
Documentation Strategies for Nurses and Therapists
January 2, 2007 at 1:00 EST
Lisa Bazemore, MBA, MS, CCC-SLP

Setting the Stage
• Why do we document care? To insure payment for the services rendered To insure continuity of care
• Principles of documentation: Document to your audience Focus on deficits Attainable goals Progress towards goals Consider barriers to discharge Consider return to both home and community

Setting the Stage
• What is Medical Necessity? A course of treatment that is seen as most helpful for the
specific health symptoms that the patient is experiencing. This course of treatment is determined by the patient and their healthcare team.

Setting the Stage
• 7 Criteria of Medical Necessity
1. Medical Supervision2. 24 Hour Rehab Nursing3. Relatively Intense Level of Services4. Multidisciplinary Approach5. Coordinated Care Plan6. Significant Practical Improvement7. Realistic Goals

Components of Medical Necessity
• Close Medical Supervision
24 hour availability of a physician Entries in the chart every 2 -3 days minimum Greater involvement that in other settings
Components of Medical Necessity
• 24 Hour Rehabilitation Nursing
Need availability of an RN with rehab experience around the clock Have clear, functional rehabilitation goals Nursing is involved in the overall plan of care, not just medical issues
and bowel and bladder management Nursing documentation supports FIM scores Nursing documentation clearly identifies how they facilitate the
carryover of learning from therapy sessions Nursing documentation supports the medical management of the
patient

Components of Medical Necessity
• Relatively Intense Level of Rehabilitation Services The 3 Hour Rule Minimum of 3 hours of therapy, 5 days per week Therapy is at a skilled level Must be necessary for meeting the basic needs of the patient’s health Must be consistent in type, frequency, and duration Consistent with the patient’s diagnosis

Components of Medical Necessity
• Interdisciplinary Approach Members work collaboratively to develop goals and the treatment
plan Team members engage and learn from each other Collaborative ownership of the patient treatment plan

Components of Medical Necessity
• Coordinated Plan of Care Records need to show a treatment plan that is:
• Derived from team assessment and patient expectations• Identifies STG’s and LTG’s• Defines how disciplines share responsibility• Supports need for intensive rehab services• Weekly team conference

Components of Medical Necessity
• Significant Practical Improvement We do not expect 100% independence for all rehab patients We do expect reasonable, practical improvement Improvement must be the result of skilled services provided Important that it is documented clearly
Components of Medical Necessity
• Realistic Goals Aim of treatment needs to be achieving the maximum level of
function possible
How Do We Document Medical Necessity?
• Team has an ongoing opportunity to document medical necessity. This is achieved by documenting:
That services needed are of a complex nature that they require a licensed clinician
Services need to be in an inpatient setting Services are consistent with diagnosis, need, and medical condition Services are consistent with the treatment plan Services are reasonable and necessary Patient is making progress towards reasonable goals

Where Do We Document Medical Necessity?
• Pre-admission Screening• Team Admission Assessments• Nursing Admission Assessments• Patient Care Plan
Long term goals Short term goals Identification of involved disciplines Weekly progress notes Discharge summaries
• Team Conference Summaries

Preadmission Screening
• Diagnoses• Comorbidities• Age• Current interventions• Functional Assessment• Vitals• Safety• History• Meds
• Pre-morbid status/function• Recommendation of need for
3 therapies• Recommendation of need for
2 disciplines• Rehab potential• Areas where improvement is
expected

Preadmission Screening
Example
Pre-morbid function: Pt. lives w/wife. Independent with ADLs, shopping, financial management, and recreation activities prior to onset of stroke.
Rehabilitation potential: Pt. has good potential for rehabilitation. He has shown some return of function, has good family support, and has a desire to get back to life as it was before his stroke.
Team Admission Assessment
• Prior level of function• Required assistance• Living situation• Anticipated D/C plans• Patients rehab expectation• Individual FIM’s with
emphasis on findings
• ROM and Strength limits• Sensation, tone, etc.• Community reintegration• Pain assessments• Summaries of findings

