E. Wesley Ely, MD, MPHProfessor of Medicine
Vanderbilt University, Nashville, TNVA TN Valley Health Care System GRECC
CUSP4MVP-VAPSATs and SBTs: of Guidelines & Implementation
Disclosures: ICU Physician Vanderbilt - Abbott, Hospira, Orion- NIH and VA U.S. Federal Funding- Author of PAD Guidelines of SCCM 2013- Chair of SCCM Delirium section for PAD - Co-Chair of SCCM ICU Liberation project to aid world-wide implementation
Barr J, et al. Crit Care Med. 2013;41:263-306.
AgitationPai
n
Delirium
Barr J et al, CCM 2013;41:263-306
Clinical Practice Guidelines for the sustained use of sedatives and analgesics in the critically ill adult
Jacobi, CCM 2002
Clinical Practice Guidelines for the management of Pain, Agitation, and Delirium in adult patients in the Intensive Care Unit
Barr, CCM 2013
New guidelines emphasize individual symptom management
OLD(2002)
New(2013)
Take Home Message
Delirium = Dangerous
Andros Island by N Rakov, NEJM 2011;365:457
Patient = Vulnerable

© r
usty
rhod
es v
ia F
lickr
50-70%Cognitively Impaired
Wolters Intensive Care Med 2013; 39: 376Jackson AJRCCM 2010; 182: 183
Girard Crit Care Med 2010; 38: 1513

Latronico Lancet Neurol 2011; 10: 931
60-80%Functionally
Impaired
Mar
cel O
oste
rwijk
via
Flic
kr
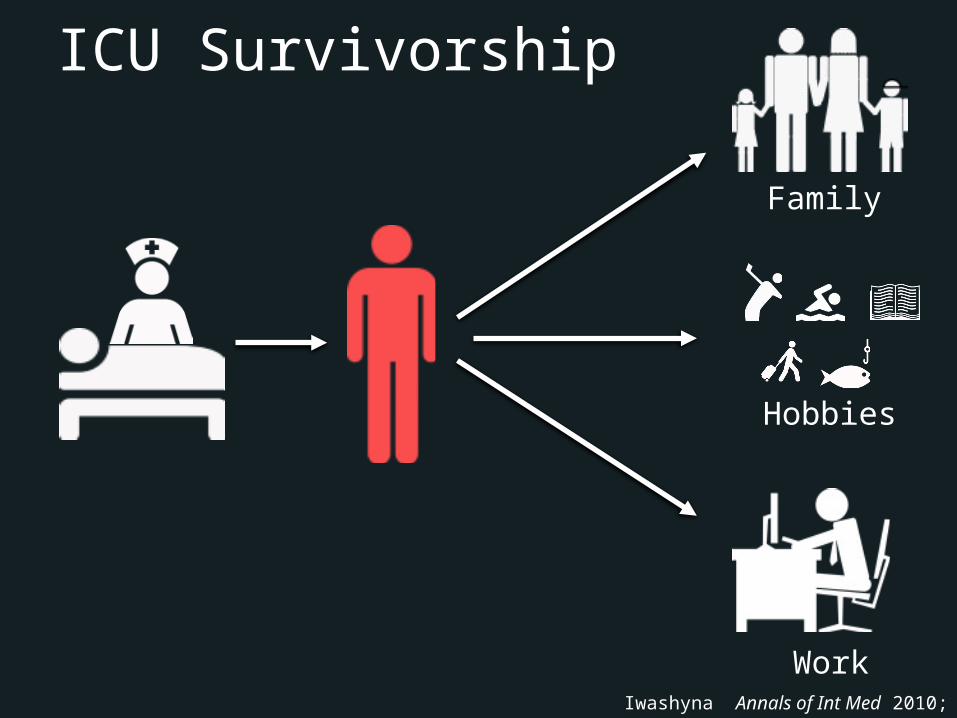
ICU Survivorship
Family
Hobbies
WorkIwashyna Annals of Int Med 2010; 153:204-5
...like it was in a huge, empty gray space, sort of like a monstrous underground parking garage with no cars, only me, floating or seeming to float, on something…
-SB
“©
Travis Sm
ith via F
lickr
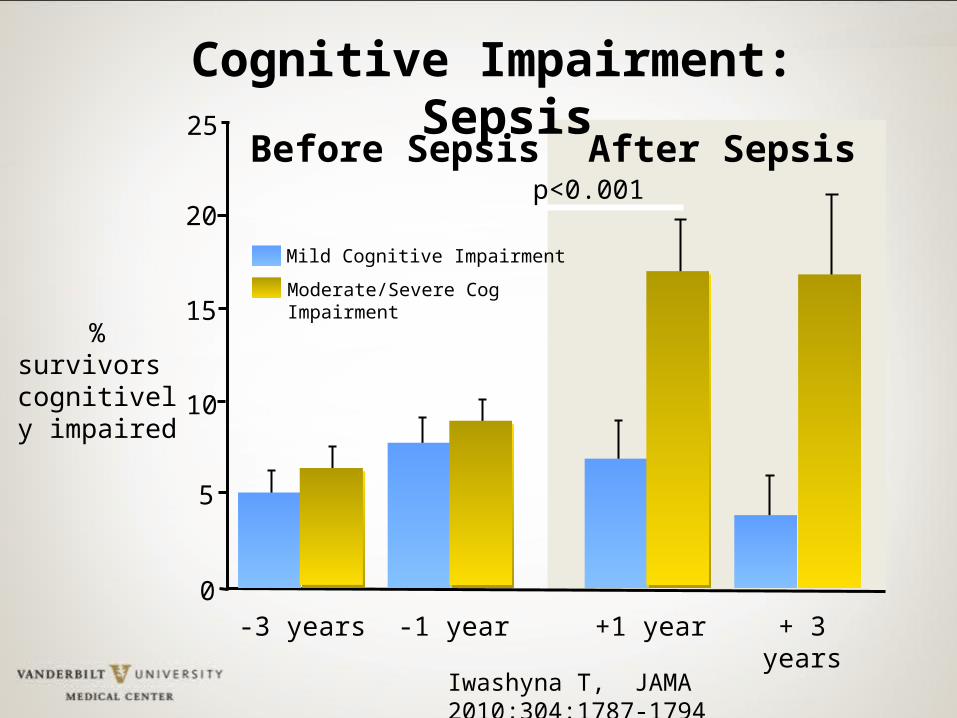
Mild Cognitive Impairment
Moderate/Severe Cog Impairment
20
15
10
5
0
% survivors cognitively impaired
-3 years -1 year +1 year + 3 years
25
p<0.001After SepsisBefore Sepsis
Iwashyna T, JAMA 2010;304:1787-1794
Cognitive Impairment: Sepsis
Ely EW, JAMA 2004;291:1753-62
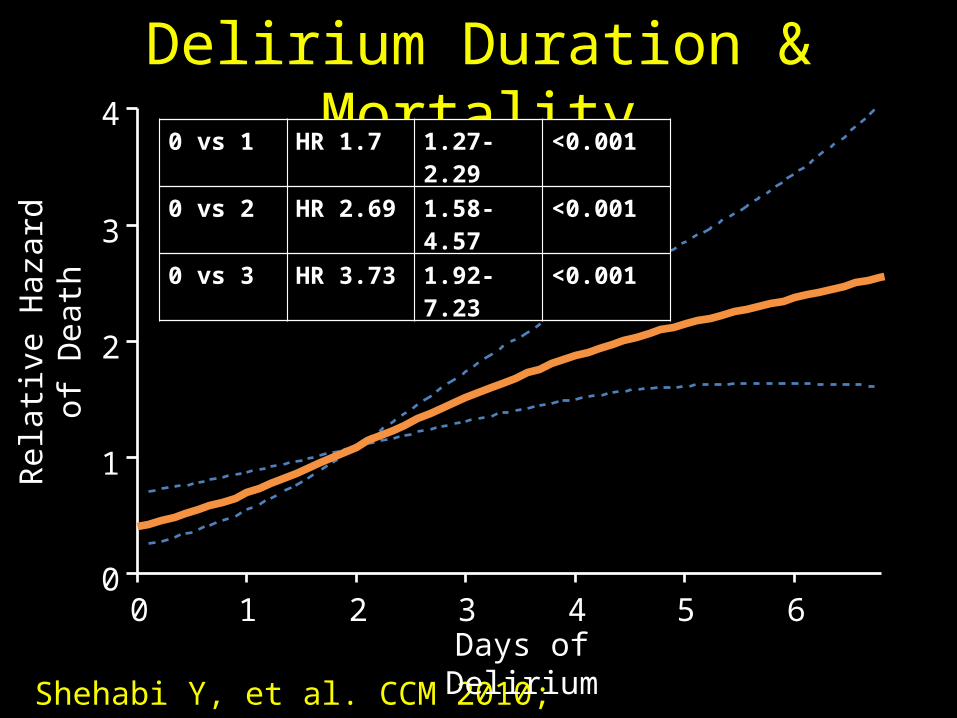
Shehabi Y, et al. CCM 2010; 38:2311–2318
Delirium Duration & MortalityRe
lativ
e H
azar
d of
D
eath
0 1 2 3 4 5 60
1
2
3
4
p<.001
