
December 2001 OI Guidelines 11/28/01
2001 USPHS/IDSA Guidelines for the Prevention of
Opportunistic Infections in Persons Infected With Human
Immunodeficiency Virus
Module 1:
Prophylaxis Core
A Training Slide Set Prepared by the AETC National Resource Center

December 2001 OI Guidelines 11/28/01
Disclaimer
These slides were developed using the most recent treatment guideline information at the time of production. However, in the rapidly changing field of HIV care this information could become out of date quickly. The user is encouraged to compare the date of this slide set with the date of the most recent guidelines. Also, it is intended that these slides be used, as prepared, without changes in either content or attribution. Users are asked to honor this intent.
AETC National Resource Center

December 2001 OI Guidelines 11/28/01
Summary of OIs for Which Prevention Is Recommended
Primary ProphylaxisP. carinii*Tuberculosis*T. gondii*M. avium*Varicella zoster*S. pneumoniae†
Hepatitis A & B†
Influenza †
Secondary ProphylaxisP. carinii*T. gondii*M. avium*Cryptococcosis*Histoplasmosis*Coccidioidomycosis*Cytomegalovirus*Salmonella bacteremia
* Standard of care† Generally recommended

December 2001 OI Guidelines 11/28/01
OIs for Which Prevention Is Not Routinely Indicated
Primary Prophylaxis
Bacteria (Neutropenia) †
Cryptococcosis†
Histoplasmosis†
Cytomegalovirus †
Secondary Prophylaxis
Herpes simplex virus §
Candida §
† Evidence for Efficacy but Not Routinely Indicated
§ Recommended only if subsequent episodes are frequent or severe
December 2001 OI Guidelines 11/28/01
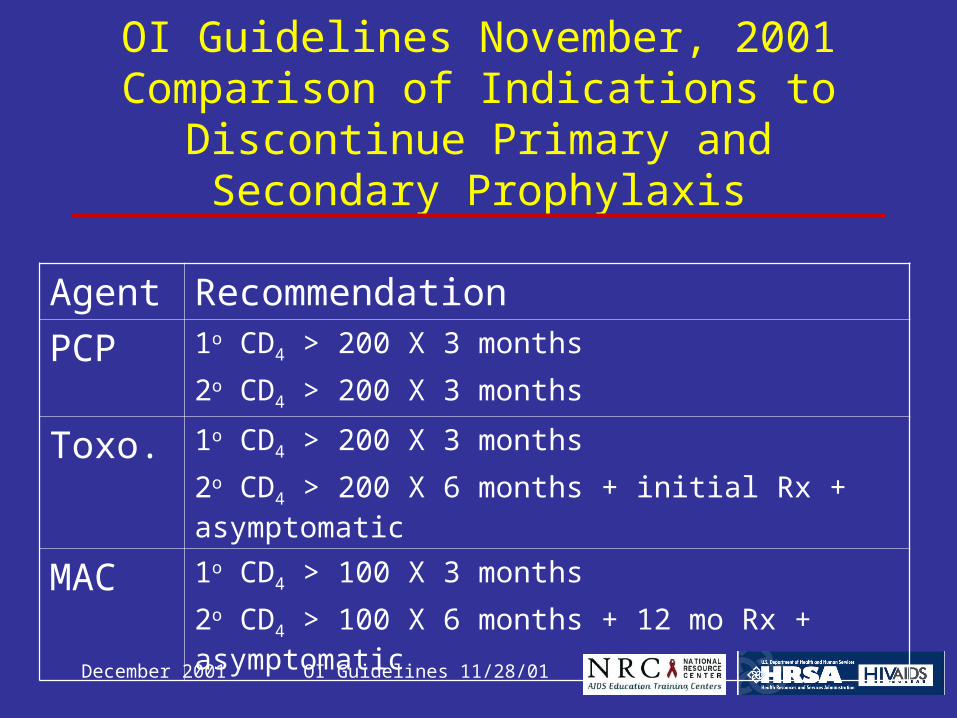
OI Guidelines November, 2001Comparison of Indications to Discontinue
Primary and Secondary Prophylaxis
Agent Recommendation
PCP 1o CD4 > 200 X 3 months
2o CD4 > 200 X 3 months
Toxo. 1o CD4 > 200 X 3 months
2o CD4 > 200 X 6 months + initial Rx + asymptomatic
MAC 1o CD4 > 100 X 3 months
2o CD4 > 100 X 6 months + 12 mo Rx + asymptomatic