Poor Team Admission Example
EatingDate: 4/3 Initials: MSM FIM 5
Date: Initials: FIM
Meal assessed: (B) L D Current diet: soft Intake mode: oral Food texture: soft
Thickened liquids No Thickness: Dentures edentulous Finishes meal timely
Able to open packages Able to scoop Able to take food to mouth Able to cut
Noted: Coughing Choking Neglect
Swallowing precautions:
Bedside swallow results: (Y) Swallow study results: Y Positioning needs:
Adaptive Equipment Needs: Safety Needs Identified:
Findings:Pt without dentures See bedside swallow eval

Why This Is Poor
• No indication that skilled intervention is needed• All items were not assessed• No safety needs identified• Findings do not provide justification for skilled therapy• No indication of why FIM was 5• No indication that intervention was needed on an inpatient basis• No indication that an interdisciplinary team is needed
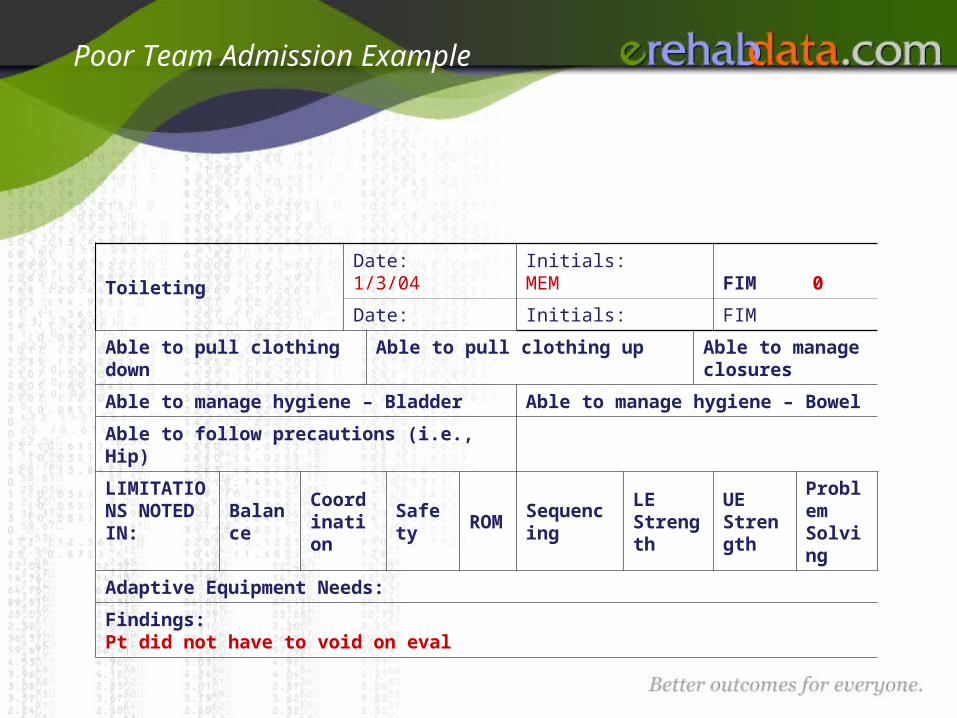
Poor Team Admission Example
ToiletingDate: 1/3/04 Initials: MEM FIM 0
Date: Initials: FIM
Able to pull clothing down Able to pull clothing up Able to manage closures
Able to manage hygiene – Bladder Able to manage hygiene – Bowel
Able to follow precautions (i.e., Hip)
LIMITATIONS NOTED IN:
BalanceCoordination
Safety ROM SequencingLE Strength
UE Strength
Problem Solving
Adaptive Equipment Needs:
Findings:Pt did not have to void on eval

Why This Is Poor
• Toileting was not assessed – this is an important area for assessment to establish the medical necessity for OT

