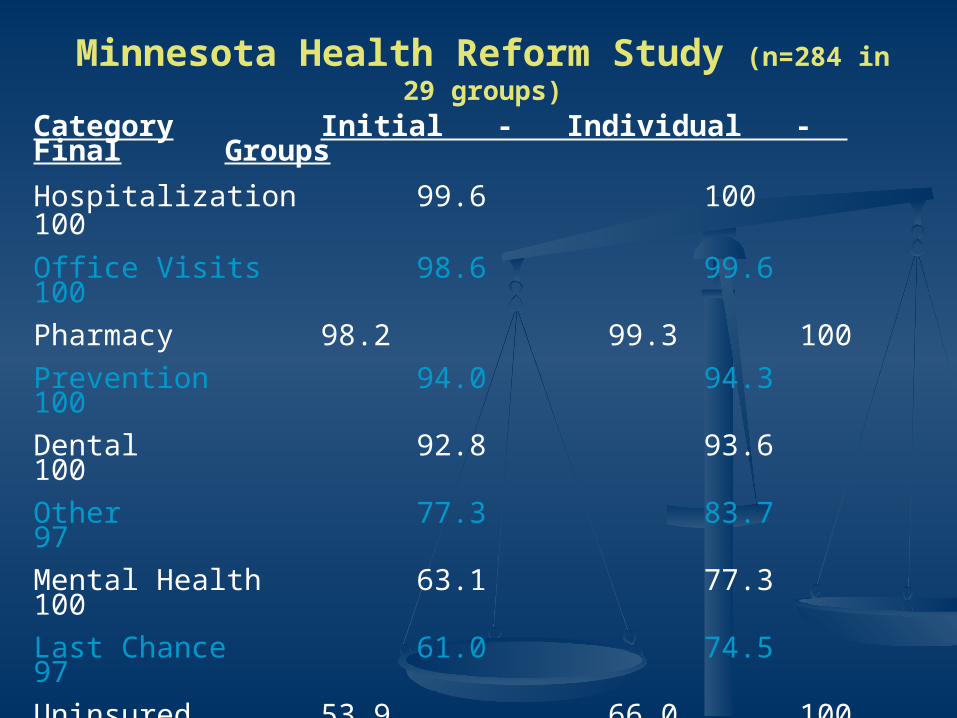
Category Initial - Individual - Final Groups
Hospitalization 99.6 100 100
Office Visits 98.6 99.6 100
Pharmacy 98.2 99.3 100
Prevention 94.0 94.3 100
Dental 92.8 93.6 100
Other 77.3 83.7 97
Mental Health 63.1 77.3 100
Last Chance 61.0 74.5 97
Uninsured 53.9 66.0 100
Long Term Care 45.4 64.5 100
Complementary 58.5 58.2 59
Quality of Life 36.2 33.3 28
Minnesota Health Reform Study (n=284 in 29 groups)

California EmployeesCalifornia EmployeesGroup Choices
Totala Basicb Medium High
100% 78% 22% -
100 96 4 -
100 99 1 -
100 100 - -
100 100 -
99 97 1
94 54 40
91 91 -
88 85 3
71 66 4
69 16
19 19
12 12 - -
10 10 -
3 3
1 1 -
Individual Choices
Category Total Basic Medium High
Primary Care 99% 62% 36% 1%
Pharmacy 99 84 14 1
Hospital 99 91 8 -
Specialty 99 92 7 -
X-rays 97 94 3
Tests 95 92 3
Dental 87 85 2
Rehabilitation 68 62 6
Vision 65 65
Mental Health 61 47 14
Last Chance 60 55 5
Complementary 25 25
Quality of Life 14 14
Long Term Care 13 12 1 -
Uninsured 10 9 1
Infertility 6 5 1

