Download - dental pulp...humayun afridi taif saqib

DENTAL PULP• Presented by:
• Taif Ahmad (10)
• Humayun Afridi (09)
• Saqib Habib (51)
ORAL BIOLOGY
Contents
• Definition
• Morphology
• Functions
• Histology
• Vasculature
• Innervation
• Age Changes
• Clinical Considerations
Learning Objectives
• At The end of this presentation, 2nd year B.D.S students will be able to know about the dental pulp INSHALLAH.
Definition
• Dental pulp can be defined as a richly vascularized and innervated connective tissue of mesodermal origin enclosed by dentin with communication to periodontal ligament.
Development of Pulp
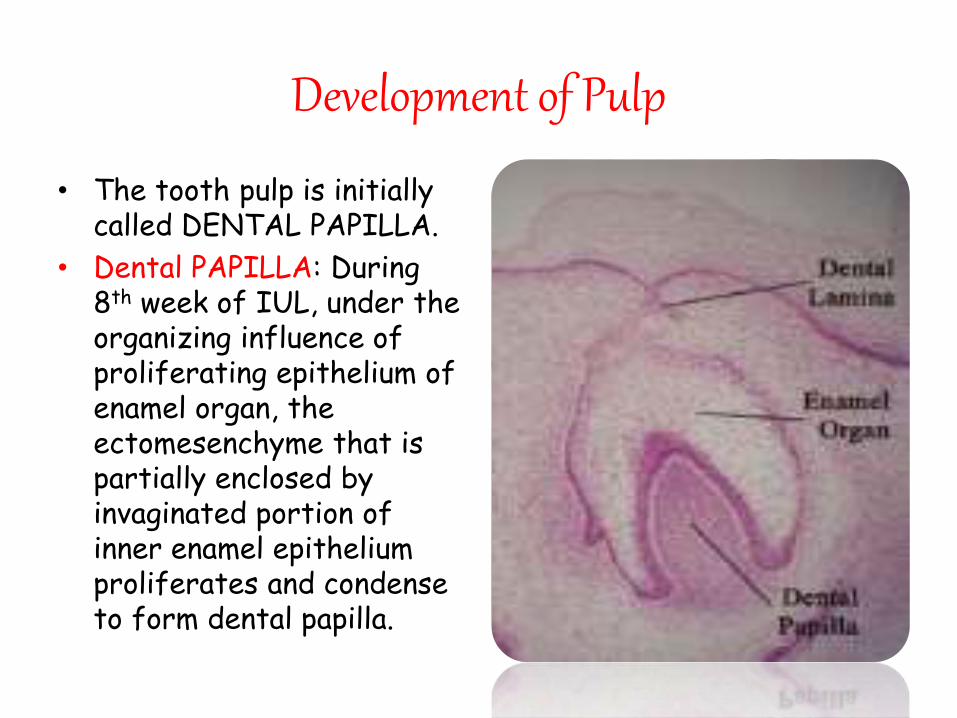
• The tooth pulp is initially called DENTAL PAPILLA.
• Dental PAPILLA: During 8th week of IUL, under the organizing influence of proliferating epithelium of enamel organ, the ectomesenchyme that is partially enclosed by invaginated portion of inner enamel epithelium proliferates and condense to form dental papilla.
Development of Pulp
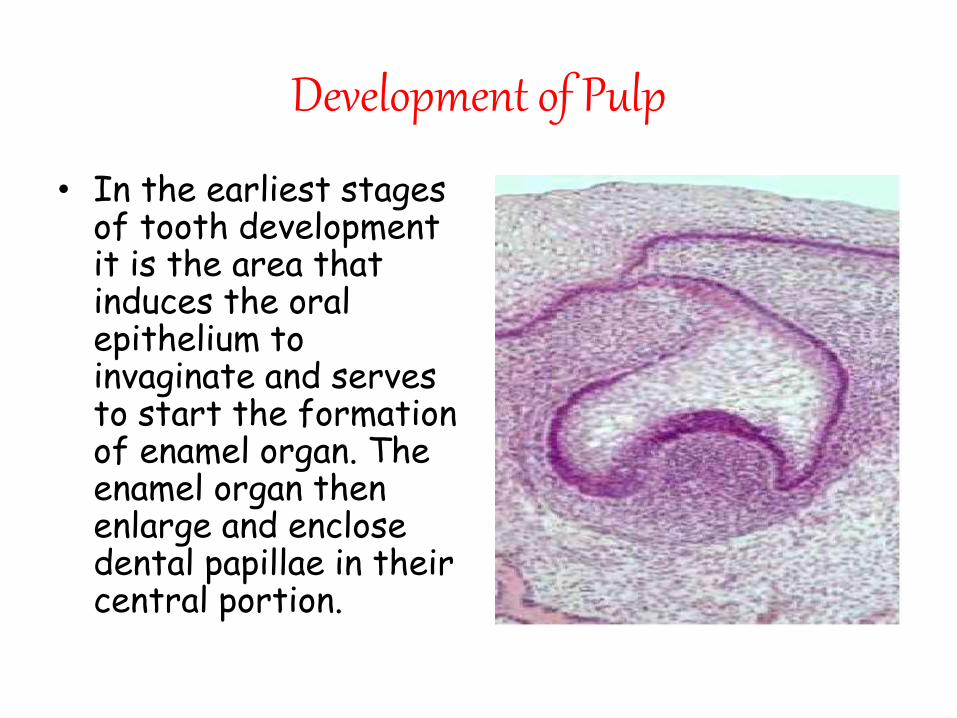
• In the earliest stages of tooth development it is the area that induces the oral epithelium to invaginate and serves to start the formation of enamel organ. The enamel organ then enlarge and enclose dental papillae in their central portion.
Development of Pulp
• The dental papilla becomes pulp only after dentin forms around it.
• After inner enamel epithelium differentiate into ameloblast, it induces the peripheral cells of dental papilla to differentiate into odontoblast and dentin formation begins. As dentin formation completed the inner portion is now called dental pulp.
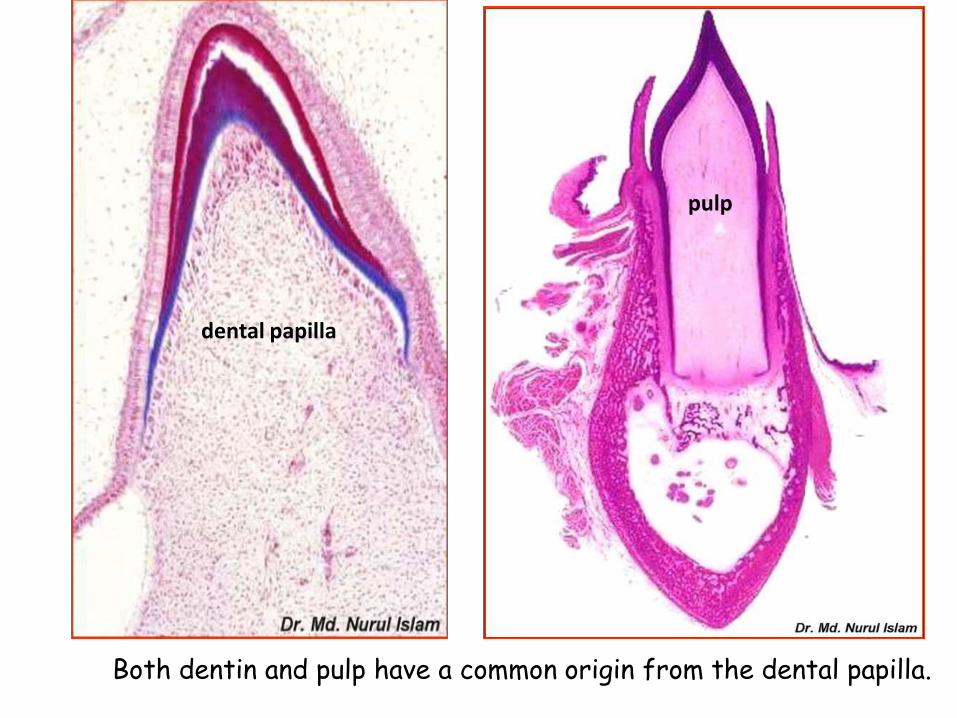
dental papilla
pulp
Both dentin and pulp have a common origin from the dental papilla.
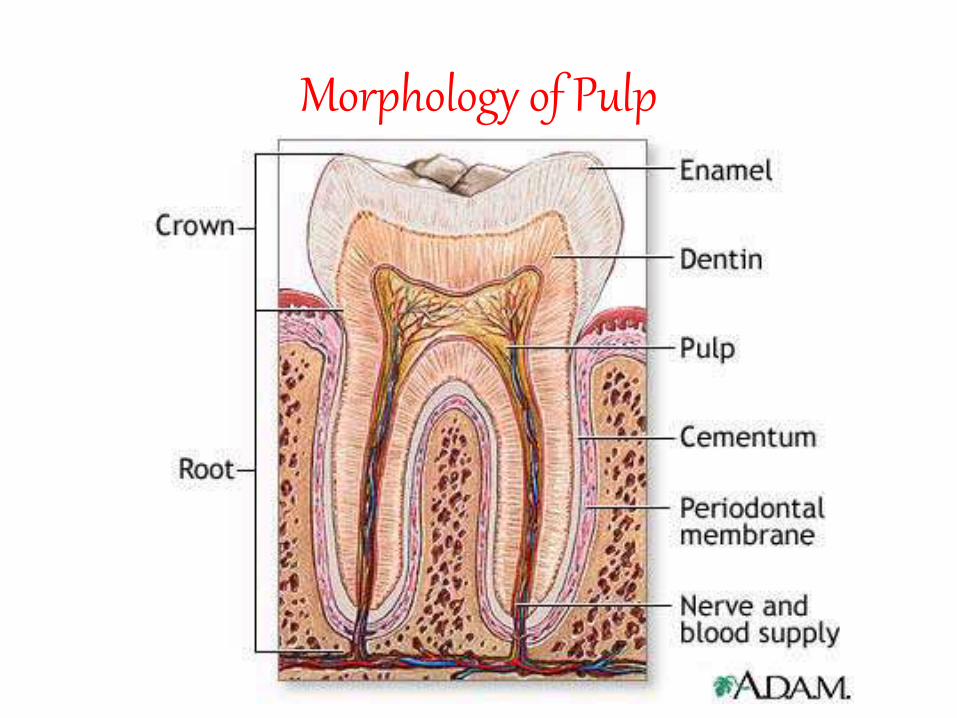
Morphology of Pulp
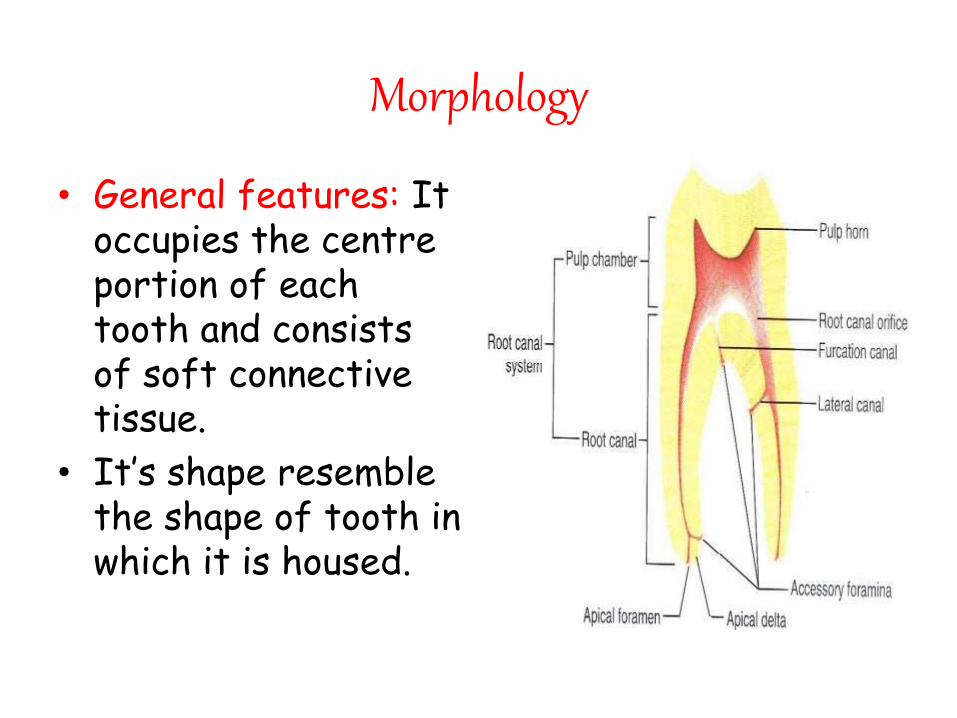
Morphology
• General features: It occupies the centre portion of each tooth and consists of soft connective tissue.
• It’s shape resemble the shape of tooth in which it is housed.
Morphology
• Every person normally has a total of 52 pulp organs, 32 in the permanent & 20 in the primary teeth.
• The total volume of all permanent teeth is 0.38cc
• The mean volume of single adult human pulp is 0.02cc
• Molar pulp are 3 to 4 times larger than incisor pulp.
• Cuspid has the longest pulp.
• Mandibular central incisor has the smallest pulp.
Pulp Space
• The entire internal space of a tooth which contains the pulp is called pulp space. It consists of the following entities.
1. Pulp chamber
2. Pulp canal
3. Pulp horn
1)Pulp chamber
• The pulp space in the crown is called pulp chamber.
• The pulp inside is called coronal pulp.
• It has six surfaces; the roof ,the floor, the mesial, the distal, the buccal and the lingual.