Poor Team Admission Example
Summary Of Findings:
Overall clinical impression/rehab potential (qualified)
SW Initials: ___ Supportive family, will need supervision at home post rehab
SLPInitials: ____ Recommend speech tx with focus on cog-ling tasks. Fair rehab potential to return
home with supervision.
OTInitials: ____ Pt to benefit from OT 5-6x/week for ADLs, transfers, strength/endurance to return
home with family with supervision as appropriate
PT Initials: ____ Good to return home alone after rehab with support services as needed.
Nursing Initials: ____

Why This Is Poor
• SW does not indicate need for skilled social services• SLP does not link need for therapy w/return home potential• PT does not show need for skilled therapy services• No indication that 24 hour setting for intervention is needed

Improved Example of Team Assessment
EatingDate: 4/3 Initials: MSM FIM 4
Date: 4/4 Initials: LF FIM 4
Meal assessed: (B) L D Current diet: soft Intake mode: oral Food texture: soft
Thickened liquids No Thickness: Dentures yes Finishes meal timely N
Able to open packages Setup Able to scoop Ind Able to take food to mouth I Able to cut Mod A
Noted: Coughing Choking Neglect
Swallowing precautions: Pt needs to take small bites; after all meals & snacks, staff needs to check for pocketing of food
Bedside swallow results: ( Y) Swallow study results: Y Positioning needs:
Adaptive Equipment Needs: Safety Needs Identified:
Findings: Bedside swallow exam attached. Requires ST is to teach patient safe swallowing techniques to risks of aspiration & to upgrade diet . MEM Requires to OT to teach scanning & compensatory techniques for eating. LF

Why This Is Improved
• Need for interdisciplinary team clearly identified• FIM score supported• Indication that intervention is needed across the day• Supports need for skilled OT and ST

Improved Example of Team Assessment
ToiletingDate: 1/3/04 Initials: MEM FIM 4
Date: 1/3/04 Initials: LP FIM 4
Able to pull clothing down Mod A Able to pull clothing up Mod A Able to manage closures Setup
Able to manage hygiene – Bladder Independent Able to manage hygiene – Bowel – Mod A
Able to follow precautions (i.e., Hip) Supervision
LIMITATIONS NOTED IN:
Balance Coordination Safety ROM Sequencing LE Strength UE StrengthProblem Solving
Adaptive Equipment Needs: Grab bars at toilet Raised toilet
Findings: Morbid obesity impairs toileting. Requires OT for neuro reed to relearn safe toileting. MEM Requires PT training to balance, coordination, and LE strength. LP

