
Touchstone Community Development Service
Presented at:
Yorkshire & Humber Public Mental Health and Suicide Prevention Forum
Leeds Civic Hall
8 July 2015
(Dis)parity in Mental Health & Physical Health
Needs of BME Communities: A Scoping Review
Bereket Loul ([email protected])
John Halsall
Sarah So
Vanysha Sahota

About Touchstone
One of the Leading Community Mental Health & Wellbeing
Providers
Operates in Leeds, Kirklees & across West Yorkshire (WYFI BME Project)
9 BME Specific
Services & 15
different services
overall
SU involvement & coproduction at the heart of governance, service delivery & design
Serve over 2000 people a year &
almost half from BME background
Over 30 years of providing
Innovative Services

Promoting
Equality
&
Diversity
Bridging the
‘Culture-Gap’
between
Services &
Communities
Challenging
Stigma &
Discrimination
Outside/Inside
Mental Health
Community
Capacity
Building
Asset-based =
Look at what
people can do,
not what they
can’t
Over 8 Years of
Effective
Engagement
with BME
Communities
Community
Development
Service
Our Service

Our Team
Crisis
Prevention:
Alcohol
Crisis Resolution:
Home Treatment
Crisis Prevention:
Mental Health
Triage
7 Community Development Workers
From 7 National/Ethnic Backgrounds
7 Lead Areas
Parity of
Esteem
Refugees &
Asylum
Seekers
Islam and
Mental Health
Community
Data &
Intelligence
One PH Contract One Key Health and Wellbeing Priority
Improving Quality, Equality and Equity of Mental Health
Access, Experience & Outcomes for Black and Minority
Ethnic Communities in Leeds
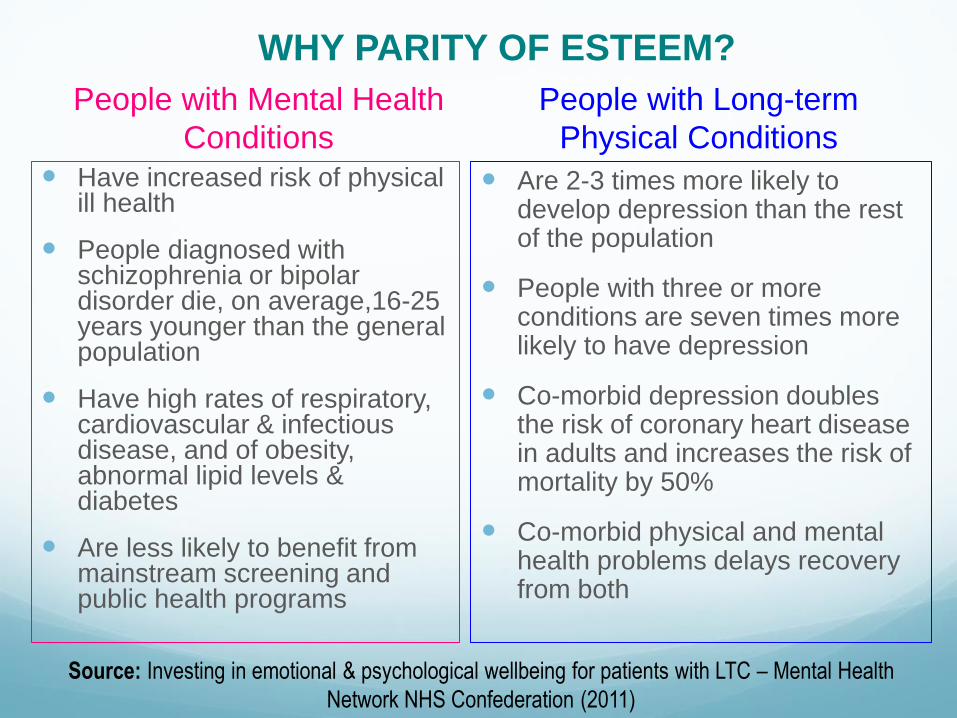
People with Mental Health
Conditions
Have increased risk of physical ill health
People diagnosed with schizophrenia or bipolar disorder die, on average,16-25 years younger than the general population
Have high rates of respiratory, cardiovascular & infectious disease, and of obesity, abnormal lipid levels & diabetes
Are less likely to benefit from mainstream screening and public health programs
People with Long-term
Physical Conditions
Are 2-3 times more likely to develop depression than the rest of the population
People with three or more conditions are seven times more likely to have depression
Co-morbid depression doubles the risk of coronary heart disease in adults and increases the risk of mortality by 50%
Co-morbid physical and mental health problems delays recovery from both
WHY PARITY OF ESTEEM?