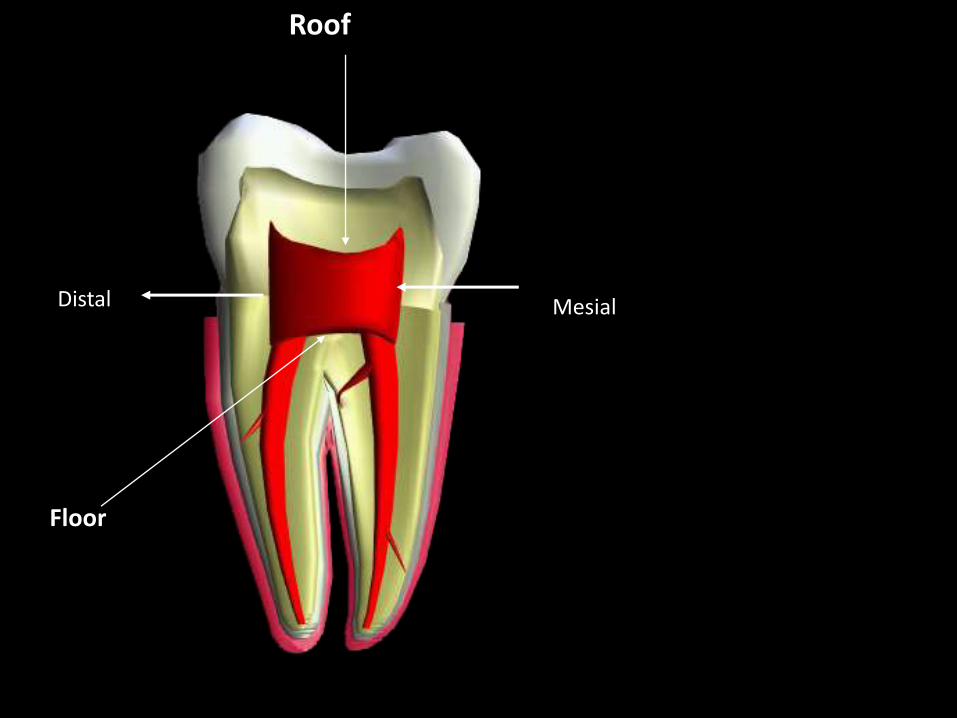
Floor
Roof
MesialDistal
2)Pulp canal (root canal)
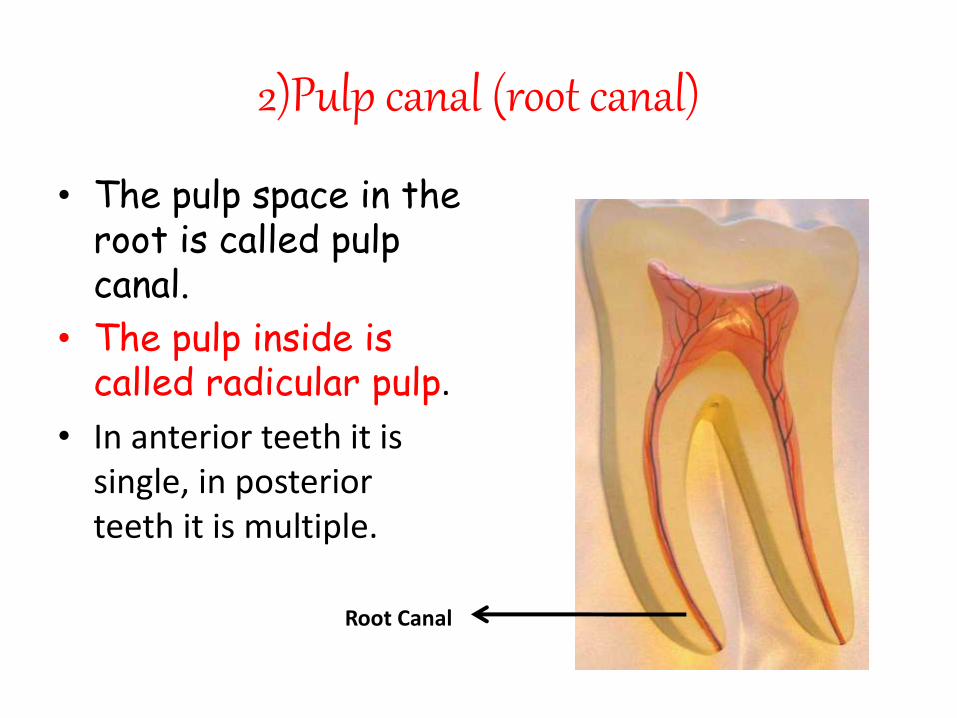
• The pulp space in the root is called pulp canal.
• The pulp inside is called radicular pulp.
• In anterior teeth it is single, in posterior teeth it is multiple.
Root Canal
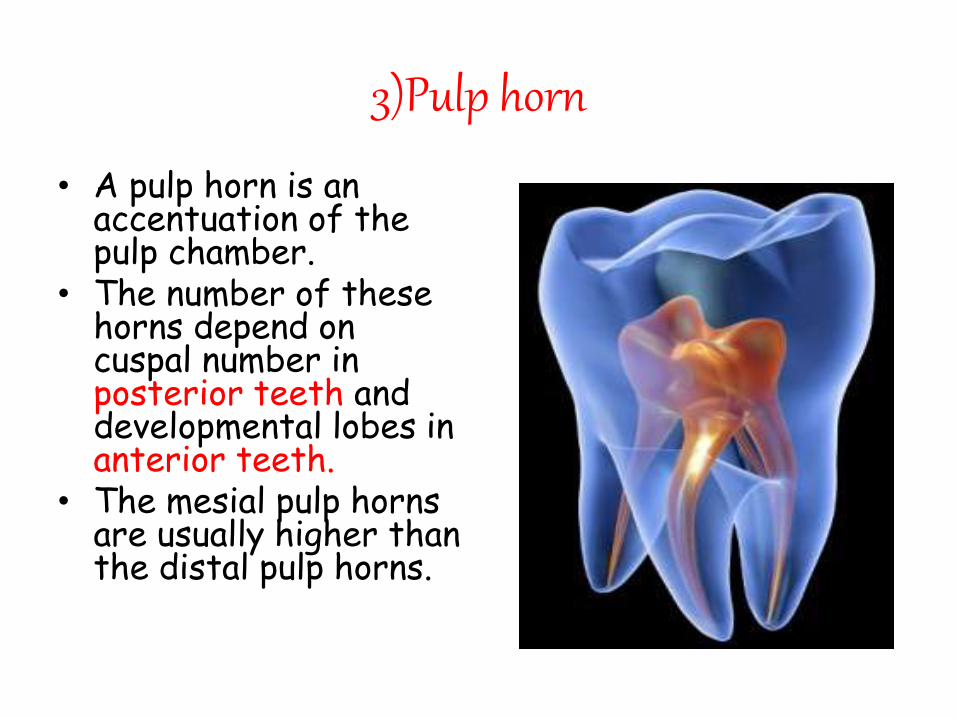
3)Pulp horn
• A pulp horn is an accentuation of the pulp chamber.
• The number of these horns depend on cuspal number in posterior teeth and developmental lobes in anterior teeth.
• The mesial pulp horns are usually higher than the distal pulp horns.
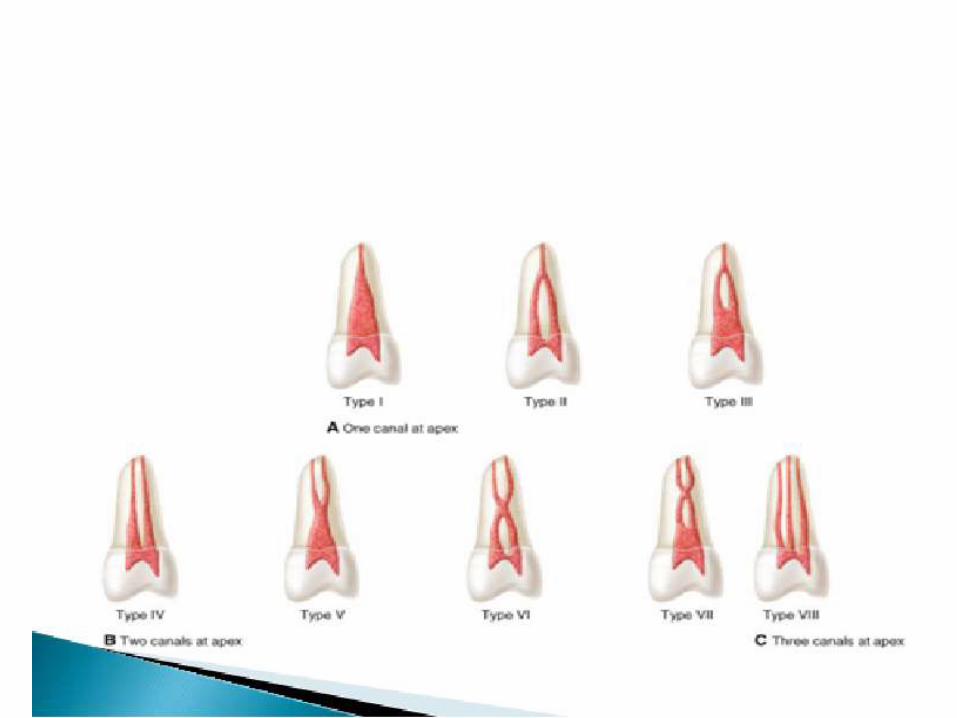
Classification of pulp space
• They are classified by F.J.Vertucci’sinto following 8 types.
• One canal at apexType I – TypeIII
• Two canals at apexType IV – Type VII
• Three canals at apexType VIII
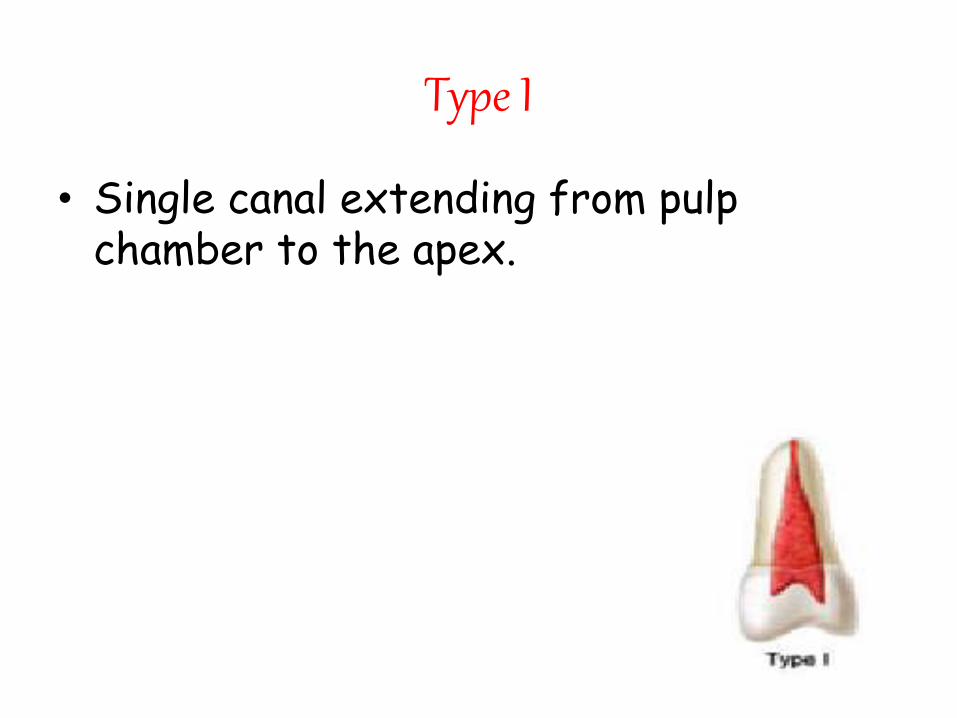
Type I
• Single canal extending from pulp chamber to the apex.
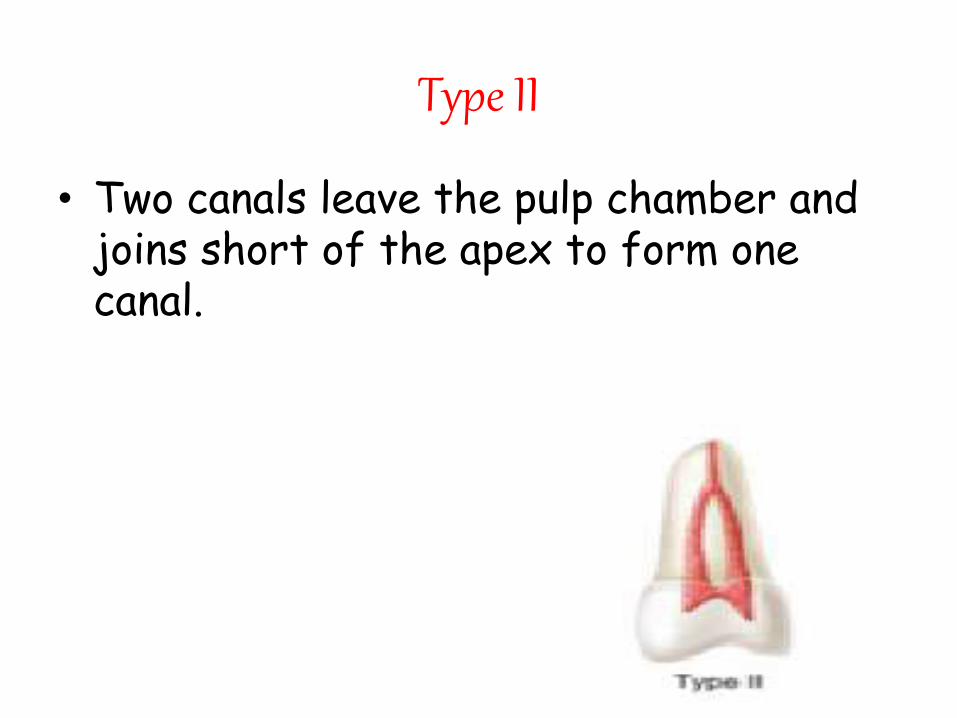
Type II
• Two canals leave the pulp chamber and joins short of the apex to form one canal.
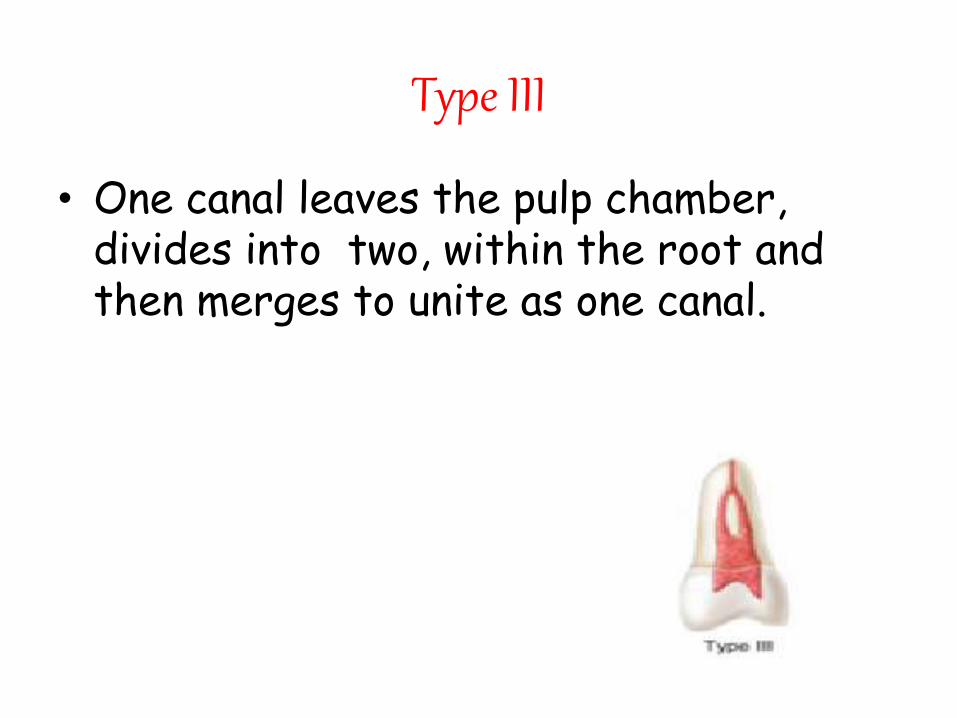
Type III
• One canal leaves the pulp chamber, divides into two, within the root and then merges to unite as one canal.