Why This Is Improved
• Supports impact of morbid obesity (comorbidity on treatment)
• Supports need for interdisciplinary team• Supports need for skilled OT and PT
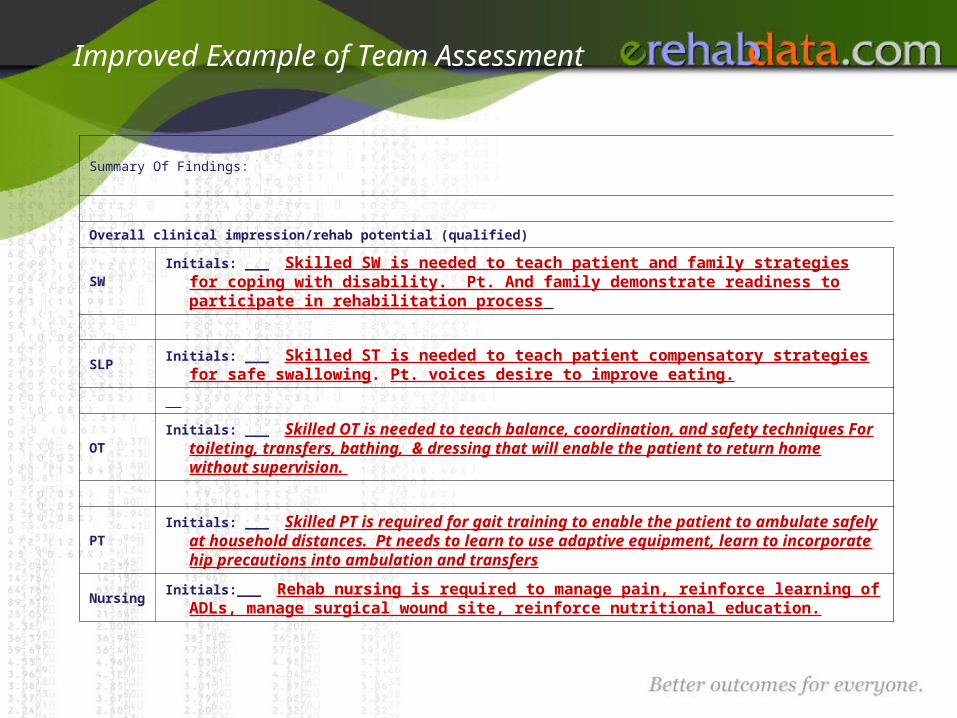
Improved Example of Team Assessment
Summary Of Findings:
Overall clinical impression/rehab potential (qualified)
SWInitials: ___ Skilled SW is needed to teach patient and family strategies for coping
with disability. Pt. And family demonstrate readiness to participate in rehabilitation process
SLPInitials: ___ Skilled ST is needed to teach patient compensatory strategies for safe
swallowing. Pt. voices desire to improve eating.
OTInitials: ___ Skilled OT is needed to teach balance, coordination, and safety
techniques For toileting, transfers, bathing, & dressing that will enable the patient to return home without supervision.
PTInitials: ___ Skilled PT is required for gait training to enable the patient to ambulate
safely at household distances. Pt needs to learn to use adaptive equipment, learn to incorporate hip precautions into ambulation and transfers
NursingInitials:___ Rehab nursing is required to manage pain, reinforce learning of ADLs,
manage surgical wound site, reinforce nutritional education.

Why This Is Improved
• All disciplines document need for skilled level of intervention• Supports need for interdisciplinary intervention• OT’s identification of the need for toileting and bathing indicate the
need for equipment that is not usually in OP clinics for patient training (bathtubs, commodes)
• Rehab nursing clearly documents their role in the POC.

Documenting on the Patient Care Plan
• The Patient Care Plan should include: Prioritized patient goals Impairments, Activity, Participation Planned Discharge Site Interdisciplinary Long Term Goals What disciplines will be involved in the care of the patient Interventions

IAP Example
Admission Discharge
Impairments
Osteoarthritis in knees, hips, back, R shoulder
Osteoarthritis in knees, hips, back, R shoulder
Activities
Impaired mobility, LB dressing, bathing & toileting
Improved to mod I in mobility, bathing & dressing w/adaptive equip.
Participation
Can’t shop for groceries, Afraid to cook, can’t perform job duties, can’t play golf
Able to shop for basic food items, can prepare simple meal, will return to work 2 weeks post d/c, return to golf 6 mo post d/c

Documenting Progress
• At least weekly, a summary of the patient’s progress should be documented.
Document progress toward goals Detail barriers to achievement of goals Describe changes to the plan of care as appropriate Describe patient’s response to treatment State the justification for continued stay on the rehab unit

Poor Documentation of Progress
Occupational Therapy Weekly D/C
Summary:
Pt mod A with bathing, UB & LB dressing; strength & endurance improved. Toileting @ Sup. 3 of 4 goals met. POC to co ntinue.
_____P.C. Perfect OTR_______3/15/04__________
Signature Date