December 2001 OI Guidelines 11/28/01
OI Guidelines November, 2001
OIs for Which Primary and Secondary Prophylaxis Is Recommended

December 2001 OI Guidelines 11/28/01
P. carinii Pneumonia
Primary ProphylaxisIndication: CD4 < 200 or thrush
When stop: CD > 200 for > 3 moWhen restart: CD4 falls to < 200
Secondary prophylaxisSame as primary

December 2001 OI Guidelines 11/28/01
P. carinii Pneumonia
Preferred Regimens:• TMP-SMX DS 1/d*• TMP-SMX SS 1/dAlternative Regimens:• Dapsone 100 mg/d• Dapsone 50 mg/d + Pyrim 50 mg/wk + Leucovorin 25
mg /wk*• Dapsone 200 mg/wk + Pyrim 75 mg/wk + Leuco 25 mg/wk*• Atovaquone 1500 mg/d*• Aerosol pentamidine 300 mg/mo• TMP-SMX DS 3/wk
* Adequate for toxoplasmosis (CD4 <100 + pos serology)

December 2001 OI Guidelines 11/28/01
Toxoplasmosis: Primary Prophylaxis
Indication: Pos lgG Toxo + CD4 < 100
When to stop: CD4 > 200 X 3 mo
When to restart: CD4 falls to < 100-200

December 2001 OI Guidelines 11/28/01
Toxoplasmosis: Primary Prophylaxis
Preferred Regimen:
TMP – SMX DS 1/d po
Alternative Regimen:
• TMP – SMX SS 1/d
• Dapsone 50 mg/d + Pyrim 50 mg/wk + Leuco 25mg /wk
• Dapsone 200 mg/wk + Pyrim 75 mg/wk + Leuco 25/wk
• Atovaquone 1500 mg/d + Pyrim 25 mg/d + leuco10 mg/d

December 2001 OI Guidelines 11/28/01
Toxoplasmosis:Secondary Prophylaxis
Indication:Completion of therapy for toxoplasmosis unless immune reconstitution occurs with HAART.
When to stop: CD4 > 200 X 6 mo + completed initial treatment + asymptomatic
When to restart: CD4 falls to < 200

December 2001 OI Guidelines 11/28/01
Toxoplasmosis:Secondary Prophylaxis
Preferred Regimen :• Sulfadiazine 500-1000 mg qid + Pyrimethamine
25-50 mg/d + Leucovorin 10-25 mg/d
Alternative Regimen : • Clindamycin 300-450 mg q 6-8 hr +
Pyrimethamine 25-50 mg/d+ leucovorin10-25 mg/d
• Atovaquone 750 mg q 6-12 hr + Pyrimethamine 25 mg/d + leucovorin 10 mg/d

December 2001 OI Guidelines 11/28/01
MAC:Primary Prophylaxis
Indication: CD4 < 50
When to stop: CD4 > 100 for > 3 month
When to restart: CD4 falls to < 50-100

December 2001 OI Guidelines 11/28/01
MAC:Primary Prophylaxis
Preferred Regimen:
• Azithromycin 1200 mg/wk or
• Clarithromycin 500 mg bid
Alternative Regimen:
• Rifabutin* 300 mg/d or
• Azithromycin 1200 mg/wk + Rifabutin* 300 mg/d
* Dose adjusted for concurrent PI or NNRTI

December 2001 OI Guidelines 11/28/01
MAC: Secondary Prophylaxis
Indication: Hx MAC
When to stop: CD4 > 100 X > 6 mo and Rx 12 mo and asymptomatic
When to restart: CD4 falls to < 100

