
DIABETES MELLITUSAhmed Al-Naher
FY2 Coventry

Case Scenario• 52 male presents to GP with 3/12 lethargy and 2/52 thirsty
and drinking more than normal. • PMH HTN• Drinks alcohol socially, non-smoker• BMI 32• Urine Dip: glucose +++• Random Blood Sugar = 13

Contents
• Diagnosis
• Risk Factors
• Complications
• Investigations
• Management
• DKA + HONK

Type 1 vs Type 2• Type 1 = Inability to produce insulin (autoimmune process
against beta islet pancreas cells)
• Type 2 = insensitivity to insulin over time• Gestational Diabetes = decreased insulin sensitivity
during pregnancy
• Secondary Diabetes:• Pancreatic Disease/CF/Chronic Pancreaitis/Pancreatic Ca• Steroid use/ antipsychotics/ thiazide diuretics

Diagnosis• Random Glucose >11.1 mmol/L• Fasting Glucose >7 mmol/L• 2x Fasting glucose samples to confirm• Or presence of symptoms• HbA1c >6.5% (48mmol/L)
• OGTT – two hour glucose after 75g glucose
• IGT = normal fasting glucose and OGTT between 7-11• IFG = OGTT <7.8 but fasting glucose 6.1 – 6.9
Risk Factors• T1: Family Hx, Caucasian/Scandinavian, Juvenile onset
• T2: • High BMI• Physical inactivity• South Asian/Afro-carribean/middle-eastern• Hx of gestational diabetes, IGT, IFG• Steroid use• PCOS• Family Hx
Presentation• Polyuria• Polydipsia• Lethargy• Recurrent infections• Complications• DKA (T1)• HONK (T2)

Presentation - case• 67 male admitted feeling generally unwell, SOB, sweating
and lethargic over last 2 days. • He is a known Type 2 diabetic on insulin with PVD,
peripheral neuropathy and previous CVA. His BM is 5.6.• ECG showed residual ST elevation in anterior leads with
Q wave and reciprocal changes. Echo showed new septal hypokinesia
• The patient had no history of chest pain

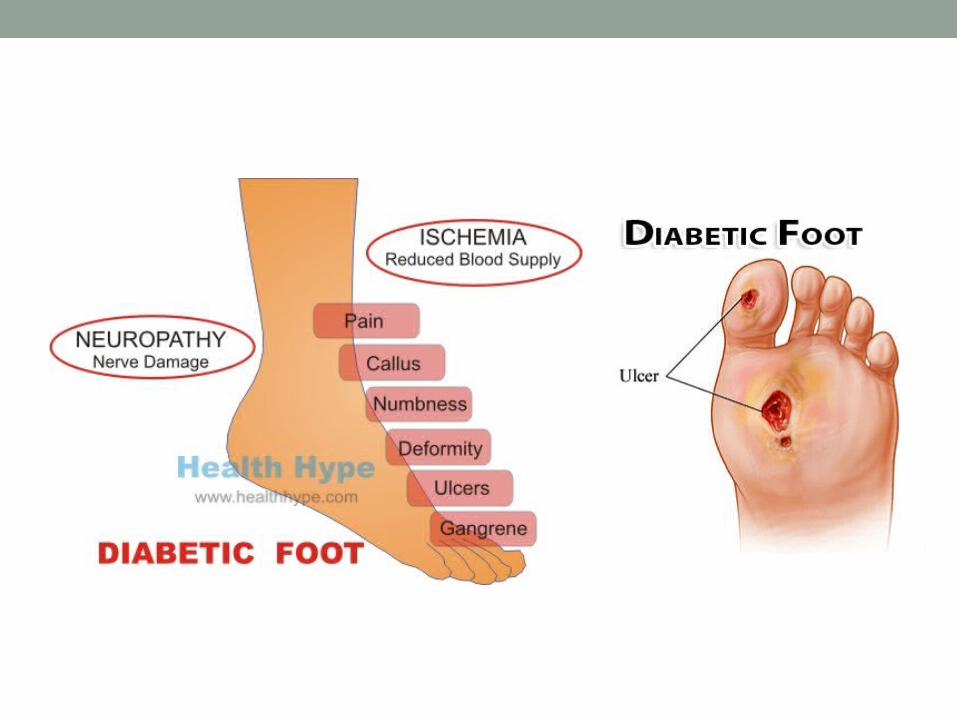
Complications• Macrovascular: Stroke, MI, PVD
• Retinopathy, Xanthelasma, Cataracts, Opthalmoplegia, maculopathy
• Peripheral Neuropathy, Diabetic amyotrophy, neuropathic pain, Autonomic neuropathy
• Nephropathy
• Recurrent infections: Cellulitis, UTI, Thrush
Investigations• Bedside: • Urine Dip: Glucose, ketones, MC+S• BM Stix, Ketone Stix• ECG, BP• Neuro, eye, foot exam• ACR, eGFR, microalbuminuria• Injection sites
• Bloods - HbA1c, lactate, pH, U+E, Lipids, LFT, TFT

Managing Risk Factors• Lifestyle – Weight loss, Exercise• Education – DESMOND (Diabetes Education and Self
Management for Ongoing and Newly Diagnosed)• Self-Monitoring of BM• Dietician, Low sugar diet• Smoking cessation• Foot Care • Eye screening• BP Control: ACEi, CCB, Diuretic, K sparing• Statins, Fibrates• Aspirin