Will Insured Citizens Give Up Benefits to Will Insured Citizens Give Up Benefits to Include the Uninsured?Include the Uninsured?
Initial Individual
46%
32%
22%
Final Individual
35%
31%34%
24%
76%
Group
No CoverageChildren Only
4% premium
Children and Adults (8% premium)
Goold SD, Green SA, Biddle AK, Benavides E, Danis M. Will Insured Citizens Give Up Benefits to Include the Uninsured? J Gen Int Med 2004

(Almost) Everyone Prioritizes (Almost) Everyone Prioritizes Preventive ServicesPreventive Services
NoneNone 6%6% BasicBasic 63%63% MediumMedium 27%27%
94%94% HighHigh 4%4%
ALL groups chose preventive services
of individuals
Individual Choices for Prevention
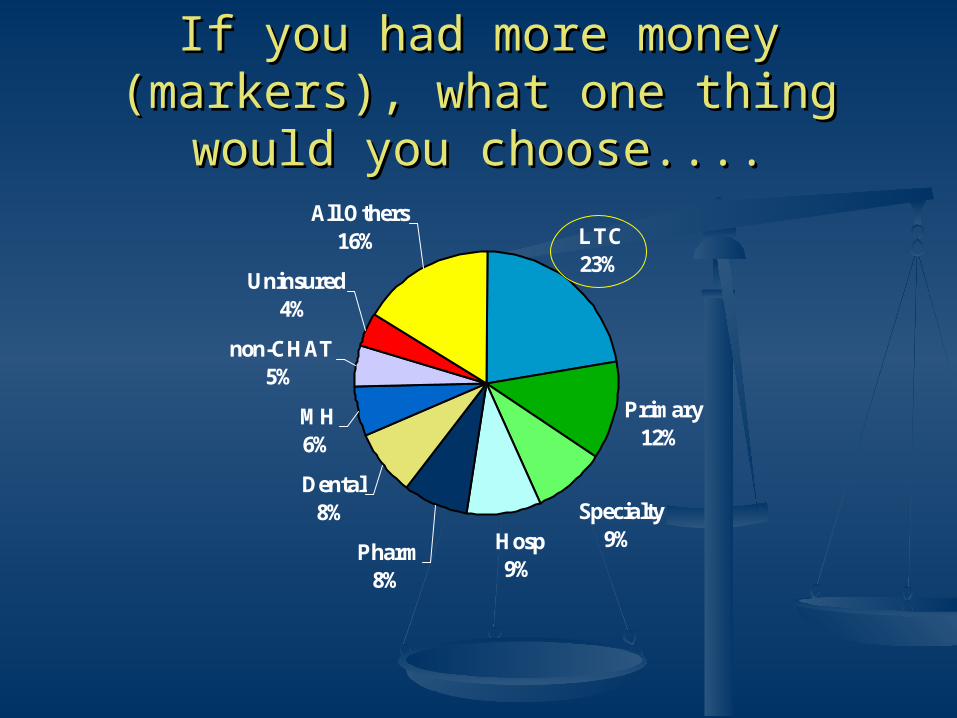
If you had more money (markers), what If you had more money (markers), what one thing would you choose....one thing would you choose....
LTC23%
Primary12%
