Download - Debonding procedures in orthodontics

PRESENTED BY:
FASAHAT AHMED BUTT
ROLL# 36
GROUP: C
DEBONDING PROCEDURES
IN ORTHODONTICS

OBJECTIVE
To remove the attachment and all the
adhesive resin from the tooth and restore
the surface as closely as possible to its
pretreatment condition without inducing
iatrogenic damage

PROCEDURES
Bracket removal
Steel bracket
Ceramic bracket
Removal of residual adhesive

Steel bracketsCeramic
brackets
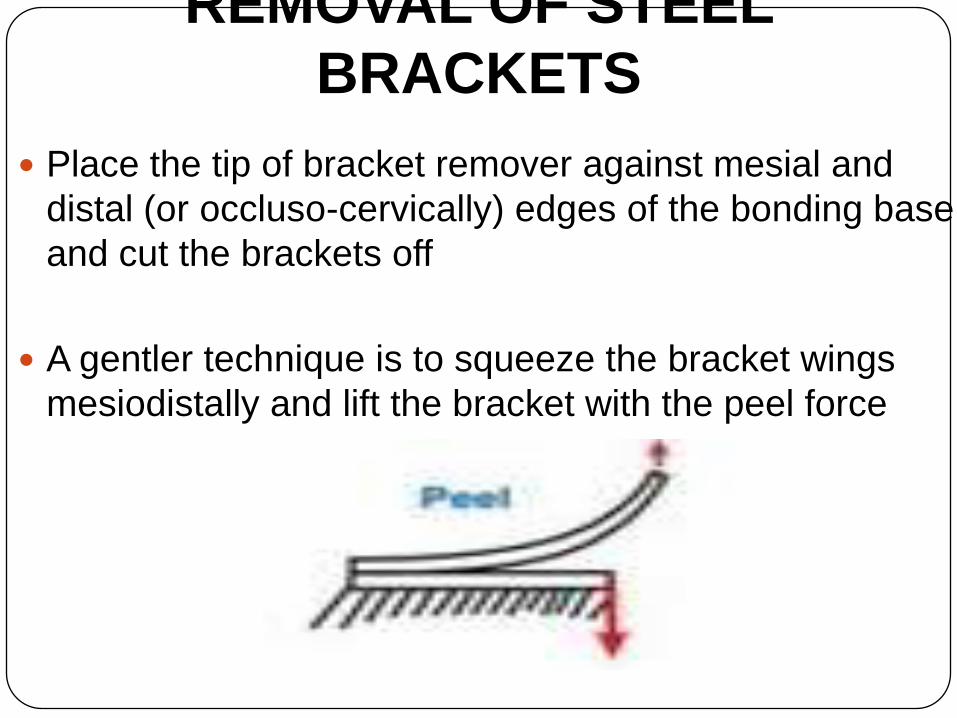
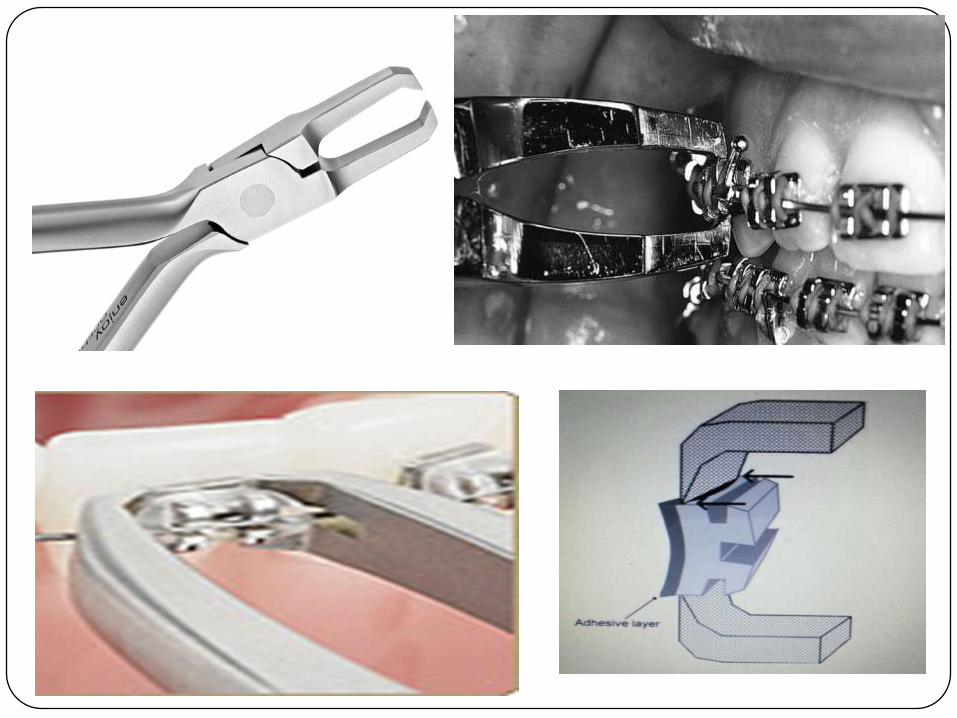
REMOVAL OF STEEL
BRACKETS
Place the tip of bracket remover against mesial and
distal (or occluso-cervically) edges of the bonding base
and cut the brackets off
A gentler technique is to squeeze the bracket wings
mesiodistally and lift the bracket with the peel force