Oral Hypoglycaemics• Biguanides – increase insulin sensitivity: Metformin
• Sulphonylureas: Gliclazide, Glibenclamide • Meglitinides: Repaglinide, Nateglinide• Thiazolidinediones: Pioglitazone• DDP-4 inhibitors: Sitagliptin, Vildagliptin• GLP-1 Agonists: Exenatide, Liraglutide• Orlistat• Ascarbose

Treatment Pathway• 1) Lifestyle Interventions• 2) Metformin• 3) Metformin + sulphonylurea• 4) Metformin + sulphonylurea + Thiazolidinedione or
GLP-1 agonist or DDP-4 inhibitor• 4) Metformin + sulphonylurea + insulin• 5) Increase insulin
Insulin Types
• Rapid-acting: Lispro (Humalog), Aspart (Novorapid)• Short-acting: Soluble Insulin (Actrapid)• Intermediate Acting: NPH (Insulatard)• Long-acting: Glargine (Lantus), Detemir (Levemir)• Ultra long-acting: Degludec• Pre-mixed: Novomix 30, Humalog Mix25, Humumlin M3
• Regimens:• Once Nightly• Twice Daily Biphasic• Basal Bolus• Continuous Pump
Prognosis• T1 = increased risk of blindness, ESRF, CVD• Control of BP, Lipids, BM and weight are prognostic
• T2 = 75% die of heart disease 15% die of stroke• Every 1% rise in HbA1c level risk of diabetes related
death increases by 21%

Case Scenario• 58 female T2DM, Portuguese, does not speak English,
not complying with medication or dietary advice, admitted with hyperglycaemia and seizures. Continues to have high BMs of >25 on wards and wishes to self-discharge.
• She has severe retinopathy blindness and PVD and no carers at home. She is prescribed a pre-mix regimen.
• What are the obstacles to safe management of this patient?
• What services/ support can be arranged?

Medical Emergency: Hypoglycaemia• BM < 3• Symptoms: low GCS, seizures, clammy, sweaty,
tachycardic, behaviour change, slurred speech, shaking• Risk: Strict BM control, Alcohol, malabsorption, Renal
failure, medication, lipohypertrophy, hypothyroid
• GlucoJuice/Glucotab 10-20g• GlucoGel (Hypostop)• 10% Dexrose IV 150-250ml• Glucagon 1mg IM/SC
• Cerebral Oedema: Mannitol, Dexamethasone, 50% Dex
Medical Emergency: DKA• Hyperglycaemia, Ketonaemia, Acidosis• Ketones >3mmol/L• BM >11• pH <7.3, HCO3 <15
• Triggered by stress: Infection, Poor compliance, endocrine crises, CVD, Alcohol, medication

DKA signs• Polydipsia, polyuria• Weight loss, lethargy• Vomiting, Abdo pain• SOB (Kussmaul’s respiration)• Low GCS, confusion
• Dehydration: dry mucus membranes, reduced skin turgor, sunken eyes, slow cap refill, tachycardia, low BP
• Pear Drop Breath• Signs of infection: Fever, crackles, cellulitis• Increased osmolality and anion gap

Specific investigations• Serial BMs and Ketones• Serial ABGs or VBGs• Septic Screen: BCM, Urine Dip, CXR• U+E including K• Trop T, CK• ECG• Amylase• CT Head
• Monitor BM, Ketones, Acidosis, mental state, fluid status

DKA Resuscitation• Correct dehydration: Fast NaCl 0.9% initially
• Fixed Rate insulin infusion: 0.1 unit/kg• Reduce BM ~3/hr to avoid cerebral oedema• Continue baseline long acting insulin• Run with NaCl 0.9% + KCl if <5.5• 10% glucose once BM <14• Treat underlying cause
• Once E+D convert back to normal insulin + DSN r/w• Indications for ITU: haemodynamic instability, cardiogenic
shock, respiratory failure, severe acidosis, coma

Complications• Cerebral oedema: headache, confusion, urinary
incontinence, coma – main mortality in children• Hypoglycaemia – arrhythmia, coma• Hypokalaemia – cardiac arrhythmia• VTE• Retinopathy• ARDS/ Pulmonary oedema
• Prognosis worsens with age, low GCS

Medical Emergency: HONK• T2DM• Hyperglycaemia, high serum osmolality, no ketosis• Osmotic diuresis -> intracellular dehydration
• Triggers: Infection, poor BM control, MI, CVA, endocrine crises, Acute abdo, medication, metformin, alcohol, first presentation
• Old age, dementia, steroid use• Severe Dehydration• Low GCS, confusion, seizures• Lethargy, weakness• Abdo Pain, N+V

HONK Mx• Ix as for DKA• Initial Fluid resuscitation• Variable Rate Insulin infusion • Run with 8 hourly NaCl + KCl• Treat underlying cause• Review medication• LMWH

Final Case• 87 yo male from nursing home with known glioblastoma
multiforme admitted with worsening confusion, reduced mobility and polyuria.
• CT shows no new haemorrhage, infarct or mass effect• DHx frusemide, aspirin and dexamethasone • pH 7.2 lactate 2.9 BM 32• Urine: Blood + Leuk + Gluc +++ Nitrites +
• Initial management?• Long-term treatment plan?

Questions?

• http://integrate.ccretherapeutics.org.au/Calculator/UkPds.aspx