Why This Is Poor
• Note does not reflect skilled intervention
• Note does not address the reasons that skilled services are needed – the teaching of hip precautions, the teaching of adaptive equipment usage
• Note does not document the need for continued skilled therapy
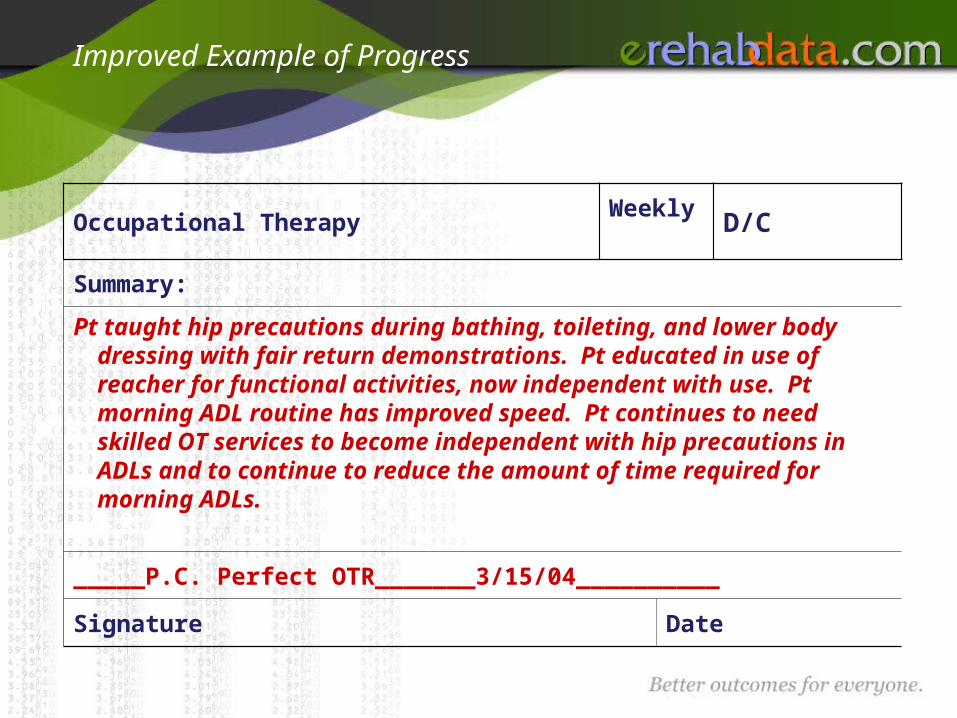
Improved Example of Progress
Occupational Therapy Weekly D/C
Summary:
Pt taught hip precautions during bathing, toileting, and lower body dressing with fair return demonstrations. Pt educated in use of reacher for functional activities, now independent with use. Pt morning ADL routine has improved speed. Pt continues to need skilled OT services to become independent with hip precautions in ADLs and to continue to reduce the amount of time required for morning ADLs.
_____P.C. Perfect OTR_______3/15/04__________
Signature Date
Why This Is Improved
• Details the skilled intervention provided by the therapist – i.e., “taught”, “educated”
• Addresses weekly short term functional goals
• Summarizes daily treatment interventions
• Documents need for continued skilled intervention
Daily Documentation of Medical Necessity
• Daily documentation should show skilled need in: Weekly short term goals Total units of therapy Treatment/training Daily comments

Poor Documentation of Goals
Weekly short-term goals: Met Not Met Cont.
1. Pt will be indep. in grooming.
2. Pt will dress UB & LB with supervision.
3. Pt will bath with min assist.
4. _______________________________________________
5. _______________________________________________

Why Is This Poor
• Typical pt. w/hip replacement would not need skilled therapy to relearn basic ADLs

Improved Example of Goals
Weekly short-term goals: Met Not Met Cont.
1. Pt will adhere to hip precautions in toileting and lower body dressing independently
2. Pt will use reacher in dressing and housekeeping tasks to maintain hip precautions independently
3. Pt will bathe lower body safely, maintaining balance and hip precautions at mod I.
4. Pt will complete morning ADL routine within 45 min at mod I
5. _______________________________________________

Why This Is Improved
• Details the need for OT in ADLS• Documents specific area requiring learning – it is not that
patient needs to relearn how to put on clothes, bathe, etc., but that patient needs to learn how to use his hip precautions in each of these basic life activities
• Puts ADLs into functional routine that has a meaningful measure to patient and family
What Constitutes a Skilled Service
• Knowledge and training of a professional is necessary• Need should be indicated in initial evaluation• Evidence that skilled services were performed should be
reflected in notes

