
Resuscitation of
neonates with Ambu
bag, Flow inflating bag
and T-pieceEbtihal Hassan Al-Oweywee

Definition of resuscitation
Ambu bag
Flow inflating bag
T-piece
Study about the hazards of T-piece without limitation of flow
rate.
Study that compare the 3 types of resuscitation devices.

DEFINITION OF NEONATAL RESUSCITATION
Neonatal Resuscitation is intervention after a baby is born to
help it breathe and to help its heart beat.
Before a baby is born, the placenta provides oxygen and nutrition
to the blood and removes carbon dioxide.
After a baby is born, the lungs provide oxygen to the blood and
remove carbon dioxide.
Many babies go through this transition without needing
intervention.
Some babies need help with establishing their air flow, breathing,
or circulation.

RESUSCITATION DEVICES
Self inflating bag
Flow inflating bag
T-piece


SELF INFLATING BAG
Fill spontaneously after they are squeezed,
pulling oxygen or air into the bag
Remain inflated at all times
Can deliver positive-pressure ventilation without
a compressed gas source.
Require attachment of an oxygen reservoir to
deliver 100% oxygen

• Does not need a gas source to inflate
• Pressure release valve
• Portable and light weight
• Available in single use, disposable bags

• Will inflate even without adequate seal.
• Requires a reservoir to deliver 100%
oxygen.
• Does not provide PEEP/CPAP (unless a PEEP
valve has been fitted).

Place the mask firmly against your
hand.
Squeeze the bag repeatedly.
You should feel air pressure against
your hand and see the lip valve open
and close
If pressure is not felt, this device is
not safe to use!
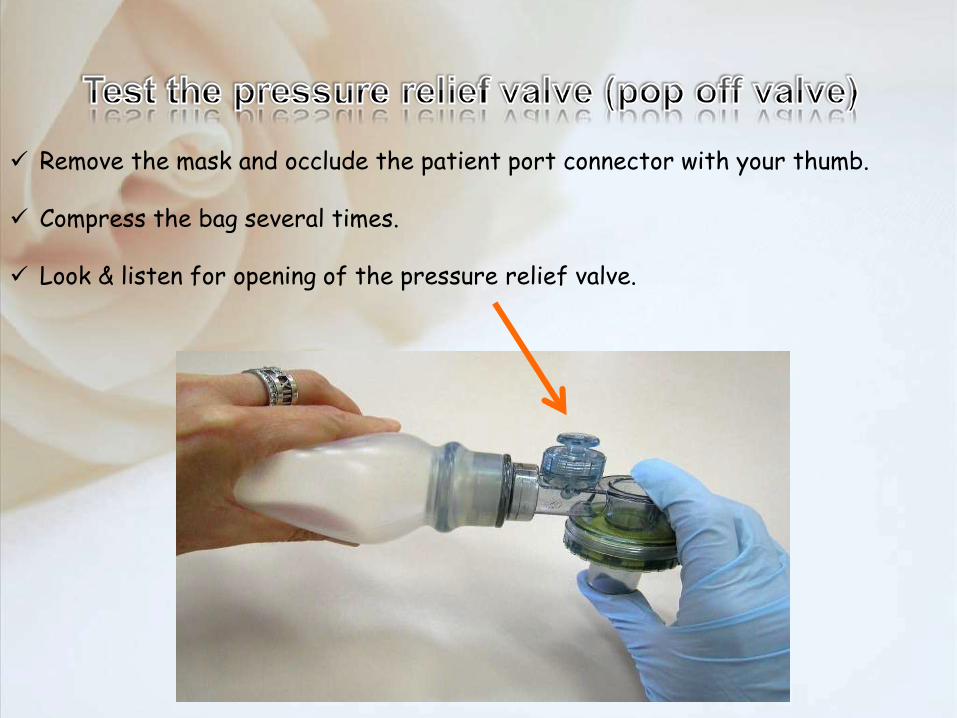
Remove the mask and occlude the patient port connector with your thumb.
Compress the bag several times.
Look & listen for opening of the pressure relief valve.


Create a good seal between the infant's
face & the mask
How to use it ??!


Incorrect ways to hold a mask
A: Do not hold the stem
B: Do not hold the outeredge
× ×

AIR OR OXYGEN FOR RESUSCITATION?
o Term newborns: Use air (21%) initially.
o Preterm newborns < 32 weeks: Use air or
blended air and oxygen
(21% to 30% oxygen to start).
o Use air if a blender is not available.

Is your technique effective? • If your ventilation technique is effective, three signs
are observed:
1. An increase in the heart rate above 100/min.
2. A slight rise and fall of the chest and upper abdomen with each
inflation.
3. An improvement in oxygenation.
If the heart rate is not improving: • The technique of ventilation needs to be improved.
• Consider increasing the PIP.
• Endotracheal intubation should also be considered.