December 2001 OI Guidelines 11/28/01
MAC: Secondary Prophylaxis
Preferred Regimen:
Clarithromycin 500 mg bid + Ethambutol 15 mg/kg/d ± Rifabutin* † 300 mg/d
Alternative Regimen:
Azithromycin 500 mg/d + Ethambutol 15 mg/kg/d ± Rifabutin* 300 mg/d
* Dose adjusted for concurrent PI..NNRTI† Rifabutin reduces levels of clarithromycin by 50%

December 2001 OI Guidelines 11/28/01
OI Guidelines November, 2001
OIs for Which Only Primary Prevention Is Generally Recommended

December 2001 OI Guidelines 11/28/01
Tuberculosis: Latent Infection
Screening: (5-TU) purified protein derivative
(PPD) by the Mantoux method • When HIV infection is first recognized.• Annual test if TST negative on initial evaluation
and continued risk.• Routine evaluation for anergy is not
recommended.

December 2001 OI Guidelines 11/28/01
Tuberculosis: Treatment of Latent Infection
Indications: • PPD > 5 mm induration at 48-72h• Hx PPD + no Rx• TB contact (D/C if PPD neg at 12 wks)
All PPD positives should be evaluated for active TB including chest x-ray.

December 2001 OI Guidelines 11/28/01
Treatment of Latent TB Infection: CDC/ATS Guidelines, August 2001*
Recommended Regimens:
• No HIV: INH X 9 mo.• HIV: INH X 9 mo. (if compliance assured)
RIF-PZA X 2 mo.
Alternative: RIF/RBT alone X 4 mo.
* Am J Resp Crit Care 2001; 164:1319

December 2001 OI Guidelines 11/28/01
Treatment of Latent TB Infection: CDC/ATS Guidelines, August 2001*
Rationale for RIF-PZA in HIV Co-infection:• Compliance & risk of active disease.• Risk of ALT greater with INH vs RIF-PZA in
HIV co-infected.• 21 reported cases severe RIF-PZA
hepatotoxicity, none had HIV.• Well tolerated in HIV co-infected patients.
* Am J Resp Crit Care 2001; 164:1319
December 2001 OI Guidelines 11/28/01
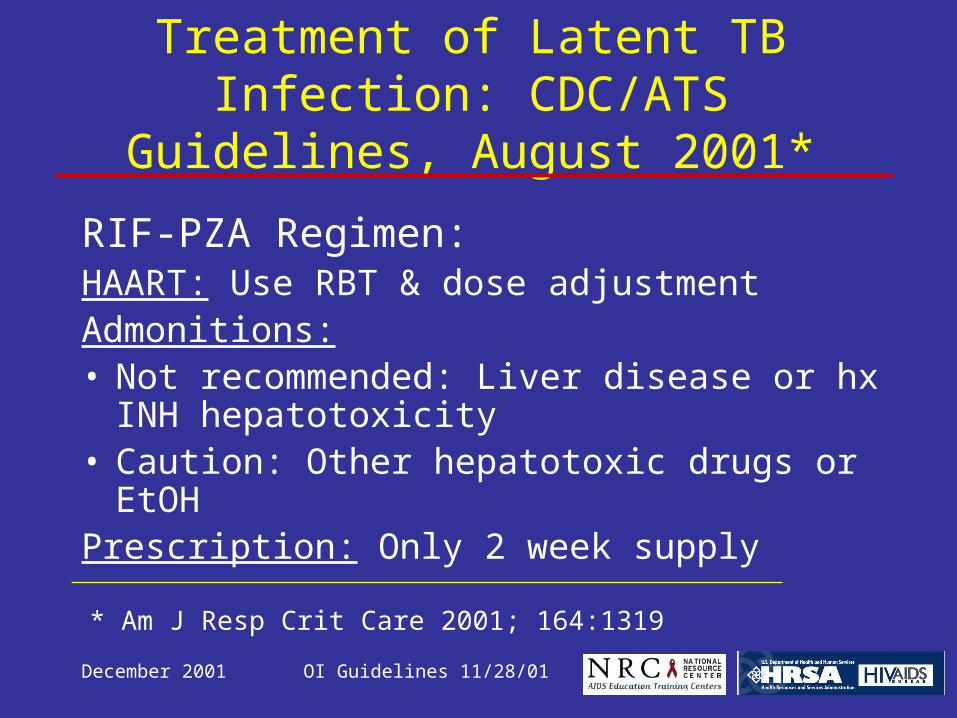
Treatment of Latent TB Infection: CDC/ATS Guidelines, August 2001*
RIF-PZA Regimen:HAART: Use RBT & dose adjustmentAdmonitions:• Not recommended: Liver disease or hx INH
hepatotoxicity• Caution: Other hepatotoxic drugs or EtOHPrescription: Only 2 week supply
* Am J Resp Crit Care 2001; 164:1319

