
Institute for Clinical Diabetology
German Diabetes Center at the Heinrich Heine University
Leibniz Center for Diabetes Research
Department of Endocrinology and Diabetology
University Hospital, Düsseldorf, Germany
Diabetic Neuropathy: New Developments
in Early Diagnosis and Treatment
Dan Ziegler, MD, FRCPE

painful painless
?
Prevalence: ≈30%
Diabetic sensorimotorpolyneuropathy (DSPN)
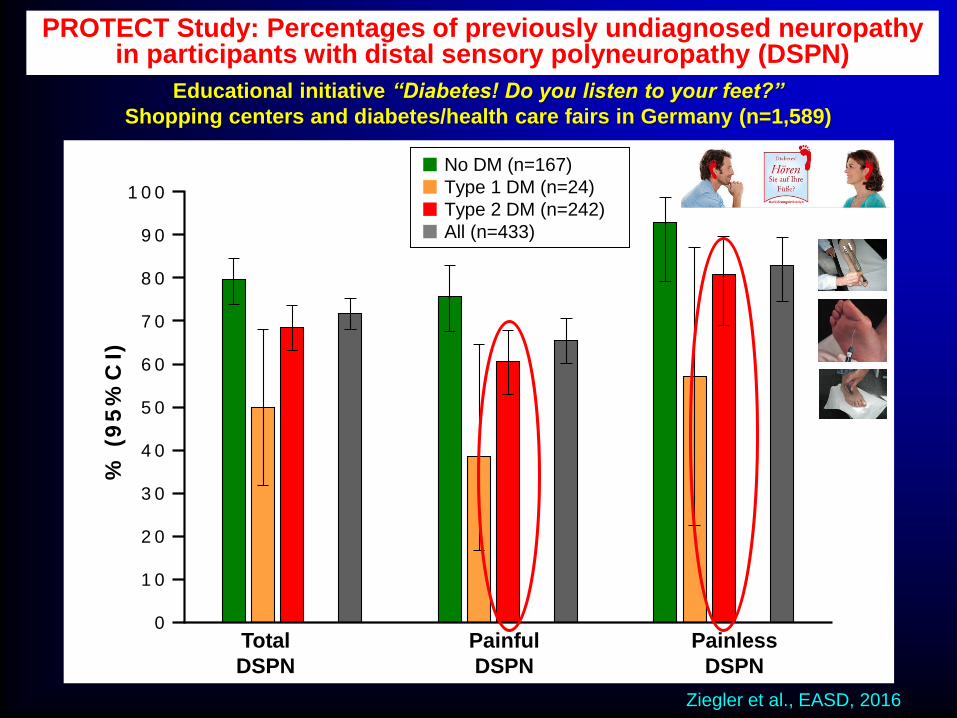
PROTECT Study: Percentages of previously undiagnosed neuropathyin participants with distal sensory polyneuropathy (DSPN)
D S P N S ch m erz h af t e D S P N * S ch m erz lo se D S P N *
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
% (
95
%C
I)
Painful
DSPN
Painless
DSPN
Total
DSPN
■ No DM (n=167)
■ Type 1 DM (n=24)
■ Type 2 DM (n=242)
■ All (n=433)
Educational initiative “Diabetes! Do you listen to your feet?”
Shopping centers and diabetes/health care fairs in Germany (n=1,589)
Ziegler et al., EASD, 2016

Curr Diab Rep 2012;12: 376-383

Prevalence of polyneuropathy, neuropathic pain, and cardiacautonomic dysfunction in prediabetes and diabetes
Ziegler et al., Diabetes Care 2008; 31: 556-561
Ziegler et al., Pain Med 2009; 10: 393-400
Ziegler et al., Eur J Pain 2009; 13: 582-587
Bongaerts et al., Diabetes Care 2012; 35: 1891-1893
Ziegler et al., Diabetologia 2015; 58: 1118-1128
Survey Measure NGT
(%)
IFG
(%)
IGT
(%)
IFG+IGT
(%)
New DM
(%)
Known DM
(%)
S2+S3 MNSI>2 7.4 11.3 13.0 28.0
F4 VPT/MF bilat. 11.1 5.5 14.8 23.9 16.1 22.0
S2+S3 MNSI>2+pain 1.2 4.2 8.7 13.3
AMIR MNSI>2+pain 3.7 5.7 14.8 21.0
S4 Reduced HRV 4.5 8.1 5.9 11.4 11.7 17.5
NGT = normal glucose tolerance
IFG = isolated impaired fasting glucose
IGT = isolated impaired glucose tolerance
New DM = newly detected diabetes mellitus
Known DM = known diabetes mellitus
MNSI = Michigan Neuropathy Screening Instrument
VPT = vibration perception threshold
MF = monofilament
HRV = heart rate variability
AMIR = Augsburg Myocardial Infarction Registry
5 min