Days of Delirium
0 vs 1 HR 1.7 1.27-2.29 <0.001
0 vs 2 HR 2.69 1.58-4.57 <0.001
0 vs 3 HR 3.73 1.92-7.23 <0.001
NEJM 2013;369:1306-16Editorial by M. Herridge
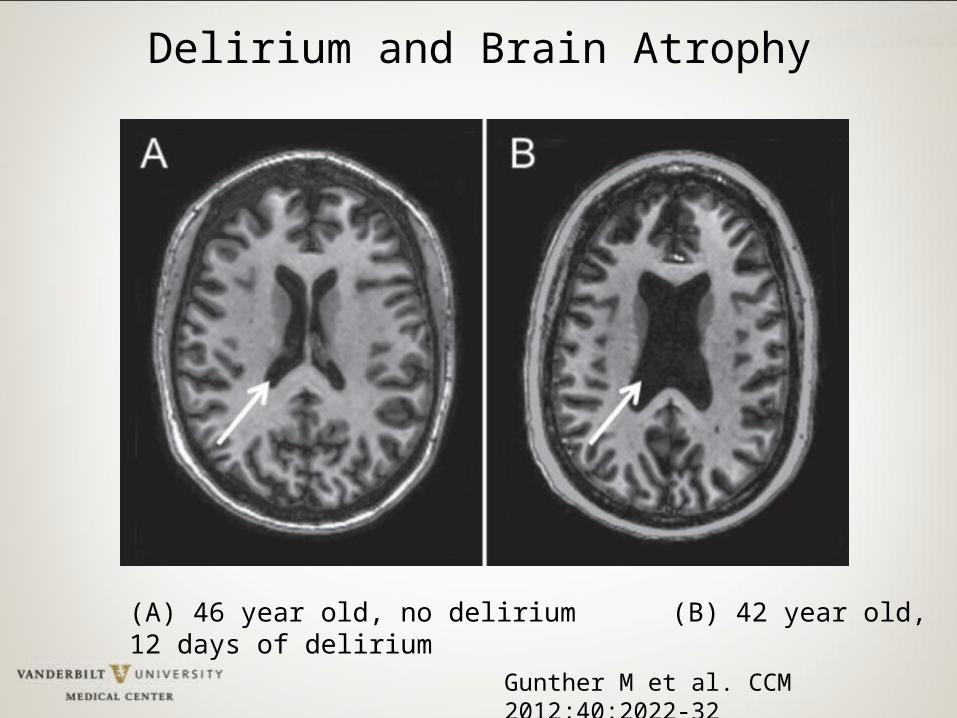
Gunther M et al. CCM 2012;40:2022-32
(A) 46 year old, no delirium (B) 42 year old, 12 days of delirium
Delirium and Brain Atrophy
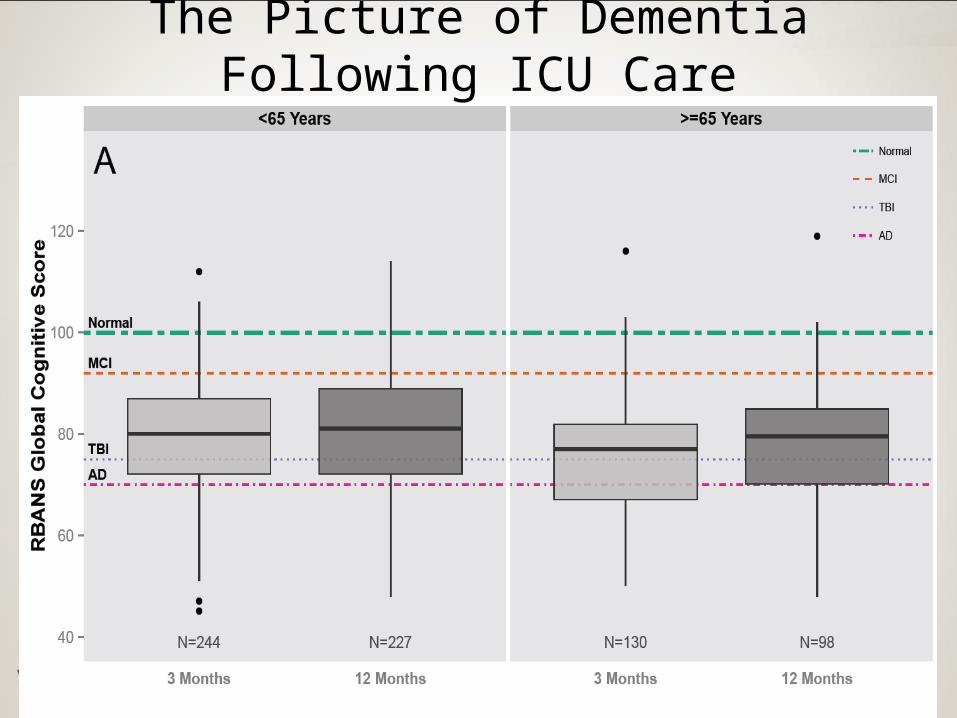
The Picture of Dementia Following ICU Care
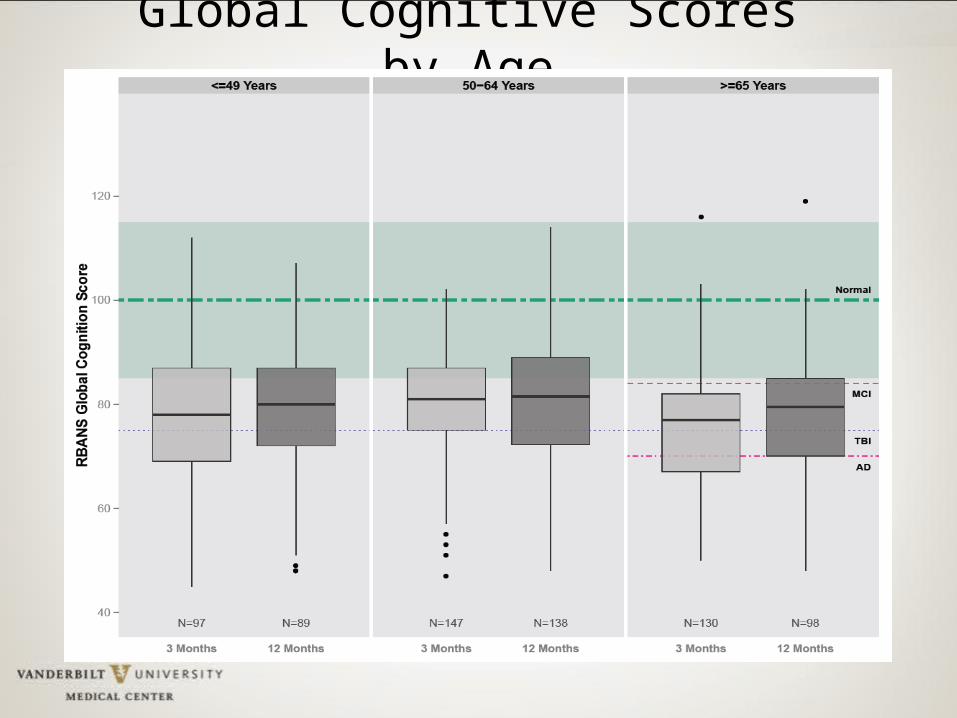
Global Cognitive Scores by Age
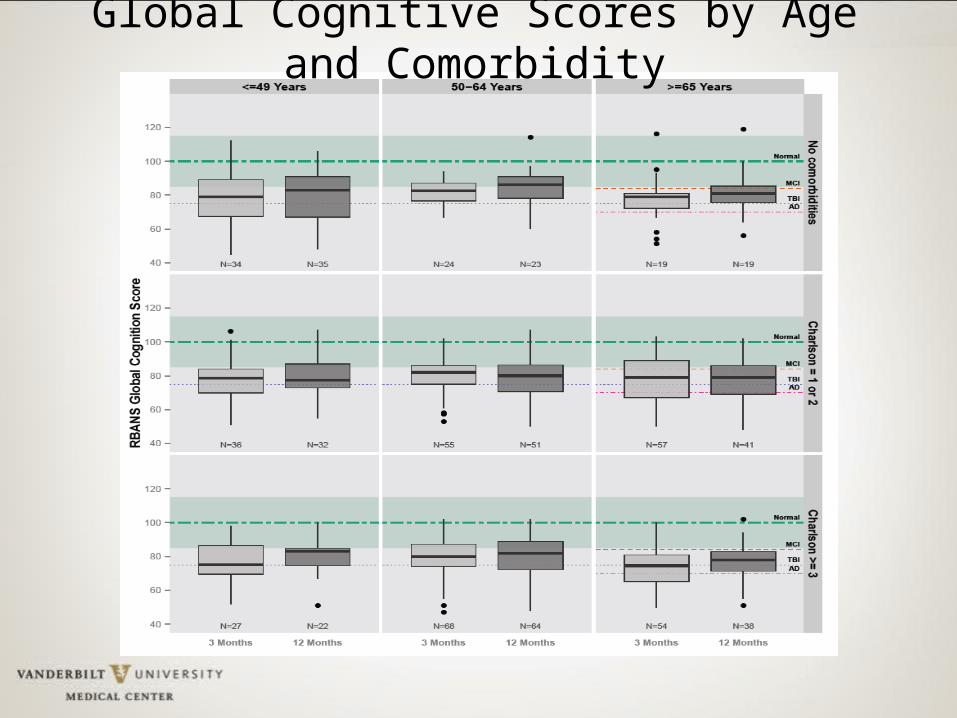
Global Cognitive Scores by Age and Comorbidity
Primum non Nocere - Hippocratic Oath- First do no harm
“Nothing to Fear but Fear Itself” - FDR inauguration, 1933- Overcome Fear of ICU Culture Change
So let’s focus on potentially modifiable aspects of care such as potent medications, delirium, and
improving care and clinical outcomes…
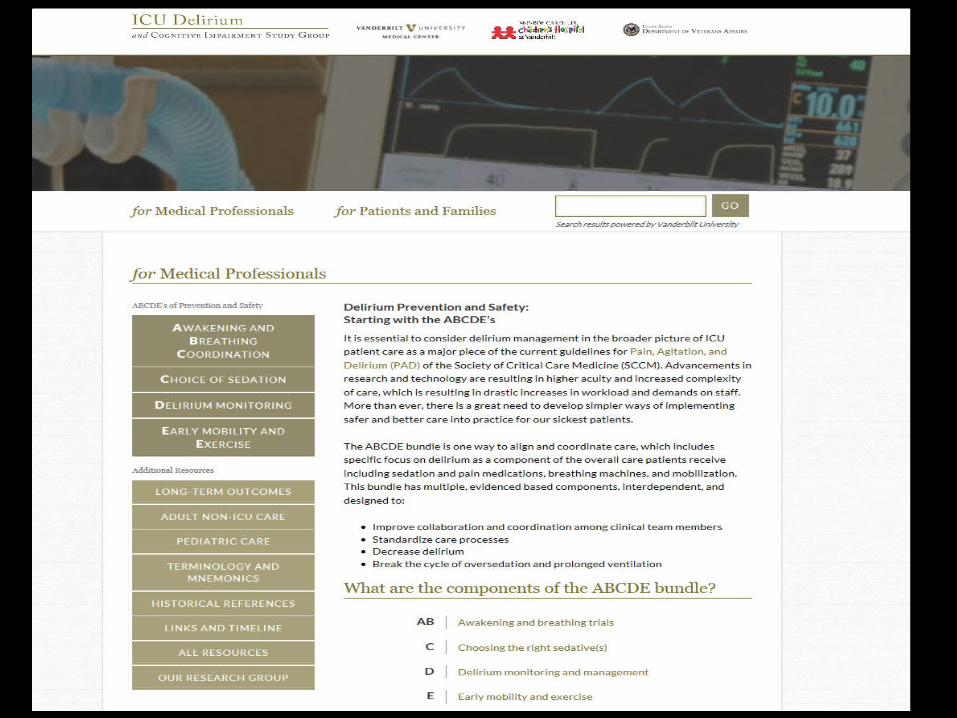
EDCBA
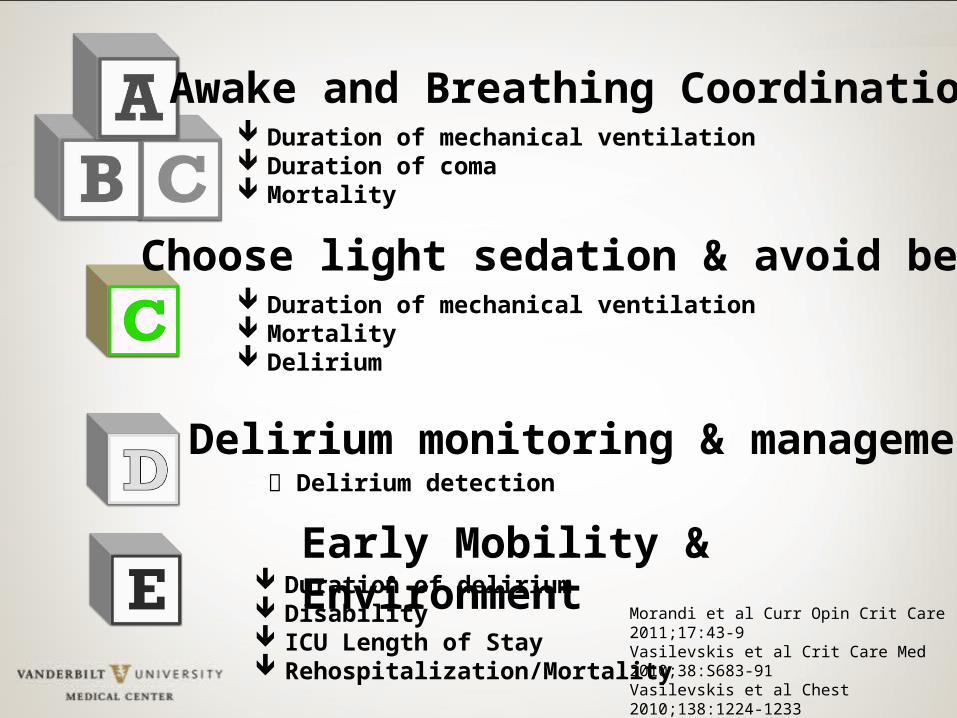
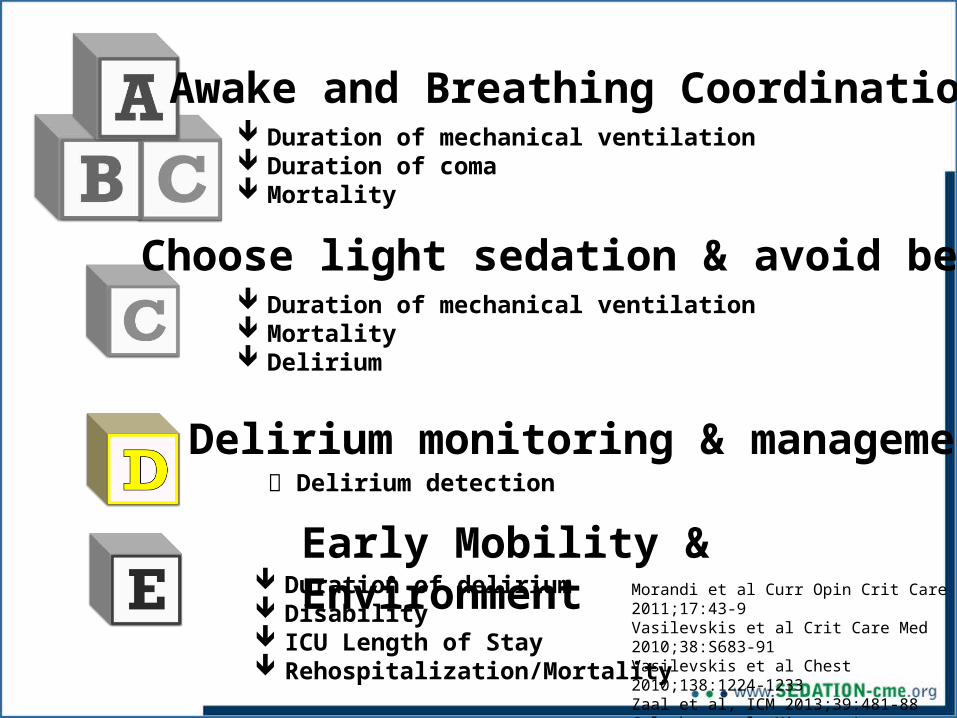
ABCDEs:Building blocks of managing