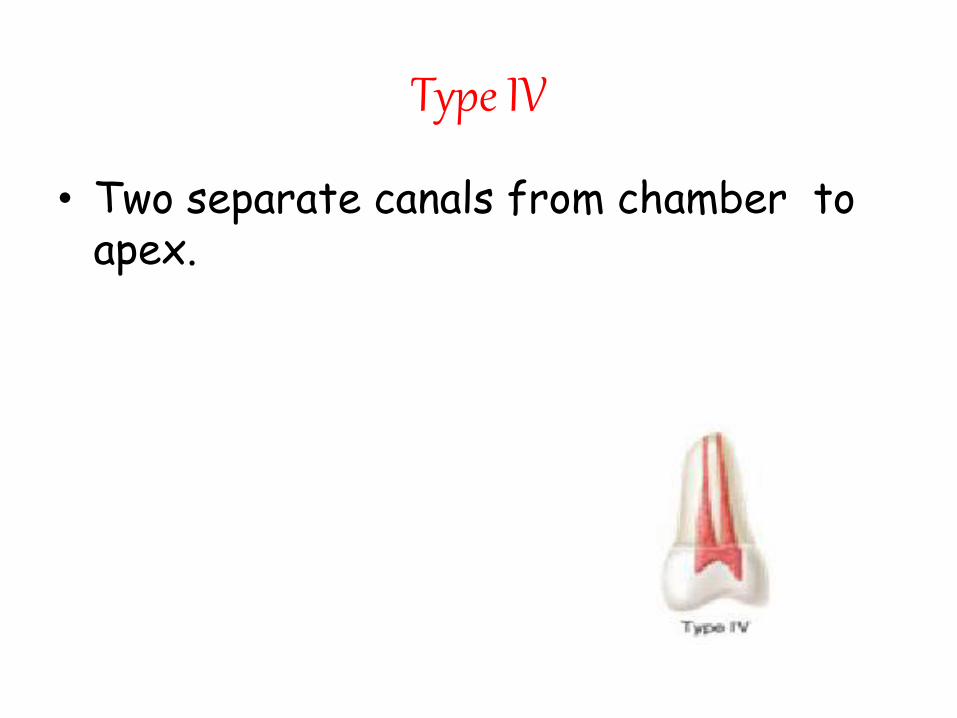
Type IV
• Two separate canals from chamber to apex.
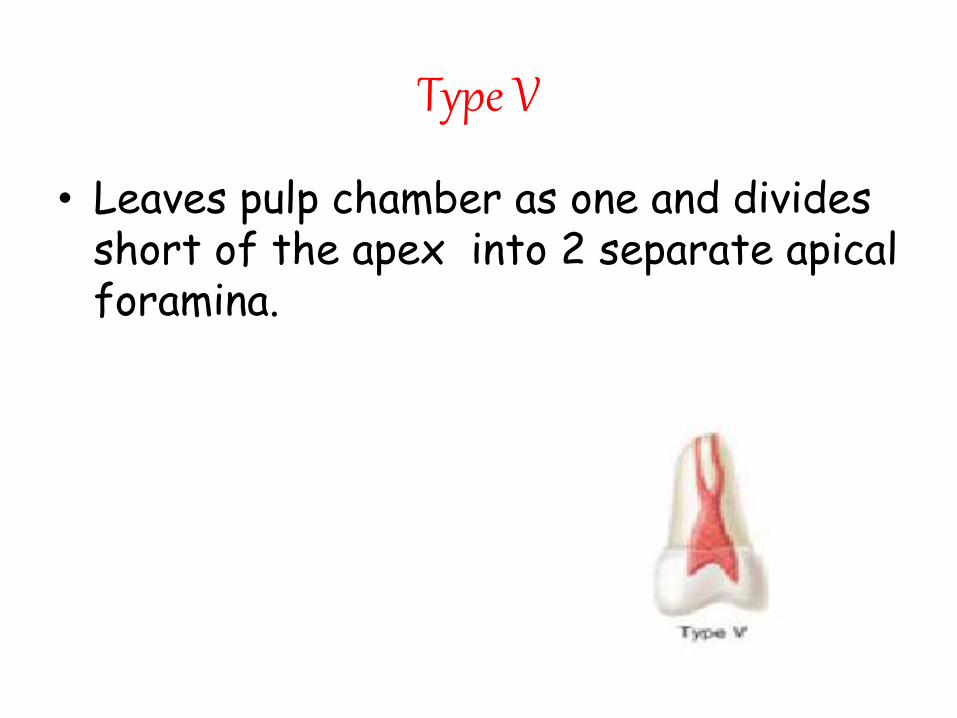
Type V
• Leaves pulp chamber as one and divides short of the apex into 2 separate apical foramina.
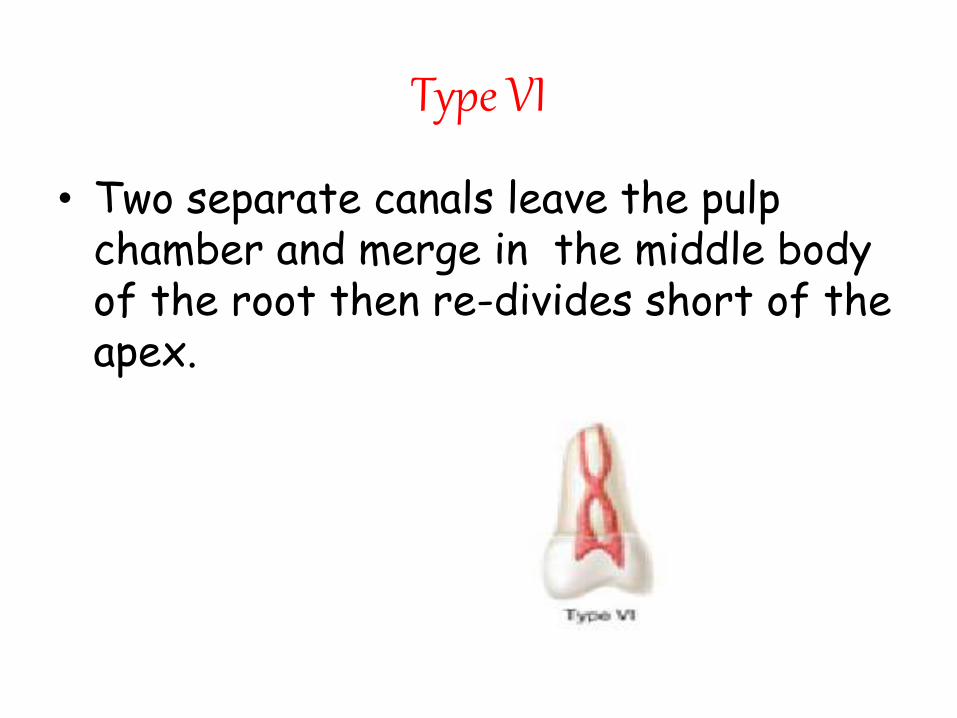
Type VI
• Two separate canals leave the pulp chamber and merge in the middle body of the root then re-divides short of the apex.
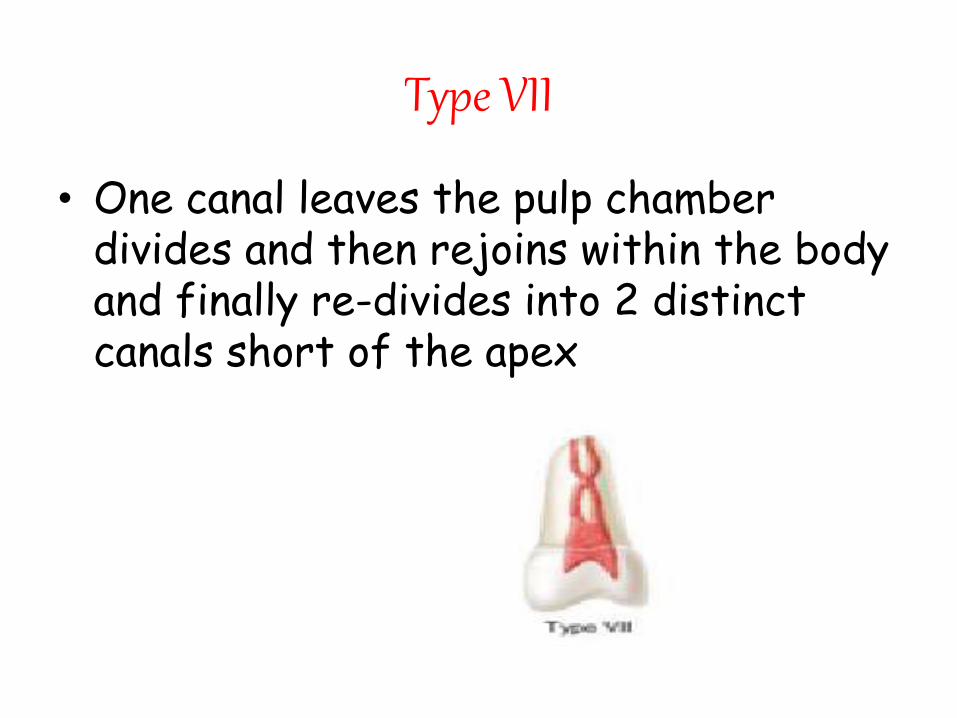
Type VII
• One canal leaves the pulp chamber divides and then rejoins within the body and finally re-divides into 2 distinct canals short of the apex
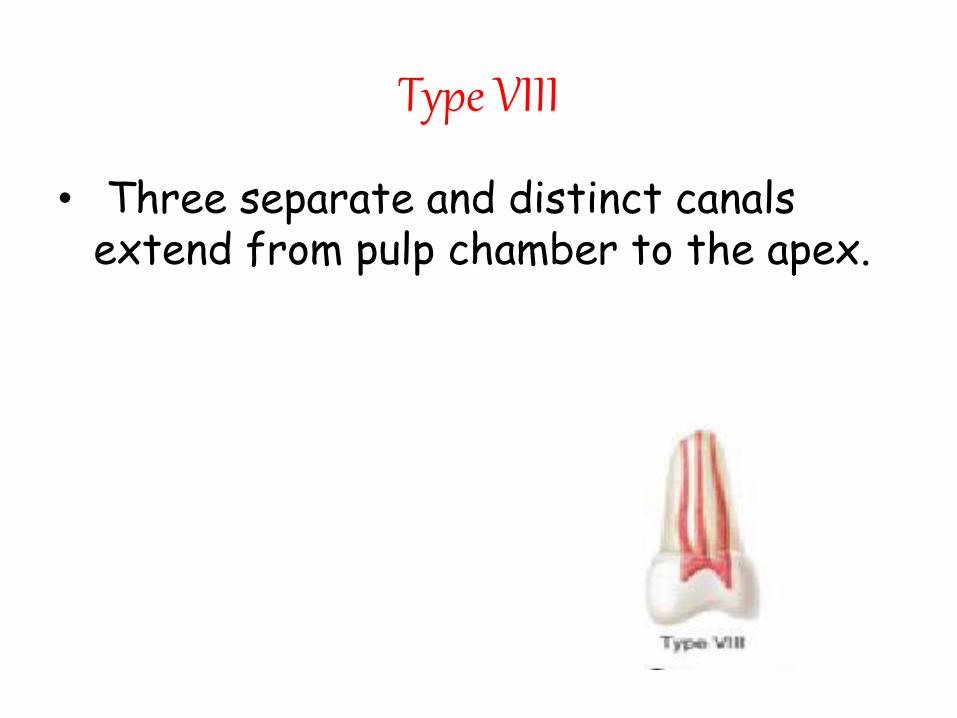
Type VIII
• Three separate and distinct canals extend from pulp chamber to the apex.
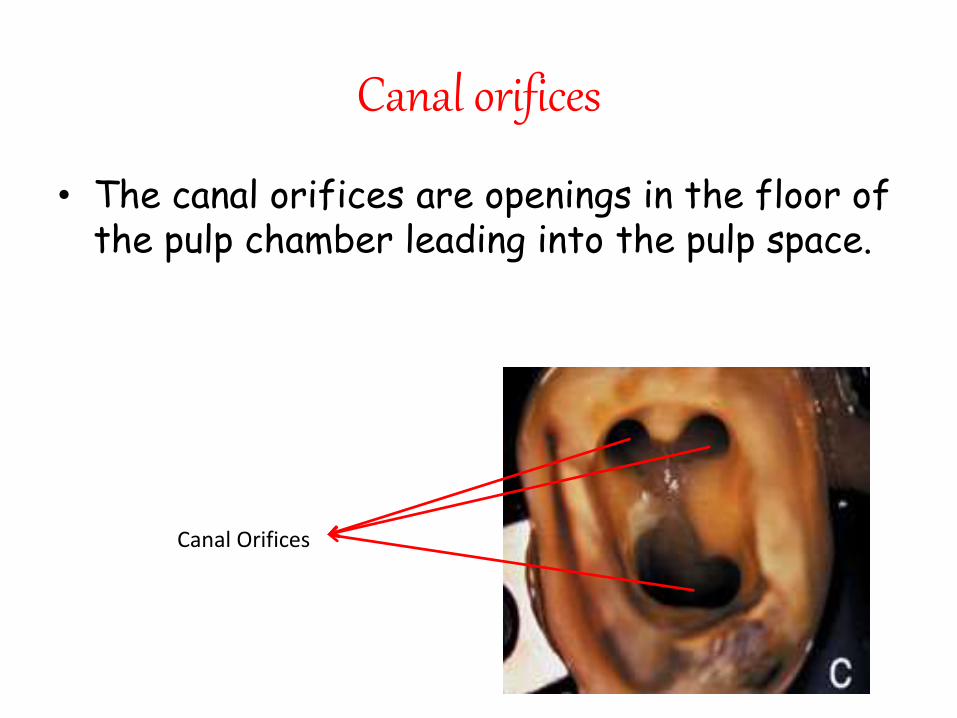
Canal orifices
• The canal orifices are openings in the floor of the pulp chamber leading into the pulp space.