Specialty9%Hosp
9%Pharm
8%
Dental8%
MH6%
non-CHAT5%
Uninsured4%
All Others16%
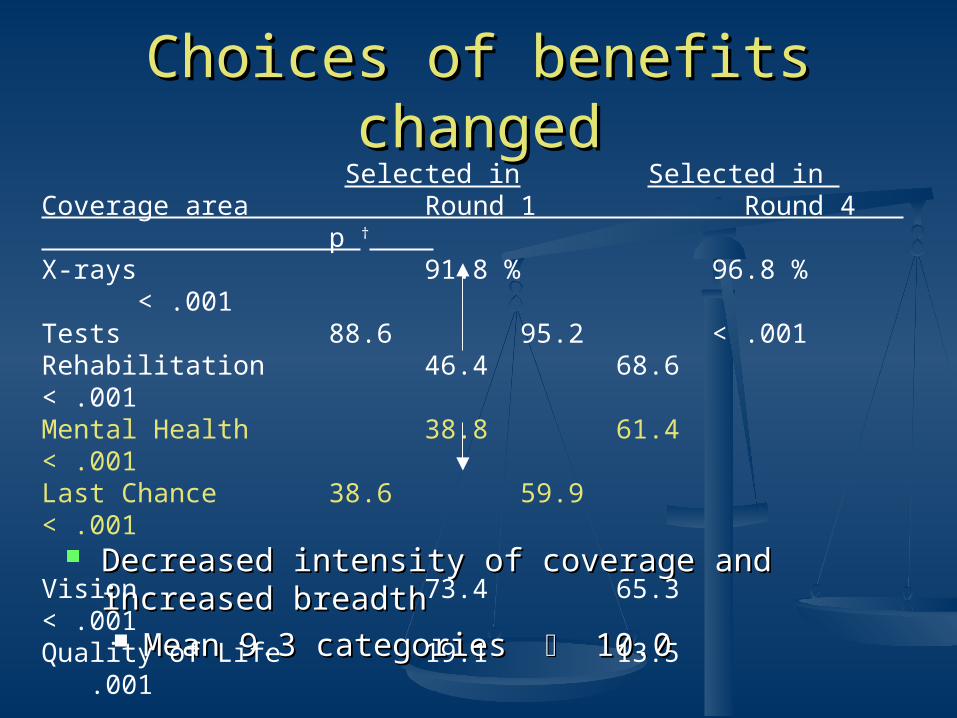
Choices of benefits changedChoices of benefits changed
Decreased intensity of coverage and increased Decreased intensity of coverage and increased breadthbreadth Mean 9.3 categories Mean 9.3 categories 10.0 10.0
Selected in Selected in Coverage area Round 1 Round 4 p † X-rays 91.8 % 96.8 % < .001Tests 88.6 95.2 < .001Rehabilitation 46.4 68.6 < .001 Mental Health 38.8 61.4 < .001Last Chance 38.6 59.9 < .001
Vision 73.4 65.3 < .001Quality of Life 19.1 13.5 .001
(N=698) † McNemar’s Chi-Square
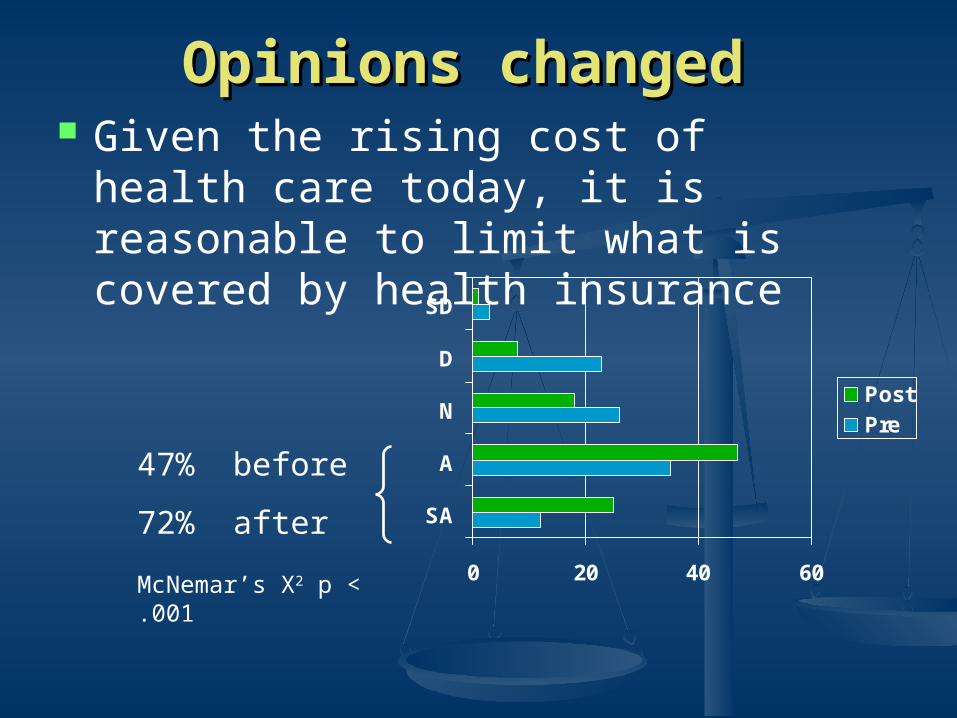
Opinions changedOpinions changed Given the rising cost of health care today, it
is reasonable to limit what is covered by health insurance
0 20 40 60
SA
A
N
D
SD
PostPre
47% before
72% after
McNemar’s X2 p < .001