REMOVAL OF CERAMIC
BRACKETS With the introduction of ceramic brackets, a new
concern over enamel fracture and loss from
debonding has arisen.
Because of differences in bracket chemistry and
bonding mechanism, various ceramic brackets
behave differently on debonding
More recent ceramic brackets have
mechanical lock base and vertical slot
that will split the bracket by squeezing
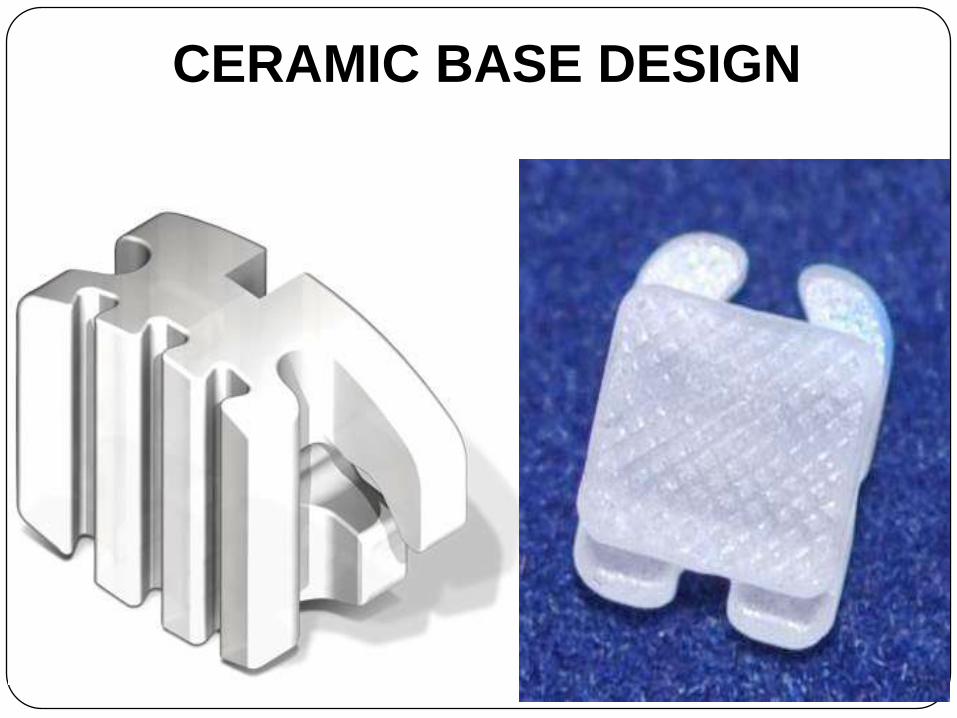
CERAMIC BASE DESIGN