Pain, Agitation & Delirium
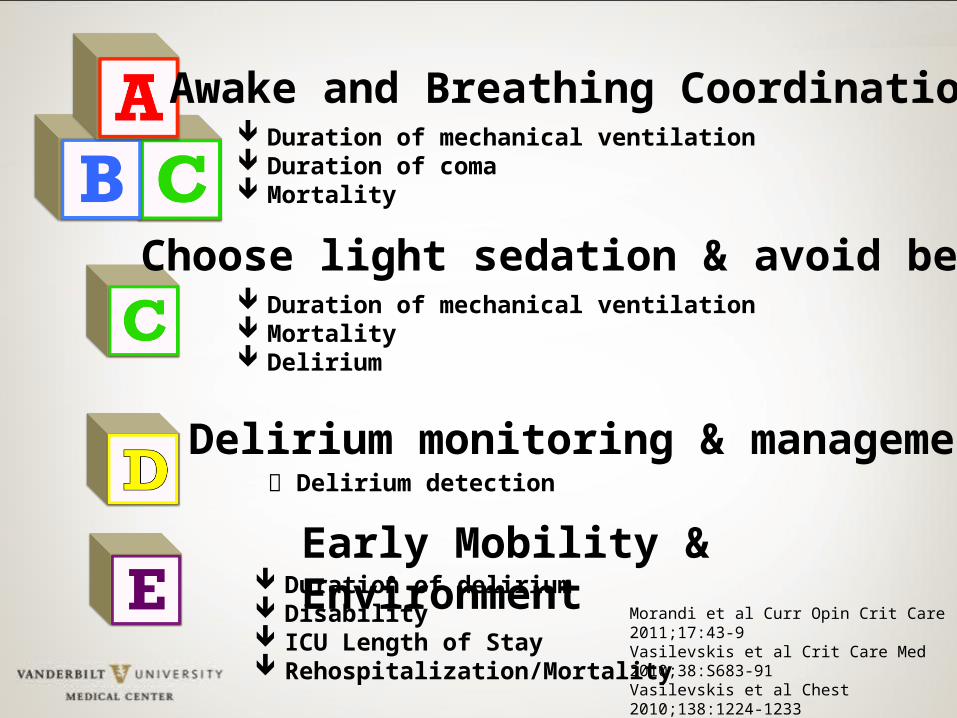
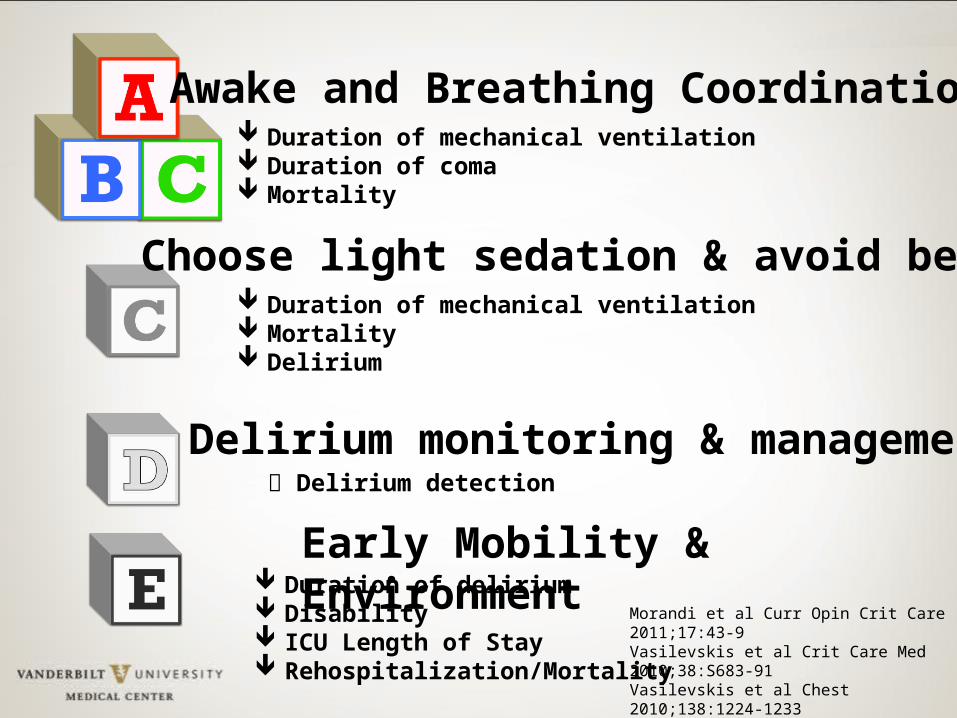
Awake and Breathing Coordination
Choose light sedation & avoid benzos
Delirium monitoring & management
Early Mobility & Environment
Duration of mechanical ventilation Duration of coma Mortality
Duration of mechanical ventilation Mortality Delirium
Duration of delirium Disability ICU Length of Stay Rehospitalization/Mortality
Morandi et al Curr Opin Crit Care 2011;17:43-9Vasilevskis et al Crit Care Med 2010;38:S683-91Vasilevskis et al Chest 2010;138:1224-1233Zaal et al, ICM 2013;39:481-88Colombo et al, Minerva Anest 1012;78:1026-33
Delirium detection
Pain, Agitation, and Delirium Are Interrelated
Barr J, et al. Crit Care Med. 2013;41:263-306.
AgitationPai
n
Delirium
“Pain should be routinely monitored in all adult ICU patients”
Grade 1B Recommendation
2013 PAD Guidelines:
Crit Care Med. 2013;41:263-308
Pain, Agitation, and Delirium Are Interrelated
Barr J, et al. Crit Care Med. 2013;41:263-306.