FLOW INFLATING BAG
Fill only when oxygen from a compressed
source flows into them
Depend on a compressed gas source
Must have a tight face-mask seal to
inflate

The mask is not properly sealed
over the newborn’s nose and mouth
There is a tear in the bag.
The pressure gauge is missing

Delivers 100% oxygen at all times.
Easy to determine the adequacy of seal.
“Stiffness” of lungs can be felt.
Provide PEEP.

Requires a tight seal to remain inflated
Requires a gas source to inflate
No safety pop-off valve
Requires more experience


Gas supply
Gas supply line
Test lung
Patient supply linewith T-piece & mask
Neopuff

• Gas flow rate10 L/min (8L /min if using cylinders)
• Maximum pressure relief valve50 cm H2O
• PIP30 cm H2O (term newborn)20 - 25 cm H2O (preterm < 32 weeks’)
• PEEP5 - 8 cm H2O
INITIAL RECOMMENDED SETTINGS

1. Connect the gas & patient supply lines

2. Connect the
test lung to T-
piece and turn
on the flow
3. Turn the inspiratory
pressure control dial
fully clockwise
Occlude the PEEP cap check
that the pressure gauge points
to 50 cmH2O

4. Set the PIP and PEEP
20 – 25 cm H2O for a premature infant
or 30 cm H2O for a term infant.
Set a PEEPof 5 cm H2O
Caution: any increase in the flow rate willresult in a dangerously high increase in PEEP.

The operator can set the (PIP) & (PEEP).
The T-piece device will not deliver PIP or
PEEP/CPAP above the set pressures if the flow
remains constant.
The PIP & PEEP are displayed on the manometer.
The operator can control the length of the
inspiratory time by varying the duration of
occlusion of the PEEP cap.

Requires a gas source to operate.
The set PIP can be reached on the manometer
despite a face mask leak of up to 90%.
As the T- piece device delivers a set pressure, it is
still possible to deliver large volumes of gas to the
infant which may cause a pneumothorax or damage
the lungs of infant.


(1)To assess (PIP), (PEEP) and (Pmax)
at different flow rates
(2)To assess maximum PIP and PEEP at
a flow rate of 10 l/min with a
simulated air leak of 50%.
THE AIM

METHOD
• 5 Neopuffs were set to
PIP of 20 PEEP of 5 Pmax of 30
flow of 5
• PIP, PEEP and Pmax were recorded at flow rates
of 10, 15 l/min and maximum flow.
• Maximum achievable PIP and PEEP at a flow rate
of 10 l/min with a simulated air leak of 50%.
At gas flow of (15 l/min)
PEEP increased to 20
PIP increase to 28
Pmax increase to 40 cm H2O
At maximum flow (85 l/min)
PEEP increase to 71
PIP increase to 92 cm H2O
At 10 l/min flow, with an air leak of 50%,
the maximum PEEP is 21
The maximum PIP is 69
RESULT

Pmax is overridden by increasing the rate of gas
flow and potentially harmful PIP and PEEP can be
generated.
Even in the presence of a 50% gas leak, more than
adequate pressures can be provided at 10 l/min gas
flow.
We recommend the limitation of gas flow to a rate
of 10 l/min as an added safety mechanism for this
device.
CONCLUSION


METHOD
We studied 31 operators using a T-piece resuscitator, a
self-inflating bag and a flow-inflating bag.
we evaluated the ability to deliver a consistent PIP of 20
or 40 cmH2O and a PEEP of 5 cmH2O .
evaluate the ability to maintain a 5 s inflation at a PIP of
20 cmH2O
Evaluate the time to transition from a PIP of 20 to 40
cmH2O.

T-Piece
resuscitator
Self inflating
bag
Flow inflating
bag
(PIP) at the target of 20
cmH2O
20 24 -
(Pmax) at the target of 40
cmH2O
39 45 44
The duration to increase
the PIP from 20 to 40
5.7 2.2 1.8
Maintaining pressure
greater than 18 for 5 s
4 2.2 3.7
RESULT

The T-piece resuscitator delivered the desired
pressures more accurately, but required greater
time to increase the PIP from 20 to 40 cmH2O.
It was difficult to maintain a prolonged inflation
time with the self-inflating bag
CONCLUSION

• Australian Resuscitation Council & the New Zealand Resuscitation
Council. (2010). Section 13: Neonatal Guidelines. Retrieved February 2,
2012 from:
http://www.resus.org.au
• Up to date
• Laerdal Medical (2006) Laerdal silicone resuscitators: Interactive
presentation. Accessed April 27, 2009 from
http://www.laerdaltraining.com/lsr
• Fisher & Paykel Healthcare. (2004). Neopuff™ Infant Resuscitator.
Optimal resuscitation in neonatal care. Auckland, New Zealand.
• http://fn.bmj.com/content/94/6/F461.short
• http://www.ncbi.nlm.nih.gov/pubmed/16081202