Source: Investing in emotional & psychological wellbeing for patients with LTC – Mental Health
Network NHS Confederation (2011)
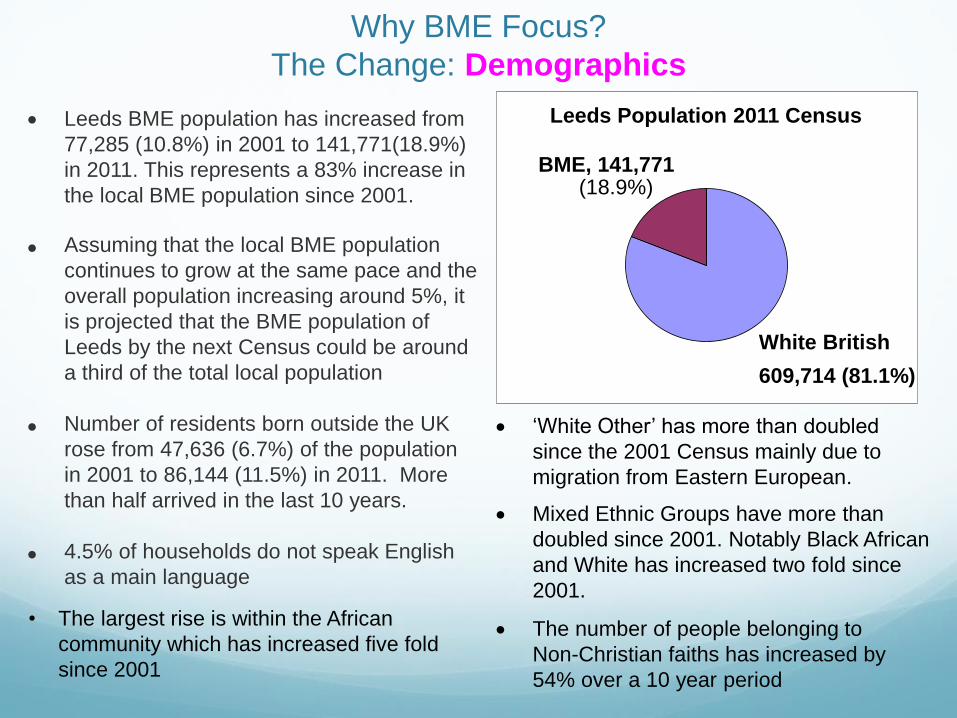
Why BME Focus?
The Change: Demographics
Leeds BME population has increased from
77,285 (10.8%) in 2001 to 141,771(18.9%)
in 2011. This represents a 83% increase in
the local BME population since 2001.
Assuming that the local BME population
continues to grow at the same pace and the
overall population increasing around 5%, it
is projected that the BME population of
Leeds by the next Census could be around
a third of the total local population
Number of residents born outside the UK
rose from 47,636 (6.7%) of the population
in 2001 to 86,144 (11.5%) in 2011. More
than half arrived in the last 10 years.
4.5% of households do not speak English
as a main language
Leeds Population 2011 Census
White British
609,714 (81.1%)
BME, 141,771 (18.9%)
‘White Other’ has more than doubled
since the 2001 Census mainly due to
migration from Eastern European.
Mixed Ethnic Groups have more than
doubled since 2001. Notably Black African
and White has increased two fold since
2001.
The number of people belonging to
Non-Christian faiths has increased by
54% over a 10 year period
• The largest rise is within the African
community which has increased five fold
since 2001
Why BME Focus?