Canal Orifices
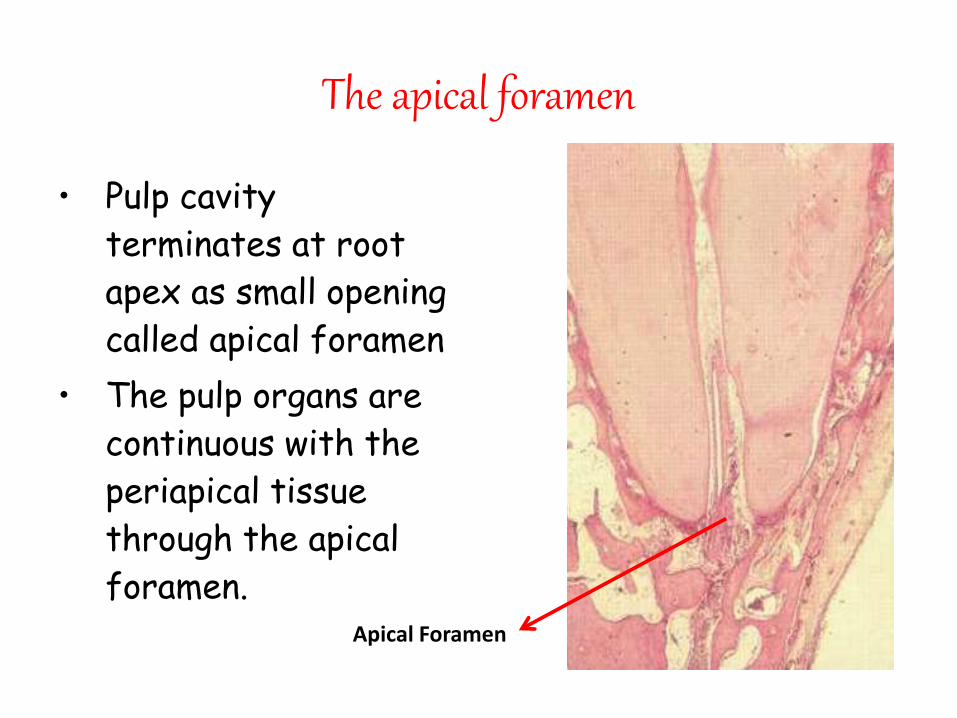
The apical foramen
• Pulp cavity
terminates at root
apex as small opening
called apical foramen
• The pulp organs are
continuous with the
periapical tissue
through the apical
foramen.Apical Foramen
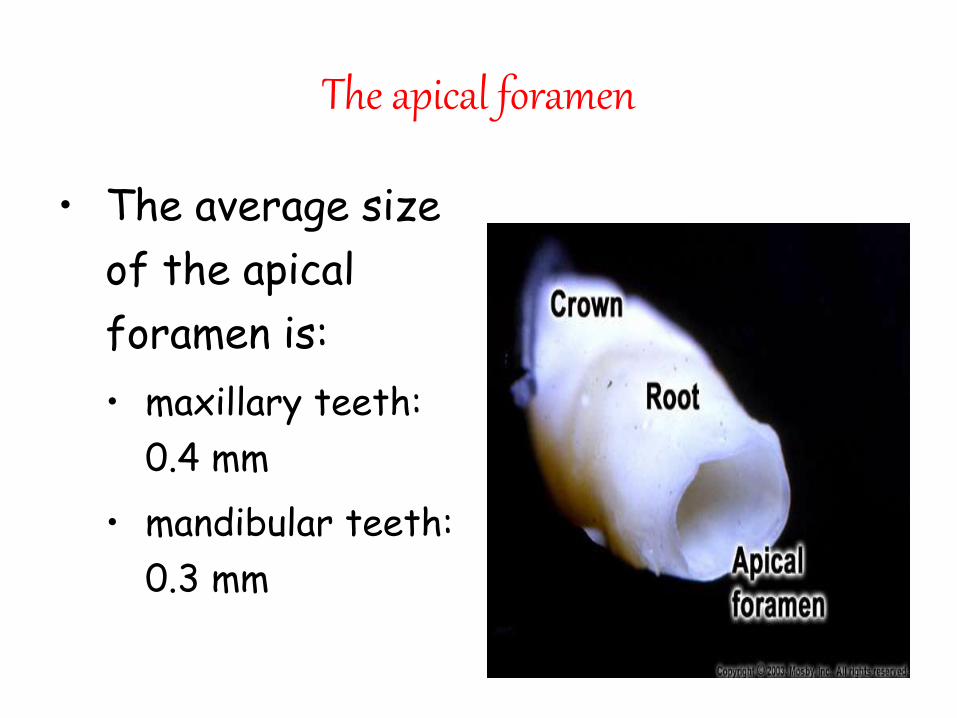
The apical foramen
• The average size
of the apical
foramen is:
• maxillary teeth:
0.4 mm
• mandibular teeth:
0.3 mm
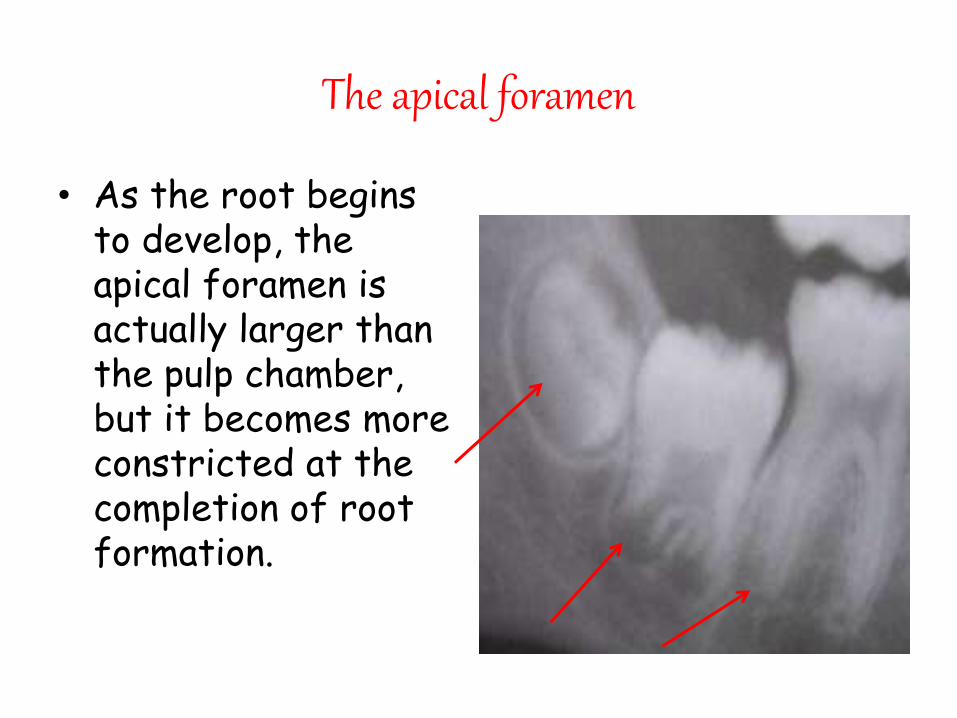
The apical foramen
• As the root begins to develop, the apical foramen is actually larger than the pulp chamber, but it becomes more constricted at the completion of root formation.
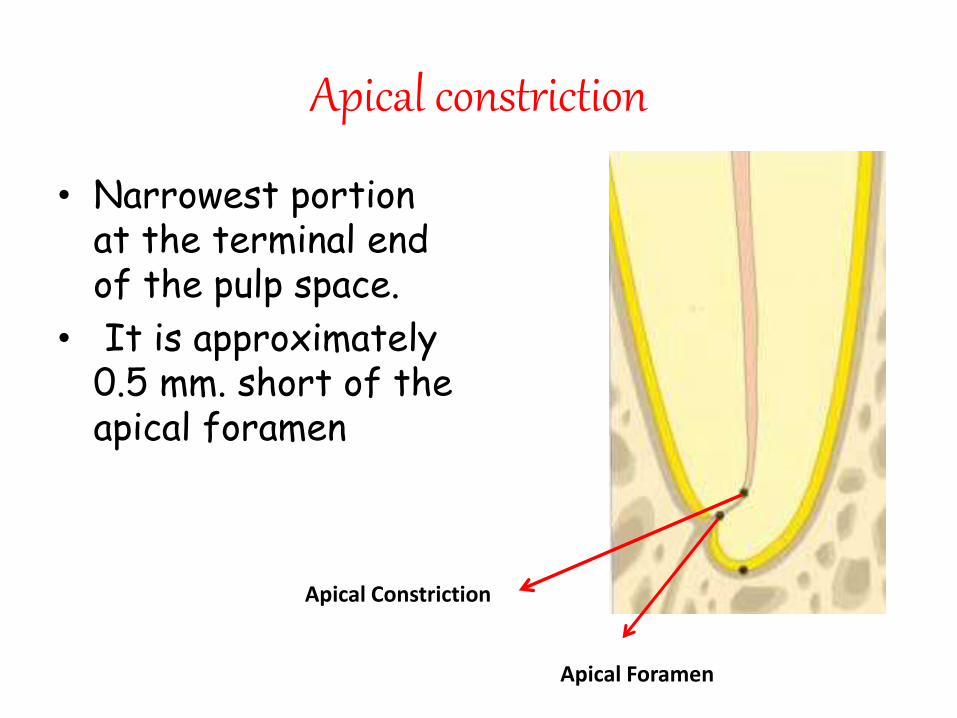
Apical constriction
• Narrowest portion at the terminal end of the pulp space.
• It is approximately 0.5 mm. short of the apical foramen
Apical Constriction
Apical Foramen
Accessory canal
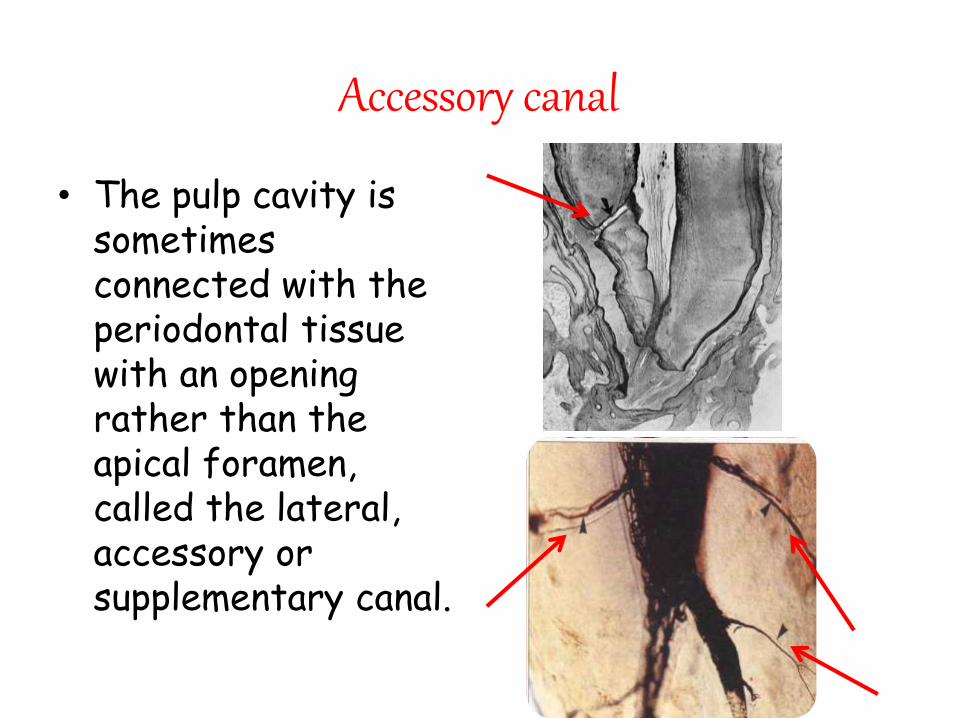
• The pulp cavity is sometimes connected with the periodontal tissue with an opening rather than the apical foramen, called the lateral, accessory or supplementary canal.
Accessory canal
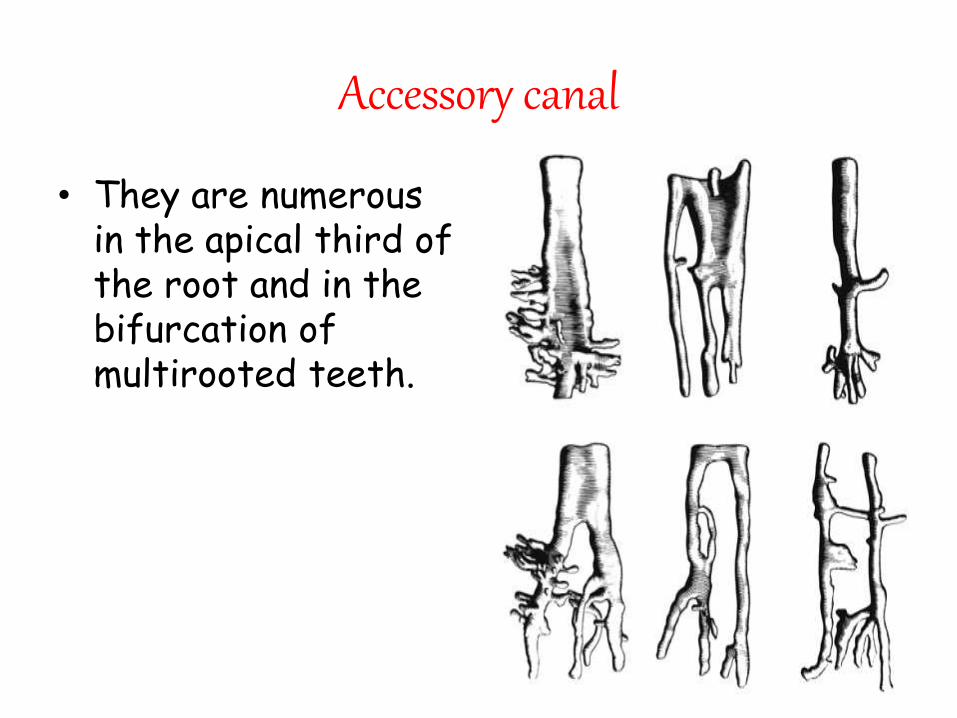
• They are numerous in the apical third of the root and in the bifurcation of multirooted teeth.
Delta System
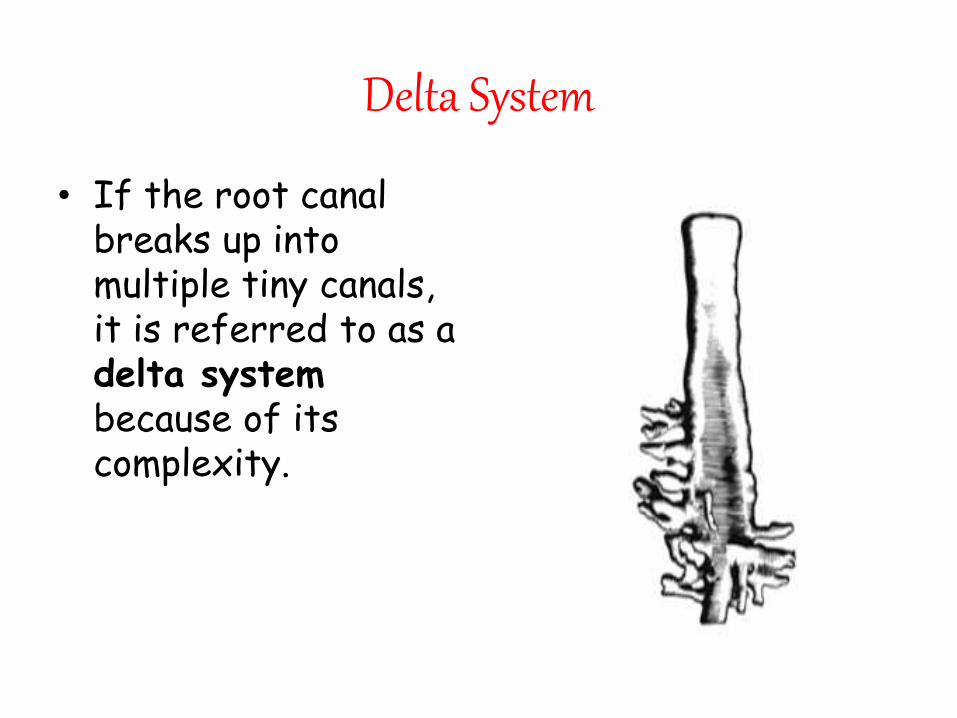
• If the root canal breaks up into multiple tiny canals, it is referred to as a delta systembecause of its complexity.
Etiology of accessory canals
1. Degeneration of the epithelial root
sheath of Hertwig before odontoblasts
differentiation.
2. Large blood vessel disturbs the course
of the root sheath.
Functions
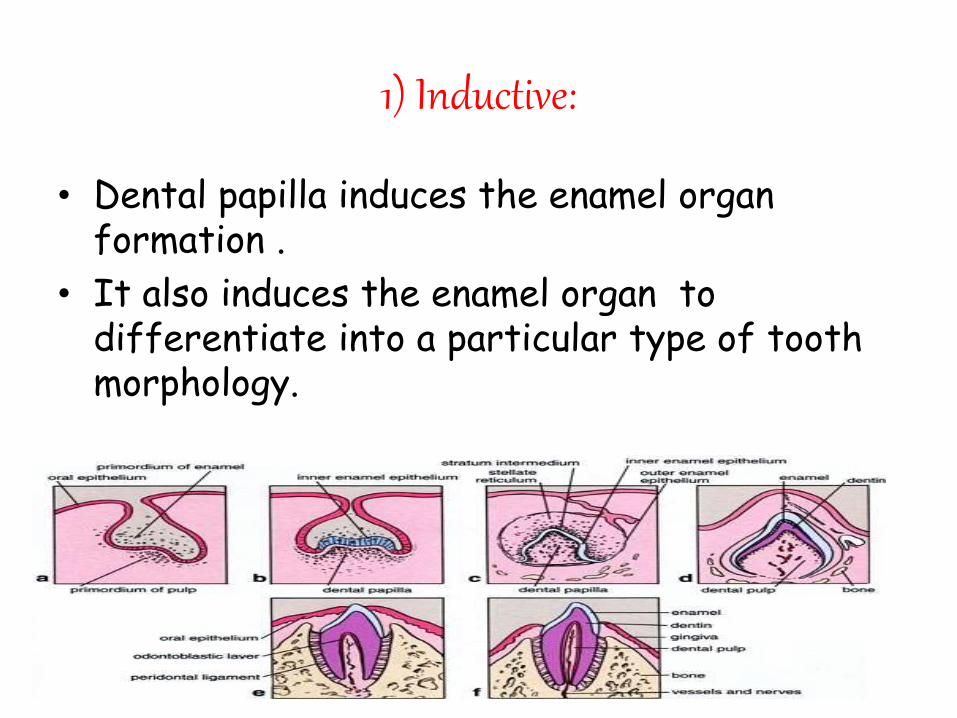
1) Inductive:
• Dental papilla induces the enamel organ formation .