AgitationPai
n
Delirium
Targeted Level of Consciousness
Choose Target RASS
Assess Actual RASS
Modify treatment so Actual = Target
“We recommend either daily sedation interruption or a light level of target
sedation be routinely used…”Grade 1B Recommendation
2013 PAD Guidelines:
Crit Care Med. 2013;41:263-308
“We recommend that sedative medications be titrated to maintain a light* rather than
deep level of sedation”
Grade 1B Recommendation
2013 PAD Guidelines:
Crit Care Med. 2013;41:263-308
*Light sedation = RASS 0 to -2
Awake and Breathing Coordination
Choose light sedation & avoid benzos
Delirium monitoring & management
Early Mobility & Environment
Duration of mechanical ventilation Duration of coma Mortality
Duration of mechanical ventilation Mortality Delirium
Duration of delirium Disability ICU Length of Stay Rehospitalization/Mortality
Morandi et al Curr Opin Crit Care 2011;17:43-9Vasilevskis et al Crit Care Med 2010;38:S683-91Vasilevskis et al Chest 2010;138:1224-1233Zaal et al, ICM 2013;39:481-88Colombo et al, Minerva Anest 1012;78:1026-33
Delirium detection
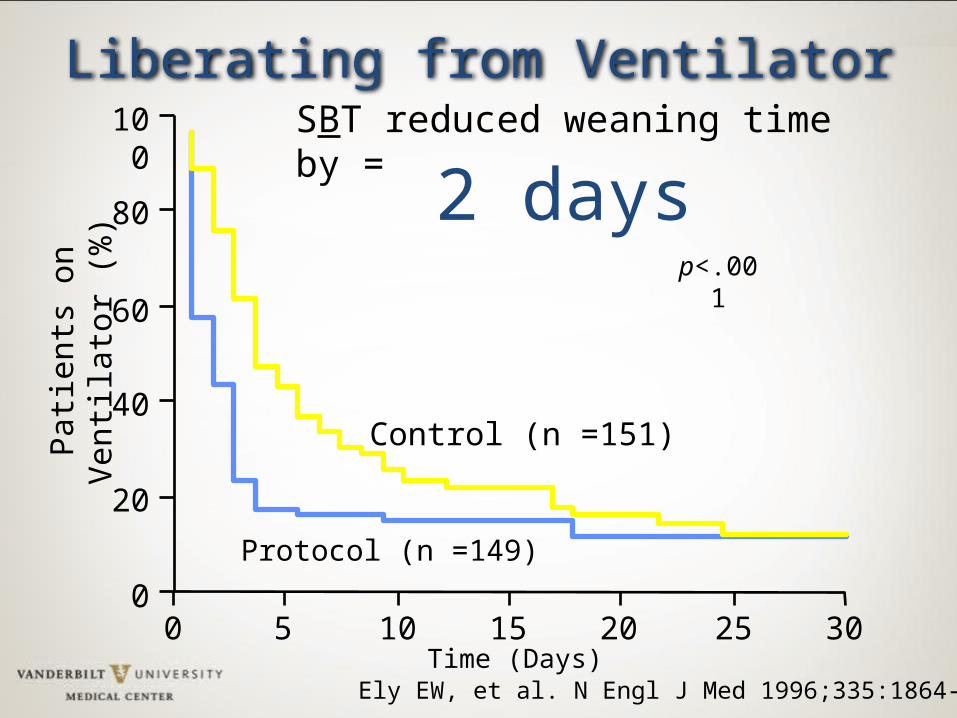
Ely EW, et al. N Engl J Med 1996;335:1864-9
0
20
40
60
80
100
Pat
ient
s on
Ven
tilat
or (
%)
0 302010 155 25
Control (n =151)
Protocol (n =149)
p<.001
Time (Days)
Liberating from VentilatorSBT reduced weaning time by =
2 days
0
20
40
60
80
100
Pat
ient
s on
Ven
tilat
or (
%)
0 302010 155 25
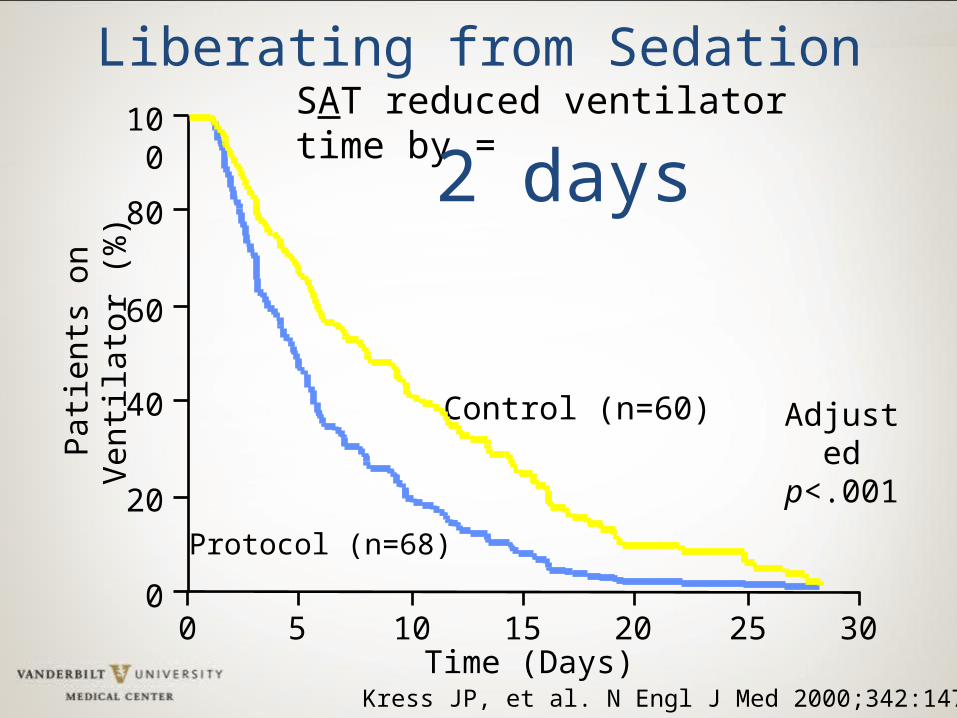
Control (n=60)
Protocol (n=68)
Adjusted p<.001
Time (Days)
Liberating from Sedation
Kress JP, et al. N Engl J Med 2000;342:1471-7