What Constitutes a Skilled Service
• Services must be of such a level of complexity and sophistication or the condition of the patient must be such that the services required can only be safely and effectively performed by qualified nurses and therapists.
• Skilled services can be: Diagnostic and assessment Designing treatment Establishment of compensatory skills Providing patient instruction Reevaluations

Skilled versus Non-Skilled
Nonskilled Skilled
Observed patient trying to get out of bed. Pt unable to come to sitting without help.
Training provided to facilitate independence in bed mobility. Tactile and verbal cuing provided to produce knee flexion and arm extension and push.
Pt expression - 2 with nurses.
Pt. taught to use call light and respond “bathroom”. Pt able to perform sequence of pushing call light and responding to nurse 4/5.
Pt – UB Dressing 4
Pt. taught strategies for compensation of left visual neglect to facilitate independence in dressing. Min assist required for buttoning shirt.

Denials
• Why do payers tell us they deny claims? Patient does not meet eligibility criteria Services are not skilled Services are not necessary for patient’s diagnosis, medical condition,
or no assessed need

Denials
• How can we avoid denials? Document interventions clearly and precisely Use active, descriptive verbs
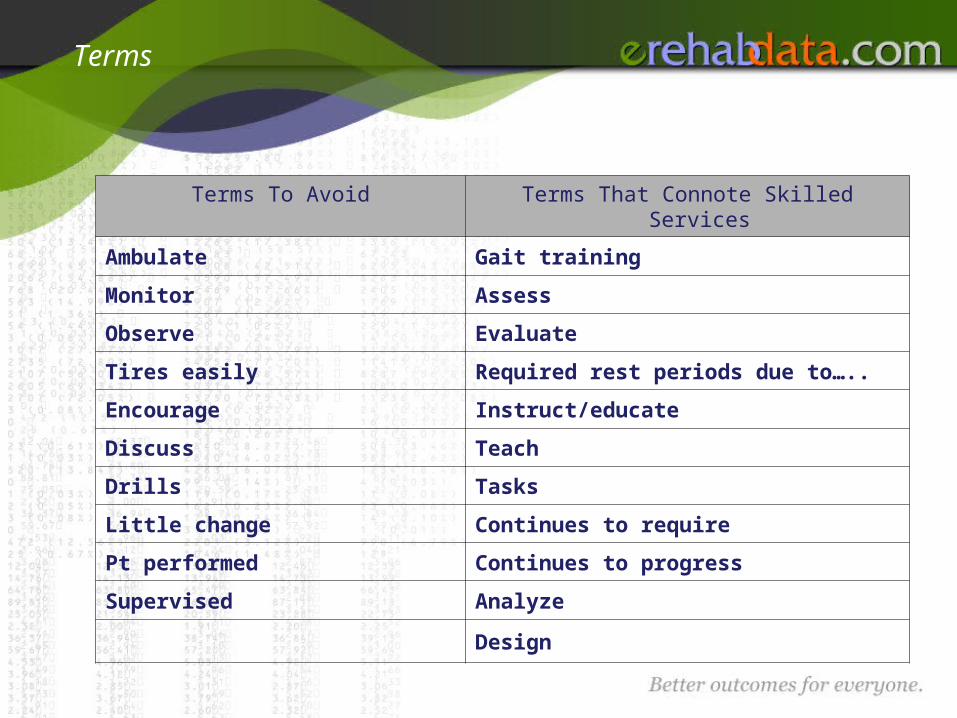
Terms
Terms To Avoid Terms That Connote Skilled Services
Ambulate Gait training
Monitor Assess
Observe Evaluate
Tires easily Required rest periods due to…..
Encourage Instruct/educate
Discuss Teach
Drills Tasks
Little change Continues to require
Pt performed Continues to progress
Supervised Analyze
Design

Questions?Next call - February 6 at 1:00
ESTLisa Bazemore, MBA, MS, CCC-SLP
[email protected](202) 588-1766