• It also induces the enamel organ to differentiate into a particular type of tooth morphology.
2) Formative
• The cells of Pulp induces dentin formation.
• This involves formation of primary and secondary dentin.
• The primary dentin is tubular and regularly arranged, formed before root closure.
• Secondary dentin contain fewer tubules and is formed after root closure.
NutritiveDental pulp maintains the vitality of dentin by providing O2 and nutrients to the odontoblasts.Nutrition is made possible by rich peripheral capillary network.
Protective
• Pulp helps in recognition of stimuli like heat, cold,pressure,chemicals by way of sensory nerve fibres.
• Vasomotor innervation controls the muscular wall of blood vessels. This regulates the blood volume and rate of blood flow and hence the intrapulpal pressure.
5- Defense:
The pulp responds to irritation by producing reparative dentin and mineralizing any affected dentinal tubules. These reparative reactions are an attempt to wall off the pulp from the source of irritation. The presence of macrophages, lymphocytes and leucocytes aid in the process of repair of the pulp.
HISTOLOGY OF PULP
By
Humayun Afridi
HISTOLOGY
• When the pulp is examined microscopically four distinct zones can be distinguished from outer to inner.
o The odontoblastic zone.
o The cell free zone or Weil’s zone.
o The cell rich zone.
o The central zone.
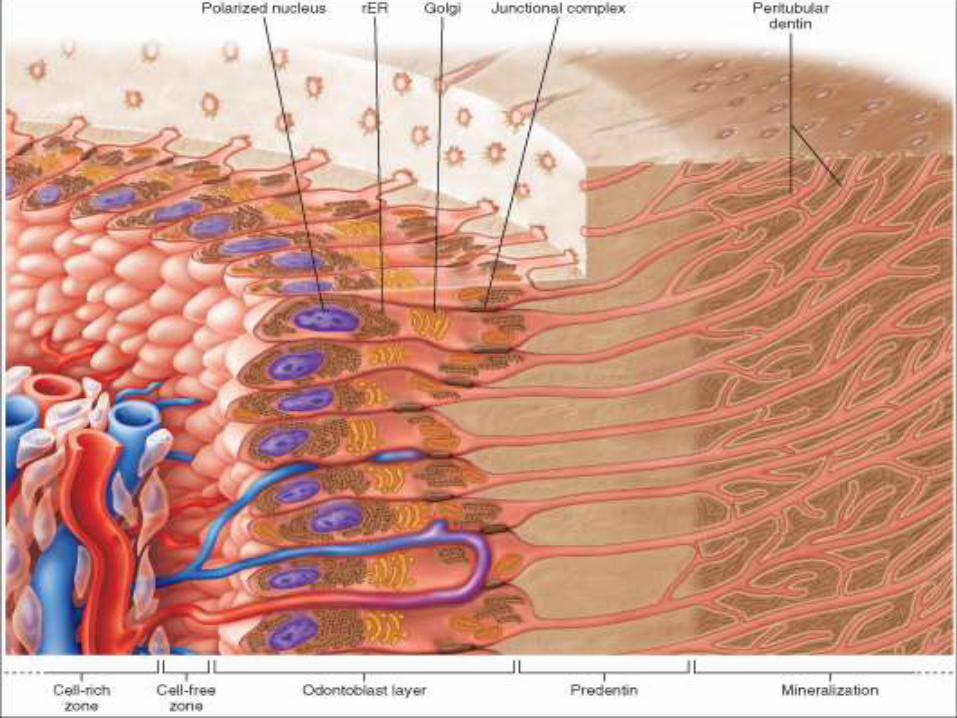
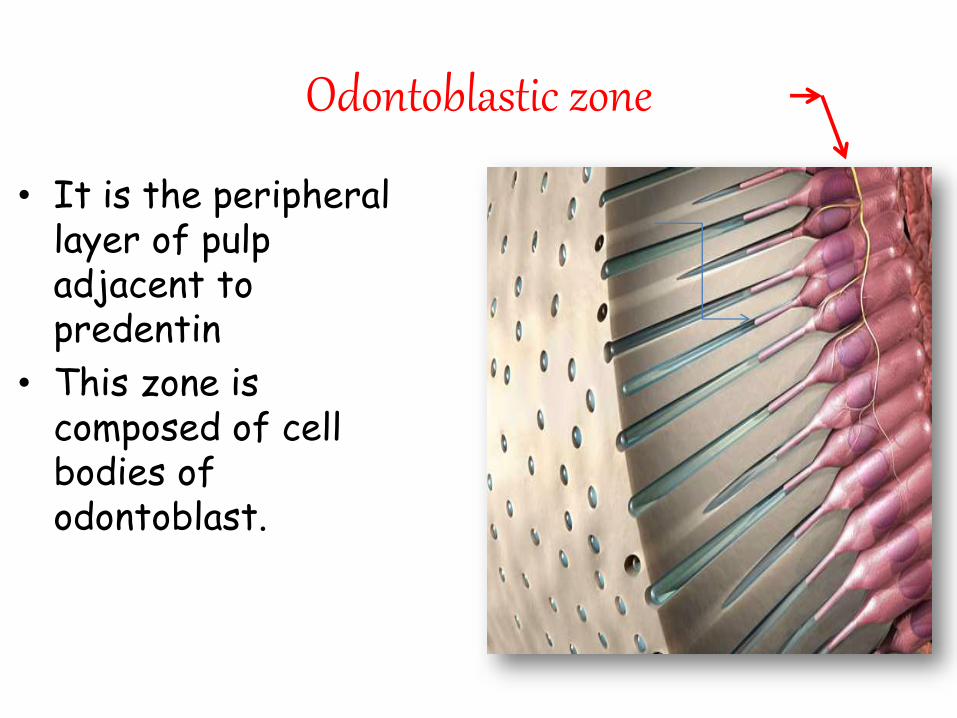
Odontoblastic zone
• It is the peripheral layer of pulp adjacent to predentin
• This zone is composed of cell bodies of odontoblast.
Cell free zone (weil’s zone)
• It is also called weil’s zone
• 40 microns wide & relativelyfree of cells, Traversed by
1. blood vessels
2. unmyelinated nerves
3.cytoplasmic process offibroblasts
• This zone is found below theodontoblastic zone
• Represents the space intowhich odontoblasts moveduring tooth development.
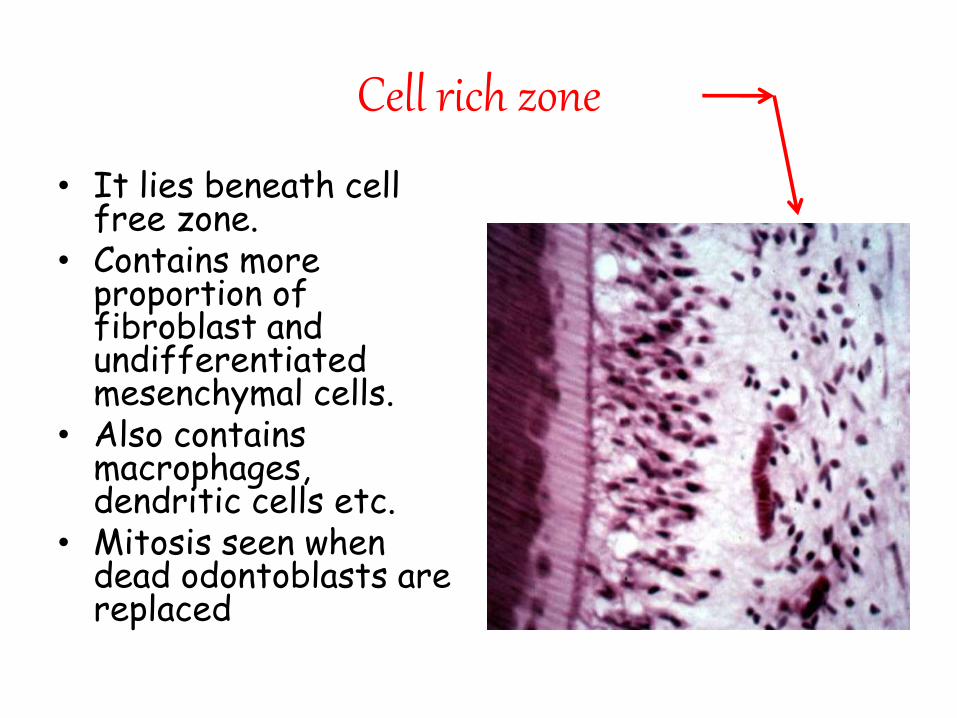
Cell rich zone
• It lies beneath cell free zone.
• Contains more proportion of fibroblast and undifferentiated mesenchymal cells.
• Also contains macrophages, dendritic cells etc.
• Mitosis seen when dead odontoblasts are replaced
Central zone
• This zone is also called pulp core
• It contains blood vessels and nerves embedded in the pulp matrix together with fibroblasts.
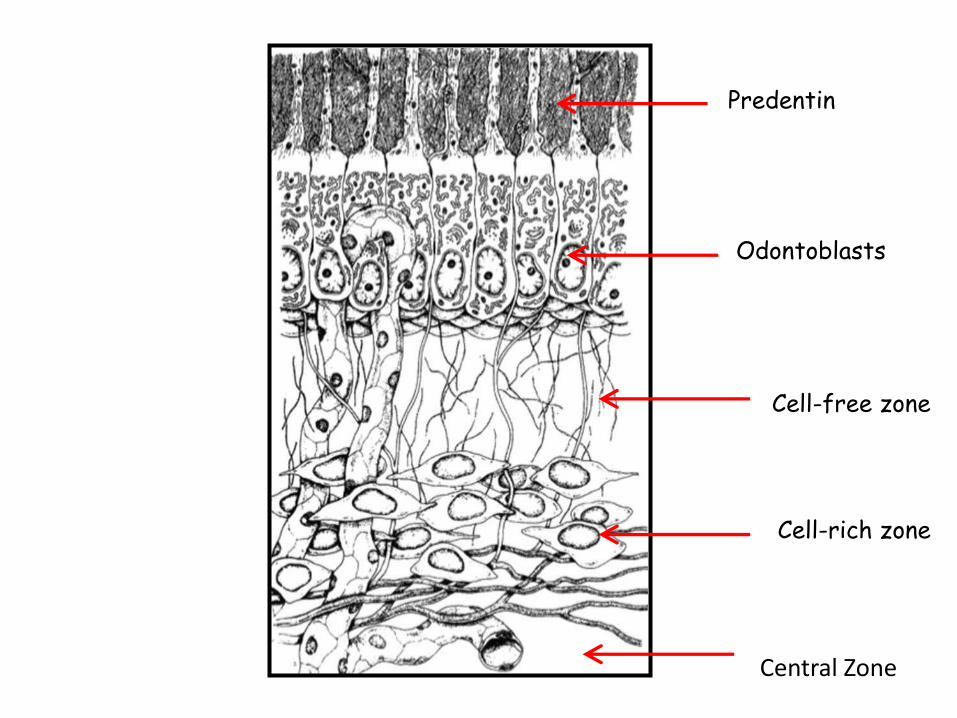
Odontoblasts
Predentin
Cell-free zone
Cell-rich zone
Central Zone
Components of Pulp
• As it is a connective tissue, it contains the following components.
• 1) Cellular elements :
a. Formative cells : Odontoblast, Fibroblast .
b. Progenitor cells : Undifferentiated mesenchymal
cells .
c. Defensive cells : Macrophages, neutrophils,
eosinophils, basophils, mast cells , plasma cells and
Lymphocytes. • 2) Matrix• 3) Neurovascular elements :
•CELLULAR ELEMENTS
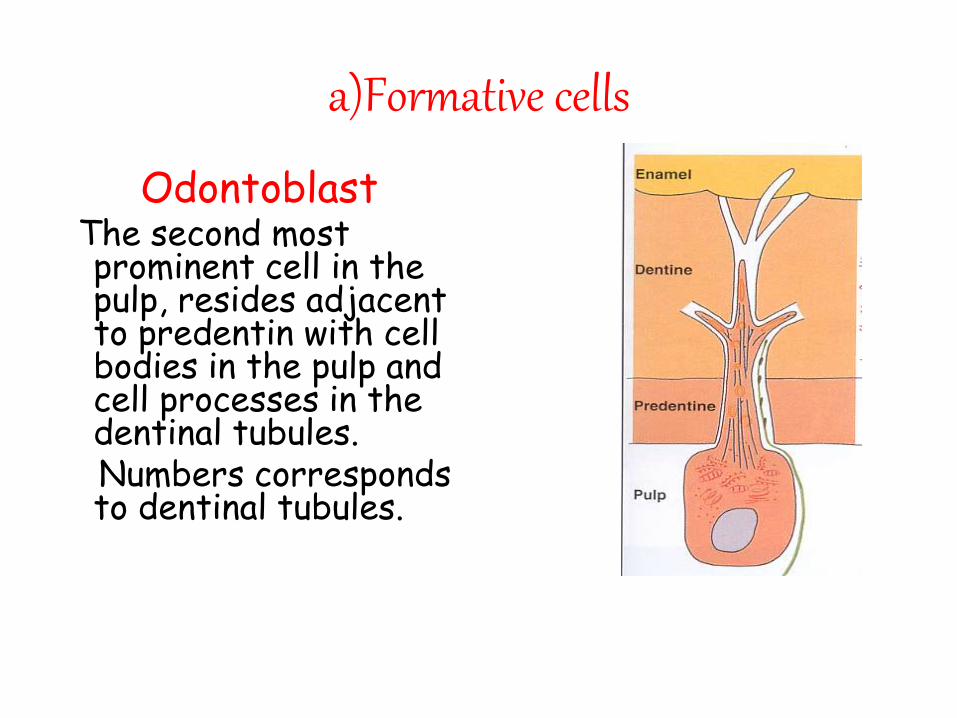
a)Formative cells
OdontoblastThe second most prominent cell in the pulp, resides adjacent to predentin with cell bodies in the pulp and cell processes in the dentinal tubules.Numbers corresponds to dentinal tubules.