SAT reduced ventilator time by =
2 days
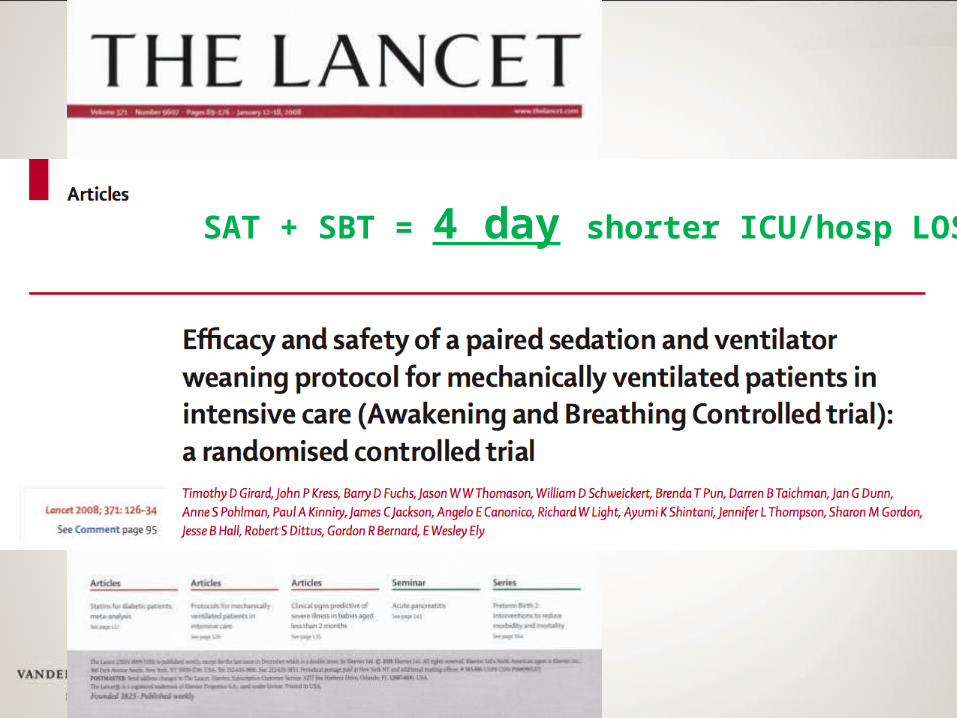
SAT + SBT = 4 day shorter ICU/hosp LOS
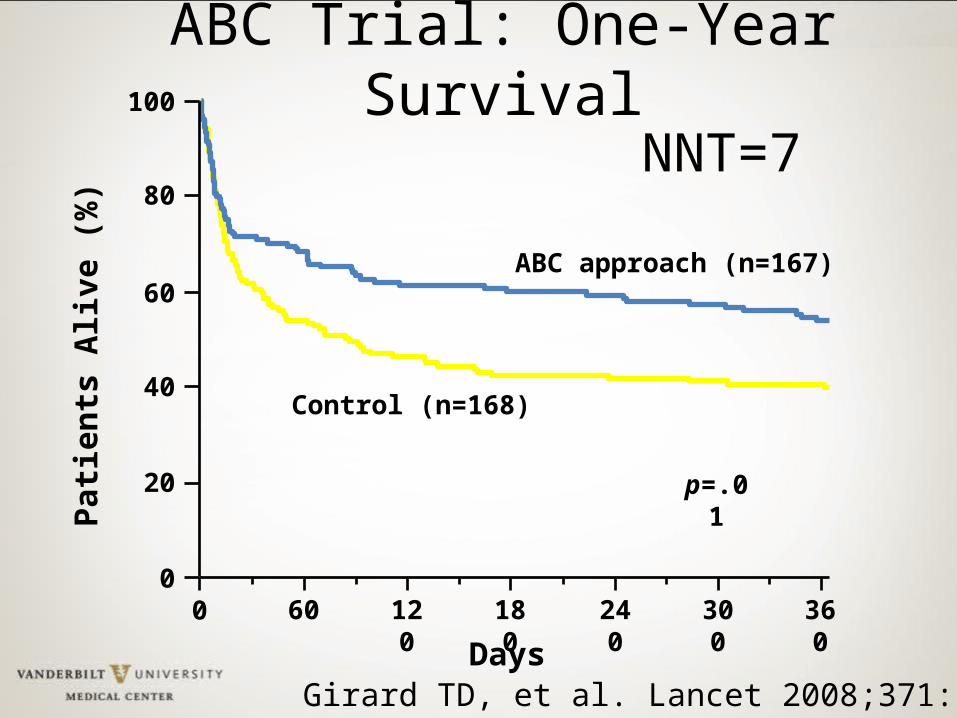
Patie
nts
Aliv
e (%
)
00
20
40
60
80
100
60 120 180 240 300 360
Days
Control (n=168)
ABC approach (n=167)
ABC Trial: One-Year Survival
p=.01
NNT=7
Girard TD, et al. Lancet 2008;371:126-34
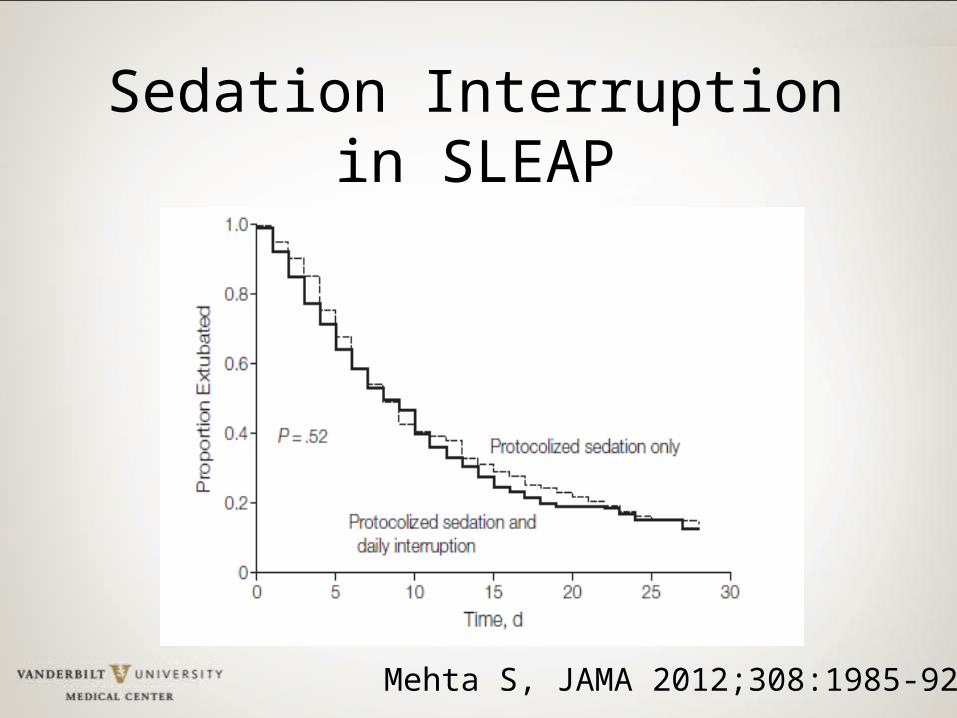
Mehta S, JAMA 2012;308:1985-92
Sedation Interruption in SLEAP
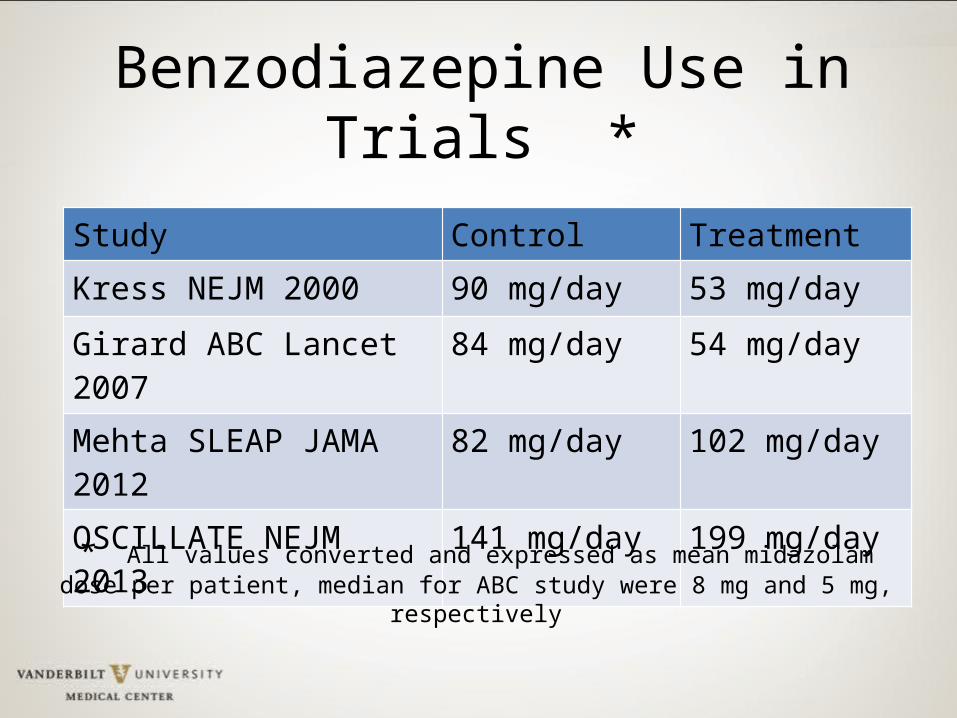
Benzodiazepine Use in Trials *
Study Control TreatmentKress NEJM 2000 90 mg/day 53 mg/day
Girard ABC Lancet 2007 84 mg/day 54 mg/day
Mehta SLEAP JAMA 2012 82 mg/day 102 mg/day
OSCILLATE NEJM 2013 141 mg/day 199 mg/day
* All values converted and expressed as mean midazolam dose per patient, median for ABC study were 8 mg and 5 mg, respectively
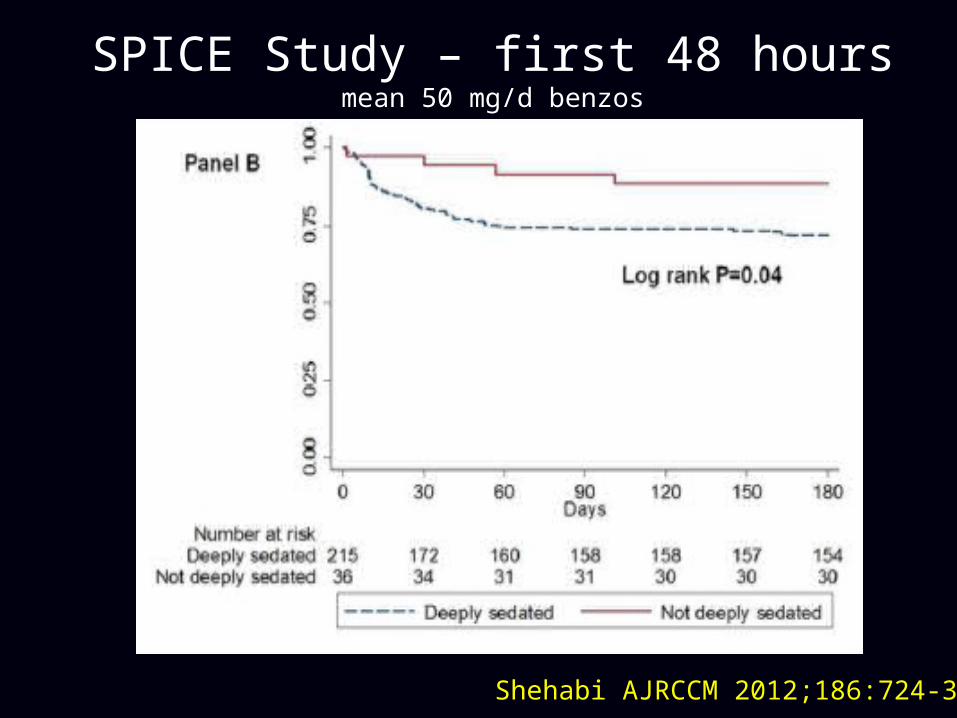
SPICE Study – first 48 hoursmean 50 mg/d benzos
Shehabi AJRCCM 2012;186:724-31
Awake and Breathing Coordination
Choose light sedation & avoid benzos
Delirium monitoring & management
Early Mobility & Environment
Duration of mechanical ventilation Duration of coma Mortality
Duration of mechanical ventilation Mortality Delirium
Duration of delirium Disability ICU Length of Stay Rehospitalization/Mortality
Morandi et al Curr Opin Crit Care 2011;17:43-9Vasilevskis et al Crit Care Med 2010;38:S683-91Vasilevskis et al Chest 2010;138:1224-1233Zaal et al, ICM 2013;39:481-88Colombo et al, Minerva Anest 1012;78:1026-33
Delirium detection
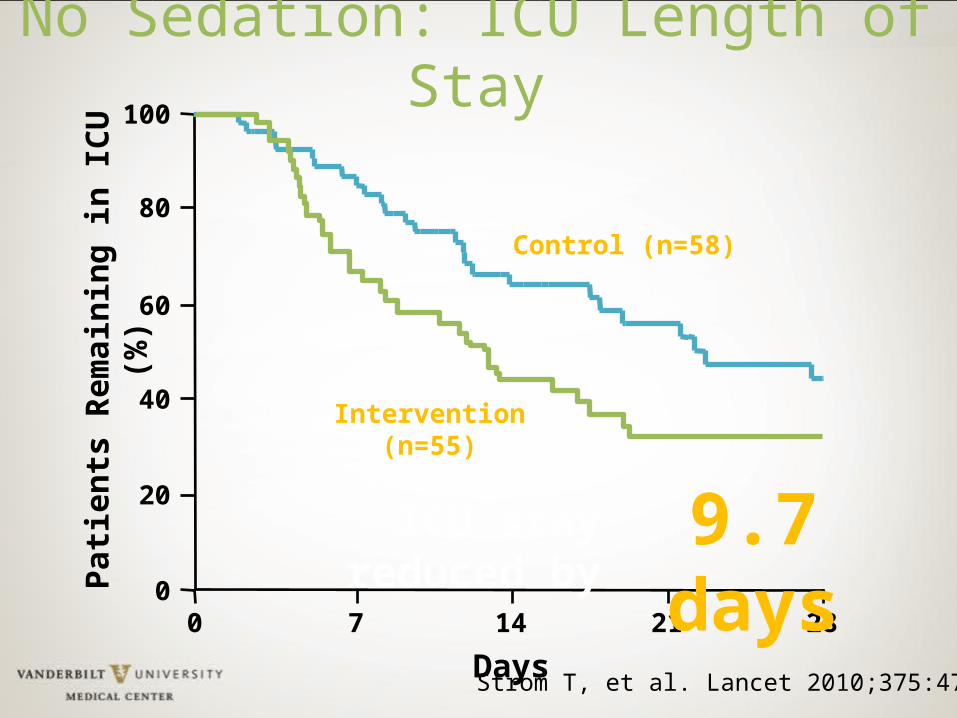