Participant ratings of Participant ratings of Decision, Process and InformationDecision, Process and Information
Decision Outcome Scale (2 items) 4.1 +/- 0.9 (1 to 5)“I was satisfied by the group’s decision”
Procedural fairness Scale (7 items) 4.3 +/- 0.9
“Disagreements in the group were resolved in a fair way”
Information adequacy Scale (6 items) 4.2 +/- 0.8
“We had enough information to make good decisions”
Mean +/- SD

Willingness to abide by the group’s decision
Agree87%
Disagree11%
Missing2%
North Carolina Minnesota California

Reasons and RationalesReasons and RationalesInsurance as protectionagainst loss/harm
ProbabilityTypeMagnitudeTiming/DurationWhose
PhysicalFinancialEmotionalSocialEffect on risk itself
Preferences for theProcess of Care
QualityChoiceTimingHassles/ConvenienceBeliefs/AttitudesControl over DecisionsDistance
Doctors -SpecialistsHospitals/FacilitiesTreatmentsLength of StayType of Provider
Economics andEfficiency
Conserving MoneyValue for MoneySupply and DemandWasteLimited Resources
Moral HazardSubstitutesComplementsAlternative sources
Equity and Fairness EqualityProportionalitySocial Justice
Caring for the worseoffWhat is better forgroup/community

Reasons Given for Covering the Reasons Given for Covering the UninsuredUninsured
It could (did) happen to me or someone I knowIt could (did) happen to me or someone I know
““I have never had health insurance in my entire life. I have never had health insurance in my entire life. Nobody in my family (did).” [“Nobody in my family (did).” [“But that’s your But that’s your choicechoice”] “But it’s not a choice, and I’ll tell you from ”] “But it’s not a choice, and I’ll tell you from personal experience that it’s not a choice.”personal experience that it’s not a choice.”
““I was thinking not just of, not necessarily about I was thinking not just of, not necessarily about myself but my sister who has 2 kids and it’s like myself but my sister who has 2 kids and it’s like well if she did lose her job... I would want them well if she did lose her job... I would want them covered somehow.”covered somehow.”

Take Care of the Children/ElderlyTake Care of the Children/Elderly
““Do we want to at least cover the children of the Do we want to at least cover the children of the uninsured?… I think even Jane agrees with that.” uninsured?… I think even Jane agrees with that.” [[LaughterLaughter]]
““When the mother or father of at least four children When the mother or father of at least four children get sick, they don’t have access…so the kids are get sick, they don’t have access…so the kids are going to be left without parents.”going to be left without parents.”
““There are so many of the elderly who cannot afford There are so many of the elderly who cannot afford any kind of insurance” any kind of insurance” “That’s a good point.” “Ok, I’ll go for it.”