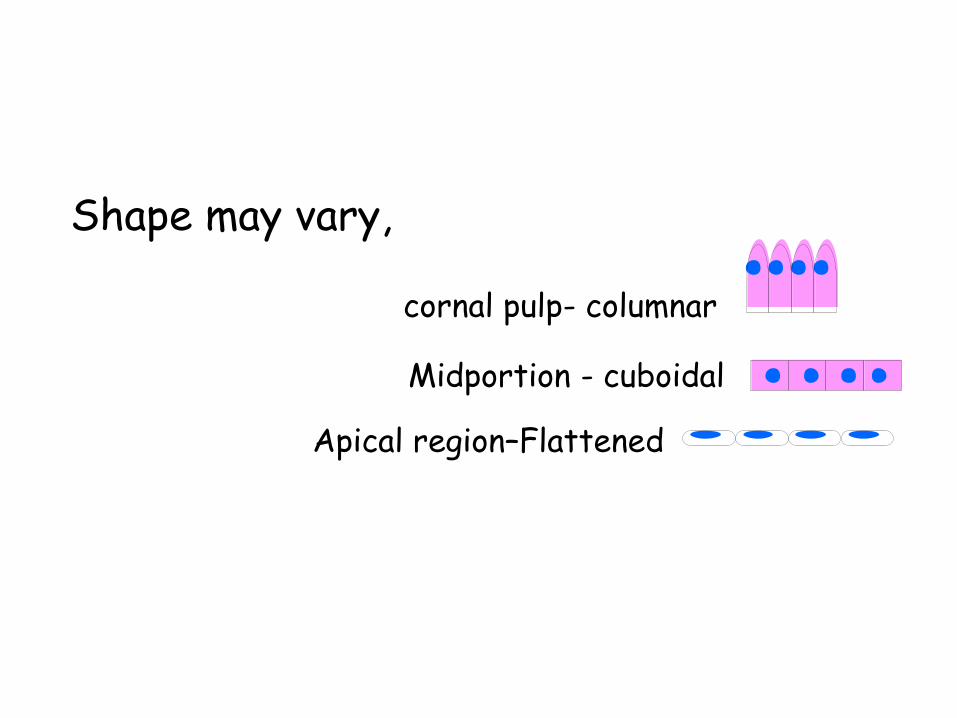
Shape may vary,
cornal pulp- columnar
Midportion - cuboidal
Apical region–Flattened
Function of odontoblast
• It’s main function is dentin formation.
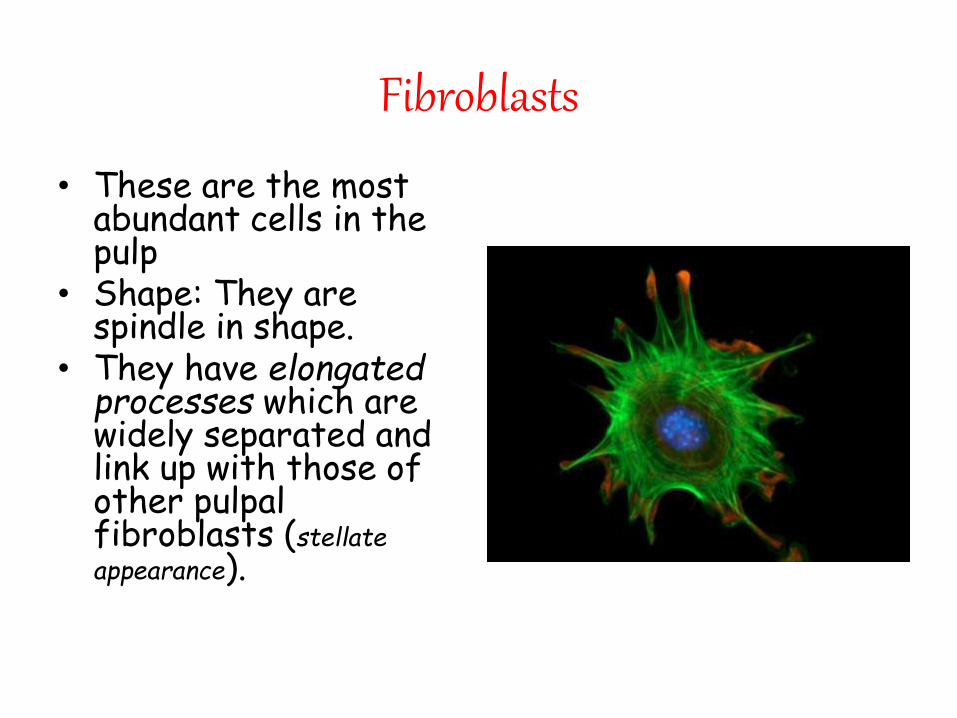
Fibroblasts
• These are the most abundant cells in the pulp
• Shape: They are spindle in shape.
• They have elongated processes which are widely separated and link up with those of other pulpalfibroblasts (stellateappearance).
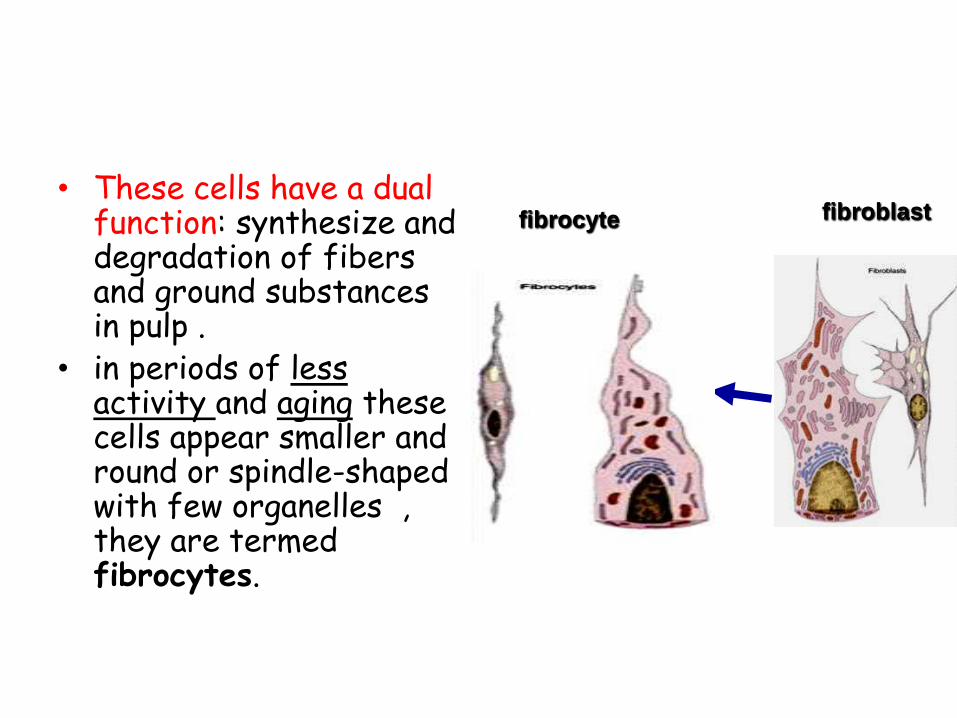
• These cells have a dual function: synthesize and degradation of fibers and ground substances in pulp .
• in periods of less activity and aging these cells appear smaller and round or spindle-shaped with few organelles , they are termed fibrocytes.
fibroblastfibrocyte
• Progenitor cells
(The undifferentiated mesenchymal cells):
They are smaller than fibroblasts but have a similar appearance.
They are usually found along the walls of blood vessels.
These cells have the potentiality of forming other types of formative or defensive connective tissue cells.

• DEFENSE CELLS
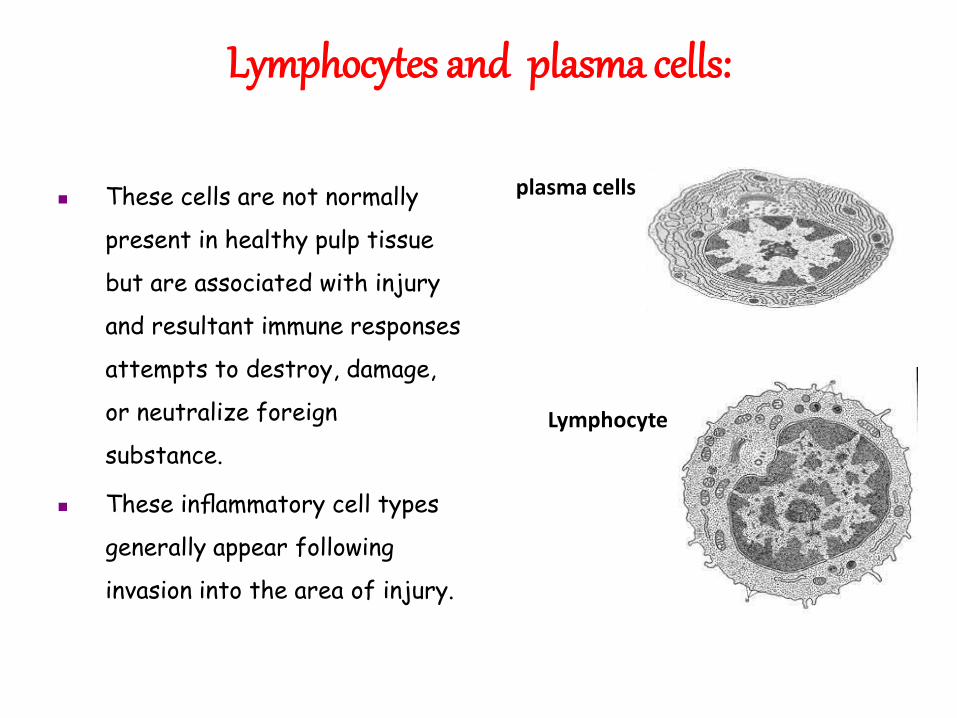
Lymphocytes and plasma cells:
These cells are not normally
present in healthy pulp tissue
but are associated with injury
and resultant immune responses
attempts to destroy, damage,
or neutralize foreign
substance.
These inflammatory cell types
generally appear following
invasion into the area of injury.
plasma cells
Lymphocyte
Macrophages
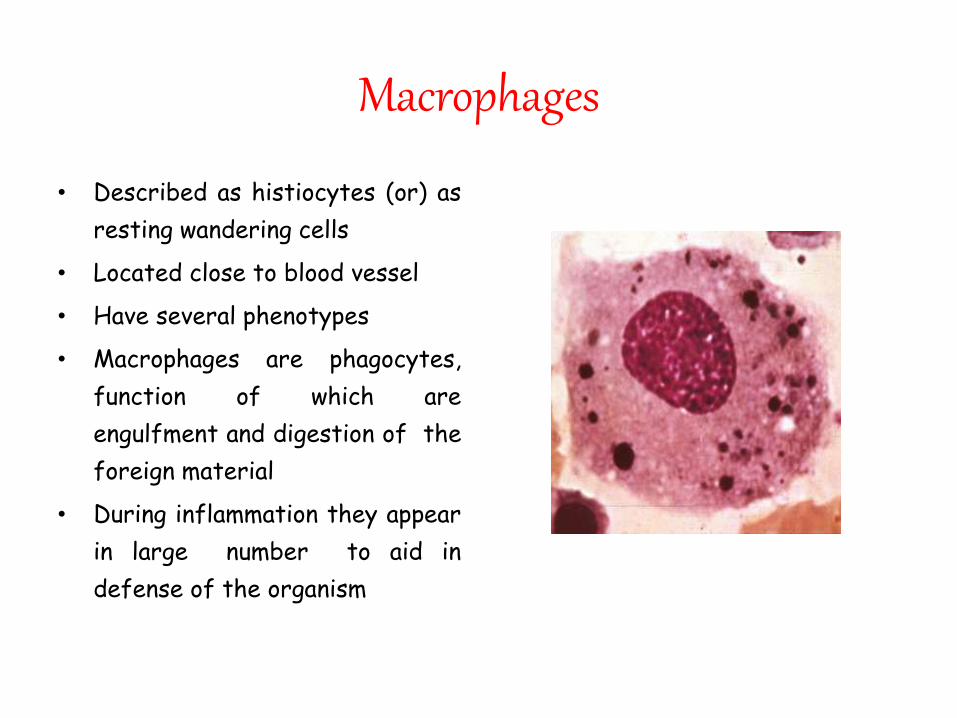
• Described as histiocytes (or) as
resting wandering cells
• Located close to blood vessel
• Have several phenotypes
• Macrophages are phagocytes,
function of which are
engulfment and digestion of the
foreign material
• During inflammation they appear
in large number to aid in
defense of the organism
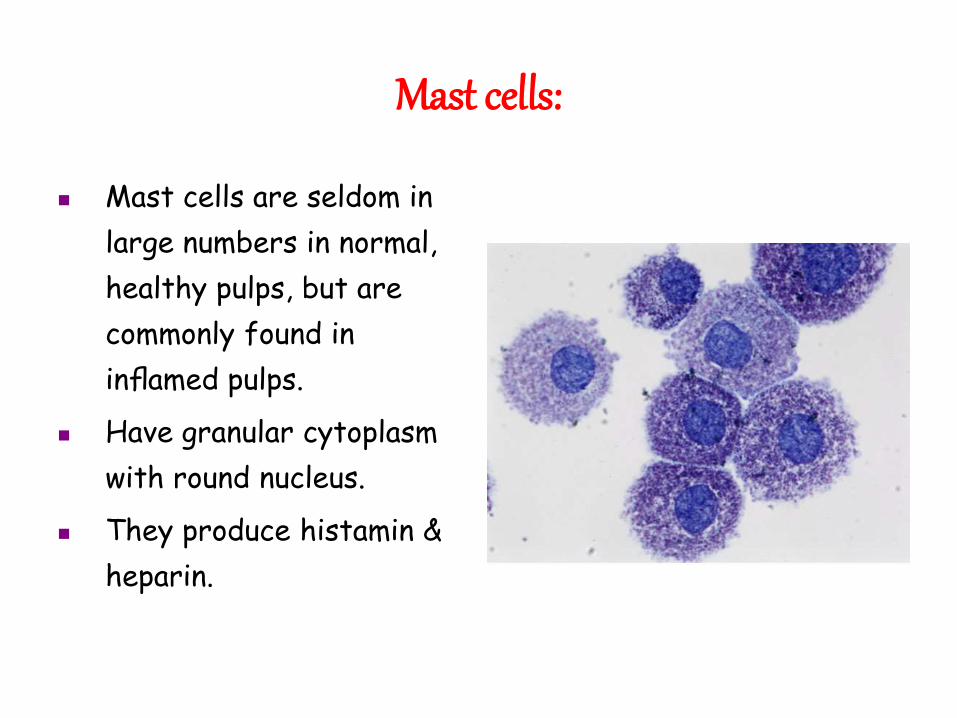
Mast cells:
Mast cells are seldom in
large numbers in normal,
healthy pulps, but are
commonly found in
inflamed pulps.
Have granular cytoplasm
with round nucleus.
They produce histamin &
heparin.
Matrix
• COLLAGEN
• ELASTIN
• FIBRONECTIN
• LAMILIN
GAG PR OTEOGLYCAN
FIBRES
• Mainly collagen fibre are type I and type III.
These fibers form a loose, reticular network to
support other structural elements of the pulp.
Collagen is synthesized and secreted by
odontoblasts and fibroblasts.
In young pulp the fibers are relatively sparse
throughout the pulp and gradually the bundles
increase in size with advancing age.
Collagen fibres
GROUND SUBSTANCE
The ground substances resembles that of other
loose connective tissue.
It consists of acid mucopolysaccharides, neutral
glycoprotein and water.
It acts as a medium for the transport of nutrients.
THE Pulp is a small tissue with a big issue
I.B.Bender
VASCULATURE OF PULP
SAQIB HABIB / KHYBER COLLEGE OF DENTISTRY
BLOOD SUPPLY
• Extensive blood supply.
• Mainly supplied through inferior & superior alveolar arteries.