The Challenge: Super-diversity & Closing the ‘Culture Gap’ between
Services & Communities ‘Culture includes a person’s beliefs, norms, values, and language. It plays key role in how
people perceive and experience mental illness, whether or not they seek help, what type of help they seek, what coping styles and supports they have, what treatment might work,
and more.’ Dr. Dawit Mengistu (MPH,DVM)
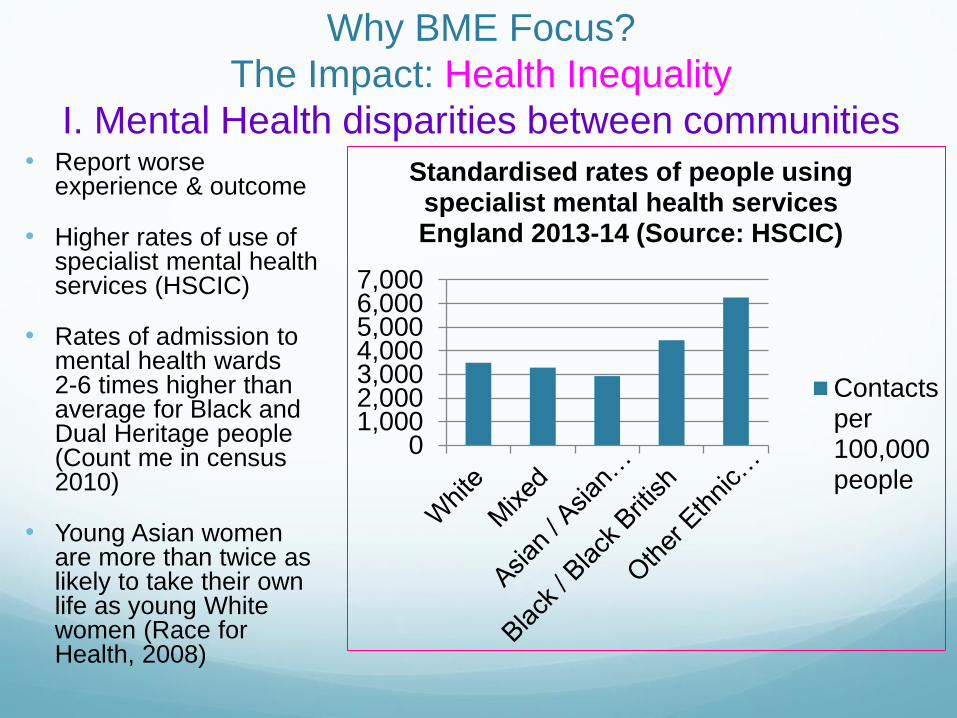
Why BME Focus?
The Impact: Health Inequality
I. Mental Health disparities between communities • Report worse
experience & outcome
• Higher rates of use of specialist mental health services (HSCIC)
• Rates of admission to mental health wards 2-6 times higher than average for Black and Dual Heritage people (Count me in census 2010)
• Young Asian women are more than twice as likely to take their own life as young White women (Race for Health, 2008)
01,0002,0003,0004,0005,0006,0007,000
Standardised rates of people using specialist mental health services England 2013-14 (Source: HSCIC)
Contactsper100,000people
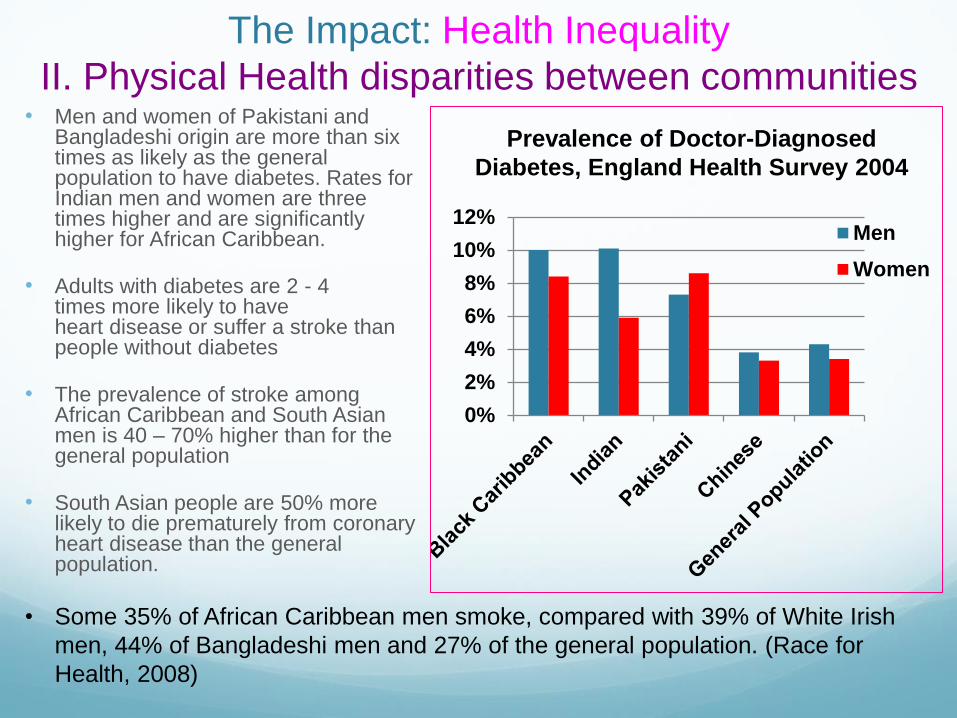
• Men and women of Pakistani and Bangladeshi origin are more than six times as likely as the general population to have diabetes. Rates for Indian men and women are three times higher and are significantly higher for African Caribbean.
• Adults with diabetes are 2 - 4 times more likely to have heart disease or suffer a stroke than people without diabetes
• The prevalence of stroke among African Caribbean and South Asian men is 40 – 70% higher than for the general population
• South Asian people are 50% more likely to die prematurely from coronary heart disease than the general population.