December 2001 OI Guidelines 11/28/01
Treatment of Latent TB Infection: CDC/ATS Guidelines, August 2001*
RIF-PZA Regimen:Monitoring:• Clinical: at 2,4,6,& 8 weeks.• Lab: ALT & Bili at baseline, 2,4, & 6 weeks.Discontinue: 1) Sx + ALT
2) ALT > 5X ULN, or 3) Bili.
* Am J Resp Crit Care 2001; 164:1319

December 2001 OI Guidelines 11/28/01
Tuberculosis: Treatment of Latent Infection - Regimens
HAART/No HAART:INH 300 mg/d + pyridoxine 50 mg/d X 9 mo (270 doses) †
INH 900 mg + pyridoxine 100 mg 2 X wk X 9 months (76 doses †
† Assuming completion of treatment can be assured.

December 2001 OI Guidelines 11/28/01
Tuberculosis: Treatment of Latent Infection - Regimens
HAART:
Rifabutin* daily X 4 months
Rifabutin* + Pyrazinamide 20 mg/kg/d X 2 months (60 doses)
No HAART:
Rifampin 600 mg/d X 4 months
Rifampin 600 mg/d + Pyrazinamide 20 mg/kg/d X 2 months (60 doses)
* Dose adjusted for PI or NNRTI

December 2001 OI Guidelines 11/28/01
Tuberculosis: Treatment of
Latent Infection
When to restart: patients previously treated for TB infection or TB disease do not require retreatment based upon diminished immune function alone. Patients with known exposure or suspected of acquiring TB infection may need retreatment. In these instances consultation with experts is strongly recommended.

December 2001 OI Guidelines 11/28/01
Rifabutin Dose Modifications With ART Agents
PI/NNRTI
Rifabutin
Daily 2-3 X / Wk
IDV 1000 mg q 8h 150 300
NFV 1250 mg bid 150 300
APV 1200 mg bid 150 300
RTV/SQV 400/400 mg - 150
LPV/RTV 400/100 - 150 qod
NVP 200 mg bid 300 -
EFV 600 hs 450 600