• Entry through apical foramina
accompained by nerve bundles
• Rapid blood flow High blood
Pressure than rest of body
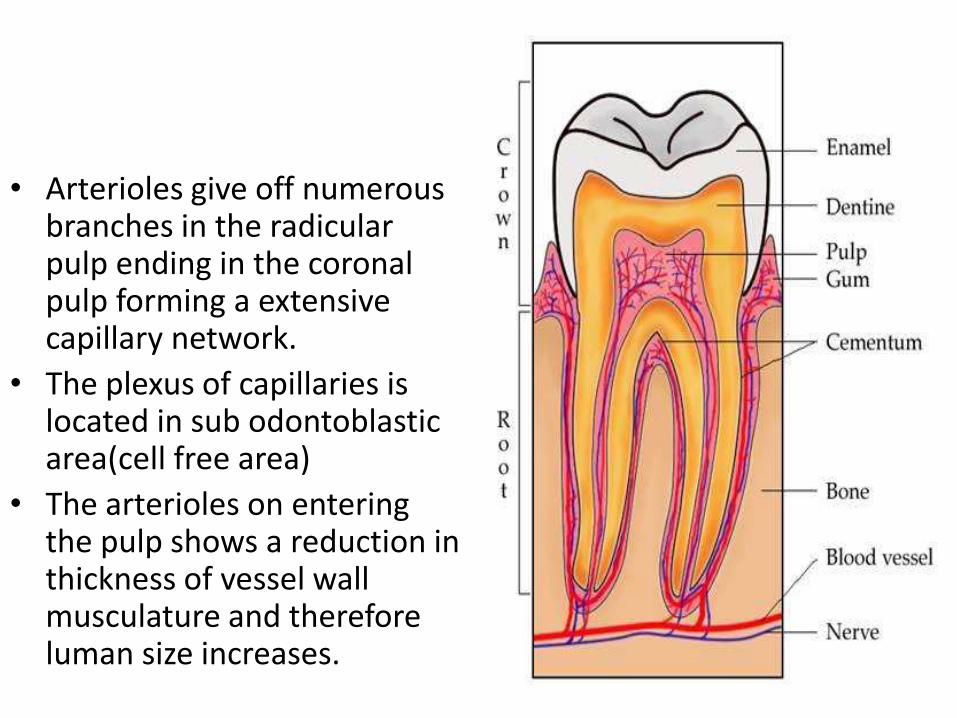
• Arterioles give off numerous branches in the radicularpulp ending in the coronal pulp forming a extensive capillary network.
• The plexus of capillaries is located in sub odontoblasticarea(cell free area)
• The arterioles on entering the pulp shows a reduction in thickness of vessel wall musculature and therefore luman size increases.
• Rate of blood flow in the pulp of tooth is four times the rate of blood flow in resting muscle
• Laser doppler flowmetry is device which measures pulpal blood flow(pulp vitality)
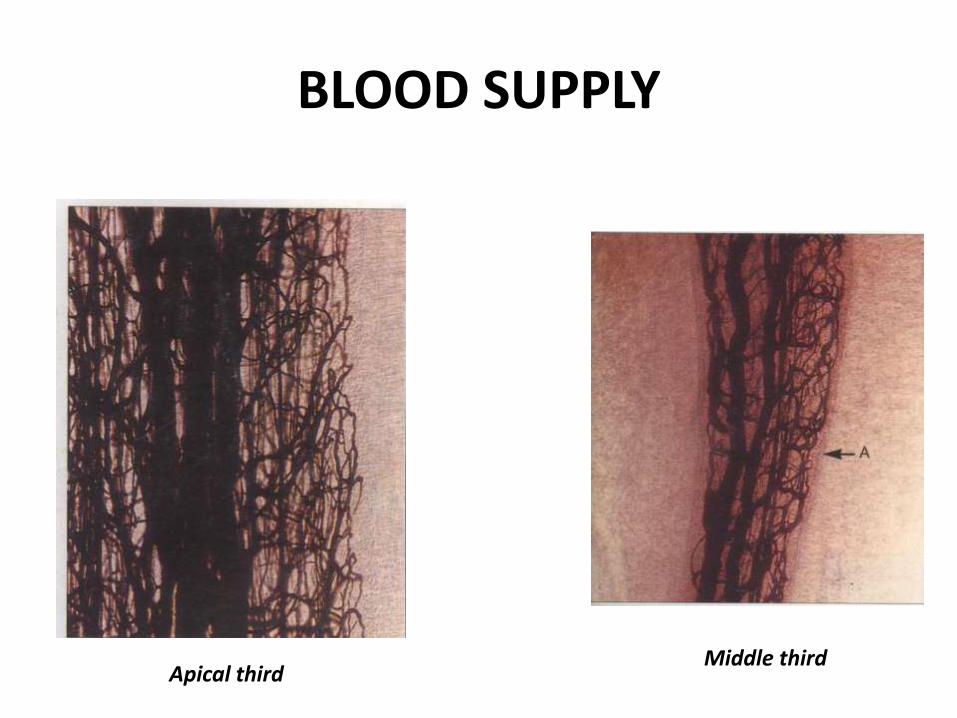
BLOOD SUPPLY
Apical thirdMiddle third
INNERVATION
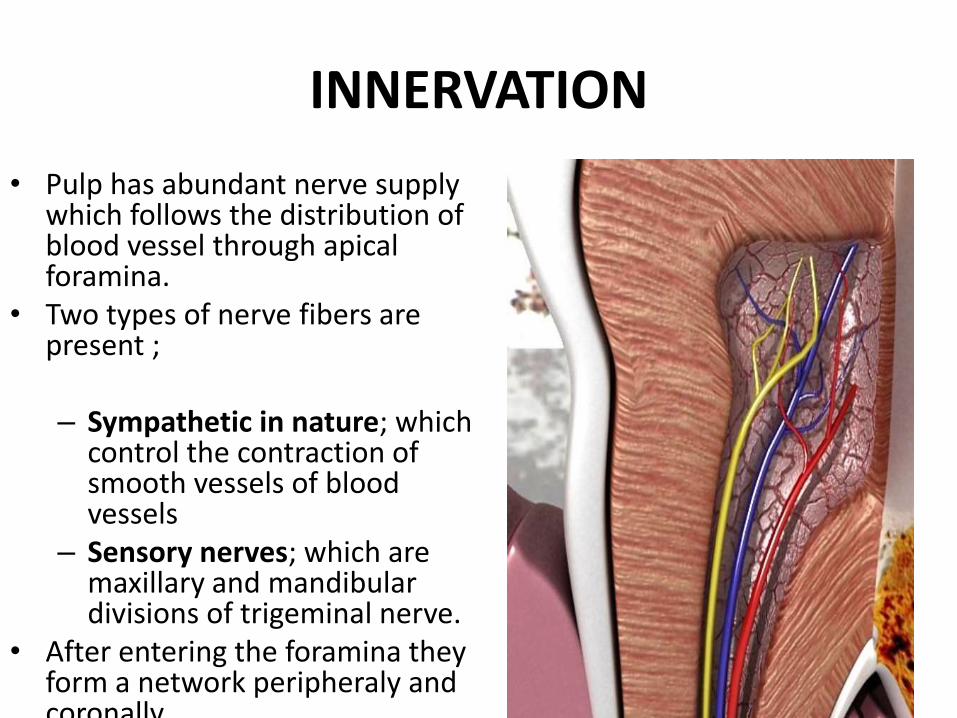
• Pulp has abundant nerve supply which follows the distribution of blood vessel through apical foramina.
• Two types of nerve fibers are present ;
– Sympathetic in nature; which control the contraction of smooth vessels of blood vessels
– Sensory nerves; which are maxillary and mandibulardivisions of trigeminal nerve.
• After entering the foramina they form a network peripheraly and coronally.
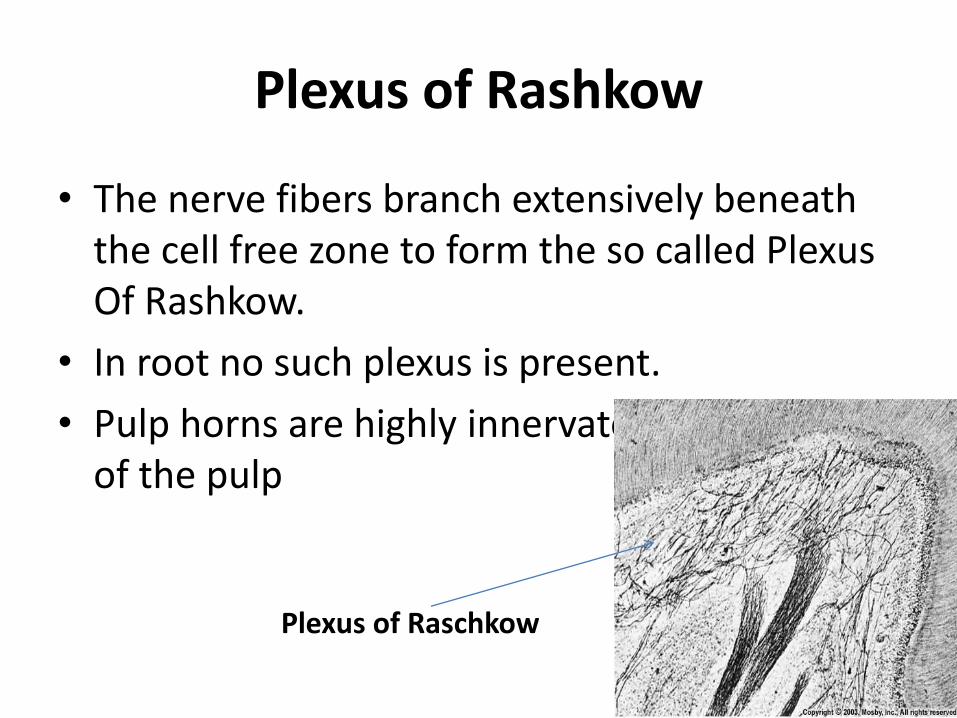
Plexus of Rashkow
• The nerve fibers branch extensively beneath the cell free zone to form the so called Plexus Of Rashkow.
• In root no such plexus is present.
• Pulp horns are highly innervated than the rest of the pulp
Plexus of Raschkow
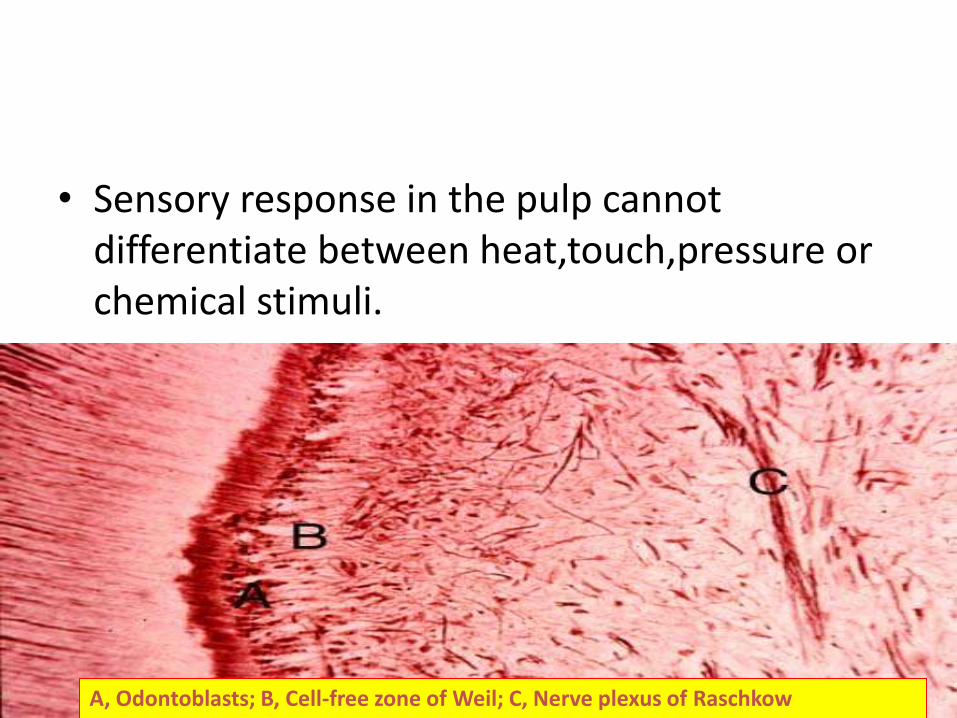
• Sensory response in the pulp cannot differentiate between heat,touch,pressure or chemical stimuli.
• Pulp has only pain receptors.
A, Odontoblasts; B, Cell-free zone of Weil; C, Nerve plexus of Raschkow

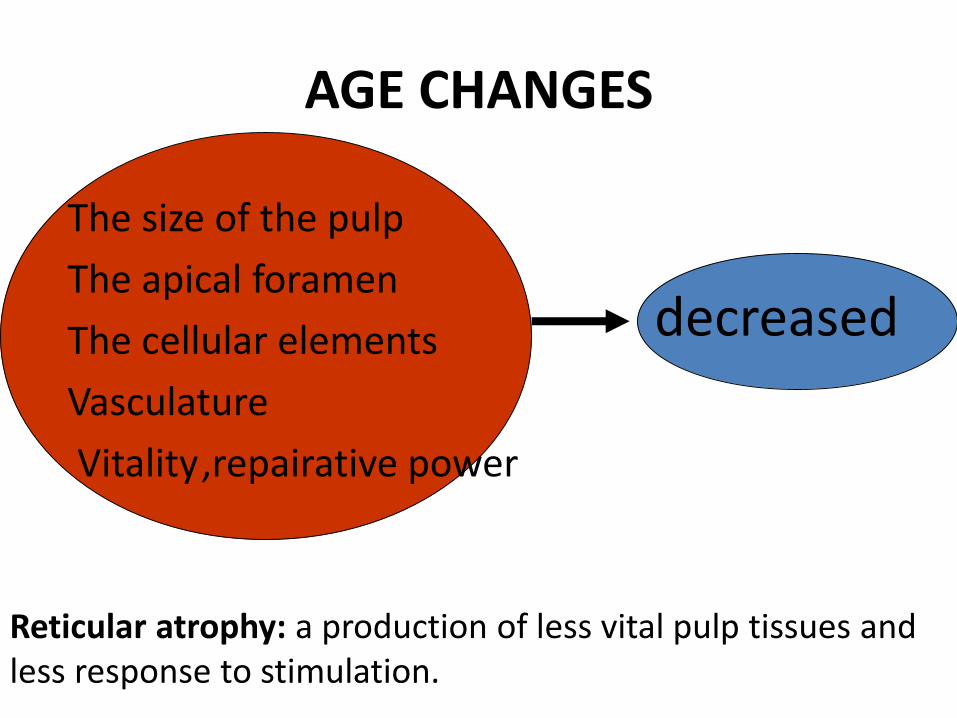
The size of the pulp
The apical foramen
The cellular elements
Vasculature
Vitality,repairative power
decreased
AGE CHANGES
Reticular atrophy: a production of less vital pulp tissues andless response to stimulation.