No Sedation: ICU Length of Stay
0
Days7
0
20
40
60
80
100Pa
tient
s Re
mai
ning
in IC
U (%
)
14 21 28
Intervention (n=55)
Control (n=58)
Strom T, et al. Lancet 2010;375:475-80
ICU stay reduced by 9.7 days
“We suggest that sedation strategies using non-benzodiazepines (propofol or
dexmedetomidine) may be preferred over sedation with benzodiazepines (midazolam
or lorazepam)”
Grade 2B Recommendation
2013 PAD Guidelines:
Crit Care Med. 2013;41:263-308
Pain, Agitation, and Delirium Are Interrelated
Barr J, et al. Crit Care Med. 2013;41:263-306.
AgitationPai
n
Delirium
Awake and Breathing Coordination
Choose light sedation & avoid benzos
Delirium monitoring & management
Early Mobility & Environment
Duration of mechanical ventilation Duration of coma Mortality
Duration of mechanical ventilation Mortality Delirium
Duration of delirium Disability ICU Length of Stay Rehospitalization/Mortality
Morandi et al Curr Opin Crit Care 2011;17:43-9Vasilevskis et al Crit Care Med 2010;38:S683-91Vasilevskis et al Chest 2010;138:1224-1233Zaal et al, ICM 2013;39:481-88Colombo et al, Minerva Anest 1012;78:1026-33
Delirium detection
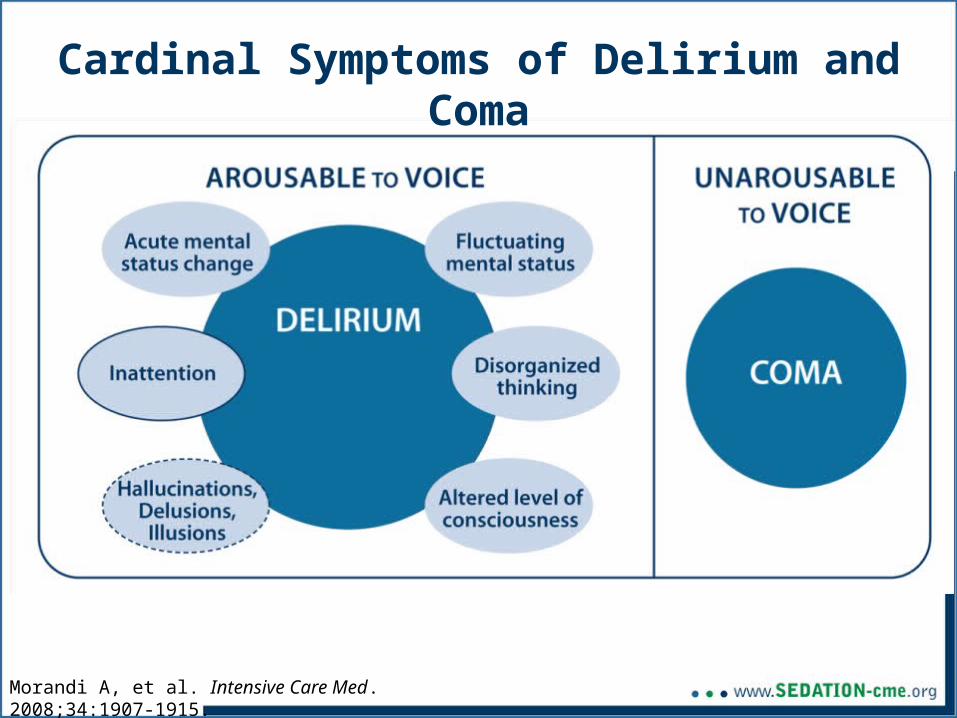
Cardinal Symptoms of Delirium and Coma
Morandi A, et al. Intensive Care Med. 2008;34:1907-1915.
“We recommend routine monitoring for delirium in adult ICU patients”
Grade 1B Recommendation
2013 PAD Guidelines:
Crit Care Med. 2013;41:263-308
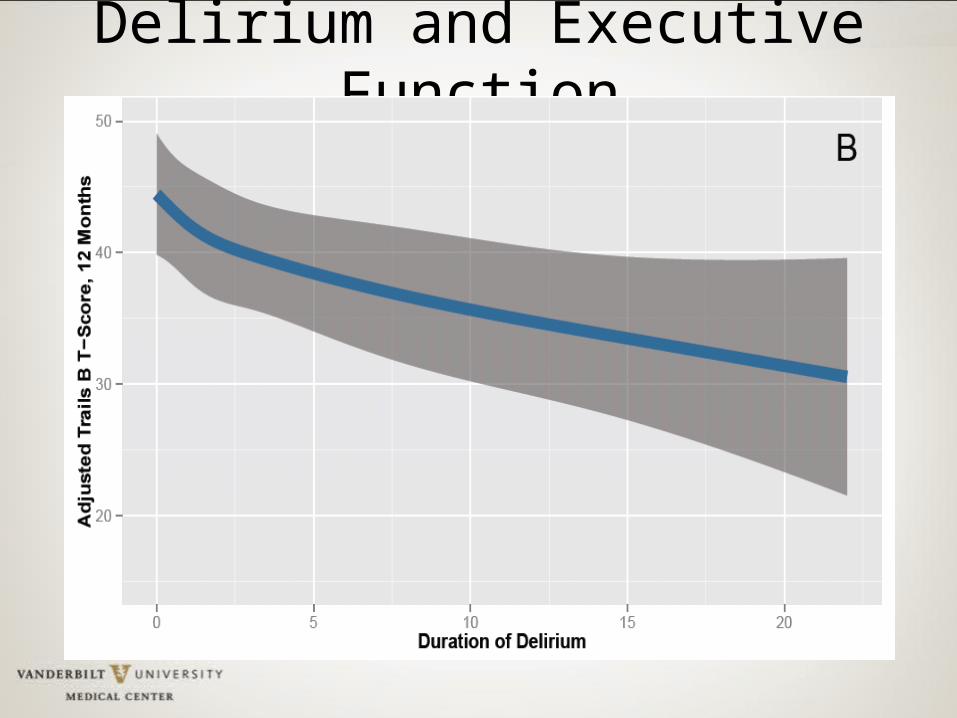
Delirium and Executive Function
If delirium is not screened for using a validated delirium screening tool it is missed ~75% of time.