0%
2%
4%
6%
8%
10%
12%Men
Women
Prevalence of Doctor-Diagnosed
Diabetes, England Health Survey 2004
The Impact: Health Inequality
II. Physical Health disparities between communities
• Some 35% of African Caribbean men smoke, compared with 39% of White Irish
men, 44% of Bangladeshi men and 27% of the general population. (Race for
Health, 2008)

Aims of our Scoping Review • To review national and local information on parity of esteem and its implications
for BME communities
• To review existing data and intelligence to see any major differences with regard
to parity of esteem between the general population and BME communities in
Leeds
• Identify good practices that promote better parity of physical and mental health
needs of BME communities in Leeds
What we found out? Very limited reports and research
No national or local research that jointly consider the
physical and mental health needs of BME communities
Higher levels of poor mental health and wellbeing are
inextricably linked with deprivation. 28% of people with
severe mental illness live in the most deprived areas of
Leeds
Third sector organisations work in more holistic way
that cater for both the mental and physical needs of
local communities
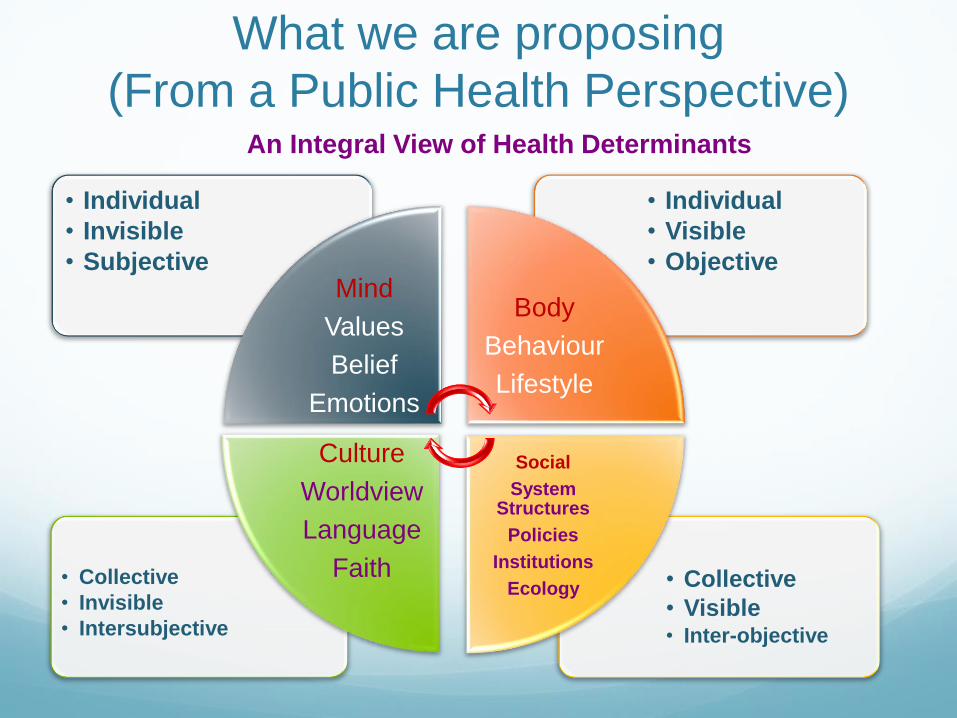
What we are proposing
(From a Public Health Perspective) An Integral View of Health Determinants
• Collective
• Visible • Inter-objective
• Collective
• Invisible
• Intersubjective
• Individual
• Visible
• Objective
• Individual
• Invisible
• Subjective Mind
Values
Belief
Emotions
Body
Behaviour
Lifestyle
Social
System Structures
Policies
Institutions
Ecology
Culture
Worldview
Language
Faith

The way forward… Towards Integral Health Development
Mental Health Physical Health
IND
IVID
UA
L • Assess & support physical health
needs
• Increase knowledge and resilience
• Support for better self-management
• Assess & support mental health
needs
• Increase knowledge and
resilience
• Support for better self-
management
CO
LLE
CT
IVE
• Community engagement and
intelligence
• Bridging the ‘culture-gap’
• Awareness raising – including the
link between culture/ethnicity and
health risk/protective factors
• KEY MESSAGE – What is not good
for you body, is not good for your
mind!
• Robust system of integrated data
and intelligence gathering
• Further research?
• Platform for best practice sharing
& collective learning
• Joined up training for health
professionals
• All Levels, All Sectors Partnership
• Parity of Investment
The ties that bind individuals to their culture and ethnic communities are invaluable and instructive resources in the
understanding of mental illness and in the delivery of responsive and responsible mental health support.
Dr. Dawit Mengistu (MPH,DVM)