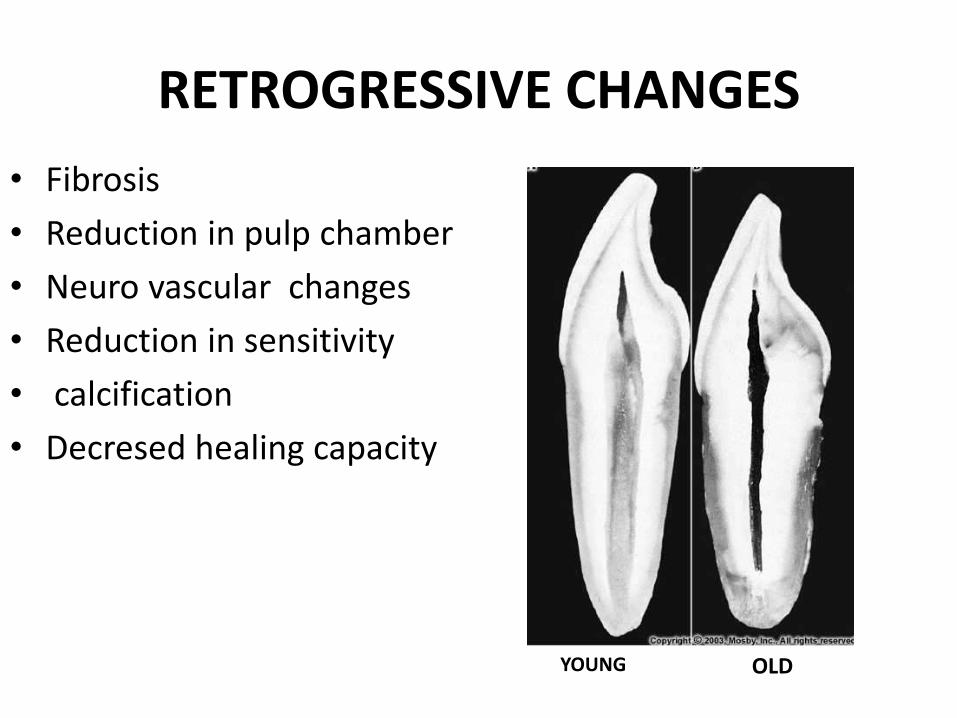
RETROGRESSIVE CHANGES
• Fibrosis
• Reduction in pulp chamber
• Neuro vascular changes
• Reduction in sensitivity
• calcification
• Decresed healing capacity
YOUNG OLD
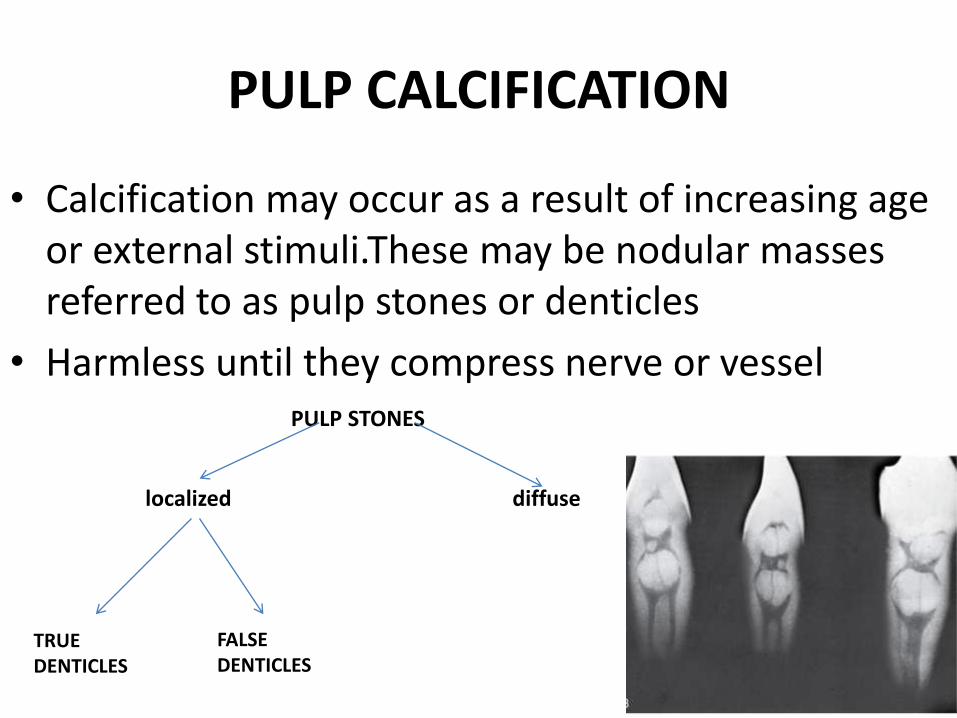
PULP CALCIFICATION
• Calcification may occur as a result of increasing age or external stimuli.These may be nodular masses referred to as pulp stones or denticles
• Harmless until they compress nerve or vesselPULP STONES
localized diffuse
TRUE DENTICLES
FALSE DENTICLES
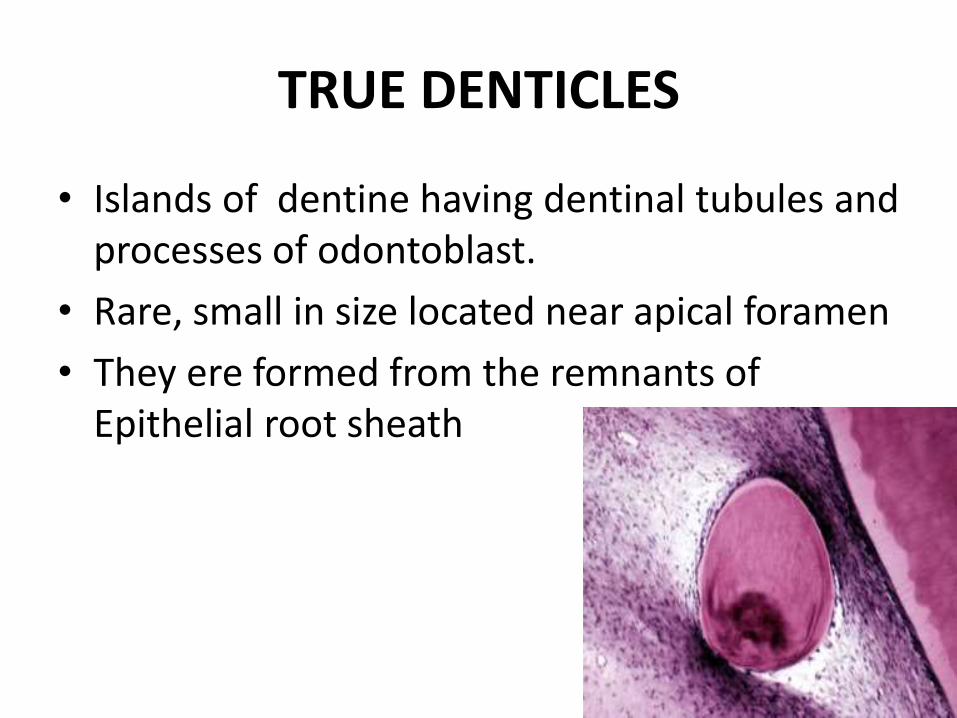
TRUE DENTICLES
• Islands of dentine having dentinal tubules and processes of odontoblast.
• Rare, small in size located near apical foramen
• They ere formed from the remnants of Epithelial root sheath
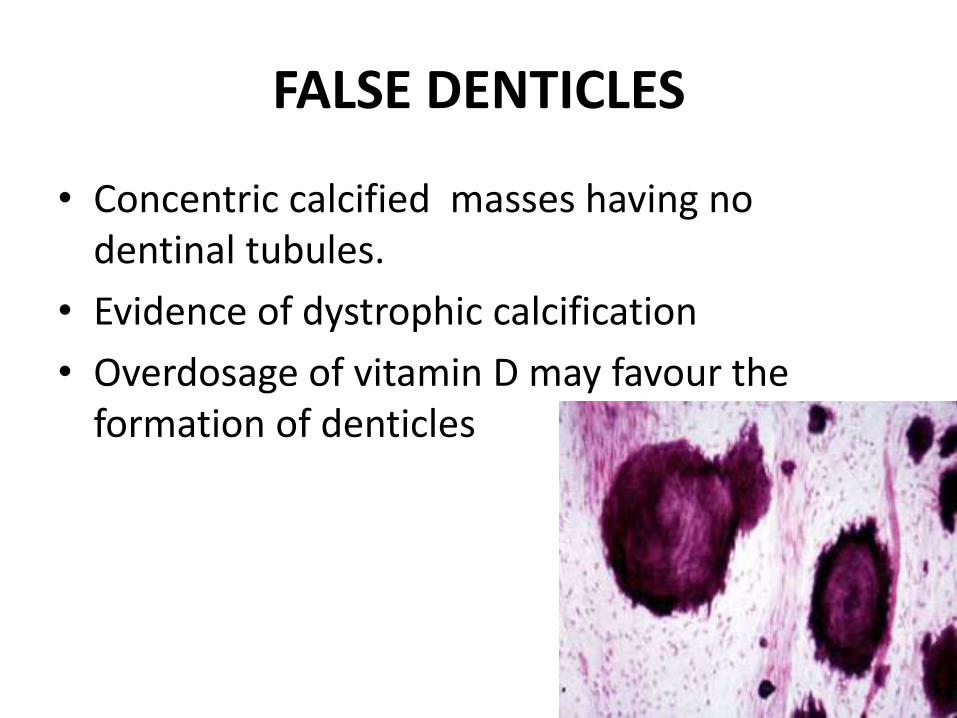
FALSE DENTICLES
• Concentric calcified masses having no dentinal tubules.
• Evidence of dystrophic calcification
• Overdosage of vitamin D may favour the formation of denticles
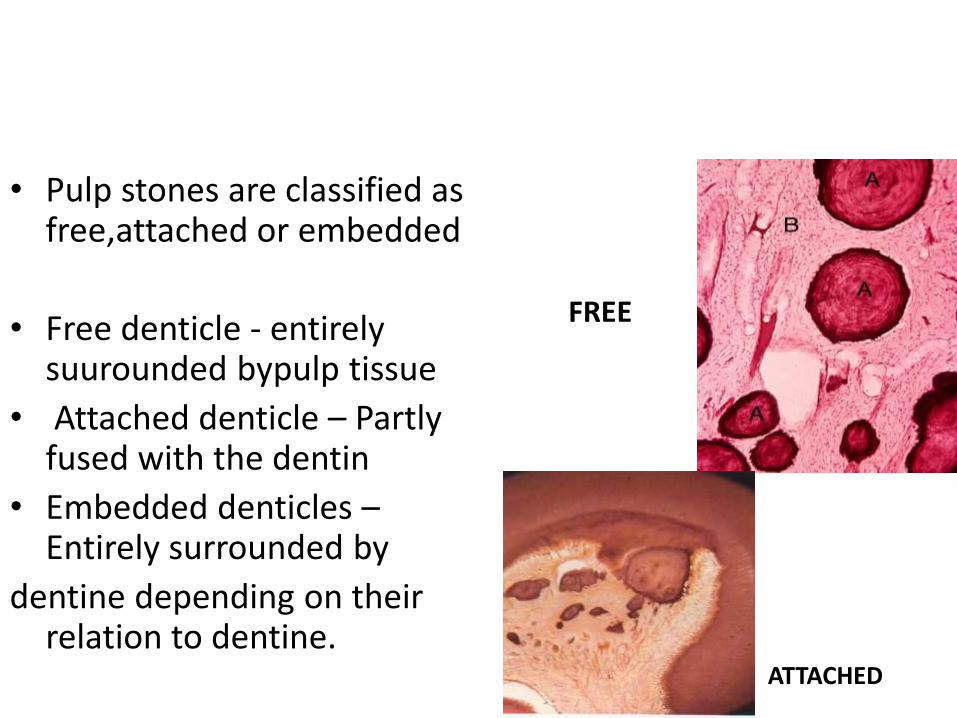
• Pulp stones are classified as free,attached or embedded
• Free denticle - entirely suurounded bypulp tissue
• Attached denticle – Partly fused with the dentin
• Embedded denticles –Entirely surrounded by
dentine depending on their relation to dentine.
FREE
ATTACHED
CLINICAL CONSIDERATIONS
• PULPITIS :
• Refers to the inflammation of dental pulp within a
tooth
CAUSES:
Bacterial infection in dental caries.
Tooth fracture
Chemical irritants
Traumatic exposure
• REVERSIBLE PULPITIS ;
Condition affecting tooth accompained by short lived pain
Heals with time by itself
• IRREVESIBLE PULPITIS ; Term referring to a dead pulp or necrosed pulp.accopanied by severe pain
Requires endodontic treatment.
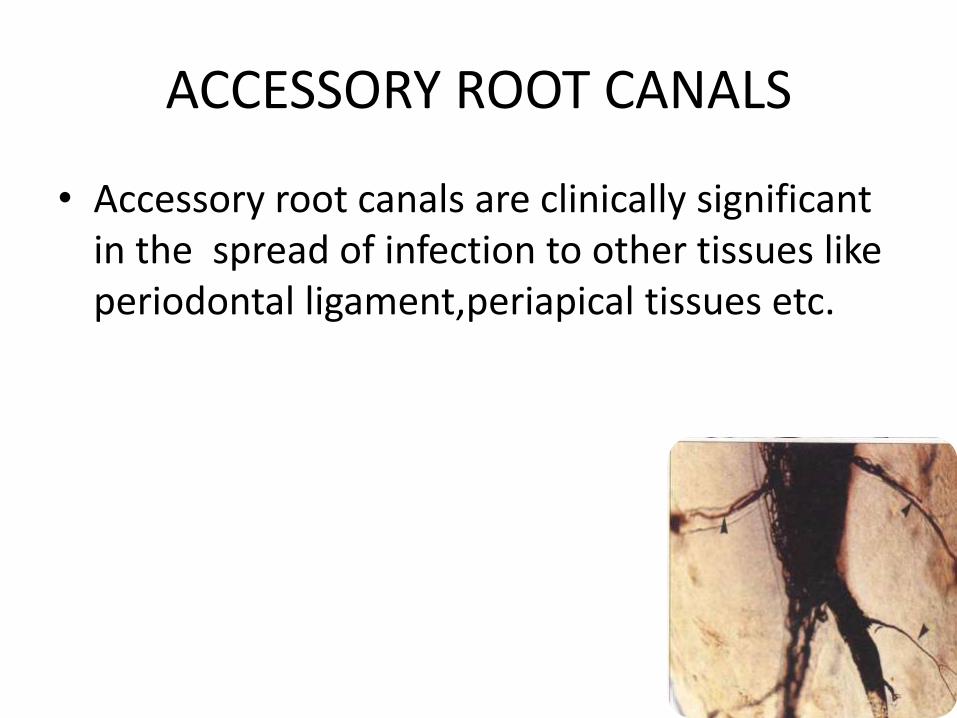
ACCESSORY ROOT CANALS
• Accessory root canals are clinically significant in the spread of infection to other tissues like periodontal ligament,periapical tissues etc.
AERODONTALGIA
• Aerodontalgia got its name during WW II when some pilots experienced toothaches while flying high in unpressurized airplanes.
• They ultimately found that this was caused by a decrease in atmospheric pressure as the planes ascended to high altitudes.
• Any tiny pocket of air trapped during RCT or filling resuts in air entrapment.
DURING OPERATIVE PRECEDURES
• Shape of the pulp chamber and its extensions into
the cusps pulpal horns is important.
• Wide pulp chamber into tooth of young person
will make a deep cavity preparation hazardous
• The pulpal horns project high into the cusps in younger ages exposure of pulp can occur
• If opening a pulp chamber for treatment its size
and variation in shape must be taken into
consideration
FACTORS TO BE CONSIDERED DURING
ENTODONTIC TREATMENT
• Age advance , the pulp chamber becomes
smaller difficult to locate the root canals.
• Shape of the apical foramen and its location
may play an important part in treatment of root
canals.
• Accessory canals, and multiple canals are rarely
seen in roentgenograms.
• Dehydration causes pulpal damage operative
procedures producing this condition should be
avoided.
EFFECT OF DENTAL MATERIALS ON PULP
• Filling material contain harmful chemicals
• Silicate cement - acid
• Composites – monomer
• GIC – Well tolerated by pulp
• Calcium hydroxide – dentin bridge formation.
CONCLUSION
• THE PRESEVATION OF A HEALTHY PULP DURING
OPERATIVE PROCEDURES AND SUCCESSFUL
MANAGEMENT IN CASES OF DISEASES ARE TWO
OF MOST IMPORTANT CHALLENGE TO THE
CLINICAL DENTIST.
OFFICIAL SIGN OF DENTISTRY