December 2001 OI Guidelines 11/28/01
Tuberculosis Prophylaxis Therapeutic Monitoring
Drug Clinical Laboratory Intervention
INH Review monthly for sx hepatitis
LFTs at baseline & 3 mo
D/C if ALT > 5 x ULN
RIF/
PZA
Clinical evaluation at wk 2, 4, 6 & 8
ALT & Bili at 2, 4 & 6 wks or with sx
D/C if:•sx + abn ALT/ AST, or
•ALT/AST > 5 x ULN, or Bilirubin
December 2001 OI Guidelines 11/28/01
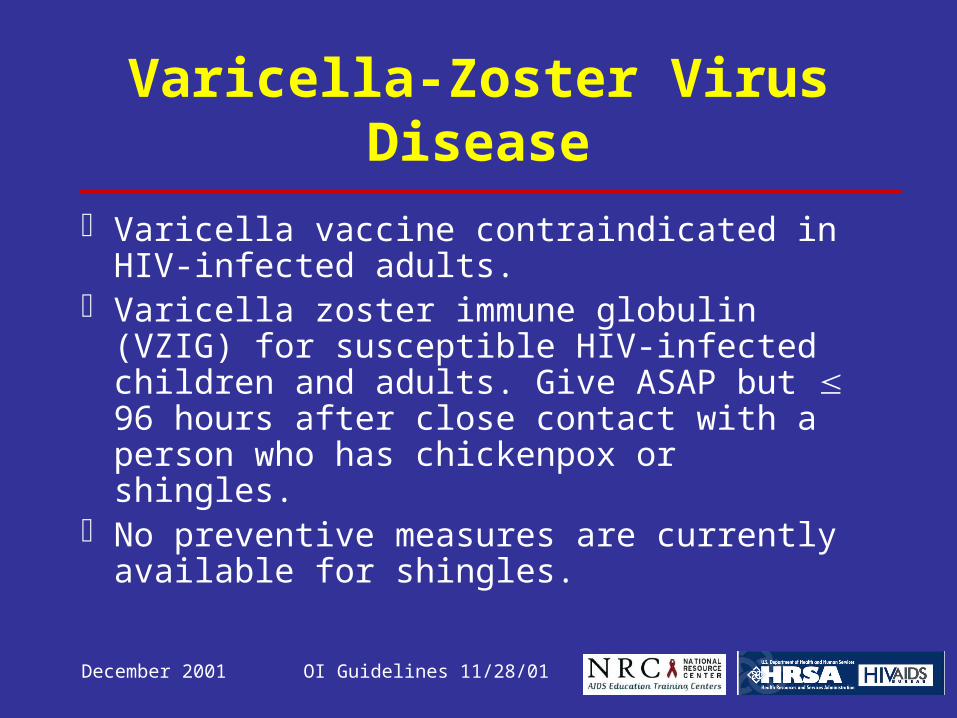
Varicella-Zoster Virus Disease
Varicella vaccine contraindicated in HIV-infected adults.
Varicella zoster immune globulin (VZIG) for susceptible HIV-infected children and adults. Give ASAP but 96 hours after close contact with a person who has chickenpox or shingles.
No preventive measures are currently available for shingles.

December 2001 OI Guidelines 11/28/01
VACCINES: ROUTINE USE
Agent Indication
Hepatitis B Anti-HBc neg
Hepatitis A Risk * + neg anti-HAV
S. pneumoniae CD4 > 200
Influenza Annually, Oct – Nov
* Risk = IDU, MSM, hemophilia, chronic HBV or HCV

December 2001 OI Guidelines 11/28/01
VACCINES: OTHER
Give if indicated:
Cholera, Japanese encephalitis, Lyme disease, Tetanus-diptheria, Typhoid inactivated (Typhim V1)

December 2001 OI Guidelines 11/28/01
VACCINES: OTHER
Contraindicated (live virus):
Varicella, Yellow Fever, Typhoid live (Ty21a), Measles, Vaccinia

December 2001 OI Guidelines 11/28/01
OI Guidelines November, 2001
OIs for Which Only Secondary Prevention Is Generally Recommended