Inouye SK Arch Intern Med. 2001;161:2467-2473.Devlin JW Crit Care Med. 2007;35:2721-2724.Spronk PE Intensive Care Med. 2009;35:1276-1280.van Eijk MM Crit Care Med. 2009;37:1881-1885.
Ely EW, JAMA 2001;286:2703-10
Ely EW, JAMA 2003;289:2983-91

Medical Intensive Care Unit
Don’t forget about Dr. DRE
Diseases Sepsis, COPD, CHF
Drug Removal SATs and stopping benzodiazepines/ narcotics
Environment Immobilization, sleep and day/night, hearing aids, glasses, noise
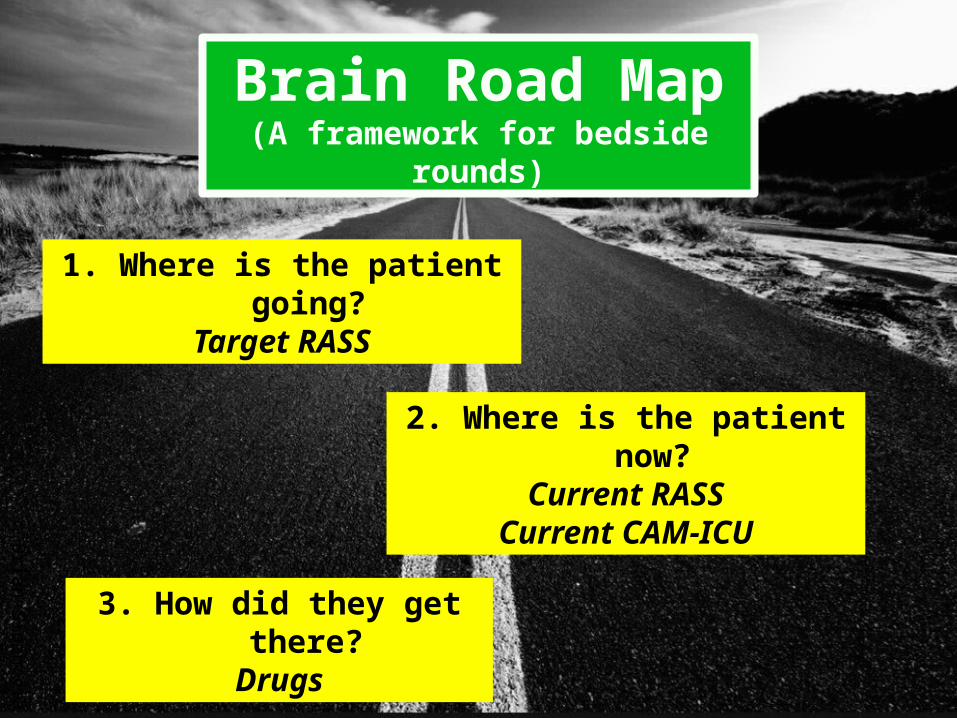
Brain Road Map(A framework for bedside rounds)
3. How did they get there?Drugs
1. Where is the patient going?Target RASS
2. Where is the patient now?Current RASS
Current CAM-ICU© B
rian Slo
an via F
lickr
ExcellenceAristotle: “We are what we repeatedly do.
Excellence is not an act, but a habit”
Jiro Dreams of Sushi - Tokyo
EDCBA
ABCDEs:Building blocks of managing
Pain, Agitation & Delirium
“ I survived and that is the main thing. And I am so grateful to God that I survived and am now off all oxygen and consider myself all well except that I can’t remember to take my medications...
-SB
“©
Ca
pp
i Th
om
pso
n via
Flick
r
The ICU Delirium and Cognitive Impairment Study Group at the Loveless Café, Nashville TN
ICU Delirium and Cognitive Impairment Study Group: selected local members
Pratik PandharipandeJim JacksonJin HanEd VasilevskisChris HughesAlessandro MorandiPaula WatsonLorraine WareGordon BernardBob DittusTed SperoffWes Ely
Leanne BoehmJoyce OkahashiCayce StrengthBrenda PunLauren HardyAmy LipseyRyan BlackJessica McCurleyMichael SantoroCarrie JonesMorgan CrawfordMayur Patel
Tim GirardJohn GoreBaxter RogersStephan HeckersCathy FuchsHeidi SmithTy BeruttiBrad StrohlerElizabeth CardJennifer ThompsonAyumi ShintaniStephanie Hamilton
Key Epidemiological Points:1) Patients suffer from long-lasting and disabling aspects of critical
illness that demand our attention as a medical community2) Acquired or accelerated cognitive impairment is a major public
health problem following ICU care for both the old and young3) This cognitive impairment appears most pronounced in domains
of executive dysfunction and memory4) Frontal lobe and hippocampal atrophy are being consistently
found in recent studies5) This injury is likely distinct from or complementary to
Alzheimer’s pathology, though we are in our infancy in learning about this entity (e.g., large pathology study under review)
6) Delirium and drug exposure appear to be the most modifiable aspects of care, with need for more trials to delineate next steps
Key Management Points:1) Establish an overarching protocolized approach to daily ICU
patient management using 2013 PAD Guidelines2) Assess & treat pain first (may be sufficient)3) If patient remains agitated after adequately treating pain, use
prn/bolus sedation initially, if frequent boluses (>3/hr) use continuous sedation
4) Avoid benzodiazepines in most patients5) Turn off sedation daily and restart only if needed at lowest dose
to maintain chosen target level of consciousness6) Deep sedation (RASS -4/-5) appears harmful; target awake/alert7) Screen for delirium (CAM-ICU or ICDSC); If delirious, first seek
reversible causes and attempt non-pharmacologic management8) Use the ABCDEs to improve outcomes for your patients
CUSP4MVP-VAP project measures
• As part of this project, teams will collect and receive reports for metrics to support your improvement efforts.
• We held calls with your data facilitator. The data collection tool, including instructions are available at:
https://armstrongresearch.hopkinsmedicine.org/cusp4mvp/datatools.aspx
Medical Intensive Care Unit
CUSP4MVP Data CollectionSedation and Delirium
1) Percentage of RASS/SAS actual being {-1, 0, 1} or {4, 5}
2) Percentage of achieving RASS/SAS target3) Distribution of RASS/SAS actual scores4) Delirium assessment compliance rate5) Percentage of incorrectly reporting CAM-ICU/
ASE UTA (higher is worse)6) Percentage of CAM-ICU negative or ASE <=2
(no delirium)Medical Intensive Care Unit
CUSP4MVP Data CollectionSAT/SBT (next call on March 18)
(1) SAT compliance rate(2) SBT compliance rate(3) SAT contraindication rate(4) SBT contraindication rate
(5) Percentage of ventilated patient days without sedation(6) SBT with Seds off compliance rate
(7) SAT contraindication distribution plot and table (counts and percentages)
(8) SBT contraindication distribution plot and table (counts and percentages)
Medical Intensive Care Unit
Your Next Steps:
• Share your protocols regarding sedation and delirium management; will share with other participating teams• Email to [email protected]
• Review data collection requirements and develop plan to collect and submit data.
Medical Intensive Care Unit
Reminder:
By Content Call, Module 5 (April 1, 2014):1. Watch the Science of Safety (SOS) Video
– http://www.ahrq.gov/professionals/education/curriculum-tools/cusptoolkit/videos/04a_scisafety/index.html
2. Develop a method to deliver the SOS Video to your entire unit’s staff
3. Administer the SSA and submit aggregated results to CE
4. Facilitate at least one team meeting
Next Call
March 18, 2014
SAT / SBTDr Mike Klompas