How to diagnose diabetic neuropathy?
Motor Sensory Autonomic
Myelinated Myelinated Thinlymyelinated
Un-myelinated
Thinlymyelinated
Un-myelinated
A A/ A C A C
Large
Motor,sensory
NCV
Touch,Vibration, Position
perception
Warm perc. Pain
IENFDCCM
HRV, AFTs, BRSSudomotor,
GIT, GUT function
Small
Modified after Vinik
Coldperception
Pain

Ziegler et al., Diabetes 2014; Diabetologia 2015
Control Type 2 DM
German Diabetes Study: Reduced epidermal nerve fiber density
and enhanced antioxidative defense in recent-onset type 2 DM
Intraepidermal nerve fiber density
PGP9.5
Control
Mean diabetes
duration: 1 year
0.16
Type 2 DM (n=69)
0.26
Increase in superoxide dismutase (SOD)2 area
Control (n=51)
Green: SOD2
Blue: nucleus
Control Type 2 DM

In vivo laser scanning
corneal confocal
microscopy (CCM)

Corneal Confocal Microscopy (CCM)
Diabetic neuropathyHealthy subject
Ziegler et al., Diabetes, 2014; 63: 2454-2463

CCM in recently diagnosed Type 2 diabetic patients
Ziegler et al., Diabetes, 2014; 63: 2454-2463

Key Messages I
Prevalence of neuropathy is increasedin prediabetes, particularly in combinedIFG-IGT.
An array of abnormalities in nerve functionand morphology are detected in conjunctionwith oxidative stress and inflammation asearly as in recent-onset DM.

Glycemiccontrol
Lifestyle/multi-factorial riskintervention
Analgesics
Pathogenetic
treatment
Treatment
of Diabetic
Neuropathy
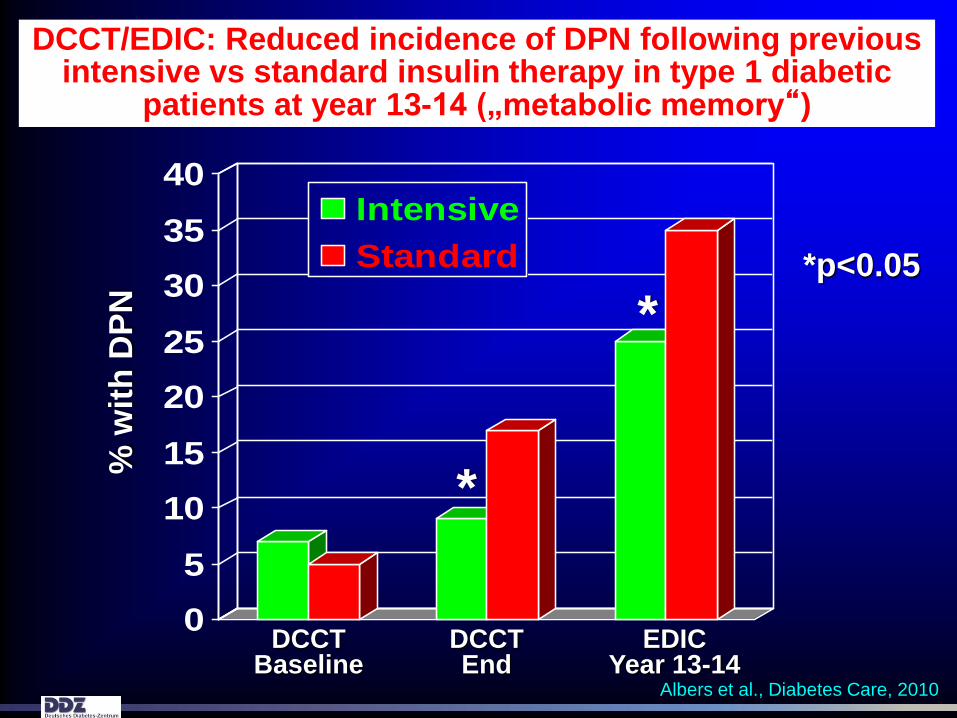
DCCT/EDIC: Reduced incidence of DPN following previousintensive vs standard insulin therapy in type 1 diabetic
patients at year 13-14 („metabolic memory“)
Albers et al., Diabetes Care, 2010
0
5
10
15
20
25
30
35
40Intensive
Standard
DCCTBaseline
DCCTEnd
EDICYear 13-14
% w
ith
DP
N **p<0.05
*