December 2001 OI Guidelines 11/28/01
Cytomegalovirus Disease
Chronic maintenance therapy following inductionPreferred Regimen:• Ganciclovir IV or PO• Foscarnet IV• Ganciclovir implant + PO (for retinitis)Alternative Regimen:• Cidofovir IV + probenecid PO• Fomivirsen injection in vitreous• Valganciclovir PO
When to stop: CD4 >100-150 X 6 mo + no active disease + negative ophthal exam.
When to restart: CD4 < 100-150
December 2001 OI Guidelines 11/28/01
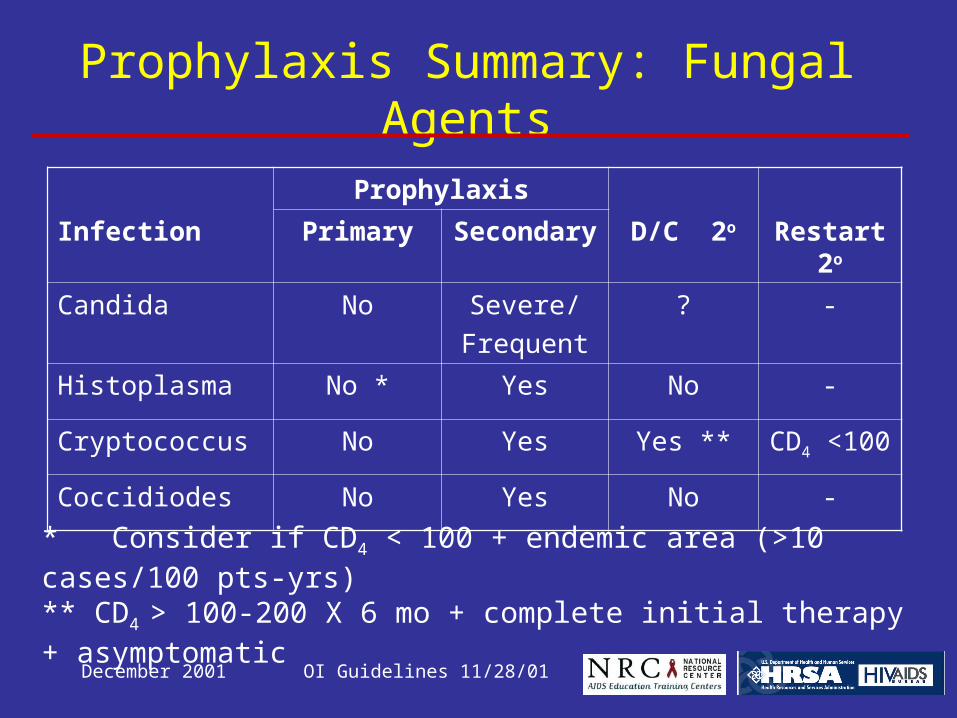
* Consider if CD4 < 100 + endemic area (>10 cases/100 pts-yrs)** CD4 > 100-200 X 6 mo + complete initial therapy + asymptomatic
Prophylaxis Summary: Fungal Agents
Prophylaxis
Infection Primary Secondary D/C 2o Restart 2o
Candida No Severe/
Frequent
? -
Histoplasma No * Yes No -
Cryptococcus No Yes Yes ** CD4 <100
Coccidiodes No Yes No -

December 2001 OI Guidelines 11/28/01
Cryptococcosis
Chronic Maintenance Therapy
Regimen: Preferred: Fluconazole (AI). Alternate: Amphotericin B, itraconazole
When to stop: completed initial treatment + asymptomatic + CD4 >100 - 200 X 6 mo on HAART
When to restart: CD4 falls to < 100 - 200
December 2001 OI Guidelines 11/28/01
Histoplasmosis
Lifelong Suppressive Therapy
Indication: Completion of therapy for histoplasmosis
Agents: itraconazole (200 mg twice a day).When to stop: Insufficient data (? CD4+ >100
cells/µL)

December 2001 OI Guidelines 11/28/01
Coccidioidomycosis
Lifelong Suppressive Therapy
Indication: Completion of therapy for coccidioidomycosis
Regimen: fluconazole PO or itraconazole. Patients with meningeal disease require consultation with an expert.
When to stop: Insufficient data (? CD4+ >100 cells/µL )

December 2001 OI Guidelines 11/28/01
Salmonella
Prevention of Reccurrence:Indication: Salmonella septicemia Regimen: Preferred: Fluoroquinolones
(ciprofloxacin) for susceptible organisms.Other Management: Household contacts should
be evaluated for carriage so that hygienic measures and/or antimicrobial therapy can be instituted and recurrent transmission prevented. (Optional)

December 2001 OI Guidelines 11/28/01
OI Guidelines November, 2001
Infections Requiring Other Management Strategies
December 2001 OI Guidelines 11/28/01
Hepatitis C Virus Infection
Prevention of Disease• Recommend screening-if positive: do RIBA/ HCV PCR, then:
– Avoid excessive amounts of alcohol – Vaccinate against hepatitis A – Evaluated for chronic liver disease and for the
possible need for treatment. – Monitor liver enzymes on patients on HAART.– HAART should not be routinely withheld from
patients co-infected with HIV and HCV

December 2001 OI Guidelines 11/28/01
Human Papillomavirus Infection
Prevention of DiseaseGenital Epithelial Cancers in HIV-infected Women
Pelvic exam + PAP X 2 in first year after HIV Dx. If normal, repeat PAP annually If abnormal, follow Interim Guidelines for
Management of Abnormal Cervical Cytology (NCI)
Prevention of Recurrence Careful follow-up and monitoring after treatment No specific therapy recommended.
December 2001 OI Guidelines 11/28/01
OI Guidelines November, 2001
Cost Considerations