Everyone Should Have Health Everyone Should Have Health InsuranceInsurance
““The bottom line is some people just can’t The bottom line is some people just can’t afford it, they can’t do it.”afford it, they can’t do it.”
“…“…the single mom, and the kid. She’s the single mom, and the kid. She’s working two jobs…and she doesn’t have a working two jobs…and she doesn’t have a health plan.” “health plan.” “Right. I don’t have a Right. I don’t have a problem with that.” problem with that.”
““To me it’s a basic human right”To me it’s a basic human right”
Better (or Cheaper) for SocietyBetter (or Cheaper) for Society
““Your children are well taken care of … and Your children are well taken care of … and healthy, not abused, not as addicted, we healthy, not abused, not as addicted, we have less violence…my world would be have less violence…my world would be safer.”safer.”
““If we don’t insure these people they’re If we don’t insure these people they’re going to end up on welfare.”going to end up on welfare.”
““They get [hospital] bills…and they can’t They get [hospital] bills…and they can’t pay. Who pays for that bill?” “pay. Who pays for that bill?” “The The hospital.” hospital.” “No, we do. It’s the people who “No, we do. It’s the people who are insured.”are insured.”

Reason Given Against Covering the Reason Given Against Covering the Uninsured:Uninsured:
It’s Their Responsibility or ChoiceIt’s Their Responsibility or Choice“…“…that Joe Blow needs insurance, can’t afford it, that Joe Blow needs insurance, can’t afford it,
they understand that. But to John Doe who they understand that. But to John Doe who doesn’t want to pay…and would rather buy the doesn’t want to pay…and would rather buy the new car….”new car….”
““If Theresa as a single parent decides to stay If Theresa as a single parent decides to stay home and care for her children, when she’s very home and care for her children, when she’s very capable of working…”capable of working…”
““Insurance is not an entitlement. It is not an Insurance is not an entitlement. It is not an entitlement. And if it is, then I should have life entitlement. And if it is, then I should have life insurance and…long-term disability and short-insurance and…long-term disability and short-term disability and everything else.”term disability and everything else.”

People Will Drop Their Current InsurancePeople Will Drop Their Current Insurance
““... everybody would drop their ... everybody would drop their insurance”insurance”
““How do we slow that uninsured group How do we slow that uninsured group from becoming half the population?”from becoming half the population?”

People Will Move Here to Get People Will Move Here to Get InsuranceInsurance
““And let’s talk about another reality. And let’s talk about another reality. If we’re going to cover the adults, If we’re going to cover the adults, we are opening the door to people we are opening the door to people from states right now that have no from states right now that have no coverage what so ever. And that coverage what so ever. And that will be a drain….Just like what’s will be a drain….Just like what’s happened with welfare.”happened with welfare.”

Preventive Services are not Preventive Services are not ControversialControversial
Preventive services choices not Preventive services choices not mentioned frequently in group mentioned frequently in group discussionsdiscussions
Perceived as valuable and cost-effectivePerceived as valuable and cost-effective ““I think prevention is real important because I think prevention is real important because
that’s where a lot of things begin and [you] that’s where a lot of things begin and [you] catch everything …”catch everything …”
““[Prevention] is a low investment for a big [Prevention] is a low investment for a big return.”return.”

SummarySummary Groups of employees and ordinary citizens can Groups of employees and ordinary citizens can
and will deliberate effectively about health and will deliberate effectively about health prioritiespriorities
The CHAT exercise is viewed by participants as The CHAT exercise is viewed by participants as enjoyable, understandable, informative and fairenjoyable, understandable, informative and fair Most participants would be willing to abide by the Most participants would be willing to abide by the
decisions made by their groupsdecisions made by their groups The exercise of prioritizing may make The exercise of prioritizing may make
individuals individuals more understanding of the needs of others and more understanding of the needs of others and
necessary tradeoffsnecessary tradeoffs more prudentmore prudent
Can CHAT be useful for the Can CHAT be useful for the Community Meetings?Community Meetings?
What health care benefits and services What health care benefits and services should be provided?should be provided?
How does the American public want health How does the American public want health care delivered?care delivered?
How should health care coverage be How should health care coverage be financed?financed?
What trade-offs are the American public What trade-offs are the American public willing to make in either benefits or financing willing to make in either benefits or financing to ensure access to affordable, high quality to ensure access to affordable, high quality health care coverage and services?health care coverage and services?