MEANS OF REMOVAL
Mechanical
Thermal debonding
Lasers
Ultrasonic

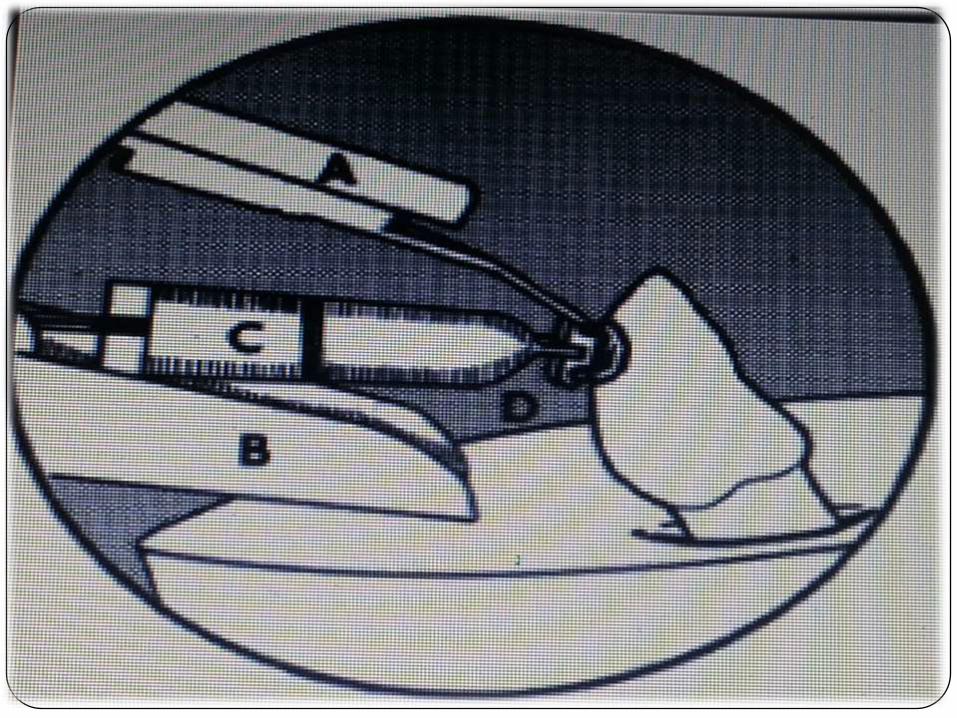
MECHANICAL

ELECTROTHERMAL

Takla and Shivapuja (1995) study in which 30 teeth were schduled for orthodontic extractions
15 extracted 24 days after ETD
7 extracted 28-32 days after ETD
8 were control teeth and debonded by conventional method, with pliers
In control group pulp was normal
Significant hyperemia in teeth extracted after 24 day
In case of teeth extracted after 28-32 day variation was seen from complete recovery to persistent inflammation
Jost-Brinkmann et al (1997) did an in vivo study in which 12 human premolars scheduled for extraction were bonded with ceramic brackets which were subsequently debonded using ETD. After 4 weeks, teeth were extracted and histologically examined . No signs of pulpal inflammation were seen

LASERS
The use of laser eliminates problems like enamel tear
outs, bracket failures and pain.
Lasers decreases debonding force and less time
consuming.
Strobl et al (1993) Removal of ceramic brackets from
enamel surface by means of laser heating was investigated
with the use of C02 and YAG laser
Polycrystalline alumina
Monocrystalline alumina
Laser-aided debonding significantly reduced debonding
force by thermal softening of adhesive resin.
In 69-75% incident light reached enamel surface when
Nd:YAG laser was used which has the potential to cause
pain or damage to tooth surface

ULTRASONIC

DEBONDIN
G
METHODS
ADVANTAGES DISADVANTAGES
Mechanical Low cost Risk of enamel fracture
Electrothermal o Reduced incidence of
bracket failure
o Short debonding time
Potential for pulpal damage
and mucosal burn
Laser Experimental, but
increased precision
regarding time and
amount of heat
application
High cost of equipment
Ultrasonic o Potentially reduced
enamel damage
o Reduced likelihood of
bracket failure
o Adhesive removal after
debonding may be
achieved with same
o Increased debonding time.
o Extensive wear of
expensive ultrasonic tip
o Some force required
o Potential for soft tissue
injury
ADHESIVE REMNANT INDEX
(ARI)
Used to evaluate the amount of adhesive left on the tooth
after debonding
SCORE 0: No adhesive left on tooth
SCORE 1: Less than half of adhesive left
SCORE 2: More than half left
SCORE 3: All adhesive left on tooth with distinct with
distinct impression of bracket mesh
RESIDUAL ADHESIVE
SCOR
E 0
SCOR
E 1
SCOR
E 2
SCOR
E 3

REMOVAL OF RESIDUAL RESIN
Ultrasonic scaler
Scraping with a sharp bond removing removing plier

Burs
Tungsten carbide bur
Ultrafine diamond bur
White stone finishing bur

ENAMEL SURFACE INDEX
SCORE 0: Instrument tested left the tooth surface with its
perikymata intact
SCORE 1: Plain cut and spiral fluted tungsten carbide burs
operated at about 25,000 rpm were the only instruments that
provided the satisfactory surface appearance

SCORE 2: Fine sandpaper disks produced several
considerable and some even deeper scratches
SCORE 3: Medium sandpaper disks and a green rubber
wheel produced similar scratches, that could not be
polished away

SCORE 4: Diamond instruments were unacceptable
and even fine diamond burs produced coarse
scratches and gave a deeply marred appearance

POLISHING