December 2001 OI Guidelines 11/28/01
Drug Costs Of PCP Prophylaxis
* Administration costs need to be considered.
Agent Dose Annual Cost
TMP – SMX 1 DS/d $ 135
Dapsone 100 mg/d $ 72
Aerosolized pentamidine
300 mg/mo $ 1,185 *
Atovaquone 1500 mg/d $ 11,627
December 2001 OI Guidelines 11/28/01
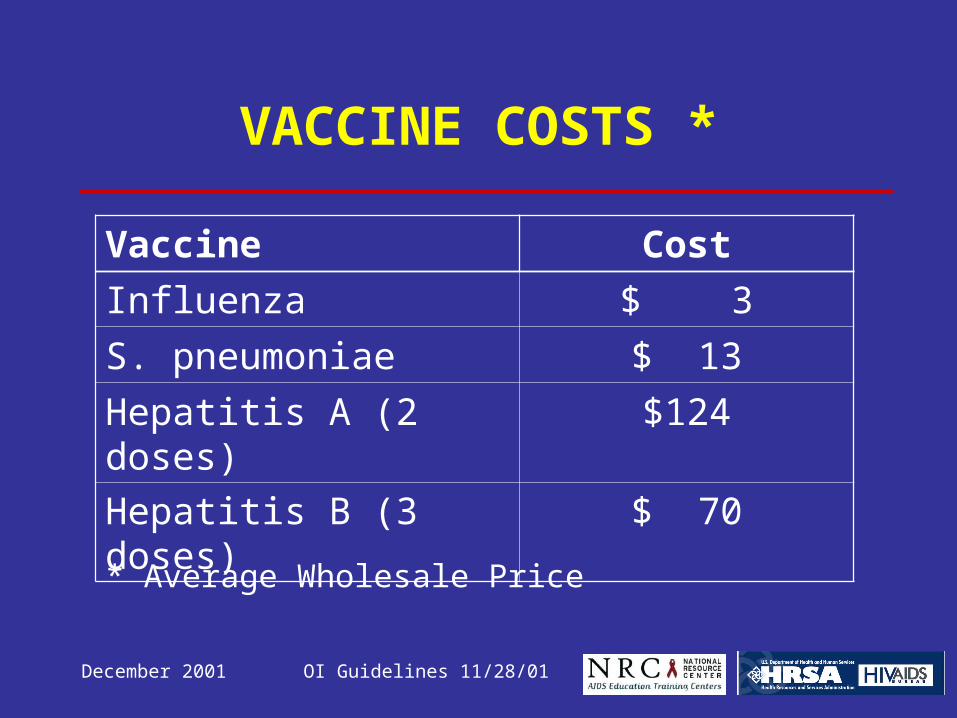
VACCINE COSTS *
* Average Wholesale Price
Vaccine Cost
Influenza $ 3
S. pneumoniae $ 13
Hepatitis A (2 doses) $124
Hepatitis B (3 doses) $ 70

December 2001 OI Guidelines 11/28/01
Drug Costs Exceeding $10,000/yr*
* Average Wholesale Price
Agent Dose Annual CostAtovaquone 1500 mg/d $11,627
Valganciclovir 900 mg/d $21,582
IV ganciclovir 5 mg/kg/d $13,093
IV foscarnet 90 mg/kg/d $27,770
Cidofovir 375 mg qow $20,904
Fomivirsen 1 vial q 4 w $12,000

December 2001 OI Guidelines 11/28/01
For Additional Information:
Sources of Complete Guidelines:– AETC Resource Center: www.aids-etc.org– AIDS Treatment Information Service:
www.hivatis.org

December 2001 OI Guidelines 11/28/01
OI Guideline SlidesDecember 2001
Author: John G. Bartlett, M.D.
Editor: Richard W. Dunning, M.H.S.
Reviewers:– Renslow Sherer, M.D.– Caroline Teter, PAC, M.P.H.