+ = benefit; = no effect; #higher mortality on IT.
ST = standard therapy; IT = intensive therapy
NCV = nerve conduction velocity; VPT = vibration perception threshold
Trial
n Duration
(years)
HbA1c(%)
ST vs IT
DSPN endpoints
Clinical NCV VPT
UKPDS 3,867 up to 15 7.9 vs 7.0 ? ? ?
Kumamoto 110 up to 10 9.4 vs 7.1 ? ? ?
VADT 1,791 5.6 8.4 vs 6.9 ? ? ?
ADVANCE 11,140 5 7.3 vs 6.5 ? ? ?
ACCORD 10,251 3.7 / 1.3 7.6 vs 6.3#/7.2 ? ? ?
HOME 390 4.3 7.9 vs 7.5 ? ? ?
BARI 2D 2,159 4 7.6 vs 7.1 (IP/IS) ? ? ?
ADDITION 1,161 6 6.4 vs 6.3 ? ? ?
Steno Type 2 160 8 / 5 9.0 vs 7.7 ? ? ?
Effects of intensive diabetes therapy on
development/progression of DSPN in type 2 DM

+ = benefit; = no effect; #higher mortality on IT.
ST = standard therapy; IT = intensive therapy
NCV = nerve conduction velocity; VPT = vibration perception threshold
Trial
n Duration
(years)
HbA1c(%)
ST vs IT
DSPN endpoints
Clinical NCV VPT
UKPDS 3,867 up to 15 7.9 vs 7.0 +
Kumamoto 110 up to 10 9.4 vs 7.1 +
VADT 1,791 5.6 8.4 vs 6.9
ADVANCE 11,140 5 7.3 vs 6.5
ACCORD 10,251 3.7 / 1.3 7.6 vs 6.3#/7.2 +
HOME 390 4.3 7.9 vs 7.5
BARI 2D 2,159 4 7.6 vs 7.1 (IP/IS) +
ADDITION 1,161 6 6.4 vs 6.3
Steno Type 2 160 8 / 5 9.0 vs 7.7
Effects of intensive diabetes therapy on
development/progression of DSPN in type 2 DM

Gibbons & Freeman, Brain, 2015; 138: 43-52
HbA1c ↓ 4–7% (n=52)HbA1c ↓ 2–3.9% (n=27) HbA1c ↓ >7% (n=25)
Treatment-induced neuropathy of diabetes (TIND)
All patients with pain
Many patients with pain

Treatment-induced neuropathy of diabetes (TIND)
HbA1c ↓ 2–3% points over 3 months: 20% risk of TIND
HbA1c ↓ >4% points over 3 months: >80% risk of TIND
Risk of developing TIND
TIND was present in 10.9% of all individuals seen in a
tertiary referral diabetic neuropathy clinic over a 5-year period
Gibbons & Freeman, Brain, 2015; 138: 43-52
X
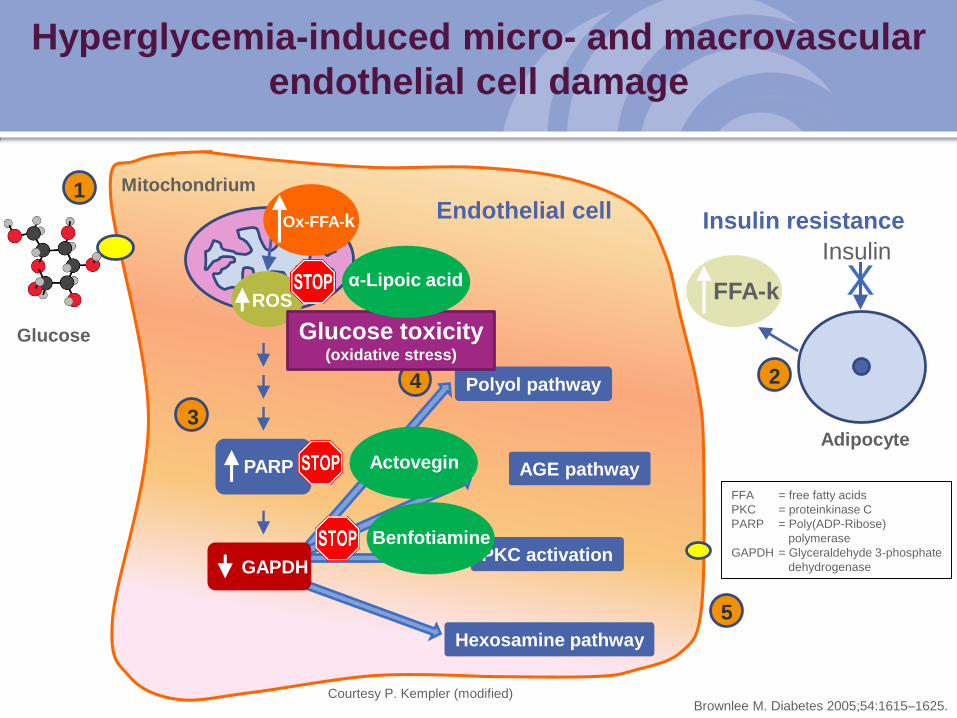
Hyperglycemia-induced micro- and macrovascular
endothelial cell damage
Glucose
ROS
Insulin resistance
Insulin
Ox-FFA-k
PARP
FFA-k
Polyol pathway
AGE pathway
PKC activation
Hexosamine pathway
Mitochondrium
Adipocyte
Endothelial cell
Brownlee M. Diabetes 2005;54:1615–1625.
GAPDH
1
2
3
4
5
Glucose toxicity(oxidative stress)
FFA = free fatty acids
PKC = proteinkinase C
PARP = Poly(ADP-Ribose)
polymerase
GAPDH = Glyceraldehyde 3-phosphate
dehydrogenase
α-Lipoic acid
Actovegin
Benfotiamine
Courtesy P. Kempler (modified)

-Lipoic Acid in Diabetic Neuropathy:
Randomized Placebo-Controlled Trials
ALADINALADIN 2ALADIN 3ORPILDEKANSYDNEYSYDNEY 2NATHAN 1NATHAN 2
R(+) S(-)
• Intravenous• Oral

Meta-Analysis of Individual Neuropathic SymptomsRelative Differences between -Lipoic Acid (600 mg/day i.v.) and Placebo after 3 Weeks
Numbness
Paresthesias
Burning
Pain
TSS
GM with 95% CI
n=1258
Favors -lipoic acid; p<0.05
% -10 0 10 20 30 40 50Ziegler et al., Diabetic Med, 2004;21:114-21

-Lipoic acid (i.v. and oral): Meta-analysis of RCTs in symptomatic DSPN
Çakici et al., Diabet Med 2016 Jan 29. doi: 10.1111/dme.13083. [Epub ahead of print]
Total Symptom Score (TSS)

20
25
30
35
40
45
%
-Lipoic acid (n=219)
Placebo (n=210)
NATHAN 1 Study: NIS-LL Responders vs NIS-LL Progressors
RespondersNIS-LL -2 pts
UnchangedNIS-LL > -2 to < +2
Progressors NIS-LL +2 pts
P=0.025
35.6
29.0
36.2 34.8
40.2
24.2
After4 years:
Ziegler et al., Diabetes Care, 2011; 34: 2054-60
NIS-LL = Neuropathy Impaiment Score- Lower Limbs

NATHAN 1 Trial: Predictors of NIS-LL Improvement
Baseline variables: diabetes-related, DSPN, and analgesic treatment
ATC codes: N02: analgesics, N03: antiepileptics, N06: psychoanaleptics
F Favors placebo Favors α-lipoic acid
Ziegler et al., J Diabetes Complications 2016; 30: 350-6

Measures of treatment effect in
neuropathic pain
Pain relief Mood Functionality
Chronic pain treatementrequires assessment of
Pain intensity Sleep
0 321 4 5 6 7 108 9No pain Intolerable pain
Numeric Analog Scale (NAS = Likert Scale)

Finnerup et al., Lancet Neurol 2015; 14: 162-73
GRADE = Grading of Recommendations Assessment, Development, and Evaluation
Pharmacotherapy of neuropathic pain
GRADE Recommendations (I)

Finnerup et al., Lancet Neurol 2015; 14: 162-73
Pharmacotherapy of neuropathic pain
GRADE Recommendations (II)

Treatment of Painful Diabetic Neuropathy
under Consideration of Comorbidities
Duloxetine(SNRI)
Amitriptyline(TCA)
Pregabalin/Gabapentin
Opioids α-Lipoicacid
Depression + + ↔ ↔ ↔Obesity ↔ ↔ ↔Coronary heart
disease↔ ↔ ↔ ↔
Autonomic
neuropathy? (+) +
Pathogenetic
treatmentNo No No No Yes
+ favorable, unfavorable, ↔ neutral

Holbech et al., Pain. 2015; 156: 958-966
Analgesic combination therapy
in painful neuropathy
●Placebo
▲Pregabalin
300 mg/Tag
Imipramine
75 mg/Tag
Combination
*P<0,05 vs Placebo†P<0,05 vs either
monotherapy
n=50, 22% DM
Cross-over
NRS: Numerical
Rating Scale

Non-pharmacological pain treatment
AcupunctureNerve
stimulationMuscle
stimulation
Psychologicalsupport
TENS

Protective effects of near-normoglycemiaon nerve function are proven in type 1 but not in type 2 diabetes.
Key Messages II
Antioxidant treatment with -lipoic acid for up to 4 years is safe and improves neuropathic symptoms and signs.
Since analgesic monotherapy of neuropathicpain is effective in 50% of the patients,drug combinations are often required.

German Diabetes Center (DDZ)
Leibniz Center for Diabetes Research
Eυχαριστώ πολύ!







